User login
AI and reality – diagnosing otitis media is a real challenge
Let’s pretend for a moment that you receive a call from one of your college roommates who thanks to his family connections has become a venture capitalist in California. His group is considering investing in a start-up that is developing a handheld instrument that it claims will use artificial intelligence to diagnose ear infections far more accurately than the human eye. He wonders if you would like to help him evaluate the company’s proposal and offers you a small percentage of the profits for your efforts should they choose to invest.
Your former roommate has done enough research on his own to understand that otitis media makes up a large chunk of a pediatrician’s workload and that making an accurate diagnosis can often be difficult in a struggling child. He describes his own experience watching a frustrated pediatrician attempting to remove wax from his child’s ear and eventually prescribing antibiotics “to be safe.”
You agree and review the prospectus, which includes a paper from a peer-reviewed journal. What you discover is that the investigators used more than 600 high-resolution images of tympanic membranes taken “during operative myringotomy and tympanostomy tube placement” and the findings at tympanocentesis to train a neural network.
Once trained, the model they developed could differentiate with 95% accuracy between an image of a tympanic membrane that covered a normal middle ear from one that merely contained fluid and from one that contained infected fluid. When these same images were shown to 39 clinicians, more than half of which were pediatricians and included both faculty-level staff and trainees, the average diagnostic accuracy was 65%.
The prospectus includes prediction that this technology could easily be developed into a handheld instrument similar to a traditional otoscope, which could then be linked to the operator’s smartphone, giving the clinician an instant treat or no-treat answer.
Now, remember you have nothing to lose except maybe a friendship. How would you advise your old college roommate?
My advice to your college buddy would be one of caution! Yes, there is a potential big upside because there is a real need for a device that could provide a diagnostic accuracy that this AI model promises. While I suspect that AI will always be more accurate in diagnosis using static images, I bet that most people, clinicians and nonclinicians, could improve their accuracy by linking photos with diagnoses with an hour of practice.
However, evaluating a high-resolution photograph taken through an operative scope inserted into the cerumenless ear canal of a sedated, afrebrile child is several orders of magnitude less difficult than the real-world environment in which the diagnosis of otitis media is usually made.
If the venture capitalists were still interested in getting into the otitis media marketplace, you might suggest they look into companies that have already developed image capture otoscopes. At this point I could only find one on the Internet that was portable and it certainly isn’t small-child friendly. Once we have a tool that can capture images in real-world situations, the next step is to train AI systems to interpret them using the approach these researchers have developed. I bet it can be done. It will be only a matter of time ... and money.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Let’s pretend for a moment that you receive a call from one of your college roommates who thanks to his family connections has become a venture capitalist in California. His group is considering investing in a start-up that is developing a handheld instrument that it claims will use artificial intelligence to diagnose ear infections far more accurately than the human eye. He wonders if you would like to help him evaluate the company’s proposal and offers you a small percentage of the profits for your efforts should they choose to invest.
Your former roommate has done enough research on his own to understand that otitis media makes up a large chunk of a pediatrician’s workload and that making an accurate diagnosis can often be difficult in a struggling child. He describes his own experience watching a frustrated pediatrician attempting to remove wax from his child’s ear and eventually prescribing antibiotics “to be safe.”
You agree and review the prospectus, which includes a paper from a peer-reviewed journal. What you discover is that the investigators used more than 600 high-resolution images of tympanic membranes taken “during operative myringotomy and tympanostomy tube placement” and the findings at tympanocentesis to train a neural network.
Once trained, the model they developed could differentiate with 95% accuracy between an image of a tympanic membrane that covered a normal middle ear from one that merely contained fluid and from one that contained infected fluid. When these same images were shown to 39 clinicians, more than half of which were pediatricians and included both faculty-level staff and trainees, the average diagnostic accuracy was 65%.
The prospectus includes prediction that this technology could easily be developed into a handheld instrument similar to a traditional otoscope, which could then be linked to the operator’s smartphone, giving the clinician an instant treat or no-treat answer.
Now, remember you have nothing to lose except maybe a friendship. How would you advise your old college roommate?
My advice to your college buddy would be one of caution! Yes, there is a potential big upside because there is a real need for a device that could provide a diagnostic accuracy that this AI model promises. While I suspect that AI will always be more accurate in diagnosis using static images, I bet that most people, clinicians and nonclinicians, could improve their accuracy by linking photos with diagnoses with an hour of practice.
However, evaluating a high-resolution photograph taken through an operative scope inserted into the cerumenless ear canal of a sedated, afrebrile child is several orders of magnitude less difficult than the real-world environment in which the diagnosis of otitis media is usually made.
If the venture capitalists were still interested in getting into the otitis media marketplace, you might suggest they look into companies that have already developed image capture otoscopes. At this point I could only find one on the Internet that was portable and it certainly isn’t small-child friendly. Once we have a tool that can capture images in real-world situations, the next step is to train AI systems to interpret them using the approach these researchers have developed. I bet it can be done. It will be only a matter of time ... and money.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Let’s pretend for a moment that you receive a call from one of your college roommates who thanks to his family connections has become a venture capitalist in California. His group is considering investing in a start-up that is developing a handheld instrument that it claims will use artificial intelligence to diagnose ear infections far more accurately than the human eye. He wonders if you would like to help him evaluate the company’s proposal and offers you a small percentage of the profits for your efforts should they choose to invest.
Your former roommate has done enough research on his own to understand that otitis media makes up a large chunk of a pediatrician’s workload and that making an accurate diagnosis can often be difficult in a struggling child. He describes his own experience watching a frustrated pediatrician attempting to remove wax from his child’s ear and eventually prescribing antibiotics “to be safe.”
You agree and review the prospectus, which includes a paper from a peer-reviewed journal. What you discover is that the investigators used more than 600 high-resolution images of tympanic membranes taken “during operative myringotomy and tympanostomy tube placement” and the findings at tympanocentesis to train a neural network.
Once trained, the model they developed could differentiate with 95% accuracy between an image of a tympanic membrane that covered a normal middle ear from one that merely contained fluid and from one that contained infected fluid. When these same images were shown to 39 clinicians, more than half of which were pediatricians and included both faculty-level staff and trainees, the average diagnostic accuracy was 65%.
The prospectus includes prediction that this technology could easily be developed into a handheld instrument similar to a traditional otoscope, which could then be linked to the operator’s smartphone, giving the clinician an instant treat or no-treat answer.
Now, remember you have nothing to lose except maybe a friendship. How would you advise your old college roommate?
My advice to your college buddy would be one of caution! Yes, there is a potential big upside because there is a real need for a device that could provide a diagnostic accuracy that this AI model promises. While I suspect that AI will always be more accurate in diagnosis using static images, I bet that most people, clinicians and nonclinicians, could improve their accuracy by linking photos with diagnoses with an hour of practice.
However, evaluating a high-resolution photograph taken through an operative scope inserted into the cerumenless ear canal of a sedated, afrebrile child is several orders of magnitude less difficult than the real-world environment in which the diagnosis of otitis media is usually made.
If the venture capitalists were still interested in getting into the otitis media marketplace, you might suggest they look into companies that have already developed image capture otoscopes. At this point I could only find one on the Internet that was portable and it certainly isn’t small-child friendly. Once we have a tool that can capture images in real-world situations, the next step is to train AI systems to interpret them using the approach these researchers have developed. I bet it can be done. It will be only a matter of time ... and money.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Psychiatrists’ views on psychoactive drugs clash with U.S. policy
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.
Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.
Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.
Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF DRUG POLICY
Five contract red flags every physician should know
Recruiting health care workers is a challenge these days for both private practice and hospital employers, and competition can be fierce. In order to be competitive, employers need to review the package they are offering potential candidates and understand that it’s more than just compensation and benefits that matter.
As someone who reviews physician contracts extensively, there are some common examples of language that may cause a candidate to choose a different position.
Probationary period
Although every employer wants to find out if they like the physician or midlevel employee that they have just hired before fully committing, the inclusion of a probationary period (usually 90 days) is offensive to a candidate, especially one with a choice of contracts.
Essentially, the employer is asking the employee to (potentially) relocate, go through the credentialing process, and turn down other potential offers, all for the possibility that they could easily be terminated. Probationary periods typically allow an employee to be immediately terminated without notice or cause, which can then leave them stranded without a paycheck (and with a new home and/or other recent commitments).
Moreover, contracts with probationary periods tend to terminate the employee without covering any tail costs or clarifying that the employer will not enforce restrictive provisions (even if unlikely to be legally enforceable based on the short relationship).
It is important to understand that the process of a person finding a new position, which includes interviewing, contract negotiation, and credentialing, can take up to 6 months. For this reason, probationary provisions create real job insecurity for a candidate.
Entering into a new affiliation is a leap of faith both for the employer and the employee. If the circumstances do not work out, the employer should fairly compensate the employee for the notice period and ask them not to return to work or otherwise allow them to keep working the notice period while they search for a new position.
Acceleration of notice
Another objectionable provision that employers like to include in their contracts is one which allows the employer to accelerate and immediately terminate an employee who has given proper notice.
The contract will contain a standard notice provision, but when the health care professional submits notice, their last date is suddenly accelerated, and they are released without further compensation, notice, or benefits. This type of provision is particularly offensive to health care employees who take the step of giving proper contractual notice and, similar to the probationary language, can create real job insecurity for an employee who suddenly loses their paycheck and has no new job to start.
Medical workers should be paid for the entire notice period whether or not they are allowed to work. Unfortunately, this type of provision is sometimes hidden in contracts and not noticed by employees, who tend to focus on the notice provision itself. I consider this provision to be a red flag about the employer when I review clients’ contracts.
Malpractice tail
Although many employers will claim it is not unusual for an employee to pay for their own malpractice tail, in the current marketplace, the payment of tail can be a deciding factor in whether a candidate accepts a contract.
At a minimum, employers should consider paying for the tail under circumstances where they non-renew a contract, terminate without cause, or the contract is terminated for the employer’s breach. Similarly, I like to seek out payment of the tail by the employer where the contract is terminated owing to a change in the law, use of a force majeure provision, loss of the employer’s hospital contract, or similar provisions where termination is outside the control of the employee.
Employers should also consider a provision where they share the cost of a tail or cover the entire cost on the basis of years of service in order to stand out to a potential candidate.
Noncompete provisions
I do not find noncompete provisions to be generally unacceptable when properly written; however, employers should reevaluate the reasonableness of their noncompete language frequently, because such language can make the difference in whether a candidate accepts a contract.
A reasonable noncompete that only protects the employer as necessary and does not restrict the reasonable practice of medicine is always preferable and can be the deciding factor for a candidate. Tying enforcement of a noncompete to reasons for termination (similar to the tail) can also make a positive difference in a candidate’s review of a contract.
Egregious noncompetes, where the candidate is simply informed that the language is “not negotiable,” are unlikely to be compelling to a candidate with other options.
Specifics on location, call, schedule
One item potential employees find extremely frustrating about contracts is when it fails to include promises made regarding location, call, and schedule.
These particular items affect a physician’s expectations about a job, including commute time, family life, and lifestyle. An employer or recruiter that makes a lot of promises on these points but won’t commit to the details in writing (or at least offer mutual agreement on these issues) can cause an uncertain candidate to choose the job that offers greater certainty.
There are many provisions of a contract that can make a difference to a particular job applicant. A savvy employer seeking to capture a particular health care professional should find out what the specific goals and needs of the candidate might be and consider adjusting the contract to best satisfy the candidate.
At the end of the day, however, at least for those physicians and others reviewing contracts that are fairly equivalent, it may be the fairness of the contract provisions that end up being the deciding factor.
Ms. Adler is Health Law Group Practice Leader for the law firm Roetzel in Chicago. She reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Recruiting health care workers is a challenge these days for both private practice and hospital employers, and competition can be fierce. In order to be competitive, employers need to review the package they are offering potential candidates and understand that it’s more than just compensation and benefits that matter.
As someone who reviews physician contracts extensively, there are some common examples of language that may cause a candidate to choose a different position.
Probationary period
Although every employer wants to find out if they like the physician or midlevel employee that they have just hired before fully committing, the inclusion of a probationary period (usually 90 days) is offensive to a candidate, especially one with a choice of contracts.
Essentially, the employer is asking the employee to (potentially) relocate, go through the credentialing process, and turn down other potential offers, all for the possibility that they could easily be terminated. Probationary periods typically allow an employee to be immediately terminated without notice or cause, which can then leave them stranded without a paycheck (and with a new home and/or other recent commitments).
Moreover, contracts with probationary periods tend to terminate the employee without covering any tail costs or clarifying that the employer will not enforce restrictive provisions (even if unlikely to be legally enforceable based on the short relationship).
It is important to understand that the process of a person finding a new position, which includes interviewing, contract negotiation, and credentialing, can take up to 6 months. For this reason, probationary provisions create real job insecurity for a candidate.
Entering into a new affiliation is a leap of faith both for the employer and the employee. If the circumstances do not work out, the employer should fairly compensate the employee for the notice period and ask them not to return to work or otherwise allow them to keep working the notice period while they search for a new position.
Acceleration of notice
Another objectionable provision that employers like to include in their contracts is one which allows the employer to accelerate and immediately terminate an employee who has given proper notice.
The contract will contain a standard notice provision, but when the health care professional submits notice, their last date is suddenly accelerated, and they are released without further compensation, notice, or benefits. This type of provision is particularly offensive to health care employees who take the step of giving proper contractual notice and, similar to the probationary language, can create real job insecurity for an employee who suddenly loses their paycheck and has no new job to start.
Medical workers should be paid for the entire notice period whether or not they are allowed to work. Unfortunately, this type of provision is sometimes hidden in contracts and not noticed by employees, who tend to focus on the notice provision itself. I consider this provision to be a red flag about the employer when I review clients’ contracts.
Malpractice tail
Although many employers will claim it is not unusual for an employee to pay for their own malpractice tail, in the current marketplace, the payment of tail can be a deciding factor in whether a candidate accepts a contract.
At a minimum, employers should consider paying for the tail under circumstances where they non-renew a contract, terminate without cause, or the contract is terminated for the employer’s breach. Similarly, I like to seek out payment of the tail by the employer where the contract is terminated owing to a change in the law, use of a force majeure provision, loss of the employer’s hospital contract, or similar provisions where termination is outside the control of the employee.
Employers should also consider a provision where they share the cost of a tail or cover the entire cost on the basis of years of service in order to stand out to a potential candidate.
Noncompete provisions
I do not find noncompete provisions to be generally unacceptable when properly written; however, employers should reevaluate the reasonableness of their noncompete language frequently, because such language can make the difference in whether a candidate accepts a contract.
A reasonable noncompete that only protects the employer as necessary and does not restrict the reasonable practice of medicine is always preferable and can be the deciding factor for a candidate. Tying enforcement of a noncompete to reasons for termination (similar to the tail) can also make a positive difference in a candidate’s review of a contract.
Egregious noncompetes, where the candidate is simply informed that the language is “not negotiable,” are unlikely to be compelling to a candidate with other options.
Specifics on location, call, schedule
One item potential employees find extremely frustrating about contracts is when it fails to include promises made regarding location, call, and schedule.
These particular items affect a physician’s expectations about a job, including commute time, family life, and lifestyle. An employer or recruiter that makes a lot of promises on these points but won’t commit to the details in writing (or at least offer mutual agreement on these issues) can cause an uncertain candidate to choose the job that offers greater certainty.
There are many provisions of a contract that can make a difference to a particular job applicant. A savvy employer seeking to capture a particular health care professional should find out what the specific goals and needs of the candidate might be and consider adjusting the contract to best satisfy the candidate.
At the end of the day, however, at least for those physicians and others reviewing contracts that are fairly equivalent, it may be the fairness of the contract provisions that end up being the deciding factor.
Ms. Adler is Health Law Group Practice Leader for the law firm Roetzel in Chicago. She reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Recruiting health care workers is a challenge these days for both private practice and hospital employers, and competition can be fierce. In order to be competitive, employers need to review the package they are offering potential candidates and understand that it’s more than just compensation and benefits that matter.
As someone who reviews physician contracts extensively, there are some common examples of language that may cause a candidate to choose a different position.
Probationary period
Although every employer wants to find out if they like the physician or midlevel employee that they have just hired before fully committing, the inclusion of a probationary period (usually 90 days) is offensive to a candidate, especially one with a choice of contracts.
Essentially, the employer is asking the employee to (potentially) relocate, go through the credentialing process, and turn down other potential offers, all for the possibility that they could easily be terminated. Probationary periods typically allow an employee to be immediately terminated without notice or cause, which can then leave them stranded without a paycheck (and with a new home and/or other recent commitments).
Moreover, contracts with probationary periods tend to terminate the employee without covering any tail costs or clarifying that the employer will not enforce restrictive provisions (even if unlikely to be legally enforceable based on the short relationship).
It is important to understand that the process of a person finding a new position, which includes interviewing, contract negotiation, and credentialing, can take up to 6 months. For this reason, probationary provisions create real job insecurity for a candidate.
Entering into a new affiliation is a leap of faith both for the employer and the employee. If the circumstances do not work out, the employer should fairly compensate the employee for the notice period and ask them not to return to work or otherwise allow them to keep working the notice period while they search for a new position.
Acceleration of notice
Another objectionable provision that employers like to include in their contracts is one which allows the employer to accelerate and immediately terminate an employee who has given proper notice.
The contract will contain a standard notice provision, but when the health care professional submits notice, their last date is suddenly accelerated, and they are released without further compensation, notice, or benefits. This type of provision is particularly offensive to health care employees who take the step of giving proper contractual notice and, similar to the probationary language, can create real job insecurity for an employee who suddenly loses their paycheck and has no new job to start.
Medical workers should be paid for the entire notice period whether or not they are allowed to work. Unfortunately, this type of provision is sometimes hidden in contracts and not noticed by employees, who tend to focus on the notice provision itself. I consider this provision to be a red flag about the employer when I review clients’ contracts.
Malpractice tail
Although many employers will claim it is not unusual for an employee to pay for their own malpractice tail, in the current marketplace, the payment of tail can be a deciding factor in whether a candidate accepts a contract.
At a minimum, employers should consider paying for the tail under circumstances where they non-renew a contract, terminate without cause, or the contract is terminated for the employer’s breach. Similarly, I like to seek out payment of the tail by the employer where the contract is terminated owing to a change in the law, use of a force majeure provision, loss of the employer’s hospital contract, or similar provisions where termination is outside the control of the employee.
Employers should also consider a provision where they share the cost of a tail or cover the entire cost on the basis of years of service in order to stand out to a potential candidate.
Noncompete provisions
I do not find noncompete provisions to be generally unacceptable when properly written; however, employers should reevaluate the reasonableness of their noncompete language frequently, because such language can make the difference in whether a candidate accepts a contract.
A reasonable noncompete that only protects the employer as necessary and does not restrict the reasonable practice of medicine is always preferable and can be the deciding factor for a candidate. Tying enforcement of a noncompete to reasons for termination (similar to the tail) can also make a positive difference in a candidate’s review of a contract.
Egregious noncompetes, where the candidate is simply informed that the language is “not negotiable,” are unlikely to be compelling to a candidate with other options.
Specifics on location, call, schedule
One item potential employees find extremely frustrating about contracts is when it fails to include promises made regarding location, call, and schedule.
These particular items affect a physician’s expectations about a job, including commute time, family life, and lifestyle. An employer or recruiter that makes a lot of promises on these points but won’t commit to the details in writing (or at least offer mutual agreement on these issues) can cause an uncertain candidate to choose the job that offers greater certainty.
There are many provisions of a contract that can make a difference to a particular job applicant. A savvy employer seeking to capture a particular health care professional should find out what the specific goals and needs of the candidate might be and consider adjusting the contract to best satisfy the candidate.
At the end of the day, however, at least for those physicians and others reviewing contracts that are fairly equivalent, it may be the fairness of the contract provisions that end up being the deciding factor.
Ms. Adler is Health Law Group Practice Leader for the law firm Roetzel in Chicago. She reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Muscling through the data
Statins have, overall, been a remarkably beneficial class of drugs. Yes, you occasionally get patients who see them as part of some huge pharma-government conspiracy (along with vaccines and 5G, presumably) but the data are there to support them.
One of the issues with them is myalgias. We all see this to varying degrees. We all warn patients about it, as do their pharmacists, the information sheets from the pharmacy, some TV show, a Facebook friend, that guy in their Tuesday bowling league ... etc.
It is a legitimate concern. Some people definitely do get muscle cramps from them and need to come off. Scanning the medication list of someone who comes in with muscle cramps is a key part of the case.
Recently, the Lancet published a meta-analysis on the subject and found that, While previous data suggested rates of myalgias as high as 29%, this paper found it was closer to 7% compared with placebo. Only one in 15 of the muscle-related reports by patients while taking statins were clearly caused by the drug.
The power of suggestion is remarkable indeed.
The study is interesting. It might be correct.
But try telling that to the patients.
We all have patients who will get pretty much any side effect we mention, or that they read about online. That’s just human nature for some. But even reasonable adults can confuse things. The guy who starts Lipitor one week then helps his daughter move into her apartment the next. The lady who starts Crestor while training for a half-marathon. And so on.
The fact is that a lot of people take statins. And a lot of people (like, pretty much all of us) do things that can cause muscle injuries. Sooner or later these lines are going to intersect, but that doesn’t mean they have anything to do with each other.
It’s a lot harder to explain that, and have people believe it, once they’ve convinced themselves otherwise. Pravachol definitely did this, Dr. Google said so. It doesn’t help that trust in doctors, and health care science in general, has been eroded by political pundits and nonmedical experts during the COVID-19 pandemic. To some people our years of experience and training are nothing compared to what an anonymous guy on Parler told them.
Certainly this paper will help. A lot of people can benefit from statins. With this data maybe we can convince some to give them a fair shot.
But, as we’ve all experienced in practice, sometimes no amount of solid data will change the mind of someone who’s already made theirs up.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Statins have, overall, been a remarkably beneficial class of drugs. Yes, you occasionally get patients who see them as part of some huge pharma-government conspiracy (along with vaccines and 5G, presumably) but the data are there to support them.
One of the issues with them is myalgias. We all see this to varying degrees. We all warn patients about it, as do their pharmacists, the information sheets from the pharmacy, some TV show, a Facebook friend, that guy in their Tuesday bowling league ... etc.
It is a legitimate concern. Some people definitely do get muscle cramps from them and need to come off. Scanning the medication list of someone who comes in with muscle cramps is a key part of the case.
Recently, the Lancet published a meta-analysis on the subject and found that, While previous data suggested rates of myalgias as high as 29%, this paper found it was closer to 7% compared with placebo. Only one in 15 of the muscle-related reports by patients while taking statins were clearly caused by the drug.
The power of suggestion is remarkable indeed.
The study is interesting. It might be correct.
But try telling that to the patients.
We all have patients who will get pretty much any side effect we mention, or that they read about online. That’s just human nature for some. But even reasonable adults can confuse things. The guy who starts Lipitor one week then helps his daughter move into her apartment the next. The lady who starts Crestor while training for a half-marathon. And so on.
The fact is that a lot of people take statins. And a lot of people (like, pretty much all of us) do things that can cause muscle injuries. Sooner or later these lines are going to intersect, but that doesn’t mean they have anything to do with each other.
It’s a lot harder to explain that, and have people believe it, once they’ve convinced themselves otherwise. Pravachol definitely did this, Dr. Google said so. It doesn’t help that trust in doctors, and health care science in general, has been eroded by political pundits and nonmedical experts during the COVID-19 pandemic. To some people our years of experience and training are nothing compared to what an anonymous guy on Parler told them.
Certainly this paper will help. A lot of people can benefit from statins. With this data maybe we can convince some to give them a fair shot.
But, as we’ve all experienced in practice, sometimes no amount of solid data will change the mind of someone who’s already made theirs up.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Statins have, overall, been a remarkably beneficial class of drugs. Yes, you occasionally get patients who see them as part of some huge pharma-government conspiracy (along with vaccines and 5G, presumably) but the data are there to support them.
One of the issues with them is myalgias. We all see this to varying degrees. We all warn patients about it, as do their pharmacists, the information sheets from the pharmacy, some TV show, a Facebook friend, that guy in their Tuesday bowling league ... etc.
It is a legitimate concern. Some people definitely do get muscle cramps from them and need to come off. Scanning the medication list of someone who comes in with muscle cramps is a key part of the case.
Recently, the Lancet published a meta-analysis on the subject and found that, While previous data suggested rates of myalgias as high as 29%, this paper found it was closer to 7% compared with placebo. Only one in 15 of the muscle-related reports by patients while taking statins were clearly caused by the drug.
The power of suggestion is remarkable indeed.
The study is interesting. It might be correct.
But try telling that to the patients.
We all have patients who will get pretty much any side effect we mention, or that they read about online. That’s just human nature for some. But even reasonable adults can confuse things. The guy who starts Lipitor one week then helps his daughter move into her apartment the next. The lady who starts Crestor while training for a half-marathon. And so on.
The fact is that a lot of people take statins. And a lot of people (like, pretty much all of us) do things that can cause muscle injuries. Sooner or later these lines are going to intersect, but that doesn’t mean they have anything to do with each other.
It’s a lot harder to explain that, and have people believe it, once they’ve convinced themselves otherwise. Pravachol definitely did this, Dr. Google said so. It doesn’t help that trust in doctors, and health care science in general, has been eroded by political pundits and nonmedical experts during the COVID-19 pandemic. To some people our years of experience and training are nothing compared to what an anonymous guy on Parler told them.
Certainly this paper will help. A lot of people can benefit from statins. With this data maybe we can convince some to give them a fair shot.
But, as we’ve all experienced in practice, sometimes no amount of solid data will change the mind of someone who’s already made theirs up.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
WIC review finds broad benefits, knowledge gaps
How exactly the national program achieves these outcomes, however, remains unclear, and study quality shows room for improvement, reported co–lead authors Maya Venkataramani, MD, MPH and S. Michelle Ogunwole, MD, PhD of Johns Hopkins University, Baltimore, and colleagues.
The WIC program, which has been serving low-income women and young children since 1974, “provides supplemental foods, nutrition education and breastfeeding support, screening and referrals to medical and social services, and support for high-risk pregnancies,” the investigators wrote in Annals of Internal Medicine. The U.S. Food and Nutrition Service administers the program.
The authors conducted a systematic review of 20 observational studies aimed at determining the impacts of WIC participation on maternal, neonatal-birth, and infant-child health outcomes.
All studies included in the review began in or after 2009, when the WIC food package was revised to better address diet-related chronic diseases. For inclusion in the review, studies were required to have a WIC-eligible comparison group. Included research also evaluated the relationship between WIC participation and the prespecified health outcomes.
“We found only 20 studies that fulfilled our rigorous study inclusion criteria for these specific outcomes,” the investigators wrote. “In some areas, the evidence was absent, and in others, the strength of evidence (SOE) was moderate or low.”
Six outcome categories were assessed: maternal morbidity, maternal pregnancy outcomes, maternal health behaviors, maternal health care utilization, child morbidity, and childhood health care utilization. Of these, maternal health care utilization had the most robust body of evidence, while data from studies evaluating maternal morbidity and child morbidity were deemed insufficient.
Based on eligible studies, WIC participation was associated with reduced risks of insufficient weight gain in pregnancy, preterm birth, low infant birthweight, and infant mortality. Participation was also associated with an increased likelihood of infant and child health care utilization, such as routine immunizations.
Growing evidence should drive enrollment
“Growing evidence points to WIC as a way to reduce risk of preterm birth and other adverse outcomes,” said Laura Jelliffe-Pawlowski, PhD, MS, professor at the University of California, San Francisco and a director for the UCSF California Preterm Birth Initiative.

Dr. Jelliffe-Pawlowski, who conducted a California-based study included in the paper, said the review is noteworthy because it shows that WIC-associated benefits are observed across locations.
“It’s not just in California; it’s across the country,” she said. “It’s a national call to action – where there’s partnership between national-, state- and community-level WIC programs – to make WIC as accessible as possible, and reflect community wants and needs, so that more people enroll, and more people stay enrolled.”
Dr. Jelliffe-Pawlowski’s coauthor on the California study, Rita Hamad, MD, PhD, associate professor of family & community medicine at UCSF and associate director of the UCSF Center for Health Equity, encouraged health care providers to drive WIC enrollment, noting that, presently, only one in four eligible 4-year-olds participates.
“Physicians and other health care stakeholders can help patients benefit from this program by encouraging them to sign up, and even by providing sign-up support in the form of a social worker or other staff member,” Dr. Hamad said. “There is also literature on the types of interventions that improve take-up of safety net programs that providers can look to.”
Goals of future research
Optimizing WIC operations, however, is only half the battle, considering the evidence gaps revealed by the review.

“We still need stronger studies that use more rigorous study designs ... to provide more convincing evidence to policymakers, as well as more evidence on long-term impacts,” Dr. Hamad said. “We also need to better understand why take-up is low in these programs despite these potential health benefits. Then we can make sure that economically disadvantaged families receive the benefits for which they are eligible through interventions to improve participation rates.”
Ideally, WIC programs would receive additional funding for independent parties to evaluate health outcomes, according to Ashwini Lakshmanan, MD, MS, MPH, associate professor in the department of health systems science at Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, Calif.
Dr. Lakshmanan, who previously evaluated the benefits of WIC participation for high-risk infants, noted that randomized clinical trials would be unethical in this setting, yet data collection can still be “very conscientious and intentional,” with a focus on policy-shaping outcome metrics like immunizations and pediatric health care visits.
“The main point is thinking about it at the forefront, and not retrospectively,” Dr. Lakshmanan said.
Dr. Ogunwole, who led the present review, suggested in a written comment that future studies “could employ robust statistical methods (propensity matching, fixed effects models, etc.) to help reduce bias.”
She also recommended evaluating innovations in WIC programs; for example, adding a health coach, or conducting a cooking skills intervention.
Studies are also needed to better understand the various obstacles to WIC success, such as misconceptions about the program, discrimination, and barriers to enrollment, Dr. Ogunwole added.
“WIC enrollment has been decreasing for a number of years, and this was occurring prepandemic as well,” she said. “More work needs to be done to understand this issue.”
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators and interviewees disclosed no conflicts of interest.
How exactly the national program achieves these outcomes, however, remains unclear, and study quality shows room for improvement, reported co–lead authors Maya Venkataramani, MD, MPH and S. Michelle Ogunwole, MD, PhD of Johns Hopkins University, Baltimore, and colleagues.
The WIC program, which has been serving low-income women and young children since 1974, “provides supplemental foods, nutrition education and breastfeeding support, screening and referrals to medical and social services, and support for high-risk pregnancies,” the investigators wrote in Annals of Internal Medicine. The U.S. Food and Nutrition Service administers the program.
The authors conducted a systematic review of 20 observational studies aimed at determining the impacts of WIC participation on maternal, neonatal-birth, and infant-child health outcomes.
All studies included in the review began in or after 2009, when the WIC food package was revised to better address diet-related chronic diseases. For inclusion in the review, studies were required to have a WIC-eligible comparison group. Included research also evaluated the relationship between WIC participation and the prespecified health outcomes.
“We found only 20 studies that fulfilled our rigorous study inclusion criteria for these specific outcomes,” the investigators wrote. “In some areas, the evidence was absent, and in others, the strength of evidence (SOE) was moderate or low.”
Six outcome categories were assessed: maternal morbidity, maternal pregnancy outcomes, maternal health behaviors, maternal health care utilization, child morbidity, and childhood health care utilization. Of these, maternal health care utilization had the most robust body of evidence, while data from studies evaluating maternal morbidity and child morbidity were deemed insufficient.
Based on eligible studies, WIC participation was associated with reduced risks of insufficient weight gain in pregnancy, preterm birth, low infant birthweight, and infant mortality. Participation was also associated with an increased likelihood of infant and child health care utilization, such as routine immunizations.
Growing evidence should drive enrollment
“Growing evidence points to WIC as a way to reduce risk of preterm birth and other adverse outcomes,” said Laura Jelliffe-Pawlowski, PhD, MS, professor at the University of California, San Francisco and a director for the UCSF California Preterm Birth Initiative.
Dr. Jelliffe-Pawlowski, who conducted a California-based study included in the paper, said the review is noteworthy because it shows that WIC-associated benefits are observed across locations.
“It’s not just in California; it’s across the country,” she said. “It’s a national call to action – where there’s partnership between national-, state- and community-level WIC programs – to make WIC as accessible as possible, and reflect community wants and needs, so that more people enroll, and more people stay enrolled.”
Dr. Jelliffe-Pawlowski’s coauthor on the California study, Rita Hamad, MD, PhD, associate professor of family & community medicine at UCSF and associate director of the UCSF Center for Health Equity, encouraged health care providers to drive WIC enrollment, noting that, presently, only one in four eligible 4-year-olds participates.
“Physicians and other health care stakeholders can help patients benefit from this program by encouraging them to sign up, and even by providing sign-up support in the form of a social worker or other staff member,” Dr. Hamad said. “There is also literature on the types of interventions that improve take-up of safety net programs that providers can look to.”
Goals of future research
Optimizing WIC operations, however, is only half the battle, considering the evidence gaps revealed by the review.
“We still need stronger studies that use more rigorous study designs ... to provide more convincing evidence to policymakers, as well as more evidence on long-term impacts,” Dr. Hamad said. “We also need to better understand why take-up is low in these programs despite these potential health benefits. Then we can make sure that economically disadvantaged families receive the benefits for which they are eligible through interventions to improve participation rates.”
Ideally, WIC programs would receive additional funding for independent parties to evaluate health outcomes, according to Ashwini Lakshmanan, MD, MS, MPH, associate professor in the department of health systems science at Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, Calif.
Dr. Lakshmanan, who previously evaluated the benefits of WIC participation for high-risk infants, noted that randomized clinical trials would be unethical in this setting, yet data collection can still be “very conscientious and intentional,” with a focus on policy-shaping outcome metrics like immunizations and pediatric health care visits.
“The main point is thinking about it at the forefront, and not retrospectively,” Dr. Lakshmanan said.
Dr. Ogunwole, who led the present review, suggested in a written comment that future studies “could employ robust statistical methods (propensity matching, fixed effects models, etc.) to help reduce bias.”
She also recommended evaluating innovations in WIC programs; for example, adding a health coach, or conducting a cooking skills intervention.
Studies are also needed to better understand the various obstacles to WIC success, such as misconceptions about the program, discrimination, and barriers to enrollment, Dr. Ogunwole added.
“WIC enrollment has been decreasing for a number of years, and this was occurring prepandemic as well,” she said. “More work needs to be done to understand this issue.”
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators and interviewees disclosed no conflicts of interest.
How exactly the national program achieves these outcomes, however, remains unclear, and study quality shows room for improvement, reported co–lead authors Maya Venkataramani, MD, MPH and S. Michelle Ogunwole, MD, PhD of Johns Hopkins University, Baltimore, and colleagues.
The WIC program, which has been serving low-income women and young children since 1974, “provides supplemental foods, nutrition education and breastfeeding support, screening and referrals to medical and social services, and support for high-risk pregnancies,” the investigators wrote in Annals of Internal Medicine. The U.S. Food and Nutrition Service administers the program.
The authors conducted a systematic review of 20 observational studies aimed at determining the impacts of WIC participation on maternal, neonatal-birth, and infant-child health outcomes.
All studies included in the review began in or after 2009, when the WIC food package was revised to better address diet-related chronic diseases. For inclusion in the review, studies were required to have a WIC-eligible comparison group. Included research also evaluated the relationship between WIC participation and the prespecified health outcomes.
“We found only 20 studies that fulfilled our rigorous study inclusion criteria for these specific outcomes,” the investigators wrote. “In some areas, the evidence was absent, and in others, the strength of evidence (SOE) was moderate or low.”
Six outcome categories were assessed: maternal morbidity, maternal pregnancy outcomes, maternal health behaviors, maternal health care utilization, child morbidity, and childhood health care utilization. Of these, maternal health care utilization had the most robust body of evidence, while data from studies evaluating maternal morbidity and child morbidity were deemed insufficient.
Based on eligible studies, WIC participation was associated with reduced risks of insufficient weight gain in pregnancy, preterm birth, low infant birthweight, and infant mortality. Participation was also associated with an increased likelihood of infant and child health care utilization, such as routine immunizations.
Growing evidence should drive enrollment
“Growing evidence points to WIC as a way to reduce risk of preterm birth and other adverse outcomes,” said Laura Jelliffe-Pawlowski, PhD, MS, professor at the University of California, San Francisco and a director for the UCSF California Preterm Birth Initiative.
Dr. Jelliffe-Pawlowski, who conducted a California-based study included in the paper, said the review is noteworthy because it shows that WIC-associated benefits are observed across locations.
“It’s not just in California; it’s across the country,” she said. “It’s a national call to action – where there’s partnership between national-, state- and community-level WIC programs – to make WIC as accessible as possible, and reflect community wants and needs, so that more people enroll, and more people stay enrolled.”
Dr. Jelliffe-Pawlowski’s coauthor on the California study, Rita Hamad, MD, PhD, associate professor of family & community medicine at UCSF and associate director of the UCSF Center for Health Equity, encouraged health care providers to drive WIC enrollment, noting that, presently, only one in four eligible 4-year-olds participates.
“Physicians and other health care stakeholders can help patients benefit from this program by encouraging them to sign up, and even by providing sign-up support in the form of a social worker or other staff member,” Dr. Hamad said. “There is also literature on the types of interventions that improve take-up of safety net programs that providers can look to.”
Goals of future research
Optimizing WIC operations, however, is only half the battle, considering the evidence gaps revealed by the review.
“We still need stronger studies that use more rigorous study designs ... to provide more convincing evidence to policymakers, as well as more evidence on long-term impacts,” Dr. Hamad said. “We also need to better understand why take-up is low in these programs despite these potential health benefits. Then we can make sure that economically disadvantaged families receive the benefits for which they are eligible through interventions to improve participation rates.”
Ideally, WIC programs would receive additional funding for independent parties to evaluate health outcomes, according to Ashwini Lakshmanan, MD, MS, MPH, associate professor in the department of health systems science at Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, Calif.
Dr. Lakshmanan, who previously evaluated the benefits of WIC participation for high-risk infants, noted that randomized clinical trials would be unethical in this setting, yet data collection can still be “very conscientious and intentional,” with a focus on policy-shaping outcome metrics like immunizations and pediatric health care visits.
“The main point is thinking about it at the forefront, and not retrospectively,” Dr. Lakshmanan said.
Dr. Ogunwole, who led the present review, suggested in a written comment that future studies “could employ robust statistical methods (propensity matching, fixed effects models, etc.) to help reduce bias.”
She also recommended evaluating innovations in WIC programs; for example, adding a health coach, or conducting a cooking skills intervention.
Studies are also needed to better understand the various obstacles to WIC success, such as misconceptions about the program, discrimination, and barriers to enrollment, Dr. Ogunwole added.
“WIC enrollment has been decreasing for a number of years, and this was occurring prepandemic as well,” she said. “More work needs to be done to understand this issue.”
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators and interviewees disclosed no conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Abbott to start making Similac baby formula again
Abbott Nutrition is resuming production of Similac, its leading baby formula, at a Michigan plant that was shut down earlier in 2022 because of contamination concerns.
The company closed the plant in February, which triggered a national shortage of baby formula amid pandemic-related supply chain issues that created a lack of formula ingredients.
“We know that the nationwide infant formula shortage has been difficult for the families we serve, and while restarting Similac production in Michigan is an important milestone, we won’t rest until this product is back on shelves,” Robert Ford, chairman and CEO of Abbott, said in a statement on Aug. 26.
“Making infant formula is a responsibility we take very seriously, and parents can feel confident in the quality and safety of Similac and other Abbott formulas,” he said. “We are committed to re-earning the trust parents and health care providers have placed in us for decades.”
Abbott estimated that it will take about 6 weeks for Similac products to ship to stores. Production has restarted, which will be followed by “enhanced” testing before and after the formula is made.
In February, Abbott voluntarily recalled batches of three formulas after the Food and Drug Administration received consumer complaints about infants becoming sick. Four babies who consumed formulas from the Michigan plant got bacterial infections, and at least two babies died.
The illnesses were linked to Cronobacter sakazakii – bacteria that can lead to life-threatening infections and inflammation of the brain and spine.
After investigations at the plant, Abbott said there is no conclusive evidence to link the formula to the illnesses. No samples of the recalled product tested positive for the bacteria, and in all four cases, unopened containers of formula in the infants’ homes tested negative for the bacteria.
At the same time, FDA officials said in May that the Michigan plant had a leaking roof, water pooling on the floor, and cracks in production equipment that could allow bacteria to grow, according to The New York Times.
Abbott agreed with the federal government to create new safeguards, such as hiring a qualified expert to oversee improvements at the plant and notify the FDA if any issues were identified, the newspaper reported.
On July 1, the company restarted production of EleCare, a specialty formula, and later resumed production of some metabolic formulas. These products will begin to ship in coming weeks, the company said.
Since July, C. sakazakii has been found in a couple of batches of formula.
“In those cases, we found the issue, addressed it and no affected product has been or will be distributed,” Abbott said in the statement. “This confirms our quality systems work.”
In August, Abbott will supply the United States with more than 8 million pounds of infant formula, which is higher than the levels in August 2021, the company said. To ensure that people in the federal Special Supplemental Nutrition Program for Women, Infants and Children have access to formula, the company is extending rebates until the end of October.
“Restarting a large manufacturing facility after a several-month shutdown is a complex process, and it takes time to ensure that equipment, processes and production are functioning smoothly and sustainably,” the company said in the statement. “There have been – and likely will be – stops and starts from time to time. We’ve experienced events like severe weather, we’ve had to make mechanical adjustments, and we’ve had to discard some early production batches that didn’t meet our standards.”
A version of this article first appeared on WebMD.com.
Abbott Nutrition is resuming production of Similac, its leading baby formula, at a Michigan plant that was shut down earlier in 2022 because of contamination concerns.
The company closed the plant in February, which triggered a national shortage of baby formula amid pandemic-related supply chain issues that created a lack of formula ingredients.
“We know that the nationwide infant formula shortage has been difficult for the families we serve, and while restarting Similac production in Michigan is an important milestone, we won’t rest until this product is back on shelves,” Robert Ford, chairman and CEO of Abbott, said in a statement on Aug. 26.
“Making infant formula is a responsibility we take very seriously, and parents can feel confident in the quality and safety of Similac and other Abbott formulas,” he said. “We are committed to re-earning the trust parents and health care providers have placed in us for decades.”
Abbott estimated that it will take about 6 weeks for Similac products to ship to stores. Production has restarted, which will be followed by “enhanced” testing before and after the formula is made.
In February, Abbott voluntarily recalled batches of three formulas after the Food and Drug Administration received consumer complaints about infants becoming sick. Four babies who consumed formulas from the Michigan plant got bacterial infections, and at least two babies died.
The illnesses were linked to Cronobacter sakazakii – bacteria that can lead to life-threatening infections and inflammation of the brain and spine.
After investigations at the plant, Abbott said there is no conclusive evidence to link the formula to the illnesses. No samples of the recalled product tested positive for the bacteria, and in all four cases, unopened containers of formula in the infants’ homes tested negative for the bacteria.
At the same time, FDA officials said in May that the Michigan plant had a leaking roof, water pooling on the floor, and cracks in production equipment that could allow bacteria to grow, according to The New York Times.
Abbott agreed with the federal government to create new safeguards, such as hiring a qualified expert to oversee improvements at the plant and notify the FDA if any issues were identified, the newspaper reported.
On July 1, the company restarted production of EleCare, a specialty formula, and later resumed production of some metabolic formulas. These products will begin to ship in coming weeks, the company said.
Since July, C. sakazakii has been found in a couple of batches of formula.
“In those cases, we found the issue, addressed it and no affected product has been or will be distributed,” Abbott said in the statement. “This confirms our quality systems work.”
In August, Abbott will supply the United States with more than 8 million pounds of infant formula, which is higher than the levels in August 2021, the company said. To ensure that people in the federal Special Supplemental Nutrition Program for Women, Infants and Children have access to formula, the company is extending rebates until the end of October.
“Restarting a large manufacturing facility after a several-month shutdown is a complex process, and it takes time to ensure that equipment, processes and production are functioning smoothly and sustainably,” the company said in the statement. “There have been – and likely will be – stops and starts from time to time. We’ve experienced events like severe weather, we’ve had to make mechanical adjustments, and we’ve had to discard some early production batches that didn’t meet our standards.”
A version of this article first appeared on WebMD.com.
Abbott Nutrition is resuming production of Similac, its leading baby formula, at a Michigan plant that was shut down earlier in 2022 because of contamination concerns.
The company closed the plant in February, which triggered a national shortage of baby formula amid pandemic-related supply chain issues that created a lack of formula ingredients.
“We know that the nationwide infant formula shortage has been difficult for the families we serve, and while restarting Similac production in Michigan is an important milestone, we won’t rest until this product is back on shelves,” Robert Ford, chairman and CEO of Abbott, said in a statement on Aug. 26.
“Making infant formula is a responsibility we take very seriously, and parents can feel confident in the quality and safety of Similac and other Abbott formulas,” he said. “We are committed to re-earning the trust parents and health care providers have placed in us for decades.”
Abbott estimated that it will take about 6 weeks for Similac products to ship to stores. Production has restarted, which will be followed by “enhanced” testing before and after the formula is made.
In February, Abbott voluntarily recalled batches of three formulas after the Food and Drug Administration received consumer complaints about infants becoming sick. Four babies who consumed formulas from the Michigan plant got bacterial infections, and at least two babies died.
The illnesses were linked to Cronobacter sakazakii – bacteria that can lead to life-threatening infections and inflammation of the brain and spine.
After investigations at the plant, Abbott said there is no conclusive evidence to link the formula to the illnesses. No samples of the recalled product tested positive for the bacteria, and in all four cases, unopened containers of formula in the infants’ homes tested negative for the bacteria.
At the same time, FDA officials said in May that the Michigan plant had a leaking roof, water pooling on the floor, and cracks in production equipment that could allow bacteria to grow, according to The New York Times.
Abbott agreed with the federal government to create new safeguards, such as hiring a qualified expert to oversee improvements at the plant and notify the FDA if any issues were identified, the newspaper reported.
On July 1, the company restarted production of EleCare, a specialty formula, and later resumed production of some metabolic formulas. These products will begin to ship in coming weeks, the company said.
Since July, C. sakazakii has been found in a couple of batches of formula.
“In those cases, we found the issue, addressed it and no affected product has been or will be distributed,” Abbott said in the statement. “This confirms our quality systems work.”
In August, Abbott will supply the United States with more than 8 million pounds of infant formula, which is higher than the levels in August 2021, the company said. To ensure that people in the federal Special Supplemental Nutrition Program for Women, Infants and Children have access to formula, the company is extending rebates until the end of October.
“Restarting a large manufacturing facility after a several-month shutdown is a complex process, and it takes time to ensure that equipment, processes and production are functioning smoothly and sustainably,” the company said in the statement. “There have been – and likely will be – stops and starts from time to time. We’ve experienced events like severe weather, we’ve had to make mechanical adjustments, and we’ve had to discard some early production batches that didn’t meet our standards.”
A version of this article first appeared on WebMD.com.
Medicare drug changes ought to benefit rheumatology patients
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.

But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.
But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.
But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
How do you live with COVID? One doctor’s personal experience
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Kicking the can
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.
For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.
For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.
For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Infographic: Is physician behavior on social media really so bad?
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
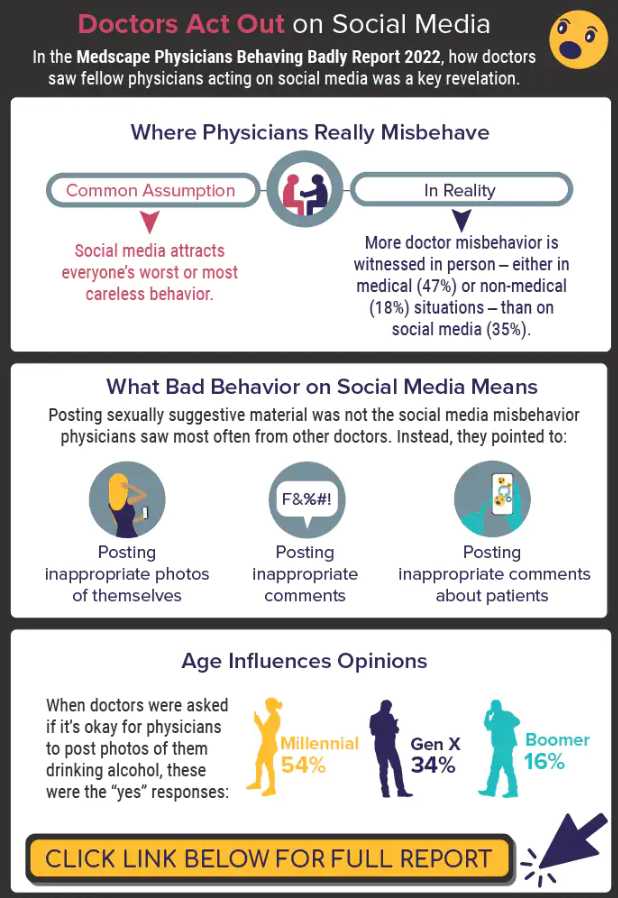
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.