User login
ASTRO Releases New EBRT Guideline for Symptomatic Bone Mets
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
The guideline was needed to update previous recommendations and incorporate new high-quality evidence for the management of symptomatic bone metastases, Sara Alcorn, MD, PhD, of the University of Minnesota, Minneapolis, and colleagues wrote in Practical Radiation Oncology.
The focus was on the efficacy of EBRT in reducing pain, improving skeletal function, and enhancing quality of life, they wrote in the clinical practice guideline.
In developing their recommendations, the ASTRO task force reviewed evidence from 53 randomized controlled trials (RCTs) and 31 nonrandomized studies, and considered clinical experience.
Indications for Palliative Radiation
EBRT is strongly recommended for reducing pain from osseous metastasis and improving ambulatory status, sphincter function, and reducing pain in patients with spinal metastases causing compression of the spinal cord or cauda equina.
For patients with symptomatic bone metastases and an anticipated life expectancy of at least 4 weeks, EBRT is conditionally recommended to improve quality of life.
Implementation of other Treatments Alongside Palliative Radiation
Instead of RT alone, surgery with postoperative RT is conditionally recommended for patients with compression of the spinal cord or cauda equina.
Postoperative RT is strongly recommended for patients who have undergone surgery for non-spine bone metastases or spine metastases without involving spinal cord or cauda equina compression.
For patients with spinal bone metastases compressing the spinal cord or cauda equina, combining RT with dexamethasone is strongly recommended over RT alone.
Techniques, Dose-Fractionation, and Dose-Constraints for Initial Palliative Radiation
For patients with symptomatic bone metastases undergoing conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 3000 cGy in 10 fractions.
For patients with spinal bone metastases causing compression of the spinal cord or cauda equina who are not candidates for initial surgical decompression and are treated with conventional palliative RT, strongly recommended doses are 800 cGy in 1 fraction, 1600 cGy in 2 fractions, 2000 cGy in 5 fractions, or 3000 cGy in 10 fractions.
When selecting dose-fractionation, consider patient and disease factors such as prognosis and radiosensitivity, the authors wrote.
Highly conformal planning and delivery techniques, such as intensity-modulated radiation therapy, are conditionally recommended for patients with spinal bone metastases compressing the spinal cord or cauda equina who are receiving dose-escalated palliative RT.
The strongly recommended stereotactic body radiotherapy (SBRT) doses for patients with symptomatic bone metastases are 1200 to 1600 cGy in 1 fraction for non-spine metastases and 2400 cGy in 2 fractions for spine metastases. Other established SBRT dose and fractionation regimens with similar biologically effective doses may be considered based on patient tumor characteristics, normal tissue factors, and physician experience.
For patients with symptomatic bone metastases who have an ECOG PS of 0-2, are not undergoing surgical intervention, and have no neurological symptoms, SBRT is conditionally recommended over conventional palliative RT. Other factors to consider include life expectancy, tumor radiosensitivity, and metastatic disease burden, the guideline says.
Techniques, Dose-Fractionation, and Dose-Constraints for Palliative Reirradiation
For patients with spinal bone metastases requiring reirradiation to the same site, the strongly recommended conventional palliative RT regimens are 800 cGy in 1 fraction, 2000 cGy in 5 fractions, 2400 cGy in 6 fractions, or 2000 cGy in 8 fractions. When determining the RT dose-fractionation, consider the prior RT dose, time interval, and total spinal cord tolerance, the guideline says.
Treatment with SBRT is conditionally recommended for patients with spinal bone metastases needing reirradiation at the same site. When determining if SBRT is appropriate, consider patient factors such as urgency of treatment, prognosis, and radio-resistance. In addition, consider the prior RT dose, time interval, and total spinal cord tolerance when determining the RT dose-fractionation, the authors say.
The strongly recommended options for patients with symptomatic non-spine bone metastases needing reirradiation at the same site are single-fraction RT (800 cGy in 1 fraction) or multifraction conventional palliative RT (2000 cGy in 5 fractions or 2400 cGy in 6 fractions).
Impact of Techniques and Dose-fractionation on Quality of Life and Toxicity
For patients with bone metastases undergoing palliative radiation, it is strongly recommended to use a shared decision-making approach to determine the dose, fractionation, and supportive measures to optimize quality of life.
“Based on published data, the ASTRO task force’s recommendations inform best clinical practices on palliative RT for symptomatic bone metastases,” the guideline panelists said.
Limitations
While the guideline provides comprehensive recommendations, the panelists underscored the importance of individualized treatment approaches. Future research is needed to address gaps in evidence, particularly regarding advanced RT techniques and reirradiation strategies.
Guideline development was funded by ASTRO, with the systematic evidence review funded by the Patient-Centered Outcomes Research Institute. The panelists disclosed relationships with AstraZeneca, Elekta, Teladoc, and others.
FROM PRACTICAL RADIATION ONCOLOGY
Clinicians Face Hurdles in Caring for the Growing Number of Cancer Survivors
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SGIM 2024
Obesity and Cancer: Untangling a Complex Web
According to the Centers for Disease Control and Prevention (CDC), over 684,000 Americans are diagnosed with an “obesity-associated” cancer each year.
The incidence of many of these cancers has been rising in recent years, particularly among younger people — a trend that sits in contrast with the overall decline in cancers with no established relationship to excess weight, such as lung and skin cancers.
Is obesity the new smoking? Not exactly.
While about 42% of cancers — including common ones such as colorectal and postmenopausal breast cancers — are considered obesity-related, only about 8% of incident cancers are attributed to excess body weight. People often develop those diseases regardless of weight.
Although plenty of evidence points to excess body fat as a cancer risk factor, it’s unclear at what point excess weight has an effect. Is gaining weight later in life, for instance, better or worse for cancer risk than being overweight or obese from a young age?
There’s another glaring knowledge gap: Does losing weight at some point in adulthood change the picture? In other words, how many of those 684,000 diagnoses might have been prevented if people shed excess pounds?
When it comes to weight and cancer risk, “there’s a lot we don’t know,” said Jennifer W. Bea, PhD, associate professor, health promotion sciences, University of Arizona, Tucson.
A Consistent but Complicated Relationship
Given the growing incidence of obesity — which currently affects about 42% of US adults and 20% of children and teenagers — it’s no surprise that many studies have delved into the potential effects of excess weight on cancer rates.
Although virtually all the evidence comes from large cohort studies, leaving the cause-effect question open, certain associations keep showing up.
“What we know is that, consistently, a higher body mass index [BMI] — particularly in the obese category — leads to a higher risk of multiple cancers,” said Jeffrey A. Meyerhardt, MD, MPH, codirector, Colon and Rectal Cancer Center, Dana-Farber Cancer Institute, Boston.
In a widely cited report published in The New England Journal of Medicine in 2016, the International Agency for Research on Cancer (IARC) analyzed over 1000 epidemiologic studies on body fat and cancer. The agency pointed to over a dozen cancers, including some of the most common and deadly, linked to excess body weight.
That list includes esophageal adenocarcinoma and endometrial cancer — associated with the highest risk — along with kidney, liver, stomach (gastric cardia), pancreatic, colorectal, postmenopausal breast, gallbladder, ovarian, and thyroid cancers, plus multiple myeloma and meningioma. There’s also “limited” evidence linking excess weight to additional cancer types, including aggressive prostate cancer and certain head and neck cancers.
At the same time, Dr. Meyerhardt said, many of those same cancers are also associated with issues that lead to, or coexist with, overweight and obesity, including poor diet, lack of exercise, and metabolic conditions such as diabetes.
It’s a complicated web, and it’s likely, Dr. Meyerhardt said, that high BMI both directly affects cancer risk and is part of a “causal pathway” of other factors that do.
Regarding direct effects, preclinical research has pointed to multiple ways in which excess body fat could contribute to cancer, said Karen M. Basen-Engquist, PhD, MPH, professor, Division of Cancer Prevention and Population Services, The University of Texas MD Anderson Cancer Center, Houston.
One broad mechanism to help explain the obesity-cancer link is chronic systemic inflammation because excess fat tissue can raise levels of substances in the body, such as tumor necrosis factor alpha and interleukin 6, which fuel inflammation. Excess fat also contributes to hyperinsulinemia — too much insulin in the blood — which can help promote the growth and spread of tumor cells.
But the underlying reasons also appear to vary by cancer type, Dr. Basen-Engquist said. With hormonally driven cancer types, such as breast and endometrial, excess body fat may alter hormone levels in ways that spur tumor growth. Extra fat tissue may, for example, convert androgens into estrogens, which could help feed estrogen-dependent tumors.
That, Dr. Basen-Engquist noted, could be why excess weight is associated with postmenopausal, not premenopausal, breast cancer: Before menopause, body fat is a relatively minor contributor to estrogen levels but becomes more important after menopause.
How Big Is the Effect?
While more than a dozen cancers have been consistently linked to excess weight, the strength of those associations varies considerably.
Endometrial and esophageal cancers are two that stand out. In the 2016 IARC analysis, people with severe obesity had a seven-times greater risk for endometrial cancer and 4.8-times greater risk for esophageal adenocarcinoma vs people with a normal BMI.
With other cancers, the risk increases for those with severe obesity compared with a normal BMI were far more modest: 10% for ovarian cancer, 30% for colorectal cancer, and 80% for kidney and stomach cancers, for example. For postmenopausal breast cancer, every five-unit increase in BMI was associated with a 10% relative risk increase.
A 2018 study from the American Cancer Society, which attempted to estimate the proportion of cancers in the United States attributable to modifiable risk factors — including alcohol consumption, ultraviolet rays exposure, and physical inactivity — found that smoking accounted for the highest proportion of cancer cases by a wide margin (19%), but excess weight came in second (7.8%).
Again, weight appeared to play a bigger role in certain cancers than others: An estimated 60% of endometrial cancers were linked to excess weight, as were roughly one third of esophageal, kidney, and liver cancers. At the other end of the spectrum, just over 11% of breast, 5% of colorectal, and 4% of ovarian cancers were attributable to excess weight.
Even at the lower end, those rates could make a big difference on the population level, especially for groups with higher rates of obesity.
CDC data show that obesity-related cancers are rising among women younger than 50 years, most rapidly among Hispanic women, and some less common obesity-related cancers, such as stomach, thyroid and pancreatic, are also rising among Black individuals and Hispanic Americans.
Obesity may be one reason for growing cancer disparities, said Leah Ferrucci, PhD, MPH, assistant professor, epidemiology, Yale School of Public Health, New Haven, Connecticut. But, she added, the evidence is limited because Black individuals and Hispanic Americans are understudied.
When Do Extra Pounds Matter?
When it comes to cancer risk, at what point in life does excess weight, or weight gain, matter? Is the standard weight gain in middle age, for instance, as hazardous as being overweight or obese from a young age?
Some evidence suggests there’s no “safe” time for putting on excess pounds.
A recent meta-analysis concluded that weight gain at any point after age 18 years is associated with incremental increases in the risk for postmenopausal breast cancer. A 2023 study in JAMA Network Open found a similar pattern with colorectal and other gastrointestinal cancers: People who had sustained overweight or obesity from age 20 years through middle age faced an increased risk of developing those cancers after age 55 years.
The timing of weight gain didn’t seem to matter either. The same elevated risk held among people who were normal weight in their younger years but became overweight after age 55 years.
Those studies focused on later-onset disease. But, in recent years, experts have tracked a troubling rise in early-onset cancers — those diagnosed before age 50 years — particularly gastrointestinal cancers.
An obvious question, Dr. Meyerhardt said, is whether the growing prevalence of obesity among young people is partly to blame.
There’s some data to support that, he said. An analysis from the Nurses’ Health Study II found that women with obesity had double the risk for early-onset colorectal cancer as those with a normal BMI. And every 5-kg increase in weight after age 18 years was associated with a 9% increase in colorectal cancer risk.
But while obesity trends probably partly explain the rise in early-onset cancers, there is likely more to the story, Dr. Meyerhardt said.
“I think all of us who see an increasing number of patients under 50 with colorectal cancer know there’s a fair number who do not fit that [high BMI] profile,” he said. “There’s a fair number over 50 who don’t either.”
Does Weight Loss Help?
With all the evidence pointing to high BMI as a cancer risk factor, a logical conclusion is that weight loss should reduce that excess risk. However, Dr. Bea said, there’s actually little data to support that, and what exists comes from observational studies.
Some research has focused on people who had substantial weight loss after bariatric surgery, with encouraging results. A study published in JAMA found that among 5053 people who underwent bariatric surgery, 2.9% developed an obesity-related cancer over 10 years compared with 4.9% in the nonsurgery group.
Most people, however, aim for less dramatic weight loss, with the help of diet and exercise or sometimes medication. Some evidence shows that a modest degree of weight loss may lower the risks for postmenopausal breast and endometrial cancers.
A 2020 pooled analysis found, for instance, that among women aged ≥ 50 years, those who lost as little as 2.0-4.5 kg, or 4.4-10.0 pounds, and kept it off for 10 years had a lower risk for breast cancer than women whose weight remained stable. And losing more weight — 9 kg, or about 20 pounds, or more — was even better for lowering cancer risk.
But other research suggests the opposite. A recent analysis found that people who lost weight within the past 2 years through diet and exercise had a higher risk for a range of cancers compared with those who did not lose weight. Overall, though, the increased risk was quite low.
Whatever the research does, or doesn’t, show about weight and cancer risk, Dr. Basen-Engquist said, it’s important that risk factors, obesity and otherwise, aren’t “used as blame tools.”
“With obesity, behavior certainly plays into it,” she said. “But there are so many influences on our behavior that are socially determined.”
Both Dr. Basen-Engquist and Dr. Meyerhardt said it’s important for clinicians to consider the individual in front of them and for everyone to set realistic expectations.
People with obesity should not feel they have to become thin to be healthier, and no one has to leap from being sedentary to exercising several hours a week.
“We don’t want patients to feel that if they don’t get to a stated goal in a guideline, it’s all for naught,” Dr. Meyerhardt said.
A version of this article appeared on Medscape.com.
According to the Centers for Disease Control and Prevention (CDC), over 684,000 Americans are diagnosed with an “obesity-associated” cancer each year.
The incidence of many of these cancers has been rising in recent years, particularly among younger people — a trend that sits in contrast with the overall decline in cancers with no established relationship to excess weight, such as lung and skin cancers.
Is obesity the new smoking? Not exactly.
While about 42% of cancers — including common ones such as colorectal and postmenopausal breast cancers — are considered obesity-related, only about 8% of incident cancers are attributed to excess body weight. People often develop those diseases regardless of weight.
Although plenty of evidence points to excess body fat as a cancer risk factor, it’s unclear at what point excess weight has an effect. Is gaining weight later in life, for instance, better or worse for cancer risk than being overweight or obese from a young age?
There’s another glaring knowledge gap: Does losing weight at some point in adulthood change the picture? In other words, how many of those 684,000 diagnoses might have been prevented if people shed excess pounds?
When it comes to weight and cancer risk, “there’s a lot we don’t know,” said Jennifer W. Bea, PhD, associate professor, health promotion sciences, University of Arizona, Tucson.
A Consistent but Complicated Relationship
Given the growing incidence of obesity — which currently affects about 42% of US adults and 20% of children and teenagers — it’s no surprise that many studies have delved into the potential effects of excess weight on cancer rates.
Although virtually all the evidence comes from large cohort studies, leaving the cause-effect question open, certain associations keep showing up.
“What we know is that, consistently, a higher body mass index [BMI] — particularly in the obese category — leads to a higher risk of multiple cancers,” said Jeffrey A. Meyerhardt, MD, MPH, codirector, Colon and Rectal Cancer Center, Dana-Farber Cancer Institute, Boston.
In a widely cited report published in The New England Journal of Medicine in 2016, the International Agency for Research on Cancer (IARC) analyzed over 1000 epidemiologic studies on body fat and cancer. The agency pointed to over a dozen cancers, including some of the most common and deadly, linked to excess body weight.
That list includes esophageal adenocarcinoma and endometrial cancer — associated with the highest risk — along with kidney, liver, stomach (gastric cardia), pancreatic, colorectal, postmenopausal breast, gallbladder, ovarian, and thyroid cancers, plus multiple myeloma and meningioma. There’s also “limited” evidence linking excess weight to additional cancer types, including aggressive prostate cancer and certain head and neck cancers.
At the same time, Dr. Meyerhardt said, many of those same cancers are also associated with issues that lead to, or coexist with, overweight and obesity, including poor diet, lack of exercise, and metabolic conditions such as diabetes.
It’s a complicated web, and it’s likely, Dr. Meyerhardt said, that high BMI both directly affects cancer risk and is part of a “causal pathway” of other factors that do.
Regarding direct effects, preclinical research has pointed to multiple ways in which excess body fat could contribute to cancer, said Karen M. Basen-Engquist, PhD, MPH, professor, Division of Cancer Prevention and Population Services, The University of Texas MD Anderson Cancer Center, Houston.
One broad mechanism to help explain the obesity-cancer link is chronic systemic inflammation because excess fat tissue can raise levels of substances in the body, such as tumor necrosis factor alpha and interleukin 6, which fuel inflammation. Excess fat also contributes to hyperinsulinemia — too much insulin in the blood — which can help promote the growth and spread of tumor cells.
But the underlying reasons also appear to vary by cancer type, Dr. Basen-Engquist said. With hormonally driven cancer types, such as breast and endometrial, excess body fat may alter hormone levels in ways that spur tumor growth. Extra fat tissue may, for example, convert androgens into estrogens, which could help feed estrogen-dependent tumors.
That, Dr. Basen-Engquist noted, could be why excess weight is associated with postmenopausal, not premenopausal, breast cancer: Before menopause, body fat is a relatively minor contributor to estrogen levels but becomes more important after menopause.
How Big Is the Effect?
While more than a dozen cancers have been consistently linked to excess weight, the strength of those associations varies considerably.
Endometrial and esophageal cancers are two that stand out. In the 2016 IARC analysis, people with severe obesity had a seven-times greater risk for endometrial cancer and 4.8-times greater risk for esophageal adenocarcinoma vs people with a normal BMI.
With other cancers, the risk increases for those with severe obesity compared with a normal BMI were far more modest: 10% for ovarian cancer, 30% for colorectal cancer, and 80% for kidney and stomach cancers, for example. For postmenopausal breast cancer, every five-unit increase in BMI was associated with a 10% relative risk increase.
A 2018 study from the American Cancer Society, which attempted to estimate the proportion of cancers in the United States attributable to modifiable risk factors — including alcohol consumption, ultraviolet rays exposure, and physical inactivity — found that smoking accounted for the highest proportion of cancer cases by a wide margin (19%), but excess weight came in second (7.8%).
Again, weight appeared to play a bigger role in certain cancers than others: An estimated 60% of endometrial cancers were linked to excess weight, as were roughly one third of esophageal, kidney, and liver cancers. At the other end of the spectrum, just over 11% of breast, 5% of colorectal, and 4% of ovarian cancers were attributable to excess weight.
Even at the lower end, those rates could make a big difference on the population level, especially for groups with higher rates of obesity.
CDC data show that obesity-related cancers are rising among women younger than 50 years, most rapidly among Hispanic women, and some less common obesity-related cancers, such as stomach, thyroid and pancreatic, are also rising among Black individuals and Hispanic Americans.
Obesity may be one reason for growing cancer disparities, said Leah Ferrucci, PhD, MPH, assistant professor, epidemiology, Yale School of Public Health, New Haven, Connecticut. But, she added, the evidence is limited because Black individuals and Hispanic Americans are understudied.
When Do Extra Pounds Matter?
When it comes to cancer risk, at what point in life does excess weight, or weight gain, matter? Is the standard weight gain in middle age, for instance, as hazardous as being overweight or obese from a young age?
Some evidence suggests there’s no “safe” time for putting on excess pounds.
A recent meta-analysis concluded that weight gain at any point after age 18 years is associated with incremental increases in the risk for postmenopausal breast cancer. A 2023 study in JAMA Network Open found a similar pattern with colorectal and other gastrointestinal cancers: People who had sustained overweight or obesity from age 20 years through middle age faced an increased risk of developing those cancers after age 55 years.
The timing of weight gain didn’t seem to matter either. The same elevated risk held among people who were normal weight in their younger years but became overweight after age 55 years.
Those studies focused on later-onset disease. But, in recent years, experts have tracked a troubling rise in early-onset cancers — those diagnosed before age 50 years — particularly gastrointestinal cancers.
An obvious question, Dr. Meyerhardt said, is whether the growing prevalence of obesity among young people is partly to blame.
There’s some data to support that, he said. An analysis from the Nurses’ Health Study II found that women with obesity had double the risk for early-onset colorectal cancer as those with a normal BMI. And every 5-kg increase in weight after age 18 years was associated with a 9% increase in colorectal cancer risk.
But while obesity trends probably partly explain the rise in early-onset cancers, there is likely more to the story, Dr. Meyerhardt said.
“I think all of us who see an increasing number of patients under 50 with colorectal cancer know there’s a fair number who do not fit that [high BMI] profile,” he said. “There’s a fair number over 50 who don’t either.”
Does Weight Loss Help?
With all the evidence pointing to high BMI as a cancer risk factor, a logical conclusion is that weight loss should reduce that excess risk. However, Dr. Bea said, there’s actually little data to support that, and what exists comes from observational studies.
Some research has focused on people who had substantial weight loss after bariatric surgery, with encouraging results. A study published in JAMA found that among 5053 people who underwent bariatric surgery, 2.9% developed an obesity-related cancer over 10 years compared with 4.9% in the nonsurgery group.
Most people, however, aim for less dramatic weight loss, with the help of diet and exercise or sometimes medication. Some evidence shows that a modest degree of weight loss may lower the risks for postmenopausal breast and endometrial cancers.
A 2020 pooled analysis found, for instance, that among women aged ≥ 50 years, those who lost as little as 2.0-4.5 kg, or 4.4-10.0 pounds, and kept it off for 10 years had a lower risk for breast cancer than women whose weight remained stable. And losing more weight — 9 kg, or about 20 pounds, or more — was even better for lowering cancer risk.
But other research suggests the opposite. A recent analysis found that people who lost weight within the past 2 years through diet and exercise had a higher risk for a range of cancers compared with those who did not lose weight. Overall, though, the increased risk was quite low.
Whatever the research does, or doesn’t, show about weight and cancer risk, Dr. Basen-Engquist said, it’s important that risk factors, obesity and otherwise, aren’t “used as blame tools.”
“With obesity, behavior certainly plays into it,” she said. “But there are so many influences on our behavior that are socially determined.”
Both Dr. Basen-Engquist and Dr. Meyerhardt said it’s important for clinicians to consider the individual in front of them and for everyone to set realistic expectations.
People with obesity should not feel they have to become thin to be healthier, and no one has to leap from being sedentary to exercising several hours a week.
“We don’t want patients to feel that if they don’t get to a stated goal in a guideline, it’s all for naught,” Dr. Meyerhardt said.
A version of this article appeared on Medscape.com.
According to the Centers for Disease Control and Prevention (CDC), over 684,000 Americans are diagnosed with an “obesity-associated” cancer each year.
The incidence of many of these cancers has been rising in recent years, particularly among younger people — a trend that sits in contrast with the overall decline in cancers with no established relationship to excess weight, such as lung and skin cancers.
Is obesity the new smoking? Not exactly.
While about 42% of cancers — including common ones such as colorectal and postmenopausal breast cancers — are considered obesity-related, only about 8% of incident cancers are attributed to excess body weight. People often develop those diseases regardless of weight.
Although plenty of evidence points to excess body fat as a cancer risk factor, it’s unclear at what point excess weight has an effect. Is gaining weight later in life, for instance, better or worse for cancer risk than being overweight or obese from a young age?
There’s another glaring knowledge gap: Does losing weight at some point in adulthood change the picture? In other words, how many of those 684,000 diagnoses might have been prevented if people shed excess pounds?
When it comes to weight and cancer risk, “there’s a lot we don’t know,” said Jennifer W. Bea, PhD, associate professor, health promotion sciences, University of Arizona, Tucson.
A Consistent but Complicated Relationship
Given the growing incidence of obesity — which currently affects about 42% of US adults and 20% of children and teenagers — it’s no surprise that many studies have delved into the potential effects of excess weight on cancer rates.
Although virtually all the evidence comes from large cohort studies, leaving the cause-effect question open, certain associations keep showing up.
“What we know is that, consistently, a higher body mass index [BMI] — particularly in the obese category — leads to a higher risk of multiple cancers,” said Jeffrey A. Meyerhardt, MD, MPH, codirector, Colon and Rectal Cancer Center, Dana-Farber Cancer Institute, Boston.
In a widely cited report published in The New England Journal of Medicine in 2016, the International Agency for Research on Cancer (IARC) analyzed over 1000 epidemiologic studies on body fat and cancer. The agency pointed to over a dozen cancers, including some of the most common and deadly, linked to excess body weight.
That list includes esophageal adenocarcinoma and endometrial cancer — associated with the highest risk — along with kidney, liver, stomach (gastric cardia), pancreatic, colorectal, postmenopausal breast, gallbladder, ovarian, and thyroid cancers, plus multiple myeloma and meningioma. There’s also “limited” evidence linking excess weight to additional cancer types, including aggressive prostate cancer and certain head and neck cancers.
At the same time, Dr. Meyerhardt said, many of those same cancers are also associated with issues that lead to, or coexist with, overweight and obesity, including poor diet, lack of exercise, and metabolic conditions such as diabetes.
It’s a complicated web, and it’s likely, Dr. Meyerhardt said, that high BMI both directly affects cancer risk and is part of a “causal pathway” of other factors that do.
Regarding direct effects, preclinical research has pointed to multiple ways in which excess body fat could contribute to cancer, said Karen M. Basen-Engquist, PhD, MPH, professor, Division of Cancer Prevention and Population Services, The University of Texas MD Anderson Cancer Center, Houston.
One broad mechanism to help explain the obesity-cancer link is chronic systemic inflammation because excess fat tissue can raise levels of substances in the body, such as tumor necrosis factor alpha and interleukin 6, which fuel inflammation. Excess fat also contributes to hyperinsulinemia — too much insulin in the blood — which can help promote the growth and spread of tumor cells.
But the underlying reasons also appear to vary by cancer type, Dr. Basen-Engquist said. With hormonally driven cancer types, such as breast and endometrial, excess body fat may alter hormone levels in ways that spur tumor growth. Extra fat tissue may, for example, convert androgens into estrogens, which could help feed estrogen-dependent tumors.
That, Dr. Basen-Engquist noted, could be why excess weight is associated with postmenopausal, not premenopausal, breast cancer: Before menopause, body fat is a relatively minor contributor to estrogen levels but becomes more important after menopause.
How Big Is the Effect?
While more than a dozen cancers have been consistently linked to excess weight, the strength of those associations varies considerably.
Endometrial and esophageal cancers are two that stand out. In the 2016 IARC analysis, people with severe obesity had a seven-times greater risk for endometrial cancer and 4.8-times greater risk for esophageal adenocarcinoma vs people with a normal BMI.
With other cancers, the risk increases for those with severe obesity compared with a normal BMI were far more modest: 10% for ovarian cancer, 30% for colorectal cancer, and 80% for kidney and stomach cancers, for example. For postmenopausal breast cancer, every five-unit increase in BMI was associated with a 10% relative risk increase.
A 2018 study from the American Cancer Society, which attempted to estimate the proportion of cancers in the United States attributable to modifiable risk factors — including alcohol consumption, ultraviolet rays exposure, and physical inactivity — found that smoking accounted for the highest proportion of cancer cases by a wide margin (19%), but excess weight came in second (7.8%).
Again, weight appeared to play a bigger role in certain cancers than others: An estimated 60% of endometrial cancers were linked to excess weight, as were roughly one third of esophageal, kidney, and liver cancers. At the other end of the spectrum, just over 11% of breast, 5% of colorectal, and 4% of ovarian cancers were attributable to excess weight.
Even at the lower end, those rates could make a big difference on the population level, especially for groups with higher rates of obesity.
CDC data show that obesity-related cancers are rising among women younger than 50 years, most rapidly among Hispanic women, and some less common obesity-related cancers, such as stomach, thyroid and pancreatic, are also rising among Black individuals and Hispanic Americans.
Obesity may be one reason for growing cancer disparities, said Leah Ferrucci, PhD, MPH, assistant professor, epidemiology, Yale School of Public Health, New Haven, Connecticut. But, she added, the evidence is limited because Black individuals and Hispanic Americans are understudied.
When Do Extra Pounds Matter?
When it comes to cancer risk, at what point in life does excess weight, or weight gain, matter? Is the standard weight gain in middle age, for instance, as hazardous as being overweight or obese from a young age?
Some evidence suggests there’s no “safe” time for putting on excess pounds.
A recent meta-analysis concluded that weight gain at any point after age 18 years is associated with incremental increases in the risk for postmenopausal breast cancer. A 2023 study in JAMA Network Open found a similar pattern with colorectal and other gastrointestinal cancers: People who had sustained overweight or obesity from age 20 years through middle age faced an increased risk of developing those cancers after age 55 years.
The timing of weight gain didn’t seem to matter either. The same elevated risk held among people who were normal weight in their younger years but became overweight after age 55 years.
Those studies focused on later-onset disease. But, in recent years, experts have tracked a troubling rise in early-onset cancers — those diagnosed before age 50 years — particularly gastrointestinal cancers.
An obvious question, Dr. Meyerhardt said, is whether the growing prevalence of obesity among young people is partly to blame.
There’s some data to support that, he said. An analysis from the Nurses’ Health Study II found that women with obesity had double the risk for early-onset colorectal cancer as those with a normal BMI. And every 5-kg increase in weight after age 18 years was associated with a 9% increase in colorectal cancer risk.
But while obesity trends probably partly explain the rise in early-onset cancers, there is likely more to the story, Dr. Meyerhardt said.
“I think all of us who see an increasing number of patients under 50 with colorectal cancer know there’s a fair number who do not fit that [high BMI] profile,” he said. “There’s a fair number over 50 who don’t either.”
Does Weight Loss Help?
With all the evidence pointing to high BMI as a cancer risk factor, a logical conclusion is that weight loss should reduce that excess risk. However, Dr. Bea said, there’s actually little data to support that, and what exists comes from observational studies.
Some research has focused on people who had substantial weight loss after bariatric surgery, with encouraging results. A study published in JAMA found that among 5053 people who underwent bariatric surgery, 2.9% developed an obesity-related cancer over 10 years compared with 4.9% in the nonsurgery group.
Most people, however, aim for less dramatic weight loss, with the help of diet and exercise or sometimes medication. Some evidence shows that a modest degree of weight loss may lower the risks for postmenopausal breast and endometrial cancers.
A 2020 pooled analysis found, for instance, that among women aged ≥ 50 years, those who lost as little as 2.0-4.5 kg, or 4.4-10.0 pounds, and kept it off for 10 years had a lower risk for breast cancer than women whose weight remained stable. And losing more weight — 9 kg, or about 20 pounds, or more — was even better for lowering cancer risk.
But other research suggests the opposite. A recent analysis found that people who lost weight within the past 2 years through diet and exercise had a higher risk for a range of cancers compared with those who did not lose weight. Overall, though, the increased risk was quite low.
Whatever the research does, or doesn’t, show about weight and cancer risk, Dr. Basen-Engquist said, it’s important that risk factors, obesity and otherwise, aren’t “used as blame tools.”
“With obesity, behavior certainly plays into it,” she said. “But there are so many influences on our behavior that are socially determined.”
Both Dr. Basen-Engquist and Dr. Meyerhardt said it’s important for clinicians to consider the individual in front of them and for everyone to set realistic expectations.
People with obesity should not feel they have to become thin to be healthier, and no one has to leap from being sedentary to exercising several hours a week.
“We don’t want patients to feel that if they don’t get to a stated goal in a guideline, it’s all for naught,” Dr. Meyerhardt said.
A version of this article appeared on Medscape.com.
Urine Tests Could Be ‘Enormous Step’ in Diagnosing Cancer
Emerging science suggests that the body’s “liquid gold” could be particularly useful for liquid biopsies, offering a convenient, pain-free, and cost-effective way to spot otherwise hard-to-detect cancers.
“The search for cancer biomarkers that can be detected in urine could provide an enormous step forward to decrease cancer patient mortality,” said Kenneth R. Shroyer, MD, PhD, a pathologist at Stony Brook University, Stony Brook, New York, who studies cancer biomarkers.
Physicians have long known that urine can reveal a lot about our health — that’s why urinalysis has been part of medicine for 6000 years. Urine tests can detect diabetes, pregnancy, drug use, and urinary or kidney conditions.
But other conditions leave clues in urine, too, and cancer may be one of the most promising. “Urine testing could detect biomarkers of early-stage cancers, not only from local but also distant sites,” Dr. Shroyer said. It could also help flag recurrence in cancer survivors who have undergone treatment.
Granted, cancer biomarkers in urine are not nearly as widely studied as those in the blood, Dr. Shroyer noted. But a new wave of urine tests suggests research is gaining pace.
“The recent availability of high-throughput screening technologies has enabled researchers to investigate cancer from a top-down, comprehensive approach,” said Pak Kin Wong, PhD, professor of mechanical engineering, biomedical engineering, and surgery at The Pennsylvania State University. “We are starting to understand the rich information that can be obtained from urine.”
Urine is mostly water (about 95%) and urea, a metabolic byproduct that imparts that signature yellow color (about 2%). The other 3% is a mix of waste products, minerals, and other compounds the kidneys removed from the blood. Even in trace amounts, these substances say a lot.
Among them are “exfoliated cancer cells, cell-free DNA, hormones, and the urine microbiota — the collection of microbes in our urinary tract system,” Dr. Wong said.
“It is highly promising to be one of the major biological fluids used for screening, diagnosis, prognosis, and monitoring treatment efficiency in the era of precision medicine,” Dr. Wong said.
How Urine Testing Could Reveal Cancer
Still, as exciting as the prospect is, there’s a lot to consider in the hunt for cancer biomarkers in urine. These biomarkers must be able to pass through the renal nephrons (filtering units), remain stable in urine, and have high-level sensitivity, Dr. Shroyer said. They should also have high specificity for cancer vs benign conditions and be expressed at early stages, before the primary tumor has spread.
“At this stage, few circulating biomarkers have been found that are both sensitive and specific for early-stage disease,” said Dr. Shroyer.
But there are a few promising examples under investigation in humans:
Prostate cancer. Researchers at the University of Michigan have developed a urine test that detects high-grade prostate cancer more accurately than existing tests, including PHI, SelectMDx, 4Kscore, EPI, MPS, and IsoPSA.
The MyProstateScore 2.0 (MPS2) test, which looks for 18 genes associated with high-grade tumors, could reduce unnecessary biopsies in men with elevated prostate-specific antigen levels, according to a paper published in JAMA Oncology.
It makes sense. The prostate gland secretes fluid that becomes part of the semen, traces of which enter urine. After a digital rectal exam, even more prostate fluid enters the urine. If a patient has prostate cancer, genetic material from the cancer cells will infiltrate the urine.
In the MPS2 test, researchers used polymerase chain reaction (PCR) testing in urine. “The technology used for COVID PCR is essentially the same as the PCR used to detect transcripts associated with high-grade prostate cancer in urine,” said study author Arul Chinnaiyan, MD, PhD, director of the Michigan Center for Translational Pathology at the University of Michigan, Ann Arbor. “In the case of the MPS2 test, we are doing PCR on 18 genes simultaneously on urine samples.”
A statistical model uses levels of that genetic material to predict the risk for high-grade disease, helping doctors decide what to do next. At 95% sensitivity, the MPS2 model could eliminate 35%-45% of unnecessary biopsies, compared with 15%-30% for the other tests, and reduce repeat biopsies by 46%-51%, compared with 9%-21% for the other tests.
Head and neck cancer. In a paper published in JCI Insight, researchers described a test that finds ultra-short fragments of DNA in urine to enable early detection of head and neck cancers caused by human papillomavirus.
“Our data show that a relatively small volume of urine (30-60 mL) gives overall detection results comparable to a tube of blood,” said study author Muneesh Tewari, MD, PhD, professor of hematology and oncology at the University of Michigan .
A larger volume of urine could potentially “make cancer detection even more sensitive than blood,” Dr. Tewari said, “allowing cancers to be detected at the earliest stages when they are more curable.”
The team used a technique called droplet digital PCR to detect DNA fragments that are “ultra-short” (less than 50 base pairs long) and usually missed by conventional PCR testing. This transrenal cell-free tumor DNA, which travels from the tumor into the bloodstream, is broken down small enough to pass through the kidneys and into the urine. But the fragments are still long enough to carry information about the tumor’s genetic signature.
This test could spot cancer before a tumor grows big enough — about a centimeter wide and carrying a billion cells — to spot on a CT scan or other imaging test. “When we are instead detecting fragments of DNA released from a tumor,” said Dr. Tewari, “our testing methods are very sensitive and can detect DNA in urine that came from just 5-10 cells in a tumor that died and released their DNA into the blood, which then made its way into the urine.”
Pancreatic cancer. Pancreatic ductal adenocarcinoma is one of the deadliest cancers, largely because it is diagnosed so late. A urine panel now in clinical trials could help doctors diagnose the cancer before it has spread so more people can have the tumor surgically removed, improving prognosis.
Using enzyme-linked immunosorbent assay test, a common lab method that detects antibodies and other proteins, the team measured expression levels for three genes (LYVE1, REG1B, and TFF1) in urine samples collected from people up to 5 years before they were diagnosed with pancreatic cancer. The researchers combined this result with patients’ urinary creatinine levels, a common component of existing urinalysis, and their age to develop a risk score.
This score performed similarly to an existing blood test, CA19-9, in predicting patients’ risk for pancreatic cancer up to 1 year before diagnosis. When combined with CA19-9, the urinary panel helped spot cancer up to 2 years before diagnosis.
According to a paper in the International Journal of Cancer, “the urine panel and affiliated PancRISK are currently being validated in a prospective clinical study (UroPanc).” If all goes well, they could be implemented in clinical practice in a few years as a “noninvasive stratification tool” to identify patients for further testing, speeding up diagnosis, and saving lives.
Limitations and Promises
Each cancer type is different, and more research is needed to map out which substances in urine predict which cancers and to develop tests for mass adoption. “There are medical and technological hurdles to the large-scale implementation of urine analysis for complex diseases such as cancer,” said Dr. Wong.
One possibility: Scientists and clinicians could collaborate and use artificial intelligence techniques to combine urine test results with other data.
“It is likely that future diagnostics may combine urine with other biological samples such as feces and saliva, among others,” said Dr. Wong. “This is especially true when novel data science and machine learning techniques can integrate comprehensive data from patients that span genetic, proteomic, metabolic, microbiomic, and even behavioral data to evaluate a patient’s condition.”
One thing that excites Dr. Tewari about urine-based cancer testing: “We think it could be especially impactful for patients living in rural areas or other areas with less access to healthcare services,” he said.
A version of this article appeared on Medscape.com.
Emerging science suggests that the body’s “liquid gold” could be particularly useful for liquid biopsies, offering a convenient, pain-free, and cost-effective way to spot otherwise hard-to-detect cancers.
“The search for cancer biomarkers that can be detected in urine could provide an enormous step forward to decrease cancer patient mortality,” said Kenneth R. Shroyer, MD, PhD, a pathologist at Stony Brook University, Stony Brook, New York, who studies cancer biomarkers.
Physicians have long known that urine can reveal a lot about our health — that’s why urinalysis has been part of medicine for 6000 years. Urine tests can detect diabetes, pregnancy, drug use, and urinary or kidney conditions.
But other conditions leave clues in urine, too, and cancer may be one of the most promising. “Urine testing could detect biomarkers of early-stage cancers, not only from local but also distant sites,” Dr. Shroyer said. It could also help flag recurrence in cancer survivors who have undergone treatment.
Granted, cancer biomarkers in urine are not nearly as widely studied as those in the blood, Dr. Shroyer noted. But a new wave of urine tests suggests research is gaining pace.
“The recent availability of high-throughput screening technologies has enabled researchers to investigate cancer from a top-down, comprehensive approach,” said Pak Kin Wong, PhD, professor of mechanical engineering, biomedical engineering, and surgery at The Pennsylvania State University. “We are starting to understand the rich information that can be obtained from urine.”
Urine is mostly water (about 95%) and urea, a metabolic byproduct that imparts that signature yellow color (about 2%). The other 3% is a mix of waste products, minerals, and other compounds the kidneys removed from the blood. Even in trace amounts, these substances say a lot.
Among them are “exfoliated cancer cells, cell-free DNA, hormones, and the urine microbiota — the collection of microbes in our urinary tract system,” Dr. Wong said.
“It is highly promising to be one of the major biological fluids used for screening, diagnosis, prognosis, and monitoring treatment efficiency in the era of precision medicine,” Dr. Wong said.
How Urine Testing Could Reveal Cancer
Still, as exciting as the prospect is, there’s a lot to consider in the hunt for cancer biomarkers in urine. These biomarkers must be able to pass through the renal nephrons (filtering units), remain stable in urine, and have high-level sensitivity, Dr. Shroyer said. They should also have high specificity for cancer vs benign conditions and be expressed at early stages, before the primary tumor has spread.
“At this stage, few circulating biomarkers have been found that are both sensitive and specific for early-stage disease,” said Dr. Shroyer.
But there are a few promising examples under investigation in humans:
Prostate cancer. Researchers at the University of Michigan have developed a urine test that detects high-grade prostate cancer more accurately than existing tests, including PHI, SelectMDx, 4Kscore, EPI, MPS, and IsoPSA.
The MyProstateScore 2.0 (MPS2) test, which looks for 18 genes associated with high-grade tumors, could reduce unnecessary biopsies in men with elevated prostate-specific antigen levels, according to a paper published in JAMA Oncology.
It makes sense. The prostate gland secretes fluid that becomes part of the semen, traces of which enter urine. After a digital rectal exam, even more prostate fluid enters the urine. If a patient has prostate cancer, genetic material from the cancer cells will infiltrate the urine.
In the MPS2 test, researchers used polymerase chain reaction (PCR) testing in urine. “The technology used for COVID PCR is essentially the same as the PCR used to detect transcripts associated with high-grade prostate cancer in urine,” said study author Arul Chinnaiyan, MD, PhD, director of the Michigan Center for Translational Pathology at the University of Michigan, Ann Arbor. “In the case of the MPS2 test, we are doing PCR on 18 genes simultaneously on urine samples.”
A statistical model uses levels of that genetic material to predict the risk for high-grade disease, helping doctors decide what to do next. At 95% sensitivity, the MPS2 model could eliminate 35%-45% of unnecessary biopsies, compared with 15%-30% for the other tests, and reduce repeat biopsies by 46%-51%, compared with 9%-21% for the other tests.
Head and neck cancer. In a paper published in JCI Insight, researchers described a test that finds ultra-short fragments of DNA in urine to enable early detection of head and neck cancers caused by human papillomavirus.
“Our data show that a relatively small volume of urine (30-60 mL) gives overall detection results comparable to a tube of blood,” said study author Muneesh Tewari, MD, PhD, professor of hematology and oncology at the University of Michigan .
A larger volume of urine could potentially “make cancer detection even more sensitive than blood,” Dr. Tewari said, “allowing cancers to be detected at the earliest stages when they are more curable.”
The team used a technique called droplet digital PCR to detect DNA fragments that are “ultra-short” (less than 50 base pairs long) and usually missed by conventional PCR testing. This transrenal cell-free tumor DNA, which travels from the tumor into the bloodstream, is broken down small enough to pass through the kidneys and into the urine. But the fragments are still long enough to carry information about the tumor’s genetic signature.
This test could spot cancer before a tumor grows big enough — about a centimeter wide and carrying a billion cells — to spot on a CT scan or other imaging test. “When we are instead detecting fragments of DNA released from a tumor,” said Dr. Tewari, “our testing methods are very sensitive and can detect DNA in urine that came from just 5-10 cells in a tumor that died and released their DNA into the blood, which then made its way into the urine.”
Pancreatic cancer. Pancreatic ductal adenocarcinoma is one of the deadliest cancers, largely because it is diagnosed so late. A urine panel now in clinical trials could help doctors diagnose the cancer before it has spread so more people can have the tumor surgically removed, improving prognosis.
Using enzyme-linked immunosorbent assay test, a common lab method that detects antibodies and other proteins, the team measured expression levels for three genes (LYVE1, REG1B, and TFF1) in urine samples collected from people up to 5 years before they were diagnosed with pancreatic cancer. The researchers combined this result with patients’ urinary creatinine levels, a common component of existing urinalysis, and their age to develop a risk score.
This score performed similarly to an existing blood test, CA19-9, in predicting patients’ risk for pancreatic cancer up to 1 year before diagnosis. When combined with CA19-9, the urinary panel helped spot cancer up to 2 years before diagnosis.
According to a paper in the International Journal of Cancer, “the urine panel and affiliated PancRISK are currently being validated in a prospective clinical study (UroPanc).” If all goes well, they could be implemented in clinical practice in a few years as a “noninvasive stratification tool” to identify patients for further testing, speeding up diagnosis, and saving lives.
Limitations and Promises
Each cancer type is different, and more research is needed to map out which substances in urine predict which cancers and to develop tests for mass adoption. “There are medical and technological hurdles to the large-scale implementation of urine analysis for complex diseases such as cancer,” said Dr. Wong.
One possibility: Scientists and clinicians could collaborate and use artificial intelligence techniques to combine urine test results with other data.
“It is likely that future diagnostics may combine urine with other biological samples such as feces and saliva, among others,” said Dr. Wong. “This is especially true when novel data science and machine learning techniques can integrate comprehensive data from patients that span genetic, proteomic, metabolic, microbiomic, and even behavioral data to evaluate a patient’s condition.”
One thing that excites Dr. Tewari about urine-based cancer testing: “We think it could be especially impactful for patients living in rural areas or other areas with less access to healthcare services,” he said.
A version of this article appeared on Medscape.com.
Emerging science suggests that the body’s “liquid gold” could be particularly useful for liquid biopsies, offering a convenient, pain-free, and cost-effective way to spot otherwise hard-to-detect cancers.
“The search for cancer biomarkers that can be detected in urine could provide an enormous step forward to decrease cancer patient mortality,” said Kenneth R. Shroyer, MD, PhD, a pathologist at Stony Brook University, Stony Brook, New York, who studies cancer biomarkers.
Physicians have long known that urine can reveal a lot about our health — that’s why urinalysis has been part of medicine for 6000 years. Urine tests can detect diabetes, pregnancy, drug use, and urinary or kidney conditions.
But other conditions leave clues in urine, too, and cancer may be one of the most promising. “Urine testing could detect biomarkers of early-stage cancers, not only from local but also distant sites,” Dr. Shroyer said. It could also help flag recurrence in cancer survivors who have undergone treatment.
Granted, cancer biomarkers in urine are not nearly as widely studied as those in the blood, Dr. Shroyer noted. But a new wave of urine tests suggests research is gaining pace.
“The recent availability of high-throughput screening technologies has enabled researchers to investigate cancer from a top-down, comprehensive approach,” said Pak Kin Wong, PhD, professor of mechanical engineering, biomedical engineering, and surgery at The Pennsylvania State University. “We are starting to understand the rich information that can be obtained from urine.”
Urine is mostly water (about 95%) and urea, a metabolic byproduct that imparts that signature yellow color (about 2%). The other 3% is a mix of waste products, minerals, and other compounds the kidneys removed from the blood. Even in trace amounts, these substances say a lot.
Among them are “exfoliated cancer cells, cell-free DNA, hormones, and the urine microbiota — the collection of microbes in our urinary tract system,” Dr. Wong said.
“It is highly promising to be one of the major biological fluids used for screening, diagnosis, prognosis, and monitoring treatment efficiency in the era of precision medicine,” Dr. Wong said.
How Urine Testing Could Reveal Cancer
Still, as exciting as the prospect is, there’s a lot to consider in the hunt for cancer biomarkers in urine. These biomarkers must be able to pass through the renal nephrons (filtering units), remain stable in urine, and have high-level sensitivity, Dr. Shroyer said. They should also have high specificity for cancer vs benign conditions and be expressed at early stages, before the primary tumor has spread.
“At this stage, few circulating biomarkers have been found that are both sensitive and specific for early-stage disease,” said Dr. Shroyer.
But there are a few promising examples under investigation in humans:
Prostate cancer. Researchers at the University of Michigan have developed a urine test that detects high-grade prostate cancer more accurately than existing tests, including PHI, SelectMDx, 4Kscore, EPI, MPS, and IsoPSA.
The MyProstateScore 2.0 (MPS2) test, which looks for 18 genes associated with high-grade tumors, could reduce unnecessary biopsies in men with elevated prostate-specific antigen levels, according to a paper published in JAMA Oncology.
It makes sense. The prostate gland secretes fluid that becomes part of the semen, traces of which enter urine. After a digital rectal exam, even more prostate fluid enters the urine. If a patient has prostate cancer, genetic material from the cancer cells will infiltrate the urine.
In the MPS2 test, researchers used polymerase chain reaction (PCR) testing in urine. “The technology used for COVID PCR is essentially the same as the PCR used to detect transcripts associated with high-grade prostate cancer in urine,” said study author Arul Chinnaiyan, MD, PhD, director of the Michigan Center for Translational Pathology at the University of Michigan, Ann Arbor. “In the case of the MPS2 test, we are doing PCR on 18 genes simultaneously on urine samples.”
A statistical model uses levels of that genetic material to predict the risk for high-grade disease, helping doctors decide what to do next. At 95% sensitivity, the MPS2 model could eliminate 35%-45% of unnecessary biopsies, compared with 15%-30% for the other tests, and reduce repeat biopsies by 46%-51%, compared with 9%-21% for the other tests.
Head and neck cancer. In a paper published in JCI Insight, researchers described a test that finds ultra-short fragments of DNA in urine to enable early detection of head and neck cancers caused by human papillomavirus.
“Our data show that a relatively small volume of urine (30-60 mL) gives overall detection results comparable to a tube of blood,” said study author Muneesh Tewari, MD, PhD, professor of hematology and oncology at the University of Michigan .
A larger volume of urine could potentially “make cancer detection even more sensitive than blood,” Dr. Tewari said, “allowing cancers to be detected at the earliest stages when they are more curable.”
The team used a technique called droplet digital PCR to detect DNA fragments that are “ultra-short” (less than 50 base pairs long) and usually missed by conventional PCR testing. This transrenal cell-free tumor DNA, which travels from the tumor into the bloodstream, is broken down small enough to pass through the kidneys and into the urine. But the fragments are still long enough to carry information about the tumor’s genetic signature.
This test could spot cancer before a tumor grows big enough — about a centimeter wide and carrying a billion cells — to spot on a CT scan or other imaging test. “When we are instead detecting fragments of DNA released from a tumor,” said Dr. Tewari, “our testing methods are very sensitive and can detect DNA in urine that came from just 5-10 cells in a tumor that died and released their DNA into the blood, which then made its way into the urine.”
Pancreatic cancer. Pancreatic ductal adenocarcinoma is one of the deadliest cancers, largely because it is diagnosed so late. A urine panel now in clinical trials could help doctors diagnose the cancer before it has spread so more people can have the tumor surgically removed, improving prognosis.
Using enzyme-linked immunosorbent assay test, a common lab method that detects antibodies and other proteins, the team measured expression levels for three genes (LYVE1, REG1B, and TFF1) in urine samples collected from people up to 5 years before they were diagnosed with pancreatic cancer. The researchers combined this result with patients’ urinary creatinine levels, a common component of existing urinalysis, and their age to develop a risk score.
This score performed similarly to an existing blood test, CA19-9, in predicting patients’ risk for pancreatic cancer up to 1 year before diagnosis. When combined with CA19-9, the urinary panel helped spot cancer up to 2 years before diagnosis.
According to a paper in the International Journal of Cancer, “the urine panel and affiliated PancRISK are currently being validated in a prospective clinical study (UroPanc).” If all goes well, they could be implemented in clinical practice in a few years as a “noninvasive stratification tool” to identify patients for further testing, speeding up diagnosis, and saving lives.
Limitations and Promises
Each cancer type is different, and more research is needed to map out which substances in urine predict which cancers and to develop tests for mass adoption. “There are medical and technological hurdles to the large-scale implementation of urine analysis for complex diseases such as cancer,” said Dr. Wong.
One possibility: Scientists and clinicians could collaborate and use artificial intelligence techniques to combine urine test results with other data.
“It is likely that future diagnostics may combine urine with other biological samples such as feces and saliva, among others,” said Dr. Wong. “This is especially true when novel data science and machine learning techniques can integrate comprehensive data from patients that span genetic, proteomic, metabolic, microbiomic, and even behavioral data to evaluate a patient’s condition.”
One thing that excites Dr. Tewari about urine-based cancer testing: “We think it could be especially impactful for patients living in rural areas or other areas with less access to healthcare services,” he said.
A version of this article appeared on Medscape.com.
Chatbots Seem More Empathetic Than Docs in Cancer Discussions
Large language models (LLM) such as ChatGPT have shown mixed results in the quality of their responses to consumer questions about cancer.
One recent study found AI chatbots to churn out incomplete, inaccurate, or even nonsensical cancer treatment recommendations, while another found them to generate largely accurate — if technical — responses to the most common cancer questions.
While researchers have seen success with purpose-built chatbots created to address patient concerns about specific cancers, the consensus to date has been that the generalized models like ChatGPT remain works in progress and that physicians should avoid pointing patients to them, for now.
Yet new findings suggest that these chatbots may do better than individual physicians, at least on some measures, when it comes to answering queries about cancer. For research published May 16 in JAMA Oncology (doi: 10.1001/jamaoncol.2024.0836), David Chen, a medical student at the University of Toronto, and his colleagues, isolated a random sample of 200 questions related to cancer care addressed to doctors on the public online forum Reddit. They then compared responses from oncologists with responses generated by three different AI chatbots. The blinded responses were rated for quality, readability, and empathy by six physicians, including oncologists and palliative and supportive care specialists.
Mr. Chen and colleagues’ research was modeled after a 2023 study that measured the quality of physician responses compared with chatbots for general medicine questions addressed to doctors on Reddit. That study found that the chatbots produced more empathetic-sounding answers, something Mr. Chen’s study also found. : quality, empathy, and readability.
Q&A With Author of New Research
Mr. Chen discussed his new study’s implications during an interview with this news organization.
Question: What is novel about this study?
Mr. Chen: We’ve seen many evaluations of chatbots that test for medical accuracy, but this study occurs in the domain of oncology care, where there are unique psychosocial and emotional considerations that are not precisely reflected in a general medicine setting. In effect, this study is putting these chatbots through a harder challenge.
Question: Why would chatbot responses seem more empathetic than those of physicians?
Mr. Chen: With the physician responses that we observed in our sample data set, we saw that there was very high variation of amount of apparent effort [in the physician responses]. Some physicians would put in a lot of time and effort, thinking through their response, and others wouldn’t do so as much. These chatbots don’t face fatigue the way humans do, or burnout. So they’re able to consistently provide responses with less variation in empathy.
Question: Do chatbots just seem empathetic because they are chattier?
Mr. Chen: We did think of verbosity as a potential confounder in this study. So we set a word count limit for the chatbot responses to keep it in the range of the physician responses. That way, verbosity was no longer a significant factor.
Question: How were quality and empathy measured by the reviewers?
Mr. Chen: For our study we used two teams of readers, each team composed of three physicians. In terms of the actual metrics we used, they were pilot metrics. There are no well-defined measurement scales or checklists that we could use to measure empathy. This is an emerging field of research. So we came up by consensus with our own set of ratings, and we feel that this is an area for the research to define a standardized set of guidelines.
Another novel aspect of this study is that we separated out different dimensions of quality and empathy. A quality response didn’t just mean it was medically accurate — quality also had to do with the focus and completeness of the response.
With empathy there are cognitive and emotional dimensions. Cognitive empathy uses critical thinking to understand the person’s emotions and thoughts and then adjusting a response to fit that. A patient may not want the best medically indicated treatment for their condition, because they want to preserve their quality of life. The chatbot may be able to adjust its recommendation with consideration of some of those humanistic elements that the patient is presenting with.
Emotional empathy is more about being supportive of the patient’s emotions by using expressions like ‘I understand where you’re coming from.’ or, ‘I can see how that makes you feel.’
Question: Why would physicians, not patients, be the best evaluators of empathy?
Mr. Chen: We’re actually very interested in evaluating patient ratings of empathy. We are conducting a follow-up study that evaluates patient ratings of empathy to the same set of chatbot and physician responses,to see if there are differences.
Question: Should cancer patients go ahead and consult chatbots?
Mr. Chen: Although we did observe increases in all of the metrics compared with physicians, this is a very specialized evaluation scenario where we’re using these Reddit questions and responses.
Naturally, we would need to do a trial, a head to head randomized comparison of physicians versus chatbots.
This pilot study does highlight the promising potential of these chatbots to suggest responses. But we can’t fully recommend that they should be used as standalone clinical tools without physicians.
This Q&A was edited for clarity.
Large language models (LLM) such as ChatGPT have shown mixed results in the quality of their responses to consumer questions about cancer.
One recent study found AI chatbots to churn out incomplete, inaccurate, or even nonsensical cancer treatment recommendations, while another found them to generate largely accurate — if technical — responses to the most common cancer questions.
While researchers have seen success with purpose-built chatbots created to address patient concerns about specific cancers, the consensus to date has been that the generalized models like ChatGPT remain works in progress and that physicians should avoid pointing patients to them, for now.
Yet new findings suggest that these chatbots may do better than individual physicians, at least on some measures, when it comes to answering queries about cancer. For research published May 16 in JAMA Oncology (doi: 10.1001/jamaoncol.2024.0836), David Chen, a medical student at the University of Toronto, and his colleagues, isolated a random sample of 200 questions related to cancer care addressed to doctors on the public online forum Reddit. They then compared responses from oncologists with responses generated by three different AI chatbots. The blinded responses were rated for quality, readability, and empathy by six physicians, including oncologists and palliative and supportive care specialists.
Mr. Chen and colleagues’ research was modeled after a 2023 study that measured the quality of physician responses compared with chatbots for general medicine questions addressed to doctors on Reddit. That study found that the chatbots produced more empathetic-sounding answers, something Mr. Chen’s study also found. : quality, empathy, and readability.
Q&A With Author of New Research
Mr. Chen discussed his new study’s implications during an interview with this news organization.
Question: What is novel about this study?
Mr. Chen: We’ve seen many evaluations of chatbots that test for medical accuracy, but this study occurs in the domain of oncology care, where there are unique psychosocial and emotional considerations that are not precisely reflected in a general medicine setting. In effect, this study is putting these chatbots through a harder challenge.
Question: Why would chatbot responses seem more empathetic than those of physicians?
Mr. Chen: With the physician responses that we observed in our sample data set, we saw that there was very high variation of amount of apparent effort [in the physician responses]. Some physicians would put in a lot of time and effort, thinking through their response, and others wouldn’t do so as much. These chatbots don’t face fatigue the way humans do, or burnout. So they’re able to consistently provide responses with less variation in empathy.
Question: Do chatbots just seem empathetic because they are chattier?
Mr. Chen: We did think of verbosity as a potential confounder in this study. So we set a word count limit for the chatbot responses to keep it in the range of the physician responses. That way, verbosity was no longer a significant factor.
Question: How were quality and empathy measured by the reviewers?
Mr. Chen: For our study we used two teams of readers, each team composed of three physicians. In terms of the actual metrics we used, they were pilot metrics. There are no well-defined measurement scales or checklists that we could use to measure empathy. This is an emerging field of research. So we came up by consensus with our own set of ratings, and we feel that this is an area for the research to define a standardized set of guidelines.
Another novel aspect of this study is that we separated out different dimensions of quality and empathy. A quality response didn’t just mean it was medically accurate — quality also had to do with the focus and completeness of the response.
With empathy there are cognitive and emotional dimensions. Cognitive empathy uses critical thinking to understand the person’s emotions and thoughts and then adjusting a response to fit that. A patient may not want the best medically indicated treatment for their condition, because they want to preserve their quality of life. The chatbot may be able to adjust its recommendation with consideration of some of those humanistic elements that the patient is presenting with.
Emotional empathy is more about being supportive of the patient’s emotions by using expressions like ‘I understand where you’re coming from.’ or, ‘I can see how that makes you feel.’
Question: Why would physicians, not patients, be the best evaluators of empathy?
Mr. Chen: We’re actually very interested in evaluating patient ratings of empathy. We are conducting a follow-up study that evaluates patient ratings of empathy to the same set of chatbot and physician responses,to see if there are differences.
Question: Should cancer patients go ahead and consult chatbots?
Mr. Chen: Although we did observe increases in all of the metrics compared with physicians, this is a very specialized evaluation scenario where we’re using these Reddit questions and responses.
Naturally, we would need to do a trial, a head to head randomized comparison of physicians versus chatbots.
This pilot study does highlight the promising potential of these chatbots to suggest responses. But we can’t fully recommend that they should be used as standalone clinical tools without physicians.
This Q&A was edited for clarity.
Large language models (LLM) such as ChatGPT have shown mixed results in the quality of their responses to consumer questions about cancer.
One recent study found AI chatbots to churn out incomplete, inaccurate, or even nonsensical cancer treatment recommendations, while another found them to generate largely accurate — if technical — responses to the most common cancer questions.
While researchers have seen success with purpose-built chatbots created to address patient concerns about specific cancers, the consensus to date has been that the generalized models like ChatGPT remain works in progress and that physicians should avoid pointing patients to them, for now.
Yet new findings suggest that these chatbots may do better than individual physicians, at least on some measures, when it comes to answering queries about cancer. For research published May 16 in JAMA Oncology (doi: 10.1001/jamaoncol.2024.0836), David Chen, a medical student at the University of Toronto, and his colleagues, isolated a random sample of 200 questions related to cancer care addressed to doctors on the public online forum Reddit. They then compared responses from oncologists with responses generated by three different AI chatbots. The blinded responses were rated for quality, readability, and empathy by six physicians, including oncologists and palliative and supportive care specialists.
Mr. Chen and colleagues’ research was modeled after a 2023 study that measured the quality of physician responses compared with chatbots for general medicine questions addressed to doctors on Reddit. That study found that the chatbots produced more empathetic-sounding answers, something Mr. Chen’s study also found. : quality, empathy, and readability.
Q&A With Author of New Research
Mr. Chen discussed his new study’s implications during an interview with this news organization.
Question: What is novel about this study?
Mr. Chen: We’ve seen many evaluations of chatbots that test for medical accuracy, but this study occurs in the domain of oncology care, where there are unique psychosocial and emotional considerations that are not precisely reflected in a general medicine setting. In effect, this study is putting these chatbots through a harder challenge.
Question: Why would chatbot responses seem more empathetic than those of physicians?
Mr. Chen: With the physician responses that we observed in our sample data set, we saw that there was very high variation of amount of apparent effort [in the physician responses]. Some physicians would put in a lot of time and effort, thinking through their response, and others wouldn’t do so as much. These chatbots don’t face fatigue the way humans do, or burnout. So they’re able to consistently provide responses with less variation in empathy.
Question: Do chatbots just seem empathetic because they are chattier?
Mr. Chen: We did think of verbosity as a potential confounder in this study. So we set a word count limit for the chatbot responses to keep it in the range of the physician responses. That way, verbosity was no longer a significant factor.
Question: How were quality and empathy measured by the reviewers?
Mr. Chen: For our study we used two teams of readers, each team composed of three physicians. In terms of the actual metrics we used, they were pilot metrics. There are no well-defined measurement scales or checklists that we could use to measure empathy. This is an emerging field of research. So we came up by consensus with our own set of ratings, and we feel that this is an area for the research to define a standardized set of guidelines.
Another novel aspect of this study is that we separated out different dimensions of quality and empathy. A quality response didn’t just mean it was medically accurate — quality also had to do with the focus and completeness of the response.
With empathy there are cognitive and emotional dimensions. Cognitive empathy uses critical thinking to understand the person’s emotions and thoughts and then adjusting a response to fit that. A patient may not want the best medically indicated treatment for their condition, because they want to preserve their quality of life. The chatbot may be able to adjust its recommendation with consideration of some of those humanistic elements that the patient is presenting with.
Emotional empathy is more about being supportive of the patient’s emotions by using expressions like ‘I understand where you’re coming from.’ or, ‘I can see how that makes you feel.’
Question: Why would physicians, not patients, be the best evaluators of empathy?
Mr. Chen: We’re actually very interested in evaluating patient ratings of empathy. We are conducting a follow-up study that evaluates patient ratings of empathy to the same set of chatbot and physician responses,to see if there are differences.
Question: Should cancer patients go ahead and consult chatbots?
Mr. Chen: Although we did observe increases in all of the metrics compared with physicians, this is a very specialized evaluation scenario where we’re using these Reddit questions and responses.
Naturally, we would need to do a trial, a head to head randomized comparison of physicians versus chatbots.
This pilot study does highlight the promising potential of these chatbots to suggest responses. But we can’t fully recommend that they should be used as standalone clinical tools without physicians.
This Q&A was edited for clarity.
FROM JAMA ONCOLOGY
Tool May Help Prioritize High-Risk Patients for Hysteroscopy
Hysteroscopy is a crucial examination for the diagnosis of endometrial cancer. In Brazil, women with postmenopausal bleeding who need to undergo this procedure in the public health system wait in line alongside patients with less severe complaints. Until now, there has been no system to prioritize patients at high risk for cancer. But this situation may change, thanks to a Brazilian study published in February in the Journal of Clinical Medicine.
Researchers from the Municipal Hospital of Vila Santa Catarina in São Paulo, a public unit managed by Hospital Israelita Albert Einstein, have developed the Endometrial Malignancy Prediction System (EMPS), a nomogram to identify patients at high risk for endometrial cancer and prioritize them in the hysteroscopy waiting list.
Bruna Bottura, MD, a gynecologist and obstetrician at Hospital Israelita Albert Einstein and the study’s lead author, told this news organization that the idea to create the nomogram arose during the COVID-19 pandemic. “We noticed that ... when outpatient clinics resumed, we were seeing many patients for intrauterine device (IUD) removal. We thought it was unfair for a patient with postmenopausal bleeding, who has a chance of having cancer, to have to wait in the same line as a patient needing IUD removal,” she said. This realization motivated the development of the tool, which was overseen by Renato Moretti-Marques, MD, PhD.
The EMPS Score
The team conducted a retrospective case-control study involving 1945 patients with suspected endometrial cancer who had undergone diagnostic hysteroscopy at Hospital Israelita Albert Einstein between March 2019 and March 2022. Among these patients, 107 were diagnosed with precursor lesions or endometrial cancer on the basis of biopsy. The other 1838 participants, who had had cancer ruled out by biopsy, formed the control group.
Through bivariate and multivariate linear regression analysis, the authors determined that the presence or absence of hypertension, diabetes, postmenopausal bleeding, endometrial polyps, uterine volume, number of pregnancies, body mass index, age, and endometrial thickness were the main risk factors for endometrial cancer diagnosis.
On the basis of these data, the group developed the EMPS nomogram. Physicians can use it to classify the patient’s risk according to the sum of the scores assigned to each of these factors.
The Table shows the classification system. The scoring tables available in the supplemental materials of the article can be accessed here.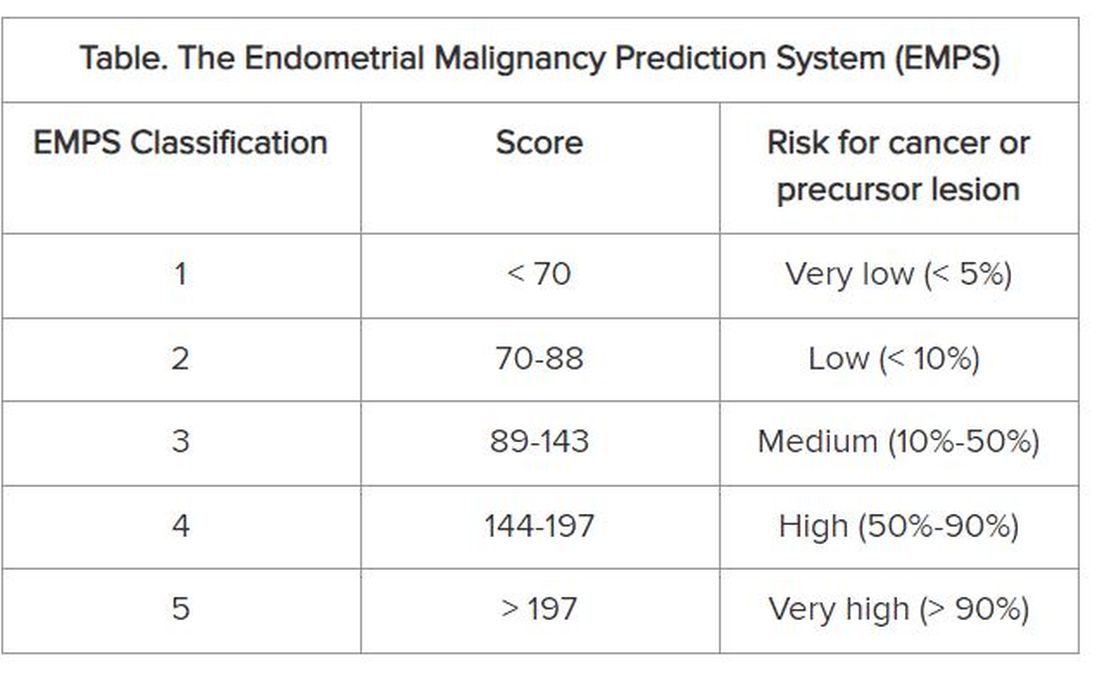
Focus on Primary Care
The goal is not to remove patients classified as low risk from the hysteroscopy waiting list, but rather to prioritize those classified as high risk to get the examination, according to Dr. Bottura.
At the Municipal Hospital of Vila Santa Catarina, the average wait time for hysteroscopy was 120 days. But because the unit is focused on oncologic patients and has a high level of organization, this time is much shorter than observed in other parts of Brazil’s National Health Service, said Dr. Bottura. “Many patients are on the hysteroscopy waiting list for 2 years. Considering patients in more advanced stages [of endometrial cancer], it makes a difference,” she said.
Although the nomogram was developed in tertiary care, it is aimed at professionals working in primary care. The reason is that physicians from primary care health units refer women with clinical indications for hysteroscopy to specialized national health services, such as the Municipal Hospital of Vila Santa Catarina. “Our goal is the primary sector, to enable the clinic to refer this high-risk patient sooner. By the time you reach the tertiary sector, where hysteroscopies are performed, all patients will undergo the procedure. Usually, it is not the hospitals that predetermine the line, but rather the health clinics,” she explained.
The researchers hope to continue the research, starting with a prospective study. “We intend to apply and evaluate the tool within our own service to observe whether any patient with a high [EMPS] score patient ended up waiting too long to be referred. In fact, this will be a system validation step,” said Dr. Bottura.
In parallel, the team has a proposal to take the tool to health clinics in the same region as the study hospital. “We know this involves changing the protocol at a national level, so it’s more challenging,” said Dr. Bottura. She added that the final goal is to create a calculator, possibly an app, that allows primary care doctors to calculate the risk score in the office. This calculator could enable risk classification to be linked to patient referrals.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Hysteroscopy is a crucial examination for the diagnosis of endometrial cancer. In Brazil, women with postmenopausal bleeding who need to undergo this procedure in the public health system wait in line alongside patients with less severe complaints. Until now, there has been no system to prioritize patients at high risk for cancer. But this situation may change, thanks to a Brazilian study published in February in the Journal of Clinical Medicine.
Researchers from the Municipal Hospital of Vila Santa Catarina in São Paulo, a public unit managed by Hospital Israelita Albert Einstein, have developed the Endometrial Malignancy Prediction System (EMPS), a nomogram to identify patients at high risk for endometrial cancer and prioritize them in the hysteroscopy waiting list.
Bruna Bottura, MD, a gynecologist and obstetrician at Hospital Israelita Albert Einstein and the study’s lead author, told this news organization that the idea to create the nomogram arose during the COVID-19 pandemic. “We noticed that ... when outpatient clinics resumed, we were seeing many patients for intrauterine device (IUD) removal. We thought it was unfair for a patient with postmenopausal bleeding, who has a chance of having cancer, to have to wait in the same line as a patient needing IUD removal,” she said. This realization motivated the development of the tool, which was overseen by Renato Moretti-Marques, MD, PhD.
The EMPS Score
The team conducted a retrospective case-control study involving 1945 patients with suspected endometrial cancer who had undergone diagnostic hysteroscopy at Hospital Israelita Albert Einstein between March 2019 and March 2022. Among these patients, 107 were diagnosed with precursor lesions or endometrial cancer on the basis of biopsy. The other 1838 participants, who had had cancer ruled out by biopsy, formed the control group.
Through bivariate and multivariate linear regression analysis, the authors determined that the presence or absence of hypertension, diabetes, postmenopausal bleeding, endometrial polyps, uterine volume, number of pregnancies, body mass index, age, and endometrial thickness were the main risk factors for endometrial cancer diagnosis.
On the basis of these data, the group developed the EMPS nomogram. Physicians can use it to classify the patient’s risk according to the sum of the scores assigned to each of these factors.
The Table shows the classification system. The scoring tables available in the supplemental materials of the article can be accessed here.
Focus on Primary Care
The goal is not to remove patients classified as low risk from the hysteroscopy waiting list, but rather to prioritize those classified as high risk to get the examination, according to Dr. Bottura.
At the Municipal Hospital of Vila Santa Catarina, the average wait time for hysteroscopy was 120 days. But because the unit is focused on oncologic patients and has a high level of organization, this time is much shorter than observed in other parts of Brazil’s National Health Service, said Dr. Bottura. “Many patients are on the hysteroscopy waiting list for 2 years. Considering patients in more advanced stages [of endometrial cancer], it makes a difference,” she said.
Although the nomogram was developed in tertiary care, it is aimed at professionals working in primary care. The reason is that physicians from primary care health units refer women with clinical indications for hysteroscopy to specialized national health services, such as the Municipal Hospital of Vila Santa Catarina. “Our goal is the primary sector, to enable the clinic to refer this high-risk patient sooner. By the time you reach the tertiary sector, where hysteroscopies are performed, all patients will undergo the procedure. Usually, it is not the hospitals that predetermine the line, but rather the health clinics,” she explained.
The researchers hope to continue the research, starting with a prospective study. “We intend to apply and evaluate the tool within our own service to observe whether any patient with a high [EMPS] score patient ended up waiting too long to be referred. In fact, this will be a system validation step,” said Dr. Bottura.
In parallel, the team has a proposal to take the tool to health clinics in the same region as the study hospital. “We know this involves changing the protocol at a national level, so it’s more challenging,” said Dr. Bottura. She added that the final goal is to create a calculator, possibly an app, that allows primary care doctors to calculate the risk score in the office. This calculator could enable risk classification to be linked to patient referrals.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Hysteroscopy is a crucial examination for the diagnosis of endometrial cancer. In Brazil, women with postmenopausal bleeding who need to undergo this procedure in the public health system wait in line alongside patients with less severe complaints. Until now, there has been no system to prioritize patients at high risk for cancer. But this situation may change, thanks to a Brazilian study published in February in the Journal of Clinical Medicine.
Researchers from the Municipal Hospital of Vila Santa Catarina in São Paulo, a public unit managed by Hospital Israelita Albert Einstein, have developed the Endometrial Malignancy Prediction System (EMPS), a nomogram to identify patients at high risk for endometrial cancer and prioritize them in the hysteroscopy waiting list.
Bruna Bottura, MD, a gynecologist and obstetrician at Hospital Israelita Albert Einstein and the study’s lead author, told this news organization that the idea to create the nomogram arose during the COVID-19 pandemic. “We noticed that ... when outpatient clinics resumed, we were seeing many patients for intrauterine device (IUD) removal. We thought it was unfair for a patient with postmenopausal bleeding, who has a chance of having cancer, to have to wait in the same line as a patient needing IUD removal,” she said. This realization motivated the development of the tool, which was overseen by Renato Moretti-Marques, MD, PhD.
The EMPS Score
The team conducted a retrospective case-control study involving 1945 patients with suspected endometrial cancer who had undergone diagnostic hysteroscopy at Hospital Israelita Albert Einstein between March 2019 and March 2022. Among these patients, 107 were diagnosed with precursor lesions or endometrial cancer on the basis of biopsy. The other 1838 participants, who had had cancer ruled out by biopsy, formed the control group.
Through bivariate and multivariate linear regression analysis, the authors determined that the presence or absence of hypertension, diabetes, postmenopausal bleeding, endometrial polyps, uterine volume, number of pregnancies, body mass index, age, and endometrial thickness were the main risk factors for endometrial cancer diagnosis.
On the basis of these data, the group developed the EMPS nomogram. Physicians can use it to classify the patient’s risk according to the sum of the scores assigned to each of these factors.
The Table shows the classification system. The scoring tables available in the supplemental materials of the article can be accessed here.
Focus on Primary Care
The goal is not to remove patients classified as low risk from the hysteroscopy waiting list, but rather to prioritize those classified as high risk to get the examination, according to Dr. Bottura.
At the Municipal Hospital of Vila Santa Catarina, the average wait time for hysteroscopy was 120 days. But because the unit is focused on oncologic patients and has a high level of organization, this time is much shorter than observed in other parts of Brazil’s National Health Service, said Dr. Bottura. “Many patients are on the hysteroscopy waiting list for 2 years. Considering patients in more advanced stages [of endometrial cancer], it makes a difference,” she said.
Although the nomogram was developed in tertiary care, it is aimed at professionals working in primary care. The reason is that physicians from primary care health units refer women with clinical indications for hysteroscopy to specialized national health services, such as the Municipal Hospital of Vila Santa Catarina. “Our goal is the primary sector, to enable the clinic to refer this high-risk patient sooner. By the time you reach the tertiary sector, where hysteroscopies are performed, all patients will undergo the procedure. Usually, it is not the hospitals that predetermine the line, but rather the health clinics,” she explained.
The researchers hope to continue the research, starting with a prospective study. “We intend to apply and evaluate the tool within our own service to observe whether any patient with a high [EMPS] score patient ended up waiting too long to be referred. In fact, this will be a system validation step,” said Dr. Bottura.
In parallel, the team has a proposal to take the tool to health clinics in the same region as the study hospital. “We know this involves changing the protocol at a national level, so it’s more challenging,” said Dr. Bottura. She added that the final goal is to create a calculator, possibly an app, that allows primary care doctors to calculate the risk score in the office. This calculator could enable risk classification to be linked to patient referrals.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Molecular Classification of Endometrial Carcinomas
Historically, endometrial cancer has been classified as type I or type II. Type I endometrial cancers are typically estrogen driven, low grade, with endometrioid histology, and have a more favorable prognosis. In contrast, type II endometrial cancers are typically high grade, have more aggressive histologies (eg, serous or clear cell), and have a poorer prognosis.1
While this system provides a helpful schema for understanding endometrial cancers, it fails to represent the immense variation of biologic behavior and outcomes in endometrial cancers and oversimplifies what has come to be understood as a complex and molecularly diverse disease.

In 2013, The Cancer Genome Atlas (TCGA) performed genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas. They identified four categories with distinct genetic profiles corresponding to clinical outcomes: 1) DNA polymerase epsilon (POLE) mutated; 2) mismatch repair deficient; 3) copy number high/p53 abnormal; and 4) copy number low/no specific molecular profile.2 By providing both predictive and prognostic information, these molecular features may be incorporated into treatment planning decisions in the future.

The POLE-mutated subtype are endometrial cancers with recurrent mutations in the POLE gene, which is involved in DNA replication and repair. POLE mutations occur in about 5%-10% of endometrial cancers. Despite some more aggressive histopathologic findings (eg, higher grade, deeper myometrial invasion, positive lymphovascular space invasion), recurrences rarely occur, and patients with POLE mutations have the best prognosis of the four molecular subtypes, with a 5-year recurrence-free survival of 92%-100%.3
The mismatch repair–deficient (MMRd) subtype are endometrial cancers with abnormalities in any of the mismatch repair proteins (MLH1, PMS2, MSH2, MSH6). These alterations may result from hereditary or somatic mutations in any of the MMR genes or epigenetic changes in the MLH1 promoter. Germ-line mutations are associated with Lynch syndrome; thus, patients found to have a germ-line mutation in any of the MMR genes necessitate a genetics referral. The MMRd subtype accounts for about 20%-30% of endometrial cancers, and patients with MMRd tumors have an intermediate prognosis, with a 5-year recurrence-free survival of about 70%.3. These tumors are more responsive to the use of immunotherapy checkpoint inhibitors. Two recent landmark trials showed improved outcomes in patients with advanced MMRd endometrial cancer treated with immune checkpoint inhibitors in addition to standard chemotherapy.4,5
The worst prognosis belongs to the copy number high subgroup, which accounts for approximately 10% of endometrial cancers. Five-year recurrence-free survival is ~50%.3 These tumors often contain TP53 mutations and are composed of aggressive histologies, such as serous, clear cell, high-grade endometrioid, and carcinosarcomas. Recent data suggests that human epidermal growth factor receptor 2 (HER2) amplification may also be prevalent in this subgroup.6
Endometrial cancers that lack any of the above alterations fall into the no specific molecular profile (NSMP) or copy number low subgroup. Mutations in other genes, such as PTEN, PIK3CA, CTNNB1, KRAS, and ARID1A, are often present in these tumors. As the most common subtype, this heterogeneous group accounts for about 50% of all endometrial cancers. These tumors frequently comprise endometrioid histology with estrogen and progesterone receptor positivity, high rates of response to hormonal therapy, and an overall intermediate to favorable prognosis, with a 5-year recurrence-free survival of ~75%.3
The use of whole-genome sequencing in TCGA limits the clinical applicability of testing because of the cost and complex methodologies involved. Multiple algorithms have been developed in the interim that approximate TCGA subtypes using relatively less expensive and more widely available testing methods, such as immunohistochemistry and next-generation sequencing. In the ProMisE algorithm, immunohistochemistry for p53 and MMR proteins is used as a surrogate for copy number high and MMRd tumors, respectively, and targeted sequencing is used to identify POLE mutations.7
Full molecular classification of endometrial tumors provides important prognostic information and allows for incorporation into treatment planning. To this end, the new 2023 International Federation of Gynecology and Obstetrics (FIGO) endometrial cancer staging incorporates an option for the addition of molecular subtype, with the stance that it allows for better prognostic prediction.8 While complete molecular classification is not required, it is encouraged. Furthermore, several clinical trials are currently investigating different treatment regimens based on these distinct molecular profiles.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecologic Oncology. 1983;15(1):10-17.
2. Kandoth C et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
3. León-Castillo A et al. Molecular classification of the PORTEC-3 trial for high-risk endometrial cancer: Impact on prognosis and benefit from adjuvant therapy. J Clin Oncology. 2020;38(29):3388-3397.
4. Mirza MR et al. Dostarlimab for primary advanced or recurrent endometrial cancer. N Engl J Med. 2023;388(23):2145-2158.
5. Eskander RN et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. N Engl J Med. 2023;388(23):2159-2170.
6. Talia KL et al. The role of HER2 as a therapeutic biomarker in gynaecological malignancy: Potential for use beyond uterine serous carcinoma. Pathology. 2023;55(1):8-18.
7. Kommoss S et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Annals Oncology. 2018;29(5):1180-1188.
8. Berek JS et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. 2023;162(2):383-394.
Historically, endometrial cancer has been classified as type I or type II. Type I endometrial cancers are typically estrogen driven, low grade, with endometrioid histology, and have a more favorable prognosis. In contrast, type II endometrial cancers are typically high grade, have more aggressive histologies (eg, serous or clear cell), and have a poorer prognosis.1
While this system provides a helpful schema for understanding endometrial cancers, it fails to represent the immense variation of biologic behavior and outcomes in endometrial cancers and oversimplifies what has come to be understood as a complex and molecularly diverse disease.
In 2013, The Cancer Genome Atlas (TCGA) performed genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas. They identified four categories with distinct genetic profiles corresponding to clinical outcomes: 1) DNA polymerase epsilon (POLE) mutated; 2) mismatch repair deficient; 3) copy number high/p53 abnormal; and 4) copy number low/no specific molecular profile.2 By providing both predictive and prognostic information, these molecular features may be incorporated into treatment planning decisions in the future.
The POLE-mutated subtype are endometrial cancers with recurrent mutations in the POLE gene, which is involved in DNA replication and repair. POLE mutations occur in about 5%-10% of endometrial cancers. Despite some more aggressive histopathologic findings (eg, higher grade, deeper myometrial invasion, positive lymphovascular space invasion), recurrences rarely occur, and patients with POLE mutations have the best prognosis of the four molecular subtypes, with a 5-year recurrence-free survival of 92%-100%.3
The mismatch repair–deficient (MMRd) subtype are endometrial cancers with abnormalities in any of the mismatch repair proteins (MLH1, PMS2, MSH2, MSH6). These alterations may result from hereditary or somatic mutations in any of the MMR genes or epigenetic changes in the MLH1 promoter. Germ-line mutations are associated with Lynch syndrome; thus, patients found to have a germ-line mutation in any of the MMR genes necessitate a genetics referral. The MMRd subtype accounts for about 20%-30% of endometrial cancers, and patients with MMRd tumors have an intermediate prognosis, with a 5-year recurrence-free survival of about 70%.3. These tumors are more responsive to the use of immunotherapy checkpoint inhibitors. Two recent landmark trials showed improved outcomes in patients with advanced MMRd endometrial cancer treated with immune checkpoint inhibitors in addition to standard chemotherapy.4,5
The worst prognosis belongs to the copy number high subgroup, which accounts for approximately 10% of endometrial cancers. Five-year recurrence-free survival is ~50%.3 These tumors often contain TP53 mutations and are composed of aggressive histologies, such as serous, clear cell, high-grade endometrioid, and carcinosarcomas. Recent data suggests that human epidermal growth factor receptor 2 (HER2) amplification may also be prevalent in this subgroup.6
Endometrial cancers that lack any of the above alterations fall into the no specific molecular profile (NSMP) or copy number low subgroup. Mutations in other genes, such as PTEN, PIK3CA, CTNNB1, KRAS, and ARID1A, are often present in these tumors. As the most common subtype, this heterogeneous group accounts for about 50% of all endometrial cancers. These tumors frequently comprise endometrioid histology with estrogen and progesterone receptor positivity, high rates of response to hormonal therapy, and an overall intermediate to favorable prognosis, with a 5-year recurrence-free survival of ~75%.3
The use of whole-genome sequencing in TCGA limits the clinical applicability of testing because of the cost and complex methodologies involved. Multiple algorithms have been developed in the interim that approximate TCGA subtypes using relatively less expensive and more widely available testing methods, such as immunohistochemistry and next-generation sequencing. In the ProMisE algorithm, immunohistochemistry for p53 and MMR proteins is used as a surrogate for copy number high and MMRd tumors, respectively, and targeted sequencing is used to identify POLE mutations.7
Full molecular classification of endometrial tumors provides important prognostic information and allows for incorporation into treatment planning. To this end, the new 2023 International Federation of Gynecology and Obstetrics (FIGO) endometrial cancer staging incorporates an option for the addition of molecular subtype, with the stance that it allows for better prognostic prediction.8 While complete molecular classification is not required, it is encouraged. Furthermore, several clinical trials are currently investigating different treatment regimens based on these distinct molecular profiles.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecologic Oncology. 1983;15(1):10-17.
2. Kandoth C et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
3. León-Castillo A et al. Molecular classification of the PORTEC-3 trial for high-risk endometrial cancer: Impact on prognosis and benefit from adjuvant therapy. J Clin Oncology. 2020;38(29):3388-3397.
4. Mirza MR et al. Dostarlimab for primary advanced or recurrent endometrial cancer. N Engl J Med. 2023;388(23):2145-2158.
5. Eskander RN et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. N Engl J Med. 2023;388(23):2159-2170.
6. Talia KL et al. The role of HER2 as a therapeutic biomarker in gynaecological malignancy: Potential for use beyond uterine serous carcinoma. Pathology. 2023;55(1):8-18.
7. Kommoss S et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Annals Oncology. 2018;29(5):1180-1188.
8. Berek JS et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. 2023;162(2):383-394.
Historically, endometrial cancer has been classified as type I or type II. Type I endometrial cancers are typically estrogen driven, low grade, with endometrioid histology, and have a more favorable prognosis. In contrast, type II endometrial cancers are typically high grade, have more aggressive histologies (eg, serous or clear cell), and have a poorer prognosis.1
While this system provides a helpful schema for understanding endometrial cancers, it fails to represent the immense variation of biologic behavior and outcomes in endometrial cancers and oversimplifies what has come to be understood as a complex and molecularly diverse disease.
In 2013, The Cancer Genome Atlas (TCGA) performed genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas. They identified four categories with distinct genetic profiles corresponding to clinical outcomes: 1) DNA polymerase epsilon (POLE) mutated; 2) mismatch repair deficient; 3) copy number high/p53 abnormal; and 4) copy number low/no specific molecular profile.2 By providing both predictive and prognostic information, these molecular features may be incorporated into treatment planning decisions in the future.
The POLE-mutated subtype are endometrial cancers with recurrent mutations in the POLE gene, which is involved in DNA replication and repair. POLE mutations occur in about 5%-10% of endometrial cancers. Despite some more aggressive histopathologic findings (eg, higher grade, deeper myometrial invasion, positive lymphovascular space invasion), recurrences rarely occur, and patients with POLE mutations have the best prognosis of the four molecular subtypes, with a 5-year recurrence-free survival of 92%-100%.3
The mismatch repair–deficient (MMRd) subtype are endometrial cancers with abnormalities in any of the mismatch repair proteins (MLH1, PMS2, MSH2, MSH6). These alterations may result from hereditary or somatic mutations in any of the MMR genes or epigenetic changes in the MLH1 promoter. Germ-line mutations are associated with Lynch syndrome; thus, patients found to have a germ-line mutation in any of the MMR genes necessitate a genetics referral. The MMRd subtype accounts for about 20%-30% of endometrial cancers, and patients with MMRd tumors have an intermediate prognosis, with a 5-year recurrence-free survival of about 70%.3. These tumors are more responsive to the use of immunotherapy checkpoint inhibitors. Two recent landmark trials showed improved outcomes in patients with advanced MMRd endometrial cancer treated with immune checkpoint inhibitors in addition to standard chemotherapy.4,5
The worst prognosis belongs to the copy number high subgroup, which accounts for approximately 10% of endometrial cancers. Five-year recurrence-free survival is ~50%.3 These tumors often contain TP53 mutations and are composed of aggressive histologies, such as serous, clear cell, high-grade endometrioid, and carcinosarcomas. Recent data suggests that human epidermal growth factor receptor 2 (HER2) amplification may also be prevalent in this subgroup.6
Endometrial cancers that lack any of the above alterations fall into the no specific molecular profile (NSMP) or copy number low subgroup. Mutations in other genes, such as PTEN, PIK3CA, CTNNB1, KRAS, and ARID1A, are often present in these tumors. As the most common subtype, this heterogeneous group accounts for about 50% of all endometrial cancers. These tumors frequently comprise endometrioid histology with estrogen and progesterone receptor positivity, high rates of response to hormonal therapy, and an overall intermediate to favorable prognosis, with a 5-year recurrence-free survival of ~75%.3
The use of whole-genome sequencing in TCGA limits the clinical applicability of testing because of the cost and complex methodologies involved. Multiple algorithms have been developed in the interim that approximate TCGA subtypes using relatively less expensive and more widely available testing methods, such as immunohistochemistry and next-generation sequencing. In the ProMisE algorithm, immunohistochemistry for p53 and MMR proteins is used as a surrogate for copy number high and MMRd tumors, respectively, and targeted sequencing is used to identify POLE mutations.7
Full molecular classification of endometrial tumors provides important prognostic information and allows for incorporation into treatment planning. To this end, the new 2023 International Federation of Gynecology and Obstetrics (FIGO) endometrial cancer staging incorporates an option for the addition of molecular subtype, with the stance that it allows for better prognostic prediction.8 While complete molecular classification is not required, it is encouraged. Furthermore, several clinical trials are currently investigating different treatment regimens based on these distinct molecular profiles.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecologic Oncology. 1983;15(1):10-17.
2. Kandoth C et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
3. León-Castillo A et al. Molecular classification of the PORTEC-3 trial for high-risk endometrial cancer: Impact on prognosis and benefit from adjuvant therapy. J Clin Oncology. 2020;38(29):3388-3397.
4. Mirza MR et al. Dostarlimab for primary advanced or recurrent endometrial cancer. N Engl J Med. 2023;388(23):2145-2158.
5. Eskander RN et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. N Engl J Med. 2023;388(23):2159-2170.
6. Talia KL et al. The role of HER2 as a therapeutic biomarker in gynaecological malignancy: Potential for use beyond uterine serous carcinoma. Pathology. 2023;55(1):8-18.
7. Kommoss S et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Annals Oncology. 2018;29(5):1180-1188.
8. Berek JS et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. 2023;162(2):383-394.
Hypofractionated Radiotherapy Limits Toxic Effects in Cervical Cancer
TOPLINE:
results from the phase 2 POHIM-CCRT trial suggested.
METHODOLOGY:
- To date, no studies have assessed the treatment outcomes and toxic effects of hypofractionated IMRT following radical hysterectomy in patients with cervical cancer undergoing curative radiotherapy.
- The team analyzed outcomes from 79 patients undergoing hypofractionated IMRT for cervical cancer after radical hysterectomy and pelvic lymph node dissection.
- Patients were a median age of 48; 29.5% had stage IB to IIA disease, another 29.5% had stage IIB disease, and 41% had stage III disease. Patients also had at least one of the following criteria following radical hysterectomy and pelvic lymph node dissection: lymph node metastasis (39.7%), parametrial invasion (54.4%), and positive resection margin (5.1%).
- The prescribed dose to the planning target volume was 40 Gy, delivered in 16 fractions to the whole pelvis, with any type of IMRT permitted. Overall, 71 patients also underwent concurrent weekly cisplatin (40 mg/m2 of body surface area for three cycles), and eight received fluorouracil (1000 mg/m2 on days 1-5) with cisplatin (60 mg/m2 for two cycles).
- The primary endpoint was the incidence of acute grade 3 or higher gastrointestinal tract, genitourinary, and hematologic toxic effects during radiotherapy or within 3 months of completing radiotherapy.
TAKEAWAY:
- After radiotherapy, only two patients (2.5%) experienced acute grade 3 or higher toxic effects. One was hospitalized for enterocolitis on the last day of radiotherapy and developed grade 3 anemia 3 months after completing radiotherapy; the other experienced hematologic toxic effects and also developed grade 3 anemia 3 months after completing radiotherapy.
- No patients experienced late grade 3 or higher toxic effects.
- When assessing toxic effects of any grade, acute and late gastrointestinal tract toxicities occurred in 76% and 31.6% of patients, respectively; acute and late genitourinary toxicities, all grade 1, occurred in 19% and 24.1% of patients, respectively; and hematologic toxicities occurred in 29.1% and 6.3% of patients, respectively.
- Overall, at 3 years, 79.3% of patients were disease-free and 98% were alive. After a median follow-up of 43 months, 16 patients (20.3%) experienced disease recurrence, four of whom were salvaged and three of whom died.
IN PRACTICE:
“This nonrandomized controlled trial is the first prospective trial, to our knowledge, to show acceptable acute toxic effects of hypofractionated IMRT for cervical cancer in a postoperative concurrent chemoradiotherapy setting,” the authors said, adding that the rate of grade 3 or higher acute toxic effects of 2.5% reported in this study was “substantially lower than our initial hypothesis of less than 15%.”
However , in an accompanying editorial, Mark E. Bernard, MD, of the University of Kentucky College of Medicine, Lexington, highlighted caveats to the study design and raised two core questions: “Should acute toxic effects be the primary endpoint of a single-group, phase 2 study using hypofractionation with fewer cycles of concurrent chemotherapy? Should the primary endpoint rather have been a cancer control endpoint, such as disease-free survival, overall survival, or local control?”
Still, Dr. Bernard wrote, “This trial does help lay the foundation for future pelvic hypofractionated trials with concurrent chemotherapy, especially for gynecological malignant tumors.”
SOURCE:
The research, led by Won Park, MD, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea, was published in JAMA Oncology.
LIMITATIONS:
The trial is a single-arm study, with a short follow-up time. In the editorial, Bernard listed several limitations, including the fact that patients received fewer cycles of concurrent chemotherapy than what’s typically given in this population.
DISCLOSURES:
No funding or relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
TOPLINE:
results from the phase 2 POHIM-CCRT trial suggested.
METHODOLOGY:
- To date, no studies have assessed the treatment outcomes and toxic effects of hypofractionated IMRT following radical hysterectomy in patients with cervical cancer undergoing curative radiotherapy.
- The team analyzed outcomes from 79 patients undergoing hypofractionated IMRT for cervical cancer after radical hysterectomy and pelvic lymph node dissection.
- Patients were a median age of 48; 29.5% had stage IB to IIA disease, another 29.5% had stage IIB disease, and 41% had stage III disease. Patients also had at least one of the following criteria following radical hysterectomy and pelvic lymph node dissection: lymph node metastasis (39.7%), parametrial invasion (54.4%), and positive resection margin (5.1%).
- The prescribed dose to the planning target volume was 40 Gy, delivered in 16 fractions to the whole pelvis, with any type of IMRT permitted. Overall, 71 patients also underwent concurrent weekly cisplatin (40 mg/m2 of body surface area for three cycles), and eight received fluorouracil (1000 mg/m2 on days 1-5) with cisplatin (60 mg/m2 for two cycles).
- The primary endpoint was the incidence of acute grade 3 or higher gastrointestinal tract, genitourinary, and hematologic toxic effects during radiotherapy or within 3 months of completing radiotherapy.
TAKEAWAY:
- After radiotherapy, only two patients (2.5%) experienced acute grade 3 or higher toxic effects. One was hospitalized for enterocolitis on the last day of radiotherapy and developed grade 3 anemia 3 months after completing radiotherapy; the other experienced hematologic toxic effects and also developed grade 3 anemia 3 months after completing radiotherapy.
- No patients experienced late grade 3 or higher toxic effects.
- When assessing toxic effects of any grade, acute and late gastrointestinal tract toxicities occurred in 76% and 31.6% of patients, respectively; acute and late genitourinary toxicities, all grade 1, occurred in 19% and 24.1% of patients, respectively; and hematologic toxicities occurred in 29.1% and 6.3% of patients, respectively.
- Overall, at 3 years, 79.3% of patients were disease-free and 98% were alive. After a median follow-up of 43 months, 16 patients (20.3%) experienced disease recurrence, four of whom were salvaged and three of whom died.
IN PRACTICE:
“This nonrandomized controlled trial is the first prospective trial, to our knowledge, to show acceptable acute toxic effects of hypofractionated IMRT for cervical cancer in a postoperative concurrent chemoradiotherapy setting,” the authors said, adding that the rate of grade 3 or higher acute toxic effects of 2.5% reported in this study was “substantially lower than our initial hypothesis of less than 15%.”
However , in an accompanying editorial, Mark E. Bernard, MD, of the University of Kentucky College of Medicine, Lexington, highlighted caveats to the study design and raised two core questions: “Should acute toxic effects be the primary endpoint of a single-group, phase 2 study using hypofractionation with fewer cycles of concurrent chemotherapy? Should the primary endpoint rather have been a cancer control endpoint, such as disease-free survival, overall survival, or local control?”
Still, Dr. Bernard wrote, “This trial does help lay the foundation for future pelvic hypofractionated trials with concurrent chemotherapy, especially for gynecological malignant tumors.”
SOURCE:
The research, led by Won Park, MD, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea, was published in JAMA Oncology.
LIMITATIONS:
The trial is a single-arm study, with a short follow-up time. In the editorial, Bernard listed several limitations, including the fact that patients received fewer cycles of concurrent chemotherapy than what’s typically given in this population.
DISCLOSURES:
No funding or relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
TOPLINE:
results from the phase 2 POHIM-CCRT trial suggested.
METHODOLOGY:
- To date, no studies have assessed the treatment outcomes and toxic effects of hypofractionated IMRT following radical hysterectomy in patients with cervical cancer undergoing curative radiotherapy.
- The team analyzed outcomes from 79 patients undergoing hypofractionated IMRT for cervical cancer after radical hysterectomy and pelvic lymph node dissection.
- Patients were a median age of 48; 29.5% had stage IB to IIA disease, another 29.5% had stage IIB disease, and 41% had stage III disease. Patients also had at least one of the following criteria following radical hysterectomy and pelvic lymph node dissection: lymph node metastasis (39.7%), parametrial invasion (54.4%), and positive resection margin (5.1%).
- The prescribed dose to the planning target volume was 40 Gy, delivered in 16 fractions to the whole pelvis, with any type of IMRT permitted. Overall, 71 patients also underwent concurrent weekly cisplatin (40 mg/m2 of body surface area for three cycles), and eight received fluorouracil (1000 mg/m2 on days 1-5) with cisplatin (60 mg/m2 for two cycles).
- The primary endpoint was the incidence of acute grade 3 or higher gastrointestinal tract, genitourinary, and hematologic toxic effects during radiotherapy or within 3 months of completing radiotherapy.
TAKEAWAY:
- After radiotherapy, only two patients (2.5%) experienced acute grade 3 or higher toxic effects. One was hospitalized for enterocolitis on the last day of radiotherapy and developed grade 3 anemia 3 months after completing radiotherapy; the other experienced hematologic toxic effects and also developed grade 3 anemia 3 months after completing radiotherapy.
- No patients experienced late grade 3 or higher toxic effects.
- When assessing toxic effects of any grade, acute and late gastrointestinal tract toxicities occurred in 76% and 31.6% of patients, respectively; acute and late genitourinary toxicities, all grade 1, occurred in 19% and 24.1% of patients, respectively; and hematologic toxicities occurred in 29.1% and 6.3% of patients, respectively.
- Overall, at 3 years, 79.3% of patients were disease-free and 98% were alive. After a median follow-up of 43 months, 16 patients (20.3%) experienced disease recurrence, four of whom were salvaged and three of whom died.
IN PRACTICE:
“This nonrandomized controlled trial is the first prospective trial, to our knowledge, to show acceptable acute toxic effects of hypofractionated IMRT for cervical cancer in a postoperative concurrent chemoradiotherapy setting,” the authors said, adding that the rate of grade 3 or higher acute toxic effects of 2.5% reported in this study was “substantially lower than our initial hypothesis of less than 15%.”
However , in an accompanying editorial, Mark E. Bernard, MD, of the University of Kentucky College of Medicine, Lexington, highlighted caveats to the study design and raised two core questions: “Should acute toxic effects be the primary endpoint of a single-group, phase 2 study using hypofractionation with fewer cycles of concurrent chemotherapy? Should the primary endpoint rather have been a cancer control endpoint, such as disease-free survival, overall survival, or local control?”
Still, Dr. Bernard wrote, “This trial does help lay the foundation for future pelvic hypofractionated trials with concurrent chemotherapy, especially for gynecological malignant tumors.”
SOURCE:
The research, led by Won Park, MD, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea, was published in JAMA Oncology.
LIMITATIONS:
The trial is a single-arm study, with a short follow-up time. In the editorial, Bernard listed several limitations, including the fact that patients received fewer cycles of concurrent chemotherapy than what’s typically given in this population.
DISCLOSURES:
No funding or relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
Survey Spotlights Identification of Dermatologic Adverse Events From Cancer Therapies
“New cancer therapies have brought a diversity of treatment-related dermatologic adverse events (dAEs) beyond those experienced with conventional chemotherapy, which has demanded an evolving assessment of toxicities,” researchers led by Nicole R. LeBoeuf, MD, MPH, of the Department of Dermatology at Brigham and Women’s Hospital and the Center for Cutaneous Oncology at the Dana-Farber Brigham Cancer Center, Boston, wrote in a poster presented at the American Academy of Dermatology annual meeting.
The authors noted that “Version 5.0 of the Common Terminology Criteria for Adverse Events (CTCAE v5.0)” serves as the current, broadly accepted criteria for classification and grading during routine medical care and clinical trials. But despite extensive utilization of CTCAE, there is little data regarding its application.”
To evaluate how CTCAE is being used in clinical practice, they sent a four-case survey of dAEs to 81 dermatologists and 182 medical oncologists at six US-based academic institutions. For three of the cases, respondents were asked to classify and grade morbilliform, psoriasiform, and papulopustular rashes based on a review of photographs and text descriptions. For the fourth case, respondents were asked to grade a dAE using only a clinic note text description. The researchers used chi-square tests in R software to compare survey responses.
Compared with medical oncologists, dermatologists were significantly more likely to provide correct responses in characterizing morbilliform and psoriasiform eruptions. “As low as 12%” of medical oncologists were correct, and “as low as 87%” of dermatologists were correct (P < .001). Similarly, dermatologists were significantly more likely to grade the psoriasiform, papulopustular, and written cases correctly compared with medical oncologists (P < .001 for all associations).
“These cases demonstrated poor concordance of classification and grading between specialties and across medical oncology,” the authors concluded in their poster, noting that 87% of medical oncologists were interested in additional educational tools on dAEs. “With correct classification as low as 12%, medical oncologists may have more difficulty delivering appropriate, toxicity-specific therapy and may consider banal eruptions dangerous.”
Poor concordance of grading among the two groups of clinicians “raises the question of whether CTCAE v5.0 is an appropriate determinant for patient continuation on therapy or in trials,” they added. “As anticancer therapy becomes more complex — with new toxicities from novel agents and combinations — we must ensure we have a grading system that is valid across investigators and does not harm patients by instituting unnecessary treatment stops.”
Future studies, they said, “can explore what interventions beyond involvement of dermatologists improve classification and grading in practice.”
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the study, noted that with the continued expansion and introduction of new targeted and immunotherapies in the oncology space, “you can be sure we will continue to appreciate the importance and value of the field of supportive oncodermatology, as hair, skin, and nails are almost guaranteed collateral damage in this story.
“Ensuring early identification and consistent grading severity is not only important for the plethora of patients who are currently developing the litany of cutaneous adverse events but to evaluate potential mitigation strategies and even push along countermeasures down the FDA approval pathway,” Dr. Friedman said. In this study, the investigators demonstrated that work “is sorely needed, not just in dermatology but even more so for our colleagues across the aisle. A central tenet of supportive oncodermatology must also be education for all stakeholders, and the good news is our oncology partners will welcome it.”
Dr. LeBoeuf disclosed that she is a consultant to and has received honoraria from Bayer, Seattle Genetics, Sanofi, Silverback, Fortress Biotech, and Synox Therapeutics outside the submitted work. No other authors reported having financial disclosures. Dr. Friedman directs the supportive oncodermatology program at GW that received independent funding from La Roche-Posay.
A version of this article first appeared on Medscape.com.
“New cancer therapies have brought a diversity of treatment-related dermatologic adverse events (dAEs) beyond those experienced with conventional chemotherapy, which has demanded an evolving assessment of toxicities,” researchers led by Nicole R. LeBoeuf, MD, MPH, of the Department of Dermatology at Brigham and Women’s Hospital and the Center for Cutaneous Oncology at the Dana-Farber Brigham Cancer Center, Boston, wrote in a poster presented at the American Academy of Dermatology annual meeting.
The authors noted that “Version 5.0 of the Common Terminology Criteria for Adverse Events (CTCAE v5.0)” serves as the current, broadly accepted criteria for classification and grading during routine medical care and clinical trials. But despite extensive utilization of CTCAE, there is little data regarding its application.”
To evaluate how CTCAE is being used in clinical practice, they sent a four-case survey of dAEs to 81 dermatologists and 182 medical oncologists at six US-based academic institutions. For three of the cases, respondents were asked to classify and grade morbilliform, psoriasiform, and papulopustular rashes based on a review of photographs and text descriptions. For the fourth case, respondents were asked to grade a dAE using only a clinic note text description. The researchers used chi-square tests in R software to compare survey responses.
Compared with medical oncologists, dermatologists were significantly more likely to provide correct responses in characterizing morbilliform and psoriasiform eruptions. “As low as 12%” of medical oncologists were correct, and “as low as 87%” of dermatologists were correct (P < .001). Similarly, dermatologists were significantly more likely to grade the psoriasiform, papulopustular, and written cases correctly compared with medical oncologists (P < .001 for all associations).
“These cases demonstrated poor concordance of classification and grading between specialties and across medical oncology,” the authors concluded in their poster, noting that 87% of medical oncologists were interested in additional educational tools on dAEs. “With correct classification as low as 12%, medical oncologists may have more difficulty delivering appropriate, toxicity-specific therapy and may consider banal eruptions dangerous.”
Poor concordance of grading among the two groups of clinicians “raises the question of whether CTCAE v5.0 is an appropriate determinant for patient continuation on therapy or in trials,” they added. “As anticancer therapy becomes more complex — with new toxicities from novel agents and combinations — we must ensure we have a grading system that is valid across investigators and does not harm patients by instituting unnecessary treatment stops.”
Future studies, they said, “can explore what interventions beyond involvement of dermatologists improve classification and grading in practice.”
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the study, noted that with the continued expansion and introduction of new targeted and immunotherapies in the oncology space, “you can be sure we will continue to appreciate the importance and value of the field of supportive oncodermatology, as hair, skin, and nails are almost guaranteed collateral damage in this story.
“Ensuring early identification and consistent grading severity is not only important for the plethora of patients who are currently developing the litany of cutaneous adverse events but to evaluate potential mitigation strategies and even push along countermeasures down the FDA approval pathway,” Dr. Friedman said. In this study, the investigators demonstrated that work “is sorely needed, not just in dermatology but even more so for our colleagues across the aisle. A central tenet of supportive oncodermatology must also be education for all stakeholders, and the good news is our oncology partners will welcome it.”
Dr. LeBoeuf disclosed that she is a consultant to and has received honoraria from Bayer, Seattle Genetics, Sanofi, Silverback, Fortress Biotech, and Synox Therapeutics outside the submitted work. No other authors reported having financial disclosures. Dr. Friedman directs the supportive oncodermatology program at GW that received independent funding from La Roche-Posay.
A version of this article first appeared on Medscape.com.
“New cancer therapies have brought a diversity of treatment-related dermatologic adverse events (dAEs) beyond those experienced with conventional chemotherapy, which has demanded an evolving assessment of toxicities,” researchers led by Nicole R. LeBoeuf, MD, MPH, of the Department of Dermatology at Brigham and Women’s Hospital and the Center for Cutaneous Oncology at the Dana-Farber Brigham Cancer Center, Boston, wrote in a poster presented at the American Academy of Dermatology annual meeting.
The authors noted that “Version 5.0 of the Common Terminology Criteria for Adverse Events (CTCAE v5.0)” serves as the current, broadly accepted criteria for classification and grading during routine medical care and clinical trials. But despite extensive utilization of CTCAE, there is little data regarding its application.”
To evaluate how CTCAE is being used in clinical practice, they sent a four-case survey of dAEs to 81 dermatologists and 182 medical oncologists at six US-based academic institutions. For three of the cases, respondents were asked to classify and grade morbilliform, psoriasiform, and papulopustular rashes based on a review of photographs and text descriptions. For the fourth case, respondents were asked to grade a dAE using only a clinic note text description. The researchers used chi-square tests in R software to compare survey responses.
Compared with medical oncologists, dermatologists were significantly more likely to provide correct responses in characterizing morbilliform and psoriasiform eruptions. “As low as 12%” of medical oncologists were correct, and “as low as 87%” of dermatologists were correct (P < .001). Similarly, dermatologists were significantly more likely to grade the psoriasiform, papulopustular, and written cases correctly compared with medical oncologists (P < .001 for all associations).
“These cases demonstrated poor concordance of classification and grading between specialties and across medical oncology,” the authors concluded in their poster, noting that 87% of medical oncologists were interested in additional educational tools on dAEs. “With correct classification as low as 12%, medical oncologists may have more difficulty delivering appropriate, toxicity-specific therapy and may consider banal eruptions dangerous.”
Poor concordance of grading among the two groups of clinicians “raises the question of whether CTCAE v5.0 is an appropriate determinant for patient continuation on therapy or in trials,” they added. “As anticancer therapy becomes more complex — with new toxicities from novel agents and combinations — we must ensure we have a grading system that is valid across investigators and does not harm patients by instituting unnecessary treatment stops.”
Future studies, they said, “can explore what interventions beyond involvement of dermatologists improve classification and grading in practice.”
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the study, noted that with the continued expansion and introduction of new targeted and immunotherapies in the oncology space, “you can be sure we will continue to appreciate the importance and value of the field of supportive oncodermatology, as hair, skin, and nails are almost guaranteed collateral damage in this story.
“Ensuring early identification and consistent grading severity is not only important for the plethora of patients who are currently developing the litany of cutaneous adverse events but to evaluate potential mitigation strategies and even push along countermeasures down the FDA approval pathway,” Dr. Friedman said. In this study, the investigators demonstrated that work “is sorely needed, not just in dermatology but even more so for our colleagues across the aisle. A central tenet of supportive oncodermatology must also be education for all stakeholders, and the good news is our oncology partners will welcome it.”
Dr. LeBoeuf disclosed that she is a consultant to and has received honoraria from Bayer, Seattle Genetics, Sanofi, Silverback, Fortress Biotech, and Synox Therapeutics outside the submitted work. No other authors reported having financial disclosures. Dr. Friedman directs the supportive oncodermatology program at GW that received independent funding from La Roche-Posay.
A version of this article first appeared on Medscape.com.
FROM AAD 2024
New mRNA Vaccines in Development for Cancer and Infections
Martina Prelog, MD, a pediatric and adolescent medicine specialist at the University Hospital of Würzburg in Germany, reported on the principles, research status, and perspectives for these vaccines at the 25th Travel and Health Forum of the Center for Travel Medicine in Berlin.
To understand the future, the immunologist first examined the past. “The induction of cellular and humoral immune responses by externally injected mRNA was discovered in the 1990s,” she said.
Instability Challenge
Significant hurdles in mRNA vaccinations included the instability of mRNA and the immune system’s ability to identify foreign mRNA as a threat and destroy mRNA fragments. “The breakthrough toward vaccination came through Dr. Katalin Karikó, who, along with Dr. Drew Weissman, both of the University of Pennsylvania School of Medicine, discovered in 2005 that modifications of mRNA (replacing the nucleoside uridine with pseudouridine) enable better stability of mRNA, reduced immunogenicity, and higher translational capacity at the ribosomes,” said Dr. Prelog.
With this discovery, the two researchers paved the way for the development of mRNA vaccines against COVID-19 and other diseases. They were awarded the Nobel Prize in medicine for their discovery last year.
Improved Scalability
“Since 2009, mRNA vaccines have been studied as a treatment option for cancer,” said Dr. Prelog. “Since 2012, they have been studied for the influenza virus and respiratory syncytial virus [RSV].” Consequently, several mRNA vaccines are currently in development or in approval studies. “The mRNA technology offers the advantage of quickly and flexibly responding to new variants of pathogens and the ability to scale up production when there is high demand for a particular vaccine.”
Different forms and designations of mRNA vaccines are used, depending on the application and desired effect, said Dr. Prelog.
In nucleoside-modified mRNA vaccines, modifications in the mRNA sequence enable the mRNA to remain in the body longer and to induce protein synthesis more effectively.
Lipid nanoparticle (LNP)–encapsulated mRNA vaccines protect the coding mRNA sequences against degradation by the body’s enzymes and facilitate the uptake of mRNA into cells, where it then triggers the production of the desired protein. In addition, LNPs are involved in cell stimulation and support the self-adjuvant effect of mRNA vaccines, thus eliminating the need for adjuvants.
Self-amplifying mRNA vaccines include a special mRNA that replicates itself in the cell and contains a sequence for RNA replicase, in addition to the coding sequence for the protein. This composition enables increased production of the target protein without the need for a high amount of external mRNA administration. Such vaccines could trigger a longer and stronger immune response because the immune system has more time to interact with the protein.
Cancer Immunotherapy
Dr. Prelog also discussed personalized vaccines for cancer immunotherapy. Personalized mRNA vaccines are tailored to the patient’s genetic characteristics and antigens. They could be used in cancer immunotherapy to activate the immune system selectively against tumor cells.
Multivalent mRNA vaccines contain mRNA that codes for multiple antigens rather than just one protein to generate an immune response. These vaccines could be particularly useful in fighting pathogens with variable or changing surface structures or in eliciting protection against multiple pathogens simultaneously.
The technology of mRNA-encoded antibodies involves introducing mRNA into the cell, which creates light and heavy chains of antibodies. This step leads to the formation of antibodies targeted against toxins (eg, diphtheria and tetanus), animal venoms, infectious agents, or tumor cells.
Genetic Engineering
Dr. Prelog also reviewed genetic engineering techniques. In regenerative therapy or protein replacement therapy, skin fibroblasts or other cells are transfected with mRNA to enable conversion into induced pluripotent stem cells. This approach avoids the risk for DNA integration into the genome and associated mutation risks.
Another approach is making post-transcriptional modifications through RNA interference. For example, RNA structures can be used to inhibit the translation of disease-causing proteins. This technique is currently being tested against HIV and tumors such as melanoma.
In addition, mRNA technologies can be combined with CRISPR/Cas9 technology (“gene scissors”) to influence the creation of gene products even more precisely. The advantage of this technique is that mRNA is only transiently expressed, thus preventing unwanted side effects. Furthermore, mRNA is translated directly in the cytoplasm, leading to a faster initiation of gene editing.
Of the numerous ongoing clinical mRNA vaccine studies, around 70% focus on infections, about 12% on cancer, and the rest on autoimmune diseases and neurodegenerative disorders, said Dr. Prelog.
Research in Infections
Research in the fields of infectious diseases and oncology is the most advanced: mRNA vaccines against influenza and RSV are already in advanced clinical trials, Dr. Prelog told this news organization.
“Conventional influenza vaccines contain immunogenic surface molecules against hemagglutinin and neuraminidase in various combinations of influenza strains A and B and are produced in egg or cell cultures,” she said. “This is a time-consuming manufacturing process that takes months and, particularly with the egg-based process, bears the risk of changing the vaccine strain.”
“Additionally, influenza viruses undergo antigenic shift and drift through recombination, thus requiring annual adjustments to the vaccines. Thus, these influenza vaccines often lose accuracy in targeting circulating seasonal influenza strains.”
Several mRNA vaccines being tested contain not only coding sequences against hemagglutinin and neuraminidase but also for structural proteins of influenza viruses. “These are more conserved and mutate less easily, meaning they could serve as the basis for universal pandemic influenza vaccines,” said Dr. Prelog.
An advantage of mRNA vaccines, she added, is the strong cellular immune response that they elicit. This response is intended to provide additional protection alongside specific antibodies. An mRNA vaccine with coding sequences for the pre-fusion protein of RSV is in phase 3 trials for approval for vaccination in patients aged 60 years and older. It shows high effectiveness even in older patients and those with comorbidities.
Elaborate Purification Process
Bacterial origin plasmid DNA is used to produce mRNA vaccines. The mRNA vaccines for COVID-19 raised concerns that production-related DNA residues could pose a safety risk and cause autoimmune diseases.
These vaccines “typically undergo a very elaborate purification process,” said Dr. Prelog. “This involves enzymatic digestion with DNase to fragment and deplete plasmid DNA, followed by purification using chromatography columns, so that no safety-relevant DNA fragments should remain afterward.”
Thus, the Paul-Ehrlich-Institut also pointed out the very small, fragmented plasmid DNA residues of bacterial origin in mRNA COVID-19 vaccines pose no risk, unlike residual DNA from animal cell culture might pose in other vaccines.
Prevention and Therapy
In addition to the numerous advantages of mRNA vaccines (such as rapid adaptability to new or mutated pathogens, scalability, rapid production capability, self-adjuvant effect, strong induction of cellular immune responses, and safety), there are also challenges in RNA technology as a preventive and therapeutic measure, according to Dr. Prelog.
“Stability and storability, as well as the costs of new vaccine developments, play a role, as do the long-term effects regarding the persistence of antibody and cellular responses,” she said. The COVID-19 mRNA vaccines, for example, showed a well-maintained cellular immune response despite a tendency toward a rapid decline in humoral immune response.
“The experience with COVID-19 mRNA vaccines and the new vaccine developments based on mRNA technology give hope for an efficient and safe preventive and therapeutic use, particularly in the fields of infectious diseases and oncology,” Dr. Prelog concluded.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Martina Prelog, MD, a pediatric and adolescent medicine specialist at the University Hospital of Würzburg in Germany, reported on the principles, research status, and perspectives for these vaccines at the 25th Travel and Health Forum of the Center for Travel Medicine in Berlin.
To understand the future, the immunologist first examined the past. “The induction of cellular and humoral immune responses by externally injected mRNA was discovered in the 1990s,” she said.
Instability Challenge
Significant hurdles in mRNA vaccinations included the instability of mRNA and the immune system’s ability to identify foreign mRNA as a threat and destroy mRNA fragments. “The breakthrough toward vaccination came through Dr. Katalin Karikó, who, along with Dr. Drew Weissman, both of the University of Pennsylvania School of Medicine, discovered in 2005 that modifications of mRNA (replacing the nucleoside uridine with pseudouridine) enable better stability of mRNA, reduced immunogenicity, and higher translational capacity at the ribosomes,” said Dr. Prelog.
With this discovery, the two researchers paved the way for the development of mRNA vaccines against COVID-19 and other diseases. They were awarded the Nobel Prize in medicine for their discovery last year.
Improved Scalability
“Since 2009, mRNA vaccines have been studied as a treatment option for cancer,” said Dr. Prelog. “Since 2012, they have been studied for the influenza virus and respiratory syncytial virus [RSV].” Consequently, several mRNA vaccines are currently in development or in approval studies. “The mRNA technology offers the advantage of quickly and flexibly responding to new variants of pathogens and the ability to scale up production when there is high demand for a particular vaccine.”
Different forms and designations of mRNA vaccines are used, depending on the application and desired effect, said Dr. Prelog.
In nucleoside-modified mRNA vaccines, modifications in the mRNA sequence enable the mRNA to remain in the body longer and to induce protein synthesis more effectively.
Lipid nanoparticle (LNP)–encapsulated mRNA vaccines protect the coding mRNA sequences against degradation by the body’s enzymes and facilitate the uptake of mRNA into cells, where it then triggers the production of the desired protein. In addition, LNPs are involved in cell stimulation and support the self-adjuvant effect of mRNA vaccines, thus eliminating the need for adjuvants.
Self-amplifying mRNA vaccines include a special mRNA that replicates itself in the cell and contains a sequence for RNA replicase, in addition to the coding sequence for the protein. This composition enables increased production of the target protein without the need for a high amount of external mRNA administration. Such vaccines could trigger a longer and stronger immune response because the immune system has more time to interact with the protein.
Cancer Immunotherapy
Dr. Prelog also discussed personalized vaccines for cancer immunotherapy. Personalized mRNA vaccines are tailored to the patient’s genetic characteristics and antigens. They could be used in cancer immunotherapy to activate the immune system selectively against tumor cells.
Multivalent mRNA vaccines contain mRNA that codes for multiple antigens rather than just one protein to generate an immune response. These vaccines could be particularly useful in fighting pathogens with variable or changing surface structures or in eliciting protection against multiple pathogens simultaneously.
The technology of mRNA-encoded antibodies involves introducing mRNA into the cell, which creates light and heavy chains of antibodies. This step leads to the formation of antibodies targeted against toxins (eg, diphtheria and tetanus), animal venoms, infectious agents, or tumor cells.
Genetic Engineering
Dr. Prelog also reviewed genetic engineering techniques. In regenerative therapy or protein replacement therapy, skin fibroblasts or other cells are transfected with mRNA to enable conversion into induced pluripotent stem cells. This approach avoids the risk for DNA integration into the genome and associated mutation risks.
Another approach is making post-transcriptional modifications through RNA interference. For example, RNA structures can be used to inhibit the translation of disease-causing proteins. This technique is currently being tested against HIV and tumors such as melanoma.
In addition, mRNA technologies can be combined with CRISPR/Cas9 technology (“gene scissors”) to influence the creation of gene products even more precisely. The advantage of this technique is that mRNA is only transiently expressed, thus preventing unwanted side effects. Furthermore, mRNA is translated directly in the cytoplasm, leading to a faster initiation of gene editing.
Of the numerous ongoing clinical mRNA vaccine studies, around 70% focus on infections, about 12% on cancer, and the rest on autoimmune diseases and neurodegenerative disorders, said Dr. Prelog.
Research in Infections
Research in the fields of infectious diseases and oncology is the most advanced: mRNA vaccines against influenza and RSV are already in advanced clinical trials, Dr. Prelog told this news organization.
“Conventional influenza vaccines contain immunogenic surface molecules against hemagglutinin and neuraminidase in various combinations of influenza strains A and B and are produced in egg or cell cultures,” she said. “This is a time-consuming manufacturing process that takes months and, particularly with the egg-based process, bears the risk of changing the vaccine strain.”
“Additionally, influenza viruses undergo antigenic shift and drift through recombination, thus requiring annual adjustments to the vaccines. Thus, these influenza vaccines often lose accuracy in targeting circulating seasonal influenza strains.”
Several mRNA vaccines being tested contain not only coding sequences against hemagglutinin and neuraminidase but also for structural proteins of influenza viruses. “These are more conserved and mutate less easily, meaning they could serve as the basis for universal pandemic influenza vaccines,” said Dr. Prelog.
An advantage of mRNA vaccines, she added, is the strong cellular immune response that they elicit. This response is intended to provide additional protection alongside specific antibodies. An mRNA vaccine with coding sequences for the pre-fusion protein of RSV is in phase 3 trials for approval for vaccination in patients aged 60 years and older. It shows high effectiveness even in older patients and those with comorbidities.
Elaborate Purification Process
Bacterial origin plasmid DNA is used to produce mRNA vaccines. The mRNA vaccines for COVID-19 raised concerns that production-related DNA residues could pose a safety risk and cause autoimmune diseases.
These vaccines “typically undergo a very elaborate purification process,” said Dr. Prelog. “This involves enzymatic digestion with DNase to fragment and deplete plasmid DNA, followed by purification using chromatography columns, so that no safety-relevant DNA fragments should remain afterward.”
Thus, the Paul-Ehrlich-Institut also pointed out the very small, fragmented plasmid DNA residues of bacterial origin in mRNA COVID-19 vaccines pose no risk, unlike residual DNA from animal cell culture might pose in other vaccines.
Prevention and Therapy
In addition to the numerous advantages of mRNA vaccines (such as rapid adaptability to new or mutated pathogens, scalability, rapid production capability, self-adjuvant effect, strong induction of cellular immune responses, and safety), there are also challenges in RNA technology as a preventive and therapeutic measure, according to Dr. Prelog.
“Stability and storability, as well as the costs of new vaccine developments, play a role, as do the long-term effects regarding the persistence of antibody and cellular responses,” she said. The COVID-19 mRNA vaccines, for example, showed a well-maintained cellular immune response despite a tendency toward a rapid decline in humoral immune response.
“The experience with COVID-19 mRNA vaccines and the new vaccine developments based on mRNA technology give hope for an efficient and safe preventive and therapeutic use, particularly in the fields of infectious diseases and oncology,” Dr. Prelog concluded.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Martina Prelog, MD, a pediatric and adolescent medicine specialist at the University Hospital of Würzburg in Germany, reported on the principles, research status, and perspectives for these vaccines at the 25th Travel and Health Forum of the Center for Travel Medicine in Berlin.
To understand the future, the immunologist first examined the past. “The induction of cellular and humoral immune responses by externally injected mRNA was discovered in the 1990s,” she said.
Instability Challenge
Significant hurdles in mRNA vaccinations included the instability of mRNA and the immune system’s ability to identify foreign mRNA as a threat and destroy mRNA fragments. “The breakthrough toward vaccination came through Dr. Katalin Karikó, who, along with Dr. Drew Weissman, both of the University of Pennsylvania School of Medicine, discovered in 2005 that modifications of mRNA (replacing the nucleoside uridine with pseudouridine) enable better stability of mRNA, reduced immunogenicity, and higher translational capacity at the ribosomes,” said Dr. Prelog.
With this discovery, the two researchers paved the way for the development of mRNA vaccines against COVID-19 and other diseases. They were awarded the Nobel Prize in medicine for their discovery last year.
Improved Scalability
“Since 2009, mRNA vaccines have been studied as a treatment option for cancer,” said Dr. Prelog. “Since 2012, they have been studied for the influenza virus and respiratory syncytial virus [RSV].” Consequently, several mRNA vaccines are currently in development or in approval studies. “The mRNA technology offers the advantage of quickly and flexibly responding to new variants of pathogens and the ability to scale up production when there is high demand for a particular vaccine.”
Different forms and designations of mRNA vaccines are used, depending on the application and desired effect, said Dr. Prelog.
In nucleoside-modified mRNA vaccines, modifications in the mRNA sequence enable the mRNA to remain in the body longer and to induce protein synthesis more effectively.
Lipid nanoparticle (LNP)–encapsulated mRNA vaccines protect the coding mRNA sequences against degradation by the body’s enzymes and facilitate the uptake of mRNA into cells, where it then triggers the production of the desired protein. In addition, LNPs are involved in cell stimulation and support the self-adjuvant effect of mRNA vaccines, thus eliminating the need for adjuvants.
Self-amplifying mRNA vaccines include a special mRNA that replicates itself in the cell and contains a sequence for RNA replicase, in addition to the coding sequence for the protein. This composition enables increased production of the target protein without the need for a high amount of external mRNA administration. Such vaccines could trigger a longer and stronger immune response because the immune system has more time to interact with the protein.
Cancer Immunotherapy
Dr. Prelog also discussed personalized vaccines for cancer immunotherapy. Personalized mRNA vaccines are tailored to the patient’s genetic characteristics and antigens. They could be used in cancer immunotherapy to activate the immune system selectively against tumor cells.
Multivalent mRNA vaccines contain mRNA that codes for multiple antigens rather than just one protein to generate an immune response. These vaccines could be particularly useful in fighting pathogens with variable or changing surface structures or in eliciting protection against multiple pathogens simultaneously.
The technology of mRNA-encoded antibodies involves introducing mRNA into the cell, which creates light and heavy chains of antibodies. This step leads to the formation of antibodies targeted against toxins (eg, diphtheria and tetanus), animal venoms, infectious agents, or tumor cells.
Genetic Engineering
Dr. Prelog also reviewed genetic engineering techniques. In regenerative therapy or protein replacement therapy, skin fibroblasts or other cells are transfected with mRNA to enable conversion into induced pluripotent stem cells. This approach avoids the risk for DNA integration into the genome and associated mutation risks.
Another approach is making post-transcriptional modifications through RNA interference. For example, RNA structures can be used to inhibit the translation of disease-causing proteins. This technique is currently being tested against HIV and tumors such as melanoma.
In addition, mRNA technologies can be combined with CRISPR/Cas9 technology (“gene scissors”) to influence the creation of gene products even more precisely. The advantage of this technique is that mRNA is only transiently expressed, thus preventing unwanted side effects. Furthermore, mRNA is translated directly in the cytoplasm, leading to a faster initiation of gene editing.
Of the numerous ongoing clinical mRNA vaccine studies, around 70% focus on infections, about 12% on cancer, and the rest on autoimmune diseases and neurodegenerative disorders, said Dr. Prelog.
Research in Infections
Research in the fields of infectious diseases and oncology is the most advanced: mRNA vaccines against influenza and RSV are already in advanced clinical trials, Dr. Prelog told this news organization.
“Conventional influenza vaccines contain immunogenic surface molecules against hemagglutinin and neuraminidase in various combinations of influenza strains A and B and are produced in egg or cell cultures,” she said. “This is a time-consuming manufacturing process that takes months and, particularly with the egg-based process, bears the risk of changing the vaccine strain.”
“Additionally, influenza viruses undergo antigenic shift and drift through recombination, thus requiring annual adjustments to the vaccines. Thus, these influenza vaccines often lose accuracy in targeting circulating seasonal influenza strains.”
Several mRNA vaccines being tested contain not only coding sequences against hemagglutinin and neuraminidase but also for structural proteins of influenza viruses. “These are more conserved and mutate less easily, meaning they could serve as the basis for universal pandemic influenza vaccines,” said Dr. Prelog.
An advantage of mRNA vaccines, she added, is the strong cellular immune response that they elicit. This response is intended to provide additional protection alongside specific antibodies. An mRNA vaccine with coding sequences for the pre-fusion protein of RSV is in phase 3 trials for approval for vaccination in patients aged 60 years and older. It shows high effectiveness even in older patients and those with comorbidities.
Elaborate Purification Process
Bacterial origin plasmid DNA is used to produce mRNA vaccines. The mRNA vaccines for COVID-19 raised concerns that production-related DNA residues could pose a safety risk and cause autoimmune diseases.
These vaccines “typically undergo a very elaborate purification process,” said Dr. Prelog. “This involves enzymatic digestion with DNase to fragment and deplete plasmid DNA, followed by purification using chromatography columns, so that no safety-relevant DNA fragments should remain afterward.”
Thus, the Paul-Ehrlich-Institut also pointed out the very small, fragmented plasmid DNA residues of bacterial origin in mRNA COVID-19 vaccines pose no risk, unlike residual DNA from animal cell culture might pose in other vaccines.
Prevention and Therapy
In addition to the numerous advantages of mRNA vaccines (such as rapid adaptability to new or mutated pathogens, scalability, rapid production capability, self-adjuvant effect, strong induction of cellular immune responses, and safety), there are also challenges in RNA technology as a preventive and therapeutic measure, according to Dr. Prelog.
“Stability and storability, as well as the costs of new vaccine developments, play a role, as do the long-term effects regarding the persistence of antibody and cellular responses,” she said. The COVID-19 mRNA vaccines, for example, showed a well-maintained cellular immune response despite a tendency toward a rapid decline in humoral immune response.
“The experience with COVID-19 mRNA vaccines and the new vaccine developments based on mRNA technology give hope for an efficient and safe preventive and therapeutic use, particularly in the fields of infectious diseases and oncology,” Dr. Prelog concluded.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.