User login
Debate: Initial combination therapy for type 2 diabetes?
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Study finds big growth in advanced-practice clinicians in Medicare dermatology
A .
Researchers from the University of Texas MD Anderson Cancer Center, Houston, and the University of Pennsylvania, Philadelphia, reported in JAMA Dermatology that in 2013 APCs made up 28% of the dermatology clinician workforce. By 2020, they made up 37% of the dermatology clinicians giving care to Medicare beneficiaries.
Retrospective cohort study
APCs provided care in 15.5% of dermatology office visits in 2013 and 27.4% in 2020 (P =.02), the authors reported. “By 2020, more than one in four dermatology visits for patients with Medicare were delivered by APCs,” wrote the authors, led by Mackenzie R. Wehner, MD, MPhil, assistant professor of dermatology and health services research at MD Anderson.
“Everyone in dermatology is aware of the increasing adoption of advanced practice clinicians in the field,” Justin D. Arnold, MD, MMSc, a 3rd-year dermatology resident at the University of California, Irvine, said in an interview. “However, seeing how quickly this happening and the absolute number of these clinicians is still startling,” said Dr. Arnold, who in 2022 published a research letter in JAMA Dermatology on the impact of physician assistants in dermatology.
In that study, he and his coauthors reported that the PA workforce in dermatology was growing faster than in other specialties.
In the current study, Dr. Wehner and her colleagues identified 8,444 dermatology APCs and 14,402 physician dermatologists who provided 109.3 million Medicare office visits from 2013 to 2020. More than 80% of the procedures were performed by physicians, but APCs appeared to increasingly be taking on more of the procedural load.
Over the study period, APCs had an average annual increase of 12.6% in the number of premalignant lesion destructions performed; physicians saw an average 1.4% decline. For skin biopsies, APCs performed 11.7% more per year on average, compared with a 1.4% drop for physicians.
“This data is not surprising given most agree that skin biopsies and destruction of premalignant lesions are well within the scope of practice of APCs,” Dr. Arnold told this news organization.
The authors also reported that, while most APCs – similar to physician dermatologists – practice in metropolitan areas, they are working in other locations also. Slightly more than half of dermatology clinicians in micropolitan areas are APCs, and in rural areas, 88% of clinicians are APCs, Dr. Wehner and colleagues found.
APCs may be filling a gap in rural areas for Medicare patients, said Dr. Arnold, but, he added, “it is unclear if dermatology APCs are growing as quickly in practices that predominantly accept Medicaid and if dermatology APCs are expanding access to these populations.”
Dr. Arnold said he expected the number of APCs in dermatology to continue growing, serving commercially insured patients, as well. “There are a multitude of potential reasons for more APCs in dermatology, including difficulty recruiting dermatologists in rural communities, financial motivators, and the expansion of private equity, and the increasing acceptance of these clinicians within medicine and by patients.”
APCs can provide good-quality care if they are properly trained and supervised, said Dr. Arnold, adding that he is concerned, however, that the training and supervision is not being provided. “This study provides further evidence that dermatologists, and national dermatology organizations such as the AAD [American Academy of Dermatology], need to take a more active role in the leadership of APC training,” he said.
Dermatology, he noted, “would benefit from consensus guidelines on clinical competencies for dermatology APCs,” similar to an effort by the American College of Cardiology.
A review* published online in July noted that, compared with dermatologists, some data suggest that non-physician operators (NPOs) may have a higher rate of adverse events when performing aesthetic procedures, according to the authors of the review, led by Shelby L. Kubicki, MD, of the department of dermatology at the UTHealth Science Center in Houston. There is no mandatory reporting of complications for nonphysician providers, so the authors relied on data from cosmetic-focused practices, medical spas, and a survey by the American Society of Dermatologic Surgery of consumers and its members. More than half of the responding physicians “reported treating complications of a cosmetic procedure performed by an NPO,” the authors wrote.
They also found higher rates of burns and discoloration among patients who were treated by NPOs. The injuries occurred primarily at medical spas.
“Although NPOs may help to meet the rising demand for dermatologic procedures, care should still be taken to prioritize patient safety and outcomes above all else, including financial profits and revenues,” the authors wrote.
Dr. Wehner and her colleagues report no relevant financial relationships. Their study research was supported, in part, by a Cancer Center Support Grant and by the Cancer Prevention and Research Institute of Texas. Dr. Arnold also reports no relevant financial relationships. No author disclosures or funding information were available for the Clinics in Dermatology paper.
*Correction, 12/8/23: An earlier version of this story misstated the study design.
A .
Researchers from the University of Texas MD Anderson Cancer Center, Houston, and the University of Pennsylvania, Philadelphia, reported in JAMA Dermatology that in 2013 APCs made up 28% of the dermatology clinician workforce. By 2020, they made up 37% of the dermatology clinicians giving care to Medicare beneficiaries.
Retrospective cohort study
APCs provided care in 15.5% of dermatology office visits in 2013 and 27.4% in 2020 (P =.02), the authors reported. “By 2020, more than one in four dermatology visits for patients with Medicare were delivered by APCs,” wrote the authors, led by Mackenzie R. Wehner, MD, MPhil, assistant professor of dermatology and health services research at MD Anderson.
“Everyone in dermatology is aware of the increasing adoption of advanced practice clinicians in the field,” Justin D. Arnold, MD, MMSc, a 3rd-year dermatology resident at the University of California, Irvine, said in an interview. “However, seeing how quickly this happening and the absolute number of these clinicians is still startling,” said Dr. Arnold, who in 2022 published a research letter in JAMA Dermatology on the impact of physician assistants in dermatology.
In that study, he and his coauthors reported that the PA workforce in dermatology was growing faster than in other specialties.
In the current study, Dr. Wehner and her colleagues identified 8,444 dermatology APCs and 14,402 physician dermatologists who provided 109.3 million Medicare office visits from 2013 to 2020. More than 80% of the procedures were performed by physicians, but APCs appeared to increasingly be taking on more of the procedural load.
Over the study period, APCs had an average annual increase of 12.6% in the number of premalignant lesion destructions performed; physicians saw an average 1.4% decline. For skin biopsies, APCs performed 11.7% more per year on average, compared with a 1.4% drop for physicians.
“This data is not surprising given most agree that skin biopsies and destruction of premalignant lesions are well within the scope of practice of APCs,” Dr. Arnold told this news organization.
The authors also reported that, while most APCs – similar to physician dermatologists – practice in metropolitan areas, they are working in other locations also. Slightly more than half of dermatology clinicians in micropolitan areas are APCs, and in rural areas, 88% of clinicians are APCs, Dr. Wehner and colleagues found.
APCs may be filling a gap in rural areas for Medicare patients, said Dr. Arnold, but, he added, “it is unclear if dermatology APCs are growing as quickly in practices that predominantly accept Medicaid and if dermatology APCs are expanding access to these populations.”
Dr. Arnold said he expected the number of APCs in dermatology to continue growing, serving commercially insured patients, as well. “There are a multitude of potential reasons for more APCs in dermatology, including difficulty recruiting dermatologists in rural communities, financial motivators, and the expansion of private equity, and the increasing acceptance of these clinicians within medicine and by patients.”
APCs can provide good-quality care if they are properly trained and supervised, said Dr. Arnold, adding that he is concerned, however, that the training and supervision is not being provided. “This study provides further evidence that dermatologists, and national dermatology organizations such as the AAD [American Academy of Dermatology], need to take a more active role in the leadership of APC training,” he said.
Dermatology, he noted, “would benefit from consensus guidelines on clinical competencies for dermatology APCs,” similar to an effort by the American College of Cardiology.
A review* published online in July noted that, compared with dermatologists, some data suggest that non-physician operators (NPOs) may have a higher rate of adverse events when performing aesthetic procedures, according to the authors of the review, led by Shelby L. Kubicki, MD, of the department of dermatology at the UTHealth Science Center in Houston. There is no mandatory reporting of complications for nonphysician providers, so the authors relied on data from cosmetic-focused practices, medical spas, and a survey by the American Society of Dermatologic Surgery of consumers and its members. More than half of the responding physicians “reported treating complications of a cosmetic procedure performed by an NPO,” the authors wrote.
They also found higher rates of burns and discoloration among patients who were treated by NPOs. The injuries occurred primarily at medical spas.
“Although NPOs may help to meet the rising demand for dermatologic procedures, care should still be taken to prioritize patient safety and outcomes above all else, including financial profits and revenues,” the authors wrote.
Dr. Wehner and her colleagues report no relevant financial relationships. Their study research was supported, in part, by a Cancer Center Support Grant and by the Cancer Prevention and Research Institute of Texas. Dr. Arnold also reports no relevant financial relationships. No author disclosures or funding information were available for the Clinics in Dermatology paper.
*Correction, 12/8/23: An earlier version of this story misstated the study design.
A .
Researchers from the University of Texas MD Anderson Cancer Center, Houston, and the University of Pennsylvania, Philadelphia, reported in JAMA Dermatology that in 2013 APCs made up 28% of the dermatology clinician workforce. By 2020, they made up 37% of the dermatology clinicians giving care to Medicare beneficiaries.
Retrospective cohort study
APCs provided care in 15.5% of dermatology office visits in 2013 and 27.4% in 2020 (P =.02), the authors reported. “By 2020, more than one in four dermatology visits for patients with Medicare were delivered by APCs,” wrote the authors, led by Mackenzie R. Wehner, MD, MPhil, assistant professor of dermatology and health services research at MD Anderson.
“Everyone in dermatology is aware of the increasing adoption of advanced practice clinicians in the field,” Justin D. Arnold, MD, MMSc, a 3rd-year dermatology resident at the University of California, Irvine, said in an interview. “However, seeing how quickly this happening and the absolute number of these clinicians is still startling,” said Dr. Arnold, who in 2022 published a research letter in JAMA Dermatology on the impact of physician assistants in dermatology.
In that study, he and his coauthors reported that the PA workforce in dermatology was growing faster than in other specialties.
In the current study, Dr. Wehner and her colleagues identified 8,444 dermatology APCs and 14,402 physician dermatologists who provided 109.3 million Medicare office visits from 2013 to 2020. More than 80% of the procedures were performed by physicians, but APCs appeared to increasingly be taking on more of the procedural load.
Over the study period, APCs had an average annual increase of 12.6% in the number of premalignant lesion destructions performed; physicians saw an average 1.4% decline. For skin biopsies, APCs performed 11.7% more per year on average, compared with a 1.4% drop for physicians.
“This data is not surprising given most agree that skin biopsies and destruction of premalignant lesions are well within the scope of practice of APCs,” Dr. Arnold told this news organization.
The authors also reported that, while most APCs – similar to physician dermatologists – practice in metropolitan areas, they are working in other locations also. Slightly more than half of dermatology clinicians in micropolitan areas are APCs, and in rural areas, 88% of clinicians are APCs, Dr. Wehner and colleagues found.
APCs may be filling a gap in rural areas for Medicare patients, said Dr. Arnold, but, he added, “it is unclear if dermatology APCs are growing as quickly in practices that predominantly accept Medicaid and if dermatology APCs are expanding access to these populations.”
Dr. Arnold said he expected the number of APCs in dermatology to continue growing, serving commercially insured patients, as well. “There are a multitude of potential reasons for more APCs in dermatology, including difficulty recruiting dermatologists in rural communities, financial motivators, and the expansion of private equity, and the increasing acceptance of these clinicians within medicine and by patients.”
APCs can provide good-quality care if they are properly trained and supervised, said Dr. Arnold, adding that he is concerned, however, that the training and supervision is not being provided. “This study provides further evidence that dermatologists, and national dermatology organizations such as the AAD [American Academy of Dermatology], need to take a more active role in the leadership of APC training,” he said.
Dermatology, he noted, “would benefit from consensus guidelines on clinical competencies for dermatology APCs,” similar to an effort by the American College of Cardiology.
A review* published online in July noted that, compared with dermatologists, some data suggest that non-physician operators (NPOs) may have a higher rate of adverse events when performing aesthetic procedures, according to the authors of the review, led by Shelby L. Kubicki, MD, of the department of dermatology at the UTHealth Science Center in Houston. There is no mandatory reporting of complications for nonphysician providers, so the authors relied on data from cosmetic-focused practices, medical spas, and a survey by the American Society of Dermatologic Surgery of consumers and its members. More than half of the responding physicians “reported treating complications of a cosmetic procedure performed by an NPO,” the authors wrote.
They also found higher rates of burns and discoloration among patients who were treated by NPOs. The injuries occurred primarily at medical spas.
“Although NPOs may help to meet the rising demand for dermatologic procedures, care should still be taken to prioritize patient safety and outcomes above all else, including financial profits and revenues,” the authors wrote.
Dr. Wehner and her colleagues report no relevant financial relationships. Their study research was supported, in part, by a Cancer Center Support Grant and by the Cancer Prevention and Research Institute of Texas. Dr. Arnold also reports no relevant financial relationships. No author disclosures or funding information were available for the Clinics in Dermatology paper.
*Correction, 12/8/23: An earlier version of this story misstated the study design.
FROM JAMA DERMATOLOGY
Expanded coverage of carotid stenting in CMS draft proposal
The new memo follows a national coverage analysis for CAS that was initiated in January 2023 and considers 193 public comments received in the ensuing month.
That analysis followed a request from the Multispecialty Carotid Alliance (MSCA) to make the existing guidelines less restrictive.
The decision proposal would expand coverage for CAS “to standard surgical risk patients by removing the limitation of coverage to only high surgical risk patients.” It would limit it to patients for whom CAS is considered “reasonable and necessary” and who are either symptomatic with carotid stenosis of 50% or greater or asymptomatic with carotid stenosis of at least 70%.
The proposal would require practitioners to “engage in a formal shared decision-making interaction with the beneficiary” that involves use of a “validated decision-making tool.” The conversation must include discussion of all treatment options and their risks and benefits and cover information from the clinical guidelines, as well as “incorporate the patient’s personal preferences and priorities.”
Much of the proposed coverage criteria resemble recommendations from several societies that offered comments in response to the Jan. 12 CMS statement that led to the current draft proposal. They include, along with MSCA, the American Association of Neurological Surgeons and the Congress of Neurological Surgeons, and jointly the American College of Cardiology and the American Heart Association.
Carotid stenting, commented the ACC/AHA, “was first introduced in 1994, and the field has matured in the last 3 decades.” The procedure “is a well-established treatment option.” The groups declared support for “removal of the facility and operator requirement for CAS consistent with the current state of the published literature and standard clinical practice.”
The current CMS draft proposal acknowledges the publication of five major randomized controlled trials and a number of “large, prospective registry-based studies” since 2009 that support its proposed coverage criteria.
Collectively, it states, the evidence “suffices to demonstrate that CAS and [carotid endarterectomy] are similarly effective” with respect to the clinical primary endpoints of recent trials “in patients with either standard or high surgical risk and who are symptomatic with carotid artery stenosis ≥ 50% or asymptomatic with stenosis ≥ 70%.”
A version of this article appeared on Medscape.com.
The new memo follows a national coverage analysis for CAS that was initiated in January 2023 and considers 193 public comments received in the ensuing month.
That analysis followed a request from the Multispecialty Carotid Alliance (MSCA) to make the existing guidelines less restrictive.
The decision proposal would expand coverage for CAS “to standard surgical risk patients by removing the limitation of coverage to only high surgical risk patients.” It would limit it to patients for whom CAS is considered “reasonable and necessary” and who are either symptomatic with carotid stenosis of 50% or greater or asymptomatic with carotid stenosis of at least 70%.
The proposal would require practitioners to “engage in a formal shared decision-making interaction with the beneficiary” that involves use of a “validated decision-making tool.” The conversation must include discussion of all treatment options and their risks and benefits and cover information from the clinical guidelines, as well as “incorporate the patient’s personal preferences and priorities.”
Much of the proposed coverage criteria resemble recommendations from several societies that offered comments in response to the Jan. 12 CMS statement that led to the current draft proposal. They include, along with MSCA, the American Association of Neurological Surgeons and the Congress of Neurological Surgeons, and jointly the American College of Cardiology and the American Heart Association.
Carotid stenting, commented the ACC/AHA, “was first introduced in 1994, and the field has matured in the last 3 decades.” The procedure “is a well-established treatment option.” The groups declared support for “removal of the facility and operator requirement for CAS consistent with the current state of the published literature and standard clinical practice.”
The current CMS draft proposal acknowledges the publication of five major randomized controlled trials and a number of “large, prospective registry-based studies” since 2009 that support its proposed coverage criteria.
Collectively, it states, the evidence “suffices to demonstrate that CAS and [carotid endarterectomy] are similarly effective” with respect to the clinical primary endpoints of recent trials “in patients with either standard or high surgical risk and who are symptomatic with carotid artery stenosis ≥ 50% or asymptomatic with stenosis ≥ 70%.”
A version of this article appeared on Medscape.com.
The new memo follows a national coverage analysis for CAS that was initiated in January 2023 and considers 193 public comments received in the ensuing month.
That analysis followed a request from the Multispecialty Carotid Alliance (MSCA) to make the existing guidelines less restrictive.
The decision proposal would expand coverage for CAS “to standard surgical risk patients by removing the limitation of coverage to only high surgical risk patients.” It would limit it to patients for whom CAS is considered “reasonable and necessary” and who are either symptomatic with carotid stenosis of 50% or greater or asymptomatic with carotid stenosis of at least 70%.
The proposal would require practitioners to “engage in a formal shared decision-making interaction with the beneficiary” that involves use of a “validated decision-making tool.” The conversation must include discussion of all treatment options and their risks and benefits and cover information from the clinical guidelines, as well as “incorporate the patient’s personal preferences and priorities.”
Much of the proposed coverage criteria resemble recommendations from several societies that offered comments in response to the Jan. 12 CMS statement that led to the current draft proposal. They include, along with MSCA, the American Association of Neurological Surgeons and the Congress of Neurological Surgeons, and jointly the American College of Cardiology and the American Heart Association.
Carotid stenting, commented the ACC/AHA, “was first introduced in 1994, and the field has matured in the last 3 decades.” The procedure “is a well-established treatment option.” The groups declared support for “removal of the facility and operator requirement for CAS consistent with the current state of the published literature and standard clinical practice.”
The current CMS draft proposal acknowledges the publication of five major randomized controlled trials and a number of “large, prospective registry-based studies” since 2009 that support its proposed coverage criteria.
Collectively, it states, the evidence “suffices to demonstrate that CAS and [carotid endarterectomy] are similarly effective” with respect to the clinical primary endpoints of recent trials “in patients with either standard or high surgical risk and who are symptomatic with carotid artery stenosis ≥ 50% or asymptomatic with stenosis ≥ 70%.”
A version of this article appeared on Medscape.com.
LAMA-LABA surpasses corticosteroid combination as COPD therapy
Use of inhalers with long-acting muscarinic antagonists and long-acting beta-agonists reduced COPD exacerbations and pneumonia hospitalizations compared with inhalers with corticosteroids and long-acting beta-agonists, based on data from more than 30,000 individuals.
Current clinical guidelines for chronic obstructive pulmonary disease (COPD) patients recommend inhalers with long-acting muscarinic antagonists (LAMAs) and long-acting beta-agonists (LABAs) over those with inhaled corticosteroids (ICSs) and LABAs, but data comparing the two formulations have been inconsistent, and concerns about generalizability persist, wrote William B. Feldman, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in JAMA Internal Medicine, the researchers reviewed data from a commercial insurance claims database of individuals diagnosed with COPD who filled a new prescription for a LAMA-LABA inhaler or ICS-LABA inhaler between Jan. 1, 2014, and Dec. 31, 2019. Patients with asthma and those younger than 40 years were excluded. The study population included 137,833 individuals with a mean age of 70.2 years; 50.4% were female. Of the 107,004 ICS-LABA users and 30,829 LAMA-LABA users, 30,216 matched pairs were included in a 1:1 propensity score matched study. The primary outcomes were effectiveness, based on the rate of first moderate or severe COPD exacerbation, and safety, based on the rate of first pneumonia hospitalization.
Use of LAMA-LABA inhalers was associated with an 8% reduction in the rate of first moderate or severe COPD exacerbation and a 20% reduction in the rate of first pneumonia hospitalization compared with use of ICS-LABA (hazard ratios 0.92 and 0.80, respectively). The absolute rate reductions with LAMA-LABA inhalers for first moderate or severe COPD exacerbations and for first pneumonia hospitalizations were was 43.0 events per 1,000 person-years and 91.8 events per person-years, respectively.
The overall rates of total moderate to severe COPD and pneumonia hospitalizations were 5% and 17% lower, respectively, among patients who used LAMA-LABA than those treated with ICS-LABA. The results were consistently robust in subgroup and sensitivity analyses, the researchers wrote in their discussion. However, the results must be interpreted cautiously in comparison to other large studies because of the significant differences in the cohorts of patients studied, notably that most patients in the current study had no received previous inhaler therapy.
The study findings were limited by several factors including the relatively short follow-up time and reliance on prescription fills as an indicator of medication use, the researchers noted. Other limitations included notable differences between the LAMA-LABA patients and ICS-LABA patients, such as more severe COPD and less access to respiratory care, they wrote.
Although the current study is not the definitive answer to conflicting results from previous trials, it is the largest know to date to compare LAMA-LABA with ICS-LABA, and the results support LAMA-LABA as the preferred therapy for COPD patients, the researchers concluded.
Findings clarify clinical practice guidelines
“This study was required to provide clarity regarding the optimal choice of treatment for COPD given conflicting data from other recent trials,” Suman Pal, MBBS, of the University of New Mexico, Albuquerque, said in an interview.
“The study findings reinforce the benefits of combined LAMA-LABA in improving clinical outcomes in COPD in a real-world setting,” and the data provide further support for choosing LAMA-LABA over ICS-LABA in COPD patients, said Dr. Pal, who was not involved in the study.
However, availability and affordability of LAMA-LABA inhalers may be barriers to expanding their use in clinical practice, he noted.
“Additional research is needed to accurately define which patient populations would benefit most from the therapy and whether patients who have previously been stabilized on ICS-LABA would derive additional benefit from a change in therapy,” Dr. Pal said.
The study was supported by the National Heart, Lung, and Blood Institute and funding from the Commonwealth Fund and Arnold Ventures.
Dr. Feldman disclosed receiving personal fees from Alosa Health and Aetion, serving as an expert witness in litigation against inhaler manufacturers, and receiving an honorarium for a presentation to Blue Cross Blue Shield of Massachusetts unrelated to the current study. Dr. Pal had no financial conflicts to disclose.
Use of inhalers with long-acting muscarinic antagonists and long-acting beta-agonists reduced COPD exacerbations and pneumonia hospitalizations compared with inhalers with corticosteroids and long-acting beta-agonists, based on data from more than 30,000 individuals.
Current clinical guidelines for chronic obstructive pulmonary disease (COPD) patients recommend inhalers with long-acting muscarinic antagonists (LAMAs) and long-acting beta-agonists (LABAs) over those with inhaled corticosteroids (ICSs) and LABAs, but data comparing the two formulations have been inconsistent, and concerns about generalizability persist, wrote William B. Feldman, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in JAMA Internal Medicine, the researchers reviewed data from a commercial insurance claims database of individuals diagnosed with COPD who filled a new prescription for a LAMA-LABA inhaler or ICS-LABA inhaler between Jan. 1, 2014, and Dec. 31, 2019. Patients with asthma and those younger than 40 years were excluded. The study population included 137,833 individuals with a mean age of 70.2 years; 50.4% were female. Of the 107,004 ICS-LABA users and 30,829 LAMA-LABA users, 30,216 matched pairs were included in a 1:1 propensity score matched study. The primary outcomes were effectiveness, based on the rate of first moderate or severe COPD exacerbation, and safety, based on the rate of first pneumonia hospitalization.
Use of LAMA-LABA inhalers was associated with an 8% reduction in the rate of first moderate or severe COPD exacerbation and a 20% reduction in the rate of first pneumonia hospitalization compared with use of ICS-LABA (hazard ratios 0.92 and 0.80, respectively). The absolute rate reductions with LAMA-LABA inhalers for first moderate or severe COPD exacerbations and for first pneumonia hospitalizations were was 43.0 events per 1,000 person-years and 91.8 events per person-years, respectively.
The overall rates of total moderate to severe COPD and pneumonia hospitalizations were 5% and 17% lower, respectively, among patients who used LAMA-LABA than those treated with ICS-LABA. The results were consistently robust in subgroup and sensitivity analyses, the researchers wrote in their discussion. However, the results must be interpreted cautiously in comparison to other large studies because of the significant differences in the cohorts of patients studied, notably that most patients in the current study had no received previous inhaler therapy.
The study findings were limited by several factors including the relatively short follow-up time and reliance on prescription fills as an indicator of medication use, the researchers noted. Other limitations included notable differences between the LAMA-LABA patients and ICS-LABA patients, such as more severe COPD and less access to respiratory care, they wrote.
Although the current study is not the definitive answer to conflicting results from previous trials, it is the largest know to date to compare LAMA-LABA with ICS-LABA, and the results support LAMA-LABA as the preferred therapy for COPD patients, the researchers concluded.
Findings clarify clinical practice guidelines
“This study was required to provide clarity regarding the optimal choice of treatment for COPD given conflicting data from other recent trials,” Suman Pal, MBBS, of the University of New Mexico, Albuquerque, said in an interview.
“The study findings reinforce the benefits of combined LAMA-LABA in improving clinical outcomes in COPD in a real-world setting,” and the data provide further support for choosing LAMA-LABA over ICS-LABA in COPD patients, said Dr. Pal, who was not involved in the study.
However, availability and affordability of LAMA-LABA inhalers may be barriers to expanding their use in clinical practice, he noted.
“Additional research is needed to accurately define which patient populations would benefit most from the therapy and whether patients who have previously been stabilized on ICS-LABA would derive additional benefit from a change in therapy,” Dr. Pal said.
The study was supported by the National Heart, Lung, and Blood Institute and funding from the Commonwealth Fund and Arnold Ventures.
Dr. Feldman disclosed receiving personal fees from Alosa Health and Aetion, serving as an expert witness in litigation against inhaler manufacturers, and receiving an honorarium for a presentation to Blue Cross Blue Shield of Massachusetts unrelated to the current study. Dr. Pal had no financial conflicts to disclose.
Use of inhalers with long-acting muscarinic antagonists and long-acting beta-agonists reduced COPD exacerbations and pneumonia hospitalizations compared with inhalers with corticosteroids and long-acting beta-agonists, based on data from more than 30,000 individuals.
Current clinical guidelines for chronic obstructive pulmonary disease (COPD) patients recommend inhalers with long-acting muscarinic antagonists (LAMAs) and long-acting beta-agonists (LABAs) over those with inhaled corticosteroids (ICSs) and LABAs, but data comparing the two formulations have been inconsistent, and concerns about generalizability persist, wrote William B. Feldman, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in JAMA Internal Medicine, the researchers reviewed data from a commercial insurance claims database of individuals diagnosed with COPD who filled a new prescription for a LAMA-LABA inhaler or ICS-LABA inhaler between Jan. 1, 2014, and Dec. 31, 2019. Patients with asthma and those younger than 40 years were excluded. The study population included 137,833 individuals with a mean age of 70.2 years; 50.4% were female. Of the 107,004 ICS-LABA users and 30,829 LAMA-LABA users, 30,216 matched pairs were included in a 1:1 propensity score matched study. The primary outcomes were effectiveness, based on the rate of first moderate or severe COPD exacerbation, and safety, based on the rate of first pneumonia hospitalization.
Use of LAMA-LABA inhalers was associated with an 8% reduction in the rate of first moderate or severe COPD exacerbation and a 20% reduction in the rate of first pneumonia hospitalization compared with use of ICS-LABA (hazard ratios 0.92 and 0.80, respectively). The absolute rate reductions with LAMA-LABA inhalers for first moderate or severe COPD exacerbations and for first pneumonia hospitalizations were was 43.0 events per 1,000 person-years and 91.8 events per person-years, respectively.
The overall rates of total moderate to severe COPD and pneumonia hospitalizations were 5% and 17% lower, respectively, among patients who used LAMA-LABA than those treated with ICS-LABA. The results were consistently robust in subgroup and sensitivity analyses, the researchers wrote in their discussion. However, the results must be interpreted cautiously in comparison to other large studies because of the significant differences in the cohorts of patients studied, notably that most patients in the current study had no received previous inhaler therapy.
The study findings were limited by several factors including the relatively short follow-up time and reliance on prescription fills as an indicator of medication use, the researchers noted. Other limitations included notable differences between the LAMA-LABA patients and ICS-LABA patients, such as more severe COPD and less access to respiratory care, they wrote.
Although the current study is not the definitive answer to conflicting results from previous trials, it is the largest know to date to compare LAMA-LABA with ICS-LABA, and the results support LAMA-LABA as the preferred therapy for COPD patients, the researchers concluded.
Findings clarify clinical practice guidelines
“This study was required to provide clarity regarding the optimal choice of treatment for COPD given conflicting data from other recent trials,” Suman Pal, MBBS, of the University of New Mexico, Albuquerque, said in an interview.
“The study findings reinforce the benefits of combined LAMA-LABA in improving clinical outcomes in COPD in a real-world setting,” and the data provide further support for choosing LAMA-LABA over ICS-LABA in COPD patients, said Dr. Pal, who was not involved in the study.
However, availability and affordability of LAMA-LABA inhalers may be barriers to expanding their use in clinical practice, he noted.
“Additional research is needed to accurately define which patient populations would benefit most from the therapy and whether patients who have previously been stabilized on ICS-LABA would derive additional benefit from a change in therapy,” Dr. Pal said.
The study was supported by the National Heart, Lung, and Blood Institute and funding from the Commonwealth Fund and Arnold Ventures.
Dr. Feldman disclosed receiving personal fees from Alosa Health and Aetion, serving as an expert witness in litigation against inhaler manufacturers, and receiving an honorarium for a presentation to Blue Cross Blue Shield of Massachusetts unrelated to the current study. Dr. Pal had no financial conflicts to disclose.
FROM JAMA INTERNAL MEDICINE
Fibromyalgia linked to higher mortality risk
People who experience chronic pain and tiredness from fibromyalgia have an increased risk for all-cause mortality, a new analysis of evidence says.
The condition can lead people to be vulnerable to accidents, infections, and even suicide, according to the report published in RMD Open.
The researchers suggest that care providers monitor physical and mental health to lower the dangers.
People with fibromyalgia often have other health issues, including rheumatic, gut, neurological, and mental health disorders, according to The BMJ. More and more people are being diagnosed with fibromyalgia. The cause of the illness remains unclear.
The researchers looked at eight studies published between 1999 and 2020 and pooled results from six of them. The studies involved a total of 188,000 adults.
The analysis of the data revealed that fibromyalgia was linked to a 27% greater risk of death from all causes.
Those with fibromyalgia were at a 44% greater risk of infections, including pneumonia. Their suicide risk was more than three times higher.
The greater risk of all-cause death could result from fatigue, poor sleep, and concentration problems, The BMJ said.
The patients had a 12% lower risk of dying from cancer, the analysis found. This could be because they tend to make more visits to health care professionals, the authors suggest.
“Fibromyalgia is often called an ‘imaginary condition,’ with ongoing debates on the legitimacy and clinical usefulness of this diagnosis. Our review provides further proof that fibromyalgia patients should be taken seriously, with particular focus on screening for suicidal ideation, prevention of accidents, and prevention and treatment of infections,” the researchers say.
A version of this article appeared on WebMD.com.
People who experience chronic pain and tiredness from fibromyalgia have an increased risk for all-cause mortality, a new analysis of evidence says.
The condition can lead people to be vulnerable to accidents, infections, and even suicide, according to the report published in RMD Open.
The researchers suggest that care providers monitor physical and mental health to lower the dangers.
People with fibromyalgia often have other health issues, including rheumatic, gut, neurological, and mental health disorders, according to The BMJ. More and more people are being diagnosed with fibromyalgia. The cause of the illness remains unclear.
The researchers looked at eight studies published between 1999 and 2020 and pooled results from six of them. The studies involved a total of 188,000 adults.
The analysis of the data revealed that fibromyalgia was linked to a 27% greater risk of death from all causes.
Those with fibromyalgia were at a 44% greater risk of infections, including pneumonia. Their suicide risk was more than three times higher.
The greater risk of all-cause death could result from fatigue, poor sleep, and concentration problems, The BMJ said.
The patients had a 12% lower risk of dying from cancer, the analysis found. This could be because they tend to make more visits to health care professionals, the authors suggest.
“Fibromyalgia is often called an ‘imaginary condition,’ with ongoing debates on the legitimacy and clinical usefulness of this diagnosis. Our review provides further proof that fibromyalgia patients should be taken seriously, with particular focus on screening for suicidal ideation, prevention of accidents, and prevention and treatment of infections,” the researchers say.
A version of this article appeared on WebMD.com.
People who experience chronic pain and tiredness from fibromyalgia have an increased risk for all-cause mortality, a new analysis of evidence says.
The condition can lead people to be vulnerable to accidents, infections, and even suicide, according to the report published in RMD Open.
The researchers suggest that care providers monitor physical and mental health to lower the dangers.
People with fibromyalgia often have other health issues, including rheumatic, gut, neurological, and mental health disorders, according to The BMJ. More and more people are being diagnosed with fibromyalgia. The cause of the illness remains unclear.
The researchers looked at eight studies published between 1999 and 2020 and pooled results from six of them. The studies involved a total of 188,000 adults.
The analysis of the data revealed that fibromyalgia was linked to a 27% greater risk of death from all causes.
Those with fibromyalgia were at a 44% greater risk of infections, including pneumonia. Their suicide risk was more than three times higher.
The greater risk of all-cause death could result from fatigue, poor sleep, and concentration problems, The BMJ said.
The patients had a 12% lower risk of dying from cancer, the analysis found. This could be because they tend to make more visits to health care professionals, the authors suggest.
“Fibromyalgia is often called an ‘imaginary condition,’ with ongoing debates on the legitimacy and clinical usefulness of this diagnosis. Our review provides further proof that fibromyalgia patients should be taken seriously, with particular focus on screening for suicidal ideation, prevention of accidents, and prevention and treatment of infections,” the researchers say.
A version of this article appeared on WebMD.com.
Mixed bag: New performance data on femoral-popliteal artery revascularization
Measured one way, success for peripheral vascular intervention (PVI) in the femoropopliteal arteries for patients with intermittent claudication has improved, as the need for repeat PVI appears to be very low, and lower than in recent years, a new analysis suggests. But measured another way, the researchers said, PVI’s record of success in peripheral arterial disease (PAD) remains marred by a substantial risk for amputation involving the treated limb.
In their analysis, The rate for popliteal interventions was significantly higher than for PVI limited to the superficial femoral artery (SFA), 7.5% and 3.4%, respectively.
The 4-year rate of repeat target-vessel revascularization, however, was “lower than expected” at 15.2% in the analysis, which was based on the PINC AI Healthcare Data database covering over 1,100 U.S. hospitals. The study was published online in JACC: Cardiovascular Interventions.
The amputation rates for index treated limbs “surprised us,” lead author S. Elissa Altin, MD, Yale University, New Haven, Conn., said in an interview. The increased rate after procedures limited to the popliteal artery, compared with the SFA, “were even more concerning,” she said. “This is higher than accepted natural history rates of amputation in patients with conservatively managed claudication.”
Of particular concern in the study, agreed the author of an accompanying editorial, “is the finding of a 1 in 25 risk for amputation among patients with [intermittent claudication] undergoing revascularization, which underscores that both patients and physicians must ensure that evidence-based lifestyle and medical therapies are exhausted prior to pursuing [femoropopliteal] revascularization.”
Given such amputation concerns “and the availability of effective lifestyle and medical therapies,” wrote Debabrata Mukherjee, MD, Texas Tech University Health Sciences Center, El Paso, “PVI should be restricted in stable PAD only for those with persistent lifestyle-limiting claudication despite [guideline-directed medical therapy] and structured exercise therapy.”
Dr. Altin and colleagues analyzed data from 19,324 patients with intermittent claudication (mean age, 69 years; 59% men) who underwent femoropopliteal PVI from 2016 to 2020.
Use of atherectomy and of drug-eluting balloons were both similarly prevalent for popliteal and SFA target arteries; however, SFA lesions were more commonly treated with stents.
The rate of amputation in the treated limb over 4 years was 4.3%; the rate of major (above the ankle) amputation was 3.2%.
The multivariable-adjusted treated-limb amputation hazard ratio for popliteal versus SFA procedures was for 2.10 (95% confidence interval, 1.52-2.92) for any amputation and 1.98 (95% CI, 1.32-2.95) for major amputation.
The 4-year rate of index-limb repeat revascularization was 16.7% overall, 20.1% for patients with an index procedure in both the popliteal and SFA segments, 19% after popliteal-only procedures, and 15.4% after SFA-only procedures (P < .0001), the report stated.
The overall lower-than-expected revascularization rates, the authors proposed, may reflect improvements in endovascular therapies for femoropopliteal lesions, such as drug-eluting stents and advances in medical therapy.
“Additionally, this may underscore a difference between trial-defined target-lesion revascularization compared with clinically driven target-lesion revascularization in practice,” they wrote.
The study’s revascularization rates could have been underestimated because “some of the patients in this study may have had procedures conducted in other hospital systems or at an office-based lab during the study period,” proposed interventional cardiologist Seyi Bolorunduro MD, MPH, INOVA Heart and Vascular Institute, Falls Church, Va.
“This and other studies highlight the need to be cautious about offering PVI to patients with intermittent claudication,” said Dr. Bolorunduro, who was not connected with the current study. On the other hand, he added, randomized trial data show “that combination therapy with PVI followed by supervised exercise results in greater improvement in walking distances and quality-of-life scores, compared with supervised exercise alone, at 1 year.’
Femoropopliteal PVI “is an important tool for patients with residual, truly lifestyle-limiting claudication after exhausting medical therapies, complete smoking cessation, and structured exercise programs,” Dr. Altin said. Future studies, she added, should look prospectively at patients with claudication who underwent early versus delayed invasive management.
In his editorial, Dr. Mukherjee said that, for patients with PAD and claudication, a proprotein convertase subtilisin/kexin type 9 inhibitor may be recommended if LDL cholesterol remains 70 mg/dL or higher and symptoms persist after a regimen of lifestyle modification, exercise, antiplatelet therapy, and high-intensity statins and other guideline-directed medical therapy. He also suggests a direct oral anticoagulant be considered before resorting to endovascular or surgical revascularization.
“We need to optimize risk-factor modification, medical therapy and exercise, and only reserve PVI for patients with severe lifestyle-limiting intermittent claudication who have tried and failed everything else,” Dr. Bolorunduro agreed in an interview. “I educate my patients about [the amputation] risk and let them know that PVI is not a panacea.”
Dr. Altin has disclosed no relevant relationships. Dr. Mukherjee and Dr. Bolorunduro have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Measured one way, success for peripheral vascular intervention (PVI) in the femoropopliteal arteries for patients with intermittent claudication has improved, as the need for repeat PVI appears to be very low, and lower than in recent years, a new analysis suggests. But measured another way, the researchers said, PVI’s record of success in peripheral arterial disease (PAD) remains marred by a substantial risk for amputation involving the treated limb.
In their analysis, The rate for popliteal interventions was significantly higher than for PVI limited to the superficial femoral artery (SFA), 7.5% and 3.4%, respectively.
The 4-year rate of repeat target-vessel revascularization, however, was “lower than expected” at 15.2% in the analysis, which was based on the PINC AI Healthcare Data database covering over 1,100 U.S. hospitals. The study was published online in JACC: Cardiovascular Interventions.
The amputation rates for index treated limbs “surprised us,” lead author S. Elissa Altin, MD, Yale University, New Haven, Conn., said in an interview. The increased rate after procedures limited to the popliteal artery, compared with the SFA, “were even more concerning,” she said. “This is higher than accepted natural history rates of amputation in patients with conservatively managed claudication.”
Of particular concern in the study, agreed the author of an accompanying editorial, “is the finding of a 1 in 25 risk for amputation among patients with [intermittent claudication] undergoing revascularization, which underscores that both patients and physicians must ensure that evidence-based lifestyle and medical therapies are exhausted prior to pursuing [femoropopliteal] revascularization.”
Given such amputation concerns “and the availability of effective lifestyle and medical therapies,” wrote Debabrata Mukherjee, MD, Texas Tech University Health Sciences Center, El Paso, “PVI should be restricted in stable PAD only for those with persistent lifestyle-limiting claudication despite [guideline-directed medical therapy] and structured exercise therapy.”
Dr. Altin and colleagues analyzed data from 19,324 patients with intermittent claudication (mean age, 69 years; 59% men) who underwent femoropopliteal PVI from 2016 to 2020.
Use of atherectomy and of drug-eluting balloons were both similarly prevalent for popliteal and SFA target arteries; however, SFA lesions were more commonly treated with stents.
The rate of amputation in the treated limb over 4 years was 4.3%; the rate of major (above the ankle) amputation was 3.2%.
The multivariable-adjusted treated-limb amputation hazard ratio for popliteal versus SFA procedures was for 2.10 (95% confidence interval, 1.52-2.92) for any amputation and 1.98 (95% CI, 1.32-2.95) for major amputation.
The 4-year rate of index-limb repeat revascularization was 16.7% overall, 20.1% for patients with an index procedure in both the popliteal and SFA segments, 19% after popliteal-only procedures, and 15.4% after SFA-only procedures (P < .0001), the report stated.
The overall lower-than-expected revascularization rates, the authors proposed, may reflect improvements in endovascular therapies for femoropopliteal lesions, such as drug-eluting stents and advances in medical therapy.
“Additionally, this may underscore a difference between trial-defined target-lesion revascularization compared with clinically driven target-lesion revascularization in practice,” they wrote.
The study’s revascularization rates could have been underestimated because “some of the patients in this study may have had procedures conducted in other hospital systems or at an office-based lab during the study period,” proposed interventional cardiologist Seyi Bolorunduro MD, MPH, INOVA Heart and Vascular Institute, Falls Church, Va.
“This and other studies highlight the need to be cautious about offering PVI to patients with intermittent claudication,” said Dr. Bolorunduro, who was not connected with the current study. On the other hand, he added, randomized trial data show “that combination therapy with PVI followed by supervised exercise results in greater improvement in walking distances and quality-of-life scores, compared with supervised exercise alone, at 1 year.’
Femoropopliteal PVI “is an important tool for patients with residual, truly lifestyle-limiting claudication after exhausting medical therapies, complete smoking cessation, and structured exercise programs,” Dr. Altin said. Future studies, she added, should look prospectively at patients with claudication who underwent early versus delayed invasive management.
In his editorial, Dr. Mukherjee said that, for patients with PAD and claudication, a proprotein convertase subtilisin/kexin type 9 inhibitor may be recommended if LDL cholesterol remains 70 mg/dL or higher and symptoms persist after a regimen of lifestyle modification, exercise, antiplatelet therapy, and high-intensity statins and other guideline-directed medical therapy. He also suggests a direct oral anticoagulant be considered before resorting to endovascular or surgical revascularization.
“We need to optimize risk-factor modification, medical therapy and exercise, and only reserve PVI for patients with severe lifestyle-limiting intermittent claudication who have tried and failed everything else,” Dr. Bolorunduro agreed in an interview. “I educate my patients about [the amputation] risk and let them know that PVI is not a panacea.”
Dr. Altin has disclosed no relevant relationships. Dr. Mukherjee and Dr. Bolorunduro have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Measured one way, success for peripheral vascular intervention (PVI) in the femoropopliteal arteries for patients with intermittent claudication has improved, as the need for repeat PVI appears to be very low, and lower than in recent years, a new analysis suggests. But measured another way, the researchers said, PVI’s record of success in peripheral arterial disease (PAD) remains marred by a substantial risk for amputation involving the treated limb.
In their analysis, The rate for popliteal interventions was significantly higher than for PVI limited to the superficial femoral artery (SFA), 7.5% and 3.4%, respectively.
The 4-year rate of repeat target-vessel revascularization, however, was “lower than expected” at 15.2% in the analysis, which was based on the PINC AI Healthcare Data database covering over 1,100 U.S. hospitals. The study was published online in JACC: Cardiovascular Interventions.
The amputation rates for index treated limbs “surprised us,” lead author S. Elissa Altin, MD, Yale University, New Haven, Conn., said in an interview. The increased rate after procedures limited to the popliteal artery, compared with the SFA, “were even more concerning,” she said. “This is higher than accepted natural history rates of amputation in patients with conservatively managed claudication.”
Of particular concern in the study, agreed the author of an accompanying editorial, “is the finding of a 1 in 25 risk for amputation among patients with [intermittent claudication] undergoing revascularization, which underscores that both patients and physicians must ensure that evidence-based lifestyle and medical therapies are exhausted prior to pursuing [femoropopliteal] revascularization.”
Given such amputation concerns “and the availability of effective lifestyle and medical therapies,” wrote Debabrata Mukherjee, MD, Texas Tech University Health Sciences Center, El Paso, “PVI should be restricted in stable PAD only for those with persistent lifestyle-limiting claudication despite [guideline-directed medical therapy] and structured exercise therapy.”
Dr. Altin and colleagues analyzed data from 19,324 patients with intermittent claudication (mean age, 69 years; 59% men) who underwent femoropopliteal PVI from 2016 to 2020.
Use of atherectomy and of drug-eluting balloons were both similarly prevalent for popliteal and SFA target arteries; however, SFA lesions were more commonly treated with stents.
The rate of amputation in the treated limb over 4 years was 4.3%; the rate of major (above the ankle) amputation was 3.2%.
The multivariable-adjusted treated-limb amputation hazard ratio for popliteal versus SFA procedures was for 2.10 (95% confidence interval, 1.52-2.92) for any amputation and 1.98 (95% CI, 1.32-2.95) for major amputation.
The 4-year rate of index-limb repeat revascularization was 16.7% overall, 20.1% for patients with an index procedure in both the popliteal and SFA segments, 19% after popliteal-only procedures, and 15.4% after SFA-only procedures (P < .0001), the report stated.
The overall lower-than-expected revascularization rates, the authors proposed, may reflect improvements in endovascular therapies for femoropopliteal lesions, such as drug-eluting stents and advances in medical therapy.
“Additionally, this may underscore a difference between trial-defined target-lesion revascularization compared with clinically driven target-lesion revascularization in practice,” they wrote.
The study’s revascularization rates could have been underestimated because “some of the patients in this study may have had procedures conducted in other hospital systems or at an office-based lab during the study period,” proposed interventional cardiologist Seyi Bolorunduro MD, MPH, INOVA Heart and Vascular Institute, Falls Church, Va.
“This and other studies highlight the need to be cautious about offering PVI to patients with intermittent claudication,” said Dr. Bolorunduro, who was not connected with the current study. On the other hand, he added, randomized trial data show “that combination therapy with PVI followed by supervised exercise results in greater improvement in walking distances and quality-of-life scores, compared with supervised exercise alone, at 1 year.’
Femoropopliteal PVI “is an important tool for patients with residual, truly lifestyle-limiting claudication after exhausting medical therapies, complete smoking cessation, and structured exercise programs,” Dr. Altin said. Future studies, she added, should look prospectively at patients with claudication who underwent early versus delayed invasive management.
In his editorial, Dr. Mukherjee said that, for patients with PAD and claudication, a proprotein convertase subtilisin/kexin type 9 inhibitor may be recommended if LDL cholesterol remains 70 mg/dL or higher and symptoms persist after a regimen of lifestyle modification, exercise, antiplatelet therapy, and high-intensity statins and other guideline-directed medical therapy. He also suggests a direct oral anticoagulant be considered before resorting to endovascular or surgical revascularization.
“We need to optimize risk-factor modification, medical therapy and exercise, and only reserve PVI for patients with severe lifestyle-limiting intermittent claudication who have tried and failed everything else,” Dr. Bolorunduro agreed in an interview. “I educate my patients about [the amputation] risk and let them know that PVI is not a panacea.”
Dr. Altin has disclosed no relevant relationships. Dr. Mukherjee and Dr. Bolorunduro have no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
What's your diagnosis?
The diagnosis
Based on the clinical and imaging findings, a diagnosis of gallbladder adenomyomatosis was made. GA is a benign and usually asymptomatic condition that occurs mainly beyond the age of 50-60 years and is very rare in childhood.1 Symptomatic gallbladder adenomyomatosis indicates cholecystectomy, considering the presence of inflammation or gallbladder stones.2 Therefore, a laparoscopic cholecystectomy was performed on our patient. Rokitansky-Aschoff sinuses were seen in the entire thickened gallbladder wall on gross pathologic examination (Figure D). Histopathologic examination confirmed the diagnosis of GA with cholecystitis. The patient was eventually diagnosed with diffuse GA. She was successfully discharged from the hospital 4 days after surgery, and 3 months of follow-up were uneventful.
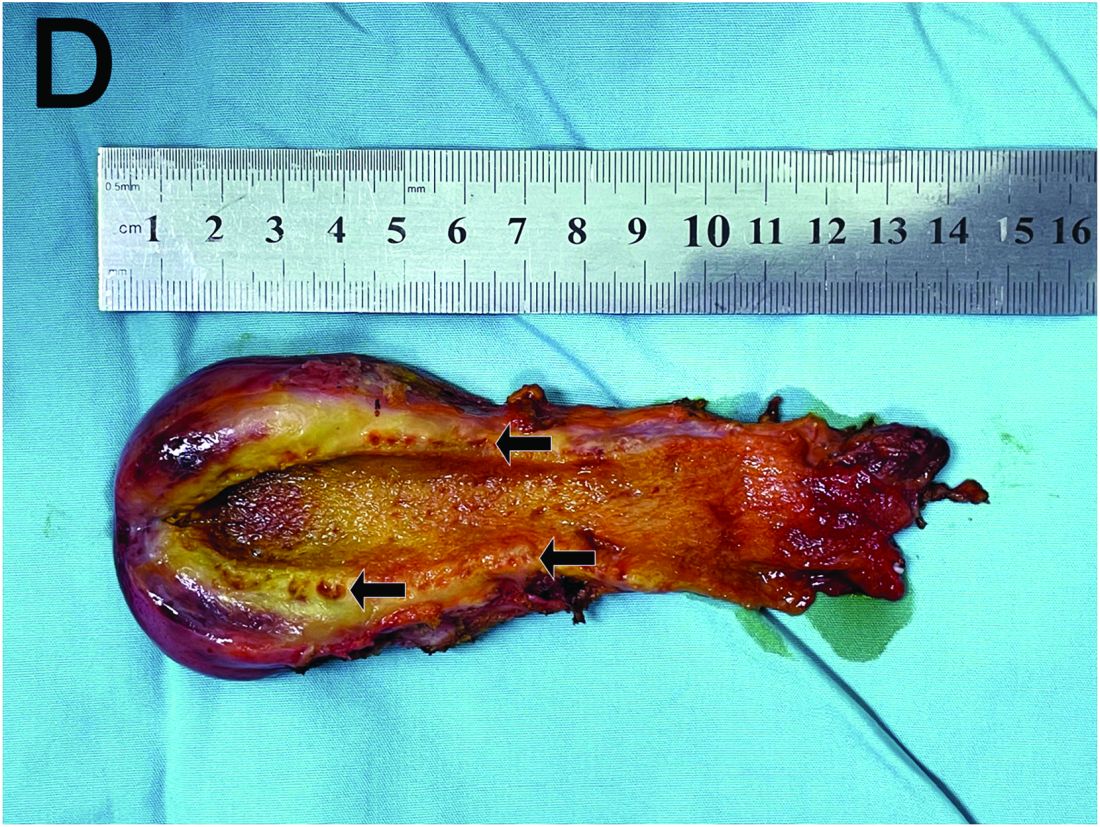
References
Eroglu N et al. Diffuse adenomyomatosis of the gallbladder in a child. J Pediatr Hematol Oncol. 2016;38:e307-9.
Bonatti M. et al. Gallbladder adenomyomatosis: imaging findings, tricks and pitfalls. Insights Imaging. 2017;8:243-53.
Hammad AY et al. A literature review of radiological findings to guide the diagnosis of gallbladder adenomyomatosis. HPB (Oxford). 2016;18:129-35.
The diagnosis
Based on the clinical and imaging findings, a diagnosis of gallbladder adenomyomatosis was made. GA is a benign and usually asymptomatic condition that occurs mainly beyond the age of 50-60 years and is very rare in childhood.1 Symptomatic gallbladder adenomyomatosis indicates cholecystectomy, considering the presence of inflammation or gallbladder stones.2 Therefore, a laparoscopic cholecystectomy was performed on our patient. Rokitansky-Aschoff sinuses were seen in the entire thickened gallbladder wall on gross pathologic examination (Figure D). Histopathologic examination confirmed the diagnosis of GA with cholecystitis. The patient was eventually diagnosed with diffuse GA. She was successfully discharged from the hospital 4 days after surgery, and 3 months of follow-up were uneventful.
References
Eroglu N et al. Diffuse adenomyomatosis of the gallbladder in a child. J Pediatr Hematol Oncol. 2016;38:e307-9.
Bonatti M. et al. Gallbladder adenomyomatosis: imaging findings, tricks and pitfalls. Insights Imaging. 2017;8:243-53.
Hammad AY et al. A literature review of radiological findings to guide the diagnosis of gallbladder adenomyomatosis. HPB (Oxford). 2016;18:129-35.
The diagnosis
Based on the clinical and imaging findings, a diagnosis of gallbladder adenomyomatosis was made. GA is a benign and usually asymptomatic condition that occurs mainly beyond the age of 50-60 years and is very rare in childhood.1 Symptomatic gallbladder adenomyomatosis indicates cholecystectomy, considering the presence of inflammation or gallbladder stones.2 Therefore, a laparoscopic cholecystectomy was performed on our patient. Rokitansky-Aschoff sinuses were seen in the entire thickened gallbladder wall on gross pathologic examination (Figure D). Histopathologic examination confirmed the diagnosis of GA with cholecystitis. The patient was eventually diagnosed with diffuse GA. She was successfully discharged from the hospital 4 days after surgery, and 3 months of follow-up were uneventful.
References
Eroglu N et al. Diffuse adenomyomatosis of the gallbladder in a child. J Pediatr Hematol Oncol. 2016;38:e307-9.
Bonatti M. et al. Gallbladder adenomyomatosis: imaging findings, tricks and pitfalls. Insights Imaging. 2017;8:243-53.
Hammad AY et al. A literature review of radiological findings to guide the diagnosis of gallbladder adenomyomatosis. HPB (Oxford). 2016;18:129-35.
A 15-year-old girl presented with an 18-month history of intermittent right upper quadrant pain that appeared after meals and was relieved after rest. She denied any nausea, vomiting, chills, diarrhea, or constipation. The patient reported no trauma. At admission, physical examination showed tenderness in the right upper abdomen without rebound or guarding. Murphy's sign was also present. The laboratory tests were unremarkable.
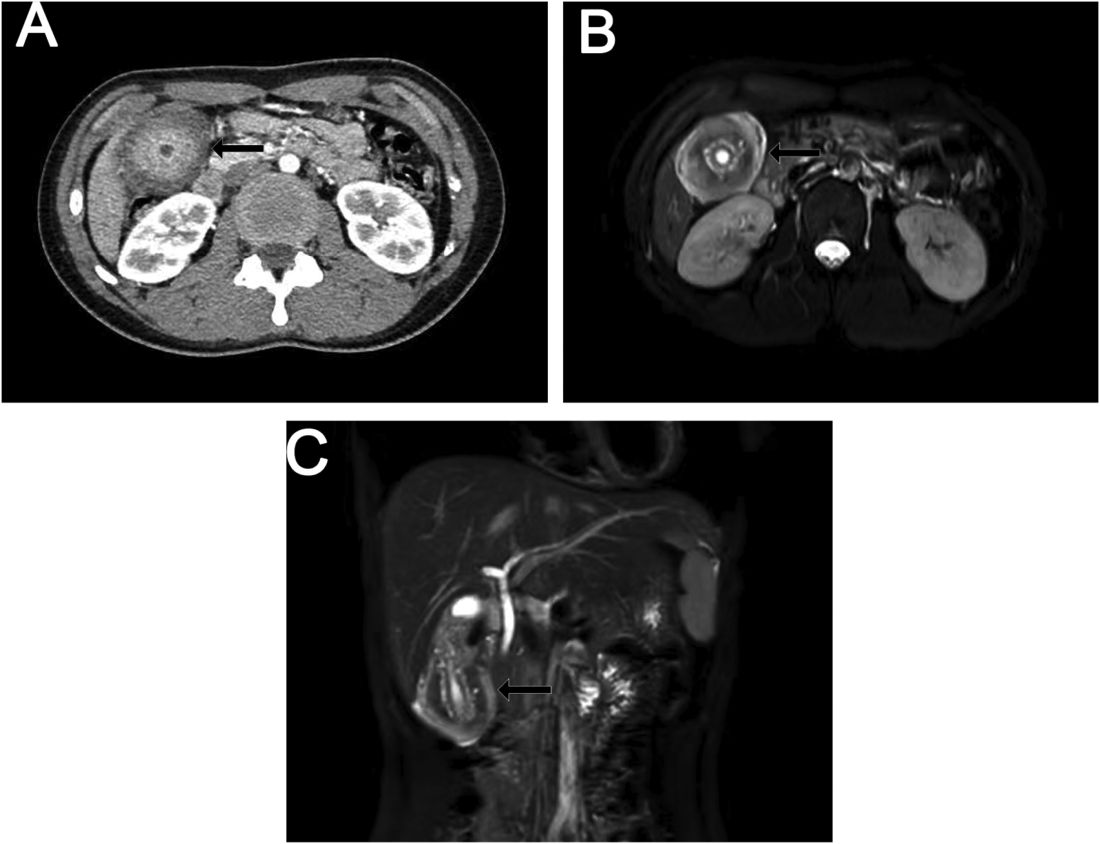
Ultrasound examination indicated gallbladder wall thickening. Furthermore, a contrast-enhanced computed tomographic scan showed marked gallbladder wall thickening with an annular unenhanced proliferative muscularis layer surrounding enhanced proliferative mucosal epithelium (Figure A), and magnetic resonance imaging showed multiple cyst-like spaces in the gallbladder wall (Figures B and C).
What is the diagnosis, and how should it be managed?
Previously published in Gastroenterology
Celiac disease: Update on diagnosis and monitoring
Celiac disease is a small bowel disorder. Specific antibodies along with a duodenal biopsy allow a secure diagnosis of celiac disease. Case detection rates have improved but many patients remain undiagnosed.
The only treatment available at present is a gluten-free diet (GFD). Most patients respond clinically to a GFD but histologic recovery is not always complete and may result in clinical consequences.
The anti-tissue transglutaminase IgA test (tTg-IgA) is the best initial serology test. A total IgA level appropriate for age is required to interpret a negative result. In patients with IgA deficiency, the deamidated gliadin peptide (DGP) antibodies, and/or tTg-IgA, may be helpful for diagnosis along with a duodenal biopsy.
First-degree female relatives with homozygous DQ2 positivity are at highest risk.
Both serology and duodenal biopsy have pitfalls in the diagnosis of celiac disease. In children, the diagnosis is secure with a tTg-IgA rate of at least 10 times the upper limit of normal (≥10×ULN) with positive endomysial antibodies (EMA).
There is less data on the correlation of tTg-IgA ≥10×ULN positive with villous atrophy in adults. All others require biopsy for diagnosis.
Considerations to forgo biopsy in adults include: tTg-IgA of ≥10×ULN positive, serology positive test in patients following GFD, or otherwise unable to undergo endoscopy with duodenal biopsy, or shared decision-making. Celiac disease recovery is assessed by clinical response to a GFD and antibody conversion to negative, which does not always correlate with histology.
Clinical consequences of persistent villous atrophy include increased risks for lymphoproliferative malignancy, hip fracture, and refractory celiac disease.
Dr. Semrad is director of the small bowel disease and nutrition program at the University of Chicago Medicine where she is a professor of medicine. She disclosed no conflicts of interest.
References
Rubio-Tapia et al. Am J Gastroenterol. 2023;118:59-76.
Husby S et al. J Pediatr Gastroenterol Nutr. 2020;70:141-57.
Celiac disease is a small bowel disorder. Specific antibodies along with a duodenal biopsy allow a secure diagnosis of celiac disease. Case detection rates have improved but many patients remain undiagnosed.
The only treatment available at present is a gluten-free diet (GFD). Most patients respond clinically to a GFD but histologic recovery is not always complete and may result in clinical consequences.
The anti-tissue transglutaminase IgA test (tTg-IgA) is the best initial serology test. A total IgA level appropriate for age is required to interpret a negative result. In patients with IgA deficiency, the deamidated gliadin peptide (DGP) antibodies, and/or tTg-IgA, may be helpful for diagnosis along with a duodenal biopsy.
First-degree female relatives with homozygous DQ2 positivity are at highest risk.
Both serology and duodenal biopsy have pitfalls in the diagnosis of celiac disease. In children, the diagnosis is secure with a tTg-IgA rate of at least 10 times the upper limit of normal (≥10×ULN) with positive endomysial antibodies (EMA).
There is less data on the correlation of tTg-IgA ≥10×ULN positive with villous atrophy in adults. All others require biopsy for diagnosis.
Considerations to forgo biopsy in adults include: tTg-IgA of ≥10×ULN positive, serology positive test in patients following GFD, or otherwise unable to undergo endoscopy with duodenal biopsy, or shared decision-making. Celiac disease recovery is assessed by clinical response to a GFD and antibody conversion to negative, which does not always correlate with histology.
Clinical consequences of persistent villous atrophy include increased risks for lymphoproliferative malignancy, hip fracture, and refractory celiac disease.
Dr. Semrad is director of the small bowel disease and nutrition program at the University of Chicago Medicine where she is a professor of medicine. She disclosed no conflicts of interest.
References
Rubio-Tapia et al. Am J Gastroenterol. 2023;118:59-76.
Husby S et al. J Pediatr Gastroenterol Nutr. 2020;70:141-57.
Celiac disease is a small bowel disorder. Specific antibodies along with a duodenal biopsy allow a secure diagnosis of celiac disease. Case detection rates have improved but many patients remain undiagnosed.
The only treatment available at present is a gluten-free diet (GFD). Most patients respond clinically to a GFD but histologic recovery is not always complete and may result in clinical consequences.
The anti-tissue transglutaminase IgA test (tTg-IgA) is the best initial serology test. A total IgA level appropriate for age is required to interpret a negative result. In patients with IgA deficiency, the deamidated gliadin peptide (DGP) antibodies, and/or tTg-IgA, may be helpful for diagnosis along with a duodenal biopsy.
First-degree female relatives with homozygous DQ2 positivity are at highest risk.
Both serology and duodenal biopsy have pitfalls in the diagnosis of celiac disease. In children, the diagnosis is secure with a tTg-IgA rate of at least 10 times the upper limit of normal (≥10×ULN) with positive endomysial antibodies (EMA).
There is less data on the correlation of tTg-IgA ≥10×ULN positive with villous atrophy in adults. All others require biopsy for diagnosis.
Considerations to forgo biopsy in adults include: tTg-IgA of ≥10×ULN positive, serology positive test in patients following GFD, or otherwise unable to undergo endoscopy with duodenal biopsy, or shared decision-making. Celiac disease recovery is assessed by clinical response to a GFD and antibody conversion to negative, which does not always correlate with histology.
Clinical consequences of persistent villous atrophy include increased risks for lymphoproliferative malignancy, hip fracture, and refractory celiac disease.
Dr. Semrad is director of the small bowel disease and nutrition program at the University of Chicago Medicine where she is a professor of medicine. She disclosed no conflicts of interest.
References
Rubio-Tapia et al. Am J Gastroenterol. 2023;118:59-76.
Husby S et al. J Pediatr Gastroenterol Nutr. 2020;70:141-57.
Advances in pancreaticobiliary disease interventions: More options and better outcomes
Highlights of advances in pancreaticobiliary disease interventions were reviewed at this year’s Digestive Disease Week (DDW) as part of the American Gastroenterological Association (AGA) postgraduate course.

Over the last several decades, the endoscopic treatment of pancreaticobiliary disease has advanced exponentially. Evidence-based advances are changing the landscape of pancreaticobiliary disease management.
While endoscopic retrograde cholangiopancreatography (ERCP) with transpapillary stent placement is first-line for the treatment of biliary obstruction, endoscopic ultrasound (EUS)-guided biliary drainage has emerged as an effective alternative in cases of failed ERCP. These procedures can be performed via a transhepatic approach (hepaticogastrostomy) from the proximal stomach, an extrahepatic approach (choledochoduodenostomy) from the duodenum, or via the gallbladder. Numerous studies have proved the safety and efficacy of these interventions in malignant biliary obstruction. A recent systematic meta-analysis pooled all of these approaches and concluded that EUS-guided biliary drainage is also reasonable to offer in benign disease when ERCP has failed or is not technically possible.
EUS-guided gallbladder drainage is similarly emerging as an alternative approach for management of acute cholecystitis. This is a reasonable option in patients with acute cholecystitis who are poor surgical candidates, have no evidence of gallbladder perforation, and will tolerate sedation. Moreover, this approach may be preferred over ERCP with cystic duct stent placement in the setting of a large stone burden, gastric outlet obstruction, or when an indwelling metal biliary stent occludes the cystic duct. Multidisciplinary discussion with surgical and interventional radiology services is essential, especially given this technique may preclude future cholecystectomy.
Indeterminate biliary strictures historically pose a major diagnostic challenge, and current approaches in the evaluation of such strictures lack diagnostic sensitivity. ERCP with concurrent brushing of the bile duct for cytology remains the most commonly used method of acquiring tissue. However, the sensitivity of diagnosis on brush cytology remains frustratingly low. Recent compelling evidence for increasing the number of brush passes to 30 in an indeterminate stricture improves diagnostic sensitivity and is a simple, safe, and low-cost intervention. This approach may ultimately decrease the number of patients requiring surgical intervention, which is particularly important when up to one-fifth of suspected biliary malignancies are found to be benign after surgical resection.
Not only have studies addressed increasing the diagnostic yield of stricture evaluation, but the treatment of biliary strictures has also evolved. Various stents are available, and different practice patterns have emerged for management of this entity. In an updated meta-analysis of randomized controlled trials evaluating multiple plastic stents versus a single covered metal stent for benign biliary strictures, no difference was found in stricture resolution, stricture recurrence, stent migration or adverse events. However, those patients treated with covered metal stents required fewer sessions of ERCP for stricture resolution. Moreover, no difference in stricture resolution was seen in subgroup analysis between anastomotic strictures, chronic pancreatitis, or bile duct injury. Despite higher cost of the stent itself, covered metal stents may ultimately lead to an overall decrease in health care expenditure.
The above examples are only a small subset of the progress that has been made in endoscopic management of pancreaticobiliary disease. The armamentarium of tools and techniques will continue to evolve to help us provide better minimally invasive care for our patients.
Dr. Schulman is associate professor in the division of gastroenterology and hepatology and the department of surgery at the University of Michigan. She is the incoming chief of endoscopy and the director of bariatric endoscopy. She disclosed consultancy work with Apollo Endosurgery, Boston Scientific, Olympus and MicroTech. She also disclosed research and grant support from GI Dynamics and Fractyl.
Highlights of advances in pancreaticobiliary disease interventions were reviewed at this year’s Digestive Disease Week (DDW) as part of the American Gastroenterological Association (AGA) postgraduate course.
Over the last several decades, the endoscopic treatment of pancreaticobiliary disease has advanced exponentially. Evidence-based advances are changing the landscape of pancreaticobiliary disease management.
While endoscopic retrograde cholangiopancreatography (ERCP) with transpapillary stent placement is first-line for the treatment of biliary obstruction, endoscopic ultrasound (EUS)-guided biliary drainage has emerged as an effective alternative in cases of failed ERCP. These procedures can be performed via a transhepatic approach (hepaticogastrostomy) from the proximal stomach, an extrahepatic approach (choledochoduodenostomy) from the duodenum, or via the gallbladder. Numerous studies have proved the safety and efficacy of these interventions in malignant biliary obstruction. A recent systematic meta-analysis pooled all of these approaches and concluded that EUS-guided biliary drainage is also reasonable to offer in benign disease when ERCP has failed or is not technically possible.
EUS-guided gallbladder drainage is similarly emerging as an alternative approach for management of acute cholecystitis. This is a reasonable option in patients with acute cholecystitis who are poor surgical candidates, have no evidence of gallbladder perforation, and will tolerate sedation. Moreover, this approach may be preferred over ERCP with cystic duct stent placement in the setting of a large stone burden, gastric outlet obstruction, or when an indwelling metal biliary stent occludes the cystic duct. Multidisciplinary discussion with surgical and interventional radiology services is essential, especially given this technique may preclude future cholecystectomy.
Indeterminate biliary strictures historically pose a major diagnostic challenge, and current approaches in the evaluation of such strictures lack diagnostic sensitivity. ERCP with concurrent brushing of the bile duct for cytology remains the most commonly used method of acquiring tissue. However, the sensitivity of diagnosis on brush cytology remains frustratingly low. Recent compelling evidence for increasing the number of brush passes to 30 in an indeterminate stricture improves diagnostic sensitivity and is a simple, safe, and low-cost intervention. This approach may ultimately decrease the number of patients requiring surgical intervention, which is particularly important when up to one-fifth of suspected biliary malignancies are found to be benign after surgical resection.
Not only have studies addressed increasing the diagnostic yield of stricture evaluation, but the treatment of biliary strictures has also evolved. Various stents are available, and different practice patterns have emerged for management of this entity. In an updated meta-analysis of randomized controlled trials evaluating multiple plastic stents versus a single covered metal stent for benign biliary strictures, no difference was found in stricture resolution, stricture recurrence, stent migration or adverse events. However, those patients treated with covered metal stents required fewer sessions of ERCP for stricture resolution. Moreover, no difference in stricture resolution was seen in subgroup analysis between anastomotic strictures, chronic pancreatitis, or bile duct injury. Despite higher cost of the stent itself, covered metal stents may ultimately lead to an overall decrease in health care expenditure.
The above examples are only a small subset of the progress that has been made in endoscopic management of pancreaticobiliary disease. The armamentarium of tools and techniques will continue to evolve to help us provide better minimally invasive care for our patients.
Dr. Schulman is associate professor in the division of gastroenterology and hepatology and the department of surgery at the University of Michigan. She is the incoming chief of endoscopy and the director of bariatric endoscopy. She disclosed consultancy work with Apollo Endosurgery, Boston Scientific, Olympus and MicroTech. She also disclosed research and grant support from GI Dynamics and Fractyl.
Highlights of advances in pancreaticobiliary disease interventions were reviewed at this year’s Digestive Disease Week (DDW) as part of the American Gastroenterological Association (AGA) postgraduate course.
Over the last several decades, the endoscopic treatment of pancreaticobiliary disease has advanced exponentially. Evidence-based advances are changing the landscape of pancreaticobiliary disease management.
While endoscopic retrograde cholangiopancreatography (ERCP) with transpapillary stent placement is first-line for the treatment of biliary obstruction, endoscopic ultrasound (EUS)-guided biliary drainage has emerged as an effective alternative in cases of failed ERCP. These procedures can be performed via a transhepatic approach (hepaticogastrostomy) from the proximal stomach, an extrahepatic approach (choledochoduodenostomy) from the duodenum, or via the gallbladder. Numerous studies have proved the safety and efficacy of these interventions in malignant biliary obstruction. A recent systematic meta-analysis pooled all of these approaches and concluded that EUS-guided biliary drainage is also reasonable to offer in benign disease when ERCP has failed or is not technically possible.
EUS-guided gallbladder drainage is similarly emerging as an alternative approach for management of acute cholecystitis. This is a reasonable option in patients with acute cholecystitis who are poor surgical candidates, have no evidence of gallbladder perforation, and will tolerate sedation. Moreover, this approach may be preferred over ERCP with cystic duct stent placement in the setting of a large stone burden, gastric outlet obstruction, or when an indwelling metal biliary stent occludes the cystic duct. Multidisciplinary discussion with surgical and interventional radiology services is essential, especially given this technique may preclude future cholecystectomy.
Indeterminate biliary strictures historically pose a major diagnostic challenge, and current approaches in the evaluation of such strictures lack diagnostic sensitivity. ERCP with concurrent brushing of the bile duct for cytology remains the most commonly used method of acquiring tissue. However, the sensitivity of diagnosis on brush cytology remains frustratingly low. Recent compelling evidence for increasing the number of brush passes to 30 in an indeterminate stricture improves diagnostic sensitivity and is a simple, safe, and low-cost intervention. This approach may ultimately decrease the number of patients requiring surgical intervention, which is particularly important when up to one-fifth of suspected biliary malignancies are found to be benign after surgical resection.
Not only have studies addressed increasing the diagnostic yield of stricture evaluation, but the treatment of biliary strictures has also evolved. Various stents are available, and different practice patterns have emerged for management of this entity. In an updated meta-analysis of randomized controlled trials evaluating multiple plastic stents versus a single covered metal stent for benign biliary strictures, no difference was found in stricture resolution, stricture recurrence, stent migration or adverse events. However, those patients treated with covered metal stents required fewer sessions of ERCP for stricture resolution. Moreover, no difference in stricture resolution was seen in subgroup analysis between anastomotic strictures, chronic pancreatitis, or bile duct injury. Despite higher cost of the stent itself, covered metal stents may ultimately lead to an overall decrease in health care expenditure.
The above examples are only a small subset of the progress that has been made in endoscopic management of pancreaticobiliary disease. The armamentarium of tools and techniques will continue to evolve to help us provide better minimally invasive care for our patients.
Dr. Schulman is associate professor in the division of gastroenterology and hepatology and the department of surgery at the University of Michigan. She is the incoming chief of endoscopy and the director of bariatric endoscopy. She disclosed consultancy work with Apollo Endosurgery, Boston Scientific, Olympus and MicroTech. She also disclosed research and grant support from GI Dynamics and Fractyl.
Conflicting blood pressure targets: Déjà vu all over again
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.