User login
Comorbidity rates remain stable over 10 years in childhood-onset epilepsy
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
REPORTING FROM AES 2019
Patient-reported outcomes highlight long-term impacts of prostatectomy
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
FROM JAMA
Key clinical point: For men with prostate cancer, prostatectomy is significantly more likely to cause long-term incontinence than are other treatment modalities.
Major finding: For each time point through 5 years, men with unfavorable-risk prostate cancer who underwent prostatectomy had significantly worse incontinence scores than did those who underwent external beam radiation therapy (EBRT) and androgen deprivation therapy (ADT) (adjusted mean difference, –23.2).
Study details: A prospective, population-based cohort study involving 2,005 men prostate cancer.
Disclosures: The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
Source: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
BET inhibitor exhibits activity in myelofibrosis
ORLANDO – The BET inhibitor CPI-0610, given alone or in combination with ruxolitinib, has demonstrated activity in a phase 2 trial of patients with relapsed/refractory myelofibrosis (MF).

Responses were best among transfusion-dependent patients who received CPI-0610 and ruxolitinib. All but one of these patients experienced symptom improvement.
In the monotherapy group, results were best among transfusion-independent patients. All of these patients had an improvement in Patient Global Impression of Change (PGIC) score, and most had a 50% or greater improvement in total symptom score (TSS).
John Mascarenhas, MD, of the Icahn School of Medicine at Mount Sinai, New York, presented these results from the phase 2 MANIFEST trial (NCT02158858) at the annual meeting of the American Society of Hematology.
Dr. Mascarenhas presented data on 90 patients – 59 with primary MF, 16 with post–polycythemia vera MF, 13 with post–essential thrombocythemia MF, and 2 whose type of MF was unknown. At baseline, the patients’ median age was 69 years and 76.7% of patients had received at least 6 months of ruxolitinib treatment.
Of the 36 patients who received CPI-0610 monotherapy, 34 were still receiving the treatment as of Oct. 17, 2019. Of the 54 patients treated with CPI-0610 and ruxolitinib, 41 were still receiving the combination at that time. The median duration of treatment was 11.3 weeks in the monotherapy arm and 25.9 weeks in the combination arm. Responses were assessed at 24 weeks.
“CPI-0610 monotherapy or added on to ruxolitinib in a relapsed/refractory MF population demonstrated antitumor activity, as evidenced by spleen and symptom improvement,” Dr. Mascarenhas said. “Symptom responses were observed in a majority of patients. We treated these patients, and they felt much better. It was impressive.”
Efficacy of monotherapy
There were two evaluable patients who had been transfusion dependent at baseline and received CPI-0610 monotherapy for at least 24 weeks. Neither patient achieved transfusion independence, and neither had a spleen volume reduction of at least 35% (SVR35). One patient had a 50% or greater improvement in TSS, and one had an improvement in PGIC score.
There were seven evaluable patients who were transfusion independent at baseline and received CPI-0610 for at least 24 weeks. None of these patients had an SVR35 response, three of five evaluable patients had a 50% or greater improvement in TSS, and all seven had an improvement in PGIC score.
Efficacy of the combination
There were 14 patients who had been transfusion dependent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. Six of these patients had become transfusion independent at week 24.
Among the patients who were transfusion dependent at baseline, 25% (3/12) had an SVR35 response at week 24, 54% (7/13) had a 50% or greater improvement in TSS, and 75% (9/12) had an improvement in PGIC score.
There were 13 evaluable patients who were transfusion independent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. None of these patients had an SVR35 response, 38% had a 50% or greater improvement in TSS, and 69% had an improvement in PGIC score.
Safety
“CPI-0610 monotherapy or as an add-on to [ruxolitinib] was generally well tolerated,” Dr. Mascarenhas said. “Thrombocytopenia was asymptomatic, generally reversible, and manageable. There were no other unanticipated safety concerns.”
All 90 patients were evaluable for safety. Hematologic adverse events included thrombocytopenia (23.3%) and anemia (8.9%).
The most common nonhematologic adverse events were diarrhea (32.2%), nausea (22.2%), cough (16.7%), fatigue (14.4%), vomiting (14.4%), and upper respiratory tract infection (14.4%).
Eight patients (8.9%) experienced grade 4 adverse events, but all events resolved. Four events occurred in the monotherapy arm, and one (rash) required dose interruption. Of the four events in the combination arm, one (anemia) was considered treatment related.
There were three fatal adverse events – acute kidney injury, traumatic subdural hematoma, and brain stem hemorrhage. None of these events were considered related to CPI-0610.
Based on these preliminary results, the cohort of transfusion-dependent patients receiving CPI-0610 and ruxolitinib has been expanded. A cohort of ruxolitinib-naive patients receiving CPI-0610 and ruxolitinib has been expanded as well.
The MANIFEST trial is funded by Constellation Pharmaceuticals in collaboration with the Leukemia & Lymphoma Society. Dr. Mascarenhas reported relationships with Incyte, Janssen, CTI Biopharma, Novartis, Roche, Merck, Celgene, Promedior, Merus, and PharmaEssentia.
SOURCE: Mascarenhas J et al. ASH 2019, Abstract 670.
ORLANDO – The BET inhibitor CPI-0610, given alone or in combination with ruxolitinib, has demonstrated activity in a phase 2 trial of patients with relapsed/refractory myelofibrosis (MF).
Responses were best among transfusion-dependent patients who received CPI-0610 and ruxolitinib. All but one of these patients experienced symptom improvement.
In the monotherapy group, results were best among transfusion-independent patients. All of these patients had an improvement in Patient Global Impression of Change (PGIC) score, and most had a 50% or greater improvement in total symptom score (TSS).
John Mascarenhas, MD, of the Icahn School of Medicine at Mount Sinai, New York, presented these results from the phase 2 MANIFEST trial (NCT02158858) at the annual meeting of the American Society of Hematology.
Dr. Mascarenhas presented data on 90 patients – 59 with primary MF, 16 with post–polycythemia vera MF, 13 with post–essential thrombocythemia MF, and 2 whose type of MF was unknown. At baseline, the patients’ median age was 69 years and 76.7% of patients had received at least 6 months of ruxolitinib treatment.
Of the 36 patients who received CPI-0610 monotherapy, 34 were still receiving the treatment as of Oct. 17, 2019. Of the 54 patients treated with CPI-0610 and ruxolitinib, 41 were still receiving the combination at that time. The median duration of treatment was 11.3 weeks in the monotherapy arm and 25.9 weeks in the combination arm. Responses were assessed at 24 weeks.
“CPI-0610 monotherapy or added on to ruxolitinib in a relapsed/refractory MF population demonstrated antitumor activity, as evidenced by spleen and symptom improvement,” Dr. Mascarenhas said. “Symptom responses were observed in a majority of patients. We treated these patients, and they felt much better. It was impressive.”
Efficacy of monotherapy
There were two evaluable patients who had been transfusion dependent at baseline and received CPI-0610 monotherapy for at least 24 weeks. Neither patient achieved transfusion independence, and neither had a spleen volume reduction of at least 35% (SVR35). One patient had a 50% or greater improvement in TSS, and one had an improvement in PGIC score.
There were seven evaluable patients who were transfusion independent at baseline and received CPI-0610 for at least 24 weeks. None of these patients had an SVR35 response, three of five evaluable patients had a 50% or greater improvement in TSS, and all seven had an improvement in PGIC score.
Efficacy of the combination
There were 14 patients who had been transfusion dependent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. Six of these patients had become transfusion independent at week 24.
Among the patients who were transfusion dependent at baseline, 25% (3/12) had an SVR35 response at week 24, 54% (7/13) had a 50% or greater improvement in TSS, and 75% (9/12) had an improvement in PGIC score.
There were 13 evaluable patients who were transfusion independent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. None of these patients had an SVR35 response, 38% had a 50% or greater improvement in TSS, and 69% had an improvement in PGIC score.
Safety
“CPI-0610 monotherapy or as an add-on to [ruxolitinib] was generally well tolerated,” Dr. Mascarenhas said. “Thrombocytopenia was asymptomatic, generally reversible, and manageable. There were no other unanticipated safety concerns.”
All 90 patients were evaluable for safety. Hematologic adverse events included thrombocytopenia (23.3%) and anemia (8.9%).
The most common nonhematologic adverse events were diarrhea (32.2%), nausea (22.2%), cough (16.7%), fatigue (14.4%), vomiting (14.4%), and upper respiratory tract infection (14.4%).
Eight patients (8.9%) experienced grade 4 adverse events, but all events resolved. Four events occurred in the monotherapy arm, and one (rash) required dose interruption. Of the four events in the combination arm, one (anemia) was considered treatment related.
There were three fatal adverse events – acute kidney injury, traumatic subdural hematoma, and brain stem hemorrhage. None of these events were considered related to CPI-0610.
Based on these preliminary results, the cohort of transfusion-dependent patients receiving CPI-0610 and ruxolitinib has been expanded. A cohort of ruxolitinib-naive patients receiving CPI-0610 and ruxolitinib has been expanded as well.
The MANIFEST trial is funded by Constellation Pharmaceuticals in collaboration with the Leukemia & Lymphoma Society. Dr. Mascarenhas reported relationships with Incyte, Janssen, CTI Biopharma, Novartis, Roche, Merck, Celgene, Promedior, Merus, and PharmaEssentia.
SOURCE: Mascarenhas J et al. ASH 2019, Abstract 670.
ORLANDO – The BET inhibitor CPI-0610, given alone or in combination with ruxolitinib, has demonstrated activity in a phase 2 trial of patients with relapsed/refractory myelofibrosis (MF).
Responses were best among transfusion-dependent patients who received CPI-0610 and ruxolitinib. All but one of these patients experienced symptom improvement.
In the monotherapy group, results were best among transfusion-independent patients. All of these patients had an improvement in Patient Global Impression of Change (PGIC) score, and most had a 50% or greater improvement in total symptom score (TSS).
John Mascarenhas, MD, of the Icahn School of Medicine at Mount Sinai, New York, presented these results from the phase 2 MANIFEST trial (NCT02158858) at the annual meeting of the American Society of Hematology.
Dr. Mascarenhas presented data on 90 patients – 59 with primary MF, 16 with post–polycythemia vera MF, 13 with post–essential thrombocythemia MF, and 2 whose type of MF was unknown. At baseline, the patients’ median age was 69 years and 76.7% of patients had received at least 6 months of ruxolitinib treatment.
Of the 36 patients who received CPI-0610 monotherapy, 34 were still receiving the treatment as of Oct. 17, 2019. Of the 54 patients treated with CPI-0610 and ruxolitinib, 41 were still receiving the combination at that time. The median duration of treatment was 11.3 weeks in the monotherapy arm and 25.9 weeks in the combination arm. Responses were assessed at 24 weeks.
“CPI-0610 monotherapy or added on to ruxolitinib in a relapsed/refractory MF population demonstrated antitumor activity, as evidenced by spleen and symptom improvement,” Dr. Mascarenhas said. “Symptom responses were observed in a majority of patients. We treated these patients, and they felt much better. It was impressive.”
Efficacy of monotherapy
There were two evaluable patients who had been transfusion dependent at baseline and received CPI-0610 monotherapy for at least 24 weeks. Neither patient achieved transfusion independence, and neither had a spleen volume reduction of at least 35% (SVR35). One patient had a 50% or greater improvement in TSS, and one had an improvement in PGIC score.
There were seven evaluable patients who were transfusion independent at baseline and received CPI-0610 for at least 24 weeks. None of these patients had an SVR35 response, three of five evaluable patients had a 50% or greater improvement in TSS, and all seven had an improvement in PGIC score.
Efficacy of the combination
There were 14 patients who had been transfusion dependent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. Six of these patients had become transfusion independent at week 24.
Among the patients who were transfusion dependent at baseline, 25% (3/12) had an SVR35 response at week 24, 54% (7/13) had a 50% or greater improvement in TSS, and 75% (9/12) had an improvement in PGIC score.
There were 13 evaluable patients who were transfusion independent at baseline and received CPI-0610 and ruxolitinib for at least 24 weeks. None of these patients had an SVR35 response, 38% had a 50% or greater improvement in TSS, and 69% had an improvement in PGIC score.
Safety
“CPI-0610 monotherapy or as an add-on to [ruxolitinib] was generally well tolerated,” Dr. Mascarenhas said. “Thrombocytopenia was asymptomatic, generally reversible, and manageable. There were no other unanticipated safety concerns.”
All 90 patients were evaluable for safety. Hematologic adverse events included thrombocytopenia (23.3%) and anemia (8.9%).
The most common nonhematologic adverse events were diarrhea (32.2%), nausea (22.2%), cough (16.7%), fatigue (14.4%), vomiting (14.4%), and upper respiratory tract infection (14.4%).
Eight patients (8.9%) experienced grade 4 adverse events, but all events resolved. Four events occurred in the monotherapy arm, and one (rash) required dose interruption. Of the four events in the combination arm, one (anemia) was considered treatment related.
There were three fatal adverse events – acute kidney injury, traumatic subdural hematoma, and brain stem hemorrhage. None of these events were considered related to CPI-0610.
Based on these preliminary results, the cohort of transfusion-dependent patients receiving CPI-0610 and ruxolitinib has been expanded. A cohort of ruxolitinib-naive patients receiving CPI-0610 and ruxolitinib has been expanded as well.
The MANIFEST trial is funded by Constellation Pharmaceuticals in collaboration with the Leukemia & Lymphoma Society. Dr. Mascarenhas reported relationships with Incyte, Janssen, CTI Biopharma, Novartis, Roche, Merck, Celgene, Promedior, Merus, and PharmaEssentia.
SOURCE: Mascarenhas J et al. ASH 2019, Abstract 670.
REPORTING FROM ASH 2019
NCCN guidelines highlight ‘complicated’ treatment for pediatric lymphomas
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.

“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.
“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.
“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
Half of SLE patients have incident neuropsychiatric events
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
FROM ANNALS OF THE RHEUMATIC DISEASES
9/11 responders show increased risk of leukemia, other cancers
New data suggest an increased risk of leukemia among responders who worked at the World Trade Center site after the attacks on Sept. 11, 2001.

Previous studies have shown that 9/11 responders have a higher incidence of cancers than does the general population. The current study is the first to show a higher incidence of leukemia among responders. It also shows a higher incidence of thyroid and prostate cancers as well as all cancer types combined.
These findings were published in JNCI Cancer Spectrum.
“This study showed increased incidence of several cancer types compared to previously conducted studies with shorter follow-up periods,” study author Susan L, Teitelbaum, PhD, of the Icahn School of Medicine at Mount Sinai, New York, said in a press release.
“Because of the long latency period of many types of cancer, it is possible that increased rates of other cancers, as well as World Trade Center exposure health issues, may emerge after longer periods of study.”
Dr. Teitelbaum and colleagues evaluated responders enrolled in the World Trade Center Health Program General Responder Cohort from when it was established in July 2002 through the end of follow-up, which was Dec. 31, 2013, for New York residents and Dec. 31, 2012, for residents of other states.
To be eligible for the cohort, responders must have worked on the World Trade Center rescue and recovery effort a minimum of 4 hours in the first 4 days from Sept. 11, 2001, 24 hours in September 2001, or 80 hours from September through December 2001. Responders also had to complete at least one monitoring visit.
Responders’ data were linked to data from cancer registries in New York, New Jersey, Pennsylvania, and Connecticut (where most responders lived at the time of the attacks), as well as Florida and North Carolina (where responders were known to retire). The responders were linked to the registries using probabilistic matching algorithms, which made use of information such as patient name, address, social security number, sex, race, and birth date.
The researchers noted that patients who enrolled in the General Responder Cohort had their cancer certified for federally funded treatment, and this factor might result in “sicker members disproportionately self-selecting into the program.” To reduce this potential bias, the researchers conducted a restricted analysis in which counts of cancer cases and person-years of observation began 6 months after responder enrollment.
The researchers analyzed data on 28,729 responders who primarily worked in protective services (49.0%) and construction (20.8%). Responders spent a median of 52 days on the rescue and recovery effort, and 44.4% of them had some exposure to the dust cloud caused by the collapse of the towers.
In the restricted analysis, there were 1,072 cancers observed in 999 responders. Compared with the general population, responders had a significantly higher incidence of all cancers combined, with a standardized incidence ratio (SIR) of 1.09.
Responders had a significantly higher incidence of prostate cancer (SIR,1.25), thyroid cancer (SIR, 2.19), and leukemia (SIR, 1.41). The leukemia category included acute myeloid leukemia (SIR,1.58) and chronic lymphocytic leukemia (SIR, 1.08).
“Although other studies have revealed elevated SIRs for other hematologic malignancies, this is the first reported, statistically significant, elevated SIR for leukemia,” the researchers wrote. “Leukemia is known to occur after exposure to occupational carcinogens, including benzene (burning jet fuel and other sources at the [World Trade Center] site), possibly at low levels of exposure and with a latency of several years from exposure.”
A multivariate analysis showed no association between cancer incidence and the length of time responders spent on the rescue and recovery effort or the intensity of their exposure to the dust cloud or debris pile.
The analysis did show an elevated risk of all cancers combined with each 1-year increase in responder age (hazard ratio, 1.09), among male responders (HR, 1.21), and among responders who smoked at baseline (HR, 1.29).
This research was supported by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health. The researchers disclosed no conflicts of interest.
SOURCE: Shapiro MZ et al. JNCI Cancer Spectr. 2020 Jan 14. doi: 10.1093/jncics/pkz090.
New data suggest an increased risk of leukemia among responders who worked at the World Trade Center site after the attacks on Sept. 11, 2001.
Previous studies have shown that 9/11 responders have a higher incidence of cancers than does the general population. The current study is the first to show a higher incidence of leukemia among responders. It also shows a higher incidence of thyroid and prostate cancers as well as all cancer types combined.
These findings were published in JNCI Cancer Spectrum.
“This study showed increased incidence of several cancer types compared to previously conducted studies with shorter follow-up periods,” study author Susan L, Teitelbaum, PhD, of the Icahn School of Medicine at Mount Sinai, New York, said in a press release.
“Because of the long latency period of many types of cancer, it is possible that increased rates of other cancers, as well as World Trade Center exposure health issues, may emerge after longer periods of study.”
Dr. Teitelbaum and colleagues evaluated responders enrolled in the World Trade Center Health Program General Responder Cohort from when it was established in July 2002 through the end of follow-up, which was Dec. 31, 2013, for New York residents and Dec. 31, 2012, for residents of other states.
To be eligible for the cohort, responders must have worked on the World Trade Center rescue and recovery effort a minimum of 4 hours in the first 4 days from Sept. 11, 2001, 24 hours in September 2001, or 80 hours from September through December 2001. Responders also had to complete at least one monitoring visit.
Responders’ data were linked to data from cancer registries in New York, New Jersey, Pennsylvania, and Connecticut (where most responders lived at the time of the attacks), as well as Florida and North Carolina (where responders were known to retire). The responders were linked to the registries using probabilistic matching algorithms, which made use of information such as patient name, address, social security number, sex, race, and birth date.
The researchers noted that patients who enrolled in the General Responder Cohort had their cancer certified for federally funded treatment, and this factor might result in “sicker members disproportionately self-selecting into the program.” To reduce this potential bias, the researchers conducted a restricted analysis in which counts of cancer cases and person-years of observation began 6 months after responder enrollment.
The researchers analyzed data on 28,729 responders who primarily worked in protective services (49.0%) and construction (20.8%). Responders spent a median of 52 days on the rescue and recovery effort, and 44.4% of them had some exposure to the dust cloud caused by the collapse of the towers.
In the restricted analysis, there were 1,072 cancers observed in 999 responders. Compared with the general population, responders had a significantly higher incidence of all cancers combined, with a standardized incidence ratio (SIR) of 1.09.
Responders had a significantly higher incidence of prostate cancer (SIR,1.25), thyroid cancer (SIR, 2.19), and leukemia (SIR, 1.41). The leukemia category included acute myeloid leukemia (SIR,1.58) and chronic lymphocytic leukemia (SIR, 1.08).
“Although other studies have revealed elevated SIRs for other hematologic malignancies, this is the first reported, statistically significant, elevated SIR for leukemia,” the researchers wrote. “Leukemia is known to occur after exposure to occupational carcinogens, including benzene (burning jet fuel and other sources at the [World Trade Center] site), possibly at low levels of exposure and with a latency of several years from exposure.”
A multivariate analysis showed no association between cancer incidence and the length of time responders spent on the rescue and recovery effort or the intensity of their exposure to the dust cloud or debris pile.
The analysis did show an elevated risk of all cancers combined with each 1-year increase in responder age (hazard ratio, 1.09), among male responders (HR, 1.21), and among responders who smoked at baseline (HR, 1.29).
This research was supported by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health. The researchers disclosed no conflicts of interest.
SOURCE: Shapiro MZ et al. JNCI Cancer Spectr. 2020 Jan 14. doi: 10.1093/jncics/pkz090.
New data suggest an increased risk of leukemia among responders who worked at the World Trade Center site after the attacks on Sept. 11, 2001.
Previous studies have shown that 9/11 responders have a higher incidence of cancers than does the general population. The current study is the first to show a higher incidence of leukemia among responders. It also shows a higher incidence of thyroid and prostate cancers as well as all cancer types combined.
These findings were published in JNCI Cancer Spectrum.
“This study showed increased incidence of several cancer types compared to previously conducted studies with shorter follow-up periods,” study author Susan L, Teitelbaum, PhD, of the Icahn School of Medicine at Mount Sinai, New York, said in a press release.
“Because of the long latency period of many types of cancer, it is possible that increased rates of other cancers, as well as World Trade Center exposure health issues, may emerge after longer periods of study.”
Dr. Teitelbaum and colleagues evaluated responders enrolled in the World Trade Center Health Program General Responder Cohort from when it was established in July 2002 through the end of follow-up, which was Dec. 31, 2013, for New York residents and Dec. 31, 2012, for residents of other states.
To be eligible for the cohort, responders must have worked on the World Trade Center rescue and recovery effort a minimum of 4 hours in the first 4 days from Sept. 11, 2001, 24 hours in September 2001, or 80 hours from September through December 2001. Responders also had to complete at least one monitoring visit.
Responders’ data were linked to data from cancer registries in New York, New Jersey, Pennsylvania, and Connecticut (where most responders lived at the time of the attacks), as well as Florida and North Carolina (where responders were known to retire). The responders were linked to the registries using probabilistic matching algorithms, which made use of information such as patient name, address, social security number, sex, race, and birth date.
The researchers noted that patients who enrolled in the General Responder Cohort had their cancer certified for federally funded treatment, and this factor might result in “sicker members disproportionately self-selecting into the program.” To reduce this potential bias, the researchers conducted a restricted analysis in which counts of cancer cases and person-years of observation began 6 months after responder enrollment.
The researchers analyzed data on 28,729 responders who primarily worked in protective services (49.0%) and construction (20.8%). Responders spent a median of 52 days on the rescue and recovery effort, and 44.4% of them had some exposure to the dust cloud caused by the collapse of the towers.
In the restricted analysis, there were 1,072 cancers observed in 999 responders. Compared with the general population, responders had a significantly higher incidence of all cancers combined, with a standardized incidence ratio (SIR) of 1.09.
Responders had a significantly higher incidence of prostate cancer (SIR,1.25), thyroid cancer (SIR, 2.19), and leukemia (SIR, 1.41). The leukemia category included acute myeloid leukemia (SIR,1.58) and chronic lymphocytic leukemia (SIR, 1.08).
“Although other studies have revealed elevated SIRs for other hematologic malignancies, this is the first reported, statistically significant, elevated SIR for leukemia,” the researchers wrote. “Leukemia is known to occur after exposure to occupational carcinogens, including benzene (burning jet fuel and other sources at the [World Trade Center] site), possibly at low levels of exposure and with a latency of several years from exposure.”
A multivariate analysis showed no association between cancer incidence and the length of time responders spent on the rescue and recovery effort or the intensity of their exposure to the dust cloud or debris pile.
The analysis did show an elevated risk of all cancers combined with each 1-year increase in responder age (hazard ratio, 1.09), among male responders (HR, 1.21), and among responders who smoked at baseline (HR, 1.29).
This research was supported by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health. The researchers disclosed no conflicts of interest.
SOURCE: Shapiro MZ et al. JNCI Cancer Spectr. 2020 Jan 14. doi: 10.1093/jncics/pkz090.
FROM JNCI CANCER SPECTRUM
Gout rates reduced with SGLT2 inhibitors
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Sodium-glucose cotransporter 2 (SGLT2) inhibitor use was associated with lower rates of gout in type 2 diabetes patients compared with glucagonlike peptide–1 (GLP-1) agonist use.
Major finding: The incidence of gout was 4.9 per 1,000 person-years in patients on SGLT2 inhibitors and 7.8 per 1,000 person-years in patients on GLP1 agonists.
Study details: The data come from a population-based cohort study of 295,907 adults with type 2 diabetes.
Disclosures: The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
Source: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
Draft ACR Takayasu’s guidelines: Surgery is the last resort
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.

This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.
This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.
This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
REPORTING FROM ACR 2019
Drop in flu activity may not signal seasonal peak
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
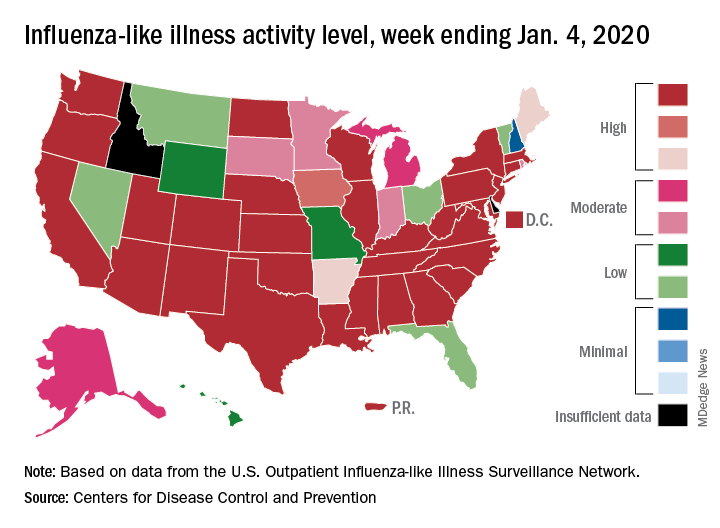
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.
For everything there is a season
2020 SoHM Survey ready to launch
Wow, the last 2 years have just flown by! I can’t believe it’s already time to launch the Society of Hospital Medicine State of Hospital Medicine survey again! Right now is the season for you to roll up your sleeves and get to work helping SHM develop the nation’s definitive resource on the current state of hospital medicine practice.

I’m really excited about this year’s survey. SHM’s Practice Analysis Committee has redesigned it to eliminate some out-of-date or little-used questions and to add a few new, more relevant questions. Even more exciting, we have a new survey platform that should massively improve your experience of submitting data for the survey and also make the back-end data tabulation and analysis much quicker and more accurate. Multisite groups will now have two options for submitting data – a redesigned, more user-friendly Excel tool, or a new pathway to submit data in the reporting platform by replicating responses.
In addition, our new survey platform should help us produce the final report a little more quickly and improve its usability.
New-for-2020 survey topics will include:
- Expanded information on nurse practitioner/physician assistant roles
- Diversity in hospital medicine physician leadership
- Specific questions for hospital medicine groups (HMGs) serving children that will better capture unique attributes of these hospital medicine practices
Why participate?
I can’t emphasize enough that each and every survey submission matters a lot. The State of Hospital Medicine report claims to be the authoritative resource for information about the specialty of hospital medicine. But the report can’t fulfill this claim if the underlying data is skimpy because people were too busy, couldn’t be bothered to participate, or if participation is not broadly representative of the amazing diversity of hospital medicine practices out there.
Your participation will help ensure that you are contributing to a robust hospital medicine database, and that your own group’s information is represented in the survey results. By doing so you will be helping to ensure hospital medicine’s place as perhaps the crucial specialty for U.S. health care in the coming decade.
In addition, participants will receive free access to the survey results, so there’s a direct benefit to you and your HMG as well.
How can you participate?
Here’s what you need to know:
1. The survey opens on Jan.6, 2020, and closes on Feb. 14, 2020.
2. You can find general information about the survey at this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/, and register to participate by using this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/sohm-survey/.
3. To participate, you’ll want to collect the following general types of information for your hospital medicine group:
- Basic group descriptive information (for example, types of patients seen, number of hospitals covered, teaching status, etc.)
- Scope of clinical services
- Nurse practitioners and physician assistants in the HMG
- Full-time equivalent (FTE) information
- Information about the physician leader(s)
- Staffing/scheduling arrangements, including backup plans, paid time off, unfilled positions, predominant scheduling pattern, night coverage arrangements, dedicated admitters, unit-based assignments, etc.
- Compensation model (but not specific amounts)
- Value of employee benefits and CME
- Total work relative value units generated by the HMG, and number of times the following CPT codes were billed: 99221, 99222, 99223, 99231, 99232, 99233, 99238, 99239
- Information about financial support provided to the HMG
- Specific questions for academic HMGs, including financial support for nonclinical work, and allocation of FTEs
- Specific questions for HMGs serving children, including the hospital settings served, proportion of part-time staff, FTE definition, and information about board certification in pediatric hospital medicine
I’m hoping that all of you will join me in working to make the 2020 State of Hospital Medicine survey and report the best one yet!
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Meeting Committees, and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
2020 SoHM Survey ready to launch
2020 SoHM Survey ready to launch
Wow, the last 2 years have just flown by! I can’t believe it’s already time to launch the Society of Hospital Medicine State of Hospital Medicine survey again! Right now is the season for you to roll up your sleeves and get to work helping SHM develop the nation’s definitive resource on the current state of hospital medicine practice.
I’m really excited about this year’s survey. SHM’s Practice Analysis Committee has redesigned it to eliminate some out-of-date or little-used questions and to add a few new, more relevant questions. Even more exciting, we have a new survey platform that should massively improve your experience of submitting data for the survey and also make the back-end data tabulation and analysis much quicker and more accurate. Multisite groups will now have two options for submitting data – a redesigned, more user-friendly Excel tool, or a new pathway to submit data in the reporting platform by replicating responses.
In addition, our new survey platform should help us produce the final report a little more quickly and improve its usability.
New-for-2020 survey topics will include:
- Expanded information on nurse practitioner/physician assistant roles
- Diversity in hospital medicine physician leadership
- Specific questions for hospital medicine groups (HMGs) serving children that will better capture unique attributes of these hospital medicine practices
Why participate?
I can’t emphasize enough that each and every survey submission matters a lot. The State of Hospital Medicine report claims to be the authoritative resource for information about the specialty of hospital medicine. But the report can’t fulfill this claim if the underlying data is skimpy because people were too busy, couldn’t be bothered to participate, or if participation is not broadly representative of the amazing diversity of hospital medicine practices out there.
Your participation will help ensure that you are contributing to a robust hospital medicine database, and that your own group’s information is represented in the survey results. By doing so you will be helping to ensure hospital medicine’s place as perhaps the crucial specialty for U.S. health care in the coming decade.
In addition, participants will receive free access to the survey results, so there’s a direct benefit to you and your HMG as well.
How can you participate?
Here’s what you need to know:
1. The survey opens on Jan.6, 2020, and closes on Feb. 14, 2020.
2. You can find general information about the survey at this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/, and register to participate by using this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/sohm-survey/.
3. To participate, you’ll want to collect the following general types of information for your hospital medicine group:
- Basic group descriptive information (for example, types of patients seen, number of hospitals covered, teaching status, etc.)
- Scope of clinical services
- Nurse practitioners and physician assistants in the HMG
- Full-time equivalent (FTE) information
- Information about the physician leader(s)
- Staffing/scheduling arrangements, including backup plans, paid time off, unfilled positions, predominant scheduling pattern, night coverage arrangements, dedicated admitters, unit-based assignments, etc.
- Compensation model (but not specific amounts)
- Value of employee benefits and CME
- Total work relative value units generated by the HMG, and number of times the following CPT codes were billed: 99221, 99222, 99223, 99231, 99232, 99233, 99238, 99239
- Information about financial support provided to the HMG
- Specific questions for academic HMGs, including financial support for nonclinical work, and allocation of FTEs
- Specific questions for HMGs serving children, including the hospital settings served, proportion of part-time staff, FTE definition, and information about board certification in pediatric hospital medicine
I’m hoping that all of you will join me in working to make the 2020 State of Hospital Medicine survey and report the best one yet!
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Meeting Committees, and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Wow, the last 2 years have just flown by! I can’t believe it’s already time to launch the Society of Hospital Medicine State of Hospital Medicine survey again! Right now is the season for you to roll up your sleeves and get to work helping SHM develop the nation’s definitive resource on the current state of hospital medicine practice.
I’m really excited about this year’s survey. SHM’s Practice Analysis Committee has redesigned it to eliminate some out-of-date or little-used questions and to add a few new, more relevant questions. Even more exciting, we have a new survey platform that should massively improve your experience of submitting data for the survey and also make the back-end data tabulation and analysis much quicker and more accurate. Multisite groups will now have two options for submitting data – a redesigned, more user-friendly Excel tool, or a new pathway to submit data in the reporting platform by replicating responses.
In addition, our new survey platform should help us produce the final report a little more quickly and improve its usability.
New-for-2020 survey topics will include:
- Expanded information on nurse practitioner/physician assistant roles
- Diversity in hospital medicine physician leadership
- Specific questions for hospital medicine groups (HMGs) serving children that will better capture unique attributes of these hospital medicine practices
Why participate?
I can’t emphasize enough that each and every survey submission matters a lot. The State of Hospital Medicine report claims to be the authoritative resource for information about the specialty of hospital medicine. But the report can’t fulfill this claim if the underlying data is skimpy because people were too busy, couldn’t be bothered to participate, or if participation is not broadly representative of the amazing diversity of hospital medicine practices out there.
Your participation will help ensure that you are contributing to a robust hospital medicine database, and that your own group’s information is represented in the survey results. By doing so you will be helping to ensure hospital medicine’s place as perhaps the crucial specialty for U.S. health care in the coming decade.
In addition, participants will receive free access to the survey results, so there’s a direct benefit to you and your HMG as well.
How can you participate?
Here’s what you need to know:
1. The survey opens on Jan.6, 2020, and closes on Feb. 14, 2020.
2. You can find general information about the survey at this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/, and register to participate by using this link: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/sohm-survey/.
3. To participate, you’ll want to collect the following general types of information for your hospital medicine group:
- Basic group descriptive information (for example, types of patients seen, number of hospitals covered, teaching status, etc.)
- Scope of clinical services
- Nurse practitioners and physician assistants in the HMG
- Full-time equivalent (FTE) information
- Information about the physician leader(s)
- Staffing/scheduling arrangements, including backup plans, paid time off, unfilled positions, predominant scheduling pattern, night coverage arrangements, dedicated admitters, unit-based assignments, etc.
- Compensation model (but not specific amounts)
- Value of employee benefits and CME
- Total work relative value units generated by the HMG, and number of times the following CPT codes were billed: 99221, 99222, 99223, 99231, 99232, 99233, 99238, 99239
- Information about financial support provided to the HMG
- Specific questions for academic HMGs, including financial support for nonclinical work, and allocation of FTEs
- Specific questions for HMGs serving children, including the hospital settings served, proportion of part-time staff, FTE definition, and information about board certification in pediatric hospital medicine
I’m hoping that all of you will join me in working to make the 2020 State of Hospital Medicine survey and report the best one yet!
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Meeting Committees, and helps to coordinate SHM’s biannual State of Hospital Medicine survey.