User login
Brussels terror attack victim euthanized in Belgium at age 23
This article was originally published on MediQuality.com, an online service for health care professionals in the Benelux and a member of the Medscape Professional Network.
Performing euthanasia for “mental suffering that cannot be alleviated” is still considered an extraordinary measure in Belgium. Indeed, fewer than 2% of the requests for euthanasia fall within that category, and few such requests are made by young patients.
to be applicable. It’s something that Belgian broadcaster RTBF brought up during a recent episode of #Investigation, which reported on the aftermath of the 2016 Brussels attacks.
On May 7, surrounded by her family, Ms. De Corte was euthanized. She was 23 years old. Six years earlier, on March 22, 2016, Ms. De Corte had been at Brussels Airport when terrorists set off bombs. She was in the departures area with 90 other students from Sint-Rita Campus College, located in the northern town of Kontich. Ms. De Corte was only a few meters away from the blast. Although she was not physically injured, the Flemish teen was traumatized by the attack. This was confirmed by the school psychologist who treated the students. “There were some students who reacted worse than others to these traumatic events. And having had two discussions with Shanti, I can tell you that she was one of these students who were more sensitive to the effects. To me, it’s quite clear. Even before the attacks, she’d experienced serious psychological issues. Therefore, I referred her for psychiatric care.”
Eleven antidepressants daily
A few weeks after that March day, Ms. De Corte was admitted to a psychiatric hospital in Antwerp. It was a place she knew well, having been an inpatient there several times before the attacks. Ms. De Corte was treated with antidepressants. She shared her thoughts about them on numerous occasions. “I get several drugs at breakfast and up to 11 antidepressants a day. I couldn’t do without them. With all the drugs I take, I feel like a ghost who doesn’t feel anything anymore. Perhaps there were solutions other than the drugs.”
It was a brief respite. In 2020, Ms. De Corte attempted suicide. Her spirits were at their lowest. She was heavily medicated, and her medication had been increased over time. She turned down therapeutic help that was offered by a therapist who specializes in treating the victims of the Brussels attacks. The student got in touch with the Life End Information Forum, an association that supports the right to die with dignity. In April 2022, Ms. De Corte submitted a new euthanasia request, stating that she was in a medically futile condition of mental suffering. Two psychiatrists granted their approval.
A small proportion
Last March, Belgium’s Federal Commission for the Control and Evaluation of Euthanasia reported on data from 2021. “There continues to be a very small number of euthanasia requests that cite mental and behavioral disorders (psychiatric conditions, such as personality disorders, and cognitive issues, like Alzheimer’s disease, are included in this group): 1.9% of all cases of euthanasia. Like all euthanasia files, these requests meet the legal conditions (the patient is legally competent, the request is in writing, the condition is medically futile, and the suffering – which is constant, unbearable, and cannot be alleviated – results from a serious and incurable disorder; the request is well-considered and repeated),” the report states.
This article was translated from MediQuality and appeared on Medscape.com.
This article was originally published on MediQuality.com, an online service for health care professionals in the Benelux and a member of the Medscape Professional Network.
Performing euthanasia for “mental suffering that cannot be alleviated” is still considered an extraordinary measure in Belgium. Indeed, fewer than 2% of the requests for euthanasia fall within that category, and few such requests are made by young patients.
to be applicable. It’s something that Belgian broadcaster RTBF brought up during a recent episode of #Investigation, which reported on the aftermath of the 2016 Brussels attacks.
On May 7, surrounded by her family, Ms. De Corte was euthanized. She was 23 years old. Six years earlier, on March 22, 2016, Ms. De Corte had been at Brussels Airport when terrorists set off bombs. She was in the departures area with 90 other students from Sint-Rita Campus College, located in the northern town of Kontich. Ms. De Corte was only a few meters away from the blast. Although she was not physically injured, the Flemish teen was traumatized by the attack. This was confirmed by the school psychologist who treated the students. “There were some students who reacted worse than others to these traumatic events. And having had two discussions with Shanti, I can tell you that she was one of these students who were more sensitive to the effects. To me, it’s quite clear. Even before the attacks, she’d experienced serious psychological issues. Therefore, I referred her for psychiatric care.”
Eleven antidepressants daily
A few weeks after that March day, Ms. De Corte was admitted to a psychiatric hospital in Antwerp. It was a place she knew well, having been an inpatient there several times before the attacks. Ms. De Corte was treated with antidepressants. She shared her thoughts about them on numerous occasions. “I get several drugs at breakfast and up to 11 antidepressants a day. I couldn’t do without them. With all the drugs I take, I feel like a ghost who doesn’t feel anything anymore. Perhaps there were solutions other than the drugs.”
It was a brief respite. In 2020, Ms. De Corte attempted suicide. Her spirits were at their lowest. She was heavily medicated, and her medication had been increased over time. She turned down therapeutic help that was offered by a therapist who specializes in treating the victims of the Brussels attacks. The student got in touch with the Life End Information Forum, an association that supports the right to die with dignity. In April 2022, Ms. De Corte submitted a new euthanasia request, stating that she was in a medically futile condition of mental suffering. Two psychiatrists granted their approval.
A small proportion
Last March, Belgium’s Federal Commission for the Control and Evaluation of Euthanasia reported on data from 2021. “There continues to be a very small number of euthanasia requests that cite mental and behavioral disorders (psychiatric conditions, such as personality disorders, and cognitive issues, like Alzheimer’s disease, are included in this group): 1.9% of all cases of euthanasia. Like all euthanasia files, these requests meet the legal conditions (the patient is legally competent, the request is in writing, the condition is medically futile, and the suffering – which is constant, unbearable, and cannot be alleviated – results from a serious and incurable disorder; the request is well-considered and repeated),” the report states.
This article was translated from MediQuality and appeared on Medscape.com.
This article was originally published on MediQuality.com, an online service for health care professionals in the Benelux and a member of the Medscape Professional Network.
Performing euthanasia for “mental suffering that cannot be alleviated” is still considered an extraordinary measure in Belgium. Indeed, fewer than 2% of the requests for euthanasia fall within that category, and few such requests are made by young patients.
to be applicable. It’s something that Belgian broadcaster RTBF brought up during a recent episode of #Investigation, which reported on the aftermath of the 2016 Brussels attacks.
On May 7, surrounded by her family, Ms. De Corte was euthanized. She was 23 years old. Six years earlier, on March 22, 2016, Ms. De Corte had been at Brussels Airport when terrorists set off bombs. She was in the departures area with 90 other students from Sint-Rita Campus College, located in the northern town of Kontich. Ms. De Corte was only a few meters away from the blast. Although she was not physically injured, the Flemish teen was traumatized by the attack. This was confirmed by the school psychologist who treated the students. “There were some students who reacted worse than others to these traumatic events. And having had two discussions with Shanti, I can tell you that she was one of these students who were more sensitive to the effects. To me, it’s quite clear. Even before the attacks, she’d experienced serious psychological issues. Therefore, I referred her for psychiatric care.”
Eleven antidepressants daily
A few weeks after that March day, Ms. De Corte was admitted to a psychiatric hospital in Antwerp. It was a place she knew well, having been an inpatient there several times before the attacks. Ms. De Corte was treated with antidepressants. She shared her thoughts about them on numerous occasions. “I get several drugs at breakfast and up to 11 antidepressants a day. I couldn’t do without them. With all the drugs I take, I feel like a ghost who doesn’t feel anything anymore. Perhaps there were solutions other than the drugs.”
It was a brief respite. In 2020, Ms. De Corte attempted suicide. Her spirits were at their lowest. She was heavily medicated, and her medication had been increased over time. She turned down therapeutic help that was offered by a therapist who specializes in treating the victims of the Brussels attacks. The student got in touch with the Life End Information Forum, an association that supports the right to die with dignity. In April 2022, Ms. De Corte submitted a new euthanasia request, stating that she was in a medically futile condition of mental suffering. Two psychiatrists granted their approval.
A small proportion
Last March, Belgium’s Federal Commission for the Control and Evaluation of Euthanasia reported on data from 2021. “There continues to be a very small number of euthanasia requests that cite mental and behavioral disorders (psychiatric conditions, such as personality disorders, and cognitive issues, like Alzheimer’s disease, are included in this group): 1.9% of all cases of euthanasia. Like all euthanasia files, these requests meet the legal conditions (the patient is legally competent, the request is in writing, the condition is medically futile, and the suffering – which is constant, unbearable, and cannot be alleviated – results from a serious and incurable disorder; the request is well-considered and repeated),” the report states.
This article was translated from MediQuality and appeared on Medscape.com.
Risk factors ID’d for acute pancreatitis from weight-loss drugs
CHARLOTTE, N.C. – a new study has found.
Type 2 diabetes, advanced chronic kidney disease, and tobacco use were associated with greater risk for acute pancreatitis, researchers report.
On the other hand, a higher body mass index (BMI) – 36 kg/m2 or higher – appeared to protect people against developing the condition.
“As this class of medications becomes increasingly popular in the United States, it is important for providers to know which patients are at a higher or lower risk of developing acute pancreatitis after being started on them,” said lead study author Robert Postlethwaite, MD, a gastroenterology resident at the University of Texas Southwestern Medical Center, Dallas.
The findings were presented at the annual meeting of the American College of Gastroenterology in Charlotte, N.C., being held in person and virtually.
Popularity comes at a price
The U.S. Food and Drug Administration has approved two GLP-1s for weight management – liraglutide (Victoza) in 2014 and semaglutide (Wegovy) in 2021. They work by targeting areas of the brain that control food intake and appetite. Other GLP-1s approved to treat type 2 diabetes include dulaglutide (Trulicity) and two other formulations of semaglutide (Rybelsus and Ozempic).
The demand for Wegovy has been so great that there is an ongoing shortage of the medication in the United States.
Although GLP-1s demonstrate a favorable side-effect profile, compared with other types of antiobesity medications, acute pancreatitis remains a serious and sometimes life-threatening complication, the researchers note. Some patients require hospitalization.
Dr. Postlethwaite and colleagues performed a retrospective, single-center study of 2,245 patients who attended an academic medical center’s Weight Wellness program from 2015 to 2019. The average age was about 50 years, and 81% were female. The average BMI of all patients was 39.7 kg/m2.
The study only included patients starting GLP-1s for treating obesity, not for diabetes.
Of the 2,245 patients, 49 (2.2%) developed acute pancreatitis after starting a GLP-1.
A history of type 2 diabetes mellitus made acute pancreatitis twice as likely (95% confidence interval, 1.04-3.96; P = .04).
Stage 3 or higher chronic kidney disease increased risk 2.3 times (95% CI, 1.18-4.55; P = .01), while tobacco use upped it 3.3 times (95% CI, 1.70-6.50; P < .001).
In contrast, researchers found those with a BMI of 36-40 kg/m2 were 88% less likely to develop acute pancreatitis (95% CI, 0.07-0.67; P = .007), compared with patients with a BMI of less than or equal to 30 kg/m2. Patients with a BMI of greater than 40 kg/m2 had a 73% lower risk (95% CI, 0.10-0.73; P = .01).
Dr. Postlethwaite and colleagues found no association with age, sex, or history of bariatric surgery or acute pancreatitis.
Because a history of acute pancreatitis was not a risk factor, he advised that clinicians not withhold these medications for this reason, “especially given the significant glycemic, cardiovascular, and weight-loss effects.”
“We hope that we can arm clinicians with evidence in order to risk stratify their patients and determine who is at high risk of developing pancreatitis,” Dr. Postlethwaite said.
“Hopefully, we can prevent the development of pancreatitis in some patients, especially high-risk individuals, or at least allow clinicians to be aware of it in higher-risk patients to identify it early enough to prevent complications of acute pancreatitis,” he added.
Larger studies needed
The study is “promising,” said session comoderator Baharak Moshiree, MD, a gastroenterologist at Atrium Health, Charlotte, N.C., who was not affiliated with the research.
However, because the study was retrospective and relatively small, it needs to be validated in larger, prospective studies, she added.
“With obesity being such a global issue, there are many patients on these GLP-1 agonists,” Dr. Moshiree said.
Generally, these medications are prescribed by endocrinologists, not gastroenterologists, she noted, and she said that gastroenterologists should be aware of the risks associated with them, including minor gastrointestinal side effects, like nausea and vomiting, that can occur because of delayed gastric emptying.
Dr. Postlethwaite noted that being unable to assess how much alcohol or tobacco individuals used was a limitation. The relatively low proportion of people who developed acute pancreatitis in the study also means larger studies are warranted, he added.
Going forward, Dr. Postlethwaite and colleagues want to study the risks for each individual GLP-1 and other therapies used to control high blood sugar in people with type 2 diabetes, such as DPP4 (dipeptidyl-peptidase 4) inhibitors.
The study was independently supported. Dr. Postlethwaite and Dr. Moshiree report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHARLOTTE, N.C. – a new study has found.
Type 2 diabetes, advanced chronic kidney disease, and tobacco use were associated with greater risk for acute pancreatitis, researchers report.
On the other hand, a higher body mass index (BMI) – 36 kg/m2 or higher – appeared to protect people against developing the condition.
“As this class of medications becomes increasingly popular in the United States, it is important for providers to know which patients are at a higher or lower risk of developing acute pancreatitis after being started on them,” said lead study author Robert Postlethwaite, MD, a gastroenterology resident at the University of Texas Southwestern Medical Center, Dallas.
The findings were presented at the annual meeting of the American College of Gastroenterology in Charlotte, N.C., being held in person and virtually.
Popularity comes at a price
The U.S. Food and Drug Administration has approved two GLP-1s for weight management – liraglutide (Victoza) in 2014 and semaglutide (Wegovy) in 2021. They work by targeting areas of the brain that control food intake and appetite. Other GLP-1s approved to treat type 2 diabetes include dulaglutide (Trulicity) and two other formulations of semaglutide (Rybelsus and Ozempic).
The demand for Wegovy has been so great that there is an ongoing shortage of the medication in the United States.
Although GLP-1s demonstrate a favorable side-effect profile, compared with other types of antiobesity medications, acute pancreatitis remains a serious and sometimes life-threatening complication, the researchers note. Some patients require hospitalization.
Dr. Postlethwaite and colleagues performed a retrospective, single-center study of 2,245 patients who attended an academic medical center’s Weight Wellness program from 2015 to 2019. The average age was about 50 years, and 81% were female. The average BMI of all patients was 39.7 kg/m2.
The study only included patients starting GLP-1s for treating obesity, not for diabetes.
Of the 2,245 patients, 49 (2.2%) developed acute pancreatitis after starting a GLP-1.
A history of type 2 diabetes mellitus made acute pancreatitis twice as likely (95% confidence interval, 1.04-3.96; P = .04).
Stage 3 or higher chronic kidney disease increased risk 2.3 times (95% CI, 1.18-4.55; P = .01), while tobacco use upped it 3.3 times (95% CI, 1.70-6.50; P < .001).
In contrast, researchers found those with a BMI of 36-40 kg/m2 were 88% less likely to develop acute pancreatitis (95% CI, 0.07-0.67; P = .007), compared with patients with a BMI of less than or equal to 30 kg/m2. Patients with a BMI of greater than 40 kg/m2 had a 73% lower risk (95% CI, 0.10-0.73; P = .01).
Dr. Postlethwaite and colleagues found no association with age, sex, or history of bariatric surgery or acute pancreatitis.
Because a history of acute pancreatitis was not a risk factor, he advised that clinicians not withhold these medications for this reason, “especially given the significant glycemic, cardiovascular, and weight-loss effects.”
“We hope that we can arm clinicians with evidence in order to risk stratify their patients and determine who is at high risk of developing pancreatitis,” Dr. Postlethwaite said.
“Hopefully, we can prevent the development of pancreatitis in some patients, especially high-risk individuals, or at least allow clinicians to be aware of it in higher-risk patients to identify it early enough to prevent complications of acute pancreatitis,” he added.
Larger studies needed
The study is “promising,” said session comoderator Baharak Moshiree, MD, a gastroenterologist at Atrium Health, Charlotte, N.C., who was not affiliated with the research.
However, because the study was retrospective and relatively small, it needs to be validated in larger, prospective studies, she added.
“With obesity being such a global issue, there are many patients on these GLP-1 agonists,” Dr. Moshiree said.
Generally, these medications are prescribed by endocrinologists, not gastroenterologists, she noted, and she said that gastroenterologists should be aware of the risks associated with them, including minor gastrointestinal side effects, like nausea and vomiting, that can occur because of delayed gastric emptying.
Dr. Postlethwaite noted that being unable to assess how much alcohol or tobacco individuals used was a limitation. The relatively low proportion of people who developed acute pancreatitis in the study also means larger studies are warranted, he added.
Going forward, Dr. Postlethwaite and colleagues want to study the risks for each individual GLP-1 and other therapies used to control high blood sugar in people with type 2 diabetes, such as DPP4 (dipeptidyl-peptidase 4) inhibitors.
The study was independently supported. Dr. Postlethwaite and Dr. Moshiree report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHARLOTTE, N.C. – a new study has found.
Type 2 diabetes, advanced chronic kidney disease, and tobacco use were associated with greater risk for acute pancreatitis, researchers report.
On the other hand, a higher body mass index (BMI) – 36 kg/m2 or higher – appeared to protect people against developing the condition.
“As this class of medications becomes increasingly popular in the United States, it is important for providers to know which patients are at a higher or lower risk of developing acute pancreatitis after being started on them,” said lead study author Robert Postlethwaite, MD, a gastroenterology resident at the University of Texas Southwestern Medical Center, Dallas.
The findings were presented at the annual meeting of the American College of Gastroenterology in Charlotte, N.C., being held in person and virtually.
Popularity comes at a price
The U.S. Food and Drug Administration has approved two GLP-1s for weight management – liraglutide (Victoza) in 2014 and semaglutide (Wegovy) in 2021. They work by targeting areas of the brain that control food intake and appetite. Other GLP-1s approved to treat type 2 diabetes include dulaglutide (Trulicity) and two other formulations of semaglutide (Rybelsus and Ozempic).
The demand for Wegovy has been so great that there is an ongoing shortage of the medication in the United States.
Although GLP-1s demonstrate a favorable side-effect profile, compared with other types of antiobesity medications, acute pancreatitis remains a serious and sometimes life-threatening complication, the researchers note. Some patients require hospitalization.
Dr. Postlethwaite and colleagues performed a retrospective, single-center study of 2,245 patients who attended an academic medical center’s Weight Wellness program from 2015 to 2019. The average age was about 50 years, and 81% were female. The average BMI of all patients was 39.7 kg/m2.
The study only included patients starting GLP-1s for treating obesity, not for diabetes.
Of the 2,245 patients, 49 (2.2%) developed acute pancreatitis after starting a GLP-1.
A history of type 2 diabetes mellitus made acute pancreatitis twice as likely (95% confidence interval, 1.04-3.96; P = .04).
Stage 3 or higher chronic kidney disease increased risk 2.3 times (95% CI, 1.18-4.55; P = .01), while tobacco use upped it 3.3 times (95% CI, 1.70-6.50; P < .001).
In contrast, researchers found those with a BMI of 36-40 kg/m2 were 88% less likely to develop acute pancreatitis (95% CI, 0.07-0.67; P = .007), compared with patients with a BMI of less than or equal to 30 kg/m2. Patients with a BMI of greater than 40 kg/m2 had a 73% lower risk (95% CI, 0.10-0.73; P = .01).
Dr. Postlethwaite and colleagues found no association with age, sex, or history of bariatric surgery or acute pancreatitis.
Because a history of acute pancreatitis was not a risk factor, he advised that clinicians not withhold these medications for this reason, “especially given the significant glycemic, cardiovascular, and weight-loss effects.”
“We hope that we can arm clinicians with evidence in order to risk stratify their patients and determine who is at high risk of developing pancreatitis,” Dr. Postlethwaite said.
“Hopefully, we can prevent the development of pancreatitis in some patients, especially high-risk individuals, or at least allow clinicians to be aware of it in higher-risk patients to identify it early enough to prevent complications of acute pancreatitis,” he added.
Larger studies needed
The study is “promising,” said session comoderator Baharak Moshiree, MD, a gastroenterologist at Atrium Health, Charlotte, N.C., who was not affiliated with the research.
However, because the study was retrospective and relatively small, it needs to be validated in larger, prospective studies, she added.
“With obesity being such a global issue, there are many patients on these GLP-1 agonists,” Dr. Moshiree said.
Generally, these medications are prescribed by endocrinologists, not gastroenterologists, she noted, and she said that gastroenterologists should be aware of the risks associated with them, including minor gastrointestinal side effects, like nausea and vomiting, that can occur because of delayed gastric emptying.
Dr. Postlethwaite noted that being unable to assess how much alcohol or tobacco individuals used was a limitation. The relatively low proportion of people who developed acute pancreatitis in the study also means larger studies are warranted, he added.
Going forward, Dr. Postlethwaite and colleagues want to study the risks for each individual GLP-1 and other therapies used to control high blood sugar in people with type 2 diabetes, such as DPP4 (dipeptidyl-peptidase 4) inhibitors.
The study was independently supported. Dr. Postlethwaite and Dr. Moshiree report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACG 2022
Ivermectin for COVID-19: Final nail in the coffin
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
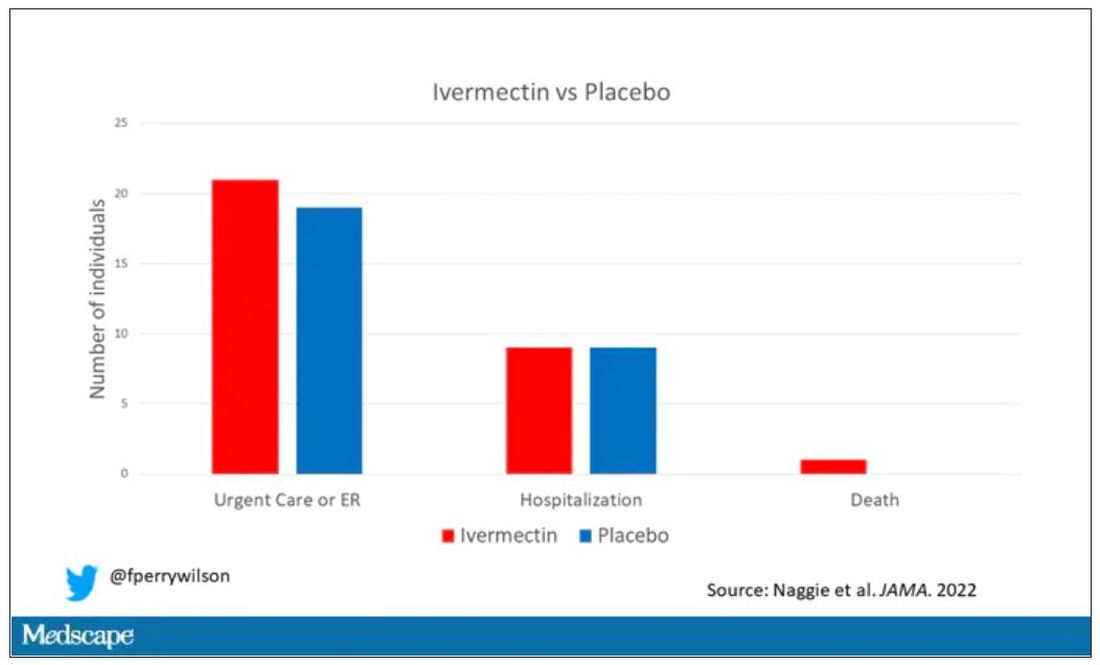
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Study affirms better breast cancer outcomes when chemo comes first
New efficacy and safety data from the monarchE study show that chemotherapy administered before treatment with abemaciclib and estrogen therapy, led to a clinically meaningful improvement in invasive disease-free survival and distant relapse-free survival for women with HR-positive, ERBB2-negative, node-positive, early breast cancer at high risk of recurrence.
The study was published earlier this year in JAMA Oncology.
Neoadjuvant chemotherapy is often provided to such patients in hopes of achieving breast-conserving surgery. Although pathologic complete response rates can be higher than 50% after chemotherapy treatment in triple-negative and ERBB2-positive breast cancer, most patients with HR-positive and ERBB2-negative breast cancer have residual tumor at surgery after neoadjuvant chemotherapy, which is associated with an increased risk of recurrence.
“To our knowledge, abemaciclib is the first agent added to standard adjuvant estrogen therapy that has been shown to reduce the risk of recurrence in patients with HR-positive, ERBB2-negative early breast cancer with residual disease after neoadjuvant chemotherapy,” wrote the authors, who were led by Miguel Martin, MD, PhD, Hospital General Universitario Gregorio Marañon, Spain.
In 2021, Food and Drug Administration approved abemaciclib (Verzenio, Lilly) with endocrine therapy for the treatment of HR-positive/ERBB2-negative, node-positive, high-risk early breast cancer. Their decision was based on data from the monarchE study.
The study is at odds with the previously published Penelope-B study, which found no benefit from treatment with the CDK4/6 inhibitor palbociclib (Ibrance, Pfizer) after 42.8 months of follow-up. The authors suggest that the disparate outcomes may be due to pharmacological differences between the two drugs as well as different dosing schedules: In monarchE, patients received abemaciclib on a continuous basis, while patients in Penelope-B received palbociclib for 21 days, followed by 7 days off. The treatment duration was 2 years in monarchE and 1 year in Penelope-B. Abemaciclib can be dosed continuously because it is a stronger inhibitor of CDK4 versus CDK6 compared to abemaciclib, and in vitro studies suggest that continuous dosing could be a key factor in creating profound inhibition of DNA synthesis.
The monarchE study included 5,637 patients who were randomized to receive standard of care estrogen therapy for 5 years with or without abemaciclib (150 mg, twice per day) for 2 years; 36.5% received abemaciclib. The mean age was 49.9 years; 70.8% were White, 22.8% Asian, and 2.7% Black.
The abemaciclib group had a clinically and statistically significant benefit in invasive disease-free survival (IDFS) (hazard ratio, 0.61; nominal P < .001) and distant relapse-free survival (DRFS) (HR, 0.61; nominal P < .001). At 2 years, DRFS was 89.5% in the abemaciclib group and 82.8% in the estrogen therapy–only group. IDFS was 87.2% and 80.6%, respectively. Patients who underwent neoadjuvant chemotherapy had a similar safety profile to the estrogen therapy–only group, although there was a higher incidence of treatment-emergent adverse events. The most common were diarrhea, infections, neutropenia, and fatigue. The most frequent grade treatment-emergent adverse events (of at least 3) were neutropenia and leucopenia.
The researchers noted that patients who underwent neoadjuvant chemotherapy had a worse prognosis than the intent-to-treat arm, as evidenced by a higher risk of 2-year recurrence (19% versus 11%). Exploratory subgroup analyses revealed that treatment with abemaciclib and estrogen therapy conferred IDFS and DRFS benefits regardless of the pathological tumor size and number of positive axillary lymph nodes.
The study was limited by the fact that it was open label, and the subgroup analyses were not powered to find statistically significant associations.
Dr. Martin has received grants from Eli Lilly, which funded monarchE.
New efficacy and safety data from the monarchE study show that chemotherapy administered before treatment with abemaciclib and estrogen therapy, led to a clinically meaningful improvement in invasive disease-free survival and distant relapse-free survival for women with HR-positive, ERBB2-negative, node-positive, early breast cancer at high risk of recurrence.
The study was published earlier this year in JAMA Oncology.
Neoadjuvant chemotherapy is often provided to such patients in hopes of achieving breast-conserving surgery. Although pathologic complete response rates can be higher than 50% after chemotherapy treatment in triple-negative and ERBB2-positive breast cancer, most patients with HR-positive and ERBB2-negative breast cancer have residual tumor at surgery after neoadjuvant chemotherapy, which is associated with an increased risk of recurrence.
“To our knowledge, abemaciclib is the first agent added to standard adjuvant estrogen therapy that has been shown to reduce the risk of recurrence in patients with HR-positive, ERBB2-negative early breast cancer with residual disease after neoadjuvant chemotherapy,” wrote the authors, who were led by Miguel Martin, MD, PhD, Hospital General Universitario Gregorio Marañon, Spain.
In 2021, Food and Drug Administration approved abemaciclib (Verzenio, Lilly) with endocrine therapy for the treatment of HR-positive/ERBB2-negative, node-positive, high-risk early breast cancer. Their decision was based on data from the monarchE study.
The study is at odds with the previously published Penelope-B study, which found no benefit from treatment with the CDK4/6 inhibitor palbociclib (Ibrance, Pfizer) after 42.8 months of follow-up. The authors suggest that the disparate outcomes may be due to pharmacological differences between the two drugs as well as different dosing schedules: In monarchE, patients received abemaciclib on a continuous basis, while patients in Penelope-B received palbociclib for 21 days, followed by 7 days off. The treatment duration was 2 years in monarchE and 1 year in Penelope-B. Abemaciclib can be dosed continuously because it is a stronger inhibitor of CDK4 versus CDK6 compared to abemaciclib, and in vitro studies suggest that continuous dosing could be a key factor in creating profound inhibition of DNA synthesis.
The monarchE study included 5,637 patients who were randomized to receive standard of care estrogen therapy for 5 years with or without abemaciclib (150 mg, twice per day) for 2 years; 36.5% received abemaciclib. The mean age was 49.9 years; 70.8% were White, 22.8% Asian, and 2.7% Black.
The abemaciclib group had a clinically and statistically significant benefit in invasive disease-free survival (IDFS) (hazard ratio, 0.61; nominal P < .001) and distant relapse-free survival (DRFS) (HR, 0.61; nominal P < .001). At 2 years, DRFS was 89.5% in the abemaciclib group and 82.8% in the estrogen therapy–only group. IDFS was 87.2% and 80.6%, respectively. Patients who underwent neoadjuvant chemotherapy had a similar safety profile to the estrogen therapy–only group, although there was a higher incidence of treatment-emergent adverse events. The most common were diarrhea, infections, neutropenia, and fatigue. The most frequent grade treatment-emergent adverse events (of at least 3) were neutropenia and leucopenia.
The researchers noted that patients who underwent neoadjuvant chemotherapy had a worse prognosis than the intent-to-treat arm, as evidenced by a higher risk of 2-year recurrence (19% versus 11%). Exploratory subgroup analyses revealed that treatment with abemaciclib and estrogen therapy conferred IDFS and DRFS benefits regardless of the pathological tumor size and number of positive axillary lymph nodes.
The study was limited by the fact that it was open label, and the subgroup analyses were not powered to find statistically significant associations.
Dr. Martin has received grants from Eli Lilly, which funded monarchE.
New efficacy and safety data from the monarchE study show that chemotherapy administered before treatment with abemaciclib and estrogen therapy, led to a clinically meaningful improvement in invasive disease-free survival and distant relapse-free survival for women with HR-positive, ERBB2-negative, node-positive, early breast cancer at high risk of recurrence.
The study was published earlier this year in JAMA Oncology.
Neoadjuvant chemotherapy is often provided to such patients in hopes of achieving breast-conserving surgery. Although pathologic complete response rates can be higher than 50% after chemotherapy treatment in triple-negative and ERBB2-positive breast cancer, most patients with HR-positive and ERBB2-negative breast cancer have residual tumor at surgery after neoadjuvant chemotherapy, which is associated with an increased risk of recurrence.
“To our knowledge, abemaciclib is the first agent added to standard adjuvant estrogen therapy that has been shown to reduce the risk of recurrence in patients with HR-positive, ERBB2-negative early breast cancer with residual disease after neoadjuvant chemotherapy,” wrote the authors, who were led by Miguel Martin, MD, PhD, Hospital General Universitario Gregorio Marañon, Spain.
In 2021, Food and Drug Administration approved abemaciclib (Verzenio, Lilly) with endocrine therapy for the treatment of HR-positive/ERBB2-negative, node-positive, high-risk early breast cancer. Their decision was based on data from the monarchE study.
The study is at odds with the previously published Penelope-B study, which found no benefit from treatment with the CDK4/6 inhibitor palbociclib (Ibrance, Pfizer) after 42.8 months of follow-up. The authors suggest that the disparate outcomes may be due to pharmacological differences between the two drugs as well as different dosing schedules: In monarchE, patients received abemaciclib on a continuous basis, while patients in Penelope-B received palbociclib for 21 days, followed by 7 days off. The treatment duration was 2 years in monarchE and 1 year in Penelope-B. Abemaciclib can be dosed continuously because it is a stronger inhibitor of CDK4 versus CDK6 compared to abemaciclib, and in vitro studies suggest that continuous dosing could be a key factor in creating profound inhibition of DNA synthesis.
The monarchE study included 5,637 patients who were randomized to receive standard of care estrogen therapy for 5 years with or without abemaciclib (150 mg, twice per day) for 2 years; 36.5% received abemaciclib. The mean age was 49.9 years; 70.8% were White, 22.8% Asian, and 2.7% Black.
The abemaciclib group had a clinically and statistically significant benefit in invasive disease-free survival (IDFS) (hazard ratio, 0.61; nominal P < .001) and distant relapse-free survival (DRFS) (HR, 0.61; nominal P < .001). At 2 years, DRFS was 89.5% in the abemaciclib group and 82.8% in the estrogen therapy–only group. IDFS was 87.2% and 80.6%, respectively. Patients who underwent neoadjuvant chemotherapy had a similar safety profile to the estrogen therapy–only group, although there was a higher incidence of treatment-emergent adverse events. The most common were diarrhea, infections, neutropenia, and fatigue. The most frequent grade treatment-emergent adverse events (of at least 3) were neutropenia and leucopenia.
The researchers noted that patients who underwent neoadjuvant chemotherapy had a worse prognosis than the intent-to-treat arm, as evidenced by a higher risk of 2-year recurrence (19% versus 11%). Exploratory subgroup analyses revealed that treatment with abemaciclib and estrogen therapy conferred IDFS and DRFS benefits regardless of the pathological tumor size and number of positive axillary lymph nodes.
The study was limited by the fact that it was open label, and the subgroup analyses were not powered to find statistically significant associations.
Dr. Martin has received grants from Eli Lilly, which funded monarchE.
FROM JAMA ONCOLOGY
Side effects from COVID vaccine show its effectiveness
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
FROM JAMA NETWORK OPEN
Vitamin D deficiency linked to death, new study finds
Vitamin D deficiency increases mortality risk and raising levels even slightly could decrease the risk, researchers examining data from the UK Biobank have found.
They used a Mendelian randomization approach, which uses genetic variants as “proxy indicators” for external factors that affect vitamin D levels, such as sun exposure or dietary intake. It allows for analysis of the relationship between deficiency and outcomes including mortality, which can’t be done in randomized clinical trials for ethical reasons.
Using this method, nutritionist Joshua P. Sutherland, PhD, of the Australian Centre for Precision Health, Adelaide, and colleagues found an association between genetically predicted vitamin D levels [25-(OH)D] and mortality from several major causes, with evidence of causality among people with measured concentrations below, but not above, 50 nmol/L. The findings were published online in Annals of Internal Medicine.

“Unlike other types of observational studies, we have overcome some of the methodological obstacles. What is special about this new study is we were able to look at people with very low vitamin D concentrations and what would happen if their concentrations were a little bit higher. Most randomized controlled trials don’t show much of an effect. That’s because most people have sufficient concentrations. Ethically you can’t do a trial of people with very low levels without treating them,” senior author Elina Hypp
The data support the 50 nmol/L cut-off endorsed by the United States National Academy of Medicine and align with previous data suggesting the benefit of vitamin D supplementation is largely seen in people with deficiency.
“Everybody with vitamin D levels less than 50 nmol/L is recommended to increase their levels. Our results suggest there’s no need to go very high. The positive message is that if we are able to raise levels to just the current U.S. recommendations, that’s fine. There’s no need to use large supplement doses,” Dr. Hyppönen explained.
Thus, she advised, “Supplementation will clearly help, especially during wintertime or if a person isn’t getting enough vitamin D from the sun or in places where food isn’t fortified with vitamin D.”
But the data don’t support the approach of using large intermittent doses, she added.
“Sometimes doctors want to fix the deficiency quickly with a large ‘bolus’ dose, then continue with a maintenance dose. Increasing evidence suggests that’s not beneficial and might disturb the body’s metabolism so that it can’t get the amount it needs. It’s safe overall but might not work the way we want it to work.”
Rather, Dr. Hyppönen said, “My sense is that daily modest vitamin D dose supplementation when it’s needed is the best way forward.”
Genetic approach reveals causal relationship
The investigators analyzed data from 307,601 individuals in the UK Biobank, a prospective cohort of people recruited from England, Scotland, and Wales during March 2006 and July 2010. Most were of White European ancestry and were aged 37-73 years at baseline.
Genetically predicted vitamin D levels were estimated using 35 confirmed 25-(OH)D variants. Participants were followed for outcomes up to June 2020.
The average baseline measured 25-(OH)D concentration was 45.2 nmol/L, and 11.7% (n = 36,009) of participants had levels between 10.0 and 24.9 nmol/L. Higher levels were seen in people living in southern areas and nonsmokers as well as those with a higher level of physical activity, less socioeconomic deprivation, and lower body mass index.
During follow-up, 6.1% of participants died (n = 18,700). After adjustment for variables, odds ratios for all causes of mortality were highest among people with 25-(OH)D levels below 25 nmol/L and appeared to plateau between 50 and 75 nmol/L, with no further reduction in mortality at values of 75-125 nmol/L.
Mortality 36% higher in those deficient in vitamin D
The risk for mortality was a significant 36% higher for participants with 25-(OH)D 25 nmol/L compared with 50 nmol/L.
With the Mendelian randomization, there was an L-shaped association between genetically predicted 25-(OH)D level and all-cause mortality (P for nonlinearity < .001) and for mortality because of cancer and cardiovascular disease (P for nonlinearity ≤ .033).
Again, the strongest association with those outcomes and genetically predicted 25-(OH)D was found at levels below 25 nmol/L and a plateau was seen by 50 nmol/L.
Compared with a measured 25-(OH)D concentration of 50 nmol/L, investigators estimated that the genetically predicted odds of all-cause mortality would increase sixfold (odds ratio, 6.00) for participants at 10 nmol/L and by 25% (OR, 1.25) for those at 25 nmol/L.
And, compared with a measured 25-(OH)D concentration of 50 nmol/L, those with 10 nmol/L had genetically predicted odds ratios of 5.98 for cardiovascular mortality, 3.37 for cancer mortality, and 12.44 for respiratory mortality.
Comparing measured 25-(OH)D concentrations of 25 nmol/L versus 50 nmol/L, odds ratios for those outcomes were 1.25, 1.16, and 1.96 (95% confidence interval, 1.88-4.67), respectively. All were statistically significant.
Consistent results supportive of a causal effect of genetically predicted 25-(OH)D on all-cause mortality in those with low measured vitamin D concentrations were also found in a sensitivity analysis of 20,837 people of non-White ethnic origin.
The study was funded by the Australian National Health and Medical Research Council. Dr. Sutherland’s studentship is funded by an Australian Research Training Program Scholarship.
A version of this article first appeared on Medscape.com.
Vitamin D deficiency increases mortality risk and raising levels even slightly could decrease the risk, researchers examining data from the UK Biobank have found.
They used a Mendelian randomization approach, which uses genetic variants as “proxy indicators” for external factors that affect vitamin D levels, such as sun exposure or dietary intake. It allows for analysis of the relationship between deficiency and outcomes including mortality, which can’t be done in randomized clinical trials for ethical reasons.
Using this method, nutritionist Joshua P. Sutherland, PhD, of the Australian Centre for Precision Health, Adelaide, and colleagues found an association between genetically predicted vitamin D levels [25-(OH)D] and mortality from several major causes, with evidence of causality among people with measured concentrations below, but not above, 50 nmol/L. The findings were published online in Annals of Internal Medicine.
“Unlike other types of observational studies, we have overcome some of the methodological obstacles. What is special about this new study is we were able to look at people with very low vitamin D concentrations and what would happen if their concentrations were a little bit higher. Most randomized controlled trials don’t show much of an effect. That’s because most people have sufficient concentrations. Ethically you can’t do a trial of people with very low levels without treating them,” senior author Elina Hypp
The data support the 50 nmol/L cut-off endorsed by the United States National Academy of Medicine and align with previous data suggesting the benefit of vitamin D supplementation is largely seen in people with deficiency.
“Everybody with vitamin D levels less than 50 nmol/L is recommended to increase their levels. Our results suggest there’s no need to go very high. The positive message is that if we are able to raise levels to just the current U.S. recommendations, that’s fine. There’s no need to use large supplement doses,” Dr. Hyppönen explained.
Thus, she advised, “Supplementation will clearly help, especially during wintertime or if a person isn’t getting enough vitamin D from the sun or in places where food isn’t fortified with vitamin D.”
But the data don’t support the approach of using large intermittent doses, she added.
“Sometimes doctors want to fix the deficiency quickly with a large ‘bolus’ dose, then continue with a maintenance dose. Increasing evidence suggests that’s not beneficial and might disturb the body’s metabolism so that it can’t get the amount it needs. It’s safe overall but might not work the way we want it to work.”
Rather, Dr. Hyppönen said, “My sense is that daily modest vitamin D dose supplementation when it’s needed is the best way forward.”
Genetic approach reveals causal relationship
The investigators analyzed data from 307,601 individuals in the UK Biobank, a prospective cohort of people recruited from England, Scotland, and Wales during March 2006 and July 2010. Most were of White European ancestry and were aged 37-73 years at baseline.
Genetically predicted vitamin D levels were estimated using 35 confirmed 25-(OH)D variants. Participants were followed for outcomes up to June 2020.
The average baseline measured 25-(OH)D concentration was 45.2 nmol/L, and 11.7% (n = 36,009) of participants had levels between 10.0 and 24.9 nmol/L. Higher levels were seen in people living in southern areas and nonsmokers as well as those with a higher level of physical activity, less socioeconomic deprivation, and lower body mass index.
During follow-up, 6.1% of participants died (n = 18,700). After adjustment for variables, odds ratios for all causes of mortality were highest among people with 25-(OH)D levels below 25 nmol/L and appeared to plateau between 50 and 75 nmol/L, with no further reduction in mortality at values of 75-125 nmol/L.
Mortality 36% higher in those deficient in vitamin D
The risk for mortality was a significant 36% higher for participants with 25-(OH)D 25 nmol/L compared with 50 nmol/L.
With the Mendelian randomization, there was an L-shaped association between genetically predicted 25-(OH)D level and all-cause mortality (P for nonlinearity < .001) and for mortality because of cancer and cardiovascular disease (P for nonlinearity ≤ .033).
Again, the strongest association with those outcomes and genetically predicted 25-(OH)D was found at levels below 25 nmol/L and a plateau was seen by 50 nmol/L.
Compared with a measured 25-(OH)D concentration of 50 nmol/L, investigators estimated that the genetically predicted odds of all-cause mortality would increase sixfold (odds ratio, 6.00) for participants at 10 nmol/L and by 25% (OR, 1.25) for those at 25 nmol/L.
And, compared with a measured 25-(OH)D concentration of 50 nmol/L, those with 10 nmol/L had genetically predicted odds ratios of 5.98 for cardiovascular mortality, 3.37 for cancer mortality, and 12.44 for respiratory mortality.
Comparing measured 25-(OH)D concentrations of 25 nmol/L versus 50 nmol/L, odds ratios for those outcomes were 1.25, 1.16, and 1.96 (95% confidence interval, 1.88-4.67), respectively. All were statistically significant.
Consistent results supportive of a causal effect of genetically predicted 25-(OH)D on all-cause mortality in those with low measured vitamin D concentrations were also found in a sensitivity analysis of 20,837 people of non-White ethnic origin.
The study was funded by the Australian National Health and Medical Research Council. Dr. Sutherland’s studentship is funded by an Australian Research Training Program Scholarship.
A version of this article first appeared on Medscape.com.
Vitamin D deficiency increases mortality risk and raising levels even slightly could decrease the risk, researchers examining data from the UK Biobank have found.
They used a Mendelian randomization approach, which uses genetic variants as “proxy indicators” for external factors that affect vitamin D levels, such as sun exposure or dietary intake. It allows for analysis of the relationship between deficiency and outcomes including mortality, which can’t be done in randomized clinical trials for ethical reasons.
Using this method, nutritionist Joshua P. Sutherland, PhD, of the Australian Centre for Precision Health, Adelaide, and colleagues found an association between genetically predicted vitamin D levels [25-(OH)D] and mortality from several major causes, with evidence of causality among people with measured concentrations below, but not above, 50 nmol/L. The findings were published online in Annals of Internal Medicine.
“Unlike other types of observational studies, we have overcome some of the methodological obstacles. What is special about this new study is we were able to look at people with very low vitamin D concentrations and what would happen if their concentrations were a little bit higher. Most randomized controlled trials don’t show much of an effect. That’s because most people have sufficient concentrations. Ethically you can’t do a trial of people with very low levels without treating them,” senior author Elina Hypp
The data support the 50 nmol/L cut-off endorsed by the United States National Academy of Medicine and align with previous data suggesting the benefit of vitamin D supplementation is largely seen in people with deficiency.
“Everybody with vitamin D levels less than 50 nmol/L is recommended to increase their levels. Our results suggest there’s no need to go very high. The positive message is that if we are able to raise levels to just the current U.S. recommendations, that’s fine. There’s no need to use large supplement doses,” Dr. Hyppönen explained.
Thus, she advised, “Supplementation will clearly help, especially during wintertime or if a person isn’t getting enough vitamin D from the sun or in places where food isn’t fortified with vitamin D.”
But the data don’t support the approach of using large intermittent doses, she added.
“Sometimes doctors want to fix the deficiency quickly with a large ‘bolus’ dose, then continue with a maintenance dose. Increasing evidence suggests that’s not beneficial and might disturb the body’s metabolism so that it can’t get the amount it needs. It’s safe overall but might not work the way we want it to work.”
Rather, Dr. Hyppönen said, “My sense is that daily modest vitamin D dose supplementation when it’s needed is the best way forward.”
Genetic approach reveals causal relationship
The investigators analyzed data from 307,601 individuals in the UK Biobank, a prospective cohort of people recruited from England, Scotland, and Wales during March 2006 and July 2010. Most were of White European ancestry and were aged 37-73 years at baseline.
Genetically predicted vitamin D levels were estimated using 35 confirmed 25-(OH)D variants. Participants were followed for outcomes up to June 2020.
The average baseline measured 25-(OH)D concentration was 45.2 nmol/L, and 11.7% (n = 36,009) of participants had levels between 10.0 and 24.9 nmol/L. Higher levels were seen in people living in southern areas and nonsmokers as well as those with a higher level of physical activity, less socioeconomic deprivation, and lower body mass index.
During follow-up, 6.1% of participants died (n = 18,700). After adjustment for variables, odds ratios for all causes of mortality were highest among people with 25-(OH)D levels below 25 nmol/L and appeared to plateau between 50 and 75 nmol/L, with no further reduction in mortality at values of 75-125 nmol/L.
Mortality 36% higher in those deficient in vitamin D
The risk for mortality was a significant 36% higher for participants with 25-(OH)D 25 nmol/L compared with 50 nmol/L.
With the Mendelian randomization, there was an L-shaped association between genetically predicted 25-(OH)D level and all-cause mortality (P for nonlinearity < .001) and for mortality because of cancer and cardiovascular disease (P for nonlinearity ≤ .033).
Again, the strongest association with those outcomes and genetically predicted 25-(OH)D was found at levels below 25 nmol/L and a plateau was seen by 50 nmol/L.
Compared with a measured 25-(OH)D concentration of 50 nmol/L, investigators estimated that the genetically predicted odds of all-cause mortality would increase sixfold (odds ratio, 6.00) for participants at 10 nmol/L and by 25% (OR, 1.25) for those at 25 nmol/L.
And, compared with a measured 25-(OH)D concentration of 50 nmol/L, those with 10 nmol/L had genetically predicted odds ratios of 5.98 for cardiovascular mortality, 3.37 for cancer mortality, and 12.44 for respiratory mortality.
Comparing measured 25-(OH)D concentrations of 25 nmol/L versus 50 nmol/L, odds ratios for those outcomes were 1.25, 1.16, and 1.96 (95% confidence interval, 1.88-4.67), respectively. All were statistically significant.
Consistent results supportive of a causal effect of genetically predicted 25-(OH)D on all-cause mortality in those with low measured vitamin D concentrations were also found in a sensitivity analysis of 20,837 people of non-White ethnic origin.
The study was funded by the Australian National Health and Medical Research Council. Dr. Sutherland’s studentship is funded by an Australian Research Training Program Scholarship.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE

Early estrogen loss increases cardiovascular risk in women
The relationship between estrogen levels and heart health makes it particularly important for clinicians to be aware of those patients who might be at risk for cardiovascular disease despite not having other traditional risk factors, according to a presentation Oct. 12 at the North American Menopause Society annual meeting in Atlanta.
”Endogenous estrogens are protective for cardiovascular disease in premenopausal women,” Chrisandra L. Shufelt, MD, chair of the division of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Fla., told attendees. Yet, “a substantial population of young women are dying prematurely from cardiovascular disease,” with rates of cardiovascular death increasing in women aged 35-44 even as rates have decreased in postmenopausal women and in men. One potential reason may be premature estrogen loss.

Dr. Shufelt reminded attendees of four major causes of premature estrogen loss: Natural premature menopause, surgical menopause, chemotherapy-induced menopause, and premature ovarian insufficiency. But she would go on to discuss a less widely recognized condition, functional hypothalamic amenorrhea, that also may be contributing to increased cardiovascular risk.
First, Dr. Shufelt reviewed the evidence supporting the relationship between estrogen and cardiovascular health, starting with the Framingham study’s findings that cardiovascular disease is approximately two to four times more common in postmenopausal women than in premenopausal women, depending on the age range.
“Menopause at an early age, particularly under the age of 40, matters,” Dr. Shufelt said. “So we should be discussing this with our patients.”
Surgical menopause makes a difference to cardiovascular health as well, she said. In women under age 35, for example, the risk of a nonfatal heart attack in those with a bilateral oophorectomy was 7.7 times greater than in women who retained both ovaries and their uterus, and 1.5 times greater in women who had a hysterectomy without bilateral oophorectomy.
In a 2019 study, surgical premature menopause was associated with an 87% increased risk of heart disease even after researchers accounted for age, cardiovascular risk factors, and some forms of hormone therapy. The increased risk from natural premature menopause, on the other hand, was lower – a 36% increased risk of heart disease – compared with those producing endogenous hormones. Although randomized controlled trials are unavailable and unlikely to be done, the Nurses’ Health Study and the Danish Nurses Cohort Study, both observational studies, found that heart disease risk was diminished in those taking hormone therapy after surgical premature menopause.
Recommendations for premature or early menopause, from a wide range of different medical societies including NAMS, are that women without contraindications be given estrogen-based hormone therapy until the average age of natural menopause. Though not included in the same guidance, research has also shown that estrogen after oophorectomy does not increase the risk of breast cancer in women with a BRCA1 mutation, Dr. Shufelt said. Hormone therapy for premature or early menopause should adequately replace the levels women have lost and that means younger menopausal women often need higher doses than what older women receive, such as 2 mg/day of oral estradiol rather than the standard doses of 0.5 or 1 mg/day.
Functional hypothalamic amenorrhea and cardiovascular risk
Dr. Shufelt then discussed functional hypothalamic amenorrhea (hypogonadotropic hypogonadism), a common type of secondary amenorrhea that affects at least 1.4 million U.S. women. Diagnosis includes lack of a period for at least 3 months in someone who previously menstruated plus lab values below 50 pg/mL for estradiol, below 10 mIU/L for follicle stimulating hormone, and below 10 mIU/L for luteinizing hormone. Causes of this reversible form of infertility can include stress, overexercising, undereating, or some combination of these, plus an underlying genetic predisposition.
“After ruling out polycystic ovary syndrome, prolactinoma, and thyroid dysfunction, clinicians need to consider the diagnosis of hypothalamic amenorrhea,” Dr. Shufelt said. This condition goes beyond low estrogen levels: Women have elevated cortisol, low thyroid levels, low leptin levels, and increased ghrelin.
”This is not going away,” Dr. Shufelt said, sharing data on stress levels among U.S. adults, particularly Gen Z and millennial adults, noting that the ongoing “national mental health crisis” may be contributing to functional hypothalamic amenorrhea.
A 2020 substudy from the Nurses’ Health Study II found an increased risk of premature death in those who didn’t have a period or always had irregular periods starting as early as 14-17 years old. The increased risk of premature death rose with age in those with irregular or absent cycles – a 37% higher risk in 18- to 22-year-olds and a 39% increased risk in 29- to 46-year-olds.
But clinicians aren’t adequately identifying the “phenotype of the hypothalamic women,” Dr. Shufelt said, despite research showing overlap between hypothalamic amenorrhea and a higher risk of cardiovascular disease. Hypothalamic amenorrhea is so understudied that the last original research on the topic was in 2008, Dr. Shufelt said in an interview. ”No research except mine has been done to evaluate heart health in these young women,” she said.
Dr. Shufelt described a study she led involving 30 women with functional hypothalamic amenorrhea, 29 women with normal menstrual cycles, and 30 women who were recently menopausal and not on hormone therapy. The women with hypothalamic amenorrhea had average stress levels but their depression scores were higher than those of the other two groups.
The results showed that women with hypothalamic amenorrhea had lower estradiol and leptin levels and higher testosterone levels compared with the control group, and they had higher cortisol levels than those of both groups. Despite having similar body mass indexes as the control and menopausal groups, women with hypothalamic amenorrhea had lower blood pressure than that of the other two groups, yet they had higher cholesterol levels than those of the control group. EndoPAT© (Itamar Medical) testing showed that they had poor vascular function.
“In fact, one-third of the women [with hypothalamic amenorrhea] entered the trial with a diagnosis of what would be considered endothelial dysfunction,” Dr. Shufelt said. “Our results demonstrated significantly higher circulating levels of serum proinflammatory cytokines in the women with hypothalamic amenorrhea compared to eumenorrheic controls.”
Dr. Shufelt’s team then tested whether giving estradiol to the women with hypothalamic amenorrhea for 12 weeks would improve their vascular health, but they saw no significant differences between the women who received estrogen and those who received placebo.
“Endothelial function is partly mediated by estrogen, and it was expected that giving back estrogen would ‘fix’ the endothelium, but that is not what happened,” Nanette Santoro, MD, professor and chair of obstetrics and gynecology at the University of Colorado at Denver, Aurora, said in interview. “The mechanisms that maintain vascular function in women are not limited to hormones,” said Dr. Santoro, who was not involved in Dr. Shufelt’s study but attended her lecture. “We need to think beyond the simple model of estrogen-good, no-estrogen-bad.”
Dr. Santoro noted how easy it is to overlook the women who may have cardiovascular risk because of hypothalamic amenorrhea.
“Because many women with functional hypothalamic amenorrhea are super athletic and do not have the typical features of people with cardiometabolic disease – such as glucose intolerance, obesity, abnormal cholesterol or triglycerides, or high blood pressure – clinicians tend to think of them as healthy and to think that simply giving back hormones will fix the problems with bone density and vascular function, but that is not enough,” Dr. Santoro said. “The cognitive-behavioral therapy model for treatment of women with functional hypothalamic amenorrhea addresses the stress-related factors that drive the disorder, and this needs to be considered the standard of care for treatment.”
Stephanie S. Faubion, MD, professor of medicine and director of Mayo Clinic’s Center for Women’s Health in Jacksonville, Fla., who was not involved in Dr. Shufelt’s presentation, also emphasized the importance of recognizing functional hypothalamic amenorrhea.
“This is an underrecognized entity to begin with, and the fact that these women appear to be at increased risk for vascular dysfunction and potentially increased risk for cardiovascular disease down the road makes it even more important for clinicians to identify them and provide interventions early on,” Dr. Faubion said in an interview. “These women need to be identified and the etiology of the amenorrhea addressed, whether it relates to overexercising, being underweight, or experiencing significant stressors that have led to the loss of menstrual cycles.”
Dr. Shufelt’s research was funded by the National Institutes of Health. She had no disclosures. Dr. Santoro is a member of the scientific advisory board for Astellas, Menogenix, Amazon Ember, and Que Oncology, and she consults for Ansh Labs. Dr. Faubion had no disclosures.
The relationship between estrogen levels and heart health makes it particularly important for clinicians to be aware of those patients who might be at risk for cardiovascular disease despite not having other traditional risk factors, according to a presentation Oct. 12 at the North American Menopause Society annual meeting in Atlanta.
”Endogenous estrogens are protective for cardiovascular disease in premenopausal women,” Chrisandra L. Shufelt, MD, chair of the division of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Fla., told attendees. Yet, “a substantial population of young women are dying prematurely from cardiovascular disease,” with rates of cardiovascular death increasing in women aged 35-44 even as rates have decreased in postmenopausal women and in men. One potential reason may be premature estrogen loss.
Dr. Shufelt reminded attendees of four major causes of premature estrogen loss: Natural premature menopause, surgical menopause, chemotherapy-induced menopause, and premature ovarian insufficiency. But she would go on to discuss a less widely recognized condition, functional hypothalamic amenorrhea, that also may be contributing to increased cardiovascular risk.
First, Dr. Shufelt reviewed the evidence supporting the relationship between estrogen and cardiovascular health, starting with the Framingham study’s findings that cardiovascular disease is approximately two to four times more common in postmenopausal women than in premenopausal women, depending on the age range.
“Menopause at an early age, particularly under the age of 40, matters,” Dr. Shufelt said. “So we should be discussing this with our patients.”
Surgical menopause makes a difference to cardiovascular health as well, she said. In women under age 35, for example, the risk of a nonfatal heart attack in those with a bilateral oophorectomy was 7.7 times greater than in women who retained both ovaries and their uterus, and 1.5 times greater in women who had a hysterectomy without bilateral oophorectomy.
In a 2019 study, surgical premature menopause was associated with an 87% increased risk of heart disease even after researchers accounted for age, cardiovascular risk factors, and some forms of hormone therapy. The increased risk from natural premature menopause, on the other hand, was lower – a 36% increased risk of heart disease – compared with those producing endogenous hormones. Although randomized controlled trials are unavailable and unlikely to be done, the Nurses’ Health Study and the Danish Nurses Cohort Study, both observational studies, found that heart disease risk was diminished in those taking hormone therapy after surgical premature menopause.
Recommendations for premature or early menopause, from a wide range of different medical societies including NAMS, are that women without contraindications be given estrogen-based hormone therapy until the average age of natural menopause. Though not included in the same guidance, research has also shown that estrogen after oophorectomy does not increase the risk of breast cancer in women with a BRCA1 mutation, Dr. Shufelt said. Hormone therapy for premature or early menopause should adequately replace the levels women have lost and that means younger menopausal women often need higher doses than what older women receive, such as 2 mg/day of oral estradiol rather than the standard doses of 0.5 or 1 mg/day.
Functional hypothalamic amenorrhea and cardiovascular risk
Dr. Shufelt then discussed functional hypothalamic amenorrhea (hypogonadotropic hypogonadism), a common type of secondary amenorrhea that affects at least 1.4 million U.S. women. Diagnosis includes lack of a period for at least 3 months in someone who previously menstruated plus lab values below 50 pg/mL for estradiol, below 10 mIU/L for follicle stimulating hormone, and below 10 mIU/L for luteinizing hormone. Causes of this reversible form of infertility can include stress, overexercising, undereating, or some combination of these, plus an underlying genetic predisposition.
“After ruling out polycystic ovary syndrome, prolactinoma, and thyroid dysfunction, clinicians need to consider the diagnosis of hypothalamic amenorrhea,” Dr. Shufelt said. This condition goes beyond low estrogen levels: Women have elevated cortisol, low thyroid levels, low leptin levels, and increased ghrelin.
”This is not going away,” Dr. Shufelt said, sharing data on stress levels among U.S. adults, particularly Gen Z and millennial adults, noting that the ongoing “national mental health crisis” may be contributing to functional hypothalamic amenorrhea.
A 2020 substudy from the Nurses’ Health Study II found an increased risk of premature death in those who didn’t have a period or always had irregular periods starting as early as 14-17 years old. The increased risk of premature death rose with age in those with irregular or absent cycles – a 37% higher risk in 18- to 22-year-olds and a 39% increased risk in 29- to 46-year-olds.
But clinicians aren’t adequately identifying the “phenotype of the hypothalamic women,” Dr. Shufelt said, despite research showing overlap between hypothalamic amenorrhea and a higher risk of cardiovascular disease. Hypothalamic amenorrhea is so understudied that the last original research on the topic was in 2008, Dr. Shufelt said in an interview. ”No research except mine has been done to evaluate heart health in these young women,” she said.
Dr. Shufelt described a study she led involving 30 women with functional hypothalamic amenorrhea, 29 women with normal menstrual cycles, and 30 women who were recently menopausal and not on hormone therapy. The women with hypothalamic amenorrhea had average stress levels but their depression scores were higher than those of the other two groups.
The results showed that women with hypothalamic amenorrhea had lower estradiol and leptin levels and higher testosterone levels compared with the control group, and they had higher cortisol levels than those of both groups. Despite having similar body mass indexes as the control and menopausal groups, women with hypothalamic amenorrhea had lower blood pressure than that of the other two groups, yet they had higher cholesterol levels than those of the control group. EndoPAT© (Itamar Medical) testing showed that they had poor vascular function.
“In fact, one-third of the women [with hypothalamic amenorrhea] entered the trial with a diagnosis of what would be considered endothelial dysfunction,” Dr. Shufelt said. “Our results demonstrated significantly higher circulating levels of serum proinflammatory cytokines in the women with hypothalamic amenorrhea compared to eumenorrheic controls.”
Dr. Shufelt’s team then tested whether giving estradiol to the women with hypothalamic amenorrhea for 12 weeks would improve their vascular health, but they saw no significant differences between the women who received estrogen and those who received placebo.
“Endothelial function is partly mediated by estrogen, and it was expected that giving back estrogen would ‘fix’ the endothelium, but that is not what happened,” Nanette Santoro, MD, professor and chair of obstetrics and gynecology at the University of Colorado at Denver, Aurora, said in interview. “The mechanisms that maintain vascular function in women are not limited to hormones,” said Dr. Santoro, who was not involved in Dr. Shufelt’s study but attended her lecture. “We need to think beyond the simple model of estrogen-good, no-estrogen-bad.”
Dr. Santoro noted how easy it is to overlook the women who may have cardiovascular risk because of hypothalamic amenorrhea.
“Because many women with functional hypothalamic amenorrhea are super athletic and do not have the typical features of people with cardiometabolic disease – such as glucose intolerance, obesity, abnormal cholesterol or triglycerides, or high blood pressure – clinicians tend to think of them as healthy and to think that simply giving back hormones will fix the problems with bone density and vascular function, but that is not enough,” Dr. Santoro said. “The cognitive-behavioral therapy model for treatment of women with functional hypothalamic amenorrhea addresses the stress-related factors that drive the disorder, and this needs to be considered the standard of care for treatment.”
Stephanie S. Faubion, MD, professor of medicine and director of Mayo Clinic’s Center for Women’s Health in Jacksonville, Fla., who was not involved in Dr. Shufelt’s presentation, also emphasized the importance of recognizing functional hypothalamic amenorrhea.
“This is an underrecognized entity to begin with, and the fact that these women appear to be at increased risk for vascular dysfunction and potentially increased risk for cardiovascular disease down the road makes it even more important for clinicians to identify them and provide interventions early on,” Dr. Faubion said in an interview. “These women need to be identified and the etiology of the amenorrhea addressed, whether it relates to overexercising, being underweight, or experiencing significant stressors that have led to the loss of menstrual cycles.”
Dr. Shufelt’s research was funded by the National Institutes of Health. She had no disclosures. Dr. Santoro is a member of the scientific advisory board for Astellas, Menogenix, Amazon Ember, and Que Oncology, and she consults for Ansh Labs. Dr. Faubion had no disclosures.
The relationship between estrogen levels and heart health makes it particularly important for clinicians to be aware of those patients who might be at risk for cardiovascular disease despite not having other traditional risk factors, according to a presentation Oct. 12 at the North American Menopause Society annual meeting in Atlanta.
”Endogenous estrogens are protective for cardiovascular disease in premenopausal women,” Chrisandra L. Shufelt, MD, chair of the division of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Fla., told attendees. Yet, “a substantial population of young women are dying prematurely from cardiovascular disease,” with rates of cardiovascular death increasing in women aged 35-44 even as rates have decreased in postmenopausal women and in men. One potential reason may be premature estrogen loss.
Dr. Shufelt reminded attendees of four major causes of premature estrogen loss: Natural premature menopause, surgical menopause, chemotherapy-induced menopause, and premature ovarian insufficiency. But she would go on to discuss a less widely recognized condition, functional hypothalamic amenorrhea, that also may be contributing to increased cardiovascular risk.
First, Dr. Shufelt reviewed the evidence supporting the relationship between estrogen and cardiovascular health, starting with the Framingham study’s findings that cardiovascular disease is approximately two to four times more common in postmenopausal women than in premenopausal women, depending on the age range.
“Menopause at an early age, particularly under the age of 40, matters,” Dr. Shufelt said. “So we should be discussing this with our patients.”
Surgical menopause makes a difference to cardiovascular health as well, she said. In women under age 35, for example, the risk of a nonfatal heart attack in those with a bilateral oophorectomy was 7.7 times greater than in women who retained both ovaries and their uterus, and 1.5 times greater in women who had a hysterectomy without bilateral oophorectomy.
In a 2019 study, surgical premature menopause was associated with an 87% increased risk of heart disease even after researchers accounted for age, cardiovascular risk factors, and some forms of hormone therapy. The increased risk from natural premature menopause, on the other hand, was lower – a 36% increased risk of heart disease – compared with those producing endogenous hormones. Although randomized controlled trials are unavailable and unlikely to be done, the Nurses’ Health Study and the Danish Nurses Cohort Study, both observational studies, found that heart disease risk was diminished in those taking hormone therapy after surgical premature menopause.
Recommendations for premature or early menopause, from a wide range of different medical societies including NAMS, are that women without contraindications be given estrogen-based hormone therapy until the average age of natural menopause. Though not included in the same guidance, research has also shown that estrogen after oophorectomy does not increase the risk of breast cancer in women with a BRCA1 mutation, Dr. Shufelt said. Hormone therapy for premature or early menopause should adequately replace the levels women have lost and that means younger menopausal women often need higher doses than what older women receive, such as 2 mg/day of oral estradiol rather than the standard doses of 0.5 or 1 mg/day.
Functional hypothalamic amenorrhea and cardiovascular risk
Dr. Shufelt then discussed functional hypothalamic amenorrhea (hypogonadotropic hypogonadism), a common type of secondary amenorrhea that affects at least 1.4 million U.S. women. Diagnosis includes lack of a period for at least 3 months in someone who previously menstruated plus lab values below 50 pg/mL for estradiol, below 10 mIU/L for follicle stimulating hormone, and below 10 mIU/L for luteinizing hormone. Causes of this reversible form of infertility can include stress, overexercising, undereating, or some combination of these, plus an underlying genetic predisposition.
“After ruling out polycystic ovary syndrome, prolactinoma, and thyroid dysfunction, clinicians need to consider the diagnosis of hypothalamic amenorrhea,” Dr. Shufelt said. This condition goes beyond low estrogen levels: Women have elevated cortisol, low thyroid levels, low leptin levels, and increased ghrelin.
”This is not going away,” Dr. Shufelt said, sharing data on stress levels among U.S. adults, particularly Gen Z and millennial adults, noting that the ongoing “national mental health crisis” may be contributing to functional hypothalamic amenorrhea.
A 2020 substudy from the Nurses’ Health Study II found an increased risk of premature death in those who didn’t have a period or always had irregular periods starting as early as 14-17 years old. The increased risk of premature death rose with age in those with irregular or absent cycles – a 37% higher risk in 18- to 22-year-olds and a 39% increased risk in 29- to 46-year-olds.
But clinicians aren’t adequately identifying the “phenotype of the hypothalamic women,” Dr. Shufelt said, despite research showing overlap between hypothalamic amenorrhea and a higher risk of cardiovascular disease. Hypothalamic amenorrhea is so understudied that the last original research on the topic was in 2008, Dr. Shufelt said in an interview. ”No research except mine has been done to evaluate heart health in these young women,” she said.
Dr. Shufelt described a study she led involving 30 women with functional hypothalamic amenorrhea, 29 women with normal menstrual cycles, and 30 women who were recently menopausal and not on hormone therapy. The women with hypothalamic amenorrhea had average stress levels but their depression scores were higher than those of the other two groups.
The results showed that women with hypothalamic amenorrhea had lower estradiol and leptin levels and higher testosterone levels compared with the control group, and they had higher cortisol levels than those of both groups. Despite having similar body mass indexes as the control and menopausal groups, women with hypothalamic amenorrhea had lower blood pressure than that of the other two groups, yet they had higher cholesterol levels than those of the control group. EndoPAT© (Itamar Medical) testing showed that they had poor vascular function.
“In fact, one-third of the women [with hypothalamic amenorrhea] entered the trial with a diagnosis of what would be considered endothelial dysfunction,” Dr. Shufelt said. “Our results demonstrated significantly higher circulating levels of serum proinflammatory cytokines in the women with hypothalamic amenorrhea compared to eumenorrheic controls.”
Dr. Shufelt’s team then tested whether giving estradiol to the women with hypothalamic amenorrhea for 12 weeks would improve their vascular health, but they saw no significant differences between the women who received estrogen and those who received placebo.
“Endothelial function is partly mediated by estrogen, and it was expected that giving back estrogen would ‘fix’ the endothelium, but that is not what happened,” Nanette Santoro, MD, professor and chair of obstetrics and gynecology at the University of Colorado at Denver, Aurora, said in interview. “The mechanisms that maintain vascular function in women are not limited to hormones,” said Dr. Santoro, who was not involved in Dr. Shufelt’s study but attended her lecture. “We need to think beyond the simple model of estrogen-good, no-estrogen-bad.”
Dr. Santoro noted how easy it is to overlook the women who may have cardiovascular risk because of hypothalamic amenorrhea.
“Because many women with functional hypothalamic amenorrhea are super athletic and do not have the typical features of people with cardiometabolic disease – such as glucose intolerance, obesity, abnormal cholesterol or triglycerides, or high blood pressure – clinicians tend to think of them as healthy and to think that simply giving back hormones will fix the problems with bone density and vascular function, but that is not enough,” Dr. Santoro said. “The cognitive-behavioral therapy model for treatment of women with functional hypothalamic amenorrhea addresses the stress-related factors that drive the disorder, and this needs to be considered the standard of care for treatment.”
Stephanie S. Faubion, MD, professor of medicine and director of Mayo Clinic’s Center for Women’s Health in Jacksonville, Fla., who was not involved in Dr. Shufelt’s presentation, also emphasized the importance of recognizing functional hypothalamic amenorrhea.
“This is an underrecognized entity to begin with, and the fact that these women appear to be at increased risk for vascular dysfunction and potentially increased risk for cardiovascular disease down the road makes it even more important for clinicians to identify them and provide interventions early on,” Dr. Faubion said in an interview. “These women need to be identified and the etiology of the amenorrhea addressed, whether it relates to overexercising, being underweight, or experiencing significant stressors that have led to the loss of menstrual cycles.”
Dr. Shufelt’s research was funded by the National Institutes of Health. She had no disclosures. Dr. Santoro is a member of the scientific advisory board for Astellas, Menogenix, Amazon Ember, and Que Oncology, and she consults for Ansh Labs. Dr. Faubion had no disclosures.
FROM NAMS 2022
Remote assessment of atopic dermatitis is feasible with patient-provided images: Study
MONTREAL – , as well as the possibility of conducting remote clinical trials that would be less expensive and less burdensome for participants, according to investigators, who presented the study at the annual meeting of the International Society of Atopic Dermatitis.
Still, practical barriers need to be addressed, particularly the problem of image quality, noted study investigator Aviël Ragamin, MD, from the department of dermatology, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
“Good-quality images are crucial, [and] in our study, patients didn’t have any incentive to provide images because they had already received their medical consultation,” he explained. He suggested that this problem could be overcome by providing technical support for patients and compensation for trial participants.
The study included 87 children (median age, 7 years), who were assessed for AD severity at an academic outpatient clinic. The in-person visit included assessment with the Eczema Area and Severity Index (EASI) score, as well as the collection of whole-body clinical images. Parents were then asked to return home and to provide their own clinical images and self-administered EASI assessments of their child for comparison. Four raters were asked to rate all images twice and to compare in-clinic and self-administered EASI scores based on the images.
At the in-clinic visit, the median EASI score of the group was 8.8. The majority of patients had moderate (46.6%) or severe (14.8%) AD. Roughly 40% of the patients had darker skin (Fitzpatrick skin types IV–VI).
Using Spearman rank correlation of 1,534 in-clinic and 425 patient-provided images, the study found good inter- and intra-rater reliability for clinical image assessment and strong agreement between images and the in-clinic EASI scores. The top outliers in the assessment were individuals with either darker skin or significant postinflammatory hyperpigmentation, which are “the most difficult cases to rate, based on images,” Dr. Ragamin noted.
There was only moderate correlation between the in-clinic and self-administered EASI scores, with a significant number of patients either underestimating or overestimating their AD severity, he added.
Overall, the main problem with remote assessment seems to be the feasibility of patients providing images, said Dr. Ragamin. Only 36.8% of parents provided any images at all, and of these, 1 of 5 were deemed too blurry, leaving just 13 for final assessment, he explained.
“Pragmatically, it’s tricky,” said Aaron Drucker, MD, a dermatologist at Women’s College Hospital and associate professor at the University of Toronto, who was asked to comment on the study. “It takes long enough to do an EASI score in person, let alone looking through blurry pictures that take too long to load into your electronic medical record. We know it works, but when our hospital went virtual [during the COVID pandemic] ... most of my patients with chronic eczema weren’t even sending me pictures.”
Regarding the utility of remote, full-body photography in clinical practice, he said, “There’s too many feasibility hoops to jump through at this point. The most promise I see is for clinical trials, where it’s hard to get people to come in.”
Dr. Ragamin and Dr. Drucker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , as well as the possibility of conducting remote clinical trials that would be less expensive and less burdensome for participants, according to investigators, who presented the study at the annual meeting of the International Society of Atopic Dermatitis.
Still, practical barriers need to be addressed, particularly the problem of image quality, noted study investigator Aviël Ragamin, MD, from the department of dermatology, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
“Good-quality images are crucial, [and] in our study, patients didn’t have any incentive to provide images because they had already received their medical consultation,” he explained. He suggested that this problem could be overcome by providing technical support for patients and compensation for trial participants.
The study included 87 children (median age, 7 years), who were assessed for AD severity at an academic outpatient clinic. The in-person visit included assessment with the Eczema Area and Severity Index (EASI) score, as well as the collection of whole-body clinical images. Parents were then asked to return home and to provide their own clinical images and self-administered EASI assessments of their child for comparison. Four raters were asked to rate all images twice and to compare in-clinic and self-administered EASI scores based on the images.
At the in-clinic visit, the median EASI score of the group was 8.8. The majority of patients had moderate (46.6%) or severe (14.8%) AD. Roughly 40% of the patients had darker skin (Fitzpatrick skin types IV–VI).
Using Spearman rank correlation of 1,534 in-clinic and 425 patient-provided images, the study found good inter- and intra-rater reliability for clinical image assessment and strong agreement between images and the in-clinic EASI scores. The top outliers in the assessment were individuals with either darker skin or significant postinflammatory hyperpigmentation, which are “the most difficult cases to rate, based on images,” Dr. Ragamin noted.
There was only moderate correlation between the in-clinic and self-administered EASI scores, with a significant number of patients either underestimating or overestimating their AD severity, he added.
Overall, the main problem with remote assessment seems to be the feasibility of patients providing images, said Dr. Ragamin. Only 36.8% of parents provided any images at all, and of these, 1 of 5 were deemed too blurry, leaving just 13 for final assessment, he explained.
“Pragmatically, it’s tricky,” said Aaron Drucker, MD, a dermatologist at Women’s College Hospital and associate professor at the University of Toronto, who was asked to comment on the study. “It takes long enough to do an EASI score in person, let alone looking through blurry pictures that take too long to load into your electronic medical record. We know it works, but when our hospital went virtual [during the COVID pandemic] ... most of my patients with chronic eczema weren’t even sending me pictures.”
Regarding the utility of remote, full-body photography in clinical practice, he said, “There’s too many feasibility hoops to jump through at this point. The most promise I see is for clinical trials, where it’s hard to get people to come in.”
Dr. Ragamin and Dr. Drucker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , as well as the possibility of conducting remote clinical trials that would be less expensive and less burdensome for participants, according to investigators, who presented the study at the annual meeting of the International Society of Atopic Dermatitis.
Still, practical barriers need to be addressed, particularly the problem of image quality, noted study investigator Aviël Ragamin, MD, from the department of dermatology, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
“Good-quality images are crucial, [and] in our study, patients didn’t have any incentive to provide images because they had already received their medical consultation,” he explained. He suggested that this problem could be overcome by providing technical support for patients and compensation for trial participants.
The study included 87 children (median age, 7 years), who were assessed for AD severity at an academic outpatient clinic. The in-person visit included assessment with the Eczema Area and Severity Index (EASI) score, as well as the collection of whole-body clinical images. Parents were then asked to return home and to provide their own clinical images and self-administered EASI assessments of their child for comparison. Four raters were asked to rate all images twice and to compare in-clinic and self-administered EASI scores based on the images.
At the in-clinic visit, the median EASI score of the group was 8.8. The majority of patients had moderate (46.6%) or severe (14.8%) AD. Roughly 40% of the patients had darker skin (Fitzpatrick skin types IV–VI).
Using Spearman rank correlation of 1,534 in-clinic and 425 patient-provided images, the study found good inter- and intra-rater reliability for clinical image assessment and strong agreement between images and the in-clinic EASI scores. The top outliers in the assessment were individuals with either darker skin or significant postinflammatory hyperpigmentation, which are “the most difficult cases to rate, based on images,” Dr. Ragamin noted.
There was only moderate correlation between the in-clinic and self-administered EASI scores, with a significant number of patients either underestimating or overestimating their AD severity, he added.
Overall, the main problem with remote assessment seems to be the feasibility of patients providing images, said Dr. Ragamin. Only 36.8% of parents provided any images at all, and of these, 1 of 5 were deemed too blurry, leaving just 13 for final assessment, he explained.
“Pragmatically, it’s tricky,” said Aaron Drucker, MD, a dermatologist at Women’s College Hospital and associate professor at the University of Toronto, who was asked to comment on the study. “It takes long enough to do an EASI score in person, let alone looking through blurry pictures that take too long to load into your electronic medical record. We know it works, but when our hospital went virtual [during the COVID pandemic] ... most of my patients with chronic eczema weren’t even sending me pictures.”
Regarding the utility of remote, full-body photography in clinical practice, he said, “There’s too many feasibility hoops to jump through at this point. The most promise I see is for clinical trials, where it’s hard to get people to come in.”
Dr. Ragamin and Dr. Drucker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Study reveals racial disparities in advanced HF therapies
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”

Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”
Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”
Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
How can I keep from losing my mind?
A) Thiamine
B) Vitamin E
C) Multivitamin (MV)
D) Keto diet
E) Red wine
FDA-approved therapies for dementia
To date the actual therapies for dementia have been disappointing. Donepezil, the most prescribed medication for the treatment of dementia has a number-needed-to treat (NNT) over 17, and causes frequent side effects. Aducanumab was recently approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD), but controversy has arisen, as the clinical results were modest, and the price tag will be large – estimated at $30,000-$50,000/year.
Preventive options that may decrease the likelihood of dementia
Patients often ask the question stated above. Regarding how to respond to that question, choice C, MV, has some recent evidence of benefit. Baker and colleagues studied the effect of cocoa extract and multivitamins on cognitive function in the COSMOS-Mind trial.1 A total of 2,262 people were enrolled, and over 90% completed baseline and at least one annual cognitive assessment. Cocoa extract had no impact on global cognition (confidence interval [CI], –.02-.08, P = .28), but MV supplementation did have a statistically significant impact on global cognition (CI, .02-.12, P less than .007).

Vitamin E has been enthusiastically endorsed in the past as a treatment to prevent cognitive decline. The most recent Cochrane review on vitamin E concluded there was no evidence that the alpha-tocopherol form of vitamin E given to people with MCI prevents progression to dementia, or that it improves cognitive function in people with MCI or dementia due to AD.2
Exercise has long been a mainstay of our advice to patients as something they can do to help prevent dementia. Yu and colleagues did a meta-analysis of almost 400 randomized controlled trials and observational studies to grade the evidence on different interventions.3 They gave exercise a grade B for evidence of benefit.
A recent study addressed this issue, and I think it is helpful on quantifying how much exercise is needed. Del Pozo Cruz and colleagues did a prospective population-based cohort study of 78,000 adults aged 40-79, with an average of 6.9 years of follow up.4 The optimal step count was 9,826 steps (hazard ratio [HR], 0.49; 95% CI, 0.39-0.62) and the minimal step count for benefit was 3,826 steps (HR, 0.75; 95% CI, 0.67-0.83).
Modifiable factors
The other major modifiable factors to consider are problems with special senses. Both vision loss and hearing loss have been associated with cognitive impairment.
Shang and colleagues published a meta-analysis of 14 cohort studies addressing vision impairment and cognitive function involving more than 6 million individuals.5 They concluded that vision impairment is associated with an increased risk of both dementia and cognitive impairment in older adults.
Loughrey and colleagues performed a meta-analysis of 36 studies addressing hearing loss and cognitive decline.6 They reported that, among cross-sectional studies, a significant association was found for cognitive impairment (odds ratio [OR], 2.00; 95% CI, 1.39-2.89) and dementia (OR, 2.42; 95% CI, 1.24-4.72). A similar finding was present in prospective cohort studies with a significant association being found for cognitive impairment (OR, 1.22; 95% CI, 1.09-1.36) and dementia (OR, 1.28; 95% CI, 1.02-1.59).
A 25-year prospective, population-based study of patients with hearing loss revealed a difference in the rate of change in MMSE score over the 25-year follow-up between participants with hearing loss not using hearing aids matched with controls who didn’t have hearing loss. Those with untreated hearing loss had more cognitive decline than that of patients without hearing loss.7 The subjects with hearing loss using a hearing aid had no difference in cognitive decline from controls.
Pearl
Several simple and safe interventions may protect our patients from cognitive decline. These include taking a daily multivitamin, walking more than 4,000 steps a day, and optimizing vision and hearing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. Baker LD et al. Effects of cocoa extract and a multivitamin on cognitive function: A randomized clinical trial. Alzheimer’s Dement. 2022 Sep 14. doi: 10.1002/alz.12767.
2. Farina N et al. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst Rev. 2017 Apr 18;4(4):CD002854. doi: 10.1002/14651858.CD002854.pub5.
3. Yu JT et al. Evidence-based prevention of Alzheimer’s disease: Systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-9.
4. Del Pozo Cruz B et al. Association of daily step count and intensity with incident dementia in 78,430 adults living in the UK. JAMA Neurol. 2022 Oct 1;79(10):1059-63.
5. Shang X et al. The association between vision impairment and incidence of dementia and cognitive impairment: A systematic review and meta-analysis. Ophthalmology. 2021 Aug;128(8):1135-49.
6. Loughrey DG et al. Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2018 Feb 1;144(2):115-26.
7. Amieva H et al. Self-reported hearing loss, hearing aids, and cognitive decline in elderly adults: A 25-year study. J Am Geriatr Soc. 2015 Oct;63(10):2099-104.
A) Thiamine
B) Vitamin E
C) Multivitamin (MV)
D) Keto diet
E) Red wine
FDA-approved therapies for dementia
To date the actual therapies for dementia have been disappointing. Donepezil, the most prescribed medication for the treatment of dementia has a number-needed-to treat (NNT) over 17, and causes frequent side effects. Aducanumab was recently approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD), but controversy has arisen, as the clinical results were modest, and the price tag will be large – estimated at $30,000-$50,000/year.
Preventive options that may decrease the likelihood of dementia
Patients often ask the question stated above. Regarding how to respond to that question, choice C, MV, has some recent evidence of benefit. Baker and colleagues studied the effect of cocoa extract and multivitamins on cognitive function in the COSMOS-Mind trial.1 A total of 2,262 people were enrolled, and over 90% completed baseline and at least one annual cognitive assessment. Cocoa extract had no impact on global cognition (confidence interval [CI], –.02-.08, P = .28), but MV supplementation did have a statistically significant impact on global cognition (CI, .02-.12, P less than .007).
Vitamin E has been enthusiastically endorsed in the past as a treatment to prevent cognitive decline. The most recent Cochrane review on vitamin E concluded there was no evidence that the alpha-tocopherol form of vitamin E given to people with MCI prevents progression to dementia, or that it improves cognitive function in people with MCI or dementia due to AD.2
Exercise has long been a mainstay of our advice to patients as something they can do to help prevent dementia. Yu and colleagues did a meta-analysis of almost 400 randomized controlled trials and observational studies to grade the evidence on different interventions.3 They gave exercise a grade B for evidence of benefit.
A recent study addressed this issue, and I think it is helpful on quantifying how much exercise is needed. Del Pozo Cruz and colleagues did a prospective population-based cohort study of 78,000 adults aged 40-79, with an average of 6.9 years of follow up.4 The optimal step count was 9,826 steps (hazard ratio [HR], 0.49; 95% CI, 0.39-0.62) and the minimal step count for benefit was 3,826 steps (HR, 0.75; 95% CI, 0.67-0.83).
Modifiable factors
The other major modifiable factors to consider are problems with special senses. Both vision loss and hearing loss have been associated with cognitive impairment.
Shang and colleagues published a meta-analysis of 14 cohort studies addressing vision impairment and cognitive function involving more than 6 million individuals.5 They concluded that vision impairment is associated with an increased risk of both dementia and cognitive impairment in older adults.
Loughrey and colleagues performed a meta-analysis of 36 studies addressing hearing loss and cognitive decline.6 They reported that, among cross-sectional studies, a significant association was found for cognitive impairment (odds ratio [OR], 2.00; 95% CI, 1.39-2.89) and dementia (OR, 2.42; 95% CI, 1.24-4.72). A similar finding was present in prospective cohort studies with a significant association being found for cognitive impairment (OR, 1.22; 95% CI, 1.09-1.36) and dementia (OR, 1.28; 95% CI, 1.02-1.59).
A 25-year prospective, population-based study of patients with hearing loss revealed a difference in the rate of change in MMSE score over the 25-year follow-up between participants with hearing loss not using hearing aids matched with controls who didn’t have hearing loss. Those with untreated hearing loss had more cognitive decline than that of patients without hearing loss.7 The subjects with hearing loss using a hearing aid had no difference in cognitive decline from controls.
Pearl
Several simple and safe interventions may protect our patients from cognitive decline. These include taking a daily multivitamin, walking more than 4,000 steps a day, and optimizing vision and hearing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. Baker LD et al. Effects of cocoa extract and a multivitamin on cognitive function: A randomized clinical trial. Alzheimer’s Dement. 2022 Sep 14. doi: 10.1002/alz.12767.
2. Farina N et al. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst Rev. 2017 Apr 18;4(4):CD002854. doi: 10.1002/14651858.CD002854.pub5.
3. Yu JT et al. Evidence-based prevention of Alzheimer’s disease: Systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-9.
4. Del Pozo Cruz B et al. Association of daily step count and intensity with incident dementia in 78,430 adults living in the UK. JAMA Neurol. 2022 Oct 1;79(10):1059-63.
5. Shang X et al. The association between vision impairment and incidence of dementia and cognitive impairment: A systematic review and meta-analysis. Ophthalmology. 2021 Aug;128(8):1135-49.
6. Loughrey DG et al. Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2018 Feb 1;144(2):115-26.
7. Amieva H et al. Self-reported hearing loss, hearing aids, and cognitive decline in elderly adults: A 25-year study. J Am Geriatr Soc. 2015 Oct;63(10):2099-104.
A) Thiamine
B) Vitamin E
C) Multivitamin (MV)
D) Keto diet
E) Red wine
FDA-approved therapies for dementia
To date the actual therapies for dementia have been disappointing. Donepezil, the most prescribed medication for the treatment of dementia has a number-needed-to treat (NNT) over 17, and causes frequent side effects. Aducanumab was recently approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD), but controversy has arisen, as the clinical results were modest, and the price tag will be large – estimated at $30,000-$50,000/year.
Preventive options that may decrease the likelihood of dementia
Patients often ask the question stated above. Regarding how to respond to that question, choice C, MV, has some recent evidence of benefit. Baker and colleagues studied the effect of cocoa extract and multivitamins on cognitive function in the COSMOS-Mind trial.1 A total of 2,262 people were enrolled, and over 90% completed baseline and at least one annual cognitive assessment. Cocoa extract had no impact on global cognition (confidence interval [CI], –.02-.08, P = .28), but MV supplementation did have a statistically significant impact on global cognition (CI, .02-.12, P less than .007).
Vitamin E has been enthusiastically endorsed in the past as a treatment to prevent cognitive decline. The most recent Cochrane review on vitamin E concluded there was no evidence that the alpha-tocopherol form of vitamin E given to people with MCI prevents progression to dementia, or that it improves cognitive function in people with MCI or dementia due to AD.2
Exercise has long been a mainstay of our advice to patients as something they can do to help prevent dementia. Yu and colleagues did a meta-analysis of almost 400 randomized controlled trials and observational studies to grade the evidence on different interventions.3 They gave exercise a grade B for evidence of benefit.
A recent study addressed this issue, and I think it is helpful on quantifying how much exercise is needed. Del Pozo Cruz and colleagues did a prospective population-based cohort study of 78,000 adults aged 40-79, with an average of 6.9 years of follow up.4 The optimal step count was 9,826 steps (hazard ratio [HR], 0.49; 95% CI, 0.39-0.62) and the minimal step count for benefit was 3,826 steps (HR, 0.75; 95% CI, 0.67-0.83).
Modifiable factors
The other major modifiable factors to consider are problems with special senses. Both vision loss and hearing loss have been associated with cognitive impairment.
Shang and colleagues published a meta-analysis of 14 cohort studies addressing vision impairment and cognitive function involving more than 6 million individuals.5 They concluded that vision impairment is associated with an increased risk of both dementia and cognitive impairment in older adults.
Loughrey and colleagues performed a meta-analysis of 36 studies addressing hearing loss and cognitive decline.6 They reported that, among cross-sectional studies, a significant association was found for cognitive impairment (odds ratio [OR], 2.00; 95% CI, 1.39-2.89) and dementia (OR, 2.42; 95% CI, 1.24-4.72). A similar finding was present in prospective cohort studies with a significant association being found for cognitive impairment (OR, 1.22; 95% CI, 1.09-1.36) and dementia (OR, 1.28; 95% CI, 1.02-1.59).
A 25-year prospective, population-based study of patients with hearing loss revealed a difference in the rate of change in MMSE score over the 25-year follow-up between participants with hearing loss not using hearing aids matched with controls who didn’t have hearing loss. Those with untreated hearing loss had more cognitive decline than that of patients without hearing loss.7 The subjects with hearing loss using a hearing aid had no difference in cognitive decline from controls.
Pearl
Several simple and safe interventions may protect our patients from cognitive decline. These include taking a daily multivitamin, walking more than 4,000 steps a day, and optimizing vision and hearing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. Baker LD et al. Effects of cocoa extract and a multivitamin on cognitive function: A randomized clinical trial. Alzheimer’s Dement. 2022 Sep 14. doi: 10.1002/alz.12767.
2. Farina N et al. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst Rev. 2017 Apr 18;4(4):CD002854. doi: 10.1002/14651858.CD002854.pub5.
3. Yu JT et al. Evidence-based prevention of Alzheimer’s disease: Systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-9.
4. Del Pozo Cruz B et al. Association of daily step count and intensity with incident dementia in 78,430 adults living in the UK. JAMA Neurol. 2022 Oct 1;79(10):1059-63.
5. Shang X et al. The association between vision impairment and incidence of dementia and cognitive impairment: A systematic review and meta-analysis. Ophthalmology. 2021 Aug;128(8):1135-49.
6. Loughrey DG et al. Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2018 Feb 1;144(2):115-26.
7. Amieva H et al. Self-reported hearing loss, hearing aids, and cognitive decline in elderly adults: A 25-year study. J Am Geriatr Soc. 2015 Oct;63(10):2099-104.