User login
Treating the unvaccinated
The following is not anything I’m doing. It’s written solely as a thought exercise.
I don’t think it’s illegal, any more than if I refused to see smokers, or gum chewers. I mean, it’s my practice. I’m the only one here.
It’s certainly unethical, though. Part of being a doctor is caring for those who need our help. I’m vaccinated, so hopefully I’m at lower risk of getting sick if exposed. But that’s not a guarantee.
The vaccine is 95% effective. But that still means 1 in 20 vaccinated people can still contract the disease. Of course, people who aren’t vaccinated have no protection at all, aside from their immune system.
If the decision to not vaccinate, or not wear a mask, only affected themselves, I wouldn’t have as much of an issue with it. Like bungee jumping, the consequences of something going wrong affect only the person who made the choice (not including costs to the health care system or loved ones, now caretakers).
But with an easily spread infectious disease, a better analogy is probably that of drunk drivers. Their actions affect not only themselves, but everyone else on (or near) the road: other drivers, their passengers, pedestrians. ...
In a neurology practice not all of my patients have great immune systems. Sure, there are healthy migraine patients, but I also see patients with multiple sclerosis (on drugs like Ocrevus), patients with myasthenia gravis (on steroids or Imuran), and other folks whose survival depends on keeping their immune systems working at a suboptimal level. Not to mention those with malignancies, leukemias, and lymphomas.
These people have no real defense against the virus, and many of them can’t even get the vaccine. They depend on precautions, herd immunity, and luck. So, to protect them, maybe I should keep the unvaccinated out. Granted, this isn’t a guarantee, either, and doesn’t protect them during more mundane activities, such as grocery shopping or filling up their car.
Besides, the unvaccinated have their own, unrelated, neurological issues. Migraines, seizures, neuropathy, and so they need to see me. My job is to help anyone who needs me. Isn’t that what being a doctor is all about?
It’s an interesting question. Like most things in medicine, there is no black or white, just different shades of gray.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The following is not anything I’m doing. It’s written solely as a thought exercise.
I don’t think it’s illegal, any more than if I refused to see smokers, or gum chewers. I mean, it’s my practice. I’m the only one here.
It’s certainly unethical, though. Part of being a doctor is caring for those who need our help. I’m vaccinated, so hopefully I’m at lower risk of getting sick if exposed. But that’s not a guarantee.
The vaccine is 95% effective. But that still means 1 in 20 vaccinated people can still contract the disease. Of course, people who aren’t vaccinated have no protection at all, aside from their immune system.
If the decision to not vaccinate, or not wear a mask, only affected themselves, I wouldn’t have as much of an issue with it. Like bungee jumping, the consequences of something going wrong affect only the person who made the choice (not including costs to the health care system or loved ones, now caretakers).
But with an easily spread infectious disease, a better analogy is probably that of drunk drivers. Their actions affect not only themselves, but everyone else on (or near) the road: other drivers, their passengers, pedestrians. ...
In a neurology practice not all of my patients have great immune systems. Sure, there are healthy migraine patients, but I also see patients with multiple sclerosis (on drugs like Ocrevus), patients with myasthenia gravis (on steroids or Imuran), and other folks whose survival depends on keeping their immune systems working at a suboptimal level. Not to mention those with malignancies, leukemias, and lymphomas.
These people have no real defense against the virus, and many of them can’t even get the vaccine. They depend on precautions, herd immunity, and luck. So, to protect them, maybe I should keep the unvaccinated out. Granted, this isn’t a guarantee, either, and doesn’t protect them during more mundane activities, such as grocery shopping or filling up their car.
Besides, the unvaccinated have their own, unrelated, neurological issues. Migraines, seizures, neuropathy, and so they need to see me. My job is to help anyone who needs me. Isn’t that what being a doctor is all about?
It’s an interesting question. Like most things in medicine, there is no black or white, just different shades of gray.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The following is not anything I’m doing. It’s written solely as a thought exercise.
I don’t think it’s illegal, any more than if I refused to see smokers, or gum chewers. I mean, it’s my practice. I’m the only one here.
It’s certainly unethical, though. Part of being a doctor is caring for those who need our help. I’m vaccinated, so hopefully I’m at lower risk of getting sick if exposed. But that’s not a guarantee.
The vaccine is 95% effective. But that still means 1 in 20 vaccinated people can still contract the disease. Of course, people who aren’t vaccinated have no protection at all, aside from their immune system.
If the decision to not vaccinate, or not wear a mask, only affected themselves, I wouldn’t have as much of an issue with it. Like bungee jumping, the consequences of something going wrong affect only the person who made the choice (not including costs to the health care system or loved ones, now caretakers).
But with an easily spread infectious disease, a better analogy is probably that of drunk drivers. Their actions affect not only themselves, but everyone else on (or near) the road: other drivers, their passengers, pedestrians. ...
In a neurology practice not all of my patients have great immune systems. Sure, there are healthy migraine patients, but I also see patients with multiple sclerosis (on drugs like Ocrevus), patients with myasthenia gravis (on steroids or Imuran), and other folks whose survival depends on keeping their immune systems working at a suboptimal level. Not to mention those with malignancies, leukemias, and lymphomas.
These people have no real defense against the virus, and many of them can’t even get the vaccine. They depend on precautions, herd immunity, and luck. So, to protect them, maybe I should keep the unvaccinated out. Granted, this isn’t a guarantee, either, and doesn’t protect them during more mundane activities, such as grocery shopping or filling up their car.
Besides, the unvaccinated have their own, unrelated, neurological issues. Migraines, seizures, neuropathy, and so they need to see me. My job is to help anyone who needs me. Isn’t that what being a doctor is all about?
It’s an interesting question. Like most things in medicine, there is no black or white, just different shades of gray.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Surgeon marks ‘right’ instead of ‘left’ testicle, then operates
Wrong-site surgery
Florida regulators have imposed a fine and other measures on a Tampa doctor who made a crucial error prior to his patient’s testicular surgery, as a story in the Miami Herald, among other news sites, reports.
On Sept. 10, 2019, a patient referred to in state documents as “C.F.” showed up for a procedure – a varicocelectomy – that would remove the enlarged veins in his left testicle. His doctor that day was Raul Fernandez-Crespo, MD, a urologist who had been licensed to practice in Florida since April of the same year. Dr. Fernandez-Crespo completed his urology residency at the University of Puerto Rico in 2019.
Following a conversation with C.F., Dr. Fernandez-Crespo designated what he believed was the proper surgical site – his patient’s right testicle.
He then proceeded to operate, but at some point during the procedure – news accounts don’t make clear when or how he became aware of his error – he realized C.F. had actually consented to a left-testicle varicocelectomy. With his patient still sedated, Dr. Fernandez-Crespo also completed the second procedure.
His mistake came to the attention of the Department of Health, which filed an administrative complaint against the surgeon. On June 17, 2021, the department’s medical licensing body, the Florida Board of Medicine, handed down its final order about the case.
In addition to imposing a $2,500 fine on Dr. Fernandez-Crespo and issuing “a letter of concern” – a public document that can be used as evidence in any relevant future disciplinary action against him – regulators said the surgeon must reimburse $2,045.56 to the department for its case-related administrative costs; take a 5-hour CME course in risk management or attend 8 hours of board disciplinary hearings; and, finally, give a 1-hour lecture on wrong-site surgeries at a board-approved medical facility.
Before this, Dr. Fernandez-Crespo had no previous disciplinary history with the Florida Board of Medicine.
Huge judgment after fertility procedure goes wrong
A Connecticut couple whose fertility and prenatal care at a state university health center proved disastrous will receive millions of dollars in damages, according to a report in the Hartford Courant.
In 2014, Jean-Marie Monroe-Lynch and her husband, Aaron Lynch, went to UConn Health, in Farmington, for treatment of Jean-Marie’s infertility. Her care was overseen by the Center for Advanced Reproductive Services (CARS), a private company then under contract with UConn Health. (The contract, which ended in 2014, obligated UConn to provide CARS providers with medical malpractice coverage.)
There, Jean-Marie was inseminated with sperm from a donor who turned out to be a carrier for cytomegalovirus (CMV), the herpes virus that can cause severe birth defects, or fetal death, when contracted by a pregnant woman. The insemination resulted in a twin pregnancy, a boy and a girl. The girl, Shay, died in utero after several of her organs became infected with CMV; the boy, Joshua, was born with severe mental and physical disabilities.
In their suit, Ms. Monroe-Lynch and her husband alleged that they were never cautioned about the risks associated with using a sperm donor whose blood had tested positive for CMV antibodies. Their suit further alleged that, at the 20-week ultrasound, UConn’s prenatal team failed to detect evidence of congenital CMV infection and again failed, at the 22-week ultrasound, to properly recognize and respond to abnormal findings.
“They totally dropped the ball,” said the couple’s attorney. “If you’re a pregnant woman and contract the virus for the first time, the results can be devastating.”
CARS disputes this conclusion, arguing that the plaintiffs failed to prove as a “matter of scientific fact” that Ms. Monroe-Lynch was infected with CMV as the result of her intrauterine insemination.
But Superior Court Judge Mark H. Taylor disagreed. In his 107-page ruling, he said that the court “agrees with the vast majority of superior courts, concluding that a physician providing obstetric care owes a direct duty to a mother to prevent harm to her child during gestation and delivery.”
Jean-Marie Monroe-Lynch and Aaron Lynch received a $37.6 million award, consisting of $24.1 million in economic damages and $13.5 million in noneconomic damages.
Their surviving child, Joshua, will reportedly require a lifetime of medical and other care. In the meantime, UConn Health vows to appeal the Superior Court’s decision.
COVID patient’s relative demands justice for fatal outcome
An Indiana man whose grandfather recently died after suffering a stroke is calling on state lawmakers to rethink legislation passed earlier this year to protect health care providers during the COVID-19 pandemic, according to a story reported by CBS4Indy.
Late last year, Daniel Enlow’s 83-year-old grandfather, Edward Rigney, was checked into Eskenazi Hospital, in Indianapolis. Mr. Rigney suffered from COPD and had also been diagnosed with COVID-19.
At some point during his hospitalization, medical staff attempted to place what seems to have been an arterial line in order to monitor his condition. During the procedure, or at some point shortly thereafter, an “iatrogenic air embolus” was released into his veins and caused a stroke, according to medical records and Mr. Rigney’s death certificate.
“I started asking for medical records because I wanted to know what was happening leading up to it in black and white in front of me,” said Mr. Enlow, who wished to present his evidence to a medical review panel, as required by Indiana law. The first step in this process would have been to consult with a medical malpractice attorney, but several declined to take his case.
Why? Because a pair of bills passed by Indiana legislators in early 2021 make COVID-19–related suits – even tangentially related ones – potentially difficult to take to court.
The bills raised the bar to file a medical malpractice claim in COVID-19 cases and to allow only those that involve “gross negligence or willful or wanton misconduct.”
“In the vast majority of cases, it’s impossible to prove that,” said Fred Schultz, immediate past president of the Indiana Trial Lawyers Association, who lobbied against the legislation.
The bills were never designed to offer “blanket freedom,” said GOP State Senator Aaron Freeman, sponsor of one of the bills. “If something is being used in a way that it is a complete bar to certain claims, then maybe we need to go back and look at it and open that up a little bit and make it less restrictive. I’m certainly open to having those conversations.”
Meanwhile, Mr. Enlow has vowed to keep pushing in the name of his late grandfather. The hospital’s parent company, Eskenazi Health, has declined to comment.
A version of this article first appeared on Medscape.com.
Wrong-site surgery
Florida regulators have imposed a fine and other measures on a Tampa doctor who made a crucial error prior to his patient’s testicular surgery, as a story in the Miami Herald, among other news sites, reports.
On Sept. 10, 2019, a patient referred to in state documents as “C.F.” showed up for a procedure – a varicocelectomy – that would remove the enlarged veins in his left testicle. His doctor that day was Raul Fernandez-Crespo, MD, a urologist who had been licensed to practice in Florida since April of the same year. Dr. Fernandez-Crespo completed his urology residency at the University of Puerto Rico in 2019.
Following a conversation with C.F., Dr. Fernandez-Crespo designated what he believed was the proper surgical site – his patient’s right testicle.
He then proceeded to operate, but at some point during the procedure – news accounts don’t make clear when or how he became aware of his error – he realized C.F. had actually consented to a left-testicle varicocelectomy. With his patient still sedated, Dr. Fernandez-Crespo also completed the second procedure.
His mistake came to the attention of the Department of Health, which filed an administrative complaint against the surgeon. On June 17, 2021, the department’s medical licensing body, the Florida Board of Medicine, handed down its final order about the case.
In addition to imposing a $2,500 fine on Dr. Fernandez-Crespo and issuing “a letter of concern” – a public document that can be used as evidence in any relevant future disciplinary action against him – regulators said the surgeon must reimburse $2,045.56 to the department for its case-related administrative costs; take a 5-hour CME course in risk management or attend 8 hours of board disciplinary hearings; and, finally, give a 1-hour lecture on wrong-site surgeries at a board-approved medical facility.
Before this, Dr. Fernandez-Crespo had no previous disciplinary history with the Florida Board of Medicine.
Huge judgment after fertility procedure goes wrong
A Connecticut couple whose fertility and prenatal care at a state university health center proved disastrous will receive millions of dollars in damages, according to a report in the Hartford Courant.
In 2014, Jean-Marie Monroe-Lynch and her husband, Aaron Lynch, went to UConn Health, in Farmington, for treatment of Jean-Marie’s infertility. Her care was overseen by the Center for Advanced Reproductive Services (CARS), a private company then under contract with UConn Health. (The contract, which ended in 2014, obligated UConn to provide CARS providers with medical malpractice coverage.)
There, Jean-Marie was inseminated with sperm from a donor who turned out to be a carrier for cytomegalovirus (CMV), the herpes virus that can cause severe birth defects, or fetal death, when contracted by a pregnant woman. The insemination resulted in a twin pregnancy, a boy and a girl. The girl, Shay, died in utero after several of her organs became infected with CMV; the boy, Joshua, was born with severe mental and physical disabilities.
In their suit, Ms. Monroe-Lynch and her husband alleged that they were never cautioned about the risks associated with using a sperm donor whose blood had tested positive for CMV antibodies. Their suit further alleged that, at the 20-week ultrasound, UConn’s prenatal team failed to detect evidence of congenital CMV infection and again failed, at the 22-week ultrasound, to properly recognize and respond to abnormal findings.
“They totally dropped the ball,” said the couple’s attorney. “If you’re a pregnant woman and contract the virus for the first time, the results can be devastating.”
CARS disputes this conclusion, arguing that the plaintiffs failed to prove as a “matter of scientific fact” that Ms. Monroe-Lynch was infected with CMV as the result of her intrauterine insemination.
But Superior Court Judge Mark H. Taylor disagreed. In his 107-page ruling, he said that the court “agrees with the vast majority of superior courts, concluding that a physician providing obstetric care owes a direct duty to a mother to prevent harm to her child during gestation and delivery.”
Jean-Marie Monroe-Lynch and Aaron Lynch received a $37.6 million award, consisting of $24.1 million in economic damages and $13.5 million in noneconomic damages.
Their surviving child, Joshua, will reportedly require a lifetime of medical and other care. In the meantime, UConn Health vows to appeal the Superior Court’s decision.
COVID patient’s relative demands justice for fatal outcome
An Indiana man whose grandfather recently died after suffering a stroke is calling on state lawmakers to rethink legislation passed earlier this year to protect health care providers during the COVID-19 pandemic, according to a story reported by CBS4Indy.
Late last year, Daniel Enlow’s 83-year-old grandfather, Edward Rigney, was checked into Eskenazi Hospital, in Indianapolis. Mr. Rigney suffered from COPD and had also been diagnosed with COVID-19.
At some point during his hospitalization, medical staff attempted to place what seems to have been an arterial line in order to monitor his condition. During the procedure, or at some point shortly thereafter, an “iatrogenic air embolus” was released into his veins and caused a stroke, according to medical records and Mr. Rigney’s death certificate.
“I started asking for medical records because I wanted to know what was happening leading up to it in black and white in front of me,” said Mr. Enlow, who wished to present his evidence to a medical review panel, as required by Indiana law. The first step in this process would have been to consult with a medical malpractice attorney, but several declined to take his case.
Why? Because a pair of bills passed by Indiana legislators in early 2021 make COVID-19–related suits – even tangentially related ones – potentially difficult to take to court.
The bills raised the bar to file a medical malpractice claim in COVID-19 cases and to allow only those that involve “gross negligence or willful or wanton misconduct.”
“In the vast majority of cases, it’s impossible to prove that,” said Fred Schultz, immediate past president of the Indiana Trial Lawyers Association, who lobbied against the legislation.
The bills were never designed to offer “blanket freedom,” said GOP State Senator Aaron Freeman, sponsor of one of the bills. “If something is being used in a way that it is a complete bar to certain claims, then maybe we need to go back and look at it and open that up a little bit and make it less restrictive. I’m certainly open to having those conversations.”
Meanwhile, Mr. Enlow has vowed to keep pushing in the name of his late grandfather. The hospital’s parent company, Eskenazi Health, has declined to comment.
A version of this article first appeared on Medscape.com.
Wrong-site surgery
Florida regulators have imposed a fine and other measures on a Tampa doctor who made a crucial error prior to his patient’s testicular surgery, as a story in the Miami Herald, among other news sites, reports.
On Sept. 10, 2019, a patient referred to in state documents as “C.F.” showed up for a procedure – a varicocelectomy – that would remove the enlarged veins in his left testicle. His doctor that day was Raul Fernandez-Crespo, MD, a urologist who had been licensed to practice in Florida since April of the same year. Dr. Fernandez-Crespo completed his urology residency at the University of Puerto Rico in 2019.
Following a conversation with C.F., Dr. Fernandez-Crespo designated what he believed was the proper surgical site – his patient’s right testicle.
He then proceeded to operate, but at some point during the procedure – news accounts don’t make clear when or how he became aware of his error – he realized C.F. had actually consented to a left-testicle varicocelectomy. With his patient still sedated, Dr. Fernandez-Crespo also completed the second procedure.
His mistake came to the attention of the Department of Health, which filed an administrative complaint against the surgeon. On June 17, 2021, the department’s medical licensing body, the Florida Board of Medicine, handed down its final order about the case.
In addition to imposing a $2,500 fine on Dr. Fernandez-Crespo and issuing “a letter of concern” – a public document that can be used as evidence in any relevant future disciplinary action against him – regulators said the surgeon must reimburse $2,045.56 to the department for its case-related administrative costs; take a 5-hour CME course in risk management or attend 8 hours of board disciplinary hearings; and, finally, give a 1-hour lecture on wrong-site surgeries at a board-approved medical facility.
Before this, Dr. Fernandez-Crespo had no previous disciplinary history with the Florida Board of Medicine.
Huge judgment after fertility procedure goes wrong
A Connecticut couple whose fertility and prenatal care at a state university health center proved disastrous will receive millions of dollars in damages, according to a report in the Hartford Courant.
In 2014, Jean-Marie Monroe-Lynch and her husband, Aaron Lynch, went to UConn Health, in Farmington, for treatment of Jean-Marie’s infertility. Her care was overseen by the Center for Advanced Reproductive Services (CARS), a private company then under contract with UConn Health. (The contract, which ended in 2014, obligated UConn to provide CARS providers with medical malpractice coverage.)
There, Jean-Marie was inseminated with sperm from a donor who turned out to be a carrier for cytomegalovirus (CMV), the herpes virus that can cause severe birth defects, or fetal death, when contracted by a pregnant woman. The insemination resulted in a twin pregnancy, a boy and a girl. The girl, Shay, died in utero after several of her organs became infected with CMV; the boy, Joshua, was born with severe mental and physical disabilities.
In their suit, Ms. Monroe-Lynch and her husband alleged that they were never cautioned about the risks associated with using a sperm donor whose blood had tested positive for CMV antibodies. Their suit further alleged that, at the 20-week ultrasound, UConn’s prenatal team failed to detect evidence of congenital CMV infection and again failed, at the 22-week ultrasound, to properly recognize and respond to abnormal findings.
“They totally dropped the ball,” said the couple’s attorney. “If you’re a pregnant woman and contract the virus for the first time, the results can be devastating.”
CARS disputes this conclusion, arguing that the plaintiffs failed to prove as a “matter of scientific fact” that Ms. Monroe-Lynch was infected with CMV as the result of her intrauterine insemination.
But Superior Court Judge Mark H. Taylor disagreed. In his 107-page ruling, he said that the court “agrees with the vast majority of superior courts, concluding that a physician providing obstetric care owes a direct duty to a mother to prevent harm to her child during gestation and delivery.”
Jean-Marie Monroe-Lynch and Aaron Lynch received a $37.6 million award, consisting of $24.1 million in economic damages and $13.5 million in noneconomic damages.
Their surviving child, Joshua, will reportedly require a lifetime of medical and other care. In the meantime, UConn Health vows to appeal the Superior Court’s decision.
COVID patient’s relative demands justice for fatal outcome
An Indiana man whose grandfather recently died after suffering a stroke is calling on state lawmakers to rethink legislation passed earlier this year to protect health care providers during the COVID-19 pandemic, according to a story reported by CBS4Indy.
Late last year, Daniel Enlow’s 83-year-old grandfather, Edward Rigney, was checked into Eskenazi Hospital, in Indianapolis. Mr. Rigney suffered from COPD and had also been diagnosed with COVID-19.
At some point during his hospitalization, medical staff attempted to place what seems to have been an arterial line in order to monitor his condition. During the procedure, or at some point shortly thereafter, an “iatrogenic air embolus” was released into his veins and caused a stroke, according to medical records and Mr. Rigney’s death certificate.
“I started asking for medical records because I wanted to know what was happening leading up to it in black and white in front of me,” said Mr. Enlow, who wished to present his evidence to a medical review panel, as required by Indiana law. The first step in this process would have been to consult with a medical malpractice attorney, but several declined to take his case.
Why? Because a pair of bills passed by Indiana legislators in early 2021 make COVID-19–related suits – even tangentially related ones – potentially difficult to take to court.
The bills raised the bar to file a medical malpractice claim in COVID-19 cases and to allow only those that involve “gross negligence or willful or wanton misconduct.”
“In the vast majority of cases, it’s impossible to prove that,” said Fred Schultz, immediate past president of the Indiana Trial Lawyers Association, who lobbied against the legislation.
The bills were never designed to offer “blanket freedom,” said GOP State Senator Aaron Freeman, sponsor of one of the bills. “If something is being used in a way that it is a complete bar to certain claims, then maybe we need to go back and look at it and open that up a little bit and make it less restrictive. I’m certainly open to having those conversations.”
Meanwhile, Mr. Enlow has vowed to keep pushing in the name of his late grandfather. The hospital’s parent company, Eskenazi Health, has declined to comment.
A version of this article first appeared on Medscape.com.
Nearly half of female surgeons surveyed lost a pregnancy
– according to an article published online July 28 in JAMA Surgery.
The authors, led by Erika L. Rangel, MD, division of general and gastrointestinal surgery, department of surgery, Brigham and Women’s Hospital, Boston, found that after the losses, the women took little or no time off.
Of 692 surgeons surveyed, 347 female surgeons had experienced a pregnancy loss. Of those, 244 had had a miscarriage at less than 10 weeks’ gestation, 92 had had a miscarriage between 10 and 20 weeks’ gestation, and 11 had had a stillbirth (loss at 20 weeks or later).
Most took no time off after miscarriage
After a miscarriage, 225 of 336 women (75%) took no time off work, and after a stillbirth, 5 of 11 (45%) took off 1 week or less, the authors found.
The study addressed an issue that people have talked about anecdotally or on social media, Dr. Rangel told this news organization.
“This was finally an opportunity to do a study of enough magnitude to show that there is a very quantifiable difference in complication rate, use of IVF [in vitro fertilization], and the age at which we have children. These are not just anecdotal stories,” she said.
For the study, a self-administered questionnaire was distributed electronically. Answers were collected from November 2020 to January 2021 through multiple U.S. surgical societies and social media among attending and resident surgeons with children. The control group for the study comprised 158 male surgeons who answered questions regarding their partners’ pregnancies.
Female surgeons had fewer children compared with male surgeons and their female partners (mean [SD],1.8 [0.8], versus 2.3 [1.1]; P < .001) and were more likely to delay having children because of surgical training (450 of 692 [65.0%] versus 69 of 158 [43.7%]; P < .001).
In addition, Dr. Rangel and colleagues found that 57% of female surgeons worked more than 60 hours a week during pregnancy and that 37% took more than six overnight calls.
The data show that female surgeons who operated 12 or more hours per week during the last trimester of pregnancy were at higher risk compared with those who operated fewer hours (odds ratio, 1.57; 95% confidence interval, 1.08-2.26).
“Pregnant surgeons should not be operating more than 12 hours a week when they are in the third trimester,” Dr. Rangel said.
“That is a modifiable risk factor,” she told this news organization. “It’s a very brief period of support – a couple of months of support for a woman who may do 25-30 more years of serving the public with surgical skills.”
She said that training programs should be organized so as to have colleagues cover operating room (OR) shifts to reduce the operating hours for pregnant colleagues. In addition, advanced practice health care professionals should be paid to take up the paperwork and perform non-OR care to reduce the stigma associated with pregnant trainees overburdening other surgical trainees.
‘It’s too big an ask’
Obstetrician-gynecologist Maryam Siddiqui, MD, said in an interview that she was particularly struck by the number of female surgeons who experience involuntary childlessness.
“That’s a big ask for people who want childbearing to be a part of the fulfillment of their life. It’s too big,” said Dr. Siddiqui, a gynecologic surgeon at UChicago Medicine.
She said the amount of detail in the article and the large number of participants were persuasive factors that can support establishing a more humane system than one in which one person at a time has to ask for change.
Pointing to the finding that three-fourths of the women in the study who had had miscarriages didn’t take time off, she said, “That’s not really humane. But they’re afraid to ask or they don’t want to reveal they’re trying [to get pregnant]. Why should you be afraid of building your family?”
The authors also found other adverse outcomes. Female surgeons were more likely to have musculoskeletal disorders compared with female nonsurgeon partners (36.9% versus 18.4%; P < .001), and they were more likely to undergo nonelective cesarean delivery (25.5% versus 15.3%; P = .01) and to experience postpartum depression (11.1% versus 5.7%; P = .04).
Dr. Siddiqui said the conditions that surgeons encounter on their return to work after childbirth are “a perfect storm” for postpartum depression among women who are not accustomed to being reliant on others.
Women often feel coerced into returning to work before they are physically or emotionally ready, then toggle back and forth from night shift to day shift, losing sleep, she said. “We can do better.”
One of the solutions, she said, is to provide better work coverage for the surgeon while she is pregnant and when she returns to work. That includes properly compensating the person covering for the surgeon by giving that person extra pay or additional time off.
“You have to value both people,” she said. “If both people are valued, there’s still collegiality.”
She acknowledged that that kind of compensation may be more readily available at large academic centers.
At UChicago, she said, they are creative with scheduling in training. For women at the height of pregnancy, rotations are less intensive, and trauma rotations are avoided.
Dr. Siddiqui said one of the most important aspects of the article is the authors’ list of two dozen ways, both big and small, to improve conditions.
Adopting such changes will become increasingly important for hiring and retaining female surgeons. “You want to work someplace where you’re respected as a whole person,” she said.
Sarah Blair, MD, a surgical oncologist at University of California, San Diego, stated that the number of miscarriages in particular provides disturbing proof of a problem women in surgery frequently discuss.
For nearly a decade, she led a women-in-surgery committee at UCSD in which they discussed such issues regarding pregnancy and medicine.
She said she hopes these data can help push for change in flexibility in residency so that women can graduate on time and have the families they want.
“There’s a movement away from time-based training to competency-based training, so maybe that will help women,” she said.
‘We have to figure this out’
“We will have to figure this out, because more than half of the people in medical school are women, and there are a lot more women in surgery than when I trained more than 20 years ago. It’s not a problem that’s going away,” she said.
One sign of improvement happened recently, Dr. Rangel said.
As previously reported, according to the American Board of Medical Specialties, as of July 1, 2021, residents and fellows are allowed a minimum 6 weeks away for medical leave or caregiving once during training, without having to use vacation time or sick leave and without having to extend their training.
“That’s huge,” she said. “But we still have a long way to go, because the residency programs still don’t have to have policy that abides that. It merely says you can take 6 weeks off and take your boards. It doesn’t say that the residency program has to allow you to take 6 weeks off.”
The authors noted that the United States and Papua New Guinea are the only countries in the world without federally mandated paid parental leave.
“Most U.S. female surgeons rely on their employer for this benefit, but only half of top-ranked medical schools offer paid leave, and 33%-65% of U.S. surgical training programs lack clear maternity leave policies,” she said.
Funding for the study was provided by the department of surgery at Brigham and Women’s Hospital. The study authors, Dr. Blair, and Dr. Siddiqui have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
– according to an article published online July 28 in JAMA Surgery.
The authors, led by Erika L. Rangel, MD, division of general and gastrointestinal surgery, department of surgery, Brigham and Women’s Hospital, Boston, found that after the losses, the women took little or no time off.
Of 692 surgeons surveyed, 347 female surgeons had experienced a pregnancy loss. Of those, 244 had had a miscarriage at less than 10 weeks’ gestation, 92 had had a miscarriage between 10 and 20 weeks’ gestation, and 11 had had a stillbirth (loss at 20 weeks or later).
Most took no time off after miscarriage
After a miscarriage, 225 of 336 women (75%) took no time off work, and after a stillbirth, 5 of 11 (45%) took off 1 week or less, the authors found.
The study addressed an issue that people have talked about anecdotally or on social media, Dr. Rangel told this news organization.
“This was finally an opportunity to do a study of enough magnitude to show that there is a very quantifiable difference in complication rate, use of IVF [in vitro fertilization], and the age at which we have children. These are not just anecdotal stories,” she said.
For the study, a self-administered questionnaire was distributed electronically. Answers were collected from November 2020 to January 2021 through multiple U.S. surgical societies and social media among attending and resident surgeons with children. The control group for the study comprised 158 male surgeons who answered questions regarding their partners’ pregnancies.
Female surgeons had fewer children compared with male surgeons and their female partners (mean [SD],1.8 [0.8], versus 2.3 [1.1]; P < .001) and were more likely to delay having children because of surgical training (450 of 692 [65.0%] versus 69 of 158 [43.7%]; P < .001).
In addition, Dr. Rangel and colleagues found that 57% of female surgeons worked more than 60 hours a week during pregnancy and that 37% took more than six overnight calls.
The data show that female surgeons who operated 12 or more hours per week during the last trimester of pregnancy were at higher risk compared with those who operated fewer hours (odds ratio, 1.57; 95% confidence interval, 1.08-2.26).
“Pregnant surgeons should not be operating more than 12 hours a week when they are in the third trimester,” Dr. Rangel said.
“That is a modifiable risk factor,” she told this news organization. “It’s a very brief period of support – a couple of months of support for a woman who may do 25-30 more years of serving the public with surgical skills.”
She said that training programs should be organized so as to have colleagues cover operating room (OR) shifts to reduce the operating hours for pregnant colleagues. In addition, advanced practice health care professionals should be paid to take up the paperwork and perform non-OR care to reduce the stigma associated with pregnant trainees overburdening other surgical trainees.
‘It’s too big an ask’
Obstetrician-gynecologist Maryam Siddiqui, MD, said in an interview that she was particularly struck by the number of female surgeons who experience involuntary childlessness.
“That’s a big ask for people who want childbearing to be a part of the fulfillment of their life. It’s too big,” said Dr. Siddiqui, a gynecologic surgeon at UChicago Medicine.
She said the amount of detail in the article and the large number of participants were persuasive factors that can support establishing a more humane system than one in which one person at a time has to ask for change.
Pointing to the finding that three-fourths of the women in the study who had had miscarriages didn’t take time off, she said, “That’s not really humane. But they’re afraid to ask or they don’t want to reveal they’re trying [to get pregnant]. Why should you be afraid of building your family?”
The authors also found other adverse outcomes. Female surgeons were more likely to have musculoskeletal disorders compared with female nonsurgeon partners (36.9% versus 18.4%; P < .001), and they were more likely to undergo nonelective cesarean delivery (25.5% versus 15.3%; P = .01) and to experience postpartum depression (11.1% versus 5.7%; P = .04).
Dr. Siddiqui said the conditions that surgeons encounter on their return to work after childbirth are “a perfect storm” for postpartum depression among women who are not accustomed to being reliant on others.
Women often feel coerced into returning to work before they are physically or emotionally ready, then toggle back and forth from night shift to day shift, losing sleep, she said. “We can do better.”
One of the solutions, she said, is to provide better work coverage for the surgeon while she is pregnant and when she returns to work. That includes properly compensating the person covering for the surgeon by giving that person extra pay or additional time off.
“You have to value both people,” she said. “If both people are valued, there’s still collegiality.”
She acknowledged that that kind of compensation may be more readily available at large academic centers.
At UChicago, she said, they are creative with scheduling in training. For women at the height of pregnancy, rotations are less intensive, and trauma rotations are avoided.
Dr. Siddiqui said one of the most important aspects of the article is the authors’ list of two dozen ways, both big and small, to improve conditions.
Adopting such changes will become increasingly important for hiring and retaining female surgeons. “You want to work someplace where you’re respected as a whole person,” she said.
Sarah Blair, MD, a surgical oncologist at University of California, San Diego, stated that the number of miscarriages in particular provides disturbing proof of a problem women in surgery frequently discuss.
For nearly a decade, she led a women-in-surgery committee at UCSD in which they discussed such issues regarding pregnancy and medicine.
She said she hopes these data can help push for change in flexibility in residency so that women can graduate on time and have the families they want.
“There’s a movement away from time-based training to competency-based training, so maybe that will help women,” she said.
‘We have to figure this out’
“We will have to figure this out, because more than half of the people in medical school are women, and there are a lot more women in surgery than when I trained more than 20 years ago. It’s not a problem that’s going away,” she said.
One sign of improvement happened recently, Dr. Rangel said.
As previously reported, according to the American Board of Medical Specialties, as of July 1, 2021, residents and fellows are allowed a minimum 6 weeks away for medical leave or caregiving once during training, without having to use vacation time or sick leave and without having to extend their training.
“That’s huge,” she said. “But we still have a long way to go, because the residency programs still don’t have to have policy that abides that. It merely says you can take 6 weeks off and take your boards. It doesn’t say that the residency program has to allow you to take 6 weeks off.”
The authors noted that the United States and Papua New Guinea are the only countries in the world without federally mandated paid parental leave.
“Most U.S. female surgeons rely on their employer for this benefit, but only half of top-ranked medical schools offer paid leave, and 33%-65% of U.S. surgical training programs lack clear maternity leave policies,” she said.
Funding for the study was provided by the department of surgery at Brigham and Women’s Hospital. The study authors, Dr. Blair, and Dr. Siddiqui have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
– according to an article published online July 28 in JAMA Surgery.
The authors, led by Erika L. Rangel, MD, division of general and gastrointestinal surgery, department of surgery, Brigham and Women’s Hospital, Boston, found that after the losses, the women took little or no time off.
Of 692 surgeons surveyed, 347 female surgeons had experienced a pregnancy loss. Of those, 244 had had a miscarriage at less than 10 weeks’ gestation, 92 had had a miscarriage between 10 and 20 weeks’ gestation, and 11 had had a stillbirth (loss at 20 weeks or later).
Most took no time off after miscarriage
After a miscarriage, 225 of 336 women (75%) took no time off work, and after a stillbirth, 5 of 11 (45%) took off 1 week or less, the authors found.
The study addressed an issue that people have talked about anecdotally or on social media, Dr. Rangel told this news organization.
“This was finally an opportunity to do a study of enough magnitude to show that there is a very quantifiable difference in complication rate, use of IVF [in vitro fertilization], and the age at which we have children. These are not just anecdotal stories,” she said.
For the study, a self-administered questionnaire was distributed electronically. Answers were collected from November 2020 to January 2021 through multiple U.S. surgical societies and social media among attending and resident surgeons with children. The control group for the study comprised 158 male surgeons who answered questions regarding their partners’ pregnancies.
Female surgeons had fewer children compared with male surgeons and their female partners (mean [SD],1.8 [0.8], versus 2.3 [1.1]; P < .001) and were more likely to delay having children because of surgical training (450 of 692 [65.0%] versus 69 of 158 [43.7%]; P < .001).
In addition, Dr. Rangel and colleagues found that 57% of female surgeons worked more than 60 hours a week during pregnancy and that 37% took more than six overnight calls.
The data show that female surgeons who operated 12 or more hours per week during the last trimester of pregnancy were at higher risk compared with those who operated fewer hours (odds ratio, 1.57; 95% confidence interval, 1.08-2.26).
“Pregnant surgeons should not be operating more than 12 hours a week when they are in the third trimester,” Dr. Rangel said.
“That is a modifiable risk factor,” she told this news organization. “It’s a very brief period of support – a couple of months of support for a woman who may do 25-30 more years of serving the public with surgical skills.”
She said that training programs should be organized so as to have colleagues cover operating room (OR) shifts to reduce the operating hours for pregnant colleagues. In addition, advanced practice health care professionals should be paid to take up the paperwork and perform non-OR care to reduce the stigma associated with pregnant trainees overburdening other surgical trainees.
‘It’s too big an ask’
Obstetrician-gynecologist Maryam Siddiqui, MD, said in an interview that she was particularly struck by the number of female surgeons who experience involuntary childlessness.
“That’s a big ask for people who want childbearing to be a part of the fulfillment of their life. It’s too big,” said Dr. Siddiqui, a gynecologic surgeon at UChicago Medicine.
She said the amount of detail in the article and the large number of participants were persuasive factors that can support establishing a more humane system than one in which one person at a time has to ask for change.
Pointing to the finding that three-fourths of the women in the study who had had miscarriages didn’t take time off, she said, “That’s not really humane. But they’re afraid to ask or they don’t want to reveal they’re trying [to get pregnant]. Why should you be afraid of building your family?”
The authors also found other adverse outcomes. Female surgeons were more likely to have musculoskeletal disorders compared with female nonsurgeon partners (36.9% versus 18.4%; P < .001), and they were more likely to undergo nonelective cesarean delivery (25.5% versus 15.3%; P = .01) and to experience postpartum depression (11.1% versus 5.7%; P = .04).
Dr. Siddiqui said the conditions that surgeons encounter on their return to work after childbirth are “a perfect storm” for postpartum depression among women who are not accustomed to being reliant on others.
Women often feel coerced into returning to work before they are physically or emotionally ready, then toggle back and forth from night shift to day shift, losing sleep, she said. “We can do better.”
One of the solutions, she said, is to provide better work coverage for the surgeon while she is pregnant and when she returns to work. That includes properly compensating the person covering for the surgeon by giving that person extra pay or additional time off.
“You have to value both people,” she said. “If both people are valued, there’s still collegiality.”
She acknowledged that that kind of compensation may be more readily available at large academic centers.
At UChicago, she said, they are creative with scheduling in training. For women at the height of pregnancy, rotations are less intensive, and trauma rotations are avoided.
Dr. Siddiqui said one of the most important aspects of the article is the authors’ list of two dozen ways, both big and small, to improve conditions.
Adopting such changes will become increasingly important for hiring and retaining female surgeons. “You want to work someplace where you’re respected as a whole person,” she said.
Sarah Blair, MD, a surgical oncologist at University of California, San Diego, stated that the number of miscarriages in particular provides disturbing proof of a problem women in surgery frequently discuss.
For nearly a decade, she led a women-in-surgery committee at UCSD in which they discussed such issues regarding pregnancy and medicine.
She said she hopes these data can help push for change in flexibility in residency so that women can graduate on time and have the families they want.
“There’s a movement away from time-based training to competency-based training, so maybe that will help women,” she said.
‘We have to figure this out’
“We will have to figure this out, because more than half of the people in medical school are women, and there are a lot more women in surgery than when I trained more than 20 years ago. It’s not a problem that’s going away,” she said.
One sign of improvement happened recently, Dr. Rangel said.
As previously reported, according to the American Board of Medical Specialties, as of July 1, 2021, residents and fellows are allowed a minimum 6 weeks away for medical leave or caregiving once during training, without having to use vacation time or sick leave and without having to extend their training.
“That’s huge,” she said. “But we still have a long way to go, because the residency programs still don’t have to have policy that abides that. It merely says you can take 6 weeks off and take your boards. It doesn’t say that the residency program has to allow you to take 6 weeks off.”
The authors noted that the United States and Papua New Guinea are the only countries in the world without federally mandated paid parental leave.
“Most U.S. female surgeons rely on their employer for this benefit, but only half of top-ranked medical schools offer paid leave, and 33%-65% of U.S. surgical training programs lack clear maternity leave policies,” she said.
Funding for the study was provided by the department of surgery at Brigham and Women’s Hospital. The study authors, Dr. Blair, and Dr. Siddiqui have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA’s fast-track approval process exposed as lax, in need of reform
an in-depth investigation published in The BMJ has determined.
“Despite the pathway’s good intentions to accelerate ‘the availability of drugs that treat serious diseases,’ experts are concerned that it is now being exploited – to the detriment of patients, who may be prescribed a drug that offers little benefit and possible harm, and to taxpayers,” writes Elisabeth Mahase, clinical reporter at The BMJ, who carried out the analysis.
The FDA’s accelerated approval pathway is intended to provide earlier access to drugs for serious diseases when there is lingering uncertainty at the time of approval regarding the drug’s ultimate clinical benefit.
Required studies rarely completed
As part of this fast-track pathway, drug manufacturers must conduct postapproval, phase 4 confirmatory trials to verify the anticipated clinical benefit. If these trials indicate no benefit, FDA approval can be withdrawn.
However, the analysis of FDA data shows once they are approved drugs are rarely taken off the market.
The BMJ investigation that analyzed data up to the end of 2020 shows that 112 of the 253 (44%) medications granted accelerated approval have not been confirmed to be effective.
In addition, 24 (21%) of these questionable drugs have been on the market for more than 5 years and some have been on the market for more than 20 years – often with a hefty price tag.
Furthermore, only 16 drugs approved through the accelerated approval process have ever been withdrawn, and most were shown to be ineffective, but in some cases the confirmatory trials were never done, Ms. Mahase reports.
For example, the COX-2 inhibitor celecoxib (Celebrex), which was granted accelerated approval in 1999 for the treatment of familial adenomatous polyposis, was on the market for 12 years before the FDA finally asked Pfizer to voluntarily withdraw it for this indication because efficacy trials were never completed.
As part of The BMJ’s investigation, Ms. Mahase asked manufacturers of the 24 drugs that have remained on the market for more than 5 years whether they had conducted the required phase 4 confirmatory trials. Six of the drugs had been withdrawn, approved, or postponed.
Of the remaining 18 drugs, the manufacturers provided the relevant trial information for only six. Only four drugmakers had started to recruit patients; two said they were still in discussion with the FDA over the final trial design.
“These products routinely have side effects, but the benefit information is a lot less certain. That’s what we’re concerned about – that we may have drugs on the market that don’t have any benefits, but certainly predictably have harms associated with them,” Huseyin Naci, PhD, MHS, with the London School of Economics, comments in the report.
Call for reform
As reported by this news organization, a 2015 report by the General Accountability Office (GAO) concluded that the FDA does not do an effective job of tracking the clinical efficacy or the safety of drugs with expedited approval after they hit the market.
In April of this year, the Institute for Clinical and Economic Review (ICER) cited a lack of “credible threats” to withdraw approval if companies don’t do confirmatory trials – meaning drugmakers have little incentive to do the trials.
“There are some instances where the companies really do seem to be taking advantage of the accelerated approval pathway and are using it in a way that makes it harder to get at the truth about whether these products really are safe and effective,” Rachel Sachs, JD, MPH, Washington University, St. Louis, said in The BMJ article.
In addition, the authors of a recent viewpoint article in JAMA Internal Medicine assert the recent approval of the controversial anti-amyloid drug aducanumab (Aduhelm, Biogen) shows that the accelerated approval pathway needs to be reformed.
Despite the concerns, Ms. Mahase said all experts who spoke to The BMJ believe the accelerated approval pathway is still useful and can be beneficial to patients, although some changes are needed.
One effective reform might be to have confirmatory trials designed, and even started, as part of accelerated approval.
“One important piece of the puzzle is for the FDA itself to be tougher on these companies, to hold them to the bargain that they have agreed to, and to take action when the company has not met their obligations,” Ms. Sachs told the journal.
An FDA spokesperson told the BMJ that the agency is “committed to working with sponsors to ensure that confirmatory studies are completed in a timely manner.”
“We expect sponsors to commit all resources needed to move trials forward as effectively as possible, with the aim of completing trials as soon as is feasible, while assuring the quality of the data and the robustness of the results,” the agency said.
A version of this article first appeared on Medscape.com.
an in-depth investigation published in The BMJ has determined.
“Despite the pathway’s good intentions to accelerate ‘the availability of drugs that treat serious diseases,’ experts are concerned that it is now being exploited – to the detriment of patients, who may be prescribed a drug that offers little benefit and possible harm, and to taxpayers,” writes Elisabeth Mahase, clinical reporter at The BMJ, who carried out the analysis.
The FDA’s accelerated approval pathway is intended to provide earlier access to drugs for serious diseases when there is lingering uncertainty at the time of approval regarding the drug’s ultimate clinical benefit.
Required studies rarely completed
As part of this fast-track pathway, drug manufacturers must conduct postapproval, phase 4 confirmatory trials to verify the anticipated clinical benefit. If these trials indicate no benefit, FDA approval can be withdrawn.
However, the analysis of FDA data shows once they are approved drugs are rarely taken off the market.
The BMJ investigation that analyzed data up to the end of 2020 shows that 112 of the 253 (44%) medications granted accelerated approval have not been confirmed to be effective.
In addition, 24 (21%) of these questionable drugs have been on the market for more than 5 years and some have been on the market for more than 20 years – often with a hefty price tag.
Furthermore, only 16 drugs approved through the accelerated approval process have ever been withdrawn, and most were shown to be ineffective, but in some cases the confirmatory trials were never done, Ms. Mahase reports.
For example, the COX-2 inhibitor celecoxib (Celebrex), which was granted accelerated approval in 1999 for the treatment of familial adenomatous polyposis, was on the market for 12 years before the FDA finally asked Pfizer to voluntarily withdraw it for this indication because efficacy trials were never completed.
As part of The BMJ’s investigation, Ms. Mahase asked manufacturers of the 24 drugs that have remained on the market for more than 5 years whether they had conducted the required phase 4 confirmatory trials. Six of the drugs had been withdrawn, approved, or postponed.
Of the remaining 18 drugs, the manufacturers provided the relevant trial information for only six. Only four drugmakers had started to recruit patients; two said they were still in discussion with the FDA over the final trial design.
“These products routinely have side effects, but the benefit information is a lot less certain. That’s what we’re concerned about – that we may have drugs on the market that don’t have any benefits, but certainly predictably have harms associated with them,” Huseyin Naci, PhD, MHS, with the London School of Economics, comments in the report.
Call for reform
As reported by this news organization, a 2015 report by the General Accountability Office (GAO) concluded that the FDA does not do an effective job of tracking the clinical efficacy or the safety of drugs with expedited approval after they hit the market.
In April of this year, the Institute for Clinical and Economic Review (ICER) cited a lack of “credible threats” to withdraw approval if companies don’t do confirmatory trials – meaning drugmakers have little incentive to do the trials.
“There are some instances where the companies really do seem to be taking advantage of the accelerated approval pathway and are using it in a way that makes it harder to get at the truth about whether these products really are safe and effective,” Rachel Sachs, JD, MPH, Washington University, St. Louis, said in The BMJ article.
In addition, the authors of a recent viewpoint article in JAMA Internal Medicine assert the recent approval of the controversial anti-amyloid drug aducanumab (Aduhelm, Biogen) shows that the accelerated approval pathway needs to be reformed.
Despite the concerns, Ms. Mahase said all experts who spoke to The BMJ believe the accelerated approval pathway is still useful and can be beneficial to patients, although some changes are needed.
One effective reform might be to have confirmatory trials designed, and even started, as part of accelerated approval.
“One important piece of the puzzle is for the FDA itself to be tougher on these companies, to hold them to the bargain that they have agreed to, and to take action when the company has not met their obligations,” Ms. Sachs told the journal.
An FDA spokesperson told the BMJ that the agency is “committed to working with sponsors to ensure that confirmatory studies are completed in a timely manner.”
“We expect sponsors to commit all resources needed to move trials forward as effectively as possible, with the aim of completing trials as soon as is feasible, while assuring the quality of the data and the robustness of the results,” the agency said.
A version of this article first appeared on Medscape.com.
an in-depth investigation published in The BMJ has determined.
“Despite the pathway’s good intentions to accelerate ‘the availability of drugs that treat serious diseases,’ experts are concerned that it is now being exploited – to the detriment of patients, who may be prescribed a drug that offers little benefit and possible harm, and to taxpayers,” writes Elisabeth Mahase, clinical reporter at The BMJ, who carried out the analysis.
The FDA’s accelerated approval pathway is intended to provide earlier access to drugs for serious diseases when there is lingering uncertainty at the time of approval regarding the drug’s ultimate clinical benefit.
Required studies rarely completed
As part of this fast-track pathway, drug manufacturers must conduct postapproval, phase 4 confirmatory trials to verify the anticipated clinical benefit. If these trials indicate no benefit, FDA approval can be withdrawn.
However, the analysis of FDA data shows once they are approved drugs are rarely taken off the market.
The BMJ investigation that analyzed data up to the end of 2020 shows that 112 of the 253 (44%) medications granted accelerated approval have not been confirmed to be effective.
In addition, 24 (21%) of these questionable drugs have been on the market for more than 5 years and some have been on the market for more than 20 years – often with a hefty price tag.
Furthermore, only 16 drugs approved through the accelerated approval process have ever been withdrawn, and most were shown to be ineffective, but in some cases the confirmatory trials were never done, Ms. Mahase reports.
For example, the COX-2 inhibitor celecoxib (Celebrex), which was granted accelerated approval in 1999 for the treatment of familial adenomatous polyposis, was on the market for 12 years before the FDA finally asked Pfizer to voluntarily withdraw it for this indication because efficacy trials were never completed.
As part of The BMJ’s investigation, Ms. Mahase asked manufacturers of the 24 drugs that have remained on the market for more than 5 years whether they had conducted the required phase 4 confirmatory trials. Six of the drugs had been withdrawn, approved, or postponed.
Of the remaining 18 drugs, the manufacturers provided the relevant trial information for only six. Only four drugmakers had started to recruit patients; two said they were still in discussion with the FDA over the final trial design.
“These products routinely have side effects, but the benefit information is a lot less certain. That’s what we’re concerned about – that we may have drugs on the market that don’t have any benefits, but certainly predictably have harms associated with them,” Huseyin Naci, PhD, MHS, with the London School of Economics, comments in the report.
Call for reform
As reported by this news organization, a 2015 report by the General Accountability Office (GAO) concluded that the FDA does not do an effective job of tracking the clinical efficacy or the safety of drugs with expedited approval after they hit the market.
In April of this year, the Institute for Clinical and Economic Review (ICER) cited a lack of “credible threats” to withdraw approval if companies don’t do confirmatory trials – meaning drugmakers have little incentive to do the trials.
“There are some instances where the companies really do seem to be taking advantage of the accelerated approval pathway and are using it in a way that makes it harder to get at the truth about whether these products really are safe and effective,” Rachel Sachs, JD, MPH, Washington University, St. Louis, said in The BMJ article.
In addition, the authors of a recent viewpoint article in JAMA Internal Medicine assert the recent approval of the controversial anti-amyloid drug aducanumab (Aduhelm, Biogen) shows that the accelerated approval pathway needs to be reformed.
Despite the concerns, Ms. Mahase said all experts who spoke to The BMJ believe the accelerated approval pathway is still useful and can be beneficial to patients, although some changes are needed.
One effective reform might be to have confirmatory trials designed, and even started, as part of accelerated approval.
“One important piece of the puzzle is for the FDA itself to be tougher on these companies, to hold them to the bargain that they have agreed to, and to take action when the company has not met their obligations,” Ms. Sachs told the journal.
An FDA spokesperson told the BMJ that the agency is “committed to working with sponsors to ensure that confirmatory studies are completed in a timely manner.”
“We expect sponsors to commit all resources needed to move trials forward as effectively as possible, with the aim of completing trials as soon as is feasible, while assuring the quality of the data and the robustness of the results,” the agency said.
A version of this article first appeared on Medscape.com.
COVID-19 leaves wake of medical debt among U.S. adults
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
Cost Comparison of 2 Video Laryngoscopes in a Large Academic Center
From the Department of Anesthesiology, Thomas Jefferson University and Hospitals, Sidney Kimmel Medical College, Philadelphia, PA, and Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA.
Objective: Retrospective study examining hospital cost information of patients requiring endotracheal intubation with video laryngoscopy. Provide a practical cost assessment on use of the McGRATH and GlideScope video laryngoscopes (VLs).
Methods: This study examined 52 hospital locations within a single, large university hospital, with most of those locations being hospital operating rooms. A total of 34 600 endotracheal intubations performed over 24 months, of which 11 345 were video laryngoscopies. Electronic medical records containing demographic data and information related to endotracheal intubation procedures, with monthly breakdowns between GlideScope and McGRATH intubations, were reviewed. Cost information calculated for equipment, blades, batteries, repairs, and subsequent analysis performed to determine cost differences between those 2 instruments during the COVID-19 period.
Results: A total of 5501 video laryngoscopy procedures were performed using the McGRATH VL and 5305 were performed using the GlideScope VL. Costs over 24 months were $181 093 lower (55.5%) for McGRATH compared to GlideScope. The mean (SD) monthly costs for GlideScope blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for McGRATH blades (P < .001). Most total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for GlideScope. During the COVID-19 period, the use of the McGRATH increased to 61% of all video laryngoscopy cases, compared to 37% for GlideScope (P < .001). Blade cost difference for the COVID-19 period was $128 higher for the McGRATH even though 293 more intubations were performed with that device.
Conclusions: Use of the McGRATH resulted in a cost savings of 55% compared to the GlideScope, and its use was highest during the COVID-19 period, which may be explained by its more portable and practical features.
Keywords: video laryngoscope; McGRATH; GlideScope; endotracheal intubation; hospital costs; COVID-19.
Hospitals have come to rely on video laryngoscopes (VLs) for tracheal intubation as necessary tools for better visualization of airways. Modern video laryngoscopy developed in the 2000s1 as a progression from direct laryngoscopy, which began in 1852 when Horace Green used a bent tongue spatula and sunlight to examine a child.2 VLs have seen many improvements and adaptations of their own, resulting in many different styles and types circulating around hospitals. The GlideScope (Verathon Inc, Bothell, WA) and the McGRATH (Medtronic, Minneapolis, MN) are examples of such instruments, which are now widely used in the US and are the 2 VLs of choice at our institution.
A few studies have compared VLs to direct laryngoscopes. In their systematic review, Lewis et al have shown the numerous benefits of using a VL over a direct laryngoscope. Some general conclusions were that the use of video laryngoscopy reduced the number of failed intubations, decreased laryngeal trauma, and provided improved visualizations.3 Other studies have compared the different types of VLs, including the McGRATH and the GlideScope, examining factors such as intubation time and display quality of the image. Two studies found that medical students were equally successful at using both the McGRATH and the GlideScope,4,5 while another study found that care providers using the GlideScope had quicker intubation times.6 Lastly, Savoldelli et al concluded that more providers preferred the McGRATH, which provided better laryngeal views,7 while their subsequent study showed more favorable learning curves of the Airtraq compared to the McGRATH and other VLs.8
Although there have been no reported differences in safety and effectiveness of the McGRATH and GlideScope devices, cost data on the use of these 2 popular laryngoscopes are lacking. Such information is important considering the increasing costs of medical technologies and the significant financial losses experienced by health care systems due to the COVID-19 crisis. The purpose of this retrospective cohort study was to compare the cost efficiency of the McGRATH MAC and GlideScope Core VLs at a large academic center.
Methods
This retrospective study was performed under exemption from the Thomas Jefferson University Institutional Review Board. The primary data sources consisted of hospital electronic patient records (EPIC) and cost information from the device manufacturers and hospital staff. The electronic patient data were provided by the EPIC Enterprise Analytics Business Intelligence group at Thomas Jefferson University Hospital (Center City Campus, Philadelphia, PA), while device costs were obtained from Verathon, Medtronic, and departmental staff responsible for purchasing equipment. Monthly data were obtained over a 24-month period (June 2018 through May 2020) when the McGRATH VL was placed into use in the department of anesthesiology. The 2 types of VLs were made available for use in a total of 52 locations, with the majority being hospital operating rooms.
The following variables were recorded: number of endotracheal intubations performed each month with breakdown between video laryngoscopy and flexible bronchoscopy airways, frequency of use for each type of laryngoscope, blades used, and equipment costs for use of each laryngoscope. Hospital cost estimates for both the McGRATH and GlideScope laryngoscopes included batteries, handles, blades, and the devices themselves. Cost data were also collected on frequency of device failure, maintenance, and replacement of parts and lost equipment.
Analysis
De-identified electronic medical records consisted of nominal and quantitative variables, with demographic data and information related to the endotracheal intubation procedure. All data were in chronological order and sorted by date after which coding was applied, to identify device type and allocate pertinent cost information. Descriptive statistics were reported as mean (SD) and sum for costs; frequency tables were generated for intubation procedures according to device type and time periods. Data were analyzed using the χ2 test, the student t test, and the Wilcoxon Mann-Whitney U test, with a P value set at .05 for statistical significance. SPSS version 26 and GraphPad Prism version 6 were used for all statistical analyses.
Results
A total of 34 600 endotracheal intubations were performed over the 24-month study period, and 11 345 (32.8%) were video laryngoscopy procedures. Out of all video laryngoscopy procedures, 5501 (48.5%) were performed using the McGRATH VL and 5305 (46.8%) were conducted using the GlideScope VL. The difference of 539 (4.8%) cases accounts for flexible bronchoscopy procedures and endotracheal intubations using other video laryngoscopy equipment. The mean (SD) monthly number of video laryngoscopy procedures for the 24 months was 221 (54) and 229 (89) for the GlideScope and McGRATH devices, respectively. Monthly endotracheal intubation distributions over 24 months trended upward for the McGRATH VL and downward for the GlideScope, but there was no statistically significant (P = .71) difference in overall use between the 2 instruments (Figure 1).
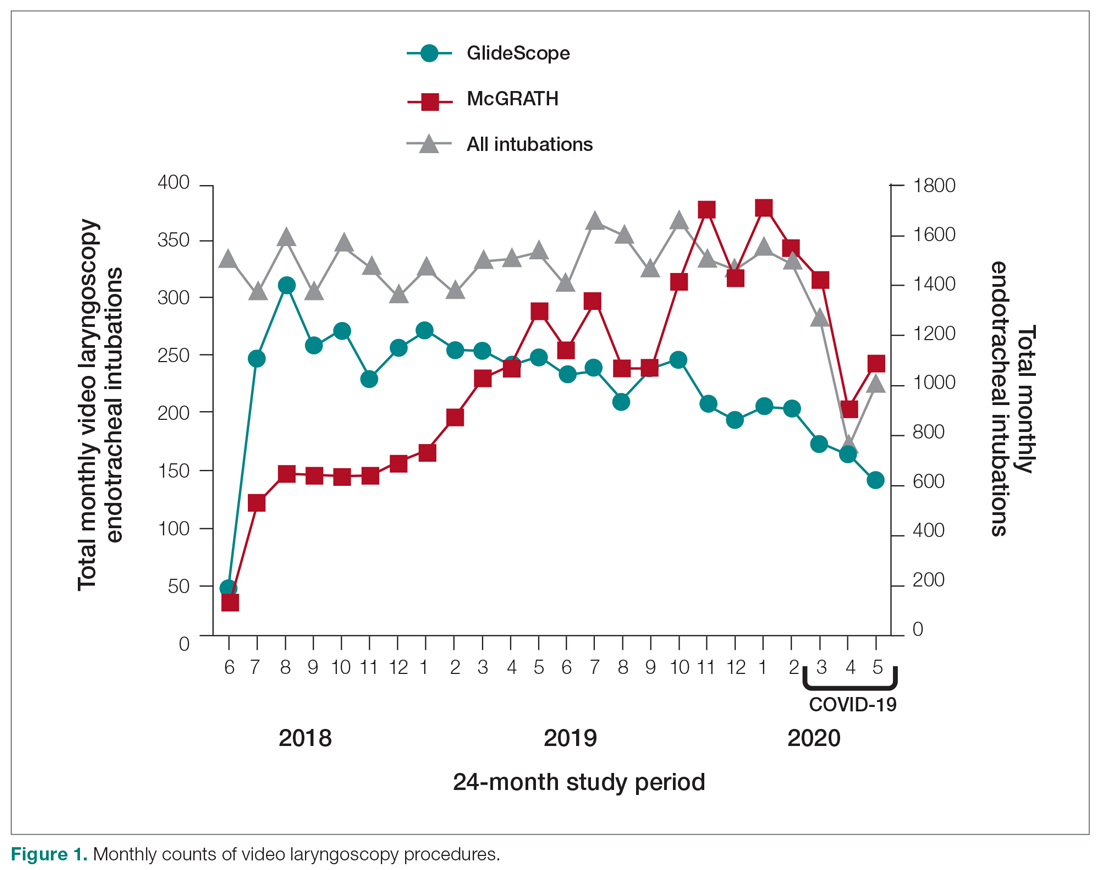
To examine the observed usage trends between the 2 VL during the first and last 12 months, a univariate ANOVA was conducted with the 2 time periods entered as predictors in the model. Video laryngoscopy intubations were performed (P = .001) more frequently with the GlideScope during the first 12 months; however, use of the McGRATH VL increased (P < .001) during the following 12 months compared to GlideScope. The GlideScope accounted for 54% of all VL intubations during the first 12 months, with the McGRATH accounting for 58% of all video laryngoscopy procedures for months 12 to 24. Additionally, the increase in video laryngoscopy procedures with the McGRATH during the last 3 months of the study period was despite an overall reduction in surgical volume due to the COVID-19 crisis, defined for this study as March 1, 2020, to May 31, 2020 (Figure 1). There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VL for that period. The anesthesia personnel’s use of the McGRATH VL increased to 61% of all video laryngoscopy cases, compared to 37% for the GlideScope (Figure 2).
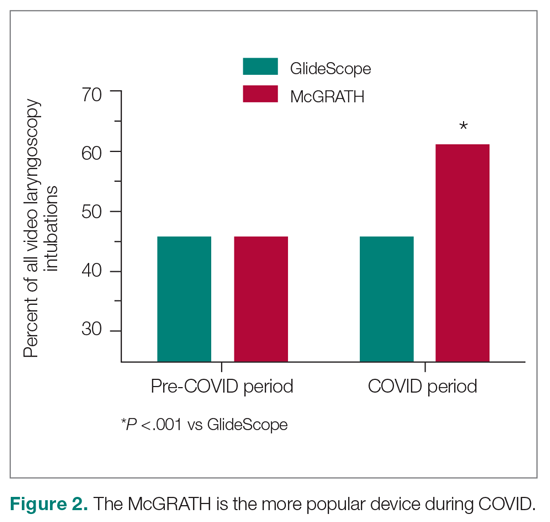
The total costs calculated for equipment, blades, and repairs are presented in Table 1 and yearly total costs are shown in Figure 3. Overall costs were $181 093 lower (55.5%) for the McGRATH VL compared to the GlideScope over the 24-month period. The mean (SD) monthly costs for GlideScope VL blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for the McGRATH VL blades. Most of the total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for the GlideScope compared to the McGRATH VL. The monthly blade costs alone were higher (P < .001) for the GlideScope over the 2-year period; however, the McGRATH VL required use of disposable stylets at a cost of $10 177 for all endotracheal intubations, compared to $700 for the GlideScope device.
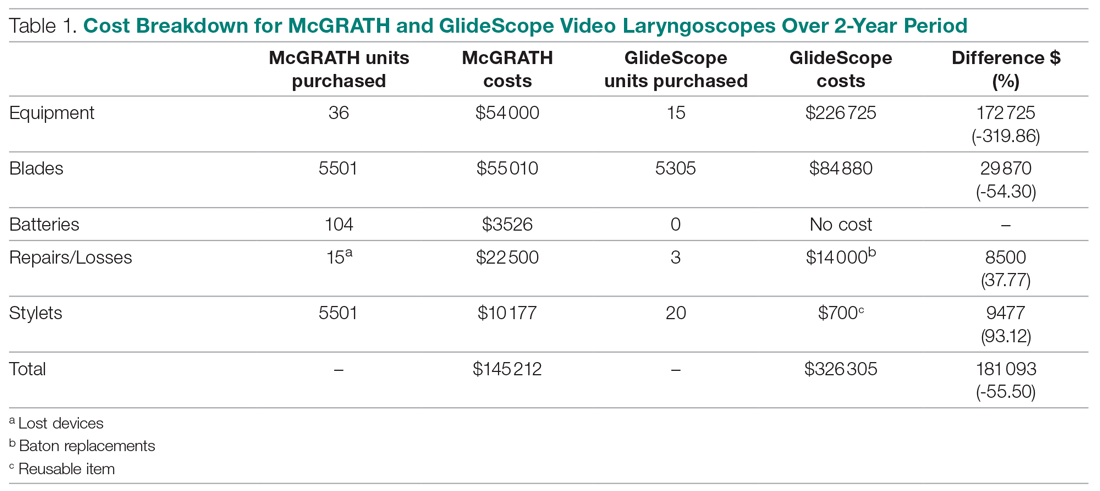
An analysis was performed to determine whether costs differed between those 2 instruments during the COVID-19 period. There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VLs during that period. The calculated blade cost difference for the COVID period was $128 higher for the McGRATH even though 293 more intubations were performed with that device (Table 2).
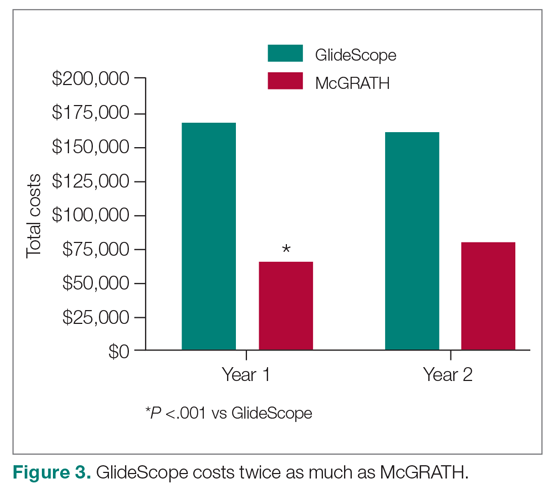
Discussion
We attempted to provide useful cost estimates by presenting pricing data reflecting the approximate cost that most large institutional anesthesia practices would incur for using those 2 specific devices and related peripherals. The main findings of our analysis showed that use of the McGRATH MAC VL resulted in a 55% cost savings compared to the GlideScope, with a similar number of cases performed with each device over the 24-month study period. We believe this represents a substantial savings to the department and institution, which has prompted internal review on the use of video laryngoscopy equipment. None of the McGRATH units failed; however, the GlideScope required 3 baton replacements.
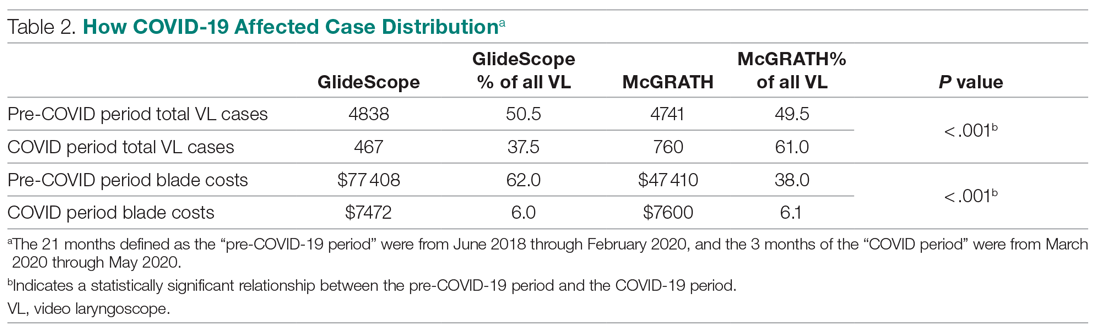
Of note, use of the McGRATH MAC increased during the COVID-19 period, which may be explained by the fact that the operators found it to be a more portable device. Several physicians in the department commented that its smaller size made the McGRATH MAC more practical during the time when a plexiglass box was being used around the patient’s head to shield the intubator from aerosolized viral particles.
Although this study demonstrated the cost-saving value of the McGRATH over the GlideScope, a suggested next step would be to examine resource utilization related to video laryngoscopy use. The more dynamic tracking of the use of these devices should facilitate the assessment of existing related resources and decision making, to optimize the benefits of this initiative. We would anticipate reduced use of anesthesia personnel, such as technicians to assist with the management of this device which could be significant. As new respiratory viruses are appearing each year, video laryngoscopy will continue to gain increasing use in operating rooms and acute care locations. The adding of protective barriers between patients and providers calls for use of the most practical and effective VL devices, to protect personnel who are at high risk of contamination from airway secretions and aerosolized particles.9,10
The COVID-19 pandemic has demonstrated the value of anesthesiology in regards to analyzing and finding solutions to effectively manage infected patients or those suspected of infection in the perioperative environment. Inexpensive products are often avoided because cheaper devices are associated with being of lower quality. However, the association with cost and quality—and the assumption that a higher price is positively correlated with higher quality—is overall inconsistent in the medical literature.11 A more effective or higher quality treatment does not necessarily cost more and may actually end up costing less,12 as was the case in this study. We have been able to directly cut departmental expenses by using a more efficient and cost-effective device for intubations, without compromising safety and efficacy. Future studies should determine whether this significant reduction in costs from video laryngoscopy intubations with the McGRATH VL will be sustained across anesthesiology departments in the Jefferson Health Enterprise Hospitals, or other health systems, as well as its impact on workflow and personnel resources.
This analysis was restricted to one of the campuses of the Jefferson Health Enterprise. However, this is the largest anesthesia practice, encompassing several locations, which should reflect the general practice patterns across other anesthesiology departments in this large institution. The costs for the devices and peripherals may vary across anesthesia practices depending on volume and contracts negotiated with the suppliers. It was not possible to estimate this variability, which could change the total costs by a few percentage points. We recognize that there may be other costs associated with securing the McGRATH VL to prevent loss from theft or misplacement, which were not included in the study. Lastly, the inability to obtain randomized samples for the 2 groups treated with each device opens up the possibility of selection bias. There were, however, multiple intubators who were free to select 1 of the devices for endotracheal intubation, which may have reduced the effect of selection bias.
Conclusion
This study demonstrated that over a 24-month period use of the McGRATH MAC VL resulted in a cost reduction of around 55% compared to using the GlideScope for endotracheal intubation procedures performed at a major academic center. Over the first 3 months of the COVID-19 crisis, which our study included, use of the McGRATH VL increased while GlideScope use decreased. This was most likely related to the portability and smaller size of the McGRATH, which better facilitated intubations of COVID-19 patients.
Acknowledgements: The authors thank Craig Smith, Senior Anesthesia Technician, for his assistance with the cost information and excellent record-keeping related to the use of video laryngoscopes.
Corresponding author: Marc C. Torjman, PhD, Professor, Department of Anesthesiology, Sidney Kimmel Medical College at Thomas Jefferson University, 111 South 11th St, Suite G-8290, Philadelphia, PA 19107; Marc.Torjman@Jefferson.edu.
Financial disclosures: Dr. Thaler has served as a consultant for Medtronic since September 2020. He has participated in 2 webinars on the routine use of video laryngoscopy.
Funding: This study was supported by the Department of Anesthesiology at Thomas Jefferson University.
1. Channa AB. Video laryngoscopes. Saudi J Anaesth. 2011;5(4):357-359.
2. Pieters BM, Eindhoven GB, Acott C, Van Zundert AAJ. Pioneers of laryngoscopy: indirect, direct and video laryngoscopy. Anaesth Intensive Care. 2015;43(suppl):4-11.
3. Lewis SR, Butler AR, Parker J, et al. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev. 2016;11(11):CD011136.
4. Kim W, Choi HJ, Lim T, Kang BS. Can the new McGrath laryngoscope rival the GlideScope Ranger portable video laryngoscope? A randomized manikin study. Am J Emerg Med. 2014;32(10):1225-1229.
5. Kim W, Choi HJ, Lim T, et al. Is McGrath MAC better than Glidescope Ranger for novice providers in the simulated difficult airway? A randomized manikin study. Resuscitation. 2014;85(suppl 1):S32.
6. Jeon WJ, Kim KH, Yeom JH, et al. A comparison of the Glidescope to the McGrath videolaryngoscope in patients. Korean J Anesthesiol. 2011;61(1):19-23.
7. Savoldelli GL, Schiffer E, Abegg C, et al. Comparison of the Glidescope, the McGrath, the Airtraq and the Macintosh laryngoscopes in simulated difficult airways. Anaesthesia. 2008;63(12):1358-1364.
8. Savoldelli GL, Schiffer E, Abegg C, et al. Learning curves of the Glidescope, the McGrath and the Airtraq laryngoscopes: a manikin study. Eur J Anaesthesiol. 2009;26(7):554-558.
9. Schumacher J, Arlidge J, Dudley D, et al. The impact of respiratory protective equipment on difficult airway management: a randomised, crossover, simulation study. Anaesthesia. 2020;75(10):1301-1306.
10. De Jong A, Pardo E, Rolle A, et al. Airway management for COVID-19: a move towards universal videolaryngoscope? Lancet Respir Med. 2020;8(6):555.
11. Hussey PS, Wertheimer S, Mehrotra A. The association between health care quality and cost: a systematic review. Ann Intern Med. 2013;158(1):27-34.
12. Mitton C, Dionne F, Peacock S, Sheps S. Quality and cost in healthcare: a relationship worth examining. Appl Health Econ Health Policy. 2006;5(4):201-208.
From the Department of Anesthesiology, Thomas Jefferson University and Hospitals, Sidney Kimmel Medical College, Philadelphia, PA, and Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA.
Objective: Retrospective study examining hospital cost information of patients requiring endotracheal intubation with video laryngoscopy. Provide a practical cost assessment on use of the McGRATH and GlideScope video laryngoscopes (VLs).
Methods: This study examined 52 hospital locations within a single, large university hospital, with most of those locations being hospital operating rooms. A total of 34 600 endotracheal intubations performed over 24 months, of which 11 345 were video laryngoscopies. Electronic medical records containing demographic data and information related to endotracheal intubation procedures, with monthly breakdowns between GlideScope and McGRATH intubations, were reviewed. Cost information calculated for equipment, blades, batteries, repairs, and subsequent analysis performed to determine cost differences between those 2 instruments during the COVID-19 period.
Results: A total of 5501 video laryngoscopy procedures were performed using the McGRATH VL and 5305 were performed using the GlideScope VL. Costs over 24 months were $181 093 lower (55.5%) for McGRATH compared to GlideScope. The mean (SD) monthly costs for GlideScope blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for McGRATH blades (P < .001). Most total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for GlideScope. During the COVID-19 period, the use of the McGRATH increased to 61% of all video laryngoscopy cases, compared to 37% for GlideScope (P < .001). Blade cost difference for the COVID-19 period was $128 higher for the McGRATH even though 293 more intubations were performed with that device.
Conclusions: Use of the McGRATH resulted in a cost savings of 55% compared to the GlideScope, and its use was highest during the COVID-19 period, which may be explained by its more portable and practical features.
Keywords: video laryngoscope; McGRATH; GlideScope; endotracheal intubation; hospital costs; COVID-19.
Hospitals have come to rely on video laryngoscopes (VLs) for tracheal intubation as necessary tools for better visualization of airways. Modern video laryngoscopy developed in the 2000s1 as a progression from direct laryngoscopy, which began in 1852 when Horace Green used a bent tongue spatula and sunlight to examine a child.2 VLs have seen many improvements and adaptations of their own, resulting in many different styles and types circulating around hospitals. The GlideScope (Verathon Inc, Bothell, WA) and the McGRATH (Medtronic, Minneapolis, MN) are examples of such instruments, which are now widely used in the US and are the 2 VLs of choice at our institution.
A few studies have compared VLs to direct laryngoscopes. In their systematic review, Lewis et al have shown the numerous benefits of using a VL over a direct laryngoscope. Some general conclusions were that the use of video laryngoscopy reduced the number of failed intubations, decreased laryngeal trauma, and provided improved visualizations.3 Other studies have compared the different types of VLs, including the McGRATH and the GlideScope, examining factors such as intubation time and display quality of the image. Two studies found that medical students were equally successful at using both the McGRATH and the GlideScope,4,5 while another study found that care providers using the GlideScope had quicker intubation times.6 Lastly, Savoldelli et al concluded that more providers preferred the McGRATH, which provided better laryngeal views,7 while their subsequent study showed more favorable learning curves of the Airtraq compared to the McGRATH and other VLs.8
Although there have been no reported differences in safety and effectiveness of the McGRATH and GlideScope devices, cost data on the use of these 2 popular laryngoscopes are lacking. Such information is important considering the increasing costs of medical technologies and the significant financial losses experienced by health care systems due to the COVID-19 crisis. The purpose of this retrospective cohort study was to compare the cost efficiency of the McGRATH MAC and GlideScope Core VLs at a large academic center.
Methods
This retrospective study was performed under exemption from the Thomas Jefferson University Institutional Review Board. The primary data sources consisted of hospital electronic patient records (EPIC) and cost information from the device manufacturers and hospital staff. The electronic patient data were provided by the EPIC Enterprise Analytics Business Intelligence group at Thomas Jefferson University Hospital (Center City Campus, Philadelphia, PA), while device costs were obtained from Verathon, Medtronic, and departmental staff responsible for purchasing equipment. Monthly data were obtained over a 24-month period (June 2018 through May 2020) when the McGRATH VL was placed into use in the department of anesthesiology. The 2 types of VLs were made available for use in a total of 52 locations, with the majority being hospital operating rooms.
The following variables were recorded: number of endotracheal intubations performed each month with breakdown between video laryngoscopy and flexible bronchoscopy airways, frequency of use for each type of laryngoscope, blades used, and equipment costs for use of each laryngoscope. Hospital cost estimates for both the McGRATH and GlideScope laryngoscopes included batteries, handles, blades, and the devices themselves. Cost data were also collected on frequency of device failure, maintenance, and replacement of parts and lost equipment.
Analysis
De-identified electronic medical records consisted of nominal and quantitative variables, with demographic data and information related to the endotracheal intubation procedure. All data were in chronological order and sorted by date after which coding was applied, to identify device type and allocate pertinent cost information. Descriptive statistics were reported as mean (SD) and sum for costs; frequency tables were generated for intubation procedures according to device type and time periods. Data were analyzed using the χ2 test, the student t test, and the Wilcoxon Mann-Whitney U test, with a P value set at .05 for statistical significance. SPSS version 26 and GraphPad Prism version 6 were used for all statistical analyses.
Results
A total of 34 600 endotracheal intubations were performed over the 24-month study period, and 11 345 (32.8%) were video laryngoscopy procedures. Out of all video laryngoscopy procedures, 5501 (48.5%) were performed using the McGRATH VL and 5305 (46.8%) were conducted using the GlideScope VL. The difference of 539 (4.8%) cases accounts for flexible bronchoscopy procedures and endotracheal intubations using other video laryngoscopy equipment. The mean (SD) monthly number of video laryngoscopy procedures for the 24 months was 221 (54) and 229 (89) for the GlideScope and McGRATH devices, respectively. Monthly endotracheal intubation distributions over 24 months trended upward for the McGRATH VL and downward for the GlideScope, but there was no statistically significant (P = .71) difference in overall use between the 2 instruments (Figure 1).
To examine the observed usage trends between the 2 VL during the first and last 12 months, a univariate ANOVA was conducted with the 2 time periods entered as predictors in the model. Video laryngoscopy intubations were performed (P = .001) more frequently with the GlideScope during the first 12 months; however, use of the McGRATH VL increased (P < .001) during the following 12 months compared to GlideScope. The GlideScope accounted for 54% of all VL intubations during the first 12 months, with the McGRATH accounting for 58% of all video laryngoscopy procedures for months 12 to 24. Additionally, the increase in video laryngoscopy procedures with the McGRATH during the last 3 months of the study period was despite an overall reduction in surgical volume due to the COVID-19 crisis, defined for this study as March 1, 2020, to May 31, 2020 (Figure 1). There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VL for that period. The anesthesia personnel’s use of the McGRATH VL increased to 61% of all video laryngoscopy cases, compared to 37% for the GlideScope (Figure 2).
The total costs calculated for equipment, blades, and repairs are presented in Table 1 and yearly total costs are shown in Figure 3. Overall costs were $181 093 lower (55.5%) for the McGRATH VL compared to the GlideScope over the 24-month period. The mean (SD) monthly costs for GlideScope VL blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for the McGRATH VL blades. Most of the total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for the GlideScope compared to the McGRATH VL. The monthly blade costs alone were higher (P < .001) for the GlideScope over the 2-year period; however, the McGRATH VL required use of disposable stylets at a cost of $10 177 for all endotracheal intubations, compared to $700 for the GlideScope device.
An analysis was performed to determine whether costs differed between those 2 instruments during the COVID-19 period. There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VLs during that period. The calculated blade cost difference for the COVID period was $128 higher for the McGRATH even though 293 more intubations were performed with that device (Table 2).
Discussion
We attempted to provide useful cost estimates by presenting pricing data reflecting the approximate cost that most large institutional anesthesia practices would incur for using those 2 specific devices and related peripherals. The main findings of our analysis showed that use of the McGRATH MAC VL resulted in a 55% cost savings compared to the GlideScope, with a similar number of cases performed with each device over the 24-month study period. We believe this represents a substantial savings to the department and institution, which has prompted internal review on the use of video laryngoscopy equipment. None of the McGRATH units failed; however, the GlideScope required 3 baton replacements.
Of note, use of the McGRATH MAC increased during the COVID-19 period, which may be explained by the fact that the operators found it to be a more portable device. Several physicians in the department commented that its smaller size made the McGRATH MAC more practical during the time when a plexiglass box was being used around the patient’s head to shield the intubator from aerosolized viral particles.
Although this study demonstrated the cost-saving value of the McGRATH over the GlideScope, a suggested next step would be to examine resource utilization related to video laryngoscopy use. The more dynamic tracking of the use of these devices should facilitate the assessment of existing related resources and decision making, to optimize the benefits of this initiative. We would anticipate reduced use of anesthesia personnel, such as technicians to assist with the management of this device which could be significant. As new respiratory viruses are appearing each year, video laryngoscopy will continue to gain increasing use in operating rooms and acute care locations. The adding of protective barriers between patients and providers calls for use of the most practical and effective VL devices, to protect personnel who are at high risk of contamination from airway secretions and aerosolized particles.9,10
The COVID-19 pandemic has demonstrated the value of anesthesiology in regards to analyzing and finding solutions to effectively manage infected patients or those suspected of infection in the perioperative environment. Inexpensive products are often avoided because cheaper devices are associated with being of lower quality. However, the association with cost and quality—and the assumption that a higher price is positively correlated with higher quality—is overall inconsistent in the medical literature.11 A more effective or higher quality treatment does not necessarily cost more and may actually end up costing less,12 as was the case in this study. We have been able to directly cut departmental expenses by using a more efficient and cost-effective device for intubations, without compromising safety and efficacy. Future studies should determine whether this significant reduction in costs from video laryngoscopy intubations with the McGRATH VL will be sustained across anesthesiology departments in the Jefferson Health Enterprise Hospitals, or other health systems, as well as its impact on workflow and personnel resources.
This analysis was restricted to one of the campuses of the Jefferson Health Enterprise. However, this is the largest anesthesia practice, encompassing several locations, which should reflect the general practice patterns across other anesthesiology departments in this large institution. The costs for the devices and peripherals may vary across anesthesia practices depending on volume and contracts negotiated with the suppliers. It was not possible to estimate this variability, which could change the total costs by a few percentage points. We recognize that there may be other costs associated with securing the McGRATH VL to prevent loss from theft or misplacement, which were not included in the study. Lastly, the inability to obtain randomized samples for the 2 groups treated with each device opens up the possibility of selection bias. There were, however, multiple intubators who were free to select 1 of the devices for endotracheal intubation, which may have reduced the effect of selection bias.
Conclusion
This study demonstrated that over a 24-month period use of the McGRATH MAC VL resulted in a cost reduction of around 55% compared to using the GlideScope for endotracheal intubation procedures performed at a major academic center. Over the first 3 months of the COVID-19 crisis, which our study included, use of the McGRATH VL increased while GlideScope use decreased. This was most likely related to the portability and smaller size of the McGRATH, which better facilitated intubations of COVID-19 patients.
Acknowledgements: The authors thank Craig Smith, Senior Anesthesia Technician, for his assistance with the cost information and excellent record-keeping related to the use of video laryngoscopes.
Corresponding author: Marc C. Torjman, PhD, Professor, Department of Anesthesiology, Sidney Kimmel Medical College at Thomas Jefferson University, 111 South 11th St, Suite G-8290, Philadelphia, PA 19107; Marc.Torjman@Jefferson.edu.
Financial disclosures: Dr. Thaler has served as a consultant for Medtronic since September 2020. He has participated in 2 webinars on the routine use of video laryngoscopy.
Funding: This study was supported by the Department of Anesthesiology at Thomas Jefferson University.
From the Department of Anesthesiology, Thomas Jefferson University and Hospitals, Sidney Kimmel Medical College, Philadelphia, PA, and Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA.
Objective: Retrospective study examining hospital cost information of patients requiring endotracheal intubation with video laryngoscopy. Provide a practical cost assessment on use of the McGRATH and GlideScope video laryngoscopes (VLs).
Methods: This study examined 52 hospital locations within a single, large university hospital, with most of those locations being hospital operating rooms. A total of 34 600 endotracheal intubations performed over 24 months, of which 11 345 were video laryngoscopies. Electronic medical records containing demographic data and information related to endotracheal intubation procedures, with monthly breakdowns between GlideScope and McGRATH intubations, were reviewed. Cost information calculated for equipment, blades, batteries, repairs, and subsequent analysis performed to determine cost differences between those 2 instruments during the COVID-19 period.
Results: A total of 5501 video laryngoscopy procedures were performed using the McGRATH VL and 5305 were performed using the GlideScope VL. Costs over 24 months were $181 093 lower (55.5%) for McGRATH compared to GlideScope. The mean (SD) monthly costs for GlideScope blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for McGRATH blades (P < .001). Most total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for GlideScope. During the COVID-19 period, the use of the McGRATH increased to 61% of all video laryngoscopy cases, compared to 37% for GlideScope (P < .001). Blade cost difference for the COVID-19 period was $128 higher for the McGRATH even though 293 more intubations were performed with that device.
Conclusions: Use of the McGRATH resulted in a cost savings of 55% compared to the GlideScope, and its use was highest during the COVID-19 period, which may be explained by its more portable and practical features.
Keywords: video laryngoscope; McGRATH; GlideScope; endotracheal intubation; hospital costs; COVID-19.
Hospitals have come to rely on video laryngoscopes (VLs) for tracheal intubation as necessary tools for better visualization of airways. Modern video laryngoscopy developed in the 2000s1 as a progression from direct laryngoscopy, which began in 1852 when Horace Green used a bent tongue spatula and sunlight to examine a child.2 VLs have seen many improvements and adaptations of their own, resulting in many different styles and types circulating around hospitals. The GlideScope (Verathon Inc, Bothell, WA) and the McGRATH (Medtronic, Minneapolis, MN) are examples of such instruments, which are now widely used in the US and are the 2 VLs of choice at our institution.
A few studies have compared VLs to direct laryngoscopes. In their systematic review, Lewis et al have shown the numerous benefits of using a VL over a direct laryngoscope. Some general conclusions were that the use of video laryngoscopy reduced the number of failed intubations, decreased laryngeal trauma, and provided improved visualizations.3 Other studies have compared the different types of VLs, including the McGRATH and the GlideScope, examining factors such as intubation time and display quality of the image. Two studies found that medical students were equally successful at using both the McGRATH and the GlideScope,4,5 while another study found that care providers using the GlideScope had quicker intubation times.6 Lastly, Savoldelli et al concluded that more providers preferred the McGRATH, which provided better laryngeal views,7 while their subsequent study showed more favorable learning curves of the Airtraq compared to the McGRATH and other VLs.8
Although there have been no reported differences in safety and effectiveness of the McGRATH and GlideScope devices, cost data on the use of these 2 popular laryngoscopes are lacking. Such information is important considering the increasing costs of medical technologies and the significant financial losses experienced by health care systems due to the COVID-19 crisis. The purpose of this retrospective cohort study was to compare the cost efficiency of the McGRATH MAC and GlideScope Core VLs at a large academic center.
Methods
This retrospective study was performed under exemption from the Thomas Jefferson University Institutional Review Board. The primary data sources consisted of hospital electronic patient records (EPIC) and cost information from the device manufacturers and hospital staff. The electronic patient data were provided by the EPIC Enterprise Analytics Business Intelligence group at Thomas Jefferson University Hospital (Center City Campus, Philadelphia, PA), while device costs were obtained from Verathon, Medtronic, and departmental staff responsible for purchasing equipment. Monthly data were obtained over a 24-month period (June 2018 through May 2020) when the McGRATH VL was placed into use in the department of anesthesiology. The 2 types of VLs were made available for use in a total of 52 locations, with the majority being hospital operating rooms.
The following variables were recorded: number of endotracheal intubations performed each month with breakdown between video laryngoscopy and flexible bronchoscopy airways, frequency of use for each type of laryngoscope, blades used, and equipment costs for use of each laryngoscope. Hospital cost estimates for both the McGRATH and GlideScope laryngoscopes included batteries, handles, blades, and the devices themselves. Cost data were also collected on frequency of device failure, maintenance, and replacement of parts and lost equipment.
Analysis
De-identified electronic medical records consisted of nominal and quantitative variables, with demographic data and information related to the endotracheal intubation procedure. All data were in chronological order and sorted by date after which coding was applied, to identify device type and allocate pertinent cost information. Descriptive statistics were reported as mean (SD) and sum for costs; frequency tables were generated for intubation procedures according to device type and time periods. Data were analyzed using the χ2 test, the student t test, and the Wilcoxon Mann-Whitney U test, with a P value set at .05 for statistical significance. SPSS version 26 and GraphPad Prism version 6 were used for all statistical analyses.
Results
A total of 34 600 endotracheal intubations were performed over the 24-month study period, and 11 345 (32.8%) were video laryngoscopy procedures. Out of all video laryngoscopy procedures, 5501 (48.5%) were performed using the McGRATH VL and 5305 (46.8%) were conducted using the GlideScope VL. The difference of 539 (4.8%) cases accounts for flexible bronchoscopy procedures and endotracheal intubations using other video laryngoscopy equipment. The mean (SD) monthly number of video laryngoscopy procedures for the 24 months was 221 (54) and 229 (89) for the GlideScope and McGRATH devices, respectively. Monthly endotracheal intubation distributions over 24 months trended upward for the McGRATH VL and downward for the GlideScope, but there was no statistically significant (P = .71) difference in overall use between the 2 instruments (Figure 1).
To examine the observed usage trends between the 2 VL during the first and last 12 months, a univariate ANOVA was conducted with the 2 time periods entered as predictors in the model. Video laryngoscopy intubations were performed (P = .001) more frequently with the GlideScope during the first 12 months; however, use of the McGRATH VL increased (P < .001) during the following 12 months compared to GlideScope. The GlideScope accounted for 54% of all VL intubations during the first 12 months, with the McGRATH accounting for 58% of all video laryngoscopy procedures for months 12 to 24. Additionally, the increase in video laryngoscopy procedures with the McGRATH during the last 3 months of the study period was despite an overall reduction in surgical volume due to the COVID-19 crisis, defined for this study as March 1, 2020, to May 31, 2020 (Figure 1). There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VL for that period. The anesthesia personnel’s use of the McGRATH VL increased to 61% of all video laryngoscopy cases, compared to 37% for the GlideScope (Figure 2).
The total costs calculated for equipment, blades, and repairs are presented in Table 1 and yearly total costs are shown in Figure 3. Overall costs were $181 093 lower (55.5%) for the McGRATH VL compared to the GlideScope over the 24-month period. The mean (SD) monthly costs for GlideScope VL blades were $3837 ($1050) and $3236 ($538) for years 1 and 2, respectively, vs $1652 ($663) and $2933 ($585) for the McGRATH VL blades. Most of the total cost differences were attributed to equipment and blade purchases, which were $202 595 (65.0%) higher for the GlideScope compared to the McGRATH VL. The monthly blade costs alone were higher (P < .001) for the GlideScope over the 2-year period; however, the McGRATH VL required use of disposable stylets at a cost of $10 177 for all endotracheal intubations, compared to $700 for the GlideScope device.
An analysis was performed to determine whether costs differed between those 2 instruments during the COVID-19 period. There was a statistically significant (P < .001) difference in the case distribution between use of the McGRATH and GlideScope VLs during that period. The calculated blade cost difference for the COVID period was $128 higher for the McGRATH even though 293 more intubations were performed with that device (Table 2).
Discussion
We attempted to provide useful cost estimates by presenting pricing data reflecting the approximate cost that most large institutional anesthesia practices would incur for using those 2 specific devices and related peripherals. The main findings of our analysis showed that use of the McGRATH MAC VL resulted in a 55% cost savings compared to the GlideScope, with a similar number of cases performed with each device over the 24-month study period. We believe this represents a substantial savings to the department and institution, which has prompted internal review on the use of video laryngoscopy equipment. None of the McGRATH units failed; however, the GlideScope required 3 baton replacements.
Of note, use of the McGRATH MAC increased during the COVID-19 period, which may be explained by the fact that the operators found it to be a more portable device. Several physicians in the department commented that its smaller size made the McGRATH MAC more practical during the time when a plexiglass box was being used around the patient’s head to shield the intubator from aerosolized viral particles.
Although this study demonstrated the cost-saving value of the McGRATH over the GlideScope, a suggested next step would be to examine resource utilization related to video laryngoscopy use. The more dynamic tracking of the use of these devices should facilitate the assessment of existing related resources and decision making, to optimize the benefits of this initiative. We would anticipate reduced use of anesthesia personnel, such as technicians to assist with the management of this device which could be significant. As new respiratory viruses are appearing each year, video laryngoscopy will continue to gain increasing use in operating rooms and acute care locations. The adding of protective barriers between patients and providers calls for use of the most practical and effective VL devices, to protect personnel who are at high risk of contamination from airway secretions and aerosolized particles.9,10
The COVID-19 pandemic has demonstrated the value of anesthesiology in regards to analyzing and finding solutions to effectively manage infected patients or those suspected of infection in the perioperative environment. Inexpensive products are often avoided because cheaper devices are associated with being of lower quality. However, the association with cost and quality—and the assumption that a higher price is positively correlated with higher quality—is overall inconsistent in the medical literature.11 A more effective or higher quality treatment does not necessarily cost more and may actually end up costing less,12 as was the case in this study. We have been able to directly cut departmental expenses by using a more efficient and cost-effective device for intubations, without compromising safety and efficacy. Future studies should determine whether this significant reduction in costs from video laryngoscopy intubations with the McGRATH VL will be sustained across anesthesiology departments in the Jefferson Health Enterprise Hospitals, or other health systems, as well as its impact on workflow and personnel resources.
This analysis was restricted to one of the campuses of the Jefferson Health Enterprise. However, this is the largest anesthesia practice, encompassing several locations, which should reflect the general practice patterns across other anesthesiology departments in this large institution. The costs for the devices and peripherals may vary across anesthesia practices depending on volume and contracts negotiated with the suppliers. It was not possible to estimate this variability, which could change the total costs by a few percentage points. We recognize that there may be other costs associated with securing the McGRATH VL to prevent loss from theft or misplacement, which were not included in the study. Lastly, the inability to obtain randomized samples for the 2 groups treated with each device opens up the possibility of selection bias. There were, however, multiple intubators who were free to select 1 of the devices for endotracheal intubation, which may have reduced the effect of selection bias.
Conclusion
This study demonstrated that over a 24-month period use of the McGRATH MAC VL resulted in a cost reduction of around 55% compared to using the GlideScope for endotracheal intubation procedures performed at a major academic center. Over the first 3 months of the COVID-19 crisis, which our study included, use of the McGRATH VL increased while GlideScope use decreased. This was most likely related to the portability and smaller size of the McGRATH, which better facilitated intubations of COVID-19 patients.
Acknowledgements: The authors thank Craig Smith, Senior Anesthesia Technician, for his assistance with the cost information and excellent record-keeping related to the use of video laryngoscopes.
Corresponding author: Marc C. Torjman, PhD, Professor, Department of Anesthesiology, Sidney Kimmel Medical College at Thomas Jefferson University, 111 South 11th St, Suite G-8290, Philadelphia, PA 19107; Marc.Torjman@Jefferson.edu.
Financial disclosures: Dr. Thaler has served as a consultant for Medtronic since September 2020. He has participated in 2 webinars on the routine use of video laryngoscopy.
Funding: This study was supported by the Department of Anesthesiology at Thomas Jefferson University.
1. Channa AB. Video laryngoscopes. Saudi J Anaesth. 2011;5(4):357-359.
2. Pieters BM, Eindhoven GB, Acott C, Van Zundert AAJ. Pioneers of laryngoscopy: indirect, direct and video laryngoscopy. Anaesth Intensive Care. 2015;43(suppl):4-11.
3. Lewis SR, Butler AR, Parker J, et al. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev. 2016;11(11):CD011136.
4. Kim W, Choi HJ, Lim T, Kang BS. Can the new McGrath laryngoscope rival the GlideScope Ranger portable video laryngoscope? A randomized manikin study. Am J Emerg Med. 2014;32(10):1225-1229.
5. Kim W, Choi HJ, Lim T, et al. Is McGrath MAC better than Glidescope Ranger for novice providers in the simulated difficult airway? A randomized manikin study. Resuscitation. 2014;85(suppl 1):S32.
6. Jeon WJ, Kim KH, Yeom JH, et al. A comparison of the Glidescope to the McGrath videolaryngoscope in patients. Korean J Anesthesiol. 2011;61(1):19-23.
7. Savoldelli GL, Schiffer E, Abegg C, et al. Comparison of the Glidescope, the McGrath, the Airtraq and the Macintosh laryngoscopes in simulated difficult airways. Anaesthesia. 2008;63(12):1358-1364.
8. Savoldelli GL, Schiffer E, Abegg C, et al. Learning curves of the Glidescope, the McGrath and the Airtraq laryngoscopes: a manikin study. Eur J Anaesthesiol. 2009;26(7):554-558.
9. Schumacher J, Arlidge J, Dudley D, et al. The impact of respiratory protective equipment on difficult airway management: a randomised, crossover, simulation study. Anaesthesia. 2020;75(10):1301-1306.
10. De Jong A, Pardo E, Rolle A, et al. Airway management for COVID-19: a move towards universal videolaryngoscope? Lancet Respir Med. 2020;8(6):555.
11. Hussey PS, Wertheimer S, Mehrotra A. The association between health care quality and cost: a systematic review. Ann Intern Med. 2013;158(1):27-34.
12. Mitton C, Dionne F, Peacock S, Sheps S. Quality and cost in healthcare: a relationship worth examining. Appl Health Econ Health Policy. 2006;5(4):201-208.
1. Channa AB. Video laryngoscopes. Saudi J Anaesth. 2011;5(4):357-359.
2. Pieters BM, Eindhoven GB, Acott C, Van Zundert AAJ. Pioneers of laryngoscopy: indirect, direct and video laryngoscopy. Anaesth Intensive Care. 2015;43(suppl):4-11.
3. Lewis SR, Butler AR, Parker J, et al. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev. 2016;11(11):CD011136.
4. Kim W, Choi HJ, Lim T, Kang BS. Can the new McGrath laryngoscope rival the GlideScope Ranger portable video laryngoscope? A randomized manikin study. Am J Emerg Med. 2014;32(10):1225-1229.
5. Kim W, Choi HJ, Lim T, et al. Is McGrath MAC better than Glidescope Ranger for novice providers in the simulated difficult airway? A randomized manikin study. Resuscitation. 2014;85(suppl 1):S32.
6. Jeon WJ, Kim KH, Yeom JH, et al. A comparison of the Glidescope to the McGrath videolaryngoscope in patients. Korean J Anesthesiol. 2011;61(1):19-23.
7. Savoldelli GL, Schiffer E, Abegg C, et al. Comparison of the Glidescope, the McGrath, the Airtraq and the Macintosh laryngoscopes in simulated difficult airways. Anaesthesia. 2008;63(12):1358-1364.
8. Savoldelli GL, Schiffer E, Abegg C, et al. Learning curves of the Glidescope, the McGrath and the Airtraq laryngoscopes: a manikin study. Eur J Anaesthesiol. 2009;26(7):554-558.
9. Schumacher J, Arlidge J, Dudley D, et al. The impact of respiratory protective equipment on difficult airway management: a randomised, crossover, simulation study. Anaesthesia. 2020;75(10):1301-1306.
10. De Jong A, Pardo E, Rolle A, et al. Airway management for COVID-19: a move towards universal videolaryngoscope? Lancet Respir Med. 2020;8(6):555.
11. Hussey PS, Wertheimer S, Mehrotra A. The association between health care quality and cost: a systematic review. Ann Intern Med. 2013;158(1):27-34.
12. Mitton C, Dionne F, Peacock S, Sheps S. Quality and cost in healthcare: a relationship worth examining. Appl Health Econ Health Policy. 2006;5(4):201-208.
Doctor, PA, face lawsuit after patient dies of COVID-19
, claiming the health providers failed to properly test the man and rendered improper care that led to his demise.
Shirley Dimoh of Memphis alleges her husband Peter Dimoh, 66, received inadequate care when he presented with COVID-19 symptoms to May Medical Group in Munford, Tenn., on November 19, 2020. Physician assistant Robert Moody ordered a COVID-19 blood test for Mr. Dimoh, rather than a nasal swab test, which was sent to an Atlanta lab for analysis, according to the lawsuit.
By the time the Dimohs were informed of the positive result on November 23, Mr. Dimoh was seriously ill and showed signs of severe infection, the claim alleges. Family physician David Krapf, DO, then prescribed methocarbamol, a muscle relaxant, which the complaint claims exacerbated Mr. Dimoh’s infection, caused serious adverse reactions, and led to his death on December 16, 2020.
“Mr. Dimoh had multiple comorbid conditions and he had a positive test, he should have been referred to a specialist at a higher level of care,” said Duncan E. Ragsdale, a Memphis-based attorney representing Shirley Dimoh. “This is not something for a family physician or a physician assistant to be attempting to handle. It’s my belief this was a preventable death.”
Shirley Dimoh filed a lawsuit against May Medical Group, Moody, Krapf, and several others on June 23, 2021, in the Circuit Court of Tennessee, 13th Judicial District. She accuses the group of negligence, failure to refer, and failure to supervise, among other claims. She is requesting $5 million in damages.
May Medical Group did not return phone or email messages seeking comment for this story. The group had not issued a reply to the lawsuit as of this article’s deadline. An attorney for the practice is not yet listed in court records.
Wife had COVID-19 first, treated by same PA
Shirley Dimoh was the first of the couple to contract COVID-19. She visited May Medical Group with COVID-19 symptoms on November 9, according to the lawsuit. The same physician assistant allegedly prescribed antibiotics and sent Shirley Dimoh to the health department for a rapid nasal swab test. After a positive test resulted, she was prescribed more antibiotics, steroids, and other medications, according to the claim. She recovered without complications.
The plaintiff alleges the medical practice did not warn Peter Dimoh of the risk of contracting COVID-19 from contact with Shirley Dimoh or offer prophylactics against infection. Peter Dimoh had underlying conditions that included diabetes and kidney failure, according to Mr. Ragsdale.
It’s unclear why Peter Dimoh may have been prescribed methocarbamol after his positive COVID-19 test on November 23. The same day, Shirley Dimoh went to the pharmacy to pick up her husband’s prescription because he was too sick to go himself, the complaint states. Mr. Dimoh took the medication three times a day as prescribed. The methocarbamol was “unreasonably dangerous” for Mr. Dimoh at the time and caused an injury he would have not incurred otherwise, the suit claims.
On November 28, Mr. Dimoh collapsed and was taken by ambulance to Methodist Hospital in Memphis. He was treated for COVID-19 as well as bacterial pneumonia, severe sepsis, and sytemic inflammatory response syndrome, according to the complaint. He died December 16 from respiratory and heart failure.
“What’s interesting about this case is that you’ve got a good example and a bad example together,” Mr. Ragsdale said. “In other words, the good example is they treated her appropriately, she recovered. They didn’t treat him at all, he died. I don’t know how you could have a better counter position established by the same practice.”
Family has sued for malpractice before
Before his death, Peter Dimoh was the plaintiff in another medical negligence suit. In 2013, he sued the Center for Oral and Facial Surgery of Memphis and two oral surgeons for allegedly operating on him improperly and causing an adverse outcome.
Mr. Dimoh underwent oral surgery on February 8, 2012, at the center. The day of his operation, Mr. Dimoh’s A1c and glucose levels were grossly elevated, according to the claim, which was also represented by Mr. Ragsdale. Surgeons concluded, incorrectly, that Mr. Dimoh’s diabetes was under control, the complaint alleges, failed to order preoperative antibiotics, operated on him, and caused a bacterial infection at the operative site. The infection allegedly resulted in osteomyelitis of Mr. Dimoh’s left mandible with a pathologic fracture.
The complaint also alleges that although Mr. Dimoh signed a consent form for the surgery, the defendants failed to obtain his consent because they were unaware his diabetes was not under control and they did not explain the risks of surgery while in such a condition. The suit alleges lack of informed consent, negligence, and gross negligence by the practice and requests $2 million in damages.
Court documents show the suit was voluntarily withdrawn in 2018 without prejudice and reissued in 2019. In January 2021, the court was given notice of Mr. Dimoh’s death, and a motion was made to substitute another plaintiff, according to Shelby County court records.
An attorney for the Center for Oral and Facial Surgery of Memphis did not return a message seeking comment.
A version of this article first appeared on Medscape.com.
, claiming the health providers failed to properly test the man and rendered improper care that led to his demise.
Shirley Dimoh of Memphis alleges her husband Peter Dimoh, 66, received inadequate care when he presented with COVID-19 symptoms to May Medical Group in Munford, Tenn., on November 19, 2020. Physician assistant Robert Moody ordered a COVID-19 blood test for Mr. Dimoh, rather than a nasal swab test, which was sent to an Atlanta lab for analysis, according to the lawsuit.
By the time the Dimohs were informed of the positive result on November 23, Mr. Dimoh was seriously ill and showed signs of severe infection, the claim alleges. Family physician David Krapf, DO, then prescribed methocarbamol, a muscle relaxant, which the complaint claims exacerbated Mr. Dimoh’s infection, caused serious adverse reactions, and led to his death on December 16, 2020.
“Mr. Dimoh had multiple comorbid conditions and he had a positive test, he should have been referred to a specialist at a higher level of care,” said Duncan E. Ragsdale, a Memphis-based attorney representing Shirley Dimoh. “This is not something for a family physician or a physician assistant to be attempting to handle. It’s my belief this was a preventable death.”
Shirley Dimoh filed a lawsuit against May Medical Group, Moody, Krapf, and several others on June 23, 2021, in the Circuit Court of Tennessee, 13th Judicial District. She accuses the group of negligence, failure to refer, and failure to supervise, among other claims. She is requesting $5 million in damages.
May Medical Group did not return phone or email messages seeking comment for this story. The group had not issued a reply to the lawsuit as of this article’s deadline. An attorney for the practice is not yet listed in court records.
Wife had COVID-19 first, treated by same PA
Shirley Dimoh was the first of the couple to contract COVID-19. She visited May Medical Group with COVID-19 symptoms on November 9, according to the lawsuit. The same physician assistant allegedly prescribed antibiotics and sent Shirley Dimoh to the health department for a rapid nasal swab test. After a positive test resulted, she was prescribed more antibiotics, steroids, and other medications, according to the claim. She recovered without complications.
The plaintiff alleges the medical practice did not warn Peter Dimoh of the risk of contracting COVID-19 from contact with Shirley Dimoh or offer prophylactics against infection. Peter Dimoh had underlying conditions that included diabetes and kidney failure, according to Mr. Ragsdale.
It’s unclear why Peter Dimoh may have been prescribed methocarbamol after his positive COVID-19 test on November 23. The same day, Shirley Dimoh went to the pharmacy to pick up her husband’s prescription because he was too sick to go himself, the complaint states. Mr. Dimoh took the medication three times a day as prescribed. The methocarbamol was “unreasonably dangerous” for Mr. Dimoh at the time and caused an injury he would have not incurred otherwise, the suit claims.
On November 28, Mr. Dimoh collapsed and was taken by ambulance to Methodist Hospital in Memphis. He was treated for COVID-19 as well as bacterial pneumonia, severe sepsis, and sytemic inflammatory response syndrome, according to the complaint. He died December 16 from respiratory and heart failure.
“What’s interesting about this case is that you’ve got a good example and a bad example together,” Mr. Ragsdale said. “In other words, the good example is they treated her appropriately, she recovered. They didn’t treat him at all, he died. I don’t know how you could have a better counter position established by the same practice.”
Family has sued for malpractice before
Before his death, Peter Dimoh was the plaintiff in another medical negligence suit. In 2013, he sued the Center for Oral and Facial Surgery of Memphis and two oral surgeons for allegedly operating on him improperly and causing an adverse outcome.
Mr. Dimoh underwent oral surgery on February 8, 2012, at the center. The day of his operation, Mr. Dimoh’s A1c and glucose levels were grossly elevated, according to the claim, which was also represented by Mr. Ragsdale. Surgeons concluded, incorrectly, that Mr. Dimoh’s diabetes was under control, the complaint alleges, failed to order preoperative antibiotics, operated on him, and caused a bacterial infection at the operative site. The infection allegedly resulted in osteomyelitis of Mr. Dimoh’s left mandible with a pathologic fracture.
The complaint also alleges that although Mr. Dimoh signed a consent form for the surgery, the defendants failed to obtain his consent because they were unaware his diabetes was not under control and they did not explain the risks of surgery while in such a condition. The suit alleges lack of informed consent, negligence, and gross negligence by the practice and requests $2 million in damages.
Court documents show the suit was voluntarily withdrawn in 2018 without prejudice and reissued in 2019. In January 2021, the court was given notice of Mr. Dimoh’s death, and a motion was made to substitute another plaintiff, according to Shelby County court records.
An attorney for the Center for Oral and Facial Surgery of Memphis did not return a message seeking comment.
A version of this article first appeared on Medscape.com.
, claiming the health providers failed to properly test the man and rendered improper care that led to his demise.
Shirley Dimoh of Memphis alleges her husband Peter Dimoh, 66, received inadequate care when he presented with COVID-19 symptoms to May Medical Group in Munford, Tenn., on November 19, 2020. Physician assistant Robert Moody ordered a COVID-19 blood test for Mr. Dimoh, rather than a nasal swab test, which was sent to an Atlanta lab for analysis, according to the lawsuit.
By the time the Dimohs were informed of the positive result on November 23, Mr. Dimoh was seriously ill and showed signs of severe infection, the claim alleges. Family physician David Krapf, DO, then prescribed methocarbamol, a muscle relaxant, which the complaint claims exacerbated Mr. Dimoh’s infection, caused serious adverse reactions, and led to his death on December 16, 2020.
“Mr. Dimoh had multiple comorbid conditions and he had a positive test, he should have been referred to a specialist at a higher level of care,” said Duncan E. Ragsdale, a Memphis-based attorney representing Shirley Dimoh. “This is not something for a family physician or a physician assistant to be attempting to handle. It’s my belief this was a preventable death.”
Shirley Dimoh filed a lawsuit against May Medical Group, Moody, Krapf, and several others on June 23, 2021, in the Circuit Court of Tennessee, 13th Judicial District. She accuses the group of negligence, failure to refer, and failure to supervise, among other claims. She is requesting $5 million in damages.
May Medical Group did not return phone or email messages seeking comment for this story. The group had not issued a reply to the lawsuit as of this article’s deadline. An attorney for the practice is not yet listed in court records.
Wife had COVID-19 first, treated by same PA
Shirley Dimoh was the first of the couple to contract COVID-19. She visited May Medical Group with COVID-19 symptoms on November 9, according to the lawsuit. The same physician assistant allegedly prescribed antibiotics and sent Shirley Dimoh to the health department for a rapid nasal swab test. After a positive test resulted, she was prescribed more antibiotics, steroids, and other medications, according to the claim. She recovered without complications.
The plaintiff alleges the medical practice did not warn Peter Dimoh of the risk of contracting COVID-19 from contact with Shirley Dimoh or offer prophylactics against infection. Peter Dimoh had underlying conditions that included diabetes and kidney failure, according to Mr. Ragsdale.
It’s unclear why Peter Dimoh may have been prescribed methocarbamol after his positive COVID-19 test on November 23. The same day, Shirley Dimoh went to the pharmacy to pick up her husband’s prescription because he was too sick to go himself, the complaint states. Mr. Dimoh took the medication three times a day as prescribed. The methocarbamol was “unreasonably dangerous” for Mr. Dimoh at the time and caused an injury he would have not incurred otherwise, the suit claims.
On November 28, Mr. Dimoh collapsed and was taken by ambulance to Methodist Hospital in Memphis. He was treated for COVID-19 as well as bacterial pneumonia, severe sepsis, and sytemic inflammatory response syndrome, according to the complaint. He died December 16 from respiratory and heart failure.
“What’s interesting about this case is that you’ve got a good example and a bad example together,” Mr. Ragsdale said. “In other words, the good example is they treated her appropriately, she recovered. They didn’t treat him at all, he died. I don’t know how you could have a better counter position established by the same practice.”
Family has sued for malpractice before
Before his death, Peter Dimoh was the plaintiff in another medical negligence suit. In 2013, he sued the Center for Oral and Facial Surgery of Memphis and two oral surgeons for allegedly operating on him improperly and causing an adverse outcome.
Mr. Dimoh underwent oral surgery on February 8, 2012, at the center. The day of his operation, Mr. Dimoh’s A1c and glucose levels were grossly elevated, according to the claim, which was also represented by Mr. Ragsdale. Surgeons concluded, incorrectly, that Mr. Dimoh’s diabetes was under control, the complaint alleges, failed to order preoperative antibiotics, operated on him, and caused a bacterial infection at the operative site. The infection allegedly resulted in osteomyelitis of Mr. Dimoh’s left mandible with a pathologic fracture.
The complaint also alleges that although Mr. Dimoh signed a consent form for the surgery, the defendants failed to obtain his consent because they were unaware his diabetes was not under control and they did not explain the risks of surgery while in such a condition. The suit alleges lack of informed consent, negligence, and gross negligence by the practice and requests $2 million in damages.
Court documents show the suit was voluntarily withdrawn in 2018 without prejudice and reissued in 2019. In January 2021, the court was given notice of Mr. Dimoh’s death, and a motion was made to substitute another plaintiff, according to Shelby County court records.
An attorney for the Center for Oral and Facial Surgery of Memphis did not return a message seeking comment.
A version of this article first appeared on Medscape.com.
Mt. Sinai leads nation in geriatric hospital services
The Cleveland Clinic in Ohio, and the Mayo Clinic in Rochester, Minn., followed.
Rounding out the top 10 hospitals in caring for patients older than age 75 were (4) UCLA Medical Center, Los Angeles; (5) NYU Langone Hospitals in New York; (6) Johns Hopkins Hospital in Baltimore; (7) New York–Presbyterian Hospital–Columbia and Cornell, New York; (8) Northwestern Memorial Hospital, Chicago; (9) UCSF Medical Center, San Francisco; and (10) Cedars-Sinai Medical Center, Los Angeles.
Those were followed by (11) Keck Medical Center of USC, Los Angeles; (12) University of Michigan Hospitals–Michigan Medicine, Ann Arbor; (13) UC San Diego Health–Jacobs Medical Center, San Diego; (14) Massachusetts General Hospital, Boston; (15) Stanford Health Care–Stanford Hospital, Palo Alto, Calif.; (16) Rush University Medical Center, Chicago; (17) Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia; (18) Brigham and Women’s Hospital, Boston; (19) Barnes-Jewish Hospital, St. Louis, Mo.; (tied for 19) UPMC Presbyterian Shadyside, Pittsburgh.
Data for the 2021-2022 edition of the “Best Hospitals” were not affected by the COVID-19 pandemic, which began after the end of the data collection period.
U.S. News also investigated racial disparities in health care and debuted health equity measures alongside each hospital’s rankings. Among other aspects of health equity, the new measures examine whether the patients each hospital treated reflect the racial and ethnic diversity of its community.
Ben Harder, managing editor and chief of health analysis, said in a statement, “At roughly four out of five hospitals, we found that the community’s minority residents were underrepresented among patients receiving services such as joint replacement, cancer surgery, and common heart procedures. Against this backdrop, however, we found important exceptions – hospitals that provide care to a disproportionate share of their community’s minority residents.”
U.S. News compared more than 4,750 medical centers nationwide in 15 specialties. Of those, 531 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care.
The top 20 hospitals overall were also named to the Honor Roll.
Mayo Clinic was again No. 1 on the honor roll, a ranking it has held for 6 years in a row, according to a press release. The Cleveland Clinic ranked No. 2, followed by UCLA Medical Center at No. 3.
In other top specialties, the University of Texas MD Anderson Cancer Center in Houston ranked No. 1 in cancer; the Cleveland Clinic is No. 1 in cardiology and heart surgery; and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
A full list of rankings is available on the website.
In 12 of the 15 specialty areas, including geriatrics, rankings are derived from data sources such as Medicare. In the other three specialties – ophthalmology, psychiatry, and rheumatology – ranking is determined by expert opinion based on responses from 3 years of surveys of physician specialists who were asked to name the hospitals to which they would likely refer their sickest patients.
This year’s analysis adds seven new procedures and conditions: Heart attack, stroke, pneumonia, diabetes, kidney failure, hip fracture, and back surgery (spinal fusion).
The expanded list will help patients, in consultation with their physicians, choose their hospital on the basis of the specific type of care they need with consideration of distance to a facility and insurance coverage.
A version of this article first appeared on Medscape.com.
The Cleveland Clinic in Ohio, and the Mayo Clinic in Rochester, Minn., followed.
Rounding out the top 10 hospitals in caring for patients older than age 75 were (4) UCLA Medical Center, Los Angeles; (5) NYU Langone Hospitals in New York; (6) Johns Hopkins Hospital in Baltimore; (7) New York–Presbyterian Hospital–Columbia and Cornell, New York; (8) Northwestern Memorial Hospital, Chicago; (9) UCSF Medical Center, San Francisco; and (10) Cedars-Sinai Medical Center, Los Angeles.
Those were followed by (11) Keck Medical Center of USC, Los Angeles; (12) University of Michigan Hospitals–Michigan Medicine, Ann Arbor; (13) UC San Diego Health–Jacobs Medical Center, San Diego; (14) Massachusetts General Hospital, Boston; (15) Stanford Health Care–Stanford Hospital, Palo Alto, Calif.; (16) Rush University Medical Center, Chicago; (17) Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia; (18) Brigham and Women’s Hospital, Boston; (19) Barnes-Jewish Hospital, St. Louis, Mo.; (tied for 19) UPMC Presbyterian Shadyside, Pittsburgh.
Data for the 2021-2022 edition of the “Best Hospitals” were not affected by the COVID-19 pandemic, which began after the end of the data collection period.
U.S. News also investigated racial disparities in health care and debuted health equity measures alongside each hospital’s rankings. Among other aspects of health equity, the new measures examine whether the patients each hospital treated reflect the racial and ethnic diversity of its community.
Ben Harder, managing editor and chief of health analysis, said in a statement, “At roughly four out of five hospitals, we found that the community’s minority residents were underrepresented among patients receiving services such as joint replacement, cancer surgery, and common heart procedures. Against this backdrop, however, we found important exceptions – hospitals that provide care to a disproportionate share of their community’s minority residents.”
U.S. News compared more than 4,750 medical centers nationwide in 15 specialties. Of those, 531 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care.
The top 20 hospitals overall were also named to the Honor Roll.
Mayo Clinic was again No. 1 on the honor roll, a ranking it has held for 6 years in a row, according to a press release. The Cleveland Clinic ranked No. 2, followed by UCLA Medical Center at No. 3.
In other top specialties, the University of Texas MD Anderson Cancer Center in Houston ranked No. 1 in cancer; the Cleveland Clinic is No. 1 in cardiology and heart surgery; and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
A full list of rankings is available on the website.
In 12 of the 15 specialty areas, including geriatrics, rankings are derived from data sources such as Medicare. In the other three specialties – ophthalmology, psychiatry, and rheumatology – ranking is determined by expert opinion based on responses from 3 years of surveys of physician specialists who were asked to name the hospitals to which they would likely refer their sickest patients.
This year’s analysis adds seven new procedures and conditions: Heart attack, stroke, pneumonia, diabetes, kidney failure, hip fracture, and back surgery (spinal fusion).
The expanded list will help patients, in consultation with their physicians, choose their hospital on the basis of the specific type of care they need with consideration of distance to a facility and insurance coverage.
A version of this article first appeared on Medscape.com.
The Cleveland Clinic in Ohio, and the Mayo Clinic in Rochester, Minn., followed.
Rounding out the top 10 hospitals in caring for patients older than age 75 were (4) UCLA Medical Center, Los Angeles; (5) NYU Langone Hospitals in New York; (6) Johns Hopkins Hospital in Baltimore; (7) New York–Presbyterian Hospital–Columbia and Cornell, New York; (8) Northwestern Memorial Hospital, Chicago; (9) UCSF Medical Center, San Francisco; and (10) Cedars-Sinai Medical Center, Los Angeles.
Those were followed by (11) Keck Medical Center of USC, Los Angeles; (12) University of Michigan Hospitals–Michigan Medicine, Ann Arbor; (13) UC San Diego Health–Jacobs Medical Center, San Diego; (14) Massachusetts General Hospital, Boston; (15) Stanford Health Care–Stanford Hospital, Palo Alto, Calif.; (16) Rush University Medical Center, Chicago; (17) Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia; (18) Brigham and Women’s Hospital, Boston; (19) Barnes-Jewish Hospital, St. Louis, Mo.; (tied for 19) UPMC Presbyterian Shadyside, Pittsburgh.
Data for the 2021-2022 edition of the “Best Hospitals” were not affected by the COVID-19 pandemic, which began after the end of the data collection period.
U.S. News also investigated racial disparities in health care and debuted health equity measures alongside each hospital’s rankings. Among other aspects of health equity, the new measures examine whether the patients each hospital treated reflect the racial and ethnic diversity of its community.
Ben Harder, managing editor and chief of health analysis, said in a statement, “At roughly four out of five hospitals, we found that the community’s minority residents were underrepresented among patients receiving services such as joint replacement, cancer surgery, and common heart procedures. Against this backdrop, however, we found important exceptions – hospitals that provide care to a disproportionate share of their community’s minority residents.”
U.S. News compared more than 4,750 medical centers nationwide in 15 specialties. Of those, 531 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care.
The top 20 hospitals overall were also named to the Honor Roll.
Mayo Clinic was again No. 1 on the honor roll, a ranking it has held for 6 years in a row, according to a press release. The Cleveland Clinic ranked No. 2, followed by UCLA Medical Center at No. 3.
In other top specialties, the University of Texas MD Anderson Cancer Center in Houston ranked No. 1 in cancer; the Cleveland Clinic is No. 1 in cardiology and heart surgery; and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
A full list of rankings is available on the website.
In 12 of the 15 specialty areas, including geriatrics, rankings are derived from data sources such as Medicare. In the other three specialties – ophthalmology, psychiatry, and rheumatology – ranking is determined by expert opinion based on responses from 3 years of surveys of physician specialists who were asked to name the hospitals to which they would likely refer their sickest patients.
This year’s analysis adds seven new procedures and conditions: Heart attack, stroke, pneumonia, diabetes, kidney failure, hip fracture, and back surgery (spinal fusion).
The expanded list will help patients, in consultation with their physicians, choose their hospital on the basis of the specific type of care they need with consideration of distance to a facility and insurance coverage.
A version of this article first appeared on Medscape.com.
Money buys life, and a cigarette maker wants to ‘unsmoke the world’
With COVID, the fun never ends
Welcome to America’s favorite pandemic-themed game show! Let’s play Covidiot Proof! And now, here’s your host, the lovely and talented Anthony Grouchy!

Tony: Hello everyone! Our first category today is America or [blank], and the first clue is for you, Don. This country requires “individuals to use a health pass to patronize indoor establishments such as restaurants, bars, nightclubs and cinemas.”
Don: Freedom-loving Americans would never stand for that, Tony, so I’m going to say Greece.
Tony: That’s correct, Don. One hundred points for you. Okay Joe, here’s your clue: In this country, some people wear disguises to get a COVID vaccination so their friends and families won’t find out.
Joe: Sounds like communism to me, Tony. I’ll say Cuba.
Tony: Sorry Joe, that’s incorrect. Don?
Don: The friends and families sound like freedom-loving Americans, so it must be America.
Tony: It is America. Missouri, to be exact. And now, one last question for both of you to win the game. True or false? Did the pastor of a church in Tennessee say that mask-wearers would be kicked out of the building because “I am not playing these Democrat games up in this church”?
Joe: That’s fake news, Tony. It’s gotta be false.
Tony: Incorrect! It’s absolutely true. That means today’s winner is … Joe? Yes, I’m being told that Tennessee goes to Joe.
Don: That’s bulls#&@! I won this thing! I’ll see you in court!
More money, more life
Does it seem to you that the wealthy live forever, while the less financially comfortable live shorter lives? If you answered, yes, it turns out that you’re right.

Researchers analyzed the effect of net worth at midlife with mortality. To take out genetic differences among the sample of 5,400 adults aged 46 years, the investigators also studied a subset of 2,490 twin and sibling pairs.
“The within-family association provides strong evidence that an association between wealth accumulation and life expectancy exists, because comparing siblings within the same family to each other controls for all of the life experience and biology that they share,” said coauthor Eric Finegood of Northwestern University, Chicago.
But what if one sibling has a history of cancer, heart disease, or other health conditions? The cost of treatment and employment limitations could affect someone’s ability to stack their wealth, right? Absolutely. The researchers took that into account and looked at only healthy individuals and found the same results. More money, longer life.
We have the policies and programs in place for heart health, diabetes prevention, and smoking cessation, as they are seen as major threats to public health. So why not do the same for financial security? A low bank account may just be more harmful.
Holding the ‘health care and wellness’ gun
Cigarettes are not good for us. We know this.

It’s, therefore, not surprising to learn that a business has requested for a U.K. ban on the sale of cigarettes by 2030. However, when that someone turns out to be the CEO of Philip Morris International, tobacco company and maker of Marlboro cigarettes, things get a little confusing.
Banning cigarettes, according to Jacek Olczak, would reduce confusion among consumers, many of whom feel that the alternatives are worse for their health. His company can “see the world without cigarettes ... and actually, the sooner it happens, the better it is for everyone.” A truly noble sentiment from the CEO of a large tobacco company. Nothing nefarious going on here.
And if those aren’t egregious business euphemisms, we don’t know what is.
Of course, for all the completely believable and sincere rhetoric, the fact is that Marlboros are still on the shelves. Philip Morris is still making and advertising them. If their concern was genuine, why wouldn’t they just stop manufacturing them now?
So, we ask ourselves if this a selfless act of kindness or is it an unscrupulous corporate act to get a leg up on their competitors? We’ll leave it up to the readers to decide.
Okay, we lied, it’s the second one.
Autopsy of the living dead
Imagine the absolute terror you’d feel if you opened your eyes to bright, blinding white lights only to see a bone saw 3 inches from your forehead and getting closer by the second. Horrifying for you, certainly, but think about the poor pathologist behind the saw who probably thought a zombie apocalypse was coming. This was close to being a reality for a 29-year-old prisoner at the Asturias Central Penitentiary in Spain.

Gonzalo Montoya Jiménez was discovered in his cell unresponsive. Three physicians examined him and found he was showing signs of death, such as cyanosis and rigor mortis. Mr. Jiménez was processed like any other body and was sent, in a body bag, to a hospital mortuary, where he spent time in a freezer for body preservation. Just before he was due for his autopsy, he began showing signs of life.
It’s not completely clear why this happened to poor Mr. Jiménez, but it was reported that he wasn’t feeling well the day before and that he has epilepsy. Hospital officials suggested he may have been cataleptic, possibly because he had trouble adhering to his medication schedule.
Mr. Jiménez was moved to another hospital under armed guard after coming back to life and regained consciousness after a day or so. Talk about cheating death.
With COVID, the fun never ends
Welcome to America’s favorite pandemic-themed game show! Let’s play Covidiot Proof! And now, here’s your host, the lovely and talented Anthony Grouchy!
Tony: Hello everyone! Our first category today is America or [blank], and the first clue is for you, Don. This country requires “individuals to use a health pass to patronize indoor establishments such as restaurants, bars, nightclubs and cinemas.”
Don: Freedom-loving Americans would never stand for that, Tony, so I’m going to say Greece.
Tony: That’s correct, Don. One hundred points for you. Okay Joe, here’s your clue: In this country, some people wear disguises to get a COVID vaccination so their friends and families won’t find out.
Joe: Sounds like communism to me, Tony. I’ll say Cuba.
Tony: Sorry Joe, that’s incorrect. Don?
Don: The friends and families sound like freedom-loving Americans, so it must be America.
Tony: It is America. Missouri, to be exact. And now, one last question for both of you to win the game. True or false? Did the pastor of a church in Tennessee say that mask-wearers would be kicked out of the building because “I am not playing these Democrat games up in this church”?
Joe: That’s fake news, Tony. It’s gotta be false.
Tony: Incorrect! It’s absolutely true. That means today’s winner is … Joe? Yes, I’m being told that Tennessee goes to Joe.
Don: That’s bulls#&@! I won this thing! I’ll see you in court!
More money, more life
Does it seem to you that the wealthy live forever, while the less financially comfortable live shorter lives? If you answered, yes, it turns out that you’re right.
Researchers analyzed the effect of net worth at midlife with mortality. To take out genetic differences among the sample of 5,400 adults aged 46 years, the investigators also studied a subset of 2,490 twin and sibling pairs.
“The within-family association provides strong evidence that an association between wealth accumulation and life expectancy exists, because comparing siblings within the same family to each other controls for all of the life experience and biology that they share,” said coauthor Eric Finegood of Northwestern University, Chicago.
But what if one sibling has a history of cancer, heart disease, or other health conditions? The cost of treatment and employment limitations could affect someone’s ability to stack their wealth, right? Absolutely. The researchers took that into account and looked at only healthy individuals and found the same results. More money, longer life.
We have the policies and programs in place for heart health, diabetes prevention, and smoking cessation, as they are seen as major threats to public health. So why not do the same for financial security? A low bank account may just be more harmful.
Holding the ‘health care and wellness’ gun
Cigarettes are not good for us. We know this.
It’s, therefore, not surprising to learn that a business has requested for a U.K. ban on the sale of cigarettes by 2030. However, when that someone turns out to be the CEO of Philip Morris International, tobacco company and maker of Marlboro cigarettes, things get a little confusing.
Banning cigarettes, according to Jacek Olczak, would reduce confusion among consumers, many of whom feel that the alternatives are worse for their health. His company can “see the world without cigarettes ... and actually, the sooner it happens, the better it is for everyone.” A truly noble sentiment from the CEO of a large tobacco company. Nothing nefarious going on here.
And if those aren’t egregious business euphemisms, we don’t know what is.
Of course, for all the completely believable and sincere rhetoric, the fact is that Marlboros are still on the shelves. Philip Morris is still making and advertising them. If their concern was genuine, why wouldn’t they just stop manufacturing them now?
So, we ask ourselves if this a selfless act of kindness or is it an unscrupulous corporate act to get a leg up on their competitors? We’ll leave it up to the readers to decide.
Okay, we lied, it’s the second one.
Autopsy of the living dead
Imagine the absolute terror you’d feel if you opened your eyes to bright, blinding white lights only to see a bone saw 3 inches from your forehead and getting closer by the second. Horrifying for you, certainly, but think about the poor pathologist behind the saw who probably thought a zombie apocalypse was coming. This was close to being a reality for a 29-year-old prisoner at the Asturias Central Penitentiary in Spain.
Gonzalo Montoya Jiménez was discovered in his cell unresponsive. Three physicians examined him and found he was showing signs of death, such as cyanosis and rigor mortis. Mr. Jiménez was processed like any other body and was sent, in a body bag, to a hospital mortuary, where he spent time in a freezer for body preservation. Just before he was due for his autopsy, he began showing signs of life.
It’s not completely clear why this happened to poor Mr. Jiménez, but it was reported that he wasn’t feeling well the day before and that he has epilepsy. Hospital officials suggested he may have been cataleptic, possibly because he had trouble adhering to his medication schedule.
Mr. Jiménez was moved to another hospital under armed guard after coming back to life and regained consciousness after a day or so. Talk about cheating death.
With COVID, the fun never ends
Welcome to America’s favorite pandemic-themed game show! Let’s play Covidiot Proof! And now, here’s your host, the lovely and talented Anthony Grouchy!
Tony: Hello everyone! Our first category today is America or [blank], and the first clue is for you, Don. This country requires “individuals to use a health pass to patronize indoor establishments such as restaurants, bars, nightclubs and cinemas.”
Don: Freedom-loving Americans would never stand for that, Tony, so I’m going to say Greece.
Tony: That’s correct, Don. One hundred points for you. Okay Joe, here’s your clue: In this country, some people wear disguises to get a COVID vaccination so their friends and families won’t find out.
Joe: Sounds like communism to me, Tony. I’ll say Cuba.
Tony: Sorry Joe, that’s incorrect. Don?
Don: The friends and families sound like freedom-loving Americans, so it must be America.
Tony: It is America. Missouri, to be exact. And now, one last question for both of you to win the game. True or false? Did the pastor of a church in Tennessee say that mask-wearers would be kicked out of the building because “I am not playing these Democrat games up in this church”?
Joe: That’s fake news, Tony. It’s gotta be false.
Tony: Incorrect! It’s absolutely true. That means today’s winner is … Joe? Yes, I’m being told that Tennessee goes to Joe.
Don: That’s bulls#&@! I won this thing! I’ll see you in court!
More money, more life
Does it seem to you that the wealthy live forever, while the less financially comfortable live shorter lives? If you answered, yes, it turns out that you’re right.
Researchers analyzed the effect of net worth at midlife with mortality. To take out genetic differences among the sample of 5,400 adults aged 46 years, the investigators also studied a subset of 2,490 twin and sibling pairs.
“The within-family association provides strong evidence that an association between wealth accumulation and life expectancy exists, because comparing siblings within the same family to each other controls for all of the life experience and biology that they share,” said coauthor Eric Finegood of Northwestern University, Chicago.
But what if one sibling has a history of cancer, heart disease, or other health conditions? The cost of treatment and employment limitations could affect someone’s ability to stack their wealth, right? Absolutely. The researchers took that into account and looked at only healthy individuals and found the same results. More money, longer life.
We have the policies and programs in place for heart health, diabetes prevention, and smoking cessation, as they are seen as major threats to public health. So why not do the same for financial security? A low bank account may just be more harmful.
Holding the ‘health care and wellness’ gun
Cigarettes are not good for us. We know this.
It’s, therefore, not surprising to learn that a business has requested for a U.K. ban on the sale of cigarettes by 2030. However, when that someone turns out to be the CEO of Philip Morris International, tobacco company and maker of Marlboro cigarettes, things get a little confusing.
Banning cigarettes, according to Jacek Olczak, would reduce confusion among consumers, many of whom feel that the alternatives are worse for their health. His company can “see the world without cigarettes ... and actually, the sooner it happens, the better it is for everyone.” A truly noble sentiment from the CEO of a large tobacco company. Nothing nefarious going on here.
And if those aren’t egregious business euphemisms, we don’t know what is.
Of course, for all the completely believable and sincere rhetoric, the fact is that Marlboros are still on the shelves. Philip Morris is still making and advertising them. If their concern was genuine, why wouldn’t they just stop manufacturing them now?
So, we ask ourselves if this a selfless act of kindness or is it an unscrupulous corporate act to get a leg up on their competitors? We’ll leave it up to the readers to decide.
Okay, we lied, it’s the second one.
Autopsy of the living dead
Imagine the absolute terror you’d feel if you opened your eyes to bright, blinding white lights only to see a bone saw 3 inches from your forehead and getting closer by the second. Horrifying for you, certainly, but think about the poor pathologist behind the saw who probably thought a zombie apocalypse was coming. This was close to being a reality for a 29-year-old prisoner at the Asturias Central Penitentiary in Spain.
Gonzalo Montoya Jiménez was discovered in his cell unresponsive. Three physicians examined him and found he was showing signs of death, such as cyanosis and rigor mortis. Mr. Jiménez was processed like any other body and was sent, in a body bag, to a hospital mortuary, where he spent time in a freezer for body preservation. Just before he was due for his autopsy, he began showing signs of life.
It’s not completely clear why this happened to poor Mr. Jiménez, but it was reported that he wasn’t feeling well the day before and that he has epilepsy. Hospital officials suggested he may have been cataleptic, possibly because he had trouble adhering to his medication schedule.
Mr. Jiménez was moved to another hospital under armed guard after coming back to life and regained consciousness after a day or so. Talk about cheating death.
Texas doctor stole identities, forged patient records in fraud scheme; more
Doctor guilty of fraud and identity theft gets 7 years in jail
Grigoriy T. Rodonaia, MD, a family physician in Port Neches, Tex., was convicted of 12 counts of healthcare fraud, three counts of aggravated identity theft, and one count of making a false statement toward the end of 2020.
Dr. Rodonaia began his criminal activity in 2015, when he issued more than 600 prescriptions for scar creams using information from more than 140 beneficiaries of TRICARE, a military healthcare program, without their knowledge or consent. Dr. Rodonaia also forged patients’ records to say that he had examined the patients, and he submitted fraudulent records to the Defense Health Agency in response to an audit.
Dr. Rodonaia was sentenced to 7 years in federal prison on June 24, 2021, and was ordered to pay $195,607.76 in restitution.
Psychiatric hospital and nursing staff sued for death of patient
Jeremiah Bagley, 37, died after being restrained by psychiatric nursing staff and injected with an antipsychotic and a sedative at the Rio Grande State Center, in Harlingen, Tex.
An autopsy revealed that Mr. Bagley had several fractured vertebrae, cracked ribs, a lacerated spleen, and multiple contusions on his upper body. The autopsy report lists the cause of death as “excited delirium due to psychosis with restraint-associated blunt force trauma.”
Mr. Bagley’s father filed a lawsuit naming the hospital and 10 employees as defendants, saying that his son’s civil rights were violated. The Texas Supreme Court ruled on April 16, 2021, that the staffers who were charged must submit expert reports, despite the fact that medical malpractice was not alleged. Usually, such a lawsuit would be dismissed because a report was not served by the statutory deadline, but in a 9-0 decision, the high court allowed the case to proceed.
Plaintiff attorney Katie P. Klein told the Claims Journal, “He probably struck someone and everybody got mad and they jumped him. He had four or five people on him, which was not permitted.”
Ob.gyn. gets 59 years in prison
Javaid Perwaiz, MD, a 71-year-old ob/gyn from Chesapeake, Va., was convicted of performing medically unnecessary and irreversible surgeries, including hysterectomies and sterilizations, on multiple patients for more than 10 years.
Karl Schumann, acting special agent in charge of the Federal Bureau of Investigation’s (FBI’s) Norfolk, Va. field office, said in a statement, “With unnecessary, invasive medical procedures, Dr Perwaiz not only caused enduring complications, pain, and anxiety to his patients, but he assaulted the most personal part of their lives and even robbed some of their future.”
Dr. Perwaiz was also convicted of 52 counts of healthcare fraud and of making false statements in late 2020. His fraud allegedly cost insurance programs nearly $21 million. The investigation began in September 2018 after a hospital employee contacted the FBI after suspecting that Dr. Perwaiz was performing unnecessary surgeries. More than 25 former patients testified at the trial, and the court received more than 60 victim impact statements.
Dr. Perwaiz had a long criminal history, according to the New York Times. In 1982, Dr. Perwaiz lost medical privileges at Maryview Hospital, in Portsmouth, Va., because of performing unnecessary surgeries and displaying poor clinical judgment. His medical license was reinstated in 1998.
Doctor who prescribed opioids out of car charged with murder
George M. Blatti, MD, a family physician in New York, was charged with five counts of murder for the opioid-related deaths of his patients and 11 counts of reckless endangerment in the first degree, according to the New York Times. Dr. Blatti’s medical license has been revoked, and he has pleaded not guilty.
Dr. Blatti had been seeing patients and giving prescriptions out of his car in parking lots, where he would prescribe pain medications without examining the patients. Many of these patients were struggling with addiction to opioids or other drugs. The alleged victims — three men and two women, who were between the ages of 30 and 60 — were prescribed 45,000 pills over 4 years, despite the fact that each showed clear signs of addiction, according to prosecutors.
Prosecutors allege that Dr. Blatti knew that several of his patients had died of overdoses, and he ignored pleas from their family members to stop enabling their addictions. They also say he ignored warnings from insurers about excessive opioid prescribing and was questioned by the New York State Office of Professional Medical Conduct about it in 2017.
A version of this article first appeared on Medscape.com.
Doctor guilty of fraud and identity theft gets 7 years in jail
Grigoriy T. Rodonaia, MD, a family physician in Port Neches, Tex., was convicted of 12 counts of healthcare fraud, three counts of aggravated identity theft, and one count of making a false statement toward the end of 2020.
Dr. Rodonaia began his criminal activity in 2015, when he issued more than 600 prescriptions for scar creams using information from more than 140 beneficiaries of TRICARE, a military healthcare program, without their knowledge or consent. Dr. Rodonaia also forged patients’ records to say that he had examined the patients, and he submitted fraudulent records to the Defense Health Agency in response to an audit.
Dr. Rodonaia was sentenced to 7 years in federal prison on June 24, 2021, and was ordered to pay $195,607.76 in restitution.
Psychiatric hospital and nursing staff sued for death of patient
Jeremiah Bagley, 37, died after being restrained by psychiatric nursing staff and injected with an antipsychotic and a sedative at the Rio Grande State Center, in Harlingen, Tex.
An autopsy revealed that Mr. Bagley had several fractured vertebrae, cracked ribs, a lacerated spleen, and multiple contusions on his upper body. The autopsy report lists the cause of death as “excited delirium due to psychosis with restraint-associated blunt force trauma.”
Mr. Bagley’s father filed a lawsuit naming the hospital and 10 employees as defendants, saying that his son’s civil rights were violated. The Texas Supreme Court ruled on April 16, 2021, that the staffers who were charged must submit expert reports, despite the fact that medical malpractice was not alleged. Usually, such a lawsuit would be dismissed because a report was not served by the statutory deadline, but in a 9-0 decision, the high court allowed the case to proceed.
Plaintiff attorney Katie P. Klein told the Claims Journal, “He probably struck someone and everybody got mad and they jumped him. He had four or five people on him, which was not permitted.”
Ob.gyn. gets 59 years in prison
Javaid Perwaiz, MD, a 71-year-old ob/gyn from Chesapeake, Va., was convicted of performing medically unnecessary and irreversible surgeries, including hysterectomies and sterilizations, on multiple patients for more than 10 years.
Karl Schumann, acting special agent in charge of the Federal Bureau of Investigation’s (FBI’s) Norfolk, Va. field office, said in a statement, “With unnecessary, invasive medical procedures, Dr Perwaiz not only caused enduring complications, pain, and anxiety to his patients, but he assaulted the most personal part of their lives and even robbed some of their future.”
Dr. Perwaiz was also convicted of 52 counts of healthcare fraud and of making false statements in late 2020. His fraud allegedly cost insurance programs nearly $21 million. The investigation began in September 2018 after a hospital employee contacted the FBI after suspecting that Dr. Perwaiz was performing unnecessary surgeries. More than 25 former patients testified at the trial, and the court received more than 60 victim impact statements.
Dr. Perwaiz had a long criminal history, according to the New York Times. In 1982, Dr. Perwaiz lost medical privileges at Maryview Hospital, in Portsmouth, Va., because of performing unnecessary surgeries and displaying poor clinical judgment. His medical license was reinstated in 1998.
Doctor who prescribed opioids out of car charged with murder
George M. Blatti, MD, a family physician in New York, was charged with five counts of murder for the opioid-related deaths of his patients and 11 counts of reckless endangerment in the first degree, according to the New York Times. Dr. Blatti’s medical license has been revoked, and he has pleaded not guilty.
Dr. Blatti had been seeing patients and giving prescriptions out of his car in parking lots, where he would prescribe pain medications without examining the patients. Many of these patients were struggling with addiction to opioids or other drugs. The alleged victims — three men and two women, who were between the ages of 30 and 60 — were prescribed 45,000 pills over 4 years, despite the fact that each showed clear signs of addiction, according to prosecutors.
Prosecutors allege that Dr. Blatti knew that several of his patients had died of overdoses, and he ignored pleas from their family members to stop enabling their addictions. They also say he ignored warnings from insurers about excessive opioid prescribing and was questioned by the New York State Office of Professional Medical Conduct about it in 2017.
A version of this article first appeared on Medscape.com.
Doctor guilty of fraud and identity theft gets 7 years in jail
Grigoriy T. Rodonaia, MD, a family physician in Port Neches, Tex., was convicted of 12 counts of healthcare fraud, three counts of aggravated identity theft, and one count of making a false statement toward the end of 2020.
Dr. Rodonaia began his criminal activity in 2015, when he issued more than 600 prescriptions for scar creams using information from more than 140 beneficiaries of TRICARE, a military healthcare program, without their knowledge or consent. Dr. Rodonaia also forged patients’ records to say that he had examined the patients, and he submitted fraudulent records to the Defense Health Agency in response to an audit.
Dr. Rodonaia was sentenced to 7 years in federal prison on June 24, 2021, and was ordered to pay $195,607.76 in restitution.
Psychiatric hospital and nursing staff sued for death of patient
Jeremiah Bagley, 37, died after being restrained by psychiatric nursing staff and injected with an antipsychotic and a sedative at the Rio Grande State Center, in Harlingen, Tex.
An autopsy revealed that Mr. Bagley had several fractured vertebrae, cracked ribs, a lacerated spleen, and multiple contusions on his upper body. The autopsy report lists the cause of death as “excited delirium due to psychosis with restraint-associated blunt force trauma.”
Mr. Bagley’s father filed a lawsuit naming the hospital and 10 employees as defendants, saying that his son’s civil rights were violated. The Texas Supreme Court ruled on April 16, 2021, that the staffers who were charged must submit expert reports, despite the fact that medical malpractice was not alleged. Usually, such a lawsuit would be dismissed because a report was not served by the statutory deadline, but in a 9-0 decision, the high court allowed the case to proceed.
Plaintiff attorney Katie P. Klein told the Claims Journal, “He probably struck someone and everybody got mad and they jumped him. He had four or five people on him, which was not permitted.”
Ob.gyn. gets 59 years in prison
Javaid Perwaiz, MD, a 71-year-old ob/gyn from Chesapeake, Va., was convicted of performing medically unnecessary and irreversible surgeries, including hysterectomies and sterilizations, on multiple patients for more than 10 years.
Karl Schumann, acting special agent in charge of the Federal Bureau of Investigation’s (FBI’s) Norfolk, Va. field office, said in a statement, “With unnecessary, invasive medical procedures, Dr Perwaiz not only caused enduring complications, pain, and anxiety to his patients, but he assaulted the most personal part of their lives and even robbed some of their future.”
Dr. Perwaiz was also convicted of 52 counts of healthcare fraud and of making false statements in late 2020. His fraud allegedly cost insurance programs nearly $21 million. The investigation began in September 2018 after a hospital employee contacted the FBI after suspecting that Dr. Perwaiz was performing unnecessary surgeries. More than 25 former patients testified at the trial, and the court received more than 60 victim impact statements.
Dr. Perwaiz had a long criminal history, according to the New York Times. In 1982, Dr. Perwaiz lost medical privileges at Maryview Hospital, in Portsmouth, Va., because of performing unnecessary surgeries and displaying poor clinical judgment. His medical license was reinstated in 1998.
Doctor who prescribed opioids out of car charged with murder
George M. Blatti, MD, a family physician in New York, was charged with five counts of murder for the opioid-related deaths of his patients and 11 counts of reckless endangerment in the first degree, according to the New York Times. Dr. Blatti’s medical license has been revoked, and he has pleaded not guilty.
Dr. Blatti had been seeing patients and giving prescriptions out of his car in parking lots, where he would prescribe pain medications without examining the patients. Many of these patients were struggling with addiction to opioids or other drugs. The alleged victims — three men and two women, who were between the ages of 30 and 60 — were prescribed 45,000 pills over 4 years, despite the fact that each showed clear signs of addiction, according to prosecutors.
Prosecutors allege that Dr. Blatti knew that several of his patients had died of overdoses, and he ignored pleas from their family members to stop enabling their addictions. They also say he ignored warnings from insurers about excessive opioid prescribing and was questioned by the New York State Office of Professional Medical Conduct about it in 2017.
A version of this article first appeared on Medscape.com.