User login
Ultraprocessed Foods Associated With Relapse Risk in Crohn’s Disease
VIENNA —
Certain subgroups of UPFs, specifically bread, pastries, and starch as well as oil and spreads, exhibited the strongest association with relapse risks of approximately threefold.
“In addition to treating active inflammatory bowel disease (IBD), we want to maintain remission for the long term,” Chen Sarbagili Shabat, PhD, clinical dietitian from Tel Aviv Medical Center in Israel, said in an interview. “It’s highly important. We know environmental factors are associated with the disease, which is why we can treat active disease with diet. Likewise, we can manage CD in a remission state with diet.”
This is the first prospective study of this particular level of UPFs in people with Crohn’s disease who are in remission, noted Shabat, who presented the findings at United European Gastroenterology (UEG) Week 2024.
Previously, a meta-analysis of prospective cohort studies showed that a diet high in UPFs is associated with a 70% increased risk for development of CD, and a longitudinal study showed that “Western” dietary patterns were associated with relapse risk in patients with IBD, Shabat reported.
Effect of High vs Low Intake of UPFs
The current single-center, prospective cohort study, followed 111 patients with CD every 3 months until relapse for up to 1 year.
Participants were aged 18-75 years (mean age, 38 years), with a median disease duration of 8.7 years. They were required to have maintained steroid-free clinical remission (Harvey-Bradshaw Index (HBI), < 5) for 3 months or more. The median duration of clinical remission at recruitment was 3 years.
Data collection included HBI level, medication type and dosage to ensure constant therapy and full compliance, and a stool sample for fecal calprotectin measurement.
The primary outcome comprised a clinical relapse HBI ≥ 5 over the 12-month follow-up or a change in disease activity requiring a change in medication, hospitalization, or any IBD-related surgery.
Participants were asked to complete a processed food questionnaire to assess the intake of UPFs and a food frequency questionnaire to assess the total intake of energy, macronutrients, and micronutrients. UPFs were divided into high and low intakes using a median cutoff of 3.6 servings/day.
The low intake group included 57 participants, and the high intake group included 54.
A total of 24 patients (21.6%) experienced a clinical relapse event, 7 in the low intake group vs 17 in the high intake group (hazard ratio [HR], 3.86; 95% CI, 1.30-11.47; P = .015 after adjustments).
In a subset of 97 patients with baseline fecal calprotectin measurements, 6 (n = 50) in the low intake group experienced a clinical relapse vs 15 (n = 47) in the high intake group (HR, 4.32; 95% CI, 1.36-13.73; P = .013 after adjustments).
Fecal calprotectin results were also suggestive of an association between high intake of UPFs and gut inflammation, Shabat reported.
Food Groups and Emulsifiers
UPFs were divided into subgroups: Bread, pastries, and starch; oils and spreads; ultraprocessed meat; sweet products and desserts; and ultraprocessed beverages.
The highest associations with relapse were in the subgroup of bread, pastries, and starch (HR, 3.37; 95% CI, 1.26-8.25) and the subgroup of oils and spreads (HR, 2.76; 95% CI, 1.02-7.45).
“The selection of healthy food is highly important, especially since we know that certain food ingredients can contribute to the pathogenesis of CD,” Shabat said. Patients can use partial enteral nutrition to provide 40%-50% of daily caloric intake in order to maintain remission, but she acknowledged it can be really difficult to adhere to.
She concluded by asserting that the study results, along with future research, should contribute to establishing nutritional guidelines to reduce UPF consumption in patients with CD in order to maintain remission.
Commenting on the study, Kevin Whelan, PhD, professor of dietetics and head of the Department of Nutritional Sciences at King’s College London in England, said that he was intrigued by the subgroup analysis that showed breads, pastries, oils, and spreads as having the strongest association with relapse risk.
He also remarked that these foods almost ubiquitously contain emulsifiers, and so the association might have less to do with UPFs in general and more to do with emulsifiers.
Concurring, Shabat noted that, while emulsifiers can negatively influence the microbiota and the gut barrier function, as well as contribute to intestinal inflammation, further mechanistic studies are required to understand these effects.
We need to determine if all additives have the same effect on the inflammatory process and also need studies looking at UPFs alone, she added.
Shabat reported receiving personal fees from Nestle Health Science (Wolfson Medical Center IP) for consulting and speaking and from Takeda and Ferring for speaking. Whelan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA —
Certain subgroups of UPFs, specifically bread, pastries, and starch as well as oil and spreads, exhibited the strongest association with relapse risks of approximately threefold.
“In addition to treating active inflammatory bowel disease (IBD), we want to maintain remission for the long term,” Chen Sarbagili Shabat, PhD, clinical dietitian from Tel Aviv Medical Center in Israel, said in an interview. “It’s highly important. We know environmental factors are associated with the disease, which is why we can treat active disease with diet. Likewise, we can manage CD in a remission state with diet.”
This is the first prospective study of this particular level of UPFs in people with Crohn’s disease who are in remission, noted Shabat, who presented the findings at United European Gastroenterology (UEG) Week 2024.
Previously, a meta-analysis of prospective cohort studies showed that a diet high in UPFs is associated with a 70% increased risk for development of CD, and a longitudinal study showed that “Western” dietary patterns were associated with relapse risk in patients with IBD, Shabat reported.
Effect of High vs Low Intake of UPFs
The current single-center, prospective cohort study, followed 111 patients with CD every 3 months until relapse for up to 1 year.
Participants were aged 18-75 years (mean age, 38 years), with a median disease duration of 8.7 years. They were required to have maintained steroid-free clinical remission (Harvey-Bradshaw Index (HBI), < 5) for 3 months or more. The median duration of clinical remission at recruitment was 3 years.
Data collection included HBI level, medication type and dosage to ensure constant therapy and full compliance, and a stool sample for fecal calprotectin measurement.
The primary outcome comprised a clinical relapse HBI ≥ 5 over the 12-month follow-up or a change in disease activity requiring a change in medication, hospitalization, or any IBD-related surgery.
Participants were asked to complete a processed food questionnaire to assess the intake of UPFs and a food frequency questionnaire to assess the total intake of energy, macronutrients, and micronutrients. UPFs were divided into high and low intakes using a median cutoff of 3.6 servings/day.
The low intake group included 57 participants, and the high intake group included 54.
A total of 24 patients (21.6%) experienced a clinical relapse event, 7 in the low intake group vs 17 in the high intake group (hazard ratio [HR], 3.86; 95% CI, 1.30-11.47; P = .015 after adjustments).
In a subset of 97 patients with baseline fecal calprotectin measurements, 6 (n = 50) in the low intake group experienced a clinical relapse vs 15 (n = 47) in the high intake group (HR, 4.32; 95% CI, 1.36-13.73; P = .013 after adjustments).
Fecal calprotectin results were also suggestive of an association between high intake of UPFs and gut inflammation, Shabat reported.
Food Groups and Emulsifiers
UPFs were divided into subgroups: Bread, pastries, and starch; oils and spreads; ultraprocessed meat; sweet products and desserts; and ultraprocessed beverages.
The highest associations with relapse were in the subgroup of bread, pastries, and starch (HR, 3.37; 95% CI, 1.26-8.25) and the subgroup of oils and spreads (HR, 2.76; 95% CI, 1.02-7.45).
“The selection of healthy food is highly important, especially since we know that certain food ingredients can contribute to the pathogenesis of CD,” Shabat said. Patients can use partial enteral nutrition to provide 40%-50% of daily caloric intake in order to maintain remission, but she acknowledged it can be really difficult to adhere to.
She concluded by asserting that the study results, along with future research, should contribute to establishing nutritional guidelines to reduce UPF consumption in patients with CD in order to maintain remission.
Commenting on the study, Kevin Whelan, PhD, professor of dietetics and head of the Department of Nutritional Sciences at King’s College London in England, said that he was intrigued by the subgroup analysis that showed breads, pastries, oils, and spreads as having the strongest association with relapse risk.
He also remarked that these foods almost ubiquitously contain emulsifiers, and so the association might have less to do with UPFs in general and more to do with emulsifiers.
Concurring, Shabat noted that, while emulsifiers can negatively influence the microbiota and the gut barrier function, as well as contribute to intestinal inflammation, further mechanistic studies are required to understand these effects.
We need to determine if all additives have the same effect on the inflammatory process and also need studies looking at UPFs alone, she added.
Shabat reported receiving personal fees from Nestle Health Science (Wolfson Medical Center IP) for consulting and speaking and from Takeda and Ferring for speaking. Whelan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA —
Certain subgroups of UPFs, specifically bread, pastries, and starch as well as oil and spreads, exhibited the strongest association with relapse risks of approximately threefold.
“In addition to treating active inflammatory bowel disease (IBD), we want to maintain remission for the long term,” Chen Sarbagili Shabat, PhD, clinical dietitian from Tel Aviv Medical Center in Israel, said in an interview. “It’s highly important. We know environmental factors are associated with the disease, which is why we can treat active disease with diet. Likewise, we can manage CD in a remission state with diet.”
This is the first prospective study of this particular level of UPFs in people with Crohn’s disease who are in remission, noted Shabat, who presented the findings at United European Gastroenterology (UEG) Week 2024.
Previously, a meta-analysis of prospective cohort studies showed that a diet high in UPFs is associated with a 70% increased risk for development of CD, and a longitudinal study showed that “Western” dietary patterns were associated with relapse risk in patients with IBD, Shabat reported.
Effect of High vs Low Intake of UPFs
The current single-center, prospective cohort study, followed 111 patients with CD every 3 months until relapse for up to 1 year.
Participants were aged 18-75 years (mean age, 38 years), with a median disease duration of 8.7 years. They were required to have maintained steroid-free clinical remission (Harvey-Bradshaw Index (HBI), < 5) for 3 months or more. The median duration of clinical remission at recruitment was 3 years.
Data collection included HBI level, medication type and dosage to ensure constant therapy and full compliance, and a stool sample for fecal calprotectin measurement.
The primary outcome comprised a clinical relapse HBI ≥ 5 over the 12-month follow-up or a change in disease activity requiring a change in medication, hospitalization, or any IBD-related surgery.
Participants were asked to complete a processed food questionnaire to assess the intake of UPFs and a food frequency questionnaire to assess the total intake of energy, macronutrients, and micronutrients. UPFs were divided into high and low intakes using a median cutoff of 3.6 servings/day.
The low intake group included 57 participants, and the high intake group included 54.
A total of 24 patients (21.6%) experienced a clinical relapse event, 7 in the low intake group vs 17 in the high intake group (hazard ratio [HR], 3.86; 95% CI, 1.30-11.47; P = .015 after adjustments).
In a subset of 97 patients with baseline fecal calprotectin measurements, 6 (n = 50) in the low intake group experienced a clinical relapse vs 15 (n = 47) in the high intake group (HR, 4.32; 95% CI, 1.36-13.73; P = .013 after adjustments).
Fecal calprotectin results were also suggestive of an association between high intake of UPFs and gut inflammation, Shabat reported.
Food Groups and Emulsifiers
UPFs were divided into subgroups: Bread, pastries, and starch; oils and spreads; ultraprocessed meat; sweet products and desserts; and ultraprocessed beverages.
The highest associations with relapse were in the subgroup of bread, pastries, and starch (HR, 3.37; 95% CI, 1.26-8.25) and the subgroup of oils and spreads (HR, 2.76; 95% CI, 1.02-7.45).
“The selection of healthy food is highly important, especially since we know that certain food ingredients can contribute to the pathogenesis of CD,” Shabat said. Patients can use partial enteral nutrition to provide 40%-50% of daily caloric intake in order to maintain remission, but she acknowledged it can be really difficult to adhere to.
She concluded by asserting that the study results, along with future research, should contribute to establishing nutritional guidelines to reduce UPF consumption in patients with CD in order to maintain remission.
Commenting on the study, Kevin Whelan, PhD, professor of dietetics and head of the Department of Nutritional Sciences at King’s College London in England, said that he was intrigued by the subgroup analysis that showed breads, pastries, oils, and spreads as having the strongest association with relapse risk.
He also remarked that these foods almost ubiquitously contain emulsifiers, and so the association might have less to do with UPFs in general and more to do with emulsifiers.
Concurring, Shabat noted that, while emulsifiers can negatively influence the microbiota and the gut barrier function, as well as contribute to intestinal inflammation, further mechanistic studies are required to understand these effects.
We need to determine if all additives have the same effect on the inflammatory process and also need studies looking at UPFs alone, she added.
Shabat reported receiving personal fees from Nestle Health Science (Wolfson Medical Center IP) for consulting and speaking and from Takeda and Ferring for speaking. Whelan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM UEG 2024
Starting Mammograms at Age 40: Will Women Benefit?
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.
The Impact of a Metformin Recall on Patient Hemoglobin A1c Levels at a VA Network
About 1 in 10 Americans have diabetes mellitus (DM), of which about 90% to 95% are diagnosed with type 2 DM (T2DM) and veterans are disproportionately affected.1,2 About 25% enrolled in the Veterans Health Administration (VHA) have T2DM, which has been attributed to exposure to herbicides (eg, Agent Orange), decreased physical activity resulting from past physical strain, chronic pain, and other physical limitations resulting from military service.3-5
Pharmacologic management of DM is guided by the effectiveness of lifestyle interventions and comorbid diagnoses. Current DM management guidelines recommend patients with comorbid atherosclerotic cardiovascular disease, chronic kidney disease, or congestive heart failure receive first-line diabetes therapy with a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or glucagon-like peptide-1 receptor (GLP-1) agonist.
Metformin remains a first-line pharmacologic option for the treatment of T2DM with the goal of achieving glycemic management when lifestyle interventions are insufficient.6,7 Newer antihyperglycemic therapies have been studied as adjunct therapy to metformin. However, there is limited literature comparing metformin directly to other medication classes for the treatment of T2DM.8-13 A systematic review of treatment-naive patients found HbA1c reductions were similar whether patients received metformin vs an SGLT-2 inhibitor, GLP-1 agonist, sulfonylurea, or thiazolidinedione monotherapy.10 The analysis found dipeptidyl-peptidase-4 (DPP-4) inhibitors had inferior HbA1c reduction compared to metformin.10 A Japanese systematic review compared metformin to thiazolidinediones, sulfonylureas, glinides, DPP-4 inhibitors, α-glucosidase inhibitors, or SGLT-2 inhibitors for ≥ 12 weeks but found no statistically significant differences in
On May 28, 2020, the US Food and Drug Administration (FDA) asked 5 pharmaceutical companies to voluntarily recall certain formulations of metformin. This action was taken when FDA testing revealed unacceptably high levels of N-Nitrosodimethylamine, a probable carcinogen.14 This FDA recall of metformin extended-release, referred to as metformin sustained-action (SA) within the VHA electronic medication file but the same type of formulation, prompted clinicians to revisit and revise the pharmacologic regimens of patients taking the drug. Because of the paucity of head-to-head trials comparing metformin with newer alternative antihyperglycemic therapies, the effect of treatment change was unknown. In response, we aimed to establish a data registry within Veterans Integrated Service Network (VISN) 6.
Registry Development
The VISN 6 registry was established to gather long-term, observational, head-to-head data that would allow review of HbA1c levels before and after the recall, as well as HbA1c levels broken down by the agent that patients were switched to after the recall. Another goal was to explore prescribing trends following the recall.
Data Access Request Tracker approval was obtained and a US Department of Veterans Affairs (VA) Information and Computing Infrastructure workspace was developed to host the registry data. The research cohort was established from this data, and the registry framework was finalized using Structured Query Language (SQL). The SQL coding allows for recurring data updates for all individuals within the cohort including date of birth, race, sex, ethnicity, VHA facility visited, weight, body mass index, HbA1c level, creatinine clearance, serum creatinine, antihyperglycemic medication prescriptions, adverse drug reactions, medication adherence (as defined by ≥ 80% refill history), and hospitalizations related to diabetes. For the purposes of this initial analysis, registry data included demographics, diabetes medications, and HbA1c results.
METHODS
This study was a concurrent, observational, multicenter, registry-based study conducted at the Western North Carolina VA Health Care System (WNCVAHCS). The study was approved by the WNCVAHCS institutional review board and research and development committees.
All patients aged ≥ 18 years with T2DM and receiving health care from VISN 6 facilities who had an active metformin SA prescription on, and 1 year prior to, June 1, 2020 (the initial date VHA began implementing the FDA metformin recall) were entered into the registry. Data from 1 year prior were collected to provide a baseline. Veterans were excluded if they received metformin SA for any indication other than T2DM, there was no pre- or postrecall HbA1c measurement, or death. We included 15,594 VISN 6 veterans.
Registry data were analyzed to determine whether a significant change in HbA1c level occurred after the metformin recall and in response to alternative agents being prescribed. Data from veterans who met all inclusion criteria were assessed during the year before and after June 1, 2020. Demographic data were analyzed using frequency and descriptive statistics. The Shapiro Wilkes test was performed, and data were found to be nonparametric; therefore the Wilcoxon signed-rank test was used to evaluate the hypothesis that HbA1c levels were not impacted by the recall.
Our sample size allowed us to create exact matched pairs of 9130 individuals and utilize rank-biserial correlation to establish effect size. Following this initial population-level test, we constructed 2 models. The first, a linear mixed-effects model, focused solely on the interaction effects between the pre- and postrecall periods and various medication classes on HbA1c levels. Second, we constructed a random-effects within-between model (REWB) to evaluate the impact ofmedication classes and demographic variables. Statistical significance was measured at P < .05 with conservative power at .90. The effect size was set to 1.0, reflecting a minimum clinically important difference. Literature establishes 0.5 as a modest level of HbA1c improvement and 1.0 as a clinically significant improvement.
RESULTS
Preliminary results included 15,594 veterans who received a metformin SA prescription as of June 1, 2020 from VISN 6 facilities; 15,392 veterans had a drug exposure end on June 1, 2020, indicating their standard therapy of metformin SA was discontinued following the FDA recall. Two hundred and two veterans were excluded from the registry because they continued to receive metformin SA from existing stock at a VISN6 facility.

Wilcoxon Signed-Rank Test
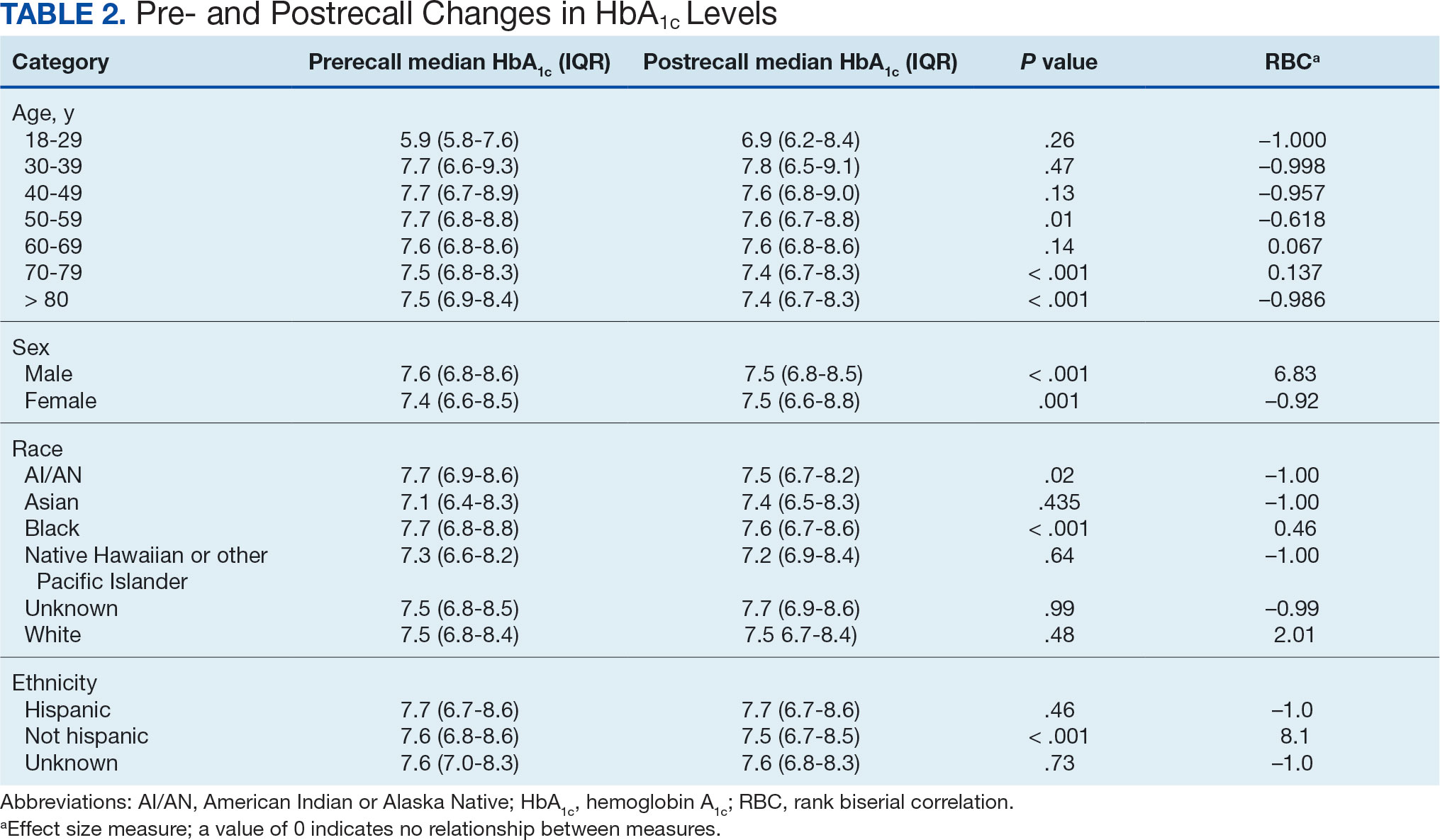
We created exact pairs by iterating the data and finding the closest measurements for each patient before and after the recall. This has the advantage over averaging a patient’s pre- and post-HbA1c levels, as it allows for a rank-biserial correlation. Using the nonparametric Wilcoxon signed-rank test, V was 20,100,707 (P < .001), indicating a significant effect. The –0.29 rank-biserial correlation, which was computed to assess the effect size of the recall, suggests that the median HbA1c level was lower postrecall vs prerecall. The magnitude of the correlation suggests a moderate effect size, and while the recall had a noticeable impact at a population level, it was not extreme (Table 2).
Linear Mixed-Effects Model
The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We employed a linear mixed-effects model to investigate the impact that switching from metformin SA to other T2DM medications had on HbA1c levels. The model was adjusted for patient-specific random effects and included interaction terms between the recall period (before and after) and the usage of different T2DM medications.
Model Fit and Random Effects
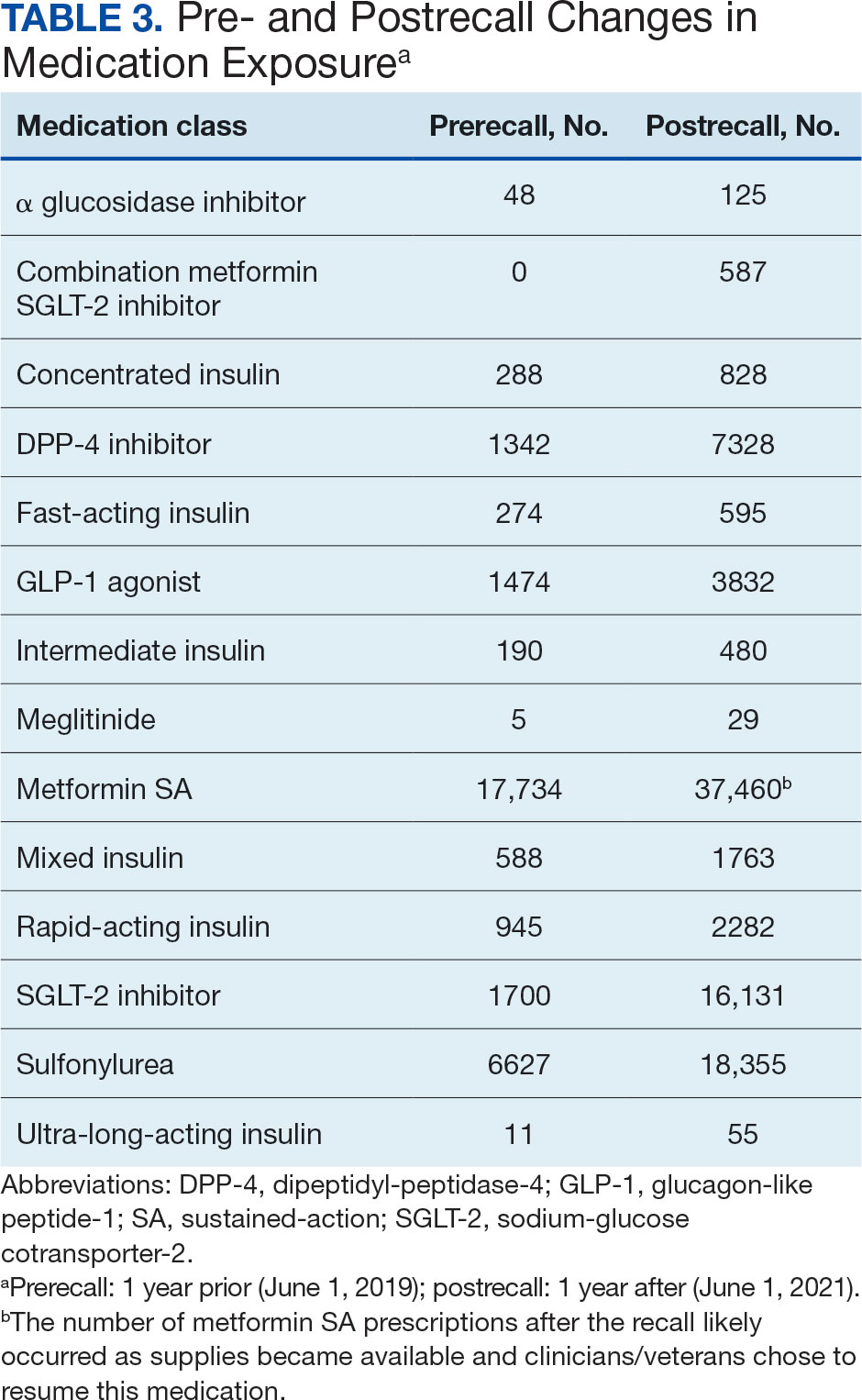
The model demonstrated a residual maximum likelihood criterion of 100,219.7, indicating its fit to the data. Notably, the random effects analysis revealed a substantial variability in baseline HbA1c levels across patients (SD, 0.94), highlighting the importance of individual differences in DM management. Medication classes with zero or near-zero exposure rate were removed. Due to demographic homogeneity, the model did not converge on demographic variables. Veterans were taking a mean of 1.8 T2DM medications and metformin SA was most common (Table 3).
During the postrecall period, metformin SA remained the most frequently prescribed medication class. This may be attributed to the existence of multiple manufacturers of metformin SA, some of which may not have been impacted by the recall. VISN 6 medical centers could have sought metformin SA outside of the usual procurement path following the recall.
Complex Random Effects Model
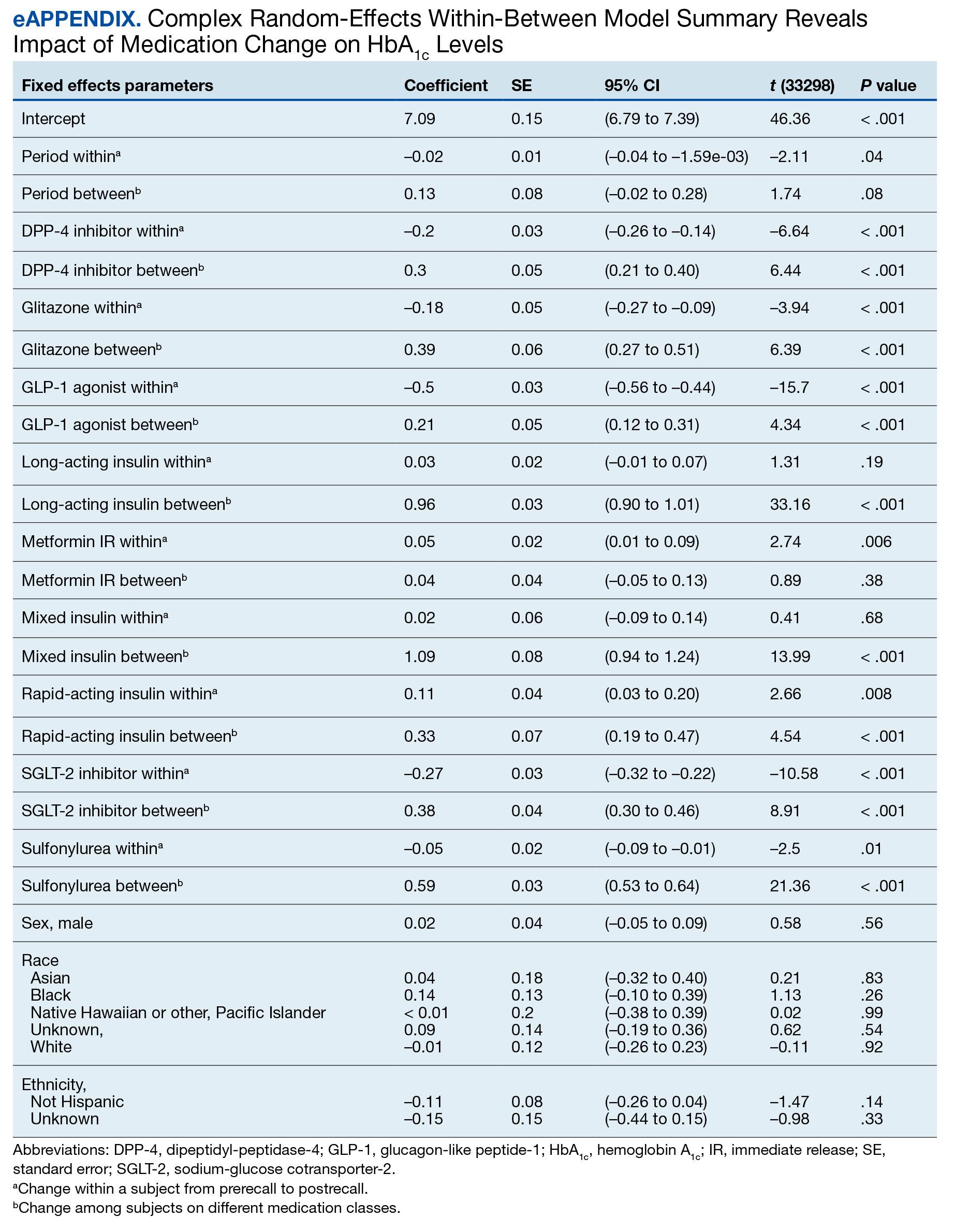
We employed a complex REWB model that evaluated the impact of medication classes on HbA1c levels, accounting for both within and between subject effects of these medications, along with demographic variables (sex, race, and ethnicity) (eAppendix). This model accounts for individual-level changes over time (within-patient effects) and between groups of patients (between-patient effects). This is a more comprehensive model aimed at understanding the broader impact of medications on HbA1c levels across diverse patient groups.
Most demographic categories did not demonstrate significant effects in this model. Black individuals experienced a slight increase in HbA1c levels compared with other racial categories that was not statistically significant. However, this model confirms the findings from the linear mixed-effects model that GLP-1 agonists showed a substantial decrease in HbA1c levels within patients (coefficient –0.5; 95% CI, –0.56 to –0.44; P < .001) and a moderate increase between patients (coefficient, 0.21; 95% CI, 0.12-0.31; P < .001). Additionally, SGLT-2 inhibitors had a notable decrease within patients (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001).Another notable finding with our REWB model is insulin usage was associated with high HbA1c levels, but only between subjects. Long-acting insulin (coefficient, 0.96; 95% CI, 0.90-1.01; P <. 001) and mixed insulin (coefficient, 1.09; 95% CI, 0.94-1.24; P < .001) both displayed marked increases between patients, suggesting future analysis may benefit from stratifying across insulin users and nonusers.
Fixed Effect Analysis
The fixed effects analysis yielded several notable findings. The intercept, representing the mean baseline HbA1c level, was estimated at 7.8% (58 mmol/mol). The coefficient for the period (postrecall) was not statistically significant, indicating no overall change in HbA1c levels from before to after the recall when specific medication classes were not considered (Table 4). Among medication classes examined, several showed significant associations with HbA1c levels. DPP-4 inhibitors and GLP-1 agonists were associated with a decrease in HbA1c levels, with coefficients of −0.08 and −0.24, respectively. Long-acting insulin and metformin immediate-release (IR) were associated with an increase in HbA1c levels, as indicated by their positive coefficients of 0.38 and 0.16, respectively. Mixed insulin formulations and sulfonylureas showed an association with decreased HbA1c levels.
Interaction Effects
The interaction terms between the recall period and the medication classes provided insights into the differential impact of the medication switch postrecall. Notably, the interaction term for long-acting insulin (coefficient, −0.10) was significant, suggesting a differential effect on HbA1c levels postrecall. Other medications, like metformin IR, also exhibited significant interaction effects, indicating changes in the impact on HbA1c levels in the postrecall period. The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We did not address the potential for cross cluster heterogeneity due to different medication classes.
DISCUSSION
This study is an ongoing, concurrent, observational, multicenter, registry-based study consisting of VISN 6 veterans who have T2DM and were prescribed metformin SA on June 1, 2020. This initial aim was to evaluate change in HbA1c levels following the FDA metformin recall. While there was substantial variability in baseline HbA1c levels across the patients, the mean baseline HbA1c level at 7.5% (58 mmol/mol). Patients taking GLP-1 agonists showed substantial decrease in HbA1c levels (coefficient; –0.5; 95% CI, –0.56 to –0.44; P <. 001). Patients taking SGLT-2 inhibitors had a notable decrease in HbA1c (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001). Despite this, the coefficient for the postrecall period was not statistically significant, indicating no overall change in HbA1c levels from pre- to postrecall when specific medication classes were not considered.
Further analysis included assessment of prescribing trends postrecall. There was an increase in SGLT-2 inhibitor, GLP-1 agonist, and DPP-4 inhibitor prescribing. Considering the growing evidence of the cardiovascular and renal benefits of these medication classes, specifically the GLP-1 agonists and SGLT-2 inhibitors, this trend would be expected.
Limitations
This study cohort did not capture veterans with T2DM who transferred their health care to VISN 6 after June 1, 2020, and continued to receive metformin SA from the prior facility. Inclusion of these veterans would have increased the registry population. Additionally, the cohort did not identify veterans who continued to receive metformin SA through a source other than the VA. Without that information, the registry cohort may include veterans thought to have either transitioned to a different therapy or to no other T2DM therapy after the recall.
Given that DM can progress over time, it is possible the transition to a new medication after the recall was the result of suboptimal management, or in response to an adverse effect from a previous medication, and not solely due to the metformin SA recall. In addition, there are several factors that could impact HbA1c level over time that were not accounted for in this study, such as medication adherence and lifestyle modifications.
The notable level of metformin SA prescriptions, despite the recall, may be attributed to several factors. First, not all patients stopped metformin completely. Review of the prescription data indicated that some veterans were provided with limited refills at select VA medical centers that had supplies (medication lots not recalled). Access to a safe supply of metformin SA after the recall may have varied among VISN 6 facilities. It is also possible that as new supplies of metformin SA became available, veterans restarted metformin SA. This may have been resumed while continuing a new medication prescribed at the beginning of the recall. As the year progressed after the recall, an increase in metformin SA prescriptions likely occurred as supplies became available and clinicians/veterans chose to resume this medication therapy.
Conclusions
Results of this initial registry study found no difference in HbA1c levels across the study population after the metformin SA recall. However, there was clinical difference in the HbA1c within veterans prescribed SGLT-2 inhibitors and GLP-1 agonists. As expected, prescribing trends showed an increase in these agents after the recall. With the known benefits of these medications beyond glucose lowering, it is anticipated the cohort of veterans prescribed these medications will continue to grow.
The VISN 6 research registry allowed this study to gain an important snapshot in time following the metformin SA recall, and will serve as an important resource for future DM research endeavors. It will allow for ongoing evaluation of the impact of the transition to alternative T2DM medications after the metformin SA recall. Future exploration will include evaluation of adverse drug reactions, DM-related hospitalizations, emergency department visits related to T2DM, changes in renal function, and cardiovascular events among all diabetes medication classes.
Acknowledgments
The study team thanks the Veterans Affairs Informatics and Computing Infrastructure for their help and expertise throughout this project. The authors acknowledge the contributions of Philip Nelson, PharmD, and Brian Peek, PharmD.
- Centers for Disease Control and Prevention. Type 2 diabetes. Updated April 18, 2023. Accessed September 18, 2023. https://www.cdc.gov/diabetes/basics/type2.html
- ElSayed NA, Aleppo G, Aroda VR, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes Care. 2023;46(Supplement_1):S19-S40. doi:10.2337/dc23-S002
- Liu Y, Sayam S, Shao X, et al. Prevalence of and trends in diabetes among veterans, United States, 2005–2014. Prev Chronic Dis. 2017;14:E135. doi:10.5888/pcd14.170230
- Yi SW, Hong JS, Ohrr H, Yi JJ. Agent Orange exposure and disease prevalence in Korean Vietnam veterans: the Korean veterans health study. Environ Res. 2014;133:56-65. doi:10.1016/j.envres.2014.04.027
- Price LE, Gephart S, Shea K. The VA’s Corporate Data Warehouse: Uses and Implications for Nursing Research and Practice. Nurs Adm Q. 2015;39(4):311-318. doi:10.1097/NAQ.0000000000000118
- ElSayed NA, Aleppo G, Aroda VR, et al. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(suppl 1):S140-S157. doi:10.2337/dc23-S009
- Samson SL, Vellanki P, Blonde L, et al. American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm - 2023 Update. Endocr Pract. 2023;29(5):305-340. doi:10.1016/j.eprac.2023.02.001
- Bennett WL, Maruthur NM, Singh S, et al. Comparative effectiveness and safety of medications for type 2 diabetes: an update including new drugs and 2-drug combinations. Ann Intern Med. 2011;154(9):602-613. doi:10.7326/0003-4819-154-9-201105030-00336
- Bolen S, Feldman L, Vassy J, et al. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007;147(6):386-399. doi:10.7326/0003-4819-147-6-200709180-00178
- Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278-286. doi:10.7326/M20-0864
- Nishimura R, Taniguchi M, Takeshima T, Iwasaki K. Efficacy and safety of metformin versus the other oral antidiabetic drugs in Japanese type 2 diabetes patients: a network meta-analysis. Adv Ther. 2022;39(1):632-654. doi:10.1007/s12325-021-01979-1
- Russell-Jones D, Cuddihy RM, Hanefeld M, et al. Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care. 2012;35(2):252-258. doi:10.2337/dc11-1107
- Umpierrez G, Tofé Povedano S, Pérez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monotherapy versus metformin in type 2 diabetes in a randomized controlled trial (AWARD-3). Diabetes Care. 2014;37(8):2168-2176. doi:10.2337/dc13-2759
- US Food and Drug Administration. FDA alerts patients and health care professionals to nitrosamine impurity findings in certain metformin extended-release products [press release]. May 28, 2020. Accessed October 16, 2024. https://www.fda.gov/news-events/press-announcements/fda-alerts-patients-and-health-care-professionals-nitrosamine-impurity-findings-certain-metformin
- Bell A, Jones K. Explaining fixed effects: random effects modeling of time-series cross-sectional and panel data. PSRM. 2015;3(1):133-153. doi:10.1017/psrm.2014.7
About 1 in 10 Americans have diabetes mellitus (DM), of which about 90% to 95% are diagnosed with type 2 DM (T2DM) and veterans are disproportionately affected.1,2 About 25% enrolled in the Veterans Health Administration (VHA) have T2DM, which has been attributed to exposure to herbicides (eg, Agent Orange), decreased physical activity resulting from past physical strain, chronic pain, and other physical limitations resulting from military service.3-5
Pharmacologic management of DM is guided by the effectiveness of lifestyle interventions and comorbid diagnoses. Current DM management guidelines recommend patients with comorbid atherosclerotic cardiovascular disease, chronic kidney disease, or congestive heart failure receive first-line diabetes therapy with a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or glucagon-like peptide-1 receptor (GLP-1) agonist.
Metformin remains a first-line pharmacologic option for the treatment of T2DM with the goal of achieving glycemic management when lifestyle interventions are insufficient.6,7 Newer antihyperglycemic therapies have been studied as adjunct therapy to metformin. However, there is limited literature comparing metformin directly to other medication classes for the treatment of T2DM.8-13 A systematic review of treatment-naive patients found HbA1c reductions were similar whether patients received metformin vs an SGLT-2 inhibitor, GLP-1 agonist, sulfonylurea, or thiazolidinedione monotherapy.10 The analysis found dipeptidyl-peptidase-4 (DPP-4) inhibitors had inferior HbA1c reduction compared to metformin.10 A Japanese systematic review compared metformin to thiazolidinediones, sulfonylureas, glinides, DPP-4 inhibitors, α-glucosidase inhibitors, or SGLT-2 inhibitors for ≥ 12 weeks but found no statistically significant differences in
On May 28, 2020, the US Food and Drug Administration (FDA) asked 5 pharmaceutical companies to voluntarily recall certain formulations of metformin. This action was taken when FDA testing revealed unacceptably high levels of N-Nitrosodimethylamine, a probable carcinogen.14 This FDA recall of metformin extended-release, referred to as metformin sustained-action (SA) within the VHA electronic medication file but the same type of formulation, prompted clinicians to revisit and revise the pharmacologic regimens of patients taking the drug. Because of the paucity of head-to-head trials comparing metformin with newer alternative antihyperglycemic therapies, the effect of treatment change was unknown. In response, we aimed to establish a data registry within Veterans Integrated Service Network (VISN) 6.
Registry Development
The VISN 6 registry was established to gather long-term, observational, head-to-head data that would allow review of HbA1c levels before and after the recall, as well as HbA1c levels broken down by the agent that patients were switched to after the recall. Another goal was to explore prescribing trends following the recall.
Data Access Request Tracker approval was obtained and a US Department of Veterans Affairs (VA) Information and Computing Infrastructure workspace was developed to host the registry data. The research cohort was established from this data, and the registry framework was finalized using Structured Query Language (SQL). The SQL coding allows for recurring data updates for all individuals within the cohort including date of birth, race, sex, ethnicity, VHA facility visited, weight, body mass index, HbA1c level, creatinine clearance, serum creatinine, antihyperglycemic medication prescriptions, adverse drug reactions, medication adherence (as defined by ≥ 80% refill history), and hospitalizations related to diabetes. For the purposes of this initial analysis, registry data included demographics, diabetes medications, and HbA1c results.
METHODS
This study was a concurrent, observational, multicenter, registry-based study conducted at the Western North Carolina VA Health Care System (WNCVAHCS). The study was approved by the WNCVAHCS institutional review board and research and development committees.
All patients aged ≥ 18 years with T2DM and receiving health care from VISN 6 facilities who had an active metformin SA prescription on, and 1 year prior to, June 1, 2020 (the initial date VHA began implementing the FDA metformin recall) were entered into the registry. Data from 1 year prior were collected to provide a baseline. Veterans were excluded if they received metformin SA for any indication other than T2DM, there was no pre- or postrecall HbA1c measurement, or death. We included 15,594 VISN 6 veterans.
Registry data were analyzed to determine whether a significant change in HbA1c level occurred after the metformin recall and in response to alternative agents being prescribed. Data from veterans who met all inclusion criteria were assessed during the year before and after June 1, 2020. Demographic data were analyzed using frequency and descriptive statistics. The Shapiro Wilkes test was performed, and data were found to be nonparametric; therefore the Wilcoxon signed-rank test was used to evaluate the hypothesis that HbA1c levels were not impacted by the recall.
Our sample size allowed us to create exact matched pairs of 9130 individuals and utilize rank-biserial correlation to establish effect size. Following this initial population-level test, we constructed 2 models. The first, a linear mixed-effects model, focused solely on the interaction effects between the pre- and postrecall periods and various medication classes on HbA1c levels. Second, we constructed a random-effects within-between model (REWB) to evaluate the impact ofmedication classes and demographic variables. Statistical significance was measured at P < .05 with conservative power at .90. The effect size was set to 1.0, reflecting a minimum clinically important difference. Literature establishes 0.5 as a modest level of HbA1c improvement and 1.0 as a clinically significant improvement.
RESULTS
Preliminary results included 15,594 veterans who received a metformin SA prescription as of June 1, 2020 from VISN 6 facilities; 15,392 veterans had a drug exposure end on June 1, 2020, indicating their standard therapy of metformin SA was discontinued following the FDA recall. Two hundred and two veterans were excluded from the registry because they continued to receive metformin SA from existing stock at a VISN6 facility.
Wilcoxon Signed-Rank Test
We created exact pairs by iterating the data and finding the closest measurements for each patient before and after the recall. This has the advantage over averaging a patient’s pre- and post-HbA1c levels, as it allows for a rank-biserial correlation. Using the nonparametric Wilcoxon signed-rank test, V was 20,100,707 (P < .001), indicating a significant effect. The –0.29 rank-biserial correlation, which was computed to assess the effect size of the recall, suggests that the median HbA1c level was lower postrecall vs prerecall. The magnitude of the correlation suggests a moderate effect size, and while the recall had a noticeable impact at a population level, it was not extreme (Table 2).
Linear Mixed-Effects Model
The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We employed a linear mixed-effects model to investigate the impact that switching from metformin SA to other T2DM medications had on HbA1c levels. The model was adjusted for patient-specific random effects and included interaction terms between the recall period (before and after) and the usage of different T2DM medications.
Model Fit and Random Effects
The model demonstrated a residual maximum likelihood criterion of 100,219.7, indicating its fit to the data. Notably, the random effects analysis revealed a substantial variability in baseline HbA1c levels across patients (SD, 0.94), highlighting the importance of individual differences in DM management. Medication classes with zero or near-zero exposure rate were removed. Due to demographic homogeneity, the model did not converge on demographic variables. Veterans were taking a mean of 1.8 T2DM medications and metformin SA was most common (Table 3).
During the postrecall period, metformin SA remained the most frequently prescribed medication class. This may be attributed to the existence of multiple manufacturers of metformin SA, some of which may not have been impacted by the recall. VISN 6 medical centers could have sought metformin SA outside of the usual procurement path following the recall.
Complex Random Effects Model
We employed a complex REWB model that evaluated the impact of medication classes on HbA1c levels, accounting for both within and between subject effects of these medications, along with demographic variables (sex, race, and ethnicity) (eAppendix). This model accounts for individual-level changes over time (within-patient effects) and between groups of patients (between-patient effects). This is a more comprehensive model aimed at understanding the broader impact of medications on HbA1c levels across diverse patient groups.
Most demographic categories did not demonstrate significant effects in this model. Black individuals experienced a slight increase in HbA1c levels compared with other racial categories that was not statistically significant. However, this model confirms the findings from the linear mixed-effects model that GLP-1 agonists showed a substantial decrease in HbA1c levels within patients (coefficient –0.5; 95% CI, –0.56 to –0.44; P < .001) and a moderate increase between patients (coefficient, 0.21; 95% CI, 0.12-0.31; P < .001). Additionally, SGLT-2 inhibitors had a notable decrease within patients (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001).Another notable finding with our REWB model is insulin usage was associated with high HbA1c levels, but only between subjects. Long-acting insulin (coefficient, 0.96; 95% CI, 0.90-1.01; P <. 001) and mixed insulin (coefficient, 1.09; 95% CI, 0.94-1.24; P < .001) both displayed marked increases between patients, suggesting future analysis may benefit from stratifying across insulin users and nonusers.
Fixed Effect Analysis
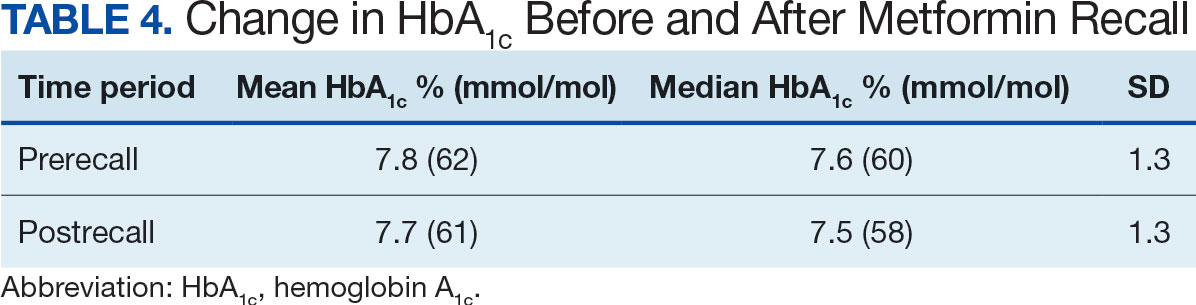
The fixed effects analysis yielded several notable findings. The intercept, representing the mean baseline HbA1c level, was estimated at 7.8% (58 mmol/mol). The coefficient for the period (postrecall) was not statistically significant, indicating no overall change in HbA1c levels from before to after the recall when specific medication classes were not considered (Table 4). Among medication classes examined, several showed significant associations with HbA1c levels. DPP-4 inhibitors and GLP-1 agonists were associated with a decrease in HbA1c levels, with coefficients of −0.08 and −0.24, respectively. Long-acting insulin and metformin immediate-release (IR) were associated with an increase in HbA1c levels, as indicated by their positive coefficients of 0.38 and 0.16, respectively. Mixed insulin formulations and sulfonylureas showed an association with decreased HbA1c levels.
Interaction Effects
The interaction terms between the recall period and the medication classes provided insights into the differential impact of the medication switch postrecall. Notably, the interaction term for long-acting insulin (coefficient, −0.10) was significant, suggesting a differential effect on HbA1c levels postrecall. Other medications, like metformin IR, also exhibited significant interaction effects, indicating changes in the impact on HbA1c levels in the postrecall period. The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We did not address the potential for cross cluster heterogeneity due to different medication classes.
DISCUSSION
This study is an ongoing, concurrent, observational, multicenter, registry-based study consisting of VISN 6 veterans who have T2DM and were prescribed metformin SA on June 1, 2020. This initial aim was to evaluate change in HbA1c levels following the FDA metformin recall. While there was substantial variability in baseline HbA1c levels across the patients, the mean baseline HbA1c level at 7.5% (58 mmol/mol). Patients taking GLP-1 agonists showed substantial decrease in HbA1c levels (coefficient; –0.5; 95% CI, –0.56 to –0.44; P <. 001). Patients taking SGLT-2 inhibitors had a notable decrease in HbA1c (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001). Despite this, the coefficient for the postrecall period was not statistically significant, indicating no overall change in HbA1c levels from pre- to postrecall when specific medication classes were not considered.
Further analysis included assessment of prescribing trends postrecall. There was an increase in SGLT-2 inhibitor, GLP-1 agonist, and DPP-4 inhibitor prescribing. Considering the growing evidence of the cardiovascular and renal benefits of these medication classes, specifically the GLP-1 agonists and SGLT-2 inhibitors, this trend would be expected.
Limitations
This study cohort did not capture veterans with T2DM who transferred their health care to VISN 6 after June 1, 2020, and continued to receive metformin SA from the prior facility. Inclusion of these veterans would have increased the registry population. Additionally, the cohort did not identify veterans who continued to receive metformin SA through a source other than the VA. Without that information, the registry cohort may include veterans thought to have either transitioned to a different therapy or to no other T2DM therapy after the recall.
Given that DM can progress over time, it is possible the transition to a new medication after the recall was the result of suboptimal management, or in response to an adverse effect from a previous medication, and not solely due to the metformin SA recall. In addition, there are several factors that could impact HbA1c level over time that were not accounted for in this study, such as medication adherence and lifestyle modifications.
The notable level of metformin SA prescriptions, despite the recall, may be attributed to several factors. First, not all patients stopped metformin completely. Review of the prescription data indicated that some veterans were provided with limited refills at select VA medical centers that had supplies (medication lots not recalled). Access to a safe supply of metformin SA after the recall may have varied among VISN 6 facilities. It is also possible that as new supplies of metformin SA became available, veterans restarted metformin SA. This may have been resumed while continuing a new medication prescribed at the beginning of the recall. As the year progressed after the recall, an increase in metformin SA prescriptions likely occurred as supplies became available and clinicians/veterans chose to resume this medication therapy.
Conclusions
Results of this initial registry study found no difference in HbA1c levels across the study population after the metformin SA recall. However, there was clinical difference in the HbA1c within veterans prescribed SGLT-2 inhibitors and GLP-1 agonists. As expected, prescribing trends showed an increase in these agents after the recall. With the known benefits of these medications beyond glucose lowering, it is anticipated the cohort of veterans prescribed these medications will continue to grow.
The VISN 6 research registry allowed this study to gain an important snapshot in time following the metformin SA recall, and will serve as an important resource for future DM research endeavors. It will allow for ongoing evaluation of the impact of the transition to alternative T2DM medications after the metformin SA recall. Future exploration will include evaluation of adverse drug reactions, DM-related hospitalizations, emergency department visits related to T2DM, changes in renal function, and cardiovascular events among all diabetes medication classes.
Acknowledgments
The study team thanks the Veterans Affairs Informatics and Computing Infrastructure for their help and expertise throughout this project. The authors acknowledge the contributions of Philip Nelson, PharmD, and Brian Peek, PharmD.
About 1 in 10 Americans have diabetes mellitus (DM), of which about 90% to 95% are diagnosed with type 2 DM (T2DM) and veterans are disproportionately affected.1,2 About 25% enrolled in the Veterans Health Administration (VHA) have T2DM, which has been attributed to exposure to herbicides (eg, Agent Orange), decreased physical activity resulting from past physical strain, chronic pain, and other physical limitations resulting from military service.3-5
Pharmacologic management of DM is guided by the effectiveness of lifestyle interventions and comorbid diagnoses. Current DM management guidelines recommend patients with comorbid atherosclerotic cardiovascular disease, chronic kidney disease, or congestive heart failure receive first-line diabetes therapy with a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or glucagon-like peptide-1 receptor (GLP-1) agonist.
Metformin remains a first-line pharmacologic option for the treatment of T2DM with the goal of achieving glycemic management when lifestyle interventions are insufficient.6,7 Newer antihyperglycemic therapies have been studied as adjunct therapy to metformin. However, there is limited literature comparing metformin directly to other medication classes for the treatment of T2DM.8-13 A systematic review of treatment-naive patients found HbA1c reductions were similar whether patients received metformin vs an SGLT-2 inhibitor, GLP-1 agonist, sulfonylurea, or thiazolidinedione monotherapy.10 The analysis found dipeptidyl-peptidase-4 (DPP-4) inhibitors had inferior HbA1c reduction compared to metformin.10 A Japanese systematic review compared metformin to thiazolidinediones, sulfonylureas, glinides, DPP-4 inhibitors, α-glucosidase inhibitors, or SGLT-2 inhibitors for ≥ 12 weeks but found no statistically significant differences in
On May 28, 2020, the US Food and Drug Administration (FDA) asked 5 pharmaceutical companies to voluntarily recall certain formulations of metformin. This action was taken when FDA testing revealed unacceptably high levels of N-Nitrosodimethylamine, a probable carcinogen.14 This FDA recall of metformin extended-release, referred to as metformin sustained-action (SA) within the VHA electronic medication file but the same type of formulation, prompted clinicians to revisit and revise the pharmacologic regimens of patients taking the drug. Because of the paucity of head-to-head trials comparing metformin with newer alternative antihyperglycemic therapies, the effect of treatment change was unknown. In response, we aimed to establish a data registry within Veterans Integrated Service Network (VISN) 6.
Registry Development
The VISN 6 registry was established to gather long-term, observational, head-to-head data that would allow review of HbA1c levels before and after the recall, as well as HbA1c levels broken down by the agent that patients were switched to after the recall. Another goal was to explore prescribing trends following the recall.
Data Access Request Tracker approval was obtained and a US Department of Veterans Affairs (VA) Information and Computing Infrastructure workspace was developed to host the registry data. The research cohort was established from this data, and the registry framework was finalized using Structured Query Language (SQL). The SQL coding allows for recurring data updates for all individuals within the cohort including date of birth, race, sex, ethnicity, VHA facility visited, weight, body mass index, HbA1c level, creatinine clearance, serum creatinine, antihyperglycemic medication prescriptions, adverse drug reactions, medication adherence (as defined by ≥ 80% refill history), and hospitalizations related to diabetes. For the purposes of this initial analysis, registry data included demographics, diabetes medications, and HbA1c results.
METHODS
This study was a concurrent, observational, multicenter, registry-based study conducted at the Western North Carolina VA Health Care System (WNCVAHCS). The study was approved by the WNCVAHCS institutional review board and research and development committees.
All patients aged ≥ 18 years with T2DM and receiving health care from VISN 6 facilities who had an active metformin SA prescription on, and 1 year prior to, June 1, 2020 (the initial date VHA began implementing the FDA metformin recall) were entered into the registry. Data from 1 year prior were collected to provide a baseline. Veterans were excluded if they received metformin SA for any indication other than T2DM, there was no pre- or postrecall HbA1c measurement, or death. We included 15,594 VISN 6 veterans.
Registry data were analyzed to determine whether a significant change in HbA1c level occurred after the metformin recall and in response to alternative agents being prescribed. Data from veterans who met all inclusion criteria were assessed during the year before and after June 1, 2020. Demographic data were analyzed using frequency and descriptive statistics. The Shapiro Wilkes test was performed, and data were found to be nonparametric; therefore the Wilcoxon signed-rank test was used to evaluate the hypothesis that HbA1c levels were not impacted by the recall.
Our sample size allowed us to create exact matched pairs of 9130 individuals and utilize rank-biserial correlation to establish effect size. Following this initial population-level test, we constructed 2 models. The first, a linear mixed-effects model, focused solely on the interaction effects between the pre- and postrecall periods and various medication classes on HbA1c levels. Second, we constructed a random-effects within-between model (REWB) to evaluate the impact ofmedication classes and demographic variables. Statistical significance was measured at P < .05 with conservative power at .90. The effect size was set to 1.0, reflecting a minimum clinically important difference. Literature establishes 0.5 as a modest level of HbA1c improvement and 1.0 as a clinically significant improvement.
RESULTS
Preliminary results included 15,594 veterans who received a metformin SA prescription as of June 1, 2020 from VISN 6 facilities; 15,392 veterans had a drug exposure end on June 1, 2020, indicating their standard therapy of metformin SA was discontinued following the FDA recall. Two hundred and two veterans were excluded from the registry because they continued to receive metformin SA from existing stock at a VISN6 facility.
Wilcoxon Signed-Rank Test
We created exact pairs by iterating the data and finding the closest measurements for each patient before and after the recall. This has the advantage over averaging a patient’s pre- and post-HbA1c levels, as it allows for a rank-biserial correlation. Using the nonparametric Wilcoxon signed-rank test, V was 20,100,707 (P < .001), indicating a significant effect. The –0.29 rank-biserial correlation, which was computed to assess the effect size of the recall, suggests that the median HbA1c level was lower postrecall vs prerecall. The magnitude of the correlation suggests a moderate effect size, and while the recall had a noticeable impact at a population level, it was not extreme (Table 2).
Linear Mixed-Effects Model
The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We employed a linear mixed-effects model to investigate the impact that switching from metformin SA to other T2DM medications had on HbA1c levels. The model was adjusted for patient-specific random effects and included interaction terms between the recall period (before and after) and the usage of different T2DM medications.
Model Fit and Random Effects
The model demonstrated a residual maximum likelihood criterion of 100,219.7, indicating its fit to the data. Notably, the random effects analysis revealed a substantial variability in baseline HbA1c levels across patients (SD, 0.94), highlighting the importance of individual differences in DM management. Medication classes with zero or near-zero exposure rate were removed. Due to demographic homogeneity, the model did not converge on demographic variables. Veterans were taking a mean of 1.8 T2DM medications and metformin SA was most common (Table 3).
During the postrecall period, metformin SA remained the most frequently prescribed medication class. This may be attributed to the existence of multiple manufacturers of metformin SA, some of which may not have been impacted by the recall. VISN 6 medical centers could have sought metformin SA outside of the usual procurement path following the recall.
Complex Random Effects Model
We employed a complex REWB model that evaluated the impact of medication classes on HbA1c levels, accounting for both within and between subject effects of these medications, along with demographic variables (sex, race, and ethnicity) (eAppendix). This model accounts for individual-level changes over time (within-patient effects) and between groups of patients (between-patient effects). This is a more comprehensive model aimed at understanding the broader impact of medications on HbA1c levels across diverse patient groups.
Most demographic categories did not demonstrate significant effects in this model. Black individuals experienced a slight increase in HbA1c levels compared with other racial categories that was not statistically significant. However, this model confirms the findings from the linear mixed-effects model that GLP-1 agonists showed a substantial decrease in HbA1c levels within patients (coefficient –0.5; 95% CI, –0.56 to –0.44; P < .001) and a moderate increase between patients (coefficient, 0.21; 95% CI, 0.12-0.31; P < .001). Additionally, SGLT-2 inhibitors had a notable decrease within patients (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001).Another notable finding with our REWB model is insulin usage was associated with high HbA1c levels, but only between subjects. Long-acting insulin (coefficient, 0.96; 95% CI, 0.90-1.01; P <. 001) and mixed insulin (coefficient, 1.09; 95% CI, 0.94-1.24; P < .001) both displayed marked increases between patients, suggesting future analysis may benefit from stratifying across insulin users and nonusers.
Fixed Effect Analysis
The fixed effects analysis yielded several notable findings. The intercept, representing the mean baseline HbA1c level, was estimated at 7.8% (58 mmol/mol). The coefficient for the period (postrecall) was not statistically significant, indicating no overall change in HbA1c levels from before to after the recall when specific medication classes were not considered (Table 4). Among medication classes examined, several showed significant associations with HbA1c levels. DPP-4 inhibitors and GLP-1 agonists were associated with a decrease in HbA1c levels, with coefficients of −0.08 and −0.24, respectively. Long-acting insulin and metformin immediate-release (IR) were associated with an increase in HbA1c levels, as indicated by their positive coefficients of 0.38 and 0.16, respectively. Mixed insulin formulations and sulfonylureas showed an association with decreased HbA1c levels.
Interaction Effects
The interaction terms between the recall period and the medication classes provided insights into the differential impact of the medication switch postrecall. Notably, the interaction term for long-acting insulin (coefficient, −0.10) was significant, suggesting a differential effect on HbA1c levels postrecall. Other medications, like metformin IR, also exhibited significant interaction effects, indicating changes in the impact on HbA1c levels in the postrecall period. The binary variable for medication class exposure suggests the use of a logit link function for binary outcomes within the multilevel modeling framework.15 We did not address the potential for cross cluster heterogeneity due to different medication classes.
DISCUSSION
This study is an ongoing, concurrent, observational, multicenter, registry-based study consisting of VISN 6 veterans who have T2DM and were prescribed metformin SA on June 1, 2020. This initial aim was to evaluate change in HbA1c levels following the FDA metformin recall. While there was substantial variability in baseline HbA1c levels across the patients, the mean baseline HbA1c level at 7.5% (58 mmol/mol). Patients taking GLP-1 agonists showed substantial decrease in HbA1c levels (coefficient; –0.5; 95% CI, –0.56 to –0.44; P <. 001). Patients taking SGLT-2 inhibitors had a notable decrease in HbA1c (coefficient, –0.27; 95% CI, –0.32 to –0.22; P < .001). Despite this, the coefficient for the postrecall period was not statistically significant, indicating no overall change in HbA1c levels from pre- to postrecall when specific medication classes were not considered.
Further analysis included assessment of prescribing trends postrecall. There was an increase in SGLT-2 inhibitor, GLP-1 agonist, and DPP-4 inhibitor prescribing. Considering the growing evidence of the cardiovascular and renal benefits of these medication classes, specifically the GLP-1 agonists and SGLT-2 inhibitors, this trend would be expected.
Limitations
This study cohort did not capture veterans with T2DM who transferred their health care to VISN 6 after June 1, 2020, and continued to receive metformin SA from the prior facility. Inclusion of these veterans would have increased the registry population. Additionally, the cohort did not identify veterans who continued to receive metformin SA through a source other than the VA. Without that information, the registry cohort may include veterans thought to have either transitioned to a different therapy or to no other T2DM therapy after the recall.
Given that DM can progress over time, it is possible the transition to a new medication after the recall was the result of suboptimal management, or in response to an adverse effect from a previous medication, and not solely due to the metformin SA recall. In addition, there are several factors that could impact HbA1c level over time that were not accounted for in this study, such as medication adherence and lifestyle modifications.
The notable level of metformin SA prescriptions, despite the recall, may be attributed to several factors. First, not all patients stopped metformin completely. Review of the prescription data indicated that some veterans were provided with limited refills at select VA medical centers that had supplies (medication lots not recalled). Access to a safe supply of metformin SA after the recall may have varied among VISN 6 facilities. It is also possible that as new supplies of metformin SA became available, veterans restarted metformin SA. This may have been resumed while continuing a new medication prescribed at the beginning of the recall. As the year progressed after the recall, an increase in metformin SA prescriptions likely occurred as supplies became available and clinicians/veterans chose to resume this medication therapy.
Conclusions
Results of this initial registry study found no difference in HbA1c levels across the study population after the metformin SA recall. However, there was clinical difference in the HbA1c within veterans prescribed SGLT-2 inhibitors and GLP-1 agonists. As expected, prescribing trends showed an increase in these agents after the recall. With the known benefits of these medications beyond glucose lowering, it is anticipated the cohort of veterans prescribed these medications will continue to grow.
The VISN 6 research registry allowed this study to gain an important snapshot in time following the metformin SA recall, and will serve as an important resource for future DM research endeavors. It will allow for ongoing evaluation of the impact of the transition to alternative T2DM medications after the metformin SA recall. Future exploration will include evaluation of adverse drug reactions, DM-related hospitalizations, emergency department visits related to T2DM, changes in renal function, and cardiovascular events among all diabetes medication classes.
Acknowledgments
The study team thanks the Veterans Affairs Informatics and Computing Infrastructure for their help and expertise throughout this project. The authors acknowledge the contributions of Philip Nelson, PharmD, and Brian Peek, PharmD.
- Centers for Disease Control and Prevention. Type 2 diabetes. Updated April 18, 2023. Accessed September 18, 2023. https://www.cdc.gov/diabetes/basics/type2.html
- ElSayed NA, Aleppo G, Aroda VR, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes Care. 2023;46(Supplement_1):S19-S40. doi:10.2337/dc23-S002
- Liu Y, Sayam S, Shao X, et al. Prevalence of and trends in diabetes among veterans, United States, 2005–2014. Prev Chronic Dis. 2017;14:E135. doi:10.5888/pcd14.170230
- Yi SW, Hong JS, Ohrr H, Yi JJ. Agent Orange exposure and disease prevalence in Korean Vietnam veterans: the Korean veterans health study. Environ Res. 2014;133:56-65. doi:10.1016/j.envres.2014.04.027
- Price LE, Gephart S, Shea K. The VA’s Corporate Data Warehouse: Uses and Implications for Nursing Research and Practice. Nurs Adm Q. 2015;39(4):311-318. doi:10.1097/NAQ.0000000000000118
- ElSayed NA, Aleppo G, Aroda VR, et al. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(suppl 1):S140-S157. doi:10.2337/dc23-S009
- Samson SL, Vellanki P, Blonde L, et al. American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm - 2023 Update. Endocr Pract. 2023;29(5):305-340. doi:10.1016/j.eprac.2023.02.001
- Bennett WL, Maruthur NM, Singh S, et al. Comparative effectiveness and safety of medications for type 2 diabetes: an update including new drugs and 2-drug combinations. Ann Intern Med. 2011;154(9):602-613. doi:10.7326/0003-4819-154-9-201105030-00336
- Bolen S, Feldman L, Vassy J, et al. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007;147(6):386-399. doi:10.7326/0003-4819-147-6-200709180-00178
- Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278-286. doi:10.7326/M20-0864
- Nishimura R, Taniguchi M, Takeshima T, Iwasaki K. Efficacy and safety of metformin versus the other oral antidiabetic drugs in Japanese type 2 diabetes patients: a network meta-analysis. Adv Ther. 2022;39(1):632-654. doi:10.1007/s12325-021-01979-1
- Russell-Jones D, Cuddihy RM, Hanefeld M, et al. Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care. 2012;35(2):252-258. doi:10.2337/dc11-1107
- Umpierrez G, Tofé Povedano S, Pérez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monotherapy versus metformin in type 2 diabetes in a randomized controlled trial (AWARD-3). Diabetes Care. 2014;37(8):2168-2176. doi:10.2337/dc13-2759
- US Food and Drug Administration. FDA alerts patients and health care professionals to nitrosamine impurity findings in certain metformin extended-release products [press release]. May 28, 2020. Accessed October 16, 2024. https://www.fda.gov/news-events/press-announcements/fda-alerts-patients-and-health-care-professionals-nitrosamine-impurity-findings-certain-metformin
- Bell A, Jones K. Explaining fixed effects: random effects modeling of time-series cross-sectional and panel data. PSRM. 2015;3(1):133-153. doi:10.1017/psrm.2014.7
- Centers for Disease Control and Prevention. Type 2 diabetes. Updated April 18, 2023. Accessed September 18, 2023. https://www.cdc.gov/diabetes/basics/type2.html
- ElSayed NA, Aleppo G, Aroda VR, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes Care. 2023;46(Supplement_1):S19-S40. doi:10.2337/dc23-S002
- Liu Y, Sayam S, Shao X, et al. Prevalence of and trends in diabetes among veterans, United States, 2005–2014. Prev Chronic Dis. 2017;14:E135. doi:10.5888/pcd14.170230
- Yi SW, Hong JS, Ohrr H, Yi JJ. Agent Orange exposure and disease prevalence in Korean Vietnam veterans: the Korean veterans health study. Environ Res. 2014;133:56-65. doi:10.1016/j.envres.2014.04.027
- Price LE, Gephart S, Shea K. The VA’s Corporate Data Warehouse: Uses and Implications for Nursing Research and Practice. Nurs Adm Q. 2015;39(4):311-318. doi:10.1097/NAQ.0000000000000118
- ElSayed NA, Aleppo G, Aroda VR, et al. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(suppl 1):S140-S157. doi:10.2337/dc23-S009
- Samson SL, Vellanki P, Blonde L, et al. American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm - 2023 Update. Endocr Pract. 2023;29(5):305-340. doi:10.1016/j.eprac.2023.02.001
- Bennett WL, Maruthur NM, Singh S, et al. Comparative effectiveness and safety of medications for type 2 diabetes: an update including new drugs and 2-drug combinations. Ann Intern Med. 2011;154(9):602-613. doi:10.7326/0003-4819-154-9-201105030-00336
- Bolen S, Feldman L, Vassy J, et al. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007;147(6):386-399. doi:10.7326/0003-4819-147-6-200709180-00178
- Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278-286. doi:10.7326/M20-0864
- Nishimura R, Taniguchi M, Takeshima T, Iwasaki K. Efficacy and safety of metformin versus the other oral antidiabetic drugs in Japanese type 2 diabetes patients: a network meta-analysis. Adv Ther. 2022;39(1):632-654. doi:10.1007/s12325-021-01979-1
- Russell-Jones D, Cuddihy RM, Hanefeld M, et al. Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care. 2012;35(2):252-258. doi:10.2337/dc11-1107
- Umpierrez G, Tofé Povedano S, Pérez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monotherapy versus metformin in type 2 diabetes in a randomized controlled trial (AWARD-3). Diabetes Care. 2014;37(8):2168-2176. doi:10.2337/dc13-2759
- US Food and Drug Administration. FDA alerts patients and health care professionals to nitrosamine impurity findings in certain metformin extended-release products [press release]. May 28, 2020. Accessed October 16, 2024. https://www.fda.gov/news-events/press-announcements/fda-alerts-patients-and-health-care-professionals-nitrosamine-impurity-findings-certain-metformin
- Bell A, Jones K. Explaining fixed effects: random effects modeling of time-series cross-sectional and panel data. PSRM. 2015;3(1):133-153. doi:10.1017/psrm.2014.7
Cendakimab That Targets IL-13 Shows Promise in Eosinophilic Esophagitis
VIENNA — , according to interim results of a pivotal phase 3 trial.
Treatment with cendakimab also improved key endoscopic and histologic features, even in patients who had an inadequate response or intolerance to steroids, reported Alain Schoepfer, MD, gastroenterologist from Centre Hospitalier Universitaire Vaudois and University of Lausanne, in Switzerland.
The drug was generally safe and well tolerated up to 24 weeks of treatment, added Schoepfer, who presented the results during a presentation at the United European Gastroenterology (UEG) Week 2024.
Targeting IL-13 Shows ‘Surprisingly Good Results’
EoE is a chronic, progressive, immune-mediated, inflammatory disease that is mainly driven by the cytokine, IL-13.
In a prior phase 2 study, cendakimab, which selectively binds to IL-13 and blocks its interaction with both the IL-13Ra1 and the IL-13Ra2 receptors, was shown to improve symptoms and endoscopic features of EoE.
For the current phase 3 trial, participants were required to have a peak eosinophil count (PEC) of ≥ 15 eosinophils (eos)/high power field (hpf) and 4 or more days of dysphagia over the 2 weeks prior to the start of the study. In addition, they had to have shown a complete lack of response to proton pump inhibitor (PPI) treatment for 8 weeks or more.
A total of 430 patients were randomized 1:1:1 to subcutaneous cendakimab (360 mg) once weekly for 48 weeks; subcutaneous cendakimab (360 mg) once weekly for 24 weeks, then once every 2 weeks for a further 24 weeks; or subcutaneous placebo once weekly for 48 weeks.
Patient characteristics were similar across randomization groups. The majority of participants were men, with a mean age of 35 years (range, 12-75 years); adolescents comprised 6%-11% of the total. The disease duration was around 5-6 years for all participants, of which 45% were on a stable PPI dosage and around 65% had steroid intolerance or an inadequate response. The endoscopic reference score was around 10 across all groups. The mean PEC was around 160 eos/hpf in the cendakimab arms vs 200 eos/hpf in the placebo arm.
Schoepfer reported results for the coprimary endpoints — the mean change from baseline in dysphagia days and the proportion of patients with eosinophil histologic response (PEC ≤ 6 eos/hpf) — at week 24. At this point, a total of 286 patients had received treatment with 360 mg of cendakimab once weekly, and 143 had received placebo.
The change in dysphagia days was −6.1 in patients on cendakimab once weekly vs −4.2 in patients on placebo (P = .0005). The proportion of patients with eosinophil histologic response was 28.6% in the treatment arm vs 2.2% in the placebo arm.
The results were similar for patients who were classified as having had a steroid inadequate response. The change in dysphagia days was −6.3 in the cendakimab group vs −4.7 in the placebo group (P = .0156). The eosinophil histologic response was 29.5% in the treatment group vs 2.1% in the placebo group (P < .0001).
Endoscopic response, a key secondary endpoint, showed a change from baseline to week 24 in the endoscopic features of EoE. The total endoscopic reference scores were −5.2 for patients on cendakimab once weekly and −1.2 for patients on placebo (P < .0001).
The safety profile of cendakimab was “unspectacular,” Schoepfer said, with adverse events related to the study drug occurring in 30% of patients in the treatment arm vs 18.9% of those in the placebo arm. He noted that as the trial was conducted during the COVID pandemic, there were some infections.
Serious adverse events, which were assessed by investigators to not be related to the study drug, occurred in 1.8% and 2.8% of patients on cendakimab and placebo, respectively. Drug discontinuation occurred in 1.4% in the cendakimab group and 0.7% in the placebo group. There were no deaths.
“We really need drugs for this disease, given that there are very few alternatives to steroids and PPIs,” Co-moderator Ram Dickman, MD, Division of Gastroenterology, Rabin Medical Center, Petah Tikva, Israel, said in an interview.
Right now, we have dupilumab, which targets two receptors: IL-4 and IL-13. But targeting IL-13 by itself “is showing surprisingly good results,” so cendakimab is a good candidate to be in “the first line of biologic treatments,” Dickman said.
“It’s safe and works rapidly,” he added. “Given this is a phase 3 study, I believe we’ll see it on the market.”
Schoepfer has served as a consultant for Regeneron/Sanofi, Adare/Ellodi, AbbVie, AstraZeneca, Celgene/Receptos/Bristol Myers Squibb, Dr. Falk Pharma, Gossamer Bio, GSK, Janssen, MSD, Pfizer, Regeneron/Sanofi, Takeda, and Vifor; received grant/research support from Adare/Ellodi, Celgene/Receptos/Bristol Myers Squibb, GSK, and Regeneron/Sanofi. Dickman has declared no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — , according to interim results of a pivotal phase 3 trial.
Treatment with cendakimab also improved key endoscopic and histologic features, even in patients who had an inadequate response or intolerance to steroids, reported Alain Schoepfer, MD, gastroenterologist from Centre Hospitalier Universitaire Vaudois and University of Lausanne, in Switzerland.
The drug was generally safe and well tolerated up to 24 weeks of treatment, added Schoepfer, who presented the results during a presentation at the United European Gastroenterology (UEG) Week 2024.
Targeting IL-13 Shows ‘Surprisingly Good Results’
EoE is a chronic, progressive, immune-mediated, inflammatory disease that is mainly driven by the cytokine, IL-13.
In a prior phase 2 study, cendakimab, which selectively binds to IL-13 and blocks its interaction with both the IL-13Ra1 and the IL-13Ra2 receptors, was shown to improve symptoms and endoscopic features of EoE.
For the current phase 3 trial, participants were required to have a peak eosinophil count (PEC) of ≥ 15 eosinophils (eos)/high power field (hpf) and 4 or more days of dysphagia over the 2 weeks prior to the start of the study. In addition, they had to have shown a complete lack of response to proton pump inhibitor (PPI) treatment for 8 weeks or more.
A total of 430 patients were randomized 1:1:1 to subcutaneous cendakimab (360 mg) once weekly for 48 weeks; subcutaneous cendakimab (360 mg) once weekly for 24 weeks, then once every 2 weeks for a further 24 weeks; or subcutaneous placebo once weekly for 48 weeks.
Patient characteristics were similar across randomization groups. The majority of participants were men, with a mean age of 35 years (range, 12-75 years); adolescents comprised 6%-11% of the total. The disease duration was around 5-6 years for all participants, of which 45% were on a stable PPI dosage and around 65% had steroid intolerance or an inadequate response. The endoscopic reference score was around 10 across all groups. The mean PEC was around 160 eos/hpf in the cendakimab arms vs 200 eos/hpf in the placebo arm.
Schoepfer reported results for the coprimary endpoints — the mean change from baseline in dysphagia days and the proportion of patients with eosinophil histologic response (PEC ≤ 6 eos/hpf) — at week 24. At this point, a total of 286 patients had received treatment with 360 mg of cendakimab once weekly, and 143 had received placebo.
The change in dysphagia days was −6.1 in patients on cendakimab once weekly vs −4.2 in patients on placebo (P = .0005). The proportion of patients with eosinophil histologic response was 28.6% in the treatment arm vs 2.2% in the placebo arm.
The results were similar for patients who were classified as having had a steroid inadequate response. The change in dysphagia days was −6.3 in the cendakimab group vs −4.7 in the placebo group (P = .0156). The eosinophil histologic response was 29.5% in the treatment group vs 2.1% in the placebo group (P < .0001).
Endoscopic response, a key secondary endpoint, showed a change from baseline to week 24 in the endoscopic features of EoE. The total endoscopic reference scores were −5.2 for patients on cendakimab once weekly and −1.2 for patients on placebo (P < .0001).
The safety profile of cendakimab was “unspectacular,” Schoepfer said, with adverse events related to the study drug occurring in 30% of patients in the treatment arm vs 18.9% of those in the placebo arm. He noted that as the trial was conducted during the COVID pandemic, there were some infections.
Serious adverse events, which were assessed by investigators to not be related to the study drug, occurred in 1.8% and 2.8% of patients on cendakimab and placebo, respectively. Drug discontinuation occurred in 1.4% in the cendakimab group and 0.7% in the placebo group. There were no deaths.
“We really need drugs for this disease, given that there are very few alternatives to steroids and PPIs,” Co-moderator Ram Dickman, MD, Division of Gastroenterology, Rabin Medical Center, Petah Tikva, Israel, said in an interview.
Right now, we have dupilumab, which targets two receptors: IL-4 and IL-13. But targeting IL-13 by itself “is showing surprisingly good results,” so cendakimab is a good candidate to be in “the first line of biologic treatments,” Dickman said.
“It’s safe and works rapidly,” he added. “Given this is a phase 3 study, I believe we’ll see it on the market.”
Schoepfer has served as a consultant for Regeneron/Sanofi, Adare/Ellodi, AbbVie, AstraZeneca, Celgene/Receptos/Bristol Myers Squibb, Dr. Falk Pharma, Gossamer Bio, GSK, Janssen, MSD, Pfizer, Regeneron/Sanofi, Takeda, and Vifor; received grant/research support from Adare/Ellodi, Celgene/Receptos/Bristol Myers Squibb, GSK, and Regeneron/Sanofi. Dickman has declared no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — , according to interim results of a pivotal phase 3 trial.
Treatment with cendakimab also improved key endoscopic and histologic features, even in patients who had an inadequate response or intolerance to steroids, reported Alain Schoepfer, MD, gastroenterologist from Centre Hospitalier Universitaire Vaudois and University of Lausanne, in Switzerland.
The drug was generally safe and well tolerated up to 24 weeks of treatment, added Schoepfer, who presented the results during a presentation at the United European Gastroenterology (UEG) Week 2024.
Targeting IL-13 Shows ‘Surprisingly Good Results’
EoE is a chronic, progressive, immune-mediated, inflammatory disease that is mainly driven by the cytokine, IL-13.
In a prior phase 2 study, cendakimab, which selectively binds to IL-13 and blocks its interaction with both the IL-13Ra1 and the IL-13Ra2 receptors, was shown to improve symptoms and endoscopic features of EoE.
For the current phase 3 trial, participants were required to have a peak eosinophil count (PEC) of ≥ 15 eosinophils (eos)/high power field (hpf) and 4 or more days of dysphagia over the 2 weeks prior to the start of the study. In addition, they had to have shown a complete lack of response to proton pump inhibitor (PPI) treatment for 8 weeks or more.
A total of 430 patients were randomized 1:1:1 to subcutaneous cendakimab (360 mg) once weekly for 48 weeks; subcutaneous cendakimab (360 mg) once weekly for 24 weeks, then once every 2 weeks for a further 24 weeks; or subcutaneous placebo once weekly for 48 weeks.
Patient characteristics were similar across randomization groups. The majority of participants were men, with a mean age of 35 years (range, 12-75 years); adolescents comprised 6%-11% of the total. The disease duration was around 5-6 years for all participants, of which 45% were on a stable PPI dosage and around 65% had steroid intolerance or an inadequate response. The endoscopic reference score was around 10 across all groups. The mean PEC was around 160 eos/hpf in the cendakimab arms vs 200 eos/hpf in the placebo arm.
Schoepfer reported results for the coprimary endpoints — the mean change from baseline in dysphagia days and the proportion of patients with eosinophil histologic response (PEC ≤ 6 eos/hpf) — at week 24. At this point, a total of 286 patients had received treatment with 360 mg of cendakimab once weekly, and 143 had received placebo.
The change in dysphagia days was −6.1 in patients on cendakimab once weekly vs −4.2 in patients on placebo (P = .0005). The proportion of patients with eosinophil histologic response was 28.6% in the treatment arm vs 2.2% in the placebo arm.
The results were similar for patients who were classified as having had a steroid inadequate response. The change in dysphagia days was −6.3 in the cendakimab group vs −4.7 in the placebo group (P = .0156). The eosinophil histologic response was 29.5% in the treatment group vs 2.1% in the placebo group (P < .0001).
Endoscopic response, a key secondary endpoint, showed a change from baseline to week 24 in the endoscopic features of EoE. The total endoscopic reference scores were −5.2 for patients on cendakimab once weekly and −1.2 for patients on placebo (P < .0001).
The safety profile of cendakimab was “unspectacular,” Schoepfer said, with adverse events related to the study drug occurring in 30% of patients in the treatment arm vs 18.9% of those in the placebo arm. He noted that as the trial was conducted during the COVID pandemic, there were some infections.
Serious adverse events, which were assessed by investigators to not be related to the study drug, occurred in 1.8% and 2.8% of patients on cendakimab and placebo, respectively. Drug discontinuation occurred in 1.4% in the cendakimab group and 0.7% in the placebo group. There were no deaths.
“We really need drugs for this disease, given that there are very few alternatives to steroids and PPIs,” Co-moderator Ram Dickman, MD, Division of Gastroenterology, Rabin Medical Center, Petah Tikva, Israel, said in an interview.
Right now, we have dupilumab, which targets two receptors: IL-4 and IL-13. But targeting IL-13 by itself “is showing surprisingly good results,” so cendakimab is a good candidate to be in “the first line of biologic treatments,” Dickman said.
“It’s safe and works rapidly,” he added. “Given this is a phase 3 study, I believe we’ll see it on the market.”
Schoepfer has served as a consultant for Regeneron/Sanofi, Adare/Ellodi, AbbVie, AstraZeneca, Celgene/Receptos/Bristol Myers Squibb, Dr. Falk Pharma, Gossamer Bio, GSK, Janssen, MSD, Pfizer, Regeneron/Sanofi, Takeda, and Vifor; received grant/research support from Adare/Ellodi, Celgene/Receptos/Bristol Myers Squibb, GSK, and Regeneron/Sanofi. Dickman has declared no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM UEG 2024
American Diabetes Association Advises on Hospital CGM Use
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
New mRNA Vaccine May Shield Against C difficile Infections
A group of researchers from the University of Pennsylvania, Philadelphia, has developed a messenger RNA (mRNA) vaccine, delivered via lipid nanoparticles (LNPs) — the same type as the COVID-19 vaccine produced by Moderna and Pfizer — targeting Clostridioides difficile (formerly Clostridium difficile). According to the authors, the results of their preclinical study, published in Science, demonstrated this technology as a promising platform for C difficile vaccine development and could be the starting point for curbing intestinal infections that, in their most severe forms (pseudomembranous colitis, toxic megacolon), can be fatal.
An Increasingly Pressing Issue
C difficile is the leading cause of infectious diarrhea acquired in healthcare settings.
A 2019 study reported a global incidence of C difficile infections at 2.2 per 1000 hospital admissions per year and 3.5 per 10,000 patient-days per year.
The Vaccine Candidate
Vaccine candidates tested so far have used toxoids or recombinant proteins targeting the combined repetitive oligopeptide (CROP) or receptor-binding domain (RBD) of the two primary C difficile toxins, TcdA and TcdB. The US researchers are now exploring the mRNA-LNP vaccine approach to target multiple antigens simultaneously. They developed a bivalent vaccine (including the CROP and RBD domains of both toxins) and a trivalent vaccine (with an additional virulence factor, the metalloprotease Pro-Pro endopeptidase-1).
Mice vaccinated with the bivalent and trivalent vaccines produced immunoglobulin G antibody titers two to four times higher than those elicited by recombinant protein with an adjuvant. The vaccination stimulated the proliferation of follicular T helper cells and the antigen-specific response of B lymphocytes, laying the foundation for a strong and long-lasting humoral response. The vaccines were also immunogenic in hamsters.
Vaccinated mice not only survived a toxin dose five times higher than the 100% lethal dose but also demonstrated the vaccine’s protective effect through serum transfer; unvaccinated mice given serum from vaccinated mice survived the lethal challenge. More importantly, when exposed to a lethal dose of the bacterium itself, all vaccinated mice survived.
To demonstrate the vaccine’s efficacy in patients with a history of C difficile infection and high recurrence risk — ideal candidates for vaccination — the researchers vaccinated mice that had previously survived a sublethal infection. Six months after the initial infection and vaccination, these mice remained protected against mortality when reexposed to the bacterium.
Additionally, a quadrivalent vaccine that included an immunogen targeting C difficile spores — key agents in transmission — also proved effective. Low levels of bacteria and toxins in the feces of mice vaccinated in this way suggested that spore vaccination could limit initial colonization.
In tests with nonhuman primates, two doses of the vaccines targeting either the vegetative form or the spores elicited strong immune responses against bacterial toxins and virulence factors. Human trials may indeed be on the horizon.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
A group of researchers from the University of Pennsylvania, Philadelphia, has developed a messenger RNA (mRNA) vaccine, delivered via lipid nanoparticles (LNPs) — the same type as the COVID-19 vaccine produced by Moderna and Pfizer — targeting Clostridioides difficile (formerly Clostridium difficile). According to the authors, the results of their preclinical study, published in Science, demonstrated this technology as a promising platform for C difficile vaccine development and could be the starting point for curbing intestinal infections that, in their most severe forms (pseudomembranous colitis, toxic megacolon), can be fatal.
An Increasingly Pressing Issue
C difficile is the leading cause of infectious diarrhea acquired in healthcare settings.
A 2019 study reported a global incidence of C difficile infections at 2.2 per 1000 hospital admissions per year and 3.5 per 10,000 patient-days per year.
The Vaccine Candidate
Vaccine candidates tested so far have used toxoids or recombinant proteins targeting the combined repetitive oligopeptide (CROP) or receptor-binding domain (RBD) of the two primary C difficile toxins, TcdA and TcdB. The US researchers are now exploring the mRNA-LNP vaccine approach to target multiple antigens simultaneously. They developed a bivalent vaccine (including the CROP and RBD domains of both toxins) and a trivalent vaccine (with an additional virulence factor, the metalloprotease Pro-Pro endopeptidase-1).
Mice vaccinated with the bivalent and trivalent vaccines produced immunoglobulin G antibody titers two to four times higher than those elicited by recombinant protein with an adjuvant. The vaccination stimulated the proliferation of follicular T helper cells and the antigen-specific response of B lymphocytes, laying the foundation for a strong and long-lasting humoral response. The vaccines were also immunogenic in hamsters.
Vaccinated mice not only survived a toxin dose five times higher than the 100% lethal dose but also demonstrated the vaccine’s protective effect through serum transfer; unvaccinated mice given serum from vaccinated mice survived the lethal challenge. More importantly, when exposed to a lethal dose of the bacterium itself, all vaccinated mice survived.
To demonstrate the vaccine’s efficacy in patients with a history of C difficile infection and high recurrence risk — ideal candidates for vaccination — the researchers vaccinated mice that had previously survived a sublethal infection. Six months after the initial infection and vaccination, these mice remained protected against mortality when reexposed to the bacterium.
Additionally, a quadrivalent vaccine that included an immunogen targeting C difficile spores — key agents in transmission — also proved effective. Low levels of bacteria and toxins in the feces of mice vaccinated in this way suggested that spore vaccination could limit initial colonization.
In tests with nonhuman primates, two doses of the vaccines targeting either the vegetative form or the spores elicited strong immune responses against bacterial toxins and virulence factors. Human trials may indeed be on the horizon.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
A group of researchers from the University of Pennsylvania, Philadelphia, has developed a messenger RNA (mRNA) vaccine, delivered via lipid nanoparticles (LNPs) — the same type as the COVID-19 vaccine produced by Moderna and Pfizer — targeting Clostridioides difficile (formerly Clostridium difficile). According to the authors, the results of their preclinical study, published in Science, demonstrated this technology as a promising platform for C difficile vaccine development and could be the starting point for curbing intestinal infections that, in their most severe forms (pseudomembranous colitis, toxic megacolon), can be fatal.
An Increasingly Pressing Issue
C difficile is the leading cause of infectious diarrhea acquired in healthcare settings.
A 2019 study reported a global incidence of C difficile infections at 2.2 per 1000 hospital admissions per year and 3.5 per 10,000 patient-days per year.
The Vaccine Candidate
Vaccine candidates tested so far have used toxoids or recombinant proteins targeting the combined repetitive oligopeptide (CROP) or receptor-binding domain (RBD) of the two primary C difficile toxins, TcdA and TcdB. The US researchers are now exploring the mRNA-LNP vaccine approach to target multiple antigens simultaneously. They developed a bivalent vaccine (including the CROP and RBD domains of both toxins) and a trivalent vaccine (with an additional virulence factor, the metalloprotease Pro-Pro endopeptidase-1).
Mice vaccinated with the bivalent and trivalent vaccines produced immunoglobulin G antibody titers two to four times higher than those elicited by recombinant protein with an adjuvant. The vaccination stimulated the proliferation of follicular T helper cells and the antigen-specific response of B lymphocytes, laying the foundation for a strong and long-lasting humoral response. The vaccines were also immunogenic in hamsters.
Vaccinated mice not only survived a toxin dose five times higher than the 100% lethal dose but also demonstrated the vaccine’s protective effect through serum transfer; unvaccinated mice given serum from vaccinated mice survived the lethal challenge. More importantly, when exposed to a lethal dose of the bacterium itself, all vaccinated mice survived.
To demonstrate the vaccine’s efficacy in patients with a history of C difficile infection and high recurrence risk — ideal candidates for vaccination — the researchers vaccinated mice that had previously survived a sublethal infection. Six months after the initial infection and vaccination, these mice remained protected against mortality when reexposed to the bacterium.
Additionally, a quadrivalent vaccine that included an immunogen targeting C difficile spores — key agents in transmission — also proved effective. Low levels of bacteria and toxins in the feces of mice vaccinated in this way suggested that spore vaccination could limit initial colonization.
In tests with nonhuman primates, two doses of the vaccines targeting either the vegetative form or the spores elicited strong immune responses against bacterial toxins and virulence factors. Human trials may indeed be on the horizon.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
More Evidence Avatar Therapy Quiets Auditory Hallucinations in Psychosis
, results from the largest study of avatar therapy to date show.
The therapy allows patients to interact with a “digital embodiment” of the voice they hear, which is represented by a computer-generated face, also known as an avatar.
In the randomized, multisite, phase 2/3 AVATAR2 trial, patients who received AVATAR-Extended therapy, which included a personalized series of voiced dialogues based on their life history, plus treatment as usual (TAU) showed significantly greater improvement in distress and voice severity levels at 16 weeks vs those who received TAU only. They also had significant reductions in voice frequency at 16 and 28 weeks.
Patients in a third arm who were assigned to TAU plus AVATAR-Brief therapy, which included six sessions of a standardized version of the therapy, also showed improvements at 16 weeks, compared with TAU alone — but the clinical impact was stronger with the extended version.
“I was surprised at the extent to which the extended version seemed to be a more optimal version, and it should be the way forward with this therapy,” said study investigator Philippa A. Garety, PhD, professor emerita of clinical psychology at the Institute of Psychiatry, Psychology, and Neuroscience at King’s College, London, England.
With more than 300 participants, AVATAR2 is the largest trial to access avatar therapy to date, Garety noted.
“What’s unique about this work is that technology allows us to create safe face-to-face encounters with a representation of a person’s voice and allows them to relate to that voice in a new way,” she added.
The findings were published online in Nature Medicine.
A Decade of Research
Auditory verbal hallucinations are common in patients with schizophrenia, but currently available therapies can be ineffective, investigators wrote.
The therapy allows patients to customize how the avatar looks and sounds. Face-to-face dialogues are then conducted between the patients and avatars in order to build empowerment. A trained therapist provides support during these sessions.
As previously reported, the creator of avatar therapy, Julian Leff, MD, presented promising results from a pilot study of 26 patients at the International Congress of the Royal College of Psychiatrists in 2014.
“Opening up a dialogue between a patient and the voice they’ve been hearing is powerful,” said Leff, who was emeritus professor at the Institute of Psychiatry in London at the time.
In 2018, a randomized single-site study (AVATAR1) of 150 participants showed that the intervention was associated with a greater decrease in voice severity at 12 weeks vs supportive therapy. Past research led to the idea of incorporating personalization to better optimize the experience.
Garety noted that AVATAR2 is the largest trial to date of the therapy, as well as the first multisite trial to test the intervention, which was important in order to determine whether it could work outside of a research setting.
The study included 345 participants (61.4% men; mean age, 39.6 years) from three sites in England and one in Scotland. All were randomly assigned to receive TAU alone (n = 115), TAU plus AVATAR-Brief (n = 116), or TAU plus AVATAR-Extended (n = 114).
TAU typically included use of antipsychotics, as well as outpatient psychiatric visits and follow-up by case managers and care coordinators.
“We didn’t interfere with treatment as usual. We wanted to test whether adding this therapy to [TAU] would enhance effects and provide better treatment for their voices,” Garety noted.
AVATAR-Brief included a standardized process that focused on such things as self-esteem and assertiveness. AVATAR-Extended had two phases. In the first, participants received AVATAR-Brief therapy, whereas the second phase offered a more personalized intervention.
An ‘Unusual Finding’
The study’s primary outcome was voice-related distress at 16 and 28 weeks. Although the TAU plus AVATAR-Extended group did show a significant decrease in distress at 16 weeks vs TAU alone (–1.6 points; P = .029), the improvement was no longer significant at the 28-week follow-up (P = .175). The same was also true for the key secondary outcome of reduction in voice severity (–2.32 points; P = .009 at 16 weeks but P =.1 at 28 weeks).
The investigators noted that this might be caused by the number of dropouts in the AVATAR-Extended group by the 28-week timepoint. The completion rate for those patients was only 58%. The completion rate for the shorter, AVATAR-Brief group was 82%.
On the other hand, the other key secondary outcome of voice frequency was significantly reduced with AVATAR-Extended at both 16 weeks (–0.62 point; P = .01) and 28 weeks (–0.89 point; P = .003).
“This is an unusual finding. We’re not aware of any other psychological therapy that shows a reduction in the occurrence of the voice,” Garety said.
For TAU plus AVATAR-Brief, there were improvements at 16 weeks for distress (-1.05 points; P = .035) vs TAU alone. However, the researchers noted that this version of the therapy was just below the prespecified threshold for a clinically significant change and was at the threshold for statistical significance.
Although the shorter therapy was associated with a reduction in voice severity level at 16 weeks (–2.04 points; P = .017) vs TAU alone, there was no reduction in distress or voice severity at 28 weeks. There was no improvement in voice frequency at either timepoint.
Both the brief and the extended versions of AVATAR therapy showed improved mood and anxiety levels at 16 weeks and sustained improvement in well-being and recovery, the researchers noted.
“The short version, as expected, did deliver benefits posttreatment, but clearly the extended, optimized version outperformed the brief version. It had stronger and more lasting effects across quite a wide range of outcomes that matter to people who hear voices,” Garety said.
“In the extended version, people felt more empowered. And in just that version, the frequency of voices was reduced, which is a very important outcome,” she added.
Safety Issues?
There were 58 serious adverse events (SAEs) in total, with 51% of those occurring in the AVATAR-Extended group. Two participants in that group died; however, independent reviews deemed these events as not related to the intervention.
In addition, there were no “definitely related” SAEs and only a small number of “possibly related” SAEs, which typically included hospitalization with other contributory factors.
Garety noted during a press briefing that AVATAR therapy has now been demonstrated to be safe across two large trials.
Study limitations cited included no direct comparison between AVATAR-Brief and AVATAR-Extended or between AVATAR therapy and a different type of psychological treatment.
Overall, “we recommend that future development and provision of AVATAR therapy is primarily guided” by the AVATAR-Extended protocol, the investigators wrote.
Because the therapy was recommended by a National Institute for Health and Care Excellence Early Value Assessment, the investigators are now seeking to provide it in routine National Health Service settings to gather further real-world evidence of effectiveness over the next 3 years.
Next Steps
Although the intervention isn’t currently available to everybody who might be seeking it, “there’s a pipeline of movement from research into treatment and it’s moving towards the next stage of delivery,” Garety said.
Investigators are also looking into cultural adaptations for the therapy so it can be used in different locales, including Ethiopia and India, she added. There isn’t a US version yet, but Garety noted that investigators in Canada are looking at similar research and suspects that will also occur in the United States soon.
“We’re pioneers in this work, and it now needs to be going international and into services,” she said. “We have had many people who hear voices say what an amazing experience this has been. So, I feel very proud and excited to have been able to be part of this.”
At the press briefing, Miranda Wolpert, director of mental health at Wellcome, which funded the study, noted that it is encouraging to see the development of a new intervention that could potentially change the lives of patients across the world.
“We know that psychosis can start early in life, stopping people from having the jobs and relationships they want and from achieving the goals they want. This intervention was developed with those people to help them address an issue that really troubles them,” Wolpert said.
“For me, this represents part of a revolution we are starting to see in terms of mental health interventions and the potential impact on mental health science,” she added.
Digital Placebo Effect?
Commenting on the findings, John Torous, MD, a psychiatrist and director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said there is a need for new treatments for schizophrenia that work with different mechanisms.
“We have a lot of medication studies but not as many innovative therapy studies. I think it’s exciting that the results, at least in the shorter-term outcome, were positive. And I think that’s something that can give people hope in using these new technologies,” said Torous, who is also an assistant professor of psychiatry at Harvard Medical School, Boston, and was not involved with the research.
Still, he did note some study limitations, including whether there could have been some type of “digital placebo effect” from the therapy.
“If you tell people they’re getting high-tech advanced digital care, that may have some effect,” he said, adding that “it’s always interesting” to tease out the benefit being delivered by the technology vs the delivery mechanism itself — or some combination of both.
Torous added, though, that it’s very difficult to have a rigorous digital control group. “It’s not necessarily a fault of their study, but it’s something to keep in mind when interpreting what the results are.”
He also noted that he would have liked to have seen a direct comparison between this new kind of psychological therapy vs standard psychological therapy, such as cognitive-behavioral therapy.
In addition, he wondered about expenses and scalability of the intervention, and whether patients would need to go to a specialized center to undergo treatment. Torous mentioned that a version involving virtual reality could perhaps make this more scalable in the future.
Overall, he said that what the investigators are currently doing is very innovative. “It’s exciting that we’re talking about the next steps. Giving people new options for psychological therapy that may be effective for their disorders is really wonderful to see,” Torous said.
The study was funded by the National Institute for Health and Care Research (NIHR), the Wellcome Trust King’s Clinical Research Facility, the NIHR Maudsley Biomedical Research Centre and Maudsley NHS Foundation Trust, King’s College London, the Manchester Biomedical Research Centre, and NHS Research Scotland, as well as by a grant from Wellcome. Garety reports being an unpaid scientific adviser to Avatar Therapy. Financial disclosures for the other investigators are fully listed in the original article. Torous reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, results from the largest study of avatar therapy to date show.
The therapy allows patients to interact with a “digital embodiment” of the voice they hear, which is represented by a computer-generated face, also known as an avatar.
In the randomized, multisite, phase 2/3 AVATAR2 trial, patients who received AVATAR-Extended therapy, which included a personalized series of voiced dialogues based on their life history, plus treatment as usual (TAU) showed significantly greater improvement in distress and voice severity levels at 16 weeks vs those who received TAU only. They also had significant reductions in voice frequency at 16 and 28 weeks.
Patients in a third arm who were assigned to TAU plus AVATAR-Brief therapy, which included six sessions of a standardized version of the therapy, also showed improvements at 16 weeks, compared with TAU alone — but the clinical impact was stronger with the extended version.
“I was surprised at the extent to which the extended version seemed to be a more optimal version, and it should be the way forward with this therapy,” said study investigator Philippa A. Garety, PhD, professor emerita of clinical psychology at the Institute of Psychiatry, Psychology, and Neuroscience at King’s College, London, England.
With more than 300 participants, AVATAR2 is the largest trial to access avatar therapy to date, Garety noted.
“What’s unique about this work is that technology allows us to create safe face-to-face encounters with a representation of a person’s voice and allows them to relate to that voice in a new way,” she added.
The findings were published online in Nature Medicine.
A Decade of Research
Auditory verbal hallucinations are common in patients with schizophrenia, but currently available therapies can be ineffective, investigators wrote.
The therapy allows patients to customize how the avatar looks and sounds. Face-to-face dialogues are then conducted between the patients and avatars in order to build empowerment. A trained therapist provides support during these sessions.
As previously reported, the creator of avatar therapy, Julian Leff, MD, presented promising results from a pilot study of 26 patients at the International Congress of the Royal College of Psychiatrists in 2014.
“Opening up a dialogue between a patient and the voice they’ve been hearing is powerful,” said Leff, who was emeritus professor at the Institute of Psychiatry in London at the time.
In 2018, a randomized single-site study (AVATAR1) of 150 participants showed that the intervention was associated with a greater decrease in voice severity at 12 weeks vs supportive therapy. Past research led to the idea of incorporating personalization to better optimize the experience.
Garety noted that AVATAR2 is the largest trial to date of the therapy, as well as the first multisite trial to test the intervention, which was important in order to determine whether it could work outside of a research setting.
The study included 345 participants (61.4% men; mean age, 39.6 years) from three sites in England and one in Scotland. All were randomly assigned to receive TAU alone (n = 115), TAU plus AVATAR-Brief (n = 116), or TAU plus AVATAR-Extended (n = 114).
TAU typically included use of antipsychotics, as well as outpatient psychiatric visits and follow-up by case managers and care coordinators.
“We didn’t interfere with treatment as usual. We wanted to test whether adding this therapy to [TAU] would enhance effects and provide better treatment for their voices,” Garety noted.
AVATAR-Brief included a standardized process that focused on such things as self-esteem and assertiveness. AVATAR-Extended had two phases. In the first, participants received AVATAR-Brief therapy, whereas the second phase offered a more personalized intervention.
An ‘Unusual Finding’
The study’s primary outcome was voice-related distress at 16 and 28 weeks. Although the TAU plus AVATAR-Extended group did show a significant decrease in distress at 16 weeks vs TAU alone (–1.6 points; P = .029), the improvement was no longer significant at the 28-week follow-up (P = .175). The same was also true for the key secondary outcome of reduction in voice severity (–2.32 points; P = .009 at 16 weeks but P =.1 at 28 weeks).
The investigators noted that this might be caused by the number of dropouts in the AVATAR-Extended group by the 28-week timepoint. The completion rate for those patients was only 58%. The completion rate for the shorter, AVATAR-Brief group was 82%.
On the other hand, the other key secondary outcome of voice frequency was significantly reduced with AVATAR-Extended at both 16 weeks (–0.62 point; P = .01) and 28 weeks (–0.89 point; P = .003).
“This is an unusual finding. We’re not aware of any other psychological therapy that shows a reduction in the occurrence of the voice,” Garety said.
For TAU plus AVATAR-Brief, there were improvements at 16 weeks for distress (-1.05 points; P = .035) vs TAU alone. However, the researchers noted that this version of the therapy was just below the prespecified threshold for a clinically significant change and was at the threshold for statistical significance.
Although the shorter therapy was associated with a reduction in voice severity level at 16 weeks (–2.04 points; P = .017) vs TAU alone, there was no reduction in distress or voice severity at 28 weeks. There was no improvement in voice frequency at either timepoint.
Both the brief and the extended versions of AVATAR therapy showed improved mood and anxiety levels at 16 weeks and sustained improvement in well-being and recovery, the researchers noted.
“The short version, as expected, did deliver benefits posttreatment, but clearly the extended, optimized version outperformed the brief version. It had stronger and more lasting effects across quite a wide range of outcomes that matter to people who hear voices,” Garety said.
“In the extended version, people felt more empowered. And in just that version, the frequency of voices was reduced, which is a very important outcome,” she added.
Safety Issues?
There were 58 serious adverse events (SAEs) in total, with 51% of those occurring in the AVATAR-Extended group. Two participants in that group died; however, independent reviews deemed these events as not related to the intervention.
In addition, there were no “definitely related” SAEs and only a small number of “possibly related” SAEs, which typically included hospitalization with other contributory factors.
Garety noted during a press briefing that AVATAR therapy has now been demonstrated to be safe across two large trials.
Study limitations cited included no direct comparison between AVATAR-Brief and AVATAR-Extended or between AVATAR therapy and a different type of psychological treatment.
Overall, “we recommend that future development and provision of AVATAR therapy is primarily guided” by the AVATAR-Extended protocol, the investigators wrote.
Because the therapy was recommended by a National Institute for Health and Care Excellence Early Value Assessment, the investigators are now seeking to provide it in routine National Health Service settings to gather further real-world evidence of effectiveness over the next 3 years.
Next Steps
Although the intervention isn’t currently available to everybody who might be seeking it, “there’s a pipeline of movement from research into treatment and it’s moving towards the next stage of delivery,” Garety said.
Investigators are also looking into cultural adaptations for the therapy so it can be used in different locales, including Ethiopia and India, she added. There isn’t a US version yet, but Garety noted that investigators in Canada are looking at similar research and suspects that will also occur in the United States soon.
“We’re pioneers in this work, and it now needs to be going international and into services,” she said. “We have had many people who hear voices say what an amazing experience this has been. So, I feel very proud and excited to have been able to be part of this.”
At the press briefing, Miranda Wolpert, director of mental health at Wellcome, which funded the study, noted that it is encouraging to see the development of a new intervention that could potentially change the lives of patients across the world.
“We know that psychosis can start early in life, stopping people from having the jobs and relationships they want and from achieving the goals they want. This intervention was developed with those people to help them address an issue that really troubles them,” Wolpert said.
“For me, this represents part of a revolution we are starting to see in terms of mental health interventions and the potential impact on mental health science,” she added.
Digital Placebo Effect?
Commenting on the findings, John Torous, MD, a psychiatrist and director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said there is a need for new treatments for schizophrenia that work with different mechanisms.
“We have a lot of medication studies but not as many innovative therapy studies. I think it’s exciting that the results, at least in the shorter-term outcome, were positive. And I think that’s something that can give people hope in using these new technologies,” said Torous, who is also an assistant professor of psychiatry at Harvard Medical School, Boston, and was not involved with the research.
Still, he did note some study limitations, including whether there could have been some type of “digital placebo effect” from the therapy.
“If you tell people they’re getting high-tech advanced digital care, that may have some effect,” he said, adding that “it’s always interesting” to tease out the benefit being delivered by the technology vs the delivery mechanism itself — or some combination of both.
Torous added, though, that it’s very difficult to have a rigorous digital control group. “It’s not necessarily a fault of their study, but it’s something to keep in mind when interpreting what the results are.”
He also noted that he would have liked to have seen a direct comparison between this new kind of psychological therapy vs standard psychological therapy, such as cognitive-behavioral therapy.
In addition, he wondered about expenses and scalability of the intervention, and whether patients would need to go to a specialized center to undergo treatment. Torous mentioned that a version involving virtual reality could perhaps make this more scalable in the future.
Overall, he said that what the investigators are currently doing is very innovative. “It’s exciting that we’re talking about the next steps. Giving people new options for psychological therapy that may be effective for their disorders is really wonderful to see,” Torous said.
The study was funded by the National Institute for Health and Care Research (NIHR), the Wellcome Trust King’s Clinical Research Facility, the NIHR Maudsley Biomedical Research Centre and Maudsley NHS Foundation Trust, King’s College London, the Manchester Biomedical Research Centre, and NHS Research Scotland, as well as by a grant from Wellcome. Garety reports being an unpaid scientific adviser to Avatar Therapy. Financial disclosures for the other investigators are fully listed in the original article. Torous reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, results from the largest study of avatar therapy to date show.
The therapy allows patients to interact with a “digital embodiment” of the voice they hear, which is represented by a computer-generated face, also known as an avatar.
In the randomized, multisite, phase 2/3 AVATAR2 trial, patients who received AVATAR-Extended therapy, which included a personalized series of voiced dialogues based on their life history, plus treatment as usual (TAU) showed significantly greater improvement in distress and voice severity levels at 16 weeks vs those who received TAU only. They also had significant reductions in voice frequency at 16 and 28 weeks.
Patients in a third arm who were assigned to TAU plus AVATAR-Brief therapy, which included six sessions of a standardized version of the therapy, also showed improvements at 16 weeks, compared with TAU alone — but the clinical impact was stronger with the extended version.
“I was surprised at the extent to which the extended version seemed to be a more optimal version, and it should be the way forward with this therapy,” said study investigator Philippa A. Garety, PhD, professor emerita of clinical psychology at the Institute of Psychiatry, Psychology, and Neuroscience at King’s College, London, England.
With more than 300 participants, AVATAR2 is the largest trial to access avatar therapy to date, Garety noted.
“What’s unique about this work is that technology allows us to create safe face-to-face encounters with a representation of a person’s voice and allows them to relate to that voice in a new way,” she added.
The findings were published online in Nature Medicine.
A Decade of Research
Auditory verbal hallucinations are common in patients with schizophrenia, but currently available therapies can be ineffective, investigators wrote.
The therapy allows patients to customize how the avatar looks and sounds. Face-to-face dialogues are then conducted between the patients and avatars in order to build empowerment. A trained therapist provides support during these sessions.
As previously reported, the creator of avatar therapy, Julian Leff, MD, presented promising results from a pilot study of 26 patients at the International Congress of the Royal College of Psychiatrists in 2014.
“Opening up a dialogue between a patient and the voice they’ve been hearing is powerful,” said Leff, who was emeritus professor at the Institute of Psychiatry in London at the time.
In 2018, a randomized single-site study (AVATAR1) of 150 participants showed that the intervention was associated with a greater decrease in voice severity at 12 weeks vs supportive therapy. Past research led to the idea of incorporating personalization to better optimize the experience.
Garety noted that AVATAR2 is the largest trial to date of the therapy, as well as the first multisite trial to test the intervention, which was important in order to determine whether it could work outside of a research setting.
The study included 345 participants (61.4% men; mean age, 39.6 years) from three sites in England and one in Scotland. All were randomly assigned to receive TAU alone (n = 115), TAU plus AVATAR-Brief (n = 116), or TAU plus AVATAR-Extended (n = 114).
TAU typically included use of antipsychotics, as well as outpatient psychiatric visits and follow-up by case managers and care coordinators.
“We didn’t interfere with treatment as usual. We wanted to test whether adding this therapy to [TAU] would enhance effects and provide better treatment for their voices,” Garety noted.
AVATAR-Brief included a standardized process that focused on such things as self-esteem and assertiveness. AVATAR-Extended had two phases. In the first, participants received AVATAR-Brief therapy, whereas the second phase offered a more personalized intervention.
An ‘Unusual Finding’
The study’s primary outcome was voice-related distress at 16 and 28 weeks. Although the TAU plus AVATAR-Extended group did show a significant decrease in distress at 16 weeks vs TAU alone (–1.6 points; P = .029), the improvement was no longer significant at the 28-week follow-up (P = .175). The same was also true for the key secondary outcome of reduction in voice severity (–2.32 points; P = .009 at 16 weeks but P =.1 at 28 weeks).
The investigators noted that this might be caused by the number of dropouts in the AVATAR-Extended group by the 28-week timepoint. The completion rate for those patients was only 58%. The completion rate for the shorter, AVATAR-Brief group was 82%.
On the other hand, the other key secondary outcome of voice frequency was significantly reduced with AVATAR-Extended at both 16 weeks (–0.62 point; P = .01) and 28 weeks (–0.89 point; P = .003).
“This is an unusual finding. We’re not aware of any other psychological therapy that shows a reduction in the occurrence of the voice,” Garety said.
For TAU plus AVATAR-Brief, there were improvements at 16 weeks for distress (-1.05 points; P = .035) vs TAU alone. However, the researchers noted that this version of the therapy was just below the prespecified threshold for a clinically significant change and was at the threshold for statistical significance.
Although the shorter therapy was associated with a reduction in voice severity level at 16 weeks (–2.04 points; P = .017) vs TAU alone, there was no reduction in distress or voice severity at 28 weeks. There was no improvement in voice frequency at either timepoint.
Both the brief and the extended versions of AVATAR therapy showed improved mood and anxiety levels at 16 weeks and sustained improvement in well-being and recovery, the researchers noted.
“The short version, as expected, did deliver benefits posttreatment, but clearly the extended, optimized version outperformed the brief version. It had stronger and more lasting effects across quite a wide range of outcomes that matter to people who hear voices,” Garety said.
“In the extended version, people felt more empowered. And in just that version, the frequency of voices was reduced, which is a very important outcome,” she added.
Safety Issues?
There were 58 serious adverse events (SAEs) in total, with 51% of those occurring in the AVATAR-Extended group. Two participants in that group died; however, independent reviews deemed these events as not related to the intervention.
In addition, there were no “definitely related” SAEs and only a small number of “possibly related” SAEs, which typically included hospitalization with other contributory factors.
Garety noted during a press briefing that AVATAR therapy has now been demonstrated to be safe across two large trials.
Study limitations cited included no direct comparison between AVATAR-Brief and AVATAR-Extended or between AVATAR therapy and a different type of psychological treatment.
Overall, “we recommend that future development and provision of AVATAR therapy is primarily guided” by the AVATAR-Extended protocol, the investigators wrote.
Because the therapy was recommended by a National Institute for Health and Care Excellence Early Value Assessment, the investigators are now seeking to provide it in routine National Health Service settings to gather further real-world evidence of effectiveness over the next 3 years.
Next Steps
Although the intervention isn’t currently available to everybody who might be seeking it, “there’s a pipeline of movement from research into treatment and it’s moving towards the next stage of delivery,” Garety said.
Investigators are also looking into cultural adaptations for the therapy so it can be used in different locales, including Ethiopia and India, she added. There isn’t a US version yet, but Garety noted that investigators in Canada are looking at similar research and suspects that will also occur in the United States soon.
“We’re pioneers in this work, and it now needs to be going international and into services,” she said. “We have had many people who hear voices say what an amazing experience this has been. So, I feel very proud and excited to have been able to be part of this.”
At the press briefing, Miranda Wolpert, director of mental health at Wellcome, which funded the study, noted that it is encouraging to see the development of a new intervention that could potentially change the lives of patients across the world.
“We know that psychosis can start early in life, stopping people from having the jobs and relationships they want and from achieving the goals they want. This intervention was developed with those people to help them address an issue that really troubles them,” Wolpert said.
“For me, this represents part of a revolution we are starting to see in terms of mental health interventions and the potential impact on mental health science,” she added.
Digital Placebo Effect?
Commenting on the findings, John Torous, MD, a psychiatrist and director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said there is a need for new treatments for schizophrenia that work with different mechanisms.
“We have a lot of medication studies but not as many innovative therapy studies. I think it’s exciting that the results, at least in the shorter-term outcome, were positive. And I think that’s something that can give people hope in using these new technologies,” said Torous, who is also an assistant professor of psychiatry at Harvard Medical School, Boston, and was not involved with the research.
Still, he did note some study limitations, including whether there could have been some type of “digital placebo effect” from the therapy.
“If you tell people they’re getting high-tech advanced digital care, that may have some effect,” he said, adding that “it’s always interesting” to tease out the benefit being delivered by the technology vs the delivery mechanism itself — or some combination of both.
Torous added, though, that it’s very difficult to have a rigorous digital control group. “It’s not necessarily a fault of their study, but it’s something to keep in mind when interpreting what the results are.”
He also noted that he would have liked to have seen a direct comparison between this new kind of psychological therapy vs standard psychological therapy, such as cognitive-behavioral therapy.
In addition, he wondered about expenses and scalability of the intervention, and whether patients would need to go to a specialized center to undergo treatment. Torous mentioned that a version involving virtual reality could perhaps make this more scalable in the future.
Overall, he said that what the investigators are currently doing is very innovative. “It’s exciting that we’re talking about the next steps. Giving people new options for psychological therapy that may be effective for their disorders is really wonderful to see,” Torous said.
The study was funded by the National Institute for Health and Care Research (NIHR), the Wellcome Trust King’s Clinical Research Facility, the NIHR Maudsley Biomedical Research Centre and Maudsley NHS Foundation Trust, King’s College London, the Manchester Biomedical Research Centre, and NHS Research Scotland, as well as by a grant from Wellcome. Garety reports being an unpaid scientific adviser to Avatar Therapy. Financial disclosures for the other investigators are fully listed in the original article. Torous reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM NATURE MEDICINE
Commentary: Factors Affecting PsA and Updated Therapy Efficacy Data, November 2024

Smoking is another important modifiable environmental factor. Smoking generally has an adverse impact on treatment. In a post hoc analysis of pooled data from phase 2 and 3 trials and a long-term extension study involving 914 patients with PsA and 372 patients with ankylosing spondylitis who received tofacitinib (a Janus kinase inhibitor) or placebo, Ogdie and coworkers assessed the impact of smoking on treatment efficacy and safety. The efficacy rates were generally similar in current/past smokers and never-smokers. The incidence rates of treatment-emergent adverse events were higher in current/past smokers compared with never-smokers. Thus, in contrast to tumor necrosis factor inhibitors, smoking status may not have an impact on tofacitinib efficacy. However, current/past smokers experienced increased rates of adverse events.
Secukinumab, an anti-interleukin (IL)-17A antibody, is an established treatment for PsA and is approved for use as fixed-dose (150/300 mg) subcutaneous injections. The efficacy and safety of weight-based intravenous (IV) therapy is unknown. Kivitz and colleagues recently reported the results of the phase 3 INVIGORATE-2 trial, in which 381 patients with active PsA and either plaque psoriasis or nail psoriasis were randomly assigned to receive IV secukinumab or placebo with crossover to IV secukinumab at week 16. They demonstrated that at week 16, IV secukinumab significantly improved the American College of Rheumatology 50 response rate (ACR50) compared with placebo (31.4% vs 6.3%; adjusted P < .0001). Improvements were observed as early as week 4 and were sustained through week 52. No new safety signals were reported. Thus, IV secukinumab is a safe and efficacious treatment for PsA. This mode of administration of secukinumab is a welcome addition to the PsA therapeutic armamentarium.
There are many targeted therapies available for PsA. However, data on comparative effectiveness is lacking. Kristensen and associates reported the results of an interim analysis of the PRO-SPIRIT real-world study that included 1192 patients with PsA across six countries who initiated or switched to a new biologic or targeted synthetic disease-modifying antirheumatic drug. They showed that at 3 months, ixekizumab significantly improved clinical disease activity in patients with PsA compared with IL-12/23 inhibitors and IL-23 inhibitors. The improvements in the joints were similar to those with TNF inhibitors and JAK inhibitors, but the improvement in psoriasis was higher. Thus, ixekizumab leads to rapid response to active skin and musculoskeletal disease activity in PsA. Comparative data on treatment persistence as well as adverse events are required.
Smoking is another important modifiable environmental factor. Smoking generally has an adverse impact on treatment. In a post hoc analysis of pooled data from phase 2 and 3 trials and a long-term extension study involving 914 patients with PsA and 372 patients with ankylosing spondylitis who received tofacitinib (a Janus kinase inhibitor) or placebo, Ogdie and coworkers assessed the impact of smoking on treatment efficacy and safety. The efficacy rates were generally similar in current/past smokers and never-smokers. The incidence rates of treatment-emergent adverse events were higher in current/past smokers compared with never-smokers. Thus, in contrast to tumor necrosis factor inhibitors, smoking status may not have an impact on tofacitinib efficacy. However, current/past smokers experienced increased rates of adverse events.
Secukinumab, an anti-interleukin (IL)-17A antibody, is an established treatment for PsA and is approved for use as fixed-dose (150/300 mg) subcutaneous injections. The efficacy and safety of weight-based intravenous (IV) therapy is unknown. Kivitz and colleagues recently reported the results of the phase 3 INVIGORATE-2 trial, in which 381 patients with active PsA and either plaque psoriasis or nail psoriasis were randomly assigned to receive IV secukinumab or placebo with crossover to IV secukinumab at week 16. They demonstrated that at week 16, IV secukinumab significantly improved the American College of Rheumatology 50 response rate (ACR50) compared with placebo (31.4% vs 6.3%; adjusted P < .0001). Improvements were observed as early as week 4 and were sustained through week 52. No new safety signals were reported. Thus, IV secukinumab is a safe and efficacious treatment for PsA. This mode of administration of secukinumab is a welcome addition to the PsA therapeutic armamentarium.
There are many targeted therapies available for PsA. However, data on comparative effectiveness is lacking. Kristensen and associates reported the results of an interim analysis of the PRO-SPIRIT real-world study that included 1192 patients with PsA across six countries who initiated or switched to a new biologic or targeted synthetic disease-modifying antirheumatic drug. They showed that at 3 months, ixekizumab significantly improved clinical disease activity in patients with PsA compared with IL-12/23 inhibitors and IL-23 inhibitors. The improvements in the joints were similar to those with TNF inhibitors and JAK inhibitors, but the improvement in psoriasis was higher. Thus, ixekizumab leads to rapid response to active skin and musculoskeletal disease activity in PsA. Comparative data on treatment persistence as well as adverse events are required.
Smoking is another important modifiable environmental factor. Smoking generally has an adverse impact on treatment. In a post hoc analysis of pooled data from phase 2 and 3 trials and a long-term extension study involving 914 patients with PsA and 372 patients with ankylosing spondylitis who received tofacitinib (a Janus kinase inhibitor) or placebo, Ogdie and coworkers assessed the impact of smoking on treatment efficacy and safety. The efficacy rates were generally similar in current/past smokers and never-smokers. The incidence rates of treatment-emergent adverse events were higher in current/past smokers compared with never-smokers. Thus, in contrast to tumor necrosis factor inhibitors, smoking status may not have an impact on tofacitinib efficacy. However, current/past smokers experienced increased rates of adverse events.
Secukinumab, an anti-interleukin (IL)-17A antibody, is an established treatment for PsA and is approved for use as fixed-dose (150/300 mg) subcutaneous injections. The efficacy and safety of weight-based intravenous (IV) therapy is unknown. Kivitz and colleagues recently reported the results of the phase 3 INVIGORATE-2 trial, in which 381 patients with active PsA and either plaque psoriasis or nail psoriasis were randomly assigned to receive IV secukinumab or placebo with crossover to IV secukinumab at week 16. They demonstrated that at week 16, IV secukinumab significantly improved the American College of Rheumatology 50 response rate (ACR50) compared with placebo (31.4% vs 6.3%; adjusted P < .0001). Improvements were observed as early as week 4 and were sustained through week 52. No new safety signals were reported. Thus, IV secukinumab is a safe and efficacious treatment for PsA. This mode of administration of secukinumab is a welcome addition to the PsA therapeutic armamentarium.
There are many targeted therapies available for PsA. However, data on comparative effectiveness is lacking. Kristensen and associates reported the results of an interim analysis of the PRO-SPIRIT real-world study that included 1192 patients with PsA across six countries who initiated or switched to a new biologic or targeted synthetic disease-modifying antirheumatic drug. They showed that at 3 months, ixekizumab significantly improved clinical disease activity in patients with PsA compared with IL-12/23 inhibitors and IL-23 inhibitors. The improvements in the joints were similar to those with TNF inhibitors and JAK inhibitors, but the improvement in psoriasis was higher. Thus, ixekizumab leads to rapid response to active skin and musculoskeletal disease activity in PsA. Comparative data on treatment persistence as well as adverse events are required.
Expanding Treatment Options for Psoriatic Arthritis in Adults
Over the past two decades, the treatment of active psoriatic arthritis (PsA) has been transformed by targeted biologic therapies. In this ReCAP, Dr Eric Ruderman, from the Feinberg School of Medicine at Northwestern University, reports on the safety and efficacy of several approved therapies.
Dr Ruderman first discusses different treatment options, including TNF inhibitors, which have been the standard first-line therapy for nearly two decades. He also reports that other agents, including Il-12/23 inhibitors abatacept, apremilast, and a number of JAK inhibitors, have shown efficacy for patients who don’t respond well or are intolerant to TNF inhibitors.
In recent years, various specific IL-23 inhibitors have been approved to treat psoriasis and, most recently, psoriatic arthritis in psoriasis. Guselkumab, risankizumab, and tildrakizumab were approved to treat the skin disease.
In psoriatic arthritis, guselkumab and risankizumab have also been approved. These drugs have shown more efficacy than the IL-12/23 inhibitor, according to Ruderman, and show a lower risk for infection compared with some of the other agents.
--
Eric M. Ruderman, MD, Professor, Department of Medicine, Division of Rheumatology, Northwestern University Feinberg School of Medicine; Associate Division Chief, Clinical Affairs, Department of Rheumatology, Northwestern Medical Group, Chicago, Illinois
Eric M. Ruderman, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Amgen; Bristol Myers Squibb; Janssen; Lilly; Merck; Novartis; NS Pharma; UCB
Over the past two decades, the treatment of active psoriatic arthritis (PsA) has been transformed by targeted biologic therapies. In this ReCAP, Dr Eric Ruderman, from the Feinberg School of Medicine at Northwestern University, reports on the safety and efficacy of several approved therapies.
Dr Ruderman first discusses different treatment options, including TNF inhibitors, which have been the standard first-line therapy for nearly two decades. He also reports that other agents, including Il-12/23 inhibitors abatacept, apremilast, and a number of JAK inhibitors, have shown efficacy for patients who don’t respond well or are intolerant to TNF inhibitors.
In recent years, various specific IL-23 inhibitors have been approved to treat psoriasis and, most recently, psoriatic arthritis in psoriasis. Guselkumab, risankizumab, and tildrakizumab were approved to treat the skin disease.
In psoriatic arthritis, guselkumab and risankizumab have also been approved. These drugs have shown more efficacy than the IL-12/23 inhibitor, according to Ruderman, and show a lower risk for infection compared with some of the other agents.
--
Eric M. Ruderman, MD, Professor, Department of Medicine, Division of Rheumatology, Northwestern University Feinberg School of Medicine; Associate Division Chief, Clinical Affairs, Department of Rheumatology, Northwestern Medical Group, Chicago, Illinois
Eric M. Ruderman, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Amgen; Bristol Myers Squibb; Janssen; Lilly; Merck; Novartis; NS Pharma; UCB
Over the past two decades, the treatment of active psoriatic arthritis (PsA) has been transformed by targeted biologic therapies. In this ReCAP, Dr Eric Ruderman, from the Feinberg School of Medicine at Northwestern University, reports on the safety and efficacy of several approved therapies.
Dr Ruderman first discusses different treatment options, including TNF inhibitors, which have been the standard first-line therapy for nearly two decades. He also reports that other agents, including Il-12/23 inhibitors abatacept, apremilast, and a number of JAK inhibitors, have shown efficacy for patients who don’t respond well or are intolerant to TNF inhibitors.
In recent years, various specific IL-23 inhibitors have been approved to treat psoriasis and, most recently, psoriatic arthritis in psoriasis. Guselkumab, risankizumab, and tildrakizumab were approved to treat the skin disease.
In psoriatic arthritis, guselkumab and risankizumab have also been approved. These drugs have shown more efficacy than the IL-12/23 inhibitor, according to Ruderman, and show a lower risk for infection compared with some of the other agents.
--
Eric M. Ruderman, MD, Professor, Department of Medicine, Division of Rheumatology, Northwestern University Feinberg School of Medicine; Associate Division Chief, Clinical Affairs, Department of Rheumatology, Northwestern Medical Group, Chicago, Illinois
Eric M. Ruderman, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Amgen; Bristol Myers Squibb; Janssen; Lilly; Merck; Novartis; NS Pharma; UCB

Will Psychedelics Break the Major Depression Logjam?
With tens of millions of Euros in the offing, researchers across the European Union have eagerly taken up the gauntlet to find novel interventions for difficult-to-treat mental health and pain conditions. Their target is psychedelics, including classic compounds like psilocybin and atypical ones like ketamine and MDMA. Some of these still carry a stigma as party drugs and spiritual gateways to holotropic experiences.
Twelve groups make up the European College of Neuropsychopharmacology’s psychedelic research network. Along with several affiliates, the groups span nine countries (Denmark, Sweden, Finland, Switzerland, Germany, the Netherlands, the Czech Republic, Greece, and the United Kingdom) and are focused on the use of psychedelic compounds as potential treatments for psychiatric conditions like treatment-resistant depression, addiction, attention-deficit/hyperactivity disorder, anorexia, and obsessive-compulsive disorder.
One of the largest endeavors is PsyPal, a 4-year, randomized controlled trial investigating the potential of psilocybin for treating psychological distress in palliative care patients with life-limiting conditions. PsyPal is the first multisite clinical trial funded by the European Union to explore psychedelic-assisted therapy.
At PsyPal’s helm is Robert Schoevers, MD, PhD, professor of psychiatry and Department Head at University Medical Center Groningen (UMCG), Groningen, the Netherlands, a major hub for psychedelic research.
Schoevers is a bit of a pioneer who said he entered psychedelic research somewhat reluctantly. A decade ago, a colleague showed him a few papers on ketamine and depression. Because UMCG has a large population of patients with treatment-resistant depression, he agreed to do a pilot study. Since then, he has put together an interdisciplinary team of 25 researchers, published numerous papers, and currently has seven studies, including PsyPal, in various stages of progress.
Schoevers is also building a large national consortium that aims to investigate and, if shown effective, implement novel psychiatry treatments much more rapidly and efficiently than current drug development and approval processes, which can take 12 years or longer. He has just secured millions in government funding to start this process.
Next year, Schoevers and his team will decide to test either MDMA for posttraumatic stress disorder (PTSD) or psilocybin for depression in a large clinical trial, with the aim of getting a treatment as near to formal registration as possible. This will involve working with the European Medicines Agency and its Dutch counterpart, talking to experts who are familiar with the US Food and Drug Administration’s rejection of Lykos Therapeutics’ MDMA treatment for PTSD, and working directly with patients through the National Patient Alliance. The team is also talking to insurers and pharma companies.
The ultimate goal is to “see if we can build a platform in the Netherlands that would have a European perspective, serve as a point of entry for researchers with good ideas, and [attract] public funding as well as companies who have interesting compounds we think would be worthwhile to study,” Schoevers said.
His multiple endeavors emphasize a transdisciplinary and transdiagnostic approach he has been honing for decades. He and his colleagues are investigating the clinical, psychological, and neurobiological parallels between different treatment- resistant conditions and seeking to understand how contextual factors might influence patients, experiences, and outcomes.
Connecting the Dots
Jens H. van Dalfsen, PhD, a postdoctoral researcher in biological psychiatry, is the principal investigator of another UMCG group looking into the neurobiological mechanisms of major depressive disorder and treatment-resistant depression. His team’s strategy entails an elaborate coordination between the preclinical and clinical research settings.
For example, Sarah Massetti, a PhD candidate in biological psychiatry, is using blood samples collected in clinical trials to investigate the molecular mechanisms underpinning the neuroplasticity and immune-modulating effects produced by psychedelic compounds.
Another line of research spearheaded by Rutger Boesjes, a PhD candidate in biological psychiatry, is exploring the interactions between drugs like ketamine and the circadian system and how they might relate to antidepressant responses in animal models. It could be that the timing of administration of these drugs is relevant, he explained.
The Patient Factor
How psychedelics work and in whom is a big question for the UMCG team and across the research landscape.
“When researchers and the general public talk about psychedelics, they frequently refer to how they promote synaptic plasticity and new connections in the brain,” said van Dalfsen. “But traditional compounds also do that. So the ultimate question that we’ve been exploring is whether findings reflect an actual pharmacological effect or if expectancy also plays a role. In other words: How can we explain why psychedelics might or might not be effective in treatment-resistant patients?” he explained.
This is where the connection to the clinical experience becomes paramount and Joost Breeksema, PhD, comes in.
Breeksema divides his time between UMCG research and his role as executive director and co-founder of the Open Foundation, a nonprofit dedicated to advancing scientific psychedelic research. The work he’s doing outside the university is helping to frame the investigations of the wider group.
So far he has conducted two qualitative studies.
One was an off-label study in which patients with treatment-resistant depression were administered esketamine.
The other was a randomized clinical trial in which participants were blinded to a single 10- or 25-mg dose of psilocybin versus a 1-mg psilocybin microdose placebo that is too small to invoke any effects.
A key insight was the degree to which participants were unprepared for the intensity of their experiences, especially with regards to ketamine. Breeksema said the sessions might not have been so intense or negative for some participants had they been informed beforehand to expect the drugs could provoke “quite overwhelming experiences” and had they been accompanied by an experienced guide providing reassurance and support.
The format for the psilocybin trial met part of this criteria. Participants received a micro (placebo), medium, or high dose in a single session accompanied by two trained therapists. They then engaged in two sessions afterward to process their experiences. A single psilocybin experience appeared to be not enough or too much depending on the dose they were assigned and if they had prior experience with the compound.
Trial participants also felt they needed more help making sense of the experience. “This is a common and important theme,” said Breeksema. “Think about it. If you’ve been depressed for 10, 15 years and … you uncover something and break through something that’s been stuck, you need to process it.”
Jeanine Kamphuis, PhD, a psychiatrist and senior researcher at UMCG and one of the trial study co-authors, explained that they want to find a way to identify who will be too overwhelmed by these experiences if the dose should be adjusted or if some time needs to pass between dosing sessions. They also want to spend more time preparing patients for these sessions.
She emphasized that the studies have provided a reality check. “These are not wonder pills or wonder experiences. And in these types of patients, they’re not intended for a personal growth experience,” she said. “You have a patient who is sitting in front of you who seeks therapy and relief from very severe mood complaints, and the suffering is high,” she said, adding that expectancy bias further complicates patient participation and, likely, outcomes.
The Challenges
For all the potential and opportunity that psychedelics may hold for treatment, UMCG’s work has underscored some challenges.
The field of psychedelic research is characterized by methodological issues, explained van Dalfsen, such as blinding, expectancy, and overestimation of treatment effects. When looking at efficacy, “Is it the compound or the expectancy and promise? This is why it’s important to study how the drugs differ from each other in their biological effects and why they are or are not effective,” he said.
The team has also experienced issues with trial recruitment.
Martijn Godschalk, MD, a PhD candidate in psychiatry, has been addressing this problem while working on RESET-TRD, a phase 3, randomized controlled trial comparing an oral esketamine drink with electroconvulsive therapy in patients with treatment-resistant depression.
He’s been coordinating with local university hospitals, general hospitals, and municipal healthcare clinics to meet inclusion criteria and ensure the trial has enough power to demonstrate effectiveness. In turn, these sites are able to participate in a trial they wouldn’t normally be involved in due to lack of resources.
But Godschalk said he was concerned that many patients have gotten wind of the hype surrounding psychedelic treatments within psychiatry — a factor that has contributed to recruitment challenges. “There are a lot of patients who are interested in the non-registered drug and don’t necessarily have an interest in the other [control] arm,” he said.
Despite the challenges, the classic psychedelics such as MDMA and psilocybin “seem to catalyze a psychological process that may be harder to get with regular psychotherapies,” said Schoevers.
He remains cautious, noting there are still unanswered questions, such as who are the best candidates for these drugs and whether they might cause harm in certain patients while benefiting others. “I do think that this is the first time in 20 or 30 years that there is a group of potential treatments that would really make a difference.”
Schoevers received grants and other funding from The Netherlands Organisation for Health Research & Development, Horizon 2020, Horizon 2023, the National Institute of Mental Health (USA), UMCG, Stichting tot Steun VCVGZ, Nationaal programma Groningen, Healthcare Innovation Funds, Janssen Pharmaceuticals, Novartis, Compass Pathways, Clexio Biosciences, and GH research.
A version of this article appeared on Medscape.com.
With tens of millions of Euros in the offing, researchers across the European Union have eagerly taken up the gauntlet to find novel interventions for difficult-to-treat mental health and pain conditions. Their target is psychedelics, including classic compounds like psilocybin and atypical ones like ketamine and MDMA. Some of these still carry a stigma as party drugs and spiritual gateways to holotropic experiences.
Twelve groups make up the European College of Neuropsychopharmacology’s psychedelic research network. Along with several affiliates, the groups span nine countries (Denmark, Sweden, Finland, Switzerland, Germany, the Netherlands, the Czech Republic, Greece, and the United Kingdom) and are focused on the use of psychedelic compounds as potential treatments for psychiatric conditions like treatment-resistant depression, addiction, attention-deficit/hyperactivity disorder, anorexia, and obsessive-compulsive disorder.
One of the largest endeavors is PsyPal, a 4-year, randomized controlled trial investigating the potential of psilocybin for treating psychological distress in palliative care patients with life-limiting conditions. PsyPal is the first multisite clinical trial funded by the European Union to explore psychedelic-assisted therapy.
At PsyPal’s helm is Robert Schoevers, MD, PhD, professor of psychiatry and Department Head at University Medical Center Groningen (UMCG), Groningen, the Netherlands, a major hub for psychedelic research.
Schoevers is a bit of a pioneer who said he entered psychedelic research somewhat reluctantly. A decade ago, a colleague showed him a few papers on ketamine and depression. Because UMCG has a large population of patients with treatment-resistant depression, he agreed to do a pilot study. Since then, he has put together an interdisciplinary team of 25 researchers, published numerous papers, and currently has seven studies, including PsyPal, in various stages of progress.
Schoevers is also building a large national consortium that aims to investigate and, if shown effective, implement novel psychiatry treatments much more rapidly and efficiently than current drug development and approval processes, which can take 12 years or longer. He has just secured millions in government funding to start this process.
Next year, Schoevers and his team will decide to test either MDMA for posttraumatic stress disorder (PTSD) or psilocybin for depression in a large clinical trial, with the aim of getting a treatment as near to formal registration as possible. This will involve working with the European Medicines Agency and its Dutch counterpart, talking to experts who are familiar with the US Food and Drug Administration’s rejection of Lykos Therapeutics’ MDMA treatment for PTSD, and working directly with patients through the National Patient Alliance. The team is also talking to insurers and pharma companies.
The ultimate goal is to “see if we can build a platform in the Netherlands that would have a European perspective, serve as a point of entry for researchers with good ideas, and [attract] public funding as well as companies who have interesting compounds we think would be worthwhile to study,” Schoevers said.
His multiple endeavors emphasize a transdisciplinary and transdiagnostic approach he has been honing for decades. He and his colleagues are investigating the clinical, psychological, and neurobiological parallels between different treatment- resistant conditions and seeking to understand how contextual factors might influence patients, experiences, and outcomes.
Connecting the Dots
Jens H. van Dalfsen, PhD, a postdoctoral researcher in biological psychiatry, is the principal investigator of another UMCG group looking into the neurobiological mechanisms of major depressive disorder and treatment-resistant depression. His team’s strategy entails an elaborate coordination between the preclinical and clinical research settings.
For example, Sarah Massetti, a PhD candidate in biological psychiatry, is using blood samples collected in clinical trials to investigate the molecular mechanisms underpinning the neuroplasticity and immune-modulating effects produced by psychedelic compounds.
Another line of research spearheaded by Rutger Boesjes, a PhD candidate in biological psychiatry, is exploring the interactions between drugs like ketamine and the circadian system and how they might relate to antidepressant responses in animal models. It could be that the timing of administration of these drugs is relevant, he explained.
The Patient Factor
How psychedelics work and in whom is a big question for the UMCG team and across the research landscape.
“When researchers and the general public talk about psychedelics, they frequently refer to how they promote synaptic plasticity and new connections in the brain,” said van Dalfsen. “But traditional compounds also do that. So the ultimate question that we’ve been exploring is whether findings reflect an actual pharmacological effect or if expectancy also plays a role. In other words: How can we explain why psychedelics might or might not be effective in treatment-resistant patients?” he explained.
This is where the connection to the clinical experience becomes paramount and Joost Breeksema, PhD, comes in.
Breeksema divides his time between UMCG research and his role as executive director and co-founder of the Open Foundation, a nonprofit dedicated to advancing scientific psychedelic research. The work he’s doing outside the university is helping to frame the investigations of the wider group.
So far he has conducted two qualitative studies.
One was an off-label study in which patients with treatment-resistant depression were administered esketamine.
The other was a randomized clinical trial in which participants were blinded to a single 10- or 25-mg dose of psilocybin versus a 1-mg psilocybin microdose placebo that is too small to invoke any effects.
A key insight was the degree to which participants were unprepared for the intensity of their experiences, especially with regards to ketamine. Breeksema said the sessions might not have been so intense or negative for some participants had they been informed beforehand to expect the drugs could provoke “quite overwhelming experiences” and had they been accompanied by an experienced guide providing reassurance and support.
The format for the psilocybin trial met part of this criteria. Participants received a micro (placebo), medium, or high dose in a single session accompanied by two trained therapists. They then engaged in two sessions afterward to process their experiences. A single psilocybin experience appeared to be not enough or too much depending on the dose they were assigned and if they had prior experience with the compound.
Trial participants also felt they needed more help making sense of the experience. “This is a common and important theme,” said Breeksema. “Think about it. If you’ve been depressed for 10, 15 years and … you uncover something and break through something that’s been stuck, you need to process it.”
Jeanine Kamphuis, PhD, a psychiatrist and senior researcher at UMCG and one of the trial study co-authors, explained that they want to find a way to identify who will be too overwhelmed by these experiences if the dose should be adjusted or if some time needs to pass between dosing sessions. They also want to spend more time preparing patients for these sessions.
She emphasized that the studies have provided a reality check. “These are not wonder pills or wonder experiences. And in these types of patients, they’re not intended for a personal growth experience,” she said. “You have a patient who is sitting in front of you who seeks therapy and relief from very severe mood complaints, and the suffering is high,” she said, adding that expectancy bias further complicates patient participation and, likely, outcomes.
The Challenges
For all the potential and opportunity that psychedelics may hold for treatment, UMCG’s work has underscored some challenges.
The field of psychedelic research is characterized by methodological issues, explained van Dalfsen, such as blinding, expectancy, and overestimation of treatment effects. When looking at efficacy, “Is it the compound or the expectancy and promise? This is why it’s important to study how the drugs differ from each other in their biological effects and why they are or are not effective,” he said.
The team has also experienced issues with trial recruitment.
Martijn Godschalk, MD, a PhD candidate in psychiatry, has been addressing this problem while working on RESET-TRD, a phase 3, randomized controlled trial comparing an oral esketamine drink with electroconvulsive therapy in patients with treatment-resistant depression.
He’s been coordinating with local university hospitals, general hospitals, and municipal healthcare clinics to meet inclusion criteria and ensure the trial has enough power to demonstrate effectiveness. In turn, these sites are able to participate in a trial they wouldn’t normally be involved in due to lack of resources.
But Godschalk said he was concerned that many patients have gotten wind of the hype surrounding psychedelic treatments within psychiatry — a factor that has contributed to recruitment challenges. “There are a lot of patients who are interested in the non-registered drug and don’t necessarily have an interest in the other [control] arm,” he said.
Despite the challenges, the classic psychedelics such as MDMA and psilocybin “seem to catalyze a psychological process that may be harder to get with regular psychotherapies,” said Schoevers.
He remains cautious, noting there are still unanswered questions, such as who are the best candidates for these drugs and whether they might cause harm in certain patients while benefiting others. “I do think that this is the first time in 20 or 30 years that there is a group of potential treatments that would really make a difference.”
Schoevers received grants and other funding from The Netherlands Organisation for Health Research & Development, Horizon 2020, Horizon 2023, the National Institute of Mental Health (USA), UMCG, Stichting tot Steun VCVGZ, Nationaal programma Groningen, Healthcare Innovation Funds, Janssen Pharmaceuticals, Novartis, Compass Pathways, Clexio Biosciences, and GH research.
A version of this article appeared on Medscape.com.
With tens of millions of Euros in the offing, researchers across the European Union have eagerly taken up the gauntlet to find novel interventions for difficult-to-treat mental health and pain conditions. Their target is psychedelics, including classic compounds like psilocybin and atypical ones like ketamine and MDMA. Some of these still carry a stigma as party drugs and spiritual gateways to holotropic experiences.
Twelve groups make up the European College of Neuropsychopharmacology’s psychedelic research network. Along with several affiliates, the groups span nine countries (Denmark, Sweden, Finland, Switzerland, Germany, the Netherlands, the Czech Republic, Greece, and the United Kingdom) and are focused on the use of psychedelic compounds as potential treatments for psychiatric conditions like treatment-resistant depression, addiction, attention-deficit/hyperactivity disorder, anorexia, and obsessive-compulsive disorder.
One of the largest endeavors is PsyPal, a 4-year, randomized controlled trial investigating the potential of psilocybin for treating psychological distress in palliative care patients with life-limiting conditions. PsyPal is the first multisite clinical trial funded by the European Union to explore psychedelic-assisted therapy.
At PsyPal’s helm is Robert Schoevers, MD, PhD, professor of psychiatry and Department Head at University Medical Center Groningen (UMCG), Groningen, the Netherlands, a major hub for psychedelic research.
Schoevers is a bit of a pioneer who said he entered psychedelic research somewhat reluctantly. A decade ago, a colleague showed him a few papers on ketamine and depression. Because UMCG has a large population of patients with treatment-resistant depression, he agreed to do a pilot study. Since then, he has put together an interdisciplinary team of 25 researchers, published numerous papers, and currently has seven studies, including PsyPal, in various stages of progress.
Schoevers is also building a large national consortium that aims to investigate and, if shown effective, implement novel psychiatry treatments much more rapidly and efficiently than current drug development and approval processes, which can take 12 years or longer. He has just secured millions in government funding to start this process.
Next year, Schoevers and his team will decide to test either MDMA for posttraumatic stress disorder (PTSD) or psilocybin for depression in a large clinical trial, with the aim of getting a treatment as near to formal registration as possible. This will involve working with the European Medicines Agency and its Dutch counterpart, talking to experts who are familiar with the US Food and Drug Administration’s rejection of Lykos Therapeutics’ MDMA treatment for PTSD, and working directly with patients through the National Patient Alliance. The team is also talking to insurers and pharma companies.
The ultimate goal is to “see if we can build a platform in the Netherlands that would have a European perspective, serve as a point of entry for researchers with good ideas, and [attract] public funding as well as companies who have interesting compounds we think would be worthwhile to study,” Schoevers said.
His multiple endeavors emphasize a transdisciplinary and transdiagnostic approach he has been honing for decades. He and his colleagues are investigating the clinical, psychological, and neurobiological parallels between different treatment- resistant conditions and seeking to understand how contextual factors might influence patients, experiences, and outcomes.
Connecting the Dots
Jens H. van Dalfsen, PhD, a postdoctoral researcher in biological psychiatry, is the principal investigator of another UMCG group looking into the neurobiological mechanisms of major depressive disorder and treatment-resistant depression. His team’s strategy entails an elaborate coordination between the preclinical and clinical research settings.
For example, Sarah Massetti, a PhD candidate in biological psychiatry, is using blood samples collected in clinical trials to investigate the molecular mechanisms underpinning the neuroplasticity and immune-modulating effects produced by psychedelic compounds.
Another line of research spearheaded by Rutger Boesjes, a PhD candidate in biological psychiatry, is exploring the interactions between drugs like ketamine and the circadian system and how they might relate to antidepressant responses in animal models. It could be that the timing of administration of these drugs is relevant, he explained.
The Patient Factor
How psychedelics work and in whom is a big question for the UMCG team and across the research landscape.
“When researchers and the general public talk about psychedelics, they frequently refer to how they promote synaptic plasticity and new connections in the brain,” said van Dalfsen. “But traditional compounds also do that. So the ultimate question that we’ve been exploring is whether findings reflect an actual pharmacological effect or if expectancy also plays a role. In other words: How can we explain why psychedelics might or might not be effective in treatment-resistant patients?” he explained.
This is where the connection to the clinical experience becomes paramount and Joost Breeksema, PhD, comes in.
Breeksema divides his time between UMCG research and his role as executive director and co-founder of the Open Foundation, a nonprofit dedicated to advancing scientific psychedelic research. The work he’s doing outside the university is helping to frame the investigations of the wider group.
So far he has conducted two qualitative studies.
One was an off-label study in which patients with treatment-resistant depression were administered esketamine.
The other was a randomized clinical trial in which participants were blinded to a single 10- or 25-mg dose of psilocybin versus a 1-mg psilocybin microdose placebo that is too small to invoke any effects.
A key insight was the degree to which participants were unprepared for the intensity of their experiences, especially with regards to ketamine. Breeksema said the sessions might not have been so intense or negative for some participants had they been informed beforehand to expect the drugs could provoke “quite overwhelming experiences” and had they been accompanied by an experienced guide providing reassurance and support.
The format for the psilocybin trial met part of this criteria. Participants received a micro (placebo), medium, or high dose in a single session accompanied by two trained therapists. They then engaged in two sessions afterward to process their experiences. A single psilocybin experience appeared to be not enough or too much depending on the dose they were assigned and if they had prior experience with the compound.
Trial participants also felt they needed more help making sense of the experience. “This is a common and important theme,” said Breeksema. “Think about it. If you’ve been depressed for 10, 15 years and … you uncover something and break through something that’s been stuck, you need to process it.”
Jeanine Kamphuis, PhD, a psychiatrist and senior researcher at UMCG and one of the trial study co-authors, explained that they want to find a way to identify who will be too overwhelmed by these experiences if the dose should be adjusted or if some time needs to pass between dosing sessions. They also want to spend more time preparing patients for these sessions.
She emphasized that the studies have provided a reality check. “These are not wonder pills or wonder experiences. And in these types of patients, they’re not intended for a personal growth experience,” she said. “You have a patient who is sitting in front of you who seeks therapy and relief from very severe mood complaints, and the suffering is high,” she said, adding that expectancy bias further complicates patient participation and, likely, outcomes.
The Challenges
For all the potential and opportunity that psychedelics may hold for treatment, UMCG’s work has underscored some challenges.
The field of psychedelic research is characterized by methodological issues, explained van Dalfsen, such as blinding, expectancy, and overestimation of treatment effects. When looking at efficacy, “Is it the compound or the expectancy and promise? This is why it’s important to study how the drugs differ from each other in their biological effects and why they are or are not effective,” he said.
The team has also experienced issues with trial recruitment.
Martijn Godschalk, MD, a PhD candidate in psychiatry, has been addressing this problem while working on RESET-TRD, a phase 3, randomized controlled trial comparing an oral esketamine drink with electroconvulsive therapy in patients with treatment-resistant depression.
He’s been coordinating with local university hospitals, general hospitals, and municipal healthcare clinics to meet inclusion criteria and ensure the trial has enough power to demonstrate effectiveness. In turn, these sites are able to participate in a trial they wouldn’t normally be involved in due to lack of resources.
But Godschalk said he was concerned that many patients have gotten wind of the hype surrounding psychedelic treatments within psychiatry — a factor that has contributed to recruitment challenges. “There are a lot of patients who are interested in the non-registered drug and don’t necessarily have an interest in the other [control] arm,” he said.
Despite the challenges, the classic psychedelics such as MDMA and psilocybin “seem to catalyze a psychological process that may be harder to get with regular psychotherapies,” said Schoevers.
He remains cautious, noting there are still unanswered questions, such as who are the best candidates for these drugs and whether they might cause harm in certain patients while benefiting others. “I do think that this is the first time in 20 or 30 years that there is a group of potential treatments that would really make a difference.”
Schoevers received grants and other funding from The Netherlands Organisation for Health Research & Development, Horizon 2020, Horizon 2023, the National Institute of Mental Health (USA), UMCG, Stichting tot Steun VCVGZ, Nationaal programma Groningen, Healthcare Innovation Funds, Janssen Pharmaceuticals, Novartis, Compass Pathways, Clexio Biosciences, and GH research.
A version of this article appeared on Medscape.com.