User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
High and low HDL cholesterol levels linked to dementia risk
TOPLINE:
High and low levels of HDL cholesterol but not levels of LDL cholesterol are associated with an increased risk for dementia in older adults, a new study found.
METHODOLOGY:
- Electronic health record and survey data on 184,367 Kaiser Permanente Northern California participants (median age, 69.5 years) with no history of dementia were taken.
- Cholesterol levels were measured within 2 years of survey completion.
TAKEAWAY:
- There were 25,214 incident cases of dementia reported over an average follow-up of 8.77 years.
- Dementia risk was significantly higher in people with low HDL cholesterol (11-41 mg/dL; adjusted hazard ratio, 1.07; 95% confidence interval, 1.03-1.11) and high HDL cholesterol (> 65 mg/dL; aHR, 1.15; 95% CI, 1.11-1.20).
- The study demonstrates an association between low and high levels of “good” cholesterol but not a causal link.
- There was no significant association between LDL cholesterol and dementia risk.
IN PRACTICE:
“These results support the conclusion that some lipoproteins may be modifiable risk factors for dementia, even in late life,” the authors wrote.
SOURCE:
The study was conducted by Erin L. Ferguson, MPH, department of epidemiology & biostatistics, University of California, San Francisco, and was funded by the National Institutes of Health. It was published online in Neurology.
LIMITATIONS:
There were no adjustments for apo E status and confounding and selection bias.
DISCLOSURES:
The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
High and low levels of HDL cholesterol but not levels of LDL cholesterol are associated with an increased risk for dementia in older adults, a new study found.
METHODOLOGY:
- Electronic health record and survey data on 184,367 Kaiser Permanente Northern California participants (median age, 69.5 years) with no history of dementia were taken.
- Cholesterol levels were measured within 2 years of survey completion.
TAKEAWAY:
- There were 25,214 incident cases of dementia reported over an average follow-up of 8.77 years.
- Dementia risk was significantly higher in people with low HDL cholesterol (11-41 mg/dL; adjusted hazard ratio, 1.07; 95% confidence interval, 1.03-1.11) and high HDL cholesterol (> 65 mg/dL; aHR, 1.15; 95% CI, 1.11-1.20).
- The study demonstrates an association between low and high levels of “good” cholesterol but not a causal link.
- There was no significant association between LDL cholesterol and dementia risk.
IN PRACTICE:
“These results support the conclusion that some lipoproteins may be modifiable risk factors for dementia, even in late life,” the authors wrote.
SOURCE:
The study was conducted by Erin L. Ferguson, MPH, department of epidemiology & biostatistics, University of California, San Francisco, and was funded by the National Institutes of Health. It was published online in Neurology.
LIMITATIONS:
There were no adjustments for apo E status and confounding and selection bias.
DISCLOSURES:
The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
High and low levels of HDL cholesterol but not levels of LDL cholesterol are associated with an increased risk for dementia in older adults, a new study found.
METHODOLOGY:
- Electronic health record and survey data on 184,367 Kaiser Permanente Northern California participants (median age, 69.5 years) with no history of dementia were taken.
- Cholesterol levels were measured within 2 years of survey completion.
TAKEAWAY:
- There were 25,214 incident cases of dementia reported over an average follow-up of 8.77 years.
- Dementia risk was significantly higher in people with low HDL cholesterol (11-41 mg/dL; adjusted hazard ratio, 1.07; 95% confidence interval, 1.03-1.11) and high HDL cholesterol (> 65 mg/dL; aHR, 1.15; 95% CI, 1.11-1.20).
- The study demonstrates an association between low and high levels of “good” cholesterol but not a causal link.
- There was no significant association between LDL cholesterol and dementia risk.
IN PRACTICE:
“These results support the conclusion that some lipoproteins may be modifiable risk factors for dementia, even in late life,” the authors wrote.
SOURCE:
The study was conducted by Erin L. Ferguson, MPH, department of epidemiology & biostatistics, University of California, San Francisco, and was funded by the National Institutes of Health. It was published online in Neurology.
LIMITATIONS:
There were no adjustments for apo E status and confounding and selection bias.
DISCLOSURES:
The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
Hopeful insights, no overall HFpEF gains from splanchnic nerve ablation: REBALANCE-HF
It’s still early days for a potential transcatheter technique that tones down sympathetic activation mediating blood volume shifts to the heart and lungs. Such volume transfers can contribute to congestion and acute decompensation in some patients with heart failure. But a randomized trial with negative overall results still may have moved the novel procedure a modest step forward.
The procedure, right-sided splanchnic-nerve ablation for volume management (SAVM), failed to show significant effects on hemodynamics, exercise capacity, natriuretic peptides, or quality of life in a trial covering a broad population of patients with heart failure with preserved ejection fraction (HFpEF).
The study, called REBALANCE-HF, compared ablation of the right greater splanchnic nerve with a sham version of the procedure for any effects on hemodynamic or functional outcomes.
Among such “potential responders,” those undergoing SAVM trended better than patients receiving the sham procedure with respect to hemodynamic, functional, natriuretic peptide, and quality of life endpoints.
The potential predictors of SAVM success included elevated or preserved cardiac output and pulse pressure with exercise or on standing up; appropriate heart-rate exercise responses; and little or no echocardiographic evidence of diastolic dysfunction.
The panel of features might potentially identify patients more likely to respond to the procedure and perhaps sharpen entry criteria in future clinical trials, Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., said in an interview.
Dr. Fudim presented the REBALANCE-HF findings at the annual meeting of the Heart Failure Society of America.
How SAVM works
Sympathetic activation can lead to acute or chronic constriction of vessels in the splanchnic bed within the upper and lower abdomen, one of the body’s largest blood reservoirs, Dr. Fudim explained. Resulting volume shifts to the general circulation, and therefore the heart and lungs, are a normal exercise response that, in HF, can fall out of balance and excessively raise cardiac filling pressure.
Lessened sympathetic tone after unilateral GNS ablation can promote splanchnic venous dilation that reduces intrathoracic blood volume, potentially averting congestion, and decompensation, observed Kavita Sharma, MD, invited discussant for Dr. Fudim’s presentation.
The trial’s potential-responder cohort “seemed able to augment cardiac output in response to stress” and to “maintain or augment their orthostatic pulse pressure,” more effectively than the other participants, said Dr. Sharma, of Johns Hopkins University, Baltimore.
Although the trial was overall negative for 1-month change in pulmonary capillary wedge pressure (PCWP), the primary efficacy endpoint, Dr. Sharma said, it confirmed SAVM as a safe procedure in HFpEF and “ensured its replicability and technical success.”
Future studies should explore ways to characterize unlikely SAVM responders, she proposed. “I would argue these patients are probably more important than even the responders.”
Yet it’s unknown why, for example, cardiac output wouldn’t increase with exercise in a patient with HFpEF. “Is it related to preload insufficiency, right ventricular failure, atrial myopathy, perhaps more restrictive physiology, chronotropic incompetence, or medications – or a combination of the above?”
REBALANCE-HF assigned 90 patients with HFpEF to either the active or sham SAVM groups, 44 and 46 patients, respectively. To be eligible, patients were stable on HF meds and had either elevated natriuretic peptides or, within the past year, at least one HF hospitalization or escalation of intravenous diuretics for worsening HF.
The active and sham control groups fared similarly for the primary PCWP endpoint and for the secondary endpoints of Kansas City Cardiomyopathy Questionnaire (KCCQ) overall summary score, 6-minute walk distance (6MWD), and natriuretic peptide levels at 6 and 12 months.
Predicting SAVM response
In analysis limited to potential responders, PCWP, KCCQ, 6MWD, and natriuretic peptide outcomes for patients were combined into z scores, a single metric that reflects multiple outcomes, Dr. Fudim explained.
The z scores were derived for tertiles of patients in subgroups defined by a range of parameters that included demographics, medical history, and hemodynamic and echocardiographic variables.
Four such variables were found to interact across tertiles in a way that suggested their value as SAVM outcome predictors and were then used to select the cohort of potential responders. The variables were exertion-related changes in cardiac index, pulse pressure, and heart rate, and mitral E/A ratio – the latter a measure of diastolic dysfunction.
Among potential responders, those who underwent SAVM showed a 2.9–mm Hg steeper drop in peak PCWP at 1 month (P = .02), compared with patients getting the sham procedure.
They also bested control patients at both 6 and 12 months for KCCQ score, 6MWD, and natriuretic peptide levels, the latter of which fell in the SAVM group and climbed in control patients at both follow-ups.
“Hypothetically, it makes sense” to target the splanchnic nerve in HFpEF, and indeed in HF with reduced ejection fraction, Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, said in an interview.
And should SAVM enter the mainstream, it would definitely be important to identify “the right” patients for such an invasive procedure, those likely to show “efficacy with a good safety margin,” said Dr. Bozkurt, who was not associated with REBALANCE-HF.
But the trial, she said, “unfortunately did not give real signals of outcome benefit.”
REBALANCE-HF was supported by Axon Therapies. Dr. Fudim disclosed consulting, receiving royalties, or having ownership or equity in Axon Therapies. Dr. Sharma disclosed receiving honoraria for speaking from Novartis and Janssen and serving on an advisory board or consulting for Novartis, Janssen, and Bayer. Dr. Bozkurt disclosed receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion.
A version of this article first appeared on Medscape.com.
It’s still early days for a potential transcatheter technique that tones down sympathetic activation mediating blood volume shifts to the heart and lungs. Such volume transfers can contribute to congestion and acute decompensation in some patients with heart failure. But a randomized trial with negative overall results still may have moved the novel procedure a modest step forward.
The procedure, right-sided splanchnic-nerve ablation for volume management (SAVM), failed to show significant effects on hemodynamics, exercise capacity, natriuretic peptides, or quality of life in a trial covering a broad population of patients with heart failure with preserved ejection fraction (HFpEF).
The study, called REBALANCE-HF, compared ablation of the right greater splanchnic nerve with a sham version of the procedure for any effects on hemodynamic or functional outcomes.
Among such “potential responders,” those undergoing SAVM trended better than patients receiving the sham procedure with respect to hemodynamic, functional, natriuretic peptide, and quality of life endpoints.
The potential predictors of SAVM success included elevated or preserved cardiac output and pulse pressure with exercise or on standing up; appropriate heart-rate exercise responses; and little or no echocardiographic evidence of diastolic dysfunction.
The panel of features might potentially identify patients more likely to respond to the procedure and perhaps sharpen entry criteria in future clinical trials, Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., said in an interview.
Dr. Fudim presented the REBALANCE-HF findings at the annual meeting of the Heart Failure Society of America.
How SAVM works
Sympathetic activation can lead to acute or chronic constriction of vessels in the splanchnic bed within the upper and lower abdomen, one of the body’s largest blood reservoirs, Dr. Fudim explained. Resulting volume shifts to the general circulation, and therefore the heart and lungs, are a normal exercise response that, in HF, can fall out of balance and excessively raise cardiac filling pressure.
Lessened sympathetic tone after unilateral GNS ablation can promote splanchnic venous dilation that reduces intrathoracic blood volume, potentially averting congestion, and decompensation, observed Kavita Sharma, MD, invited discussant for Dr. Fudim’s presentation.
The trial’s potential-responder cohort “seemed able to augment cardiac output in response to stress” and to “maintain or augment their orthostatic pulse pressure,” more effectively than the other participants, said Dr. Sharma, of Johns Hopkins University, Baltimore.
Although the trial was overall negative for 1-month change in pulmonary capillary wedge pressure (PCWP), the primary efficacy endpoint, Dr. Sharma said, it confirmed SAVM as a safe procedure in HFpEF and “ensured its replicability and technical success.”
Future studies should explore ways to characterize unlikely SAVM responders, she proposed. “I would argue these patients are probably more important than even the responders.”
Yet it’s unknown why, for example, cardiac output wouldn’t increase with exercise in a patient with HFpEF. “Is it related to preload insufficiency, right ventricular failure, atrial myopathy, perhaps more restrictive physiology, chronotropic incompetence, or medications – or a combination of the above?”
REBALANCE-HF assigned 90 patients with HFpEF to either the active or sham SAVM groups, 44 and 46 patients, respectively. To be eligible, patients were stable on HF meds and had either elevated natriuretic peptides or, within the past year, at least one HF hospitalization or escalation of intravenous diuretics for worsening HF.
The active and sham control groups fared similarly for the primary PCWP endpoint and for the secondary endpoints of Kansas City Cardiomyopathy Questionnaire (KCCQ) overall summary score, 6-minute walk distance (6MWD), and natriuretic peptide levels at 6 and 12 months.
Predicting SAVM response
In analysis limited to potential responders, PCWP, KCCQ, 6MWD, and natriuretic peptide outcomes for patients were combined into z scores, a single metric that reflects multiple outcomes, Dr. Fudim explained.
The z scores were derived for tertiles of patients in subgroups defined by a range of parameters that included demographics, medical history, and hemodynamic and echocardiographic variables.
Four such variables were found to interact across tertiles in a way that suggested their value as SAVM outcome predictors and were then used to select the cohort of potential responders. The variables were exertion-related changes in cardiac index, pulse pressure, and heart rate, and mitral E/A ratio – the latter a measure of diastolic dysfunction.
Among potential responders, those who underwent SAVM showed a 2.9–mm Hg steeper drop in peak PCWP at 1 month (P = .02), compared with patients getting the sham procedure.
They also bested control patients at both 6 and 12 months for KCCQ score, 6MWD, and natriuretic peptide levels, the latter of which fell in the SAVM group and climbed in control patients at both follow-ups.
“Hypothetically, it makes sense” to target the splanchnic nerve in HFpEF, and indeed in HF with reduced ejection fraction, Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, said in an interview.
And should SAVM enter the mainstream, it would definitely be important to identify “the right” patients for such an invasive procedure, those likely to show “efficacy with a good safety margin,” said Dr. Bozkurt, who was not associated with REBALANCE-HF.
But the trial, she said, “unfortunately did not give real signals of outcome benefit.”
REBALANCE-HF was supported by Axon Therapies. Dr. Fudim disclosed consulting, receiving royalties, or having ownership or equity in Axon Therapies. Dr. Sharma disclosed receiving honoraria for speaking from Novartis and Janssen and serving on an advisory board or consulting for Novartis, Janssen, and Bayer. Dr. Bozkurt disclosed receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion.
A version of this article first appeared on Medscape.com.
It’s still early days for a potential transcatheter technique that tones down sympathetic activation mediating blood volume shifts to the heart and lungs. Such volume transfers can contribute to congestion and acute decompensation in some patients with heart failure. But a randomized trial with negative overall results still may have moved the novel procedure a modest step forward.
The procedure, right-sided splanchnic-nerve ablation for volume management (SAVM), failed to show significant effects on hemodynamics, exercise capacity, natriuretic peptides, or quality of life in a trial covering a broad population of patients with heart failure with preserved ejection fraction (HFpEF).
The study, called REBALANCE-HF, compared ablation of the right greater splanchnic nerve with a sham version of the procedure for any effects on hemodynamic or functional outcomes.
Among such “potential responders,” those undergoing SAVM trended better than patients receiving the sham procedure with respect to hemodynamic, functional, natriuretic peptide, and quality of life endpoints.
The potential predictors of SAVM success included elevated or preserved cardiac output and pulse pressure with exercise or on standing up; appropriate heart-rate exercise responses; and little or no echocardiographic evidence of diastolic dysfunction.
The panel of features might potentially identify patients more likely to respond to the procedure and perhaps sharpen entry criteria in future clinical trials, Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., said in an interview.
Dr. Fudim presented the REBALANCE-HF findings at the annual meeting of the Heart Failure Society of America.
How SAVM works
Sympathetic activation can lead to acute or chronic constriction of vessels in the splanchnic bed within the upper and lower abdomen, one of the body’s largest blood reservoirs, Dr. Fudim explained. Resulting volume shifts to the general circulation, and therefore the heart and lungs, are a normal exercise response that, in HF, can fall out of balance and excessively raise cardiac filling pressure.
Lessened sympathetic tone after unilateral GNS ablation can promote splanchnic venous dilation that reduces intrathoracic blood volume, potentially averting congestion, and decompensation, observed Kavita Sharma, MD, invited discussant for Dr. Fudim’s presentation.
The trial’s potential-responder cohort “seemed able to augment cardiac output in response to stress” and to “maintain or augment their orthostatic pulse pressure,” more effectively than the other participants, said Dr. Sharma, of Johns Hopkins University, Baltimore.
Although the trial was overall negative for 1-month change in pulmonary capillary wedge pressure (PCWP), the primary efficacy endpoint, Dr. Sharma said, it confirmed SAVM as a safe procedure in HFpEF and “ensured its replicability and technical success.”
Future studies should explore ways to characterize unlikely SAVM responders, she proposed. “I would argue these patients are probably more important than even the responders.”
Yet it’s unknown why, for example, cardiac output wouldn’t increase with exercise in a patient with HFpEF. “Is it related to preload insufficiency, right ventricular failure, atrial myopathy, perhaps more restrictive physiology, chronotropic incompetence, or medications – or a combination of the above?”
REBALANCE-HF assigned 90 patients with HFpEF to either the active or sham SAVM groups, 44 and 46 patients, respectively. To be eligible, patients were stable on HF meds and had either elevated natriuretic peptides or, within the past year, at least one HF hospitalization or escalation of intravenous diuretics for worsening HF.
The active and sham control groups fared similarly for the primary PCWP endpoint and for the secondary endpoints of Kansas City Cardiomyopathy Questionnaire (KCCQ) overall summary score, 6-minute walk distance (6MWD), and natriuretic peptide levels at 6 and 12 months.
Predicting SAVM response
In analysis limited to potential responders, PCWP, KCCQ, 6MWD, and natriuretic peptide outcomes for patients were combined into z scores, a single metric that reflects multiple outcomes, Dr. Fudim explained.
The z scores were derived for tertiles of patients in subgroups defined by a range of parameters that included demographics, medical history, and hemodynamic and echocardiographic variables.
Four such variables were found to interact across tertiles in a way that suggested their value as SAVM outcome predictors and were then used to select the cohort of potential responders. The variables were exertion-related changes in cardiac index, pulse pressure, and heart rate, and mitral E/A ratio – the latter a measure of diastolic dysfunction.
Among potential responders, those who underwent SAVM showed a 2.9–mm Hg steeper drop in peak PCWP at 1 month (P = .02), compared with patients getting the sham procedure.
They also bested control patients at both 6 and 12 months for KCCQ score, 6MWD, and natriuretic peptide levels, the latter of which fell in the SAVM group and climbed in control patients at both follow-ups.
“Hypothetically, it makes sense” to target the splanchnic nerve in HFpEF, and indeed in HF with reduced ejection fraction, Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, said in an interview.
And should SAVM enter the mainstream, it would definitely be important to identify “the right” patients for such an invasive procedure, those likely to show “efficacy with a good safety margin,” said Dr. Bozkurt, who was not associated with REBALANCE-HF.
But the trial, she said, “unfortunately did not give real signals of outcome benefit.”
REBALANCE-HF was supported by Axon Therapies. Dr. Fudim disclosed consulting, receiving royalties, or having ownership or equity in Axon Therapies. Dr. Sharma disclosed receiving honoraria for speaking from Novartis and Janssen and serving on an advisory board or consulting for Novartis, Janssen, and Bayer. Dr. Bozkurt disclosed receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion.
A version of this article first appeared on Medscape.com.
FROM HFSA 2023
Pragmatic solutions to ‘catastrophic’ global stroke burden
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
FROM THE LANCET NEUROLOGY
Alert! A decade of type 2 diabetes shortens life by 3.5 years
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.
Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.
Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.
Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET – DIABETES AND ENDOCRINOLOGY
FDA denies approval for patisiran in ATTR cardiomyopathy, despite panel nod
the company has announced.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.

In September, the FDA Cardiovascular and Renal Drugs Advisory Committee voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy on the basis of the results of the APOLLO-B phase 3 study.
However, many panel members questioned whether the benefits are clinically meaningful – a view shared by the FDA in a complete response letter (CRL) the FDA sent to Alnylam.
According to the company, the FDA indicated in the letter that the clinical meaningfulness of patisiran’s treatment effects for the cardiomyopathy of ATTR amyloidosis have “not been established,” and therefore, the supplemental new drug application for patisiran “could not be approved in its present form.”
The FDA did not identify any issues with respect to clinical safety, study conduct, drug quality, or manufacturing.
Nonetheless, as a result of the CRL, the company said it will no longer pursue an expanded indication for patisiran in cardiomyopathy of ATTR amyloidosis in the United States.
The company said it will continue to make patisiran available for patients with cardiomyopathy of ATTR amyloidosis who are enrolled in the open-label extension period of the APOLLO-B study and the patisiran expanded access protocol.
The company also said it will continue to focus on the HELIOS-B phase 3 study of vutrisiran, an investigational RNAi therapeutic in development for the treatment of cardiomyopathy of ATTR amyloidosis.
“We remain confident in the HELIOS-B phase 3 study of vutrisiran and look forward to sharing topline results in early 2024. If successful, we believe vutrisiran will offer convenient, quarterly subcutaneous dosing with a therapeutic profile that may potentially include cardiovascular outcome benefits,” Alnylam CEO Yvonne Greenstreet, MBChB, said in the statement.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of polyneuropathy of hereditary ATTR amyloidosis in adults.
A version of this article first appeared on Medscape.com.
the company has announced.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.
In September, the FDA Cardiovascular and Renal Drugs Advisory Committee voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy on the basis of the results of the APOLLO-B phase 3 study.
However, many panel members questioned whether the benefits are clinically meaningful – a view shared by the FDA in a complete response letter (CRL) the FDA sent to Alnylam.
According to the company, the FDA indicated in the letter that the clinical meaningfulness of patisiran’s treatment effects for the cardiomyopathy of ATTR amyloidosis have “not been established,” and therefore, the supplemental new drug application for patisiran “could not be approved in its present form.”
The FDA did not identify any issues with respect to clinical safety, study conduct, drug quality, or manufacturing.
Nonetheless, as a result of the CRL, the company said it will no longer pursue an expanded indication for patisiran in cardiomyopathy of ATTR amyloidosis in the United States.
The company said it will continue to make patisiran available for patients with cardiomyopathy of ATTR amyloidosis who are enrolled in the open-label extension period of the APOLLO-B study and the patisiran expanded access protocol.
The company also said it will continue to focus on the HELIOS-B phase 3 study of vutrisiran, an investigational RNAi therapeutic in development for the treatment of cardiomyopathy of ATTR amyloidosis.
“We remain confident in the HELIOS-B phase 3 study of vutrisiran and look forward to sharing topline results in early 2024. If successful, we believe vutrisiran will offer convenient, quarterly subcutaneous dosing with a therapeutic profile that may potentially include cardiovascular outcome benefits,” Alnylam CEO Yvonne Greenstreet, MBChB, said in the statement.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of polyneuropathy of hereditary ATTR amyloidosis in adults.
A version of this article first appeared on Medscape.com.
the company has announced.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.
In September, the FDA Cardiovascular and Renal Drugs Advisory Committee voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy on the basis of the results of the APOLLO-B phase 3 study.
However, many panel members questioned whether the benefits are clinically meaningful – a view shared by the FDA in a complete response letter (CRL) the FDA sent to Alnylam.
According to the company, the FDA indicated in the letter that the clinical meaningfulness of patisiran’s treatment effects for the cardiomyopathy of ATTR amyloidosis have “not been established,” and therefore, the supplemental new drug application for patisiran “could not be approved in its present form.”
The FDA did not identify any issues with respect to clinical safety, study conduct, drug quality, or manufacturing.
Nonetheless, as a result of the CRL, the company said it will no longer pursue an expanded indication for patisiran in cardiomyopathy of ATTR amyloidosis in the United States.
The company said it will continue to make patisiran available for patients with cardiomyopathy of ATTR amyloidosis who are enrolled in the open-label extension period of the APOLLO-B study and the patisiran expanded access protocol.
The company also said it will continue to focus on the HELIOS-B phase 3 study of vutrisiran, an investigational RNAi therapeutic in development for the treatment of cardiomyopathy of ATTR amyloidosis.
“We remain confident in the HELIOS-B phase 3 study of vutrisiran and look forward to sharing topline results in early 2024. If successful, we believe vutrisiran will offer convenient, quarterly subcutaneous dosing with a therapeutic profile that may potentially include cardiovascular outcome benefits,” Alnylam CEO Yvonne Greenstreet, MBChB, said in the statement.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of polyneuropathy of hereditary ATTR amyloidosis in adults.
A version of this article first appeared on Medscape.com.
Redefining CVD risk: Cardiovascular-kidney-metabolic (CKM) syndrome
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Every click you make, the EHR is watching you
This transcript has been edited for clarity.
When I close my eyes and imagine what it is I do for a living, I see a computer screen.
I’m primarily a clinical researcher, so much of what I do is looking at statistical software, or, more recently, writing grant applications. But even when I think of my clinical duties, I see that computer screen.
The reason? The electronic health record (EHR) – the hot, beating heart of medical care in the modern era. Our most powerful tool and our greatest enemy.
The EHR records everything – not just the vital signs and lab values of our patients, not just our notes and billing codes. Everything. Every interaction we have is tracked and can be analyzed. The EHR is basically Sting in the song “Every Breath You Take.” Every click you make, it is watching you.
Researchers are leveraging that panopticon to give insight into something we don’t talk about frequently: the issue of racial bias in medicine. Is our true nature revealed by our interactions with the EHR?
We’re talking about this study in JAMA Network Open.
Researchers leveraged huge amounts of EHR data from two big academic medical centers, Vanderbilt University Medical Center and Northwestern University Medical Center. All told, there are data from nearly 250,000 hospitalizations here.
The researchers created a metric for EHR engagement. Basically, they summed the amount of clicks and other EHR interactions that occurred during the hospitalization, divided by the length of stay in days, to create a sort of average “engagement per day” metric. This number was categorized into four groups: low engagement, medium engagement, high engagement, and very high engagement.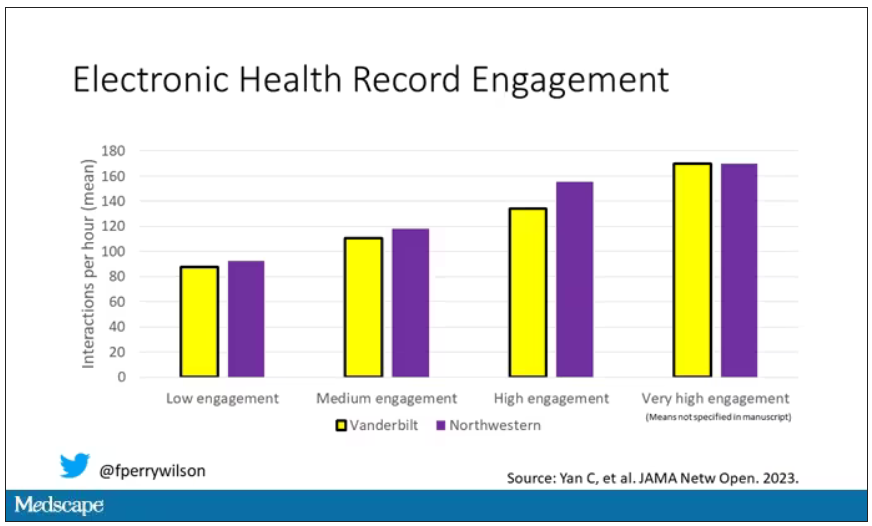
What factors would predict higher engagement? Well, , except among Black patients who actually got a bit more engagement.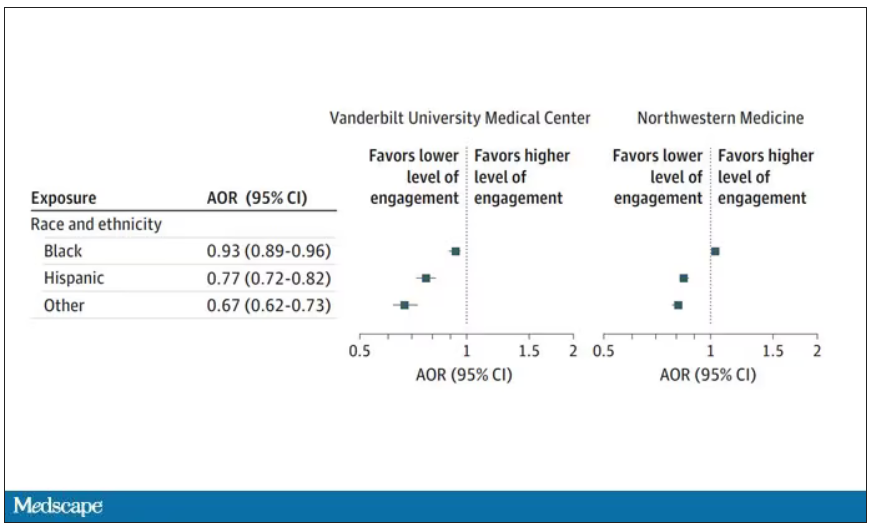
So, right away we need to be concerned about the obvious implications. Less engagement with the EHR may mean lower-quality care, right? Less attention to medical issues. And if that differs systematically by race, that’s a problem.
But we need to be careful here, because engagement in the health record is not random. Many factors would lead you to spend more time in one patient’s chart vs. another. Medical complexity is the most obvious one. The authors did their best to account for this, adjusting for patients’ age, sex, insurance status, comorbidity score, and social deprivation index based on their ZIP code. But notably, they did not account for the acuity of illness during the hospitalization. If individuals identifying as a minority were, all else being equal, less likely to be severely ill by the time they were hospitalized, you might see results like this.
The authors also restrict their analysis to individuals who were discharged alive. I’m not entirely clear why they made this choice. Most people don’t die in the hospital; the inpatient mortality rate at most centers is 1%-1.5%. But excluding those patients could potentially bias these results, especially if race is, all else being equal, a predictor of inpatient mortality, as some studies have shown.
But the truth is, these data aren’t coming out of nowhere; they don’t exist in a vacuum. Numerous studies demonstrate different intensity of care among minority vs. nonminority individuals. There is this study, which shows that minority populations are less likely to be placed on the liver transplant waitlist.
There is this study, which found that minority kids with type 1 diabetes were less likely to get insulin pumps than were their White counterparts. And this one, which showed that kids with acute appendicitis were less likely to get pain-control medications if they were Black.
This study shows that although life expectancy decreased across all races during the pandemic, it decreased the most among minority populations.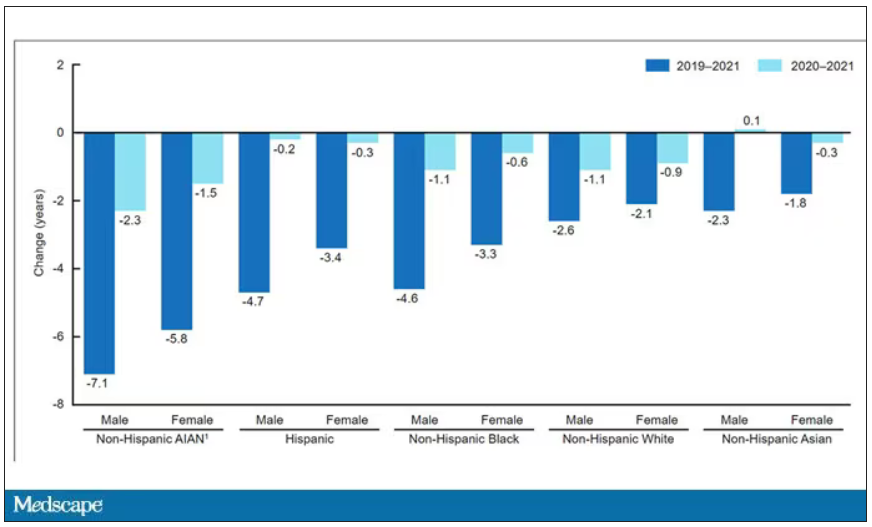
This list goes on. It’s why the CDC has called racism a “fundamental cause of ... disease.”
So, yes, it is clear that there are racial disparities in health care outcomes. It is clear that there are racial disparities in treatments. It is also clear that virtually every physician believes they deliver equitable care. Somewhere, this disconnect arises. Could the actions we take in the EHR reveal the unconscious biases we have? Does the all-seeing eye of the EHR see not only into our brains but into our hearts? And if it can, are we ready to confront what it sees?
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When I close my eyes and imagine what it is I do for a living, I see a computer screen.
I’m primarily a clinical researcher, so much of what I do is looking at statistical software, or, more recently, writing grant applications. But even when I think of my clinical duties, I see that computer screen.
The reason? The electronic health record (EHR) – the hot, beating heart of medical care in the modern era. Our most powerful tool and our greatest enemy.
The EHR records everything – not just the vital signs and lab values of our patients, not just our notes and billing codes. Everything. Every interaction we have is tracked and can be analyzed. The EHR is basically Sting in the song “Every Breath You Take.” Every click you make, it is watching you.
Researchers are leveraging that panopticon to give insight into something we don’t talk about frequently: the issue of racial bias in medicine. Is our true nature revealed by our interactions with the EHR?
We’re talking about this study in JAMA Network Open.
Researchers leveraged huge amounts of EHR data from two big academic medical centers, Vanderbilt University Medical Center and Northwestern University Medical Center. All told, there are data from nearly 250,000 hospitalizations here.
The researchers created a metric for EHR engagement. Basically, they summed the amount of clicks and other EHR interactions that occurred during the hospitalization, divided by the length of stay in days, to create a sort of average “engagement per day” metric. This number was categorized into four groups: low engagement, medium engagement, high engagement, and very high engagement.
What factors would predict higher engagement? Well, , except among Black patients who actually got a bit more engagement.
So, right away we need to be concerned about the obvious implications. Less engagement with the EHR may mean lower-quality care, right? Less attention to medical issues. And if that differs systematically by race, that’s a problem.
But we need to be careful here, because engagement in the health record is not random. Many factors would lead you to spend more time in one patient’s chart vs. another. Medical complexity is the most obvious one. The authors did their best to account for this, adjusting for patients’ age, sex, insurance status, comorbidity score, and social deprivation index based on their ZIP code. But notably, they did not account for the acuity of illness during the hospitalization. If individuals identifying as a minority were, all else being equal, less likely to be severely ill by the time they were hospitalized, you might see results like this.
The authors also restrict their analysis to individuals who were discharged alive. I’m not entirely clear why they made this choice. Most people don’t die in the hospital; the inpatient mortality rate at most centers is 1%-1.5%. But excluding those patients could potentially bias these results, especially if race is, all else being equal, a predictor of inpatient mortality, as some studies have shown.
But the truth is, these data aren’t coming out of nowhere; they don’t exist in a vacuum. Numerous studies demonstrate different intensity of care among minority vs. nonminority individuals. There is this study, which shows that minority populations are less likely to be placed on the liver transplant waitlist.
There is this study, which found that minority kids with type 1 diabetes were less likely to get insulin pumps than were their White counterparts. And this one, which showed that kids with acute appendicitis were less likely to get pain-control medications if they were Black.
This study shows that although life expectancy decreased across all races during the pandemic, it decreased the most among minority populations.
This list goes on. It’s why the CDC has called racism a “fundamental cause of ... disease.”
So, yes, it is clear that there are racial disparities in health care outcomes. It is clear that there are racial disparities in treatments. It is also clear that virtually every physician believes they deliver equitable care. Somewhere, this disconnect arises. Could the actions we take in the EHR reveal the unconscious biases we have? Does the all-seeing eye of the EHR see not only into our brains but into our hearts? And if it can, are we ready to confront what it sees?
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When I close my eyes and imagine what it is I do for a living, I see a computer screen.
I’m primarily a clinical researcher, so much of what I do is looking at statistical software, or, more recently, writing grant applications. But even when I think of my clinical duties, I see that computer screen.
The reason? The electronic health record (EHR) – the hot, beating heart of medical care in the modern era. Our most powerful tool and our greatest enemy.
The EHR records everything – not just the vital signs and lab values of our patients, not just our notes and billing codes. Everything. Every interaction we have is tracked and can be analyzed. The EHR is basically Sting in the song “Every Breath You Take.” Every click you make, it is watching you.
Researchers are leveraging that panopticon to give insight into something we don’t talk about frequently: the issue of racial bias in medicine. Is our true nature revealed by our interactions with the EHR?
We’re talking about this study in JAMA Network Open.
Researchers leveraged huge amounts of EHR data from two big academic medical centers, Vanderbilt University Medical Center and Northwestern University Medical Center. All told, there are data from nearly 250,000 hospitalizations here.
The researchers created a metric for EHR engagement. Basically, they summed the amount of clicks and other EHR interactions that occurred during the hospitalization, divided by the length of stay in days, to create a sort of average “engagement per day” metric. This number was categorized into four groups: low engagement, medium engagement, high engagement, and very high engagement.
What factors would predict higher engagement? Well, , except among Black patients who actually got a bit more engagement.
So, right away we need to be concerned about the obvious implications. Less engagement with the EHR may mean lower-quality care, right? Less attention to medical issues. And if that differs systematically by race, that’s a problem.
But we need to be careful here, because engagement in the health record is not random. Many factors would lead you to spend more time in one patient’s chart vs. another. Medical complexity is the most obvious one. The authors did their best to account for this, adjusting for patients’ age, sex, insurance status, comorbidity score, and social deprivation index based on their ZIP code. But notably, they did not account for the acuity of illness during the hospitalization. If individuals identifying as a minority were, all else being equal, less likely to be severely ill by the time they were hospitalized, you might see results like this.
The authors also restrict their analysis to individuals who were discharged alive. I’m not entirely clear why they made this choice. Most people don’t die in the hospital; the inpatient mortality rate at most centers is 1%-1.5%. But excluding those patients could potentially bias these results, especially if race is, all else being equal, a predictor of inpatient mortality, as some studies have shown.
But the truth is, these data aren’t coming out of nowhere; they don’t exist in a vacuum. Numerous studies demonstrate different intensity of care among minority vs. nonminority individuals. There is this study, which shows that minority populations are less likely to be placed on the liver transplant waitlist.
There is this study, which found that minority kids with type 1 diabetes were less likely to get insulin pumps than were their White counterparts. And this one, which showed that kids with acute appendicitis were less likely to get pain-control medications if they were Black.
This study shows that although life expectancy decreased across all races during the pandemic, it decreased the most among minority populations.
This list goes on. It’s why the CDC has called racism a “fundamental cause of ... disease.”
So, yes, it is clear that there are racial disparities in health care outcomes. It is clear that there are racial disparities in treatments. It is also clear that virtually every physician believes they deliver equitable care. Somewhere, this disconnect arises. Could the actions we take in the EHR reveal the unconscious biases we have? Does the all-seeing eye of the EHR see not only into our brains but into our hearts? And if it can, are we ready to confront what it sees?
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Spreading out daily meals and snacks may boost heart failure survival
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT HFSA 2023
Don’t fear POTS: Tips for diagnosis and treatment
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
Supplemental oxygen fails to improve echocardiographic measures in PE patients
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
FROM THE JOURNAL CHEST