User login
Asymptomatic Pink Plaque on the Scapula
The Diagnosis: Primary Cutaneous Follicle Center Lymphoma
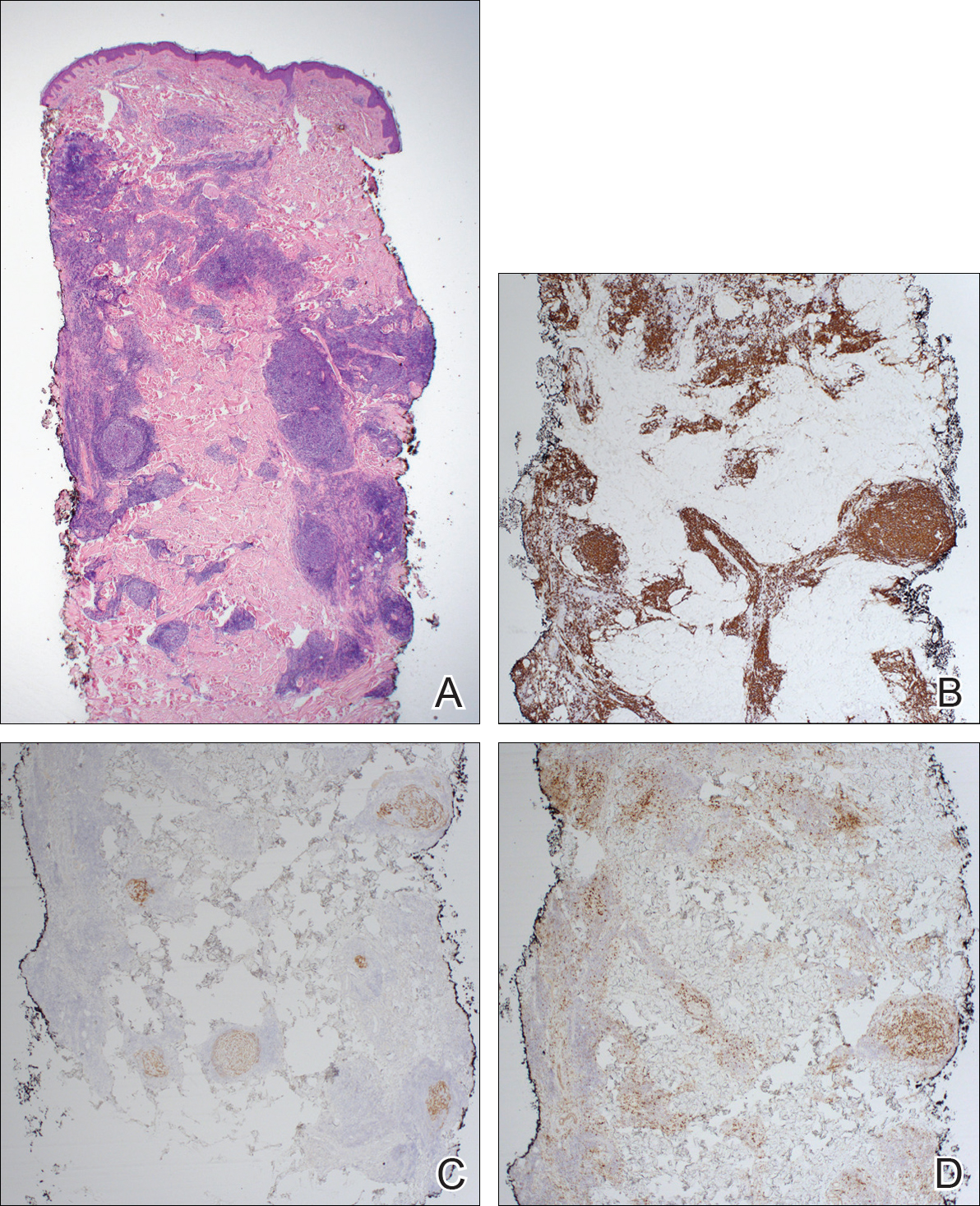
Immunohistochemistry revealed a nodular infiltrate consisting of small to large atypical lymphocytes forming an irregular germinal center with notably thinned mantle zones and lack of polarization (Figure, A). Atypical cells stained positively with Bcl-6, and CD20 was diffusely positive (Figure, B-D). Bcl-2 and CD3 colocalized to the reactive T-cell infiltrate, and CD10 was largely negative. Further workup with bone marrow biopsy and full-body positron emission tomography-computed tomography was unremarkable. Given these findings, a diagnosis of primary cutaneous follicle center lymphoma (FCL) was made. At 1 month following radiation therapy, complete clinical clearance of the lymphoma was achieved.
Follicle center lymphoma, also known as cutaneous follicular lymphoma, is the most common subtype of primary cutaneous B-cell lymphomas, representing approximately 57% of cases.1 Follicle center lymphoma typically affects older, non-Hispanic white adults with a median age of onset of 60 years. It has a predilection for the head, neck, and trunk.2 Lesions present as solitary erythematous to violaceous papules, plaques, or nodules, but they can more rarely be multifocal.3 Clinical diagnosis of FCL can be difficult, with papular lesions resembling acne, rosacea, folliculitis, or arthropod assault.4,5 As such, diagnosis of FCL typically relies on histopathologic analysis.
Histologically, FCL can present in several different patterns including follicular, nodular, diffuse, or a pleomorphic mix of these.2,6 The cells are comprised of germinal center B cells, staining positively for Bcl-6, CD20, and CD79a.7 Tumor cells do not exhibit the t(14;18) translocation seen in nodal follicular lymphomas.2,8 Unlike marginal zone lymphoma, FCL stains negatively for Bcl-2 and multiple myeloma 1/interferon regulatory factor 4 (MUM1/IRF-4).2,9 Forkhead box P1 (FOXP1) also is usually negative, but its presence can indicate a poorer prognosis.2 It is important to distinguish primary cutaneous B-cell lymphomas from systemic B-cell lymphoma with secondary cutaneous involvement, as they have a different clinical prognosis and management course. Further workup includes bone marrow biopsy, serum analysis for clonal involvement, and positron emission tomography-computed tomography imaging. Follicle center lymphoma generally has an indolent disease course with a favorable 5-year survival rate of approximately 95%.6,8
Untreated lesions may enlarge slowly or even spontaneously involute.10 The histologic growth pattern and number of lesions do not affect prognosis, but presence on the legs has a 5-year survival rate of 41%.2 Extracutaneous dissemination can occur in 5% to 10% of cases.2 Given the slow progression of FCL, conservative management with observation is an option. However, curative treatment can be reasonably attempted for solitary lesions by excision or radiation. Treatment of FCL often can be complicated by its predilection for the head and neck. Other treatment modalities include topical steroids, imiquimod, nitrogen mustard, and bexarotene.10 More generalized involvement may require systemic therapy with rituximab or chemotherapy. Recurrence after therapy is common, reported in 46.5% of patients, but does not affect prognosis.2
- Zinzani PL, Quaglino P, Pimpinelli N, et al. Prognostic factors in primary cutaneous B-cell lymphoma: The Italian Study Group for Cutaneous Lymphomas. J Clin Oncol. 2006;24:1376-1382.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:1-13.
- Grange F, Bekkenk MW, Wechsler J, et al. Prognostic factors in primary cutaneous large B-cell lymphomas: a European multicenter study. J Clin Oncol. 2001;19:3602-3610.
- Soon CW, Pincus LB, Ai WZ, et al. Acneiform presentation of primary cutaneous follicle center lymphoma. J Am Acad Dermatol. 2011;65:887-889.
- Massone C, Fink-Puches R, Laimer M, et al. Miliary and agminated-type primary cutaneous follicle center lymphoma: a report of 18 cases. J Am Acad Dermatol. 2011;65:749-755.
- Wilcox RA. CME information: cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90:73-76.
- Franco R, Fernandez-Vazquez A, Rodriguez-Peralto JL, et al. Cutaneous follicular B-cell lymphoma: description of a series of 18 cases. Am J Surg Pathol. 2001;25:875-883.
- Kempf W, Denisjuk N, Kerl K, et al. Primary cutaneous B-cell lymphomas. J Dtsch Dermatol Ges. 2012;10:12-22; quiz 23.
- de Leval L HN, Longtine J, Ferry JA, et al. Cutaneous B-cell lymphomas of follicular and marginal zone types: use of Bcl-6, CD10, Bcl-2, and CD21 in differential diagnosis and classification. Am J Surg Pathol. 2001;25:732-741.
- Suárez AL, Querfeld C, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part II. therapy and future directions. J Am Acad Dermatol. 2013;69:1-11.
The Diagnosis: Primary Cutaneous Follicle Center Lymphoma
Immunohistochemistry revealed a nodular infiltrate consisting of small to large atypical lymphocytes forming an irregular germinal center with notably thinned mantle zones and lack of polarization (Figure, A). Atypical cells stained positively with Bcl-6, and CD20 was diffusely positive (Figure, B-D). Bcl-2 and CD3 colocalized to the reactive T-cell infiltrate, and CD10 was largely negative. Further workup with bone marrow biopsy and full-body positron emission tomography-computed tomography was unremarkable. Given these findings, a diagnosis of primary cutaneous follicle center lymphoma (FCL) was made. At 1 month following radiation therapy, complete clinical clearance of the lymphoma was achieved.
Follicle center lymphoma, also known as cutaneous follicular lymphoma, is the most common subtype of primary cutaneous B-cell lymphomas, representing approximately 57% of cases.1 Follicle center lymphoma typically affects older, non-Hispanic white adults with a median age of onset of 60 years. It has a predilection for the head, neck, and trunk.2 Lesions present as solitary erythematous to violaceous papules, plaques, or nodules, but they can more rarely be multifocal.3 Clinical diagnosis of FCL can be difficult, with papular lesions resembling acne, rosacea, folliculitis, or arthropod assault.4,5 As such, diagnosis of FCL typically relies on histopathologic analysis.
Histologically, FCL can present in several different patterns including follicular, nodular, diffuse, or a pleomorphic mix of these.2,6 The cells are comprised of germinal center B cells, staining positively for Bcl-6, CD20, and CD79a.7 Tumor cells do not exhibit the t(14;18) translocation seen in nodal follicular lymphomas.2,8 Unlike marginal zone lymphoma, FCL stains negatively for Bcl-2 and multiple myeloma 1/interferon regulatory factor 4 (MUM1/IRF-4).2,9 Forkhead box P1 (FOXP1) also is usually negative, but its presence can indicate a poorer prognosis.2 It is important to distinguish primary cutaneous B-cell lymphomas from systemic B-cell lymphoma with secondary cutaneous involvement, as they have a different clinical prognosis and management course. Further workup includes bone marrow biopsy, serum analysis for clonal involvement, and positron emission tomography-computed tomography imaging. Follicle center lymphoma generally has an indolent disease course with a favorable 5-year survival rate of approximately 95%.6,8
Untreated lesions may enlarge slowly or even spontaneously involute.10 The histologic growth pattern and number of lesions do not affect prognosis, but presence on the legs has a 5-year survival rate of 41%.2 Extracutaneous dissemination can occur in 5% to 10% of cases.2 Given the slow progression of FCL, conservative management with observation is an option. However, curative treatment can be reasonably attempted for solitary lesions by excision or radiation. Treatment of FCL often can be complicated by its predilection for the head and neck. Other treatment modalities include topical steroids, imiquimod, nitrogen mustard, and bexarotene.10 More generalized involvement may require systemic therapy with rituximab or chemotherapy. Recurrence after therapy is common, reported in 46.5% of patients, but does not affect prognosis.2
The Diagnosis: Primary Cutaneous Follicle Center Lymphoma
Immunohistochemistry revealed a nodular infiltrate consisting of small to large atypical lymphocytes forming an irregular germinal center with notably thinned mantle zones and lack of polarization (Figure, A). Atypical cells stained positively with Bcl-6, and CD20 was diffusely positive (Figure, B-D). Bcl-2 and CD3 colocalized to the reactive T-cell infiltrate, and CD10 was largely negative. Further workup with bone marrow biopsy and full-body positron emission tomography-computed tomography was unremarkable. Given these findings, a diagnosis of primary cutaneous follicle center lymphoma (FCL) was made. At 1 month following radiation therapy, complete clinical clearance of the lymphoma was achieved.
Follicle center lymphoma, also known as cutaneous follicular lymphoma, is the most common subtype of primary cutaneous B-cell lymphomas, representing approximately 57% of cases.1 Follicle center lymphoma typically affects older, non-Hispanic white adults with a median age of onset of 60 years. It has a predilection for the head, neck, and trunk.2 Lesions present as solitary erythematous to violaceous papules, plaques, or nodules, but they can more rarely be multifocal.3 Clinical diagnosis of FCL can be difficult, with papular lesions resembling acne, rosacea, folliculitis, or arthropod assault.4,5 As such, diagnosis of FCL typically relies on histopathologic analysis.
Histologically, FCL can present in several different patterns including follicular, nodular, diffuse, or a pleomorphic mix of these.2,6 The cells are comprised of germinal center B cells, staining positively for Bcl-6, CD20, and CD79a.7 Tumor cells do not exhibit the t(14;18) translocation seen in nodal follicular lymphomas.2,8 Unlike marginal zone lymphoma, FCL stains negatively for Bcl-2 and multiple myeloma 1/interferon regulatory factor 4 (MUM1/IRF-4).2,9 Forkhead box P1 (FOXP1) also is usually negative, but its presence can indicate a poorer prognosis.2 It is important to distinguish primary cutaneous B-cell lymphomas from systemic B-cell lymphoma with secondary cutaneous involvement, as they have a different clinical prognosis and management course. Further workup includes bone marrow biopsy, serum analysis for clonal involvement, and positron emission tomography-computed tomography imaging. Follicle center lymphoma generally has an indolent disease course with a favorable 5-year survival rate of approximately 95%.6,8
Untreated lesions may enlarge slowly or even spontaneously involute.10 The histologic growth pattern and number of lesions do not affect prognosis, but presence on the legs has a 5-year survival rate of 41%.2 Extracutaneous dissemination can occur in 5% to 10% of cases.2 Given the slow progression of FCL, conservative management with observation is an option. However, curative treatment can be reasonably attempted for solitary lesions by excision or radiation. Treatment of FCL often can be complicated by its predilection for the head and neck. Other treatment modalities include topical steroids, imiquimod, nitrogen mustard, and bexarotene.10 More generalized involvement may require systemic therapy with rituximab or chemotherapy. Recurrence after therapy is common, reported in 46.5% of patients, but does not affect prognosis.2
- Zinzani PL, Quaglino P, Pimpinelli N, et al. Prognostic factors in primary cutaneous B-cell lymphoma: The Italian Study Group for Cutaneous Lymphomas. J Clin Oncol. 2006;24:1376-1382.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:1-13.
- Grange F, Bekkenk MW, Wechsler J, et al. Prognostic factors in primary cutaneous large B-cell lymphomas: a European multicenter study. J Clin Oncol. 2001;19:3602-3610.
- Soon CW, Pincus LB, Ai WZ, et al. Acneiform presentation of primary cutaneous follicle center lymphoma. J Am Acad Dermatol. 2011;65:887-889.
- Massone C, Fink-Puches R, Laimer M, et al. Miliary and agminated-type primary cutaneous follicle center lymphoma: a report of 18 cases. J Am Acad Dermatol. 2011;65:749-755.
- Wilcox RA. CME information: cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90:73-76.
- Franco R, Fernandez-Vazquez A, Rodriguez-Peralto JL, et al. Cutaneous follicular B-cell lymphoma: description of a series of 18 cases. Am J Surg Pathol. 2001;25:875-883.
- Kempf W, Denisjuk N, Kerl K, et al. Primary cutaneous B-cell lymphomas. J Dtsch Dermatol Ges. 2012;10:12-22; quiz 23.
- de Leval L HN, Longtine J, Ferry JA, et al. Cutaneous B-cell lymphomas of follicular and marginal zone types: use of Bcl-6, CD10, Bcl-2, and CD21 in differential diagnosis and classification. Am J Surg Pathol. 2001;25:732-741.
- Suárez AL, Querfeld C, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part II. therapy and future directions. J Am Acad Dermatol. 2013;69:1-11.
- Zinzani PL, Quaglino P, Pimpinelli N, et al. Prognostic factors in primary cutaneous B-cell lymphoma: The Italian Study Group for Cutaneous Lymphomas. J Clin Oncol. 2006;24:1376-1382.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:1-13.
- Grange F, Bekkenk MW, Wechsler J, et al. Prognostic factors in primary cutaneous large B-cell lymphomas: a European multicenter study. J Clin Oncol. 2001;19:3602-3610.
- Soon CW, Pincus LB, Ai WZ, et al. Acneiform presentation of primary cutaneous follicle center lymphoma. J Am Acad Dermatol. 2011;65:887-889.
- Massone C, Fink-Puches R, Laimer M, et al. Miliary and agminated-type primary cutaneous follicle center lymphoma: a report of 18 cases. J Am Acad Dermatol. 2011;65:749-755.
- Wilcox RA. CME information: cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90:73-76.
- Franco R, Fernandez-Vazquez A, Rodriguez-Peralto JL, et al. Cutaneous follicular B-cell lymphoma: description of a series of 18 cases. Am J Surg Pathol. 2001;25:875-883.
- Kempf W, Denisjuk N, Kerl K, et al. Primary cutaneous B-cell lymphomas. J Dtsch Dermatol Ges. 2012;10:12-22; quiz 23.
- de Leval L HN, Longtine J, Ferry JA, et al. Cutaneous B-cell lymphomas of follicular and marginal zone types: use of Bcl-6, CD10, Bcl-2, and CD21 in differential diagnosis and classification. Am J Surg Pathol. 2001;25:732-741.
- Suárez AL, Querfeld C, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part II. therapy and future directions. J Am Acad Dermatol. 2013;69:1-11.

A 36-year-old man presented with a pink plaque on the right side of the scapula of 1 year's duration. The plaque had not grown and was completely asymptomatic. Physical examination revealed a violaceous, pink, 2-cm nodule with overlying telangiectasia. No other concerning lesions were identified on total-body skin examination. A punch biopsy was obtained.

GSI may boost BCMA CAR T-cell therapy efficacy in myeloma
NATIONAL HARBOR, MD. – Gamma secretase inhibition may lead to improved outcomes in multiple myeloma patients treated with B-cell maturation antigen (BCMA)–specific CAR T-cell therapy, according to Margot J. Pont, PhD.
In a preclinical myeloma model, gamma secretase inhibition (GSI) increased antitumor efficacy of BCMA-specific chimeric antigen receptor modified T-cells (BCMA CAR T), Dr. Pont of Fred Hutchinson Cancer Research Center, Seattle, reported at the annual meeting of the Society for Immunotherapy of Cancer.
BCMA is expressed in most multiple myeloma patients, and can be targeted by T cells that have been transduced with an anti-BCMA CAR. Other studies have shown efficacy of BCMA CAR T cells, and Dr. Pont and her colleagues have developed and optimized a CAR, based on a previously described single-chain variable fragment (scFv), that performs at least as well as a similar CAR developed previously by another group.
Previous studies have found that antigen down-regulation and escape can be an important escape mechanism by the tumor, so low-to-negative antigen expression could lead to failure in CAR T-cell recognition, resulting in relapse, she explained.
“We need the antigen density to be high enough,” she said, noting that BCMA, specifically, can be susceptible to antigen down-regulation, because its extracellular component is cleaved off the cell membrane by the enzyme gamma-secretase.
“That leads to two things: It reduces the surface expression of BCMA and it sheds soluble BCMA into the circulation, so you get high concentrations of soluble BCMA in the tumor microenvironment,” she said.
Inhibiting BCMA shedding with GSI can increase surface expression and reduce levels of soluble BCMA, thereby potentially enhancing the CAR activity.
First, soluble BCMA levels were measured in bone marrow sera from myeloma patients.
“We indeed saw high levels of soluble BCMA in these patients, and they roughly correlated with tumor burden. When culturing myeloma cell lines in vitro, we detected sBCMA in the culture supernatant within 24 hours,” Dr. Pont said, adding that the introduction of recombinant BCMA to the cultures showed that increasing levels of recombinant BCMA reduced staining of the CAR, demonstrating binding to the receptor.
Next, GSI was used to increase BCMA levels, and with increasing concentrations of the drug, BCMA surface expression was increased, she said, noting that this coincided with a reduction of soluble BCMA in the culture supernatant.
This also worked in patient samples, and was achieved with low doses of GSI, which upregulated surface BCMA levels on primary multiple myeloma by up to tenfold, she said.
In vivo testing of CAR T-cell efficacy was performed in tumor-bearing mice, which were treated with either BCMA-specific CAR T cells alone or in combination with GSI.
In this preclinical model of myeloma, RO4929097 increased BCMA on tumor cells in bone marrow and decreased soluble BCMA in peripheral blood. The myeloma-bearing mice treated with both BCMA CAR T cells and intermittent doses of RO4929097 experienced improved antitumor effects of the BCMA CAR T-cell therapy, as well as increased survival versus mice that did not receive RO4929097, she said.
“We’re currently optimizing these dosing regimens,” she said, concluding that “combining GSI and BCMA CAR T is an attractive option to improve the level of efficacy and prevent the outgrowth of BCMA-low tumor cells.”
Dr. Pont reported having no relevant financial disclosures.
NATIONAL HARBOR, MD. – Gamma secretase inhibition may lead to improved outcomes in multiple myeloma patients treated with B-cell maturation antigen (BCMA)–specific CAR T-cell therapy, according to Margot J. Pont, PhD.
In a preclinical myeloma model, gamma secretase inhibition (GSI) increased antitumor efficacy of BCMA-specific chimeric antigen receptor modified T-cells (BCMA CAR T), Dr. Pont of Fred Hutchinson Cancer Research Center, Seattle, reported at the annual meeting of the Society for Immunotherapy of Cancer.
BCMA is expressed in most multiple myeloma patients, and can be targeted by T cells that have been transduced with an anti-BCMA CAR. Other studies have shown efficacy of BCMA CAR T cells, and Dr. Pont and her colleagues have developed and optimized a CAR, based on a previously described single-chain variable fragment (scFv), that performs at least as well as a similar CAR developed previously by another group.
Previous studies have found that antigen down-regulation and escape can be an important escape mechanism by the tumor, so low-to-negative antigen expression could lead to failure in CAR T-cell recognition, resulting in relapse, she explained.
“We need the antigen density to be high enough,” she said, noting that BCMA, specifically, can be susceptible to antigen down-regulation, because its extracellular component is cleaved off the cell membrane by the enzyme gamma-secretase.
“That leads to two things: It reduces the surface expression of BCMA and it sheds soluble BCMA into the circulation, so you get high concentrations of soluble BCMA in the tumor microenvironment,” she said.
Inhibiting BCMA shedding with GSI can increase surface expression and reduce levels of soluble BCMA, thereby potentially enhancing the CAR activity.
First, soluble BCMA levels were measured in bone marrow sera from myeloma patients.
“We indeed saw high levels of soluble BCMA in these patients, and they roughly correlated with tumor burden. When culturing myeloma cell lines in vitro, we detected sBCMA in the culture supernatant within 24 hours,” Dr. Pont said, adding that the introduction of recombinant BCMA to the cultures showed that increasing levels of recombinant BCMA reduced staining of the CAR, demonstrating binding to the receptor.
Next, GSI was used to increase BCMA levels, and with increasing concentrations of the drug, BCMA surface expression was increased, she said, noting that this coincided with a reduction of soluble BCMA in the culture supernatant.
This also worked in patient samples, and was achieved with low doses of GSI, which upregulated surface BCMA levels on primary multiple myeloma by up to tenfold, she said.
In vivo testing of CAR T-cell efficacy was performed in tumor-bearing mice, which were treated with either BCMA-specific CAR T cells alone or in combination with GSI.
In this preclinical model of myeloma, RO4929097 increased BCMA on tumor cells in bone marrow and decreased soluble BCMA in peripheral blood. The myeloma-bearing mice treated with both BCMA CAR T cells and intermittent doses of RO4929097 experienced improved antitumor effects of the BCMA CAR T-cell therapy, as well as increased survival versus mice that did not receive RO4929097, she said.
“We’re currently optimizing these dosing regimens,” she said, concluding that “combining GSI and BCMA CAR T is an attractive option to improve the level of efficacy and prevent the outgrowth of BCMA-low tumor cells.”
Dr. Pont reported having no relevant financial disclosures.
NATIONAL HARBOR, MD. – Gamma secretase inhibition may lead to improved outcomes in multiple myeloma patients treated with B-cell maturation antigen (BCMA)–specific CAR T-cell therapy, according to Margot J. Pont, PhD.
In a preclinical myeloma model, gamma secretase inhibition (GSI) increased antitumor efficacy of BCMA-specific chimeric antigen receptor modified T-cells (BCMA CAR T), Dr. Pont of Fred Hutchinson Cancer Research Center, Seattle, reported at the annual meeting of the Society for Immunotherapy of Cancer.
BCMA is expressed in most multiple myeloma patients, and can be targeted by T cells that have been transduced with an anti-BCMA CAR. Other studies have shown efficacy of BCMA CAR T cells, and Dr. Pont and her colleagues have developed and optimized a CAR, based on a previously described single-chain variable fragment (scFv), that performs at least as well as a similar CAR developed previously by another group.
Previous studies have found that antigen down-regulation and escape can be an important escape mechanism by the tumor, so low-to-negative antigen expression could lead to failure in CAR T-cell recognition, resulting in relapse, she explained.
“We need the antigen density to be high enough,” she said, noting that BCMA, specifically, can be susceptible to antigen down-regulation, because its extracellular component is cleaved off the cell membrane by the enzyme gamma-secretase.
“That leads to two things: It reduces the surface expression of BCMA and it sheds soluble BCMA into the circulation, so you get high concentrations of soluble BCMA in the tumor microenvironment,” she said.
Inhibiting BCMA shedding with GSI can increase surface expression and reduce levels of soluble BCMA, thereby potentially enhancing the CAR activity.
First, soluble BCMA levels were measured in bone marrow sera from myeloma patients.
“We indeed saw high levels of soluble BCMA in these patients, and they roughly correlated with tumor burden. When culturing myeloma cell lines in vitro, we detected sBCMA in the culture supernatant within 24 hours,” Dr. Pont said, adding that the introduction of recombinant BCMA to the cultures showed that increasing levels of recombinant BCMA reduced staining of the CAR, demonstrating binding to the receptor.
Next, GSI was used to increase BCMA levels, and with increasing concentrations of the drug, BCMA surface expression was increased, she said, noting that this coincided with a reduction of soluble BCMA in the culture supernatant.
This also worked in patient samples, and was achieved with low doses of GSI, which upregulated surface BCMA levels on primary multiple myeloma by up to tenfold, she said.
In vivo testing of CAR T-cell efficacy was performed in tumor-bearing mice, which were treated with either BCMA-specific CAR T cells alone or in combination with GSI.
In this preclinical model of myeloma, RO4929097 increased BCMA on tumor cells in bone marrow and decreased soluble BCMA in peripheral blood. The myeloma-bearing mice treated with both BCMA CAR T cells and intermittent doses of RO4929097 experienced improved antitumor effects of the BCMA CAR T-cell therapy, as well as increased survival versus mice that did not receive RO4929097, she said.
“We’re currently optimizing these dosing regimens,” she said, concluding that “combining GSI and BCMA CAR T is an attractive option to improve the level of efficacy and prevent the outgrowth of BCMA-low tumor cells.”
Dr. Pont reported having no relevant financial disclosures.
AT SITC 2017
MACRA Monday: Pneumococcal vaccination
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, the Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Measure #111: Pneumococcal Vaccination Status for Older Adults
This measure is aimed at capturing the percentage of patients aged 65 years and older who have ever received a pneumococcal vaccine.
What you need to do: Review the medical record to find out if the patient has ever received a pneumococcal vaccine and if not, administer the vaccine.
Eligible cases include patients who were aged 65 years or older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, CPT II 4040F indicates that the pneumococcal vaccine was administered or previously received. Use exclusion code G9707 to indicate that the patient was not eligible because they received hospice services at any time during the measurement period.
CMS has a full list measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
• Those who enrolled in Medicare for the first time during a performance period.
• Those who have Medicare Part B allowed charges of $30,000 or less.
• Those who have 100 or fewer Medicare Part B patients.
• Those who are significantly participating in an Advanced Alternative Payment Model (APM).
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, the Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Measure #111: Pneumococcal Vaccination Status for Older Adults
This measure is aimed at capturing the percentage of patients aged 65 years and older who have ever received a pneumococcal vaccine.
What you need to do: Review the medical record to find out if the patient has ever received a pneumococcal vaccine and if not, administer the vaccine.
Eligible cases include patients who were aged 65 years or older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, CPT II 4040F indicates that the pneumococcal vaccine was administered or previously received. Use exclusion code G9707 to indicate that the patient was not eligible because they received hospice services at any time during the measurement period.
CMS has a full list measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
• Those who enrolled in Medicare for the first time during a performance period.
• Those who have Medicare Part B allowed charges of $30,000 or less.
• Those who have 100 or fewer Medicare Part B patients.
• Those who are significantly participating in an Advanced Alternative Payment Model (APM).
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, the Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Measure #111: Pneumococcal Vaccination Status for Older Adults
This measure is aimed at capturing the percentage of patients aged 65 years and older who have ever received a pneumococcal vaccine.
What you need to do: Review the medical record to find out if the patient has ever received a pneumococcal vaccine and if not, administer the vaccine.
Eligible cases include patients who were aged 65 years or older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, CPT II 4040F indicates that the pneumococcal vaccine was administered or previously received. Use exclusion code G9707 to indicate that the patient was not eligible because they received hospice services at any time during the measurement period.
CMS has a full list measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
• Those who enrolled in Medicare for the first time during a performance period.
• Those who have Medicare Part B allowed charges of $30,000 or less.
• Those who have 100 or fewer Medicare Part B patients.
• Those who are significantly participating in an Advanced Alternative Payment Model (APM).

Bryant Homer Womack: Honoring Sacrifice
Bryant Homer Womack was born in 1931 and raised in Mill Spring in southwestern North Carolina. He and his 4 siblings grew up doing farmwork. Womack enjoyed the outdoors, especially hunting and fishing. After completing high school, he was drafted into the U.S. Army in 1950 and later deployed to Korea.
PFC Womack was assigned to the Medical Company, 14th Infantry Regiment, 25th Infantry Division. During a firefight near Sokso-ri, Korea, on March 12, 1952, his night combat patrol began taking heavy casualties. Womack exposed himself to enemy fire in order to treat his wounded. Although wounded, PFC Womack refused medical treatment and continued to provide aid to others. He was the last soldier to withdraw from the engagement and died of his wounds soon after. Not yet 21 at the time of his death, Womack was buried at Lebanon Methodist Church in his hometown.
PFC Womack received a posthumous Medal of Honor in 1953 (Sidebar) and Womack Army Community Hospital, located on Fort Bragg near Fayetteville, North Carolina, was named for him in 1958. The first medical facility to serve Fort Bragg was constructed in September 1918 as a U.S. States Army Hospital. In June 1932, an 83-bed, 3-story hospital was built and designated Station Hospital One; it was closed in 1941. The building is now Headquarters for XVIII Airborne Corps and Fort Bragg. Station Hospital Two and Station Hospital Three were cantonment style hospitals that replaced Station Hospital One. In 1949, the medical facilities were combined and became the U.S. Army Station Hospital.
On August 3, 1958, a new 9-story facility was opened and named Womack Army Community Hospital in honor of combat medic and Medal of Honor recipient PFC Bryant H. Womack. It was renamed the Womack Army Medical Center in 1991. This facility was the principal medical facility for the Fort Bragg community for more than 40 years.
In March, 2000, a new Womack Army Medical Center with more than 1 million square feet of space was dedicated. This new health care complex was part of the U.S. Army Medical Department’s plan to increase patient access to more medical and specialized resources at Fort Bragg.
1. U.S. Army Center of Military History. Medal of Honor Recipients Korean War. https://history.army.mil/moh/koreanwar.html#WOMACK. Updated April 2, 2014. Accessed October 12, 2017.
Bryant Homer Womack was born in 1931 and raised in Mill Spring in southwestern North Carolina. He and his 4 siblings grew up doing farmwork. Womack enjoyed the outdoors, especially hunting and fishing. After completing high school, he was drafted into the U.S. Army in 1950 and later deployed to Korea.
PFC Womack was assigned to the Medical Company, 14th Infantry Regiment, 25th Infantry Division. During a firefight near Sokso-ri, Korea, on March 12, 1952, his night combat patrol began taking heavy casualties. Womack exposed himself to enemy fire in order to treat his wounded. Although wounded, PFC Womack refused medical treatment and continued to provide aid to others. He was the last soldier to withdraw from the engagement and died of his wounds soon after. Not yet 21 at the time of his death, Womack was buried at Lebanon Methodist Church in his hometown.
PFC Womack received a posthumous Medal of Honor in 1953 (Sidebar) and Womack Army Community Hospital, located on Fort Bragg near Fayetteville, North Carolina, was named for him in 1958. The first medical facility to serve Fort Bragg was constructed in September 1918 as a U.S. States Army Hospital. In June 1932, an 83-bed, 3-story hospital was built and designated Station Hospital One; it was closed in 1941. The building is now Headquarters for XVIII Airborne Corps and Fort Bragg. Station Hospital Two and Station Hospital Three were cantonment style hospitals that replaced Station Hospital One. In 1949, the medical facilities were combined and became the U.S. Army Station Hospital.
On August 3, 1958, a new 9-story facility was opened and named Womack Army Community Hospital in honor of combat medic and Medal of Honor recipient PFC Bryant H. Womack. It was renamed the Womack Army Medical Center in 1991. This facility was the principal medical facility for the Fort Bragg community for more than 40 years.
In March, 2000, a new Womack Army Medical Center with more than 1 million square feet of space was dedicated. This new health care complex was part of the U.S. Army Medical Department’s plan to increase patient access to more medical and specialized resources at Fort Bragg.
Bryant Homer Womack was born in 1931 and raised in Mill Spring in southwestern North Carolina. He and his 4 siblings grew up doing farmwork. Womack enjoyed the outdoors, especially hunting and fishing. After completing high school, he was drafted into the U.S. Army in 1950 and later deployed to Korea.
PFC Womack was assigned to the Medical Company, 14th Infantry Regiment, 25th Infantry Division. During a firefight near Sokso-ri, Korea, on March 12, 1952, his night combat patrol began taking heavy casualties. Womack exposed himself to enemy fire in order to treat his wounded. Although wounded, PFC Womack refused medical treatment and continued to provide aid to others. He was the last soldier to withdraw from the engagement and died of his wounds soon after. Not yet 21 at the time of his death, Womack was buried at Lebanon Methodist Church in his hometown.
PFC Womack received a posthumous Medal of Honor in 1953 (Sidebar) and Womack Army Community Hospital, located on Fort Bragg near Fayetteville, North Carolina, was named for him in 1958. The first medical facility to serve Fort Bragg was constructed in September 1918 as a U.S. States Army Hospital. In June 1932, an 83-bed, 3-story hospital was built and designated Station Hospital One; it was closed in 1941. The building is now Headquarters for XVIII Airborne Corps and Fort Bragg. Station Hospital Two and Station Hospital Three were cantonment style hospitals that replaced Station Hospital One. In 1949, the medical facilities were combined and became the U.S. Army Station Hospital.
On August 3, 1958, a new 9-story facility was opened and named Womack Army Community Hospital in honor of combat medic and Medal of Honor recipient PFC Bryant H. Womack. It was renamed the Womack Army Medical Center in 1991. This facility was the principal medical facility for the Fort Bragg community for more than 40 years.
In March, 2000, a new Womack Army Medical Center with more than 1 million square feet of space was dedicated. This new health care complex was part of the U.S. Army Medical Department’s plan to increase patient access to more medical and specialized resources at Fort Bragg.
1. U.S. Army Center of Military History. Medal of Honor Recipients Korean War. https://history.army.mil/moh/koreanwar.html#WOMACK. Updated April 2, 2014. Accessed October 12, 2017.
1. U.S. Army Center of Military History. Medal of Honor Recipients Korean War. https://history.army.mil/moh/koreanwar.html#WOMACK. Updated April 2, 2014. Accessed October 12, 2017.

Team identifies genetic differences between MM patients

Researchers say they have identified significant genetic differences between African-American patients with multiple myeloma (MM) and Caucasian patients with the disease.
For example, the researchers found that African Americans were more likely to have mutations in BCL7A, BRWD3, and AUTS2, but Caucasians were more likely to have mutations in IRF4 and TP53.
“A cancer therapy that targets TP53 would not be as effective for African Americans with multiple myeloma as it would be for a white population because doctors would be trying to fix the wrong mutated gene,” said Zarko Manojlovic, PhD, of the University of Southern California in Los Angeles.
Dr Manojlovic and his colleagues conducted this research and detailed the results in PLOS Genetics.
The researchers analyzed genetic sequencing data and clinical data from 718 MM patients participating in the MMRF CoMMpass Study.
Race was reported by the patients, but the researchers also used the genetic data to determine that 127 patients were of African descent and 591 were of European descent. The researchers noted that the mean European admixture among self-reported African Americans was 31% (range; 11%-67.8%). And the mean west-African admixture among self-reported Caucasians was 0.1% (range; 0-34.3).
The African-American patients were significantly more likely than the Caucasians to have early onset MM (at ages 40-49)—11% and 4.6%, respectively (P=0.004). And Caucasians were significantly more likely than African Americans to have late-onset MM (at ages 70-79)—22% and 14%, respectively (P=0.04).
There was no significant difference in overall survival based on race, age of onset, or MM karyotype in this population.
Mutations in the following genes occurred at significantly higher frequencies in African-American patients than in Caucasians: RYR1, RPL10, PTCHD3, BCL7A, SPEF2, MYH13, ABI3BP, BRWD3, GRM7, AUTS2, PARP4, PLD1, ANKRD26, DDX17, and STXBP4.
On the other hand, Caucasians had a significantly higher frequency of mutations in IRF4 and TP53. In fact, there was a TP53 somatic mutation frequency of 6.3% in Caucasians and 1.6% in African Americans (P=0.035).
“One of the most surprising discoveries from this large cohort is that cancers from patients of European descent were 6 times more likely than their African-descent counterparts to have mutations in TP53, a known tumor suppressor gene,” Dr Manojlovic said.
“Biologically speaking, higher mutation rates in this gene should lead to overall lower survival rates among patients of European descent, but that does not correlate with what we see in clinical outcomes. Going forward, we hope to functionally validate these results for more insight into the underlying biology.”
“We in the cancer genomics community have a responsibility to ensure that our studies represent true population diversity so we can understand the role of ancestry and biology in health outcomes,” added study author John D. Carpten, PhD, of the University of Southern California.
“The new candidate myeloma genes we identified in the African-American population may have been overlooked because of the lack of diversity in previous genomic efforts. There are clearly molecular differences between African-American and Caucasian multiple myeloma cases, and it will be critical to pursue these observations to better improve clinical management of the disease for all patients.” ![]()
Researchers say they have identified significant genetic differences between African-American patients with multiple myeloma (MM) and Caucasian patients with the disease.
For example, the researchers found that African Americans were more likely to have mutations in BCL7A, BRWD3, and AUTS2, but Caucasians were more likely to have mutations in IRF4 and TP53.
“A cancer therapy that targets TP53 would not be as effective for African Americans with multiple myeloma as it would be for a white population because doctors would be trying to fix the wrong mutated gene,” said Zarko Manojlovic, PhD, of the University of Southern California in Los Angeles.
Dr Manojlovic and his colleagues conducted this research and detailed the results in PLOS Genetics.
The researchers analyzed genetic sequencing data and clinical data from 718 MM patients participating in the MMRF CoMMpass Study.
Race was reported by the patients, but the researchers also used the genetic data to determine that 127 patients were of African descent and 591 were of European descent. The researchers noted that the mean European admixture among self-reported African Americans was 31% (range; 11%-67.8%). And the mean west-African admixture among self-reported Caucasians was 0.1% (range; 0-34.3).
The African-American patients were significantly more likely than the Caucasians to have early onset MM (at ages 40-49)—11% and 4.6%, respectively (P=0.004). And Caucasians were significantly more likely than African Americans to have late-onset MM (at ages 70-79)—22% and 14%, respectively (P=0.04).
There was no significant difference in overall survival based on race, age of onset, or MM karyotype in this population.
Mutations in the following genes occurred at significantly higher frequencies in African-American patients than in Caucasians: RYR1, RPL10, PTCHD3, BCL7A, SPEF2, MYH13, ABI3BP, BRWD3, GRM7, AUTS2, PARP4, PLD1, ANKRD26, DDX17, and STXBP4.
On the other hand, Caucasians had a significantly higher frequency of mutations in IRF4 and TP53. In fact, there was a TP53 somatic mutation frequency of 6.3% in Caucasians and 1.6% in African Americans (P=0.035).
“One of the most surprising discoveries from this large cohort is that cancers from patients of European descent were 6 times more likely than their African-descent counterparts to have mutations in TP53, a known tumor suppressor gene,” Dr Manojlovic said.
“Biologically speaking, higher mutation rates in this gene should lead to overall lower survival rates among patients of European descent, but that does not correlate with what we see in clinical outcomes. Going forward, we hope to functionally validate these results for more insight into the underlying biology.”
“We in the cancer genomics community have a responsibility to ensure that our studies represent true population diversity so we can understand the role of ancestry and biology in health outcomes,” added study author John D. Carpten, PhD, of the University of Southern California.
“The new candidate myeloma genes we identified in the African-American population may have been overlooked because of the lack of diversity in previous genomic efforts. There are clearly molecular differences between African-American and Caucasian multiple myeloma cases, and it will be critical to pursue these observations to better improve clinical management of the disease for all patients.” ![]()
Researchers say they have identified significant genetic differences between African-American patients with multiple myeloma (MM) and Caucasian patients with the disease.
For example, the researchers found that African Americans were more likely to have mutations in BCL7A, BRWD3, and AUTS2, but Caucasians were more likely to have mutations in IRF4 and TP53.
“A cancer therapy that targets TP53 would not be as effective for African Americans with multiple myeloma as it would be for a white population because doctors would be trying to fix the wrong mutated gene,” said Zarko Manojlovic, PhD, of the University of Southern California in Los Angeles.
Dr Manojlovic and his colleagues conducted this research and detailed the results in PLOS Genetics.
The researchers analyzed genetic sequencing data and clinical data from 718 MM patients participating in the MMRF CoMMpass Study.
Race was reported by the patients, but the researchers also used the genetic data to determine that 127 patients were of African descent and 591 were of European descent. The researchers noted that the mean European admixture among self-reported African Americans was 31% (range; 11%-67.8%). And the mean west-African admixture among self-reported Caucasians was 0.1% (range; 0-34.3).
The African-American patients were significantly more likely than the Caucasians to have early onset MM (at ages 40-49)—11% and 4.6%, respectively (P=0.004). And Caucasians were significantly more likely than African Americans to have late-onset MM (at ages 70-79)—22% and 14%, respectively (P=0.04).
There was no significant difference in overall survival based on race, age of onset, or MM karyotype in this population.
Mutations in the following genes occurred at significantly higher frequencies in African-American patients than in Caucasians: RYR1, RPL10, PTCHD3, BCL7A, SPEF2, MYH13, ABI3BP, BRWD3, GRM7, AUTS2, PARP4, PLD1, ANKRD26, DDX17, and STXBP4.
On the other hand, Caucasians had a significantly higher frequency of mutations in IRF4 and TP53. In fact, there was a TP53 somatic mutation frequency of 6.3% in Caucasians and 1.6% in African Americans (P=0.035).
“One of the most surprising discoveries from this large cohort is that cancers from patients of European descent were 6 times more likely than their African-descent counterparts to have mutations in TP53, a known tumor suppressor gene,” Dr Manojlovic said.
“Biologically speaking, higher mutation rates in this gene should lead to overall lower survival rates among patients of European descent, but that does not correlate with what we see in clinical outcomes. Going forward, we hope to functionally validate these results for more insight into the underlying biology.”
“We in the cancer genomics community have a responsibility to ensure that our studies represent true population diversity so we can understand the role of ancestry and biology in health outcomes,” added study author John D. Carpten, PhD, of the University of Southern California.
“The new candidate myeloma genes we identified in the African-American population may have been overlooked because of the lack of diversity in previous genomic efforts. There are clearly molecular differences between African-American and Caucasian multiple myeloma cases, and it will be critical to pursue these observations to better improve clinical management of the disease for all patients.” ![]()
Anaphylaxis Controversy and Consensus
Simplify Your Life; Pay Dues Invoice Online
Don't forget that the end of the year is the time to keep up to date with your SVS membership dues. Invoices were emailed to all members earlier this month and are due by Dec. 31.
It's simple to pay your 2018 dues online -- and there's no need to write out a check or find a stamp! Just log on to vascular.org/payinvoice. (While you're at it, please make sure your record is up to date.) You also can make a donation to the SVS Foundation at the same time. For membership help, e-mail the SVS membership department, or call 312-334-2313
Don't forget that the end of the year is the time to keep up to date with your SVS membership dues. Invoices were emailed to all members earlier this month and are due by Dec. 31.
It's simple to pay your 2018 dues online -- and there's no need to write out a check or find a stamp! Just log on to vascular.org/payinvoice. (While you're at it, please make sure your record is up to date.) You also can make a donation to the SVS Foundation at the same time. For membership help, e-mail the SVS membership department, or call 312-334-2313
Don't forget that the end of the year is the time to keep up to date with your SVS membership dues. Invoices were emailed to all members earlier this month and are due by Dec. 31.
It's simple to pay your 2018 dues online -- and there's no need to write out a check or find a stamp! Just log on to vascular.org/payinvoice. (While you're at it, please make sure your record is up to date.) You also can make a donation to the SVS Foundation at the same time. For membership help, e-mail the SVS membership department, or call 312-334-2313
How CLL patients weigh treatment efficacy, safety, and cost

New research suggests patients with chronic lymphocytic leukemia (CLL) are willing to trade treatment efficacy for a reduced risk of side effects, but the cost of treatment may trump other factors.
The patients studied placed the highest value on treatments that deliver the longest progression-free survival (PFS), but the patients were also willing to swap some efficacy for a reduced risk of serious adverse events (AEs).
Study results also indicated that factoring out-of-pocket costs into the decision-making process can significantly influence a patient’s choice of treatment.
Carol Mansfield, PhD, of RTI Health Solutions in Research Triangle Park, North Carolina, and her colleagues conducted this study and reported the results in Blood Advances. The study was supported by funding from Genentech, Inc., to RTI Health Solutions.
The researchers surveyed 384 patients with CLL. Patients were asked to choose between hypothetical treatment options, each of which was defined by 5 variable attributes—PFS, mode of administration, typical severity of diarrhea, chance of serious infection, and chance of organ damage.
The attribute patients ranked highest was a change in PFS from 10 months to 60 months. This was followed by a change in infection risk from 30% to 0%, a change in the risk of organ damage from 8% to 0%, a change in diarrhea from severe to none, and a change in the mode of administration from intravenous to oral.
On average, a gain in PFS of 35.9 months was needed for patients to accept a 30% risk of serious infection. A gain in PFS of 26.3 months was needed for patients to accept an 8% risk of organ damage.
A gain in PFS of 21.6 months was needed for patients to accept severe diarrhea. And a gain in PFS of 3.5 months was needed for patients to accept the change from a daily pill to intravenous administration for 6 months.
There were no significant differences in preferences among treatment-naïve patients, first-line patients, and relapsed/refractory patients.
Impact of cost
When the researchers conducted a supplemental cost analysis, they found that out-of-pocket cost had a substantial impact on treatment choice.
The cost analysis included 2 treatments—medicines A and B. Based on the prior analysis, the researchers predicted that 91% of patients would choose medicine B if cost were not a concern because B offered longer PFS than A.
“We used the results from the discrete-choice experiment to forecast the probability that a respondent would pick each hypothetical drug without any mention of cost and then compared that to the choices people made when out-of-pocket costs for these medicines were included,” Dr Mansfield explained.
Patients were asked to choose between medicines A and B under 2 circumstances in which B cost more than A.
When medicine B had a monthly out-of-pocket cost that was $75 more than medicine A, 50% of patients chose medicine A.
When medicine B had a monthly out-of-pocket cost that was $400 more than medicine A, 74% of patients chose medicine A.
“Cost is clearly something that has an impact,” Dr Mansfield said. “When patients get prescribed something they can’t afford, they have to make very difficult choices.”
Dr Mansfield and her colleagues believe their findings will help doctors and patients focus on treatments that account for a patient’s unique circumstances and goals.
“Patients don’t always know that they could be making these tradeoffs,” Dr Mansfield said. “We hope that our findings can help doctors to have frank discussions with their patients about the differences between treatments and how these might affect their lives.” ![]()
New research suggests patients with chronic lymphocytic leukemia (CLL) are willing to trade treatment efficacy for a reduced risk of side effects, but the cost of treatment may trump other factors.
The patients studied placed the highest value on treatments that deliver the longest progression-free survival (PFS), but the patients were also willing to swap some efficacy for a reduced risk of serious adverse events (AEs).
Study results also indicated that factoring out-of-pocket costs into the decision-making process can significantly influence a patient’s choice of treatment.
Carol Mansfield, PhD, of RTI Health Solutions in Research Triangle Park, North Carolina, and her colleagues conducted this study and reported the results in Blood Advances. The study was supported by funding from Genentech, Inc., to RTI Health Solutions.
The researchers surveyed 384 patients with CLL. Patients were asked to choose between hypothetical treatment options, each of which was defined by 5 variable attributes—PFS, mode of administration, typical severity of diarrhea, chance of serious infection, and chance of organ damage.
The attribute patients ranked highest was a change in PFS from 10 months to 60 months. This was followed by a change in infection risk from 30% to 0%, a change in the risk of organ damage from 8% to 0%, a change in diarrhea from severe to none, and a change in the mode of administration from intravenous to oral.
On average, a gain in PFS of 35.9 months was needed for patients to accept a 30% risk of serious infection. A gain in PFS of 26.3 months was needed for patients to accept an 8% risk of organ damage.
A gain in PFS of 21.6 months was needed for patients to accept severe diarrhea. And a gain in PFS of 3.5 months was needed for patients to accept the change from a daily pill to intravenous administration for 6 months.
There were no significant differences in preferences among treatment-naïve patients, first-line patients, and relapsed/refractory patients.
Impact of cost
When the researchers conducted a supplemental cost analysis, they found that out-of-pocket cost had a substantial impact on treatment choice.
The cost analysis included 2 treatments—medicines A and B. Based on the prior analysis, the researchers predicted that 91% of patients would choose medicine B if cost were not a concern because B offered longer PFS than A.
“We used the results from the discrete-choice experiment to forecast the probability that a respondent would pick each hypothetical drug without any mention of cost and then compared that to the choices people made when out-of-pocket costs for these medicines were included,” Dr Mansfield explained.
Patients were asked to choose between medicines A and B under 2 circumstances in which B cost more than A.
When medicine B had a monthly out-of-pocket cost that was $75 more than medicine A, 50% of patients chose medicine A.
When medicine B had a monthly out-of-pocket cost that was $400 more than medicine A, 74% of patients chose medicine A.
“Cost is clearly something that has an impact,” Dr Mansfield said. “When patients get prescribed something they can’t afford, they have to make very difficult choices.”
Dr Mansfield and her colleagues believe their findings will help doctors and patients focus on treatments that account for a patient’s unique circumstances and goals.
“Patients don’t always know that they could be making these tradeoffs,” Dr Mansfield said. “We hope that our findings can help doctors to have frank discussions with their patients about the differences between treatments and how these might affect their lives.” ![]()
New research suggests patients with chronic lymphocytic leukemia (CLL) are willing to trade treatment efficacy for a reduced risk of side effects, but the cost of treatment may trump other factors.
The patients studied placed the highest value on treatments that deliver the longest progression-free survival (PFS), but the patients were also willing to swap some efficacy for a reduced risk of serious adverse events (AEs).
Study results also indicated that factoring out-of-pocket costs into the decision-making process can significantly influence a patient’s choice of treatment.
Carol Mansfield, PhD, of RTI Health Solutions in Research Triangle Park, North Carolina, and her colleagues conducted this study and reported the results in Blood Advances. The study was supported by funding from Genentech, Inc., to RTI Health Solutions.
The researchers surveyed 384 patients with CLL. Patients were asked to choose between hypothetical treatment options, each of which was defined by 5 variable attributes—PFS, mode of administration, typical severity of diarrhea, chance of serious infection, and chance of organ damage.
The attribute patients ranked highest was a change in PFS from 10 months to 60 months. This was followed by a change in infection risk from 30% to 0%, a change in the risk of organ damage from 8% to 0%, a change in diarrhea from severe to none, and a change in the mode of administration from intravenous to oral.
On average, a gain in PFS of 35.9 months was needed for patients to accept a 30% risk of serious infection. A gain in PFS of 26.3 months was needed for patients to accept an 8% risk of organ damage.
A gain in PFS of 21.6 months was needed for patients to accept severe diarrhea. And a gain in PFS of 3.5 months was needed for patients to accept the change from a daily pill to intravenous administration for 6 months.
There were no significant differences in preferences among treatment-naïve patients, first-line patients, and relapsed/refractory patients.
Impact of cost
When the researchers conducted a supplemental cost analysis, they found that out-of-pocket cost had a substantial impact on treatment choice.
The cost analysis included 2 treatments—medicines A and B. Based on the prior analysis, the researchers predicted that 91% of patients would choose medicine B if cost were not a concern because B offered longer PFS than A.
“We used the results from the discrete-choice experiment to forecast the probability that a respondent would pick each hypothetical drug without any mention of cost and then compared that to the choices people made when out-of-pocket costs for these medicines were included,” Dr Mansfield explained.
Patients were asked to choose between medicines A and B under 2 circumstances in which B cost more than A.
When medicine B had a monthly out-of-pocket cost that was $75 more than medicine A, 50% of patients chose medicine A.
When medicine B had a monthly out-of-pocket cost that was $400 more than medicine A, 74% of patients chose medicine A.
“Cost is clearly something that has an impact,” Dr Mansfield said. “When patients get prescribed something they can’t afford, they have to make very difficult choices.”
Dr Mansfield and her colleagues believe their findings will help doctors and patients focus on treatments that account for a patient’s unique circumstances and goals.
“Patients don’t always know that they could be making these tradeoffs,” Dr Mansfield said. “We hope that our findings can help doctors to have frank discussions with their patients about the differences between treatments and how these might affect their lives.” ![]()
Physicians do not trust bone biopsy culture data
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I approach the end of my summer research project, my team and I have reflected on what we’ve learned from both the research itself and the experience of working on the project.
As work-life balance is important to me, I would usually I would balk at the idea of sacrificing my personal time, but in this case, I am driven by a sense of ownership and pride over the project that I haven’t felt with past projects. I truly believe the results of this research have the potential to change the way physicians think about and manage patients with osteomyelitis, and I am eager to publish our results and attend conferences where I can present and discuss the findings with the medical community.
We hypothesized that the use of image-guided bone biopsies in patients with non-vertebral osteomyelitis would not have a significant impact on antibiotic management. Our results showed that physicians usually do not trust culture data provided by bone biopsy results. Negative bone cultures almost never lead physicians to discontinue antibiotics due to the low yield and reliability of bone biopsy culture data. Similarly, positive cultures almost never lead physicians to prescribe targeted antibiotics. 75% of the patients in our study had contiguous osteomyelitis caused by an overlying ulcer (e.g., diabetic foot ulcers or sacral decubitus ulcers). Exposure of the wound to the outside world often results in polymicrobial infections, and as such physicians rarely narrowed antibiotic coverage when a single organism was cultured. We also found that empiric antibiotic therapy adequately treated cultured micro-organisms in 95% of cases.
While many questions remained unanswered by this study, our results are an important contribution to the body of evidence that image-guided bone biopsies have low utility in the management of contiguous non-vertebral osteomyelitis. I look forward to seeing how the results of future research will compare with our findings. I am grateful to have had the opportunity to work in such an exciting area of research and I hope to continue participating in research projects throughout my medical career.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I approach the end of my summer research project, my team and I have reflected on what we’ve learned from both the research itself and the experience of working on the project.
As work-life balance is important to me, I would usually I would balk at the idea of sacrificing my personal time, but in this case, I am driven by a sense of ownership and pride over the project that I haven’t felt with past projects. I truly believe the results of this research have the potential to change the way physicians think about and manage patients with osteomyelitis, and I am eager to publish our results and attend conferences where I can present and discuss the findings with the medical community.
We hypothesized that the use of image-guided bone biopsies in patients with non-vertebral osteomyelitis would not have a significant impact on antibiotic management. Our results showed that physicians usually do not trust culture data provided by bone biopsy results. Negative bone cultures almost never lead physicians to discontinue antibiotics due to the low yield and reliability of bone biopsy culture data. Similarly, positive cultures almost never lead physicians to prescribe targeted antibiotics. 75% of the patients in our study had contiguous osteomyelitis caused by an overlying ulcer (e.g., diabetic foot ulcers or sacral decubitus ulcers). Exposure of the wound to the outside world often results in polymicrobial infections, and as such physicians rarely narrowed antibiotic coverage when a single organism was cultured. We also found that empiric antibiotic therapy adequately treated cultured micro-organisms in 95% of cases.
While many questions remained unanswered by this study, our results are an important contribution to the body of evidence that image-guided bone biopsies have low utility in the management of contiguous non-vertebral osteomyelitis. I look forward to seeing how the results of future research will compare with our findings. I am grateful to have had the opportunity to work in such an exciting area of research and I hope to continue participating in research projects throughout my medical career.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I approach the end of my summer research project, my team and I have reflected on what we’ve learned from both the research itself and the experience of working on the project.
As work-life balance is important to me, I would usually I would balk at the idea of sacrificing my personal time, but in this case, I am driven by a sense of ownership and pride over the project that I haven’t felt with past projects. I truly believe the results of this research have the potential to change the way physicians think about and manage patients with osteomyelitis, and I am eager to publish our results and attend conferences where I can present and discuss the findings with the medical community.
We hypothesized that the use of image-guided bone biopsies in patients with non-vertebral osteomyelitis would not have a significant impact on antibiotic management. Our results showed that physicians usually do not trust culture data provided by bone biopsy results. Negative bone cultures almost never lead physicians to discontinue antibiotics due to the low yield and reliability of bone biopsy culture data. Similarly, positive cultures almost never lead physicians to prescribe targeted antibiotics. 75% of the patients in our study had contiguous osteomyelitis caused by an overlying ulcer (e.g., diabetic foot ulcers or sacral decubitus ulcers). Exposure of the wound to the outside world often results in polymicrobial infections, and as such physicians rarely narrowed antibiotic coverage when a single organism was cultured. We also found that empiric antibiotic therapy adequately treated cultured micro-organisms in 95% of cases.
While many questions remained unanswered by this study, our results are an important contribution to the body of evidence that image-guided bone biopsies have low utility in the management of contiguous non-vertebral osteomyelitis. I look forward to seeing how the results of future research will compare with our findings. I am grateful to have had the opportunity to work in such an exciting area of research and I hope to continue participating in research projects throughout my medical career.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Review suggests low incidence of BIA-ALCL in Canada
Results of a safety review suggest there is a low incidence of breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) in Canada.
Health Canada undertook the review because of an increase in reporting of BIA-ALCL internationally.
The review showed that 5 confirmed cases of BIA-ALCL have been reported by Canadian manufacturers in the last 10 years.
This is equal to 1 case of BIA-ALCL per 77,190 implants sold, or 0.0013%.
However, Health Canada acknowledges that some cases may not have been reported to the manufacturers or Health Canada.
Available data suggest that BIA-ALCL is more frequently reported with textured surface implants than smooth surface implants. Textured surface implants account for a quarter of all breast implants sold in Canada.
Four of the 5 reported Canadian cases of BIA-ALCL involved textured implants. The surface type was not reported in the remaining case.
The rate of occurrence of BIA‑ALCL per textured implant sold in Canada is 1 case per 24,177 or 0.0041%.
As a result of its safety review, Health Canada is working with manufacturers to update the safety information on the product labeling for all breast implants.
The agency is also communicating this safety information to Canadians through the Recalls and Safety Alerts database on the Healthy Canadians website.
Health Canada continues to monitor the safety profile of breast implants through its post-market surveillance program.
The agency will also monitor cases of BIA-ALCL through an annual follow-up with manufacturers of breast implants.
Health Canada is recommending that healthcare professionals learn about the signs, symptoms, and testing steps to recognize and diagnose BIA‑ALCL.
In addition, healthcare professionals in Canada should report incidents of BIA-ALCL to Health Canada. These reports should include specific details, such as symptoms, how BIA-ALCL was discovered, the age of the patient at implantation, prior implant history, the age of the patient at discovery, tests conducted to diagnose BIA-ALCL, staging information, the course of therapy, and clinical outcomes.
Reports can be made by calling Health Canada at 1-866-234-2345. Alternatively, visit Health Canada’s webpage on Adverse Reaction Reporting for information on how to report online, by mail, or by fax. ![]()
Results of a safety review suggest there is a low incidence of breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) in Canada.
Health Canada undertook the review because of an increase in reporting of BIA-ALCL internationally.
The review showed that 5 confirmed cases of BIA-ALCL have been reported by Canadian manufacturers in the last 10 years.
This is equal to 1 case of BIA-ALCL per 77,190 implants sold, or 0.0013%.
However, Health Canada acknowledges that some cases may not have been reported to the manufacturers or Health Canada.
Available data suggest that BIA-ALCL is more frequently reported with textured surface implants than smooth surface implants. Textured surface implants account for a quarter of all breast implants sold in Canada.
Four of the 5 reported Canadian cases of BIA-ALCL involved textured implants. The surface type was not reported in the remaining case.
The rate of occurrence of BIA‑ALCL per textured implant sold in Canada is 1 case per 24,177 or 0.0041%.
As a result of its safety review, Health Canada is working with manufacturers to update the safety information on the product labeling for all breast implants.
The agency is also communicating this safety information to Canadians through the Recalls and Safety Alerts database on the Healthy Canadians website.
Health Canada continues to monitor the safety profile of breast implants through its post-market surveillance program.
The agency will also monitor cases of BIA-ALCL through an annual follow-up with manufacturers of breast implants.
Health Canada is recommending that healthcare professionals learn about the signs, symptoms, and testing steps to recognize and diagnose BIA‑ALCL.
In addition, healthcare professionals in Canada should report incidents of BIA-ALCL to Health Canada. These reports should include specific details, such as symptoms, how BIA-ALCL was discovered, the age of the patient at implantation, prior implant history, the age of the patient at discovery, tests conducted to diagnose BIA-ALCL, staging information, the course of therapy, and clinical outcomes.
Reports can be made by calling Health Canada at 1-866-234-2345. Alternatively, visit Health Canada’s webpage on Adverse Reaction Reporting for information on how to report online, by mail, or by fax. ![]()
Results of a safety review suggest there is a low incidence of breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) in Canada.
Health Canada undertook the review because of an increase in reporting of BIA-ALCL internationally.
The review showed that 5 confirmed cases of BIA-ALCL have been reported by Canadian manufacturers in the last 10 years.
This is equal to 1 case of BIA-ALCL per 77,190 implants sold, or 0.0013%.
However, Health Canada acknowledges that some cases may not have been reported to the manufacturers or Health Canada.
Available data suggest that BIA-ALCL is more frequently reported with textured surface implants than smooth surface implants. Textured surface implants account for a quarter of all breast implants sold in Canada.
Four of the 5 reported Canadian cases of BIA-ALCL involved textured implants. The surface type was not reported in the remaining case.
The rate of occurrence of BIA‑ALCL per textured implant sold in Canada is 1 case per 24,177 or 0.0041%.
As a result of its safety review, Health Canada is working with manufacturers to update the safety information on the product labeling for all breast implants.
The agency is also communicating this safety information to Canadians through the Recalls and Safety Alerts database on the Healthy Canadians website.
Health Canada continues to monitor the safety profile of breast implants through its post-market surveillance program.
The agency will also monitor cases of BIA-ALCL through an annual follow-up with manufacturers of breast implants.
Health Canada is recommending that healthcare professionals learn about the signs, symptoms, and testing steps to recognize and diagnose BIA‑ALCL.
In addition, healthcare professionals in Canada should report incidents of BIA-ALCL to Health Canada. These reports should include specific details, such as symptoms, how BIA-ALCL was discovered, the age of the patient at implantation, prior implant history, the age of the patient at discovery, tests conducted to diagnose BIA-ALCL, staging information, the course of therapy, and clinical outcomes.
Reports can be made by calling Health Canada at 1-866-234-2345. Alternatively, visit Health Canada’s webpage on Adverse Reaction Reporting for information on how to report online, by mail, or by fax. ![]()