User login
Plastic Surgeon to Pay $5 Million for Restriction of Negative Reviews, Directing Fake Reviews
A Seattle plastic surgeon who illegally restricted patients from posting negative reviews about his practice and directed his staff to post fake positive reviews will pay $5 million for violating Washington state’s consumer protection law.
According to a July 1 consent decree, Javad Sajan, MD, and his practice Allure Esthetic must pay $1.5 million in restitution to 21,000 patients and $3.5 million to the state for manipulation of patient ratings.
In an April decision, US District Judge Ricardo S. Martinez sided with the state, ruling that Allure Esthetic’s actions violated the federal Consumer Review Fairness Act (CRFA).
“Writing a truthful review about a business should not subject you to threats or intimidation,” Mr. Ferguson said in a July 2 statement. “Consumers rely on reviews when determining who to trust, especially services that affect their health and safety. This resolution holds Allure accountable for brazenly violating that trust — and the law — and ensures the clinic stops its harmful conduct.”
In court documents, Dr. Sajan’s attorneys had argued that the agreements did not violate CRFA because patients had the opportunity to modify the language or decline signing them.
The surgeon’s practice is “pleased to have resolved its case with the Attorney General’s Office,” according to a statement provided by Dr. Sajan’s attorney. “The cooperative settlement, while not admitting fault and resolving claims asserted by both sides, allows Allure Esthetic to continue to focus on its core mission of providing compassionate care to patients and serving the community. The decision to settle was not an easy one, but it was necessary to allocate time and resources where they matter most — the patients.”
The dispute stemmed from NDAs that Dr. Sajan’s practice required patients to sign starting in 2017, according to Mr. Ferguson’s complaint. The terms instructed patients to contact the business directly if they had concerns rather than post a negative review.
If patients posted negative reviews, the clinic, in some cases, threatened litigation, according to the lawsuit. In other cases, patients were allegedly offered money and free services in exchange for taking the reviews down. Patients who accepted cash or services were required to sign a second agreement forbidding them from posting future negative reviews and imposing a $250,000 penalty for failure to comply, according to court documents.
In addition, Mr. Ferguson accused Dr. Sajan of creating fake positive accounts of patient experiences and buying fake followers on social media. State investigators found Dr. Sajan directed Allure Esthetic’s employees to create fake Gmail accounts to post the false reviews, many of which are still online today, according to the state’s complaint.
Mr. Ferguson also claimed Dr. Sajan and his practice manipulated social media to appear more popular by purchasing followers through an online vendor. The practice also allegedly used a social media bot tool to buy thousands of fake likes on Instagram, YouTube, and other social media.
After filing the lawsuit, Mr. Ferguson’s office uncovered further evidence of Dr. Sajan’s efforts to influence his professional reputation through fabrication, according to the July 2 release. Allure Esthetic “rigged” “best doctor” competitions hosted by local media outlets by paying staff and contractors to vote for Dr. Sajan as “best plastic surgeon” in the region, according to the release. The staff cast as many votes as websites allowed, despite not being patients of Allure Esthetic.
The practice also allegedly edited before-and-after photos of patients to make their results appear better and kept tens of thousands of dollars in rebates intended for its patients.
In addition to paying $5 million, the consent decree requires Dr. Sajan and his practice also:
- Stop posting or influencing consumer reviews; perform a full audit of all public reviews on Google, Yelp, and other third-party review platforms; and request removal of every review Allure Esthetic was involved in creating, posting, or shaping in any manner.
- Remove all misleading “before-and-after” photographs of plastic surgery procedures from its website and social media and stop altering photographs of future procedures.
- Cease use of and attempts to enforce all illegal NDAs and notify patients who previously signed them that they are released from the terms of those NDAs.
- Pay a third-party forensic accounting firm to perform a full, independent audit of Allure Esthetic’s consumer rebate program to identify consumers who are owed rebates that were unlawfully claimed by Allure Esthetic.
Additionally, the attorney general’s office will continue to monitor Allure Esthetic, and upon request, the practice must provide information that demonstrates its compliance with the consent decree for the next 10 years.
The practice must also develop internal policies and implement a training program to educate staff about nondeceptive advertising and compliance with consumer protection laws.
Dr. Sajan and his practice agreed to the terms of the consent decree, and the settlement is not considered an admission of liability.
A version of this article first appeared on Medscape.com.
A Seattle plastic surgeon who illegally restricted patients from posting negative reviews about his practice and directed his staff to post fake positive reviews will pay $5 million for violating Washington state’s consumer protection law.
According to a July 1 consent decree, Javad Sajan, MD, and his practice Allure Esthetic must pay $1.5 million in restitution to 21,000 patients and $3.5 million to the state for manipulation of patient ratings.
In an April decision, US District Judge Ricardo S. Martinez sided with the state, ruling that Allure Esthetic’s actions violated the federal Consumer Review Fairness Act (CRFA).
“Writing a truthful review about a business should not subject you to threats or intimidation,” Mr. Ferguson said in a July 2 statement. “Consumers rely on reviews when determining who to trust, especially services that affect their health and safety. This resolution holds Allure accountable for brazenly violating that trust — and the law — and ensures the clinic stops its harmful conduct.”
In court documents, Dr. Sajan’s attorneys had argued that the agreements did not violate CRFA because patients had the opportunity to modify the language or decline signing them.
The surgeon’s practice is “pleased to have resolved its case with the Attorney General’s Office,” according to a statement provided by Dr. Sajan’s attorney. “The cooperative settlement, while not admitting fault and resolving claims asserted by both sides, allows Allure Esthetic to continue to focus on its core mission of providing compassionate care to patients and serving the community. The decision to settle was not an easy one, but it was necessary to allocate time and resources where they matter most — the patients.”
The dispute stemmed from NDAs that Dr. Sajan’s practice required patients to sign starting in 2017, according to Mr. Ferguson’s complaint. The terms instructed patients to contact the business directly if they had concerns rather than post a negative review.
If patients posted negative reviews, the clinic, in some cases, threatened litigation, according to the lawsuit. In other cases, patients were allegedly offered money and free services in exchange for taking the reviews down. Patients who accepted cash or services were required to sign a second agreement forbidding them from posting future negative reviews and imposing a $250,000 penalty for failure to comply, according to court documents.
In addition, Mr. Ferguson accused Dr. Sajan of creating fake positive accounts of patient experiences and buying fake followers on social media. State investigators found Dr. Sajan directed Allure Esthetic’s employees to create fake Gmail accounts to post the false reviews, many of which are still online today, according to the state’s complaint.
Mr. Ferguson also claimed Dr. Sajan and his practice manipulated social media to appear more popular by purchasing followers through an online vendor. The practice also allegedly used a social media bot tool to buy thousands of fake likes on Instagram, YouTube, and other social media.
After filing the lawsuit, Mr. Ferguson’s office uncovered further evidence of Dr. Sajan’s efforts to influence his professional reputation through fabrication, according to the July 2 release. Allure Esthetic “rigged” “best doctor” competitions hosted by local media outlets by paying staff and contractors to vote for Dr. Sajan as “best plastic surgeon” in the region, according to the release. The staff cast as many votes as websites allowed, despite not being patients of Allure Esthetic.
The practice also allegedly edited before-and-after photos of patients to make their results appear better and kept tens of thousands of dollars in rebates intended for its patients.
In addition to paying $5 million, the consent decree requires Dr. Sajan and his practice also:
- Stop posting or influencing consumer reviews; perform a full audit of all public reviews on Google, Yelp, and other third-party review platforms; and request removal of every review Allure Esthetic was involved in creating, posting, or shaping in any manner.
- Remove all misleading “before-and-after” photographs of plastic surgery procedures from its website and social media and stop altering photographs of future procedures.
- Cease use of and attempts to enforce all illegal NDAs and notify patients who previously signed them that they are released from the terms of those NDAs.
- Pay a third-party forensic accounting firm to perform a full, independent audit of Allure Esthetic’s consumer rebate program to identify consumers who are owed rebates that were unlawfully claimed by Allure Esthetic.
Additionally, the attorney general’s office will continue to monitor Allure Esthetic, and upon request, the practice must provide information that demonstrates its compliance with the consent decree for the next 10 years.
The practice must also develop internal policies and implement a training program to educate staff about nondeceptive advertising and compliance with consumer protection laws.
Dr. Sajan and his practice agreed to the terms of the consent decree, and the settlement is not considered an admission of liability.
A version of this article first appeared on Medscape.com.
A Seattle plastic surgeon who illegally restricted patients from posting negative reviews about his practice and directed his staff to post fake positive reviews will pay $5 million for violating Washington state’s consumer protection law.
According to a July 1 consent decree, Javad Sajan, MD, and his practice Allure Esthetic must pay $1.5 million in restitution to 21,000 patients and $3.5 million to the state for manipulation of patient ratings.
In an April decision, US District Judge Ricardo S. Martinez sided with the state, ruling that Allure Esthetic’s actions violated the federal Consumer Review Fairness Act (CRFA).
“Writing a truthful review about a business should not subject you to threats or intimidation,” Mr. Ferguson said in a July 2 statement. “Consumers rely on reviews when determining who to trust, especially services that affect their health and safety. This resolution holds Allure accountable for brazenly violating that trust — and the law — and ensures the clinic stops its harmful conduct.”
In court documents, Dr. Sajan’s attorneys had argued that the agreements did not violate CRFA because patients had the opportunity to modify the language or decline signing them.
The surgeon’s practice is “pleased to have resolved its case with the Attorney General’s Office,” according to a statement provided by Dr. Sajan’s attorney. “The cooperative settlement, while not admitting fault and resolving claims asserted by both sides, allows Allure Esthetic to continue to focus on its core mission of providing compassionate care to patients and serving the community. The decision to settle was not an easy one, but it was necessary to allocate time and resources where they matter most — the patients.”
The dispute stemmed from NDAs that Dr. Sajan’s practice required patients to sign starting in 2017, according to Mr. Ferguson’s complaint. The terms instructed patients to contact the business directly if they had concerns rather than post a negative review.
If patients posted negative reviews, the clinic, in some cases, threatened litigation, according to the lawsuit. In other cases, patients were allegedly offered money and free services in exchange for taking the reviews down. Patients who accepted cash or services were required to sign a second agreement forbidding them from posting future negative reviews and imposing a $250,000 penalty for failure to comply, according to court documents.
In addition, Mr. Ferguson accused Dr. Sajan of creating fake positive accounts of patient experiences and buying fake followers on social media. State investigators found Dr. Sajan directed Allure Esthetic’s employees to create fake Gmail accounts to post the false reviews, many of which are still online today, according to the state’s complaint.
Mr. Ferguson also claimed Dr. Sajan and his practice manipulated social media to appear more popular by purchasing followers through an online vendor. The practice also allegedly used a social media bot tool to buy thousands of fake likes on Instagram, YouTube, and other social media.
After filing the lawsuit, Mr. Ferguson’s office uncovered further evidence of Dr. Sajan’s efforts to influence his professional reputation through fabrication, according to the July 2 release. Allure Esthetic “rigged” “best doctor” competitions hosted by local media outlets by paying staff and contractors to vote for Dr. Sajan as “best plastic surgeon” in the region, according to the release. The staff cast as many votes as websites allowed, despite not being patients of Allure Esthetic.
The practice also allegedly edited before-and-after photos of patients to make their results appear better and kept tens of thousands of dollars in rebates intended for its patients.
In addition to paying $5 million, the consent decree requires Dr. Sajan and his practice also:
- Stop posting or influencing consumer reviews; perform a full audit of all public reviews on Google, Yelp, and other third-party review platforms; and request removal of every review Allure Esthetic was involved in creating, posting, or shaping in any manner.
- Remove all misleading “before-and-after” photographs of plastic surgery procedures from its website and social media and stop altering photographs of future procedures.
- Cease use of and attempts to enforce all illegal NDAs and notify patients who previously signed them that they are released from the terms of those NDAs.
- Pay a third-party forensic accounting firm to perform a full, independent audit of Allure Esthetic’s consumer rebate program to identify consumers who are owed rebates that were unlawfully claimed by Allure Esthetic.
Additionally, the attorney general’s office will continue to monitor Allure Esthetic, and upon request, the practice must provide information that demonstrates its compliance with the consent decree for the next 10 years.
The practice must also develop internal policies and implement a training program to educate staff about nondeceptive advertising and compliance with consumer protection laws.
Dr. Sajan and his practice agreed to the terms of the consent decree, and the settlement is not considered an admission of liability.
A version of this article first appeared on Medscape.com.
Whether GLP-1 RAs Significantly Delay Gastric Emptying Called into Question
TOPLINE:
Patients taking a glucagon-like peptide 1 receptor agonist (GLP-1 RA) experience only a modest delay in gastric emptying of solid foods and no significant delay for liquids, compared with those receiving placebo, indicating that patients may not need to discontinue these medications before surgery.
METHODOLOGY:
- GLP-1 RAs, while effective in managing diabetes and obesity, are linked to delayed gastric emptying, which may pose risks during procedures requiring anesthesia or sedation due to potential aspiration of gastric contents.
- Researchers conducted a meta-analysis to quantify the duration of delay in gastric emptying caused by GLP-1 RAs in patients with diabetes and/or excessive body weight, which could guide periprocedural management decisions in the future.
- The primary outcome was halftime, the time required for 50% of solid gastric contents to empty, measured using scintigraphy. This analysis included data from five studies involving 247 patients who received either a GLP-1 RA or placebo.
- The secondary outcome was gastric emptying of liquids measured using the acetaminophen absorption test. Ten studies including 411 patients who received either a GLP-1 RA or placebo were included in this analysis.
TAKEAWAY:
- The mean gastric emptying halftime for solid foods was 138.4 minutes with a GLP-1 RA and 95.0 minutes with placebo, resulting in a pooled mean difference of 36.0 minutes (P < .01).
- Furthermore, the amount of gastric emptying noted at 4 or 5 hours on the acetaminophen absorption test was comparable between these groups.
- The gastric emptying time for both solids and liquids did not differ between GLP-1 RA formulations or between short-acting or long-acting GLP-1 RAs.
IN PRACTICE:
“Based on current evidence, a conservative approach with a liquid diet on the day before procedures while continuing GLP-1 RA therapy would represent the most sensible approach until more conclusive data on a solid diet are available,” the authors wrote.
SOURCE:
The study, led by Brent Hiramoto, MD, MPH, of the Center for Gastrointestinal Motility at Brigham and Women’s Hospital and Harvard Medical School, Boston, was published online in The American Journal of Gastroenterology.
LIMITATIONS:
The small number of studies utilizing some diagnostic modalities, such as breath testing, precluded a formal meta-analysis of these subgroups. The results could not be stratified by indication for GLP-1 RA (diabetes or obesity) because of insufficient studies in each category.
DISCLOSURES:
The lead author was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One author declared serving on the advisory boards of three pharmaceutical companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients taking a glucagon-like peptide 1 receptor agonist (GLP-1 RA) experience only a modest delay in gastric emptying of solid foods and no significant delay for liquids, compared with those receiving placebo, indicating that patients may not need to discontinue these medications before surgery.
METHODOLOGY:
- GLP-1 RAs, while effective in managing diabetes and obesity, are linked to delayed gastric emptying, which may pose risks during procedures requiring anesthesia or sedation due to potential aspiration of gastric contents.
- Researchers conducted a meta-analysis to quantify the duration of delay in gastric emptying caused by GLP-1 RAs in patients with diabetes and/or excessive body weight, which could guide periprocedural management decisions in the future.
- The primary outcome was halftime, the time required for 50% of solid gastric contents to empty, measured using scintigraphy. This analysis included data from five studies involving 247 patients who received either a GLP-1 RA or placebo.
- The secondary outcome was gastric emptying of liquids measured using the acetaminophen absorption test. Ten studies including 411 patients who received either a GLP-1 RA or placebo were included in this analysis.
TAKEAWAY:
- The mean gastric emptying halftime for solid foods was 138.4 minutes with a GLP-1 RA and 95.0 minutes with placebo, resulting in a pooled mean difference of 36.0 minutes (P < .01).
- Furthermore, the amount of gastric emptying noted at 4 or 5 hours on the acetaminophen absorption test was comparable between these groups.
- The gastric emptying time for both solids and liquids did not differ between GLP-1 RA formulations or between short-acting or long-acting GLP-1 RAs.
IN PRACTICE:
“Based on current evidence, a conservative approach with a liquid diet on the day before procedures while continuing GLP-1 RA therapy would represent the most sensible approach until more conclusive data on a solid diet are available,” the authors wrote.
SOURCE:
The study, led by Brent Hiramoto, MD, MPH, of the Center for Gastrointestinal Motility at Brigham and Women’s Hospital and Harvard Medical School, Boston, was published online in The American Journal of Gastroenterology.
LIMITATIONS:
The small number of studies utilizing some diagnostic modalities, such as breath testing, precluded a formal meta-analysis of these subgroups. The results could not be stratified by indication for GLP-1 RA (diabetes or obesity) because of insufficient studies in each category.
DISCLOSURES:
The lead author was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One author declared serving on the advisory boards of three pharmaceutical companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients taking a glucagon-like peptide 1 receptor agonist (GLP-1 RA) experience only a modest delay in gastric emptying of solid foods and no significant delay for liquids, compared with those receiving placebo, indicating that patients may not need to discontinue these medications before surgery.
METHODOLOGY:
- GLP-1 RAs, while effective in managing diabetes and obesity, are linked to delayed gastric emptying, which may pose risks during procedures requiring anesthesia or sedation due to potential aspiration of gastric contents.
- Researchers conducted a meta-analysis to quantify the duration of delay in gastric emptying caused by GLP-1 RAs in patients with diabetes and/or excessive body weight, which could guide periprocedural management decisions in the future.
- The primary outcome was halftime, the time required for 50% of solid gastric contents to empty, measured using scintigraphy. This analysis included data from five studies involving 247 patients who received either a GLP-1 RA or placebo.
- The secondary outcome was gastric emptying of liquids measured using the acetaminophen absorption test. Ten studies including 411 patients who received either a GLP-1 RA or placebo were included in this analysis.
TAKEAWAY:
- The mean gastric emptying halftime for solid foods was 138.4 minutes with a GLP-1 RA and 95.0 minutes with placebo, resulting in a pooled mean difference of 36.0 minutes (P < .01).
- Furthermore, the amount of gastric emptying noted at 4 or 5 hours on the acetaminophen absorption test was comparable between these groups.
- The gastric emptying time for both solids and liquids did not differ between GLP-1 RA formulations or between short-acting or long-acting GLP-1 RAs.
IN PRACTICE:
“Based on current evidence, a conservative approach with a liquid diet on the day before procedures while continuing GLP-1 RA therapy would represent the most sensible approach until more conclusive data on a solid diet are available,” the authors wrote.
SOURCE:
The study, led by Brent Hiramoto, MD, MPH, of the Center for Gastrointestinal Motility at Brigham and Women’s Hospital and Harvard Medical School, Boston, was published online in The American Journal of Gastroenterology.
LIMITATIONS:
The small number of studies utilizing some diagnostic modalities, such as breath testing, precluded a formal meta-analysis of these subgroups. The results could not be stratified by indication for GLP-1 RA (diabetes or obesity) because of insufficient studies in each category.
DISCLOSURES:
The lead author was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One author declared serving on the advisory boards of three pharmaceutical companies.
A version of this article first appeared on Medscape.com.
Clinical Controversy: Standard Dose or Baby TAM for Breast Cancer Prevention?
Should 5 mg of tamoxifen — known as “baby TAM” — or the usual 20 mg dose be standard of care for breast cancer prevention in high-risk women?
Research to date clearly shows that tamoxifen can reduce the risk for breast cancer in high-risk individuals by 30%-50%. Recent evidence also indicates that this chemoprevention approach can reduce the risk of dying from breast cancer by as much as 57%.
In 2019, the US Preventive Services Task Force issued updated recommendations that clinicians offer risk-reducing medications, such as tamoxifen, raloxifene, or aromatase inhibitors, to women at an increased risk for breast cancer and a low risk for adverse medication effects.
However, this prophylactic strategy remains underused.
A major roadblock: The drugs’ side effects, which include venous thromboembolic events and endometrial cancer as well as symptoms of menopause, such as hot flashes and sexual issues, have made uptake and adherence a challenge.
Offering women a lower dose of tamoxifen could allay fears about toxicities and improve uptake as well as reduce side effects and boost long-term adherence among those receiving baby TAM.
However,
The Debate
Years ago, Andrea De Censi, MD, a breast cancer researcher at the Galliera Hospital in Genova, Italy, and his colleagues reasoned that, because tamoxifen is a competitive estrogen receptor inhibitor, it may indeed have a minimal effective dose below 20 mg/d.
The fruits of that line of thought were presented to the world in the TAM-01 trial, first published in 2019, which pitted tamoxifen 5 mg/d for 3 years against placebo in 500 women with high-risk lesions, including lobular and ductal carcinoma in situ.
Dr. De Censi and colleagues found that baby TAM reduced the risk for invasive breast cancer by 52% and the risk for contralateral breast cancer by 75%.
Treatment adherence was slightly higher in the baby TAM group at 65% vs 61% in the placebo group.
A recent 10-year follow-up showed ongoing benefits associated with baby TAM vs placebo — a 42% reduction in breast cancer and a 64% drop in contralateral lesions.
The baby TAM group vs placebo experienced a slight increase in hot flashes but no significant increase in other common side effects.
Regarding serious adverse events, the baby TAM arm had one case of stage 1 endometrial cancer (0.4% of patients) and 20 cases of endometrial polyps (5%) vs 13 cases of endometrial polyps in the placebo arm. But there were no significant differences in thrombosis, cataracts, bone fractures, and other serious events.
Dr. De Censi said he’s surprised the baby TAM vs tamoxifen topic is still being debated. “Baby TAM, in my opinion, is a new standard of care for endocrine prevention of breast cancer in high-risk [women],” and baby TAM over 3 years is enough, said Dr. De Censi during a debate on the topic at the 2024 European Society for Medical Oncology Breast Cancer Congress in Berlin.
Gareth Evans, MD, a cancer genetics and prevention specialist at the University of Manchester, Manchester, England, however, isn’t convinced.
During the debate, Dr. Evans explained that his main concern was that the baby TAM trial was limited to women with high-risk lesions, not other common reasons for tamoxifen prophylaxis, such as a positive family history or BRCA mutations.
“In Manchester, we have put over a thousand women on tamoxifen who have a family history or other risk factors, not high-risk lesions,” and there simply isn’t definitive evidence for baby TAM in these women, Dr. Evans said.
The vast weight of evidence for tamoxifen prophylaxis, he added, is in trials involving tens of thousands of women, followed in some cases for 20 years, who received the 20 mg dose for 5 years.
As a result, women in Manchester are started on 20 mg and dropped down to 5 mg only for side effects. That way, Evans explained, we are not taking away the benefit among women who can tolerate 20 mg.
Meanwhile, there’s no evidence that baby TAM improves medication adherence, he noted. Trials have reported similar adherence rates to baby TAM and standard dose tamoxifen as well as no definitive evidence that the risk for cancer and thrombosis is less with baby TAM, he said.
In fact, Dr. Evans noted, “many women take tamoxifen 20 mg for 5 years with no side effects.”
Overall, “I don’t think we’ve got the evidence yet to drop” dosages, particularly in women without high-risk lesions, Dr. Evans said. A real concern, he added, is poor metabolizers for whom 5 mg won’t be enough to have a preventive effect.
Dr. De Censi noted, however, that there will likely never be a definitive answer to the question of baby TAM vs standard dosing because industry has no financial incentive to do a head-to-head trial; tamoxifen went off patent over 30 years ago.
Still, a poll of the audience favored Evans’ approach — 80% said they would start high-risk women on 20 mg for breast cancer prophylaxis and reduce for side effects as needed.
Dr. De Censi didn’t have any disclosures. Dr. Evans is a consultant/advisor for AstraZeneca, SpringWorks, Recursion, Everything Genetic, and Syantra.
A version of this article first appeared on Medscape.com.
Should 5 mg of tamoxifen — known as “baby TAM” — or the usual 20 mg dose be standard of care for breast cancer prevention in high-risk women?
Research to date clearly shows that tamoxifen can reduce the risk for breast cancer in high-risk individuals by 30%-50%. Recent evidence also indicates that this chemoprevention approach can reduce the risk of dying from breast cancer by as much as 57%.
In 2019, the US Preventive Services Task Force issued updated recommendations that clinicians offer risk-reducing medications, such as tamoxifen, raloxifene, or aromatase inhibitors, to women at an increased risk for breast cancer and a low risk for adverse medication effects.
However, this prophylactic strategy remains underused.
A major roadblock: The drugs’ side effects, which include venous thromboembolic events and endometrial cancer as well as symptoms of menopause, such as hot flashes and sexual issues, have made uptake and adherence a challenge.
Offering women a lower dose of tamoxifen could allay fears about toxicities and improve uptake as well as reduce side effects and boost long-term adherence among those receiving baby TAM.
However,
The Debate
Years ago, Andrea De Censi, MD, a breast cancer researcher at the Galliera Hospital in Genova, Italy, and his colleagues reasoned that, because tamoxifen is a competitive estrogen receptor inhibitor, it may indeed have a minimal effective dose below 20 mg/d.
The fruits of that line of thought were presented to the world in the TAM-01 trial, first published in 2019, which pitted tamoxifen 5 mg/d for 3 years against placebo in 500 women with high-risk lesions, including lobular and ductal carcinoma in situ.
Dr. De Censi and colleagues found that baby TAM reduced the risk for invasive breast cancer by 52% and the risk for contralateral breast cancer by 75%.
Treatment adherence was slightly higher in the baby TAM group at 65% vs 61% in the placebo group.
A recent 10-year follow-up showed ongoing benefits associated with baby TAM vs placebo — a 42% reduction in breast cancer and a 64% drop in contralateral lesions.
The baby TAM group vs placebo experienced a slight increase in hot flashes but no significant increase in other common side effects.
Regarding serious adverse events, the baby TAM arm had one case of stage 1 endometrial cancer (0.4% of patients) and 20 cases of endometrial polyps (5%) vs 13 cases of endometrial polyps in the placebo arm. But there were no significant differences in thrombosis, cataracts, bone fractures, and other serious events.
Dr. De Censi said he’s surprised the baby TAM vs tamoxifen topic is still being debated. “Baby TAM, in my opinion, is a new standard of care for endocrine prevention of breast cancer in high-risk [women],” and baby TAM over 3 years is enough, said Dr. De Censi during a debate on the topic at the 2024 European Society for Medical Oncology Breast Cancer Congress in Berlin.
Gareth Evans, MD, a cancer genetics and prevention specialist at the University of Manchester, Manchester, England, however, isn’t convinced.
During the debate, Dr. Evans explained that his main concern was that the baby TAM trial was limited to women with high-risk lesions, not other common reasons for tamoxifen prophylaxis, such as a positive family history or BRCA mutations.
“In Manchester, we have put over a thousand women on tamoxifen who have a family history or other risk factors, not high-risk lesions,” and there simply isn’t definitive evidence for baby TAM in these women, Dr. Evans said.
The vast weight of evidence for tamoxifen prophylaxis, he added, is in trials involving tens of thousands of women, followed in some cases for 20 years, who received the 20 mg dose for 5 years.
As a result, women in Manchester are started on 20 mg and dropped down to 5 mg only for side effects. That way, Evans explained, we are not taking away the benefit among women who can tolerate 20 mg.
Meanwhile, there’s no evidence that baby TAM improves medication adherence, he noted. Trials have reported similar adherence rates to baby TAM and standard dose tamoxifen as well as no definitive evidence that the risk for cancer and thrombosis is less with baby TAM, he said.
In fact, Dr. Evans noted, “many women take tamoxifen 20 mg for 5 years with no side effects.”
Overall, “I don’t think we’ve got the evidence yet to drop” dosages, particularly in women without high-risk lesions, Dr. Evans said. A real concern, he added, is poor metabolizers for whom 5 mg won’t be enough to have a preventive effect.
Dr. De Censi noted, however, that there will likely never be a definitive answer to the question of baby TAM vs standard dosing because industry has no financial incentive to do a head-to-head trial; tamoxifen went off patent over 30 years ago.
Still, a poll of the audience favored Evans’ approach — 80% said they would start high-risk women on 20 mg for breast cancer prophylaxis and reduce for side effects as needed.
Dr. De Censi didn’t have any disclosures. Dr. Evans is a consultant/advisor for AstraZeneca, SpringWorks, Recursion, Everything Genetic, and Syantra.
A version of this article first appeared on Medscape.com.
Should 5 mg of tamoxifen — known as “baby TAM” — or the usual 20 mg dose be standard of care for breast cancer prevention in high-risk women?
Research to date clearly shows that tamoxifen can reduce the risk for breast cancer in high-risk individuals by 30%-50%. Recent evidence also indicates that this chemoprevention approach can reduce the risk of dying from breast cancer by as much as 57%.
In 2019, the US Preventive Services Task Force issued updated recommendations that clinicians offer risk-reducing medications, such as tamoxifen, raloxifene, or aromatase inhibitors, to women at an increased risk for breast cancer and a low risk for adverse medication effects.
However, this prophylactic strategy remains underused.
A major roadblock: The drugs’ side effects, which include venous thromboembolic events and endometrial cancer as well as symptoms of menopause, such as hot flashes and sexual issues, have made uptake and adherence a challenge.
Offering women a lower dose of tamoxifen could allay fears about toxicities and improve uptake as well as reduce side effects and boost long-term adherence among those receiving baby TAM.
However,
The Debate
Years ago, Andrea De Censi, MD, a breast cancer researcher at the Galliera Hospital in Genova, Italy, and his colleagues reasoned that, because tamoxifen is a competitive estrogen receptor inhibitor, it may indeed have a minimal effective dose below 20 mg/d.
The fruits of that line of thought were presented to the world in the TAM-01 trial, first published in 2019, which pitted tamoxifen 5 mg/d for 3 years against placebo in 500 women with high-risk lesions, including lobular and ductal carcinoma in situ.
Dr. De Censi and colleagues found that baby TAM reduced the risk for invasive breast cancer by 52% and the risk for contralateral breast cancer by 75%.
Treatment adherence was slightly higher in the baby TAM group at 65% vs 61% in the placebo group.
A recent 10-year follow-up showed ongoing benefits associated with baby TAM vs placebo — a 42% reduction in breast cancer and a 64% drop in contralateral lesions.
The baby TAM group vs placebo experienced a slight increase in hot flashes but no significant increase in other common side effects.
Regarding serious adverse events, the baby TAM arm had one case of stage 1 endometrial cancer (0.4% of patients) and 20 cases of endometrial polyps (5%) vs 13 cases of endometrial polyps in the placebo arm. But there were no significant differences in thrombosis, cataracts, bone fractures, and other serious events.
Dr. De Censi said he’s surprised the baby TAM vs tamoxifen topic is still being debated. “Baby TAM, in my opinion, is a new standard of care for endocrine prevention of breast cancer in high-risk [women],” and baby TAM over 3 years is enough, said Dr. De Censi during a debate on the topic at the 2024 European Society for Medical Oncology Breast Cancer Congress in Berlin.
Gareth Evans, MD, a cancer genetics and prevention specialist at the University of Manchester, Manchester, England, however, isn’t convinced.
During the debate, Dr. Evans explained that his main concern was that the baby TAM trial was limited to women with high-risk lesions, not other common reasons for tamoxifen prophylaxis, such as a positive family history or BRCA mutations.
“In Manchester, we have put over a thousand women on tamoxifen who have a family history or other risk factors, not high-risk lesions,” and there simply isn’t definitive evidence for baby TAM in these women, Dr. Evans said.
The vast weight of evidence for tamoxifen prophylaxis, he added, is in trials involving tens of thousands of women, followed in some cases for 20 years, who received the 20 mg dose for 5 years.
As a result, women in Manchester are started on 20 mg and dropped down to 5 mg only for side effects. That way, Evans explained, we are not taking away the benefit among women who can tolerate 20 mg.
Meanwhile, there’s no evidence that baby TAM improves medication adherence, he noted. Trials have reported similar adherence rates to baby TAM and standard dose tamoxifen as well as no definitive evidence that the risk for cancer and thrombosis is less with baby TAM, he said.
In fact, Dr. Evans noted, “many women take tamoxifen 20 mg for 5 years with no side effects.”
Overall, “I don’t think we’ve got the evidence yet to drop” dosages, particularly in women without high-risk lesions, Dr. Evans said. A real concern, he added, is poor metabolizers for whom 5 mg won’t be enough to have a preventive effect.
Dr. De Censi noted, however, that there will likely never be a definitive answer to the question of baby TAM vs standard dosing because industry has no financial incentive to do a head-to-head trial; tamoxifen went off patent over 30 years ago.
Still, a poll of the audience favored Evans’ approach — 80% said they would start high-risk women on 20 mg for breast cancer prophylaxis and reduce for side effects as needed.
Dr. De Censi didn’t have any disclosures. Dr. Evans is a consultant/advisor for AstraZeneca, SpringWorks, Recursion, Everything Genetic, and Syantra.
A version of this article first appeared on Medscape.com.
Pediatric Studies Produce Mixed Messages on Relationship Between COVID and Asthma
In one of several recently published studies on the relationship between COVID-19 infection and asthma, according to data drawn from the National Survey of Children’s Health (NSCH).
The inverse correlation between symptoms and vaccination was strong and statistically significant, according to investigators led by Matthew M. Davis, MD, Physician in Chief and Chief Scientific Officer, Nemours Children’s Health, Wilmington, Delaware.
“With each increase of 10 percentage points in COVID-19 vaccination coverage, the parent-reported child asthma symptoms prevalence decreased by 0.36 percentage points (P < .05),” Dr. Davis and his coinvestigators reported in a research letter published in JAMA Network Open.
Studies Explore Relationship of COVID and Asthma
The reduced risk of asthma symptoms with COVID-19 vaccination in children at the population level is just one of several recently published studies exploring the interaction between COVID-19 infection and asthma, but two studies that posed the same question did not reach the same conclusion.
In one, COVID-19 infection in children was not found to be a trigger for new-onset asthma, but the second found that it was. In a third study, the preponderance of evidence from a meta-analysis found that patients with asthma – whether children or adults – did not necessarily experience a more severe course of COVID-19 infection than in those without asthma.
The NSCH database study calculated state-level change in scores for patient-reported childhood asthma symptoms in the years in the years 2018-2019, which preceded the pandemic and the years 2020-2021, when the pandemic began. The hypothesis was that the proportion of the population 5 years of age or older who completed the COVID-19 primary vaccination would be inversely related to asthma symptom prevalence.
Relative to the 2018-2019 years, the mean rate of parent-reported asthma symptoms was 0.85% lower (6.93% vs 7.77%; P < .001) in 2020-2021, when the mean primary series COVID-19 vaccination rate was 72.3%.
The study was not able to evaluate the impact of COVID-19 vaccination specifically in children with asthma, because history of asthma is not captured in the NSCH data, but Dr. Davis contended that the reduction in symptomatic asthma among children with increased vaccination offers validation for the state-level findings.
“Moreover, the absence of an association of COVID-19 vaccination administered predominantly in 2021 with population-level COVID-19 mortality in 2020 serves as a negative control,” he and his colleagues wrote in their research letter.
Protection from Respiratory Viruses Seen for Asthma Patients
In an interview, Dr. Davis reported that these data are consistent with previous evidence that immunization against influenza also reduces risk of asthma symptoms. In a meta-analysis published in 2017, it was estimated that live vaccines reduced risk of influenza by 81% and prevented 59%-72% of asthma attacks leading to hospitalizations or emergency room visits.
“The similarity of our findings regarding COVID-19 vaccination to prior data regarding influenza vaccination underscores the importance of preventing viral illnesses in individuals with a history of asthma,” Dr. Davis said. It is not yet clear if this is true of respiratory syncytial virus (RSV). Because of the short time that the RSV vaccine has been available, it is too soon to conduct an analysis.
One message from this study is that “clinicians should continue to encourage COVID-19 vaccination for children because of its general benefits in preventing coronavirus-related illness and the apparent specific benefits for children with a history of asthma,” he said.
While vaccination appears to reduce asthmatic symptoms related to COVID-19 infection, one study suggests that COVID-19 does not trigger new-onset asthma. In a retrospective study published in Pediatrics, no association between COVID-19 infection and new-onset asthma could be made in an analysis of 27,423 children (ages, 1-16 years) from the Children’s Hospital of Philadelphia (CHOP) Care Network.
Across all the pediatric age groups evaluated, the consistent finding was “SARS-CoV-2 positivity does not confer an additional risk for asthma diagnosis at least within the first 18 months after a [polymerase chain reaction] test,” concluded the investigators, led by David A. Hill, MD, PhD, Division of Allergy and Immunology, CHOP, Philadelphia, Pennsylvania.
Risk of Asthma Doubled After COVID-19 Infection
However, the opposite conclusion was reached by investigators evaluating data from two cohorts of children ages 5-18 drawn from the TriNetX database, a global health research network with data on more than 250 million individuals. Cohort 1 included more than 250,000 children. These children had never received COVID-19 vaccination. The 50,000 patients in cohort 2 had all received COVID19 vaccination.
To compare the impact of COVID-19 infection on new-onset asthma, the patients who were infected with COVID-19 were compared with those who were not infected after propensity score matching over 18 months of follow-up.
In cohort 1, the rate of new onset asthma was more than twofold greater among those with COVID-19 infection (4.7% vs 2.0%). The hazard ratio (HR) of 2.25 had tight confidence intervals (95% CI, 2.158-2.367).
In cohort 2, the risk of new-onset asthma at 18 months among those who had a COVID-19 infection relative to those without was even greater (8.3% vs 3.1%). The relative risk approached a 3-fold increase (HR 2.745; 95% CI, 2.521-2.99).
The conclusion of these investigators, led by Chia-Chi Lung, PhD, Department of Public Health, Chung Shan Medical University, Taichung City, Taiwan, was that there is “a critical need for ongoing monitoring and customized healthcare strategies to mitigate the long-term respiratory impacts of COVID-19 in children.”
These health risks might not be as significant as once feared. In the recently published study from Environmental Health Insights, the goal of a meta-analysis was to determine if patients with asthma relative to those without asthma face a higher risk of serious disease from COVID-19 infection. The meta-analysis included studies of children and adults. The answer, according an in-depth analysis of 21 articles in a “scoping review,” was a qualified no.
Of the 21 articles, 4 concluded that asthma is a risk factor for serious COVID-19 infection, but 17 did not, according to Chukwudi S. Ubah, PhD, Department of Public Health, Brody School of Medicine, East Caroline University, Greenville, North Carolina.
None of These Questions are Fully Resolved
However, given the disparity in the results and the fact that many of the studies included in this analysis had small sample sizes, Dr. Ubah called for larger studies and studies with better controls. He noted, for example, that the studies did not consistently evaluate mitigating factors, such as used of inhaled or oral corticosteroids, which might affect risk of the severity of a COVID-19 infection.
Rather, “our findings pointed out that the type of medication prescribed for asthma may have implications for the severity of COVID-19 infection in these patients,” Dr. Ubah said in an interview.
Overall, the data do not support a major interaction between asthma and COVID-19, even if the data are not conclusive. Each of the senior authors of these studies called for larger and better investigations to further explore whether COVID-19 infection and preexisting asthma interact. So far, the data indicate that if COVID-19 infection poses a risk of precipitating new-onset asthma or inducing a more severe infection in children with asthma, it is low, but the degree of risk, if any, remains unresolved in subgroups defined by asthma treatment or asthma severity.
Dr. Davis, Dr. Hill, Dr. Lung, and Dr. Ubah reported no potential conflicts of interest. None of these studies received funding from commercial interests.
In one of several recently published studies on the relationship between COVID-19 infection and asthma, according to data drawn from the National Survey of Children’s Health (NSCH).
The inverse correlation between symptoms and vaccination was strong and statistically significant, according to investigators led by Matthew M. Davis, MD, Physician in Chief and Chief Scientific Officer, Nemours Children’s Health, Wilmington, Delaware.
“With each increase of 10 percentage points in COVID-19 vaccination coverage, the parent-reported child asthma symptoms prevalence decreased by 0.36 percentage points (P < .05),” Dr. Davis and his coinvestigators reported in a research letter published in JAMA Network Open.
Studies Explore Relationship of COVID and Asthma
The reduced risk of asthma symptoms with COVID-19 vaccination in children at the population level is just one of several recently published studies exploring the interaction between COVID-19 infection and asthma, but two studies that posed the same question did not reach the same conclusion.
In one, COVID-19 infection in children was not found to be a trigger for new-onset asthma, but the second found that it was. In a third study, the preponderance of evidence from a meta-analysis found that patients with asthma – whether children or adults – did not necessarily experience a more severe course of COVID-19 infection than in those without asthma.
The NSCH database study calculated state-level change in scores for patient-reported childhood asthma symptoms in the years in the years 2018-2019, which preceded the pandemic and the years 2020-2021, when the pandemic began. The hypothesis was that the proportion of the population 5 years of age or older who completed the COVID-19 primary vaccination would be inversely related to asthma symptom prevalence.
Relative to the 2018-2019 years, the mean rate of parent-reported asthma symptoms was 0.85% lower (6.93% vs 7.77%; P < .001) in 2020-2021, when the mean primary series COVID-19 vaccination rate was 72.3%.
The study was not able to evaluate the impact of COVID-19 vaccination specifically in children with asthma, because history of asthma is not captured in the NSCH data, but Dr. Davis contended that the reduction in symptomatic asthma among children with increased vaccination offers validation for the state-level findings.
“Moreover, the absence of an association of COVID-19 vaccination administered predominantly in 2021 with population-level COVID-19 mortality in 2020 serves as a negative control,” he and his colleagues wrote in their research letter.
Protection from Respiratory Viruses Seen for Asthma Patients
In an interview, Dr. Davis reported that these data are consistent with previous evidence that immunization against influenza also reduces risk of asthma symptoms. In a meta-analysis published in 2017, it was estimated that live vaccines reduced risk of influenza by 81% and prevented 59%-72% of asthma attacks leading to hospitalizations or emergency room visits.
“The similarity of our findings regarding COVID-19 vaccination to prior data regarding influenza vaccination underscores the importance of preventing viral illnesses in individuals with a history of asthma,” Dr. Davis said. It is not yet clear if this is true of respiratory syncytial virus (RSV). Because of the short time that the RSV vaccine has been available, it is too soon to conduct an analysis.
One message from this study is that “clinicians should continue to encourage COVID-19 vaccination for children because of its general benefits in preventing coronavirus-related illness and the apparent specific benefits for children with a history of asthma,” he said.
While vaccination appears to reduce asthmatic symptoms related to COVID-19 infection, one study suggests that COVID-19 does not trigger new-onset asthma. In a retrospective study published in Pediatrics, no association between COVID-19 infection and new-onset asthma could be made in an analysis of 27,423 children (ages, 1-16 years) from the Children’s Hospital of Philadelphia (CHOP) Care Network.
Across all the pediatric age groups evaluated, the consistent finding was “SARS-CoV-2 positivity does not confer an additional risk for asthma diagnosis at least within the first 18 months after a [polymerase chain reaction] test,” concluded the investigators, led by David A. Hill, MD, PhD, Division of Allergy and Immunology, CHOP, Philadelphia, Pennsylvania.
Risk of Asthma Doubled After COVID-19 Infection
However, the opposite conclusion was reached by investigators evaluating data from two cohorts of children ages 5-18 drawn from the TriNetX database, a global health research network with data on more than 250 million individuals. Cohort 1 included more than 250,000 children. These children had never received COVID-19 vaccination. The 50,000 patients in cohort 2 had all received COVID19 vaccination.
To compare the impact of COVID-19 infection on new-onset asthma, the patients who were infected with COVID-19 were compared with those who were not infected after propensity score matching over 18 months of follow-up.
In cohort 1, the rate of new onset asthma was more than twofold greater among those with COVID-19 infection (4.7% vs 2.0%). The hazard ratio (HR) of 2.25 had tight confidence intervals (95% CI, 2.158-2.367).
In cohort 2, the risk of new-onset asthma at 18 months among those who had a COVID-19 infection relative to those without was even greater (8.3% vs 3.1%). The relative risk approached a 3-fold increase (HR 2.745; 95% CI, 2.521-2.99).
The conclusion of these investigators, led by Chia-Chi Lung, PhD, Department of Public Health, Chung Shan Medical University, Taichung City, Taiwan, was that there is “a critical need for ongoing monitoring and customized healthcare strategies to mitigate the long-term respiratory impacts of COVID-19 in children.”
These health risks might not be as significant as once feared. In the recently published study from Environmental Health Insights, the goal of a meta-analysis was to determine if patients with asthma relative to those without asthma face a higher risk of serious disease from COVID-19 infection. The meta-analysis included studies of children and adults. The answer, according an in-depth analysis of 21 articles in a “scoping review,” was a qualified no.
Of the 21 articles, 4 concluded that asthma is a risk factor for serious COVID-19 infection, but 17 did not, according to Chukwudi S. Ubah, PhD, Department of Public Health, Brody School of Medicine, East Caroline University, Greenville, North Carolina.
None of These Questions are Fully Resolved
However, given the disparity in the results and the fact that many of the studies included in this analysis had small sample sizes, Dr. Ubah called for larger studies and studies with better controls. He noted, for example, that the studies did not consistently evaluate mitigating factors, such as used of inhaled or oral corticosteroids, which might affect risk of the severity of a COVID-19 infection.
Rather, “our findings pointed out that the type of medication prescribed for asthma may have implications for the severity of COVID-19 infection in these patients,” Dr. Ubah said in an interview.
Overall, the data do not support a major interaction between asthma and COVID-19, even if the data are not conclusive. Each of the senior authors of these studies called for larger and better investigations to further explore whether COVID-19 infection and preexisting asthma interact. So far, the data indicate that if COVID-19 infection poses a risk of precipitating new-onset asthma or inducing a more severe infection in children with asthma, it is low, but the degree of risk, if any, remains unresolved in subgroups defined by asthma treatment or asthma severity.
Dr. Davis, Dr. Hill, Dr. Lung, and Dr. Ubah reported no potential conflicts of interest. None of these studies received funding from commercial interests.
In one of several recently published studies on the relationship between COVID-19 infection and asthma, according to data drawn from the National Survey of Children’s Health (NSCH).
The inverse correlation between symptoms and vaccination was strong and statistically significant, according to investigators led by Matthew M. Davis, MD, Physician in Chief and Chief Scientific Officer, Nemours Children’s Health, Wilmington, Delaware.
“With each increase of 10 percentage points in COVID-19 vaccination coverage, the parent-reported child asthma symptoms prevalence decreased by 0.36 percentage points (P < .05),” Dr. Davis and his coinvestigators reported in a research letter published in JAMA Network Open.
Studies Explore Relationship of COVID and Asthma
The reduced risk of asthma symptoms with COVID-19 vaccination in children at the population level is just one of several recently published studies exploring the interaction between COVID-19 infection and asthma, but two studies that posed the same question did not reach the same conclusion.
In one, COVID-19 infection in children was not found to be a trigger for new-onset asthma, but the second found that it was. In a third study, the preponderance of evidence from a meta-analysis found that patients with asthma – whether children or adults – did not necessarily experience a more severe course of COVID-19 infection than in those without asthma.
The NSCH database study calculated state-level change in scores for patient-reported childhood asthma symptoms in the years in the years 2018-2019, which preceded the pandemic and the years 2020-2021, when the pandemic began. The hypothesis was that the proportion of the population 5 years of age or older who completed the COVID-19 primary vaccination would be inversely related to asthma symptom prevalence.
Relative to the 2018-2019 years, the mean rate of parent-reported asthma symptoms was 0.85% lower (6.93% vs 7.77%; P < .001) in 2020-2021, when the mean primary series COVID-19 vaccination rate was 72.3%.
The study was not able to evaluate the impact of COVID-19 vaccination specifically in children with asthma, because history of asthma is not captured in the NSCH data, but Dr. Davis contended that the reduction in symptomatic asthma among children with increased vaccination offers validation for the state-level findings.
“Moreover, the absence of an association of COVID-19 vaccination administered predominantly in 2021 with population-level COVID-19 mortality in 2020 serves as a negative control,” he and his colleagues wrote in their research letter.
Protection from Respiratory Viruses Seen for Asthma Patients
In an interview, Dr. Davis reported that these data are consistent with previous evidence that immunization against influenza also reduces risk of asthma symptoms. In a meta-analysis published in 2017, it was estimated that live vaccines reduced risk of influenza by 81% and prevented 59%-72% of asthma attacks leading to hospitalizations or emergency room visits.
“The similarity of our findings regarding COVID-19 vaccination to prior data regarding influenza vaccination underscores the importance of preventing viral illnesses in individuals with a history of asthma,” Dr. Davis said. It is not yet clear if this is true of respiratory syncytial virus (RSV). Because of the short time that the RSV vaccine has been available, it is too soon to conduct an analysis.
One message from this study is that “clinicians should continue to encourage COVID-19 vaccination for children because of its general benefits in preventing coronavirus-related illness and the apparent specific benefits for children with a history of asthma,” he said.
While vaccination appears to reduce asthmatic symptoms related to COVID-19 infection, one study suggests that COVID-19 does not trigger new-onset asthma. In a retrospective study published in Pediatrics, no association between COVID-19 infection and new-onset asthma could be made in an analysis of 27,423 children (ages, 1-16 years) from the Children’s Hospital of Philadelphia (CHOP) Care Network.
Across all the pediatric age groups evaluated, the consistent finding was “SARS-CoV-2 positivity does not confer an additional risk for asthma diagnosis at least within the first 18 months after a [polymerase chain reaction] test,” concluded the investigators, led by David A. Hill, MD, PhD, Division of Allergy and Immunology, CHOP, Philadelphia, Pennsylvania.
Risk of Asthma Doubled After COVID-19 Infection
However, the opposite conclusion was reached by investigators evaluating data from two cohorts of children ages 5-18 drawn from the TriNetX database, a global health research network with data on more than 250 million individuals. Cohort 1 included more than 250,000 children. These children had never received COVID-19 vaccination. The 50,000 patients in cohort 2 had all received COVID19 vaccination.
To compare the impact of COVID-19 infection on new-onset asthma, the patients who were infected with COVID-19 were compared with those who were not infected after propensity score matching over 18 months of follow-up.
In cohort 1, the rate of new onset asthma was more than twofold greater among those with COVID-19 infection (4.7% vs 2.0%). The hazard ratio (HR) of 2.25 had tight confidence intervals (95% CI, 2.158-2.367).
In cohort 2, the risk of new-onset asthma at 18 months among those who had a COVID-19 infection relative to those without was even greater (8.3% vs 3.1%). The relative risk approached a 3-fold increase (HR 2.745; 95% CI, 2.521-2.99).
The conclusion of these investigators, led by Chia-Chi Lung, PhD, Department of Public Health, Chung Shan Medical University, Taichung City, Taiwan, was that there is “a critical need for ongoing monitoring and customized healthcare strategies to mitigate the long-term respiratory impacts of COVID-19 in children.”
These health risks might not be as significant as once feared. In the recently published study from Environmental Health Insights, the goal of a meta-analysis was to determine if patients with asthma relative to those without asthma face a higher risk of serious disease from COVID-19 infection. The meta-analysis included studies of children and adults. The answer, according an in-depth analysis of 21 articles in a “scoping review,” was a qualified no.
Of the 21 articles, 4 concluded that asthma is a risk factor for serious COVID-19 infection, but 17 did not, according to Chukwudi S. Ubah, PhD, Department of Public Health, Brody School of Medicine, East Caroline University, Greenville, North Carolina.
None of These Questions are Fully Resolved
However, given the disparity in the results and the fact that many of the studies included in this analysis had small sample sizes, Dr. Ubah called for larger studies and studies with better controls. He noted, for example, that the studies did not consistently evaluate mitigating factors, such as used of inhaled or oral corticosteroids, which might affect risk of the severity of a COVID-19 infection.
Rather, “our findings pointed out that the type of medication prescribed for asthma may have implications for the severity of COVID-19 infection in these patients,” Dr. Ubah said in an interview.
Overall, the data do not support a major interaction between asthma and COVID-19, even if the data are not conclusive. Each of the senior authors of these studies called for larger and better investigations to further explore whether COVID-19 infection and preexisting asthma interact. So far, the data indicate that if COVID-19 infection poses a risk of precipitating new-onset asthma or inducing a more severe infection in children with asthma, it is low, but the degree of risk, if any, remains unresolved in subgroups defined by asthma treatment or asthma severity.
Dr. Davis, Dr. Hill, Dr. Lung, and Dr. Ubah reported no potential conflicts of interest. None of these studies received funding from commercial interests.
FROM JAMA NETWORK OPEN
Nail Alterations From Musical Instruments: Insights for Dermatologists Treating Musicians
A variety of skin problems can occur in musicians due to the repetitive movements of playing instruments.1,2 Musicians’ nails are continuously exposed to the mechanical forces and chemical substances characteristic of their instruments.3 Occupational nail alterations in musicians caused by repetitive physical trauma, allergic contact dermatitis, and/or infection may lead to disability and compromise their professional career.
We conducted a systematic review of the literature on the clinical features of musical instrument–related nail alterations to optimize the management and prevention of these conditions.
Methods
We conducted a systematic review of PubMed, Scopus, and Google Scholar databases for eligible publications on instrument-related nail alterations in musicians using the search terms musicians with nail, onychopathy, and Raynaud. No time or language criteria were applied. Reviews, editorials, and articles not related to the topic were excluded. Bibliographies/reference lists were checked to find any additional relevant publications. Relevant articles in English and French were screened by 2 independent reviewers (A.G. and N.L.), and the following data were extracted for qualitative synthesis: sex, age, musical instrument, clinical features, number of years practicing the instrument, laboratory investigations, and disease course.
Results
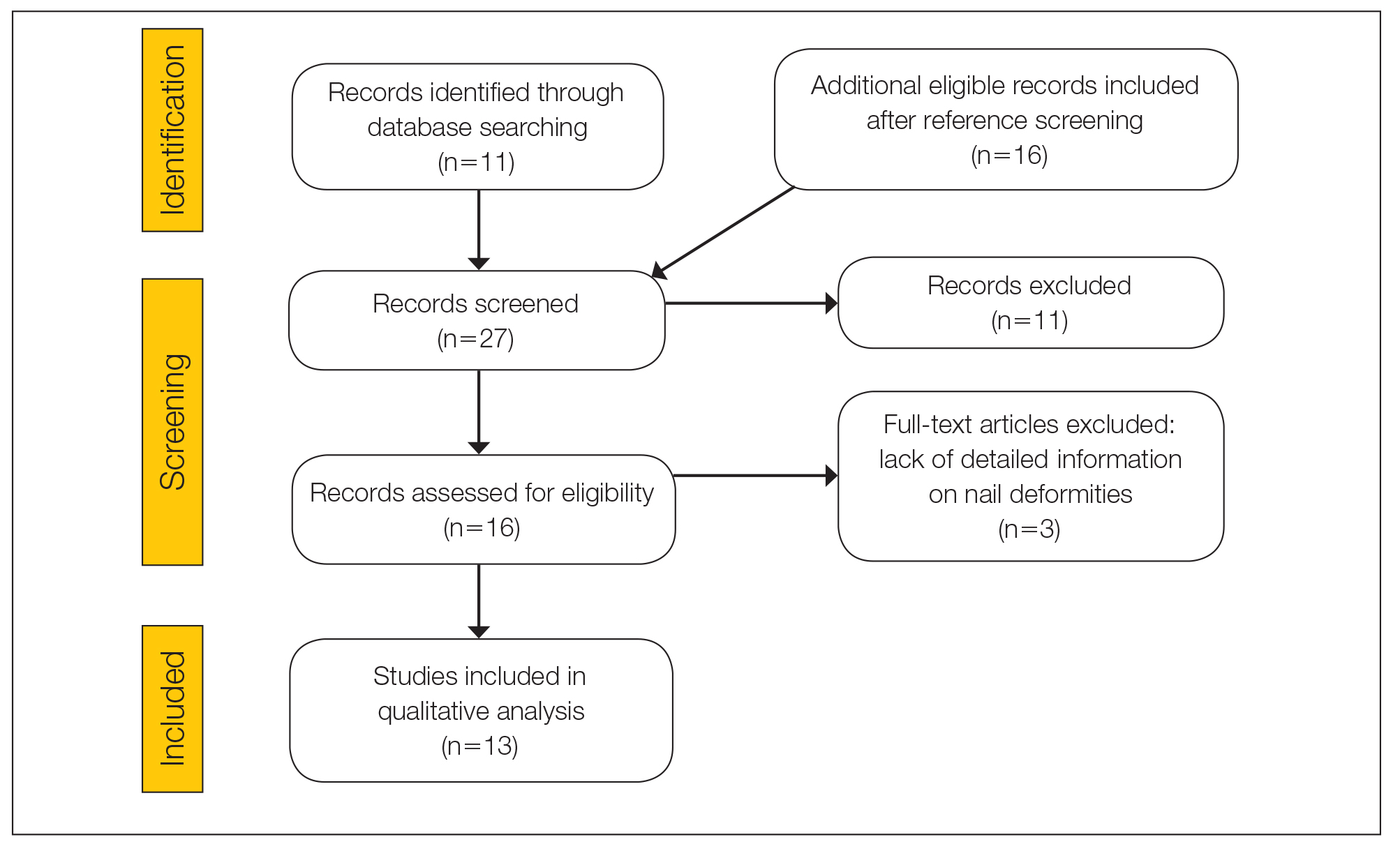
The literature search yielded 11 publications. Sixteen additional articles were identified by other methods (ie, references, related publications). Overall, 3 full-text articles described general nail alterations but did not describe the clinical data, and 11 publications were editorials, commentaries, reviews, or not relevant. Thirteen contributions fulfilled the inclusion criteria and were eligible for qualitative synthesis. The flow diagram illustrates the screening process (Figure 1).
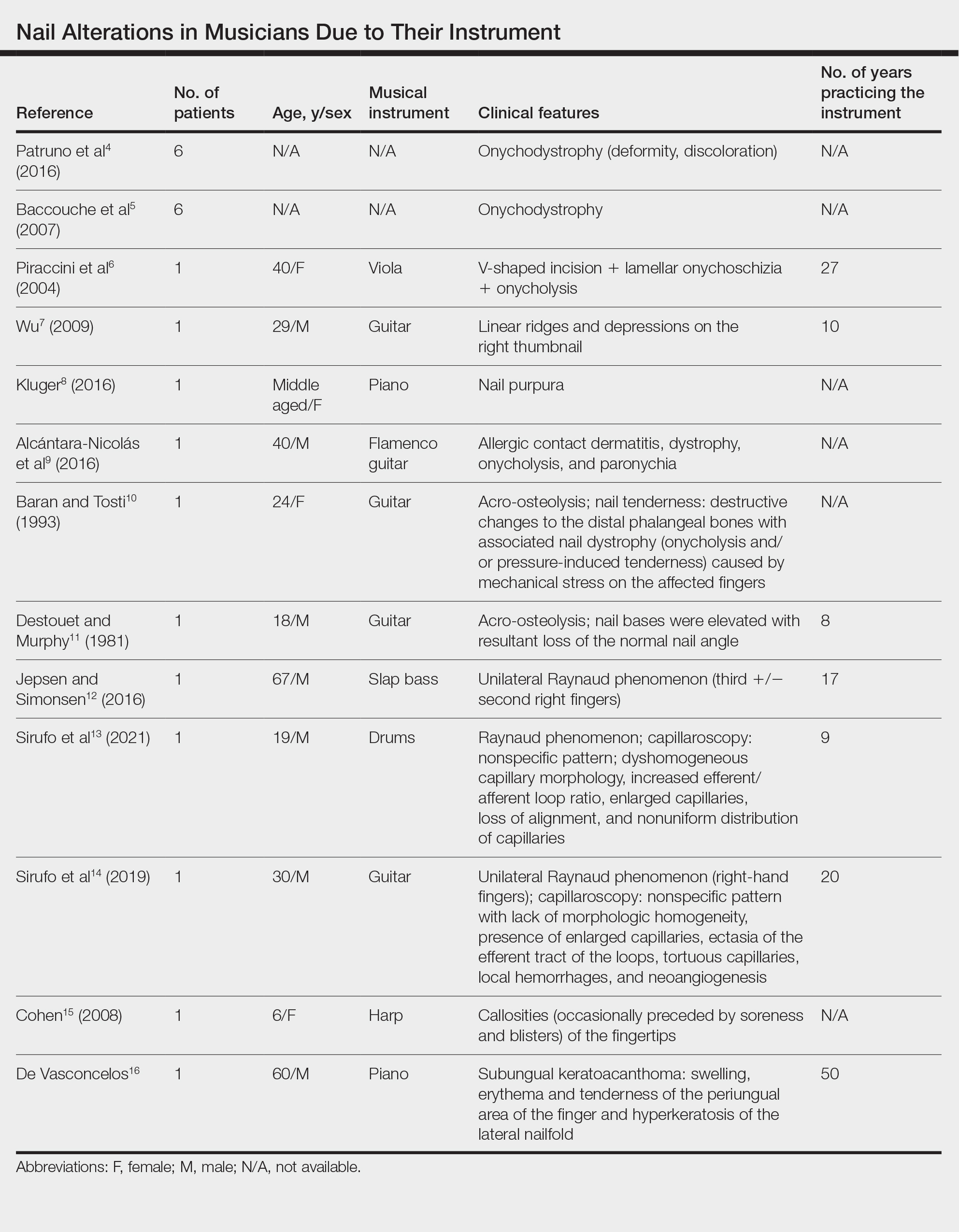
Twenty-three patients were included. The instruments identified were divided into 2 groups: string instruments (ie, guitar, violin, harp) and percussion instruments (ie, drums, piano, slap bass). Nail alterations were clinically expressed as: (1) modifications of the nail surface; (2) nail bed, soft-tissue, and bone abnormalities; and (3) periungual tissue and distal pulp disorders. All cases are summarized in the Table.4-16 Three articles described occupational Raynaud phenomenon.12-14
Comment
Modifications of the Nail Surface—Onychodystrophy, such as deformity or discoloration of the nail plate, was described in 6 patients among a cohort of 295 musicians and an additional 6 patients among 199 musicians with induced skin lesions. This condition was most common in string instrument players and pianists due to injury and irritation.
One patient, who had been a professional violist for 27 years, presented with lamellar onychoschizia, which corresponds to a horizontal splitting of the nail toward its distal portion (Figure 2). The 3 fingernails of the dominant hand were involved with a V-shaped incision of the distal margin of the nail due to the repetitive friction of the nails with the strings.6
Striations of the nail plate were reported in a guitarist who played for 10 years.7 Physical examination revealed linear transverse ridges alternating with depressions on the central aspect of the nail plate of the right thumbnail, as the patient was right-handed. This condition, attributed to sustained pressure on the string applied by the thumb, also has been called habit tic deformity.7
Nail Bed, Soft-Tissue, and Bone Lesions—Purpura (or hemorrhage) of the nail bed was associated with a percussion instrument (ie, piano) in 1 patient, affecting the second, third, and fourth fingernails of the right hand.8 Especially when performing ascending glissando passages, the pianist applies pressure that may damage the finger and cause fingernail purpura. This condition improved after the patient stopping practicing glissandi.8

Three patients—2 guitarists and 1 violist—had onycholysis, defined by a loss of the attachment between the nail bed and the nail plate (Figure 3). It may result from repetitive trauma when strings are plucked.6,9,10
Acro-osteolysis associated with pain was reported in 2 guitarists.10,11 This condition is defined as transverse lytic bands in the distal phalanges (Figure 4). Acro-osteolysis may be secondary to multiple causes, such as vinyl chloride exposure, connective tissue diseases, thermal injuries, neuropathic diseases, hyperparathyroidism, nutritional deficiencies, psoriasis, and biomechanical stress.10 In musicians playing instruments, the mechanical stress to the guitar-playing fingers is the causative factor.17
Periungual Tissue and Distal Pulp Disorders—Paronychia is an important occupational hazard of harpists, violists, and pianists.2 It represents an inflammatory condition involving the folds of tissue surrounding fingernails. Pizzicato paronychia is related to infection in the nail fold in string players and secondary to pizzicato playing, whereby the musician plucks the instrument strings with the nails and fingertips.3
Acrylates in artificial nails frequently are used among guitarists to strengthen their nails. A case of occupational allergic contact dermatitis induced by acrylic gel nails in a flamenco guitarist was described.9 The patient developed dystrophy, onycholysis, and paronychia involving the nails of the right hand where acrylic materials were used, which resolved following the removal of the artificial nails. Patch tests were performed and were positive for 2-hydroxyethyl methacrylate, 2-hydroxyethyl acrylate, ethylene glycol dimethacrylate, and 2-hydroxypropyl methacrylate, supporting the diagnosis of allergic contact dermatitis to acrylates.9 Therefore, musicians should be aware of the sensitizing potential of acrylates and adopt preventive measures.
Unilateral Raynaud phenomenon of the dominant hand was noted in 3 cases of musicians who played string instruments due to the increased tendency to vasospasm in the digital capillaries from the direct transmission of vibrations of the strings (>100 Hz).12-14 Consequently, the disruption of the digital blood circulation leads to an abnormal reaction to cold, which is called vibration-induced white fingers or vasospastic white finger disease.19 In these 3 patients, capillaroscopy showed a nonspecific pattern with a lack of morphologic homogeneity of capillaries, the presence of enlarged capillaries, ectasia of the efferent tract of the loops, tortuous capillaries, local hemorrhages, and neoangiogenesis.13,14


A middle-aged professional concert pianist presented with paronychia with hyperkeratosis of the lateral nail fold. Histopathology revealed a subungual keratoacanthoma eroding the distal phalanx tip, which was removed by surgical excision. The repeated fingertip trauma associated with pianistic activity was suspected to be the causative event.16
Callosities also are common on the fingertips of musicians, including 18.4% of patients in a cohort of 628 musicians, and involving fingers in 64.6% of these patients.4 These callosities are explained by the chronic mechanical forces and characterize the way musicians grasp and hold their instruments. Callosities could be preceded by soreness and blisters of the fingertips in a harpist (harpist’s finger).1,15 Calluses were located on the lateral fourth fingertip of a drummer corresponding to the friction with the drumsticks (drummer’s digit) and on the thumb of a bassoon player. Trumpet calluses generally overlie the proximal interphalangeal joint of the left index finger.
Conclusion
Healthy nails are essential for playing a musical instrument. This review highlights the occurrence of fingertip callosities, paronychia, onycholysis, and subungual hemorrhages among musicians who play instruments. Additionally, the transmission of string-vibratory movements can produce microvascular damage and occupational Raynaud phenomenon in some musicians. These occupational nail disorders are underrecognized and may be underdiagnosed. Thus, musicians and clinicians must be aware of these alterations to adopt preventive measures and to provide adequate treatment.
- Rimmer S, Spielvogel RL. Dermatologic problems of musicians. J Am Acad Dermatol. 1990;22:657-663.
- Adams RM. Skin conditions of musicians. Cutis. 2000;65:37-38.
- Vine K, DeLeo V. Dermatologic manifestations of musicians: a case report and review of skin conditions in musicians. Cutis. 2011;87:117-121.
- Patruno C, Napolitano M, La Bella S, et al. Instrument-related skin disorders in musicians. Dermatitis. 2016;27:26-29.
- Baccouche D, Mokni M, Ben Abdelaziz A, et al. Dermatological problems of musicians: a prospective study in musical students . Article in French. Ann Dermatol Venereol. 2007;134(5 Pt 1):445-449.
- Piraccini BM, Antonucci A, Iorizzo M, et al. Occupational nail fragility in a professional violist. Contact Dermatitis. 2004;51:35-36.
- Wu JJ. Habit tic deformity secondary to guitar playing. Dermatol Online J. 2009;15:16.
- Kluger N. Piano glissando purpura: another cutaneous curiosity in musicians. J Eur Acad Dermatol Venereol. 2016;30:683.
- Alcántara-Nicolás FA, Pastor-Nieto MA, Sánchez-Herreros C, et al. Allergic contact dermatitis from acrylic nails in a flamenco guitarist. Occup Med (Lond). 2016;66:751-753.
- Baran R, Tosti A. Occupational acroosteolysis in a guitar player. Acta Derm Venereol. 1993;73:64-65.
- Destouet JM, Murphy WA. Guitar player acro-osteolysis. Skeletal Radiol. 1981;6:275-277.
- Jepsen JR, Simonsen JA. Raynaud’s phenomenon in a slap bass player: a case report. Med Probl Perform Art. 2016;31:51-53.
- Sirufo MM, Catalogna A, De Pietro F, et al. Raynaud’s phenomenon in a drummer player: microvascular disorder and nailfold video capillaroscopic findings. EXCLI J. 2021;20:1526-1531.
- Sirufo MM, Ginaldi L, De Martinis M. Raynaud’s phenomenon and the nailfold capillaroscopic findings in a guitar player. QJM. 2019;112:531-533.
- Cohen PR. Harpist’s finger: case report of a trauma-induced blister in a beginner harpist and review of string instrument-associated skin problems in musicians. Cutis. 2008;82:329-334.
- De Vasconcelos P, Soares-Almeida L, Filipe P. Subungual keratoacanthoma in a pianist. G Ital Dermatol Venereol. 2016;151:455-456.
- Young RS, Bryk D, Ratner H. Selective phalangeal tuft fractures in a guitar player. Br J Radiol. 1977;50:147-148.
- Vázquez-Osorio I, Espasandín-Arias M, García-Gavín J, et al. Allergic contact dermatitis due to acrylates in acrylic gel nails: a report of 3 cases. Actas Dermosifiliogr. 2014;105:430-432.
- Atashpaz S, Ghabili K. Color triad in guitarist’s fingers: a probable case of Raynaud’s phenomenon due to string vibration phenomenon. Med Probl Perform Art. 2008;23:143.
A variety of skin problems can occur in musicians due to the repetitive movements of playing instruments.1,2 Musicians’ nails are continuously exposed to the mechanical forces and chemical substances characteristic of their instruments.3 Occupational nail alterations in musicians caused by repetitive physical trauma, allergic contact dermatitis, and/or infection may lead to disability and compromise their professional career.
We conducted a systematic review of the literature on the clinical features of musical instrument–related nail alterations to optimize the management and prevention of these conditions.
Methods
We conducted a systematic review of PubMed, Scopus, and Google Scholar databases for eligible publications on instrument-related nail alterations in musicians using the search terms musicians with nail, onychopathy, and Raynaud. No time or language criteria were applied. Reviews, editorials, and articles not related to the topic were excluded. Bibliographies/reference lists were checked to find any additional relevant publications. Relevant articles in English and French were screened by 2 independent reviewers (A.G. and N.L.), and the following data were extracted for qualitative synthesis: sex, age, musical instrument, clinical features, number of years practicing the instrument, laboratory investigations, and disease course.
Results
The literature search yielded 11 publications. Sixteen additional articles were identified by other methods (ie, references, related publications). Overall, 3 full-text articles described general nail alterations but did not describe the clinical data, and 11 publications were editorials, commentaries, reviews, or not relevant. Thirteen contributions fulfilled the inclusion criteria and were eligible for qualitative synthesis. The flow diagram illustrates the screening process (Figure 1).
Twenty-three patients were included. The instruments identified were divided into 2 groups: string instruments (ie, guitar, violin, harp) and percussion instruments (ie, drums, piano, slap bass). Nail alterations were clinically expressed as: (1) modifications of the nail surface; (2) nail bed, soft-tissue, and bone abnormalities; and (3) periungual tissue and distal pulp disorders. All cases are summarized in the Table.4-16 Three articles described occupational Raynaud phenomenon.12-14
Comment
Modifications of the Nail Surface—Onychodystrophy, such as deformity or discoloration of the nail plate, was described in 6 patients among a cohort of 295 musicians and an additional 6 patients among 199 musicians with induced skin lesions. This condition was most common in string instrument players and pianists due to injury and irritation.
One patient, who had been a professional violist for 27 years, presented with lamellar onychoschizia, which corresponds to a horizontal splitting of the nail toward its distal portion (Figure 2). The 3 fingernails of the dominant hand were involved with a V-shaped incision of the distal margin of the nail due to the repetitive friction of the nails with the strings.6
Striations of the nail plate were reported in a guitarist who played for 10 years.7 Physical examination revealed linear transverse ridges alternating with depressions on the central aspect of the nail plate of the right thumbnail, as the patient was right-handed. This condition, attributed to sustained pressure on the string applied by the thumb, also has been called habit tic deformity.7
Nail Bed, Soft-Tissue, and Bone Lesions—Purpura (or hemorrhage) of the nail bed was associated with a percussion instrument (ie, piano) in 1 patient, affecting the second, third, and fourth fingernails of the right hand.8 Especially when performing ascending glissando passages, the pianist applies pressure that may damage the finger and cause fingernail purpura. This condition improved after the patient stopping practicing glissandi.8
Three patients—2 guitarists and 1 violist—had onycholysis, defined by a loss of the attachment between the nail bed and the nail plate (Figure 3). It may result from repetitive trauma when strings are plucked.6,9,10
Acro-osteolysis associated with pain was reported in 2 guitarists.10,11 This condition is defined as transverse lytic bands in the distal phalanges (Figure 4). Acro-osteolysis may be secondary to multiple causes, such as vinyl chloride exposure, connective tissue diseases, thermal injuries, neuropathic diseases, hyperparathyroidism, nutritional deficiencies, psoriasis, and biomechanical stress.10 In musicians playing instruments, the mechanical stress to the guitar-playing fingers is the causative factor.17
Periungual Tissue and Distal Pulp Disorders—Paronychia is an important occupational hazard of harpists, violists, and pianists.2 It represents an inflammatory condition involving the folds of tissue surrounding fingernails. Pizzicato paronychia is related to infection in the nail fold in string players and secondary to pizzicato playing, whereby the musician plucks the instrument strings with the nails and fingertips.3
Acrylates in artificial nails frequently are used among guitarists to strengthen their nails. A case of occupational allergic contact dermatitis induced by acrylic gel nails in a flamenco guitarist was described.9 The patient developed dystrophy, onycholysis, and paronychia involving the nails of the right hand where acrylic materials were used, which resolved following the removal of the artificial nails. Patch tests were performed and were positive for 2-hydroxyethyl methacrylate, 2-hydroxyethyl acrylate, ethylene glycol dimethacrylate, and 2-hydroxypropyl methacrylate, supporting the diagnosis of allergic contact dermatitis to acrylates.9 Therefore, musicians should be aware of the sensitizing potential of acrylates and adopt preventive measures.
Unilateral Raynaud phenomenon of the dominant hand was noted in 3 cases of musicians who played string instruments due to the increased tendency to vasospasm in the digital capillaries from the direct transmission of vibrations of the strings (>100 Hz).12-14 Consequently, the disruption of the digital blood circulation leads to an abnormal reaction to cold, which is called vibration-induced white fingers or vasospastic white finger disease.19 In these 3 patients, capillaroscopy showed a nonspecific pattern with a lack of morphologic homogeneity of capillaries, the presence of enlarged capillaries, ectasia of the efferent tract of the loops, tortuous capillaries, local hemorrhages, and neoangiogenesis.13,14
A middle-aged professional concert pianist presented with paronychia with hyperkeratosis of the lateral nail fold. Histopathology revealed a subungual keratoacanthoma eroding the distal phalanx tip, which was removed by surgical excision. The repeated fingertip trauma associated with pianistic activity was suspected to be the causative event.16
Callosities also are common on the fingertips of musicians, including 18.4% of patients in a cohort of 628 musicians, and involving fingers in 64.6% of these patients.4 These callosities are explained by the chronic mechanical forces and characterize the way musicians grasp and hold their instruments. Callosities could be preceded by soreness and blisters of the fingertips in a harpist (harpist’s finger).1,15 Calluses were located on the lateral fourth fingertip of a drummer corresponding to the friction with the drumsticks (drummer’s digit) and on the thumb of a bassoon player. Trumpet calluses generally overlie the proximal interphalangeal joint of the left index finger.
Conclusion
Healthy nails are essential for playing a musical instrument. This review highlights the occurrence of fingertip callosities, paronychia, onycholysis, and subungual hemorrhages among musicians who play instruments. Additionally, the transmission of string-vibratory movements can produce microvascular damage and occupational Raynaud phenomenon in some musicians. These occupational nail disorders are underrecognized and may be underdiagnosed. Thus, musicians and clinicians must be aware of these alterations to adopt preventive measures and to provide adequate treatment.
A variety of skin problems can occur in musicians due to the repetitive movements of playing instruments.1,2 Musicians’ nails are continuously exposed to the mechanical forces and chemical substances characteristic of their instruments.3 Occupational nail alterations in musicians caused by repetitive physical trauma, allergic contact dermatitis, and/or infection may lead to disability and compromise their professional career.
We conducted a systematic review of the literature on the clinical features of musical instrument–related nail alterations to optimize the management and prevention of these conditions.
Methods
We conducted a systematic review of PubMed, Scopus, and Google Scholar databases for eligible publications on instrument-related nail alterations in musicians using the search terms musicians with nail, onychopathy, and Raynaud. No time or language criteria were applied. Reviews, editorials, and articles not related to the topic were excluded. Bibliographies/reference lists were checked to find any additional relevant publications. Relevant articles in English and French were screened by 2 independent reviewers (A.G. and N.L.), and the following data were extracted for qualitative synthesis: sex, age, musical instrument, clinical features, number of years practicing the instrument, laboratory investigations, and disease course.
Results
The literature search yielded 11 publications. Sixteen additional articles were identified by other methods (ie, references, related publications). Overall, 3 full-text articles described general nail alterations but did not describe the clinical data, and 11 publications were editorials, commentaries, reviews, or not relevant. Thirteen contributions fulfilled the inclusion criteria and were eligible for qualitative synthesis. The flow diagram illustrates the screening process (Figure 1).
Twenty-three patients were included. The instruments identified were divided into 2 groups: string instruments (ie, guitar, violin, harp) and percussion instruments (ie, drums, piano, slap bass). Nail alterations were clinically expressed as: (1) modifications of the nail surface; (2) nail bed, soft-tissue, and bone abnormalities; and (3) periungual tissue and distal pulp disorders. All cases are summarized in the Table.4-16 Three articles described occupational Raynaud phenomenon.12-14
Comment
Modifications of the Nail Surface—Onychodystrophy, such as deformity or discoloration of the nail plate, was described in 6 patients among a cohort of 295 musicians and an additional 6 patients among 199 musicians with induced skin lesions. This condition was most common in string instrument players and pianists due to injury and irritation.
One patient, who had been a professional violist for 27 years, presented with lamellar onychoschizia, which corresponds to a horizontal splitting of the nail toward its distal portion (Figure 2). The 3 fingernails of the dominant hand were involved with a V-shaped incision of the distal margin of the nail due to the repetitive friction of the nails with the strings.6
Striations of the nail plate were reported in a guitarist who played for 10 years.7 Physical examination revealed linear transverse ridges alternating with depressions on the central aspect of the nail plate of the right thumbnail, as the patient was right-handed. This condition, attributed to sustained pressure on the string applied by the thumb, also has been called habit tic deformity.7
Nail Bed, Soft-Tissue, and Bone Lesions—Purpura (or hemorrhage) of the nail bed was associated with a percussion instrument (ie, piano) in 1 patient, affecting the second, third, and fourth fingernails of the right hand.8 Especially when performing ascending glissando passages, the pianist applies pressure that may damage the finger and cause fingernail purpura. This condition improved after the patient stopping practicing glissandi.8
Three patients—2 guitarists and 1 violist—had onycholysis, defined by a loss of the attachment between the nail bed and the nail plate (Figure 3). It may result from repetitive trauma when strings are plucked.6,9,10
Acro-osteolysis associated with pain was reported in 2 guitarists.10,11 This condition is defined as transverse lytic bands in the distal phalanges (Figure 4). Acro-osteolysis may be secondary to multiple causes, such as vinyl chloride exposure, connective tissue diseases, thermal injuries, neuropathic diseases, hyperparathyroidism, nutritional deficiencies, psoriasis, and biomechanical stress.10 In musicians playing instruments, the mechanical stress to the guitar-playing fingers is the causative factor.17
Periungual Tissue and Distal Pulp Disorders—Paronychia is an important occupational hazard of harpists, violists, and pianists.2 It represents an inflammatory condition involving the folds of tissue surrounding fingernails. Pizzicato paronychia is related to infection in the nail fold in string players and secondary to pizzicato playing, whereby the musician plucks the instrument strings with the nails and fingertips.3
Acrylates in artificial nails frequently are used among guitarists to strengthen their nails. A case of occupational allergic contact dermatitis induced by acrylic gel nails in a flamenco guitarist was described.9 The patient developed dystrophy, onycholysis, and paronychia involving the nails of the right hand where acrylic materials were used, which resolved following the removal of the artificial nails. Patch tests were performed and were positive for 2-hydroxyethyl methacrylate, 2-hydroxyethyl acrylate, ethylene glycol dimethacrylate, and 2-hydroxypropyl methacrylate, supporting the diagnosis of allergic contact dermatitis to acrylates.9 Therefore, musicians should be aware of the sensitizing potential of acrylates and adopt preventive measures.
Unilateral Raynaud phenomenon of the dominant hand was noted in 3 cases of musicians who played string instruments due to the increased tendency to vasospasm in the digital capillaries from the direct transmission of vibrations of the strings (>100 Hz).12-14 Consequently, the disruption of the digital blood circulation leads to an abnormal reaction to cold, which is called vibration-induced white fingers or vasospastic white finger disease.19 In these 3 patients, capillaroscopy showed a nonspecific pattern with a lack of morphologic homogeneity of capillaries, the presence of enlarged capillaries, ectasia of the efferent tract of the loops, tortuous capillaries, local hemorrhages, and neoangiogenesis.13,14
A middle-aged professional concert pianist presented with paronychia with hyperkeratosis of the lateral nail fold. Histopathology revealed a subungual keratoacanthoma eroding the distal phalanx tip, which was removed by surgical excision. The repeated fingertip trauma associated with pianistic activity was suspected to be the causative event.16
Callosities also are common on the fingertips of musicians, including 18.4% of patients in a cohort of 628 musicians, and involving fingers in 64.6% of these patients.4 These callosities are explained by the chronic mechanical forces and characterize the way musicians grasp and hold their instruments. Callosities could be preceded by soreness and blisters of the fingertips in a harpist (harpist’s finger).1,15 Calluses were located on the lateral fourth fingertip of a drummer corresponding to the friction with the drumsticks (drummer’s digit) and on the thumb of a bassoon player. Trumpet calluses generally overlie the proximal interphalangeal joint of the left index finger.
Conclusion
Healthy nails are essential for playing a musical instrument. This review highlights the occurrence of fingertip callosities, paronychia, onycholysis, and subungual hemorrhages among musicians who play instruments. Additionally, the transmission of string-vibratory movements can produce microvascular damage and occupational Raynaud phenomenon in some musicians. These occupational nail disorders are underrecognized and may be underdiagnosed. Thus, musicians and clinicians must be aware of these alterations to adopt preventive measures and to provide adequate treatment.
- Rimmer S, Spielvogel RL. Dermatologic problems of musicians. J Am Acad Dermatol. 1990;22:657-663.
- Adams RM. Skin conditions of musicians. Cutis. 2000;65:37-38.
- Vine K, DeLeo V. Dermatologic manifestations of musicians: a case report and review of skin conditions in musicians. Cutis. 2011;87:117-121.
- Patruno C, Napolitano M, La Bella S, et al. Instrument-related skin disorders in musicians. Dermatitis. 2016;27:26-29.
- Baccouche D, Mokni M, Ben Abdelaziz A, et al. Dermatological problems of musicians: a prospective study in musical students . Article in French. Ann Dermatol Venereol. 2007;134(5 Pt 1):445-449.
- Piraccini BM, Antonucci A, Iorizzo M, et al. Occupational nail fragility in a professional violist. Contact Dermatitis. 2004;51:35-36.
- Wu JJ. Habit tic deformity secondary to guitar playing. Dermatol Online J. 2009;15:16.
- Kluger N. Piano glissando purpura: another cutaneous curiosity in musicians. J Eur Acad Dermatol Venereol. 2016;30:683.
- Alcántara-Nicolás FA, Pastor-Nieto MA, Sánchez-Herreros C, et al. Allergic contact dermatitis from acrylic nails in a flamenco guitarist. Occup Med (Lond). 2016;66:751-753.
- Baran R, Tosti A. Occupational acroosteolysis in a guitar player. Acta Derm Venereol. 1993;73:64-65.
- Destouet JM, Murphy WA. Guitar player acro-osteolysis. Skeletal Radiol. 1981;6:275-277.
- Jepsen JR, Simonsen JA. Raynaud’s phenomenon in a slap bass player: a case report. Med Probl Perform Art. 2016;31:51-53.
- Sirufo MM, Catalogna A, De Pietro F, et al. Raynaud’s phenomenon in a drummer player: microvascular disorder and nailfold video capillaroscopic findings. EXCLI J. 2021;20:1526-1531.
- Sirufo MM, Ginaldi L, De Martinis M. Raynaud’s phenomenon and the nailfold capillaroscopic findings in a guitar player. QJM. 2019;112:531-533.
- Cohen PR. Harpist’s finger: case report of a trauma-induced blister in a beginner harpist and review of string instrument-associated skin problems in musicians. Cutis. 2008;82:329-334.
- De Vasconcelos P, Soares-Almeida L, Filipe P. Subungual keratoacanthoma in a pianist. G Ital Dermatol Venereol. 2016;151:455-456.
- Young RS, Bryk D, Ratner H. Selective phalangeal tuft fractures in a guitar player. Br J Radiol. 1977;50:147-148.
- Vázquez-Osorio I, Espasandín-Arias M, García-Gavín J, et al. Allergic contact dermatitis due to acrylates in acrylic gel nails: a report of 3 cases. Actas Dermosifiliogr. 2014;105:430-432.
- Atashpaz S, Ghabili K. Color triad in guitarist’s fingers: a probable case of Raynaud’s phenomenon due to string vibration phenomenon. Med Probl Perform Art. 2008;23:143.
- Rimmer S, Spielvogel RL. Dermatologic problems of musicians. J Am Acad Dermatol. 1990;22:657-663.
- Adams RM. Skin conditions of musicians. Cutis. 2000;65:37-38.
- Vine K, DeLeo V. Dermatologic manifestations of musicians: a case report and review of skin conditions in musicians. Cutis. 2011;87:117-121.
- Patruno C, Napolitano M, La Bella S, et al. Instrument-related skin disorders in musicians. Dermatitis. 2016;27:26-29.
- Baccouche D, Mokni M, Ben Abdelaziz A, et al. Dermatological problems of musicians: a prospective study in musical students . Article in French. Ann Dermatol Venereol. 2007;134(5 Pt 1):445-449.
- Piraccini BM, Antonucci A, Iorizzo M, et al. Occupational nail fragility in a professional violist. Contact Dermatitis. 2004;51:35-36.
- Wu JJ. Habit tic deformity secondary to guitar playing. Dermatol Online J. 2009;15:16.
- Kluger N. Piano glissando purpura: another cutaneous curiosity in musicians. J Eur Acad Dermatol Venereol. 2016;30:683.
- Alcántara-Nicolás FA, Pastor-Nieto MA, Sánchez-Herreros C, et al. Allergic contact dermatitis from acrylic nails in a flamenco guitarist. Occup Med (Lond). 2016;66:751-753.
- Baran R, Tosti A. Occupational acroosteolysis in a guitar player. Acta Derm Venereol. 1993;73:64-65.
- Destouet JM, Murphy WA. Guitar player acro-osteolysis. Skeletal Radiol. 1981;6:275-277.
- Jepsen JR, Simonsen JA. Raynaud’s phenomenon in a slap bass player: a case report. Med Probl Perform Art. 2016;31:51-53.
- Sirufo MM, Catalogna A, De Pietro F, et al. Raynaud’s phenomenon in a drummer player: microvascular disorder and nailfold video capillaroscopic findings. EXCLI J. 2021;20:1526-1531.
- Sirufo MM, Ginaldi L, De Martinis M. Raynaud’s phenomenon and the nailfold capillaroscopic findings in a guitar player. QJM. 2019;112:531-533.
- Cohen PR. Harpist’s finger: case report of a trauma-induced blister in a beginner harpist and review of string instrument-associated skin problems in musicians. Cutis. 2008;82:329-334.
- De Vasconcelos P, Soares-Almeida L, Filipe P. Subungual keratoacanthoma in a pianist. G Ital Dermatol Venereol. 2016;151:455-456.
- Young RS, Bryk D, Ratner H. Selective phalangeal tuft fractures in a guitar player. Br J Radiol. 1977;50:147-148.
- Vázquez-Osorio I, Espasandín-Arias M, García-Gavín J, et al. Allergic contact dermatitis due to acrylates in acrylic gel nails: a report of 3 cases. Actas Dermosifiliogr. 2014;105:430-432.
- Atashpaz S, Ghabili K. Color triad in guitarist’s fingers: a probable case of Raynaud’s phenomenon due to string vibration phenomenon. Med Probl Perform Art. 2008;23:143.
Practice Points
- Long-term practice and performance with a musical instrument predispose musicians to several skin conditions and nail disorders.
- Nail alterations in musicians include onychodystrophy, callosities of the fingertips, paronychia, distal onycholysis, lamellar onychoschizia, striations, subungual hemorrhage, and occupational Raynaud phenomenon.
- Nail lesions in musicians may be caused by localized pressure, friction-induced mechanical forces, allergic or irritant contact dermatitis, or infections.

Urticaria Linked to Higher Cancer Risk, Study Finds
TOPLINE:
which decreased to 6% in subsequent years, in a cohort study using Danish healthcare databases.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from Danish healthcare registries and compared the incident cancer risk between patients with urticaria and the risk in the general population.
- They identified 87,507 patients (58% women) with a primary or secondary first-time hospital outpatient clinic, emergency room, or inpatient diagnosis of urticaria between 1980 and 2022, who were followed for a median of 10.1 years.
- Incident cancers, including nonmelanoma skin cancer, were identified using the Danish Cancer Registry and classified by the extent of spread at the time of diagnosis.
- This study computed the absolute cancer risk within the first year of an urticaria diagnosis and standardized incidence ratios (SIRs), with 95% CIs standardized to Danish national cancer rates.
TAKEAWAY:
- For the first year of follow-up, the absolute risk for all cancer types was 0.7%, and it was 29.5% for subsequent years. The overall SIR for all types of cancer was 1.09 (95% CI, 1.06-1.11), which was based on 7788 observed cancer cases compared with 7161 cases expected over the entire follow-up period.
- Within the first year of follow-up, 588 patients with urticaria were diagnosed with cancer, for an SIR of 1.49 (95% CI, 1.38-1.62) for all cancer types.
- After the first year, the SIR for all cancer sites decreased and stabilized at 1.06 (95% CI, 1.04-1.09), with 7200 observed cancer cases.
- The risk was highest for hematological cancers in the first year, particularly Hodgkin lymphoma (SIR, 5.35; 95% CI, 2.56-9.85).
IN PRACTICE:
“Our study suggests that urticaria may be a marker of occult cancer and that it is associated with a slightly increased long-term cancer risk,” the authors wrote.
SOURCE:
The study was led by Sissel B.T. Sørensen, departments of dermatology and rheumatology, Aarhus University Hospital, Aarhus, Denmark. It was published online on June 27, 2024, in the British Journal of Dermatology.
LIMITATIONS:
The study is limited by its observational design and reliance on registry data, which may be subject to misclassification or incomplete information. In addition, the study could not assess individual patient factors such as lifestyle or genetic predispositions that may influence cancer risk, and the results may not be generalizable to other populations. Finally, the exact biologic mechanisms linking urticaria and cancer remain unclear, warranting further investigation.
DISCLOSURES:
The study did not receive any funding. The authors reported that they had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
which decreased to 6% in subsequent years, in a cohort study using Danish healthcare databases.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from Danish healthcare registries and compared the incident cancer risk between patients with urticaria and the risk in the general population.
- They identified 87,507 patients (58% women) with a primary or secondary first-time hospital outpatient clinic, emergency room, or inpatient diagnosis of urticaria between 1980 and 2022, who were followed for a median of 10.1 years.
- Incident cancers, including nonmelanoma skin cancer, were identified using the Danish Cancer Registry and classified by the extent of spread at the time of diagnosis.
- This study computed the absolute cancer risk within the first year of an urticaria diagnosis and standardized incidence ratios (SIRs), with 95% CIs standardized to Danish national cancer rates.
TAKEAWAY:
- For the first year of follow-up, the absolute risk for all cancer types was 0.7%, and it was 29.5% for subsequent years. The overall SIR for all types of cancer was 1.09 (95% CI, 1.06-1.11), which was based on 7788 observed cancer cases compared with 7161 cases expected over the entire follow-up period.
- Within the first year of follow-up, 588 patients with urticaria were diagnosed with cancer, for an SIR of 1.49 (95% CI, 1.38-1.62) for all cancer types.
- After the first year, the SIR for all cancer sites decreased and stabilized at 1.06 (95% CI, 1.04-1.09), with 7200 observed cancer cases.
- The risk was highest for hematological cancers in the first year, particularly Hodgkin lymphoma (SIR, 5.35; 95% CI, 2.56-9.85).
IN PRACTICE:
“Our study suggests that urticaria may be a marker of occult cancer and that it is associated with a slightly increased long-term cancer risk,” the authors wrote.
SOURCE:
The study was led by Sissel B.T. Sørensen, departments of dermatology and rheumatology, Aarhus University Hospital, Aarhus, Denmark. It was published online on June 27, 2024, in the British Journal of Dermatology.
LIMITATIONS:
The study is limited by its observational design and reliance on registry data, which may be subject to misclassification or incomplete information. In addition, the study could not assess individual patient factors such as lifestyle or genetic predispositions that may influence cancer risk, and the results may not be generalizable to other populations. Finally, the exact biologic mechanisms linking urticaria and cancer remain unclear, warranting further investigation.
DISCLOSURES:
The study did not receive any funding. The authors reported that they had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
which decreased to 6% in subsequent years, in a cohort study using Danish healthcare databases.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from Danish healthcare registries and compared the incident cancer risk between patients with urticaria and the risk in the general population.
- They identified 87,507 patients (58% women) with a primary or secondary first-time hospital outpatient clinic, emergency room, or inpatient diagnosis of urticaria between 1980 and 2022, who were followed for a median of 10.1 years.
- Incident cancers, including nonmelanoma skin cancer, were identified using the Danish Cancer Registry and classified by the extent of spread at the time of diagnosis.
- This study computed the absolute cancer risk within the first year of an urticaria diagnosis and standardized incidence ratios (SIRs), with 95% CIs standardized to Danish national cancer rates.
TAKEAWAY:
- For the first year of follow-up, the absolute risk for all cancer types was 0.7%, and it was 29.5% for subsequent years. The overall SIR for all types of cancer was 1.09 (95% CI, 1.06-1.11), which was based on 7788 observed cancer cases compared with 7161 cases expected over the entire follow-up period.
- Within the first year of follow-up, 588 patients with urticaria were diagnosed with cancer, for an SIR of 1.49 (95% CI, 1.38-1.62) for all cancer types.
- After the first year, the SIR for all cancer sites decreased and stabilized at 1.06 (95% CI, 1.04-1.09), with 7200 observed cancer cases.
- The risk was highest for hematological cancers in the first year, particularly Hodgkin lymphoma (SIR, 5.35; 95% CI, 2.56-9.85).
IN PRACTICE:
“Our study suggests that urticaria may be a marker of occult cancer and that it is associated with a slightly increased long-term cancer risk,” the authors wrote.
SOURCE:
The study was led by Sissel B.T. Sørensen, departments of dermatology and rheumatology, Aarhus University Hospital, Aarhus, Denmark. It was published online on June 27, 2024, in the British Journal of Dermatology.
LIMITATIONS:
The study is limited by its observational design and reliance on registry data, which may be subject to misclassification or incomplete information. In addition, the study could not assess individual patient factors such as lifestyle or genetic predispositions that may influence cancer risk, and the results may not be generalizable to other populations. Finally, the exact biologic mechanisms linking urticaria and cancer remain unclear, warranting further investigation.
DISCLOSURES:
The study did not receive any funding. The authors reported that they had no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Postpartum Screening Critical for Urinary Symptoms and Related Mental Health
Bothersome urinary symptoms and incontinence at 12 months post partum are common and treatable, so screening for those symptoms as well as associated depression and anxiety is essential, write authors of a new study.
Sonia Bhandari Randhawa, MD, with the Department of Obstetrics and Gynecology, University of Texas Southwestern Medical Center in Dallas, led the study published in Urogynecology, which identified factors associated with persistent stress urinary incontinence (SUI), marked by leakage from sudden movements such as coughing or jumping; urgency UI (UUI), leakage after a sudden and intense need to urinate, even if the bladder isn’t full; and other overall bothersome urinary symptoms 1 year after delivery.
Associations by Subtype
Dr. Randhawa analyzed data provided by 419 patients (77% Hispanic White and 22% non-Hispanic Black). After multivariable analysis, SUI (n = 136, 32.5%) was significantly associated with greater body mass index (BMI) at the time of delivery and greater depression screening scores. Factors not associated included fetal birth weight, mode of delivery, degree of laceration, and breastfeeding status.
UUI (n = 69, 16.5%) was significantly associated with more births and higher anxiety screening scores. Women with overall urinary symptom bother also had significantly more births and higher anxiety screening scores.
“These findings support the [American College of Obstetricians and Gynecologists] recommendations for routine mental health and urinary incontinence screening in the postpartum period,” said Gena Dunivan, MD, director of the Division of Urogynecology and Pelvic Reconstructive Surgery at University of Alabama–Birmingham, who was not part of the study. “Routine screening for these issues will hopefully reduce the stigma, allowing more patients to receive the help they deserve.”
1 in 3 Postpartum Patients Affected by Urinary Incontinence
About one third of postpartum patients are affected by urinary incontinence, which is linked with poorer quality of life and mental health outcomes, the authors note.
Estimates of incontinence frequency post partum vary depending on the population studied, differences in subgroups, and definition of urinary incontinence. A strength of the study was its sizable population, made up almost entirely of Hispanic White and non-Hispanic Black women receiving care at a large safety-net hospital.
“This study has important clinical implications for postpartum patients,” the authors write. “Given an array of proven treatment options for both UUI and SUI, maternal health surveillance needs to include routine inquiry about UI to overcome patients’ reluctance for seeking care. Next, as elevated BMI was identified as a risk factor for persistent postpartum SUI, maintaining a healthy weight should be routinely encouraged during antenatal and postpartum clinic visits.”
Lauren Giugale, MD, director of UPMC’s Magee-Womens Hospital Postpartum Pelvic Floor Healing Clinic in Pittsburgh, Pennsylvania, says an important aspect of the study is that it measured urinary symptoms 1 year after delivery and shows that these symptoms persist. “A lot of studies look more short term,” she noted.
She also pointed to the study’s population of Black and Hispanic women, populations which “have been pretty hard to capture in urogynecology research. It’s important for us to understand these urinary symptoms are affecting those women as well as White women.”
Association With Anxiety
The association between postpartum depression scores and SUI is important, she says, but Dr. Randhawa’s team also “uniquely looked at anxiety scores in postpartum women. They showed an association between anxiety scores and UUI, so there’s certainly a potential impact of postpartum urinary symptoms on maternal mental health and maternal well-being.” The relationship between anxiety and depression and postpartum urinary symptoms is not well understood and warrants further research, she says.
In her role, Dr. Giugale says, she always asks about urinary symptoms, particularly in postpartum women. But she notes that some ob.gyn.s without urogynecology training may not prioritize those questions amid all the other information they need to cover.
She says she tells her residents to ask patients pointedly, “Are you having any urine leakage? Patients may not think it’s a problem that can be addressed. We do patients a disservice when we don’t ask the important questions that might potentially impact patients’ lives.”
The authors and Dr. Giugale and Dr. Dunivan report no relevant financial relationships.
Bothersome urinary symptoms and incontinence at 12 months post partum are common and treatable, so screening for those symptoms as well as associated depression and anxiety is essential, write authors of a new study.
Sonia Bhandari Randhawa, MD, with the Department of Obstetrics and Gynecology, University of Texas Southwestern Medical Center in Dallas, led the study published in Urogynecology, which identified factors associated with persistent stress urinary incontinence (SUI), marked by leakage from sudden movements such as coughing or jumping; urgency UI (UUI), leakage after a sudden and intense need to urinate, even if the bladder isn’t full; and other overall bothersome urinary symptoms 1 year after delivery.
Associations by Subtype
Dr. Randhawa analyzed data provided by 419 patients (77% Hispanic White and 22% non-Hispanic Black). After multivariable analysis, SUI (n = 136, 32.5%) was significantly associated with greater body mass index (BMI) at the time of delivery and greater depression screening scores. Factors not associated included fetal birth weight, mode of delivery, degree of laceration, and breastfeeding status.
UUI (n = 69, 16.5%) was significantly associated with more births and higher anxiety screening scores. Women with overall urinary symptom bother also had significantly more births and higher anxiety screening scores.
“These findings support the [American College of Obstetricians and Gynecologists] recommendations for routine mental health and urinary incontinence screening in the postpartum period,” said Gena Dunivan, MD, director of the Division of Urogynecology and Pelvic Reconstructive Surgery at University of Alabama–Birmingham, who was not part of the study. “Routine screening for these issues will hopefully reduce the stigma, allowing more patients to receive the help they deserve.”
1 in 3 Postpartum Patients Affected by Urinary Incontinence
About one third of postpartum patients are affected by urinary incontinence, which is linked with poorer quality of life and mental health outcomes, the authors note.
Estimates of incontinence frequency post partum vary depending on the population studied, differences in subgroups, and definition of urinary incontinence. A strength of the study was its sizable population, made up almost entirely of Hispanic White and non-Hispanic Black women receiving care at a large safety-net hospital.
“This study has important clinical implications for postpartum patients,” the authors write. “Given an array of proven treatment options for both UUI and SUI, maternal health surveillance needs to include routine inquiry about UI to overcome patients’ reluctance for seeking care. Next, as elevated BMI was identified as a risk factor for persistent postpartum SUI, maintaining a healthy weight should be routinely encouraged during antenatal and postpartum clinic visits.”
Lauren Giugale, MD, director of UPMC’s Magee-Womens Hospital Postpartum Pelvic Floor Healing Clinic in Pittsburgh, Pennsylvania, says an important aspect of the study is that it measured urinary symptoms 1 year after delivery and shows that these symptoms persist. “A lot of studies look more short term,” she noted.
She also pointed to the study’s population of Black and Hispanic women, populations which “have been pretty hard to capture in urogynecology research. It’s important for us to understand these urinary symptoms are affecting those women as well as White women.”
Association With Anxiety
The association between postpartum depression scores and SUI is important, she says, but Dr. Randhawa’s team also “uniquely looked at anxiety scores in postpartum women. They showed an association between anxiety scores and UUI, so there’s certainly a potential impact of postpartum urinary symptoms on maternal mental health and maternal well-being.” The relationship between anxiety and depression and postpartum urinary symptoms is not well understood and warrants further research, she says.
In her role, Dr. Giugale says, she always asks about urinary symptoms, particularly in postpartum women. But she notes that some ob.gyn.s without urogynecology training may not prioritize those questions amid all the other information they need to cover.
She says she tells her residents to ask patients pointedly, “Are you having any urine leakage? Patients may not think it’s a problem that can be addressed. We do patients a disservice when we don’t ask the important questions that might potentially impact patients’ lives.”
The authors and Dr. Giugale and Dr. Dunivan report no relevant financial relationships.
Bothersome urinary symptoms and incontinence at 12 months post partum are common and treatable, so screening for those symptoms as well as associated depression and anxiety is essential, write authors of a new study.
Sonia Bhandari Randhawa, MD, with the Department of Obstetrics and Gynecology, University of Texas Southwestern Medical Center in Dallas, led the study published in Urogynecology, which identified factors associated with persistent stress urinary incontinence (SUI), marked by leakage from sudden movements such as coughing or jumping; urgency UI (UUI), leakage after a sudden and intense need to urinate, even if the bladder isn’t full; and other overall bothersome urinary symptoms 1 year after delivery.
Associations by Subtype
Dr. Randhawa analyzed data provided by 419 patients (77% Hispanic White and 22% non-Hispanic Black). After multivariable analysis, SUI (n = 136, 32.5%) was significantly associated with greater body mass index (BMI) at the time of delivery and greater depression screening scores. Factors not associated included fetal birth weight, mode of delivery, degree of laceration, and breastfeeding status.
UUI (n = 69, 16.5%) was significantly associated with more births and higher anxiety screening scores. Women with overall urinary symptom bother also had significantly more births and higher anxiety screening scores.
“These findings support the [American College of Obstetricians and Gynecologists] recommendations for routine mental health and urinary incontinence screening in the postpartum period,” said Gena Dunivan, MD, director of the Division of Urogynecology and Pelvic Reconstructive Surgery at University of Alabama–Birmingham, who was not part of the study. “Routine screening for these issues will hopefully reduce the stigma, allowing more patients to receive the help they deserve.”
1 in 3 Postpartum Patients Affected by Urinary Incontinence
About one third of postpartum patients are affected by urinary incontinence, which is linked with poorer quality of life and mental health outcomes, the authors note.
Estimates of incontinence frequency post partum vary depending on the population studied, differences in subgroups, and definition of urinary incontinence. A strength of the study was its sizable population, made up almost entirely of Hispanic White and non-Hispanic Black women receiving care at a large safety-net hospital.
“This study has important clinical implications for postpartum patients,” the authors write. “Given an array of proven treatment options for both UUI and SUI, maternal health surveillance needs to include routine inquiry about UI to overcome patients’ reluctance for seeking care. Next, as elevated BMI was identified as a risk factor for persistent postpartum SUI, maintaining a healthy weight should be routinely encouraged during antenatal and postpartum clinic visits.”
Lauren Giugale, MD, director of UPMC’s Magee-Womens Hospital Postpartum Pelvic Floor Healing Clinic in Pittsburgh, Pennsylvania, says an important aspect of the study is that it measured urinary symptoms 1 year after delivery and shows that these symptoms persist. “A lot of studies look more short term,” she noted.
She also pointed to the study’s population of Black and Hispanic women, populations which “have been pretty hard to capture in urogynecology research. It’s important for us to understand these urinary symptoms are affecting those women as well as White women.”
Association With Anxiety
The association between postpartum depression scores and SUI is important, she says, but Dr. Randhawa’s team also “uniquely looked at anxiety scores in postpartum women. They showed an association between anxiety scores and UUI, so there’s certainly a potential impact of postpartum urinary symptoms on maternal mental health and maternal well-being.” The relationship between anxiety and depression and postpartum urinary symptoms is not well understood and warrants further research, she says.
In her role, Dr. Giugale says, she always asks about urinary symptoms, particularly in postpartum women. But she notes that some ob.gyn.s without urogynecology training may not prioritize those questions amid all the other information they need to cover.
She says she tells her residents to ask patients pointedly, “Are you having any urine leakage? Patients may not think it’s a problem that can be addressed. We do patients a disservice when we don’t ask the important questions that might potentially impact patients’ lives.”
The authors and Dr. Giugale and Dr. Dunivan report no relevant financial relationships.
UROGYNECOLOGY
Does An Elevated Lp(a) Call for Low-dose Aspirin?
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
How Well Do Clinicians Support Patients’ Sexual Health?
From adolescence onward, the need for sexual health is particularly important. Yet, information and healthcare services are limited, which often leaves patients in distress and subject to misconceptions. What are the specific issues related to sexuality in adolescence, middle age, and beyond? This news organization interviewed Carol Burté, MD, a specialist in sexual medicine from Monaco.
Question: Regarding young individuals, what about sex education in schools?
Dr. Burté: The French law of 2018 specifies that at least three annual sessions must be devoted to sex education in elementary school, middle school, and high school.
In practice, this is not always the case, and interventions are very focused on prevention and rules. Sexuality is almost always absent from the program. Sexuality means: What does it mean to have desire? How does pleasure work? At what age do we have sex? etc. Young people receive prevention advice, but the link with sexuality is not made.
Sexuality remains taboo. You know, like in books: “They got married and had many children ...” End of the story, we don’t know more [laughs].
Question: And outside the school setting, do doctors sufficiently address sexual health issues with adolescents?
Dr. Burté: Rarely. I understand that a general practitioner has little time, but they can still ask the young person if they have any questions. They can refer them to someone or provide reading recommendations. Regarding sex education on the Internet, there are many well-made websites, such as the one by the national education system.
Also, it is important to give young people lifestyle advice to combat overweight, sedentary behavior, etc., by explaining to them that these factors can lead to sexual disorders later as well as infertility.
Another very important point: There is an inequality between boys and girls, but this time, to the disadvantage of boys. We have a sexual health consultation dedicated to young girls for the pill, but no one examines the boys. However, testicular cancer or undescended testicles can occur. I think we really need to change things and establish a clinical examination for boys in adolescence.
Question: More and more young people identify as asexual. What do you think of this?
Dr. Burté: People who identify as asexual represent about 1% of the population. These are individuals who are not attracted to having sexual relationships with someone. This does not prevent them from having a boyfriend, a girlfriend, masturbating, etc. It is sexual intercourse that does not interest them. These young people often say they have done it all. They have seen a lot of images, viewed sexuality as gymnastics with all the positions, tricks. They are jaded. Also, when you are faced with an image that provides a very strong and rapid stimulation, human relationships seem much more difficult because, obviously, you will never reproduce that sensation when you are with your partner with whom you must connect. The relationship is no longer emotional and shared. Yet, sexuality is emotional, relational, intellectual.
I think people go through phases. At a certain point, they feel asexual, but they can change their minds and think differently if they have real encounters, encounters that are increasingly difficult. Today, we are witnessing a loss of confidence. Young people, but also others, want to protect themselves from everything, especially from falling in love, not get back into a relationship because it is constraining.
Question: Data show that young people are exposed to pornography at an increasingly early age. Is this a problem for their future sexuality?
Dr. Burté: The exposure to pornography at an early age, around 11 years old, has only been a reality for the past decade. It is too early to say how it will impact their sexuality. When examining the literature on this subject, some publications indicate that the consequences can be dramatic for children. Others show that children can distinguish between reality and fantasy.
Whenever I see young people in consultation, I ask them whether they feel pornography has helped or hindered them, whether it is the cause of the issue they are facing. I would say that, other than those who have viewed pornography under duress, which is of the order of violence, pornography does not seem to pose a problem. It can even provide certain knowledge.
Question: What about sexual violence in children? What are the consequences?
Dr. Burté: In sexual medicine, this is one of the questions we ask systematically because it is very common. It is important to keep in mind that this not only affects girls; boys are also sexually abused. The consequences are dramatic in terms of psychosexual development. Each case is different.
Question: At the other end of life, is it “normal” to have sexual disorders at a certain age? Should we resign ourselves?
Dr. Burté: When it comes to sexuality, people have many misconceptions and beliefs that are conveyed through media and the Internet. One of them is to believe that because we are aging, we cannot have a proper sexuality. Sexuality slows down with age, as all sensitivities decrease, but desire is something present throughout life. Yet, seniors are rarely questioned about their sexual health by the media.
Note that older people in institutions face an additional obstacle: lack of privacy. Is this normal? Sexuality releases endorphins, oxytocin, it is well-being that costs nothing. It is something that should be prescribed!
Question: Chronic diseases, disabilities with incidence increases with age — are they not inevitable obstacles to a fulfilling sexuality?
Dr. Burté: It is possible to have a sexual life regardless of the disease one has, cancer, diabetes, rheumatic disease — regardless of the disability.
A collaboration with the National Cancer Institute on the preservation of sexual health after cancer in which I participated shows that people are extremely demanding of care and that this care is still very insufficient, unfortunately, even in the case of prostate cancer, for example, when it should be obvious.
Question: But aging itself brings challenges in terms of sexuality.
Dr. Burté: Yes, in men, the consequences of low testosterone levels are well known. Therefore, we must stop thinking that men do not have their “menopause.” Men often have a testosterone deficiency after a certain age. This is very annoying because they have many symptoms that are truly unpleasant and yet can be corrected by completely reliable treatments.
Men are very misinformed on this subject. We talk about gender inequality, but in this area, a young woman who has her first period knows very well that one day she will go through menopause, but a boy has no idea that one day he will have hormone problems.
Question: Therefore, is it important to question men past the age of 50 years?
Dr. Burté: Yes. Faced with sexual symptoms or simply fatigue, or among those who are a bit depressed, investigating a testosterone deficiency should be part of the reflexes.
Also, if you ask a man in general, “How is it going from a sexual point of view,” and he answers that everything is going well, this means he has good arteries, good veins, a good nervous system, sufficient hormones, and psychologically, everything is going rather well. Conversely, erectile dysfunction can be one of the first symptoms of cardiovascular pathologies.
After a certain age, there is no test that provides as much information about people’s health as this question about sexual health.
Question: On their side, are women better cared for at menopause?
Dr. Burté: Yes, but women still lack explanations. I work in sexual medicine, and in my consultation, I see women who come simply to get information about menopause.
Women must know that menopause is a turning point in life because they will spend 30%-40% of their lives without hormones.
It is important to explain that indeed, after menopause, without treatment, it is not the same. There are genital and urinary, psychological, sexual, and skin consequences. It is important to provide true data on the influence of hormonal treatments. Today, hormone fear is not over. I think we need to rehabilitate treatments, care for women.
Question: So we must not forget men or women.
Dr. Burté: Yes. It is also very important to adopt a perspective not only for the individual but also for the couple. If you treat a man with testosterone, after 3 months, he will be in great shape. However, if the couple has long been accustomed to having a limited sexual life, if the woman is not supported on her side, the couple will be unbalanced. The couple is concerned with managing the hormonal changes of both.
Question: Sexual medicine is essential, yet it seems inaccessible.
Dr. Burté: There are very few specialists in sexual medicine because there is no legal provision for it. These consultations are lengthy but not valued. Who wants to work for that?
If there was reimbursement for sexual medicine consultations at age 15 years, at menopause, and for men around the age of 50 years, it would change mentalities. Sexual medicine must be integrated into medicine. It should also be noted that not all sexologists are physicians.
Some people are very well trained through universities, and others are not. Ideally, someone with a sexual disorder should first have a sexual medicine consultation to understand the situation. Then, the physician can refer the patient to a competent sexologist because we work in a network.
Dr. Burté has no conflicts of interest related to the subject.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
From adolescence onward, the need for sexual health is particularly important. Yet, information and healthcare services are limited, which often leaves patients in distress and subject to misconceptions. What are the specific issues related to sexuality in adolescence, middle age, and beyond? This news organization interviewed Carol Burté, MD, a specialist in sexual medicine from Monaco.
Question: Regarding young individuals, what about sex education in schools?
Dr. Burté: The French law of 2018 specifies that at least three annual sessions must be devoted to sex education in elementary school, middle school, and high school.
In practice, this is not always the case, and interventions are very focused on prevention and rules. Sexuality is almost always absent from the program. Sexuality means: What does it mean to have desire? How does pleasure work? At what age do we have sex? etc. Young people receive prevention advice, but the link with sexuality is not made.
Sexuality remains taboo. You know, like in books: “They got married and had many children ...” End of the story, we don’t know more [laughs].
Question: And outside the school setting, do doctors sufficiently address sexual health issues with adolescents?
Dr. Burté: Rarely. I understand that a general practitioner has little time, but they can still ask the young person if they have any questions. They can refer them to someone or provide reading recommendations. Regarding sex education on the Internet, there are many well-made websites, such as the one by the national education system.
Also, it is important to give young people lifestyle advice to combat overweight, sedentary behavior, etc., by explaining to them that these factors can lead to sexual disorders later as well as infertility.
Another very important point: There is an inequality between boys and girls, but this time, to the disadvantage of boys. We have a sexual health consultation dedicated to young girls for the pill, but no one examines the boys. However, testicular cancer or undescended testicles can occur. I think we really need to change things and establish a clinical examination for boys in adolescence.
Question: More and more young people identify as asexual. What do you think of this?
Dr. Burté: People who identify as asexual represent about 1% of the population. These are individuals who are not attracted to having sexual relationships with someone. This does not prevent them from having a boyfriend, a girlfriend, masturbating, etc. It is sexual intercourse that does not interest them. These young people often say they have done it all. They have seen a lot of images, viewed sexuality as gymnastics with all the positions, tricks. They are jaded. Also, when you are faced with an image that provides a very strong and rapid stimulation, human relationships seem much more difficult because, obviously, you will never reproduce that sensation when you are with your partner with whom you must connect. The relationship is no longer emotional and shared. Yet, sexuality is emotional, relational, intellectual.
I think people go through phases. At a certain point, they feel asexual, but they can change their minds and think differently if they have real encounters, encounters that are increasingly difficult. Today, we are witnessing a loss of confidence. Young people, but also others, want to protect themselves from everything, especially from falling in love, not get back into a relationship because it is constraining.
Question: Data show that young people are exposed to pornography at an increasingly early age. Is this a problem for their future sexuality?
Dr. Burté: The exposure to pornography at an early age, around 11 years old, has only been a reality for the past decade. It is too early to say how it will impact their sexuality. When examining the literature on this subject, some publications indicate that the consequences can be dramatic for children. Others show that children can distinguish between reality and fantasy.
Whenever I see young people in consultation, I ask them whether they feel pornography has helped or hindered them, whether it is the cause of the issue they are facing. I would say that, other than those who have viewed pornography under duress, which is of the order of violence, pornography does not seem to pose a problem. It can even provide certain knowledge.
Question: What about sexual violence in children? What are the consequences?
Dr. Burté: In sexual medicine, this is one of the questions we ask systematically because it is very common. It is important to keep in mind that this not only affects girls; boys are also sexually abused. The consequences are dramatic in terms of psychosexual development. Each case is different.
Question: At the other end of life, is it “normal” to have sexual disorders at a certain age? Should we resign ourselves?
Dr. Burté: When it comes to sexuality, people have many misconceptions and beliefs that are conveyed through media and the Internet. One of them is to believe that because we are aging, we cannot have a proper sexuality. Sexuality slows down with age, as all sensitivities decrease, but desire is something present throughout life. Yet, seniors are rarely questioned about their sexual health by the media.
Note that older people in institutions face an additional obstacle: lack of privacy. Is this normal? Sexuality releases endorphins, oxytocin, it is well-being that costs nothing. It is something that should be prescribed!
Question: Chronic diseases, disabilities with incidence increases with age — are they not inevitable obstacles to a fulfilling sexuality?
Dr. Burté: It is possible to have a sexual life regardless of the disease one has, cancer, diabetes, rheumatic disease — regardless of the disability.
A collaboration with the National Cancer Institute on the preservation of sexual health after cancer in which I participated shows that people are extremely demanding of care and that this care is still very insufficient, unfortunately, even in the case of prostate cancer, for example, when it should be obvious.
Question: But aging itself brings challenges in terms of sexuality.
Dr. Burté: Yes, in men, the consequences of low testosterone levels are well known. Therefore, we must stop thinking that men do not have their “menopause.” Men often have a testosterone deficiency after a certain age. This is very annoying because they have many symptoms that are truly unpleasant and yet can be corrected by completely reliable treatments.
Men are very misinformed on this subject. We talk about gender inequality, but in this area, a young woman who has her first period knows very well that one day she will go through menopause, but a boy has no idea that one day he will have hormone problems.
Question: Therefore, is it important to question men past the age of 50 years?
Dr. Burté: Yes. Faced with sexual symptoms or simply fatigue, or among those who are a bit depressed, investigating a testosterone deficiency should be part of the reflexes.
Also, if you ask a man in general, “How is it going from a sexual point of view,” and he answers that everything is going well, this means he has good arteries, good veins, a good nervous system, sufficient hormones, and psychologically, everything is going rather well. Conversely, erectile dysfunction can be one of the first symptoms of cardiovascular pathologies.
After a certain age, there is no test that provides as much information about people’s health as this question about sexual health.
Question: On their side, are women better cared for at menopause?
Dr. Burté: Yes, but women still lack explanations. I work in sexual medicine, and in my consultation, I see women who come simply to get information about menopause.
Women must know that menopause is a turning point in life because they will spend 30%-40% of their lives without hormones.
It is important to explain that indeed, after menopause, without treatment, it is not the same. There are genital and urinary, psychological, sexual, and skin consequences. It is important to provide true data on the influence of hormonal treatments. Today, hormone fear is not over. I think we need to rehabilitate treatments, care for women.
Question: So we must not forget men or women.
Dr. Burté: Yes. It is also very important to adopt a perspective not only for the individual but also for the couple. If you treat a man with testosterone, after 3 months, he will be in great shape. However, if the couple has long been accustomed to having a limited sexual life, if the woman is not supported on her side, the couple will be unbalanced. The couple is concerned with managing the hormonal changes of both.
Question: Sexual medicine is essential, yet it seems inaccessible.
Dr. Burté: There are very few specialists in sexual medicine because there is no legal provision for it. These consultations are lengthy but not valued. Who wants to work for that?
If there was reimbursement for sexual medicine consultations at age 15 years, at menopause, and for men around the age of 50 years, it would change mentalities. Sexual medicine must be integrated into medicine. It should also be noted that not all sexologists are physicians.
Some people are very well trained through universities, and others are not. Ideally, someone with a sexual disorder should first have a sexual medicine consultation to understand the situation. Then, the physician can refer the patient to a competent sexologist because we work in a network.
Dr. Burté has no conflicts of interest related to the subject.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
From adolescence onward, the need for sexual health is particularly important. Yet, information and healthcare services are limited, which often leaves patients in distress and subject to misconceptions. What are the specific issues related to sexuality in adolescence, middle age, and beyond? This news organization interviewed Carol Burté, MD, a specialist in sexual medicine from Monaco.
Question: Regarding young individuals, what about sex education in schools?
Dr. Burté: The French law of 2018 specifies that at least three annual sessions must be devoted to sex education in elementary school, middle school, and high school.
In practice, this is not always the case, and interventions are very focused on prevention and rules. Sexuality is almost always absent from the program. Sexuality means: What does it mean to have desire? How does pleasure work? At what age do we have sex? etc. Young people receive prevention advice, but the link with sexuality is not made.
Sexuality remains taboo. You know, like in books: “They got married and had many children ...” End of the story, we don’t know more [laughs].
Question: And outside the school setting, do doctors sufficiently address sexual health issues with adolescents?
Dr. Burté: Rarely. I understand that a general practitioner has little time, but they can still ask the young person if they have any questions. They can refer them to someone or provide reading recommendations. Regarding sex education on the Internet, there are many well-made websites, such as the one by the national education system.
Also, it is important to give young people lifestyle advice to combat overweight, sedentary behavior, etc., by explaining to them that these factors can lead to sexual disorders later as well as infertility.
Another very important point: There is an inequality between boys and girls, but this time, to the disadvantage of boys. We have a sexual health consultation dedicated to young girls for the pill, but no one examines the boys. However, testicular cancer or undescended testicles can occur. I think we really need to change things and establish a clinical examination for boys in adolescence.
Question: More and more young people identify as asexual. What do you think of this?
Dr. Burté: People who identify as asexual represent about 1% of the population. These are individuals who are not attracted to having sexual relationships with someone. This does not prevent them from having a boyfriend, a girlfriend, masturbating, etc. It is sexual intercourse that does not interest them. These young people often say they have done it all. They have seen a lot of images, viewed sexuality as gymnastics with all the positions, tricks. They are jaded. Also, when you are faced with an image that provides a very strong and rapid stimulation, human relationships seem much more difficult because, obviously, you will never reproduce that sensation when you are with your partner with whom you must connect. The relationship is no longer emotional and shared. Yet, sexuality is emotional, relational, intellectual.
I think people go through phases. At a certain point, they feel asexual, but they can change their minds and think differently if they have real encounters, encounters that are increasingly difficult. Today, we are witnessing a loss of confidence. Young people, but also others, want to protect themselves from everything, especially from falling in love, not get back into a relationship because it is constraining.
Question: Data show that young people are exposed to pornography at an increasingly early age. Is this a problem for their future sexuality?
Dr. Burté: The exposure to pornography at an early age, around 11 years old, has only been a reality for the past decade. It is too early to say how it will impact their sexuality. When examining the literature on this subject, some publications indicate that the consequences can be dramatic for children. Others show that children can distinguish between reality and fantasy.
Whenever I see young people in consultation, I ask them whether they feel pornography has helped or hindered them, whether it is the cause of the issue they are facing. I would say that, other than those who have viewed pornography under duress, which is of the order of violence, pornography does not seem to pose a problem. It can even provide certain knowledge.
Question: What about sexual violence in children? What are the consequences?
Dr. Burté: In sexual medicine, this is one of the questions we ask systematically because it is very common. It is important to keep in mind that this not only affects girls; boys are also sexually abused. The consequences are dramatic in terms of psychosexual development. Each case is different.
Question: At the other end of life, is it “normal” to have sexual disorders at a certain age? Should we resign ourselves?
Dr. Burté: When it comes to sexuality, people have many misconceptions and beliefs that are conveyed through media and the Internet. One of them is to believe that because we are aging, we cannot have a proper sexuality. Sexuality slows down with age, as all sensitivities decrease, but desire is something present throughout life. Yet, seniors are rarely questioned about their sexual health by the media.
Note that older people in institutions face an additional obstacle: lack of privacy. Is this normal? Sexuality releases endorphins, oxytocin, it is well-being that costs nothing. It is something that should be prescribed!
Question: Chronic diseases, disabilities with incidence increases with age — are they not inevitable obstacles to a fulfilling sexuality?
Dr. Burté: It is possible to have a sexual life regardless of the disease one has, cancer, diabetes, rheumatic disease — regardless of the disability.
A collaboration with the National Cancer Institute on the preservation of sexual health after cancer in which I participated shows that people are extremely demanding of care and that this care is still very insufficient, unfortunately, even in the case of prostate cancer, for example, when it should be obvious.
Question: But aging itself brings challenges in terms of sexuality.
Dr. Burté: Yes, in men, the consequences of low testosterone levels are well known. Therefore, we must stop thinking that men do not have their “menopause.” Men often have a testosterone deficiency after a certain age. This is very annoying because they have many symptoms that are truly unpleasant and yet can be corrected by completely reliable treatments.
Men are very misinformed on this subject. We talk about gender inequality, but in this area, a young woman who has her first period knows very well that one day she will go through menopause, but a boy has no idea that one day he will have hormone problems.
Question: Therefore, is it important to question men past the age of 50 years?
Dr. Burté: Yes. Faced with sexual symptoms or simply fatigue, or among those who are a bit depressed, investigating a testosterone deficiency should be part of the reflexes.
Also, if you ask a man in general, “How is it going from a sexual point of view,” and he answers that everything is going well, this means he has good arteries, good veins, a good nervous system, sufficient hormones, and psychologically, everything is going rather well. Conversely, erectile dysfunction can be one of the first symptoms of cardiovascular pathologies.
After a certain age, there is no test that provides as much information about people’s health as this question about sexual health.
Question: On their side, are women better cared for at menopause?
Dr. Burté: Yes, but women still lack explanations. I work in sexual medicine, and in my consultation, I see women who come simply to get information about menopause.
Women must know that menopause is a turning point in life because they will spend 30%-40% of their lives without hormones.
It is important to explain that indeed, after menopause, without treatment, it is not the same. There are genital and urinary, psychological, sexual, and skin consequences. It is important to provide true data on the influence of hormonal treatments. Today, hormone fear is not over. I think we need to rehabilitate treatments, care for women.
Question: So we must not forget men or women.
Dr. Burté: Yes. It is also very important to adopt a perspective not only for the individual but also for the couple. If you treat a man with testosterone, after 3 months, he will be in great shape. However, if the couple has long been accustomed to having a limited sexual life, if the woman is not supported on her side, the couple will be unbalanced. The couple is concerned with managing the hormonal changes of both.
Question: Sexual medicine is essential, yet it seems inaccessible.
Dr. Burté: There are very few specialists in sexual medicine because there is no legal provision for it. These consultations are lengthy but not valued. Who wants to work for that?
If there was reimbursement for sexual medicine consultations at age 15 years, at menopause, and for men around the age of 50 years, it would change mentalities. Sexual medicine must be integrated into medicine. It should also be noted that not all sexologists are physicians.
Some people are very well trained through universities, and others are not. Ideally, someone with a sexual disorder should first have a sexual medicine consultation to understand the situation. Then, the physician can refer the patient to a competent sexologist because we work in a network.
Dr. Burté has no conflicts of interest related to the subject.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
Primary Care: Try These Steps to Boost Lung Cancer Screens
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.