User login
Atopic dermatitis not linked with increased venous thromboembolism risk
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
Atopic dermatitis not linked with increased venous thromboembolism risk
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
Key clinical point: Atopic dermatitis (AD) is associated with a lower risk for venous thromboembolism (VTE) than several rheumatologic and gastrointestinal immune-mediated inflammatory diseases (IMID).
Major finding: Patients with AD vs AD-matched control individuals did not have a higher risk for VTE (adjusted hazard ratio [aHR] 0.96; 95% CI 0.90-1.02). Compared with patients having AD, those with Crohn’s disease (aHR 1.71; 95% CI 1.47-1.99), rheumatoid arthritis (aHR 1.57; 95% CI 1.43-1.72), ulcerative colitis (aHR 1.84; 95% CI 1.63-2.09), and ankylosing spondylitis (aHR 1.45; 95% CI 1.03-2.03) had higher risks for VTE.
Study details: This retrospective observational cohort study analyzed 2,061,222 adult patients with IMID, including 1,098,633 patients with AD who were matched with 1,098,633 control individuals without IMID.
Disclosures: This study was funded by AbbVie Inc. JF Merola declared being a consultant or investigator for AbbVie and others. The other authors declared being current or former employees of or owning stocks or stock options in AbbVie.
Source: Merola JF et al. Venous thromboembolism risk is lower in patients with atopic dermatitis than other immune-mediated inflammatory diseases: A retrospective, observational, comparative cohort study using US claims data. J Am Acad Dermatol. 2023 (Dec 23). doi: 10.1016/j.jaad.2023.12.027
AI Aids in Monitoring Asthma in Young Children
Can asthma symptoms be monitored reliably at home? Until now, the answer would have been yes, but not in preschool-age patients. Recent findings in Annals of Family Medicine suggest that this limitation can be overcome with the assistance of artificial intelligence (AI).
Objectivity Challenge
A timely diagnosis of asthma exacerbations, which is crucial for proper disease management, requires effective home monitoring. While some lung function parameters, like peak expiratory flow (PEF), can be measured by patients at home, tools for this purpose are not designed for very young children.
“To achieve effective asthma management, patients should be given the necessary tools to allow them to recognize and respond to worsening asthma,” wrote the study authors. Despite the Global Initiative for Asthma identifying respiratory sounds as a fundamental parameter for exacerbation recognition, these are almost exclusively evaluated during doctor visits. Recognizing respiratory sounds and judging whether there has been a change can be challenging for those outside the medical profession.
To enhance home monitoring, researchers from the Department of Pediatric Pneumology and Rheumatology at the University of Lublin, Poland, experimented with the StethoMe stethoscope, which enables the recognition of pathologic signs, including continuous and transient noises. This AI-assisted stethoscope, trained on over 10,000 respiratory sound recordings, is certified as a Class IIa medical device in Europe.
The ‘Smart’ Stethoscope
The 6-month study enlisted 149 patients with asthma (90 children and 59 adults). Participants self-monitored (but parents or caregivers managed for children) once daily in the first 2 weeks and at least once weekly thereafter using three tools. The first was the StethoMe stethoscope, which was used for detecting respiratory sounds, respiratory rate (RR), heart rate (HR), and inspiration/expiration ratio (I/E). Patients were provided a “map” of chest points at which to position the stethoscope. The second was a pulse oximeter, which was used to measure oxygen saturation. The third was a peak flow meter for quantifying PEF. Simultaneously, a health questionnaire was completed.
Data from 6029 completed self-monitoring sessions were used to determine the most effective parameter for exacerbation recognition, quantified by the area under the receiver operating characteristic curve (AUC). The researchers concluded that the parameter with the best performance was wheeze intensity in young children (AUC 84%, 95% CI, 82%-85%), wheeze intensity in older children (AUC, 81%; 95% CI, 79%-84%), and questionnaire response for adults (AUC, 92%; 95% CI, 89%-95%). Combining multiple parameters increased effectiveness.
“The present results clearly show that a set of parameters (wheezes, rhonchi, coarse and fine crackles, HR, RR, and I/E) measured by a device such as an AI-aided home stethoscope allows for the detection of exacerbations without the need for performing PEF measurements, which can be equivocal,” the study authors concluded. “In addition, in the case of younger children (age, < 5 years), when introduced on a large scale, the analyzed home stethoscope appears to be a promising tool that might make asthma diagnosis more straightforward and substantially facilitate asthma monitoring.”
A version of this article first appeared on Medscape.com. This article was translated from Univadis Italy, which is part of the Medscape professional network.
Can asthma symptoms be monitored reliably at home? Until now, the answer would have been yes, but not in preschool-age patients. Recent findings in Annals of Family Medicine suggest that this limitation can be overcome with the assistance of artificial intelligence (AI).
Objectivity Challenge
A timely diagnosis of asthma exacerbations, which is crucial for proper disease management, requires effective home monitoring. While some lung function parameters, like peak expiratory flow (PEF), can be measured by patients at home, tools for this purpose are not designed for very young children.
“To achieve effective asthma management, patients should be given the necessary tools to allow them to recognize and respond to worsening asthma,” wrote the study authors. Despite the Global Initiative for Asthma identifying respiratory sounds as a fundamental parameter for exacerbation recognition, these are almost exclusively evaluated during doctor visits. Recognizing respiratory sounds and judging whether there has been a change can be challenging for those outside the medical profession.
To enhance home monitoring, researchers from the Department of Pediatric Pneumology and Rheumatology at the University of Lublin, Poland, experimented with the StethoMe stethoscope, which enables the recognition of pathologic signs, including continuous and transient noises. This AI-assisted stethoscope, trained on over 10,000 respiratory sound recordings, is certified as a Class IIa medical device in Europe.
The ‘Smart’ Stethoscope
The 6-month study enlisted 149 patients with asthma (90 children and 59 adults). Participants self-monitored (but parents or caregivers managed for children) once daily in the first 2 weeks and at least once weekly thereafter using three tools. The first was the StethoMe stethoscope, which was used for detecting respiratory sounds, respiratory rate (RR), heart rate (HR), and inspiration/expiration ratio (I/E). Patients were provided a “map” of chest points at which to position the stethoscope. The second was a pulse oximeter, which was used to measure oxygen saturation. The third was a peak flow meter for quantifying PEF. Simultaneously, a health questionnaire was completed.
Data from 6029 completed self-monitoring sessions were used to determine the most effective parameter for exacerbation recognition, quantified by the area under the receiver operating characteristic curve (AUC). The researchers concluded that the parameter with the best performance was wheeze intensity in young children (AUC 84%, 95% CI, 82%-85%), wheeze intensity in older children (AUC, 81%; 95% CI, 79%-84%), and questionnaire response for adults (AUC, 92%; 95% CI, 89%-95%). Combining multiple parameters increased effectiveness.
“The present results clearly show that a set of parameters (wheezes, rhonchi, coarse and fine crackles, HR, RR, and I/E) measured by a device such as an AI-aided home stethoscope allows for the detection of exacerbations without the need for performing PEF measurements, which can be equivocal,” the study authors concluded. “In addition, in the case of younger children (age, < 5 years), when introduced on a large scale, the analyzed home stethoscope appears to be a promising tool that might make asthma diagnosis more straightforward and substantially facilitate asthma monitoring.”
A version of this article first appeared on Medscape.com. This article was translated from Univadis Italy, which is part of the Medscape professional network.
Can asthma symptoms be monitored reliably at home? Until now, the answer would have been yes, but not in preschool-age patients. Recent findings in Annals of Family Medicine suggest that this limitation can be overcome with the assistance of artificial intelligence (AI).
Objectivity Challenge
A timely diagnosis of asthma exacerbations, which is crucial for proper disease management, requires effective home monitoring. While some lung function parameters, like peak expiratory flow (PEF), can be measured by patients at home, tools for this purpose are not designed for very young children.
“To achieve effective asthma management, patients should be given the necessary tools to allow them to recognize and respond to worsening asthma,” wrote the study authors. Despite the Global Initiative for Asthma identifying respiratory sounds as a fundamental parameter for exacerbation recognition, these are almost exclusively evaluated during doctor visits. Recognizing respiratory sounds and judging whether there has been a change can be challenging for those outside the medical profession.
To enhance home monitoring, researchers from the Department of Pediatric Pneumology and Rheumatology at the University of Lublin, Poland, experimented with the StethoMe stethoscope, which enables the recognition of pathologic signs, including continuous and transient noises. This AI-assisted stethoscope, trained on over 10,000 respiratory sound recordings, is certified as a Class IIa medical device in Europe.
The ‘Smart’ Stethoscope
The 6-month study enlisted 149 patients with asthma (90 children and 59 adults). Participants self-monitored (but parents or caregivers managed for children) once daily in the first 2 weeks and at least once weekly thereafter using three tools. The first was the StethoMe stethoscope, which was used for detecting respiratory sounds, respiratory rate (RR), heart rate (HR), and inspiration/expiration ratio (I/E). Patients were provided a “map” of chest points at which to position the stethoscope. The second was a pulse oximeter, which was used to measure oxygen saturation. The third was a peak flow meter for quantifying PEF. Simultaneously, a health questionnaire was completed.
Data from 6029 completed self-monitoring sessions were used to determine the most effective parameter for exacerbation recognition, quantified by the area under the receiver operating characteristic curve (AUC). The researchers concluded that the parameter with the best performance was wheeze intensity in young children (AUC 84%, 95% CI, 82%-85%), wheeze intensity in older children (AUC, 81%; 95% CI, 79%-84%), and questionnaire response for adults (AUC, 92%; 95% CI, 89%-95%). Combining multiple parameters increased effectiveness.
“The present results clearly show that a set of parameters (wheezes, rhonchi, coarse and fine crackles, HR, RR, and I/E) measured by a device such as an AI-aided home stethoscope allows for the detection of exacerbations without the need for performing PEF measurements, which can be equivocal,” the study authors concluded. “In addition, in the case of younger children (age, < 5 years), when introduced on a large scale, the analyzed home stethoscope appears to be a promising tool that might make asthma diagnosis more straightforward and substantially facilitate asthma monitoring.”
A version of this article first appeared on Medscape.com. This article was translated from Univadis Italy, which is part of the Medscape professional network.
FROM ANNALS OF FAMILY MEDICINE
Impact of Pregnancy on Rosacea Unpredictable, Study Suggests
TOPLINE:
Among women diagnosed with rosacea, the impact of pregnancy on the disease is unpredictable.
METHODOLOGY:
- Researchers conducted a telephone survey of 39 women with a diagnosis of rosacea in the electronic medical records prior to the onset of pregnancy who had been admitted to Oregon Health & Science University for labor and delivery from June 27, 2015, to June 27, 2020.
- Patient global assessment of clear (0), mild (1), moderate (2), or severe (3) rosacea was rated across five timepoints: 1-3 months preconception; first, second, and third trimesters; and 6 weeks postpartum.
TAKEAWAY:
- The mean age of the survey participants was 35.5 years, the mean gestational age at delivery was 39.4 weeks, and most had singleton pregnancies.
- All but one study participant (97.4%) reported symptoms of erythematotelangiectatic rosacea, while 26 (67%) reported symptoms of papulopustular rosacea.
- Nearly half of the participants (19, 48.7%) said their rosacea worsened during pregnancy, 13 (33.3%) reported no change in rosacea severity during pregnancy, and 7 (17.9%) reported that their rosacea improved during pregnancy.
- Before conceiving, the mean rosacea severity score among participants was mild (1.10; 95% CI, 0.92-1.29) and did not change significantly over time, a reflection of individual variations. In addition, 83.3% of participants did not use prescription rosacea treatments prior to pregnancy, and 89.6% did not use them during pregnancy.
IN PRACTICE:
“Rosacea, like acne, lacks a predictable group effect, and instead, each individual may have a different response to the physiologic changes of pregnancy,” the authors concluded.
SOURCE:
Genevieve Benedetti, MD, MPP, of the Department of Dermatology at Oregon Health & Science University, Portland, Oregon, led the research, published as a research letter in the International Journal of Women’s Dermatology.
LIMITATIONS:
The small sample size, single-center design, and overall prevalence of mild disease limit the ability to detect change.
DISCLOSURES:
The researchers reported having no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Among women diagnosed with rosacea, the impact of pregnancy on the disease is unpredictable.
METHODOLOGY:
- Researchers conducted a telephone survey of 39 women with a diagnosis of rosacea in the electronic medical records prior to the onset of pregnancy who had been admitted to Oregon Health & Science University for labor and delivery from June 27, 2015, to June 27, 2020.
- Patient global assessment of clear (0), mild (1), moderate (2), or severe (3) rosacea was rated across five timepoints: 1-3 months preconception; first, second, and third trimesters; and 6 weeks postpartum.
TAKEAWAY:
- The mean age of the survey participants was 35.5 years, the mean gestational age at delivery was 39.4 weeks, and most had singleton pregnancies.
- All but one study participant (97.4%) reported symptoms of erythematotelangiectatic rosacea, while 26 (67%) reported symptoms of papulopustular rosacea.
- Nearly half of the participants (19, 48.7%) said their rosacea worsened during pregnancy, 13 (33.3%) reported no change in rosacea severity during pregnancy, and 7 (17.9%) reported that their rosacea improved during pregnancy.
- Before conceiving, the mean rosacea severity score among participants was mild (1.10; 95% CI, 0.92-1.29) and did not change significantly over time, a reflection of individual variations. In addition, 83.3% of participants did not use prescription rosacea treatments prior to pregnancy, and 89.6% did not use them during pregnancy.
IN PRACTICE:
“Rosacea, like acne, lacks a predictable group effect, and instead, each individual may have a different response to the physiologic changes of pregnancy,” the authors concluded.
SOURCE:
Genevieve Benedetti, MD, MPP, of the Department of Dermatology at Oregon Health & Science University, Portland, Oregon, led the research, published as a research letter in the International Journal of Women’s Dermatology.
LIMITATIONS:
The small sample size, single-center design, and overall prevalence of mild disease limit the ability to detect change.
DISCLOSURES:
The researchers reported having no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Among women diagnosed with rosacea, the impact of pregnancy on the disease is unpredictable.
METHODOLOGY:
- Researchers conducted a telephone survey of 39 women with a diagnosis of rosacea in the electronic medical records prior to the onset of pregnancy who had been admitted to Oregon Health & Science University for labor and delivery from June 27, 2015, to June 27, 2020.
- Patient global assessment of clear (0), mild (1), moderate (2), or severe (3) rosacea was rated across five timepoints: 1-3 months preconception; first, second, and third trimesters; and 6 weeks postpartum.
TAKEAWAY:
- The mean age of the survey participants was 35.5 years, the mean gestational age at delivery was 39.4 weeks, and most had singleton pregnancies.
- All but one study participant (97.4%) reported symptoms of erythematotelangiectatic rosacea, while 26 (67%) reported symptoms of papulopustular rosacea.
- Nearly half of the participants (19, 48.7%) said their rosacea worsened during pregnancy, 13 (33.3%) reported no change in rosacea severity during pregnancy, and 7 (17.9%) reported that their rosacea improved during pregnancy.
- Before conceiving, the mean rosacea severity score among participants was mild (1.10; 95% CI, 0.92-1.29) and did not change significantly over time, a reflection of individual variations. In addition, 83.3% of participants did not use prescription rosacea treatments prior to pregnancy, and 89.6% did not use them during pregnancy.
IN PRACTICE:
“Rosacea, like acne, lacks a predictable group effect, and instead, each individual may have a different response to the physiologic changes of pregnancy,” the authors concluded.
SOURCE:
Genevieve Benedetti, MD, MPP, of the Department of Dermatology at Oregon Health & Science University, Portland, Oregon, led the research, published as a research letter in the International Journal of Women’s Dermatology.
LIMITATIONS:
The small sample size, single-center design, and overall prevalence of mild disease limit the ability to detect change.
DISCLOSURES:
The researchers reported having no disclosures.
A version of this article appeared on Medscape.com.
Study Identifies Cardiovascular Comorbidities Associated With Dermatomyositis
TOPLINE:
METHODOLOGY:
- DM is associated with cardiovascular disease (CVD), but US-based data studies on CVD comorbidities in patients with DM are lacking.
- In a cross-sectional analysis of participants in the All of Us research program aged 18 years and older with at least 1 year of electronic health record (EHR) data, researchers identified DM cases and controls with nearest neighbor propensity score matching by age, sex, race/ethnicity, EHR duration, and healthcare visit quantity.
- They used the Pearson’s chi-squared test, Fisher’s exact test, unpaired t-test, or Mann-Whitney U test to compare clinical characteristics and traditional CV comorbidities.
- Multivariable conditional logistic regression was used with backward elimination of comorbidities with P > .1 or evidence of collinearity.
TAKEAWAY:
- Among 235,161 All of Us participants, researchers identified 206 DM cases and 824 matched controls with largely similar demographic characteristics, including smoking status, obesity, and indicators of socioeconomic status.
- Participants with DM were more likely to have a history of atrial fibrillation (10.1% vs 16.0%, respectively), chronic kidney disease (15.2% vs 29.1%), congestive heart failure (9.6% vs 18.0%), coronary artery disease (CAD) (18.2% vs 34.0%), hypertension (52.5% vs 60.7%), myocardial infarction (7.4% vs 15.0), type 2 diabetes (27.3% vs 47.6%), and valvular heart disease (8.7% vs 16.5%) than matched controls.
- In a multivariable analysis that adjusted for potential confounders, three comorbidities remained associated with DM: CAD (odds ratio [OR], 2.0; P < .001), type 2 diabetes (OR, 2.2; P < .001), and chronic kidney disease (OR, 1.7; P = .015).
IN PRACTICE:
“Our findings are important both for prognosis and clinical care, suggesting DM patients should be screened for CVD risk factors to potentially reduce the increased risk for cardiovascular events and CVD-related mortality in DM,” the authors concluded.
SOURCE:
Corresponding author Alisa N. Femia, MD, of the department of dermatology at NYU Grossman School of Medicine, led the research. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
How DM treatments might influence CVD development was not addressed. EHRs may have diagnostic inaccuracies and omissions and lack data on clinical features and severity.
DISCLOSURES:
The project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Femia reported consulting fees from Octagon Therapeutics, Timber Pharmaceuticals, and Guidepoint. Study author Michael S. Garshick, MD, reported consulting fees from AbbVie and Horizon Therapeutics. The remaining authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- DM is associated with cardiovascular disease (CVD), but US-based data studies on CVD comorbidities in patients with DM are lacking.
- In a cross-sectional analysis of participants in the All of Us research program aged 18 years and older with at least 1 year of electronic health record (EHR) data, researchers identified DM cases and controls with nearest neighbor propensity score matching by age, sex, race/ethnicity, EHR duration, and healthcare visit quantity.
- They used the Pearson’s chi-squared test, Fisher’s exact test, unpaired t-test, or Mann-Whitney U test to compare clinical characteristics and traditional CV comorbidities.
- Multivariable conditional logistic regression was used with backward elimination of comorbidities with P > .1 or evidence of collinearity.
TAKEAWAY:
- Among 235,161 All of Us participants, researchers identified 206 DM cases and 824 matched controls with largely similar demographic characteristics, including smoking status, obesity, and indicators of socioeconomic status.
- Participants with DM were more likely to have a history of atrial fibrillation (10.1% vs 16.0%, respectively), chronic kidney disease (15.2% vs 29.1%), congestive heart failure (9.6% vs 18.0%), coronary artery disease (CAD) (18.2% vs 34.0%), hypertension (52.5% vs 60.7%), myocardial infarction (7.4% vs 15.0), type 2 diabetes (27.3% vs 47.6%), and valvular heart disease (8.7% vs 16.5%) than matched controls.
- In a multivariable analysis that adjusted for potential confounders, three comorbidities remained associated with DM: CAD (odds ratio [OR], 2.0; P < .001), type 2 diabetes (OR, 2.2; P < .001), and chronic kidney disease (OR, 1.7; P = .015).
IN PRACTICE:
“Our findings are important both for prognosis and clinical care, suggesting DM patients should be screened for CVD risk factors to potentially reduce the increased risk for cardiovascular events and CVD-related mortality in DM,” the authors concluded.
SOURCE:
Corresponding author Alisa N. Femia, MD, of the department of dermatology at NYU Grossman School of Medicine, led the research. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
How DM treatments might influence CVD development was not addressed. EHRs may have diagnostic inaccuracies and omissions and lack data on clinical features and severity.
DISCLOSURES:
The project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Femia reported consulting fees from Octagon Therapeutics, Timber Pharmaceuticals, and Guidepoint. Study author Michael S. Garshick, MD, reported consulting fees from AbbVie and Horizon Therapeutics. The remaining authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- DM is associated with cardiovascular disease (CVD), but US-based data studies on CVD comorbidities in patients with DM are lacking.
- In a cross-sectional analysis of participants in the All of Us research program aged 18 years and older with at least 1 year of electronic health record (EHR) data, researchers identified DM cases and controls with nearest neighbor propensity score matching by age, sex, race/ethnicity, EHR duration, and healthcare visit quantity.
- They used the Pearson’s chi-squared test, Fisher’s exact test, unpaired t-test, or Mann-Whitney U test to compare clinical characteristics and traditional CV comorbidities.
- Multivariable conditional logistic regression was used with backward elimination of comorbidities with P > .1 or evidence of collinearity.
TAKEAWAY:
- Among 235,161 All of Us participants, researchers identified 206 DM cases and 824 matched controls with largely similar demographic characteristics, including smoking status, obesity, and indicators of socioeconomic status.
- Participants with DM were more likely to have a history of atrial fibrillation (10.1% vs 16.0%, respectively), chronic kidney disease (15.2% vs 29.1%), congestive heart failure (9.6% vs 18.0%), coronary artery disease (CAD) (18.2% vs 34.0%), hypertension (52.5% vs 60.7%), myocardial infarction (7.4% vs 15.0), type 2 diabetes (27.3% vs 47.6%), and valvular heart disease (8.7% vs 16.5%) than matched controls.
- In a multivariable analysis that adjusted for potential confounders, three comorbidities remained associated with DM: CAD (odds ratio [OR], 2.0; P < .001), type 2 diabetes (OR, 2.2; P < .001), and chronic kidney disease (OR, 1.7; P = .015).
IN PRACTICE:
“Our findings are important both for prognosis and clinical care, suggesting DM patients should be screened for CVD risk factors to potentially reduce the increased risk for cardiovascular events and CVD-related mortality in DM,” the authors concluded.
SOURCE:
Corresponding author Alisa N. Femia, MD, of the department of dermatology at NYU Grossman School of Medicine, led the research. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
How DM treatments might influence CVD development was not addressed. EHRs may have diagnostic inaccuracies and omissions and lack data on clinical features and severity.
DISCLOSURES:
The project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Femia reported consulting fees from Octagon Therapeutics, Timber Pharmaceuticals, and Guidepoint. Study author Michael S. Garshick, MD, reported consulting fees from AbbVie and Horizon Therapeutics. The remaining authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Spike in Schizophrenia-Related ED Visits During COVID
TOPLINE:
, a new study showed. Researchers said the findings suggested a need for social policies that strengthen mental health prevention systems.
METHODOLOGY:
Investigators obtained data from the University of California (UC) Health Data Warehouse on ED visits at five large UC health systems.
They captured the ICD-10 codes relating to schizophrenia spectrum disorders for ED visits from January 2016 to December 2021 for patients aged 18 years and older.
TAKEAWAY:
Between January 2016 and December 2021, there were 377,800 psychiatric ED visits, 10% of which involved schizophrenia spectrum disorders.
The mean number of visits per month for schizophrenia spectrum disorders rose from 520 before the pandemic to 558 visits per month after March 2020.
Compared to prepandemic numbers and after controlling for visits for other psychiatric disorders, there were 70.5 additional visits (P = .02) for schizophrenia spectrum disorders at 1 month and 74.9 additional visits (P = .005) at 3 months following the initial phase of the COVID-19 pandemic in California.
Investigators noted that prior studies indicated that COVID-19 infections may induce psychosis in some individuals, which could have been one underlying factor in the spike in cases.
IN PRACTICE:
“The COVID-19 pandemic draws attention to the vulnerability of patients with schizophrenia to macrosocial shocks, underscoring the importance of social policies related to income support, housing, and health insurance for future emergency preparedness and the need to strengthen mental healthcare systems,” the authors wrote.
SOURCE:
Parvita Singh, PhD, of The Ohio State University in Columbus, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Data used in the study excluded patients younger than 18 years. In addition, there was no analysis for trends by age or sex, which could have added valuable information to the study, the authors wrote. There was also no way to identify patients with newly diagnosed schizophrenia.
DISCLOSURES:
The study was funded through the Coronavirus Response and Relief Supplemental Appropriations Act and the Ohio Department of Mental Health and Addiction Services. Study disclosures are noted in the original study.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new study showed. Researchers said the findings suggested a need for social policies that strengthen mental health prevention systems.
METHODOLOGY:
Investigators obtained data from the University of California (UC) Health Data Warehouse on ED visits at five large UC health systems.
They captured the ICD-10 codes relating to schizophrenia spectrum disorders for ED visits from January 2016 to December 2021 for patients aged 18 years and older.
TAKEAWAY:
Between January 2016 and December 2021, there were 377,800 psychiatric ED visits, 10% of which involved schizophrenia spectrum disorders.
The mean number of visits per month for schizophrenia spectrum disorders rose from 520 before the pandemic to 558 visits per month after March 2020.
Compared to prepandemic numbers and after controlling for visits for other psychiatric disorders, there were 70.5 additional visits (P = .02) for schizophrenia spectrum disorders at 1 month and 74.9 additional visits (P = .005) at 3 months following the initial phase of the COVID-19 pandemic in California.
Investigators noted that prior studies indicated that COVID-19 infections may induce psychosis in some individuals, which could have been one underlying factor in the spike in cases.
IN PRACTICE:
“The COVID-19 pandemic draws attention to the vulnerability of patients with schizophrenia to macrosocial shocks, underscoring the importance of social policies related to income support, housing, and health insurance for future emergency preparedness and the need to strengthen mental healthcare systems,” the authors wrote.
SOURCE:
Parvita Singh, PhD, of The Ohio State University in Columbus, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Data used in the study excluded patients younger than 18 years. In addition, there was no analysis for trends by age or sex, which could have added valuable information to the study, the authors wrote. There was also no way to identify patients with newly diagnosed schizophrenia.
DISCLOSURES:
The study was funded through the Coronavirus Response and Relief Supplemental Appropriations Act and the Ohio Department of Mental Health and Addiction Services. Study disclosures are noted in the original study.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new study showed. Researchers said the findings suggested a need for social policies that strengthen mental health prevention systems.
METHODOLOGY:
Investigators obtained data from the University of California (UC) Health Data Warehouse on ED visits at five large UC health systems.
They captured the ICD-10 codes relating to schizophrenia spectrum disorders for ED visits from January 2016 to December 2021 for patients aged 18 years and older.
TAKEAWAY:
Between January 2016 and December 2021, there were 377,800 psychiatric ED visits, 10% of which involved schizophrenia spectrum disorders.
The mean number of visits per month for schizophrenia spectrum disorders rose from 520 before the pandemic to 558 visits per month after March 2020.
Compared to prepandemic numbers and after controlling for visits for other psychiatric disorders, there were 70.5 additional visits (P = .02) for schizophrenia spectrum disorders at 1 month and 74.9 additional visits (P = .005) at 3 months following the initial phase of the COVID-19 pandemic in California.
Investigators noted that prior studies indicated that COVID-19 infections may induce psychosis in some individuals, which could have been one underlying factor in the spike in cases.
IN PRACTICE:
“The COVID-19 pandemic draws attention to the vulnerability of patients with schizophrenia to macrosocial shocks, underscoring the importance of social policies related to income support, housing, and health insurance for future emergency preparedness and the need to strengthen mental healthcare systems,” the authors wrote.
SOURCE:
Parvita Singh, PhD, of The Ohio State University in Columbus, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Data used in the study excluded patients younger than 18 years. In addition, there was no analysis for trends by age or sex, which could have added valuable information to the study, the authors wrote. There was also no way to identify patients with newly diagnosed schizophrenia.
DISCLOSURES:
The study was funded through the Coronavirus Response and Relief Supplemental Appropriations Act and the Ohio Department of Mental Health and Addiction Services. Study disclosures are noted in the original study.
A version of this article appeared on Medscape.com.
Higher-Dose Atypical Antipsychotics Risky in Young Adults
High doses of a second-generation antipsychotic are associated with a significantly increased risk for death in young adults, adding to longstanding safety concerns regarding the use of higher doses of antipsychotic medication in this age group.
In a large cohort study, people aged 18-24 years had a significantly higher risk for death when starting a second-generation antipsychotic at doses greater than 100-mg chlorpromazine equivalents, but no increased mortality risk with lower doses.
There was no association with mortality risk in children aged 5-17 years with either dose.
“This finding suggests that antipsychotic medication–related fatalities are rare in healthy children without psychosis,” lead investigator Wayne Ray, PhD, from Vanderbilt University School of Medicine in Nashville, Tennessee, and colleagues wrote in a recent study that was published online in JAMA Psychiatry.
“In contrast, young adults aged 18-24 years treated with doses greater than 100-mg chlorpromazine equivalents had 127.5 additional deaths for every 100,000 person-years of exposure, suggesting further investigations of antipsychotic medication safety in this population are needed.”
Large, Retrospective Study
The researchers compared mortality for more than 2 million Medicaid patients aged 5-24 years (mean age, 13 years; 51% men) starting treatment with a second-generation antipsychotic vs control psychiatric medications. None of them had a diagnosis of severe somatic illness, schizophrenia, or related psychosis.
From January 2004 through September 2013, more than 21 million prescriptions were filled — roughly 5.4 million for antipsychotic doses of 100 mg or less, 2.8 million for doses greater than 100 mg, and 13.5 million for control medications.
The most commonly prescribed antipsychotic medication was risperidone, followed by aripiprazole, quetiapine, ziprasidone, and olanzapine. The most commonly prescribed control medication was clonidine, followed by atomoxetine, guanfacine, and sertraline.
In the overall study population, there was no significant association with risk for death for antipsychotic doses less than or equal to 100-mg chlorpromazine equivalents (hazard ratio [HR], 1.08; 95% CI, 0.89-1.32). However, mortality risk was increased at doses greater than 100 mg (HR, 1.37; 95% CI, 1.11-1.70).
Looking at mortality risk by age, for children aged 5-17 years, there was no significant association with either antipsychotic dose, whereas young adults aged 18-24 years had increased risk for doses greater than 100 mg (HR, 1.68; 95% CI, 1.23-2.29).
Start Low, Go Slow
“Start low and go slow is always a good rule of thumb when it comes to the use of these and any medicines, especially among especially among children and adolescents,” Caleb Alexander, MD, codirector of the Center for Drug Safety and Effectiveness at Johns Hopkins University in Baltimore, Maryland, who wasn’t involved in the study, told this news organization.

Higher-dose antipsychotic treatment was significantly associated with overdose deaths (HR, 1.57; 95% CI, 1.02-2.42) and other unintentional injury deaths (HR, 1.57; 95% CI, 1.12-2.22), but not with nonoverdose suicide deaths or cardiovascular/metabolic deaths.
Death certificates listed opioid involvement in more than half of overdose deaths in those taking higher antipsychotic doses as well as those taking control medications.
“That’s a good reminder that the risk of these medicines may increase markedly when they’re combined with other treatments, such as prescription opioids,” Dr. Alexander said.
Also weighing in on the research, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the study is “notable for both the increased risk of death among young adults 18-24 prescribed treatment with antipsychotics at doses greater than 100-mg chlorpromazine equivalents, but also for the absence of such a finding with antipsychotic use in younger age groups,” he said.
“This suggests an interaction between other factors more common to young adults, such as substance use as mentioned by the authors, and concurrent treatment with antipsychotic medications at doses greater than 100-mg chlorpromazine equivalents,” said Dr. Dube.
“As the authors point out, additional research is needed to help clarify the observed increased risk of death at this developmental juncture so as to allow us to better predict which young adults may be especially vulnerable,” Dr. Dube said.
The findings also point to a need for caution when prescribing any antipsychotic medications off label, Dr. Dube added, especially among people aged 18-24 years, and other treatments should be considered when possible.
“Thankfully, with greater awareness and increased scrutiny, overall prescriptions for antipsychotic medications in the pediatric and young adult populations have likely decreased since the study period,” he said.
Limitations of the study include potential residual confounding, confining the study population to Medicaid recipients, restriction to second-generation antipsychotics, and exclusion of individuals with psychoses or severe somatic illness. Also, insufficient numbers of deaths from specific causes precluded an examination of individual antipsychotics or more detailed dose categories.
“No study is perfect,” said Dr. Alexander, “and some of the findings may be due to unmeasured differences between the groups that were being compared. That’s the elephant in the room.”
The study was funded by a grant from the National Institute for Child Health and Human Development. Dr. Ray, Dr. Alexander, and Dr. Dube have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
High doses of a second-generation antipsychotic are associated with a significantly increased risk for death in young adults, adding to longstanding safety concerns regarding the use of higher doses of antipsychotic medication in this age group.
In a large cohort study, people aged 18-24 years had a significantly higher risk for death when starting a second-generation antipsychotic at doses greater than 100-mg chlorpromazine equivalents, but no increased mortality risk with lower doses.
There was no association with mortality risk in children aged 5-17 years with either dose.
“This finding suggests that antipsychotic medication–related fatalities are rare in healthy children without psychosis,” lead investigator Wayne Ray, PhD, from Vanderbilt University School of Medicine in Nashville, Tennessee, and colleagues wrote in a recent study that was published online in JAMA Psychiatry.
“In contrast, young adults aged 18-24 years treated with doses greater than 100-mg chlorpromazine equivalents had 127.5 additional deaths for every 100,000 person-years of exposure, suggesting further investigations of antipsychotic medication safety in this population are needed.”
Large, Retrospective Study
The researchers compared mortality for more than 2 million Medicaid patients aged 5-24 years (mean age, 13 years; 51% men) starting treatment with a second-generation antipsychotic vs control psychiatric medications. None of them had a diagnosis of severe somatic illness, schizophrenia, or related psychosis.
From January 2004 through September 2013, more than 21 million prescriptions were filled — roughly 5.4 million for antipsychotic doses of 100 mg or less, 2.8 million for doses greater than 100 mg, and 13.5 million for control medications.
The most commonly prescribed antipsychotic medication was risperidone, followed by aripiprazole, quetiapine, ziprasidone, and olanzapine. The most commonly prescribed control medication was clonidine, followed by atomoxetine, guanfacine, and sertraline.
In the overall study population, there was no significant association with risk for death for antipsychotic doses less than or equal to 100-mg chlorpromazine equivalents (hazard ratio [HR], 1.08; 95% CI, 0.89-1.32). However, mortality risk was increased at doses greater than 100 mg (HR, 1.37; 95% CI, 1.11-1.70).
Looking at mortality risk by age, for children aged 5-17 years, there was no significant association with either antipsychotic dose, whereas young adults aged 18-24 years had increased risk for doses greater than 100 mg (HR, 1.68; 95% CI, 1.23-2.29).
Start Low, Go Slow
“Start low and go slow is always a good rule of thumb when it comes to the use of these and any medicines, especially among especially among children and adolescents,” Caleb Alexander, MD, codirector of the Center for Drug Safety and Effectiveness at Johns Hopkins University in Baltimore, Maryland, who wasn’t involved in the study, told this news organization.
Higher-dose antipsychotic treatment was significantly associated with overdose deaths (HR, 1.57; 95% CI, 1.02-2.42) and other unintentional injury deaths (HR, 1.57; 95% CI, 1.12-2.22), but not with nonoverdose suicide deaths or cardiovascular/metabolic deaths.
Death certificates listed opioid involvement in more than half of overdose deaths in those taking higher antipsychotic doses as well as those taking control medications.
“That’s a good reminder that the risk of these medicines may increase markedly when they’re combined with other treatments, such as prescription opioids,” Dr. Alexander said.
Also weighing in on the research, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the study is “notable for both the increased risk of death among young adults 18-24 prescribed treatment with antipsychotics at doses greater than 100-mg chlorpromazine equivalents, but also for the absence of such a finding with antipsychotic use in younger age groups,” he said.
“This suggests an interaction between other factors more common to young adults, such as substance use as mentioned by the authors, and concurrent treatment with antipsychotic medications at doses greater than 100-mg chlorpromazine equivalents,” said Dr. Dube.
“As the authors point out, additional research is needed to help clarify the observed increased risk of death at this developmental juncture so as to allow us to better predict which young adults may be especially vulnerable,” Dr. Dube said.
The findings also point to a need for caution when prescribing any antipsychotic medications off label, Dr. Dube added, especially among people aged 18-24 years, and other treatments should be considered when possible.
“Thankfully, with greater awareness and increased scrutiny, overall prescriptions for antipsychotic medications in the pediatric and young adult populations have likely decreased since the study period,” he said.
Limitations of the study include potential residual confounding, confining the study population to Medicaid recipients, restriction to second-generation antipsychotics, and exclusion of individuals with psychoses or severe somatic illness. Also, insufficient numbers of deaths from specific causes precluded an examination of individual antipsychotics or more detailed dose categories.
“No study is perfect,” said Dr. Alexander, “and some of the findings may be due to unmeasured differences between the groups that were being compared. That’s the elephant in the room.”
The study was funded by a grant from the National Institute for Child Health and Human Development. Dr. Ray, Dr. Alexander, and Dr. Dube have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
High doses of a second-generation antipsychotic are associated with a significantly increased risk for death in young adults, adding to longstanding safety concerns regarding the use of higher doses of antipsychotic medication in this age group.
In a large cohort study, people aged 18-24 years had a significantly higher risk for death when starting a second-generation antipsychotic at doses greater than 100-mg chlorpromazine equivalents, but no increased mortality risk with lower doses.
There was no association with mortality risk in children aged 5-17 years with either dose.
“This finding suggests that antipsychotic medication–related fatalities are rare in healthy children without psychosis,” lead investigator Wayne Ray, PhD, from Vanderbilt University School of Medicine in Nashville, Tennessee, and colleagues wrote in a recent study that was published online in JAMA Psychiatry.
“In contrast, young adults aged 18-24 years treated with doses greater than 100-mg chlorpromazine equivalents had 127.5 additional deaths for every 100,000 person-years of exposure, suggesting further investigations of antipsychotic medication safety in this population are needed.”
Large, Retrospective Study
The researchers compared mortality for more than 2 million Medicaid patients aged 5-24 years (mean age, 13 years; 51% men) starting treatment with a second-generation antipsychotic vs control psychiatric medications. None of them had a diagnosis of severe somatic illness, schizophrenia, or related psychosis.
From January 2004 through September 2013, more than 21 million prescriptions were filled — roughly 5.4 million for antipsychotic doses of 100 mg or less, 2.8 million for doses greater than 100 mg, and 13.5 million for control medications.
The most commonly prescribed antipsychotic medication was risperidone, followed by aripiprazole, quetiapine, ziprasidone, and olanzapine. The most commonly prescribed control medication was clonidine, followed by atomoxetine, guanfacine, and sertraline.
In the overall study population, there was no significant association with risk for death for antipsychotic doses less than or equal to 100-mg chlorpromazine equivalents (hazard ratio [HR], 1.08; 95% CI, 0.89-1.32). However, mortality risk was increased at doses greater than 100 mg (HR, 1.37; 95% CI, 1.11-1.70).
Looking at mortality risk by age, for children aged 5-17 years, there was no significant association with either antipsychotic dose, whereas young adults aged 18-24 years had increased risk for doses greater than 100 mg (HR, 1.68; 95% CI, 1.23-2.29).
Start Low, Go Slow
“Start low and go slow is always a good rule of thumb when it comes to the use of these and any medicines, especially among especially among children and adolescents,” Caleb Alexander, MD, codirector of the Center for Drug Safety and Effectiveness at Johns Hopkins University in Baltimore, Maryland, who wasn’t involved in the study, told this news organization.
Higher-dose antipsychotic treatment was significantly associated with overdose deaths (HR, 1.57; 95% CI, 1.02-2.42) and other unintentional injury deaths (HR, 1.57; 95% CI, 1.12-2.22), but not with nonoverdose suicide deaths or cardiovascular/metabolic deaths.
Death certificates listed opioid involvement in more than half of overdose deaths in those taking higher antipsychotic doses as well as those taking control medications.
“That’s a good reminder that the risk of these medicines may increase markedly when they’re combined with other treatments, such as prescription opioids,” Dr. Alexander said.
Also weighing in on the research, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the study is “notable for both the increased risk of death among young adults 18-24 prescribed treatment with antipsychotics at doses greater than 100-mg chlorpromazine equivalents, but also for the absence of such a finding with antipsychotic use in younger age groups,” he said.
“This suggests an interaction between other factors more common to young adults, such as substance use as mentioned by the authors, and concurrent treatment with antipsychotic medications at doses greater than 100-mg chlorpromazine equivalents,” said Dr. Dube.
“As the authors point out, additional research is needed to help clarify the observed increased risk of death at this developmental juncture so as to allow us to better predict which young adults may be especially vulnerable,” Dr. Dube said.
The findings also point to a need for caution when prescribing any antipsychotic medications off label, Dr. Dube added, especially among people aged 18-24 years, and other treatments should be considered when possible.
“Thankfully, with greater awareness and increased scrutiny, overall prescriptions for antipsychotic medications in the pediatric and young adult populations have likely decreased since the study period,” he said.
Limitations of the study include potential residual confounding, confining the study population to Medicaid recipients, restriction to second-generation antipsychotics, and exclusion of individuals with psychoses or severe somatic illness. Also, insufficient numbers of deaths from specific causes precluded an examination of individual antipsychotics or more detailed dose categories.
“No study is perfect,” said Dr. Alexander, “and some of the findings may be due to unmeasured differences between the groups that were being compared. That’s the elephant in the room.”
The study was funded by a grant from the National Institute for Child Health and Human Development. Dr. Ray, Dr. Alexander, and Dr. Dube have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JAMA PSYCHIATRY
AGA Publishes New Pouchitis Management Guideline
The American Gastroenterological Association (AGA) has published a new clinical practice guideline on the management of pouchitis and inflammatory pouch disorders.
The guidance document, authored by Edward L. Barnes, MD, of the University of North Carolina at Chapel Hill and colleagues, includes eleven conditional recommendations that steer usage of probiotics, antibiotics, and immunosuppressive therapies in patients with these conditions, which occur most often after restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC).

“Multiple strategies have been utilized in the treatment and prevention of pouchitis and inflammatory pouch conditions, including antibiotics, probiotics, corticosteroids, and advanced immunosuppressive therapies including biologics and oral small-molecule drugs,” the guideline panelists wrote on the AGA website. “However, most of the evidence base is primarily derived from retrospective observational studies or comparisons of small cohorts. Data on patients’ values and preferences for specific management decisions and treatment choices are also limited. This results in substantial practice variability.”
Still, the area is advancing. Dr. Barnes and colleagues highlighted new scoring systems for characterizing endoscopic findings and patient-reported outcomes, as well as the recent EARNEST trial (N Engl J Med. 2023 Mar 30;388(13):1191-1200), which compared vedolizumab with placebo in patients with chronic refractory pouchitis, and should be considered a “landmark study in the field,” as it could shape future trial design.
Based on all available evidence and clinical experience, the panelists issued the following recommendations, which were approved by the AGA Governing Board.
Probiotics
Because of a knowledge gap, the guideline makes no recommendation for or against use of probiotics for either the primary prevention or treatment of pouchitis.
They offered a similar explanation for the lack of guidance on using probiotics to treat pouchitis, and noted that antibiotics have demonstrated effectiveness where probiotics have not, making them the preferred treatment choice.
“There is potential that delaying therapy or using probiotics when they are not as effective as antibiotics may have significant impact on an individual patient’s quality of life,” Dr. Barnes and colleagues noted.
In contrast with the above statements, the guideline recommends usage of probiotics to prevent recurrent pouchitis in patients with recurrent, antibiotic-responsive pouchitis.
The De Simone formulation of multistrain probiotics is best supported in this scenario, the guideline notes, as this product was used in clinical trials, which collectively showed an 87% reduced risk of relapse over 12 months.
Antibiotics
Although the guideline supports antibiotics for prevention of pouchitis, the panelists noted that only one randomized controlled trial supports this recommendation, and negative effects of long-term usage need to be considered, including promotion of drug-resistant organisms and risk of Clostridioides difficile infection.
Dr. Barnes and colleagues cited more data supporting antibiotics for treatment of pouchitis, and noted that metronidazole and/or ciprofloxacin remain the preferred choices, with a typical duration of 2-4 weeks.
“An approach using a combination of antibiotics may be more effective in patients who do not respond to single-antibiotic therapy,” the panelists wrote, noting that oral vancomycin may also be considered when a patient does not respond to initial therapy.
For patients with recurrent pouchitis that relapses shortly after discontinuing antibiotics, chronic antibiotics should be considered, according to the guideline.
Immunosuppressive therapies
Advanced immunosuppressive therapies are recommended for patients with chronic antibiotic-dependent pouchitis, including those approved for treatment of UC or Crohn’s disease.
“Advanced immunosuppressive therapies may be used in lieu of chronic, continuous antibiotic therapy, particularly in patients who are intolerant to antibiotics or where patients and/or providers are concerned about risks of long-term antibiotic therapy,” the panelists wrote.
For patients with chronic antibiotic-refractory pouchitis, the guideline makes a general recommendation for advanced immunosuppressive therapies while specifically noting that vedolizumab has a greater strength of evidence in this scenario, citing the EARNEST trial.
A separate recommendation for corticosteroids is made for the same patient group, with ileal-release budesonide remaining the preferred formulation. In contrast, mesalamine is not recommended, based on a lack of supporting evidence.
Finally, the panelists recommend using corticosteroids in patients with Crohn’s-like disease of the pouch.
Future directions
“Even though pouchitis is relatively common after IPAA for UC, we observed that most of the evidence informing these guidelines was low to very low quality, derived from case series or small cohort studies, and several knowledge gaps exist,” Dr. Barnes and colleagues wrote. “Several initiatives towards improving management of inflammatory pouch disorders are already underway. However, concerted efforts in key domains are central towards improving patient care.”
They suggested that research should focus on standardizing disease entities, characterizing natural history and risk factors for inflammatory disorders of the pouch, and improving clinical trial design.The guideline was funded by the AGA Institute. The panelists disclosed relationships with Bristol-Myers Squibb, Sandoz, AbbVie, and others.
The American Gastroenterological Association (AGA) has published a new clinical practice guideline on the management of pouchitis and inflammatory pouch disorders.
The guidance document, authored by Edward L. Barnes, MD, of the University of North Carolina at Chapel Hill and colleagues, includes eleven conditional recommendations that steer usage of probiotics, antibiotics, and immunosuppressive therapies in patients with these conditions, which occur most often after restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC).
“Multiple strategies have been utilized in the treatment and prevention of pouchitis and inflammatory pouch conditions, including antibiotics, probiotics, corticosteroids, and advanced immunosuppressive therapies including biologics and oral small-molecule drugs,” the guideline panelists wrote on the AGA website. “However, most of the evidence base is primarily derived from retrospective observational studies or comparisons of small cohorts. Data on patients’ values and preferences for specific management decisions and treatment choices are also limited. This results in substantial practice variability.”
Still, the area is advancing. Dr. Barnes and colleagues highlighted new scoring systems for characterizing endoscopic findings and patient-reported outcomes, as well as the recent EARNEST trial (N Engl J Med. 2023 Mar 30;388(13):1191-1200), which compared vedolizumab with placebo in patients with chronic refractory pouchitis, and should be considered a “landmark study in the field,” as it could shape future trial design.
Based on all available evidence and clinical experience, the panelists issued the following recommendations, which were approved by the AGA Governing Board.
Probiotics
Because of a knowledge gap, the guideline makes no recommendation for or against use of probiotics for either the primary prevention or treatment of pouchitis.
They offered a similar explanation for the lack of guidance on using probiotics to treat pouchitis, and noted that antibiotics have demonstrated effectiveness where probiotics have not, making them the preferred treatment choice.
“There is potential that delaying therapy or using probiotics when they are not as effective as antibiotics may have significant impact on an individual patient’s quality of life,” Dr. Barnes and colleagues noted.
In contrast with the above statements, the guideline recommends usage of probiotics to prevent recurrent pouchitis in patients with recurrent, antibiotic-responsive pouchitis.
The De Simone formulation of multistrain probiotics is best supported in this scenario, the guideline notes, as this product was used in clinical trials, which collectively showed an 87% reduced risk of relapse over 12 months.
Antibiotics
Although the guideline supports antibiotics for prevention of pouchitis, the panelists noted that only one randomized controlled trial supports this recommendation, and negative effects of long-term usage need to be considered, including promotion of drug-resistant organisms and risk of Clostridioides difficile infection.
Dr. Barnes and colleagues cited more data supporting antibiotics for treatment of pouchitis, and noted that metronidazole and/or ciprofloxacin remain the preferred choices, with a typical duration of 2-4 weeks.
“An approach using a combination of antibiotics may be more effective in patients who do not respond to single-antibiotic therapy,” the panelists wrote, noting that oral vancomycin may also be considered when a patient does not respond to initial therapy.
For patients with recurrent pouchitis that relapses shortly after discontinuing antibiotics, chronic antibiotics should be considered, according to the guideline.
Immunosuppressive therapies
Advanced immunosuppressive therapies are recommended for patients with chronic antibiotic-dependent pouchitis, including those approved for treatment of UC or Crohn’s disease.
“Advanced immunosuppressive therapies may be used in lieu of chronic, continuous antibiotic therapy, particularly in patients who are intolerant to antibiotics or where patients and/or providers are concerned about risks of long-term antibiotic therapy,” the panelists wrote.
For patients with chronic antibiotic-refractory pouchitis, the guideline makes a general recommendation for advanced immunosuppressive therapies while specifically noting that vedolizumab has a greater strength of evidence in this scenario, citing the EARNEST trial.
A separate recommendation for corticosteroids is made for the same patient group, with ileal-release budesonide remaining the preferred formulation. In contrast, mesalamine is not recommended, based on a lack of supporting evidence.
Finally, the panelists recommend using corticosteroids in patients with Crohn’s-like disease of the pouch.
Future directions
“Even though pouchitis is relatively common after IPAA for UC, we observed that most of the evidence informing these guidelines was low to very low quality, derived from case series or small cohort studies, and several knowledge gaps exist,” Dr. Barnes and colleagues wrote. “Several initiatives towards improving management of inflammatory pouch disorders are already underway. However, concerted efforts in key domains are central towards improving patient care.”
They suggested that research should focus on standardizing disease entities, characterizing natural history and risk factors for inflammatory disorders of the pouch, and improving clinical trial design.The guideline was funded by the AGA Institute. The panelists disclosed relationships with Bristol-Myers Squibb, Sandoz, AbbVie, and others.
The American Gastroenterological Association (AGA) has published a new clinical practice guideline on the management of pouchitis and inflammatory pouch disorders.
The guidance document, authored by Edward L. Barnes, MD, of the University of North Carolina at Chapel Hill and colleagues, includes eleven conditional recommendations that steer usage of probiotics, antibiotics, and immunosuppressive therapies in patients with these conditions, which occur most often after restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC).
“Multiple strategies have been utilized in the treatment and prevention of pouchitis and inflammatory pouch conditions, including antibiotics, probiotics, corticosteroids, and advanced immunosuppressive therapies including biologics and oral small-molecule drugs,” the guideline panelists wrote on the AGA website. “However, most of the evidence base is primarily derived from retrospective observational studies or comparisons of small cohorts. Data on patients’ values and preferences for specific management decisions and treatment choices are also limited. This results in substantial practice variability.”
Still, the area is advancing. Dr. Barnes and colleagues highlighted new scoring systems for characterizing endoscopic findings and patient-reported outcomes, as well as the recent EARNEST trial (N Engl J Med. 2023 Mar 30;388(13):1191-1200), which compared vedolizumab with placebo in patients with chronic refractory pouchitis, and should be considered a “landmark study in the field,” as it could shape future trial design.
Based on all available evidence and clinical experience, the panelists issued the following recommendations, which were approved by the AGA Governing Board.
Probiotics
Because of a knowledge gap, the guideline makes no recommendation for or against use of probiotics for either the primary prevention or treatment of pouchitis.
They offered a similar explanation for the lack of guidance on using probiotics to treat pouchitis, and noted that antibiotics have demonstrated effectiveness where probiotics have not, making them the preferred treatment choice.
“There is potential that delaying therapy or using probiotics when they are not as effective as antibiotics may have significant impact on an individual patient’s quality of life,” Dr. Barnes and colleagues noted.
In contrast with the above statements, the guideline recommends usage of probiotics to prevent recurrent pouchitis in patients with recurrent, antibiotic-responsive pouchitis.
The De Simone formulation of multistrain probiotics is best supported in this scenario, the guideline notes, as this product was used in clinical trials, which collectively showed an 87% reduced risk of relapse over 12 months.
Antibiotics
Although the guideline supports antibiotics for prevention of pouchitis, the panelists noted that only one randomized controlled trial supports this recommendation, and negative effects of long-term usage need to be considered, including promotion of drug-resistant organisms and risk of Clostridioides difficile infection.
Dr. Barnes and colleagues cited more data supporting antibiotics for treatment of pouchitis, and noted that metronidazole and/or ciprofloxacin remain the preferred choices, with a typical duration of 2-4 weeks.
“An approach using a combination of antibiotics may be more effective in patients who do not respond to single-antibiotic therapy,” the panelists wrote, noting that oral vancomycin may also be considered when a patient does not respond to initial therapy.
For patients with recurrent pouchitis that relapses shortly after discontinuing antibiotics, chronic antibiotics should be considered, according to the guideline.
Immunosuppressive therapies
Advanced immunosuppressive therapies are recommended for patients with chronic antibiotic-dependent pouchitis, including those approved for treatment of UC or Crohn’s disease.
“Advanced immunosuppressive therapies may be used in lieu of chronic, continuous antibiotic therapy, particularly in patients who are intolerant to antibiotics or where patients and/or providers are concerned about risks of long-term antibiotic therapy,” the panelists wrote.
For patients with chronic antibiotic-refractory pouchitis, the guideline makes a general recommendation for advanced immunosuppressive therapies while specifically noting that vedolizumab has a greater strength of evidence in this scenario, citing the EARNEST trial.
A separate recommendation for corticosteroids is made for the same patient group, with ileal-release budesonide remaining the preferred formulation. In contrast, mesalamine is not recommended, based on a lack of supporting evidence.
Finally, the panelists recommend using corticosteroids in patients with Crohn’s-like disease of the pouch.
Future directions
“Even though pouchitis is relatively common after IPAA for UC, we observed that most of the evidence informing these guidelines was low to very low quality, derived from case series or small cohort studies, and several knowledge gaps exist,” Dr. Barnes and colleagues wrote. “Several initiatives towards improving management of inflammatory pouch disorders are already underway. However, concerted efforts in key domains are central towards improving patient care.”
They suggested that research should focus on standardizing disease entities, characterizing natural history and risk factors for inflammatory disorders of the pouch, and improving clinical trial design.The guideline was funded by the AGA Institute. The panelists disclosed relationships with Bristol-Myers Squibb, Sandoz, AbbVie, and others.
FROM THE AMERICAN GASTROENTEROLOGICAL ASSOCIATION
Chest pain and shortness of breath
In a lifelong smoker, a tumor in the periphery of the lung and histology showing glandular cells with some neuroendocrine differentiation is most likely large cell carcinoma, a type of non–small cell lung cancer (NSCLC). Although small cell lung cancer is also associated with smoking, histology typically demonstrates highly cellular aspirates with small blue cells with very scant or null cytoplasm, loosely arranged or in a syncytial pattern. Bronchial adenoma is unlikely, given the patient's unintentional weight loss and fatigue over the past few months. Mesothelioma is most associated with asbestos exposure and is found in the lung pleura, which typically presents with pleural effusion.
Lung cancer is the top cause of cancer deaths in the US, second only to prostate cancer in men and breast cancer in women; approximately 85% of all lung cancers are classified as NSCLC. Histologically, NSCLC is further categorized into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma (LCC). When a patient presents with intrathoracic symptoms (including cough, chest pain, wheezing, or dyspnea) and a pulmonary nodule on chest radiography, NSCLC is typically suspected as a possible diagnosis. Smoking is the most common cause of this lung cancer (78% in men, 90% in women).
Several methods confirm the diagnosis of NSCLC, including bronchoscopy, sputum cytology, mediastinoscopy, thoracentesis, thoracoscopy, and transthoracic needle biopsy. Which method is chosen depends on the primary lesion location and accessibility. Histologic evaluation helps differentiate between the various subtypes of NSCLC. LCC is a subset of NSCLC that is a diagnosis of exclusion. Histologically, LCC is poorly differentiated, and 90% of cases will show squamous, glandular, or neuroendocrine differentiation.
When first diagnosed with NSCLC, 20% of patients have cancer confined to a specific area, 25% of patients have cancer that has spread to nearby areas, and 55% of patients have cancer that has spread to distant body parts. The specific symptoms experienced by patients will vary depending on the location of the cancer. The prognosis for NSCLC depends on the staging of the tumor, nodes, and metastases, the patient's performance status, and any existing health conditions. In the US, the 5-year relative survival rate is 61.2% for localized disease, 33.5% for regional disease, and 7.0% for disease with distant metastases.
Treatment of NSCLC also varies according to the patient's functional status, tumor stage, molecular characteristics, and comorbidities. Generally, patients with stage I, II, or III NSCLC are treated with the intent to cure, which can include surgery, chemotherapy, radiation therapy, or a combined approach. Lobectomy or resection is generally accepted as an approach for surgical intervention on early-stage NSCLC; however, for stages higher than IB (including stage II/III), patients are recommended to undergo adjuvant chemotherapy. Patients with stage IV disease (or recurrence after initial management) are typically treated with systemic therapy or should be considered for palliative treatment to improve quality of life and overall survival.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
In a lifelong smoker, a tumor in the periphery of the lung and histology showing glandular cells with some neuroendocrine differentiation is most likely large cell carcinoma, a type of non–small cell lung cancer (NSCLC). Although small cell lung cancer is also associated with smoking, histology typically demonstrates highly cellular aspirates with small blue cells with very scant or null cytoplasm, loosely arranged or in a syncytial pattern. Bronchial adenoma is unlikely, given the patient's unintentional weight loss and fatigue over the past few months. Mesothelioma is most associated with asbestos exposure and is found in the lung pleura, which typically presents with pleural effusion.
Lung cancer is the top cause of cancer deaths in the US, second only to prostate cancer in men and breast cancer in women; approximately 85% of all lung cancers are classified as NSCLC. Histologically, NSCLC is further categorized into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma (LCC). When a patient presents with intrathoracic symptoms (including cough, chest pain, wheezing, or dyspnea) and a pulmonary nodule on chest radiography, NSCLC is typically suspected as a possible diagnosis. Smoking is the most common cause of this lung cancer (78% in men, 90% in women).
Several methods confirm the diagnosis of NSCLC, including bronchoscopy, sputum cytology, mediastinoscopy, thoracentesis, thoracoscopy, and transthoracic needle biopsy. Which method is chosen depends on the primary lesion location and accessibility. Histologic evaluation helps differentiate between the various subtypes of NSCLC. LCC is a subset of NSCLC that is a diagnosis of exclusion. Histologically, LCC is poorly differentiated, and 90% of cases will show squamous, glandular, or neuroendocrine differentiation.
When first diagnosed with NSCLC, 20% of patients have cancer confined to a specific area, 25% of patients have cancer that has spread to nearby areas, and 55% of patients have cancer that has spread to distant body parts. The specific symptoms experienced by patients will vary depending on the location of the cancer. The prognosis for NSCLC depends on the staging of the tumor, nodes, and metastases, the patient's performance status, and any existing health conditions. In the US, the 5-year relative survival rate is 61.2% for localized disease, 33.5% for regional disease, and 7.0% for disease with distant metastases.
Treatment of NSCLC also varies according to the patient's functional status, tumor stage, molecular characteristics, and comorbidities. Generally, patients with stage I, II, or III NSCLC are treated with the intent to cure, which can include surgery, chemotherapy, radiation therapy, or a combined approach. Lobectomy or resection is generally accepted as an approach for surgical intervention on early-stage NSCLC; however, for stages higher than IB (including stage II/III), patients are recommended to undergo adjuvant chemotherapy. Patients with stage IV disease (or recurrence after initial management) are typically treated with systemic therapy or should be considered for palliative treatment to improve quality of life and overall survival.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
In a lifelong smoker, a tumor in the periphery of the lung and histology showing glandular cells with some neuroendocrine differentiation is most likely large cell carcinoma, a type of non–small cell lung cancer (NSCLC). Although small cell lung cancer is also associated with smoking, histology typically demonstrates highly cellular aspirates with small blue cells with very scant or null cytoplasm, loosely arranged or in a syncytial pattern. Bronchial adenoma is unlikely, given the patient's unintentional weight loss and fatigue over the past few months. Mesothelioma is most associated with asbestos exposure and is found in the lung pleura, which typically presents with pleural effusion.
Lung cancer is the top cause of cancer deaths in the US, second only to prostate cancer in men and breast cancer in women; approximately 85% of all lung cancers are classified as NSCLC. Histologically, NSCLC is further categorized into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma (LCC). When a patient presents with intrathoracic symptoms (including cough, chest pain, wheezing, or dyspnea) and a pulmonary nodule on chest radiography, NSCLC is typically suspected as a possible diagnosis. Smoking is the most common cause of this lung cancer (78% in men, 90% in women).
Several methods confirm the diagnosis of NSCLC, including bronchoscopy, sputum cytology, mediastinoscopy, thoracentesis, thoracoscopy, and transthoracic needle biopsy. Which method is chosen depends on the primary lesion location and accessibility. Histologic evaluation helps differentiate between the various subtypes of NSCLC. LCC is a subset of NSCLC that is a diagnosis of exclusion. Histologically, LCC is poorly differentiated, and 90% of cases will show squamous, glandular, or neuroendocrine differentiation.
When first diagnosed with NSCLC, 20% of patients have cancer confined to a specific area, 25% of patients have cancer that has spread to nearby areas, and 55% of patients have cancer that has spread to distant body parts. The specific symptoms experienced by patients will vary depending on the location of the cancer. The prognosis for NSCLC depends on the staging of the tumor, nodes, and metastases, the patient's performance status, and any existing health conditions. In the US, the 5-year relative survival rate is 61.2% for localized disease, 33.5% for regional disease, and 7.0% for disease with distant metastases.
Treatment of NSCLC also varies according to the patient's functional status, tumor stage, molecular characteristics, and comorbidities. Generally, patients with stage I, II, or III NSCLC are treated with the intent to cure, which can include surgery, chemotherapy, radiation therapy, or a combined approach. Lobectomy or resection is generally accepted as an approach for surgical intervention on early-stage NSCLC; however, for stages higher than IB (including stage II/III), patients are recommended to undergo adjuvant chemotherapy. Patients with stage IV disease (or recurrence after initial management) are typically treated with systemic therapy or should be considered for palliative treatment to improve quality of life and overall survival.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
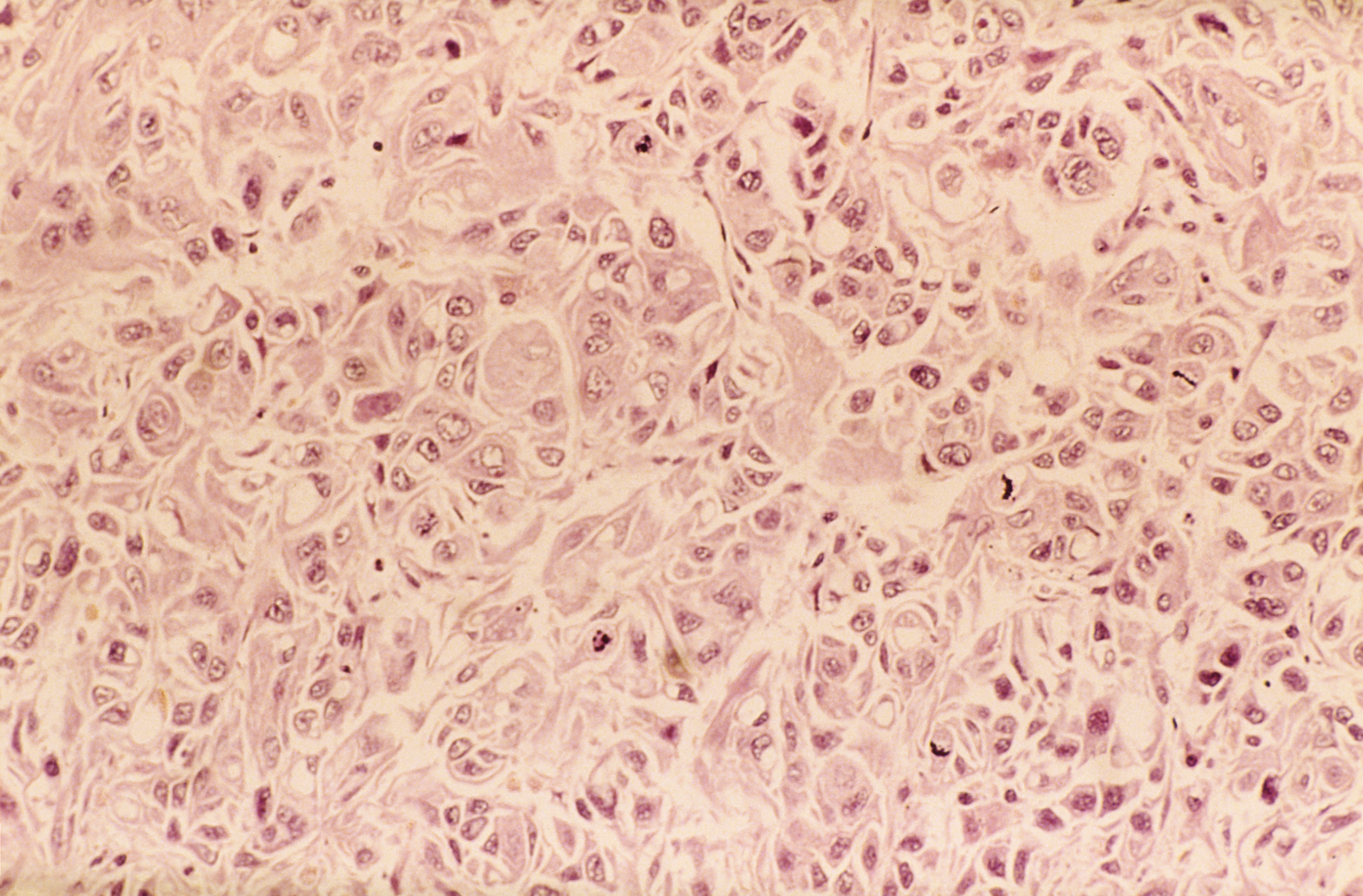
A 62-year-old man presents to his primary care physician with a persistent cough, dyspnea, unintentional weight loss, and fatigue over the past few months. He has a history of smoking for 30 years but quit 5 years ago. He also reports occasional chest pain and shortness of breath during physical activities. Physical examination reveals crackles in the middle lobe of the right lung. The patient occasionally coughs up blood. Chest radiography shows a large mass in the right lung, and a subsequent CT scan confirms a large peripheral mass of solid attenuation with an irregular margin. The patient undergoes thoracoscopy to obtain a biopsy sample from the tumor for further analysis. The biopsy reveals glandular cells with some neuroendocrine differentiation.
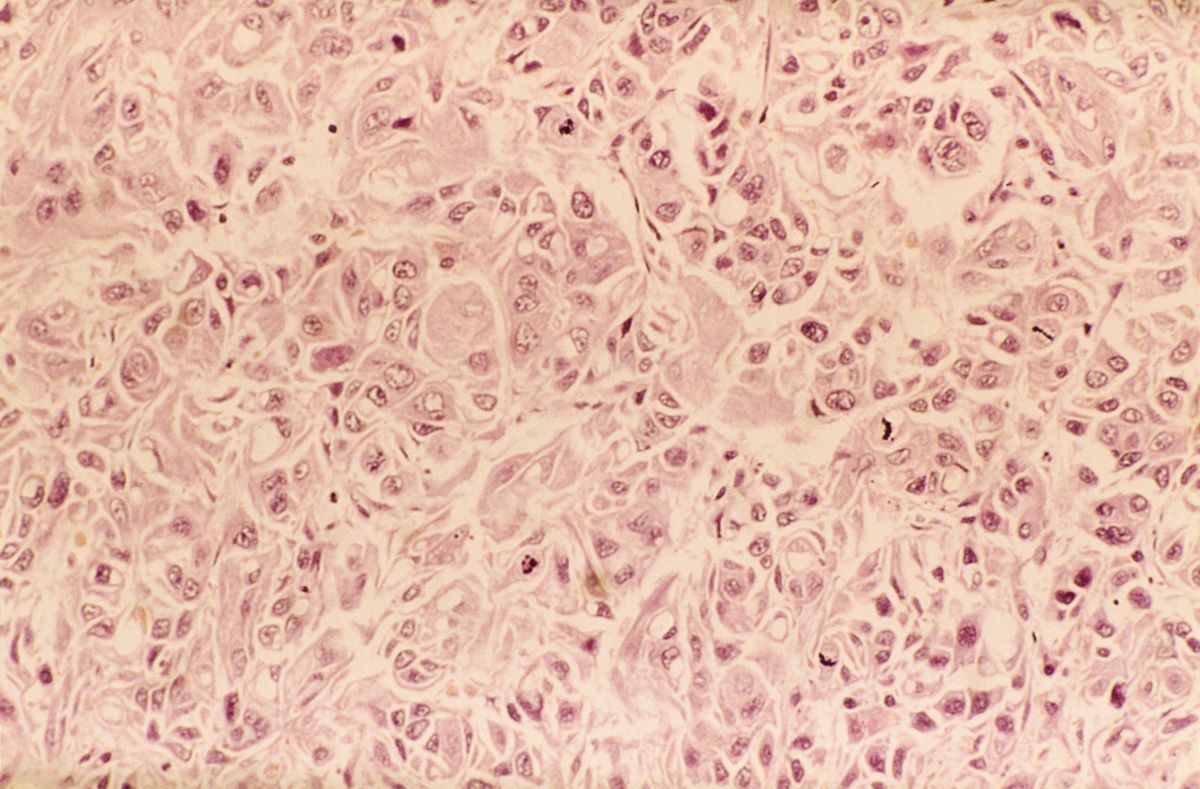
Delayed Meals Tied to Increased CVD Risk
TOPLINE:
(CVDs), especially in women, results of a large prospective study suggested.
METHODOLOGY:
- The study included 103,389 participants, mean baseline age 42.6 years and 79% women, who were volunteers in the ongoing NutriNet-Santé, a cohort study launched in France to better understand the relationship between nutrition and health.
- Participants completed questionnaires that in addition to data on socio-demographics, lifestyle, and physical activity provided information on when foods and beverages were consumed during each day, and they self-reported major health events, including CVDs.
- Researchers assessed associations between time of first meal of the day (before 8 am, 8-9 am, after 9 am) and last meal (before 8 pm, 8-9 pm, after 9 pm), number of eating occasions, and duration of nighttime fasting (12 h or less, 12-13 h, more than 13 h) and the risk for CVD, controlling for a large number of potential confounders, among them age, sex, education, income, smoking, and physical activity level.
- During a median follow-up of 7.2 years, 2036 cases of overall CVD, 988 cases of cerebrovascular disease (stroke, transient ischemic attack), and 1071 cases of coronary heart diseases (myocardial infraction, angina pectoris, acute coronary syndrome, angioplasty) were reported.
TAKEAWAY:
- Each additional hour delaying the time of the first meal of the day was associated with a higher risk for overall CVD (hazard ratio [HR], 1.06; 95% CI, 1.01-1.12; P = .02), with the association stronger in women than in men.
- Each additional hour in delaying the time of the last meal was associated with an increased risk for cerebrovascular disease; here, a last meal after 9 pm was associated with a 28% higher risk than a meal before 8 pm (HR, 1.28; 95% CI, 1.05-1.55; P < .01).
- There was no association between number of eating occasions and either overall CVD or cerebrovascular disease and no association between meal timing or number of eating occasions and risk for coronary heart disease.
- Each hour increase in nighttime fasting was associated with a 7% lower risk for cerebrovascular disease (HR, 0.93; 95% CI, 0.87-0.99; P = .02) but not with a risk for overall CVD or coronary heart disease.
IN PRACTICE:
“Our results suggest a potential benefit of adopting earlier eating timing patterns and coupling a longer nighttime fasting period with an early last meal, rather than breakfast skipping, in CVD prevention,” the authors wrote.
SOURCE:
The study was conducted by Anna Palomar-Cros, Barcelona Institute for Global Health and Department of Experimental and Health Sciences, Universitat Pompeu Fabra, Barcelona, Spain, and colleagues. It was published online on December 14, 2023, in Nature Communications.
LIMITATIONS:
Information on shift work, exposure to night light, use of recreational drugs, and timing of physical activity, medication or alcohol consumption, all of which are potential disruptors of circadian rhythms, was not available, and sleep time and duration were available for only a subgroup of patients. Unknown or unmeasured potential confounders (eg, being awakened by children) could have contributed to residual confounding. Reverse causation bias linked to change in behaviors in people with poor health having difficulty getting out of bed in the mornings can’t be ruled out. Participants in the NutriNet-Santé cohort are more likely to be women, have a higher socioeconomic status, and healthier behavior patterns than the general population, perhaps limiting extrapolation of results.
DISCLOSURES:
The NutriNet-Santé study is supported by Ministère de la Santé, Santé Publique France, Institut National de la Santé et de la Recherche Médicale (INSERM), Institut national de recherche pour l’agriculture, l’alimentation et l’environnement (INRAE), Conservatoire National des Arts et Métiers (CNAM), and Université Sorbonne Paris Nord. The authors had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
(CVDs), especially in women, results of a large prospective study suggested.
METHODOLOGY:
- The study included 103,389 participants, mean baseline age 42.6 years and 79% women, who were volunteers in the ongoing NutriNet-Santé, a cohort study launched in France to better understand the relationship between nutrition and health.
- Participants completed questionnaires that in addition to data on socio-demographics, lifestyle, and physical activity provided information on when foods and beverages were consumed during each day, and they self-reported major health events, including CVDs.
- Researchers assessed associations between time of first meal of the day (before 8 am, 8-9 am, after 9 am) and last meal (before 8 pm, 8-9 pm, after 9 pm), number of eating occasions, and duration of nighttime fasting (12 h or less, 12-13 h, more than 13 h) and the risk for CVD, controlling for a large number of potential confounders, among them age, sex, education, income, smoking, and physical activity level.
- During a median follow-up of 7.2 years, 2036 cases of overall CVD, 988 cases of cerebrovascular disease (stroke, transient ischemic attack), and 1071 cases of coronary heart diseases (myocardial infraction, angina pectoris, acute coronary syndrome, angioplasty) were reported.
TAKEAWAY:
- Each additional hour delaying the time of the first meal of the day was associated with a higher risk for overall CVD (hazard ratio [HR], 1.06; 95% CI, 1.01-1.12; P = .02), with the association stronger in women than in men.
- Each additional hour in delaying the time of the last meal was associated with an increased risk for cerebrovascular disease; here, a last meal after 9 pm was associated with a 28% higher risk than a meal before 8 pm (HR, 1.28; 95% CI, 1.05-1.55; P < .01).
- There was no association between number of eating occasions and either overall CVD or cerebrovascular disease and no association between meal timing or number of eating occasions and risk for coronary heart disease.
- Each hour increase in nighttime fasting was associated with a 7% lower risk for cerebrovascular disease (HR, 0.93; 95% CI, 0.87-0.99; P = .02) but not with a risk for overall CVD or coronary heart disease.
IN PRACTICE:
“Our results suggest a potential benefit of adopting earlier eating timing patterns and coupling a longer nighttime fasting period with an early last meal, rather than breakfast skipping, in CVD prevention,” the authors wrote.
SOURCE:
The study was conducted by Anna Palomar-Cros, Barcelona Institute for Global Health and Department of Experimental and Health Sciences, Universitat Pompeu Fabra, Barcelona, Spain, and colleagues. It was published online on December 14, 2023, in Nature Communications.
LIMITATIONS:
Information on shift work, exposure to night light, use of recreational drugs, and timing of physical activity, medication or alcohol consumption, all of which are potential disruptors of circadian rhythms, was not available, and sleep time and duration were available for only a subgroup of patients. Unknown or unmeasured potential confounders (eg, being awakened by children) could have contributed to residual confounding. Reverse causation bias linked to change in behaviors in people with poor health having difficulty getting out of bed in the mornings can’t be ruled out. Participants in the NutriNet-Santé cohort are more likely to be women, have a higher socioeconomic status, and healthier behavior patterns than the general population, perhaps limiting extrapolation of results.
DISCLOSURES:
The NutriNet-Santé study is supported by Ministère de la Santé, Santé Publique France, Institut National de la Santé et de la Recherche Médicale (INSERM), Institut national de recherche pour l’agriculture, l’alimentation et l’environnement (INRAE), Conservatoire National des Arts et Métiers (CNAM), and Université Sorbonne Paris Nord. The authors had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
(CVDs), especially in women, results of a large prospective study suggested.
METHODOLOGY:
- The study included 103,389 participants, mean baseline age 42.6 years and 79% women, who were volunteers in the ongoing NutriNet-Santé, a cohort study launched in France to better understand the relationship between nutrition and health.
- Participants completed questionnaires that in addition to data on socio-demographics, lifestyle, and physical activity provided information on when foods and beverages were consumed during each day, and they self-reported major health events, including CVDs.
- Researchers assessed associations between time of first meal of the day (before 8 am, 8-9 am, after 9 am) and last meal (before 8 pm, 8-9 pm, after 9 pm), number of eating occasions, and duration of nighttime fasting (12 h or less, 12-13 h, more than 13 h) and the risk for CVD, controlling for a large number of potential confounders, among them age, sex, education, income, smoking, and physical activity level.
- During a median follow-up of 7.2 years, 2036 cases of overall CVD, 988 cases of cerebrovascular disease (stroke, transient ischemic attack), and 1071 cases of coronary heart diseases (myocardial infraction, angina pectoris, acute coronary syndrome, angioplasty) were reported.
TAKEAWAY:
- Each additional hour delaying the time of the first meal of the day was associated with a higher risk for overall CVD (hazard ratio [HR], 1.06; 95% CI, 1.01-1.12; P = .02), with the association stronger in women than in men.
- Each additional hour in delaying the time of the last meal was associated with an increased risk for cerebrovascular disease; here, a last meal after 9 pm was associated with a 28% higher risk than a meal before 8 pm (HR, 1.28; 95% CI, 1.05-1.55; P < .01).
- There was no association between number of eating occasions and either overall CVD or cerebrovascular disease and no association between meal timing or number of eating occasions and risk for coronary heart disease.
- Each hour increase in nighttime fasting was associated with a 7% lower risk for cerebrovascular disease (HR, 0.93; 95% CI, 0.87-0.99; P = .02) but not with a risk for overall CVD or coronary heart disease.
IN PRACTICE:
“Our results suggest a potential benefit of adopting earlier eating timing patterns and coupling a longer nighttime fasting period with an early last meal, rather than breakfast skipping, in CVD prevention,” the authors wrote.
SOURCE:
The study was conducted by Anna Palomar-Cros, Barcelona Institute for Global Health and Department of Experimental and Health Sciences, Universitat Pompeu Fabra, Barcelona, Spain, and colleagues. It was published online on December 14, 2023, in Nature Communications.
LIMITATIONS:
Information on shift work, exposure to night light, use of recreational drugs, and timing of physical activity, medication or alcohol consumption, all of which are potential disruptors of circadian rhythms, was not available, and sleep time and duration were available for only a subgroup of patients. Unknown or unmeasured potential confounders (eg, being awakened by children) could have contributed to residual confounding. Reverse causation bias linked to change in behaviors in people with poor health having difficulty getting out of bed in the mornings can’t be ruled out. Participants in the NutriNet-Santé cohort are more likely to be women, have a higher socioeconomic status, and healthier behavior patterns than the general population, perhaps limiting extrapolation of results.
DISCLOSURES:
The NutriNet-Santé study is supported by Ministère de la Santé, Santé Publique France, Institut National de la Santé et de la Recherche Médicale (INSERM), Institut national de recherche pour l’agriculture, l’alimentation et l’environnement (INRAE), Conservatoire National des Arts et Métiers (CNAM), and Université Sorbonne Paris Nord. The authors had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.