User login
Children and COVID: New cases fall again, ED rates rebound for some
The 7-day average percentage of ED visits with diagnosed COVID, which had reached a post-Omicron high of 3.5% in late July for those aged 12-15, began to fall and was down to 3.0% on Aug. 12. That trend reversed, however, and the rate was up to 3.6% on Aug. 19, the last date for which data are available from the Centers for Disease Control and Prevention.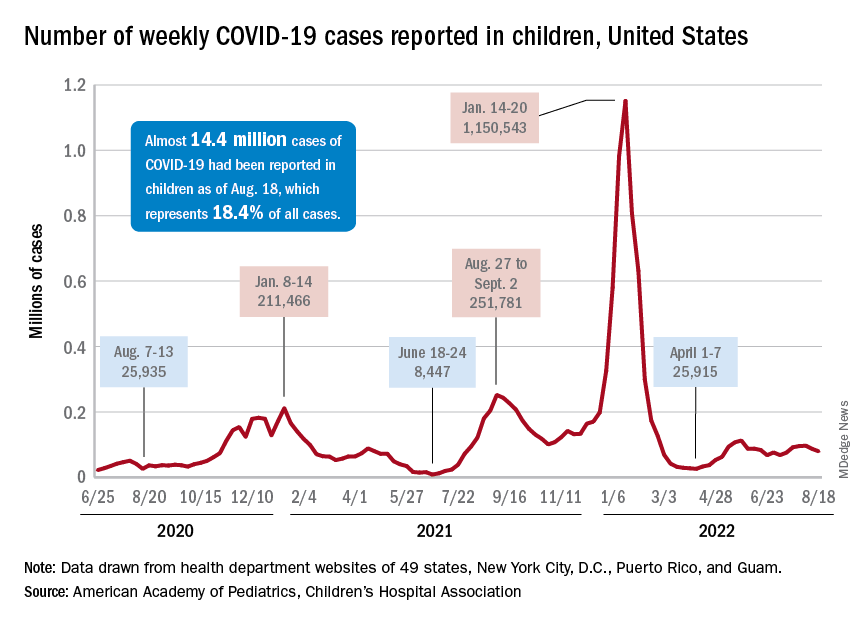
That change of COVID fortunes cannot yet be seen for all children. The 7-day average ED visit rate for those aged 0-11 years peaked at 6.8% during the last week of July and has continued to fall, dropping from 5.7% on Aug. 12 to 5.1% on Aug. 19. Children aged 16-17 years seem to be taking a middle path: Their ED-visit rate declined from late July into mid-August but held steady over the last week, according to the CDC’s COVID Data Tracker.
There is a hint of the same trend regarding new admissions among children aged 0-17 years. The national rate, which had declined in recent weeks, ticked up from 0.42 to 0.43 new admissions per 100,000 population over the last week of available data, the CDC said.
Weekly cases fall below 80,000
New cases in general were down by 8.5% from the previous week, dropping from 87,902 for the week of Aug. 5-11 to 79,525 for Aug. 12-18. That marked the second straight week with fewer cases after a 4-week period that saw weekly totals increase from almost 68,000 to nearly 97,000, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP and CHA put the cumulative number of child COVID-19 cases at just under 14.4 million since the pandemic began, which represents 18.4% of cases among all ages. The CDC estimates that there have been almost 14.7 million cases in children aged 0-17 years, as well as 1,750 deaths, of which 14 were reported in the last week (Aug. 16-22).
The CDC age subgroups indicate that children aged 0-4 years have experienced fewer cases (2.9 million) than children aged 5-11 years (5.6 million cases) and 12-15 (3.0 million cases) but more deaths: 548 so far, versus 432 for 5- to 11-year-olds and 437 for 12- to 15-year-olds, the COVID Data Tracker shows. Those aged 0-4 make up 6% of the total U.S. population, compared with 8.7% and 5.1%, respectively, for the older children.
Most younger children still not vaccinated
Although it may not qualify as a big push to vaccinate children before the start of the new school year, first-time vaccinations did rise somewhat in late July and August for children aged 5-17 years. Among children younger than 5 years, though, initial doses of the vaccine fell during the second full week of August, especially in 2- to 4-year-olds, based on the CDC data.
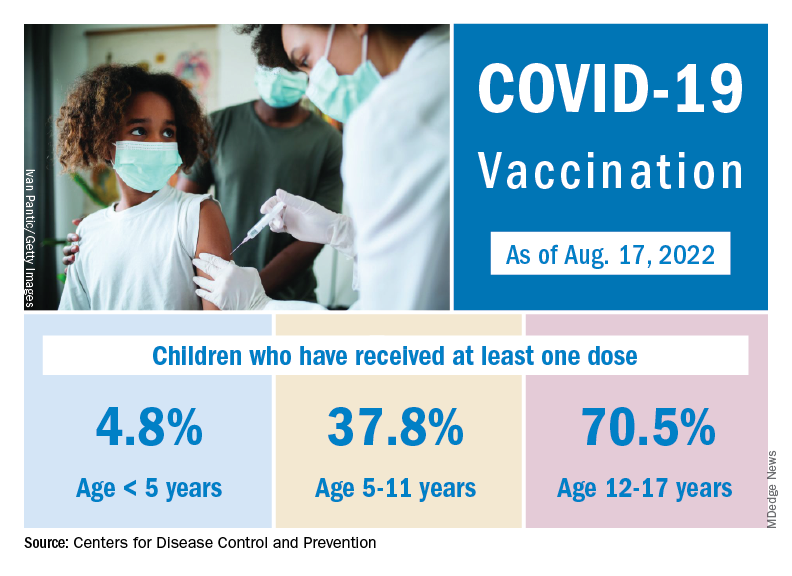
Through almost 2 months of vaccine eligibility, 4.8% of children under age 5 have received at least one dose and 0.9% are fully vaccinated as of Aug. 17. The current rates are 37.8% (one dose) and 30.4% (completed) for those aged 5-11 and 70.5% and 60.3% for 12- to 17-year-olds.
The 7-day average percentage of ED visits with diagnosed COVID, which had reached a post-Omicron high of 3.5% in late July for those aged 12-15, began to fall and was down to 3.0% on Aug. 12. That trend reversed, however, and the rate was up to 3.6% on Aug. 19, the last date for which data are available from the Centers for Disease Control and Prevention.
That change of COVID fortunes cannot yet be seen for all children. The 7-day average ED visit rate for those aged 0-11 years peaked at 6.8% during the last week of July and has continued to fall, dropping from 5.7% on Aug. 12 to 5.1% on Aug. 19. Children aged 16-17 years seem to be taking a middle path: Their ED-visit rate declined from late July into mid-August but held steady over the last week, according to the CDC’s COVID Data Tracker.
There is a hint of the same trend regarding new admissions among children aged 0-17 years. The national rate, which had declined in recent weeks, ticked up from 0.42 to 0.43 new admissions per 100,000 population over the last week of available data, the CDC said.
Weekly cases fall below 80,000
New cases in general were down by 8.5% from the previous week, dropping from 87,902 for the week of Aug. 5-11 to 79,525 for Aug. 12-18. That marked the second straight week with fewer cases after a 4-week period that saw weekly totals increase from almost 68,000 to nearly 97,000, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP and CHA put the cumulative number of child COVID-19 cases at just under 14.4 million since the pandemic began, which represents 18.4% of cases among all ages. The CDC estimates that there have been almost 14.7 million cases in children aged 0-17 years, as well as 1,750 deaths, of which 14 were reported in the last week (Aug. 16-22).
The CDC age subgroups indicate that children aged 0-4 years have experienced fewer cases (2.9 million) than children aged 5-11 years (5.6 million cases) and 12-15 (3.0 million cases) but more deaths: 548 so far, versus 432 for 5- to 11-year-olds and 437 for 12- to 15-year-olds, the COVID Data Tracker shows. Those aged 0-4 make up 6% of the total U.S. population, compared with 8.7% and 5.1%, respectively, for the older children.
Most younger children still not vaccinated
Although it may not qualify as a big push to vaccinate children before the start of the new school year, first-time vaccinations did rise somewhat in late July and August for children aged 5-17 years. Among children younger than 5 years, though, initial doses of the vaccine fell during the second full week of August, especially in 2- to 4-year-olds, based on the CDC data.
Through almost 2 months of vaccine eligibility, 4.8% of children under age 5 have received at least one dose and 0.9% are fully vaccinated as of Aug. 17. The current rates are 37.8% (one dose) and 30.4% (completed) for those aged 5-11 and 70.5% and 60.3% for 12- to 17-year-olds.
The 7-day average percentage of ED visits with diagnosed COVID, which had reached a post-Omicron high of 3.5% in late July for those aged 12-15, began to fall and was down to 3.0% on Aug. 12. That trend reversed, however, and the rate was up to 3.6% on Aug. 19, the last date for which data are available from the Centers for Disease Control and Prevention.
That change of COVID fortunes cannot yet be seen for all children. The 7-day average ED visit rate for those aged 0-11 years peaked at 6.8% during the last week of July and has continued to fall, dropping from 5.7% on Aug. 12 to 5.1% on Aug. 19. Children aged 16-17 years seem to be taking a middle path: Their ED-visit rate declined from late July into mid-August but held steady over the last week, according to the CDC’s COVID Data Tracker.
There is a hint of the same trend regarding new admissions among children aged 0-17 years. The national rate, which had declined in recent weeks, ticked up from 0.42 to 0.43 new admissions per 100,000 population over the last week of available data, the CDC said.
Weekly cases fall below 80,000
New cases in general were down by 8.5% from the previous week, dropping from 87,902 for the week of Aug. 5-11 to 79,525 for Aug. 12-18. That marked the second straight week with fewer cases after a 4-week period that saw weekly totals increase from almost 68,000 to nearly 97,000, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP and CHA put the cumulative number of child COVID-19 cases at just under 14.4 million since the pandemic began, which represents 18.4% of cases among all ages. The CDC estimates that there have been almost 14.7 million cases in children aged 0-17 years, as well as 1,750 deaths, of which 14 were reported in the last week (Aug. 16-22).
The CDC age subgroups indicate that children aged 0-4 years have experienced fewer cases (2.9 million) than children aged 5-11 years (5.6 million cases) and 12-15 (3.0 million cases) but more deaths: 548 so far, versus 432 for 5- to 11-year-olds and 437 for 12- to 15-year-olds, the COVID Data Tracker shows. Those aged 0-4 make up 6% of the total U.S. population, compared with 8.7% and 5.1%, respectively, for the older children.
Most younger children still not vaccinated
Although it may not qualify as a big push to vaccinate children before the start of the new school year, first-time vaccinations did rise somewhat in late July and August for children aged 5-17 years. Among children younger than 5 years, though, initial doses of the vaccine fell during the second full week of August, especially in 2- to 4-year-olds, based on the CDC data.
Through almost 2 months of vaccine eligibility, 4.8% of children under age 5 have received at least one dose and 0.9% are fully vaccinated as of Aug. 17. The current rates are 37.8% (one dose) and 30.4% (completed) for those aged 5-11 and 70.5% and 60.3% for 12- to 17-year-olds.
How does not getting enough sleep affect the developing brain?
Children who do not get enough sleep for one night can be cranky, groggy, or meltdown prone the next day.
Over time, though, insufficient sleep may impair neurodevelopment in ways that can be measured on brain scans and tests long term, a new study shows.
Research published in The Lancet Child & Adolescent Health found that 9- and 10-year-olds who do not get at least 9 hours of sleep most nights tend to have less gray matter and smaller areas of the brain responsible for attention, memory, and inhibition control, relative to children who do get enough sleep.
The researchers also found a relationship between insufficient sleep and disrupted connections between the basal ganglia and cortical regions of the brain. These disruptions appeared to be linked to depression, thought problems, and impairments in crystallized intelligence, a type of intelligence that depends on memory.
The overall patterns persisted 2 years later, even as those who got enough sleep at baseline gradually slept less over time, while those who were not getting enough sleep to begin with continued to sleep about the same amount, the researchers reported.
The results bolster the case for delaying school start times, as California recently did, according one researcher who was not involved in the study.
The ABCD Study
To examine how insufficient sleep affects children’s mental health, cognition, brain function, and brain structure over 2 years, Ze Wang, PhD, professor of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, and colleagues analyzed data from the ongoing Adolescent Brain Cognitive Development (ABCD) Study. The ABCD Study is tracking the biologic and behavioral development of more than 11,000 children in the United States who were recruited for the study when they were 9 or 10 years old.

For their new analysis, Dr. Wang’s group focused on 6,042 participants: 3,021 children with insufficient sleep who were matched with an equal number of participants who were similar in many respects, including sex, socioeconomic status, and puberty status, except they got at least 9 hours of sleep. They also looked at outcomes 2 years later from 749 of the matched pairs who had results available.
The investigators determined sleep duration based on how parents answered the question: “How many hours of sleep does your child get on most nights in the past 6 months?” Possible answers included at least 9 hours, 8-9 hours, 7-8 hours, 5-7 hours, or less than 5 hours. They also looked at functional and structural MRI scans, test results, and responses to questionnaires.
Negative effects of inadequate sleep were spread over “several different domains including brain structure, function, cognition, behavior, and mental health,” Dr. Wang said.
The strength of the relationship between sleep duration and the various outcomes was “modest” and based on group averages, he said. So, a given child who does not sleep for 9 hours most nights won’t necessarily perform worse than a child who gets enough sleep.
Still, modest effects may accumulate and have lasting consequences, Dr. Wang said.
Crystallized intelligence
The researchers looked at 42 behavioral outcomes, 32 of which were significantly different between the groups. Four outcomes in particular – depression, thought problems, performance on a picture-vocabulary test, and crystallized intelligence – were areas where insufficient sleep seemed to have a larger negative effect.
Sleep duration’s relationship with crystallized intelligence was twice that for fluid intelligence, which does not depend on memory.
“Sleep affects memory,” Dr. Wang said. “Crystallized intelligence depends on learned skills and knowledge, which are memory. In this sense, sleep is related to crystallized intelligence.”
One limitation of the study is that some parents may not accurately report how much sleep their child gets, Dr. Wang acknowledged. Children may be awake when parents think they are asleep, for example.
And although the results show getting 9 hours of sleep may help neurocognitive development, it’s also possible that excessive amounts of sleep could be problematic, the study authors wrote.
Further experiments are needed to prove that insufficient sleep – and not some other, unaccounted for factor – causes the observed impairments in neurodevelopment.
To promote healthy sleep, parents should keep a strict routine for their children, such as a regular bedtime and no electronic devices in the bedroom, Dr. Wang suggested. More physical activity during the day also should help.
If children have high levels of stress and depression, “finding the source is critical,” he said. Likewise, clinicians should consider how mental health can affect their patients’ sleep.
More to healthy sleep than duration
“This study both aligns with and advances existing research on the importance of sufficient sleep for child well-being,” said Ariel A. Williamson, PhD, DBSM, a psychologist and pediatric sleep expert in the department of child and adolescent psychiatry and behavioral sciences at Children’s Hospital of Philadelphia and assistant professor of psychiatry and pediatrics at University of Pennsylvania, also in Philadelphia.

The researchers used rigorous propensity score matching, longitudinal data, and brain imaging, which are “innovative methods that provide more evidence on potential mechanisms linking insufficient sleep and child outcomes,” said Dr. Williamson, who was not involved in the study.
While the investigators focused on sleep duration, child sleep health is multidimensional and includes other elements like timing and perception of sleep quality, Dr. Williamson noted. “For example, some research shows that having a sleep schedule that varies night to night is linked to poor child outcomes.”
Dr. Williamson tells families and clinicians that “sleep is a pillar of health,” equal to diet and exercise. That said, sleep recommendations need to fit within a family’s life – taking into account after school activities and late-night homework sessions. But extending sleep by just “20-30 minutes can make a meaningful difference for daytime functioning,” Dr. Williamson said.
Start school later?
Researchers have only relatively recently begun to understand how insufficient sleep affects adolescent neurocognitive development long term, and this study provides “crucial evidence” about the consequences, Lydia Gabriela Speyer, PhD, said in an editorial published with the study. Dr. Speyer is affiliated with the department of psychology at the University of Cambridge (England).
“Given the novel finding that insufficient sleep is associated with changes in brain structure and connectivity that are long-lasting, early intervention is crucial because such neural changes are probably not reversible and might consequently affect adolescents’ development into adulthood,” Dr. Speyer wrote.
Delaying school start times could be one way to help kids get more sleep. The American Academy of Pediatrics and the American Academy of Sleep Medicine recommend that middle schools and high schools start no earlier than 8:30 a.m. to better align with students’ circadian rhythm, Dr. Speyer noted.
As it is in the United States, most schools start closer to 8 a.m. In California, though, a law that went into effect on July 1 prohibits high schools from starting before 8:30 a.m. Other states are weighing similar legislation.
The research was supported by the National Institutes of Health. Dr. Wang and his coauthors and Dr. Speyer had no conflict of interest disclosures. Dr. Williamson is a sleep expert for the Pediatric Sleep Council (www.babysleep.com), which provides free information about early childhood sleep, but she does not receive compensation for this role.
Children who do not get enough sleep for one night can be cranky, groggy, or meltdown prone the next day.
Over time, though, insufficient sleep may impair neurodevelopment in ways that can be measured on brain scans and tests long term, a new study shows.
Research published in The Lancet Child & Adolescent Health found that 9- and 10-year-olds who do not get at least 9 hours of sleep most nights tend to have less gray matter and smaller areas of the brain responsible for attention, memory, and inhibition control, relative to children who do get enough sleep.
The researchers also found a relationship between insufficient sleep and disrupted connections between the basal ganglia and cortical regions of the brain. These disruptions appeared to be linked to depression, thought problems, and impairments in crystallized intelligence, a type of intelligence that depends on memory.
The overall patterns persisted 2 years later, even as those who got enough sleep at baseline gradually slept less over time, while those who were not getting enough sleep to begin with continued to sleep about the same amount, the researchers reported.
The results bolster the case for delaying school start times, as California recently did, according one researcher who was not involved in the study.
The ABCD Study
To examine how insufficient sleep affects children’s mental health, cognition, brain function, and brain structure over 2 years, Ze Wang, PhD, professor of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, and colleagues analyzed data from the ongoing Adolescent Brain Cognitive Development (ABCD) Study. The ABCD Study is tracking the biologic and behavioral development of more than 11,000 children in the United States who were recruited for the study when they were 9 or 10 years old.
For their new analysis, Dr. Wang’s group focused on 6,042 participants: 3,021 children with insufficient sleep who were matched with an equal number of participants who were similar in many respects, including sex, socioeconomic status, and puberty status, except they got at least 9 hours of sleep. They also looked at outcomes 2 years later from 749 of the matched pairs who had results available.
The investigators determined sleep duration based on how parents answered the question: “How many hours of sleep does your child get on most nights in the past 6 months?” Possible answers included at least 9 hours, 8-9 hours, 7-8 hours, 5-7 hours, or less than 5 hours. They also looked at functional and structural MRI scans, test results, and responses to questionnaires.
Negative effects of inadequate sleep were spread over “several different domains including brain structure, function, cognition, behavior, and mental health,” Dr. Wang said.
The strength of the relationship between sleep duration and the various outcomes was “modest” and based on group averages, he said. So, a given child who does not sleep for 9 hours most nights won’t necessarily perform worse than a child who gets enough sleep.
Still, modest effects may accumulate and have lasting consequences, Dr. Wang said.
Crystallized intelligence
The researchers looked at 42 behavioral outcomes, 32 of which were significantly different between the groups. Four outcomes in particular – depression, thought problems, performance on a picture-vocabulary test, and crystallized intelligence – were areas where insufficient sleep seemed to have a larger negative effect.
Sleep duration’s relationship with crystallized intelligence was twice that for fluid intelligence, which does not depend on memory.
“Sleep affects memory,” Dr. Wang said. “Crystallized intelligence depends on learned skills and knowledge, which are memory. In this sense, sleep is related to crystallized intelligence.”
One limitation of the study is that some parents may not accurately report how much sleep their child gets, Dr. Wang acknowledged. Children may be awake when parents think they are asleep, for example.
And although the results show getting 9 hours of sleep may help neurocognitive development, it’s also possible that excessive amounts of sleep could be problematic, the study authors wrote.
Further experiments are needed to prove that insufficient sleep – and not some other, unaccounted for factor – causes the observed impairments in neurodevelopment.
To promote healthy sleep, parents should keep a strict routine for their children, such as a regular bedtime and no electronic devices in the bedroom, Dr. Wang suggested. More physical activity during the day also should help.
If children have high levels of stress and depression, “finding the source is critical,” he said. Likewise, clinicians should consider how mental health can affect their patients’ sleep.
More to healthy sleep than duration
“This study both aligns with and advances existing research on the importance of sufficient sleep for child well-being,” said Ariel A. Williamson, PhD, DBSM, a psychologist and pediatric sleep expert in the department of child and adolescent psychiatry and behavioral sciences at Children’s Hospital of Philadelphia and assistant professor of psychiatry and pediatrics at University of Pennsylvania, also in Philadelphia.
The researchers used rigorous propensity score matching, longitudinal data, and brain imaging, which are “innovative methods that provide more evidence on potential mechanisms linking insufficient sleep and child outcomes,” said Dr. Williamson, who was not involved in the study.
While the investigators focused on sleep duration, child sleep health is multidimensional and includes other elements like timing and perception of sleep quality, Dr. Williamson noted. “For example, some research shows that having a sleep schedule that varies night to night is linked to poor child outcomes.”
Dr. Williamson tells families and clinicians that “sleep is a pillar of health,” equal to diet and exercise. That said, sleep recommendations need to fit within a family’s life – taking into account after school activities and late-night homework sessions. But extending sleep by just “20-30 minutes can make a meaningful difference for daytime functioning,” Dr. Williamson said.
Start school later?
Researchers have only relatively recently begun to understand how insufficient sleep affects adolescent neurocognitive development long term, and this study provides “crucial evidence” about the consequences, Lydia Gabriela Speyer, PhD, said in an editorial published with the study. Dr. Speyer is affiliated with the department of psychology at the University of Cambridge (England).
“Given the novel finding that insufficient sleep is associated with changes in brain structure and connectivity that are long-lasting, early intervention is crucial because such neural changes are probably not reversible and might consequently affect adolescents’ development into adulthood,” Dr. Speyer wrote.
Delaying school start times could be one way to help kids get more sleep. The American Academy of Pediatrics and the American Academy of Sleep Medicine recommend that middle schools and high schools start no earlier than 8:30 a.m. to better align with students’ circadian rhythm, Dr. Speyer noted.
As it is in the United States, most schools start closer to 8 a.m. In California, though, a law that went into effect on July 1 prohibits high schools from starting before 8:30 a.m. Other states are weighing similar legislation.
The research was supported by the National Institutes of Health. Dr. Wang and his coauthors and Dr. Speyer had no conflict of interest disclosures. Dr. Williamson is a sleep expert for the Pediatric Sleep Council (www.babysleep.com), which provides free information about early childhood sleep, but she does not receive compensation for this role.
Children who do not get enough sleep for one night can be cranky, groggy, or meltdown prone the next day.
Over time, though, insufficient sleep may impair neurodevelopment in ways that can be measured on brain scans and tests long term, a new study shows.
Research published in The Lancet Child & Adolescent Health found that 9- and 10-year-olds who do not get at least 9 hours of sleep most nights tend to have less gray matter and smaller areas of the brain responsible for attention, memory, and inhibition control, relative to children who do get enough sleep.
The researchers also found a relationship between insufficient sleep and disrupted connections between the basal ganglia and cortical regions of the brain. These disruptions appeared to be linked to depression, thought problems, and impairments in crystallized intelligence, a type of intelligence that depends on memory.
The overall patterns persisted 2 years later, even as those who got enough sleep at baseline gradually slept less over time, while those who were not getting enough sleep to begin with continued to sleep about the same amount, the researchers reported.
The results bolster the case for delaying school start times, as California recently did, according one researcher who was not involved in the study.
The ABCD Study
To examine how insufficient sleep affects children’s mental health, cognition, brain function, and brain structure over 2 years, Ze Wang, PhD, professor of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, and colleagues analyzed data from the ongoing Adolescent Brain Cognitive Development (ABCD) Study. The ABCD Study is tracking the biologic and behavioral development of more than 11,000 children in the United States who were recruited for the study when they were 9 or 10 years old.
For their new analysis, Dr. Wang’s group focused on 6,042 participants: 3,021 children with insufficient sleep who were matched with an equal number of participants who were similar in many respects, including sex, socioeconomic status, and puberty status, except they got at least 9 hours of sleep. They also looked at outcomes 2 years later from 749 of the matched pairs who had results available.
The investigators determined sleep duration based on how parents answered the question: “How many hours of sleep does your child get on most nights in the past 6 months?” Possible answers included at least 9 hours, 8-9 hours, 7-8 hours, 5-7 hours, or less than 5 hours. They also looked at functional and structural MRI scans, test results, and responses to questionnaires.
Negative effects of inadequate sleep were spread over “several different domains including brain structure, function, cognition, behavior, and mental health,” Dr. Wang said.
The strength of the relationship between sleep duration and the various outcomes was “modest” and based on group averages, he said. So, a given child who does not sleep for 9 hours most nights won’t necessarily perform worse than a child who gets enough sleep.
Still, modest effects may accumulate and have lasting consequences, Dr. Wang said.
Crystallized intelligence
The researchers looked at 42 behavioral outcomes, 32 of which were significantly different between the groups. Four outcomes in particular – depression, thought problems, performance on a picture-vocabulary test, and crystallized intelligence – were areas where insufficient sleep seemed to have a larger negative effect.
Sleep duration’s relationship with crystallized intelligence was twice that for fluid intelligence, which does not depend on memory.
“Sleep affects memory,” Dr. Wang said. “Crystallized intelligence depends on learned skills and knowledge, which are memory. In this sense, sleep is related to crystallized intelligence.”
One limitation of the study is that some parents may not accurately report how much sleep their child gets, Dr. Wang acknowledged. Children may be awake when parents think they are asleep, for example.
And although the results show getting 9 hours of sleep may help neurocognitive development, it’s also possible that excessive amounts of sleep could be problematic, the study authors wrote.
Further experiments are needed to prove that insufficient sleep – and not some other, unaccounted for factor – causes the observed impairments in neurodevelopment.
To promote healthy sleep, parents should keep a strict routine for their children, such as a regular bedtime and no electronic devices in the bedroom, Dr. Wang suggested. More physical activity during the day also should help.
If children have high levels of stress and depression, “finding the source is critical,” he said. Likewise, clinicians should consider how mental health can affect their patients’ sleep.
More to healthy sleep than duration
“This study both aligns with and advances existing research on the importance of sufficient sleep for child well-being,” said Ariel A. Williamson, PhD, DBSM, a psychologist and pediatric sleep expert in the department of child and adolescent psychiatry and behavioral sciences at Children’s Hospital of Philadelphia and assistant professor of psychiatry and pediatrics at University of Pennsylvania, also in Philadelphia.
The researchers used rigorous propensity score matching, longitudinal data, and brain imaging, which are “innovative methods that provide more evidence on potential mechanisms linking insufficient sleep and child outcomes,” said Dr. Williamson, who was not involved in the study.
While the investigators focused on sleep duration, child sleep health is multidimensional and includes other elements like timing and perception of sleep quality, Dr. Williamson noted. “For example, some research shows that having a sleep schedule that varies night to night is linked to poor child outcomes.”
Dr. Williamson tells families and clinicians that “sleep is a pillar of health,” equal to diet and exercise. That said, sleep recommendations need to fit within a family’s life – taking into account after school activities and late-night homework sessions. But extending sleep by just “20-30 minutes can make a meaningful difference for daytime functioning,” Dr. Williamson said.
Start school later?
Researchers have only relatively recently begun to understand how insufficient sleep affects adolescent neurocognitive development long term, and this study provides “crucial evidence” about the consequences, Lydia Gabriela Speyer, PhD, said in an editorial published with the study. Dr. Speyer is affiliated with the department of psychology at the University of Cambridge (England).
“Given the novel finding that insufficient sleep is associated with changes in brain structure and connectivity that are long-lasting, early intervention is crucial because such neural changes are probably not reversible and might consequently affect adolescents’ development into adulthood,” Dr. Speyer wrote.
Delaying school start times could be one way to help kids get more sleep. The American Academy of Pediatrics and the American Academy of Sleep Medicine recommend that middle schools and high schools start no earlier than 8:30 a.m. to better align with students’ circadian rhythm, Dr. Speyer noted.
As it is in the United States, most schools start closer to 8 a.m. In California, though, a law that went into effect on July 1 prohibits high schools from starting before 8:30 a.m. Other states are weighing similar legislation.
The research was supported by the National Institutes of Health. Dr. Wang and his coauthors and Dr. Speyer had no conflict of interest disclosures. Dr. Williamson is a sleep expert for the Pediatric Sleep Council (www.babysleep.com), which provides free information about early childhood sleep, but she does not receive compensation for this role.
FROM THE LANCET CHILD & ADOLESCENT HEALTH
Leukemia rates two to three times higher in children born near fracking
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Children born near fracking and other “unconventional” drilling sites are at two to three times greater risk of developing childhood leukemia, according to new research.
The study, published in the journal Environmental Health Perspectives, compared proximity of homes to unconventional oil and gas development (UOGD) sites and risk of the most common form of childhood leukemia, acute lymphoblastic leukemia (ALL).
Researchers looked at 405 children aged 2-7 diagnosed with ALL in Pennsylvania from 2009 to 2017. These children were compared to a control group of 2,080 without the disease matched on the year of birth.
“Unconventional oil and gas development can both use and release chemicals that have been linked to cancer,” study coauthor Nicole Deziel, PhD, of the Yale School of Public Health, New Haven, Conn., said in a statement . She noted that the possibility that children living in close proximity to such sites are “exposed to these chemical carcinogens is a major public health concern.”
About 17 million Americans live within a half-mile of active oil and gas production, according to the Oil & Gas Threat Map, Common Dreams reports. That number includes 4 million children.
The Yale study also found that drinking water could be an important pathway of exposure to oil- and gas-related chemicals used in the UOGD methods of extraction.
Researchers used a new metric that measures exposure to contaminated drinking water and distance to a well. They were able to identify UOGD-affected wells that fell within watersheds where children and their families likely obtained their water.
“Previous health studies have found links between proximity to oil and gas drilling and various children’s health outcomes,” said Dr. Deziel. “This study is among the few to focus on drinking water specifically and the first to apply a novel metric designed to capture potential exposure through this pathway.”
A version of this article first appeared on WebMD.com.
Higher rates of group B strep disease found in Black and Asian newborns
Health charities called for action to address racial health disparities after population-wide analysis by the UK Health Security Agency found that Black and Asian neonates had a significantly higher risk of early-onset group B streptococcal disease (GBS), compared with White infants.
One support group said more research was now needed to identify the cause of the disparity, and called for pregnant women to be better informed about the disease and what it could mean for them and their baby.
The study, published in Pediatrics, used UKHSA data on laboratory-confirmed infant group B streptococcal (iGBS) disease cases between Jan. 1, 2016, and Dec. 31, 2020, and were linked to hospital ethnicity records.
Cases of iGBS were defined as isolation of Streptococcus agalactiae from a normally sterile site at 0-6 days of life for early-onset iGBS and 7-90 days for late-onset disease.
Hospital data and parent-reported ethnicity
Researchers found 2,512 iGBS cases in England during the study period, 65.3% were early onset and 34.8% late onset, equivalent to 0.52 and 0.28 cases per 1000 live births respectively.
Researchers were able to link 85.6% of those to ethnicity. Among those 2,149 cases, Black infants had a 48% higher risk, and Asian infants a 40% higher risk of early onset iGBS, compared with White infants. Among those from an Asian background, the risk was 87% higher for Bangladeshi and 38% higher for Pakistani neonates.
Rates of early onset iGBS per 1,000 live births were 0.43 for White infants, 0.63 for Black infants, and 0.60 for those of Asian ethnicity.
In contrast, Indian infants had an early-onset rate of 0.47 per 1,000 live births, which was similar to White infants.
Black infants had 57% higher rates of late-onset iGBS (0.37) than White infants (0.24), the researchers reported.
The study authors highlighted previous research which found higher prevalence of group B streptococcal colonization in mothers from Black and some Asian ethnic groups, but lower prevalence in mothers from the Indian subcontinent. More research was needed to establish causes, the researchers said, including whether higher preterm birth rates in minority ethnic groups led to increased iGBS risk in neonates, or whether maternal group B streptococcal disease led to higher preterm birth rates and subsequent neonatal iGBS.
The researchers concluded: “Understanding the factors underpinning differences in rates of early-onset iGBS within south Asian groups in England may lead to new opportunities for prevention such as prioritized antenatal screening. Strategies to prevent neonatal iGBS must be tailored from high-quality quantitative and qualitative data to reach all women and protect all infants, irrespective of racial or ethnic background.”
‘Shocking but not surprising’
Commenting on the study, Edward Morris, president of the Royal College of Obstetricians and Gynaecologists, said: “This research is striking reading, and is yet another example of how far we have to go to tackle health inequalities within women’s health care.”
Philip Steer, professor emeritus at Imperial College London, said that the results were “consistent with previous reports of higher GBS carriage and higher maternal and neonatal mortality rates in minority groups” and “emphasize the importance of studying not just whether, but why, these differences exist.” He added: “We need to understand the reasons for the differences before we can design much-needed intervention to eliminate them.”
Jane Plumb, chief executive of Group B Strep Support, called the findings “shocking, but unfortunately not surprising” and said that they offered “another example of racial disparities in maternal and neonatal health.” She said: “We’re calling for all pregnant women and birthing people to be informed about GBS and its risks, so they can make empowered choices for themselves and their baby. It is also critical that trusts sign up to take part in the internationally significant [National Institute for Health and Care Research]–funded GBS3 clinical trial, designed to improve the prevention of GBS infection.”
Baroness Shaista Gohir, chief executive of the Muslim Women’s Network, said: “With significantly higher rates of group B Strep infection in Black and Asian babies, greater efforts must be made to improve awareness among pregnant women within these communities.”
A version of this article first appeared on Medscape UK.
Health charities called for action to address racial health disparities after population-wide analysis by the UK Health Security Agency found that Black and Asian neonates had a significantly higher risk of early-onset group B streptococcal disease (GBS), compared with White infants.
One support group said more research was now needed to identify the cause of the disparity, and called for pregnant women to be better informed about the disease and what it could mean for them and their baby.
The study, published in Pediatrics, used UKHSA data on laboratory-confirmed infant group B streptococcal (iGBS) disease cases between Jan. 1, 2016, and Dec. 31, 2020, and were linked to hospital ethnicity records.
Cases of iGBS were defined as isolation of Streptococcus agalactiae from a normally sterile site at 0-6 days of life for early-onset iGBS and 7-90 days for late-onset disease.
Hospital data and parent-reported ethnicity
Researchers found 2,512 iGBS cases in England during the study period, 65.3% were early onset and 34.8% late onset, equivalent to 0.52 and 0.28 cases per 1000 live births respectively.
Researchers were able to link 85.6% of those to ethnicity. Among those 2,149 cases, Black infants had a 48% higher risk, and Asian infants a 40% higher risk of early onset iGBS, compared with White infants. Among those from an Asian background, the risk was 87% higher for Bangladeshi and 38% higher for Pakistani neonates.
Rates of early onset iGBS per 1,000 live births were 0.43 for White infants, 0.63 for Black infants, and 0.60 for those of Asian ethnicity.
In contrast, Indian infants had an early-onset rate of 0.47 per 1,000 live births, which was similar to White infants.
Black infants had 57% higher rates of late-onset iGBS (0.37) than White infants (0.24), the researchers reported.
The study authors highlighted previous research which found higher prevalence of group B streptococcal colonization in mothers from Black and some Asian ethnic groups, but lower prevalence in mothers from the Indian subcontinent. More research was needed to establish causes, the researchers said, including whether higher preterm birth rates in minority ethnic groups led to increased iGBS risk in neonates, or whether maternal group B streptococcal disease led to higher preterm birth rates and subsequent neonatal iGBS.
The researchers concluded: “Understanding the factors underpinning differences in rates of early-onset iGBS within south Asian groups in England may lead to new opportunities for prevention such as prioritized antenatal screening. Strategies to prevent neonatal iGBS must be tailored from high-quality quantitative and qualitative data to reach all women and protect all infants, irrespective of racial or ethnic background.”
‘Shocking but not surprising’
Commenting on the study, Edward Morris, president of the Royal College of Obstetricians and Gynaecologists, said: “This research is striking reading, and is yet another example of how far we have to go to tackle health inequalities within women’s health care.”
Philip Steer, professor emeritus at Imperial College London, said that the results were “consistent with previous reports of higher GBS carriage and higher maternal and neonatal mortality rates in minority groups” and “emphasize the importance of studying not just whether, but why, these differences exist.” He added: “We need to understand the reasons for the differences before we can design much-needed intervention to eliminate them.”
Jane Plumb, chief executive of Group B Strep Support, called the findings “shocking, but unfortunately not surprising” and said that they offered “another example of racial disparities in maternal and neonatal health.” She said: “We’re calling for all pregnant women and birthing people to be informed about GBS and its risks, so they can make empowered choices for themselves and their baby. It is also critical that trusts sign up to take part in the internationally significant [National Institute for Health and Care Research]–funded GBS3 clinical trial, designed to improve the prevention of GBS infection.”
Baroness Shaista Gohir, chief executive of the Muslim Women’s Network, said: “With significantly higher rates of group B Strep infection in Black and Asian babies, greater efforts must be made to improve awareness among pregnant women within these communities.”
A version of this article first appeared on Medscape UK.
Health charities called for action to address racial health disparities after population-wide analysis by the UK Health Security Agency found that Black and Asian neonates had a significantly higher risk of early-onset group B streptococcal disease (GBS), compared with White infants.
One support group said more research was now needed to identify the cause of the disparity, and called for pregnant women to be better informed about the disease and what it could mean for them and their baby.
The study, published in Pediatrics, used UKHSA data on laboratory-confirmed infant group B streptococcal (iGBS) disease cases between Jan. 1, 2016, and Dec. 31, 2020, and were linked to hospital ethnicity records.
Cases of iGBS were defined as isolation of Streptococcus agalactiae from a normally sterile site at 0-6 days of life for early-onset iGBS and 7-90 days for late-onset disease.
Hospital data and parent-reported ethnicity
Researchers found 2,512 iGBS cases in England during the study period, 65.3% were early onset and 34.8% late onset, equivalent to 0.52 and 0.28 cases per 1000 live births respectively.
Researchers were able to link 85.6% of those to ethnicity. Among those 2,149 cases, Black infants had a 48% higher risk, and Asian infants a 40% higher risk of early onset iGBS, compared with White infants. Among those from an Asian background, the risk was 87% higher for Bangladeshi and 38% higher for Pakistani neonates.
Rates of early onset iGBS per 1,000 live births were 0.43 for White infants, 0.63 for Black infants, and 0.60 for those of Asian ethnicity.
In contrast, Indian infants had an early-onset rate of 0.47 per 1,000 live births, which was similar to White infants.
Black infants had 57% higher rates of late-onset iGBS (0.37) than White infants (0.24), the researchers reported.
The study authors highlighted previous research which found higher prevalence of group B streptococcal colonization in mothers from Black and some Asian ethnic groups, but lower prevalence in mothers from the Indian subcontinent. More research was needed to establish causes, the researchers said, including whether higher preterm birth rates in minority ethnic groups led to increased iGBS risk in neonates, or whether maternal group B streptococcal disease led to higher preterm birth rates and subsequent neonatal iGBS.
The researchers concluded: “Understanding the factors underpinning differences in rates of early-onset iGBS within south Asian groups in England may lead to new opportunities for prevention such as prioritized antenatal screening. Strategies to prevent neonatal iGBS must be tailored from high-quality quantitative and qualitative data to reach all women and protect all infants, irrespective of racial or ethnic background.”
‘Shocking but not surprising’
Commenting on the study, Edward Morris, president of the Royal College of Obstetricians and Gynaecologists, said: “This research is striking reading, and is yet another example of how far we have to go to tackle health inequalities within women’s health care.”
Philip Steer, professor emeritus at Imperial College London, said that the results were “consistent with previous reports of higher GBS carriage and higher maternal and neonatal mortality rates in minority groups” and “emphasize the importance of studying not just whether, but why, these differences exist.” He added: “We need to understand the reasons for the differences before we can design much-needed intervention to eliminate them.”
Jane Plumb, chief executive of Group B Strep Support, called the findings “shocking, but unfortunately not surprising” and said that they offered “another example of racial disparities in maternal and neonatal health.” She said: “We’re calling for all pregnant women and birthing people to be informed about GBS and its risks, so they can make empowered choices for themselves and their baby. It is also critical that trusts sign up to take part in the internationally significant [National Institute for Health and Care Research]–funded GBS3 clinical trial, designed to improve the prevention of GBS infection.”
Baroness Shaista Gohir, chief executive of the Muslim Women’s Network, said: “With significantly higher rates of group B Strep infection in Black and Asian babies, greater efforts must be made to improve awareness among pregnant women within these communities.”
A version of this article first appeared on Medscape UK.
FROM PEDIATRICS
Siblings of children with chronic health conditions may have increased mental health risks
Siblings of children with chronic health conditions could be at an increased risk for depression, according to a new report.
In a systematic review of 34 studies, siblings of children with chronic health conditions had significantly higher scores on depressive rating scales than individuals without a sibling with a chronic health condition (standardized mean difference = 0.53; P < .001). Findings related to other clinical health outcomes, such as physical health conditions or mortality, were inconsistent.
“We’ve known for a long time that siblings of kids with chronic conditions undergo stress, and there have been conflicting data on how that stress is manifested in terms of their own health,” senior study author Eyal Cohen, MD, program head for child health evaluative sciences at the Hospital for Sick Children, Toronto, told this news organization.
“For some siblings, having the experience of being raised with a child with a chronic condition may be an asset and build resiliency, while other siblings may feel strong negative emotions, such as sadness, anger, and fear,” he said. “Although we know that this experience is stressful for many siblings, it is important to know whether it changes their health outcomes, so that appropriate support can be put in place for those who need it.”
The study was published online in the Journal of Pediatrics.
Risk for psychological challenges
About a quarter of children in the United States have a mental, emotional, developmental, or behavioral condition, and more than a third have at least one current or lifelong health condition, the study authors write. A childhood chronic health condition can affect family members through worse mental health outcomes, increased stress, and poorer health-related quality of life.
Dr. Cohen and colleagues conducted a systematic review and meta-analysis to assess the clinical mental and physical health outcomes of siblings of children with chronic health conditions in comparison with siblings of healthy children or normative data.
The research team included English-language studies that reported on clinically diagnosable mental or physical health outcomes among siblings of persons younger than 18 years who had a chronic health condition. They included a comparison group and used an experimental or observational design for their study. The researchers analyzed 34 studies, including 28 that reported on mental health, 3 that reported on physical health, and 3 that reported on mortality.
Overall, siblings of children with chronic health conditions had significantly higher scores on depression rating scales than their comparison groups. Siblings’ anxiety scores weren’t substantially higher, however (standard mean difference = 0.21; P = .07).
The effects for confirmed psychiatric diagnoses, physical health outcomes, and mortality could not be included in the meta-analysis, owing to the limited number of studies and the high level of heterogeneity among the studies.
Dr. Cohen noted that although the researchers weren’t surprised that siblings may be at increased risk of mental health challenges, they were surprised by the limited data regarding physical health.
“At a minimum, our findings support the importance of asking open-ended questions about how a family is doing during clinical encounters,” he said. “These siblings may also benefit from programs such as support groups or summer camps, which have been shown to improve mental health and behavioral outcomes in siblings of children with chronic health conditions, such as cancer and neurodevelopmental disabilities.”
Future studies should assess the specific risk factors for mental health problems in siblings of children with chronic health conditions, Dr. Cohen said. Additional research could also investigate the design and effectiveness of interventions that address these concerns.
Message of inclusiveness
“The message that resonates with me is about the interventions and resources needed to support siblings,” Linda Nguyen, a doctoral student in rehabilitation science and researcher with the CanChild Center for Childhood Disability Research at McMaster University in Hamilton, Ont., told this news organization.

Ms. Nguyen, who wasn’t involved with this study, has researched the resources available to siblings in Canada and has found a lack of support options, particularly when it comes to specific health care management roles.
“Consistently throughout my research, I’ve seen the need for resources that go beyond a focus on siblings’ well-being and instead support them in their different roles,” she said. “Some want to be friends, mentors, supporters, and caregivers for their siblings in the future.”
Siblings often adopt different roles as they form their own identity, Ms. Nguyen noted, which becomes a larger part of the health care conversation as children with chronic conditions make the transition from pediatric to adult health care. Siblings want to be asked how they’d like to be involved, she said. Some would like to be involved with health care appointments, the chronic condition community, research, and policy making.
“At the societal level and public level, there’s also a message of inclusiveness and making sure that we’re welcoming youth with disabilities and chronic conditions,” Jan Willem Gorter, MD, PhD, a professor of pediatrics and scientist for CanChild at McMaster University, told this news organization.
Dr. Gorter, who also was not involved with this study, noted that children with chronic conditions often feel left behind, which can influence the involvement of their siblings as well.
“There are a lot of places in the world where children with disabilities go to special schools, and they spend a lot of time in a different world, with different experiences than their siblings,” he said. “At the public health level, we want to advocate for an inclusive society and support the whole family, which benefits everybody.”
The study was funded by the Canadian Institutes of Health Research and the CHILD-BRIGHT Network summer studentship, which is supported by the Canadian Institute for Health Research Strategy for Patient-Oriented Research. Dr. Cohen, Ms. Nguyen, and Dr. Gorter have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Siblings of children with chronic health conditions could be at an increased risk for depression, according to a new report.
In a systematic review of 34 studies, siblings of children with chronic health conditions had significantly higher scores on depressive rating scales than individuals without a sibling with a chronic health condition (standardized mean difference = 0.53; P < .001). Findings related to other clinical health outcomes, such as physical health conditions or mortality, were inconsistent.
“We’ve known for a long time that siblings of kids with chronic conditions undergo stress, and there have been conflicting data on how that stress is manifested in terms of their own health,” senior study author Eyal Cohen, MD, program head for child health evaluative sciences at the Hospital for Sick Children, Toronto, told this news organization.
“For some siblings, having the experience of being raised with a child with a chronic condition may be an asset and build resiliency, while other siblings may feel strong negative emotions, such as sadness, anger, and fear,” he said. “Although we know that this experience is stressful for many siblings, it is important to know whether it changes their health outcomes, so that appropriate support can be put in place for those who need it.”
The study was published online in the Journal of Pediatrics.
Risk for psychological challenges
About a quarter of children in the United States have a mental, emotional, developmental, or behavioral condition, and more than a third have at least one current or lifelong health condition, the study authors write. A childhood chronic health condition can affect family members through worse mental health outcomes, increased stress, and poorer health-related quality of life.
Dr. Cohen and colleagues conducted a systematic review and meta-analysis to assess the clinical mental and physical health outcomes of siblings of children with chronic health conditions in comparison with siblings of healthy children or normative data.
The research team included English-language studies that reported on clinically diagnosable mental or physical health outcomes among siblings of persons younger than 18 years who had a chronic health condition. They included a comparison group and used an experimental or observational design for their study. The researchers analyzed 34 studies, including 28 that reported on mental health, 3 that reported on physical health, and 3 that reported on mortality.
Overall, siblings of children with chronic health conditions had significantly higher scores on depression rating scales than their comparison groups. Siblings’ anxiety scores weren’t substantially higher, however (standard mean difference = 0.21; P = .07).
The effects for confirmed psychiatric diagnoses, physical health outcomes, and mortality could not be included in the meta-analysis, owing to the limited number of studies and the high level of heterogeneity among the studies.
Dr. Cohen noted that although the researchers weren’t surprised that siblings may be at increased risk of mental health challenges, they were surprised by the limited data regarding physical health.
“At a minimum, our findings support the importance of asking open-ended questions about how a family is doing during clinical encounters,” he said. “These siblings may also benefit from programs such as support groups or summer camps, which have been shown to improve mental health and behavioral outcomes in siblings of children with chronic health conditions, such as cancer and neurodevelopmental disabilities.”
Future studies should assess the specific risk factors for mental health problems in siblings of children with chronic health conditions, Dr. Cohen said. Additional research could also investigate the design and effectiveness of interventions that address these concerns.
Message of inclusiveness
“The message that resonates with me is about the interventions and resources needed to support siblings,” Linda Nguyen, a doctoral student in rehabilitation science and researcher with the CanChild Center for Childhood Disability Research at McMaster University in Hamilton, Ont., told this news organization.
Ms. Nguyen, who wasn’t involved with this study, has researched the resources available to siblings in Canada and has found a lack of support options, particularly when it comes to specific health care management roles.
“Consistently throughout my research, I’ve seen the need for resources that go beyond a focus on siblings’ well-being and instead support them in their different roles,” she said. “Some want to be friends, mentors, supporters, and caregivers for their siblings in the future.”
Siblings often adopt different roles as they form their own identity, Ms. Nguyen noted, which becomes a larger part of the health care conversation as children with chronic conditions make the transition from pediatric to adult health care. Siblings want to be asked how they’d like to be involved, she said. Some would like to be involved with health care appointments, the chronic condition community, research, and policy making.
“At the societal level and public level, there’s also a message of inclusiveness and making sure that we’re welcoming youth with disabilities and chronic conditions,” Jan Willem Gorter, MD, PhD, a professor of pediatrics and scientist for CanChild at McMaster University, told this news organization.
Dr. Gorter, who also was not involved with this study, noted that children with chronic conditions often feel left behind, which can influence the involvement of their siblings as well.
“There are a lot of places in the world where children with disabilities go to special schools, and they spend a lot of time in a different world, with different experiences than their siblings,” he said. “At the public health level, we want to advocate for an inclusive society and support the whole family, which benefits everybody.”
The study was funded by the Canadian Institutes of Health Research and the CHILD-BRIGHT Network summer studentship, which is supported by the Canadian Institute for Health Research Strategy for Patient-Oriented Research. Dr. Cohen, Ms. Nguyen, and Dr. Gorter have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Siblings of children with chronic health conditions could be at an increased risk for depression, according to a new report.
In a systematic review of 34 studies, siblings of children with chronic health conditions had significantly higher scores on depressive rating scales than individuals without a sibling with a chronic health condition (standardized mean difference = 0.53; P < .001). Findings related to other clinical health outcomes, such as physical health conditions or mortality, were inconsistent.
“We’ve known for a long time that siblings of kids with chronic conditions undergo stress, and there have been conflicting data on how that stress is manifested in terms of their own health,” senior study author Eyal Cohen, MD, program head for child health evaluative sciences at the Hospital for Sick Children, Toronto, told this news organization.
“For some siblings, having the experience of being raised with a child with a chronic condition may be an asset and build resiliency, while other siblings may feel strong negative emotions, such as sadness, anger, and fear,” he said. “Although we know that this experience is stressful for many siblings, it is important to know whether it changes their health outcomes, so that appropriate support can be put in place for those who need it.”
The study was published online in the Journal of Pediatrics.
Risk for psychological challenges
About a quarter of children in the United States have a mental, emotional, developmental, or behavioral condition, and more than a third have at least one current or lifelong health condition, the study authors write. A childhood chronic health condition can affect family members through worse mental health outcomes, increased stress, and poorer health-related quality of life.
Dr. Cohen and colleagues conducted a systematic review and meta-analysis to assess the clinical mental and physical health outcomes of siblings of children with chronic health conditions in comparison with siblings of healthy children or normative data.
The research team included English-language studies that reported on clinically diagnosable mental or physical health outcomes among siblings of persons younger than 18 years who had a chronic health condition. They included a comparison group and used an experimental or observational design for their study. The researchers analyzed 34 studies, including 28 that reported on mental health, 3 that reported on physical health, and 3 that reported on mortality.
Overall, siblings of children with chronic health conditions had significantly higher scores on depression rating scales than their comparison groups. Siblings’ anxiety scores weren’t substantially higher, however (standard mean difference = 0.21; P = .07).
The effects for confirmed psychiatric diagnoses, physical health outcomes, and mortality could not be included in the meta-analysis, owing to the limited number of studies and the high level of heterogeneity among the studies.
Dr. Cohen noted that although the researchers weren’t surprised that siblings may be at increased risk of mental health challenges, they were surprised by the limited data regarding physical health.
“At a minimum, our findings support the importance of asking open-ended questions about how a family is doing during clinical encounters,” he said. “These siblings may also benefit from programs such as support groups or summer camps, which have been shown to improve mental health and behavioral outcomes in siblings of children with chronic health conditions, such as cancer and neurodevelopmental disabilities.”
Future studies should assess the specific risk factors for mental health problems in siblings of children with chronic health conditions, Dr. Cohen said. Additional research could also investigate the design and effectiveness of interventions that address these concerns.
Message of inclusiveness
“The message that resonates with me is about the interventions and resources needed to support siblings,” Linda Nguyen, a doctoral student in rehabilitation science and researcher with the CanChild Center for Childhood Disability Research at McMaster University in Hamilton, Ont., told this news organization.
Ms. Nguyen, who wasn’t involved with this study, has researched the resources available to siblings in Canada and has found a lack of support options, particularly when it comes to specific health care management roles.
“Consistently throughout my research, I’ve seen the need for resources that go beyond a focus on siblings’ well-being and instead support them in their different roles,” she said. “Some want to be friends, mentors, supporters, and caregivers for their siblings in the future.”
Siblings often adopt different roles as they form their own identity, Ms. Nguyen noted, which becomes a larger part of the health care conversation as children with chronic conditions make the transition from pediatric to adult health care. Siblings want to be asked how they’d like to be involved, she said. Some would like to be involved with health care appointments, the chronic condition community, research, and policy making.
“At the societal level and public level, there’s also a message of inclusiveness and making sure that we’re welcoming youth with disabilities and chronic conditions,” Jan Willem Gorter, MD, PhD, a professor of pediatrics and scientist for CanChild at McMaster University, told this news organization.
Dr. Gorter, who also was not involved with this study, noted that children with chronic conditions often feel left behind, which can influence the involvement of their siblings as well.
“There are a lot of places in the world where children with disabilities go to special schools, and they spend a lot of time in a different world, with different experiences than their siblings,” he said. “At the public health level, we want to advocate for an inclusive society and support the whole family, which benefits everybody.”
The study was funded by the Canadian Institutes of Health Research and the CHILD-BRIGHT Network summer studentship, which is supported by the Canadian Institute for Health Research Strategy for Patient-Oriented Research. Dr. Cohen, Ms. Nguyen, and Dr. Gorter have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF PEDIATRICS
Children born very prematurely at higher risk to struggle in secondary school
A new study of educational attainment among U.K. primary and secondary schoolchildren born prematurely now provides some reassurance about the longer-term outcomes for many of these children.
For the study, published in the open-access journal PLOS ONE, researchers from the University of Oxford with colleagues from the University of Leicester and City University, London, used data from 11,695 children in the population-based UK Millennium Cohort Study, which included children born in England from Sept. 1, 2000 to Aug. 31, 2001. They analyzed data on educational attainment in primary school, at age 11, for 6,950 pupils and in secondary school, at age 16, for 7,131 pupils.
Preterm birth is a known risk factor for developmental impairment, lower educational performance and reduced academic attainment, with the impact proportional to the degree of prematurity. Not every child born prematurely will experience learning or developmental challenges, but studies of children born before 34 weeks gestation have shown that they are more likely to have cognitive difficulties, particularly poorer reading and maths skills, at primary school, and to have special educational needs by the end of primary education.
Elevated risk of all preterm children in primary school
Until now, few studies have followed these children through secondary school or examined the full spectrum of gestational ages at birth. Yet as neonatal care advances and more premature babies now survive, an average primary class in the United Kingdom now includes two preterm children.
Among the primary school children overall, 17.7% had not achieved their expected level in English and mathematics at age 11. Children born very preterm, before 32 weeks or at 32-33 weeks gestation, were more than twice as likely as full term children to fail to meet these benchmarks, with adjusted relative risks of 2.06 and 2.13, respectively. Those born late preterm, at 34-36 weeks, or early term, at 37-38 weeks, were at lesser risk, with RRs of 1.18 and 1.21, respectively.
By the end of secondary school, 45.2% of pupils had not passed the benchmark of at least five General Certificate of Secondary Education (GCSE) examinations, including English and mathematics. The RR for children born very preterm, compared with full term children, was 1.26, with 60% of students in this group failing to achieve five GCSEs. However, children born at gestations between 32 and 38 weeks were not at elevated risk, compared with children born at full term.
Risk persists to secondary level only for very preterm children
A similar pattern was seen with English and mathematics analyzed separately, with no additional risk of not passing among children born at 32 weeks or above, but adjusted RRs of 1.33 for not passing English and 1.42 for not passing maths among pupils who had been born very preterm, compared with full term children.
“All children born before full term are more likely to have poorer attainment during primary school, compared with children born full term (39-41 weeks), but only children born very preterm (before 32 weeks) remain at risk of poor attainment at the end of secondary schooling,” the researchers concluded.
“Further studies are needed in order to confirm this result,” they acknowledge. They suggested their results could be explained by catch-up in academic attainment among children born moderately or late preterm or at early term. However, “very preterm children appear to be a high-risk group with persistent difficulties in terms of educational outcomes,” they said, noting that even this risk was of lower magnitude than the reduced attainment scores they found among pupils eligible for free school meals, meaning those from disadvantaged socioeconomic backgrounds.
Extra educational support needed
The researchers concluded: “Children born very preterm may benefit from screening for cognitive and language difficulties prior to school entry to guide the provision of additional support during schooling.” In addition, those born very preterm “may require additional educational support throughout compulsory schooling.”
Commenting on the study, Caroline Lee-Davey, chief executive of premature baby charity Bliss, told this news organization: “Every child who is born premature is unique, and their development and achievements will be individual to them. However, these new findings are significant and add to our understanding of how prematurity is related to longer-term educational attainment, particularly for children who were born very preterm.”
“Most importantly, they highlight the need for all children who were born premature – and particularly those who were born before 32 weeks – to have access to early support. This means ensuring all eligible babies receive a follow-up check at 2 and 4 years as recommended by NICE and for early years and educational professionals to be aware of the relationship between premature birth and development.”
“We know how concerning these findings might be for families with babies and very young children right now. That’s why Bliss has developed a suite of information to support families as they make choices about their child’s education.”
A version of this article first appeared on Medscape UK.
A new study of educational attainment among U.K. primary and secondary schoolchildren born prematurely now provides some reassurance about the longer-term outcomes for many of these children.
For the study, published in the open-access journal PLOS ONE, researchers from the University of Oxford with colleagues from the University of Leicester and City University, London, used data from 11,695 children in the population-based UK Millennium Cohort Study, which included children born in England from Sept. 1, 2000 to Aug. 31, 2001. They analyzed data on educational attainment in primary school, at age 11, for 6,950 pupils and in secondary school, at age 16, for 7,131 pupils.
Preterm birth is a known risk factor for developmental impairment, lower educational performance and reduced academic attainment, with the impact proportional to the degree of prematurity. Not every child born prematurely will experience learning or developmental challenges, but studies of children born before 34 weeks gestation have shown that they are more likely to have cognitive difficulties, particularly poorer reading and maths skills, at primary school, and to have special educational needs by the end of primary education.
Elevated risk of all preterm children in primary school
Until now, few studies have followed these children through secondary school or examined the full spectrum of gestational ages at birth. Yet as neonatal care advances and more premature babies now survive, an average primary class in the United Kingdom now includes two preterm children.
Among the primary school children overall, 17.7% had not achieved their expected level in English and mathematics at age 11. Children born very preterm, before 32 weeks or at 32-33 weeks gestation, were more than twice as likely as full term children to fail to meet these benchmarks, with adjusted relative risks of 2.06 and 2.13, respectively. Those born late preterm, at 34-36 weeks, or early term, at 37-38 weeks, were at lesser risk, with RRs of 1.18 and 1.21, respectively.
By the end of secondary school, 45.2% of pupils had not passed the benchmark of at least five General Certificate of Secondary Education (GCSE) examinations, including English and mathematics. The RR for children born very preterm, compared with full term children, was 1.26, with 60% of students in this group failing to achieve five GCSEs. However, children born at gestations between 32 and 38 weeks were not at elevated risk, compared with children born at full term.
Risk persists to secondary level only for very preterm children
A similar pattern was seen with English and mathematics analyzed separately, with no additional risk of not passing among children born at 32 weeks or above, but adjusted RRs of 1.33 for not passing English and 1.42 for not passing maths among pupils who had been born very preterm, compared with full term children.
“All children born before full term are more likely to have poorer attainment during primary school, compared with children born full term (39-41 weeks), but only children born very preterm (before 32 weeks) remain at risk of poor attainment at the end of secondary schooling,” the researchers concluded.
“Further studies are needed in order to confirm this result,” they acknowledge. They suggested their results could be explained by catch-up in academic attainment among children born moderately or late preterm or at early term. However, “very preterm children appear to be a high-risk group with persistent difficulties in terms of educational outcomes,” they said, noting that even this risk was of lower magnitude than the reduced attainment scores they found among pupils eligible for free school meals, meaning those from disadvantaged socioeconomic backgrounds.
Extra educational support needed
The researchers concluded: “Children born very preterm may benefit from screening for cognitive and language difficulties prior to school entry to guide the provision of additional support during schooling.” In addition, those born very preterm “may require additional educational support throughout compulsory schooling.”
Commenting on the study, Caroline Lee-Davey, chief executive of premature baby charity Bliss, told this news organization: “Every child who is born premature is unique, and their development and achievements will be individual to them. However, these new findings are significant and add to our understanding of how prematurity is related to longer-term educational attainment, particularly for children who were born very preterm.”
“Most importantly, they highlight the need for all children who were born premature – and particularly those who were born before 32 weeks – to have access to early support. This means ensuring all eligible babies receive a follow-up check at 2 and 4 years as recommended by NICE and for early years and educational professionals to be aware of the relationship between premature birth and development.”
“We know how concerning these findings might be for families with babies and very young children right now. That’s why Bliss has developed a suite of information to support families as they make choices about their child’s education.”
A version of this article first appeared on Medscape UK.
A new study of educational attainment among U.K. primary and secondary schoolchildren born prematurely now provides some reassurance about the longer-term outcomes for many of these children.
For the study, published in the open-access journal PLOS ONE, researchers from the University of Oxford with colleagues from the University of Leicester and City University, London, used data from 11,695 children in the population-based UK Millennium Cohort Study, which included children born in England from Sept. 1, 2000 to Aug. 31, 2001. They analyzed data on educational attainment in primary school, at age 11, for 6,950 pupils and in secondary school, at age 16, for 7,131 pupils.
Preterm birth is a known risk factor for developmental impairment, lower educational performance and reduced academic attainment, with the impact proportional to the degree of prematurity. Not every child born prematurely will experience learning or developmental challenges, but studies of children born before 34 weeks gestation have shown that they are more likely to have cognitive difficulties, particularly poorer reading and maths skills, at primary school, and to have special educational needs by the end of primary education.
Elevated risk of all preterm children in primary school
Until now, few studies have followed these children through secondary school or examined the full spectrum of gestational ages at birth. Yet as neonatal care advances and more premature babies now survive, an average primary class in the United Kingdom now includes two preterm children.
Among the primary school children overall, 17.7% had not achieved their expected level in English and mathematics at age 11. Children born very preterm, before 32 weeks or at 32-33 weeks gestation, were more than twice as likely as full term children to fail to meet these benchmarks, with adjusted relative risks of 2.06 and 2.13, respectively. Those born late preterm, at 34-36 weeks, or early term, at 37-38 weeks, were at lesser risk, with RRs of 1.18 and 1.21, respectively.
By the end of secondary school, 45.2% of pupils had not passed the benchmark of at least five General Certificate of Secondary Education (GCSE) examinations, including English and mathematics. The RR for children born very preterm, compared with full term children, was 1.26, with 60% of students in this group failing to achieve five GCSEs. However, children born at gestations between 32 and 38 weeks were not at elevated risk, compared with children born at full term.
Risk persists to secondary level only for very preterm children
A similar pattern was seen with English and mathematics analyzed separately, with no additional risk of not passing among children born at 32 weeks or above, but adjusted RRs of 1.33 for not passing English and 1.42 for not passing maths among pupils who had been born very preterm, compared with full term children.
“All children born before full term are more likely to have poorer attainment during primary school, compared with children born full term (39-41 weeks), but only children born very preterm (before 32 weeks) remain at risk of poor attainment at the end of secondary schooling,” the researchers concluded.
“Further studies are needed in order to confirm this result,” they acknowledge. They suggested their results could be explained by catch-up in academic attainment among children born moderately or late preterm or at early term. However, “very preterm children appear to be a high-risk group with persistent difficulties in terms of educational outcomes,” they said, noting that even this risk was of lower magnitude than the reduced attainment scores they found among pupils eligible for free school meals, meaning those from disadvantaged socioeconomic backgrounds.
Extra educational support needed
The researchers concluded: “Children born very preterm may benefit from screening for cognitive and language difficulties prior to school entry to guide the provision of additional support during schooling.” In addition, those born very preterm “may require additional educational support throughout compulsory schooling.”
Commenting on the study, Caroline Lee-Davey, chief executive of premature baby charity Bliss, told this news organization: “Every child who is born premature is unique, and their development and achievements will be individual to them. However, these new findings are significant and add to our understanding of how prematurity is related to longer-term educational attainment, particularly for children who were born very preterm.”
“Most importantly, they highlight the need for all children who were born premature – and particularly those who were born before 32 weeks – to have access to early support. This means ensuring all eligible babies receive a follow-up check at 2 and 4 years as recommended by NICE and for early years and educational professionals to be aware of the relationship between premature birth and development.”
“We know how concerning these findings might be for families with babies and very young children right now. That’s why Bliss has developed a suite of information to support families as they make choices about their child’s education.”
A version of this article first appeared on Medscape UK.
FROM PLOS ONE
Large study amplifies evidence of COVID vaccine safety in pregnancy
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
FROM BMJ
Reliably solving complex problems
The James Webb Space Telescope (JWST) is an engineering marvel. Costing over $10 billion, it should be. The project cost overrun was 900%. The launch was delayed by more than a decade. The Human Genome Project from 1990 to 2003 was completed slightly ahead of schedule and for less than the $4-$5 billion original estimates. This HGP success story is partly because of private entrepreneurial involvement. The Superconducting Super Collider in Texas spent $2 billion but never got off the ground. Successfully shepherding huge public projects like these involves the art of politics and management as well as science.
Whatever the earlier missteps, the JWST project is now performing above expectations. It has launched, taken up residence a million miles from Earth, deployed its mirrors (a process that had more than 300 possible single points of failure, any one of which would reduce the thing to scrap metal), and been calibrated. The JWST has even been dented by a micrometeoroid – sort of like a parking lot ding on the door of your brand new car. The first images are visually amazing and producing new scientific insights. This is a pinnacle of scientific achievement.
What characteristics enable such an achievement? How do we foster those same characteristics in the practice of medicine and medical research? Will the success of the JWST increase and restore the public’s trust in science and scientists?
After all the bickering over vaccines and masks for the past 2+ years, medical science could use a boost. The gravitas of scientists, and indeed all experts, has diminished over the 5 decades since humans walked on the moon. It has been harmed by mercenary scientists who sought to sow doubt about whether smoking caused cancer and whether fossil fuels created climate change. No proof was needed, just doubt.
The trust in science has also been harmed by the vast amount of published medical research that is wrong. An effort was made 20 years ago to rid research of the bias of taking money from drug companies. To my observation, that change produced only a small benefit that has been overwhelmed by the unintended harms. The large, well-funded academic labs of full-time researchers have been replaced with unfunded, undertrained, and inadequately supported part-time junior faculty trying to publish enough articles to be promoted. In my opinion, this change is worse than funding from Big Pharma. (Disclosure – I worked in industry prior to graduate school.)
The pressure to publish reduces skepticism, so more incorrect data are published. The small size of these amateur studies produces unconvincing conclusions that feed an industry of meta-analysis that tries to overcome the deficiencies of the individual studies. This fragmented, biased approach is not how you build, launch, deploy, and operate the JWST, which requires very high reliability.
This approach is not working well for pediatrics either. I look at the history of the recommended workup of the febrile young infant from the 1980s until today. I see constant changes to the guidelines but no real progress toward a validated, evidence-based approach. A similar history is behind treatment of neonatal hyperbilirubinemia. In the 1994 publication, there was a movement toward being less aggressive. The 2004 and 2009 editions increased the frequency of screening and phototherapy. Now, the 2022 guidelines have moved in the direction we were headed in the 1990s. The workup of infants and children with possible urinary tract infections has undergone a similar trajectory. So has the screening for neonatal herpes infections. The practice changes are more like Brownian motion than real progress. This inconsistency has led me to be skeptical of the process the American Academy of Pediatrics uses to create guidelines.
Part of solving complex problems is allowing all stakeholders’ voices to be heard. On Jan. 28, 1986, seconds after liftoff, the space shuttle Challenger exploded. In the aftermath, it was determined that some engineers had expressed concern about the very cold weather that morning. The rubber in the O-ring would not be as flexible as designed. Their objection was not listened to. The O-ring failed, the fuel tank exploded, and the ship and crew were lost. It is a lesson many engineers of my generation took to heart. Do not suppress voices.
For example, 1 year ago (September 2021), the Royal Australian and New Zealand College of Psychiatrists published a position statement, “Recognising and addressing the mental health needs of people experiencing gender dysphoria/gender incongruence.” The statement expressed concern about the marked increase in incidence of rapid-onset gender dysphoria and therefore urged more thorough assessment by psychiatry before embarking on puberty-blocking therapies. The RANZCP position is at variance with recent trends in the United States. The topic was censored at the 2021 AAP national conference. Lately, I have heard the words disinformation and homophobic used to describe my RANZCP colleagues. I have been comparing AAP, Britain’s National Institute for Health and Care Excellence, and Royal Children’s Hospital Melbourne guidelines for 20 years. The variation is enlightening. I do not know the correct answer to treating gender dysphoria, but I know suppressing viewpoints and debate leads to exploding spaceships.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
The James Webb Space Telescope (JWST) is an engineering marvel. Costing over $10 billion, it should be. The project cost overrun was 900%. The launch was delayed by more than a decade. The Human Genome Project from 1990 to 2003 was completed slightly ahead of schedule and for less than the $4-$5 billion original estimates. This HGP success story is partly because of private entrepreneurial involvement. The Superconducting Super Collider in Texas spent $2 billion but never got off the ground. Successfully shepherding huge public projects like these involves the art of politics and management as well as science.
Whatever the earlier missteps, the JWST project is now performing above expectations. It has launched, taken up residence a million miles from Earth, deployed its mirrors (a process that had more than 300 possible single points of failure, any one of which would reduce the thing to scrap metal), and been calibrated. The JWST has even been dented by a micrometeoroid – sort of like a parking lot ding on the door of your brand new car. The first images are visually amazing and producing new scientific insights. This is a pinnacle of scientific achievement.
What characteristics enable such an achievement? How do we foster those same characteristics in the practice of medicine and medical research? Will the success of the JWST increase and restore the public’s trust in science and scientists?
After all the bickering over vaccines and masks for the past 2+ years, medical science could use a boost. The gravitas of scientists, and indeed all experts, has diminished over the 5 decades since humans walked on the moon. It has been harmed by mercenary scientists who sought to sow doubt about whether smoking caused cancer and whether fossil fuels created climate change. No proof was needed, just doubt.
The trust in science has also been harmed by the vast amount of published medical research that is wrong. An effort was made 20 years ago to rid research of the bias of taking money from drug companies. To my observation, that change produced only a small benefit that has been overwhelmed by the unintended harms. The large, well-funded academic labs of full-time researchers have been replaced with unfunded, undertrained, and inadequately supported part-time junior faculty trying to publish enough articles to be promoted. In my opinion, this change is worse than funding from Big Pharma. (Disclosure – I worked in industry prior to graduate school.)
The pressure to publish reduces skepticism, so more incorrect data are published. The small size of these amateur studies produces unconvincing conclusions that feed an industry of meta-analysis that tries to overcome the deficiencies of the individual studies. This fragmented, biased approach is not how you build, launch, deploy, and operate the JWST, which requires very high reliability.
This approach is not working well for pediatrics either. I look at the history of the recommended workup of the febrile young infant from the 1980s until today. I see constant changes to the guidelines but no real progress toward a validated, evidence-based approach. A similar history is behind treatment of neonatal hyperbilirubinemia. In the 1994 publication, there was a movement toward being less aggressive. The 2004 and 2009 editions increased the frequency of screening and phototherapy. Now, the 2022 guidelines have moved in the direction we were headed in the 1990s. The workup of infants and children with possible urinary tract infections has undergone a similar trajectory. So has the screening for neonatal herpes infections. The practice changes are more like Brownian motion than real progress. This inconsistency has led me to be skeptical of the process the American Academy of Pediatrics uses to create guidelines.
Part of solving complex problems is allowing all stakeholders’ voices to be heard. On Jan. 28, 1986, seconds after liftoff, the space shuttle Challenger exploded. In the aftermath, it was determined that some engineers had expressed concern about the very cold weather that morning. The rubber in the O-ring would not be as flexible as designed. Their objection was not listened to. The O-ring failed, the fuel tank exploded, and the ship and crew were lost. It is a lesson many engineers of my generation took to heart. Do not suppress voices.
For example, 1 year ago (September 2021), the Royal Australian and New Zealand College of Psychiatrists published a position statement, “Recognising and addressing the mental health needs of people experiencing gender dysphoria/gender incongruence.” The statement expressed concern about the marked increase in incidence of rapid-onset gender dysphoria and therefore urged more thorough assessment by psychiatry before embarking on puberty-blocking therapies. The RANZCP position is at variance with recent trends in the United States. The topic was censored at the 2021 AAP national conference. Lately, I have heard the words disinformation and homophobic used to describe my RANZCP colleagues. I have been comparing AAP, Britain’s National Institute for Health and Care Excellence, and Royal Children’s Hospital Melbourne guidelines for 20 years. The variation is enlightening. I do not know the correct answer to treating gender dysphoria, but I know suppressing viewpoints and debate leads to exploding spaceships.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
The James Webb Space Telescope (JWST) is an engineering marvel. Costing over $10 billion, it should be. The project cost overrun was 900%. The launch was delayed by more than a decade. The Human Genome Project from 1990 to 2003 was completed slightly ahead of schedule and for less than the $4-$5 billion original estimates. This HGP success story is partly because of private entrepreneurial involvement. The Superconducting Super Collider in Texas spent $2 billion but never got off the ground. Successfully shepherding huge public projects like these involves the art of politics and management as well as science.
Whatever the earlier missteps, the JWST project is now performing above expectations. It has launched, taken up residence a million miles from Earth, deployed its mirrors (a process that had more than 300 possible single points of failure, any one of which would reduce the thing to scrap metal), and been calibrated. The JWST has even been dented by a micrometeoroid – sort of like a parking lot ding on the door of your brand new car. The first images are visually amazing and producing new scientific insights. This is a pinnacle of scientific achievement.
What characteristics enable such an achievement? How do we foster those same characteristics in the practice of medicine and medical research? Will the success of the JWST increase and restore the public’s trust in science and scientists?
After all the bickering over vaccines and masks for the past 2+ years, medical science could use a boost. The gravitas of scientists, and indeed all experts, has diminished over the 5 decades since humans walked on the moon. It has been harmed by mercenary scientists who sought to sow doubt about whether smoking caused cancer and whether fossil fuels created climate change. No proof was needed, just doubt.
The trust in science has also been harmed by the vast amount of published medical research that is wrong. An effort was made 20 years ago to rid research of the bias of taking money from drug companies. To my observation, that change produced only a small benefit that has been overwhelmed by the unintended harms. The large, well-funded academic labs of full-time researchers have been replaced with unfunded, undertrained, and inadequately supported part-time junior faculty trying to publish enough articles to be promoted. In my opinion, this change is worse than funding from Big Pharma. (Disclosure – I worked in industry prior to graduate school.)
The pressure to publish reduces skepticism, so more incorrect data are published. The small size of these amateur studies produces unconvincing conclusions that feed an industry of meta-analysis that tries to overcome the deficiencies of the individual studies. This fragmented, biased approach is not how you build, launch, deploy, and operate the JWST, which requires very high reliability.
This approach is not working well for pediatrics either. I look at the history of the recommended workup of the febrile young infant from the 1980s until today. I see constant changes to the guidelines but no real progress toward a validated, evidence-based approach. A similar history is behind treatment of neonatal hyperbilirubinemia. In the 1994 publication, there was a movement toward being less aggressive. The 2004 and 2009 editions increased the frequency of screening and phototherapy. Now, the 2022 guidelines have moved in the direction we were headed in the 1990s. The workup of infants and children with possible urinary tract infections has undergone a similar trajectory. So has the screening for neonatal herpes infections. The practice changes are more like Brownian motion than real progress. This inconsistency has led me to be skeptical of the process the American Academy of Pediatrics uses to create guidelines.
Part of solving complex problems is allowing all stakeholders’ voices to be heard. On Jan. 28, 1986, seconds after liftoff, the space shuttle Challenger exploded. In the aftermath, it was determined that some engineers had expressed concern about the very cold weather that morning. The rubber in the O-ring would not be as flexible as designed. Their objection was not listened to. The O-ring failed, the fuel tank exploded, and the ship and crew were lost. It is a lesson many engineers of my generation took to heart. Do not suppress voices.
For example, 1 year ago (September 2021), the Royal Australian and New Zealand College of Psychiatrists published a position statement, “Recognising and addressing the mental health needs of people experiencing gender dysphoria/gender incongruence.” The statement expressed concern about the marked increase in incidence of rapid-onset gender dysphoria and therefore urged more thorough assessment by psychiatry before embarking on puberty-blocking therapies. The RANZCP position is at variance with recent trends in the United States. The topic was censored at the 2021 AAP national conference. Lately, I have heard the words disinformation and homophobic used to describe my RANZCP colleagues. I have been comparing AAP, Britain’s National Institute for Health and Care Excellence, and Royal Children’s Hospital Melbourne guidelines for 20 years. The variation is enlightening. I do not know the correct answer to treating gender dysphoria, but I know suppressing viewpoints and debate leads to exploding spaceships.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
FDA approves first gene therapy, betibeglogene autotemcel (Zynteglo), for beta-thalassemia

Betibeglogene autotemcel, a one-time gene therapy, represents a potential cure in which functional copies of the mutated gene are inserted into patients’ hematopoietic stem cells via a replication-defective lentivirus.
“Today’s approval is an important advance in the treatment of beta-thalassemia, particularly in individuals who require ongoing red blood cell transfusions,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in an FDA press release. “Given the potential health complications associated with this serious disease, this action highlights the FDA’s continued commitment to supporting development of innovative therapies for patients who have limited treatment options.”
The approval was based on phase 3 trials, in which 89% of 41 patients aged 4-34 years who received the therapy maintained normal or near-normal hemoglobin levels and didn’t need transfusions for at least a year. The patients were as young as age 4, maker Bluebird Bio said in a press release.
FDA’s Cellular, Tissue, and Gene Therapies Advisory Committee unanimously recommended approval in June. The gene therapy had been approved in Europe, where it carried a price tag of about $1.8 million, but Bluebird pulled it from the market in 2021 because of problems with reimbursement.
“The decision to discontinue operations in Europe resulted from prolonged negotiations with European payers and challenges to achieving appropriate value recognition and market access,” the company said in a Securities and Exchange Commission filing.
The projected price in the United States is even higher: $2.1 million.
But the Institute for Clinical and Economic Review, an influential Boston-based nonprofit organization that specializes in medical cost-effectiveness analyses, concluded in June that, “given the high annual costs of standard care ... this new treatment meets commonly accepted value thresholds at an anticipated price of $2.1 million,” particularly with Bluebird’s proposal to pay back 80% of the cost if patients need a transfusion within 5 years.
The company is planning an October 2022 launch and estimates the U.S. market for betibeglogene autotemcel to be about 1,500 patients.
Adverse events in studies were “infrequent and consisted primarily of nonserious infusion-related reactions,” such as abdominal pain, hot flush, dyspnea, tachycardia, noncardiac chest pain, and cytopenias, including thrombocytopenia, leukopenia, and neutropenia. One case of thrombocytopenia was considered serious but resolved, according to the company.
Most of the serious adverse events were related to hematopoietic stem cell collection and the busulfan conditioning regimen. Insertional oncogenesis and/or cancer have been reported with Bluebird’s other gene therapy products, but no cases have been associated with betibeglogene autotemcel.
A version of this article first appeared on Medscape.com.
Betibeglogene autotemcel, a one-time gene therapy, represents a potential cure in which functional copies of the mutated gene are inserted into patients’ hematopoietic stem cells via a replication-defective lentivirus.
“Today’s approval is an important advance in the treatment of beta-thalassemia, particularly in individuals who require ongoing red blood cell transfusions,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in an FDA press release. “Given the potential health complications associated with this serious disease, this action highlights the FDA’s continued commitment to supporting development of innovative therapies for patients who have limited treatment options.”
The approval was based on phase 3 trials, in which 89% of 41 patients aged 4-34 years who received the therapy maintained normal or near-normal hemoglobin levels and didn’t need transfusions for at least a year. The patients were as young as age 4, maker Bluebird Bio said in a press release.
FDA’s Cellular, Tissue, and Gene Therapies Advisory Committee unanimously recommended approval in June. The gene therapy had been approved in Europe, where it carried a price tag of about $1.8 million, but Bluebird pulled it from the market in 2021 because of problems with reimbursement.
“The decision to discontinue operations in Europe resulted from prolonged negotiations with European payers and challenges to achieving appropriate value recognition and market access,” the company said in a Securities and Exchange Commission filing.
The projected price in the United States is even higher: $2.1 million.
But the Institute for Clinical and Economic Review, an influential Boston-based nonprofit organization that specializes in medical cost-effectiveness analyses, concluded in June that, “given the high annual costs of standard care ... this new treatment meets commonly accepted value thresholds at an anticipated price of $2.1 million,” particularly with Bluebird’s proposal to pay back 80% of the cost if patients need a transfusion within 5 years.
The company is planning an October 2022 launch and estimates the U.S. market for betibeglogene autotemcel to be about 1,500 patients.
Adverse events in studies were “infrequent and consisted primarily of nonserious infusion-related reactions,” such as abdominal pain, hot flush, dyspnea, tachycardia, noncardiac chest pain, and cytopenias, including thrombocytopenia, leukopenia, and neutropenia. One case of thrombocytopenia was considered serious but resolved, according to the company.
Most of the serious adverse events were related to hematopoietic stem cell collection and the busulfan conditioning regimen. Insertional oncogenesis and/or cancer have been reported with Bluebird’s other gene therapy products, but no cases have been associated with betibeglogene autotemcel.
A version of this article first appeared on Medscape.com.
Betibeglogene autotemcel, a one-time gene therapy, represents a potential cure in which functional copies of the mutated gene are inserted into patients’ hematopoietic stem cells via a replication-defective lentivirus.
“Today’s approval is an important advance in the treatment of beta-thalassemia, particularly in individuals who require ongoing red blood cell transfusions,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in an FDA press release. “Given the potential health complications associated with this serious disease, this action highlights the FDA’s continued commitment to supporting development of innovative therapies for patients who have limited treatment options.”
The approval was based on phase 3 trials, in which 89% of 41 patients aged 4-34 years who received the therapy maintained normal or near-normal hemoglobin levels and didn’t need transfusions for at least a year. The patients were as young as age 4, maker Bluebird Bio said in a press release.
FDA’s Cellular, Tissue, and Gene Therapies Advisory Committee unanimously recommended approval in June. The gene therapy had been approved in Europe, where it carried a price tag of about $1.8 million, but Bluebird pulled it from the market in 2021 because of problems with reimbursement.
“The decision to discontinue operations in Europe resulted from prolonged negotiations with European payers and challenges to achieving appropriate value recognition and market access,” the company said in a Securities and Exchange Commission filing.
The projected price in the United States is even higher: $2.1 million.
But the Institute for Clinical and Economic Review, an influential Boston-based nonprofit organization that specializes in medical cost-effectiveness analyses, concluded in June that, “given the high annual costs of standard care ... this new treatment meets commonly accepted value thresholds at an anticipated price of $2.1 million,” particularly with Bluebird’s proposal to pay back 80% of the cost if patients need a transfusion within 5 years.
The company is planning an October 2022 launch and estimates the U.S. market for betibeglogene autotemcel to be about 1,500 patients.
Adverse events in studies were “infrequent and consisted primarily of nonserious infusion-related reactions,” such as abdominal pain, hot flush, dyspnea, tachycardia, noncardiac chest pain, and cytopenias, including thrombocytopenia, leukopenia, and neutropenia. One case of thrombocytopenia was considered serious but resolved, according to the company.
Most of the serious adverse events were related to hematopoietic stem cell collection and the busulfan conditioning regimen. Insertional oncogenesis and/or cancer have been reported with Bluebird’s other gene therapy products, but no cases have been associated with betibeglogene autotemcel.
A version of this article first appeared on Medscape.com.
FDA approves adalimumab-bwwd biosimilar (Hadlima) in high-concentration form
The U.S. Food and Drug Administration today approved a citrate-free, high-concentration formulation of adalimumab-bwwd (Hadlima), the manufacturer, Samsung Bioepis, and its commercialization partner Organon said in an announcement.
Hadlima is a biosimilar of the tumor necrosis factor inhibitor reference product adalimumab (Humira).
Hadlima was first approved in July 2019 in a citrated, 50-mg/mL formulation. The new citrate-free, 100-mg/mL version will be available in prefilled syringe and autoinjector options.
The 100-mg/mL formulation is indicated for the same seven conditions as its 50-mg/mL counterpart: rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, adult and pediatric Crohn’s disease, and ulcerative colitis.
The approval was based on clinical data from a randomized, single-blind, two-arm, parallel group, single-dose study that compared the pharmacokinetics, safety, tolerability, and immunogenicity of the 100-mg/mL and 50-mg/mL formulations of Hadlima in healthy volunteers.
Both low- and high-concentration formulations of Humira are currently marketed in the United States. Organon said that it expects to market Hadlima in the United States on or after July 1, 2023, in accordance with a licensing agreement with AbbVie.
The prescribing information for Hadlima includes specific warnings and areas of concern. The drug should not be administered to individuals who are known to be hypersensitive to adalimumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, including serious infections leading to hospitalization or death, such as tuberculosis, bacterial sepsis, invasive fungal infections (such as histoplasmosis), and infections attributable to other opportunistic pathogens.
A test for latent TB infection should be given before administration, and treatment of TB should begin before administration of Hadlima.
Patients taking Hadlima should not take a live vaccine.
The most common adverse effects (incidence > 10%) include infections (for example, upper respiratory infections, sinusitis), injection site reactions, headache, and rash.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration today approved a citrate-free, high-concentration formulation of adalimumab-bwwd (Hadlima), the manufacturer, Samsung Bioepis, and its commercialization partner Organon said in an announcement.
Hadlima is a biosimilar of the tumor necrosis factor inhibitor reference product adalimumab (Humira).
Hadlima was first approved in July 2019 in a citrated, 50-mg/mL formulation. The new citrate-free, 100-mg/mL version will be available in prefilled syringe and autoinjector options.
The 100-mg/mL formulation is indicated for the same seven conditions as its 50-mg/mL counterpart: rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, adult and pediatric Crohn’s disease, and ulcerative colitis.
The approval was based on clinical data from a randomized, single-blind, two-arm, parallel group, single-dose study that compared the pharmacokinetics, safety, tolerability, and immunogenicity of the 100-mg/mL and 50-mg/mL formulations of Hadlima in healthy volunteers.
Both low- and high-concentration formulations of Humira are currently marketed in the United States. Organon said that it expects to market Hadlima in the United States on or after July 1, 2023, in accordance with a licensing agreement with AbbVie.
The prescribing information for Hadlima includes specific warnings and areas of concern. The drug should not be administered to individuals who are known to be hypersensitive to adalimumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, including serious infections leading to hospitalization or death, such as tuberculosis, bacterial sepsis, invasive fungal infections (such as histoplasmosis), and infections attributable to other opportunistic pathogens.
A test for latent TB infection should be given before administration, and treatment of TB should begin before administration of Hadlima.
Patients taking Hadlima should not take a live vaccine.
The most common adverse effects (incidence > 10%) include infections (for example, upper respiratory infections, sinusitis), injection site reactions, headache, and rash.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration today approved a citrate-free, high-concentration formulation of adalimumab-bwwd (Hadlima), the manufacturer, Samsung Bioepis, and its commercialization partner Organon said in an announcement.
Hadlima is a biosimilar of the tumor necrosis factor inhibitor reference product adalimumab (Humira).
Hadlima was first approved in July 2019 in a citrated, 50-mg/mL formulation. The new citrate-free, 100-mg/mL version will be available in prefilled syringe and autoinjector options.
The 100-mg/mL formulation is indicated for the same seven conditions as its 50-mg/mL counterpart: rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, adult and pediatric Crohn’s disease, and ulcerative colitis.
The approval was based on clinical data from a randomized, single-blind, two-arm, parallel group, single-dose study that compared the pharmacokinetics, safety, tolerability, and immunogenicity of the 100-mg/mL and 50-mg/mL formulations of Hadlima in healthy volunteers.
Both low- and high-concentration formulations of Humira are currently marketed in the United States. Organon said that it expects to market Hadlima in the United States on or after July 1, 2023, in accordance with a licensing agreement with AbbVie.
The prescribing information for Hadlima includes specific warnings and areas of concern. The drug should not be administered to individuals who are known to be hypersensitive to adalimumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, including serious infections leading to hospitalization or death, such as tuberculosis, bacterial sepsis, invasive fungal infections (such as histoplasmosis), and infections attributable to other opportunistic pathogens.
A test for latent TB infection should be given before administration, and treatment of TB should begin before administration of Hadlima.
Patients taking Hadlima should not take a live vaccine.
The most common adverse effects (incidence > 10%) include infections (for example, upper respiratory infections, sinusitis), injection site reactions, headache, and rash.
A version of this article first appeared on Medscape.com.