User login
The Genitals Are a Window Into Health: Sex as a Vital Sign
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
A Brief Glimpse Into 80,000 Years of Human History
Like millions of other modern humans, my daughter and I stood in the backyard recently and watched comet C/2023 A3 (Tsuchinshan–ATLAS) with binoculars. It took a few minutes to locate, but once you see it is unmistakable.
It’s got a long (at least in human terms) orbit, roughly 80,000 years. So what was going on here, on our pale blue dot, the last time it graced our skies?
Well, here in Phoenix, the people were ... not here. Nor were they in Arizona, or North America, or pretty much the entire Western Hemisphere.
In fact, Homo sapiens were confined to Africa. The hardier Neanderthals had successfully moved into Eurasia, but our lineage was just starting to migrate there. There’s some evidence that we numbered maybe 10,000-15,000 at that point. Far more people saw the comet that night in the United States than our entire population count last time it swung by.
But we were moving up in the world. Our ancestors at the time had developed the first forms of jewelry, using seashells. There’s evidence that we’d learned to trade with other, distant, communities. We were using spears to put dinner on the table with less risk to ourselves than clubs posed.
And, in what’s now Kenya, in the same time frame, a pair of grieving parents carefully buried their 3-year-old child, wrapped in a covering and gently placed on a pillow.
Sadly, this isn’t a scene we’re unfamiliar with. Possibly the most famous painting of a physician is “The Doctor” (1891) by Luke Fildes, showing a physician trying to treat a seriously ill child while the parents look on helplessly.

What did the Kenyan child die from? We’ll probably never know. Did they try to treat it? Most likely.
Humans, by nature, form societies. The size varies, but everyone has a role. There was probably some ancestor of Fildes’ doctor in the group who tried to help. Perhaps with prayers in an unknown tongue, or a preparation of certain leaves, or placing the child near a fire. When whatever they tried failed, the same person likely consoled the parents. Maybe they were involved in the burial, too.
The child would be found in 2017, giving us the first clear evidence of a ritual human burial in Africa. Just like today, we let go of our lost ones with ceremony. Perhaps the parents noticed the comet and thought it was their child’s spirit departing.
Now the comet is back. The planet hasn’t changed dramatically in 80,000 years (which isn’t much in geological time), but we have.
Would today’s doctors have been able to save the child? No idea, though we probably have a better chance than our professional ancestor did.

But our job hasn’t changed. Like us, the ancient practitioner probably tried to figure out why the child was sick and what could be done about it. When it was over they, and others, grieved with the parents.
The comet will be back in 80,000 years. On our scale, that’s a long time. The entire recorded history of our species is only 5,000 to 8,000 years. We’ve come a long way, but where we’re going in 80,000 years is anyone’s guess.
Will doctors in the year 82024 even know what we do now to care for people? Will they still be practicing on the third rock from the sun, or spread out across the galaxy? Will there even be doctors? (Probably, in one form or another.)
But We do our best to care, heal, and hope now, as we did then, and as our descendants will.
And, like my daughter and I did, no matter where we are, we will still look up at the sky with wonder.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Like millions of other modern humans, my daughter and I stood in the backyard recently and watched comet C/2023 A3 (Tsuchinshan–ATLAS) with binoculars. It took a few minutes to locate, but once you see it is unmistakable.
It’s got a long (at least in human terms) orbit, roughly 80,000 years. So what was going on here, on our pale blue dot, the last time it graced our skies?
Well, here in Phoenix, the people were ... not here. Nor were they in Arizona, or North America, or pretty much the entire Western Hemisphere.
In fact, Homo sapiens were confined to Africa. The hardier Neanderthals had successfully moved into Eurasia, but our lineage was just starting to migrate there. There’s some evidence that we numbered maybe 10,000-15,000 at that point. Far more people saw the comet that night in the United States than our entire population count last time it swung by.
But we were moving up in the world. Our ancestors at the time had developed the first forms of jewelry, using seashells. There’s evidence that we’d learned to trade with other, distant, communities. We were using spears to put dinner on the table with less risk to ourselves than clubs posed.
And, in what’s now Kenya, in the same time frame, a pair of grieving parents carefully buried their 3-year-old child, wrapped in a covering and gently placed on a pillow.
Sadly, this isn’t a scene we’re unfamiliar with. Possibly the most famous painting of a physician is “The Doctor” (1891) by Luke Fildes, showing a physician trying to treat a seriously ill child while the parents look on helplessly.
What did the Kenyan child die from? We’ll probably never know. Did they try to treat it? Most likely.
Humans, by nature, form societies. The size varies, but everyone has a role. There was probably some ancestor of Fildes’ doctor in the group who tried to help. Perhaps with prayers in an unknown tongue, or a preparation of certain leaves, or placing the child near a fire. When whatever they tried failed, the same person likely consoled the parents. Maybe they were involved in the burial, too.
The child would be found in 2017, giving us the first clear evidence of a ritual human burial in Africa. Just like today, we let go of our lost ones with ceremony. Perhaps the parents noticed the comet and thought it was their child’s spirit departing.
Now the comet is back. The planet hasn’t changed dramatically in 80,000 years (which isn’t much in geological time), but we have.
Would today’s doctors have been able to save the child? No idea, though we probably have a better chance than our professional ancestor did.
But our job hasn’t changed. Like us, the ancient practitioner probably tried to figure out why the child was sick and what could be done about it. When it was over they, and others, grieved with the parents.
The comet will be back in 80,000 years. On our scale, that’s a long time. The entire recorded history of our species is only 5,000 to 8,000 years. We’ve come a long way, but where we’re going in 80,000 years is anyone’s guess.
Will doctors in the year 82024 even know what we do now to care for people? Will they still be practicing on the third rock from the sun, or spread out across the galaxy? Will there even be doctors? (Probably, in one form or another.)
But We do our best to care, heal, and hope now, as we did then, and as our descendants will.
And, like my daughter and I did, no matter where we are, we will still look up at the sky with wonder.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Like millions of other modern humans, my daughter and I stood in the backyard recently and watched comet C/2023 A3 (Tsuchinshan–ATLAS) with binoculars. It took a few minutes to locate, but once you see it is unmistakable.
It’s got a long (at least in human terms) orbit, roughly 80,000 years. So what was going on here, on our pale blue dot, the last time it graced our skies?
Well, here in Phoenix, the people were ... not here. Nor were they in Arizona, or North America, or pretty much the entire Western Hemisphere.
In fact, Homo sapiens were confined to Africa. The hardier Neanderthals had successfully moved into Eurasia, but our lineage was just starting to migrate there. There’s some evidence that we numbered maybe 10,000-15,000 at that point. Far more people saw the comet that night in the United States than our entire population count last time it swung by.
But we were moving up in the world. Our ancestors at the time had developed the first forms of jewelry, using seashells. There’s evidence that we’d learned to trade with other, distant, communities. We were using spears to put dinner on the table with less risk to ourselves than clubs posed.
And, in what’s now Kenya, in the same time frame, a pair of grieving parents carefully buried their 3-year-old child, wrapped in a covering and gently placed on a pillow.
Sadly, this isn’t a scene we’re unfamiliar with. Possibly the most famous painting of a physician is “The Doctor” (1891) by Luke Fildes, showing a physician trying to treat a seriously ill child while the parents look on helplessly.
What did the Kenyan child die from? We’ll probably never know. Did they try to treat it? Most likely.
Humans, by nature, form societies. The size varies, but everyone has a role. There was probably some ancestor of Fildes’ doctor in the group who tried to help. Perhaps with prayers in an unknown tongue, or a preparation of certain leaves, or placing the child near a fire. When whatever they tried failed, the same person likely consoled the parents. Maybe they were involved in the burial, too.
The child would be found in 2017, giving us the first clear evidence of a ritual human burial in Africa. Just like today, we let go of our lost ones with ceremony. Perhaps the parents noticed the comet and thought it was their child’s spirit departing.
Now the comet is back. The planet hasn’t changed dramatically in 80,000 years (which isn’t much in geological time), but we have.
Would today’s doctors have been able to save the child? No idea, though we probably have a better chance than our professional ancestor did.
But our job hasn’t changed. Like us, the ancient practitioner probably tried to figure out why the child was sick and what could be done about it. When it was over they, and others, grieved with the parents.
The comet will be back in 80,000 years. On our scale, that’s a long time. The entire recorded history of our species is only 5,000 to 8,000 years. We’ve come a long way, but where we’re going in 80,000 years is anyone’s guess.
Will doctors in the year 82024 even know what we do now to care for people? Will they still be practicing on the third rock from the sun, or spread out across the galaxy? Will there even be doctors? (Probably, in one form or another.)
But We do our best to care, heal, and hope now, as we did then, and as our descendants will.
And, like my daughter and I did, no matter where we are, we will still look up at the sky with wonder.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Overuse of Digital Devices in the Exam Room: A Teaching Opportunity
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.
At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.
At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.
At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
The New Cancer Stats Might Look Like a Death Sentence. They Aren’t.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Heard of ApoB Testing? New Guidelines
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
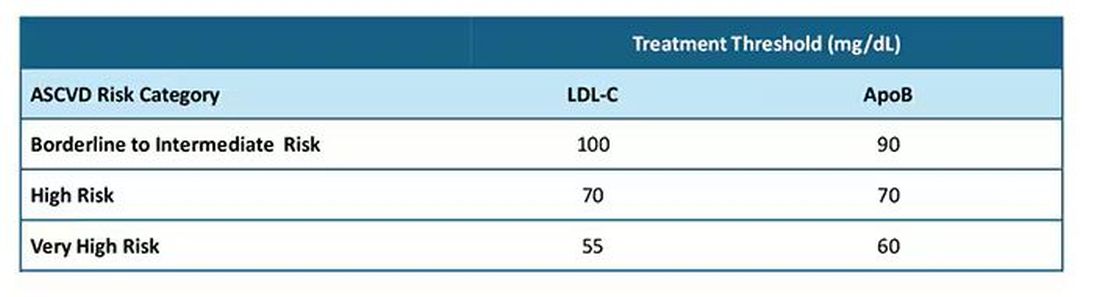
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
Mechanism of Action
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
What Should You Do When a Patient Asks for a PSA Test?
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Maternal Immunization to Prevent Serious Respiratory Illness
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.

Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.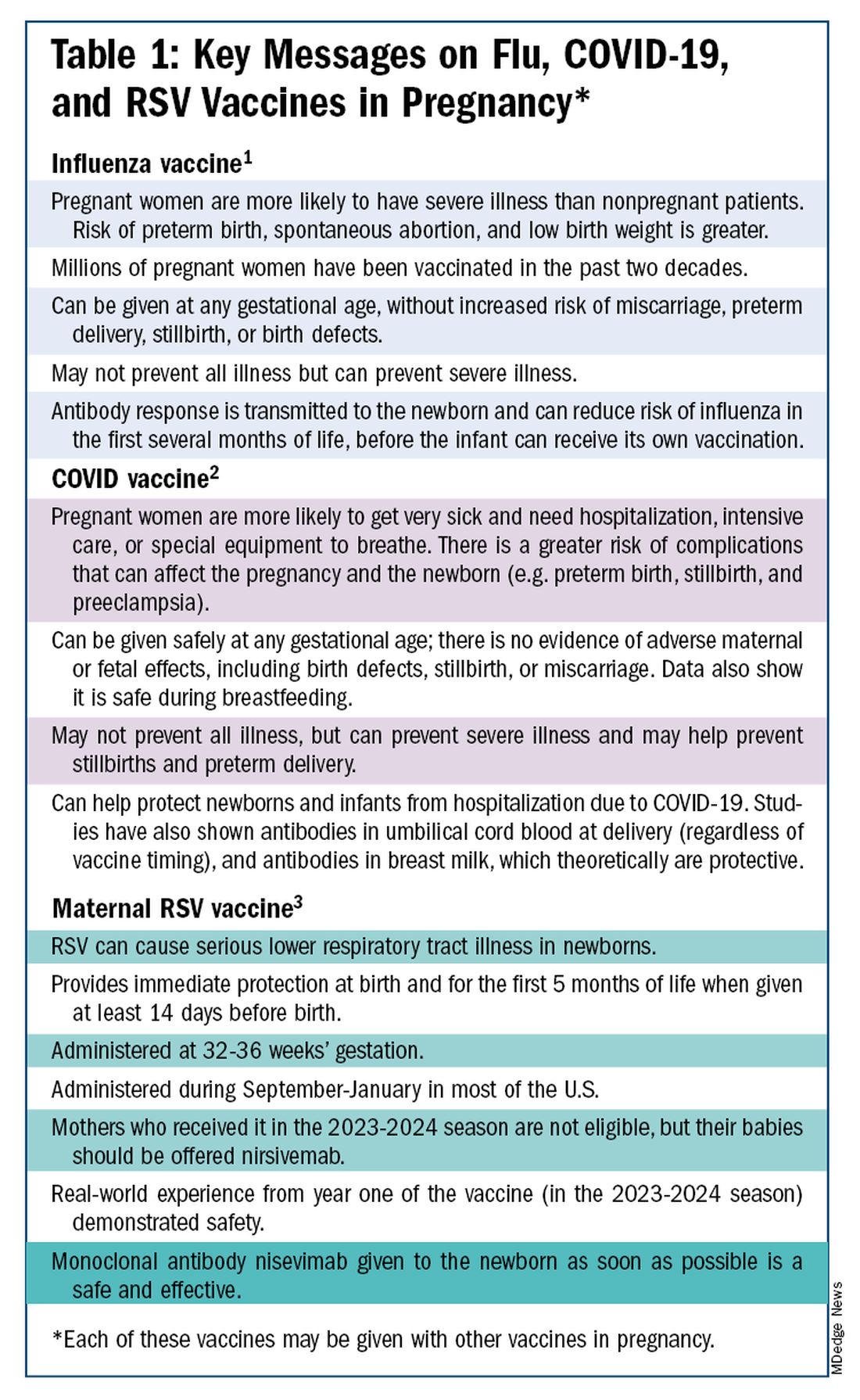
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.

With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)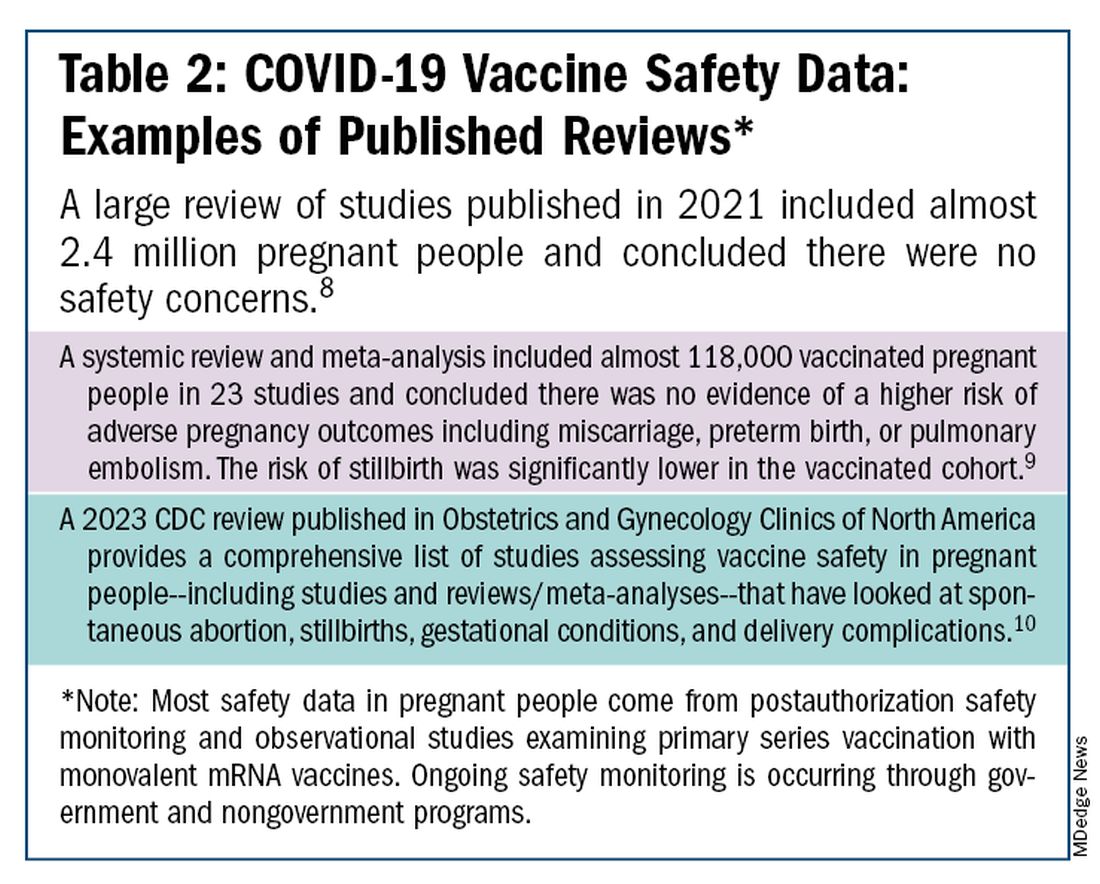
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
SAFE: Ensuring Access for Children With Neurodevelopmental Disabilities
We pediatricians consider ourselves as compassionate professionals, optimistic about the potential of all children. This is reflected in the American Academy of Pediatrics’ equity statement of “its mission to ensure the health and well-being of all children. This includes promoting nurturing, inclusive environments and actively opposing intolerance, bigotry, bias, and discrimination.”
A committee of the Developmental Behavioral Pediatric Network developed and published a consensus statement specifically about problems in the care of individuals with neurodevelopmental disabilities (NDD) called the Supporting Access for Everyone (SAFE) initiative. All of us care for children with NDD as one in six are affected with these conditions that impact cognition, communication, motor, social, and/or behavior skills such as autism, ADHD, intellectual disabilities (ID), learning disorders, hearing or vision impairment, and motor disabilities such as cerebral palsy. Children with NDD are overrepresented in our daily practice schedule due to their multiple medical, behavioral, and social needs. NDD are also more common among marginalized children with racial, ethnic, sexual, or gender identity minority status compounding their difficulties in accessing quality care.
NDD present similar challenges to care as other chronic conditions that also require longer visits, more documentation, long-term monitoring, team-based care, care coordination, and often referrals. But most chronic medical conditions we care for such as asthma, diabetes, cancer, hypertension, and renal disease have clear national guidelines and appropriate billing codes and are not stigmatizing. Most also do not intrinsically affect the nervous system or cause disability as for NDD that alter the behavioral presentation of the individual in a way that changes their care.
Discrimination against individuals with NDD and other disabilities, called “ableism,” can take many forms: assuming a child with communication difficulty or ID is unable to understand explanations about their care; the presence of one NDD condition ending the clinician’s search for other issues; complicated problems or difficult behaviors in the medical setting truncating care, etc.
Adjustments Needed for Special Needs
As pediatricians we already adjust our interactions, starting instinctively, to the development level of the child we perceive before us. We approach infants slowly and softly, we speak in shorter sentences to toddlers, we joke around with school-aged children, and we take extra care about privacy with teens. This serves the relationships well for neurotypical children. But our (and our staff’s) perceptions of children with autism, ID, genetic syndromes that include NDD, or motor disabilities based on their behavioral presentation may not accurately recognize or accommodate their abilities or needs. Communication and environmental adjustments may need to be much more individualized to provide respectful care, comfort and even safety.
As an example, at this time 1 in 36 children have autism with or without ID. Defining features of autism include differences in social communication, repetitive or restrictive interests or behaviors, and hypersensitivity to the environment plus any coexisting conditions such as anxiety and hyperactivity. But most children with autism have completely age appropriate and typical physical appearance and their underlying condition may not even be known. The office setting, without special attention to the needs of a child with autism, may be frightening, loud, too bright, too crowded, fast paced, and confusing. The result of their sensitivities and difficulty communicating may lead to increased agitation, repetitive behaviors (sometimes called “stimming”), shrieking, attempts to escape the room, refusal to allow for vital signs or undressing, even aggression. Strategies for calming a neurotypical child such as talking or touching may make matters worse instead of better. We need help from the child and family and a plan to optimize their medical encounters.
If not adequately accommodated, children with many varieties of NDD end up not getting all the routine healthcare they need (eg vaccinations, blood tests, vital signs, even complete physical exams including dental) as well as having more adverse events during health care, including traumatizing seclusion, not allowing a support person to be present, restraint, injuries, and accidents. When more complex procedures are needed, eg x-ray, MRI, EEG, lab studies, or surgery, successful outcomes may be lower. Children with NDD have higher rates of often avoidable morbidity and mortality than those without, in part due to these barriers to complete care. While environmental accommodations to wheelchair users for accessibility has greatly improved in recent years, access to other kinds of individualized accommodations have lagged behind.
Accommodation Planning
There are a variety of factors that need to be taken into consideration in accommodating an individual with NDD. The family becomes the expert, along with the child, in knowing the child’s triggers, preferences, abilities, and level of understanding to accept and consent for care. An accommodation plan should be created using shared and supported decision making with the family and child and allowing for child preferences, regardless of their ability level, whenever possible. Development of an accommodation plan may benefit from multidisciplinary input, eg psychology, physical therapy, speech pathology, depending on the child’s needs and the practice’s ability to adapt.
The SAFE initiative is in the process of creating a checklist aiming to facilitate a description being created for each individual to help plan for a successful medical encounter while optimizing the child’s comfort, participation, and safety. While the checklist is not yet ready, we can start now by asking families and children in preparation for or at the start of a visit about their needs and writing a shared document that can also be placed in the electronic health record for the entire care team for informing care going forward.
It is especially important for the family to keep a copy of the care plan and for it to be sent as part of referrals for procedures or specialty visits so that the professionals can prepare and adapt the encounter. An excellent example is a how some hospitals schedule a practice visit for the child to experience the sights and sounds and people the child will encounter, for example, before an EEG, when nothing is required of the child. Scheduling the actual procedure at times of day when clinics are less crowded and wait times are shorter can improve the chances of success.
Some categories and details that might be included in an accommodation plan are listed below:
You might start the plan with the child’s preferred name/nickname, family member or support person names, and diagnoses along with a brief overview of the child’s level of functioning. Then list categories of needs and preferences along with suggestions or requests.
- Motor: Does the child have or need assistance entering the building, visit room, bathroom, or transferring to the exam table? What kind of assistance, if any, and by whom?
- Sensory: Is the child disturbed by noise, lights, or being touched? Does the child want to use equipment to be comfortable such as headphones, earplugs, or sunglasses or need a quiet room, care without perfumes, or dimmed lighting? Does the child typically refuse aspects of the physical examination?
- Behavioral regulation: What helps the child to stay calm? Are there certain triggers to becoming upset? Are there early cues that an upset is coming? What and who can help in the case of an upset?
- Habits/preferences: Are there certain comfort objects or habits your child needs? Are there habits your child needs to do, such as a certain order of events, or use of social stories or pictures, to cooperate or feel comfortable?
- Communication: How does the child make his/her needs known? Does the child/family speak English or another language? Does he/she use sign language or an augmentative communication device? What level of understanding does your child have; for example, similar to what age for a typical child? Is there a care plan with accommodations already available that needs review or needs revision with the child’s development or is a new one needed? Was the care plan developed including the child’s participation and assent or is more collaboration needed?
- History: Has your child had any very upsetting experiences in healthcare settings? What happened? Has the trauma been addressed? Are there reminders of the trauma that should be avoided?
- Other: Are there other things we should know about your child as an individual to provide the best care?
There are many actions needed to do better at ensuring equitable care for individuals with NDD. We should educate our office and medical staff about NDD in children and the importance of accommodating their needs, and ways to do it. The morning huddle can be used to remind staff of upcoming visits of children who may need accommodations. We then need to use quality improvement methods to check in periodically on how the changes are working for the children, families, and practice in order to continually improve.
The overall healthcare system also needs to change. Billing codes should reflect the time, complexity of accommodations, and documentation that were required for care. Episodes of the visit may need to be broken up within the day or over several days to allow the child to practice, calm down, and cooperate and this should be accounted for in billing. Given that NDD are generally lifelong conditions, payment systems that require measures of progress such as value-based payment based on improved outcomes will need to be adjusted to measure quality of care rather than significant progress.
We need to advocate for both individual children and for system changes to work toward equity of care for those with disabilities to make their lives more comfortable as well as ours.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
We pediatricians consider ourselves as compassionate professionals, optimistic about the potential of all children. This is reflected in the American Academy of Pediatrics’ equity statement of “its mission to ensure the health and well-being of all children. This includes promoting nurturing, inclusive environments and actively opposing intolerance, bigotry, bias, and discrimination.”
A committee of the Developmental Behavioral Pediatric Network developed and published a consensus statement specifically about problems in the care of individuals with neurodevelopmental disabilities (NDD) called the Supporting Access for Everyone (SAFE) initiative. All of us care for children with NDD as one in six are affected with these conditions that impact cognition, communication, motor, social, and/or behavior skills such as autism, ADHD, intellectual disabilities (ID), learning disorders, hearing or vision impairment, and motor disabilities such as cerebral palsy. Children with NDD are overrepresented in our daily practice schedule due to their multiple medical, behavioral, and social needs. NDD are also more common among marginalized children with racial, ethnic, sexual, or gender identity minority status compounding their difficulties in accessing quality care.
NDD present similar challenges to care as other chronic conditions that also require longer visits, more documentation, long-term monitoring, team-based care, care coordination, and often referrals. But most chronic medical conditions we care for such as asthma, diabetes, cancer, hypertension, and renal disease have clear national guidelines and appropriate billing codes and are not stigmatizing. Most also do not intrinsically affect the nervous system or cause disability as for NDD that alter the behavioral presentation of the individual in a way that changes their care.
Discrimination against individuals with NDD and other disabilities, called “ableism,” can take many forms: assuming a child with communication difficulty or ID is unable to understand explanations about their care; the presence of one NDD condition ending the clinician’s search for other issues; complicated problems or difficult behaviors in the medical setting truncating care, etc.
Adjustments Needed for Special Needs
As pediatricians we already adjust our interactions, starting instinctively, to the development level of the child we perceive before us. We approach infants slowly and softly, we speak in shorter sentences to toddlers, we joke around with school-aged children, and we take extra care about privacy with teens. This serves the relationships well for neurotypical children. But our (and our staff’s) perceptions of children with autism, ID, genetic syndromes that include NDD, or motor disabilities based on their behavioral presentation may not accurately recognize or accommodate their abilities or needs. Communication and environmental adjustments may need to be much more individualized to provide respectful care, comfort and even safety.
As an example, at this time 1 in 36 children have autism with or without ID. Defining features of autism include differences in social communication, repetitive or restrictive interests or behaviors, and hypersensitivity to the environment plus any coexisting conditions such as anxiety and hyperactivity. But most children with autism have completely age appropriate and typical physical appearance and their underlying condition may not even be known. The office setting, without special attention to the needs of a child with autism, may be frightening, loud, too bright, too crowded, fast paced, and confusing. The result of their sensitivities and difficulty communicating may lead to increased agitation, repetitive behaviors (sometimes called “stimming”), shrieking, attempts to escape the room, refusal to allow for vital signs or undressing, even aggression. Strategies for calming a neurotypical child such as talking or touching may make matters worse instead of better. We need help from the child and family and a plan to optimize their medical encounters.
If not adequately accommodated, children with many varieties of NDD end up not getting all the routine healthcare they need (eg vaccinations, blood tests, vital signs, even complete physical exams including dental) as well as having more adverse events during health care, including traumatizing seclusion, not allowing a support person to be present, restraint, injuries, and accidents. When more complex procedures are needed, eg x-ray, MRI, EEG, lab studies, or surgery, successful outcomes may be lower. Children with NDD have higher rates of often avoidable morbidity and mortality than those without, in part due to these barriers to complete care. While environmental accommodations to wheelchair users for accessibility has greatly improved in recent years, access to other kinds of individualized accommodations have lagged behind.
Accommodation Planning
There are a variety of factors that need to be taken into consideration in accommodating an individual with NDD. The family becomes the expert, along with the child, in knowing the child’s triggers, preferences, abilities, and level of understanding to accept and consent for care. An accommodation plan should be created using shared and supported decision making with the family and child and allowing for child preferences, regardless of their ability level, whenever possible. Development of an accommodation plan may benefit from multidisciplinary input, eg psychology, physical therapy, speech pathology, depending on the child’s needs and the practice’s ability to adapt.
The SAFE initiative is in the process of creating a checklist aiming to facilitate a description being created for each individual to help plan for a successful medical encounter while optimizing the child’s comfort, participation, and safety. While the checklist is not yet ready, we can start now by asking families and children in preparation for or at the start of a visit about their needs and writing a shared document that can also be placed in the electronic health record for the entire care team for informing care going forward.
It is especially important for the family to keep a copy of the care plan and for it to be sent as part of referrals for procedures or specialty visits so that the professionals can prepare and adapt the encounter. An excellent example is a how some hospitals schedule a practice visit for the child to experience the sights and sounds and people the child will encounter, for example, before an EEG, when nothing is required of the child. Scheduling the actual procedure at times of day when clinics are less crowded and wait times are shorter can improve the chances of success.
Some categories and details that might be included in an accommodation plan are listed below:
You might start the plan with the child’s preferred name/nickname, family member or support person names, and diagnoses along with a brief overview of the child’s level of functioning. Then list categories of needs and preferences along with suggestions or requests.
- Motor: Does the child have or need assistance entering the building, visit room, bathroom, or transferring to the exam table? What kind of assistance, if any, and by whom?
- Sensory: Is the child disturbed by noise, lights, or being touched? Does the child want to use equipment to be comfortable such as headphones, earplugs, or sunglasses or need a quiet room, care without perfumes, or dimmed lighting? Does the child typically refuse aspects of the physical examination?
- Behavioral regulation: What helps the child to stay calm? Are there certain triggers to becoming upset? Are there early cues that an upset is coming? What and who can help in the case of an upset?
- Habits/preferences: Are there certain comfort objects or habits your child needs? Are there habits your child needs to do, such as a certain order of events, or use of social stories or pictures, to cooperate or feel comfortable?
- Communication: How does the child make his/her needs known? Does the child/family speak English or another language? Does he/she use sign language or an augmentative communication device? What level of understanding does your child have; for example, similar to what age for a typical child? Is there a care plan with accommodations already available that needs review or needs revision with the child’s development or is a new one needed? Was the care plan developed including the child’s participation and assent or is more collaboration needed?
- History: Has your child had any very upsetting experiences in healthcare settings? What happened? Has the trauma been addressed? Are there reminders of the trauma that should be avoided?
- Other: Are there other things we should know about your child as an individual to provide the best care?
There are many actions needed to do better at ensuring equitable care for individuals with NDD. We should educate our office and medical staff about NDD in children and the importance of accommodating their needs, and ways to do it. The morning huddle can be used to remind staff of upcoming visits of children who may need accommodations. We then need to use quality improvement methods to check in periodically on how the changes are working for the children, families, and practice in order to continually improve.
The overall healthcare system also needs to change. Billing codes should reflect the time, complexity of accommodations, and documentation that were required for care. Episodes of the visit may need to be broken up within the day or over several days to allow the child to practice, calm down, and cooperate and this should be accounted for in billing. Given that NDD are generally lifelong conditions, payment systems that require measures of progress such as value-based payment based on improved outcomes will need to be adjusted to measure quality of care rather than significant progress.
We need to advocate for both individual children and for system changes to work toward equity of care for those with disabilities to make their lives more comfortable as well as ours.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
We pediatricians consider ourselves as compassionate professionals, optimistic about the potential of all children. This is reflected in the American Academy of Pediatrics’ equity statement of “its mission to ensure the health and well-being of all children. This includes promoting nurturing, inclusive environments and actively opposing intolerance, bigotry, bias, and discrimination.”
A committee of the Developmental Behavioral Pediatric Network developed and published a consensus statement specifically about problems in the care of individuals with neurodevelopmental disabilities (NDD) called the Supporting Access for Everyone (SAFE) initiative. All of us care for children with NDD as one in six are affected with these conditions that impact cognition, communication, motor, social, and/or behavior skills such as autism, ADHD, intellectual disabilities (ID), learning disorders, hearing or vision impairment, and motor disabilities such as cerebral palsy. Children with NDD are overrepresented in our daily practice schedule due to their multiple medical, behavioral, and social needs. NDD are also more common among marginalized children with racial, ethnic, sexual, or gender identity minority status compounding their difficulties in accessing quality care.
NDD present similar challenges to care as other chronic conditions that also require longer visits, more documentation, long-term monitoring, team-based care, care coordination, and often referrals. But most chronic medical conditions we care for such as asthma, diabetes, cancer, hypertension, and renal disease have clear national guidelines and appropriate billing codes and are not stigmatizing. Most also do not intrinsically affect the nervous system or cause disability as for NDD that alter the behavioral presentation of the individual in a way that changes their care.
Discrimination against individuals with NDD and other disabilities, called “ableism,” can take many forms: assuming a child with communication difficulty or ID is unable to understand explanations about their care; the presence of one NDD condition ending the clinician’s search for other issues; complicated problems or difficult behaviors in the medical setting truncating care, etc.
Adjustments Needed for Special Needs
As pediatricians we already adjust our interactions, starting instinctively, to the development level of the child we perceive before us. We approach infants slowly and softly, we speak in shorter sentences to toddlers, we joke around with school-aged children, and we take extra care about privacy with teens. This serves the relationships well for neurotypical children. But our (and our staff’s) perceptions of children with autism, ID, genetic syndromes that include NDD, or motor disabilities based on their behavioral presentation may not accurately recognize or accommodate their abilities or needs. Communication and environmental adjustments may need to be much more individualized to provide respectful care, comfort and even safety.
As an example, at this time 1 in 36 children have autism with or without ID. Defining features of autism include differences in social communication, repetitive or restrictive interests or behaviors, and hypersensitivity to the environment plus any coexisting conditions such as anxiety and hyperactivity. But most children with autism have completely age appropriate and typical physical appearance and their underlying condition may not even be known. The office setting, without special attention to the needs of a child with autism, may be frightening, loud, too bright, too crowded, fast paced, and confusing. The result of their sensitivities and difficulty communicating may lead to increased agitation, repetitive behaviors (sometimes called “stimming”), shrieking, attempts to escape the room, refusal to allow for vital signs or undressing, even aggression. Strategies for calming a neurotypical child such as talking or touching may make matters worse instead of better. We need help from the child and family and a plan to optimize their medical encounters.
If not adequately accommodated, children with many varieties of NDD end up not getting all the routine healthcare they need (eg vaccinations, blood tests, vital signs, even complete physical exams including dental) as well as having more adverse events during health care, including traumatizing seclusion, not allowing a support person to be present, restraint, injuries, and accidents. When more complex procedures are needed, eg x-ray, MRI, EEG, lab studies, or surgery, successful outcomes may be lower. Children with NDD have higher rates of often avoidable morbidity and mortality than those without, in part due to these barriers to complete care. While environmental accommodations to wheelchair users for accessibility has greatly improved in recent years, access to other kinds of individualized accommodations have lagged behind.
Accommodation Planning
There are a variety of factors that need to be taken into consideration in accommodating an individual with NDD. The family becomes the expert, along with the child, in knowing the child’s triggers, preferences, abilities, and level of understanding to accept and consent for care. An accommodation plan should be created using shared and supported decision making with the family and child and allowing for child preferences, regardless of their ability level, whenever possible. Development of an accommodation plan may benefit from multidisciplinary input, eg psychology, physical therapy, speech pathology, depending on the child’s needs and the practice’s ability to adapt.
The SAFE initiative is in the process of creating a checklist aiming to facilitate a description being created for each individual to help plan for a successful medical encounter while optimizing the child’s comfort, participation, and safety. While the checklist is not yet ready, we can start now by asking families and children in preparation for or at the start of a visit about their needs and writing a shared document that can also be placed in the electronic health record for the entire care team for informing care going forward.
It is especially important for the family to keep a copy of the care plan and for it to be sent as part of referrals for procedures or specialty visits so that the professionals can prepare and adapt the encounter. An excellent example is a how some hospitals schedule a practice visit for the child to experience the sights and sounds and people the child will encounter, for example, before an EEG, when nothing is required of the child. Scheduling the actual procedure at times of day when clinics are less crowded and wait times are shorter can improve the chances of success.
Some categories and details that might be included in an accommodation plan are listed below:
You might start the plan with the child’s preferred name/nickname, family member or support person names, and diagnoses along with a brief overview of the child’s level of functioning. Then list categories of needs and preferences along with suggestions or requests.
- Motor: Does the child have or need assistance entering the building, visit room, bathroom, or transferring to the exam table? What kind of assistance, if any, and by whom?
- Sensory: Is the child disturbed by noise, lights, or being touched? Does the child want to use equipment to be comfortable such as headphones, earplugs, or sunglasses or need a quiet room, care without perfumes, or dimmed lighting? Does the child typically refuse aspects of the physical examination?
- Behavioral regulation: What helps the child to stay calm? Are there certain triggers to becoming upset? Are there early cues that an upset is coming? What and who can help in the case of an upset?
- Habits/preferences: Are there certain comfort objects or habits your child needs? Are there habits your child needs to do, such as a certain order of events, or use of social stories or pictures, to cooperate or feel comfortable?
- Communication: How does the child make his/her needs known? Does the child/family speak English or another language? Does he/she use sign language or an augmentative communication device? What level of understanding does your child have; for example, similar to what age for a typical child? Is there a care plan with accommodations already available that needs review or needs revision with the child’s development or is a new one needed? Was the care plan developed including the child’s participation and assent or is more collaboration needed?
- History: Has your child had any very upsetting experiences in healthcare settings? What happened? Has the trauma been addressed? Are there reminders of the trauma that should be avoided?
- Other: Are there other things we should know about your child as an individual to provide the best care?
There are many actions needed to do better at ensuring equitable care for individuals with NDD. We should educate our office and medical staff about NDD in children and the importance of accommodating their needs, and ways to do it. The morning huddle can be used to remind staff of upcoming visits of children who may need accommodations. We then need to use quality improvement methods to check in periodically on how the changes are working for the children, families, and practice in order to continually improve.
The overall healthcare system also needs to change. Billing codes should reflect the time, complexity of accommodations, and documentation that were required for care. Episodes of the visit may need to be broken up within the day or over several days to allow the child to practice, calm down, and cooperate and this should be accounted for in billing. Given that NDD are generally lifelong conditions, payment systems that require measures of progress such as value-based payment based on improved outcomes will need to be adjusted to measure quality of care rather than significant progress.
We need to advocate for both individual children and for system changes to work toward equity of care for those with disabilities to make their lives more comfortable as well as ours.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Are Targeted Drugs the Future in Colorectal Cancer?
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.