User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Differences in brain structure linked to social disadvantage
Brain volume disparities among young children of different races may be attributable to adverse childhood experiences related to socioeconomic conditions and structural racism, new research suggests.
Investigators from the Belmont, Mass.–based McLean Hospital, an affiliate of Mass General Brigham, found that 9- and 10-year-old children of different racial and socioeconomic backgrounds have subtle neurobiological differences in gray matter volume in certain brain regions associated with trauma and stress.
Lead investigator Nathaniel Harnett, PhD, of the department of psychiatry at Harvard Medical School, Boston, believes this research shows evidence that “structural racism” – broad socioeconomic disadvantages that lead to poverty and emotional trauma – may affect brain structures and growth and ultimately may lead to psychiatric illness.
“For clinicians, I think the take-home message is that we really need to be more aware about the ways in which the disproportionate burden of stress might impact some groups,” Dr. Harnett told this news organization.
“This in turn can affect the way they respond either to later stress or maybe even treatment outcomes.” He added that other brain regions and compensatory mechanisms are likely to be involved, and more work needs to explore these connections.
The study was published online in the American Journal of Psychiatry.
‘Toxic stressor’
Dr. Harnett and colleagues used MRI and survey data from the 2019 Adolescent Brain Cognitive Development (ABCD) study involving over 12,000 children from 21 sites across the United States.
Participating children provided information about emotional and physical conflicts in the household. The ABCD study also surveyed the parents about their race and ethnicity, parental education, employment, and family income. Another factor in the analysis was neighborhood disadvantage, based on the Area Deprivation Index utilizing 17 socioeconomic indicators from the U.S. Census, including poverty and housing.
Comparing brain MRI findings from approximately 7,300 White children and 1,800 Black children in the ABCD study, Dr. Harnett’s group found that Black children had lower gray matter volume in the amygdala, hippocampus, and other subregions of the prefrontal cortex.
Experience of adversity was the “sole factor” explaining brain volume differences, with household income being the predominant factor.
Compared with White children, Black children were three times less likely to have parents who were currently employed. In addition, White parents were more likely than Black parents to have higher education at 75.2% versus 40.6%. Black families had significantly lower household income than White families and experienced more family conflict, material hardship, neighborhood disadvantage, and traumatic events.
The researchers analyzed race-related differences in posttraumatic stress disorder symptoms and the relationship with adversity and found that Black children had significantly greater PTSD symptom severity, and that symptom severity was “further predicted by adversity.”
“Taken together, early-life adversity may act as a toxic stressor that disproportionately impacts Black children as a result of their significantly greater exposure to adversity and contributes to differential neural development of key threat-processing regions,” the investigators write.
“These parts of the brain are involved in what we typically call threat learning,” Dr. Harnett explained. “Threat learning is basically learning to recognize potential dangers in our environment and selecting behaviors to keep us safe, whether we’re going to run away from a danger or face it head on. When you have chronic exposure to things that can be dangerous or can make you feel unsafe, that might have an impact on how these brain regions develop, with potential implications for how these regions function later on in life.”
A consequence of toxic stress
This study is part of a growing body of work on the influence of “toxic stress” and other forms of PTSD on brain architecture. The authors note that prolonged exposure to adverse experiences leads to excessive activation of stress-response systems and accumulation of stress hormones. This disrupts immune and metabolic regulatory systems that influence the developing structures of the brain.
The study helps to contradict the “pseudoscientific falsehood” of biologic race-related differences in brain volume, instead emphasizing the role of adversity brought on by structural racism, the authors add.
In an accompanying editor’s note, the publication’s Editor-in-Chief Ned H. Kalin, MD, called childhood adversity, maltreatment, and stress, “significant risk factors for the development of psychopathology.”
These findings are “critically important, as they speak to the need for psychiatry as a field to be outspoken about the detrimental psychological impacts of race-related disparities in childhood adversity, to call out the fact that these disparities stem from structural racism, and to vigorously support rectifying efforts by pursuing policy changes,” he stated in a news release.
Social construct?
Joan Luby, MD, coauthor of an accompanying editorial, said she and her coauthor “really appreciate the study and think the findings are overall very consistent with the emerging literature, increasing the confidence [in the findings].”
Dr. Luby, a professor of child psychiatry and director of the Early Emotional Development Program, Washington University, St. Louis, noted that she “takes issue” with the fact that the study “makes inferences regarding race, when we think those inferences aren’t well justified, are misinterpretations, and could be misleading.”
Race is a “social construct” and there are many sources of adversity that the authors didn’t measure in the study and are likely the source of any remaining variance they found, including experiences of structural racism and discrimination,” said Dr. Luby, who was not involved in the study.
“How people look doesn’t have any bearing on their inherent biological characteristics, and more [needs to be studied] on how they experience the psychosocial environment and how the psychosocial environment rejects or reacts to them.”
These psychosocial issues “have to be taken into account and measured in a very comprehensive way,” she added.
The ABCD study was supported by the National Institutes of Health and additional federal partners. Dr. Harnett reports no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Luby receives royalties from Guilford Press. Her coauthor reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Brain volume disparities among young children of different races may be attributable to adverse childhood experiences related to socioeconomic conditions and structural racism, new research suggests.
Investigators from the Belmont, Mass.–based McLean Hospital, an affiliate of Mass General Brigham, found that 9- and 10-year-old children of different racial and socioeconomic backgrounds have subtle neurobiological differences in gray matter volume in certain brain regions associated with trauma and stress.
Lead investigator Nathaniel Harnett, PhD, of the department of psychiatry at Harvard Medical School, Boston, believes this research shows evidence that “structural racism” – broad socioeconomic disadvantages that lead to poverty and emotional trauma – may affect brain structures and growth and ultimately may lead to psychiatric illness.
“For clinicians, I think the take-home message is that we really need to be more aware about the ways in which the disproportionate burden of stress might impact some groups,” Dr. Harnett told this news organization.
“This in turn can affect the way they respond either to later stress or maybe even treatment outcomes.” He added that other brain regions and compensatory mechanisms are likely to be involved, and more work needs to explore these connections.
The study was published online in the American Journal of Psychiatry.
‘Toxic stressor’
Dr. Harnett and colleagues used MRI and survey data from the 2019 Adolescent Brain Cognitive Development (ABCD) study involving over 12,000 children from 21 sites across the United States.
Participating children provided information about emotional and physical conflicts in the household. The ABCD study also surveyed the parents about their race and ethnicity, parental education, employment, and family income. Another factor in the analysis was neighborhood disadvantage, based on the Area Deprivation Index utilizing 17 socioeconomic indicators from the U.S. Census, including poverty and housing.
Comparing brain MRI findings from approximately 7,300 White children and 1,800 Black children in the ABCD study, Dr. Harnett’s group found that Black children had lower gray matter volume in the amygdala, hippocampus, and other subregions of the prefrontal cortex.
Experience of adversity was the “sole factor” explaining brain volume differences, with household income being the predominant factor.
Compared with White children, Black children were three times less likely to have parents who were currently employed. In addition, White parents were more likely than Black parents to have higher education at 75.2% versus 40.6%. Black families had significantly lower household income than White families and experienced more family conflict, material hardship, neighborhood disadvantage, and traumatic events.
The researchers analyzed race-related differences in posttraumatic stress disorder symptoms and the relationship with adversity and found that Black children had significantly greater PTSD symptom severity, and that symptom severity was “further predicted by adversity.”
“Taken together, early-life adversity may act as a toxic stressor that disproportionately impacts Black children as a result of their significantly greater exposure to adversity and contributes to differential neural development of key threat-processing regions,” the investigators write.
“These parts of the brain are involved in what we typically call threat learning,” Dr. Harnett explained. “Threat learning is basically learning to recognize potential dangers in our environment and selecting behaviors to keep us safe, whether we’re going to run away from a danger or face it head on. When you have chronic exposure to things that can be dangerous or can make you feel unsafe, that might have an impact on how these brain regions develop, with potential implications for how these regions function later on in life.”
A consequence of toxic stress
This study is part of a growing body of work on the influence of “toxic stress” and other forms of PTSD on brain architecture. The authors note that prolonged exposure to adverse experiences leads to excessive activation of stress-response systems and accumulation of stress hormones. This disrupts immune and metabolic regulatory systems that influence the developing structures of the brain.
The study helps to contradict the “pseudoscientific falsehood” of biologic race-related differences in brain volume, instead emphasizing the role of adversity brought on by structural racism, the authors add.
In an accompanying editor’s note, the publication’s Editor-in-Chief Ned H. Kalin, MD, called childhood adversity, maltreatment, and stress, “significant risk factors for the development of psychopathology.”
These findings are “critically important, as they speak to the need for psychiatry as a field to be outspoken about the detrimental psychological impacts of race-related disparities in childhood adversity, to call out the fact that these disparities stem from structural racism, and to vigorously support rectifying efforts by pursuing policy changes,” he stated in a news release.
Social construct?
Joan Luby, MD, coauthor of an accompanying editorial, said she and her coauthor “really appreciate the study and think the findings are overall very consistent with the emerging literature, increasing the confidence [in the findings].”
Dr. Luby, a professor of child psychiatry and director of the Early Emotional Development Program, Washington University, St. Louis, noted that she “takes issue” with the fact that the study “makes inferences regarding race, when we think those inferences aren’t well justified, are misinterpretations, and could be misleading.”
Race is a “social construct” and there are many sources of adversity that the authors didn’t measure in the study and are likely the source of any remaining variance they found, including experiences of structural racism and discrimination,” said Dr. Luby, who was not involved in the study.
“How people look doesn’t have any bearing on their inherent biological characteristics, and more [needs to be studied] on how they experience the psychosocial environment and how the psychosocial environment rejects or reacts to them.”
These psychosocial issues “have to be taken into account and measured in a very comprehensive way,” she added.
The ABCD study was supported by the National Institutes of Health and additional federal partners. Dr. Harnett reports no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Luby receives royalties from Guilford Press. Her coauthor reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Brain volume disparities among young children of different races may be attributable to adverse childhood experiences related to socioeconomic conditions and structural racism, new research suggests.
Investigators from the Belmont, Mass.–based McLean Hospital, an affiliate of Mass General Brigham, found that 9- and 10-year-old children of different racial and socioeconomic backgrounds have subtle neurobiological differences in gray matter volume in certain brain regions associated with trauma and stress.
Lead investigator Nathaniel Harnett, PhD, of the department of psychiatry at Harvard Medical School, Boston, believes this research shows evidence that “structural racism” – broad socioeconomic disadvantages that lead to poverty and emotional trauma – may affect brain structures and growth and ultimately may lead to psychiatric illness.
“For clinicians, I think the take-home message is that we really need to be more aware about the ways in which the disproportionate burden of stress might impact some groups,” Dr. Harnett told this news organization.
“This in turn can affect the way they respond either to later stress or maybe even treatment outcomes.” He added that other brain regions and compensatory mechanisms are likely to be involved, and more work needs to explore these connections.
The study was published online in the American Journal of Psychiatry.
‘Toxic stressor’
Dr. Harnett and colleagues used MRI and survey data from the 2019 Adolescent Brain Cognitive Development (ABCD) study involving over 12,000 children from 21 sites across the United States.
Participating children provided information about emotional and physical conflicts in the household. The ABCD study also surveyed the parents about their race and ethnicity, parental education, employment, and family income. Another factor in the analysis was neighborhood disadvantage, based on the Area Deprivation Index utilizing 17 socioeconomic indicators from the U.S. Census, including poverty and housing.
Comparing brain MRI findings from approximately 7,300 White children and 1,800 Black children in the ABCD study, Dr. Harnett’s group found that Black children had lower gray matter volume in the amygdala, hippocampus, and other subregions of the prefrontal cortex.
Experience of adversity was the “sole factor” explaining brain volume differences, with household income being the predominant factor.
Compared with White children, Black children were three times less likely to have parents who were currently employed. In addition, White parents were more likely than Black parents to have higher education at 75.2% versus 40.6%. Black families had significantly lower household income than White families and experienced more family conflict, material hardship, neighborhood disadvantage, and traumatic events.
The researchers analyzed race-related differences in posttraumatic stress disorder symptoms and the relationship with adversity and found that Black children had significantly greater PTSD symptom severity, and that symptom severity was “further predicted by adversity.”
“Taken together, early-life adversity may act as a toxic stressor that disproportionately impacts Black children as a result of their significantly greater exposure to adversity and contributes to differential neural development of key threat-processing regions,” the investigators write.
“These parts of the brain are involved in what we typically call threat learning,” Dr. Harnett explained. “Threat learning is basically learning to recognize potential dangers in our environment and selecting behaviors to keep us safe, whether we’re going to run away from a danger or face it head on. When you have chronic exposure to things that can be dangerous or can make you feel unsafe, that might have an impact on how these brain regions develop, with potential implications for how these regions function later on in life.”
A consequence of toxic stress
This study is part of a growing body of work on the influence of “toxic stress” and other forms of PTSD on brain architecture. The authors note that prolonged exposure to adverse experiences leads to excessive activation of stress-response systems and accumulation of stress hormones. This disrupts immune and metabolic regulatory systems that influence the developing structures of the brain.
The study helps to contradict the “pseudoscientific falsehood” of biologic race-related differences in brain volume, instead emphasizing the role of adversity brought on by structural racism, the authors add.
In an accompanying editor’s note, the publication’s Editor-in-Chief Ned H. Kalin, MD, called childhood adversity, maltreatment, and stress, “significant risk factors for the development of psychopathology.”
These findings are “critically important, as they speak to the need for psychiatry as a field to be outspoken about the detrimental psychological impacts of race-related disparities in childhood adversity, to call out the fact that these disparities stem from structural racism, and to vigorously support rectifying efforts by pursuing policy changes,” he stated in a news release.
Social construct?
Joan Luby, MD, coauthor of an accompanying editorial, said she and her coauthor “really appreciate the study and think the findings are overall very consistent with the emerging literature, increasing the confidence [in the findings].”
Dr. Luby, a professor of child psychiatry and director of the Early Emotional Development Program, Washington University, St. Louis, noted that she “takes issue” with the fact that the study “makes inferences regarding race, when we think those inferences aren’t well justified, are misinterpretations, and could be misleading.”
Race is a “social construct” and there are many sources of adversity that the authors didn’t measure in the study and are likely the source of any remaining variance they found, including experiences of structural racism and discrimination,” said Dr. Luby, who was not involved in the study.
“How people look doesn’t have any bearing on their inherent biological characteristics, and more [needs to be studied] on how they experience the psychosocial environment and how the psychosocial environment rejects or reacts to them.”
These psychosocial issues “have to be taken into account and measured in a very comprehensive way,” she added.
The ABCD study was supported by the National Institutes of Health and additional federal partners. Dr. Harnett reports no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Luby receives royalties from Guilford Press. Her coauthor reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Bright light therapy boosts therapeutic response

Both depression and bipolar disorder are leading causes of disability worldwide, and data show that only 50%-60% of these patients respond to first-line antidepressants, wrote Alessandro Cuomo, MD, of the University of Siena Medical Center, Italy, and colleagues.
Bright light therapy (BLT) was originally introduced as a treatment for seasonal affective disorder, but its use has been expanded to treat nonseasonal depression and bipolar disorder, they said. However, the impact of BLT on depressive symptoms in bipolar depression in particular has not been examined, they noted.
In a study published in the Journal of Affective Disorders, the researchers identified 18 men and 23 women aged 18 years and older with bipolar depression based on DSM-5 criteria who had already been treated with antidepressants. The participants were randomized to antidepressants combined with BLT or antidepressants combined with red light exposure (controls). The participants were positioned at 30-80 cm from the 10,000-lux light source for 30 minutes daily. The mean age of the participants was 49.1 years.
The primary outcome was scores on the Montgomery-Åsberg Depression Scale (MADRS), Hamilton Depression Rating Scale (HAMD-17), and CGI-Severity of illness (CGI-S), Fatigue Severity Scale (FSS), and Quality of Life Scale (QOLS) after the 8 weeks of treatment.
After 4 weeks, MADRS scores and HAMD-17 scores were significantly lower in the treatment group, compared with the controls (20 and 18 vs. 27.5 and 24.9, respectively; P < .001). Quality of life scores increased in the treatment group, compared with controls, with median scores of 39 vs. 29.50, respectively.
After 8 weeks, the treatment group continued to show significant improvement, compared with the control group, with scores on the MADRS, HAMD-17, CGI-S, and QOLS of 14.0, 9.0, 1.0, and 62.0 vs. 16.0, 15.5, 2.0, and 40.0, respectively. No side effects were reported.
“From our findings, BLT [proved] particularly effective in bipolar patients without triggering any manic switch, as evidenced instead in some similar studies,” the researchers wrote in their discussion.
Although the mechanism of action for BLT remains unclear, the current study findings confirm the existing knowledge of BLT, they noted. The positive effect of BLT on quality of life “might be attributable to the ability of BLT to reduce the latency times of antidepressants and increase the production of serotonin and melatonin,” as shown in previous work, they said.
The study findings were limited by several factors including the small sample size, which prevents definitive conclusions about the effectiveness of BLT in combination with different antidepressants, and the heterogeneity of the antidepressant treatments, the researchers noted. Larger, prospective studies and randomized, controlled trials are needed, as are studies of special populations such as older adults or those with degenerative diseases, they said.
However, the results suggest BLT has value as a safe and effective treatment and a way to boost therapeutic response and reduce the impact of long-lasting therapies, they concluded.
The study received no outside funding. Dr. Cuomo disclosed serving as a consultant and/or a speaker for Angelini, Glaxo Smith Kline, Lundbeck, Janssen, Otsuka, Pfizer, and Recordati.
Both depression and bipolar disorder are leading causes of disability worldwide, and data show that only 50%-60% of these patients respond to first-line antidepressants, wrote Alessandro Cuomo, MD, of the University of Siena Medical Center, Italy, and colleagues.
Bright light therapy (BLT) was originally introduced as a treatment for seasonal affective disorder, but its use has been expanded to treat nonseasonal depression and bipolar disorder, they said. However, the impact of BLT on depressive symptoms in bipolar depression in particular has not been examined, they noted.
In a study published in the Journal of Affective Disorders, the researchers identified 18 men and 23 women aged 18 years and older with bipolar depression based on DSM-5 criteria who had already been treated with antidepressants. The participants were randomized to antidepressants combined with BLT or antidepressants combined with red light exposure (controls). The participants were positioned at 30-80 cm from the 10,000-lux light source for 30 minutes daily. The mean age of the participants was 49.1 years.
The primary outcome was scores on the Montgomery-Åsberg Depression Scale (MADRS), Hamilton Depression Rating Scale (HAMD-17), and CGI-Severity of illness (CGI-S), Fatigue Severity Scale (FSS), and Quality of Life Scale (QOLS) after the 8 weeks of treatment.
After 4 weeks, MADRS scores and HAMD-17 scores were significantly lower in the treatment group, compared with the controls (20 and 18 vs. 27.5 and 24.9, respectively; P < .001). Quality of life scores increased in the treatment group, compared with controls, with median scores of 39 vs. 29.50, respectively.
After 8 weeks, the treatment group continued to show significant improvement, compared with the control group, with scores on the MADRS, HAMD-17, CGI-S, and QOLS of 14.0, 9.0, 1.0, and 62.0 vs. 16.0, 15.5, 2.0, and 40.0, respectively. No side effects were reported.
“From our findings, BLT [proved] particularly effective in bipolar patients without triggering any manic switch, as evidenced instead in some similar studies,” the researchers wrote in their discussion.
Although the mechanism of action for BLT remains unclear, the current study findings confirm the existing knowledge of BLT, they noted. The positive effect of BLT on quality of life “might be attributable to the ability of BLT to reduce the latency times of antidepressants and increase the production of serotonin and melatonin,” as shown in previous work, they said.
The study findings were limited by several factors including the small sample size, which prevents definitive conclusions about the effectiveness of BLT in combination with different antidepressants, and the heterogeneity of the antidepressant treatments, the researchers noted. Larger, prospective studies and randomized, controlled trials are needed, as are studies of special populations such as older adults or those with degenerative diseases, they said.
However, the results suggest BLT has value as a safe and effective treatment and a way to boost therapeutic response and reduce the impact of long-lasting therapies, they concluded.
The study received no outside funding. Dr. Cuomo disclosed serving as a consultant and/or a speaker for Angelini, Glaxo Smith Kline, Lundbeck, Janssen, Otsuka, Pfizer, and Recordati.
Both depression and bipolar disorder are leading causes of disability worldwide, and data show that only 50%-60% of these patients respond to first-line antidepressants, wrote Alessandro Cuomo, MD, of the University of Siena Medical Center, Italy, and colleagues.
Bright light therapy (BLT) was originally introduced as a treatment for seasonal affective disorder, but its use has been expanded to treat nonseasonal depression and bipolar disorder, they said. However, the impact of BLT on depressive symptoms in bipolar depression in particular has not been examined, they noted.
In a study published in the Journal of Affective Disorders, the researchers identified 18 men and 23 women aged 18 years and older with bipolar depression based on DSM-5 criteria who had already been treated with antidepressants. The participants were randomized to antidepressants combined with BLT or antidepressants combined with red light exposure (controls). The participants were positioned at 30-80 cm from the 10,000-lux light source for 30 minutes daily. The mean age of the participants was 49.1 years.
The primary outcome was scores on the Montgomery-Åsberg Depression Scale (MADRS), Hamilton Depression Rating Scale (HAMD-17), and CGI-Severity of illness (CGI-S), Fatigue Severity Scale (FSS), and Quality of Life Scale (QOLS) after the 8 weeks of treatment.
After 4 weeks, MADRS scores and HAMD-17 scores were significantly lower in the treatment group, compared with the controls (20 and 18 vs. 27.5 and 24.9, respectively; P < .001). Quality of life scores increased in the treatment group, compared with controls, with median scores of 39 vs. 29.50, respectively.
After 8 weeks, the treatment group continued to show significant improvement, compared with the control group, with scores on the MADRS, HAMD-17, CGI-S, and QOLS of 14.0, 9.0, 1.0, and 62.0 vs. 16.0, 15.5, 2.0, and 40.0, respectively. No side effects were reported.
“From our findings, BLT [proved] particularly effective in bipolar patients without triggering any manic switch, as evidenced instead in some similar studies,” the researchers wrote in their discussion.
Although the mechanism of action for BLT remains unclear, the current study findings confirm the existing knowledge of BLT, they noted. The positive effect of BLT on quality of life “might be attributable to the ability of BLT to reduce the latency times of antidepressants and increase the production of serotonin and melatonin,” as shown in previous work, they said.
The study findings were limited by several factors including the small sample size, which prevents definitive conclusions about the effectiveness of BLT in combination with different antidepressants, and the heterogeneity of the antidepressant treatments, the researchers noted. Larger, prospective studies and randomized, controlled trials are needed, as are studies of special populations such as older adults or those with degenerative diseases, they said.
However, the results suggest BLT has value as a safe and effective treatment and a way to boost therapeutic response and reduce the impact of long-lasting therapies, they concluded.
The study received no outside funding. Dr. Cuomo disclosed serving as a consultant and/or a speaker for Angelini, Glaxo Smith Kline, Lundbeck, Janssen, Otsuka, Pfizer, and Recordati.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
How a concussion led a former football player/WWE star to a pioneering neuroscience career
On Oct. 5, 2022, at 10:24 a.m., Chris Nowinski, PhD, cofounder of the Boston-based Concussion Legacy Foundation (CLF), was in his home office when the email came through.
“I pounded my desk, shouted YES! and went to find my wife so I could pick her up and give her a big hug,” he recalled. “It was the culmination of 15 years of research and hard work.”
Robert Cantu, MD, who has been studying head trauma for 50+ years and has published more than 500 papers about it, compares the announcement to the 1964 Surgeon General’s report that linked cigarette smoking with lung cancer and heart disease. With the NIH and the Centers of Disease Control and Prevention (CDC) now in agreement about the risks of participating in impact sports and activities, he said, “We’ve reached a tipping point that should finally prompt deniers such as the NHL, NCAA, FIFA, World Rugby, the International Olympic Committee, and other [sports organizations] to remove all unnecessary head trauma from their sports.”
“A lot of the credit for this must go to Chris,” added Dr. Cantu, medical director and director of clinical research at the Cantu Concussion Center at Emerson Hospital in Concord, Mass. “Clinicians like myself can reach only so many people by writing papers and giving speeches at medical conferences. For this to happen, the message needed to get out to parents, athletes, and society in general. And Chris was the vehicle for doing that.”
Dr. Nowinski didn’t set out to be the messenger. He played football at Harvard in the late 1990s, making second-team All-Ivy as a defensive tackle his senior year. In 2000, he enrolled in Killer Kowalski’s Wrestling Institute and eventually joined Vince McMahon’s World Wrestling Entertainment (WWE).
There he played the role of 295-pound villain “Chris Harvard,” an intellectual snob who dressed in crimson tights and insulted the crowd’s IQ. “Roses are red. Violets are blue. The reason I’m talking so slowly is because no one in [insert name of town he was appearing in] has passed grade 2!”
“I’d often apply my education during a match,” he wrote in his book, “Head Games: Football’s Concussion Crisis.“ In a match in Bridgeport, Conn., I assaulted [my opponent] with a human skeleton, ripped off the skull, got down on bended knee, and began reciting Hamlet. Those were good times.”
Those good times ended abruptly, however, during a match with Bubba Ray Dudley at the Hartford Civic Center in Connecticut in 2003. Even though pro wrestling matches are rehearsed, and the blows aren’t real, accidents happen. Mr. Dudley mistakenly kicked Dr. Nowinski in the jaw with enough force to put him on his back and make the whole ring shake.
“Holy shit, kid! You okay?” asked the referee. Before a foggy Dr. Nowinski could reply, 300-pound Mr. Dudley crashed down on him, hooked his leg, and the ref began counting, “One! Two! …” Dr. Nowinski instinctively kicked out but had forgotten the rest of the script. He managed to finish the match and stagger backstage.
His coherence and awareness gradually returned, but a “throbbing headache” persisted. A locker room doctor said he might have a concussion and recommended he wait to see how he felt before wrestling in Albany, N.Y., the next evening.
The following day the headache had subsided, but he still felt “a little strange.” Nonetheless, he told the doctor he was fine and strutted out to again battle Bubba Ray, this time in a match where he eventually got thrown through a ringside table and suffered the Dudley Death Drop. Afterward, “I crawled backstage and laid down. The headache was much, much worse.”
An event and a process
Dr. Nowinski continued to insist he was “fine” and wrestled a few more matches in the following days before finally acknowledging something was wrong. He’d had his bell rung numerous times in football, but this was different. Even more worrisome, none of the doctors he consulted could give him any definitive answers. He finally found his way to Emerson Hospital, where Dr. Cantu was the chief of neurosurgery.
“I remember that day vividly,” said Dr. Cantu. “Chris was this big, strapping, handsome guy – a hell of an athlete whose star was rising. He didn’t realize that he’d suffered a series of concussions and that trying to push through them was the worst thing he could be doing.”
Concussions and their effects were misunderstood by many athletes, coaches, and even physicians back then. It was assumed that the quarter inch of bone surrounding the adult brain provided adequate protection from common sports impacts and that any aftereffects were temporary. A common treatment was smelling salts and a pat on the back as the athlete returned to action.
However, the brain floats inside the skull in a bath of cerebral fluid. Any significant impact causes it to slosh violently from side to side, damaging tissue, synapses, and cells resulting in inflammation that can manifest as confusion and brain fog.
“A concussion is actually not defined by a physical injury,” explained Dr. Nowinski, “but by a loss of brain function that is induced by trauma. Concussion is not just an event, but also a process.” It’s almost as if the person has suffered a small seizure.
Fortunately, most concussion symptoms resolve within 2 weeks, but in some cases, especially if there’s been additional head trauma, they can persist, causing anxiety, depression, anger, and/or sleep disorders. Known as postconcussion syndrome (PCS), this is what Dr. Nowinski was unknowingly suffering from when he consulted Dr. Cantu.
In fact, one night it an Indianapolis hotel, weeks after his initial concussion, he awoke to find himself on the floor and the room in shambles. His girlfriend was yelling his name and shaking him. She told him he’d been having a nightmare and had suddenly started screaming and tearing up the room. “I didn’t remember any of it,” he said.
Dr. Cantu eventually advised Dr. Nowinski against ever returning to the ring or any activity with the risk for head injury. Research shows that sustaining a single significant concussion increases the risk of subsequent more-severe brain injuries.
“My diagnosis could have sent Chris off the deep end because he could no longer do what he wanted to do with this life,” said Dr. Cantu. “But instead, he used it as a tool to find meaning for his life.”
Dr. Nowinski decided to use his experience as a teaching opportunity, not just for other athletes but also for sports organizations and the medical community.
His book, which focused on the NFL’s “tobacco-industry-like refusal to acknowledge the depths of the problem,” was published in 2006. A year later, Dr. Nowinski partnered with Dr. Cantu to found the Sports Legacy Institute, which eventually became the Concussion Legacy Foundation (CLF).
Cold calling for brain donations
Robert Stern, PhD, is another highly respected authority in the study of neurodegenerative disease. In 2007, he was directing the clinical core of Boston University’s Alzheimer’s Disease Center. After giving a lecture to a group of financial planners and elder-law attorneys one morning, he got a request for a private meeting from a fellow named Chris Nowinski.
“I’d never heard of him, but I agreed,” recalled Dr. Stern, a professor of neurology, neurosurgery, anatomy, and neurobiology at Boston University. “A few days later, this larger-than-life guy walked into our conference room at the BU School of Medicine, exuding a great deal of passion, intellect, and determination. He told me his story and then started talking about the long-term consequences of concussions in sports.”
Dr. Stern had seen patients with dementia pugilistica, the old-school term for CTE. These were mostly boxers with cognitive and behavioral impairment. “But I had not heard about football players,” he said. “I hadn’t put the two together. And as I was listening to Chris, I realized if what he was saying was true then it was not only a potentially huge public health issue, but it was also a potentially huge scientific issue in the field of neurodegenerative disease.”
Dr. Nowinski introduced Dr. Stern to Dr. Cantu, and together with Ann McKee, MD, professor of neurology and pathology at BU, they cofounded the Center for the Study of Traumatic Encephalopathy (CSTE) in 2008. It was the first center of its kind devoted to the study of CTE in the world.
One of Dr. Nowinski’s first jobs at the CSTE was soliciting and procuring brain donations. Since CTE is generally a progressive condition that can take decades to manifest, autopsy was the only way to detect it.
The brains of two former Pittsburgh Steelers, Mike Webster and Terry Long, had been examined after their untimely deaths. After immunostaining, investigators found both former NFL players had “protein misfolds” characteristic of CTE.
This finding drew a lot of public and scientific attention, given that Mr. Long died by suicide and Mr. Webster was homeless when he died of a heart attack. But more scientific evidence was needed to prove a causal link between the head trauma and CTE.
Dr. Nowinski scoured obituaries looking for potential brains to study. When he found one, he would cold call the family and try to convince them to donate it to science. The first brain he secured for the center belonged to John Grimsley, a former NFL linebacker who in 2008 died at age 45 of an accidental gunshot wound. Often, Dr. Nowinski would even be the courier, traveling to pick up the brain after it had been harvested.
Over the next 10 years, Dr. Nowinski and his research team secured 500 brain donations. The research that resulted was staggering. In the beginning only 45 cases of CTE had been identified in the world, but in the first 111 NFL players who were autopsied, 110 had the disorder.
Of the first 53 college football players autopsied, 48 had CTE. Although Dr. Nowinski’s initial focus was football, evidence of CTE was soon detected among athletes in boxing, hockey, soccer, and rugby, as well as in combat veterans. However, the National Football League and other governing sports bodies initially denied any connection between sport-related head trauma and CTE.
Cumulative damage
In 2017, after 7 years of study, Dr. Nowinski earned a PhD in neurology. As the scientific evidence continued to accumulate, two shifts occurred that Dr. Stern said represent Dr. Nowinski’s greatest contributions. First, concussion is now widely recognized as an acute brain injury with symptoms that need to be immediately diagnosed and addressed.
“This is a completely different story from where things were just 10 years ago,” said Dr. Stern, “and Chris played a central role, if not the central role, in raising awareness about that.”
All 50 states and the District of Columbia now have laws regarding sports-related concussion. And there are brain banks in Australia, Canada, New Zealand, Brazil, and the United Kingdom studying CTE. More than 2,500 athletes in a variety of sports, including NASCAR’s Dale Earnhardt Jr. and NFL hall of famer Nick Buoniconti, have publicly pledged to donate their brains to science after their deaths.
Second, said Dr. Stern, we now know that although concussions can contribute to CTE, they are not the sole cause. It’s repetitive subconcussive trauma, without symptoms of concussion, that do the most damage.
“These happen during every practice and in every game,” said Dr. Stern. In fact, it’s estimated that pro football players suffer thousands of subconcussive incidents over the course of their careers. So, a player doesn’t have to see stars or lose consciousness to suffer brain damage; small impacts can accumulate over time.
Understanding this point is crucial for making youth sports safer. “Chris has played a critical role in raising awareness here, too,” said Dr. Stern. “Allowing our kids to get hit in the head over and over can put them at greater risk for later problems, plus it just doesn’t make common sense.”
“The biggest misconception surrounding head trauma in sports,” said Dr. Nowinski, “is the belief among players, coaches, and even the medical and scientific communities that if you get hit in the head and don’t have any symptoms then you’re okay and there hasn’t been any damage. That couldn’t be further from the truth. We now know that people are suffering serious brain injuries due to the accumulated effect of subconcussive impacts, and we need to get the word out about that.”
A major initiative from the Concussion Legacy Foundation called “Stop Hitting Kids in the Head” has the goal of convincing every sport to eliminate repetitive head impacts in players under age 14 – the time when the skull and brain are still developing and most vulnerable – by 2026. In fact, Dr. Nowinski wrote that “there could be a lot of kids who are misdiagnosed and medicated for various behavioral or emotional problems that may actually be head injury–related.”
Starting in 2009, the NFL adopted a series of rule changes designed to better protect its players against repeated head trauma. Among them is a ban on spearing or leading with the helmet, penalties for hitting defenseless players, and more stringent return-to-play guidelines, including concussion protocols.
The NFL has also put more emphasis on flag football options for youngsters and, for the first time, showcased this alternative in the 2023 Pro Bowl. But Dr. Nowinski is pressuring the league to go further. “While acknowledging that the game causes CTE, the NFL still underwrites recruiting 5-year-olds to play tackle football,” he said. “In my opinion, that’s unethical, and it needs to be addressed.”
WWE one of the most responsive organizations
Dr. Nowinski said WWE has been one of the most responsive sports organizations for protecting athletes. A doctor is now ringside at every match as is an observer who knows the script, thereby allowing for instant medical intervention if something goes wrong. “Since everyone is trying to look like they have a concussion all the time, it takes a deep understanding of the business to recognize a real one,” he said.
But this hasn’t been the case with other sports. “I am eternally disappointed in the response of the professional sports industry to the knowledge of CTE and long-term concussion symptoms,” said Dr. Nowinski.
“For example, FIFA [international soccer’s governing body] still doesn’t allow doctors to evaluate [potentially concussed] players on the sidelines and put them back in the game with a free substitution [if they’re deemed okay]. Not giving players proper medical care for a brain injury is unethical,” he said. BU’s Center for the Study of Traumatic Encephalopathy diagnosed the first CTE case in soccer in 2012, and in 2015 Dr. Nowinski successfully lobbied U.S. Soccer to ban heading the ball before age 11.
“Unfortunately, many governing bodies have circled the wagons in denying their sport causes CTE,” he continued. “FIFA, World Rugby, the NHL, even the NCAA and International Olympic Committee refuse to acknowledge it and, therefore, aren’t taking any steps to prevent it. They see it as a threat to their business model. Hopefully, now that the NIH and CDC are aligned about the risks of head impact in sports, this will begin to change.”
Meanwhile, research is continuing. Scientists are getting closer to being able to diagnose CTE in living humans, with ongoing studies using PET scans, blood markers, and spinal fluid markers. In 2019, researchers identified tau proteins specific to CTE that they believe are distinct from those of Alzheimer’s and other neurodegenerative diseases. Next step would be developing a drug to slow the development of CTE once detected.
Nonetheless, athletes at all levels in impact sports still don’t fully appreciate the risks of repeated head trauma and especially subconcussive blows. “I talk to former NFL and college players every week,” said Dr. Stern. “Some tell me, ‘I love the sport, it gave me so much, and I would do it again, but I’m not letting my grandchildren play.’ But others say, ‘As long as they know the risks, they can make their own decision.’ “
Dr. Nowinski has a daughter who is 4 and a son who’s 2. Both play soccer but, thanks to dad, heading isn’t allowed in their age groups. If they continue playing sports, Dr. Nowinski said he’ll make sure they understand the risks and how to protect themselves. This is a conversation all parents should have with their kids at every level to make sure they play safe, he added.
Those in the medical community can also volunteer their time to explain head trauma to athletes, coaches, and school administrators to be sure they understand its seriousness and are doing everything to protect players.
As you watch this year’s Super Bowl, Dr. Nowinski and his team would like you to keep something in mind. Those young men on the field for your entertainment are receiving mild brain trauma repeatedly throughout the game.
Even if it’s not a huge hit that gets replayed and makes everyone gasp, even if no one gets ushered into the little sideline tent for a concussion screening, even if no one loses consciousness, brain damage is still occurring. Watch the heads of the players during every play and think about what’s going on inside their skulls regardless of how big and strong those helmets look.
A version of this article first appeared on Medscape.com.
On Oct. 5, 2022, at 10:24 a.m., Chris Nowinski, PhD, cofounder of the Boston-based Concussion Legacy Foundation (CLF), was in his home office when the email came through.
“I pounded my desk, shouted YES! and went to find my wife so I could pick her up and give her a big hug,” he recalled. “It was the culmination of 15 years of research and hard work.”
Robert Cantu, MD, who has been studying head trauma for 50+ years and has published more than 500 papers about it, compares the announcement to the 1964 Surgeon General’s report that linked cigarette smoking with lung cancer and heart disease. With the NIH and the Centers of Disease Control and Prevention (CDC) now in agreement about the risks of participating in impact sports and activities, he said, “We’ve reached a tipping point that should finally prompt deniers such as the NHL, NCAA, FIFA, World Rugby, the International Olympic Committee, and other [sports organizations] to remove all unnecessary head trauma from their sports.”
“A lot of the credit for this must go to Chris,” added Dr. Cantu, medical director and director of clinical research at the Cantu Concussion Center at Emerson Hospital in Concord, Mass. “Clinicians like myself can reach only so many people by writing papers and giving speeches at medical conferences. For this to happen, the message needed to get out to parents, athletes, and society in general. And Chris was the vehicle for doing that.”
Dr. Nowinski didn’t set out to be the messenger. He played football at Harvard in the late 1990s, making second-team All-Ivy as a defensive tackle his senior year. In 2000, he enrolled in Killer Kowalski’s Wrestling Institute and eventually joined Vince McMahon’s World Wrestling Entertainment (WWE).
There he played the role of 295-pound villain “Chris Harvard,” an intellectual snob who dressed in crimson tights and insulted the crowd’s IQ. “Roses are red. Violets are blue. The reason I’m talking so slowly is because no one in [insert name of town he was appearing in] has passed grade 2!”
“I’d often apply my education during a match,” he wrote in his book, “Head Games: Football’s Concussion Crisis.“ In a match in Bridgeport, Conn., I assaulted [my opponent] with a human skeleton, ripped off the skull, got down on bended knee, and began reciting Hamlet. Those were good times.”
Those good times ended abruptly, however, during a match with Bubba Ray Dudley at the Hartford Civic Center in Connecticut in 2003. Even though pro wrestling matches are rehearsed, and the blows aren’t real, accidents happen. Mr. Dudley mistakenly kicked Dr. Nowinski in the jaw with enough force to put him on his back and make the whole ring shake.
“Holy shit, kid! You okay?” asked the referee. Before a foggy Dr. Nowinski could reply, 300-pound Mr. Dudley crashed down on him, hooked his leg, and the ref began counting, “One! Two! …” Dr. Nowinski instinctively kicked out but had forgotten the rest of the script. He managed to finish the match and stagger backstage.
His coherence and awareness gradually returned, but a “throbbing headache” persisted. A locker room doctor said he might have a concussion and recommended he wait to see how he felt before wrestling in Albany, N.Y., the next evening.
The following day the headache had subsided, but he still felt “a little strange.” Nonetheless, he told the doctor he was fine and strutted out to again battle Bubba Ray, this time in a match where he eventually got thrown through a ringside table and suffered the Dudley Death Drop. Afterward, “I crawled backstage and laid down. The headache was much, much worse.”
An event and a process
Dr. Nowinski continued to insist he was “fine” and wrestled a few more matches in the following days before finally acknowledging something was wrong. He’d had his bell rung numerous times in football, but this was different. Even more worrisome, none of the doctors he consulted could give him any definitive answers. He finally found his way to Emerson Hospital, where Dr. Cantu was the chief of neurosurgery.
“I remember that day vividly,” said Dr. Cantu. “Chris was this big, strapping, handsome guy – a hell of an athlete whose star was rising. He didn’t realize that he’d suffered a series of concussions and that trying to push through them was the worst thing he could be doing.”
Concussions and their effects were misunderstood by many athletes, coaches, and even physicians back then. It was assumed that the quarter inch of bone surrounding the adult brain provided adequate protection from common sports impacts and that any aftereffects were temporary. A common treatment was smelling salts and a pat on the back as the athlete returned to action.
However, the brain floats inside the skull in a bath of cerebral fluid. Any significant impact causes it to slosh violently from side to side, damaging tissue, synapses, and cells resulting in inflammation that can manifest as confusion and brain fog.
“A concussion is actually not defined by a physical injury,” explained Dr. Nowinski, “but by a loss of brain function that is induced by trauma. Concussion is not just an event, but also a process.” It’s almost as if the person has suffered a small seizure.
Fortunately, most concussion symptoms resolve within 2 weeks, but in some cases, especially if there’s been additional head trauma, they can persist, causing anxiety, depression, anger, and/or sleep disorders. Known as postconcussion syndrome (PCS), this is what Dr. Nowinski was unknowingly suffering from when he consulted Dr. Cantu.
In fact, one night it an Indianapolis hotel, weeks after his initial concussion, he awoke to find himself on the floor and the room in shambles. His girlfriend was yelling his name and shaking him. She told him he’d been having a nightmare and had suddenly started screaming and tearing up the room. “I didn’t remember any of it,” he said.
Dr. Cantu eventually advised Dr. Nowinski against ever returning to the ring or any activity with the risk for head injury. Research shows that sustaining a single significant concussion increases the risk of subsequent more-severe brain injuries.
“My diagnosis could have sent Chris off the deep end because he could no longer do what he wanted to do with this life,” said Dr. Cantu. “But instead, he used it as a tool to find meaning for his life.”
Dr. Nowinski decided to use his experience as a teaching opportunity, not just for other athletes but also for sports organizations and the medical community.
His book, which focused on the NFL’s “tobacco-industry-like refusal to acknowledge the depths of the problem,” was published in 2006. A year later, Dr. Nowinski partnered with Dr. Cantu to found the Sports Legacy Institute, which eventually became the Concussion Legacy Foundation (CLF).
Cold calling for brain donations
Robert Stern, PhD, is another highly respected authority in the study of neurodegenerative disease. In 2007, he was directing the clinical core of Boston University’s Alzheimer’s Disease Center. After giving a lecture to a group of financial planners and elder-law attorneys one morning, he got a request for a private meeting from a fellow named Chris Nowinski.
“I’d never heard of him, but I agreed,” recalled Dr. Stern, a professor of neurology, neurosurgery, anatomy, and neurobiology at Boston University. “A few days later, this larger-than-life guy walked into our conference room at the BU School of Medicine, exuding a great deal of passion, intellect, and determination. He told me his story and then started talking about the long-term consequences of concussions in sports.”
Dr. Stern had seen patients with dementia pugilistica, the old-school term for CTE. These were mostly boxers with cognitive and behavioral impairment. “But I had not heard about football players,” he said. “I hadn’t put the two together. And as I was listening to Chris, I realized if what he was saying was true then it was not only a potentially huge public health issue, but it was also a potentially huge scientific issue in the field of neurodegenerative disease.”
Dr. Nowinski introduced Dr. Stern to Dr. Cantu, and together with Ann McKee, MD, professor of neurology and pathology at BU, they cofounded the Center for the Study of Traumatic Encephalopathy (CSTE) in 2008. It was the first center of its kind devoted to the study of CTE in the world.
One of Dr. Nowinski’s first jobs at the CSTE was soliciting and procuring brain donations. Since CTE is generally a progressive condition that can take decades to manifest, autopsy was the only way to detect it.
The brains of two former Pittsburgh Steelers, Mike Webster and Terry Long, had been examined after their untimely deaths. After immunostaining, investigators found both former NFL players had “protein misfolds” characteristic of CTE.
This finding drew a lot of public and scientific attention, given that Mr. Long died by suicide and Mr. Webster was homeless when he died of a heart attack. But more scientific evidence was needed to prove a causal link between the head trauma and CTE.
Dr. Nowinski scoured obituaries looking for potential brains to study. When he found one, he would cold call the family and try to convince them to donate it to science. The first brain he secured for the center belonged to John Grimsley, a former NFL linebacker who in 2008 died at age 45 of an accidental gunshot wound. Often, Dr. Nowinski would even be the courier, traveling to pick up the brain after it had been harvested.
Over the next 10 years, Dr. Nowinski and his research team secured 500 brain donations. The research that resulted was staggering. In the beginning only 45 cases of CTE had been identified in the world, but in the first 111 NFL players who were autopsied, 110 had the disorder.
Of the first 53 college football players autopsied, 48 had CTE. Although Dr. Nowinski’s initial focus was football, evidence of CTE was soon detected among athletes in boxing, hockey, soccer, and rugby, as well as in combat veterans. However, the National Football League and other governing sports bodies initially denied any connection between sport-related head trauma and CTE.
Cumulative damage
In 2017, after 7 years of study, Dr. Nowinski earned a PhD in neurology. As the scientific evidence continued to accumulate, two shifts occurred that Dr. Stern said represent Dr. Nowinski’s greatest contributions. First, concussion is now widely recognized as an acute brain injury with symptoms that need to be immediately diagnosed and addressed.
“This is a completely different story from where things were just 10 years ago,” said Dr. Stern, “and Chris played a central role, if not the central role, in raising awareness about that.”
All 50 states and the District of Columbia now have laws regarding sports-related concussion. And there are brain banks in Australia, Canada, New Zealand, Brazil, and the United Kingdom studying CTE. More than 2,500 athletes in a variety of sports, including NASCAR’s Dale Earnhardt Jr. and NFL hall of famer Nick Buoniconti, have publicly pledged to donate their brains to science after their deaths.
Second, said Dr. Stern, we now know that although concussions can contribute to CTE, they are not the sole cause. It’s repetitive subconcussive trauma, without symptoms of concussion, that do the most damage.
“These happen during every practice and in every game,” said Dr. Stern. In fact, it’s estimated that pro football players suffer thousands of subconcussive incidents over the course of their careers. So, a player doesn’t have to see stars or lose consciousness to suffer brain damage; small impacts can accumulate over time.
Understanding this point is crucial for making youth sports safer. “Chris has played a critical role in raising awareness here, too,” said Dr. Stern. “Allowing our kids to get hit in the head over and over can put them at greater risk for later problems, plus it just doesn’t make common sense.”
“The biggest misconception surrounding head trauma in sports,” said Dr. Nowinski, “is the belief among players, coaches, and even the medical and scientific communities that if you get hit in the head and don’t have any symptoms then you’re okay and there hasn’t been any damage. That couldn’t be further from the truth. We now know that people are suffering serious brain injuries due to the accumulated effect of subconcussive impacts, and we need to get the word out about that.”
A major initiative from the Concussion Legacy Foundation called “Stop Hitting Kids in the Head” has the goal of convincing every sport to eliminate repetitive head impacts in players under age 14 – the time when the skull and brain are still developing and most vulnerable – by 2026. In fact, Dr. Nowinski wrote that “there could be a lot of kids who are misdiagnosed and medicated for various behavioral or emotional problems that may actually be head injury–related.”
Starting in 2009, the NFL adopted a series of rule changes designed to better protect its players against repeated head trauma. Among them is a ban on spearing or leading with the helmet, penalties for hitting defenseless players, and more stringent return-to-play guidelines, including concussion protocols.
The NFL has also put more emphasis on flag football options for youngsters and, for the first time, showcased this alternative in the 2023 Pro Bowl. But Dr. Nowinski is pressuring the league to go further. “While acknowledging that the game causes CTE, the NFL still underwrites recruiting 5-year-olds to play tackle football,” he said. “In my opinion, that’s unethical, and it needs to be addressed.”
WWE one of the most responsive organizations
Dr. Nowinski said WWE has been one of the most responsive sports organizations for protecting athletes. A doctor is now ringside at every match as is an observer who knows the script, thereby allowing for instant medical intervention if something goes wrong. “Since everyone is trying to look like they have a concussion all the time, it takes a deep understanding of the business to recognize a real one,” he said.
But this hasn’t been the case with other sports. “I am eternally disappointed in the response of the professional sports industry to the knowledge of CTE and long-term concussion symptoms,” said Dr. Nowinski.
“For example, FIFA [international soccer’s governing body] still doesn’t allow doctors to evaluate [potentially concussed] players on the sidelines and put them back in the game with a free substitution [if they’re deemed okay]. Not giving players proper medical care for a brain injury is unethical,” he said. BU’s Center for the Study of Traumatic Encephalopathy diagnosed the first CTE case in soccer in 2012, and in 2015 Dr. Nowinski successfully lobbied U.S. Soccer to ban heading the ball before age 11.
“Unfortunately, many governing bodies have circled the wagons in denying their sport causes CTE,” he continued. “FIFA, World Rugby, the NHL, even the NCAA and International Olympic Committee refuse to acknowledge it and, therefore, aren’t taking any steps to prevent it. They see it as a threat to their business model. Hopefully, now that the NIH and CDC are aligned about the risks of head impact in sports, this will begin to change.”
Meanwhile, research is continuing. Scientists are getting closer to being able to diagnose CTE in living humans, with ongoing studies using PET scans, blood markers, and spinal fluid markers. In 2019, researchers identified tau proteins specific to CTE that they believe are distinct from those of Alzheimer’s and other neurodegenerative diseases. Next step would be developing a drug to slow the development of CTE once detected.
Nonetheless, athletes at all levels in impact sports still don’t fully appreciate the risks of repeated head trauma and especially subconcussive blows. “I talk to former NFL and college players every week,” said Dr. Stern. “Some tell me, ‘I love the sport, it gave me so much, and I would do it again, but I’m not letting my grandchildren play.’ But others say, ‘As long as they know the risks, they can make their own decision.’ “
Dr. Nowinski has a daughter who is 4 and a son who’s 2. Both play soccer but, thanks to dad, heading isn’t allowed in their age groups. If they continue playing sports, Dr. Nowinski said he’ll make sure they understand the risks and how to protect themselves. This is a conversation all parents should have with their kids at every level to make sure they play safe, he added.
Those in the medical community can also volunteer their time to explain head trauma to athletes, coaches, and school administrators to be sure they understand its seriousness and are doing everything to protect players.
As you watch this year’s Super Bowl, Dr. Nowinski and his team would like you to keep something in mind. Those young men on the field for your entertainment are receiving mild brain trauma repeatedly throughout the game.
Even if it’s not a huge hit that gets replayed and makes everyone gasp, even if no one gets ushered into the little sideline tent for a concussion screening, even if no one loses consciousness, brain damage is still occurring. Watch the heads of the players during every play and think about what’s going on inside their skulls regardless of how big and strong those helmets look.
A version of this article first appeared on Medscape.com.
On Oct. 5, 2022, at 10:24 a.m., Chris Nowinski, PhD, cofounder of the Boston-based Concussion Legacy Foundation (CLF), was in his home office when the email came through.
“I pounded my desk, shouted YES! and went to find my wife so I could pick her up and give her a big hug,” he recalled. “It was the culmination of 15 years of research and hard work.”
Robert Cantu, MD, who has been studying head trauma for 50+ years and has published more than 500 papers about it, compares the announcement to the 1964 Surgeon General’s report that linked cigarette smoking with lung cancer and heart disease. With the NIH and the Centers of Disease Control and Prevention (CDC) now in agreement about the risks of participating in impact sports and activities, he said, “We’ve reached a tipping point that should finally prompt deniers such as the NHL, NCAA, FIFA, World Rugby, the International Olympic Committee, and other [sports organizations] to remove all unnecessary head trauma from their sports.”
“A lot of the credit for this must go to Chris,” added Dr. Cantu, medical director and director of clinical research at the Cantu Concussion Center at Emerson Hospital in Concord, Mass. “Clinicians like myself can reach only so many people by writing papers and giving speeches at medical conferences. For this to happen, the message needed to get out to parents, athletes, and society in general. And Chris was the vehicle for doing that.”
Dr. Nowinski didn’t set out to be the messenger. He played football at Harvard in the late 1990s, making second-team All-Ivy as a defensive tackle his senior year. In 2000, he enrolled in Killer Kowalski’s Wrestling Institute and eventually joined Vince McMahon’s World Wrestling Entertainment (WWE).
There he played the role of 295-pound villain “Chris Harvard,” an intellectual snob who dressed in crimson tights and insulted the crowd’s IQ. “Roses are red. Violets are blue. The reason I’m talking so slowly is because no one in [insert name of town he was appearing in] has passed grade 2!”
“I’d often apply my education during a match,” he wrote in his book, “Head Games: Football’s Concussion Crisis.“ In a match in Bridgeport, Conn., I assaulted [my opponent] with a human skeleton, ripped off the skull, got down on bended knee, and began reciting Hamlet. Those were good times.”
Those good times ended abruptly, however, during a match with Bubba Ray Dudley at the Hartford Civic Center in Connecticut in 2003. Even though pro wrestling matches are rehearsed, and the blows aren’t real, accidents happen. Mr. Dudley mistakenly kicked Dr. Nowinski in the jaw with enough force to put him on his back and make the whole ring shake.
“Holy shit, kid! You okay?” asked the referee. Before a foggy Dr. Nowinski could reply, 300-pound Mr. Dudley crashed down on him, hooked his leg, and the ref began counting, “One! Two! …” Dr. Nowinski instinctively kicked out but had forgotten the rest of the script. He managed to finish the match and stagger backstage.
His coherence and awareness gradually returned, but a “throbbing headache” persisted. A locker room doctor said he might have a concussion and recommended he wait to see how he felt before wrestling in Albany, N.Y., the next evening.
The following day the headache had subsided, but he still felt “a little strange.” Nonetheless, he told the doctor he was fine and strutted out to again battle Bubba Ray, this time in a match where he eventually got thrown through a ringside table and suffered the Dudley Death Drop. Afterward, “I crawled backstage and laid down. The headache was much, much worse.”
An event and a process
Dr. Nowinski continued to insist he was “fine” and wrestled a few more matches in the following days before finally acknowledging something was wrong. He’d had his bell rung numerous times in football, but this was different. Even more worrisome, none of the doctors he consulted could give him any definitive answers. He finally found his way to Emerson Hospital, where Dr. Cantu was the chief of neurosurgery.
“I remember that day vividly,” said Dr. Cantu. “Chris was this big, strapping, handsome guy – a hell of an athlete whose star was rising. He didn’t realize that he’d suffered a series of concussions and that trying to push through them was the worst thing he could be doing.”
Concussions and their effects were misunderstood by many athletes, coaches, and even physicians back then. It was assumed that the quarter inch of bone surrounding the adult brain provided adequate protection from common sports impacts and that any aftereffects were temporary. A common treatment was smelling salts and a pat on the back as the athlete returned to action.
However, the brain floats inside the skull in a bath of cerebral fluid. Any significant impact causes it to slosh violently from side to side, damaging tissue, synapses, and cells resulting in inflammation that can manifest as confusion and brain fog.
“A concussion is actually not defined by a physical injury,” explained Dr. Nowinski, “but by a loss of brain function that is induced by trauma. Concussion is not just an event, but also a process.” It’s almost as if the person has suffered a small seizure.
Fortunately, most concussion symptoms resolve within 2 weeks, but in some cases, especially if there’s been additional head trauma, they can persist, causing anxiety, depression, anger, and/or sleep disorders. Known as postconcussion syndrome (PCS), this is what Dr. Nowinski was unknowingly suffering from when he consulted Dr. Cantu.
In fact, one night it an Indianapolis hotel, weeks after his initial concussion, he awoke to find himself on the floor and the room in shambles. His girlfriend was yelling his name and shaking him. She told him he’d been having a nightmare and had suddenly started screaming and tearing up the room. “I didn’t remember any of it,” he said.
Dr. Cantu eventually advised Dr. Nowinski against ever returning to the ring or any activity with the risk for head injury. Research shows that sustaining a single significant concussion increases the risk of subsequent more-severe brain injuries.
“My diagnosis could have sent Chris off the deep end because he could no longer do what he wanted to do with this life,” said Dr. Cantu. “But instead, he used it as a tool to find meaning for his life.”
Dr. Nowinski decided to use his experience as a teaching opportunity, not just for other athletes but also for sports organizations and the medical community.
His book, which focused on the NFL’s “tobacco-industry-like refusal to acknowledge the depths of the problem,” was published in 2006. A year later, Dr. Nowinski partnered with Dr. Cantu to found the Sports Legacy Institute, which eventually became the Concussion Legacy Foundation (CLF).
Cold calling for brain donations
Robert Stern, PhD, is another highly respected authority in the study of neurodegenerative disease. In 2007, he was directing the clinical core of Boston University’s Alzheimer’s Disease Center. After giving a lecture to a group of financial planners and elder-law attorneys one morning, he got a request for a private meeting from a fellow named Chris Nowinski.
“I’d never heard of him, but I agreed,” recalled Dr. Stern, a professor of neurology, neurosurgery, anatomy, and neurobiology at Boston University. “A few days later, this larger-than-life guy walked into our conference room at the BU School of Medicine, exuding a great deal of passion, intellect, and determination. He told me his story and then started talking about the long-term consequences of concussions in sports.”
Dr. Stern had seen patients with dementia pugilistica, the old-school term for CTE. These were mostly boxers with cognitive and behavioral impairment. “But I had not heard about football players,” he said. “I hadn’t put the two together. And as I was listening to Chris, I realized if what he was saying was true then it was not only a potentially huge public health issue, but it was also a potentially huge scientific issue in the field of neurodegenerative disease.”
Dr. Nowinski introduced Dr. Stern to Dr. Cantu, and together with Ann McKee, MD, professor of neurology and pathology at BU, they cofounded the Center for the Study of Traumatic Encephalopathy (CSTE) in 2008. It was the first center of its kind devoted to the study of CTE in the world.
One of Dr. Nowinski’s first jobs at the CSTE was soliciting and procuring brain donations. Since CTE is generally a progressive condition that can take decades to manifest, autopsy was the only way to detect it.
The brains of two former Pittsburgh Steelers, Mike Webster and Terry Long, had been examined after their untimely deaths. After immunostaining, investigators found both former NFL players had “protein misfolds” characteristic of CTE.
This finding drew a lot of public and scientific attention, given that Mr. Long died by suicide and Mr. Webster was homeless when he died of a heart attack. But more scientific evidence was needed to prove a causal link between the head trauma and CTE.
Dr. Nowinski scoured obituaries looking for potential brains to study. When he found one, he would cold call the family and try to convince them to donate it to science. The first brain he secured for the center belonged to John Grimsley, a former NFL linebacker who in 2008 died at age 45 of an accidental gunshot wound. Often, Dr. Nowinski would even be the courier, traveling to pick up the brain after it had been harvested.
Over the next 10 years, Dr. Nowinski and his research team secured 500 brain donations. The research that resulted was staggering. In the beginning only 45 cases of CTE had been identified in the world, but in the first 111 NFL players who were autopsied, 110 had the disorder.
Of the first 53 college football players autopsied, 48 had CTE. Although Dr. Nowinski’s initial focus was football, evidence of CTE was soon detected among athletes in boxing, hockey, soccer, and rugby, as well as in combat veterans. However, the National Football League and other governing sports bodies initially denied any connection between sport-related head trauma and CTE.
Cumulative damage
In 2017, after 7 years of study, Dr. Nowinski earned a PhD in neurology. As the scientific evidence continued to accumulate, two shifts occurred that Dr. Stern said represent Dr. Nowinski’s greatest contributions. First, concussion is now widely recognized as an acute brain injury with symptoms that need to be immediately diagnosed and addressed.
“This is a completely different story from where things were just 10 years ago,” said Dr. Stern, “and Chris played a central role, if not the central role, in raising awareness about that.”
All 50 states and the District of Columbia now have laws regarding sports-related concussion. And there are brain banks in Australia, Canada, New Zealand, Brazil, and the United Kingdom studying CTE. More than 2,500 athletes in a variety of sports, including NASCAR’s Dale Earnhardt Jr. and NFL hall of famer Nick Buoniconti, have publicly pledged to donate their brains to science after their deaths.
Second, said Dr. Stern, we now know that although concussions can contribute to CTE, they are not the sole cause. It’s repetitive subconcussive trauma, without symptoms of concussion, that do the most damage.
“These happen during every practice and in every game,” said Dr. Stern. In fact, it’s estimated that pro football players suffer thousands of subconcussive incidents over the course of their careers. So, a player doesn’t have to see stars or lose consciousness to suffer brain damage; small impacts can accumulate over time.
Understanding this point is crucial for making youth sports safer. “Chris has played a critical role in raising awareness here, too,” said Dr. Stern. “Allowing our kids to get hit in the head over and over can put them at greater risk for later problems, plus it just doesn’t make common sense.”
“The biggest misconception surrounding head trauma in sports,” said Dr. Nowinski, “is the belief among players, coaches, and even the medical and scientific communities that if you get hit in the head and don’t have any symptoms then you’re okay and there hasn’t been any damage. That couldn’t be further from the truth. We now know that people are suffering serious brain injuries due to the accumulated effect of subconcussive impacts, and we need to get the word out about that.”
A major initiative from the Concussion Legacy Foundation called “Stop Hitting Kids in the Head” has the goal of convincing every sport to eliminate repetitive head impacts in players under age 14 – the time when the skull and brain are still developing and most vulnerable – by 2026. In fact, Dr. Nowinski wrote that “there could be a lot of kids who are misdiagnosed and medicated for various behavioral or emotional problems that may actually be head injury–related.”
Starting in 2009, the NFL adopted a series of rule changes designed to better protect its players against repeated head trauma. Among them is a ban on spearing or leading with the helmet, penalties for hitting defenseless players, and more stringent return-to-play guidelines, including concussion protocols.
The NFL has also put more emphasis on flag football options for youngsters and, for the first time, showcased this alternative in the 2023 Pro Bowl. But Dr. Nowinski is pressuring the league to go further. “While acknowledging that the game causes CTE, the NFL still underwrites recruiting 5-year-olds to play tackle football,” he said. “In my opinion, that’s unethical, and it needs to be addressed.”
WWE one of the most responsive organizations
Dr. Nowinski said WWE has been one of the most responsive sports organizations for protecting athletes. A doctor is now ringside at every match as is an observer who knows the script, thereby allowing for instant medical intervention if something goes wrong. “Since everyone is trying to look like they have a concussion all the time, it takes a deep understanding of the business to recognize a real one,” he said.
But this hasn’t been the case with other sports. “I am eternally disappointed in the response of the professional sports industry to the knowledge of CTE and long-term concussion symptoms,” said Dr. Nowinski.
“For example, FIFA [international soccer’s governing body] still doesn’t allow doctors to evaluate [potentially concussed] players on the sidelines and put them back in the game with a free substitution [if they’re deemed okay]. Not giving players proper medical care for a brain injury is unethical,” he said. BU’s Center for the Study of Traumatic Encephalopathy diagnosed the first CTE case in soccer in 2012, and in 2015 Dr. Nowinski successfully lobbied U.S. Soccer to ban heading the ball before age 11.
“Unfortunately, many governing bodies have circled the wagons in denying their sport causes CTE,” he continued. “FIFA, World Rugby, the NHL, even the NCAA and International Olympic Committee refuse to acknowledge it and, therefore, aren’t taking any steps to prevent it. They see it as a threat to their business model. Hopefully, now that the NIH and CDC are aligned about the risks of head impact in sports, this will begin to change.”
Meanwhile, research is continuing. Scientists are getting closer to being able to diagnose CTE in living humans, with ongoing studies using PET scans, blood markers, and spinal fluid markers. In 2019, researchers identified tau proteins specific to CTE that they believe are distinct from those of Alzheimer’s and other neurodegenerative diseases. Next step would be developing a drug to slow the development of CTE once detected.
Nonetheless, athletes at all levels in impact sports still don’t fully appreciate the risks of repeated head trauma and especially subconcussive blows. “I talk to former NFL and college players every week,” said Dr. Stern. “Some tell me, ‘I love the sport, it gave me so much, and I would do it again, but I’m not letting my grandchildren play.’ But others say, ‘As long as they know the risks, they can make their own decision.’ “
Dr. Nowinski has a daughter who is 4 and a son who’s 2. Both play soccer but, thanks to dad, heading isn’t allowed in their age groups. If they continue playing sports, Dr. Nowinski said he’ll make sure they understand the risks and how to protect themselves. This is a conversation all parents should have with their kids at every level to make sure they play safe, he added.
Those in the medical community can also volunteer their time to explain head trauma to athletes, coaches, and school administrators to be sure they understand its seriousness and are doing everything to protect players.
As you watch this year’s Super Bowl, Dr. Nowinski and his team would like you to keep something in mind. Those young men on the field for your entertainment are receiving mild brain trauma repeatedly throughout the game.
Even if it’s not a huge hit that gets replayed and makes everyone gasp, even if no one gets ushered into the little sideline tent for a concussion screening, even if no one loses consciousness, brain damage is still occurring. Watch the heads of the players during every play and think about what’s going on inside their skulls regardless of how big and strong those helmets look.
A version of this article first appeared on Medscape.com.
Mental health system failing kids leaving ED
Only 56% of children enrolled in Medicaid received any outpatient follow-up within 30 days after a mental health emergency department discharge, according to results of a large study released in Pediatrics.
Fewer than one-third (31.2%) had an outpatient visit within a week after a mental health ED discharge.
Researchers conducted a retrospective study of 28,551 children ages 6-17 years old who had mental health discharges from EDs from January 2018 to June 2019.
The researchers, led by Jennifer A. Hoffmann, MD, MS, with the division of emergency medicine, Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, Chicago, also analyzed the effect that having a timely follow-up had on whether the child was likely to return to the ED.
Follow-up within 30 days cuts risk of quick return to ED
They found that follow-up within 30 days was linked with a 26% decreased risk of return within 5 days of the initial ED discharge (hazard ratio, 0.74; 95% confidence interval, 0.63-0.91).
The researchers also found racial disparities in the data. The odds for getting follow-up outpatient care were lower for non-Hispanic Black children, for children with fee-for-service insurance, and for children with no previous mental health outpatient visits.
The numbers were particularly striking for Black children, who were 10% less likely to get outpatient follow-up than their White counterparts.
In addition, 27% of all children in this sample returned to the ED for mental health-related symptoms within 6 months, 20% spent more than 48 hours in the ED for their initial mental health visit, and children with 14 or more mental health outpatient visits had five times higher adjusted odds of follow-up within 7 days and 9.5 times higher adjusted odds of follow-up within 30 days, compared with children with no outpatient mental health visits in the previous year.
A ‘mental health system of care in crisis’
In an accompanying editorial, Hannah E. Karpman, MSW, PhD, with the department of pediatrics, University of Massachusetts, Worcester, and colleagues said those statistics help expose other signs of “a pediatric mental health system of care in crisis.”
If one in five children are spending more than 2 days in the ED for their initial mental health visit, they wrote, that signals the follow-up care they need is not readily available.
The 27% returning to the ED shows that, even if the children are getting outpatient services, that environment is failing them, they noted.
Additionally, 28% of children presented with more than four mental health diagnoses, “suggesting poor diagnostic specificity or perhaps inadequate diagnostic categories to characterize their needs.”
The authors called for interventions that link patients to outpatient care within 5 days of a mental health ED discharge.
The editorialists wrote: “We believe it is time for a “child mental health moonshot,” and call on the field and its funders to come together to launch the next wave of bold mental health research for the benefit of these children and their families who so desperately need our support.”
Things may even be worse in light of COVID
David Rettew, MD, a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland, said in an interview the numbers won’t surprise clinicians who support these children or the patients’ families.
He added that he wouldn’t be surprised if things are even worse now after this study’s data collection, “as COVID and other factors have driven more mental health professionals away from many of the people who need them the most.”
The study does present new evidence that quick access to care is particularly tough for young people who aren’t already established in care, he noted.
“As wait lists grow at outpatient clinics, we are seeing ever stronger need for centers willing and able to provide actual mental health assessment and treatment for people right ‘off the street,’” he said.
Dr. Rettew emphasized that, because mental health conditions rarely improve quickly, having a timely follow-up appointment is important, but won’t likely bring quick improvement.
He agreed with the editorialists’ argument and emphasized, “not only do we need to focus on more rapid care, but also more comprehensive and effective care.
“For an adolescent in crisis, achieving stability often involves more than a medication tweak and a supportive conversation,” Dr. Rettew said. “Rather, it can require an intensive multimodal approach that addresses things like family financial stressors, parental mental health and substance use concerns, school supports, and health promotion or lifestyle changes. What we desperately need are more teams that can quickly intervene on all these levels.”
Addressing problems before crisis is essential
Ideally, teams would address these issues before a crisis. That helps support the “moonshot” charge the editorialists suggest, which “would significantly disrupt the current way we value different components of our health care system,” Dr. Rettew said.
He highlighted a statistic that may get lost in the data: Nearly 40% of youth in enough danger to need an ED visit had no more than one health-related appointment of any kind in the previous year.
“To me, this speaks volumes about the need for earlier involvement before things escalate to the level of an emergency,” Dr. Rettew said.
The authors and editorialists declared no relevant financial relationships. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
Only 56% of children enrolled in Medicaid received any outpatient follow-up within 30 days after a mental health emergency department discharge, according to results of a large study released in Pediatrics.
Fewer than one-third (31.2%) had an outpatient visit within a week after a mental health ED discharge.
Researchers conducted a retrospective study of 28,551 children ages 6-17 years old who had mental health discharges from EDs from January 2018 to June 2019.
The researchers, led by Jennifer A. Hoffmann, MD, MS, with the division of emergency medicine, Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, Chicago, also analyzed the effect that having a timely follow-up had on whether the child was likely to return to the ED.
Follow-up within 30 days cuts risk of quick return to ED
They found that follow-up within 30 days was linked with a 26% decreased risk of return within 5 days of the initial ED discharge (hazard ratio, 0.74; 95% confidence interval, 0.63-0.91).
The researchers also found racial disparities in the data. The odds for getting follow-up outpatient care were lower for non-Hispanic Black children, for children with fee-for-service insurance, and for children with no previous mental health outpatient visits.
The numbers were particularly striking for Black children, who were 10% less likely to get outpatient follow-up than their White counterparts.
In addition, 27% of all children in this sample returned to the ED for mental health-related symptoms within 6 months, 20% spent more than 48 hours in the ED for their initial mental health visit, and children with 14 or more mental health outpatient visits had five times higher adjusted odds of follow-up within 7 days and 9.5 times higher adjusted odds of follow-up within 30 days, compared with children with no outpatient mental health visits in the previous year.
A ‘mental health system of care in crisis’
In an accompanying editorial, Hannah E. Karpman, MSW, PhD, with the department of pediatrics, University of Massachusetts, Worcester, and colleagues said those statistics help expose other signs of “a pediatric mental health system of care in crisis.”
If one in five children are spending more than 2 days in the ED for their initial mental health visit, they wrote, that signals the follow-up care they need is not readily available.
The 27% returning to the ED shows that, even if the children are getting outpatient services, that environment is failing them, they noted.
Additionally, 28% of children presented with more than four mental health diagnoses, “suggesting poor diagnostic specificity or perhaps inadequate diagnostic categories to characterize their needs.”
The authors called for interventions that link patients to outpatient care within 5 days of a mental health ED discharge.
The editorialists wrote: “We believe it is time for a “child mental health moonshot,” and call on the field and its funders to come together to launch the next wave of bold mental health research for the benefit of these children and their families who so desperately need our support.”
Things may even be worse in light of COVID
David Rettew, MD, a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland, said in an interview the numbers won’t surprise clinicians who support these children or the patients’ families.
He added that he wouldn’t be surprised if things are even worse now after this study’s data collection, “as COVID and other factors have driven more mental health professionals away from many of the people who need them the most.”
The study does present new evidence that quick access to care is particularly tough for young people who aren’t already established in care, he noted.
“As wait lists grow at outpatient clinics, we are seeing ever stronger need for centers willing and able to provide actual mental health assessment and treatment for people right ‘off the street,’” he said.
Dr. Rettew emphasized that, because mental health conditions rarely improve quickly, having a timely follow-up appointment is important, but won’t likely bring quick improvement.
He agreed with the editorialists’ argument and emphasized, “not only do we need to focus on more rapid care, but also more comprehensive and effective care.
“For an adolescent in crisis, achieving stability often involves more than a medication tweak and a supportive conversation,” Dr. Rettew said. “Rather, it can require an intensive multimodal approach that addresses things like family financial stressors, parental mental health and substance use concerns, school supports, and health promotion or lifestyle changes. What we desperately need are more teams that can quickly intervene on all these levels.”
Addressing problems before crisis is essential
Ideally, teams would address these issues before a crisis. That helps support the “moonshot” charge the editorialists suggest, which “would significantly disrupt the current way we value different components of our health care system,” Dr. Rettew said.
He highlighted a statistic that may get lost in the data: Nearly 40% of youth in enough danger to need an ED visit had no more than one health-related appointment of any kind in the previous year.
“To me, this speaks volumes about the need for earlier involvement before things escalate to the level of an emergency,” Dr. Rettew said.
The authors and editorialists declared no relevant financial relationships. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
Only 56% of children enrolled in Medicaid received any outpatient follow-up within 30 days after a mental health emergency department discharge, according to results of a large study released in Pediatrics.
Fewer than one-third (31.2%) had an outpatient visit within a week after a mental health ED discharge.
Researchers conducted a retrospective study of 28,551 children ages 6-17 years old who had mental health discharges from EDs from January 2018 to June 2019.
The researchers, led by Jennifer A. Hoffmann, MD, MS, with the division of emergency medicine, Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, Chicago, also analyzed the effect that having a timely follow-up had on whether the child was likely to return to the ED.
Follow-up within 30 days cuts risk of quick return to ED
They found that follow-up within 30 days was linked with a 26% decreased risk of return within 5 days of the initial ED discharge (hazard ratio, 0.74; 95% confidence interval, 0.63-0.91).
The researchers also found racial disparities in the data. The odds for getting follow-up outpatient care were lower for non-Hispanic Black children, for children with fee-for-service insurance, and for children with no previous mental health outpatient visits.
The numbers were particularly striking for Black children, who were 10% less likely to get outpatient follow-up than their White counterparts.
In addition, 27% of all children in this sample returned to the ED for mental health-related symptoms within 6 months, 20% spent more than 48 hours in the ED for their initial mental health visit, and children with 14 or more mental health outpatient visits had five times higher adjusted odds of follow-up within 7 days and 9.5 times higher adjusted odds of follow-up within 30 days, compared with children with no outpatient mental health visits in the previous year.
A ‘mental health system of care in crisis’
In an accompanying editorial, Hannah E. Karpman, MSW, PhD, with the department of pediatrics, University of Massachusetts, Worcester, and colleagues said those statistics help expose other signs of “a pediatric mental health system of care in crisis.”
If one in five children are spending more than 2 days in the ED for their initial mental health visit, they wrote, that signals the follow-up care they need is not readily available.
The 27% returning to the ED shows that, even if the children are getting outpatient services, that environment is failing them, they noted.
Additionally, 28% of children presented with more than four mental health diagnoses, “suggesting poor diagnostic specificity or perhaps inadequate diagnostic categories to characterize their needs.”
The authors called for interventions that link patients to outpatient care within 5 days of a mental health ED discharge.
The editorialists wrote: “We believe it is time for a “child mental health moonshot,” and call on the field and its funders to come together to launch the next wave of bold mental health research for the benefit of these children and their families who so desperately need our support.”
Things may even be worse in light of COVID
David Rettew, MD, a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland, said in an interview the numbers won’t surprise clinicians who support these children or the patients’ families.
He added that he wouldn’t be surprised if things are even worse now after this study’s data collection, “as COVID and other factors have driven more mental health professionals away from many of the people who need them the most.”
The study does present new evidence that quick access to care is particularly tough for young people who aren’t already established in care, he noted.
“As wait lists grow at outpatient clinics, we are seeing ever stronger need for centers willing and able to provide actual mental health assessment and treatment for people right ‘off the street,’” he said.
Dr. Rettew emphasized that, because mental health conditions rarely improve quickly, having a timely follow-up appointment is important, but won’t likely bring quick improvement.
He agreed with the editorialists’ argument and emphasized, “not only do we need to focus on more rapid care, but also more comprehensive and effective care.
“For an adolescent in crisis, achieving stability often involves more than a medication tweak and a supportive conversation,” Dr. Rettew said. “Rather, it can require an intensive multimodal approach that addresses things like family financial stressors, parental mental health and substance use concerns, school supports, and health promotion or lifestyle changes. What we desperately need are more teams that can quickly intervene on all these levels.”
Addressing problems before crisis is essential
Ideally, teams would address these issues before a crisis. That helps support the “moonshot” charge the editorialists suggest, which “would significantly disrupt the current way we value different components of our health care system,” Dr. Rettew said.
He highlighted a statistic that may get lost in the data: Nearly 40% of youth in enough danger to need an ED visit had no more than one health-related appointment of any kind in the previous year.
“To me, this speaks volumes about the need for earlier involvement before things escalate to the level of an emergency,” Dr. Rettew said.
The authors and editorialists declared no relevant financial relationships. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
FROM PEDIATRICS
The X-waiver is dead
In 2016, when Erin Schanning lost her brother Ethan to an overdose, she wanted to know what could have been done to have helped him. Ethan, who had struggled with opioids since getting a prescription for the drugs after a dental procedure in middle school, had tried dozens of treatments. But at the age of 30, he was gone.
“After my brother died, I started researching and was surprised to learn that there were many evidence-based ways to treat substance use disorder that he hadn’t had access to, even though he had doggedly pursued treatment,” Ms. Schanning told me in an interview. One of those treatments, buprenorphine, is one of the most effective tools that health care providers have to treat opioid use disorder. A partial opioid agonist, it reduces cravings and prevents overdose, decreasing mortality more effectively than almost any medication for any disease. Yet most providers have never prescribed it.
That may be about to change. The special license to prescribe the medication, commonly known as the “X-waiver,” was officially eliminated as part of the passage of the Mainstreaming Addiction Treatment (MAT) Act. Immediately, following the passage of the Act, any provider with a DEA license became eligible to prescribe buprenorphine to treat opioid use disorder, and limits on the number of patients they could treat were eliminated.
Previously, buprenorphine, which has a better safety profile than almost any other prescription opioid because of its ceiling effect on respiratory depression,nonetheless required providers to obtain a special license to prescribe it, and – prior to an executive order from the Biden administration – 8 to 24 hours of training to do so. This led to a misconception that buprenorphine was dangerous, and created barriers for treatment during the worst overdose crisis in our country’s history. More than 110,00 overdose deaths occurred in 2021, representing a 468% increase in the last 2 decades.
Along with the MAT Act, the Medication Access and Training Expansion Act was passed in the same spending bill, requiring all prescribers who obtain a DEA license to do 8 hours of training on the treatment of substance use disorders. According to the Act, addiction specialty societies will have a role in creating trainings. Medical schools and residencies will also be able to fulfill this requirement with a “comprehensive” curriculum that covers all approved medications for the treatment of substance use disorders.
The DEA has not yet confirmed what training will be accepted, according to the Chief Medical Officer of the Substance Abuse and Mental Health Services Administration, Neeraj Gandotra, MD, who spoke to me in an interview. However, it is required to do so by April 5, 2023. Dr. Gandotra also emphasized that state and local laws, as well as insurance requirements, remain in place, and may place other constraints on prescribing. According to the Act, this new rule will be in effect by June 2023.
As an addiction medicine specialist and longtime buprenorphine prescriber, I am excited about these changes but wary of lingering resistance among health care providers. Will providers who have chosen not to get an X-waiver now look for another reason to not treat patients with substance use disorders?
Ms. Schanning remains hopeful. “I’m incredibly optimistic that health care providers are going to learn about buprenorphine and prescribe it to patients, and that patients are going to start asking about this medication,” she told me. “Seven in 10 providers say that they do feel an obligation to treat their patients with [opioid use disorder], but the federal government has made it very difficult to do so.”
Now with the X-waiver gone, providers and patients may be able to push for a long overdue shift in how we treat and conceptualize substance use disorders, she noted.
“Health care providers need to recognize substance use disorder as a medical condition that deserves treatment, and to speak about it like a medical condition,” Ms. Schanning said, by, for instance, moving away from using words such as “abuse” and “clean” and, instead, talking about treatable substance use disorders that can improve with evidence-based care, such as buprenorphine and methadone. “We also need to share stories of success and hope with people,” she added. “Once you’ve seen how someone can be transformed by treatment, it’s really difficult to say that substance use disorder is a character flaw, or their fault.”
A patient-centered approach
Over the past decade of practicing medicine, I have experienced this transformation personally. In residency, I believed that people had to be ready for help, to stop using, to change. I failed to recognize that many of those same people were asking me for help, and I wasn’t offering what they needed. The person who had to change was me.
As I moved toward a patient-centered approach, lowering barriers to starting and remaining in treatment, and collaborating with teams that could meet people wherever they might be, addictions became the most rewarding part of my practice.
I have never had more people thank me spontaneously and deeply for the care I provide. Plus, I have never seen a more profound change in the students I work with than when they witness someone with a substance use disorder offered treatment that works.
The X-waiver was not the only barrier to care, and the overdose crisis is not slowing down. But maybe with a new tool widely accessible, more of us will be ready to help.
Dr. Poorman is board certified in internal medicine and addiction medicine, assistant professor of medicine, University of Illinois at Chicago, and provides primary care and addiction services in Chicago. Her views do not necessarily reflect the views of her employer. She has reported no relevant disclosures, and she serves on the editorial advisory board of Internal Medicine News.
In 2016, when Erin Schanning lost her brother Ethan to an overdose, she wanted to know what could have been done to have helped him. Ethan, who had struggled with opioids since getting a prescription for the drugs after a dental procedure in middle school, had tried dozens of treatments. But at the age of 30, he was gone.
“After my brother died, I started researching and was surprised to learn that there were many evidence-based ways to treat substance use disorder that he hadn’t had access to, even though he had doggedly pursued treatment,” Ms. Schanning told me in an interview. One of those treatments, buprenorphine, is one of the most effective tools that health care providers have to treat opioid use disorder. A partial opioid agonist, it reduces cravings and prevents overdose, decreasing mortality more effectively than almost any medication for any disease. Yet most providers have never prescribed it.
That may be about to change. The special license to prescribe the medication, commonly known as the “X-waiver,” was officially eliminated as part of the passage of the Mainstreaming Addiction Treatment (MAT) Act. Immediately, following the passage of the Act, any provider with a DEA license became eligible to prescribe buprenorphine to treat opioid use disorder, and limits on the number of patients they could treat were eliminated.
Previously, buprenorphine, which has a better safety profile than almost any other prescription opioid because of its ceiling effect on respiratory depression,nonetheless required providers to obtain a special license to prescribe it, and – prior to an executive order from the Biden administration – 8 to 24 hours of training to do so. This led to a misconception that buprenorphine was dangerous, and created barriers for treatment during the worst overdose crisis in our country’s history. More than 110,00 overdose deaths occurred in 2021, representing a 468% increase in the last 2 decades.
Along with the MAT Act, the Medication Access and Training Expansion Act was passed in the same spending bill, requiring all prescribers who obtain a DEA license to do 8 hours of training on the treatment of substance use disorders. According to the Act, addiction specialty societies will have a role in creating trainings. Medical schools and residencies will also be able to fulfill this requirement with a “comprehensive” curriculum that covers all approved medications for the treatment of substance use disorders.
The DEA has not yet confirmed what training will be accepted, according to the Chief Medical Officer of the Substance Abuse and Mental Health Services Administration, Neeraj Gandotra, MD, who spoke to me in an interview. However, it is required to do so by April 5, 2023. Dr. Gandotra also emphasized that state and local laws, as well as insurance requirements, remain in place, and may place other constraints on prescribing. According to the Act, this new rule will be in effect by June 2023.
As an addiction medicine specialist and longtime buprenorphine prescriber, I am excited about these changes but wary of lingering resistance among health care providers. Will providers who have chosen not to get an X-waiver now look for another reason to not treat patients with substance use disorders?
Ms. Schanning remains hopeful. “I’m incredibly optimistic that health care providers are going to learn about buprenorphine and prescribe it to patients, and that patients are going to start asking about this medication,” she told me. “Seven in 10 providers say that they do feel an obligation to treat their patients with [opioid use disorder], but the federal government has made it very difficult to do so.”
Now with the X-waiver gone, providers and patients may be able to push for a long overdue shift in how we treat and conceptualize substance use disorders, she noted.
“Health care providers need to recognize substance use disorder as a medical condition that deserves treatment, and to speak about it like a medical condition,” Ms. Schanning said, by, for instance, moving away from using words such as “abuse” and “clean” and, instead, talking about treatable substance use disorders that can improve with evidence-based care, such as buprenorphine and methadone. “We also need to share stories of success and hope with people,” she added. “Once you’ve seen how someone can be transformed by treatment, it’s really difficult to say that substance use disorder is a character flaw, or their fault.”
A patient-centered approach
Over the past decade of practicing medicine, I have experienced this transformation personally. In residency, I believed that people had to be ready for help, to stop using, to change. I failed to recognize that many of those same people were asking me for help, and I wasn’t offering what they needed. The person who had to change was me.
As I moved toward a patient-centered approach, lowering barriers to starting and remaining in treatment, and collaborating with teams that could meet people wherever they might be, addictions became the most rewarding part of my practice.
I have never had more people thank me spontaneously and deeply for the care I provide. Plus, I have never seen a more profound change in the students I work with than when they witness someone with a substance use disorder offered treatment that works.
The X-waiver was not the only barrier to care, and the overdose crisis is not slowing down. But maybe with a new tool widely accessible, more of us will be ready to help.
Dr. Poorman is board certified in internal medicine and addiction medicine, assistant professor of medicine, University of Illinois at Chicago, and provides primary care and addiction services in Chicago. Her views do not necessarily reflect the views of her employer. She has reported no relevant disclosures, and she serves on the editorial advisory board of Internal Medicine News.
In 2016, when Erin Schanning lost her brother Ethan to an overdose, she wanted to know what could have been done to have helped him. Ethan, who had struggled with opioids since getting a prescription for the drugs after a dental procedure in middle school, had tried dozens of treatments. But at the age of 30, he was gone.
“After my brother died, I started researching and was surprised to learn that there were many evidence-based ways to treat substance use disorder that he hadn’t had access to, even though he had doggedly pursued treatment,” Ms. Schanning told me in an interview. One of those treatments, buprenorphine, is one of the most effective tools that health care providers have to treat opioid use disorder. A partial opioid agonist, it reduces cravings and prevents overdose, decreasing mortality more effectively than almost any medication for any disease. Yet most providers have never prescribed it.
That may be about to change. The special license to prescribe the medication, commonly known as the “X-waiver,” was officially eliminated as part of the passage of the Mainstreaming Addiction Treatment (MAT) Act. Immediately, following the passage of the Act, any provider with a DEA license became eligible to prescribe buprenorphine to treat opioid use disorder, and limits on the number of patients they could treat were eliminated.
Previously, buprenorphine, which has a better safety profile than almost any other prescription opioid because of its ceiling effect on respiratory depression,nonetheless required providers to obtain a special license to prescribe it, and – prior to an executive order from the Biden administration – 8 to 24 hours of training to do so. This led to a misconception that buprenorphine was dangerous, and created barriers for treatment during the worst overdose crisis in our country’s history. More than 110,00 overdose deaths occurred in 2021, representing a 468% increase in the last 2 decades.
Along with the MAT Act, the Medication Access and Training Expansion Act was passed in the same spending bill, requiring all prescribers who obtain a DEA license to do 8 hours of training on the treatment of substance use disorders. According to the Act, addiction specialty societies will have a role in creating trainings. Medical schools and residencies will also be able to fulfill this requirement with a “comprehensive” curriculum that covers all approved medications for the treatment of substance use disorders.
The DEA has not yet confirmed what training will be accepted, according to the Chief Medical Officer of the Substance Abuse and Mental Health Services Administration, Neeraj Gandotra, MD, who spoke to me in an interview. However, it is required to do so by April 5, 2023. Dr. Gandotra also emphasized that state and local laws, as well as insurance requirements, remain in place, and may place other constraints on prescribing. According to the Act, this new rule will be in effect by June 2023.
As an addiction medicine specialist and longtime buprenorphine prescriber, I am excited about these changes but wary of lingering resistance among health care providers. Will providers who have chosen not to get an X-waiver now look for another reason to not treat patients with substance use disorders?
Ms. Schanning remains hopeful. “I’m incredibly optimistic that health care providers are going to learn about buprenorphine and prescribe it to patients, and that patients are going to start asking about this medication,” she told me. “Seven in 10 providers say that they do feel an obligation to treat their patients with [opioid use disorder], but the federal government has made it very difficult to do so.”
Now with the X-waiver gone, providers and patients may be able to push for a long overdue shift in how we treat and conceptualize substance use disorders, she noted.
“Health care providers need to recognize substance use disorder as a medical condition that deserves treatment, and to speak about it like a medical condition,” Ms. Schanning said, by, for instance, moving away from using words such as “abuse” and “clean” and, instead, talking about treatable substance use disorders that can improve with evidence-based care, such as buprenorphine and methadone. “We also need to share stories of success and hope with people,” she added. “Once you’ve seen how someone can be transformed by treatment, it’s really difficult to say that substance use disorder is a character flaw, or their fault.”
A patient-centered approach
Over the past decade of practicing medicine, I have experienced this transformation personally. In residency, I believed that people had to be ready for help, to stop using, to change. I failed to recognize that many of those same people were asking me for help, and I wasn’t offering what they needed. The person who had to change was me.
As I moved toward a patient-centered approach, lowering barriers to starting and remaining in treatment, and collaborating with teams that could meet people wherever they might be, addictions became the most rewarding part of my practice.
I have never had more people thank me spontaneously and deeply for the care I provide. Plus, I have never seen a more profound change in the students I work with than when they witness someone with a substance use disorder offered treatment that works.
The X-waiver was not the only barrier to care, and the overdose crisis is not slowing down. But maybe with a new tool widely accessible, more of us will be ready to help.
Dr. Poorman is board certified in internal medicine and addiction medicine, assistant professor of medicine, University of Illinois at Chicago, and provides primary care and addiction services in Chicago. Her views do not necessarily reflect the views of her employer. She has reported no relevant disclosures, and she serves on the editorial advisory board of Internal Medicine News.
Unexpected link between light drinking and dementia risk
new research suggests.
Investigators assessed dementia risk using changes in alcohol consumption over a 2-year period in nearly 4 million people in South Korea. After about 7 years, dementia was 21% less likely in mild drinkers and 17% less likely in moderate drinkers. Heavy drinking was linked to an 8% increased risk.
Other studies of the relationship between alcohol and dementia have yielded mixed results, and this study does little to clear those murky waters. Nor do the results mean that drinking is recommended, the investigators note.
But the study does offer new information on how risk changes over time as people change their drinking habits, lead investigator Keun Hye Jeon, MD, assistant professor of family medicine at Cha Gumi Medical Center at Cha University, Gumi, South Korea, told this news organization.
“Although numerous studies have shown a relationship between alcohol consumption and dementia, there is a paucity of understanding as to how the incidence of dementia changes with changes in drinking habits,” Dr. Jeon said.
“By measuring alcohol consumption at two time points, we were able to study the relationship between reducing, ceasing, maintaining, and increasing alcohol consumption and incident dementia,” he added.
The findings were published online in JAMA Network Open.
Tracking drinking habits
Researchers analyzed data from nearly 4 million individuals aged 40 years and older in the Korean National Health Insurance Service who completed questionnaires and underwent physical exams in 2009 and 2011.
Study participants completed questionnaires on their drinking habits and were assigned to one of five groups according to change in alcohol consumption during the study period. These groups consisted of sustained nondrinkers; those who stopped drinking (quitters); those who reduced their consumption of alcohol but did not stop drinking (reducers); those who maintained the same level of consumption (sustainers); and those who increased their level of consumption (increasers).
A standard drink in the United States contains 14 g of alcohol. For this study, mild drinking was defined as less than 15 g/day, or one drink; moderate consumption as 15-29.9 g/day, or one to two drinks; and heavy drinking as 30 g/day or more, or three or more drinks.
At baseline, 54.8% of participants were nondrinkers, 26.7% were mild drinkers, 11.0% were moderate drinkers, and 7.5% were heavy drinkers.
From 2009 to 2011, 24.2% of mild drinkers, 8.4% of moderate drinkers, and 7.6% of heavy drinkers became quitters. In the same period, 13.9% of nondrinkers, 16.1% of mild drinkers, and 17.4% of moderate drinkers increased their drinking level.
After a mean follow-up of 6.3 years, 2.5% of participants were diagnosed with dementia, 2.0% with Alzheimer’s disease, and 0.3% with vascular dementia.
Unexpected finding
Compared with consistently not drinking, mild and moderate alcohol consumption was associated with a 21% (adjust hazard ratio, 0.79; 95% confidence interval, 0.77-0.81) and 17% (aHR, 0.83; 95% CI, 0.79-0.88) decreased risk for dementia, respectively.
Heavy drinking was linked to an 8% increased risk (aHR, 1.08; 95% CI, 1.03-1.12).
Similar associations were found between alcohol consumption and risk for Alzheimer’s disease and vascular dementia.
Reducing drinking habits from heavy to moderate led to a reduction in risk for dementia and Alzheimer’s, and increasing drinking levels led to an increase in risk for both conditions.
But when the researchers analyzed dementia risk for nondrinkers who began drinking at mild levels during the study period, they found something unexpected – the risk in this group decreased by 7% for dementia (aHR, 0.93; 95% CI, 0.90-0.96) and by 8% for Alzheimer’s (aHR, 0.92; 95% CI, 0.89-0.95), compared with sustained mild drinkers.
“Our study showed that initiation of mild alcohol consumption leads to a reduced risk of all-cause dementia and Alzheimer’s disease, which has never been reported in previous studies,” Dr. Jeon said.
However, Dr. Jeon was quick to point out that this doesn’t mean that people who don’t drink should start.
Previous studies have shown that heavy alcohol use can triple an individual’s dementia risk, while other studies have shown that no amount of alcohol consumption is good for the brain.
“None of the existing health guidelines recommend starting alcohol drinking,” Dr. Jeon said. “Our findings regarding an initiation of mild alcohol consumption cannot be directly translated into clinical recommendations,” but the findings do warrant additional study, he added.
Risks persist
Commenting on the findings, Percy Griffin, PhD, director of scientific engagement for the Alzheimer’s Association in Chicago, agrees.
“While this study is interesting, and this topic deserves further study, no one should drink alcohol as a method of reducing risk of Alzheimer’s disease or other dementia based on this study,” said Dr. Griffin, who was not part of the study.
The exact tipping point in alcohol consumption that can lead to problems with cognition or increased dementia risk is unknown, Dr. Griffin said. Nor do researchers understand why mild drinking may have a protective effect.
“We do know, however, that excessive alcohol consumption has negative effects on heart health and general health, which can lead to problems with brain function,” he said. “Clinicians should have discussions with their patients around their alcohol consumption patterns and the risks associated with drinking in excess, including potential damage to their cognition.”
Funding for the study was not disclosed. Dr. Jeon and Dr. Griffin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators assessed dementia risk using changes in alcohol consumption over a 2-year period in nearly 4 million people in South Korea. After about 7 years, dementia was 21% less likely in mild drinkers and 17% less likely in moderate drinkers. Heavy drinking was linked to an 8% increased risk.
Other studies of the relationship between alcohol and dementia have yielded mixed results, and this study does little to clear those murky waters. Nor do the results mean that drinking is recommended, the investigators note.
But the study does offer new information on how risk changes over time as people change their drinking habits, lead investigator Keun Hye Jeon, MD, assistant professor of family medicine at Cha Gumi Medical Center at Cha University, Gumi, South Korea, told this news organization.
“Although numerous studies have shown a relationship between alcohol consumption and dementia, there is a paucity of understanding as to how the incidence of dementia changes with changes in drinking habits,” Dr. Jeon said.
“By measuring alcohol consumption at two time points, we were able to study the relationship between reducing, ceasing, maintaining, and increasing alcohol consumption and incident dementia,” he added.
The findings were published online in JAMA Network Open.
Tracking drinking habits
Researchers analyzed data from nearly 4 million individuals aged 40 years and older in the Korean National Health Insurance Service who completed questionnaires and underwent physical exams in 2009 and 2011.
Study participants completed questionnaires on their drinking habits and were assigned to one of five groups according to change in alcohol consumption during the study period. These groups consisted of sustained nondrinkers; those who stopped drinking (quitters); those who reduced their consumption of alcohol but did not stop drinking (reducers); those who maintained the same level of consumption (sustainers); and those who increased their level of consumption (increasers).
A standard drink in the United States contains 14 g of alcohol. For this study, mild drinking was defined as less than 15 g/day, or one drink; moderate consumption as 15-29.9 g/day, or one to two drinks; and heavy drinking as 30 g/day or more, or three or more drinks.
At baseline, 54.8% of participants were nondrinkers, 26.7% were mild drinkers, 11.0% were moderate drinkers, and 7.5% were heavy drinkers.
From 2009 to 2011, 24.2% of mild drinkers, 8.4% of moderate drinkers, and 7.6% of heavy drinkers became quitters. In the same period, 13.9% of nondrinkers, 16.1% of mild drinkers, and 17.4% of moderate drinkers increased their drinking level.
After a mean follow-up of 6.3 years, 2.5% of participants were diagnosed with dementia, 2.0% with Alzheimer’s disease, and 0.3% with vascular dementia.
Unexpected finding
Compared with consistently not drinking, mild and moderate alcohol consumption was associated with a 21% (adjust hazard ratio, 0.79; 95% confidence interval, 0.77-0.81) and 17% (aHR, 0.83; 95% CI, 0.79-0.88) decreased risk for dementia, respectively.
Heavy drinking was linked to an 8% increased risk (aHR, 1.08; 95% CI, 1.03-1.12).
Similar associations were found between alcohol consumption and risk for Alzheimer’s disease and vascular dementia.
Reducing drinking habits from heavy to moderate led to a reduction in risk for dementia and Alzheimer’s, and increasing drinking levels led to an increase in risk for both conditions.
But when the researchers analyzed dementia risk for nondrinkers who began drinking at mild levels during the study period, they found something unexpected – the risk in this group decreased by 7% for dementia (aHR, 0.93; 95% CI, 0.90-0.96) and by 8% for Alzheimer’s (aHR, 0.92; 95% CI, 0.89-0.95), compared with sustained mild drinkers.
“Our study showed that initiation of mild alcohol consumption leads to a reduced risk of all-cause dementia and Alzheimer’s disease, which has never been reported in previous studies,” Dr. Jeon said.
However, Dr. Jeon was quick to point out that this doesn’t mean that people who don’t drink should start.
Previous studies have shown that heavy alcohol use can triple an individual’s dementia risk, while other studies have shown that no amount of alcohol consumption is good for the brain.
“None of the existing health guidelines recommend starting alcohol drinking,” Dr. Jeon said. “Our findings regarding an initiation of mild alcohol consumption cannot be directly translated into clinical recommendations,” but the findings do warrant additional study, he added.
Risks persist
Commenting on the findings, Percy Griffin, PhD, director of scientific engagement for the Alzheimer’s Association in Chicago, agrees.
“While this study is interesting, and this topic deserves further study, no one should drink alcohol as a method of reducing risk of Alzheimer’s disease or other dementia based on this study,” said Dr. Griffin, who was not part of the study.
The exact tipping point in alcohol consumption that can lead to problems with cognition or increased dementia risk is unknown, Dr. Griffin said. Nor do researchers understand why mild drinking may have a protective effect.
“We do know, however, that excessive alcohol consumption has negative effects on heart health and general health, which can lead to problems with brain function,” he said. “Clinicians should have discussions with their patients around their alcohol consumption patterns and the risks associated with drinking in excess, including potential damage to their cognition.”
Funding for the study was not disclosed. Dr. Jeon and Dr. Griffin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators assessed dementia risk using changes in alcohol consumption over a 2-year period in nearly 4 million people in South Korea. After about 7 years, dementia was 21% less likely in mild drinkers and 17% less likely in moderate drinkers. Heavy drinking was linked to an 8% increased risk.
Other studies of the relationship between alcohol and dementia have yielded mixed results, and this study does little to clear those murky waters. Nor do the results mean that drinking is recommended, the investigators note.
But the study does offer new information on how risk changes over time as people change their drinking habits, lead investigator Keun Hye Jeon, MD, assistant professor of family medicine at Cha Gumi Medical Center at Cha University, Gumi, South Korea, told this news organization.
“Although numerous studies have shown a relationship between alcohol consumption and dementia, there is a paucity of understanding as to how the incidence of dementia changes with changes in drinking habits,” Dr. Jeon said.
“By measuring alcohol consumption at two time points, we were able to study the relationship between reducing, ceasing, maintaining, and increasing alcohol consumption and incident dementia,” he added.
The findings were published online in JAMA Network Open.
Tracking drinking habits
Researchers analyzed data from nearly 4 million individuals aged 40 years and older in the Korean National Health Insurance Service who completed questionnaires and underwent physical exams in 2009 and 2011.
Study participants completed questionnaires on their drinking habits and were assigned to one of five groups according to change in alcohol consumption during the study period. These groups consisted of sustained nondrinkers; those who stopped drinking (quitters); those who reduced their consumption of alcohol but did not stop drinking (reducers); those who maintained the same level of consumption (sustainers); and those who increased their level of consumption (increasers).
A standard drink in the United States contains 14 g of alcohol. For this study, mild drinking was defined as less than 15 g/day, or one drink; moderate consumption as 15-29.9 g/day, or one to two drinks; and heavy drinking as 30 g/day or more, or three or more drinks.
At baseline, 54.8% of participants were nondrinkers, 26.7% were mild drinkers, 11.0% were moderate drinkers, and 7.5% were heavy drinkers.
From 2009 to 2011, 24.2% of mild drinkers, 8.4% of moderate drinkers, and 7.6% of heavy drinkers became quitters. In the same period, 13.9% of nondrinkers, 16.1% of mild drinkers, and 17.4% of moderate drinkers increased their drinking level.
After a mean follow-up of 6.3 years, 2.5% of participants were diagnosed with dementia, 2.0% with Alzheimer’s disease, and 0.3% with vascular dementia.
Unexpected finding
Compared with consistently not drinking, mild and moderate alcohol consumption was associated with a 21% (adjust hazard ratio, 0.79; 95% confidence interval, 0.77-0.81) and 17% (aHR, 0.83; 95% CI, 0.79-0.88) decreased risk for dementia, respectively.
Heavy drinking was linked to an 8% increased risk (aHR, 1.08; 95% CI, 1.03-1.12).
Similar associations were found between alcohol consumption and risk for Alzheimer’s disease and vascular dementia.
Reducing drinking habits from heavy to moderate led to a reduction in risk for dementia and Alzheimer’s, and increasing drinking levels led to an increase in risk for both conditions.
But when the researchers analyzed dementia risk for nondrinkers who began drinking at mild levels during the study period, they found something unexpected – the risk in this group decreased by 7% for dementia (aHR, 0.93; 95% CI, 0.90-0.96) and by 8% for Alzheimer’s (aHR, 0.92; 95% CI, 0.89-0.95), compared with sustained mild drinkers.
“Our study showed that initiation of mild alcohol consumption leads to a reduced risk of all-cause dementia and Alzheimer’s disease, which has never been reported in previous studies,” Dr. Jeon said.
However, Dr. Jeon was quick to point out that this doesn’t mean that people who don’t drink should start.
Previous studies have shown that heavy alcohol use can triple an individual’s dementia risk, while other studies have shown that no amount of alcohol consumption is good for the brain.
“None of the existing health guidelines recommend starting alcohol drinking,” Dr. Jeon said. “Our findings regarding an initiation of mild alcohol consumption cannot be directly translated into clinical recommendations,” but the findings do warrant additional study, he added.
Risks persist
Commenting on the findings, Percy Griffin, PhD, director of scientific engagement for the Alzheimer’s Association in Chicago, agrees.
“While this study is interesting, and this topic deserves further study, no one should drink alcohol as a method of reducing risk of Alzheimer’s disease or other dementia based on this study,” said Dr. Griffin, who was not part of the study.
The exact tipping point in alcohol consumption that can lead to problems with cognition or increased dementia risk is unknown, Dr. Griffin said. Nor do researchers understand why mild drinking may have a protective effect.
“We do know, however, that excessive alcohol consumption has negative effects on heart health and general health, which can lead to problems with brain function,” he said. “Clinicians should have discussions with their patients around their alcohol consumption patterns and the risks associated with drinking in excess, including potential damage to their cognition.”
Funding for the study was not disclosed. Dr. Jeon and Dr. Griffin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Finding catatonia requires knowing what to look for
Catatonia is a psychomotor syndrome identified by its clinical phenotype. Unlike common psychiatric syndromes such as major depression that are characterized by self-report of symptoms, catatonia is identified chiefly by empirically evaluated signs on clinical evaluation. Its signs are recognized through observation, physical examination, or elicitation by clinical maneuvers or the presentation of stimuli. However, catatonia is often overlooked even though its clinical signs are often visibly apparent, including to the casual observer.
Why is catatonia underdiagnosed? A key modifiable factor appears to be a prevalent misunderstanding over what catatonia looks like.1 We have sought to address this in a few ways.
First identified was the need for comprehensive educational resources on how to assess for and recognize catatonia. Using the Bush-Francis Catatonia Rating Scale – the most widely used scale for catatonia in both research and clinical settings and the most cited publication in the catatonia literature– our team developed the BFCRS Training Manual and Coding Guide.2,3 This manual expands on the definitions of each BFCRS item based on how it was originally operationalized by the scale’s authors. Subsequently, we created a comprehensive set of educational resources including videos illustrating how to assess for catatonia, a video for each of the 23 items on the BFCRS, and self-assessment tools. All resources are freely available online at https://bfcrs.urmc.edu.4
Through this project it became apparent that there are many discrepancies across the field regarding the phenotype of catatonia. Specifically, a recent review inspired by this project set about to characterize the scope of distinctions across diagnostic systems and rating scales.5 For instance, each diagnostic system and rating scale includes a unique set of signs, approaches diagnostic thresholds differently, and often operationalizes clinical features in ways that lead either to criterion overlap (for example, combativeness would be scored both as combativeness and agitation on ICD-11) or contradictions with other systems or scales (for example, varied definitions of waxy flexibility). In the face of so many inconsistencies, what is a clinician to do? What follows is a discussion of how to apply the insights from this recent review in clinical and research settings.
Starting with DSM-5-TR and ICD-11 – the current editions of the two leading diagnostic systems – one might ask: How do they compare?6,7 Overall, these two systems are broadly aligned in terms of the catatonic syndrome. Both systems identify individual clinical signs (as opposed to symptom complexes). Both require three features as a diagnostic threshold. Most of the same clinical signs are included in both systems, and the definitions of individual items are largely equivalent. Additionally, both systems allow for diagnosis of catatonia in association with psychiatric and medical conditions and include a category for unspecified catatonia.
Despite these core agreements, though, there are several important distinctions. First, whereas all 12 signs included in DSM-5-TR count toward an ICD-11 catatonia diagnosis, the opposite cannot be said. ICD-11 includes several features that are not in DSM-5-TR: rigidity, verbigeration, withdrawal, staring, ambitendency, impulsivity, and combativeness. Next, autonomic abnormality, which signifies the most severe type of catatonia called malignant catatonia, is included as a potential comorbidity in ICD-11 but not mentioned in DSM-5-TR. Third, ICD-11 includes a separate diagnosis for substance-induced catatonia, whereas this condition would be diagnosed as unspecified catatonia in DSM-5-TR.
There are also elements missing from both systems. The most notable of these is that neither system specifies the period over which findings must be present for diagnosis. By clinical convention, the practical definition of 24 hours is appropriate in most instances. The clinical features identified during direct evaluation are usually sufficient for diagnosis, but additional signs observed or documented over the prior 24 hours should be incorporated as part of the clinical evaluation. Another distinction is how to handle clinical features before and after lorazepam challenge. As noted in the BFCRS Training Manual, it would be appropriate to compare “state assessments” (that is, restricted to features identified only during direct, in-person assessment) from before and after lorazepam administration to document improvement.4
Whereas DSM-5-TR and ICD-11 are broadly in agreement, comparing these systems with catatonia rating scales reveals many sources of potential confusion, but also concrete guidance on operationalizing individual items.5 How exactly should each of catatonia’s clinical signs be defined? Descriptions differ, and thresholds of duration and frequency vary considerably across scales. As a result, clinicians who use different scales and then convert these results to diagnostic criteria are liable to come to different clinical conclusions. For instance, both echophenomena and negativism must be elicited more than five times to be scored per Northoff,8 but even a single convincing instance of either would be scored on the BFCRS as “occasional.”2
Such discrepancies are important because, whereas the psychometric properties of several catatonia scales have been documented, there are no analogous studies on the DSM-5-TR and ICD-11 criteria. Therefore, it is essential for clinicians and researchers to document how diagnostic criteria have been operationalized. The most practical and evidence-based way to do this is to use a clinically validated scale and convert these to diagnostic criteria, yet in doing so a few modifications will be necessary.
Of the available clinical scales, the BFCRS is best positioned for clinical use. The BFCRS has been validated clinically and has good reliability, detailed item definitions and audiovisual examples available. In addition, it is the only scale with a published semistructured evaluation (see initial paper and Training Manual), which takes about 5 minutes.2,4 In terms of utility, all 12 signs included by DSM-5-TR are among the first 14 items on the BFCRS, which constitutes a standalone tool known as the Bush-Francis Catatonia Screening Instrument (BFCSI, see Table).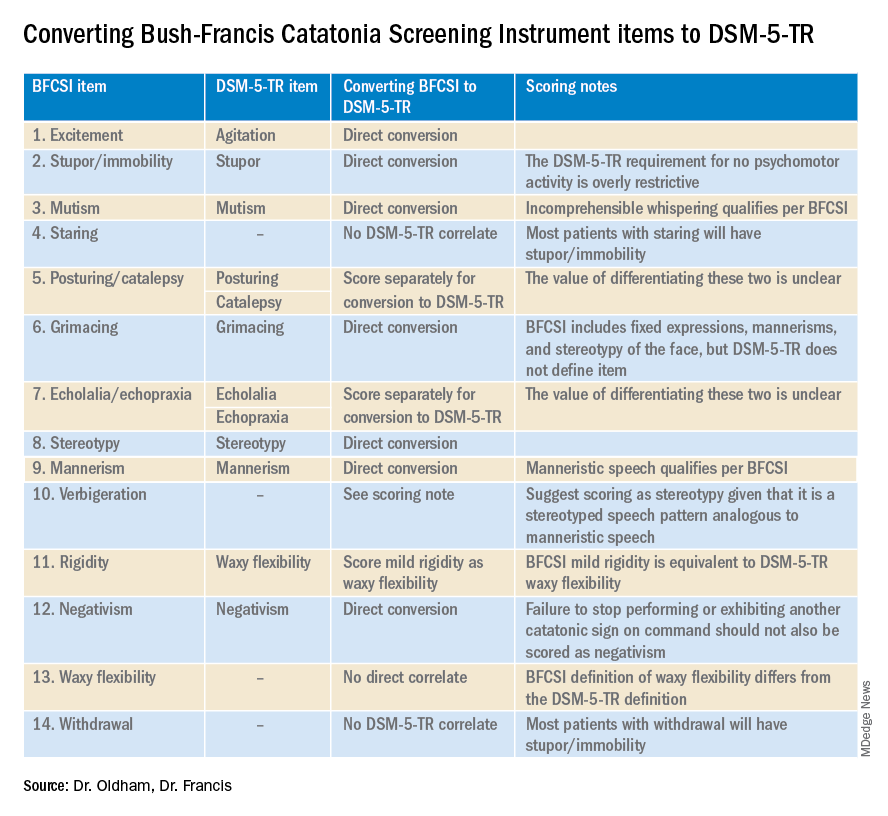
Many fundamental questions remain about catatonia,but the importance of a shared understanding of its clinical features is clear.9 Catatonia should be on the differential whenever a patient exhibits a markedly altered level of activity or grossly abnormal behavior, especially when inappropriate to context. We encourage readers to familiarize themselves with the phenotype of catatonia through online educational resources4 because the optimal care of patients with catatonia requires – at a minimum – that we know what we’re looking for.
Dr. Oldham is assistant professor of psychiatry at the University of Rochester (N.Y.) Medical Center. Dr. Francis is professor of psychiatry at Penn State University, Hershey. The authors declare no relevant conflicts of interest. Funding for the educational project hosted at https://bfcrs.urmc.edu was provided by the department of psychiatry at the University of Rochester Medical Center. Dr. Oldham is currently supported by a K23 career development award from the National Institute on Aging (AG072383). The educational resources referenced in this piece could not have been created were it not for the intellectual and thespian collaboration of Joshua R. Wortzel, MD, who is currently a fellow in child and adolescent psychiatry at Brown University, Providence, R.I. The authors are also indebted to Hochang B. Lee, MD, for his gracious support of this project.
References
1. Wortzel JR et al. J Clin Psychiatry. 2021 Aug 17;82(5):21m14025. doi: 10.4088/JCP.21m14025.
2. Bush G et al. Acta Psychiatr Scand. 1996 Feb;93(2):129-36. doi: 10.1111/j.1600-0447.1996.tb09814.x.
3. Weleff J et al. J Acad Consult Liaison Psychiatry. 2023 Jan-Feb;64(1):13-27. doi:10.1016/j.jaclp.2022.07.002.
4. Oldham MA et al. Bush-Francis Catatonia Rating Scale Assessment Resources. University of Rochester Medical Center, Department of Psychiatry. https://bfcrs.urmc.edu.
5. Oldham MA. Schizophr Res. 2022 Aug 19;S0920-9964(22)00294-8. doi: 10.1016/j.schres.2022.08.002.
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. Washington, D.C.: American Psychiatric Association Publishing, 2022.
7. World Health Organization. ICD-11 for Mortality and Morbidity Stastistics. 2022. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/486722075.
8. Northoff G et al. Mov Disord. May 1999;14(3):404-16. doi: 10.1002/1531-8257(199905)14:3<404::AID-MDS1004>3.0.CO;2-5.
9. Walther S et al. The Lancet Psychiatry. 2019 Jul;6(7):610-9. doi: 10.1016/S2215-0366(18)30474-7.
Catatonia is a psychomotor syndrome identified by its clinical phenotype. Unlike common psychiatric syndromes such as major depression that are characterized by self-report of symptoms, catatonia is identified chiefly by empirically evaluated signs on clinical evaluation. Its signs are recognized through observation, physical examination, or elicitation by clinical maneuvers or the presentation of stimuli. However, catatonia is often overlooked even though its clinical signs are often visibly apparent, including to the casual observer.
Why is catatonia underdiagnosed? A key modifiable factor appears to be a prevalent misunderstanding over what catatonia looks like.1 We have sought to address this in a few ways.
First identified was the need for comprehensive educational resources on how to assess for and recognize catatonia. Using the Bush-Francis Catatonia Rating Scale – the most widely used scale for catatonia in both research and clinical settings and the most cited publication in the catatonia literature– our team developed the BFCRS Training Manual and Coding Guide.2,3 This manual expands on the definitions of each BFCRS item based on how it was originally operationalized by the scale’s authors. Subsequently, we created a comprehensive set of educational resources including videos illustrating how to assess for catatonia, a video for each of the 23 items on the BFCRS, and self-assessment tools. All resources are freely available online at https://bfcrs.urmc.edu.4
Through this project it became apparent that there are many discrepancies across the field regarding the phenotype of catatonia. Specifically, a recent review inspired by this project set about to characterize the scope of distinctions across diagnostic systems and rating scales.5 For instance, each diagnostic system and rating scale includes a unique set of signs, approaches diagnostic thresholds differently, and often operationalizes clinical features in ways that lead either to criterion overlap (for example, combativeness would be scored both as combativeness and agitation on ICD-11) or contradictions with other systems or scales (for example, varied definitions of waxy flexibility). In the face of so many inconsistencies, what is a clinician to do? What follows is a discussion of how to apply the insights from this recent review in clinical and research settings.
Starting with DSM-5-TR and ICD-11 – the current editions of the two leading diagnostic systems – one might ask: How do they compare?6,7 Overall, these two systems are broadly aligned in terms of the catatonic syndrome. Both systems identify individual clinical signs (as opposed to symptom complexes). Both require three features as a diagnostic threshold. Most of the same clinical signs are included in both systems, and the definitions of individual items are largely equivalent. Additionally, both systems allow for diagnosis of catatonia in association with psychiatric and medical conditions and include a category for unspecified catatonia.
Despite these core agreements, though, there are several important distinctions. First, whereas all 12 signs included in DSM-5-TR count toward an ICD-11 catatonia diagnosis, the opposite cannot be said. ICD-11 includes several features that are not in DSM-5-TR: rigidity, verbigeration, withdrawal, staring, ambitendency, impulsivity, and combativeness. Next, autonomic abnormality, which signifies the most severe type of catatonia called malignant catatonia, is included as a potential comorbidity in ICD-11 but not mentioned in DSM-5-TR. Third, ICD-11 includes a separate diagnosis for substance-induced catatonia, whereas this condition would be diagnosed as unspecified catatonia in DSM-5-TR.
There are also elements missing from both systems. The most notable of these is that neither system specifies the period over which findings must be present for diagnosis. By clinical convention, the practical definition of 24 hours is appropriate in most instances. The clinical features identified during direct evaluation are usually sufficient for diagnosis, but additional signs observed or documented over the prior 24 hours should be incorporated as part of the clinical evaluation. Another distinction is how to handle clinical features before and after lorazepam challenge. As noted in the BFCRS Training Manual, it would be appropriate to compare “state assessments” (that is, restricted to features identified only during direct, in-person assessment) from before and after lorazepam administration to document improvement.4
Whereas DSM-5-TR and ICD-11 are broadly in agreement, comparing these systems with catatonia rating scales reveals many sources of potential confusion, but also concrete guidance on operationalizing individual items.5 How exactly should each of catatonia’s clinical signs be defined? Descriptions differ, and thresholds of duration and frequency vary considerably across scales. As a result, clinicians who use different scales and then convert these results to diagnostic criteria are liable to come to different clinical conclusions. For instance, both echophenomena and negativism must be elicited more than five times to be scored per Northoff,8 but even a single convincing instance of either would be scored on the BFCRS as “occasional.”2
Such discrepancies are important because, whereas the psychometric properties of several catatonia scales have been documented, there are no analogous studies on the DSM-5-TR and ICD-11 criteria. Therefore, it is essential for clinicians and researchers to document how diagnostic criteria have been operationalized. The most practical and evidence-based way to do this is to use a clinically validated scale and convert these to diagnostic criteria, yet in doing so a few modifications will be necessary.
Of the available clinical scales, the BFCRS is best positioned for clinical use. The BFCRS has been validated clinically and has good reliability, detailed item definitions and audiovisual examples available. In addition, it is the only scale with a published semistructured evaluation (see initial paper and Training Manual), which takes about 5 minutes.2,4 In terms of utility, all 12 signs included by DSM-5-TR are among the first 14 items on the BFCRS, which constitutes a standalone tool known as the Bush-Francis Catatonia Screening Instrument (BFCSI, see Table).
Many fundamental questions remain about catatonia,but the importance of a shared understanding of its clinical features is clear.9 Catatonia should be on the differential whenever a patient exhibits a markedly altered level of activity or grossly abnormal behavior, especially when inappropriate to context. We encourage readers to familiarize themselves with the phenotype of catatonia through online educational resources4 because the optimal care of patients with catatonia requires – at a minimum – that we know what we’re looking for.
Dr. Oldham is assistant professor of psychiatry at the University of Rochester (N.Y.) Medical Center. Dr. Francis is professor of psychiatry at Penn State University, Hershey. The authors declare no relevant conflicts of interest. Funding for the educational project hosted at https://bfcrs.urmc.edu was provided by the department of psychiatry at the University of Rochester Medical Center. Dr. Oldham is currently supported by a K23 career development award from the National Institute on Aging (AG072383). The educational resources referenced in this piece could not have been created were it not for the intellectual and thespian collaboration of Joshua R. Wortzel, MD, who is currently a fellow in child and adolescent psychiatry at Brown University, Providence, R.I. The authors are also indebted to Hochang B. Lee, MD, for his gracious support of this project.
References
1. Wortzel JR et al. J Clin Psychiatry. 2021 Aug 17;82(5):21m14025. doi: 10.4088/JCP.21m14025.
2. Bush G et al. Acta Psychiatr Scand. 1996 Feb;93(2):129-36. doi: 10.1111/j.1600-0447.1996.tb09814.x.
3. Weleff J et al. J Acad Consult Liaison Psychiatry. 2023 Jan-Feb;64(1):13-27. doi:10.1016/j.jaclp.2022.07.002.
4. Oldham MA et al. Bush-Francis Catatonia Rating Scale Assessment Resources. University of Rochester Medical Center, Department of Psychiatry. https://bfcrs.urmc.edu.
5. Oldham MA. Schizophr Res. 2022 Aug 19;S0920-9964(22)00294-8. doi: 10.1016/j.schres.2022.08.002.
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. Washington, D.C.: American Psychiatric Association Publishing, 2022.
7. World Health Organization. ICD-11 for Mortality and Morbidity Stastistics. 2022. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/486722075.
8. Northoff G et al. Mov Disord. May 1999;14(3):404-16. doi: 10.1002/1531-8257(199905)14:3<404::AID-MDS1004>3.0.CO;2-5.
9. Walther S et al. The Lancet Psychiatry. 2019 Jul;6(7):610-9. doi: 10.1016/S2215-0366(18)30474-7.
Catatonia is a psychomotor syndrome identified by its clinical phenotype. Unlike common psychiatric syndromes such as major depression that are characterized by self-report of symptoms, catatonia is identified chiefly by empirically evaluated signs on clinical evaluation. Its signs are recognized through observation, physical examination, or elicitation by clinical maneuvers or the presentation of stimuli. However, catatonia is often overlooked even though its clinical signs are often visibly apparent, including to the casual observer.
Why is catatonia underdiagnosed? A key modifiable factor appears to be a prevalent misunderstanding over what catatonia looks like.1 We have sought to address this in a few ways.
First identified was the need for comprehensive educational resources on how to assess for and recognize catatonia. Using the Bush-Francis Catatonia Rating Scale – the most widely used scale for catatonia in both research and clinical settings and the most cited publication in the catatonia literature– our team developed the BFCRS Training Manual and Coding Guide.2,3 This manual expands on the definitions of each BFCRS item based on how it was originally operationalized by the scale’s authors. Subsequently, we created a comprehensive set of educational resources including videos illustrating how to assess for catatonia, a video for each of the 23 items on the BFCRS, and self-assessment tools. All resources are freely available online at https://bfcrs.urmc.edu.4
Through this project it became apparent that there are many discrepancies across the field regarding the phenotype of catatonia. Specifically, a recent review inspired by this project set about to characterize the scope of distinctions across diagnostic systems and rating scales.5 For instance, each diagnostic system and rating scale includes a unique set of signs, approaches diagnostic thresholds differently, and often operationalizes clinical features in ways that lead either to criterion overlap (for example, combativeness would be scored both as combativeness and agitation on ICD-11) or contradictions with other systems or scales (for example, varied definitions of waxy flexibility). In the face of so many inconsistencies, what is a clinician to do? What follows is a discussion of how to apply the insights from this recent review in clinical and research settings.
Starting with DSM-5-TR and ICD-11 – the current editions of the two leading diagnostic systems – one might ask: How do they compare?6,7 Overall, these two systems are broadly aligned in terms of the catatonic syndrome. Both systems identify individual clinical signs (as opposed to symptom complexes). Both require three features as a diagnostic threshold. Most of the same clinical signs are included in both systems, and the definitions of individual items are largely equivalent. Additionally, both systems allow for diagnosis of catatonia in association with psychiatric and medical conditions and include a category for unspecified catatonia.
Despite these core agreements, though, there are several important distinctions. First, whereas all 12 signs included in DSM-5-TR count toward an ICD-11 catatonia diagnosis, the opposite cannot be said. ICD-11 includes several features that are not in DSM-5-TR: rigidity, verbigeration, withdrawal, staring, ambitendency, impulsivity, and combativeness. Next, autonomic abnormality, which signifies the most severe type of catatonia called malignant catatonia, is included as a potential comorbidity in ICD-11 but not mentioned in DSM-5-TR. Third, ICD-11 includes a separate diagnosis for substance-induced catatonia, whereas this condition would be diagnosed as unspecified catatonia in DSM-5-TR.
There are also elements missing from both systems. The most notable of these is that neither system specifies the period over which findings must be present for diagnosis. By clinical convention, the practical definition of 24 hours is appropriate in most instances. The clinical features identified during direct evaluation are usually sufficient for diagnosis, but additional signs observed or documented over the prior 24 hours should be incorporated as part of the clinical evaluation. Another distinction is how to handle clinical features before and after lorazepam challenge. As noted in the BFCRS Training Manual, it would be appropriate to compare “state assessments” (that is, restricted to features identified only during direct, in-person assessment) from before and after lorazepam administration to document improvement.4
Whereas DSM-5-TR and ICD-11 are broadly in agreement, comparing these systems with catatonia rating scales reveals many sources of potential confusion, but also concrete guidance on operationalizing individual items.5 How exactly should each of catatonia’s clinical signs be defined? Descriptions differ, and thresholds of duration and frequency vary considerably across scales. As a result, clinicians who use different scales and then convert these results to diagnostic criteria are liable to come to different clinical conclusions. For instance, both echophenomena and negativism must be elicited more than five times to be scored per Northoff,8 but even a single convincing instance of either would be scored on the BFCRS as “occasional.”2
Such discrepancies are important because, whereas the psychometric properties of several catatonia scales have been documented, there are no analogous studies on the DSM-5-TR and ICD-11 criteria. Therefore, it is essential for clinicians and researchers to document how diagnostic criteria have been operationalized. The most practical and evidence-based way to do this is to use a clinically validated scale and convert these to diagnostic criteria, yet in doing so a few modifications will be necessary.
Of the available clinical scales, the BFCRS is best positioned for clinical use. The BFCRS has been validated clinically and has good reliability, detailed item definitions and audiovisual examples available. In addition, it is the only scale with a published semistructured evaluation (see initial paper and Training Manual), which takes about 5 minutes.2,4 In terms of utility, all 12 signs included by DSM-5-TR are among the first 14 items on the BFCRS, which constitutes a standalone tool known as the Bush-Francis Catatonia Screening Instrument (BFCSI, see Table).
Many fundamental questions remain about catatonia,but the importance of a shared understanding of its clinical features is clear.9 Catatonia should be on the differential whenever a patient exhibits a markedly altered level of activity or grossly abnormal behavior, especially when inappropriate to context. We encourage readers to familiarize themselves with the phenotype of catatonia through online educational resources4 because the optimal care of patients with catatonia requires – at a minimum – that we know what we’re looking for.
Dr. Oldham is assistant professor of psychiatry at the University of Rochester (N.Y.) Medical Center. Dr. Francis is professor of psychiatry at Penn State University, Hershey. The authors declare no relevant conflicts of interest. Funding for the educational project hosted at https://bfcrs.urmc.edu was provided by the department of psychiatry at the University of Rochester Medical Center. Dr. Oldham is currently supported by a K23 career development award from the National Institute on Aging (AG072383). The educational resources referenced in this piece could not have been created were it not for the intellectual and thespian collaboration of Joshua R. Wortzel, MD, who is currently a fellow in child and adolescent psychiatry at Brown University, Providence, R.I. The authors are also indebted to Hochang B. Lee, MD, for his gracious support of this project.
References
1. Wortzel JR et al. J Clin Psychiatry. 2021 Aug 17;82(5):21m14025. doi: 10.4088/JCP.21m14025.
2. Bush G et al. Acta Psychiatr Scand. 1996 Feb;93(2):129-36. doi: 10.1111/j.1600-0447.1996.tb09814.x.
3. Weleff J et al. J Acad Consult Liaison Psychiatry. 2023 Jan-Feb;64(1):13-27. doi:10.1016/j.jaclp.2022.07.002.
4. Oldham MA et al. Bush-Francis Catatonia Rating Scale Assessment Resources. University of Rochester Medical Center, Department of Psychiatry. https://bfcrs.urmc.edu.
5. Oldham MA. Schizophr Res. 2022 Aug 19;S0920-9964(22)00294-8. doi: 10.1016/j.schres.2022.08.002.
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. Washington, D.C.: American Psychiatric Association Publishing, 2022.
7. World Health Organization. ICD-11 for Mortality and Morbidity Stastistics. 2022. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/486722075.
8. Northoff G et al. Mov Disord. May 1999;14(3):404-16. doi: 10.1002/1531-8257(199905)14:3<404::AID-MDS1004>3.0.CO;2-5.
9. Walther S et al. The Lancet Psychiatry. 2019 Jul;6(7):610-9. doi: 10.1016/S2215-0366(18)30474-7.
Nature, not nurture, the culprit in OCD
new research suggests.
This finding from a large, register-based study is particularly surprising because results from previous studies of major depression and anxiety disorder have shown a significant effect of parenting and a child’s home environment on the risk for these disorders, the investigators noted.
While the results likely won’t change patient treatment, one expert said it could alleviate concerns of some parents with OCD who fear that witnessing their obsessive behaviors might put their children at higher risk for the disorder.
“The evidence is consistent with the idea that the psychological transmission of OCD from parent to child, if it exists, is really pretty weak,” lead author Kenneth S. Kendler, MD, professor of psychiatry and director of the Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University, Richmond, said in an interview.
The findings were published online in JAMA Psychiatry.
Family analysis
The study is the first to include adoptive parents in an analysis of OCD transmission, which allowed investigators to answer the nature versus nurture question that is often difficult to decipher.
Working with Swedish population registries, researchers identified more than 2.4 million offspring. Of these, 27,141 individuals (1.1%) had a lifetime diagnosis of OCD.
Families were divided into four types: intact families, with kids who lived at home with their biological parents from birth to at least age 15 years; families with kids who never lived with their biological father; families with children who did not live with their biological fathers between birth and age 15 years but who lived with a stepfather for at least 10 of those years; and families with children who were adopted before the age of 5 by people with no biological connection to the child.
After analyzing data from all parent-child relationships, researchers found that genes plus rearing (odds ratio, 3.94; 95% confidence interval, 3.58-4.33) and genes only (OR, 3.34; 95% CI, 2.27-4.93) were significantly more likely to be correlated to transmission of OCD from parent to offspring than rearing alone. Rearing only (OR, 1.4; 95% CI, 0.45-4.39) was not significantly correlated with OCD transmission
“It appears from our data that the only substantial transmission that occurs is in the genes parents transmit, not by the modeling of behavior,” Dr. Kendler said.
“There’s an idea that you can learn some things from your parents from psychopathology, but we didn’t see that kids picked that up much in the case of OCD,” he added.
However, there was one outlier: Children raised by stepparents or adoptive parents with an anxiety disorder had a greater risk of developing OCD.
Given the lack of evidence of a strong rearing effect in other analyses, Dr. Kendler noted that this rogue finding could be caused by an underpowered sample; the researchers plan to study the data further.
“Psychiatric disorders, like many other conditions, are often correlated with neighboring conditions,” he said. “Our study would suggest that some of the molecular genetic variants between OCD and generalized anxiety disorder or other anxiety disorders would be shared, but some would be unique.”
Answers an old question
In a comment, Jon Grant, JD, MD, MPH, professor of psychiatry and director of the Addictive, Compulsive, and Impulsive Disorders Research Lab at the University of Chicago, said the findings fill an important gap in what is known about OCD.
“I think the findings are really answering this old question of: ‘Is OCD due to the rearing patterns in a family versus genetics?’ This was able to get at that information showing that it’s virtually all due to genetics within families, and that’s really good to know,” said Dr. Grant, who was not a part of the study.
He was also struck by the finding of a strong genetic relationship between OCD and generalized anxiety disorder (GAD).
While identifying that OCD and GAD are genetically linked likely won’t change clinical care, “I think it at least allows clinicians to know when we see that comorbidity that it may be much more genetically linked in the case of GAD,” Dr. Grant said.
The study was funded by the Swedish Research Council, as well as Avtal om Läkarutbildning och Forskning funding from Region Skåne. Dr. Kendler and Dr. Grant reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
This finding from a large, register-based study is particularly surprising because results from previous studies of major depression and anxiety disorder have shown a significant effect of parenting and a child’s home environment on the risk for these disorders, the investigators noted.
While the results likely won’t change patient treatment, one expert said it could alleviate concerns of some parents with OCD who fear that witnessing their obsessive behaviors might put their children at higher risk for the disorder.
“The evidence is consistent with the idea that the psychological transmission of OCD from parent to child, if it exists, is really pretty weak,” lead author Kenneth S. Kendler, MD, professor of psychiatry and director of the Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University, Richmond, said in an interview.
The findings were published online in JAMA Psychiatry.
Family analysis
The study is the first to include adoptive parents in an analysis of OCD transmission, which allowed investigators to answer the nature versus nurture question that is often difficult to decipher.
Working with Swedish population registries, researchers identified more than 2.4 million offspring. Of these, 27,141 individuals (1.1%) had a lifetime diagnosis of OCD.
Families were divided into four types: intact families, with kids who lived at home with their biological parents from birth to at least age 15 years; families with kids who never lived with their biological father; families with children who did not live with their biological fathers between birth and age 15 years but who lived with a stepfather for at least 10 of those years; and families with children who were adopted before the age of 5 by people with no biological connection to the child.
After analyzing data from all parent-child relationships, researchers found that genes plus rearing (odds ratio, 3.94; 95% confidence interval, 3.58-4.33) and genes only (OR, 3.34; 95% CI, 2.27-4.93) were significantly more likely to be correlated to transmission of OCD from parent to offspring than rearing alone. Rearing only (OR, 1.4; 95% CI, 0.45-4.39) was not significantly correlated with OCD transmission
“It appears from our data that the only substantial transmission that occurs is in the genes parents transmit, not by the modeling of behavior,” Dr. Kendler said.
“There’s an idea that you can learn some things from your parents from psychopathology, but we didn’t see that kids picked that up much in the case of OCD,” he added.
However, there was one outlier: Children raised by stepparents or adoptive parents with an anxiety disorder had a greater risk of developing OCD.
Given the lack of evidence of a strong rearing effect in other analyses, Dr. Kendler noted that this rogue finding could be caused by an underpowered sample; the researchers plan to study the data further.
“Psychiatric disorders, like many other conditions, are often correlated with neighboring conditions,” he said. “Our study would suggest that some of the molecular genetic variants between OCD and generalized anxiety disorder or other anxiety disorders would be shared, but some would be unique.”
Answers an old question
In a comment, Jon Grant, JD, MD, MPH, professor of psychiatry and director of the Addictive, Compulsive, and Impulsive Disorders Research Lab at the University of Chicago, said the findings fill an important gap in what is known about OCD.
“I think the findings are really answering this old question of: ‘Is OCD due to the rearing patterns in a family versus genetics?’ This was able to get at that information showing that it’s virtually all due to genetics within families, and that’s really good to know,” said Dr. Grant, who was not a part of the study.
He was also struck by the finding of a strong genetic relationship between OCD and generalized anxiety disorder (GAD).
While identifying that OCD and GAD are genetically linked likely won’t change clinical care, “I think it at least allows clinicians to know when we see that comorbidity that it may be much more genetically linked in the case of GAD,” Dr. Grant said.
The study was funded by the Swedish Research Council, as well as Avtal om Läkarutbildning och Forskning funding from Region Skåne. Dr. Kendler and Dr. Grant reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
This finding from a large, register-based study is particularly surprising because results from previous studies of major depression and anxiety disorder have shown a significant effect of parenting and a child’s home environment on the risk for these disorders, the investigators noted.
While the results likely won’t change patient treatment, one expert said it could alleviate concerns of some parents with OCD who fear that witnessing their obsessive behaviors might put their children at higher risk for the disorder.
“The evidence is consistent with the idea that the psychological transmission of OCD from parent to child, if it exists, is really pretty weak,” lead author Kenneth S. Kendler, MD, professor of psychiatry and director of the Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University, Richmond, said in an interview.
The findings were published online in JAMA Psychiatry.
Family analysis
The study is the first to include adoptive parents in an analysis of OCD transmission, which allowed investigators to answer the nature versus nurture question that is often difficult to decipher.
Working with Swedish population registries, researchers identified more than 2.4 million offspring. Of these, 27,141 individuals (1.1%) had a lifetime diagnosis of OCD.
Families were divided into four types: intact families, with kids who lived at home with their biological parents from birth to at least age 15 years; families with kids who never lived with their biological father; families with children who did not live with their biological fathers between birth and age 15 years but who lived with a stepfather for at least 10 of those years; and families with children who were adopted before the age of 5 by people with no biological connection to the child.
After analyzing data from all parent-child relationships, researchers found that genes plus rearing (odds ratio, 3.94; 95% confidence interval, 3.58-4.33) and genes only (OR, 3.34; 95% CI, 2.27-4.93) were significantly more likely to be correlated to transmission of OCD from parent to offspring than rearing alone. Rearing only (OR, 1.4; 95% CI, 0.45-4.39) was not significantly correlated with OCD transmission
“It appears from our data that the only substantial transmission that occurs is in the genes parents transmit, not by the modeling of behavior,” Dr. Kendler said.
“There’s an idea that you can learn some things from your parents from psychopathology, but we didn’t see that kids picked that up much in the case of OCD,” he added.
However, there was one outlier: Children raised by stepparents or adoptive parents with an anxiety disorder had a greater risk of developing OCD.
Given the lack of evidence of a strong rearing effect in other analyses, Dr. Kendler noted that this rogue finding could be caused by an underpowered sample; the researchers plan to study the data further.
“Psychiatric disorders, like many other conditions, are often correlated with neighboring conditions,” he said. “Our study would suggest that some of the molecular genetic variants between OCD and generalized anxiety disorder or other anxiety disorders would be shared, but some would be unique.”
Answers an old question
In a comment, Jon Grant, JD, MD, MPH, professor of psychiatry and director of the Addictive, Compulsive, and Impulsive Disorders Research Lab at the University of Chicago, said the findings fill an important gap in what is known about OCD.
“I think the findings are really answering this old question of: ‘Is OCD due to the rearing patterns in a family versus genetics?’ This was able to get at that information showing that it’s virtually all due to genetics within families, and that’s really good to know,” said Dr. Grant, who was not a part of the study.
He was also struck by the finding of a strong genetic relationship between OCD and generalized anxiety disorder (GAD).
While identifying that OCD and GAD are genetically linked likely won’t change clinical care, “I think it at least allows clinicians to know when we see that comorbidity that it may be much more genetically linked in the case of GAD,” Dr. Grant said.
The study was funded by the Swedish Research Council, as well as Avtal om Läkarutbildning och Forskning funding from Region Skåne. Dr. Kendler and Dr. Grant reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA PSYCHIATRY
Three wild technologies about to change health care
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
When I was a child, I watched syndicated episodes of the original “Star Trek.” I was dazzled by the space travel, sure, but also the medical technology.
A handheld “tricorder” detected diseases, while an intramuscular injector (“hypospray”) could treat them. Sickbay “biobeds” came with real-time health monitors that looked futuristic at the time but seem primitive today.
Such visions inspired a lot of us kids to pursue science. Little did we know the real-life advances many of us would see in our lifetimes.
Artificial intelligence helping to spot disease, robots performing surgery, even video calls between doctor and patient – all these once sounded fantastical but now happen in clinical care.
Now, in the 23rd year of the 21st century, you might not believe wht we’ll be capable of next. Three especially wild examples are moving closer to clinical reality.
Human hibernation
Captain America, Han Solo, and “Star Trek” villain Khan – all were preserved at low temperatures and then revived, waking up alive and well months, decades, or centuries later. These are fictional examples, to be sure, but the science they’re rooted in is real.
(In one extreme case, a climber survived after almost 9 hours of efforts to revive him.)
Useful for a space traveler? Maybe not. But it’s potentially huge for someone with life-threatening injuries from a car accident or a gunshot wound.
That’s the thinking behind a breakthrough procedure that came after decades of research on pigs and dogs, now in a clinical trial. The idea: A person with massive blood loss whose heart has stopped is injected with an ice-cold fluid, cooling them from the inside, down to about 50° F.
Doctors already induce more modest hypothermia to protect the brain and other organs after cardiac arrest and during surgery on the aortic arch (the main artery carrying blood from the heart).
But this experimental procedure – called emergency preservation and resuscitation (EPR) – goes far beyond that, dramatically “decreasing the body’s need for oxygen and blood flow,” says Samuel Tisherman, MD, a trauma surgeon at the University of Maryland Medical Center and the trial’s lead researcher. This puts the patient in a state of suspended animation that “could buy time for surgeons to stop the bleeding and save more of these patients.”
The technique has been done on at least six patients, though none were reported to survive. The trial is expected to include 20 people by the time it wraps up in December, according to the listing on the U.S. clinical trials database. Though given the strict requirements for candidates (emergency trauma victims who are not likely to survive), one can’t exactly rely on a set schedule.
Still, the technology is promising. Someday we may even use it to keep patients in suspended animation for months or years, experts predict, helping astronauts through decades-long spaceflights, or stalling death in sick patients awaiting a cure.
Artificial womb
Another sci-fi classic: growing human babies outside the womb. Think the fetus fields from “The Matrix,” or the frozen embryos in “Alien: Covenant.”
In 1923, British biologist J.B.S. Haldane coined a term for that – ectogenesis. He predicted that 70% of pregnancies would take place, from fertilization to birth, in artificial wombs by 2074. That many seems unlikely, but the timeline is on track.
Developing an embryo outside the womb is already routine in in vitro fertilization. And technology enables preterm babies to survive through much of the second half of gestation. Normal human pregnancy is 40 weeks, and the youngest preterm baby ever to survive was 21 weeks and 1 day old, just a few days younger than a smattering of others who lived.
The biggest obstacle for babies younger than that is lung viability. Mechanical ventilation can damage the lungs and lead to a chronic (sometimes fatal) lung disease known as bronchopulmonary dysplasia. Avoiding this would mean figuring out a way to maintain fetal circulation – the intricate system that delivers oxygenated blood from the placenta to the fetus via the umbilical cord. Researchers at Children’s Hospital of Philadelphia have done this using a fetal lamb.
The key to their invention is a substitute placenta: an oxygenator connected to the lamb’s umbilical cord. Tubes inserted through the umbilical vein and arteries carry oxygenated blood from the “placenta” to the fetus, and deoxygenated blood back out. The lamb resides in an artificial, fluid-filled amniotic sac until its lungs and other organs are developed.
Fertility treatment could benefit, too. “An artificial womb may substitute in situations in which a gestational carrier – surrogate – is indicated,” says Paula Amato, MD, a professor of obstetrics and gynecology at Oregon Health and Science University, Portland. (Dr. Amato is not involved in the CHOP research.) For example: when the mother is missing a uterus or can’t carry a pregnancy safely.
No date is set for clinical trials yet. But according to the research, the main difference between human and lamb may come down to size. A lamb’s umbilical vessels are larger, so feeding in a tube is easier. With today’s advances in miniaturizing surgical methods, that seems like a challenge scientists can overcome.
Messenger RNA therapeutics
Back to “Star Trek.” The hypospray injector’s contents could cure just about any disease, even one newly discovered on a strange planet. That’s not unlike messenger RNA (mRNA) technology, a breakthrough that enabled scientists to quickly develop some of the first COVID-19 vaccines.
But vaccines are just the beginning of what this technology can do.
A whole field of immunotherapy is emerging that uses mRNA to deliver instructions to produce chimeric antigen receptor–modified immune cells (CAR-modified immune cells). These cells are engineered to target diseased cells and tissues, like cancer cells and harmful fibroblasts (scar tissue) that promote fibrosis in, for example, the heart and lungs.
The field is bursting with rodent research, and clinical trials have started for treating some advanced-stage malignancies.
Actual clinical use may be years away, but if all goes well, these medicines could help treat or even cure the core medical problems facing humanity. We’re talking cancer, heart disease, neurodegenerative disease – transforming one therapy into another by simply changing the mRNA’s “nucleotide sequence,” the blueprint containing instructions telling it what to do, and what disease to attack.
As this technology matures, we may start to feel as if we’re really on “Star Trek,” where Dr. Leonard “Bones” McCoy pulls out the same device to treat just about every disease or injury.
A version of this article first appeared on WebMD.com.
Can a hormone shot rescue low libido?
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
according to results from two small randomized controlled trials.
The data suggest that injections of kisspeptin can boost sexual desire in men and women and can increase penile rigidity in men.
Together, these two studies provide proof of concept for the development of kisspeptin-based therapeutics for men and women with distressing hypoactive sexual desire disorder (HSDD), study investigator Alexander Comninos, MD, PhD, Imperial College London, said in a news release.
One study was published online Feb. 3, 2022, in JAMA Network Open. The other was published in October 2022.
Unmet need
HSDD affects up to 10% of women and 8% of men worldwide and leads to psychological and social harm, the news release noted.
“There is a real unmet need to find new, safer, and more effective therapies for this distressing condition for both women and men seeking treatment,” Dr. Comninos said.
Kisspeptin is a naturally occurring reproductive hormone that serves as a crucial activator of the reproductive system. Emerging evidence from animal models shows that kisspeptin signaling has key roles in modulating reproductive behavior, including sexual motivation and erections.
In a double-blind, placebo-controlled, crossover study, the researchers enrolled 32 healthy heterosexual men (mean age, 37.9 years) who had HSDD.
At the first study visit, the men were given an infusion of kisspeptin-54 (1 nmol/kg per hour) or placebo (saline) over 75 minutes. The participants then crossed over to the other treatment at a second study visit at least 7 days later.
The active treatment significantly increased circulating kisspeptin levels. A steady state was reached after 30-75 minutes of infusion, the researchers reported.
Similar data in men, women
While the men viewed sexual videos, kisspeptin significantly modulated brain activity on fMRI in key structures of the sexual-processing network, compared with placebo (P = .003).
In addition, the treatment led to significant increases in penile tumescence in response to sexual stimuli (by up to 56% more than placebo; P = .02) and behavioral measures of sexual desire – most notably increased happiness about sex (P = .02).
Given the significant stimulatory effect of kisspeptin administration on penile rigidity, coupled with its demonstrated proerectile effect in rodents, future studies should examine the use of kisspeptin for patients with erectile dysfunction, the researchers wrote.
The second study included 32 women with HSDD and had the same design. Its results also showed that kisspeptin restored sexual and attraction brain processing without adverse effects.
“It is highly encouraging to see the same boosting effect in both women and men, although the precise brain pathways were slightly different, as might be expected,” coinvestigator Waljit Dhillo, PhD, Imperial College London, said in the news release.
“Collectively, the results suggest that kisspeptin may offer a safe and much-needed treatment for HSDD that affects millions of people around the world; and we look forward to taking this forward in future larger studies and in other patient groups,” Dr. Dhillo added.
The study was funded by the National Institute for Health and Care Research Imperial Biomedical Research Centre and the Medical Research Council, part of UK Research and Innovation. Dr. Comninos reported no relevant financial relationships. Dr. Dhillo reported receiving consulting fees from Myovant Sciences and KaNDy Therapeutics outside the submitted work.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN