User login
Hospitals poised to launch first COVID-19 vaccines in clinicians
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
United States adds nearly 74,000 more children with COVID-19
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
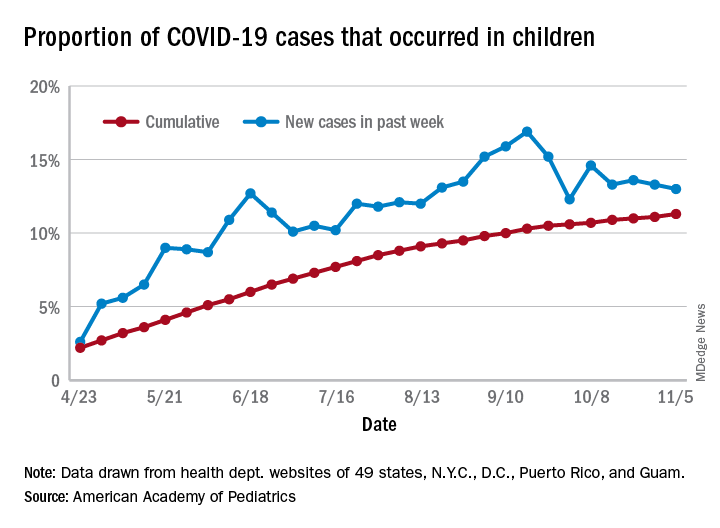
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
No link shown between thyroid dysfunction and heart failure
Thyroid dysfunction had virtually no independent impact on survival in a retrospective study of nearly 5,000 English patients with chronic heart failure, adding to evidence that subclinical thyroid disorders in these patients requires no special management beyond ongoing monitoring.

“Although thyroid dysfunction is related to outcome in patients with chronic heart failure, the association disappears when adjustment is made for established prognostic variables, such as age, NT-proBNP [N-terminal of the prohormone brain natriuretic peptide], and [New York Heart Association] class,” wrote Nathan A. Samuel, MBChB, and coauthors in the American Journal of Cardiology.
Results from several earlier studies had shown evidence for reduced survival in heart failure patients with thyroid dysfunction, but in analyses that did not adjust for heart failure severity, such as a 2013 report that used data from the Sudden Cardiac Death in Heart Failure Trial SCD-HeFT. Other studies that adjusted for heart failure severity based on serum level of natriuretic peptides did not show significant associations between thyroid function and mortality, and when those results couple with the new report they together minimize the immediate risk from subclinical thyroid dysfunction faced by heart failure patients, wrote the authors of the new report.
Don’t treat subclinical thyroid dysfunction
“Our results suggest that subclinical thyroid disease has little impact on outcomes, and that we should not treat subclinical hypothyroidism in the expectation of improving outlook,” said Andrew L. Clark, MD, senior author on the new report and professor and head of the department of academic cardiology at Hull (England) York Medical School.
“Both hyper-and hypothyroidism can cause heart failure, so thyroid function should always be checked in patients when they present with heart failure. A small proportion of patients have heart failure that is potentially reversible” with thyroid-directed treatment, Dr. Clark said in an interview.
But “subclinical disease should probably not be treated, although we have not conducted a clinical trial that proves this assertion. We speculate, based on our findings, that such a trial is unlikely to be positive.”
Patients with subclinical thyroid disorders, particularly subclinical hypothyroidism, “need to be followed and treated should they develop clinical disease,” he maintained. “Except in extreme circumstances, such as the handful of patients who might have gross myxedema and may be near coma, thyroid replacement therapy for those [with heart failure] who have clinical hypothyroidism should follow standard lines.”
It is important to monitor thyroid function,” agreed Dr. Samuel, a researcher in the department of academic cardiology at Hull York Medical School. “We found that thyroxine use was most common among patients with hyperthyroidism, suggesting that they were previously hypothyroid and had received inappropriate treatment.”
Confounder adjustment mitigates the thyroid link
The new analysis used data collected from 6,782 consecutive heart failure patients enrolled during 2000-2018 at a community heart failure clinic that serves patients in the region of Hull, England. The researchers identified 4,992 of these patients with confirmed heart failure and adequate data for their analyses, including 2,997 (60%) with heart failure with reduced ejection fraction (HFrEF) and 1,995 (40%) with heart failure with normal ejection fraction (HFnEF, the term used by the authors but often called heart failure with preserved ejection fraction).
Thyroid hormone levels showed that 90% of these patients were euthyroid, 6% were hyperthyroid, and 4% were hypothyroid, rates consistent with prior reports for both the general population and heart failure patients. Only 12 patients (0.2%) had overt hypothyroidism, and fewer that 1% (about 45 patients) had overt hyperthyroidism. Patients averaged about 73 years of age, and during a median 4.6 years of follow-up 58% died.
Both the hypo- and hyperthyroid patients showed significantly higher mortality rates than euthyroid patients in a univariate analysis. But the patients with thyroid dysfunction also had more comorbidities, more severe heart failure symptoms measured by NYHA functional class, and more severe heart failure measured as higher serum levels of NT-proBNP.
In a multivariate analysis that adjusted for these factors, the significant differences disappeared among the entire group of heart failure patients for the outcomes of all-cause mortality, and mortality or hospitalization with heart failure. The multivariate analysis also showed no significant association between higher levels of thyroid-stimulating hormone (TSH) and all-cause death or death plus heart failure hospitalization among the patients with HFrEF.
Among patients with HFnEF, the multivariate adjusted analysis showed a small increase in both mortality and mortality plus hospitalization for heart failure, a 2% rise for each of these two endpoints for each 1 mIU/L increase in TSH, the authors reported. Although the P value for each of these two significant differences among patients with HFnEF was .02, the 95% confidence interval included 1.00 and ranged from 1.00 to 1.04.
The multivariate analysis identified three variables with the strongest associations with all-cause mortality: older age, higher levels of NT-proBNP, and higher NYHA class indicating greater functional impairment.
The results support the hypothesis that “worsening heart failure can lead to down-regulation of thyroid hormone signaling,” the authors suggested. Their study is also “the first to examine the prognostic significance of thyroid dysfunction in a large population of patients with HFnEF.” This analysis showed a “weak but significant association between increasing TSH and both mortality and the composite endpoint in patients with HFnEF.”
“HFnEF is a heterogeneous group of conditions that are difficult to diagnose in many cases. Therefore, future studies are needed to provide further clarity on the effect of thyroid dysfunction in these patients,” Dr. Samuel said.
The study received no commercial funding. Dr. Samuel and Dr. Clark had no disclosures.
SOURCE: Samuel NA et al. Am J Cardiol. 2020 Oct 24. doi: 10.1016/j.amjcard.2020.10.034.
Thyroid dysfunction had virtually no independent impact on survival in a retrospective study of nearly 5,000 English patients with chronic heart failure, adding to evidence that subclinical thyroid disorders in these patients requires no special management beyond ongoing monitoring.
“Although thyroid dysfunction is related to outcome in patients with chronic heart failure, the association disappears when adjustment is made for established prognostic variables, such as age, NT-proBNP [N-terminal of the prohormone brain natriuretic peptide], and [New York Heart Association] class,” wrote Nathan A. Samuel, MBChB, and coauthors in the American Journal of Cardiology.
Results from several earlier studies had shown evidence for reduced survival in heart failure patients with thyroid dysfunction, but in analyses that did not adjust for heart failure severity, such as a 2013 report that used data from the Sudden Cardiac Death in Heart Failure Trial SCD-HeFT. Other studies that adjusted for heart failure severity based on serum level of natriuretic peptides did not show significant associations between thyroid function and mortality, and when those results couple with the new report they together minimize the immediate risk from subclinical thyroid dysfunction faced by heart failure patients, wrote the authors of the new report.
Don’t treat subclinical thyroid dysfunction
“Our results suggest that subclinical thyroid disease has little impact on outcomes, and that we should not treat subclinical hypothyroidism in the expectation of improving outlook,” said Andrew L. Clark, MD, senior author on the new report and professor and head of the department of academic cardiology at Hull (England) York Medical School.
“Both hyper-and hypothyroidism can cause heart failure, so thyroid function should always be checked in patients when they present with heart failure. A small proportion of patients have heart failure that is potentially reversible” with thyroid-directed treatment, Dr. Clark said in an interview.
But “subclinical disease should probably not be treated, although we have not conducted a clinical trial that proves this assertion. We speculate, based on our findings, that such a trial is unlikely to be positive.”
Patients with subclinical thyroid disorders, particularly subclinical hypothyroidism, “need to be followed and treated should they develop clinical disease,” he maintained. “Except in extreme circumstances, such as the handful of patients who might have gross myxedema and may be near coma, thyroid replacement therapy for those [with heart failure] who have clinical hypothyroidism should follow standard lines.”
It is important to monitor thyroid function,” agreed Dr. Samuel, a researcher in the department of academic cardiology at Hull York Medical School. “We found that thyroxine use was most common among patients with hyperthyroidism, suggesting that they were previously hypothyroid and had received inappropriate treatment.”
Confounder adjustment mitigates the thyroid link
The new analysis used data collected from 6,782 consecutive heart failure patients enrolled during 2000-2018 at a community heart failure clinic that serves patients in the region of Hull, England. The researchers identified 4,992 of these patients with confirmed heart failure and adequate data for their analyses, including 2,997 (60%) with heart failure with reduced ejection fraction (HFrEF) and 1,995 (40%) with heart failure with normal ejection fraction (HFnEF, the term used by the authors but often called heart failure with preserved ejection fraction).
Thyroid hormone levels showed that 90% of these patients were euthyroid, 6% were hyperthyroid, and 4% were hypothyroid, rates consistent with prior reports for both the general population and heart failure patients. Only 12 patients (0.2%) had overt hypothyroidism, and fewer that 1% (about 45 patients) had overt hyperthyroidism. Patients averaged about 73 years of age, and during a median 4.6 years of follow-up 58% died.
Both the hypo- and hyperthyroid patients showed significantly higher mortality rates than euthyroid patients in a univariate analysis. But the patients with thyroid dysfunction also had more comorbidities, more severe heart failure symptoms measured by NYHA functional class, and more severe heart failure measured as higher serum levels of NT-proBNP.
In a multivariate analysis that adjusted for these factors, the significant differences disappeared among the entire group of heart failure patients for the outcomes of all-cause mortality, and mortality or hospitalization with heart failure. The multivariate analysis also showed no significant association between higher levels of thyroid-stimulating hormone (TSH) and all-cause death or death plus heart failure hospitalization among the patients with HFrEF.
Among patients with HFnEF, the multivariate adjusted analysis showed a small increase in both mortality and mortality plus hospitalization for heart failure, a 2% rise for each of these two endpoints for each 1 mIU/L increase in TSH, the authors reported. Although the P value for each of these two significant differences among patients with HFnEF was .02, the 95% confidence interval included 1.00 and ranged from 1.00 to 1.04.
The multivariate analysis identified three variables with the strongest associations with all-cause mortality: older age, higher levels of NT-proBNP, and higher NYHA class indicating greater functional impairment.
The results support the hypothesis that “worsening heart failure can lead to down-regulation of thyroid hormone signaling,” the authors suggested. Their study is also “the first to examine the prognostic significance of thyroid dysfunction in a large population of patients with HFnEF.” This analysis showed a “weak but significant association between increasing TSH and both mortality and the composite endpoint in patients with HFnEF.”
“HFnEF is a heterogeneous group of conditions that are difficult to diagnose in many cases. Therefore, future studies are needed to provide further clarity on the effect of thyroid dysfunction in these patients,” Dr. Samuel said.
The study received no commercial funding. Dr. Samuel and Dr. Clark had no disclosures.
SOURCE: Samuel NA et al. Am J Cardiol. 2020 Oct 24. doi: 10.1016/j.amjcard.2020.10.034.
Thyroid dysfunction had virtually no independent impact on survival in a retrospective study of nearly 5,000 English patients with chronic heart failure, adding to evidence that subclinical thyroid disorders in these patients requires no special management beyond ongoing monitoring.
“Although thyroid dysfunction is related to outcome in patients with chronic heart failure, the association disappears when adjustment is made for established prognostic variables, such as age, NT-proBNP [N-terminal of the prohormone brain natriuretic peptide], and [New York Heart Association] class,” wrote Nathan A. Samuel, MBChB, and coauthors in the American Journal of Cardiology.
Results from several earlier studies had shown evidence for reduced survival in heart failure patients with thyroid dysfunction, but in analyses that did not adjust for heart failure severity, such as a 2013 report that used data from the Sudden Cardiac Death in Heart Failure Trial SCD-HeFT. Other studies that adjusted for heart failure severity based on serum level of natriuretic peptides did not show significant associations between thyroid function and mortality, and when those results couple with the new report they together minimize the immediate risk from subclinical thyroid dysfunction faced by heart failure patients, wrote the authors of the new report.
Don’t treat subclinical thyroid dysfunction
“Our results suggest that subclinical thyroid disease has little impact on outcomes, and that we should not treat subclinical hypothyroidism in the expectation of improving outlook,” said Andrew L. Clark, MD, senior author on the new report and professor and head of the department of academic cardiology at Hull (England) York Medical School.
“Both hyper-and hypothyroidism can cause heart failure, so thyroid function should always be checked in patients when they present with heart failure. A small proportion of patients have heart failure that is potentially reversible” with thyroid-directed treatment, Dr. Clark said in an interview.
But “subclinical disease should probably not be treated, although we have not conducted a clinical trial that proves this assertion. We speculate, based on our findings, that such a trial is unlikely to be positive.”
Patients with subclinical thyroid disorders, particularly subclinical hypothyroidism, “need to be followed and treated should they develop clinical disease,” he maintained. “Except in extreme circumstances, such as the handful of patients who might have gross myxedema and may be near coma, thyroid replacement therapy for those [with heart failure] who have clinical hypothyroidism should follow standard lines.”
It is important to monitor thyroid function,” agreed Dr. Samuel, a researcher in the department of academic cardiology at Hull York Medical School. “We found that thyroxine use was most common among patients with hyperthyroidism, suggesting that they were previously hypothyroid and had received inappropriate treatment.”
Confounder adjustment mitigates the thyroid link
The new analysis used data collected from 6,782 consecutive heart failure patients enrolled during 2000-2018 at a community heart failure clinic that serves patients in the region of Hull, England. The researchers identified 4,992 of these patients with confirmed heart failure and adequate data for their analyses, including 2,997 (60%) with heart failure with reduced ejection fraction (HFrEF) and 1,995 (40%) with heart failure with normal ejection fraction (HFnEF, the term used by the authors but often called heart failure with preserved ejection fraction).
Thyroid hormone levels showed that 90% of these patients were euthyroid, 6% were hyperthyroid, and 4% were hypothyroid, rates consistent with prior reports for both the general population and heart failure patients. Only 12 patients (0.2%) had overt hypothyroidism, and fewer that 1% (about 45 patients) had overt hyperthyroidism. Patients averaged about 73 years of age, and during a median 4.6 years of follow-up 58% died.
Both the hypo- and hyperthyroid patients showed significantly higher mortality rates than euthyroid patients in a univariate analysis. But the patients with thyroid dysfunction also had more comorbidities, more severe heart failure symptoms measured by NYHA functional class, and more severe heart failure measured as higher serum levels of NT-proBNP.
In a multivariate analysis that adjusted for these factors, the significant differences disappeared among the entire group of heart failure patients for the outcomes of all-cause mortality, and mortality or hospitalization with heart failure. The multivariate analysis also showed no significant association between higher levels of thyroid-stimulating hormone (TSH) and all-cause death or death plus heart failure hospitalization among the patients with HFrEF.
Among patients with HFnEF, the multivariate adjusted analysis showed a small increase in both mortality and mortality plus hospitalization for heart failure, a 2% rise for each of these two endpoints for each 1 mIU/L increase in TSH, the authors reported. Although the P value for each of these two significant differences among patients with HFnEF was .02, the 95% confidence interval included 1.00 and ranged from 1.00 to 1.04.
The multivariate analysis identified three variables with the strongest associations with all-cause mortality: older age, higher levels of NT-proBNP, and higher NYHA class indicating greater functional impairment.
The results support the hypothesis that “worsening heart failure can lead to down-regulation of thyroid hormone signaling,” the authors suggested. Their study is also “the first to examine the prognostic significance of thyroid dysfunction in a large population of patients with HFnEF.” This analysis showed a “weak but significant association between increasing TSH and both mortality and the composite endpoint in patients with HFnEF.”
“HFnEF is a heterogeneous group of conditions that are difficult to diagnose in many cases. Therefore, future studies are needed to provide further clarity on the effect of thyroid dysfunction in these patients,” Dr. Samuel said.
The study received no commercial funding. Dr. Samuel and Dr. Clark had no disclosures.
SOURCE: Samuel NA et al. Am J Cardiol. 2020 Oct 24. doi: 10.1016/j.amjcard.2020.10.034.
FROM THE AMERICAN JOURNAL OF CARDIOLOGY
Whales, seals, and dolphins: Will SARS-CoV-2–contaminated wastewater prove a killer?
Zoonoses are no respecter of biological boundaries and are notorious for crossing genus and even higher taxonomic boundaries. SARS-CoV-2 is no exception, the current outbreak most probably having originated in bats, a common source of human-affecting zoonoses throughout history. But it is not a one-way street, and the virus has been shown to spread from infected humans to a variety of other land mammals, including our domesticated animals and kept zoo species.
A recent troubling report, however, has indicated that sea mammals may be part of a next wave of likely candidates for infection, put at risk by the current human pandemic and environmental degradation on a global scale, according to a the results of a genomic analysis of four major groups of sea mammals.
Researchers Sabateeshan Mathavarajah and colleagues from Dalhousie University, Halifax, N.S., examined the sequences of the ACE2 receptors in the various marine mammal species. The ACE2 receptor has recently been identified as the SARS-CoV-2 receptor, which allows for infection.
The researchers examined genomic databases of the marine species to determine if their ACE2 receptor sequences indicated the potential for high, medium, or low susceptibility to infection, as reported in Science of the Total Environment. Database analysis was performed for four groups: Cetacea (whales and dolphins), Pinnepidia (seals), Sirenia (sea cows), and Fissipedia (sea otters and polar bears).
The researchers defined susceptibility values based on comparable binding with the receptor and came up with the following subgroups: higher than human, high (resembles human ACE2), medium (resembles cat ACE2), and low (resembles dog ACE2). It has yet to be established if these marine mammals actually are infected with SARS-CoV-2 and what the impact of such an infection might have on animal health or humans who come in contact with infected animals.
They also cross-referenced for the level of species endangerment and with maps of potential wastewater contamination for certain areas that species came in contact with, using Alaska as the model.
Populations in danger
The researchers found 15 species that are already at risk globally that fall under the categories of near threatened, vulnerable, endangered, and critically endangered that were predicted to be medium to higher susceptibility to the SARS-CoV-2 virus than humans. Cross infection is of particular concern because other coronaviruses have been shown to have severe and lethal effects among many of these species.
Among the potentially impacted species were the near threatened–status Antarctic Mink whale and the stellar sea lion; the vulnerable sperm whale, northern fur seal, and Atlantic walrus; the endangered northern and southern sea otters, the North Pacific right whale, and the Amazon River dolphin; and the critically threatened Baiji and Vaquita dolphin species.
Pollution risks
In Alaska, as of Aug. 7th, 2020, there were 4,221 confirmed cases of COVID-19 and this number continues to rise, according to the researchers. Since there is a diversity of marine mammals in Alaska and their populations are well documented, they compared this information with available data on the wastewater treatment plants in the state. They were thus able to determine the potential geographic locations and species at high risk for transmission of SARS-CoV-2 via wastewater effluent.
Among their findings, the city of Cold Bay discharges wastewater into Cold Bay, where there are Northern sea otter populations that are predicted to be highly susceptible to the virus. Beluga whales are also predicted to have high susceptibility and they can be found in Bristol Bay near Naknek, a city which relies only on lagoon treatment prior to the discharge of wastewater effluent; the city of Dillingham discharges wastewater into the Nushagak River where beluga whales are found. In Palmer, wastewater effluent flows into the Talkeetna River, which is a tributary to the Susitna River and home to two species predicted to have high susceptibility, beluga whales and harbor seals, the authors added.
Based on these results, the researchers predicted that there was likely a significant risk to sea mammals across the globe, especially where less-adequate treatment facilities and high population densities may lead to greater wastewater contamination.
“Given the proximity of marine animals to high-risk environments where viral spill over is likely, we must act with foresight to protect marine mammal species predicted to be at risk and mitigate the environmental impact of the COVID-19 pandemic,” the researchers concluded.
The authors reported that they had no disclosures.
SOURCE: Mathavarajah S et al. Sci Total Environ. 2020 Oct 29. doi: 10.1016/j.scitotenv.2020.143346.
Zoonoses are no respecter of biological boundaries and are notorious for crossing genus and even higher taxonomic boundaries. SARS-CoV-2 is no exception, the current outbreak most probably having originated in bats, a common source of human-affecting zoonoses throughout history. But it is not a one-way street, and the virus has been shown to spread from infected humans to a variety of other land mammals, including our domesticated animals and kept zoo species.
A recent troubling report, however, has indicated that sea mammals may be part of a next wave of likely candidates for infection, put at risk by the current human pandemic and environmental degradation on a global scale, according to a the results of a genomic analysis of four major groups of sea mammals.
Researchers Sabateeshan Mathavarajah and colleagues from Dalhousie University, Halifax, N.S., examined the sequences of the ACE2 receptors in the various marine mammal species. The ACE2 receptor has recently been identified as the SARS-CoV-2 receptor, which allows for infection.
The researchers examined genomic databases of the marine species to determine if their ACE2 receptor sequences indicated the potential for high, medium, or low susceptibility to infection, as reported in Science of the Total Environment. Database analysis was performed for four groups: Cetacea (whales and dolphins), Pinnepidia (seals), Sirenia (sea cows), and Fissipedia (sea otters and polar bears).
The researchers defined susceptibility values based on comparable binding with the receptor and came up with the following subgroups: higher than human, high (resembles human ACE2), medium (resembles cat ACE2), and low (resembles dog ACE2). It has yet to be established if these marine mammals actually are infected with SARS-CoV-2 and what the impact of such an infection might have on animal health or humans who come in contact with infected animals.
They also cross-referenced for the level of species endangerment and with maps of potential wastewater contamination for certain areas that species came in contact with, using Alaska as the model.
Populations in danger
The researchers found 15 species that are already at risk globally that fall under the categories of near threatened, vulnerable, endangered, and critically endangered that were predicted to be medium to higher susceptibility to the SARS-CoV-2 virus than humans. Cross infection is of particular concern because other coronaviruses have been shown to have severe and lethal effects among many of these species.
Among the potentially impacted species were the near threatened–status Antarctic Mink whale and the stellar sea lion; the vulnerable sperm whale, northern fur seal, and Atlantic walrus; the endangered northern and southern sea otters, the North Pacific right whale, and the Amazon River dolphin; and the critically threatened Baiji and Vaquita dolphin species.
Pollution risks
In Alaska, as of Aug. 7th, 2020, there were 4,221 confirmed cases of COVID-19 and this number continues to rise, according to the researchers. Since there is a diversity of marine mammals in Alaska and their populations are well documented, they compared this information with available data on the wastewater treatment plants in the state. They were thus able to determine the potential geographic locations and species at high risk for transmission of SARS-CoV-2 via wastewater effluent.
Among their findings, the city of Cold Bay discharges wastewater into Cold Bay, where there are Northern sea otter populations that are predicted to be highly susceptible to the virus. Beluga whales are also predicted to have high susceptibility and they can be found in Bristol Bay near Naknek, a city which relies only on lagoon treatment prior to the discharge of wastewater effluent; the city of Dillingham discharges wastewater into the Nushagak River where beluga whales are found. In Palmer, wastewater effluent flows into the Talkeetna River, which is a tributary to the Susitna River and home to two species predicted to have high susceptibility, beluga whales and harbor seals, the authors added.
Based on these results, the researchers predicted that there was likely a significant risk to sea mammals across the globe, especially where less-adequate treatment facilities and high population densities may lead to greater wastewater contamination.
“Given the proximity of marine animals to high-risk environments where viral spill over is likely, we must act with foresight to protect marine mammal species predicted to be at risk and mitigate the environmental impact of the COVID-19 pandemic,” the researchers concluded.
The authors reported that they had no disclosures.
SOURCE: Mathavarajah S et al. Sci Total Environ. 2020 Oct 29. doi: 10.1016/j.scitotenv.2020.143346.
Zoonoses are no respecter of biological boundaries and are notorious for crossing genus and even higher taxonomic boundaries. SARS-CoV-2 is no exception, the current outbreak most probably having originated in bats, a common source of human-affecting zoonoses throughout history. But it is not a one-way street, and the virus has been shown to spread from infected humans to a variety of other land mammals, including our domesticated animals and kept zoo species.
A recent troubling report, however, has indicated that sea mammals may be part of a next wave of likely candidates for infection, put at risk by the current human pandemic and environmental degradation on a global scale, according to a the results of a genomic analysis of four major groups of sea mammals.
Researchers Sabateeshan Mathavarajah and colleagues from Dalhousie University, Halifax, N.S., examined the sequences of the ACE2 receptors in the various marine mammal species. The ACE2 receptor has recently been identified as the SARS-CoV-2 receptor, which allows for infection.
The researchers examined genomic databases of the marine species to determine if their ACE2 receptor sequences indicated the potential for high, medium, or low susceptibility to infection, as reported in Science of the Total Environment. Database analysis was performed for four groups: Cetacea (whales and dolphins), Pinnepidia (seals), Sirenia (sea cows), and Fissipedia (sea otters and polar bears).
The researchers defined susceptibility values based on comparable binding with the receptor and came up with the following subgroups: higher than human, high (resembles human ACE2), medium (resembles cat ACE2), and low (resembles dog ACE2). It has yet to be established if these marine mammals actually are infected with SARS-CoV-2 and what the impact of such an infection might have on animal health or humans who come in contact with infected animals.
They also cross-referenced for the level of species endangerment and with maps of potential wastewater contamination for certain areas that species came in contact with, using Alaska as the model.
Populations in danger
The researchers found 15 species that are already at risk globally that fall under the categories of near threatened, vulnerable, endangered, and critically endangered that were predicted to be medium to higher susceptibility to the SARS-CoV-2 virus than humans. Cross infection is of particular concern because other coronaviruses have been shown to have severe and lethal effects among many of these species.
Among the potentially impacted species were the near threatened–status Antarctic Mink whale and the stellar sea lion; the vulnerable sperm whale, northern fur seal, and Atlantic walrus; the endangered northern and southern sea otters, the North Pacific right whale, and the Amazon River dolphin; and the critically threatened Baiji and Vaquita dolphin species.
Pollution risks
In Alaska, as of Aug. 7th, 2020, there were 4,221 confirmed cases of COVID-19 and this number continues to rise, according to the researchers. Since there is a diversity of marine mammals in Alaska and their populations are well documented, they compared this information with available data on the wastewater treatment plants in the state. They were thus able to determine the potential geographic locations and species at high risk for transmission of SARS-CoV-2 via wastewater effluent.
Among their findings, the city of Cold Bay discharges wastewater into Cold Bay, where there are Northern sea otter populations that are predicted to be highly susceptible to the virus. Beluga whales are also predicted to have high susceptibility and they can be found in Bristol Bay near Naknek, a city which relies only on lagoon treatment prior to the discharge of wastewater effluent; the city of Dillingham discharges wastewater into the Nushagak River where beluga whales are found. In Palmer, wastewater effluent flows into the Talkeetna River, which is a tributary to the Susitna River and home to two species predicted to have high susceptibility, beluga whales and harbor seals, the authors added.
Based on these results, the researchers predicted that there was likely a significant risk to sea mammals across the globe, especially where less-adequate treatment facilities and high population densities may lead to greater wastewater contamination.
“Given the proximity of marine animals to high-risk environments where viral spill over is likely, we must act with foresight to protect marine mammal species predicted to be at risk and mitigate the environmental impact of the COVID-19 pandemic,” the researchers concluded.
The authors reported that they had no disclosures.
SOURCE: Mathavarajah S et al. Sci Total Environ. 2020 Oct 29. doi: 10.1016/j.scitotenv.2020.143346.
FROM SCIENCE OF THE TOTAL ENVIRONMENT
Pfizer vaccine data show 90% efficacy in early results
A vaccine candidate against SARS-CoV-2 has been found to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus, results from an interim analysis of a phase 3 study demonstrated.
BTN162b2, a messenger RNA–based vaccine candidate that requires two doses, is being developed by Pfizer and BioNTech SE independently of the Trump administration’s Operation Warp Speed. A global phase 3 clinical trial of BTN162b2 began on July 27 and has enrolled 43,538 participants to date; 42% of enrollees have racially and ethnically diverse backgrounds.
According to a press release issued by the two companies, 38,955 trial volunteers had received a second dose of either vaccine or placebo as of Nov. 8. An interim analysis of 94 individuals conducted by an independent data monitoring committee (DMC) found that the vaccine efficacy rate was above 90% 7 days after the second dose. This means that protection was achieved 28 days after the first vaccine dose.
“It’s promising in that it validates the genetic strategy – whether it’s mRNA vaccines or DNA vaccines,” Paul A. Offit, MD, told Medscape Medical News. Offit is a member of the US Food and Drug Administraiton’s COVID-19 Vaccine Advisory Committee. “All of them have the same approach, which is that they introduce the gene that codes for the coronavirus spike protein into the cell. Your cell makes the spike protein, and your immune system makes antibodies to the spike protein. At least in these preliminary data, which involved 94 people getting sick, it looks like it’s effective. That’s good. We knew that it seemed to work in experimental animals, but you never know until you put it into people.”
According to Pfizer and BioNTech SE, a final data analysis is planned once 164 confirmed COVID-19 cases have accrued. So far, the DMC has not reported any serious safety concerns. It recommends that the study continue to collect safety and efficacy data as planned. The companies plan to apply to the FDA for emergency use authorization soon after the required safety milestone is achieved.
Pfizer CEO Albert Bourla, DVM, PhD, added in a separate press release, “It’s important to note that we cannot apply for FDA Emergency Use Authorization based on these efficacy results alone. More data on safety is also needed, and we are continuing to accumulate that safety data as part of our ongoing clinical study.
“We estimate that a median of two months of safety data following the second and final dose of the vaccine candidate – required by FDA’s guidance for potential Emergency Use Authorization – will be available by the third week of November.”
Offit, professor of pediatrics in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, said that, if BTN162b2 is approved, administering it will be tricky. “This particular vaccine has to be shipped and stored at –70° C or –80° C, which we’ve never done before in this country,” he said. “That means maintaining the product on dry ice. That’s going to be a challenge for distribution, I think.”
Good news, but…
In the press release, BioNTech SE’s cofounder and CEO, Ugur Sahin, MD, characterized the findings as “a victory for innovation, science and a global collaborative effort. When we embarked on this journey 10 months ago this is what we aspired to achieve. Especially today, while we are all in the midst of a second wave and many of us in lockdown, we appreciate even more how important this milestone is on our path towards ending this pandemic and for all of us to regain a sense of normality.”
President-elect Joe Biden also weighed in, calling the results “excellent news” in a news release.
“At the same time, it is also important to understand that the end of the battle against COVID-19 is still months away,” he said. “This news follows a previously announced timeline by industry officials that forecast vaccine approval by late November. Even if that is achieved, and some Americans are vaccinated later this year, it will be many more months before there is widespread vaccination in this country.
“Today’s news does not change this urgent reality. Americans will have to rely on masking, distancing, contact tracing, hand washing, and other measures to keep themselves safe well into next year,” Biden added.
This article first appeared on Medscape.com.
A vaccine candidate against SARS-CoV-2 has been found to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus, results from an interim analysis of a phase 3 study demonstrated.
BTN162b2, a messenger RNA–based vaccine candidate that requires two doses, is being developed by Pfizer and BioNTech SE independently of the Trump administration’s Operation Warp Speed. A global phase 3 clinical trial of BTN162b2 began on July 27 and has enrolled 43,538 participants to date; 42% of enrollees have racially and ethnically diverse backgrounds.
According to a press release issued by the two companies, 38,955 trial volunteers had received a second dose of either vaccine or placebo as of Nov. 8. An interim analysis of 94 individuals conducted by an independent data monitoring committee (DMC) found that the vaccine efficacy rate was above 90% 7 days after the second dose. This means that protection was achieved 28 days after the first vaccine dose.
“It’s promising in that it validates the genetic strategy – whether it’s mRNA vaccines or DNA vaccines,” Paul A. Offit, MD, told Medscape Medical News. Offit is a member of the US Food and Drug Administraiton’s COVID-19 Vaccine Advisory Committee. “All of them have the same approach, which is that they introduce the gene that codes for the coronavirus spike protein into the cell. Your cell makes the spike protein, and your immune system makes antibodies to the spike protein. At least in these preliminary data, which involved 94 people getting sick, it looks like it’s effective. That’s good. We knew that it seemed to work in experimental animals, but you never know until you put it into people.”
According to Pfizer and BioNTech SE, a final data analysis is planned once 164 confirmed COVID-19 cases have accrued. So far, the DMC has not reported any serious safety concerns. It recommends that the study continue to collect safety and efficacy data as planned. The companies plan to apply to the FDA for emergency use authorization soon after the required safety milestone is achieved.
Pfizer CEO Albert Bourla, DVM, PhD, added in a separate press release, “It’s important to note that we cannot apply for FDA Emergency Use Authorization based on these efficacy results alone. More data on safety is also needed, and we are continuing to accumulate that safety data as part of our ongoing clinical study.
“We estimate that a median of two months of safety data following the second and final dose of the vaccine candidate – required by FDA’s guidance for potential Emergency Use Authorization – will be available by the third week of November.”
Offit, professor of pediatrics in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, said that, if BTN162b2 is approved, administering it will be tricky. “This particular vaccine has to be shipped and stored at –70° C or –80° C, which we’ve never done before in this country,” he said. “That means maintaining the product on dry ice. That’s going to be a challenge for distribution, I think.”
Good news, but…
In the press release, BioNTech SE’s cofounder and CEO, Ugur Sahin, MD, characterized the findings as “a victory for innovation, science and a global collaborative effort. When we embarked on this journey 10 months ago this is what we aspired to achieve. Especially today, while we are all in the midst of a second wave and many of us in lockdown, we appreciate even more how important this milestone is on our path towards ending this pandemic and for all of us to regain a sense of normality.”
President-elect Joe Biden also weighed in, calling the results “excellent news” in a news release.
“At the same time, it is also important to understand that the end of the battle against COVID-19 is still months away,” he said. “This news follows a previously announced timeline by industry officials that forecast vaccine approval by late November. Even if that is achieved, and some Americans are vaccinated later this year, it will be many more months before there is widespread vaccination in this country.
“Today’s news does not change this urgent reality. Americans will have to rely on masking, distancing, contact tracing, hand washing, and other measures to keep themselves safe well into next year,” Biden added.
This article first appeared on Medscape.com.
A vaccine candidate against SARS-CoV-2 has been found to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus, results from an interim analysis of a phase 3 study demonstrated.
BTN162b2, a messenger RNA–based vaccine candidate that requires two doses, is being developed by Pfizer and BioNTech SE independently of the Trump administration’s Operation Warp Speed. A global phase 3 clinical trial of BTN162b2 began on July 27 and has enrolled 43,538 participants to date; 42% of enrollees have racially and ethnically diverse backgrounds.
According to a press release issued by the two companies, 38,955 trial volunteers had received a second dose of either vaccine or placebo as of Nov. 8. An interim analysis of 94 individuals conducted by an independent data monitoring committee (DMC) found that the vaccine efficacy rate was above 90% 7 days after the second dose. This means that protection was achieved 28 days after the first vaccine dose.
“It’s promising in that it validates the genetic strategy – whether it’s mRNA vaccines or DNA vaccines,” Paul A. Offit, MD, told Medscape Medical News. Offit is a member of the US Food and Drug Administraiton’s COVID-19 Vaccine Advisory Committee. “All of them have the same approach, which is that they introduce the gene that codes for the coronavirus spike protein into the cell. Your cell makes the spike protein, and your immune system makes antibodies to the spike protein. At least in these preliminary data, which involved 94 people getting sick, it looks like it’s effective. That’s good. We knew that it seemed to work in experimental animals, but you never know until you put it into people.”
According to Pfizer and BioNTech SE, a final data analysis is planned once 164 confirmed COVID-19 cases have accrued. So far, the DMC has not reported any serious safety concerns. It recommends that the study continue to collect safety and efficacy data as planned. The companies plan to apply to the FDA for emergency use authorization soon after the required safety milestone is achieved.
Pfizer CEO Albert Bourla, DVM, PhD, added in a separate press release, “It’s important to note that we cannot apply for FDA Emergency Use Authorization based on these efficacy results alone. More data on safety is also needed, and we are continuing to accumulate that safety data as part of our ongoing clinical study.
“We estimate that a median of two months of safety data following the second and final dose of the vaccine candidate – required by FDA’s guidance for potential Emergency Use Authorization – will be available by the third week of November.”
Offit, professor of pediatrics in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, said that, if BTN162b2 is approved, administering it will be tricky. “This particular vaccine has to be shipped and stored at –70° C or –80° C, which we’ve never done before in this country,” he said. “That means maintaining the product on dry ice. That’s going to be a challenge for distribution, I think.”
Good news, but…
In the press release, BioNTech SE’s cofounder and CEO, Ugur Sahin, MD, characterized the findings as “a victory for innovation, science and a global collaborative effort. When we embarked on this journey 10 months ago this is what we aspired to achieve. Especially today, while we are all in the midst of a second wave and many of us in lockdown, we appreciate even more how important this milestone is on our path towards ending this pandemic and for all of us to regain a sense of normality.”
President-elect Joe Biden also weighed in, calling the results “excellent news” in a news release.
“At the same time, it is also important to understand that the end of the battle against COVID-19 is still months away,” he said. “This news follows a previously announced timeline by industry officials that forecast vaccine approval by late November. Even if that is achieved, and some Americans are vaccinated later this year, it will be many more months before there is widespread vaccination in this country.
“Today’s news does not change this urgent reality. Americans will have to rely on masking, distancing, contact tracing, hand washing, and other measures to keep themselves safe well into next year,” Biden added.
This article first appeared on Medscape.com.
VA joins Pentagon in recruiting volunteers for COVID vaccine trials
according to officials with the VA and Operation Warp Speed, the Trump administration’s initiative to fast-track a coronavirus vaccine.
The largely unpublicized effort follows a Department of Defense announcement in September that it has partnered with AstraZeneca to recruit volunteers at five of its medical facilities, which are separate from the VA system. DOD is also is in talks with developers of other vaccine candidates, although officials won’t say which ones.
Both federal departments have long experience in medical research and diverse populations – a crucial component of effective clinical trials, said J. Stephen Morrison, senior vice president and director of global health policy at the Center for Strategic and International Studies, a bipartisan think tank in Washington.
Since active troops are essential to national security, and veterans are extremely vulnerable to COVID-19, both departments have a vested interest in supporting the development of safe, effective vaccines, Mr. Morrison said.
“On the DOD active servicemen and -women side, it’s a question of making sure they’re ready, they are protected,” Mr. Morrison said. “With VA, their population, all elderly and infirm with underlying conditions, they could really be suffering if we don’t get a vaccine.”
According to a VA website, of its 20 medical centers involved, 17 would be part of the Johnson & Johnson vaccine trial, while the three others are recruiting – or have completed recruitment – for advanced-stage trials for Moderna, AstraZeneca, and Pfizer vaccines.
Matthew Hepburn, MD, head of vaccine development at Operation Warp Speed, said the VA effort lets veterans contribute to the overall well-being of the country.
“This is another way they can continue to serve in this way, fighting the pandemic as a volunteer,” Dr. Hepburn said during a discussion of vaccine and therapeutics development hosted by the Heritage Foundation on Oct. 27.
It’s not unusual for the military to participate in multicenter trials for treatments of ailments as diverse as cancer and trauma. Historically, many vaccines have been tested first by the military.
In the general population, clinicians often have difficulty recruiting African Americans and other minorities for medical research, and “the military provides a rich opportunity to find volunteers for those groups,” said retired Rear Adm. Thomas Cullison, MD, a doctor and former deputy surgeon general for the Navy.
Military health facilities are held to the same standards as private research facilities, he said.
No service members will be required to participate in the COVID vaccine trials. All volunteers will be paid by the developer.
Support for routine vaccinations runs high in the military, but some have expressed concerns about new vaccines and mandatory inoculations, especially for anthrax. In a 2002 federal study, 85% of those who received that vaccine reported an adverse reaction, with just under half noticing minor redness at the injection site. But nearly a quarter of the side effects reported were more systemic, including fevers, chills, fatigue and joint pain.
That survey of a small group of National Guard and Reserve members found that, while 73% said they believe immunizations are effective, two-thirds said they did not support the mandatory anthrax program, and 6 in 10 said they were not satisfied with the information they were given on the vaccines.
To quell concerns over the military’s role in supporting COVID vaccine development, the Pentagon has reiterated that troops or their dependents interested in participating in the research must provide voluntary written consent, and they will be allowed to take part only if they will be in the same location for the length of the research, expected to last at least 2 years.
In addition, active-duty members such as new recruits and boot camp participants will not be allowed to volunteer because they are “considered vulnerable from an ethical and regulatory standpoint,” an official said.
At the VA, officials are seeking to recruit healthy veterans aged 18-65 years old who are not pregnant and may be at risk for exposure. As with trials conducted in civilian facilities, participants will be paid by the developer, VA spokesperson Christina Noel said.
Also, VA nurses and caseworkers also are being asked to identify their sickest, highest-risk patients to determine who should be at the top of the list once a vaccine is approved, according to a VA nurse and other health officials who asked not to be identified because they were not authorized to speak with the press.
The U.S. military has a long history of contributing to research on vaccines, including a key role in developing inoculations against yellow fever and adenovirus, and the Walter Reed Army Institute of Research is developing its own vaccine against the coronavirus.
Some segments of the population remain skeptical of federal medical experiments. A survey by AP-NORC in May found that Black people are particularly reluctant to get the coronavirus vaccine. Many have concerns about federal research in part because of associations with the infamous Tuskegee Institute syphilis experiments, in which U.S. Public Health Service officials intentionally withheld a cure from Black men infected with the disease.
But Mr. Morrison, of the Center for Strategic and International Studies, said the Defense Department and VA are a “natural fit” for the COVID vaccine trials.
“DOD has lots of expertise. They know how to vaccinate; they know how to reach communities. They have a whole science infrastructure and research-and-development infrastructure. And when you are thinking what the mission of VA is, [VA] sees this is part of their mission,” Mr. Morrison said.
The Defense Department announced its agreement with AstraZeneca in September, shortly before the drugmaker’s vaccine trial was put on hold to study a serious medical condition that one participant reported. That research was approved by the Food and Drug Administration to begin again Oct. 23. The military plans to restart its efforts to recruit 3,000 volunteers.
The Pentagon has also signed an agreement with another vaccine developer, the head of the Defense Health Agency, Army Lt. Gen. Ronald Place, told reporters Oct. 8. He wouldn’t provide the company’s name.
Senator Elizabeth Warren (D-Mass.) and Senator Mazie Hirono (D-Hawaii) have called, unsuccessfully, for the Senate Armed Services Committee to investigate what they say is a lack of Pentagon transparency on its role in vaccine development and distribution. The Defense Department has awarded more than $6 billion in Operation Warp Speed contracts through an intermediary, Advanced Technology International, and the two senators want more information about those contracts.
“There may well be a valuable role for DoD officials in [Operation Warp Speed] – particularly given the department’s logistical capacity,” they wrote to the committee chair and ranking member. “But it is important that Congress conduct appropriate oversight of, and understand, DoD’s activities in this area.”
Neither department has disclosed the financial arrangements they have made with developers to support the vaccine research.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
according to officials with the VA and Operation Warp Speed, the Trump administration’s initiative to fast-track a coronavirus vaccine.
The largely unpublicized effort follows a Department of Defense announcement in September that it has partnered with AstraZeneca to recruit volunteers at five of its medical facilities, which are separate from the VA system. DOD is also is in talks with developers of other vaccine candidates, although officials won’t say which ones.
Both federal departments have long experience in medical research and diverse populations – a crucial component of effective clinical trials, said J. Stephen Morrison, senior vice president and director of global health policy at the Center for Strategic and International Studies, a bipartisan think tank in Washington.
Since active troops are essential to national security, and veterans are extremely vulnerable to COVID-19, both departments have a vested interest in supporting the development of safe, effective vaccines, Mr. Morrison said.
“On the DOD active servicemen and -women side, it’s a question of making sure they’re ready, they are protected,” Mr. Morrison said. “With VA, their population, all elderly and infirm with underlying conditions, they could really be suffering if we don’t get a vaccine.”
According to a VA website, of its 20 medical centers involved, 17 would be part of the Johnson & Johnson vaccine trial, while the three others are recruiting – or have completed recruitment – for advanced-stage trials for Moderna, AstraZeneca, and Pfizer vaccines.
Matthew Hepburn, MD, head of vaccine development at Operation Warp Speed, said the VA effort lets veterans contribute to the overall well-being of the country.
“This is another way they can continue to serve in this way, fighting the pandemic as a volunteer,” Dr. Hepburn said during a discussion of vaccine and therapeutics development hosted by the Heritage Foundation on Oct. 27.
It’s not unusual for the military to participate in multicenter trials for treatments of ailments as diverse as cancer and trauma. Historically, many vaccines have been tested first by the military.
In the general population, clinicians often have difficulty recruiting African Americans and other minorities for medical research, and “the military provides a rich opportunity to find volunteers for those groups,” said retired Rear Adm. Thomas Cullison, MD, a doctor and former deputy surgeon general for the Navy.
Military health facilities are held to the same standards as private research facilities, he said.
No service members will be required to participate in the COVID vaccine trials. All volunteers will be paid by the developer.
Support for routine vaccinations runs high in the military, but some have expressed concerns about new vaccines and mandatory inoculations, especially for anthrax. In a 2002 federal study, 85% of those who received that vaccine reported an adverse reaction, with just under half noticing minor redness at the injection site. But nearly a quarter of the side effects reported were more systemic, including fevers, chills, fatigue and joint pain.
That survey of a small group of National Guard and Reserve members found that, while 73% said they believe immunizations are effective, two-thirds said they did not support the mandatory anthrax program, and 6 in 10 said they were not satisfied with the information they were given on the vaccines.
To quell concerns over the military’s role in supporting COVID vaccine development, the Pentagon has reiterated that troops or their dependents interested in participating in the research must provide voluntary written consent, and they will be allowed to take part only if they will be in the same location for the length of the research, expected to last at least 2 years.
In addition, active-duty members such as new recruits and boot camp participants will not be allowed to volunteer because they are “considered vulnerable from an ethical and regulatory standpoint,” an official said.
At the VA, officials are seeking to recruit healthy veterans aged 18-65 years old who are not pregnant and may be at risk for exposure. As with trials conducted in civilian facilities, participants will be paid by the developer, VA spokesperson Christina Noel said.
Also, VA nurses and caseworkers also are being asked to identify their sickest, highest-risk patients to determine who should be at the top of the list once a vaccine is approved, according to a VA nurse and other health officials who asked not to be identified because they were not authorized to speak with the press.
The U.S. military has a long history of contributing to research on vaccines, including a key role in developing inoculations against yellow fever and adenovirus, and the Walter Reed Army Institute of Research is developing its own vaccine against the coronavirus.
Some segments of the population remain skeptical of federal medical experiments. A survey by AP-NORC in May found that Black people are particularly reluctant to get the coronavirus vaccine. Many have concerns about federal research in part because of associations with the infamous Tuskegee Institute syphilis experiments, in which U.S. Public Health Service officials intentionally withheld a cure from Black men infected with the disease.
But Mr. Morrison, of the Center for Strategic and International Studies, said the Defense Department and VA are a “natural fit” for the COVID vaccine trials.
“DOD has lots of expertise. They know how to vaccinate; they know how to reach communities. They have a whole science infrastructure and research-and-development infrastructure. And when you are thinking what the mission of VA is, [VA] sees this is part of their mission,” Mr. Morrison said.
The Defense Department announced its agreement with AstraZeneca in September, shortly before the drugmaker’s vaccine trial was put on hold to study a serious medical condition that one participant reported. That research was approved by the Food and Drug Administration to begin again Oct. 23. The military plans to restart its efforts to recruit 3,000 volunteers.
The Pentagon has also signed an agreement with another vaccine developer, the head of the Defense Health Agency, Army Lt. Gen. Ronald Place, told reporters Oct. 8. He wouldn’t provide the company’s name.
Senator Elizabeth Warren (D-Mass.) and Senator Mazie Hirono (D-Hawaii) have called, unsuccessfully, for the Senate Armed Services Committee to investigate what they say is a lack of Pentagon transparency on its role in vaccine development and distribution. The Defense Department has awarded more than $6 billion in Operation Warp Speed contracts through an intermediary, Advanced Technology International, and the two senators want more information about those contracts.
“There may well be a valuable role for DoD officials in [Operation Warp Speed] – particularly given the department’s logistical capacity,” they wrote to the committee chair and ranking member. “But it is important that Congress conduct appropriate oversight of, and understand, DoD’s activities in this area.”
Neither department has disclosed the financial arrangements they have made with developers to support the vaccine research.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
according to officials with the VA and Operation Warp Speed, the Trump administration’s initiative to fast-track a coronavirus vaccine.
The largely unpublicized effort follows a Department of Defense announcement in September that it has partnered with AstraZeneca to recruit volunteers at five of its medical facilities, which are separate from the VA system. DOD is also is in talks with developers of other vaccine candidates, although officials won’t say which ones.
Both federal departments have long experience in medical research and diverse populations – a crucial component of effective clinical trials, said J. Stephen Morrison, senior vice president and director of global health policy at the Center for Strategic and International Studies, a bipartisan think tank in Washington.
Since active troops are essential to national security, and veterans are extremely vulnerable to COVID-19, both departments have a vested interest in supporting the development of safe, effective vaccines, Mr. Morrison said.
“On the DOD active servicemen and -women side, it’s a question of making sure they’re ready, they are protected,” Mr. Morrison said. “With VA, their population, all elderly and infirm with underlying conditions, they could really be suffering if we don’t get a vaccine.”
According to a VA website, of its 20 medical centers involved, 17 would be part of the Johnson & Johnson vaccine trial, while the three others are recruiting – or have completed recruitment – for advanced-stage trials for Moderna, AstraZeneca, and Pfizer vaccines.
Matthew Hepburn, MD, head of vaccine development at Operation Warp Speed, said the VA effort lets veterans contribute to the overall well-being of the country.
“This is another way they can continue to serve in this way, fighting the pandemic as a volunteer,” Dr. Hepburn said during a discussion of vaccine and therapeutics development hosted by the Heritage Foundation on Oct. 27.
It’s not unusual for the military to participate in multicenter trials for treatments of ailments as diverse as cancer and trauma. Historically, many vaccines have been tested first by the military.
In the general population, clinicians often have difficulty recruiting African Americans and other minorities for medical research, and “the military provides a rich opportunity to find volunteers for those groups,” said retired Rear Adm. Thomas Cullison, MD, a doctor and former deputy surgeon general for the Navy.
Military health facilities are held to the same standards as private research facilities, he said.
No service members will be required to participate in the COVID vaccine trials. All volunteers will be paid by the developer.
Support for routine vaccinations runs high in the military, but some have expressed concerns about new vaccines and mandatory inoculations, especially for anthrax. In a 2002 federal study, 85% of those who received that vaccine reported an adverse reaction, with just under half noticing minor redness at the injection site. But nearly a quarter of the side effects reported were more systemic, including fevers, chills, fatigue and joint pain.
That survey of a small group of National Guard and Reserve members found that, while 73% said they believe immunizations are effective, two-thirds said they did not support the mandatory anthrax program, and 6 in 10 said they were not satisfied with the information they were given on the vaccines.
To quell concerns over the military’s role in supporting COVID vaccine development, the Pentagon has reiterated that troops or their dependents interested in participating in the research must provide voluntary written consent, and they will be allowed to take part only if they will be in the same location for the length of the research, expected to last at least 2 years.
In addition, active-duty members such as new recruits and boot camp participants will not be allowed to volunteer because they are “considered vulnerable from an ethical and regulatory standpoint,” an official said.
At the VA, officials are seeking to recruit healthy veterans aged 18-65 years old who are not pregnant and may be at risk for exposure. As with trials conducted in civilian facilities, participants will be paid by the developer, VA spokesperson Christina Noel said.
Also, VA nurses and caseworkers also are being asked to identify their sickest, highest-risk patients to determine who should be at the top of the list once a vaccine is approved, according to a VA nurse and other health officials who asked not to be identified because they were not authorized to speak with the press.
The U.S. military has a long history of contributing to research on vaccines, including a key role in developing inoculations against yellow fever and adenovirus, and the Walter Reed Army Institute of Research is developing its own vaccine against the coronavirus.
Some segments of the population remain skeptical of federal medical experiments. A survey by AP-NORC in May found that Black people are particularly reluctant to get the coronavirus vaccine. Many have concerns about federal research in part because of associations with the infamous Tuskegee Institute syphilis experiments, in which U.S. Public Health Service officials intentionally withheld a cure from Black men infected with the disease.
But Mr. Morrison, of the Center for Strategic and International Studies, said the Defense Department and VA are a “natural fit” for the COVID vaccine trials.
“DOD has lots of expertise. They know how to vaccinate; they know how to reach communities. They have a whole science infrastructure and research-and-development infrastructure. And when you are thinking what the mission of VA is, [VA] sees this is part of their mission,” Mr. Morrison said.
The Defense Department announced its agreement with AstraZeneca in September, shortly before the drugmaker’s vaccine trial was put on hold to study a serious medical condition that one participant reported. That research was approved by the Food and Drug Administration to begin again Oct. 23. The military plans to restart its efforts to recruit 3,000 volunteers.
The Pentagon has also signed an agreement with another vaccine developer, the head of the Defense Health Agency, Army Lt. Gen. Ronald Place, told reporters Oct. 8. He wouldn’t provide the company’s name.
Senator Elizabeth Warren (D-Mass.) and Senator Mazie Hirono (D-Hawaii) have called, unsuccessfully, for the Senate Armed Services Committee to investigate what they say is a lack of Pentagon transparency on its role in vaccine development and distribution. The Defense Department has awarded more than $6 billion in Operation Warp Speed contracts through an intermediary, Advanced Technology International, and the two senators want more information about those contracts.
“There may well be a valuable role for DoD officials in [Operation Warp Speed] – particularly given the department’s logistical capacity,” they wrote to the committee chair and ranking member. “But it is important that Congress conduct appropriate oversight of, and understand, DoD’s activities in this area.”
Neither department has disclosed the financial arrangements they have made with developers to support the vaccine research.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Higher cardiovascular risks in Kawasaki disease persist 10-plus years
Risks are highest in first year.
Survivors of Kawasaki disease remain at a higher long-term risk for cardiovascular events into young adulthood, including myocardial infarction, compared to people without the disease, new evidence reveals. The elevated risks emerged in survivors both with and without cardiovascular involvement at the time of initial diagnosis.

Overall risk of cardiovascular events was highest in the first year following Kawasaki disease diagnosis, and about 10 times greater than in healthy children, Cal Robinson, MD, said during a press conference at the virtual annual meeting of the American College of Rheumatology.
“The risk gradually decreased over time. However, even 10 years after diagnosis of their illness, they still had a 39% higher risk,” said study author Dr. Robinson, a PGY4 pediatric nephrology fellow at The Hospital for Sick Children in Toronto.
Dr. Robinson also put the numbers in perspective. “We fully acknowledged these are very rare events in children, especially healthy children, which is why we needed such a large cohort to study this. Interpret the numbers cautiously.”
In terms of patient and family counseling, “I would say children with Kawasaki disease have a higher risk of myocardial infarction, but the absolute risk is still low,” he added. For example, 16 Kawasaki disease survivors experienced a heart attack during follow-up, or 0.4% of the affected study population, compared to a rate of 0.1% among matched controls.
“These families are often very frightened after the initial Kawasaki disease diagnosis,” Dr. Robinson said. “We have to balance some discussion with what we know about Kawasaki disease without overly scaring or terrifying these families, who are already anxious.”
To quantify the incidence and timing of cardiovascular events and cardiac disease following diagnosis, Dr. Robinson and colleagues assessed large databases representing approximately 3 million children. They focused on children hospitalized with a Kawasaki disease diagnosis between 1995 and 2018. These children had a median length of stay of 3 days and 2.5% were admitted to critical care. The investigators matched his population 1:100 to unaffected children in Ontario.
Follow-up was up to 24 years (median, 11 years) in this retrospective, population-based cohort study.
Risks raised over a decade and beyond
Compared to matched controls, Kawasaki disease survivors had a higher risk for a cardiac event in the first year following diagnosis (adjusted hazard ratio, 11.65; 95% confidence interval, 10.34-13.13). The 1- to 5-year risk was lower (aHR, 3.35), a trend that continued between 5 and 10 years (aHR, 1.87) and as well as after more than 10 years (aHR, 1.39).
The risk of major adverse cardiac events (MACE, a composite of myocardial infarction, stroke, or cardiovascular death) was likewise highest in the first year after diagnosis (aHR, 3.27), followed by a 51% greater risk at 1-5 years, a 113% increased risk at 5-10 years, and a 17% elevated risk after 10 years.
The investigators compared the 144 Kawasaki disease survivors who experienced a coronary artery aneurysm (CAA) within 90 days of hospital admission to the 4,453 others who did not have a CAA. The risk for a composite cardiovascular event was elevated at each time point among those with a history of CAA, especially in the first year. The adjusted HR was 33.12 in the CAA group versus 10.44 in the non-CAA group.
“The most interesting finding of this study was that children with Kawasaki syndrome are at higher risk for composite cardiovascular events and major adverse cardiac events even if they were not diagnosed with coronary artery aneurysm,” session comoderator Shervin Assassi, MD, professor of medicine and director of division of rheumatology at the University of Texas Health Science Center at Houston, said when asked to comment.
Dr. Robinson and colleagues also looked at outcomes based on presence or absence of coronary involvement at the time of Kawasaki disease diagnosis. For example, among those with initial coronary involvement, 15% later experienced a cardiovascular event and 10% experienced a major cardiovascular event.
“However, we were specifically interested in looking at children without initial coronary involvement. In this group, we also found these children were at increased risk for cardiovascular events compared to children without Kawasaki disease,” Dr. Robinson said. He said the distinction is important because approximately 95% of children diagnosed with Kawasaki disease do not feature initial coronary involvement.
In terms of clinical care, “our data provides an early signal that Kawasaki disease survivors – including those without initial coronary involvement – may be at higher risk of cardiovascular events into early adulthood.”
A call for closer monitoring
“Based on our results, we find that Kawasaki disease survivors may benefit from additional follow-up and surveillance for cardiovascular disease risk factors, such as obesity, high blood pressure, and high cholesterol,” Dr. Robinson said. Early identification of heightened risk could allow physicians to more closely monitor this subgroup and emphasize potentially beneficial lifestyle modifications, including increasing physical activity, implementing a heart healthy diet, and avoiding smoking.
Mortality was not significantly different between groups. “Despite the risk of cardiac events we found, death was uncommon,” Dr. Robinson said. Among children with Kawasaki disease, 1 in 500 died during follow-up, so “the risk of death was actually lower than for children without Kawasaki disease.”
Similar findings of lower mortality have been reported in research out of Japan, he added during a plenary presentation at ACR 2020. Future research is warranted to evaluate this finding further, Dr. Robinson said.
Future plans
Going forward, the investigators plan to evaluate noncardiovascular outcomes in this patient population. They would also like to examine health care utilization following a diagnosis of Kawasaki disease “to better understand what kind of follow-up is happening now in Ontario,” Dr. Robinson said.
Another unanswered question is whether the cardiovascular events observed in the study stem from atherosclerotic disease or a different mechanism among survivors of Kawasaki disease.
The research was supported by a McMaster University Resident Research Grant, a Hamilton Health Sciences New Investigator Award, and Ontario’s Institute for Clinical Evaluative Sciences. Dr. Robinson had no relevant financial disclosures.
SOURCE: Robinson C et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0937.
Risks are highest in first year.
Risks are highest in first year.
Survivors of Kawasaki disease remain at a higher long-term risk for cardiovascular events into young adulthood, including myocardial infarction, compared to people without the disease, new evidence reveals. The elevated risks emerged in survivors both with and without cardiovascular involvement at the time of initial diagnosis.
Overall risk of cardiovascular events was highest in the first year following Kawasaki disease diagnosis, and about 10 times greater than in healthy children, Cal Robinson, MD, said during a press conference at the virtual annual meeting of the American College of Rheumatology.
“The risk gradually decreased over time. However, even 10 years after diagnosis of their illness, they still had a 39% higher risk,” said study author Dr. Robinson, a PGY4 pediatric nephrology fellow at The Hospital for Sick Children in Toronto.
Dr. Robinson also put the numbers in perspective. “We fully acknowledged these are very rare events in children, especially healthy children, which is why we needed such a large cohort to study this. Interpret the numbers cautiously.”
In terms of patient and family counseling, “I would say children with Kawasaki disease have a higher risk of myocardial infarction, but the absolute risk is still low,” he added. For example, 16 Kawasaki disease survivors experienced a heart attack during follow-up, or 0.4% of the affected study population, compared to a rate of 0.1% among matched controls.
“These families are often very frightened after the initial Kawasaki disease diagnosis,” Dr. Robinson said. “We have to balance some discussion with what we know about Kawasaki disease without overly scaring or terrifying these families, who are already anxious.”
To quantify the incidence and timing of cardiovascular events and cardiac disease following diagnosis, Dr. Robinson and colleagues assessed large databases representing approximately 3 million children. They focused on children hospitalized with a Kawasaki disease diagnosis between 1995 and 2018. These children had a median length of stay of 3 days and 2.5% were admitted to critical care. The investigators matched his population 1:100 to unaffected children in Ontario.
Follow-up was up to 24 years (median, 11 years) in this retrospective, population-based cohort study.
Risks raised over a decade and beyond
Compared to matched controls, Kawasaki disease survivors had a higher risk for a cardiac event in the first year following diagnosis (adjusted hazard ratio, 11.65; 95% confidence interval, 10.34-13.13). The 1- to 5-year risk was lower (aHR, 3.35), a trend that continued between 5 and 10 years (aHR, 1.87) and as well as after more than 10 years (aHR, 1.39).
The risk of major adverse cardiac events (MACE, a composite of myocardial infarction, stroke, or cardiovascular death) was likewise highest in the first year after diagnosis (aHR, 3.27), followed by a 51% greater risk at 1-5 years, a 113% increased risk at 5-10 years, and a 17% elevated risk after 10 years.
The investigators compared the 144 Kawasaki disease survivors who experienced a coronary artery aneurysm (CAA) within 90 days of hospital admission to the 4,453 others who did not have a CAA. The risk for a composite cardiovascular event was elevated at each time point among those with a history of CAA, especially in the first year. The adjusted HR was 33.12 in the CAA group versus 10.44 in the non-CAA group.
“The most interesting finding of this study was that children with Kawasaki syndrome are at higher risk for composite cardiovascular events and major adverse cardiac events even if they were not diagnosed with coronary artery aneurysm,” session comoderator Shervin Assassi, MD, professor of medicine and director of division of rheumatology at the University of Texas Health Science Center at Houston, said when asked to comment.
Dr. Robinson and colleagues also looked at outcomes based on presence or absence of coronary involvement at the time of Kawasaki disease diagnosis. For example, among those with initial coronary involvement, 15% later experienced a cardiovascular event and 10% experienced a major cardiovascular event.
“However, we were specifically interested in looking at children without initial coronary involvement. In this group, we also found these children were at increased risk for cardiovascular events compared to children without Kawasaki disease,” Dr. Robinson said. He said the distinction is important because approximately 95% of children diagnosed with Kawasaki disease do not feature initial coronary involvement.
In terms of clinical care, “our data provides an early signal that Kawasaki disease survivors – including those without initial coronary involvement – may be at higher risk of cardiovascular events into early adulthood.”
A call for closer monitoring
“Based on our results, we find that Kawasaki disease survivors may benefit from additional follow-up and surveillance for cardiovascular disease risk factors, such as obesity, high blood pressure, and high cholesterol,” Dr. Robinson said. Early identification of heightened risk could allow physicians to more closely monitor this subgroup and emphasize potentially beneficial lifestyle modifications, including increasing physical activity, implementing a heart healthy diet, and avoiding smoking.
Mortality was not significantly different between groups. “Despite the risk of cardiac events we found, death was uncommon,” Dr. Robinson said. Among children with Kawasaki disease, 1 in 500 died during follow-up, so “the risk of death was actually lower than for children without Kawasaki disease.”
Similar findings of lower mortality have been reported in research out of Japan, he added during a plenary presentation at ACR 2020. Future research is warranted to evaluate this finding further, Dr. Robinson said.
Future plans
Going forward, the investigators plan to evaluate noncardiovascular outcomes in this patient population. They would also like to examine health care utilization following a diagnosis of Kawasaki disease “to better understand what kind of follow-up is happening now in Ontario,” Dr. Robinson said.
Another unanswered question is whether the cardiovascular events observed in the study stem from atherosclerotic disease or a different mechanism among survivors of Kawasaki disease.
The research was supported by a McMaster University Resident Research Grant, a Hamilton Health Sciences New Investigator Award, and Ontario’s Institute for Clinical Evaluative Sciences. Dr. Robinson had no relevant financial disclosures.
SOURCE: Robinson C et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0937.
Survivors of Kawasaki disease remain at a higher long-term risk for cardiovascular events into young adulthood, including myocardial infarction, compared to people without the disease, new evidence reveals. The elevated risks emerged in survivors both with and without cardiovascular involvement at the time of initial diagnosis.
Overall risk of cardiovascular events was highest in the first year following Kawasaki disease diagnosis, and about 10 times greater than in healthy children, Cal Robinson, MD, said during a press conference at the virtual annual meeting of the American College of Rheumatology.
“The risk gradually decreased over time. However, even 10 years after diagnosis of their illness, they still had a 39% higher risk,” said study author Dr. Robinson, a PGY4 pediatric nephrology fellow at The Hospital for Sick Children in Toronto.
Dr. Robinson also put the numbers in perspective. “We fully acknowledged these are very rare events in children, especially healthy children, which is why we needed such a large cohort to study this. Interpret the numbers cautiously.”
In terms of patient and family counseling, “I would say children with Kawasaki disease have a higher risk of myocardial infarction, but the absolute risk is still low,” he added. For example, 16 Kawasaki disease survivors experienced a heart attack during follow-up, or 0.4% of the affected study population, compared to a rate of 0.1% among matched controls.
“These families are often very frightened after the initial Kawasaki disease diagnosis,” Dr. Robinson said. “We have to balance some discussion with what we know about Kawasaki disease without overly scaring or terrifying these families, who are already anxious.”
To quantify the incidence and timing of cardiovascular events and cardiac disease following diagnosis, Dr. Robinson and colleagues assessed large databases representing approximately 3 million children. They focused on children hospitalized with a Kawasaki disease diagnosis between 1995 and 2018. These children had a median length of stay of 3 days and 2.5% were admitted to critical care. The investigators matched his population 1:100 to unaffected children in Ontario.
Follow-up was up to 24 years (median, 11 years) in this retrospective, population-based cohort study.
Risks raised over a decade and beyond
Compared to matched controls, Kawasaki disease survivors had a higher risk for a cardiac event in the first year following diagnosis (adjusted hazard ratio, 11.65; 95% confidence interval, 10.34-13.13). The 1- to 5-year risk was lower (aHR, 3.35), a trend that continued between 5 and 10 years (aHR, 1.87) and as well as after more than 10 years (aHR, 1.39).
The risk of major adverse cardiac events (MACE, a composite of myocardial infarction, stroke, or cardiovascular death) was likewise highest in the first year after diagnosis (aHR, 3.27), followed by a 51% greater risk at 1-5 years, a 113% increased risk at 5-10 years, and a 17% elevated risk after 10 years.
The investigators compared the 144 Kawasaki disease survivors who experienced a coronary artery aneurysm (CAA) within 90 days of hospital admission to the 4,453 others who did not have a CAA. The risk for a composite cardiovascular event was elevated at each time point among those with a history of CAA, especially in the first year. The adjusted HR was 33.12 in the CAA group versus 10.44 in the non-CAA group.
“The most interesting finding of this study was that children with Kawasaki syndrome are at higher risk for composite cardiovascular events and major adverse cardiac events even if they were not diagnosed with coronary artery aneurysm,” session comoderator Shervin Assassi, MD, professor of medicine and director of division of rheumatology at the University of Texas Health Science Center at Houston, said when asked to comment.
Dr. Robinson and colleagues also looked at outcomes based on presence or absence of coronary involvement at the time of Kawasaki disease diagnosis. For example, among those with initial coronary involvement, 15% later experienced a cardiovascular event and 10% experienced a major cardiovascular event.
“However, we were specifically interested in looking at children without initial coronary involvement. In this group, we also found these children were at increased risk for cardiovascular events compared to children without Kawasaki disease,” Dr. Robinson said. He said the distinction is important because approximately 95% of children diagnosed with Kawasaki disease do not feature initial coronary involvement.
In terms of clinical care, “our data provides an early signal that Kawasaki disease survivors – including those without initial coronary involvement – may be at higher risk of cardiovascular events into early adulthood.”
A call for closer monitoring
“Based on our results, we find that Kawasaki disease survivors may benefit from additional follow-up and surveillance for cardiovascular disease risk factors, such as obesity, high blood pressure, and high cholesterol,” Dr. Robinson said. Early identification of heightened risk could allow physicians to more closely monitor this subgroup and emphasize potentially beneficial lifestyle modifications, including increasing physical activity, implementing a heart healthy diet, and avoiding smoking.
Mortality was not significantly different between groups. “Despite the risk of cardiac events we found, death was uncommon,” Dr. Robinson said. Among children with Kawasaki disease, 1 in 500 died during follow-up, so “the risk of death was actually lower than for children without Kawasaki disease.”
Similar findings of lower mortality have been reported in research out of Japan, he added during a plenary presentation at ACR 2020. Future research is warranted to evaluate this finding further, Dr. Robinson said.
Future plans
Going forward, the investigators plan to evaluate noncardiovascular outcomes in this patient population. They would also like to examine health care utilization following a diagnosis of Kawasaki disease “to better understand what kind of follow-up is happening now in Ontario,” Dr. Robinson said.
Another unanswered question is whether the cardiovascular events observed in the study stem from atherosclerotic disease or a different mechanism among survivors of Kawasaki disease.
The research was supported by a McMaster University Resident Research Grant, a Hamilton Health Sciences New Investigator Award, and Ontario’s Institute for Clinical Evaluative Sciences. Dr. Robinson had no relevant financial disclosures.
SOURCE: Robinson C et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0937.
FROM ACR 2020
Key clinical point: Kawasaki disease survivors remain at elevated long-term risk for cardiovascular events.
Major finding: Overall cardiovascular event risk was 39% higher, even after 10 years.
Study details: A retrospective, population-based cohort study of more than 4,597 Kawasaki disease survivors and 459,700 matched children without Kawasaki disease.
Disclosures: The research was supported by a McMaster University Resident Research Grant, a Hamilton Health Sciences New Investigator Award, and Ontario’s Institute for Clinical Evaluative Sciences. Dr. Robinson had no relevant financial disclosures.
Source: Robinson C et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0937.
COVID-19 risks in rheumatic disease remain unclear
ACR 2020 studies offer conflicting findings.
Among people with COVID-19, those with systemic autoimmune rheumatic diseases had an elevated 30-day risk of hospitalization, ICU admission, need for mechanical ventilation, and acute kidney injury, compared to a group without rheumatic diseases at 4 months in a match-controlled study.

When investigators expanded the study to 6 months, the difference in need for mechanical ventilation disappeared. However, relative risk for venous thromboembolism (VTE) emerged as 74% higher among people with COVID-19 and with rheumatic disease, said Kristin D’Silva, MD, who presented the findings during a plenary session at the virtual annual meeting of the American College of Rheumatology. She noted that rheumatic disease itself could contribute to VTE risk.
Comorbidities including hypertension, diabetes, and asthma were more common among people with systemic autoimmune rheumatic diseases (SARDs). After adjustment for comorbidities, “the risks of hospitalization and ICU admission were attenuated, suggesting comorbidities are likely key mediators of the increased risk of severe COVID-19 outcomes observed in SARDs patients versus comparators,” Dr. D’Silva, a rheumatology fellow at Massachusetts General Hospital in Boston, said in an interview.
“The risk of venous thromboembolism persisted even after adjusting for comorbidities,” Dr. D’Silva said. Patients with SARDs should be closely monitored for VTE during COVID-19 infection, she added. “Patients with significant cardiovascular, pulmonary, and metabolic comorbidities should be closely monitored for severe COVID-19.”
At the same time, a systematic review of 15 published studies revealed a low incidence of COVID-19 infection among people with rheumatic disease. Furthermore, most experienced a mild clinical course and low mortality, Akhil Sood, MD, said when presenting results of his poster at the meeting.
Underlying immunosuppression, chronic inflammation, comorbidities, and disparities based on racial, ethnic, and socioeconomic status could predispose people with rheumatic disease to poorer COVID-19 outcomes. However, the risks and outcomes of COVID-19 infection among this population “are not well understood,” said Dr. Sood, a second-year resident in internal medicine at the University of Texas Medical Branch in Galveston.
Elevated risks in match-controlled study
Dr. D’Silva and colleagues examined a COVID-19 population and compared 716 people with SARDs and another 716 people from the general public at 4 months, as well as 2,379 people each in similar groups at 6 months. They used real-time electronic medical record data from the TriNetX research network to identify ICD-10 codes for inflammatory arthritis, connective tissue diseases, and systemic vasculitis. They also used ICD-10 codes and positive PCR tests to identify people with COVID-19.
Mean age was 57 years and women accounted for 79% of both groups evaluated at 4 months. Those with SARDs were 23% more likely to be hospitalized (relative risk, 1.23; 95% confidence interval, 1.01-1.50). This group was 75% more likely to be admitted to the ICU (RR, 1.75; 95% CI, 1.11-2.75), 77% more likely to require mechanical ventilation (RR, 1.77; 95% CI, 1.06-2.96), and 83% more likely to experience acute kidney injury (RR, 1.83; 95% CI, 1.11-3.00).
Risk of death was not significantly higher in the SARDs group (RR, 1.16; 95% CI, 0.73-1.86).
When Dr. D’Silva expanded the study to more people at 6 months, they added additional 30-day outcomes of interest: renal replacement therapy, VTE, and ischemic stroke. Risk of need for renal replacement therapy, for example, was 81% higher in the SARDs group (RR, 1.81; 95% CI, 1.07-3.07). Risk of stroke was not significantly different between groups.The improvement in mechanical ventilation risk between 4 and 6 months was not completely unexpected, Dr. D’Silva said. The relative risk dropped from 1.77 to 1.05. “This is not particularly surprising given national trends in the general population reporting decreased severe outcomes of COVID-19 including mortality as the pandemic progresses. This is likely multifactorial including changes in COVID-19 management (such as increasing use of nonintubated prone positioning rather than early intubation and treatments such as dexamethasone and remdesivir), decreased strain on hospitals and staffing compared to the early crisis phase of the pandemic, and higher testing capacity leading to detection of milder cases.”
When the 6-month analysis was further adjusted for comorbidities and a history of prior hospitalization within 1 year, only risk for acute kidney injury and VTE remained significant with relative risks of 1.33 and 1.60, respectively, likely because comorbidities are causal intermediates of COVID-19 30-day outcomes rather than confounders.
When asked to comment on the results, session comoderator Victoria K. Shanmugam, MD, said in an interview that the study “is of great interest both to rheumatologists and to patients with rheumatic disease.”
The higher risk of hospitalization, ICU admission, mechanical ventilation, acute kidney injury, and heart failure “is an important finding with implications for how our patients navigate risk during this pandemic,” said Dr. Shanmugam, director of the division of rheumatology at George Washington University in Washington.
Lower risks emerge in systematic review
The 15 observational studies in the systematic review included 11,815 participants. A total of 179, or 1.5%, tested positive for COVID-19.
“The incidence of COVID-19 infection among patients with rheumatic disease was low,” Dr. Sood said.
Within the COVID-19-positive group, almost 50% required hospitalization, 10% required ICU admission, and 8% died. The pooled event rate for hospitalization was 0.440 (95% CI, 0.296-0.596), while for ICU admission it was 0.132 (95% CI, 0.087-0.194) and for death it was 0.125 (95% CI, 0.082-0.182).
Different calculations of risk
The two studies seem to offer contradictory findings, but the disparities could be explained by study design differences. For example, Dr. D’Silva’s study evaluated a population with COVID-19 and compared those with SARDs versus a matched group from the general public. Dr. Sood and colleagues assessed study populations with rheumatic disease and assessed incidence of SARS-CoV-2 infection and difference in outcomes.
“We are asking very different questions,” Dr. D’Silva said.
“The study by D’Silva et al. was able to account for different factors to reduce confounding,” Dr. Sood said, adding that Dr. D’Silva and colleagues included a high proportion of minorities, compared with a less diverse population in the systematic review, which featured a large number of studies from Italy.
The authors of the two studies had no relevant financial disclosures to report.
SOURCES: D’Silva K et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0430, and Sood A et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0008.
ACR 2020 studies offer conflicting findings.
ACR 2020 studies offer conflicting findings.
Among people with COVID-19, those with systemic autoimmune rheumatic diseases had an elevated 30-day risk of hospitalization, ICU admission, need for mechanical ventilation, and acute kidney injury, compared to a group without rheumatic diseases at 4 months in a match-controlled study.
When investigators expanded the study to 6 months, the difference in need for mechanical ventilation disappeared. However, relative risk for venous thromboembolism (VTE) emerged as 74% higher among people with COVID-19 and with rheumatic disease, said Kristin D’Silva, MD, who presented the findings during a plenary session at the virtual annual meeting of the American College of Rheumatology. She noted that rheumatic disease itself could contribute to VTE risk.
Comorbidities including hypertension, diabetes, and asthma were more common among people with systemic autoimmune rheumatic diseases (SARDs). After adjustment for comorbidities, “the risks of hospitalization and ICU admission were attenuated, suggesting comorbidities are likely key mediators of the increased risk of severe COVID-19 outcomes observed in SARDs patients versus comparators,” Dr. D’Silva, a rheumatology fellow at Massachusetts General Hospital in Boston, said in an interview.
“The risk of venous thromboembolism persisted even after adjusting for comorbidities,” Dr. D’Silva said. Patients with SARDs should be closely monitored for VTE during COVID-19 infection, she added. “Patients with significant cardiovascular, pulmonary, and metabolic comorbidities should be closely monitored for severe COVID-19.”
At the same time, a systematic review of 15 published studies revealed a low incidence of COVID-19 infection among people with rheumatic disease. Furthermore, most experienced a mild clinical course and low mortality, Akhil Sood, MD, said when presenting results of his poster at the meeting.
Underlying immunosuppression, chronic inflammation, comorbidities, and disparities based on racial, ethnic, and socioeconomic status could predispose people with rheumatic disease to poorer COVID-19 outcomes. However, the risks and outcomes of COVID-19 infection among this population “are not well understood,” said Dr. Sood, a second-year resident in internal medicine at the University of Texas Medical Branch in Galveston.
Elevated risks in match-controlled study
Dr. D’Silva and colleagues examined a COVID-19 population and compared 716 people with SARDs and another 716 people from the general public at 4 months, as well as 2,379 people each in similar groups at 6 months. They used real-time electronic medical record data from the TriNetX research network to identify ICD-10 codes for inflammatory arthritis, connective tissue diseases, and systemic vasculitis. They also used ICD-10 codes and positive PCR tests to identify people with COVID-19.
Mean age was 57 years and women accounted for 79% of both groups evaluated at 4 months. Those with SARDs were 23% more likely to be hospitalized (relative risk, 1.23; 95% confidence interval, 1.01-1.50). This group was 75% more likely to be admitted to the ICU (RR, 1.75; 95% CI, 1.11-2.75), 77% more likely to require mechanical ventilation (RR, 1.77; 95% CI, 1.06-2.96), and 83% more likely to experience acute kidney injury (RR, 1.83; 95% CI, 1.11-3.00).
Risk of death was not significantly higher in the SARDs group (RR, 1.16; 95% CI, 0.73-1.86).
When Dr. D’Silva expanded the study to more people at 6 months, they added additional 30-day outcomes of interest: renal replacement therapy, VTE, and ischemic stroke. Risk of need for renal replacement therapy, for example, was 81% higher in the SARDs group (RR, 1.81; 95% CI, 1.07-3.07). Risk of stroke was not significantly different between groups.The improvement in mechanical ventilation risk between 4 and 6 months was not completely unexpected, Dr. D’Silva said. The relative risk dropped from 1.77 to 1.05. “This is not particularly surprising given national trends in the general population reporting decreased severe outcomes of COVID-19 including mortality as the pandemic progresses. This is likely multifactorial including changes in COVID-19 management (such as increasing use of nonintubated prone positioning rather than early intubation and treatments such as dexamethasone and remdesivir), decreased strain on hospitals and staffing compared to the early crisis phase of the pandemic, and higher testing capacity leading to detection of milder cases.”
When the 6-month analysis was further adjusted for comorbidities and a history of prior hospitalization within 1 year, only risk for acute kidney injury and VTE remained significant with relative risks of 1.33 and 1.60, respectively, likely because comorbidities are causal intermediates of COVID-19 30-day outcomes rather than confounders.
When asked to comment on the results, session comoderator Victoria K. Shanmugam, MD, said in an interview that the study “is of great interest both to rheumatologists and to patients with rheumatic disease.”
The higher risk of hospitalization, ICU admission, mechanical ventilation, acute kidney injury, and heart failure “is an important finding with implications for how our patients navigate risk during this pandemic,” said Dr. Shanmugam, director of the division of rheumatology at George Washington University in Washington.
Lower risks emerge in systematic review
The 15 observational studies in the systematic review included 11,815 participants. A total of 179, or 1.5%, tested positive for COVID-19.
“The incidence of COVID-19 infection among patients with rheumatic disease was low,” Dr. Sood said.
Within the COVID-19-positive group, almost 50% required hospitalization, 10% required ICU admission, and 8% died. The pooled event rate for hospitalization was 0.440 (95% CI, 0.296-0.596), while for ICU admission it was 0.132 (95% CI, 0.087-0.194) and for death it was 0.125 (95% CI, 0.082-0.182).
Different calculations of risk
The two studies seem to offer contradictory findings, but the disparities could be explained by study design differences. For example, Dr. D’Silva’s study evaluated a population with COVID-19 and compared those with SARDs versus a matched group from the general public. Dr. Sood and colleagues assessed study populations with rheumatic disease and assessed incidence of SARS-CoV-2 infection and difference in outcomes.
“We are asking very different questions,” Dr. D’Silva said.
“The study by D’Silva et al. was able to account for different factors to reduce confounding,” Dr. Sood said, adding that Dr. D’Silva and colleagues included a high proportion of minorities, compared with a less diverse population in the systematic review, which featured a large number of studies from Italy.
The authors of the two studies had no relevant financial disclosures to report.
SOURCES: D’Silva K et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0430, and Sood A et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0008.
Among people with COVID-19, those with systemic autoimmune rheumatic diseases had an elevated 30-day risk of hospitalization, ICU admission, need for mechanical ventilation, and acute kidney injury, compared to a group without rheumatic diseases at 4 months in a match-controlled study.
When investigators expanded the study to 6 months, the difference in need for mechanical ventilation disappeared. However, relative risk for venous thromboembolism (VTE) emerged as 74% higher among people with COVID-19 and with rheumatic disease, said Kristin D’Silva, MD, who presented the findings during a plenary session at the virtual annual meeting of the American College of Rheumatology. She noted that rheumatic disease itself could contribute to VTE risk.
Comorbidities including hypertension, diabetes, and asthma were more common among people with systemic autoimmune rheumatic diseases (SARDs). After adjustment for comorbidities, “the risks of hospitalization and ICU admission were attenuated, suggesting comorbidities are likely key mediators of the increased risk of severe COVID-19 outcomes observed in SARDs patients versus comparators,” Dr. D’Silva, a rheumatology fellow at Massachusetts General Hospital in Boston, said in an interview.
“The risk of venous thromboembolism persisted even after adjusting for comorbidities,” Dr. D’Silva said. Patients with SARDs should be closely monitored for VTE during COVID-19 infection, she added. “Patients with significant cardiovascular, pulmonary, and metabolic comorbidities should be closely monitored for severe COVID-19.”
At the same time, a systematic review of 15 published studies revealed a low incidence of COVID-19 infection among people with rheumatic disease. Furthermore, most experienced a mild clinical course and low mortality, Akhil Sood, MD, said when presenting results of his poster at the meeting.
Underlying immunosuppression, chronic inflammation, comorbidities, and disparities based on racial, ethnic, and socioeconomic status could predispose people with rheumatic disease to poorer COVID-19 outcomes. However, the risks and outcomes of COVID-19 infection among this population “are not well understood,” said Dr. Sood, a second-year resident in internal medicine at the University of Texas Medical Branch in Galveston.
Elevated risks in match-controlled study
Dr. D’Silva and colleagues examined a COVID-19 population and compared 716 people with SARDs and another 716 people from the general public at 4 months, as well as 2,379 people each in similar groups at 6 months. They used real-time electronic medical record data from the TriNetX research network to identify ICD-10 codes for inflammatory arthritis, connective tissue diseases, and systemic vasculitis. They also used ICD-10 codes and positive PCR tests to identify people with COVID-19.
Mean age was 57 years and women accounted for 79% of both groups evaluated at 4 months. Those with SARDs were 23% more likely to be hospitalized (relative risk, 1.23; 95% confidence interval, 1.01-1.50). This group was 75% more likely to be admitted to the ICU (RR, 1.75; 95% CI, 1.11-2.75), 77% more likely to require mechanical ventilation (RR, 1.77; 95% CI, 1.06-2.96), and 83% more likely to experience acute kidney injury (RR, 1.83; 95% CI, 1.11-3.00).
Risk of death was not significantly higher in the SARDs group (RR, 1.16; 95% CI, 0.73-1.86).
When Dr. D’Silva expanded the study to more people at 6 months, they added additional 30-day outcomes of interest: renal replacement therapy, VTE, and ischemic stroke. Risk of need for renal replacement therapy, for example, was 81% higher in the SARDs group (RR, 1.81; 95% CI, 1.07-3.07). Risk of stroke was not significantly different between groups.The improvement in mechanical ventilation risk between 4 and 6 months was not completely unexpected, Dr. D’Silva said. The relative risk dropped from 1.77 to 1.05. “This is not particularly surprising given national trends in the general population reporting decreased severe outcomes of COVID-19 including mortality as the pandemic progresses. This is likely multifactorial including changes in COVID-19 management (such as increasing use of nonintubated prone positioning rather than early intubation and treatments such as dexamethasone and remdesivir), decreased strain on hospitals and staffing compared to the early crisis phase of the pandemic, and higher testing capacity leading to detection of milder cases.”
When the 6-month analysis was further adjusted for comorbidities and a history of prior hospitalization within 1 year, only risk for acute kidney injury and VTE remained significant with relative risks of 1.33 and 1.60, respectively, likely because comorbidities are causal intermediates of COVID-19 30-day outcomes rather than confounders.
When asked to comment on the results, session comoderator Victoria K. Shanmugam, MD, said in an interview that the study “is of great interest both to rheumatologists and to patients with rheumatic disease.”
The higher risk of hospitalization, ICU admission, mechanical ventilation, acute kidney injury, and heart failure “is an important finding with implications for how our patients navigate risk during this pandemic,” said Dr. Shanmugam, director of the division of rheumatology at George Washington University in Washington.
Lower risks emerge in systematic review
The 15 observational studies in the systematic review included 11,815 participants. A total of 179, or 1.5%, tested positive for COVID-19.
“The incidence of COVID-19 infection among patients with rheumatic disease was low,” Dr. Sood said.
Within the COVID-19-positive group, almost 50% required hospitalization, 10% required ICU admission, and 8% died. The pooled event rate for hospitalization was 0.440 (95% CI, 0.296-0.596), while for ICU admission it was 0.132 (95% CI, 0.087-0.194) and for death it was 0.125 (95% CI, 0.082-0.182).
Different calculations of risk
The two studies seem to offer contradictory findings, but the disparities could be explained by study design differences. For example, Dr. D’Silva’s study evaluated a population with COVID-19 and compared those with SARDs versus a matched group from the general public. Dr. Sood and colleagues assessed study populations with rheumatic disease and assessed incidence of SARS-CoV-2 infection and difference in outcomes.
“We are asking very different questions,” Dr. D’Silva said.
“The study by D’Silva et al. was able to account for different factors to reduce confounding,” Dr. Sood said, adding that Dr. D’Silva and colleagues included a high proportion of minorities, compared with a less diverse population in the systematic review, which featured a large number of studies from Italy.
The authors of the two studies had no relevant financial disclosures to report.
SOURCES: D’Silva K et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0430, and Sood A et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0008.
FROM ACR 2020
First-of-its kind guideline on lipid monitoring in endocrine diseases
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FIT unfit for inpatient, emergency settings
Most fecal immunochemical tests (FIT) in the hospital setting or the ED are performed for inappropriate indications, according to new data.
“This is the largest study that focuses exclusively on the use of FIT in the ED, inpatient wards, and in the ICU, and it shows significant misuse,” said investigator Umer Bhatti, MD, from Indiana University, Indianapolis.
The only “validated indication” for FIT is to screen for colorectal cancer. However, “99.5% of the FIT tests done in our study were for inappropriate indications,” he reported at the annual meeting of the American College of Gastroenterology, where the study was honored with an ACG Presidential Poster Award.
And the inappropriate use of FIT in these settings had no positive effect on clinical decision-making, he added.
For their study, Dr. Bhatti and colleagues looked at all instances of FIT use in their hospital’s electronic medical records from November 2017 to October 2019 to assess how often FIT was being used, the indications for which it was being used, and the impact of its use on clinical care.
They identified 550 patients, 48% of whom were women, who underwent at least one FIT test. Mean age of the study cohort was 54 years. Only three of the tests, or 0.5%, were performed to screen for colorectal cancer (95% confidence interval, 0.09%-1.52%).
Among the indications documented for FIT were anemia in 242 (44.0%) patients, suspected GI bleeding in 225 (40.9%), abdominal pain in 31 (5.6%), and change in bowel habits in 19 (3.5%).
The tests were performed most often in the ED (45.3%) and on the hospital floor (42.2%), but were also performed in the ICU (10.5%) and burn unit (2.0%).
Overall, 297 of the tests, or 54%, were negative, and 253, or 46%, were positive.
“GI consults were obtained in 46.2% of the FIT-positive group, compared with 13.1% of the FIT-negative patients” (odds ratio, 5.93; 95% CI, 3.88-9.04, P < .0001), Dr. Bhatti reported.
Among FIT-positive patients, those with overt bleeding were more likely to receive a GI consultation than those without (OR, 3.3; 95% CI, 1.9-5.5; P < .0001).
Of the 117 FIT-positive patients who underwent a GI consultation, upper endoscopy was a more common outcome than colonoscopy (51.3% vs. 23.1%; P < .0001). Of the 34 patients who underwent colonoscopy or sigmoidoscopy, one was diagnosed with colorectal cancer and one with advanced adenoma.
Overt GI bleeding was a better predictor of a GI consultation than a positive FIT result. In fact, use of FIT for patients with overt GI bleeding indicates a poor understanding of the test’s utility, the investigators reported.
“For patients with overt GI bleeding, having a positive FIT made no difference on how often a bleeding source was identified on endoscopy, suggesting that FIT should not be used to guide decisions about endoscopy or hospitalization,” Dr. Bhatti said.
In light of these findings, the team urges their peers to consider measures to reduce FIT tests for unnecessary indications.
“We feel that FIT is unfit for use in the inpatient and emergency settings, and measures should be taken to curb its use,” Dr. Bhatti concluded. “We presented our data to our hospital leadership and a decision was made to remove the FIT as an orderable test from the EMR.”
These results are “striking,” said Jennifer Christie, MD, from the University, Atlanta.
“We should be educating our ER providers and inpatient providers about the proper use of FIT,” she said in an interview. “Another option – and this has been done in many settings with the fecal occult blood test – is just take FIT off the units or out of the ER, so providers won’t be tempted to use it as an assessment of these patients. Because often times, as this study showed, it doesn’t really impact outcomes.”
In fact, unnecessary FI testing could put patients at risk for unnecessary procedures. “We also know that calling for an inpatient or ER consult from a gastroenterologist may increase both length of stay and costs,” she added.
Dr. Bhatti and Dr. Christie disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Most fecal immunochemical tests (FIT) in the hospital setting or the ED are performed for inappropriate indications, according to new data.
“This is the largest study that focuses exclusively on the use of FIT in the ED, inpatient wards, and in the ICU, and it shows significant misuse,” said investigator Umer Bhatti, MD, from Indiana University, Indianapolis.
The only “validated indication” for FIT is to screen for colorectal cancer. However, “99.5% of the FIT tests done in our study were for inappropriate indications,” he reported at the annual meeting of the American College of Gastroenterology, where the study was honored with an ACG Presidential Poster Award.
And the inappropriate use of FIT in these settings had no positive effect on clinical decision-making, he added.
For their study, Dr. Bhatti and colleagues looked at all instances of FIT use in their hospital’s electronic medical records from November 2017 to October 2019 to assess how often FIT was being used, the indications for which it was being used, and the impact of its use on clinical care.
They identified 550 patients, 48% of whom were women, who underwent at least one FIT test. Mean age of the study cohort was 54 years. Only three of the tests, or 0.5%, were performed to screen for colorectal cancer (95% confidence interval, 0.09%-1.52%).
Among the indications documented for FIT were anemia in 242 (44.0%) patients, suspected GI bleeding in 225 (40.9%), abdominal pain in 31 (5.6%), and change in bowel habits in 19 (3.5%).
The tests were performed most often in the ED (45.3%) and on the hospital floor (42.2%), but were also performed in the ICU (10.5%) and burn unit (2.0%).
Overall, 297 of the tests, or 54%, were negative, and 253, or 46%, were positive.
“GI consults were obtained in 46.2% of the FIT-positive group, compared with 13.1% of the FIT-negative patients” (odds ratio, 5.93; 95% CI, 3.88-9.04, P < .0001), Dr. Bhatti reported.
Among FIT-positive patients, those with overt bleeding were more likely to receive a GI consultation than those without (OR, 3.3; 95% CI, 1.9-5.5; P < .0001).
Of the 117 FIT-positive patients who underwent a GI consultation, upper endoscopy was a more common outcome than colonoscopy (51.3% vs. 23.1%; P < .0001). Of the 34 patients who underwent colonoscopy or sigmoidoscopy, one was diagnosed with colorectal cancer and one with advanced adenoma.
Overt GI bleeding was a better predictor of a GI consultation than a positive FIT result. In fact, use of FIT for patients with overt GI bleeding indicates a poor understanding of the test’s utility, the investigators reported.
“For patients with overt GI bleeding, having a positive FIT made no difference on how often a bleeding source was identified on endoscopy, suggesting that FIT should not be used to guide decisions about endoscopy or hospitalization,” Dr. Bhatti said.
In light of these findings, the team urges their peers to consider measures to reduce FIT tests for unnecessary indications.
“We feel that FIT is unfit for use in the inpatient and emergency settings, and measures should be taken to curb its use,” Dr. Bhatti concluded. “We presented our data to our hospital leadership and a decision was made to remove the FIT as an orderable test from the EMR.”
These results are “striking,” said Jennifer Christie, MD, from the University, Atlanta.
“We should be educating our ER providers and inpatient providers about the proper use of FIT,” she said in an interview. “Another option – and this has been done in many settings with the fecal occult blood test – is just take FIT off the units or out of the ER, so providers won’t be tempted to use it as an assessment of these patients. Because often times, as this study showed, it doesn’t really impact outcomes.”
In fact, unnecessary FI testing could put patients at risk for unnecessary procedures. “We also know that calling for an inpatient or ER consult from a gastroenterologist may increase both length of stay and costs,” she added.
Dr. Bhatti and Dr. Christie disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Most fecal immunochemical tests (FIT) in the hospital setting or the ED are performed for inappropriate indications, according to new data.
“This is the largest study that focuses exclusively on the use of FIT in the ED, inpatient wards, and in the ICU, and it shows significant misuse,” said investigator Umer Bhatti, MD, from Indiana University, Indianapolis.
The only “validated indication” for FIT is to screen for colorectal cancer. However, “99.5% of the FIT tests done in our study were for inappropriate indications,” he reported at the annual meeting of the American College of Gastroenterology, where the study was honored with an ACG Presidential Poster Award.
And the inappropriate use of FIT in these settings had no positive effect on clinical decision-making, he added.
For their study, Dr. Bhatti and colleagues looked at all instances of FIT use in their hospital’s electronic medical records from November 2017 to October 2019 to assess how often FIT was being used, the indications for which it was being used, and the impact of its use on clinical care.
They identified 550 patients, 48% of whom were women, who underwent at least one FIT test. Mean age of the study cohort was 54 years. Only three of the tests, or 0.5%, were performed to screen for colorectal cancer (95% confidence interval, 0.09%-1.52%).
Among the indications documented for FIT were anemia in 242 (44.0%) patients, suspected GI bleeding in 225 (40.9%), abdominal pain in 31 (5.6%), and change in bowel habits in 19 (3.5%).
The tests were performed most often in the ED (45.3%) and on the hospital floor (42.2%), but were also performed in the ICU (10.5%) and burn unit (2.0%).
Overall, 297 of the tests, or 54%, were negative, and 253, or 46%, were positive.
“GI consults were obtained in 46.2% of the FIT-positive group, compared with 13.1% of the FIT-negative patients” (odds ratio, 5.93; 95% CI, 3.88-9.04, P < .0001), Dr. Bhatti reported.
Among FIT-positive patients, those with overt bleeding were more likely to receive a GI consultation than those without (OR, 3.3; 95% CI, 1.9-5.5; P < .0001).
Of the 117 FIT-positive patients who underwent a GI consultation, upper endoscopy was a more common outcome than colonoscopy (51.3% vs. 23.1%; P < .0001). Of the 34 patients who underwent colonoscopy or sigmoidoscopy, one was diagnosed with colorectal cancer and one with advanced adenoma.
Overt GI bleeding was a better predictor of a GI consultation than a positive FIT result. In fact, use of FIT for patients with overt GI bleeding indicates a poor understanding of the test’s utility, the investigators reported.
“For patients with overt GI bleeding, having a positive FIT made no difference on how often a bleeding source was identified on endoscopy, suggesting that FIT should not be used to guide decisions about endoscopy or hospitalization,” Dr. Bhatti said.
In light of these findings, the team urges their peers to consider measures to reduce FIT tests for unnecessary indications.
“We feel that FIT is unfit for use in the inpatient and emergency settings, and measures should be taken to curb its use,” Dr. Bhatti concluded. “We presented our data to our hospital leadership and a decision was made to remove the FIT as an orderable test from the EMR.”
These results are “striking,” said Jennifer Christie, MD, from the University, Atlanta.
“We should be educating our ER providers and inpatient providers about the proper use of FIT,” she said in an interview. “Another option – and this has been done in many settings with the fecal occult blood test – is just take FIT off the units or out of the ER, so providers won’t be tempted to use it as an assessment of these patients. Because often times, as this study showed, it doesn’t really impact outcomes.”
In fact, unnecessary FI testing could put patients at risk for unnecessary procedures. “We also know that calling for an inpatient or ER consult from a gastroenterologist may increase both length of stay and costs,” she added.
Dr. Bhatti and Dr. Christie disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.