User login
Original Study: Should Nitrofurantoin Be Used to Treat Alkaline Urinary Tract Infection?
Background
Urinary tract infections (UTIs), one of the most common human bacterial infections, affect approximately 150 million people annually worldwide.1,2 In the United States, UTIs account for approximately 1% of all outpatient clinic visits and about 2 to 3 million ED visits annually.1,3-5
Although the urine pH level is frequently assessed in urinalysis, it is rarely considered in the management of a patient with a UTI.
Reports correlating urine pH with urine culture data from ED patients with UTIs are lacking. While poorly studied, there are multiple factors that could potentially alter the urine pH of patients with a UTI, including blood pH, diabetes, dehydration, ketosis, drugs, and renal function, as well as factors related to the infecting microorganism. For instance, Proteus mirabilis produces urease, an enzyme that hydrolyzes urea to ammonia and carbon dioxide.6-8
Objective
The objective of this study is to assess the relationship between the urine pH and the infecting microbe in ED patients diagnosed with UTIs, and to determine if P mirabilis is associated with alkaline urine.
Methods
We obtained approval from our Institutional Review Board to retrospectively obtain electronic medical record data from patients aged 18 years and older who presented to our institution’s ED and who were diagnosed with either cystitis or a UTI between January 1, 2012 and March 31, 2015. Both urine pH level and a urine culture were obtained for all patients.
The results of all of the patients’ urinary cultures in our study were positive for one bacterial species or genera (≥100,000 CFU/mL). The International Classification of Disease, Ninth Revision/Tenth Revision codes used to identify patients with cystitis and UTI were as follows: 595.0, 595.1, 595.9, 599.0, N30.91, N30.90, N30.80, N30.81, N30.00, N30.01, N30.20, N30.20, and N39.0.
To ensure that the focus of our study was limited to cystitis and UTIs, we excluded patients who were diagnosed with pyelonephritis, sexually transmitted infection, pelvic inflammatory disease, or vaginal discharge. The urine pH values reported from the clinical laboratory were 5.0, 5.5, 6.0, 6.5, 7.0. 7.5, 8.0, 8.5, and 9.0. Our dataset contained 1,331 clinical encounters. We used descriptive statistics and unpaired t-tests to evaluate the associations between urine pH values and the different microbes.
Results
Data were categorized into 16 different bacterial genera or species. Acinetobacter (n = 1), Kluyvera ascorbata (n = 2), and Stenotrophomonas maltophilia (n = 3) were underrepresented in the dataset and therefore were not included in the data analysis. The data are summarized in the Table.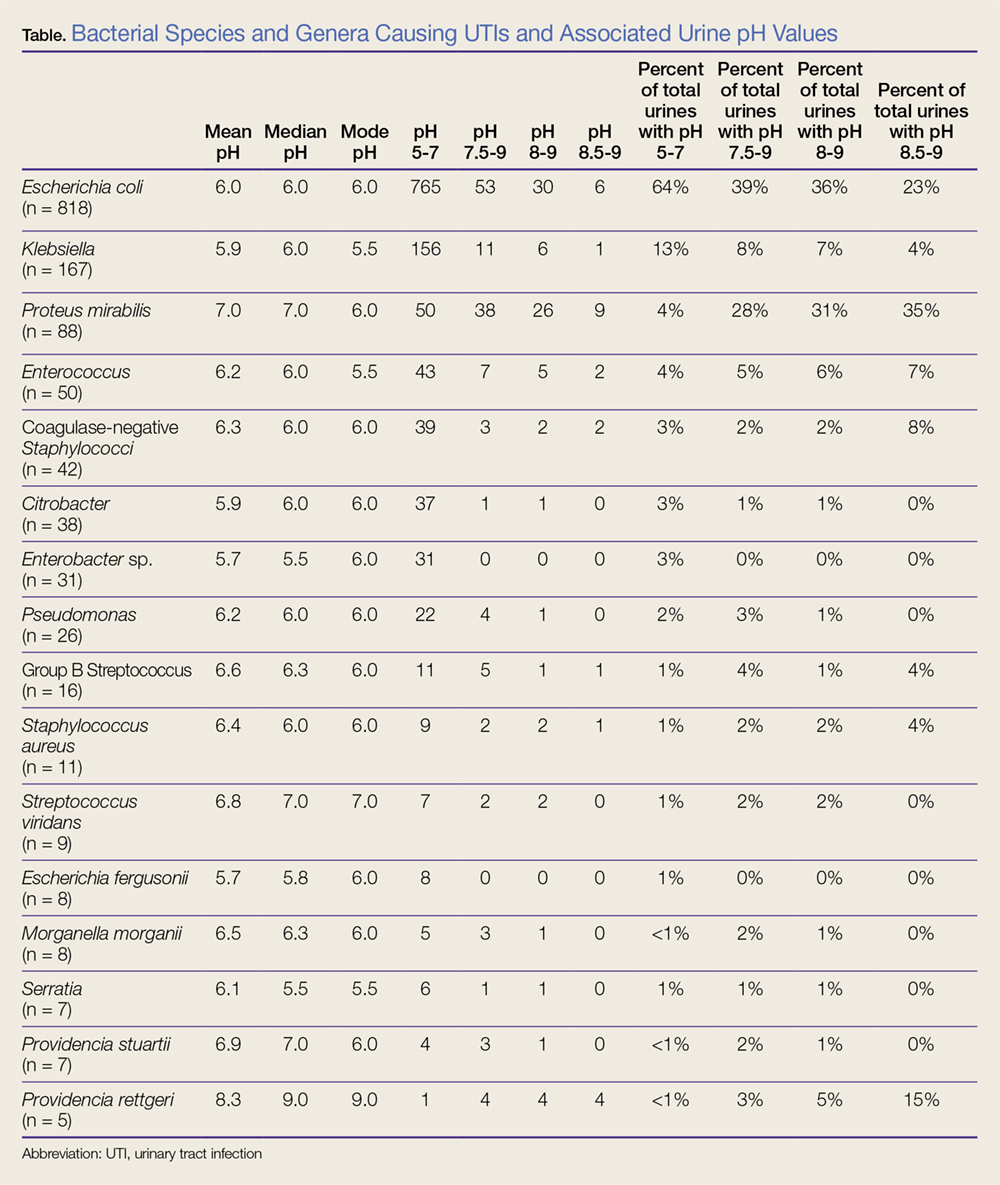
In our dataset, the most common bacteria associated with UTI, irrespective of urine pH, were Escherichia coli (n = 818/1,331; 62%), Klebsiella (n = 167/1,331; 13%), and P mirabilis (n = 88/1,331; 7%). The mean urine pH in our cohort was 6.1 (range, 5.0-9.0; SD, 0.88; median, 6; and mode, 6), and 1,194/1,331 (90%) of all urine samples had a urine pH of 5.0 to 7.0. Among patients who had a urine pH of 7.5 to 9.0, E coli was the cause of UTI in 39% (53/137) and P mirabilis was the cause of UTI in 28% (38/137). Likewise, among patients who had a urine pH of 8.0 to 9.0, E coli was the cause of UTI in 36% (30/83), and P mirabilis was the cause of UTI in 31% (26/83). Lastly, in patients who had a urine pH of 8.5 to 9.0, P mirabilis was the most common cause of UTI, present in 35% (9/26) patients.
The mean urine pH in our dataset for P mirabilis (n = 88) was 7.0, with a standard deviation (SD) of 1.03 and the standard error of the mean (SEM) of 0.11. The majority, 50/88 (57%) of P mirabilis UTIs were associated with a urine pH of 5.0 to 7.0. However, the urine pH for P mirabilis was significantly more alkaline than the combined urine pH from all of the other bacterial genera and species in our cohort (P < .0001). The mean urine pH in our cohort, excluding the P mirabilis data, was 6.01 with an SD of 0.828 and a SEM of 0.023.
Limitations
Our data were obtained retrospectively from a single ED, and did not include the following information: patient age and gender, and mode in which urine samples were obtained (eg, Foley catheter, clean catch). In addition, no reports were available regarding the sensitivity of the urine cultures with respect to urine pH.
Discussion
While alkaline urine was present in only 10% of patients, a high percentage of alkaline UTIs were associated with P mirabilis, an organism with intrinsic resistance to nitrofurantoin. Therefore, health care providers could consider obtaining a urine culture and/or prescribing an antibiotic other than nitrofurantoin for treating uncomplicated UTIs with alkaline urine. In addition, nitrofurantoin has been shown to be less effective against otherwise susceptible organisms in an alkaline urine.9
Conclusion
Our data demonstrates that urine pH of UTIs diagnosed in ED patients varied with the associated bacterial pathogen, and thus urine pH potentially could affect ED provider choice of antibiotics for the treatment of UTIs. Additional research is needed to confirm our results from a larger, more diverse dataset before changes in practice are recommended.
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269-284. doi:10.1038/nrmicro3432.
2. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183 Suppl 1:S1-S4. doi:10.1086/318850.
3. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital Health Stat 13. 2011;13(169):1-38.
4. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28(1):1-13. doi:10.1016/j.idc.2013.09.003.
5. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660. doi:10.1038/nrurol.2010.190.
6. Coker C, Poore CA, Li X, Mobley HL. Pathogenesis of Proteus mirabilis urinary tract infection. Microbes Infect. 2000;2(12):1497-1505.
7. Armbruster CE, Mobley HL. Merging mythology and morphology: the multifaceted lifestyle of Proteus mirabilis. Nat Rev Microbiol. 2012;10(11):743-754. doi:10.1038/nrmicro2890.
8. Schaffer JN, Pearson MM. Proteus mirabilis and urinary tract infections. Microbiol Spectr. 2015;3(5). doi:10.1128/microbiolspec.UTI-0017-2013.
9. Yang L, Wang K, Li H, Denstedt JD, Cadieux PA. The influence of urinary pH on antibiotic efficacy against bacterial uropathogens. Urology. 2014;84(3):731.e1-e7. doi:10.1016/j.urology.2014.04.048.
Background
Urinary tract infections (UTIs), one of the most common human bacterial infections, affect approximately 150 million people annually worldwide.1,2 In the United States, UTIs account for approximately 1% of all outpatient clinic visits and about 2 to 3 million ED visits annually.1,3-5
Although the urine pH level is frequently assessed in urinalysis, it is rarely considered in the management of a patient with a UTI.
Reports correlating urine pH with urine culture data from ED patients with UTIs are lacking. While poorly studied, there are multiple factors that could potentially alter the urine pH of patients with a UTI, including blood pH, diabetes, dehydration, ketosis, drugs, and renal function, as well as factors related to the infecting microorganism. For instance, Proteus mirabilis produces urease, an enzyme that hydrolyzes urea to ammonia and carbon dioxide.6-8
Objective
The objective of this study is to assess the relationship between the urine pH and the infecting microbe in ED patients diagnosed with UTIs, and to determine if P mirabilis is associated with alkaline urine.
Methods
We obtained approval from our Institutional Review Board to retrospectively obtain electronic medical record data from patients aged 18 years and older who presented to our institution’s ED and who were diagnosed with either cystitis or a UTI between January 1, 2012 and March 31, 2015. Both urine pH level and a urine culture were obtained for all patients.
The results of all of the patients’ urinary cultures in our study were positive for one bacterial species or genera (≥100,000 CFU/mL). The International Classification of Disease, Ninth Revision/Tenth Revision codes used to identify patients with cystitis and UTI were as follows: 595.0, 595.1, 595.9, 599.0, N30.91, N30.90, N30.80, N30.81, N30.00, N30.01, N30.20, N30.20, and N39.0.
To ensure that the focus of our study was limited to cystitis and UTIs, we excluded patients who were diagnosed with pyelonephritis, sexually transmitted infection, pelvic inflammatory disease, or vaginal discharge. The urine pH values reported from the clinical laboratory were 5.0, 5.5, 6.0, 6.5, 7.0. 7.5, 8.0, 8.5, and 9.0. Our dataset contained 1,331 clinical encounters. We used descriptive statistics and unpaired t-tests to evaluate the associations between urine pH values and the different microbes.
Results
Data were categorized into 16 different bacterial genera or species. Acinetobacter (n = 1), Kluyvera ascorbata (n = 2), and Stenotrophomonas maltophilia (n = 3) were underrepresented in the dataset and therefore were not included in the data analysis. The data are summarized in the Table.
In our dataset, the most common bacteria associated with UTI, irrespective of urine pH, were Escherichia coli (n = 818/1,331; 62%), Klebsiella (n = 167/1,331; 13%), and P mirabilis (n = 88/1,331; 7%). The mean urine pH in our cohort was 6.1 (range, 5.0-9.0; SD, 0.88; median, 6; and mode, 6), and 1,194/1,331 (90%) of all urine samples had a urine pH of 5.0 to 7.0. Among patients who had a urine pH of 7.5 to 9.0, E coli was the cause of UTI in 39% (53/137) and P mirabilis was the cause of UTI in 28% (38/137). Likewise, among patients who had a urine pH of 8.0 to 9.0, E coli was the cause of UTI in 36% (30/83), and P mirabilis was the cause of UTI in 31% (26/83). Lastly, in patients who had a urine pH of 8.5 to 9.0, P mirabilis was the most common cause of UTI, present in 35% (9/26) patients.
The mean urine pH in our dataset for P mirabilis (n = 88) was 7.0, with a standard deviation (SD) of 1.03 and the standard error of the mean (SEM) of 0.11. The majority, 50/88 (57%) of P mirabilis UTIs were associated with a urine pH of 5.0 to 7.0. However, the urine pH for P mirabilis was significantly more alkaline than the combined urine pH from all of the other bacterial genera and species in our cohort (P < .0001). The mean urine pH in our cohort, excluding the P mirabilis data, was 6.01 with an SD of 0.828 and a SEM of 0.023.
Limitations
Our data were obtained retrospectively from a single ED, and did not include the following information: patient age and gender, and mode in which urine samples were obtained (eg, Foley catheter, clean catch). In addition, no reports were available regarding the sensitivity of the urine cultures with respect to urine pH.
Discussion
While alkaline urine was present in only 10% of patients, a high percentage of alkaline UTIs were associated with P mirabilis, an organism with intrinsic resistance to nitrofurantoin. Therefore, health care providers could consider obtaining a urine culture and/or prescribing an antibiotic other than nitrofurantoin for treating uncomplicated UTIs with alkaline urine. In addition, nitrofurantoin has been shown to be less effective against otherwise susceptible organisms in an alkaline urine.9
Conclusion
Our data demonstrates that urine pH of UTIs diagnosed in ED patients varied with the associated bacterial pathogen, and thus urine pH potentially could affect ED provider choice of antibiotics for the treatment of UTIs. Additional research is needed to confirm our results from a larger, more diverse dataset before changes in practice are recommended.
Background
Urinary tract infections (UTIs), one of the most common human bacterial infections, affect approximately 150 million people annually worldwide.1,2 In the United States, UTIs account for approximately 1% of all outpatient clinic visits and about 2 to 3 million ED visits annually.1,3-5
Although the urine pH level is frequently assessed in urinalysis, it is rarely considered in the management of a patient with a UTI.
Reports correlating urine pH with urine culture data from ED patients with UTIs are lacking. While poorly studied, there are multiple factors that could potentially alter the urine pH of patients with a UTI, including blood pH, diabetes, dehydration, ketosis, drugs, and renal function, as well as factors related to the infecting microorganism. For instance, Proteus mirabilis produces urease, an enzyme that hydrolyzes urea to ammonia and carbon dioxide.6-8
Objective
The objective of this study is to assess the relationship between the urine pH and the infecting microbe in ED patients diagnosed with UTIs, and to determine if P mirabilis is associated with alkaline urine.
Methods
We obtained approval from our Institutional Review Board to retrospectively obtain electronic medical record data from patients aged 18 years and older who presented to our institution’s ED and who were diagnosed with either cystitis or a UTI between January 1, 2012 and March 31, 2015. Both urine pH level and a urine culture were obtained for all patients.
The results of all of the patients’ urinary cultures in our study were positive for one bacterial species or genera (≥100,000 CFU/mL). The International Classification of Disease, Ninth Revision/Tenth Revision codes used to identify patients with cystitis and UTI were as follows: 595.0, 595.1, 595.9, 599.0, N30.91, N30.90, N30.80, N30.81, N30.00, N30.01, N30.20, N30.20, and N39.0.
To ensure that the focus of our study was limited to cystitis and UTIs, we excluded patients who were diagnosed with pyelonephritis, sexually transmitted infection, pelvic inflammatory disease, or vaginal discharge. The urine pH values reported from the clinical laboratory were 5.0, 5.5, 6.0, 6.5, 7.0. 7.5, 8.0, 8.5, and 9.0. Our dataset contained 1,331 clinical encounters. We used descriptive statistics and unpaired t-tests to evaluate the associations between urine pH values and the different microbes.
Results
Data were categorized into 16 different bacterial genera or species. Acinetobacter (n = 1), Kluyvera ascorbata (n = 2), and Stenotrophomonas maltophilia (n = 3) were underrepresented in the dataset and therefore were not included in the data analysis. The data are summarized in the Table.
In our dataset, the most common bacteria associated with UTI, irrespective of urine pH, were Escherichia coli (n = 818/1,331; 62%), Klebsiella (n = 167/1,331; 13%), and P mirabilis (n = 88/1,331; 7%). The mean urine pH in our cohort was 6.1 (range, 5.0-9.0; SD, 0.88; median, 6; and mode, 6), and 1,194/1,331 (90%) of all urine samples had a urine pH of 5.0 to 7.0. Among patients who had a urine pH of 7.5 to 9.0, E coli was the cause of UTI in 39% (53/137) and P mirabilis was the cause of UTI in 28% (38/137). Likewise, among patients who had a urine pH of 8.0 to 9.0, E coli was the cause of UTI in 36% (30/83), and P mirabilis was the cause of UTI in 31% (26/83). Lastly, in patients who had a urine pH of 8.5 to 9.0, P mirabilis was the most common cause of UTI, present in 35% (9/26) patients.
The mean urine pH in our dataset for P mirabilis (n = 88) was 7.0, with a standard deviation (SD) of 1.03 and the standard error of the mean (SEM) of 0.11. The majority, 50/88 (57%) of P mirabilis UTIs were associated with a urine pH of 5.0 to 7.0. However, the urine pH for P mirabilis was significantly more alkaline than the combined urine pH from all of the other bacterial genera and species in our cohort (P < .0001). The mean urine pH in our cohort, excluding the P mirabilis data, was 6.01 with an SD of 0.828 and a SEM of 0.023.
Limitations
Our data were obtained retrospectively from a single ED, and did not include the following information: patient age and gender, and mode in which urine samples were obtained (eg, Foley catheter, clean catch). In addition, no reports were available regarding the sensitivity of the urine cultures with respect to urine pH.
Discussion
While alkaline urine was present in only 10% of patients, a high percentage of alkaline UTIs were associated with P mirabilis, an organism with intrinsic resistance to nitrofurantoin. Therefore, health care providers could consider obtaining a urine culture and/or prescribing an antibiotic other than nitrofurantoin for treating uncomplicated UTIs with alkaline urine. In addition, nitrofurantoin has been shown to be less effective against otherwise susceptible organisms in an alkaline urine.9
Conclusion
Our data demonstrates that urine pH of UTIs diagnosed in ED patients varied with the associated bacterial pathogen, and thus urine pH potentially could affect ED provider choice of antibiotics for the treatment of UTIs. Additional research is needed to confirm our results from a larger, more diverse dataset before changes in practice are recommended.
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269-284. doi:10.1038/nrmicro3432.
2. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183 Suppl 1:S1-S4. doi:10.1086/318850.
3. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital Health Stat 13. 2011;13(169):1-38.
4. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28(1):1-13. doi:10.1016/j.idc.2013.09.003.
5. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660. doi:10.1038/nrurol.2010.190.
6. Coker C, Poore CA, Li X, Mobley HL. Pathogenesis of Proteus mirabilis urinary tract infection. Microbes Infect. 2000;2(12):1497-1505.
7. Armbruster CE, Mobley HL. Merging mythology and morphology: the multifaceted lifestyle of Proteus mirabilis. Nat Rev Microbiol. 2012;10(11):743-754. doi:10.1038/nrmicro2890.
8. Schaffer JN, Pearson MM. Proteus mirabilis and urinary tract infections. Microbiol Spectr. 2015;3(5). doi:10.1128/microbiolspec.UTI-0017-2013.
9. Yang L, Wang K, Li H, Denstedt JD, Cadieux PA. The influence of urinary pH on antibiotic efficacy against bacterial uropathogens. Urology. 2014;84(3):731.e1-e7. doi:10.1016/j.urology.2014.04.048.
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269-284. doi:10.1038/nrmicro3432.
2. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183 Suppl 1:S1-S4. doi:10.1086/318850.
3. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital Health Stat 13. 2011;13(169):1-38.
4. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28(1):1-13. doi:10.1016/j.idc.2013.09.003.
5. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660. doi:10.1038/nrurol.2010.190.
6. Coker C, Poore CA, Li X, Mobley HL. Pathogenesis of Proteus mirabilis urinary tract infection. Microbes Infect. 2000;2(12):1497-1505.
7. Armbruster CE, Mobley HL. Merging mythology and morphology: the multifaceted lifestyle of Proteus mirabilis. Nat Rev Microbiol. 2012;10(11):743-754. doi:10.1038/nrmicro2890.
8. Schaffer JN, Pearson MM. Proteus mirabilis and urinary tract infections. Microbiol Spectr. 2015;3(5). doi:10.1128/microbiolspec.UTI-0017-2013.
9. Yang L, Wang K, Li H, Denstedt JD, Cadieux PA. The influence of urinary pH on antibiotic efficacy against bacterial uropathogens. Urology. 2014;84(3):731.e1-e7. doi:10.1016/j.urology.2014.04.048.
How to Prevent Mosquito and Tick-Borne Disease

Not Another Missed Spinal Epidural Abscess
A 55-year-old man presented for evaluation of a 2-day history of worsening left lower back pain.
Delay in the diagnosis and treatment of spinal epidural abscess (SEA) increases the likelihood of permanent disability (eg, residual motor weakness) or even death.1-5 Studies suggest that the incidence of SEA may be on the rise,6,7 which is especially troubling in an era of emerging antibiotic resistance.8 The pervasive theme among the medical literature stresses the challenges with early recognition; however, missed SEA is a theoretical mishap in a manner akin to Schrödinger’s cat or Heisenberg’s uncertainty principle.9,10
One will recall Erwin Schrödinger’s thought experiment of 1935 when he challenged the theory of quantum mechanics by asking whether or not the cat in a box is still alive if there is a 50/50 chance poisonous gas has been released. He suggested that before one looks in the box, the cat is both alive and dead—a state of superposition.
Unfortunately, medical diagnoses do not exist in dual states. Tests are either positive or negative; disease is either present or absent; and in medicine, the cat is either alive or dead. Moreover, when SEA is diagnosed after the initial presentation and workup, (ie, the “bounce-back”), the clinician cannot categorically assume the condition was present, but missed, at the initial evaluation. We present the following case, not as a miraculous catch, or a “zebra-hunting guide” but rather as a rare glimpse into the evolution of a disease process.
Case
A 55-year-old man with history of type 2 diabetes mellitus (DM), hypertension, and hyperlipidemia presented to the ED with a 2-day history of progressively worsening left lower back pain. Although the patient denied a recent history of trauma, he did state that he helped one of his friends move furniture 1 day prior to presentation and had attributed the worsening pain to this event. The patient described his pain as mild and dull when he was at rest, rating it as a 2 on a pain scale of 1 to 10; and sharp-feeling and at its worst upon movement, rating it as a 9 on a pain scale of 1 to 10. The patient noted experiencing only mild relief when he shifted to certain positions.
The patient’s pain was nonradiating and associated with dull pain in the left anterior proximal thigh. The patient denied any numbness or weakness in any of his extremities. He also denied any perineal numbness or urinary or bowel incontinence; however, he did note experiencing a sense of incomplete evacuation of stools over the past 5 mornings.
The patient denied any recent history of fever, chills, numbness, weakness, difficulty with balance, direct trauma, instrumentation or chiropractic manipulation, or unexplained or unintentional weight loss. He had no history of malignancy and vehemently denied intravenous (IV) drug use.
On physical examination, the patient’s vital signs were: blood pressure, 143/93 mm Hg; heart rate, 108 beats/min; respiratory rate, 16 breaths/min; and temperature, 97.6°F. Oxygen saturation was 95% on room air. Upon examination, the patient was in no acute distress and was resting comfortably and quietly. Pertinent findings included a supple neck examination, without lymphadenopathy or meningismus. There was no midline tenderness to palpation of the cervical spine and no step-off deformities. The lungs were clear to auscultation bilaterally and without wheezing, rhonchi, or rales. Examination of the heart revealed a regular rhythm with borderline tachycardia, but without murmurs, rubs, or gallops. The patient had 2+ pulses in all four extremities, and capillary refill was less than 2 seconds. The abdomen was soft and nontender, without rebound, guarding, or rigidity. There were no pulsatile abdominal masses or bruits, and bowel sounds were present. The patient had no costovertebral angle tenderness on percussion, and had full range of motion of all four extremities, with no tenderness to palpation and no bony deformities.
Examination of the back revealed a positive straight leg raise on the right, but there was no midline tenderness to palpation or step-off deformity of the thoracic or lumbar spine. The patient exhibited mild left-sided upper lumbar paraspinal tenderness to palpation, but had no associated muscle spasm or overlying skin changes. On neurological assessment, the patient was alert and oriented with cranial nerves II-XII intact. He had 5/5 motor strength in all four extremities, with careful attention to hip flexion and extension, knee flexion and extension, and dorsiflexion and plantar flexion at the ankle. The sensory examination was normal, as were patella and ankle reflexes. The patient was able to ambulate with a steady gait.
Laboratory evaluation included a complete blood count, basic metabolic profile (BMP), urinalysis, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. The urinalysis was negative for blood or signs of infection. The BMP demonstrated hyperglycemia without acidosis, but no additional electrolyte abnormalities or renal insufficiency. The patient did have leukocytosis (white blood cell [WBC], 19.8×109/L) with a left shift. The ESR was within normal limits (14 mm/h), but the CRP was mildly elevated (37.33 nmol/L).
Blood cultures were ordered, and the patient was given 2,500 mg vancomycin and 2,000 mg ceftriaxone IV. Given the patient’s abnormal back examination and the presence of a leukocytosis, a magnetic resonance imaging (MRI) study of the thoracic and lumbar spine was ordered. Radiology services reported the following findings from the MRI:
- Unremarkable thoracic spine MRI. No evidence of thoracic spine infection or significant degenerative changes.
- No evidence of infection involving the lumbar spine.
- L3-4 and L4-5 disc bulges and posterior element degenerative changes with moderate canal stenoses.
- Edema in the posterior paraspinous musculature on the left at the L3 and L4 levels.
The patient had DM with multiple systemic inflammatory response syndrome criteria and was admitted to the hospital for undifferentiated sepsis, clinical uncertainty, and pain control. Within 24 hours, blood cultures were positive for gram-positive cocci, later identified as methicillin-sensitive Staphylococcus aureus. However, despite treatment with antibiotics and analgesics, the patient’s back pain persisted. A repeat MRI of the lumbar spine obtained on hospital day 4 revealed the following:
At L3-4, since the comparison study, there has been development of two epidural abscesses with abnormal peripheral enhancement, one located dorsally measuring 6.8 x 8.1 x 14 mm and another located in the left lateral recess measuring 8.1 x 9.7 x 10.9 mm. The combination of the broad-based disk bulge, epidural abscesses, and hypertrophic facets resulted in severe spinal canal stenosis.
After receiving this report, the hospitalist contacted neurosurgery services. Shortly thereafter the patient underwent unilateral laminotomy with bilateral canal decompression on hospital day 5. He was discharged home on hospital day 10 without any neurological deficits, and continued IV antibiotics as an outpatient for an additional 5 weeks.
Discussion
Only a minority of patients with SEA present with the classic triad of back pain, fever, and progressive neurological findings associated with this condition.1Careful history-taking therefore is essential to identify high-risk patients. Risk factors for SEA include diabetes, IV drug abuse, immunosuppression, chronic renal failure, liver disease, alcoholism, indwelling catheter, recent invasive spinal procedure, recent vertebral fracture, cancer, and distant site of infection.1-3,5,7,11
Leukocytosis (WBC >10×109/L) is only found in two-thirds or less of patients with SEA at the time of admission.1,3,12 Inflammatory markers such as CRP and ESR are more sensitive but not specific to SEAs.1,2,5,7,11-13
An MRI study with gadolinium is the diagnostic modality of choice over computed tomography myelography to assess for SEAs due to its noninvasive nature and ability to better delineate the extent of disease.5,7,14 An MRI of the entire spine is recommended to delineate longitudinal and paraspinal extension as SEA can traverse multiple vertebral levels.15 While awaiting the results of blood cultures, patients should be treated with broad spectrum antibiotics that include coverage of the most common etiology of SEA, S aureus.1,3,4,7,11,13 While some cases of SEA may be managed medically, the emergency physician should always treat SEA as a neurosurgical emergency and obtain consultation with the appropriate services (eg, neurosurgery, infectious disease, neurology radiology).1,5
Our patient represents an unusual case of SEAs in that he presented with S aureus bacteremia while afebrile, along with back pain and tachycardia. He subsequently developed SEA, which was recognized only through serial MRI studies. The patient’s tachycardia alone could have been easily attributed to pain and anxiety associated with the ED environment. As such, he could have easily been discharged home with a prescription [for] nonsteroidal anti-inflammatory drugs and/or muscle relaxers for pain management—though it is likely that he would have returned to the ED 3 days later with persistent and even worsening symptoms, during which he would have undergone additional testing, possibly MRI, which would have revealed the missed SEA.
Our case clearly demonstrates that no SEA was present at the time of the
Studies show that half of all patients with SEAs are not diagnosed until after two or more visits to the ED.1,11 The literature posits that most cases are misdiagnosed at the time of initial evaluation. It has even been postulated that “misdiagnosis of spinal epidural abscess is the rule rather than the exception.”1 Although our patient was eventually diagnosed with a SEA, it was not present on the first MRI taken during the initial evaluation.
Summary
Unlike the rules of quantum mechanics and the paradox of Schrödinger’s cat, SEA follows a progression of disease.3,7,16 There is no superposition—the MRI is either positive or negative. However, excellent care requires the practitioner to know the risk factors of SEA, apply the appropriate screening tests, obtain MRI when necessary, and if diagnostic uncertainty remains, discuss with the patient or family signs and symptoms to monitor as well as reasons to return for re-evaluation.
1. Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26(3):285-291.
2. Bhise V, Meyer A, Singh H, et al. errors in diagnosis of spinal epidural abscesses in the era of electronic health records. Am J Med. 2017;130(8):975-981. doi:10.1016/j.amjmed.2017.03.009.
3. Darouiche RO, Hamill RJ, Greenberg SB, Weathers SW, Musher DM. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore). 1992;71(6):369-385.
4. Baker AS, Ojemann RG, Swartz MN, Richardson EP Jr. Spinal epidural abscess. N Engl J Med. 1975;293(10):463-468. doi:10.1056/NEJM197509042931001.
5. Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol. 1992;38(3):225-231.
6. Vakili M, Crum-Cianflone NF. Spinal epidural abscess: a series of 101 cases. Am J Med. 2017;130(12):1458-1463. doi:10.1016/j.amjmed.2017.07.017.
7. Rigamonti D, Liem L, Sampath P, et al. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Surg Neurol. 1999;52(2):189-196; discussion 197.
8. The World Health Organization. Antimicrobial resistance: global report on surveillance. http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua=1. Accessed June 12, 2018.
9. Schrödinger E. Die gegenwärtige situation in der quantenmechanik. Maturwissenschaften. 1935;23(48):807-812; 823-828; 844-849. doi:10.1007/BF01491891.
10. Heisenberg H. Über quantentheoretische umdeutung kinematischer und mechanischer beziehungen. Zeitschrift für Physik. 1925;33(1):879-893. doi:10.1007/BF01328377.
11. Tang HJ, Lin HJ, Liu YC, Li CM. Spinal epidural abscess—experience with 46 patients and evaluation of prognostic factors. J Infect. 2002;45(2):76-81.
12. Soehle M, Wallenfang T. Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery. 2002;51(1):79-85; discussion 86-87.
13. Del Curling O Jr, Gower DJ, McWhorter JM. Changing concepts in spinal epidural abscess: a report of 29 cases. Neurosurgery. 1990;27(2):185-192.
14. Hlavin ML, Kaminski HJ, Ross JS, Ganz E. Spinal epidural abscess: a ten-year perspective. Neurosurgery. 1990;27(2):177-184.
15. Parkinson JF, Sekhon LH. Spinal epidural abscess: appearance on magnetic resonance imaging as a guide to surgical management. Report of five cases. Neurosurg Focus. 2004;17(6):E12.
16. Heusner AP. Nontuberculous spinal epidural infections. N Engl J Med. 1948;239(23):845-854. doi:10.1056/NEJM194812022392301.
A 55-year-old man presented for evaluation of a 2-day history of worsening left lower back pain.
A 55-year-old man presented for evaluation of a 2-day history of worsening left lower back pain.
Delay in the diagnosis and treatment of spinal epidural abscess (SEA) increases the likelihood of permanent disability (eg, residual motor weakness) or even death.1-5 Studies suggest that the incidence of SEA may be on the rise,6,7 which is especially troubling in an era of emerging antibiotic resistance.8 The pervasive theme among the medical literature stresses the challenges with early recognition; however, missed SEA is a theoretical mishap in a manner akin to Schrödinger’s cat or Heisenberg’s uncertainty principle.9,10
One will recall Erwin Schrödinger’s thought experiment of 1935 when he challenged the theory of quantum mechanics by asking whether or not the cat in a box is still alive if there is a 50/50 chance poisonous gas has been released. He suggested that before one looks in the box, the cat is both alive and dead—a state of superposition.
Unfortunately, medical diagnoses do not exist in dual states. Tests are either positive or negative; disease is either present or absent; and in medicine, the cat is either alive or dead. Moreover, when SEA is diagnosed after the initial presentation and workup, (ie, the “bounce-back”), the clinician cannot categorically assume the condition was present, but missed, at the initial evaluation. We present the following case, not as a miraculous catch, or a “zebra-hunting guide” but rather as a rare glimpse into the evolution of a disease process.
Case
A 55-year-old man with history of type 2 diabetes mellitus (DM), hypertension, and hyperlipidemia presented to the ED with a 2-day history of progressively worsening left lower back pain. Although the patient denied a recent history of trauma, he did state that he helped one of his friends move furniture 1 day prior to presentation and had attributed the worsening pain to this event. The patient described his pain as mild and dull when he was at rest, rating it as a 2 on a pain scale of 1 to 10; and sharp-feeling and at its worst upon movement, rating it as a 9 on a pain scale of 1 to 10. The patient noted experiencing only mild relief when he shifted to certain positions.
The patient’s pain was nonradiating and associated with dull pain in the left anterior proximal thigh. The patient denied any numbness or weakness in any of his extremities. He also denied any perineal numbness or urinary or bowel incontinence; however, he did note experiencing a sense of incomplete evacuation of stools over the past 5 mornings.
The patient denied any recent history of fever, chills, numbness, weakness, difficulty with balance, direct trauma, instrumentation or chiropractic manipulation, or unexplained or unintentional weight loss. He had no history of malignancy and vehemently denied intravenous (IV) drug use.
On physical examination, the patient’s vital signs were: blood pressure, 143/93 mm Hg; heart rate, 108 beats/min; respiratory rate, 16 breaths/min; and temperature, 97.6°F. Oxygen saturation was 95% on room air. Upon examination, the patient was in no acute distress and was resting comfortably and quietly. Pertinent findings included a supple neck examination, without lymphadenopathy or meningismus. There was no midline tenderness to palpation of the cervical spine and no step-off deformities. The lungs were clear to auscultation bilaterally and without wheezing, rhonchi, or rales. Examination of the heart revealed a regular rhythm with borderline tachycardia, but without murmurs, rubs, or gallops. The patient had 2+ pulses in all four extremities, and capillary refill was less than 2 seconds. The abdomen was soft and nontender, without rebound, guarding, or rigidity. There were no pulsatile abdominal masses or bruits, and bowel sounds were present. The patient had no costovertebral angle tenderness on percussion, and had full range of motion of all four extremities, with no tenderness to palpation and no bony deformities.
Examination of the back revealed a positive straight leg raise on the right, but there was no midline tenderness to palpation or step-off deformity of the thoracic or lumbar spine. The patient exhibited mild left-sided upper lumbar paraspinal tenderness to palpation, but had no associated muscle spasm or overlying skin changes. On neurological assessment, the patient was alert and oriented with cranial nerves II-XII intact. He had 5/5 motor strength in all four extremities, with careful attention to hip flexion and extension, knee flexion and extension, and dorsiflexion and plantar flexion at the ankle. The sensory examination was normal, as were patella and ankle reflexes. The patient was able to ambulate with a steady gait.
Laboratory evaluation included a complete blood count, basic metabolic profile (BMP), urinalysis, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. The urinalysis was negative for blood or signs of infection. The BMP demonstrated hyperglycemia without acidosis, but no additional electrolyte abnormalities or renal insufficiency. The patient did have leukocytosis (white blood cell [WBC], 19.8×109/L) with a left shift. The ESR was within normal limits (14 mm/h), but the CRP was mildly elevated (37.33 nmol/L).
Blood cultures were ordered, and the patient was given 2,500 mg vancomycin and 2,000 mg ceftriaxone IV. Given the patient’s abnormal back examination and the presence of a leukocytosis, a magnetic resonance imaging (MRI) study of the thoracic and lumbar spine was ordered. Radiology services reported the following findings from the MRI:
- Unremarkable thoracic spine MRI. No evidence of thoracic spine infection or significant degenerative changes.
- No evidence of infection involving the lumbar spine.
- L3-4 and L4-5 disc bulges and posterior element degenerative changes with moderate canal stenoses.
- Edema in the posterior paraspinous musculature on the left at the L3 and L4 levels.
The patient had DM with multiple systemic inflammatory response syndrome criteria and was admitted to the hospital for undifferentiated sepsis, clinical uncertainty, and pain control. Within 24 hours, blood cultures were positive for gram-positive cocci, later identified as methicillin-sensitive Staphylococcus aureus. However, despite treatment with antibiotics and analgesics, the patient’s back pain persisted. A repeat MRI of the lumbar spine obtained on hospital day 4 revealed the following:
At L3-4, since the comparison study, there has been development of two epidural abscesses with abnormal peripheral enhancement, one located dorsally measuring 6.8 x 8.1 x 14 mm and another located in the left lateral recess measuring 8.1 x 9.7 x 10.9 mm. The combination of the broad-based disk bulge, epidural abscesses, and hypertrophic facets resulted in severe spinal canal stenosis.
After receiving this report, the hospitalist contacted neurosurgery services. Shortly thereafter the patient underwent unilateral laminotomy with bilateral canal decompression on hospital day 5. He was discharged home on hospital day 10 without any neurological deficits, and continued IV antibiotics as an outpatient for an additional 5 weeks.
Discussion
Only a minority of patients with SEA present with the classic triad of back pain, fever, and progressive neurological findings associated with this condition.1Careful history-taking therefore is essential to identify high-risk patients. Risk factors for SEA include diabetes, IV drug abuse, immunosuppression, chronic renal failure, liver disease, alcoholism, indwelling catheter, recent invasive spinal procedure, recent vertebral fracture, cancer, and distant site of infection.1-3,5,7,11
Leukocytosis (WBC >10×109/L) is only found in two-thirds or less of patients with SEA at the time of admission.1,3,12 Inflammatory markers such as CRP and ESR are more sensitive but not specific to SEAs.1,2,5,7,11-13
An MRI study with gadolinium is the diagnostic modality of choice over computed tomography myelography to assess for SEAs due to its noninvasive nature and ability to better delineate the extent of disease.5,7,14 An MRI of the entire spine is recommended to delineate longitudinal and paraspinal extension as SEA can traverse multiple vertebral levels.15 While awaiting the results of blood cultures, patients should be treated with broad spectrum antibiotics that include coverage of the most common etiology of SEA, S aureus.1,3,4,7,11,13 While some cases of SEA may be managed medically, the emergency physician should always treat SEA as a neurosurgical emergency and obtain consultation with the appropriate services (eg, neurosurgery, infectious disease, neurology radiology).1,5
Our patient represents an unusual case of SEAs in that he presented with S aureus bacteremia while afebrile, along with back pain and tachycardia. He subsequently developed SEA, which was recognized only through serial MRI studies. The patient’s tachycardia alone could have been easily attributed to pain and anxiety associated with the ED environment. As such, he could have easily been discharged home with a prescription [for] nonsteroidal anti-inflammatory drugs and/or muscle relaxers for pain management—though it is likely that he would have returned to the ED 3 days later with persistent and even worsening symptoms, during which he would have undergone additional testing, possibly MRI, which would have revealed the missed SEA.
Our case clearly demonstrates that no SEA was present at the time of the
Studies show that half of all patients with SEAs are not diagnosed until after two or more visits to the ED.1,11 The literature posits that most cases are misdiagnosed at the time of initial evaluation. It has even been postulated that “misdiagnosis of spinal epidural abscess is the rule rather than the exception.”1 Although our patient was eventually diagnosed with a SEA, it was not present on the first MRI taken during the initial evaluation.
Summary
Unlike the rules of quantum mechanics and the paradox of Schrödinger’s cat, SEA follows a progression of disease.3,7,16 There is no superposition—the MRI is either positive or negative. However, excellent care requires the practitioner to know the risk factors of SEA, apply the appropriate screening tests, obtain MRI when necessary, and if diagnostic uncertainty remains, discuss with the patient or family signs and symptoms to monitor as well as reasons to return for re-evaluation.
Delay in the diagnosis and treatment of spinal epidural abscess (SEA) increases the likelihood of permanent disability (eg, residual motor weakness) or even death.1-5 Studies suggest that the incidence of SEA may be on the rise,6,7 which is especially troubling in an era of emerging antibiotic resistance.8 The pervasive theme among the medical literature stresses the challenges with early recognition; however, missed SEA is a theoretical mishap in a manner akin to Schrödinger’s cat or Heisenberg’s uncertainty principle.9,10
One will recall Erwin Schrödinger’s thought experiment of 1935 when he challenged the theory of quantum mechanics by asking whether or not the cat in a box is still alive if there is a 50/50 chance poisonous gas has been released. He suggested that before one looks in the box, the cat is both alive and dead—a state of superposition.
Unfortunately, medical diagnoses do not exist in dual states. Tests are either positive or negative; disease is either present or absent; and in medicine, the cat is either alive or dead. Moreover, when SEA is diagnosed after the initial presentation and workup, (ie, the “bounce-back”), the clinician cannot categorically assume the condition was present, but missed, at the initial evaluation. We present the following case, not as a miraculous catch, or a “zebra-hunting guide” but rather as a rare glimpse into the evolution of a disease process.
Case
A 55-year-old man with history of type 2 diabetes mellitus (DM), hypertension, and hyperlipidemia presented to the ED with a 2-day history of progressively worsening left lower back pain. Although the patient denied a recent history of trauma, he did state that he helped one of his friends move furniture 1 day prior to presentation and had attributed the worsening pain to this event. The patient described his pain as mild and dull when he was at rest, rating it as a 2 on a pain scale of 1 to 10; and sharp-feeling and at its worst upon movement, rating it as a 9 on a pain scale of 1 to 10. The patient noted experiencing only mild relief when he shifted to certain positions.
The patient’s pain was nonradiating and associated with dull pain in the left anterior proximal thigh. The patient denied any numbness or weakness in any of his extremities. He also denied any perineal numbness or urinary or bowel incontinence; however, he did note experiencing a sense of incomplete evacuation of stools over the past 5 mornings.
The patient denied any recent history of fever, chills, numbness, weakness, difficulty with balance, direct trauma, instrumentation or chiropractic manipulation, or unexplained or unintentional weight loss. He had no history of malignancy and vehemently denied intravenous (IV) drug use.
On physical examination, the patient’s vital signs were: blood pressure, 143/93 mm Hg; heart rate, 108 beats/min; respiratory rate, 16 breaths/min; and temperature, 97.6°F. Oxygen saturation was 95% on room air. Upon examination, the patient was in no acute distress and was resting comfortably and quietly. Pertinent findings included a supple neck examination, without lymphadenopathy or meningismus. There was no midline tenderness to palpation of the cervical spine and no step-off deformities. The lungs were clear to auscultation bilaterally and without wheezing, rhonchi, or rales. Examination of the heart revealed a regular rhythm with borderline tachycardia, but without murmurs, rubs, or gallops. The patient had 2+ pulses in all four extremities, and capillary refill was less than 2 seconds. The abdomen was soft and nontender, without rebound, guarding, or rigidity. There were no pulsatile abdominal masses or bruits, and bowel sounds were present. The patient had no costovertebral angle tenderness on percussion, and had full range of motion of all four extremities, with no tenderness to palpation and no bony deformities.
Examination of the back revealed a positive straight leg raise on the right, but there was no midline tenderness to palpation or step-off deformity of the thoracic or lumbar spine. The patient exhibited mild left-sided upper lumbar paraspinal tenderness to palpation, but had no associated muscle spasm or overlying skin changes. On neurological assessment, the patient was alert and oriented with cranial nerves II-XII intact. He had 5/5 motor strength in all four extremities, with careful attention to hip flexion and extension, knee flexion and extension, and dorsiflexion and plantar flexion at the ankle. The sensory examination was normal, as were patella and ankle reflexes. The patient was able to ambulate with a steady gait.
Laboratory evaluation included a complete blood count, basic metabolic profile (BMP), urinalysis, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. The urinalysis was negative for blood or signs of infection. The BMP demonstrated hyperglycemia without acidosis, but no additional electrolyte abnormalities or renal insufficiency. The patient did have leukocytosis (white blood cell [WBC], 19.8×109/L) with a left shift. The ESR was within normal limits (14 mm/h), but the CRP was mildly elevated (37.33 nmol/L).
Blood cultures were ordered, and the patient was given 2,500 mg vancomycin and 2,000 mg ceftriaxone IV. Given the patient’s abnormal back examination and the presence of a leukocytosis, a magnetic resonance imaging (MRI) study of the thoracic and lumbar spine was ordered. Radiology services reported the following findings from the MRI:
- Unremarkable thoracic spine MRI. No evidence of thoracic spine infection or significant degenerative changes.
- No evidence of infection involving the lumbar spine.
- L3-4 and L4-5 disc bulges and posterior element degenerative changes with moderate canal stenoses.
- Edema in the posterior paraspinous musculature on the left at the L3 and L4 levels.
The patient had DM with multiple systemic inflammatory response syndrome criteria and was admitted to the hospital for undifferentiated sepsis, clinical uncertainty, and pain control. Within 24 hours, blood cultures were positive for gram-positive cocci, later identified as methicillin-sensitive Staphylococcus aureus. However, despite treatment with antibiotics and analgesics, the patient’s back pain persisted. A repeat MRI of the lumbar spine obtained on hospital day 4 revealed the following:
At L3-4, since the comparison study, there has been development of two epidural abscesses with abnormal peripheral enhancement, one located dorsally measuring 6.8 x 8.1 x 14 mm and another located in the left lateral recess measuring 8.1 x 9.7 x 10.9 mm. The combination of the broad-based disk bulge, epidural abscesses, and hypertrophic facets resulted in severe spinal canal stenosis.
After receiving this report, the hospitalist contacted neurosurgery services. Shortly thereafter the patient underwent unilateral laminotomy with bilateral canal decompression on hospital day 5. He was discharged home on hospital day 10 without any neurological deficits, and continued IV antibiotics as an outpatient for an additional 5 weeks.
Discussion
Only a minority of patients with SEA present with the classic triad of back pain, fever, and progressive neurological findings associated with this condition.1Careful history-taking therefore is essential to identify high-risk patients. Risk factors for SEA include diabetes, IV drug abuse, immunosuppression, chronic renal failure, liver disease, alcoholism, indwelling catheter, recent invasive spinal procedure, recent vertebral fracture, cancer, and distant site of infection.1-3,5,7,11
Leukocytosis (WBC >10×109/L) is only found in two-thirds or less of patients with SEA at the time of admission.1,3,12 Inflammatory markers such as CRP and ESR are more sensitive but not specific to SEAs.1,2,5,7,11-13
An MRI study with gadolinium is the diagnostic modality of choice over computed tomography myelography to assess for SEAs due to its noninvasive nature and ability to better delineate the extent of disease.5,7,14 An MRI of the entire spine is recommended to delineate longitudinal and paraspinal extension as SEA can traverse multiple vertebral levels.15 While awaiting the results of blood cultures, patients should be treated with broad spectrum antibiotics that include coverage of the most common etiology of SEA, S aureus.1,3,4,7,11,13 While some cases of SEA may be managed medically, the emergency physician should always treat SEA as a neurosurgical emergency and obtain consultation with the appropriate services (eg, neurosurgery, infectious disease, neurology radiology).1,5
Our patient represents an unusual case of SEAs in that he presented with S aureus bacteremia while afebrile, along with back pain and tachycardia. He subsequently developed SEA, which was recognized only through serial MRI studies. The patient’s tachycardia alone could have been easily attributed to pain and anxiety associated with the ED environment. As such, he could have easily been discharged home with a prescription [for] nonsteroidal anti-inflammatory drugs and/or muscle relaxers for pain management—though it is likely that he would have returned to the ED 3 days later with persistent and even worsening symptoms, during which he would have undergone additional testing, possibly MRI, which would have revealed the missed SEA.
Our case clearly demonstrates that no SEA was present at the time of the
Studies show that half of all patients with SEAs are not diagnosed until after two or more visits to the ED.1,11 The literature posits that most cases are misdiagnosed at the time of initial evaluation. It has even been postulated that “misdiagnosis of spinal epidural abscess is the rule rather than the exception.”1 Although our patient was eventually diagnosed with a SEA, it was not present on the first MRI taken during the initial evaluation.
Summary
Unlike the rules of quantum mechanics and the paradox of Schrödinger’s cat, SEA follows a progression of disease.3,7,16 There is no superposition—the MRI is either positive or negative. However, excellent care requires the practitioner to know the risk factors of SEA, apply the appropriate screening tests, obtain MRI when necessary, and if diagnostic uncertainty remains, discuss with the patient or family signs and symptoms to monitor as well as reasons to return for re-evaluation.
1. Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26(3):285-291.
2. Bhise V, Meyer A, Singh H, et al. errors in diagnosis of spinal epidural abscesses in the era of electronic health records. Am J Med. 2017;130(8):975-981. doi:10.1016/j.amjmed.2017.03.009.
3. Darouiche RO, Hamill RJ, Greenberg SB, Weathers SW, Musher DM. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore). 1992;71(6):369-385.
4. Baker AS, Ojemann RG, Swartz MN, Richardson EP Jr. Spinal epidural abscess. N Engl J Med. 1975;293(10):463-468. doi:10.1056/NEJM197509042931001.
5. Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol. 1992;38(3):225-231.
6. Vakili M, Crum-Cianflone NF. Spinal epidural abscess: a series of 101 cases. Am J Med. 2017;130(12):1458-1463. doi:10.1016/j.amjmed.2017.07.017.
7. Rigamonti D, Liem L, Sampath P, et al. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Surg Neurol. 1999;52(2):189-196; discussion 197.
8. The World Health Organization. Antimicrobial resistance: global report on surveillance. http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua=1. Accessed June 12, 2018.
9. Schrödinger E. Die gegenwärtige situation in der quantenmechanik. Maturwissenschaften. 1935;23(48):807-812; 823-828; 844-849. doi:10.1007/BF01491891.
10. Heisenberg H. Über quantentheoretische umdeutung kinematischer und mechanischer beziehungen. Zeitschrift für Physik. 1925;33(1):879-893. doi:10.1007/BF01328377.
11. Tang HJ, Lin HJ, Liu YC, Li CM. Spinal epidural abscess—experience with 46 patients and evaluation of prognostic factors. J Infect. 2002;45(2):76-81.
12. Soehle M, Wallenfang T. Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery. 2002;51(1):79-85; discussion 86-87.
13. Del Curling O Jr, Gower DJ, McWhorter JM. Changing concepts in spinal epidural abscess: a report of 29 cases. Neurosurgery. 1990;27(2):185-192.
14. Hlavin ML, Kaminski HJ, Ross JS, Ganz E. Spinal epidural abscess: a ten-year perspective. Neurosurgery. 1990;27(2):177-184.
15. Parkinson JF, Sekhon LH. Spinal epidural abscess: appearance on magnetic resonance imaging as a guide to surgical management. Report of five cases. Neurosurg Focus. 2004;17(6):E12.
16. Heusner AP. Nontuberculous spinal epidural infections. N Engl J Med. 1948;239(23):845-854. doi:10.1056/NEJM194812022392301.
1. Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26(3):285-291.
2. Bhise V, Meyer A, Singh H, et al. errors in diagnosis of spinal epidural abscesses in the era of electronic health records. Am J Med. 2017;130(8):975-981. doi:10.1016/j.amjmed.2017.03.009.
3. Darouiche RO, Hamill RJ, Greenberg SB, Weathers SW, Musher DM. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore). 1992;71(6):369-385.
4. Baker AS, Ojemann RG, Swartz MN, Richardson EP Jr. Spinal epidural abscess. N Engl J Med. 1975;293(10):463-468. doi:10.1056/NEJM197509042931001.
5. Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol. 1992;38(3):225-231.
6. Vakili M, Crum-Cianflone NF. Spinal epidural abscess: a series of 101 cases. Am J Med. 2017;130(12):1458-1463. doi:10.1016/j.amjmed.2017.07.017.
7. Rigamonti D, Liem L, Sampath P, et al. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Surg Neurol. 1999;52(2):189-196; discussion 197.
8. The World Health Organization. Antimicrobial resistance: global report on surveillance. http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua=1. Accessed June 12, 2018.
9. Schrödinger E. Die gegenwärtige situation in der quantenmechanik. Maturwissenschaften. 1935;23(48):807-812; 823-828; 844-849. doi:10.1007/BF01491891.
10. Heisenberg H. Über quantentheoretische umdeutung kinematischer und mechanischer beziehungen. Zeitschrift für Physik. 1925;33(1):879-893. doi:10.1007/BF01328377.
11. Tang HJ, Lin HJ, Liu YC, Li CM. Spinal epidural abscess—experience with 46 patients and evaluation of prognostic factors. J Infect. 2002;45(2):76-81.
12. Soehle M, Wallenfang T. Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery. 2002;51(1):79-85; discussion 86-87.
13. Del Curling O Jr, Gower DJ, McWhorter JM. Changing concepts in spinal epidural abscess: a report of 29 cases. Neurosurgery. 1990;27(2):185-192.
14. Hlavin ML, Kaminski HJ, Ross JS, Ganz E. Spinal epidural abscess: a ten-year perspective. Neurosurgery. 1990;27(2):177-184.
15. Parkinson JF, Sekhon LH. Spinal epidural abscess: appearance on magnetic resonance imaging as a guide to surgical management. Report of five cases. Neurosurg Focus. 2004;17(6):E12.
16. Heusner AP. Nontuberculous spinal epidural infections. N Engl J Med. 1948;239(23):845-854. doi:10.1056/NEJM194812022392301.
Transplanting HCV-infected kidneys in HCV-infected patients showed positive outcomes, costs
Transplanting a kidney infected with hepatitis C into individuals infected with HCV, followed by treatment, was more effective and less costly than transplanting an uninfected kidney, preceded by HCV treatment, according to Mark H. Eckman, MD, of the University of Cincinnati and his colleagues.

Largely because of the longer wait times for uninfected kidneys, a typical patient aged 58 years on hemodialysis would gain an average of 0.5 quality-adjusted life-years at a lifetime cost savings of $41,591 dollars, according to the model.
“In an era of increasing success for kidney transplants and demand that far outstrips supply, deferring antiviral therapy until after transplant of HCV-infected kidneys, when available, should be both cost saving and effective,” the researchers wrote.
The study was funded by grants from Merck Sharpe & Dohme and the National Center for Advancing Translational Science. Several of the authors reported having grants from Merck and grants and personal fees from a variety of other pharmaceutical companies.
SOURCE: Eckman MH et al. Ann Intern Med. 2018 Jul 10. doi: 10.7326/M17-3088.
Transplanting a kidney infected with hepatitis C into individuals infected with HCV, followed by treatment, was more effective and less costly than transplanting an uninfected kidney, preceded by HCV treatment, according to Mark H. Eckman, MD, of the University of Cincinnati and his colleagues.
Largely because of the longer wait times for uninfected kidneys, a typical patient aged 58 years on hemodialysis would gain an average of 0.5 quality-adjusted life-years at a lifetime cost savings of $41,591 dollars, according to the model.
“In an era of increasing success for kidney transplants and demand that far outstrips supply, deferring antiviral therapy until after transplant of HCV-infected kidneys, when available, should be both cost saving and effective,” the researchers wrote.
The study was funded by grants from Merck Sharpe & Dohme and the National Center for Advancing Translational Science. Several of the authors reported having grants from Merck and grants and personal fees from a variety of other pharmaceutical companies.
SOURCE: Eckman MH et al. Ann Intern Med. 2018 Jul 10. doi: 10.7326/M17-3088.
Transplanting a kidney infected with hepatitis C into individuals infected with HCV, followed by treatment, was more effective and less costly than transplanting an uninfected kidney, preceded by HCV treatment, according to Mark H. Eckman, MD, of the University of Cincinnati and his colleagues.
Largely because of the longer wait times for uninfected kidneys, a typical patient aged 58 years on hemodialysis would gain an average of 0.5 quality-adjusted life-years at a lifetime cost savings of $41,591 dollars, according to the model.
“In an era of increasing success for kidney transplants and demand that far outstrips supply, deferring antiviral therapy until after transplant of HCV-infected kidneys, when available, should be both cost saving and effective,” the researchers wrote.
The study was funded by grants from Merck Sharpe & Dohme and the National Center for Advancing Translational Science. Several of the authors reported having grants from Merck and grants and personal fees from a variety of other pharmaceutical companies.
SOURCE: Eckman MH et al. Ann Intern Med. 2018 Jul 10. doi: 10.7326/M17-3088.
FROM ANNALS OF INTERNAL MEDICINE
Obesity triples post-MI sudden cardiac death risk
Obesity is associated with an increased risk of sudden cardiac death after myocardial infarction, although the so-called “obesity paradox” is still evident in a lower risk of all-cause mortality, a new analysis suggests.
Researchers reported the results of an observational cohort study using data from two Japanese cohort studies involving a total of 6,216 patients discharged alive after acute myocardial infarction. The study was published in the Journal of the American Heart Association.
They found that obese patients – those with a body mass index of at least 27.5 kg/m2 – had a nearly threefold higher risk of sudden cardiac death within 3 years, compared with patients who had a normal BMI, even after adjustment for age, sex, and risk factors such as multivessel disease, left ventricular ejection fraction, and medications.
However, the obese group also showed lower 3-year all-cause mortality, compared with the reference group, whose BMI was 18.5-22.9 kg/m2, while individuals with a BMI below 18.5 kg/m2 had a 61% higher risk of mortality.
The overall all-cause mortality in the cohort was 10.1%, and the incidence of sudden cardiac death was 1.2%.
“For the primary prevention of [coronary artery disease], obesity is recognized as a potent risk factor and an opportunity for therapeutic intervention to prevent cardiovascular disease,” wrote Tsuyoshi Shiga, MD, of Tokyo Women’s Medical University, and coauthors. “However, recent reports have shown that obesity (high BMI) itself does not present a mortality risk but is associated with a better prognosis (obesity paradox) in CAD patients receiving secondary care; these patients received appropriate therapy, including percutaneous coronary intervention and guideline-based medications such as aspirin, beta-blockers, and statins.”
The increased risk of sudden cardiac death in obese patients after MI was harder to explain.
The authors suggested that obesity itself may increase the risk of ventricular arrhythmias developing, and it is also linked with left ventricular hypertrophy, which can lead to cardiac remodeling. Other reports have found evidence in obese individuals of QT prolongation or an increased late potential, and autonomic disturbances that could trigger arrhythmias.
Although reduced left ventricular ejection fraction is the best available predictor of sudden cardiac death, the authors noted that their study found high BMI to be a risk factor independent of left ventricular ejection fraction.
The authors also raised the question of whether intentional weight loss might be effective in reducing the risk of sudden cardiac death in obese patients after MI, but suggested more research was needed to answer this.
The two cohort studies included in the analysis were funded by the Japan Heart Foundation, and the Japan Research Promotion Society for Cardiovascular Diseases. No conflicts of interest were declared.
SOURCE: Shiga T et al. J Am Heart Assoc, 2018; July 7. doi: 10.1161/JAHA.118.008633.
Obesity is associated with an increased risk of sudden cardiac death after myocardial infarction, although the so-called “obesity paradox” is still evident in a lower risk of all-cause mortality, a new analysis suggests.
Researchers reported the results of an observational cohort study using data from two Japanese cohort studies involving a total of 6,216 patients discharged alive after acute myocardial infarction. The study was published in the Journal of the American Heart Association.
They found that obese patients – those with a body mass index of at least 27.5 kg/m2 – had a nearly threefold higher risk of sudden cardiac death within 3 years, compared with patients who had a normal BMI, even after adjustment for age, sex, and risk factors such as multivessel disease, left ventricular ejection fraction, and medications.
However, the obese group also showed lower 3-year all-cause mortality, compared with the reference group, whose BMI was 18.5-22.9 kg/m2, while individuals with a BMI below 18.5 kg/m2 had a 61% higher risk of mortality.
The overall all-cause mortality in the cohort was 10.1%, and the incidence of sudden cardiac death was 1.2%.
“For the primary prevention of [coronary artery disease], obesity is recognized as a potent risk factor and an opportunity for therapeutic intervention to prevent cardiovascular disease,” wrote Tsuyoshi Shiga, MD, of Tokyo Women’s Medical University, and coauthors. “However, recent reports have shown that obesity (high BMI) itself does not present a mortality risk but is associated with a better prognosis (obesity paradox) in CAD patients receiving secondary care; these patients received appropriate therapy, including percutaneous coronary intervention and guideline-based medications such as aspirin, beta-blockers, and statins.”
The increased risk of sudden cardiac death in obese patients after MI was harder to explain.
The authors suggested that obesity itself may increase the risk of ventricular arrhythmias developing, and it is also linked with left ventricular hypertrophy, which can lead to cardiac remodeling. Other reports have found evidence in obese individuals of QT prolongation or an increased late potential, and autonomic disturbances that could trigger arrhythmias.
Although reduced left ventricular ejection fraction is the best available predictor of sudden cardiac death, the authors noted that their study found high BMI to be a risk factor independent of left ventricular ejection fraction.
The authors also raised the question of whether intentional weight loss might be effective in reducing the risk of sudden cardiac death in obese patients after MI, but suggested more research was needed to answer this.
The two cohort studies included in the analysis were funded by the Japan Heart Foundation, and the Japan Research Promotion Society for Cardiovascular Diseases. No conflicts of interest were declared.
SOURCE: Shiga T et al. J Am Heart Assoc, 2018; July 7. doi: 10.1161/JAHA.118.008633.
Obesity is associated with an increased risk of sudden cardiac death after myocardial infarction, although the so-called “obesity paradox” is still evident in a lower risk of all-cause mortality, a new analysis suggests.
Researchers reported the results of an observational cohort study using data from two Japanese cohort studies involving a total of 6,216 patients discharged alive after acute myocardial infarction. The study was published in the Journal of the American Heart Association.
They found that obese patients – those with a body mass index of at least 27.5 kg/m2 – had a nearly threefold higher risk of sudden cardiac death within 3 years, compared with patients who had a normal BMI, even after adjustment for age, sex, and risk factors such as multivessel disease, left ventricular ejection fraction, and medications.
However, the obese group also showed lower 3-year all-cause mortality, compared with the reference group, whose BMI was 18.5-22.9 kg/m2, while individuals with a BMI below 18.5 kg/m2 had a 61% higher risk of mortality.
The overall all-cause mortality in the cohort was 10.1%, and the incidence of sudden cardiac death was 1.2%.
“For the primary prevention of [coronary artery disease], obesity is recognized as a potent risk factor and an opportunity for therapeutic intervention to prevent cardiovascular disease,” wrote Tsuyoshi Shiga, MD, of Tokyo Women’s Medical University, and coauthors. “However, recent reports have shown that obesity (high BMI) itself does not present a mortality risk but is associated with a better prognosis (obesity paradox) in CAD patients receiving secondary care; these patients received appropriate therapy, including percutaneous coronary intervention and guideline-based medications such as aspirin, beta-blockers, and statins.”
The increased risk of sudden cardiac death in obese patients after MI was harder to explain.
The authors suggested that obesity itself may increase the risk of ventricular arrhythmias developing, and it is also linked with left ventricular hypertrophy, which can lead to cardiac remodeling. Other reports have found evidence in obese individuals of QT prolongation or an increased late potential, and autonomic disturbances that could trigger arrhythmias.
Although reduced left ventricular ejection fraction is the best available predictor of sudden cardiac death, the authors noted that their study found high BMI to be a risk factor independent of left ventricular ejection fraction.
The authors also raised the question of whether intentional weight loss might be effective in reducing the risk of sudden cardiac death in obese patients after MI, but suggested more research was needed to answer this.
The two cohort studies included in the analysis were funded by the Japan Heart Foundation, and the Japan Research Promotion Society for Cardiovascular Diseases. No conflicts of interest were declared.
SOURCE: Shiga T et al. J Am Heart Assoc, 2018; July 7. doi: 10.1161/JAHA.118.008633.
FROM JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Obese MI patients have a significantly elevated risk of sudden cardiac death.
Major finding:
Study details: An Japanese observational cohort study of 6,216 patients with acute myocardial infarction.
Disclosures: The two cohort studies included in the analysis were funded by the Japan Heart Foundation, and the Japan Research Promotion Society for Cardiovascular Diseases. No conflicts of interest were declared.
Source: Shiga T et al. J Am Heart Assoc. 2018; July 7. doi: 10.1161/JAHA.118.008633.
Firehawk: A new ‘workhorse’ DES
PARIS – The Xience everolimus-eluting coronary stent is widely considered the current standard treatment, implanted by interventional cardiologists far more often than any other drug-eluting stent (DES). But judging from the results of the TARGET All Comers trial, some serious competition may be headed Xience’s way in the form of the new Firehawk rapamycin-eluting, thin-strut stent featuring a biodegradable polymer drug delivery system.

What’s more, the Firehawk offers a theoretical advantage in that the rapamycin is delivered via a polymer that’s fully absorbed by 9 months, leaving behind a bare metal stent made of cobalt chromium. This structure is believed to be less proinflammatory, atherogenic, and thrombogenic over the long haul, compared with a permanent durable polymer, such as that employed in the Xience stent. This should translate into less late restenosis and in-stent thrombosis.
Also, the Firehawk features thin, 86-mcm struts and the rapamycin, also known as sirolimus, is contained in abluminal grooves directed specifically to the vessel wall. As a result, this DES exposes patients to only one-third as much active drug as other DESs. Ninety percent of the rapamycin is released within 90 days after implantation, according to Dr. Baumbach, director of interventional research at Barts Heart Centre in London and president of the European Association of Percutaneous Cardiovascular Interventions.
The TARGET All Comers trial is a prospective, open-label, noninferiority trial comparing the safety and efficacy of the Firehawk with those of Xience stents in 1,656 DES-eligible patients with symptomatic coronary artery disease randomized at 21 centers.
The primary endpoint was the 12-month composite of target lesion failure, comprising rates of cardiac death, target vessel MI, or ischemia-driven target lesion revascularization. In an intention-to-treat analysis, the rate was 6.1% in the Firehawk patients and 5.9% in the Xience recipients. Results for each of the three components of the composite endpoint were similar in the two groups as well.
A secondary endpoint was in-stent late loss as measured by quantitative coronary angiography at 13 months in a 137-patient subgroup. The rate was 0.17 mm in the Firehawk recipients and similar at 0.11 mm in those receiving the Xience stent, again, which provided solid evidence of noninferiority.
The rate of definite stent thrombosis at 1 year was 1.2% in both study arms.
Discussant Giulio Guagliumi, MD, an interventional cardiologist at Pope Giovanni XXIII Hospital in Bergamo, Italy, pronounced the results “quite reassuring.” But where, he asked, is the evidence of late benefit for the completely biodegradable polymer utilized in the Firehawk?
“We would expect to see such an effect later on, after the stent in question becomes a simple bare metal stent as opposed to a stent with a durable polymer. But we don’t have the ultimate answer yet. In this trial we will have an extended follow-up out to 5 years to see whether there is any translation of these differences into clinical benefit,” Dr. Baumbach replied.
Discussion panelist Julinda Mehilli, MD, inquired how this new stent, which has been approved for the European market, will fit into everyday clinical practice.
“We have many biodegradable polymer DES already. We have the Ultimaster, we have Synergy – and now, the Firehawk. What kind of special features does it have? Is it for use in routine practice or in special populations?” asked Dr. Mehilli, director of interventional cardiology at the German Heart Center at the University of Munich.
“That’s of course the question: What’s the unique point of this stent? I think that the unique point is that there is really no unique point. This is a classic workhorse stent. This is a stent with good radial force and all the other features for everyday use,” according to Dr. Baumbach.
Indeed, he and his Barts colleagues did more than 100 cases in TARGET All Comers and found one of the Firehawk’s strengths was its versatility. It performed well in challenging cases, including left main interventions, as well as in more straightforward cases in this all comers trial.
The Firehawk was developed by MicroPort in China, where its safety and efficacy was established in clinical trials totaling more than 1,000 patients. It then moved to Europe, where it has earned regulatory approval. A pivotal U.S. trial is being planned with the Food and Drug Administration, which has indicated that the European TARGET All Comers data can be incorporated in the study.
Dr. Baumbach reported receiving research grants from Abbott and consultation fees from Keystone Heart, MicroPort, Sinomed, and Stentys.
PARIS – The Xience everolimus-eluting coronary stent is widely considered the current standard treatment, implanted by interventional cardiologists far more often than any other drug-eluting stent (DES). But judging from the results of the TARGET All Comers trial, some serious competition may be headed Xience’s way in the form of the new Firehawk rapamycin-eluting, thin-strut stent featuring a biodegradable polymer drug delivery system.
What’s more, the Firehawk offers a theoretical advantage in that the rapamycin is delivered via a polymer that’s fully absorbed by 9 months, leaving behind a bare metal stent made of cobalt chromium. This structure is believed to be less proinflammatory, atherogenic, and thrombogenic over the long haul, compared with a permanent durable polymer, such as that employed in the Xience stent. This should translate into less late restenosis and in-stent thrombosis.
Also, the Firehawk features thin, 86-mcm struts and the rapamycin, also known as sirolimus, is contained in abluminal grooves directed specifically to the vessel wall. As a result, this DES exposes patients to only one-third as much active drug as other DESs. Ninety percent of the rapamycin is released within 90 days after implantation, according to Dr. Baumbach, director of interventional research at Barts Heart Centre in London and president of the European Association of Percutaneous Cardiovascular Interventions.
The TARGET All Comers trial is a prospective, open-label, noninferiority trial comparing the safety and efficacy of the Firehawk with those of Xience stents in 1,656 DES-eligible patients with symptomatic coronary artery disease randomized at 21 centers.
The primary endpoint was the 12-month composite of target lesion failure, comprising rates of cardiac death, target vessel MI, or ischemia-driven target lesion revascularization. In an intention-to-treat analysis, the rate was 6.1% in the Firehawk patients and 5.9% in the Xience recipients. Results for each of the three components of the composite endpoint were similar in the two groups as well.
A secondary endpoint was in-stent late loss as measured by quantitative coronary angiography at 13 months in a 137-patient subgroup. The rate was 0.17 mm in the Firehawk recipients and similar at 0.11 mm in those receiving the Xience stent, again, which provided solid evidence of noninferiority.
The rate of definite stent thrombosis at 1 year was 1.2% in both study arms.
Discussant Giulio Guagliumi, MD, an interventional cardiologist at Pope Giovanni XXIII Hospital in Bergamo, Italy, pronounced the results “quite reassuring.” But where, he asked, is the evidence of late benefit for the completely biodegradable polymer utilized in the Firehawk?
“We would expect to see such an effect later on, after the stent in question becomes a simple bare metal stent as opposed to a stent with a durable polymer. But we don’t have the ultimate answer yet. In this trial we will have an extended follow-up out to 5 years to see whether there is any translation of these differences into clinical benefit,” Dr. Baumbach replied.
Discussion panelist Julinda Mehilli, MD, inquired how this new stent, which has been approved for the European market, will fit into everyday clinical practice.
“We have many biodegradable polymer DES already. We have the Ultimaster, we have Synergy – and now, the Firehawk. What kind of special features does it have? Is it for use in routine practice or in special populations?” asked Dr. Mehilli, director of interventional cardiology at the German Heart Center at the University of Munich.
“That’s of course the question: What’s the unique point of this stent? I think that the unique point is that there is really no unique point. This is a classic workhorse stent. This is a stent with good radial force and all the other features for everyday use,” according to Dr. Baumbach.
Indeed, he and his Barts colleagues did more than 100 cases in TARGET All Comers and found one of the Firehawk’s strengths was its versatility. It performed well in challenging cases, including left main interventions, as well as in more straightforward cases in this all comers trial.
The Firehawk was developed by MicroPort in China, where its safety and efficacy was established in clinical trials totaling more than 1,000 patients. It then moved to Europe, where it has earned regulatory approval. A pivotal U.S. trial is being planned with the Food and Drug Administration, which has indicated that the European TARGET All Comers data can be incorporated in the study.
Dr. Baumbach reported receiving research grants from Abbott and consultation fees from Keystone Heart, MicroPort, Sinomed, and Stentys.
PARIS – The Xience everolimus-eluting coronary stent is widely considered the current standard treatment, implanted by interventional cardiologists far more often than any other drug-eluting stent (DES). But judging from the results of the TARGET All Comers trial, some serious competition may be headed Xience’s way in the form of the new Firehawk rapamycin-eluting, thin-strut stent featuring a biodegradable polymer drug delivery system.
What’s more, the Firehawk offers a theoretical advantage in that the rapamycin is delivered via a polymer that’s fully absorbed by 9 months, leaving behind a bare metal stent made of cobalt chromium. This structure is believed to be less proinflammatory, atherogenic, and thrombogenic over the long haul, compared with a permanent durable polymer, such as that employed in the Xience stent. This should translate into less late restenosis and in-stent thrombosis.
Also, the Firehawk features thin, 86-mcm struts and the rapamycin, also known as sirolimus, is contained in abluminal grooves directed specifically to the vessel wall. As a result, this DES exposes patients to only one-third as much active drug as other DESs. Ninety percent of the rapamycin is released within 90 days after implantation, according to Dr. Baumbach, director of interventional research at Barts Heart Centre in London and president of the European Association of Percutaneous Cardiovascular Interventions.
The TARGET All Comers trial is a prospective, open-label, noninferiority trial comparing the safety and efficacy of the Firehawk with those of Xience stents in 1,656 DES-eligible patients with symptomatic coronary artery disease randomized at 21 centers.
The primary endpoint was the 12-month composite of target lesion failure, comprising rates of cardiac death, target vessel MI, or ischemia-driven target lesion revascularization. In an intention-to-treat analysis, the rate was 6.1% in the Firehawk patients and 5.9% in the Xience recipients. Results for each of the three components of the composite endpoint were similar in the two groups as well.
A secondary endpoint was in-stent late loss as measured by quantitative coronary angiography at 13 months in a 137-patient subgroup. The rate was 0.17 mm in the Firehawk recipients and similar at 0.11 mm in those receiving the Xience stent, again, which provided solid evidence of noninferiority.
The rate of definite stent thrombosis at 1 year was 1.2% in both study arms.
Discussant Giulio Guagliumi, MD, an interventional cardiologist at Pope Giovanni XXIII Hospital in Bergamo, Italy, pronounced the results “quite reassuring.” But where, he asked, is the evidence of late benefit for the completely biodegradable polymer utilized in the Firehawk?
“We would expect to see such an effect later on, after the stent in question becomes a simple bare metal stent as opposed to a stent with a durable polymer. But we don’t have the ultimate answer yet. In this trial we will have an extended follow-up out to 5 years to see whether there is any translation of these differences into clinical benefit,” Dr. Baumbach replied.
Discussion panelist Julinda Mehilli, MD, inquired how this new stent, which has been approved for the European market, will fit into everyday clinical practice.
“We have many biodegradable polymer DES already. We have the Ultimaster, we have Synergy – and now, the Firehawk. What kind of special features does it have? Is it for use in routine practice or in special populations?” asked Dr. Mehilli, director of interventional cardiology at the German Heart Center at the University of Munich.
“That’s of course the question: What’s the unique point of this stent? I think that the unique point is that there is really no unique point. This is a classic workhorse stent. This is a stent with good radial force and all the other features for everyday use,” according to Dr. Baumbach.
Indeed, he and his Barts colleagues did more than 100 cases in TARGET All Comers and found one of the Firehawk’s strengths was its versatility. It performed well in challenging cases, including left main interventions, as well as in more straightforward cases in this all comers trial.
The Firehawk was developed by MicroPort in China, where its safety and efficacy was established in clinical trials totaling more than 1,000 patients. It then moved to Europe, where it has earned regulatory approval. A pivotal U.S. trial is being planned with the Food and Drug Administration, which has indicated that the European TARGET All Comers data can be incorporated in the study.
Dr. Baumbach reported receiving research grants from Abbott and consultation fees from Keystone Heart, MicroPort, Sinomed, and Stentys.
REPORTING FROM EUROPCR 2018
Key clinical point: The Firehawk has established itself as a versatile workhorse coronary stent.
Major finding:
Study details: This open-label international study randomized 1,656 patients with symptomatic CAD to one of two drug-eluting stents.
Disclosures: The TARGET All Comers trial was sponsored by MicroPort. The presenter reported serving as a consultant to MicroPort and other companies.
SLE flares linked to air temperature, pollution
AMSTERDAM – Both air temperature and air pollution levels affected the likelihood of experiencing a flare in systemic lupus erythematosus (SLE) organ-specific disease activity in a study presented at the European Congress of Rheumatology.
For every 1° F increase in temperature, there was an increase in the odds of experiencing a skin flare (odds ratio, 1.0075), joint flare (OR, 1.0110), or neurologic flare (OR, 1.0096), reported George Stojan, MD, and associates during one of the poster sessions. Conversely, renal flares were less likely to occur with rising temperature (OR, 0.9960). The latter is something previously reported, Dr. Stojan said in an interview, “as we found most renal flares occur in the winter, not in the summer months.”
Furthermore, for every 1 mcg per cubic meter increase in fine particulate matter pollution (PM2.5), there were increases in serositis (OR, 1.0240) and hematologic flares (OR, 1.011).
There were two reasons for looking at the role of these environmental factors in relation to SLE flares, said Dr. Stojan, an assistant professor of medicine at Johns Hopkins University, Baltimore. “The first was a clinical observation – I was getting clusters of patients with certain disease manifestations, for example with serositis or joint flares, and there wasn’t a random distribution.”
The second was a patient observation, added Dr. Stojan, who is also codirector of the Johns Hopkins Lupus Center. Every year, patients treated at the Center have the opportunity to meet each other and hear about the research being done by the team, and it was at this meeting that patients said they felt they were experiencing similar disease flares.
To look at the underlying role of environmental exposures in the development of SLE and possible associations with disease activity, Dr. Stojan and associates used a method known as cluster detection, which is commonly used in public health studies.
The investigators used a 350-km radial zone around the Johns Hopkins Lupus Center for the analysis as this was an area where a uniform number of patients treated by the center were living. They obtained data on 1,261 patients in the Hopkins Lupus Cohort, spanning a 10-year period from 1999 to 2009, and used SaTScan software to identify clusters of disease activity occurring during 3 separate monthly time intervals in different counties. The researchers then linked these clusters to average temperature and PM2.5 data obtained from the Environmental Protection Agency for the 10 days prior to patients’ visits.
“The SaTScan system predicts how many flares per organ system you would expect in a county based on the number of patients and based on the total flares we have in our cohort,” Dr. Stojan explained. Previously, the system helped to identify areas that had a higher flare incidence for each organ system that lasted for about 2-3 years, did not overlap, and could not be explained. So, the next step was to look for potential environmental triggers.
“Basically, the SaTScan adjusts the data that’s inputted for temperature and small particulate pollution. If the cluster moves in space and time then these did affect it,” Dr. Stojan said. “It seems that these do affect certain types of organ flares,” even after adjustment for other variables such as patients’ age, gender, income, ethnicity, and living situation (rural or urban).
Flares in skin symptoms during the summer have been identified before, he acknowledged, but the link to joint flares or neurologic flares have not. The latter includes things like seizures, neuropathy, or abnormal brain imaging rather than mood changes or mild cognitive dysfunction.
These data could have an impact on how clinical trials are designed, Dr. Stojan added, suggesting that factoring in where patients live and how close they are to areas of pollution could ensure a uniform population of patients is studied.
From a more practical perspective, these data might help to develop predictive models to help understand when patients are likely to experience a flare and if any action can be taken to ameliorate the effects of exposure.
The next step is a collaboration with patients to develop software or a mobile application where patients could input information about any disease flares. This would enable a finer view of what could be happening, Dr. Stojan said, as while daily readings are available for the environmental factors studied, disease activity data is only available during 3 separate monthly intervals. It would also allow other environmental factors to be considered.
“I think this is an important step in figuring out environmental factors and their influence on lupus,” he said. “There has been an extensive amount of research into viral causes and potential infectious triggers, but spatial-temporal analysis of environmental variables have never been done before in lupus.”
The study received no commercial funding, and Dr. Stojan reported having no disclosures.
SOURCE: Stojan G et al. Ann Rheum Dis. 2018;77(Suppl 2):1191. Abstract SAT0685.
AMSTERDAM – Both air temperature and air pollution levels affected the likelihood of experiencing a flare in systemic lupus erythematosus (SLE) organ-specific disease activity in a study presented at the European Congress of Rheumatology.
For every 1° F increase in temperature, there was an increase in the odds of experiencing a skin flare (odds ratio, 1.0075), joint flare (OR, 1.0110), or neurologic flare (OR, 1.0096), reported George Stojan, MD, and associates during one of the poster sessions. Conversely, renal flares were less likely to occur with rising temperature (OR, 0.9960). The latter is something previously reported, Dr. Stojan said in an interview, “as we found most renal flares occur in the winter, not in the summer months.”
Furthermore, for every 1 mcg per cubic meter increase in fine particulate matter pollution (PM2.5), there were increases in serositis (OR, 1.0240) and hematologic flares (OR, 1.011).
There were two reasons for looking at the role of these environmental factors in relation to SLE flares, said Dr. Stojan, an assistant professor of medicine at Johns Hopkins University, Baltimore. “The first was a clinical observation – I was getting clusters of patients with certain disease manifestations, for example with serositis or joint flares, and there wasn’t a random distribution.”
The second was a patient observation, added Dr. Stojan, who is also codirector of the Johns Hopkins Lupus Center. Every year, patients treated at the Center have the opportunity to meet each other and hear about the research being done by the team, and it was at this meeting that patients said they felt they were experiencing similar disease flares.
To look at the underlying role of environmental exposures in the development of SLE and possible associations with disease activity, Dr. Stojan and associates used a method known as cluster detection, which is commonly used in public health studies.
The investigators used a 350-km radial zone around the Johns Hopkins Lupus Center for the analysis as this was an area where a uniform number of patients treated by the center were living. They obtained data on 1,261 patients in the Hopkins Lupus Cohort, spanning a 10-year period from 1999 to 2009, and used SaTScan software to identify clusters of disease activity occurring during 3 separate monthly time intervals in different counties. The researchers then linked these clusters to average temperature and PM2.5 data obtained from the Environmental Protection Agency for the 10 days prior to patients’ visits.
“The SaTScan system predicts how many flares per organ system you would expect in a county based on the number of patients and based on the total flares we have in our cohort,” Dr. Stojan explained. Previously, the system helped to identify areas that had a higher flare incidence for each organ system that lasted for about 2-3 years, did not overlap, and could not be explained. So, the next step was to look for potential environmental triggers.
“Basically, the SaTScan adjusts the data that’s inputted for temperature and small particulate pollution. If the cluster moves in space and time then these did affect it,” Dr. Stojan said. “It seems that these do affect certain types of organ flares,” even after adjustment for other variables such as patients’ age, gender, income, ethnicity, and living situation (rural or urban).
Flares in skin symptoms during the summer have been identified before, he acknowledged, but the link to joint flares or neurologic flares have not. The latter includes things like seizures, neuropathy, or abnormal brain imaging rather than mood changes or mild cognitive dysfunction.
These data could have an impact on how clinical trials are designed, Dr. Stojan added, suggesting that factoring in where patients live and how close they are to areas of pollution could ensure a uniform population of patients is studied.
From a more practical perspective, these data might help to develop predictive models to help understand when patients are likely to experience a flare and if any action can be taken to ameliorate the effects of exposure.
The next step is a collaboration with patients to develop software or a mobile application where patients could input information about any disease flares. This would enable a finer view of what could be happening, Dr. Stojan said, as while daily readings are available for the environmental factors studied, disease activity data is only available during 3 separate monthly intervals. It would also allow other environmental factors to be considered.
“I think this is an important step in figuring out environmental factors and their influence on lupus,” he said. “There has been an extensive amount of research into viral causes and potential infectious triggers, but spatial-temporal analysis of environmental variables have never been done before in lupus.”
The study received no commercial funding, and Dr. Stojan reported having no disclosures.
SOURCE: Stojan G et al. Ann Rheum Dis. 2018;77(Suppl 2):1191. Abstract SAT0685.
AMSTERDAM – Both air temperature and air pollution levels affected the likelihood of experiencing a flare in systemic lupus erythematosus (SLE) organ-specific disease activity in a study presented at the European Congress of Rheumatology.
For every 1° F increase in temperature, there was an increase in the odds of experiencing a skin flare (odds ratio, 1.0075), joint flare (OR, 1.0110), or neurologic flare (OR, 1.0096), reported George Stojan, MD, and associates during one of the poster sessions. Conversely, renal flares were less likely to occur with rising temperature (OR, 0.9960). The latter is something previously reported, Dr. Stojan said in an interview, “as we found most renal flares occur in the winter, not in the summer months.”
Furthermore, for every 1 mcg per cubic meter increase in fine particulate matter pollution (PM2.5), there were increases in serositis (OR, 1.0240) and hematologic flares (OR, 1.011).
There were two reasons for looking at the role of these environmental factors in relation to SLE flares, said Dr. Stojan, an assistant professor of medicine at Johns Hopkins University, Baltimore. “The first was a clinical observation – I was getting clusters of patients with certain disease manifestations, for example with serositis or joint flares, and there wasn’t a random distribution.”
The second was a patient observation, added Dr. Stojan, who is also codirector of the Johns Hopkins Lupus Center. Every year, patients treated at the Center have the opportunity to meet each other and hear about the research being done by the team, and it was at this meeting that patients said they felt they were experiencing similar disease flares.
To look at the underlying role of environmental exposures in the development of SLE and possible associations with disease activity, Dr. Stojan and associates used a method known as cluster detection, which is commonly used in public health studies.
The investigators used a 350-km radial zone around the Johns Hopkins Lupus Center for the analysis as this was an area where a uniform number of patients treated by the center were living. They obtained data on 1,261 patients in the Hopkins Lupus Cohort, spanning a 10-year period from 1999 to 2009, and used SaTScan software to identify clusters of disease activity occurring during 3 separate monthly time intervals in different counties. The researchers then linked these clusters to average temperature and PM2.5 data obtained from the Environmental Protection Agency for the 10 days prior to patients’ visits.
“The SaTScan system predicts how many flares per organ system you would expect in a county based on the number of patients and based on the total flares we have in our cohort,” Dr. Stojan explained. Previously, the system helped to identify areas that had a higher flare incidence for each organ system that lasted for about 2-3 years, did not overlap, and could not be explained. So, the next step was to look for potential environmental triggers.
“Basically, the SaTScan adjusts the data that’s inputted for temperature and small particulate pollution. If the cluster moves in space and time then these did affect it,” Dr. Stojan said. “It seems that these do affect certain types of organ flares,” even after adjustment for other variables such as patients’ age, gender, income, ethnicity, and living situation (rural or urban).
Flares in skin symptoms during the summer have been identified before, he acknowledged, but the link to joint flares or neurologic flares have not. The latter includes things like seizures, neuropathy, or abnormal brain imaging rather than mood changes or mild cognitive dysfunction.
These data could have an impact on how clinical trials are designed, Dr. Stojan added, suggesting that factoring in where patients live and how close they are to areas of pollution could ensure a uniform population of patients is studied.
From a more practical perspective, these data might help to develop predictive models to help understand when patients are likely to experience a flare and if any action can be taken to ameliorate the effects of exposure.
The next step is a collaboration with patients to develop software or a mobile application where patients could input information about any disease flares. This would enable a finer view of what could be happening, Dr. Stojan said, as while daily readings are available for the environmental factors studied, disease activity data is only available during 3 separate monthly intervals. It would also allow other environmental factors to be considered.
“I think this is an important step in figuring out environmental factors and their influence on lupus,” he said. “There has been an extensive amount of research into viral causes and potential infectious triggers, but spatial-temporal analysis of environmental variables have never been done before in lupus.”
The study received no commercial funding, and Dr. Stojan reported having no disclosures.
SOURCE: Stojan G et al. Ann Rheum Dis. 2018;77(Suppl 2):1191. Abstract SAT0685.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point:
Major finding: For every 1° F increase in temperature, the risk for skin, joint, or neurologic flares increased.
Study details: A spatial-time cluster analysis of 1,261 patients in the Hopkins Lupus Cohort linking disease activity to temperature changes and fine particulate matter pollution.
Disclosures: The study received no commercial funding, and Dr. Stojan reported having no disclosures.
Source: Stojan G et al. Ann Rheum Dis. 2018;77(Suppl 2):1191. Abstract SAT0685.
Negotiating physician employment agreements
You have finally completed your residency or fellowship, and now you have a job offer. With some trepidation, you decide to read the employment agreement that has been emailed to you. You quickly realize that you do not understand much of it. All those legal terms! You lament the fact that medical school never taught you about the business of medicine. What are you going to do? The choices are actually quite simple: You can take the time to educate yourself or you can hire an expert. This article will review some of the basic principles of negotiating as well as some of the critical issues found in physician employment agreements today.
Whether you represent yourself or hire someone to do it for you, it is important to understand some of the basic principles of negotiating. These principles generally are applicable whether you are buying a house or negotiating your employment agreement.
Negotiations

The most important principle is preparation. For example, many physicians negotiate their salaries during the interview process. Consequently, it is imperative that, before you negotiate your compensation, you know the range of salaries in your area for your specialty. It is also important to know whether salaries are usually guaranteed in your market, or whether production-based salaries (which are based on the amount of your billings) are the norm. Never go into an interview unprepared!
Always try to gain leverage in your negotiations. The easiest way to accomplish this is by having multiple offers, and subtly letting your suitors know this. Allow adequate time to negotiate; the more time you have, the easier it is to negotiate. Establish your objectives and try to anticipate the objectives of the other party. Determine your best-case and worse-case scenarios, as well as the most likely outcome. Do not negotiate against yourself and try to get something every time you give something. Define the nonnegotiable issues, and do not waste time on them. Keep cool and be flexible.
The first question you must answer when you receive an employment agreement is who is going to negotiate it. Many new physicians hire attorneys to help them with their employment agreements and employers expect as much. It is best to engage an attorney before you begin your job search so you can get a better understanding of how the attorney can help you. Most attorneys do not charge a prospective client for such information. However, many physicians wait until they actually receive an offer before contacting an attorney. It is not uncommon for physicians to negotiate their salaries during job interviews even if they eventually hire an attorney to help them. This is usually attributable to a lack of negotiating experience and an eagerness to determine whether a job offer is viable. Keep in mind that an attorney often can negotiate a better starting salary than you, so try to resist the temptation to negotiate your salary during the interview process.
Compensation
With compensation in mind, what are some of the important issues? Today, many physician employers are converting to production-based compensation models. Consequently, it is important for new physicians to obtain guaranteed base salaries during their first few years of employment while they are building their practices.
On occasion, new physicians initially are offered production-based compensation models, which also allocate a share of practice overhead expenses to them. This is a very dangerous compensation model for a new physician. Under such a model, it is possible that a new physician could have a negative balance in his/her cost center at the end of the year, and actually owe his/her employer money.
Some physicians may be offered income guarantees by hospitals. There are several different types of income guarantees but they are frequently categorized together even though they differ significantly. The most common income guarantees offered to physicians are physician recruitment agreements (PRAs). Under a PRA, a hospital usually guarantees that a physician who relocates to the service area of the hospital collects a minimum amount of monthly revenue for 1-2 years, which is known as the guarantee period. The hospital also guarantees to pay certain monthly expenses of the physician during the guarantee period. This arrangement is actually structured as a loan by the hospital to the physician, and requires the physician to execute a promissory note with the hospital for the amounts advanced to the physician by the hospital. The promissory note is forgiven if the physician continues to practice in the service area for 2-3 years after the guarantee period. This type of guarantee provides an excellent opportunity for a new physician to establish a solo practice. A variation of this model involves a third party such as a medical group. Under this model, the hospital continues to guarantee the revenue of the new physician and pays the medical group the expenses it incurs as a result of hiring the new physician. These expenses are known as incremental practice expenses. The medical group also becomes a signatory to the promissory note. Other health care entities also have begun to offer PRAs to physicians. For example, an independent practice association in California recently entered into a PRA with a gastroenterologist.
Keep in mind that the promissory note executed by the physician may affect the credit of the physician, especially if he/she wants to obtain financing for a home purchase. Also, a hospital may seek security for the performance of the promissory note by collateralizing the personal assets of the physician instead of just his/her practice assets; this should be avoided.
The other type of income guarantee is provided to hospital-based physicians such as pathologists, radiologists, anesthesiologists, etc. Under this type of guarantee, a hospital ensures that the physicians receive a minimum threshold of collections. This type of guarantee may be necessary to attract hospital-based physicians to a hospital which has a low-income and/or Medicaid population. This is not a typical scenario for a gastroenterologist.
Some practices create incentives for physicians by offering a variety of bonuses. Most often these bonuses are production based but sometimes they are based on such quality issues as patient satisfaction. The most common types of production bonuses are based on attaining a level of collections above a dollar threshold or exceeding a minimum level of relative value units (RVUs).
To summarize, new physicians should always try to get at least a 2-year income guarantee. They should never allow an employer to allocate overhead to them during the first 2 years of employment. In addition, they should always try to negotiate realistic production-based bonuses.
Benefits
Fringe benefits are an integral part of a compensation package for a new physician. Most physician employers offer a generous package of health insurance, retirement, reimbursable expenses, and paid time off. These benefits should be clearly delineated in the employment agreement or employee handbook. A very common question about health benefits is when they become effective (the first day of employment, 30 days after employment, the first of the month after employment, etc.). This is significant because Consolidated Omnibus Budget Reconciliation Act (COBRA) is quite expensive. Another issue is whether health insurance also will cover the physician’s spouse and dependents. Most physician employers cover only the physician, not his/her spouse and dependents. If a new physician has a spouse who already provides family health benefits, it may behoove the physician to negotiate an allowance in lieu of health benefits.
Paid time off of 10-20 days are commonly given by physician employers to new physicians. Some employers also provide 5 or more additional days of paid time off for Continuing Medical Education (CME). Of course, once a physician goes onto production-based compensation, paid time off usually is not provided.
It is very important that a physician employer offer a retirement plan. Oftentimes, there is a matching contribution by the employer. However, it is not uncommon for there to be a year waiting period for eligibility in the retirement plan. Retirement plans vary significantly so it is advisable for a new physician to meet with the employer’s human resources department to get the details of the plan offered; the physician may want to confer with a financial advisor after obtaining this information.
Most physician employers reimburse licensing and DEA fees, medical staff dues, and board certification expenses. There is often a CME allowance as well. In competitive markets, some physician employers also offer innovative benefits such as student loan repayment programs, fellowship and residency stipends, and forgivable loans for housing. Sometimes these benefits are not included in the employment agreement; you may have to ask for them.
Indemnification/noncompetition
In addition to compensation and benefits, there are several other issues which are commonly found in employment agreements. Perhaps the most controversial is the issue of indemnification. The legal concept of indemnity allows a physician employer to recover damages and defense costs from a physician employee in certain circumstances. For example, if a physician employer has a $1,000,000/$3,000,000 malpractice policy covering itself and each of its physician employees, and if a physician commits malpractice and the award is $2,000,000, the employer may seek to recover the $1,000,000 deficit from the physician. In California, for example, the physician employer would be prohibited from seeking the deficit from the physician employee, but in most states, it is permitted. Because insurance policies usually do not cover physicians for damages, expenses, costs, etc as a result of an indemnification action, there is no practical way for a physician to protect himself/herself from the consequences. It is very important that physicians not sign any type of agreement with an indemnification clause in it without consulting an attorney first.
Another controversial issue is noncompete restrictions. In many states, a physician employer can restrict a physician employee from competing with it after an employment agreement is terminated. The noncompete prohibitions usually last for 1-2 years and extend over a geographic area, which often causes a terminated physician to relocate. Importantly, noncompete clauses are generally enforceable in most states.
Tail coverage
Malpractice tail coverage often can be an issue as well. For many years, physician employers routinely paid the cost of tail coverage for a physician employee after termination of employment. Tail coverage is necessary because most malpractice policies are claims-made insurance instead of occurrence insurance. This means that the insurance is applicable when a claim is filed versus when a malpractice act or omission occurred. Because of the significant cost of tail coverage, many physician employers attempt to transfer this financial responsibility to physician employees. Depending on a physician’s specialty, tail coverage can be quite costly. Consequently, it behooves physicians to carefully negotiate this issue. If a physician employer is unwilling to provide tail coverage, a compromise may be proposed whereby the physician employee is responsible only for the cost of tail coverage if he/she terminates the employment agreement without cause or if the physician employer terminates the employment agreement for cause. Conversely, the physician employer would be responsible for the cost if the physician employer terminates the employment agreement without cause or the physician employee terminates the employment agreement for cause.
Equity accrual
Finally, new physicians always should ask whether there is an opportunity to obtain equity in the organizations that hire them. Many for-profit physician employers provide such an opportunity to new physicians after 2-3 years. However, timing is just one factor. Importantly, the cost of the buy-in is critical especially to new physicians with student loans. Recognizing this problem, the trend today is for physician employers to have nominal buy-ins. Notwithstanding this trend, some physician employers also own ambulatory surgery centers and the buy-ins for these entities must be at fair market value and cannot be financed by the center or its owners under the law. Consequently, the buy-in for ambulatory surgery centers is usually substantial and requires a physician to obtain outside financing.
In conclusion, when evaluating the viability of a physician employment opportunity, salary should be only one factor considered. Fringe benefits, the opportunity for equity, and the fairness of the employment agreement also should be weighed heavily by a physician. It is important for a physician to be comfortable with his/her peers and work environment. Selecting the right job opportunity can be challenging. However, the process will be much easier if you remember the basic principles of negotiating.
You have finally completed your residency or fellowship, and now you have a job offer. With some trepidation, you decide to read the employment agreement that has been emailed to you. You quickly realize that you do not understand much of it. All those legal terms! You lament the fact that medical school never taught you about the business of medicine. What are you going to do? The choices are actually quite simple: You can take the time to educate yourself or you can hire an expert. This article will review some of the basic principles of negotiating as well as some of the critical issues found in physician employment agreements today.
Whether you represent yourself or hire someone to do it for you, it is important to understand some of the basic principles of negotiating. These principles generally are applicable whether you are buying a house or negotiating your employment agreement.
Negotiations
The most important principle is preparation. For example, many physicians negotiate their salaries during the interview process. Consequently, it is imperative that, before you negotiate your compensation, you know the range of salaries in your area for your specialty. It is also important to know whether salaries are usually guaranteed in your market, or whether production-based salaries (which are based on the amount of your billings) are the norm. Never go into an interview unprepared!
Always try to gain leverage in your negotiations. The easiest way to accomplish this is by having multiple offers, and subtly letting your suitors know this. Allow adequate time to negotiate; the more time you have, the easier it is to negotiate. Establish your objectives and try to anticipate the objectives of the other party. Determine your best-case and worse-case scenarios, as well as the most likely outcome. Do not negotiate against yourself and try to get something every time you give something. Define the nonnegotiable issues, and do not waste time on them. Keep cool and be flexible.
The first question you must answer when you receive an employment agreement is who is going to negotiate it. Many new physicians hire attorneys to help them with their employment agreements and employers expect as much. It is best to engage an attorney before you begin your job search so you can get a better understanding of how the attorney can help you. Most attorneys do not charge a prospective client for such information. However, many physicians wait until they actually receive an offer before contacting an attorney. It is not uncommon for physicians to negotiate their salaries during job interviews even if they eventually hire an attorney to help them. This is usually attributable to a lack of negotiating experience and an eagerness to determine whether a job offer is viable. Keep in mind that an attorney often can negotiate a better starting salary than you, so try to resist the temptation to negotiate your salary during the interview process.
Compensation
With compensation in mind, what are some of the important issues? Today, many physician employers are converting to production-based compensation models. Consequently, it is important for new physicians to obtain guaranteed base salaries during their first few years of employment while they are building their practices.
On occasion, new physicians initially are offered production-based compensation models, which also allocate a share of practice overhead expenses to them. This is a very dangerous compensation model for a new physician. Under such a model, it is possible that a new physician could have a negative balance in his/her cost center at the end of the year, and actually owe his/her employer money.
Some physicians may be offered income guarantees by hospitals. There are several different types of income guarantees but they are frequently categorized together even though they differ significantly. The most common income guarantees offered to physicians are physician recruitment agreements (PRAs). Under a PRA, a hospital usually guarantees that a physician who relocates to the service area of the hospital collects a minimum amount of monthly revenue for 1-2 years, which is known as the guarantee period. The hospital also guarantees to pay certain monthly expenses of the physician during the guarantee period. This arrangement is actually structured as a loan by the hospital to the physician, and requires the physician to execute a promissory note with the hospital for the amounts advanced to the physician by the hospital. The promissory note is forgiven if the physician continues to practice in the service area for 2-3 years after the guarantee period. This type of guarantee provides an excellent opportunity for a new physician to establish a solo practice. A variation of this model involves a third party such as a medical group. Under this model, the hospital continues to guarantee the revenue of the new physician and pays the medical group the expenses it incurs as a result of hiring the new physician. These expenses are known as incremental practice expenses. The medical group also becomes a signatory to the promissory note. Other health care entities also have begun to offer PRAs to physicians. For example, an independent practice association in California recently entered into a PRA with a gastroenterologist.
Keep in mind that the promissory note executed by the physician may affect the credit of the physician, especially if he/she wants to obtain financing for a home purchase. Also, a hospital may seek security for the performance of the promissory note by collateralizing the personal assets of the physician instead of just his/her practice assets; this should be avoided.
The other type of income guarantee is provided to hospital-based physicians such as pathologists, radiologists, anesthesiologists, etc. Under this type of guarantee, a hospital ensures that the physicians receive a minimum threshold of collections. This type of guarantee may be necessary to attract hospital-based physicians to a hospital which has a low-income and/or Medicaid population. This is not a typical scenario for a gastroenterologist.
Some practices create incentives for physicians by offering a variety of bonuses. Most often these bonuses are production based but sometimes they are based on such quality issues as patient satisfaction. The most common types of production bonuses are based on attaining a level of collections above a dollar threshold or exceeding a minimum level of relative value units (RVUs).
To summarize, new physicians should always try to get at least a 2-year income guarantee. They should never allow an employer to allocate overhead to them during the first 2 years of employment. In addition, they should always try to negotiate realistic production-based bonuses.
Benefits
Fringe benefits are an integral part of a compensation package for a new physician. Most physician employers offer a generous package of health insurance, retirement, reimbursable expenses, and paid time off. These benefits should be clearly delineated in the employment agreement or employee handbook. A very common question about health benefits is when they become effective (the first day of employment, 30 days after employment, the first of the month after employment, etc.). This is significant because Consolidated Omnibus Budget Reconciliation Act (COBRA) is quite expensive. Another issue is whether health insurance also will cover the physician’s spouse and dependents. Most physician employers cover only the physician, not his/her spouse and dependents. If a new physician has a spouse who already provides family health benefits, it may behoove the physician to negotiate an allowance in lieu of health benefits.
Paid time off of 10-20 days are commonly given by physician employers to new physicians. Some employers also provide 5 or more additional days of paid time off for Continuing Medical Education (CME). Of course, once a physician goes onto production-based compensation, paid time off usually is not provided.
It is very important that a physician employer offer a retirement plan. Oftentimes, there is a matching contribution by the employer. However, it is not uncommon for there to be a year waiting period for eligibility in the retirement plan. Retirement plans vary significantly so it is advisable for a new physician to meet with the employer’s human resources department to get the details of the plan offered; the physician may want to confer with a financial advisor after obtaining this information.
Most physician employers reimburse licensing and DEA fees, medical staff dues, and board certification expenses. There is often a CME allowance as well. In competitive markets, some physician employers also offer innovative benefits such as student loan repayment programs, fellowship and residency stipends, and forgivable loans for housing. Sometimes these benefits are not included in the employment agreement; you may have to ask for them.
Indemnification/noncompetition
In addition to compensation and benefits, there are several other issues which are commonly found in employment agreements. Perhaps the most controversial is the issue of indemnification. The legal concept of indemnity allows a physician employer to recover damages and defense costs from a physician employee in certain circumstances. For example, if a physician employer has a $1,000,000/$3,000,000 malpractice policy covering itself and each of its physician employees, and if a physician commits malpractice and the award is $2,000,000, the employer may seek to recover the $1,000,000 deficit from the physician. In California, for example, the physician employer would be prohibited from seeking the deficit from the physician employee, but in most states, it is permitted. Because insurance policies usually do not cover physicians for damages, expenses, costs, etc as a result of an indemnification action, there is no practical way for a physician to protect himself/herself from the consequences. It is very important that physicians not sign any type of agreement with an indemnification clause in it without consulting an attorney first.
Another controversial issue is noncompete restrictions. In many states, a physician employer can restrict a physician employee from competing with it after an employment agreement is terminated. The noncompete prohibitions usually last for 1-2 years and extend over a geographic area, which often causes a terminated physician to relocate. Importantly, noncompete clauses are generally enforceable in most states.
Tail coverage
Malpractice tail coverage often can be an issue as well. For many years, physician employers routinely paid the cost of tail coverage for a physician employee after termination of employment. Tail coverage is necessary because most malpractice policies are claims-made insurance instead of occurrence insurance. This means that the insurance is applicable when a claim is filed versus when a malpractice act or omission occurred. Because of the significant cost of tail coverage, many physician employers attempt to transfer this financial responsibility to physician employees. Depending on a physician’s specialty, tail coverage can be quite costly. Consequently, it behooves physicians to carefully negotiate this issue. If a physician employer is unwilling to provide tail coverage, a compromise may be proposed whereby the physician employee is responsible only for the cost of tail coverage if he/she terminates the employment agreement without cause or if the physician employer terminates the employment agreement for cause. Conversely, the physician employer would be responsible for the cost if the physician employer terminates the employment agreement without cause or the physician employee terminates the employment agreement for cause.
Equity accrual
Finally, new physicians always should ask whether there is an opportunity to obtain equity in the organizations that hire them. Many for-profit physician employers provide such an opportunity to new physicians after 2-3 years. However, timing is just one factor. Importantly, the cost of the buy-in is critical especially to new physicians with student loans. Recognizing this problem, the trend today is for physician employers to have nominal buy-ins. Notwithstanding this trend, some physician employers also own ambulatory surgery centers and the buy-ins for these entities must be at fair market value and cannot be financed by the center or its owners under the law. Consequently, the buy-in for ambulatory surgery centers is usually substantial and requires a physician to obtain outside financing.
In conclusion, when evaluating the viability of a physician employment opportunity, salary should be only one factor considered. Fringe benefits, the opportunity for equity, and the fairness of the employment agreement also should be weighed heavily by a physician. It is important for a physician to be comfortable with his/her peers and work environment. Selecting the right job opportunity can be challenging. However, the process will be much easier if you remember the basic principles of negotiating.
You have finally completed your residency or fellowship, and now you have a job offer. With some trepidation, you decide to read the employment agreement that has been emailed to you. You quickly realize that you do not understand much of it. All those legal terms! You lament the fact that medical school never taught you about the business of medicine. What are you going to do? The choices are actually quite simple: You can take the time to educate yourself or you can hire an expert. This article will review some of the basic principles of negotiating as well as some of the critical issues found in physician employment agreements today.
Whether you represent yourself or hire someone to do it for you, it is important to understand some of the basic principles of negotiating. These principles generally are applicable whether you are buying a house or negotiating your employment agreement.
Negotiations
The most important principle is preparation. For example, many physicians negotiate their salaries during the interview process. Consequently, it is imperative that, before you negotiate your compensation, you know the range of salaries in your area for your specialty. It is also important to know whether salaries are usually guaranteed in your market, or whether production-based salaries (which are based on the amount of your billings) are the norm. Never go into an interview unprepared!
Always try to gain leverage in your negotiations. The easiest way to accomplish this is by having multiple offers, and subtly letting your suitors know this. Allow adequate time to negotiate; the more time you have, the easier it is to negotiate. Establish your objectives and try to anticipate the objectives of the other party. Determine your best-case and worse-case scenarios, as well as the most likely outcome. Do not negotiate against yourself and try to get something every time you give something. Define the nonnegotiable issues, and do not waste time on them. Keep cool and be flexible.
The first question you must answer when you receive an employment agreement is who is going to negotiate it. Many new physicians hire attorneys to help them with their employment agreements and employers expect as much. It is best to engage an attorney before you begin your job search so you can get a better understanding of how the attorney can help you. Most attorneys do not charge a prospective client for such information. However, many physicians wait until they actually receive an offer before contacting an attorney. It is not uncommon for physicians to negotiate their salaries during job interviews even if they eventually hire an attorney to help them. This is usually attributable to a lack of negotiating experience and an eagerness to determine whether a job offer is viable. Keep in mind that an attorney often can negotiate a better starting salary than you, so try to resist the temptation to negotiate your salary during the interview process.
Compensation
With compensation in mind, what are some of the important issues? Today, many physician employers are converting to production-based compensation models. Consequently, it is important for new physicians to obtain guaranteed base salaries during their first few years of employment while they are building their practices.
On occasion, new physicians initially are offered production-based compensation models, which also allocate a share of practice overhead expenses to them. This is a very dangerous compensation model for a new physician. Under such a model, it is possible that a new physician could have a negative balance in his/her cost center at the end of the year, and actually owe his/her employer money.
Some physicians may be offered income guarantees by hospitals. There are several different types of income guarantees but they are frequently categorized together even though they differ significantly. The most common income guarantees offered to physicians are physician recruitment agreements (PRAs). Under a PRA, a hospital usually guarantees that a physician who relocates to the service area of the hospital collects a minimum amount of monthly revenue for 1-2 years, which is known as the guarantee period. The hospital also guarantees to pay certain monthly expenses of the physician during the guarantee period. This arrangement is actually structured as a loan by the hospital to the physician, and requires the physician to execute a promissory note with the hospital for the amounts advanced to the physician by the hospital. The promissory note is forgiven if the physician continues to practice in the service area for 2-3 years after the guarantee period. This type of guarantee provides an excellent opportunity for a new physician to establish a solo practice. A variation of this model involves a third party such as a medical group. Under this model, the hospital continues to guarantee the revenue of the new physician and pays the medical group the expenses it incurs as a result of hiring the new physician. These expenses are known as incremental practice expenses. The medical group also becomes a signatory to the promissory note. Other health care entities also have begun to offer PRAs to physicians. For example, an independent practice association in California recently entered into a PRA with a gastroenterologist.
Keep in mind that the promissory note executed by the physician may affect the credit of the physician, especially if he/she wants to obtain financing for a home purchase. Also, a hospital may seek security for the performance of the promissory note by collateralizing the personal assets of the physician instead of just his/her practice assets; this should be avoided.
The other type of income guarantee is provided to hospital-based physicians such as pathologists, radiologists, anesthesiologists, etc. Under this type of guarantee, a hospital ensures that the physicians receive a minimum threshold of collections. This type of guarantee may be necessary to attract hospital-based physicians to a hospital which has a low-income and/or Medicaid population. This is not a typical scenario for a gastroenterologist.
Some practices create incentives for physicians by offering a variety of bonuses. Most often these bonuses are production based but sometimes they are based on such quality issues as patient satisfaction. The most common types of production bonuses are based on attaining a level of collections above a dollar threshold or exceeding a minimum level of relative value units (RVUs).
To summarize, new physicians should always try to get at least a 2-year income guarantee. They should never allow an employer to allocate overhead to them during the first 2 years of employment. In addition, they should always try to negotiate realistic production-based bonuses.
Benefits
Fringe benefits are an integral part of a compensation package for a new physician. Most physician employers offer a generous package of health insurance, retirement, reimbursable expenses, and paid time off. These benefits should be clearly delineated in the employment agreement or employee handbook. A very common question about health benefits is when they become effective (the first day of employment, 30 days after employment, the first of the month after employment, etc.). This is significant because Consolidated Omnibus Budget Reconciliation Act (COBRA) is quite expensive. Another issue is whether health insurance also will cover the physician’s spouse and dependents. Most physician employers cover only the physician, not his/her spouse and dependents. If a new physician has a spouse who already provides family health benefits, it may behoove the physician to negotiate an allowance in lieu of health benefits.
Paid time off of 10-20 days are commonly given by physician employers to new physicians. Some employers also provide 5 or more additional days of paid time off for Continuing Medical Education (CME). Of course, once a physician goes onto production-based compensation, paid time off usually is not provided.
It is very important that a physician employer offer a retirement plan. Oftentimes, there is a matching contribution by the employer. However, it is not uncommon for there to be a year waiting period for eligibility in the retirement plan. Retirement plans vary significantly so it is advisable for a new physician to meet with the employer’s human resources department to get the details of the plan offered; the physician may want to confer with a financial advisor after obtaining this information.
Most physician employers reimburse licensing and DEA fees, medical staff dues, and board certification expenses. There is often a CME allowance as well. In competitive markets, some physician employers also offer innovative benefits such as student loan repayment programs, fellowship and residency stipends, and forgivable loans for housing. Sometimes these benefits are not included in the employment agreement; you may have to ask for them.
Indemnification/noncompetition
In addition to compensation and benefits, there are several other issues which are commonly found in employment agreements. Perhaps the most controversial is the issue of indemnification. The legal concept of indemnity allows a physician employer to recover damages and defense costs from a physician employee in certain circumstances. For example, if a physician employer has a $1,000,000/$3,000,000 malpractice policy covering itself and each of its physician employees, and if a physician commits malpractice and the award is $2,000,000, the employer may seek to recover the $1,000,000 deficit from the physician. In California, for example, the physician employer would be prohibited from seeking the deficit from the physician employee, but in most states, it is permitted. Because insurance policies usually do not cover physicians for damages, expenses, costs, etc as a result of an indemnification action, there is no practical way for a physician to protect himself/herself from the consequences. It is very important that physicians not sign any type of agreement with an indemnification clause in it without consulting an attorney first.
Another controversial issue is noncompete restrictions. In many states, a physician employer can restrict a physician employee from competing with it after an employment agreement is terminated. The noncompete prohibitions usually last for 1-2 years and extend over a geographic area, which often causes a terminated physician to relocate. Importantly, noncompete clauses are generally enforceable in most states.
Tail coverage
Malpractice tail coverage often can be an issue as well. For many years, physician employers routinely paid the cost of tail coverage for a physician employee after termination of employment. Tail coverage is necessary because most malpractice policies are claims-made insurance instead of occurrence insurance. This means that the insurance is applicable when a claim is filed versus when a malpractice act or omission occurred. Because of the significant cost of tail coverage, many physician employers attempt to transfer this financial responsibility to physician employees. Depending on a physician’s specialty, tail coverage can be quite costly. Consequently, it behooves physicians to carefully negotiate this issue. If a physician employer is unwilling to provide tail coverage, a compromise may be proposed whereby the physician employee is responsible only for the cost of tail coverage if he/she terminates the employment agreement without cause or if the physician employer terminates the employment agreement for cause. Conversely, the physician employer would be responsible for the cost if the physician employer terminates the employment agreement without cause or the physician employee terminates the employment agreement for cause.
Equity accrual
Finally, new physicians always should ask whether there is an opportunity to obtain equity in the organizations that hire them. Many for-profit physician employers provide such an opportunity to new physicians after 2-3 years. However, timing is just one factor. Importantly, the cost of the buy-in is critical especially to new physicians with student loans. Recognizing this problem, the trend today is for physician employers to have nominal buy-ins. Notwithstanding this trend, some physician employers also own ambulatory surgery centers and the buy-ins for these entities must be at fair market value and cannot be financed by the center or its owners under the law. Consequently, the buy-in for ambulatory surgery centers is usually substantial and requires a physician to obtain outside financing.
In conclusion, when evaluating the viability of a physician employment opportunity, salary should be only one factor considered. Fringe benefits, the opportunity for equity, and the fairness of the employment agreement also should be weighed heavily by a physician. It is important for a physician to be comfortable with his/her peers and work environment. Selecting the right job opportunity can be challenging. However, the process will be much easier if you remember the basic principles of negotiating.
Fluoroquinolones can cause fatal hypoglycemia, FDA warns
Fluoroquinolones have caused at least 67 cases of life-threatening hypoglycemic coma, including 13 deaths and 9 permanent and disabling injuries, according to an internal safety review by the Food and Drug Administration. Most cases (44) were associated with levofloxacin.

The review also found new neuropsychiatric side effects associated with fluoroquinolones, including disturbances in attention, memory impairment, and delirium.
Considering these findings, the agency will strengthen warning labels on all fluoroquinolones, which already warn that the antibiotics may cause hypoglycemia and mental health issues, especially in older people, the FDA said in a press statement.
“Health care professionals should be aware of the potential risk of hypoglycemia, sometimes resulting in coma, occurring more frequently in the elderly and those with diabetes taking an oral hypoglycemic medicine or insulin,” the statement said. “Alert patients of the symptoms of hypoglycemia and carefully monitor blood glucose levels in these patients and discuss with them how to treat themselves if they have symptoms of hypoglycemia. Inform patients about the risk of psychiatric adverse reactions that can occur after just one dose. Stop fluoroquinolone treatment immediately if a patient reports any central nervous system side effects, including psychiatric adverse reactions, or blood glucose disturbances and switch to a non–fluoroquinolone antibiotic if possible. Stop fluoroquinolone treatment immediately if a patient reports serious side effects involving the tendons, muscles, joints, or nerves, and switch to a non–fluoroquinolone antibiotic to complete the patient’s treatment course.”
The statement also warned not to prescribe fluoroquinolones to patients who have other treatment options for acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections because the risks outweigh the benefits in these patients.
The FDA conducted the postmarketing review on all five of the fluoroquinolones (ciprofloxacin, gemifloxacin, levofloxacin, moxifloxacin, and ofloxacin). The newest fluoroquinolone, delafloxacin, approved a year ago, was not included in the class review. However, the agency expects that similar adverse events will be associated with delafloxacin and labeling on that drug will include the new warnings.
The agency reviewed cases in the FDA Adverse Event Reporting System, and in published medical literature, during 1987-2017. Most of the incidents (56) were in the system; 11 additional cases were published. Levofloxacin caused most of the incidents (44), followed by ciprofloxacin (12), moxifloxacin (9), and ofloxacin (2). Four of the fluoroquinolones have a labeled drug interaction with sulfonylurea agents, which can cause hypoglycemia.
Some of those who died were getting the antibiotics for complicated infections, including urinary tract and upper respiratory tract infections, and postoperative antibiotic prophylaxis. Others had renal insufficiency – a risk factor for hypoglycemia.
Of the 54 patients who survived, 9 never fully recovered and had permanent disabilities. Four patients remained in a coma for at least 1 month, despite blood sugar normalization. Five experienced some type of neurologic injury.
The new label changes will also fortify the existing warning about mental health side effects, after the review found new reactions that are not listed in the current warning, including the new reports of disturbance in attention, memory impairment, and delirium.
The FDA statement did not include the number of cases found or the associated drugs. Again, the safety review was based on reports in the FAERS database and published medical literature.
“We found that psychiatric adverse reactions were not consistent in the drug labels. The labels of fluoroquinolones currently include many psychiatric adverse reactions in the Warnings and Precautions section, for example, hallucination, psychoses, confusion, depression, anxiety, and paranoia. In an effort to harmonize the psychiatric adverse reactions described in the drug labels across the class of fluoroquinolones, we are requiring that all fluoroquinolones include six psychiatric adverse reactions (disturbance in attention, memory impairment, delirium, nervousness, agitation, and disorientation) in the Central Nervous System Effects of the Warnings and Precautions section of the labels. Disturbance in attention, memory impairment, and delirium are new adverse reactions to be added to the labels of the entire class of fluoroquinolones. Nervousness, agitation, and disorientation had been previously listed in the fluoroquinolone drug labels and will now be added to the Warnings and Precautions section of each drug label to harmonize labels across the fluoroquinolone drug class. The new label changes will make the psychiatric adverse reactions more prominent and more consistent.”
The FDA has previously warned about other adverse events associated with fluoroquinolones in May 2016, restricting use for certain uncomplicated infections; July 2016, for disabling side effects; August 2013, for peripheral neuropathy, and July 2008, for tendinitis and tendon rupture.
Fluoroquinolones have caused at least 67 cases of life-threatening hypoglycemic coma, including 13 deaths and 9 permanent and disabling injuries, according to an internal safety review by the Food and Drug Administration. Most cases (44) were associated with levofloxacin.
The review also found new neuropsychiatric side effects associated with fluoroquinolones, including disturbances in attention, memory impairment, and delirium.
Considering these findings, the agency will strengthen warning labels on all fluoroquinolones, which already warn that the antibiotics may cause hypoglycemia and mental health issues, especially in older people, the FDA said in a press statement.
“Health care professionals should be aware of the potential risk of hypoglycemia, sometimes resulting in coma, occurring more frequently in the elderly and those with diabetes taking an oral hypoglycemic medicine or insulin,” the statement said. “Alert patients of the symptoms of hypoglycemia and carefully monitor blood glucose levels in these patients and discuss with them how to treat themselves if they have symptoms of hypoglycemia. Inform patients about the risk of psychiatric adverse reactions that can occur after just one dose. Stop fluoroquinolone treatment immediately if a patient reports any central nervous system side effects, including psychiatric adverse reactions, or blood glucose disturbances and switch to a non–fluoroquinolone antibiotic if possible. Stop fluoroquinolone treatment immediately if a patient reports serious side effects involving the tendons, muscles, joints, or nerves, and switch to a non–fluoroquinolone antibiotic to complete the patient’s treatment course.”
The statement also warned not to prescribe fluoroquinolones to patients who have other treatment options for acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections because the risks outweigh the benefits in these patients.
The FDA conducted the postmarketing review on all five of the fluoroquinolones (ciprofloxacin, gemifloxacin, levofloxacin, moxifloxacin, and ofloxacin). The newest fluoroquinolone, delafloxacin, approved a year ago, was not included in the class review. However, the agency expects that similar adverse events will be associated with delafloxacin and labeling on that drug will include the new warnings.
The agency reviewed cases in the FDA Adverse Event Reporting System, and in published medical literature, during 1987-2017. Most of the incidents (56) were in the system; 11 additional cases were published. Levofloxacin caused most of the incidents (44), followed by ciprofloxacin (12), moxifloxacin (9), and ofloxacin (2). Four of the fluoroquinolones have a labeled drug interaction with sulfonylurea agents, which can cause hypoglycemia.
Some of those who died were getting the antibiotics for complicated infections, including urinary tract and upper respiratory tract infections, and postoperative antibiotic prophylaxis. Others had renal insufficiency – a risk factor for hypoglycemia.
Of the 54 patients who survived, 9 never fully recovered and had permanent disabilities. Four patients remained in a coma for at least 1 month, despite blood sugar normalization. Five experienced some type of neurologic injury.
The new label changes will also fortify the existing warning about mental health side effects, after the review found new reactions that are not listed in the current warning, including the new reports of disturbance in attention, memory impairment, and delirium.
The FDA statement did not include the number of cases found or the associated drugs. Again, the safety review was based on reports in the FAERS database and published medical literature.
“We found that psychiatric adverse reactions were not consistent in the drug labels. The labels of fluoroquinolones currently include many psychiatric adverse reactions in the Warnings and Precautions section, for example, hallucination, psychoses, confusion, depression, anxiety, and paranoia. In an effort to harmonize the psychiatric adverse reactions described in the drug labels across the class of fluoroquinolones, we are requiring that all fluoroquinolones include six psychiatric adverse reactions (disturbance in attention, memory impairment, delirium, nervousness, agitation, and disorientation) in the Central Nervous System Effects of the Warnings and Precautions section of the labels. Disturbance in attention, memory impairment, and delirium are new adverse reactions to be added to the labels of the entire class of fluoroquinolones. Nervousness, agitation, and disorientation had been previously listed in the fluoroquinolone drug labels and will now be added to the Warnings and Precautions section of each drug label to harmonize labels across the fluoroquinolone drug class. The new label changes will make the psychiatric adverse reactions more prominent and more consistent.”
The FDA has previously warned about other adverse events associated with fluoroquinolones in May 2016, restricting use for certain uncomplicated infections; July 2016, for disabling side effects; August 2013, for peripheral neuropathy, and July 2008, for tendinitis and tendon rupture.
Fluoroquinolones have caused at least 67 cases of life-threatening hypoglycemic coma, including 13 deaths and 9 permanent and disabling injuries, according to an internal safety review by the Food and Drug Administration. Most cases (44) were associated with levofloxacin.
The review also found new neuropsychiatric side effects associated with fluoroquinolones, including disturbances in attention, memory impairment, and delirium.
Considering these findings, the agency will strengthen warning labels on all fluoroquinolones, which already warn that the antibiotics may cause hypoglycemia and mental health issues, especially in older people, the FDA said in a press statement.
“Health care professionals should be aware of the potential risk of hypoglycemia, sometimes resulting in coma, occurring more frequently in the elderly and those with diabetes taking an oral hypoglycemic medicine or insulin,” the statement said. “Alert patients of the symptoms of hypoglycemia and carefully monitor blood glucose levels in these patients and discuss with them how to treat themselves if they have symptoms of hypoglycemia. Inform patients about the risk of psychiatric adverse reactions that can occur after just one dose. Stop fluoroquinolone treatment immediately if a patient reports any central nervous system side effects, including psychiatric adverse reactions, or blood glucose disturbances and switch to a non–fluoroquinolone antibiotic if possible. Stop fluoroquinolone treatment immediately if a patient reports serious side effects involving the tendons, muscles, joints, or nerves, and switch to a non–fluoroquinolone antibiotic to complete the patient’s treatment course.”
The statement also warned not to prescribe fluoroquinolones to patients who have other treatment options for acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections because the risks outweigh the benefits in these patients.
The FDA conducted the postmarketing review on all five of the fluoroquinolones (ciprofloxacin, gemifloxacin, levofloxacin, moxifloxacin, and ofloxacin). The newest fluoroquinolone, delafloxacin, approved a year ago, was not included in the class review. However, the agency expects that similar adverse events will be associated with delafloxacin and labeling on that drug will include the new warnings.
The agency reviewed cases in the FDA Adverse Event Reporting System, and in published medical literature, during 1987-2017. Most of the incidents (56) were in the system; 11 additional cases were published. Levofloxacin caused most of the incidents (44), followed by ciprofloxacin (12), moxifloxacin (9), and ofloxacin (2). Four of the fluoroquinolones have a labeled drug interaction with sulfonylurea agents, which can cause hypoglycemia.
Some of those who died were getting the antibiotics for complicated infections, including urinary tract and upper respiratory tract infections, and postoperative antibiotic prophylaxis. Others had renal insufficiency – a risk factor for hypoglycemia.
Of the 54 patients who survived, 9 never fully recovered and had permanent disabilities. Four patients remained in a coma for at least 1 month, despite blood sugar normalization. Five experienced some type of neurologic injury.
The new label changes will also fortify the existing warning about mental health side effects, after the review found new reactions that are not listed in the current warning, including the new reports of disturbance in attention, memory impairment, and delirium.
The FDA statement did not include the number of cases found or the associated drugs. Again, the safety review was based on reports in the FAERS database and published medical literature.
“We found that psychiatric adverse reactions were not consistent in the drug labels. The labels of fluoroquinolones currently include many psychiatric adverse reactions in the Warnings and Precautions section, for example, hallucination, psychoses, confusion, depression, anxiety, and paranoia. In an effort to harmonize the psychiatric adverse reactions described in the drug labels across the class of fluoroquinolones, we are requiring that all fluoroquinolones include six psychiatric adverse reactions (disturbance in attention, memory impairment, delirium, nervousness, agitation, and disorientation) in the Central Nervous System Effects of the Warnings and Precautions section of the labels. Disturbance in attention, memory impairment, and delirium are new adverse reactions to be added to the labels of the entire class of fluoroquinolones. Nervousness, agitation, and disorientation had been previously listed in the fluoroquinolone drug labels and will now be added to the Warnings and Precautions section of each drug label to harmonize labels across the fluoroquinolone drug class. The new label changes will make the psychiatric adverse reactions more prominent and more consistent.”
The FDA has previously warned about other adverse events associated with fluoroquinolones in May 2016, restricting use for certain uncomplicated infections; July 2016, for disabling side effects; August 2013, for peripheral neuropathy, and July 2008, for tendinitis and tendon rupture.
Status Epilepticus in the Emergency Department, Part 2: Treatment
In part 1 of this 2-part review, the authors detailed proper diagnosis of seizures in the ED setting. In this concluding article, they focus on appropriate management and treatment options for patients with seizure.
Status epilepticus is defined as continuous seizure activity for greater than 5 minutes, or repeated episodes of seizures without resolution of the postictal period. When the clinician arrives at the patient’s bedside or the emergency medical technician arrives at the scene in the prehospital setting, the patient may be minutes into seizure activity. If the seizure does not immediately resolve, the provider should treat as if status is imminent, if not ongoing. Regardless of setting, if the patient is discovered to be seizing, treatment should be initiated.
It is important to distinguish between provoked and unprovoked seizures, since successful management may require treating an underlying etiology. Although there are as many types of status epilepticus as there are types of seizures, the focus of this review is on generalized convulsive status epilepticus (GCSE).
As a GCSE continues, the overt seizure activity may become subtle—essentially a transformation of generalized status to a state with minimal or no motor movements. Whether or not there is an absence of, or minimal, movement, GCSE still represents a medical emergency, since the excessive neuronal activity causes neuronal injury. An electroencephalogram (EEG) may be required to detect transformed GCSE, which should be suspected if the patient does not exhibit improved mental status within 20 to 30 minutes of convulsive seizure cessation, or if neuromuscular paralysis for intubation has occurred.
Initial Management
Initial management of seizure patients is consistent with the care of any critical patient in the ED. Assessment of the airway and airway management with endotracheal intubation may be necessary for patients who are apneic or at risk for aspiration, or in whom more conservative management is inadequate.
While placing a patient in the left lateral decubitus position may mitigate aspiration risk, since vomiting is common in a postictal state, moving a convulsing patient may be challenging.1 Patients should be placed on cardiac monitoring with pulse oximetry if feasible. Intravenous (IV) access should be established if possible, though intramuscular (IM) or other alternative routes for benzodiazepines may be used if obtaining IV access will result in a delay in treatment.2
Oxygen should be administered via nonrebreather or bag-valve-mask to patients with apnea to prevent both systemic and cerebral hypoxia.3Since cardiac dysrhythmias with cerebral hypoxia may cause seizure-like activity, it is imperative to check the patient’s pulses, blood pressure, and to maintain cardiac monitoring during convulsive episodes.4 The patient’s glucose levels should be checked upon arrival to determine if the seizure is due to metabolic disturbance, which is an easily reversible cause of seizure. If glucose point-of-care testing is not available, it is reasonable to treat empirically for hypoglycemia.
Emergent Initial Therapy: First-Line Agents
Benzodiazepines
Benzodiazepines are the mainstay of emergent treatment for status epilepticus. The choice of benzodiazepine may be dependent on the clinical setting and availability of IV access or other resources. In the United States, diazepam, lorazepam, and midazolam are the common formulations used for abortive emergent initial therapy.
Diazepam. One of the advantages of diazepam is that it is has the advantage of being water soluble at room temperature, which allows rectal rescue kits for home treatment. Although diazepam is efficacious for status epilepticus, variable pharmacokinetics leading to repeat dosing and further sedation make other benzodiazepines safer.
Lorazepam. Generally accepted as the preferred IV formulation for seizure, lorazepam requires refrigeration and has a short shelf life, making its use challenging in the prehospital setting. When administered via the IV route, lorazepam works as rapidly as diazepam in treating seizures but with a longer duration of effectiveness, resulting in a decreased need to re-dose or administer an alternative antiepileptic drug (AED).5
Midazolam. Newer studies suggest that buccal, intranasal, and IM midazolam may be superior to buccal, intranasal, and IM diazepam in treating GCSE.6 The Rapid Anticonvulsant Medication Prior to Arrival Trial demonstrated IM midazolam to be at least as efficacious as IV lorazepam in the prehospital setting for treating GCSE.2
Efficacy, Route, and Dosing
A meta-analysis of all three benzodiazepines in pediatric patients with seizure showed midazolam to have the highest probability of aborting seizure activity, while lorazepam had the least likelihood of causing respiratory depression.7The authors concluded that IV lorazepam and non-IV midazolam were superior to IV and non-IV diazepam in the treatment of pediatric seizures.7
A recent retrospective study that analyzed benzodiazepine use in the emergency setting noted underdosing of benzodiazepines in the ED for nonprotocol-driven treatment of status epilepticus, resulting in the increased potential for adverse outcomes and intubations.8 Table 1 provides benzodiazepine dosing recommendations by route for adult and pediatric patients, along with potential adverse effects.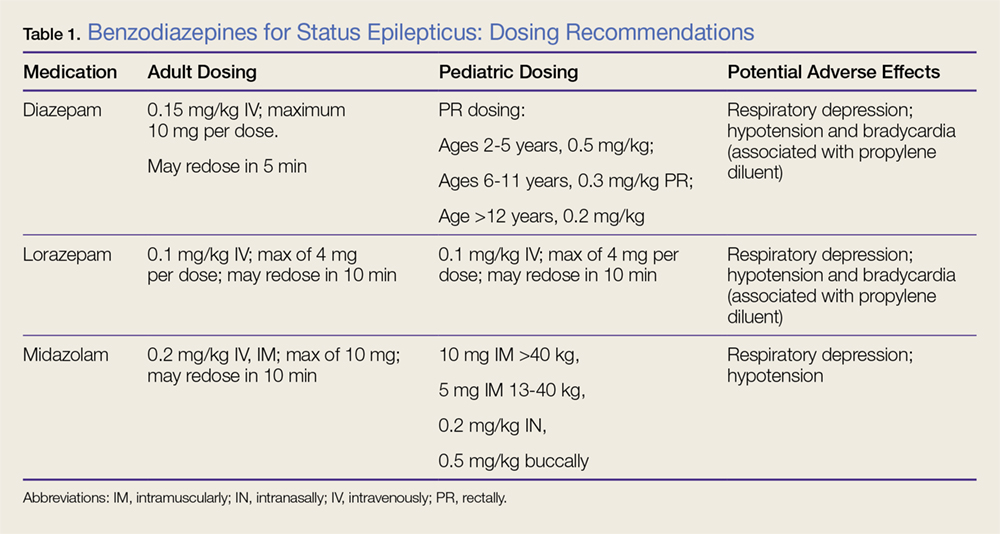
Adverse Effects
As noted previously, benzodiazepines can cause respiratory depression. Anecdotally, respiratory depression is often related to the rate at which the benzodiazepine is administered. For example, most treatment recommendations advise giving IV lorazepam over a 2-minute time period—not as an IV push.7
With respect to other adverse effects, it is important to note that IV formulations of diazepam and lorazepam contain propylene glycol as a diluent, which may lead to hypotension and bradycardia, especially when large volumes are infused over short periods of time.9
Second-Line Agents
While emergent initial therapy with benzodiazepines is well established, the preferred second-line agent, or urgent control therapy, continues to be a subject of controversy due to a lack of conclusive evidence for a superior agent.10 The Established Status Epilepticus Treatment Trial (ESETT) is currently conducting a head-to-head study to determine if any of the commonly used second-line agents (ie, fosphenytoin, levetiracetam, valproic acid) will prove to be more efficacious.11 Recently, the adult arm of the ESETT trial was halted due to futility.
All patients without an identifiable secondary cause of GCSE (eg, hypoglycemia, hyponatremia, hypocalcemia) should be started on a second-line agent. Treatment with a second-line agent provides two benefits: First, patients who experience resolution of seizure activity may rapidly attain therapeutic levels of AEDs, which may be sustained through maintenance therapy; and second, the second-line treatment may abort refractory cases of status.12 Table 2 provides dosing recommendations for second-line agents.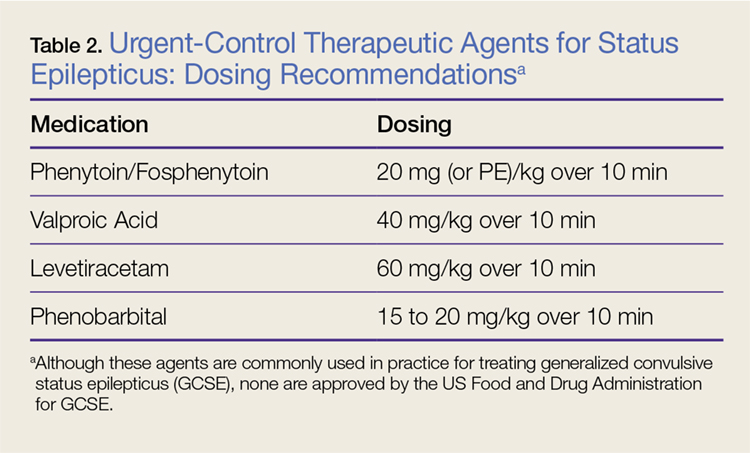
Phenytoin and Fosphenytoin
Phenytoin and the newer prodrug fosphenytoin are a mainstay urgent-control therapy for emergency physicians (EPs) and neurologists alike. In one of the few head-to-head studies of AEDs,13 phenytoin did not perform as well as the other study agents (diazepam, lorazepam, and phenobarbital); however, generalizability from this study is limited. Fosphenytoin continues to be an efficacious choice for second-line treatment of AED.
Fosphenytoin, a water-soluble prodrug of phenytoin, is given preferentially over IV phenytoin due to its decreased risk of cardiovascular (CV) side effects and more rapid administration.14 Moreover, fosphenytoin is compatible with most IV fluids (eg, dextrose, lactated Ringer’s solution, normal saline [NS]), whereas phenytoin is only compatible with NS. For convenience, fosphenytoin is dosed in phenytoin equivalents (PE/kg)—eg, administration of 20 PE/kg over 10 minutes is a potential loading dose for fosphenytoin.
Valproic Acid
Valproic acid has become a favored second-line agent for many providers due to its relatively safe profile and rapid infusion time. Most studies have shown IV valproic acid is at least as effective as phenytoin, but data continue to be somewhat weak and most of the studies are uncontrolled.15
Hepatotoxicity is generally only associated with long-term use of valproic acid, but it remains reasonable to abstain from using this agent in patients with preexisting hepatic disease. Valproic acid toxicity can lead to somnolence, ataxia, seizures, and coma with marked hyperammonemia.16
Levetiracetam
Intravenous levetiracetam is becoming a more commonly used drug both for emergent initial treatment of seizure and as a maintenance therapy. While data on levetiracetam are limited, a few studies tout the efficacy and safety of IV loading to abort GCSE.
In observational studies, levetiracetam appears to have similar efficacy to other AEDs and may be more beneficial in early therapy.17 An ongoing current study, The Emergency Treatment With Levetiracetam or Phenytoin in Status Epilepticus trial, is examining a prospective cohort of pediatric patients comparing levetiracetam against phenytoin.18
Levetiracetam is generally considered safe. The most commonly reported side effects are dizziness, somnolence, nausea, and brief transaminitis.19 Levetiracetam has also been associated with neuropsychiatric exacerbations.20
Phenobarbital
Intravenous phenobarbital has been used as an urgent-control therapy for seizure with good efficacy, even in recent years.21 Despite this, phenobarbital may cause profound CV depression necessitating the use of vasopressors.22 Large-dose phenobarbital can be used to induce coma in patients, although this should not be attempted without the guidance of a neurologist. While phenobarbital can be used safely in certain circumstances, its use has fallen out of favor in the ED due to the availability of safer alternative options.
Refractory Status Epilepticus
If after receiving two AEDs, a patient continues to demonstrate seizure activity on physical examination or EEG, she or he is considered to have refractory status epilepticus, which is a medical emergency. Patients in refractory status epilepticus will likely require a continuous infusion of an AED as well as definitive airway management as a result of either seizure or continuous treatment. In rare cases, some patients will continue to seize despite continuous treatment. Such patients are considered to have super refractory status epilepticus, which is defined as continuing seizure activity despite treatment with general anesthetics for more than 24 hours. This condition is beyond the scope of traditional EP practice, who in this scenario would consult emergently with neurology or critical care services.
Propofol
Propofol, a sedative-hypnotic agent that activates both γ-aminobutyric acid and N-methyl-D-aspartate receptors, is commonly given to patients with refractory status epilepticus. While head-to-head reviews have not shown propofol to be superior to phenobarbital or midazolam in treating refractory seizure, it is a drug that is familiar to most EPs.23 Midazolam or propofol are typically given to patients in the ED who require intubation with sedation.
With respect to side effects, propofol can cause dose-limiting hypotension. In addition, propofol infusion syndrome leading to lactic acidosis and cardiac dysfunction in patients receiving long-term propofol infusion.24 One possible infusion dose is 0.5-1 mg/kg loading dose with a continuous infusion of 2 mg/kg/h IV.
High-Dose Midazolam
High-dose midazolam may be given as an alternative to propofol as some studies have shown its efficacy in treating refractory status epilepticus.25 Continuous low-dose infusions of midazolam (0.2 mg/kg/h) have been given to patients in the neurological intensive care unit (ICU); however, there are some data to support treating with a higher dose (≥0.4 mg/kg/h).25 In one single-center retrospective trial, post discharge all-cause mortality was lower in the cohort group that received the higher dose infusion (40% vs 62%).25 Although higher rates of hypotension were noted in the high-dose group, it did not appear to affect mortality.
Ketamine
Ketamine has become a valued anesthetic in emergency medicine, and EPs have become comfortable with its dosing and safety profile. While animal studies on ketamine are promising to treat status epilepticus, human data are limited and often extrapolated from retrospective ICU data. Many patients are placed on a ketamine infusion multiple days into status epilepticus, and for this reason, ketamine is not recommended as a second-line abortive drug in the ED.26
Alternative Treatments and Super Refractory GCSE
In cases of patients with seizure activity ongoing beyond conventional therapy, other methods have been attempted to cease seizure activity and achieve burst suppression on EEG. None of these treatments is in the purview of the EP and should only be undertaken by a neurologist.
Two pharmacologic agents that have some limited efficacy include lacosamide and topiramate. Isoflurane is the most commonly used inhaled anesthetic.27 Thiopental and pentobarbital are barbiturate anesthetics which are used in super refractory GCSE. Barbiturates have a desirable theoretical neuroprotective effect, but are limited by their CV depression at high doses.28 Vagus nerve stimulation, induced hypothermia, transcranial magnetic stimulation, and neurosurgical intervention have all been attempted with varying degrees of success in select patients.29
Eclampsia and Seizures During Pregnancy
Treating a pregnant patient with status epilepticus presents a unique challenge in the ED. The EP must weigh the importance of aborting seizure activity with the possibility of teratogenic effects. All AEDs must be used carefully, but valproic acid and phenytoin are potent teratogens and should be avoided in this patient population. Most evidence points to safety with exposure to benzodiazepines during pregnancy.30 Eclampsia must be considered in patients who may be pregnant or recently pregnant; magnesium should be used with or without the use of benzodiazepines in these patients.
Summary
The diagnosis and treatment of status epilepticus in the ED can be challenging. While there is a multitude of first-, second-, and third-line agents available to treat this condition, choosing the correct therapy for a patient can be daunting, and evidence of which treatment is superior can be lacking. However, the judicious use of benzodiazepines continues to be the primary treatment option. If status epilepticus persists, alternative agents and airway management may be necessary. The goal of treatment is to abort seizure-like activity observed on physician examination or EEG. It is important to remember that symptoms of status epilepticus can be subtle (eg, mild twitching, eye deviation), particularly when airway management is required since neuromuscular blockade can mask overt symptoms. Consultation with neurology and critical care colleagues should be initiated early; when such consultation is not available, the EP should consider patient transfer to an appropriate facility.
1. DeToledo JC, Lowe MR. Seizures, lateral decubitus, aspiration, and shoulder dislocation: time to change the guidelines? Neurology. 2001;56(3):290-291. doi:10.1212/wnl.56.3.290.
2. Silbergleit R, Lowenstein D, Durkalski V, et al; Neurological Emergency Treatment Trials (NETT) Investigators. RAMPART (Rapid Anticonvulsant Medication Prior to Arrival Trial): a double-blind randomized clinical trial of the efficacy of intramuscular midazolam versus intravenous lorazepam in the prehospital treatment of status epilepticus by paramedics. Epilepsia. 2011;52(Suppl 8):45-47. doi:10.1111/j.1528-1167.2011.03235.x.
3. Kreisman NR. Cerebral hypoxia during repetitive seizures. In: Somjen G, ed. Advances in Behavioral Biology: Mechanisms of Cerebral Hypoxia and Stroke. Vol 35. Boston, MA: Springer; 1988:139-149.
4. Van der Lende M, Surges R, Sander JW, Thijs RD. Cardiac arrhythmias during or after epileptic seizures. J Neurol Neurosurg Psychiatry. 2016;87(1):69-74. doi:10.1136/jnnp-2015-310559.
5. Appletan R, Sweeney A, Choonara I, Robson J, Molyneux E. Lorazepam versus diazepam in the acute treatment of epileptic seizures and status epilepticus. Dev Med Child Neurol. 1995;37(8):682-688. doi:10.1111/j.1469-8749.1995.tb15014.x.
6. McMullan J, Sasson C, Pancioli A, Silbergleit R. Midazolam versus diazepam for the treatment of status epilepticus in children and young adults: a meta-analysis. Acad Emerg Med. 2010;17(6):575-582. doi:10.1111/j.1553-2712.2010.00751.x.
7. Zhao ZY, Wang HY, Wen B, Yang ZB, Feng K, Fan JC. A comparison of midazolam, lorazepam, and diazepam for the treatment of status epilepticus in children: a network meta-analysis. J Child Neurol. 2016;31(9):1093-1107. doi:10.1177/0883073816638757.
8. Braun J, Gau E, Revelle S, Byrne L, Kumar A. Impact of non-guideline-based treatment of status epilepticus. J Neurol Sci. 2017;382:126-130. doi:10.1016/j.jns.2017.09.031.
9. Pillai U, Hothi JC, Bhat ZY. Severe propylene glycol toxicity secondary to use of anti-epileptics. Am J Ther. 2014;21(4):e106-e109. doi:10.1097/MJT.0b013e31824c407d.
10. Berkowitz R, Koyfman A. What is the best first-line agent for benzodiazepine-resistant convulsive status epilepticus? Ann Emerg Med. 2014;64(6):656-657. doi:10.1016/j.annemergmed.2014.04.017.
11. Established Status Epilepticus Treatment Trial. U.S. National Library of Medicine. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/NCT01960075. Accessed June 7, 2018.
12. O’Phelan KH, Miller CM. Emergency neurological life support: third edition, updates in the approach to early management of a neurological emergency. Neurocrit Care. 2017;27(Suppl 1):1-3. doi:10.1007/s12028-017-0448-x.
13. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339(12):792-798. doi:10.1056/NEJM199809173391202.
14. Thomson A. Fosphenytoin for the treatment of status epilepticus: an evidence-based assessment of its clinical and economic outcomes. Core Evid. 2005;1(1):65-75. doi:10.2147/ce.s6408.
15. Kanner AM. Intravenous valproate for status epilepticus...an effective, yet still merely empirical alternative! 2008;8(3):66-67. doi:10.1111/j.1535-7511.2008.00240.x.
16. Mishra D, Jain R, Juneja M, Chakrabarty B. Valproate associated hyperammonemic encephalopathy. J Pediatr Neurol. 2015;9(1):93-95. doi:10.3233/jpn-2010-0437.
17. Aiguabella M, Falip M, Villanueva V, et al. Efficacy of intravenous levetiracetam as an add-on treatment in status epilepticus: a multicentric observational study. Seizure. 2011;20(1):60-64. doi:10.1016/j.seizure.2010.10.009.
18. Lyttle MD, Gamble C, Messahel S, et al; supported by Paediatric Emergency Research in the United Kingdom & Ireland (PERUKI). Emergency treatment with levetiracetam or phenytoin in status epilepticus in children—the EcLiPSE study: study protocol for a randomised controlled trial. Trials. 2017;18(1):283. doi:10.1186/s13063-017-2010-8.
19. Uges JW, van Huizen MD, Engelsman J, et al. Safety and pharmacokinetics of intravenous levetiracetam infusion as add-on in status epilepticus. Epilepsia. 2009;50(3):415-421. doi:10.1111/j.1528-1167.2008.01889.x.
20. Afazal U, Oostema JA, Smith B. Emergency department initiation of levetiracetam for seizure: a cohort study examining psychiatric risk assessment and counseling. Ann Emerg Med. 2013;62(4):S131. doi:10.1016/j.annemergmed.2013.07.194.
21. Muramoto E, Mizobuchi M, Sumi Y, et al. Efficacy of intravenous phenobarbital treatment for status epilepticus. Brain Nerve. 2013;65(8):983-987.
22. Wijdicks EFM. Status epilepticus. In: The Practice of Emergency and Critical Care Neurology. New York, NY: Oxford University Press; 2010:558-559.
23. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002;43(2):146-153. doi:10.1046/j.1528-1157.2002.28501.x.
24. Choi YJ, Kim MC, Lim YJ, Yoon SZ, Yoon SM, Yoon HR. Propofol infusion associated metabolic acidosis in patients undergoing neurosurgical anesthesia: a retrospective study. J Korean Neurosurg Soc. 2014;56(2):135-140. doi:10.3340/jkns.2014.56.2.135.
25. Fernandez A, Lantigua H, Lesch C, et al. High-dose midazolam infusion for refractory status epilepticus. Neurology. 2013;82(4): 359-365. doi:10.1212/wnl.0000000000000054.
26. Dorandeu F. Ketamine for the treatment of (super) refractory status epilepticus? Not quite yet. Expert Rev Neurother. 2017;17(5):419-421. doi:10.1080/14737175.2017.1288099.
27. Zeiler FA, Zeiler KJ, Teitelbaum J, Gillman LM, West M. Modern inhalational anesthetics for refractory status epilepticus. Can J Neurol Sci. 2015;42(2):106-115. doi:10.1017/cjn.2014.121.
28. Shorvon S, Ferlisi M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain. 2011;134(10):2802-2818. doi:10.1093/brain/awr215.
29. Winkler PA. Surgical treatment of status epilepticus: a palliative approach. Epilepsia. 2013;54(Suppl 6):68-71. doi:10.1111/epi.12282.
30. Eros E, Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. A population-based case-control teratologic study of nitrazepam, medazepam, tofisopam, alprazolum and clonazepam treatment during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2002;101(2):147-154. doi:10.1016/s0301-2115(01)00545-0.
In part 1 of this 2-part review, the authors detailed proper diagnosis of seizures in the ED setting. In this concluding article, they focus on appropriate management and treatment options for patients with seizure.
In part 1 of this 2-part review, the authors detailed proper diagnosis of seizures in the ED setting. In this concluding article, they focus on appropriate management and treatment options for patients with seizure.
Status epilepticus is defined as continuous seizure activity for greater than 5 minutes, or repeated episodes of seizures without resolution of the postictal period. When the clinician arrives at the patient’s bedside or the emergency medical technician arrives at the scene in the prehospital setting, the patient may be minutes into seizure activity. If the seizure does not immediately resolve, the provider should treat as if status is imminent, if not ongoing. Regardless of setting, if the patient is discovered to be seizing, treatment should be initiated.
It is important to distinguish between provoked and unprovoked seizures, since successful management may require treating an underlying etiology. Although there are as many types of status epilepticus as there are types of seizures, the focus of this review is on generalized convulsive status epilepticus (GCSE).
As a GCSE continues, the overt seizure activity may become subtle—essentially a transformation of generalized status to a state with minimal or no motor movements. Whether or not there is an absence of, or minimal, movement, GCSE still represents a medical emergency, since the excessive neuronal activity causes neuronal injury. An electroencephalogram (EEG) may be required to detect transformed GCSE, which should be suspected if the patient does not exhibit improved mental status within 20 to 30 minutes of convulsive seizure cessation, or if neuromuscular paralysis for intubation has occurred.
Initial Management
Initial management of seizure patients is consistent with the care of any critical patient in the ED. Assessment of the airway and airway management with endotracheal intubation may be necessary for patients who are apneic or at risk for aspiration, or in whom more conservative management is inadequate.
While placing a patient in the left lateral decubitus position may mitigate aspiration risk, since vomiting is common in a postictal state, moving a convulsing patient may be challenging.1 Patients should be placed on cardiac monitoring with pulse oximetry if feasible. Intravenous (IV) access should be established if possible, though intramuscular (IM) or other alternative routes for benzodiazepines may be used if obtaining IV access will result in a delay in treatment.2
Oxygen should be administered via nonrebreather or bag-valve-mask to patients with apnea to prevent both systemic and cerebral hypoxia.3Since cardiac dysrhythmias with cerebral hypoxia may cause seizure-like activity, it is imperative to check the patient’s pulses, blood pressure, and to maintain cardiac monitoring during convulsive episodes.4 The patient’s glucose levels should be checked upon arrival to determine if the seizure is due to metabolic disturbance, which is an easily reversible cause of seizure. If glucose point-of-care testing is not available, it is reasonable to treat empirically for hypoglycemia.
Emergent Initial Therapy: First-Line Agents
Benzodiazepines
Benzodiazepines are the mainstay of emergent treatment for status epilepticus. The choice of benzodiazepine may be dependent on the clinical setting and availability of IV access or other resources. In the United States, diazepam, lorazepam, and midazolam are the common formulations used for abortive emergent initial therapy.
Diazepam. One of the advantages of diazepam is that it is has the advantage of being water soluble at room temperature, which allows rectal rescue kits for home treatment. Although diazepam is efficacious for status epilepticus, variable pharmacokinetics leading to repeat dosing and further sedation make other benzodiazepines safer.
Lorazepam. Generally accepted as the preferred IV formulation for seizure, lorazepam requires refrigeration and has a short shelf life, making its use challenging in the prehospital setting. When administered via the IV route, lorazepam works as rapidly as diazepam in treating seizures but with a longer duration of effectiveness, resulting in a decreased need to re-dose or administer an alternative antiepileptic drug (AED).5
Midazolam. Newer studies suggest that buccal, intranasal, and IM midazolam may be superior to buccal, intranasal, and IM diazepam in treating GCSE.6 The Rapid Anticonvulsant Medication Prior to Arrival Trial demonstrated IM midazolam to be at least as efficacious as IV lorazepam in the prehospital setting for treating GCSE.2
Efficacy, Route, and Dosing
A meta-analysis of all three benzodiazepines in pediatric patients with seizure showed midazolam to have the highest probability of aborting seizure activity, while lorazepam had the least likelihood of causing respiratory depression.7The authors concluded that IV lorazepam and non-IV midazolam were superior to IV and non-IV diazepam in the treatment of pediatric seizures.7
A recent retrospective study that analyzed benzodiazepine use in the emergency setting noted underdosing of benzodiazepines in the ED for nonprotocol-driven treatment of status epilepticus, resulting in the increased potential for adverse outcomes and intubations.8 Table 1 provides benzodiazepine dosing recommendations by route for adult and pediatric patients, along with potential adverse effects.
Adverse Effects
As noted previously, benzodiazepines can cause respiratory depression. Anecdotally, respiratory depression is often related to the rate at which the benzodiazepine is administered. For example, most treatment recommendations advise giving IV lorazepam over a 2-minute time period—not as an IV push.7
With respect to other adverse effects, it is important to note that IV formulations of diazepam and lorazepam contain propylene glycol as a diluent, which may lead to hypotension and bradycardia, especially when large volumes are infused over short periods of time.9
Second-Line Agents
While emergent initial therapy with benzodiazepines is well established, the preferred second-line agent, or urgent control therapy, continues to be a subject of controversy due to a lack of conclusive evidence for a superior agent.10 The Established Status Epilepticus Treatment Trial (ESETT) is currently conducting a head-to-head study to determine if any of the commonly used second-line agents (ie, fosphenytoin, levetiracetam, valproic acid) will prove to be more efficacious.11 Recently, the adult arm of the ESETT trial was halted due to futility.
All patients without an identifiable secondary cause of GCSE (eg, hypoglycemia, hyponatremia, hypocalcemia) should be started on a second-line agent. Treatment with a second-line agent provides two benefits: First, patients who experience resolution of seizure activity may rapidly attain therapeutic levels of AEDs, which may be sustained through maintenance therapy; and second, the second-line treatment may abort refractory cases of status.12 Table 2 provides dosing recommendations for second-line agents.
Phenytoin and Fosphenytoin
Phenytoin and the newer prodrug fosphenytoin are a mainstay urgent-control therapy for emergency physicians (EPs) and neurologists alike. In one of the few head-to-head studies of AEDs,13 phenytoin did not perform as well as the other study agents (diazepam, lorazepam, and phenobarbital); however, generalizability from this study is limited. Fosphenytoin continues to be an efficacious choice for second-line treatment of AED.
Fosphenytoin, a water-soluble prodrug of phenytoin, is given preferentially over IV phenytoin due to its decreased risk of cardiovascular (CV) side effects and more rapid administration.14 Moreover, fosphenytoin is compatible with most IV fluids (eg, dextrose, lactated Ringer’s solution, normal saline [NS]), whereas phenytoin is only compatible with NS. For convenience, fosphenytoin is dosed in phenytoin equivalents (PE/kg)—eg, administration of 20 PE/kg over 10 minutes is a potential loading dose for fosphenytoin.
Valproic Acid
Valproic acid has become a favored second-line agent for many providers due to its relatively safe profile and rapid infusion time. Most studies have shown IV valproic acid is at least as effective as phenytoin, but data continue to be somewhat weak and most of the studies are uncontrolled.15
Hepatotoxicity is generally only associated with long-term use of valproic acid, but it remains reasonable to abstain from using this agent in patients with preexisting hepatic disease. Valproic acid toxicity can lead to somnolence, ataxia, seizures, and coma with marked hyperammonemia.16
Levetiracetam
Intravenous levetiracetam is becoming a more commonly used drug both for emergent initial treatment of seizure and as a maintenance therapy. While data on levetiracetam are limited, a few studies tout the efficacy and safety of IV loading to abort GCSE.
In observational studies, levetiracetam appears to have similar efficacy to other AEDs and may be more beneficial in early therapy.17 An ongoing current study, The Emergency Treatment With Levetiracetam or Phenytoin in Status Epilepticus trial, is examining a prospective cohort of pediatric patients comparing levetiracetam against phenytoin.18
Levetiracetam is generally considered safe. The most commonly reported side effects are dizziness, somnolence, nausea, and brief transaminitis.19 Levetiracetam has also been associated with neuropsychiatric exacerbations.20
Phenobarbital
Intravenous phenobarbital has been used as an urgent-control therapy for seizure with good efficacy, even in recent years.21 Despite this, phenobarbital may cause profound CV depression necessitating the use of vasopressors.22 Large-dose phenobarbital can be used to induce coma in patients, although this should not be attempted without the guidance of a neurologist. While phenobarbital can be used safely in certain circumstances, its use has fallen out of favor in the ED due to the availability of safer alternative options.
Refractory Status Epilepticus
If after receiving two AEDs, a patient continues to demonstrate seizure activity on physical examination or EEG, she or he is considered to have refractory status epilepticus, which is a medical emergency. Patients in refractory status epilepticus will likely require a continuous infusion of an AED as well as definitive airway management as a result of either seizure or continuous treatment. In rare cases, some patients will continue to seize despite continuous treatment. Such patients are considered to have super refractory status epilepticus, which is defined as continuing seizure activity despite treatment with general anesthetics for more than 24 hours. This condition is beyond the scope of traditional EP practice, who in this scenario would consult emergently with neurology or critical care services.
Propofol
Propofol, a sedative-hypnotic agent that activates both γ-aminobutyric acid and N-methyl-D-aspartate receptors, is commonly given to patients with refractory status epilepticus. While head-to-head reviews have not shown propofol to be superior to phenobarbital or midazolam in treating refractory seizure, it is a drug that is familiar to most EPs.23 Midazolam or propofol are typically given to patients in the ED who require intubation with sedation.
With respect to side effects, propofol can cause dose-limiting hypotension. In addition, propofol infusion syndrome leading to lactic acidosis and cardiac dysfunction in patients receiving long-term propofol infusion.24 One possible infusion dose is 0.5-1 mg/kg loading dose with a continuous infusion of 2 mg/kg/h IV.
High-Dose Midazolam
High-dose midazolam may be given as an alternative to propofol as some studies have shown its efficacy in treating refractory status epilepticus.25 Continuous low-dose infusions of midazolam (0.2 mg/kg/h) have been given to patients in the neurological intensive care unit (ICU); however, there are some data to support treating with a higher dose (≥0.4 mg/kg/h).25 In one single-center retrospective trial, post discharge all-cause mortality was lower in the cohort group that received the higher dose infusion (40% vs 62%).25 Although higher rates of hypotension were noted in the high-dose group, it did not appear to affect mortality.
Ketamine
Ketamine has become a valued anesthetic in emergency medicine, and EPs have become comfortable with its dosing and safety profile. While animal studies on ketamine are promising to treat status epilepticus, human data are limited and often extrapolated from retrospective ICU data. Many patients are placed on a ketamine infusion multiple days into status epilepticus, and for this reason, ketamine is not recommended as a second-line abortive drug in the ED.26
Alternative Treatments and Super Refractory GCSE
In cases of patients with seizure activity ongoing beyond conventional therapy, other methods have been attempted to cease seizure activity and achieve burst suppression on EEG. None of these treatments is in the purview of the EP and should only be undertaken by a neurologist.
Two pharmacologic agents that have some limited efficacy include lacosamide and topiramate. Isoflurane is the most commonly used inhaled anesthetic.27 Thiopental and pentobarbital are barbiturate anesthetics which are used in super refractory GCSE. Barbiturates have a desirable theoretical neuroprotective effect, but are limited by their CV depression at high doses.28 Vagus nerve stimulation, induced hypothermia, transcranial magnetic stimulation, and neurosurgical intervention have all been attempted with varying degrees of success in select patients.29
Eclampsia and Seizures During Pregnancy
Treating a pregnant patient with status epilepticus presents a unique challenge in the ED. The EP must weigh the importance of aborting seizure activity with the possibility of teratogenic effects. All AEDs must be used carefully, but valproic acid and phenytoin are potent teratogens and should be avoided in this patient population. Most evidence points to safety with exposure to benzodiazepines during pregnancy.30 Eclampsia must be considered in patients who may be pregnant or recently pregnant; magnesium should be used with or without the use of benzodiazepines in these patients.
Summary
The diagnosis and treatment of status epilepticus in the ED can be challenging. While there is a multitude of first-, second-, and third-line agents available to treat this condition, choosing the correct therapy for a patient can be daunting, and evidence of which treatment is superior can be lacking. However, the judicious use of benzodiazepines continues to be the primary treatment option. If status epilepticus persists, alternative agents and airway management may be necessary. The goal of treatment is to abort seizure-like activity observed on physician examination or EEG. It is important to remember that symptoms of status epilepticus can be subtle (eg, mild twitching, eye deviation), particularly when airway management is required since neuromuscular blockade can mask overt symptoms. Consultation with neurology and critical care colleagues should be initiated early; when such consultation is not available, the EP should consider patient transfer to an appropriate facility.
Status epilepticus is defined as continuous seizure activity for greater than 5 minutes, or repeated episodes of seizures without resolution of the postictal period. When the clinician arrives at the patient’s bedside or the emergency medical technician arrives at the scene in the prehospital setting, the patient may be minutes into seizure activity. If the seizure does not immediately resolve, the provider should treat as if status is imminent, if not ongoing. Regardless of setting, if the patient is discovered to be seizing, treatment should be initiated.
It is important to distinguish between provoked and unprovoked seizures, since successful management may require treating an underlying etiology. Although there are as many types of status epilepticus as there are types of seizures, the focus of this review is on generalized convulsive status epilepticus (GCSE).
As a GCSE continues, the overt seizure activity may become subtle—essentially a transformation of generalized status to a state with minimal or no motor movements. Whether or not there is an absence of, or minimal, movement, GCSE still represents a medical emergency, since the excessive neuronal activity causes neuronal injury. An electroencephalogram (EEG) may be required to detect transformed GCSE, which should be suspected if the patient does not exhibit improved mental status within 20 to 30 minutes of convulsive seizure cessation, or if neuromuscular paralysis for intubation has occurred.
Initial Management
Initial management of seizure patients is consistent with the care of any critical patient in the ED. Assessment of the airway and airway management with endotracheal intubation may be necessary for patients who are apneic or at risk for aspiration, or in whom more conservative management is inadequate.
While placing a patient in the left lateral decubitus position may mitigate aspiration risk, since vomiting is common in a postictal state, moving a convulsing patient may be challenging.1 Patients should be placed on cardiac monitoring with pulse oximetry if feasible. Intravenous (IV) access should be established if possible, though intramuscular (IM) or other alternative routes for benzodiazepines may be used if obtaining IV access will result in a delay in treatment.2
Oxygen should be administered via nonrebreather or bag-valve-mask to patients with apnea to prevent both systemic and cerebral hypoxia.3Since cardiac dysrhythmias with cerebral hypoxia may cause seizure-like activity, it is imperative to check the patient’s pulses, blood pressure, and to maintain cardiac monitoring during convulsive episodes.4 The patient’s glucose levels should be checked upon arrival to determine if the seizure is due to metabolic disturbance, which is an easily reversible cause of seizure. If glucose point-of-care testing is not available, it is reasonable to treat empirically for hypoglycemia.
Emergent Initial Therapy: First-Line Agents
Benzodiazepines
Benzodiazepines are the mainstay of emergent treatment for status epilepticus. The choice of benzodiazepine may be dependent on the clinical setting and availability of IV access or other resources. In the United States, diazepam, lorazepam, and midazolam are the common formulations used for abortive emergent initial therapy.
Diazepam. One of the advantages of diazepam is that it is has the advantage of being water soluble at room temperature, which allows rectal rescue kits for home treatment. Although diazepam is efficacious for status epilepticus, variable pharmacokinetics leading to repeat dosing and further sedation make other benzodiazepines safer.
Lorazepam. Generally accepted as the preferred IV formulation for seizure, lorazepam requires refrigeration and has a short shelf life, making its use challenging in the prehospital setting. When administered via the IV route, lorazepam works as rapidly as diazepam in treating seizures but with a longer duration of effectiveness, resulting in a decreased need to re-dose or administer an alternative antiepileptic drug (AED).5
Midazolam. Newer studies suggest that buccal, intranasal, and IM midazolam may be superior to buccal, intranasal, and IM diazepam in treating GCSE.6 The Rapid Anticonvulsant Medication Prior to Arrival Trial demonstrated IM midazolam to be at least as efficacious as IV lorazepam in the prehospital setting for treating GCSE.2
Efficacy, Route, and Dosing
A meta-analysis of all three benzodiazepines in pediatric patients with seizure showed midazolam to have the highest probability of aborting seizure activity, while lorazepam had the least likelihood of causing respiratory depression.7The authors concluded that IV lorazepam and non-IV midazolam were superior to IV and non-IV diazepam in the treatment of pediatric seizures.7
A recent retrospective study that analyzed benzodiazepine use in the emergency setting noted underdosing of benzodiazepines in the ED for nonprotocol-driven treatment of status epilepticus, resulting in the increased potential for adverse outcomes and intubations.8 Table 1 provides benzodiazepine dosing recommendations by route for adult and pediatric patients, along with potential adverse effects.
Adverse Effects
As noted previously, benzodiazepines can cause respiratory depression. Anecdotally, respiratory depression is often related to the rate at which the benzodiazepine is administered. For example, most treatment recommendations advise giving IV lorazepam over a 2-minute time period—not as an IV push.7
With respect to other adverse effects, it is important to note that IV formulations of diazepam and lorazepam contain propylene glycol as a diluent, which may lead to hypotension and bradycardia, especially when large volumes are infused over short periods of time.9
Second-Line Agents
While emergent initial therapy with benzodiazepines is well established, the preferred second-line agent, or urgent control therapy, continues to be a subject of controversy due to a lack of conclusive evidence for a superior agent.10 The Established Status Epilepticus Treatment Trial (ESETT) is currently conducting a head-to-head study to determine if any of the commonly used second-line agents (ie, fosphenytoin, levetiracetam, valproic acid) will prove to be more efficacious.11 Recently, the adult arm of the ESETT trial was halted due to futility.
All patients without an identifiable secondary cause of GCSE (eg, hypoglycemia, hyponatremia, hypocalcemia) should be started on a second-line agent. Treatment with a second-line agent provides two benefits: First, patients who experience resolution of seizure activity may rapidly attain therapeutic levels of AEDs, which may be sustained through maintenance therapy; and second, the second-line treatment may abort refractory cases of status.12 Table 2 provides dosing recommendations for second-line agents.
Phenytoin and Fosphenytoin
Phenytoin and the newer prodrug fosphenytoin are a mainstay urgent-control therapy for emergency physicians (EPs) and neurologists alike. In one of the few head-to-head studies of AEDs,13 phenytoin did not perform as well as the other study agents (diazepam, lorazepam, and phenobarbital); however, generalizability from this study is limited. Fosphenytoin continues to be an efficacious choice for second-line treatment of AED.
Fosphenytoin, a water-soluble prodrug of phenytoin, is given preferentially over IV phenytoin due to its decreased risk of cardiovascular (CV) side effects and more rapid administration.14 Moreover, fosphenytoin is compatible with most IV fluids (eg, dextrose, lactated Ringer’s solution, normal saline [NS]), whereas phenytoin is only compatible with NS. For convenience, fosphenytoin is dosed in phenytoin equivalents (PE/kg)—eg, administration of 20 PE/kg over 10 minutes is a potential loading dose for fosphenytoin.
Valproic Acid
Valproic acid has become a favored second-line agent for many providers due to its relatively safe profile and rapid infusion time. Most studies have shown IV valproic acid is at least as effective as phenytoin, but data continue to be somewhat weak and most of the studies are uncontrolled.15
Hepatotoxicity is generally only associated with long-term use of valproic acid, but it remains reasonable to abstain from using this agent in patients with preexisting hepatic disease. Valproic acid toxicity can lead to somnolence, ataxia, seizures, and coma with marked hyperammonemia.16
Levetiracetam
Intravenous levetiracetam is becoming a more commonly used drug both for emergent initial treatment of seizure and as a maintenance therapy. While data on levetiracetam are limited, a few studies tout the efficacy and safety of IV loading to abort GCSE.
In observational studies, levetiracetam appears to have similar efficacy to other AEDs and may be more beneficial in early therapy.17 An ongoing current study, The Emergency Treatment With Levetiracetam or Phenytoin in Status Epilepticus trial, is examining a prospective cohort of pediatric patients comparing levetiracetam against phenytoin.18
Levetiracetam is generally considered safe. The most commonly reported side effects are dizziness, somnolence, nausea, and brief transaminitis.19 Levetiracetam has also been associated with neuropsychiatric exacerbations.20
Phenobarbital
Intravenous phenobarbital has been used as an urgent-control therapy for seizure with good efficacy, even in recent years.21 Despite this, phenobarbital may cause profound CV depression necessitating the use of vasopressors.22 Large-dose phenobarbital can be used to induce coma in patients, although this should not be attempted without the guidance of a neurologist. While phenobarbital can be used safely in certain circumstances, its use has fallen out of favor in the ED due to the availability of safer alternative options.
Refractory Status Epilepticus
If after receiving two AEDs, a patient continues to demonstrate seizure activity on physical examination or EEG, she or he is considered to have refractory status epilepticus, which is a medical emergency. Patients in refractory status epilepticus will likely require a continuous infusion of an AED as well as definitive airway management as a result of either seizure or continuous treatment. In rare cases, some patients will continue to seize despite continuous treatment. Such patients are considered to have super refractory status epilepticus, which is defined as continuing seizure activity despite treatment with general anesthetics for more than 24 hours. This condition is beyond the scope of traditional EP practice, who in this scenario would consult emergently with neurology or critical care services.
Propofol
Propofol, a sedative-hypnotic agent that activates both γ-aminobutyric acid and N-methyl-D-aspartate receptors, is commonly given to patients with refractory status epilepticus. While head-to-head reviews have not shown propofol to be superior to phenobarbital or midazolam in treating refractory seizure, it is a drug that is familiar to most EPs.23 Midazolam or propofol are typically given to patients in the ED who require intubation with sedation.
With respect to side effects, propofol can cause dose-limiting hypotension. In addition, propofol infusion syndrome leading to lactic acidosis and cardiac dysfunction in patients receiving long-term propofol infusion.24 One possible infusion dose is 0.5-1 mg/kg loading dose with a continuous infusion of 2 mg/kg/h IV.
High-Dose Midazolam
High-dose midazolam may be given as an alternative to propofol as some studies have shown its efficacy in treating refractory status epilepticus.25 Continuous low-dose infusions of midazolam (0.2 mg/kg/h) have been given to patients in the neurological intensive care unit (ICU); however, there are some data to support treating with a higher dose (≥0.4 mg/kg/h).25 In one single-center retrospective trial, post discharge all-cause mortality was lower in the cohort group that received the higher dose infusion (40% vs 62%).25 Although higher rates of hypotension were noted in the high-dose group, it did not appear to affect mortality.
Ketamine
Ketamine has become a valued anesthetic in emergency medicine, and EPs have become comfortable with its dosing and safety profile. While animal studies on ketamine are promising to treat status epilepticus, human data are limited and often extrapolated from retrospective ICU data. Many patients are placed on a ketamine infusion multiple days into status epilepticus, and for this reason, ketamine is not recommended as a second-line abortive drug in the ED.26
Alternative Treatments and Super Refractory GCSE
In cases of patients with seizure activity ongoing beyond conventional therapy, other methods have been attempted to cease seizure activity and achieve burst suppression on EEG. None of these treatments is in the purview of the EP and should only be undertaken by a neurologist.
Two pharmacologic agents that have some limited efficacy include lacosamide and topiramate. Isoflurane is the most commonly used inhaled anesthetic.27 Thiopental and pentobarbital are barbiturate anesthetics which are used in super refractory GCSE. Barbiturates have a desirable theoretical neuroprotective effect, but are limited by their CV depression at high doses.28 Vagus nerve stimulation, induced hypothermia, transcranial magnetic stimulation, and neurosurgical intervention have all been attempted with varying degrees of success in select patients.29
Eclampsia and Seizures During Pregnancy
Treating a pregnant patient with status epilepticus presents a unique challenge in the ED. The EP must weigh the importance of aborting seizure activity with the possibility of teratogenic effects. All AEDs must be used carefully, but valproic acid and phenytoin are potent teratogens and should be avoided in this patient population. Most evidence points to safety with exposure to benzodiazepines during pregnancy.30 Eclampsia must be considered in patients who may be pregnant or recently pregnant; magnesium should be used with or without the use of benzodiazepines in these patients.
Summary
The diagnosis and treatment of status epilepticus in the ED can be challenging. While there is a multitude of first-, second-, and third-line agents available to treat this condition, choosing the correct therapy for a patient can be daunting, and evidence of which treatment is superior can be lacking. However, the judicious use of benzodiazepines continues to be the primary treatment option. If status epilepticus persists, alternative agents and airway management may be necessary. The goal of treatment is to abort seizure-like activity observed on physician examination or EEG. It is important to remember that symptoms of status epilepticus can be subtle (eg, mild twitching, eye deviation), particularly when airway management is required since neuromuscular blockade can mask overt symptoms. Consultation with neurology and critical care colleagues should be initiated early; when such consultation is not available, the EP should consider patient transfer to an appropriate facility.
1. DeToledo JC, Lowe MR. Seizures, lateral decubitus, aspiration, and shoulder dislocation: time to change the guidelines? Neurology. 2001;56(3):290-291. doi:10.1212/wnl.56.3.290.
2. Silbergleit R, Lowenstein D, Durkalski V, et al; Neurological Emergency Treatment Trials (NETT) Investigators. RAMPART (Rapid Anticonvulsant Medication Prior to Arrival Trial): a double-blind randomized clinical trial of the efficacy of intramuscular midazolam versus intravenous lorazepam in the prehospital treatment of status epilepticus by paramedics. Epilepsia. 2011;52(Suppl 8):45-47. doi:10.1111/j.1528-1167.2011.03235.x.
3. Kreisman NR. Cerebral hypoxia during repetitive seizures. In: Somjen G, ed. Advances in Behavioral Biology: Mechanisms of Cerebral Hypoxia and Stroke. Vol 35. Boston, MA: Springer; 1988:139-149.
4. Van der Lende M, Surges R, Sander JW, Thijs RD. Cardiac arrhythmias during or after epileptic seizures. J Neurol Neurosurg Psychiatry. 2016;87(1):69-74. doi:10.1136/jnnp-2015-310559.
5. Appletan R, Sweeney A, Choonara I, Robson J, Molyneux E. Lorazepam versus diazepam in the acute treatment of epileptic seizures and status epilepticus. Dev Med Child Neurol. 1995;37(8):682-688. doi:10.1111/j.1469-8749.1995.tb15014.x.
6. McMullan J, Sasson C, Pancioli A, Silbergleit R. Midazolam versus diazepam for the treatment of status epilepticus in children and young adults: a meta-analysis. Acad Emerg Med. 2010;17(6):575-582. doi:10.1111/j.1553-2712.2010.00751.x.
7. Zhao ZY, Wang HY, Wen B, Yang ZB, Feng K, Fan JC. A comparison of midazolam, lorazepam, and diazepam for the treatment of status epilepticus in children: a network meta-analysis. J Child Neurol. 2016;31(9):1093-1107. doi:10.1177/0883073816638757.
8. Braun J, Gau E, Revelle S, Byrne L, Kumar A. Impact of non-guideline-based treatment of status epilepticus. J Neurol Sci. 2017;382:126-130. doi:10.1016/j.jns.2017.09.031.
9. Pillai U, Hothi JC, Bhat ZY. Severe propylene glycol toxicity secondary to use of anti-epileptics. Am J Ther. 2014;21(4):e106-e109. doi:10.1097/MJT.0b013e31824c407d.
10. Berkowitz R, Koyfman A. What is the best first-line agent for benzodiazepine-resistant convulsive status epilepticus? Ann Emerg Med. 2014;64(6):656-657. doi:10.1016/j.annemergmed.2014.04.017.
11. Established Status Epilepticus Treatment Trial. U.S. National Library of Medicine. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/NCT01960075. Accessed June 7, 2018.
12. O’Phelan KH, Miller CM. Emergency neurological life support: third edition, updates in the approach to early management of a neurological emergency. Neurocrit Care. 2017;27(Suppl 1):1-3. doi:10.1007/s12028-017-0448-x.
13. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339(12):792-798. doi:10.1056/NEJM199809173391202.
14. Thomson A. Fosphenytoin for the treatment of status epilepticus: an evidence-based assessment of its clinical and economic outcomes. Core Evid. 2005;1(1):65-75. doi:10.2147/ce.s6408.
15. Kanner AM. Intravenous valproate for status epilepticus...an effective, yet still merely empirical alternative! 2008;8(3):66-67. doi:10.1111/j.1535-7511.2008.00240.x.
16. Mishra D, Jain R, Juneja M, Chakrabarty B. Valproate associated hyperammonemic encephalopathy. J Pediatr Neurol. 2015;9(1):93-95. doi:10.3233/jpn-2010-0437.
17. Aiguabella M, Falip M, Villanueva V, et al. Efficacy of intravenous levetiracetam as an add-on treatment in status epilepticus: a multicentric observational study. Seizure. 2011;20(1):60-64. doi:10.1016/j.seizure.2010.10.009.
18. Lyttle MD, Gamble C, Messahel S, et al; supported by Paediatric Emergency Research in the United Kingdom & Ireland (PERUKI). Emergency treatment with levetiracetam or phenytoin in status epilepticus in children—the EcLiPSE study: study protocol for a randomised controlled trial. Trials. 2017;18(1):283. doi:10.1186/s13063-017-2010-8.
19. Uges JW, van Huizen MD, Engelsman J, et al. Safety and pharmacokinetics of intravenous levetiracetam infusion as add-on in status epilepticus. Epilepsia. 2009;50(3):415-421. doi:10.1111/j.1528-1167.2008.01889.x.
20. Afazal U, Oostema JA, Smith B. Emergency department initiation of levetiracetam for seizure: a cohort study examining psychiatric risk assessment and counseling. Ann Emerg Med. 2013;62(4):S131. doi:10.1016/j.annemergmed.2013.07.194.
21. Muramoto E, Mizobuchi M, Sumi Y, et al. Efficacy of intravenous phenobarbital treatment for status epilepticus. Brain Nerve. 2013;65(8):983-987.
22. Wijdicks EFM. Status epilepticus. In: The Practice of Emergency and Critical Care Neurology. New York, NY: Oxford University Press; 2010:558-559.
23. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002;43(2):146-153. doi:10.1046/j.1528-1157.2002.28501.x.
24. Choi YJ, Kim MC, Lim YJ, Yoon SZ, Yoon SM, Yoon HR. Propofol infusion associated metabolic acidosis in patients undergoing neurosurgical anesthesia: a retrospective study. J Korean Neurosurg Soc. 2014;56(2):135-140. doi:10.3340/jkns.2014.56.2.135.
25. Fernandez A, Lantigua H, Lesch C, et al. High-dose midazolam infusion for refractory status epilepticus. Neurology. 2013;82(4): 359-365. doi:10.1212/wnl.0000000000000054.
26. Dorandeu F. Ketamine for the treatment of (super) refractory status epilepticus? Not quite yet. Expert Rev Neurother. 2017;17(5):419-421. doi:10.1080/14737175.2017.1288099.
27. Zeiler FA, Zeiler KJ, Teitelbaum J, Gillman LM, West M. Modern inhalational anesthetics for refractory status epilepticus. Can J Neurol Sci. 2015;42(2):106-115. doi:10.1017/cjn.2014.121.
28. Shorvon S, Ferlisi M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain. 2011;134(10):2802-2818. doi:10.1093/brain/awr215.
29. Winkler PA. Surgical treatment of status epilepticus: a palliative approach. Epilepsia. 2013;54(Suppl 6):68-71. doi:10.1111/epi.12282.
30. Eros E, Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. A population-based case-control teratologic study of nitrazepam, medazepam, tofisopam, alprazolum and clonazepam treatment during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2002;101(2):147-154. doi:10.1016/s0301-2115(01)00545-0.
1. DeToledo JC, Lowe MR. Seizures, lateral decubitus, aspiration, and shoulder dislocation: time to change the guidelines? Neurology. 2001;56(3):290-291. doi:10.1212/wnl.56.3.290.
2. Silbergleit R, Lowenstein D, Durkalski V, et al; Neurological Emergency Treatment Trials (NETT) Investigators. RAMPART (Rapid Anticonvulsant Medication Prior to Arrival Trial): a double-blind randomized clinical trial of the efficacy of intramuscular midazolam versus intravenous lorazepam in the prehospital treatment of status epilepticus by paramedics. Epilepsia. 2011;52(Suppl 8):45-47. doi:10.1111/j.1528-1167.2011.03235.x.
3. Kreisman NR. Cerebral hypoxia during repetitive seizures. In: Somjen G, ed. Advances in Behavioral Biology: Mechanisms of Cerebral Hypoxia and Stroke. Vol 35. Boston, MA: Springer; 1988:139-149.
4. Van der Lende M, Surges R, Sander JW, Thijs RD. Cardiac arrhythmias during or after epileptic seizures. J Neurol Neurosurg Psychiatry. 2016;87(1):69-74. doi:10.1136/jnnp-2015-310559.
5. Appletan R, Sweeney A, Choonara I, Robson J, Molyneux E. Lorazepam versus diazepam in the acute treatment of epileptic seizures and status epilepticus. Dev Med Child Neurol. 1995;37(8):682-688. doi:10.1111/j.1469-8749.1995.tb15014.x.
6. McMullan J, Sasson C, Pancioli A, Silbergleit R. Midazolam versus diazepam for the treatment of status epilepticus in children and young adults: a meta-analysis. Acad Emerg Med. 2010;17(6):575-582. doi:10.1111/j.1553-2712.2010.00751.x.
7. Zhao ZY, Wang HY, Wen B, Yang ZB, Feng K, Fan JC. A comparison of midazolam, lorazepam, and diazepam for the treatment of status epilepticus in children: a network meta-analysis. J Child Neurol. 2016;31(9):1093-1107. doi:10.1177/0883073816638757.
8. Braun J, Gau E, Revelle S, Byrne L, Kumar A. Impact of non-guideline-based treatment of status epilepticus. J Neurol Sci. 2017;382:126-130. doi:10.1016/j.jns.2017.09.031.
9. Pillai U, Hothi JC, Bhat ZY. Severe propylene glycol toxicity secondary to use of anti-epileptics. Am J Ther. 2014;21(4):e106-e109. doi:10.1097/MJT.0b013e31824c407d.
10. Berkowitz R, Koyfman A. What is the best first-line agent for benzodiazepine-resistant convulsive status epilepticus? Ann Emerg Med. 2014;64(6):656-657. doi:10.1016/j.annemergmed.2014.04.017.
11. Established Status Epilepticus Treatment Trial. U.S. National Library of Medicine. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/NCT01960075. Accessed June 7, 2018.
12. O’Phelan KH, Miller CM. Emergency neurological life support: third edition, updates in the approach to early management of a neurological emergency. Neurocrit Care. 2017;27(Suppl 1):1-3. doi:10.1007/s12028-017-0448-x.
13. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339(12):792-798. doi:10.1056/NEJM199809173391202.
14. Thomson A. Fosphenytoin for the treatment of status epilepticus: an evidence-based assessment of its clinical and economic outcomes. Core Evid. 2005;1(1):65-75. doi:10.2147/ce.s6408.
15. Kanner AM. Intravenous valproate for status epilepticus...an effective, yet still merely empirical alternative! 2008;8(3):66-67. doi:10.1111/j.1535-7511.2008.00240.x.
16. Mishra D, Jain R, Juneja M, Chakrabarty B. Valproate associated hyperammonemic encephalopathy. J Pediatr Neurol. 2015;9(1):93-95. doi:10.3233/jpn-2010-0437.
17. Aiguabella M, Falip M, Villanueva V, et al. Efficacy of intravenous levetiracetam as an add-on treatment in status epilepticus: a multicentric observational study. Seizure. 2011;20(1):60-64. doi:10.1016/j.seizure.2010.10.009.
18. Lyttle MD, Gamble C, Messahel S, et al; supported by Paediatric Emergency Research in the United Kingdom & Ireland (PERUKI). Emergency treatment with levetiracetam or phenytoin in status epilepticus in children—the EcLiPSE study: study protocol for a randomised controlled trial. Trials. 2017;18(1):283. doi:10.1186/s13063-017-2010-8.
19. Uges JW, van Huizen MD, Engelsman J, et al. Safety and pharmacokinetics of intravenous levetiracetam infusion as add-on in status epilepticus. Epilepsia. 2009;50(3):415-421. doi:10.1111/j.1528-1167.2008.01889.x.
20. Afazal U, Oostema JA, Smith B. Emergency department initiation of levetiracetam for seizure: a cohort study examining psychiatric risk assessment and counseling. Ann Emerg Med. 2013;62(4):S131. doi:10.1016/j.annemergmed.2013.07.194.
21. Muramoto E, Mizobuchi M, Sumi Y, et al. Efficacy of intravenous phenobarbital treatment for status epilepticus. Brain Nerve. 2013;65(8):983-987.
22. Wijdicks EFM. Status epilepticus. In: The Practice of Emergency and Critical Care Neurology. New York, NY: Oxford University Press; 2010:558-559.
23. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002;43(2):146-153. doi:10.1046/j.1528-1157.2002.28501.x.
24. Choi YJ, Kim MC, Lim YJ, Yoon SZ, Yoon SM, Yoon HR. Propofol infusion associated metabolic acidosis in patients undergoing neurosurgical anesthesia: a retrospective study. J Korean Neurosurg Soc. 2014;56(2):135-140. doi:10.3340/jkns.2014.56.2.135.
25. Fernandez A, Lantigua H, Lesch C, et al. High-dose midazolam infusion for refractory status epilepticus. Neurology. 2013;82(4): 359-365. doi:10.1212/wnl.0000000000000054.
26. Dorandeu F. Ketamine for the treatment of (super) refractory status epilepticus? Not quite yet. Expert Rev Neurother. 2017;17(5):419-421. doi:10.1080/14737175.2017.1288099.
27. Zeiler FA, Zeiler KJ, Teitelbaum J, Gillman LM, West M. Modern inhalational anesthetics for refractory status epilepticus. Can J Neurol Sci. 2015;42(2):106-115. doi:10.1017/cjn.2014.121.
28. Shorvon S, Ferlisi M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain. 2011;134(10):2802-2818. doi:10.1093/brain/awr215.
29. Winkler PA. Surgical treatment of status epilepticus: a palliative approach. Epilepsia. 2013;54(Suppl 6):68-71. doi:10.1111/epi.12282.
30. Eros E, Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. A population-based case-control teratologic study of nitrazepam, medazepam, tofisopam, alprazolum and clonazepam treatment during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2002;101(2):147-154. doi:10.1016/s0301-2115(01)00545-0.