User login
Bempedoic acid cuts CV events in statin-intolerant patients: CLEAR Outcomes
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.

“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.
“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.
“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
At 5 years, TAVI valves perform better than surgical ones
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.

The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”

A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.
The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”
A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.
The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”
A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
FROM CRT 2023
Risk of stent infection low, but may be underreported
Infections of coronary stents appear to be uncommon, but it is not clear if they are often missed, underreported, or truly rare, according to a new analysis.
In a search of multiple databases, 79 cases of coronary stent infections (CSI) were found in 65 published reports, according to Venkatakrishnan Ramakumar, MBBS, MD, department of cardiology, All India Institute of Medical Sciences, New Delhi.

Over the period of evaluation, which had no defined starting point but stretched to November 2021, the 79 infections reported worldwide occurred when millions of percutaneous coronary intervention (PCI) procedures were performed. In the United States alone, the current estimated annual number of PCIs is 600,000, according to an article published in the Journal of the American Heart Association.
If the number of reported CSI cases represented even a modest fraction of those that occurred, the risk would still be almost negligible. Yet, Dr. Ramakumar insisted that there has been little attention paid to the potential for CSI, creating a situation in which many or almost all cases are simply being missed.
“We do not know how many infections have gone unrecognized,” Dr. Ramakumar said in presenting his results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute. And even if they are identified and promptly treated, there “is the potential for a publication bias,” he added, referring to the reluctance of investigators to submit and publishers to accept manuscripts with negative results.
Regardless of the frequency with which they occur, CSI is associated with bad outcomes, according to the data evaluated by Dr. Ramakumar. On the basis of in-hospital mortality, the primary endpoint of this analysis, the rate of death in patients developing CSI was 30.3%.
Successful treatment varied by hospital type
This risk was not uniform. Rather, rates of in-hospital mortality and proportion of patients treated successfully varied substantially by type of hospital. At private teaching hospitals for example, successful treatment – whether medical alone or followed by bailout surgery – was 80%. The rates fell to 40% at public teaching hospitals and then to 25% at private nonteaching hospitals.
The full-text articles included in this analysis were evaluated and selected by two reviewers working independently. A CSI diagnosis made clinically or with imaging and treatment outcomes were among criteria for the case studies to be included. Dr. Ramakumar said the study, which he claimed is the largest systematic review of CSI ever conducted, has been registered with PROSPERO, an international prospective registry of systematic reviews.
The presenting symptom was fever in 72% of cases and chest pain in the others, although there was one asymptomatic CSI reported. On angiography, 62% had a concomitant mycotic aneurysm. Intramyocardial abscess (13.9%), rupture (11.3%), and coronary fistula (7.5%) were also common findings, but no angiographic abnormalities could be identified in 53% of patients.
Following PCI, most CSI developed within 8 days (43%) or the first month (23%), but CSI was reported more than 6 months after the procedure in 19%. Complex PCI accounted for 51% of cases. Of stent types, 56% were drug eluting and 13% were bare metal.
When comparing characteristics of those who survived CSI with those who did not, most (89%) of those with a non–ST-segment elevated acute coronary syndrome ultimately survived, while survival from CSI in those with structural heart disease was only 17%.
Microbiological findings were not a criterion for study inclusion, but Staphylococcus species accounted for 65% of the infections for which positive cultures were reported. Pseudomonas accounted for 13%. Less than 4% (3.8%) tested positive for multiple pathogens. A small proportion of patients had unusual infectious organisms.
As part of this analysis, the investigators developed an artificial intelligence model to predict CSI based on patient characteristics and other variables. However, the specificity of only around 70% led Dr. Ramakumar to conclude that it does not yet have practical value.
However, he believes that better methodology to detect CSI is needed, and he proposed a diagnostic algorithm that he believes would both improve detection rates and accelerate the time to diagnosis.
Algorithm proposed for detection of CSI
In this algorithm, the first step in symptomatic patients with a positive blood culture suspected of CSI is imaging, such as transthoracic echocardiography, to identify features of infective endocarditis or endarteritis. If the imaging is positive, further imaging, such as PET, that supports the diagnosis, should be adequate to support a diagnosis and treatment.
If initial imaging is negative, alternative diagnoses should be considered, but Dr. Ramakumar advised repeat imaging after 48 hours if symptoms persist and no other causes are found.
Dr. Ramakumar acknowledged the many limitations of this analysis, including the small sample size and the challenges of assembling coherent data from case reports with variable types of information submitted during different eras of PCI evolution. However, reiterating that CSI might be frequently missed, he emphasized that this problem might be bigger than currently understood.
It is difficult to rule out any possibility that CSI is frequently missed, but Andrew Sharp, MD, PhD, a consultant interventional cardiologist at the University Hospital of Wales, Cardiff, is skeptical.
“One might think this is a potential problem, but I cannot think of one patient in whom this has occurred,” Dr. Sharp said in an interview. He is fairly confident that they are extremely rare.
“When there is infection associated with a foreign body, such as a pacemaker, they do not typically resolve by themselves,” he explained. “Often the device has to be removed. If this was true for CSI, then I think we would be aware of these complications.”
However, he praised the investigators for taking a look at CSI in a systematic approach. An invited panelist during the CRT featured research, which is where these data were presented, Dr. Sharp was more interested in understanding why they do not occur now that data are available to suggest they are rare.
“Is there something in the coronary environment, such as the consistent blood flow, that protects against infection?” he asked. CSI is a valid area of further research, according to Dr. Sharp, but he does not consider infected stents to be a common threat based on his own sizable case series.
Dr. Ramakumar and Dr. Sharp reported no potential conflicts of interest.
Infections of coronary stents appear to be uncommon, but it is not clear if they are often missed, underreported, or truly rare, according to a new analysis.
In a search of multiple databases, 79 cases of coronary stent infections (CSI) were found in 65 published reports, according to Venkatakrishnan Ramakumar, MBBS, MD, department of cardiology, All India Institute of Medical Sciences, New Delhi.
Over the period of evaluation, which had no defined starting point but stretched to November 2021, the 79 infections reported worldwide occurred when millions of percutaneous coronary intervention (PCI) procedures were performed. In the United States alone, the current estimated annual number of PCIs is 600,000, according to an article published in the Journal of the American Heart Association.
If the number of reported CSI cases represented even a modest fraction of those that occurred, the risk would still be almost negligible. Yet, Dr. Ramakumar insisted that there has been little attention paid to the potential for CSI, creating a situation in which many or almost all cases are simply being missed.
“We do not know how many infections have gone unrecognized,” Dr. Ramakumar said in presenting his results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute. And even if they are identified and promptly treated, there “is the potential for a publication bias,” he added, referring to the reluctance of investigators to submit and publishers to accept manuscripts with negative results.
Regardless of the frequency with which they occur, CSI is associated with bad outcomes, according to the data evaluated by Dr. Ramakumar. On the basis of in-hospital mortality, the primary endpoint of this analysis, the rate of death in patients developing CSI was 30.3%.
Successful treatment varied by hospital type
This risk was not uniform. Rather, rates of in-hospital mortality and proportion of patients treated successfully varied substantially by type of hospital. At private teaching hospitals for example, successful treatment – whether medical alone or followed by bailout surgery – was 80%. The rates fell to 40% at public teaching hospitals and then to 25% at private nonteaching hospitals.
The full-text articles included in this analysis were evaluated and selected by two reviewers working independently. A CSI diagnosis made clinically or with imaging and treatment outcomes were among criteria for the case studies to be included. Dr. Ramakumar said the study, which he claimed is the largest systematic review of CSI ever conducted, has been registered with PROSPERO, an international prospective registry of systematic reviews.
The presenting symptom was fever in 72% of cases and chest pain in the others, although there was one asymptomatic CSI reported. On angiography, 62% had a concomitant mycotic aneurysm. Intramyocardial abscess (13.9%), rupture (11.3%), and coronary fistula (7.5%) were also common findings, but no angiographic abnormalities could be identified in 53% of patients.
Following PCI, most CSI developed within 8 days (43%) or the first month (23%), but CSI was reported more than 6 months after the procedure in 19%. Complex PCI accounted for 51% of cases. Of stent types, 56% were drug eluting and 13% were bare metal.
When comparing characteristics of those who survived CSI with those who did not, most (89%) of those with a non–ST-segment elevated acute coronary syndrome ultimately survived, while survival from CSI in those with structural heart disease was only 17%.
Microbiological findings were not a criterion for study inclusion, but Staphylococcus species accounted for 65% of the infections for which positive cultures were reported. Pseudomonas accounted for 13%. Less than 4% (3.8%) tested positive for multiple pathogens. A small proportion of patients had unusual infectious organisms.
As part of this analysis, the investigators developed an artificial intelligence model to predict CSI based on patient characteristics and other variables. However, the specificity of only around 70% led Dr. Ramakumar to conclude that it does not yet have practical value.
However, he believes that better methodology to detect CSI is needed, and he proposed a diagnostic algorithm that he believes would both improve detection rates and accelerate the time to diagnosis.
Algorithm proposed for detection of CSI
In this algorithm, the first step in symptomatic patients with a positive blood culture suspected of CSI is imaging, such as transthoracic echocardiography, to identify features of infective endocarditis or endarteritis. If the imaging is positive, further imaging, such as PET, that supports the diagnosis, should be adequate to support a diagnosis and treatment.
If initial imaging is negative, alternative diagnoses should be considered, but Dr. Ramakumar advised repeat imaging after 48 hours if symptoms persist and no other causes are found.
Dr. Ramakumar acknowledged the many limitations of this analysis, including the small sample size and the challenges of assembling coherent data from case reports with variable types of information submitted during different eras of PCI evolution. However, reiterating that CSI might be frequently missed, he emphasized that this problem might be bigger than currently understood.
It is difficult to rule out any possibility that CSI is frequently missed, but Andrew Sharp, MD, PhD, a consultant interventional cardiologist at the University Hospital of Wales, Cardiff, is skeptical.
“One might think this is a potential problem, but I cannot think of one patient in whom this has occurred,” Dr. Sharp said in an interview. He is fairly confident that they are extremely rare.
“When there is infection associated with a foreign body, such as a pacemaker, they do not typically resolve by themselves,” he explained. “Often the device has to be removed. If this was true for CSI, then I think we would be aware of these complications.”
However, he praised the investigators for taking a look at CSI in a systematic approach. An invited panelist during the CRT featured research, which is where these data were presented, Dr. Sharp was more interested in understanding why they do not occur now that data are available to suggest they are rare.
“Is there something in the coronary environment, such as the consistent blood flow, that protects against infection?” he asked. CSI is a valid area of further research, according to Dr. Sharp, but he does not consider infected stents to be a common threat based on his own sizable case series.
Dr. Ramakumar and Dr. Sharp reported no potential conflicts of interest.
Infections of coronary stents appear to be uncommon, but it is not clear if they are often missed, underreported, or truly rare, according to a new analysis.
In a search of multiple databases, 79 cases of coronary stent infections (CSI) were found in 65 published reports, according to Venkatakrishnan Ramakumar, MBBS, MD, department of cardiology, All India Institute of Medical Sciences, New Delhi.
Over the period of evaluation, which had no defined starting point but stretched to November 2021, the 79 infections reported worldwide occurred when millions of percutaneous coronary intervention (PCI) procedures were performed. In the United States alone, the current estimated annual number of PCIs is 600,000, according to an article published in the Journal of the American Heart Association.
If the number of reported CSI cases represented even a modest fraction of those that occurred, the risk would still be almost negligible. Yet, Dr. Ramakumar insisted that there has been little attention paid to the potential for CSI, creating a situation in which many or almost all cases are simply being missed.
“We do not know how many infections have gone unrecognized,” Dr. Ramakumar said in presenting his results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute. And even if they are identified and promptly treated, there “is the potential for a publication bias,” he added, referring to the reluctance of investigators to submit and publishers to accept manuscripts with negative results.
Regardless of the frequency with which they occur, CSI is associated with bad outcomes, according to the data evaluated by Dr. Ramakumar. On the basis of in-hospital mortality, the primary endpoint of this analysis, the rate of death in patients developing CSI was 30.3%.
Successful treatment varied by hospital type
This risk was not uniform. Rather, rates of in-hospital mortality and proportion of patients treated successfully varied substantially by type of hospital. At private teaching hospitals for example, successful treatment – whether medical alone or followed by bailout surgery – was 80%. The rates fell to 40% at public teaching hospitals and then to 25% at private nonteaching hospitals.
The full-text articles included in this analysis were evaluated and selected by two reviewers working independently. A CSI diagnosis made clinically or with imaging and treatment outcomes were among criteria for the case studies to be included. Dr. Ramakumar said the study, which he claimed is the largest systematic review of CSI ever conducted, has been registered with PROSPERO, an international prospective registry of systematic reviews.
The presenting symptom was fever in 72% of cases and chest pain in the others, although there was one asymptomatic CSI reported. On angiography, 62% had a concomitant mycotic aneurysm. Intramyocardial abscess (13.9%), rupture (11.3%), and coronary fistula (7.5%) were also common findings, but no angiographic abnormalities could be identified in 53% of patients.
Following PCI, most CSI developed within 8 days (43%) or the first month (23%), but CSI was reported more than 6 months after the procedure in 19%. Complex PCI accounted for 51% of cases. Of stent types, 56% were drug eluting and 13% were bare metal.
When comparing characteristics of those who survived CSI with those who did not, most (89%) of those with a non–ST-segment elevated acute coronary syndrome ultimately survived, while survival from CSI in those with structural heart disease was only 17%.
Microbiological findings were not a criterion for study inclusion, but Staphylococcus species accounted for 65% of the infections for which positive cultures were reported. Pseudomonas accounted for 13%. Less than 4% (3.8%) tested positive for multiple pathogens. A small proportion of patients had unusual infectious organisms.
As part of this analysis, the investigators developed an artificial intelligence model to predict CSI based on patient characteristics and other variables. However, the specificity of only around 70% led Dr. Ramakumar to conclude that it does not yet have practical value.
However, he believes that better methodology to detect CSI is needed, and he proposed a diagnostic algorithm that he believes would both improve detection rates and accelerate the time to diagnosis.
Algorithm proposed for detection of CSI
In this algorithm, the first step in symptomatic patients with a positive blood culture suspected of CSI is imaging, such as transthoracic echocardiography, to identify features of infective endocarditis or endarteritis. If the imaging is positive, further imaging, such as PET, that supports the diagnosis, should be adequate to support a diagnosis and treatment.
If initial imaging is negative, alternative diagnoses should be considered, but Dr. Ramakumar advised repeat imaging after 48 hours if symptoms persist and no other causes are found.
Dr. Ramakumar acknowledged the many limitations of this analysis, including the small sample size and the challenges of assembling coherent data from case reports with variable types of information submitted during different eras of PCI evolution. However, reiterating that CSI might be frequently missed, he emphasized that this problem might be bigger than currently understood.
It is difficult to rule out any possibility that CSI is frequently missed, but Andrew Sharp, MD, PhD, a consultant interventional cardiologist at the University Hospital of Wales, Cardiff, is skeptical.
“One might think this is a potential problem, but I cannot think of one patient in whom this has occurred,” Dr. Sharp said in an interview. He is fairly confident that they are extremely rare.
“When there is infection associated with a foreign body, such as a pacemaker, they do not typically resolve by themselves,” he explained. “Often the device has to be removed. If this was true for CSI, then I think we would be aware of these complications.”
However, he praised the investigators for taking a look at CSI in a systematic approach. An invited panelist during the CRT featured research, which is where these data were presented, Dr. Sharp was more interested in understanding why they do not occur now that data are available to suggest they are rare.
“Is there something in the coronary environment, such as the consistent blood flow, that protects against infection?” he asked. CSI is a valid area of further research, according to Dr. Sharp, but he does not consider infected stents to be a common threat based on his own sizable case series.
Dr. Ramakumar and Dr. Sharp reported no potential conflicts of interest.
FROM CRT 2023
500 more steps a day tied to 14% lower CVD risk in older adults
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.

The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
FROM EPI/LIFESTYLE 2023
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.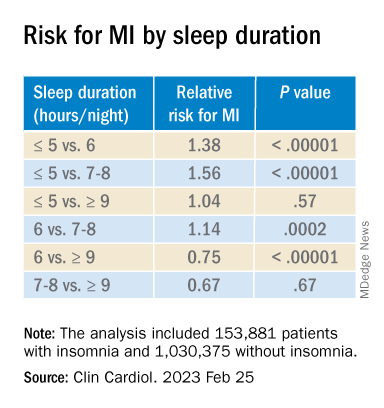
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Artificial sweetener in ‘keto foods’ tied to cardiovascular risk
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
New AHA statement urges focus on CV risk before pregnancy
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
In weighing PCI vs. CABG for left main disease, diabetes matters
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.

Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
AT CRT 2023
Drinking beet juice tied to reduced post-PCI restenosis
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
AT CRT 2023
A doctor must go to extremes to save a choking victim
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.