User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Is your job performance being evaluated for the wrong factors?
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Would you be happier in a leadership position? This hospitalist wasn’t
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.

So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.

“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.
So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.
“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.
So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.
“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
WHO plans to address airborne COVID-19 transmission
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
Goals of care conferences for incapacitated ICU patients
Background: Previous studies suggest that clinicians and surrogates rarely discuss patient values in ICU family conferences about goals of care despite recommendations from international critical care societies.
Study design: Analysis of audiotaped goals of care conferences.
Setting: ICUs in six U.S. academic centers.
Synopsis: The authors analyzed 249 audiotaped family conferences concerning goals of care for severely critically ill, incapacitated patients with acute respiratory distress syndrome and found that information about patient values and preferences was discussed in only 68.4% of the conferences.
Moreover, there was no deliberation about how to apply patient values and preferences to clinical decisions in 55.7% of the conferences. Surrogates were more likely to bring up these elements of shared decision making than were physicians.
Bottom line: Care providers and surrogates of critically ill ICU patients often fail to discuss patient preferences, values, and how they apply to care decisions in goals of care conferences.
Citation: Scheunemann LP et al. Clinician-family communication about patients’ values and preferences in intensive care units. JAMA Intern Med. 2019;179(5):676-84.
Dr. Mastalerz is a hospitalist and medical director of 9A Accountable Care Unit at the Colorado Health Foundation.
Background: Previous studies suggest that clinicians and surrogates rarely discuss patient values in ICU family conferences about goals of care despite recommendations from international critical care societies.
Study design: Analysis of audiotaped goals of care conferences.
Setting: ICUs in six U.S. academic centers.
Synopsis: The authors analyzed 249 audiotaped family conferences concerning goals of care for severely critically ill, incapacitated patients with acute respiratory distress syndrome and found that information about patient values and preferences was discussed in only 68.4% of the conferences.
Moreover, there was no deliberation about how to apply patient values and preferences to clinical decisions in 55.7% of the conferences. Surrogates were more likely to bring up these elements of shared decision making than were physicians.
Bottom line: Care providers and surrogates of critically ill ICU patients often fail to discuss patient preferences, values, and how they apply to care decisions in goals of care conferences.
Citation: Scheunemann LP et al. Clinician-family communication about patients’ values and preferences in intensive care units. JAMA Intern Med. 2019;179(5):676-84.
Dr. Mastalerz is a hospitalist and medical director of 9A Accountable Care Unit at the Colorado Health Foundation.
Background: Previous studies suggest that clinicians and surrogates rarely discuss patient values in ICU family conferences about goals of care despite recommendations from international critical care societies.
Study design: Analysis of audiotaped goals of care conferences.
Setting: ICUs in six U.S. academic centers.
Synopsis: The authors analyzed 249 audiotaped family conferences concerning goals of care for severely critically ill, incapacitated patients with acute respiratory distress syndrome and found that information about patient values and preferences was discussed in only 68.4% of the conferences.
Moreover, there was no deliberation about how to apply patient values and preferences to clinical decisions in 55.7% of the conferences. Surrogates were more likely to bring up these elements of shared decision making than were physicians.
Bottom line: Care providers and surrogates of critically ill ICU patients often fail to discuss patient preferences, values, and how they apply to care decisions in goals of care conferences.
Citation: Scheunemann LP et al. Clinician-family communication about patients’ values and preferences in intensive care units. JAMA Intern Med. 2019;179(5):676-84.
Dr. Mastalerz is a hospitalist and medical director of 9A Accountable Care Unit at the Colorado Health Foundation.
Use of nonopioid pain meds is on the rise
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
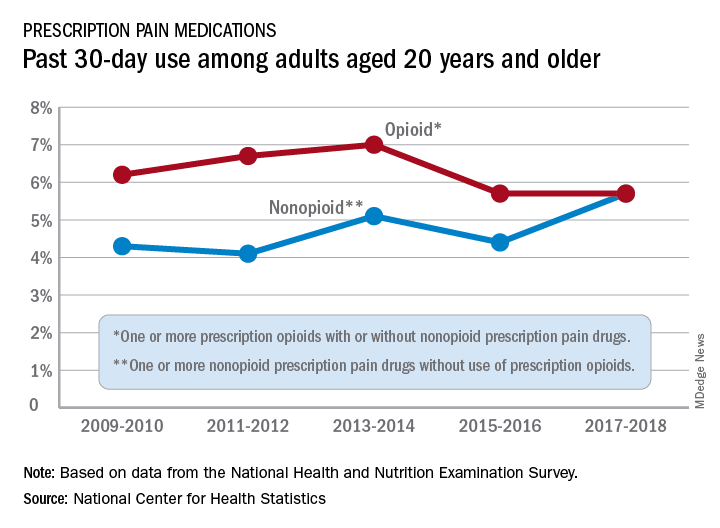
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
HIV does not appear to worsen COVID-19 outcomes
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
FROM AIDS 2020
Higher stroke rates seen among patients with COVID-19 compared with influenza
, according to a retrospective cohort study conducted at New York–Presbyterian Hospital and Weill Cornell Medicine, New York. “These findings suggest that clinicians should be vigilant for symptoms and signs of acute ischemic stroke in patients with COVID-19 so that time-sensitive interventions, such as thrombolysis and thrombectomy, can be instituted if possible to reduce the burden of long-term disability,” wrote Alexander E. Merkler and colleagues. Their report is in JAMA Neurology.
While several recent publications have “raised the possibility” of this link, none have had an appropriate control group, noted Dr. Merkler of the department of neurology, Weill Cornell Medicine. “Further elucidation of thrombotic mechanisms in patients with COVID-19 may yield better strategies to prevent disabling thrombotic complications like ischemic stroke,” he added.
An increased risk of stroke
The study included 1,916 adults with confirmed COVID-19 (median age 64 years) who were either hospitalized or visited an emergency department between March 4 and May 2, 2020. These cases were compared with a historical cohort of 1,486 patients (median age 62 years) who were hospitalized with laboratory-confirmed influenza A or B between January 1, 2016, and May 31, 2018.
Among the patients with COVID-19, a diagnosis of cerebrovascular disease during hospitalization, a brain computed tomography (CT), or brain magnetic resonance imaging (MRI) was an indication of possible ischemic stroke. These records were then independently reviewed by two board-certified attending neurologists (with a third resolving any disagreement) to adjudicate a final stroke diagnosis. In the influenza cohort, the Cornell Acute Stroke Academic Registry (CAESAR) was used to ascertain ischemic strokes.
The study identified 31 patients with stroke among the COVID-19 cohort (1.6%; 95% confidence interval, 1.1%-2.3%) and 3 in the influenza cohort (0.2%; 95% CI, 0.0%-0.6%). After adjustment for age, sex, and race, stroke risk was almost 8 times higher in the COVID-19 cohort (OR, 7.6; 95% CI, 2.3-25.2).
This association “persisted across multiple sensitivity analyses, with the magnitude of relative associations ranging from 4.0 to 9,” wrote the authors. “This included a sensitivity analysis that adjusted for the number of vascular risk factors and ICU admissions (OR, 4.6; 95% CI, 1.4-15.7).”
The median age of patients with COVID-19 and stroke was 69 years, and the median duration of COVID-19 symptom onset to stroke diagnosis was 16 days. Stroke symptoms were the presenting complaint in only 26% of the patients, while the remainder developing stroke while hospitalized, and more than a third (35%) of all strokes occurred in patients who were mechanically ventilated with severe COVID-19. Inpatient mortality was considerably higher among patients with COVID-19 with stroke versus without (32% vs. 14%; P = .003).
In patients with COVID-19 “most ischemic strokes occurred in older age groups, those with traditional stroke risk factors, and people of color,” wrote the authors. “We also noted that initial plasma D-dimer levels were nearly 3-fold higher in those who received a diagnosis of ischemic stroke than in those who did not” (1.930 mcg/mL vs. 0.682 mcg/mL).
The authors suggested several possible explanations for the elevated risk of stroke in COVID-19. Acute viral illnesses are known to trigger inflammation, and COVID-19 in particular is associated with “a vigorous inflammatory response accompanied by coagulopathy, with elevated D-dimer levels and the frequent presence of antiphospholipid antibodies,” they wrote. The infection is also associated with more severe respiratory syndrome compared with influenza, as well as a heightened risk for complications such as atrial arrhythmias, myocardial infarction, heart failure, myocarditis, and venous thromboses, all of which likely contribute to the risk of ischemic stroke.”
COVID or conventional risk factors?
Asked to comment on the study, Benedict Michael, MBChB (Hons), MRCP (Neurol), PhD, from the United Kingdom’s Coronerve Studies Group, a collaborative initiative to study the neurological features of COVID-19, said in an interview that “this study suggests many cases of stroke are occurring in older patients with multiple existing conventional and well recognized risks for stroke, and may simply represent decompensation during sepsis.”
Dr. Michael, a senior clinician scientist fellow at the University of Liverpool and an honorary consultant neurologist at the Walton Centre, was the senior author on a recently published UK-wide surveillance study on the neurological and neuropsychiatric complications of COVID-19 (Lancet Psychiatry. 2020 Jun 25. doi: 10.1016/S2215-0366[20]30287-X).
He said among patients in the New York study, “those with COVID and a stroke appeared to have many conventional risk factors for stroke (and often at higher percentages than COVID patients without a stroke), e.g. hypertension, overweight, diabetes, hyperlipidemia, existing vascular disease affecting the coronary arteries and atrial fibrillation. To establish evidence-based treatment pathways, clearly further studies are needed to determine the biological mechanisms underlying the seemingly higher rate of stroke with COVID-19 than influenza; but this must especially focus on those younger patients without conventional risk factors for stroke (which are largely not included in this study).”
SOURCE: Merkler AE et al. JAMA Neurol. doi: 10.1001/jamaneurol.2020.2730.
, according to a retrospective cohort study conducted at New York–Presbyterian Hospital and Weill Cornell Medicine, New York. “These findings suggest that clinicians should be vigilant for symptoms and signs of acute ischemic stroke in patients with COVID-19 so that time-sensitive interventions, such as thrombolysis and thrombectomy, can be instituted if possible to reduce the burden of long-term disability,” wrote Alexander E. Merkler and colleagues. Their report is in JAMA Neurology.
While several recent publications have “raised the possibility” of this link, none have had an appropriate control group, noted Dr. Merkler of the department of neurology, Weill Cornell Medicine. “Further elucidation of thrombotic mechanisms in patients with COVID-19 may yield better strategies to prevent disabling thrombotic complications like ischemic stroke,” he added.
An increased risk of stroke
The study included 1,916 adults with confirmed COVID-19 (median age 64 years) who were either hospitalized or visited an emergency department between March 4 and May 2, 2020. These cases were compared with a historical cohort of 1,486 patients (median age 62 years) who were hospitalized with laboratory-confirmed influenza A or B between January 1, 2016, and May 31, 2018.
Among the patients with COVID-19, a diagnosis of cerebrovascular disease during hospitalization, a brain computed tomography (CT), or brain magnetic resonance imaging (MRI) was an indication of possible ischemic stroke. These records were then independently reviewed by two board-certified attending neurologists (with a third resolving any disagreement) to adjudicate a final stroke diagnosis. In the influenza cohort, the Cornell Acute Stroke Academic Registry (CAESAR) was used to ascertain ischemic strokes.
The study identified 31 patients with stroke among the COVID-19 cohort (1.6%; 95% confidence interval, 1.1%-2.3%) and 3 in the influenza cohort (0.2%; 95% CI, 0.0%-0.6%). After adjustment for age, sex, and race, stroke risk was almost 8 times higher in the COVID-19 cohort (OR, 7.6; 95% CI, 2.3-25.2).
This association “persisted across multiple sensitivity analyses, with the magnitude of relative associations ranging from 4.0 to 9,” wrote the authors. “This included a sensitivity analysis that adjusted for the number of vascular risk factors and ICU admissions (OR, 4.6; 95% CI, 1.4-15.7).”
The median age of patients with COVID-19 and stroke was 69 years, and the median duration of COVID-19 symptom onset to stroke diagnosis was 16 days. Stroke symptoms were the presenting complaint in only 26% of the patients, while the remainder developing stroke while hospitalized, and more than a third (35%) of all strokes occurred in patients who were mechanically ventilated with severe COVID-19. Inpatient mortality was considerably higher among patients with COVID-19 with stroke versus without (32% vs. 14%; P = .003).
In patients with COVID-19 “most ischemic strokes occurred in older age groups, those with traditional stroke risk factors, and people of color,” wrote the authors. “We also noted that initial plasma D-dimer levels were nearly 3-fold higher in those who received a diagnosis of ischemic stroke than in those who did not” (1.930 mcg/mL vs. 0.682 mcg/mL).
The authors suggested several possible explanations for the elevated risk of stroke in COVID-19. Acute viral illnesses are known to trigger inflammation, and COVID-19 in particular is associated with “a vigorous inflammatory response accompanied by coagulopathy, with elevated D-dimer levels and the frequent presence of antiphospholipid antibodies,” they wrote. The infection is also associated with more severe respiratory syndrome compared with influenza, as well as a heightened risk for complications such as atrial arrhythmias, myocardial infarction, heart failure, myocarditis, and venous thromboses, all of which likely contribute to the risk of ischemic stroke.”
COVID or conventional risk factors?
Asked to comment on the study, Benedict Michael, MBChB (Hons), MRCP (Neurol), PhD, from the United Kingdom’s Coronerve Studies Group, a collaborative initiative to study the neurological features of COVID-19, said in an interview that “this study suggests many cases of stroke are occurring in older patients with multiple existing conventional and well recognized risks for stroke, and may simply represent decompensation during sepsis.”
Dr. Michael, a senior clinician scientist fellow at the University of Liverpool and an honorary consultant neurologist at the Walton Centre, was the senior author on a recently published UK-wide surveillance study on the neurological and neuropsychiatric complications of COVID-19 (Lancet Psychiatry. 2020 Jun 25. doi: 10.1016/S2215-0366[20]30287-X).
He said among patients in the New York study, “those with COVID and a stroke appeared to have many conventional risk factors for stroke (and often at higher percentages than COVID patients without a stroke), e.g. hypertension, overweight, diabetes, hyperlipidemia, existing vascular disease affecting the coronary arteries and atrial fibrillation. To establish evidence-based treatment pathways, clearly further studies are needed to determine the biological mechanisms underlying the seemingly higher rate of stroke with COVID-19 than influenza; but this must especially focus on those younger patients without conventional risk factors for stroke (which are largely not included in this study).”
SOURCE: Merkler AE et al. JAMA Neurol. doi: 10.1001/jamaneurol.2020.2730.
, according to a retrospective cohort study conducted at New York–Presbyterian Hospital and Weill Cornell Medicine, New York. “These findings suggest that clinicians should be vigilant for symptoms and signs of acute ischemic stroke in patients with COVID-19 so that time-sensitive interventions, such as thrombolysis and thrombectomy, can be instituted if possible to reduce the burden of long-term disability,” wrote Alexander E. Merkler and colleagues. Their report is in JAMA Neurology.
While several recent publications have “raised the possibility” of this link, none have had an appropriate control group, noted Dr. Merkler of the department of neurology, Weill Cornell Medicine. “Further elucidation of thrombotic mechanisms in patients with COVID-19 may yield better strategies to prevent disabling thrombotic complications like ischemic stroke,” he added.
An increased risk of stroke
The study included 1,916 adults with confirmed COVID-19 (median age 64 years) who were either hospitalized or visited an emergency department between March 4 and May 2, 2020. These cases were compared with a historical cohort of 1,486 patients (median age 62 years) who were hospitalized with laboratory-confirmed influenza A or B between January 1, 2016, and May 31, 2018.
Among the patients with COVID-19, a diagnosis of cerebrovascular disease during hospitalization, a brain computed tomography (CT), or brain magnetic resonance imaging (MRI) was an indication of possible ischemic stroke. These records were then independently reviewed by two board-certified attending neurologists (with a third resolving any disagreement) to adjudicate a final stroke diagnosis. In the influenza cohort, the Cornell Acute Stroke Academic Registry (CAESAR) was used to ascertain ischemic strokes.
The study identified 31 patients with stroke among the COVID-19 cohort (1.6%; 95% confidence interval, 1.1%-2.3%) and 3 in the influenza cohort (0.2%; 95% CI, 0.0%-0.6%). After adjustment for age, sex, and race, stroke risk was almost 8 times higher in the COVID-19 cohort (OR, 7.6; 95% CI, 2.3-25.2).
This association “persisted across multiple sensitivity analyses, with the magnitude of relative associations ranging from 4.0 to 9,” wrote the authors. “This included a sensitivity analysis that adjusted for the number of vascular risk factors and ICU admissions (OR, 4.6; 95% CI, 1.4-15.7).”
The median age of patients with COVID-19 and stroke was 69 years, and the median duration of COVID-19 symptom onset to stroke diagnosis was 16 days. Stroke symptoms were the presenting complaint in only 26% of the patients, while the remainder developing stroke while hospitalized, and more than a third (35%) of all strokes occurred in patients who were mechanically ventilated with severe COVID-19. Inpatient mortality was considerably higher among patients with COVID-19 with stroke versus without (32% vs. 14%; P = .003).
In patients with COVID-19 “most ischemic strokes occurred in older age groups, those with traditional stroke risk factors, and people of color,” wrote the authors. “We also noted that initial plasma D-dimer levels were nearly 3-fold higher in those who received a diagnosis of ischemic stroke than in those who did not” (1.930 mcg/mL vs. 0.682 mcg/mL).
The authors suggested several possible explanations for the elevated risk of stroke in COVID-19. Acute viral illnesses are known to trigger inflammation, and COVID-19 in particular is associated with “a vigorous inflammatory response accompanied by coagulopathy, with elevated D-dimer levels and the frequent presence of antiphospholipid antibodies,” they wrote. The infection is also associated with more severe respiratory syndrome compared with influenza, as well as a heightened risk for complications such as atrial arrhythmias, myocardial infarction, heart failure, myocarditis, and venous thromboses, all of which likely contribute to the risk of ischemic stroke.”
COVID or conventional risk factors?
Asked to comment on the study, Benedict Michael, MBChB (Hons), MRCP (Neurol), PhD, from the United Kingdom’s Coronerve Studies Group, a collaborative initiative to study the neurological features of COVID-19, said in an interview that “this study suggests many cases of stroke are occurring in older patients with multiple existing conventional and well recognized risks for stroke, and may simply represent decompensation during sepsis.”
Dr. Michael, a senior clinician scientist fellow at the University of Liverpool and an honorary consultant neurologist at the Walton Centre, was the senior author on a recently published UK-wide surveillance study on the neurological and neuropsychiatric complications of COVID-19 (Lancet Psychiatry. 2020 Jun 25. doi: 10.1016/S2215-0366[20]30287-X).
He said among patients in the New York study, “those with COVID and a stroke appeared to have many conventional risk factors for stroke (and often at higher percentages than COVID patients without a stroke), e.g. hypertension, overweight, diabetes, hyperlipidemia, existing vascular disease affecting the coronary arteries and atrial fibrillation. To establish evidence-based treatment pathways, clearly further studies are needed to determine the biological mechanisms underlying the seemingly higher rate of stroke with COVID-19 than influenza; but this must especially focus on those younger patients without conventional risk factors for stroke (which are largely not included in this study).”
SOURCE: Merkler AE et al. JAMA Neurol. doi: 10.1001/jamaneurol.2020.2730.
FROM JAMA NEUROLOGY
Anticoagulation in cirrhosis: Best practices
Background: Alterations to the coagulation cascade put cirrhotic patients at higher risk for bleeding and thrombotic complications.

Study design: Expert review.
Setting: Literature review.
Synopsis: The authors provide 12 best practice recommendations, including use blood products sparingly in the absence of active bleeding out of concern for raising portal pressures; low-risk paracentesis, thoracentesis, and upper endoscopy do not require routine correction of thrombocytopenia or coagulopathy; for active bleeding or high-risk procedures, correct hematocrit to above 25%, platelets to more than 50,000, and fibrinogen to above 120 mg/dL; the risk of thrombosis, including venous thromboembolism and portal vein thrombosis, is high in these patients despite elevated INR values.
As such, pharmacologic VTE prophylaxis is often underutilized in patients admitted with cirrhosis; for patients requiring therapeutic anticoagulation, direct oral anticoagulants are safe in stable patients with mild cirrhosis, but should be avoided in Child-Pugh B and C patients.
Bottom line: Cirrhotic patients do not require routine correction of coagulopathy prior to low-risk procedures.
Citation: O’Leary JG et al. AGA Clinical Practice Update: Coagulation in cirrhosis. Gastroenterology. 2019. doi: 10.1053/j.gastro.2019.03.070.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.
Background: Alterations to the coagulation cascade put cirrhotic patients at higher risk for bleeding and thrombotic complications.
Study design: Expert review.
Setting: Literature review.
Synopsis: The authors provide 12 best practice recommendations, including use blood products sparingly in the absence of active bleeding out of concern for raising portal pressures; low-risk paracentesis, thoracentesis, and upper endoscopy do not require routine correction of thrombocytopenia or coagulopathy; for active bleeding or high-risk procedures, correct hematocrit to above 25%, platelets to more than 50,000, and fibrinogen to above 120 mg/dL; the risk of thrombosis, including venous thromboembolism and portal vein thrombosis, is high in these patients despite elevated INR values.
As such, pharmacologic VTE prophylaxis is often underutilized in patients admitted with cirrhosis; for patients requiring therapeutic anticoagulation, direct oral anticoagulants are safe in stable patients with mild cirrhosis, but should be avoided in Child-Pugh B and C patients.
Bottom line: Cirrhotic patients do not require routine correction of coagulopathy prior to low-risk procedures.
Citation: O’Leary JG et al. AGA Clinical Practice Update: Coagulation in cirrhosis. Gastroenterology. 2019. doi: 10.1053/j.gastro.2019.03.070.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.
Background: Alterations to the coagulation cascade put cirrhotic patients at higher risk for bleeding and thrombotic complications.
Study design: Expert review.
Setting: Literature review.
Synopsis: The authors provide 12 best practice recommendations, including use blood products sparingly in the absence of active bleeding out of concern for raising portal pressures; low-risk paracentesis, thoracentesis, and upper endoscopy do not require routine correction of thrombocytopenia or coagulopathy; for active bleeding or high-risk procedures, correct hematocrit to above 25%, platelets to more than 50,000, and fibrinogen to above 120 mg/dL; the risk of thrombosis, including venous thromboembolism and portal vein thrombosis, is high in these patients despite elevated INR values.
As such, pharmacologic VTE prophylaxis is often underutilized in patients admitted with cirrhosis; for patients requiring therapeutic anticoagulation, direct oral anticoagulants are safe in stable patients with mild cirrhosis, but should be avoided in Child-Pugh B and C patients.
Bottom line: Cirrhotic patients do not require routine correction of coagulopathy prior to low-risk procedures.
Citation: O’Leary JG et al. AGA Clinical Practice Update: Coagulation in cirrhosis. Gastroenterology. 2019. doi: 10.1053/j.gastro.2019.03.070.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.
Dr. Eric E. Howell assumes new role as CEO of SHM
The Society of Hospital Medicine officially welcomed Eric E. Howell, MD, MHM, as chief executive officer on July 1, 2020. Dr. Howell reports to the Society of Hospital Medicine board of directors and is tasked with ensuring that SHM continues to serve the evolving needs and interests of its members while overseeing the organization’s strategic direction.

“The SHM board of directors is excited to work with Dr. Howell to navigate the future of SHM and of the hospital medicine specialty,” said Danielle Scheurer, MD, MSCR, SFHM, SHM president and chair of the CEO Search Committee. “With his extensive knowledge of the health care landscape and of SHM, Dr. Howell embodies the society’s dedication to empowering hospitalists to be positive change agents in their institutions and in the health care system as a whole.”
Prior to his current role, Dr. Howell served as chief operating officer of SHM for 2 years; in that role, he led senior management’s planning and defined organizational goals to drive growth. As the senior physician adviser to SHM’s Center for Quality Improvement for 5 years, he consulted for the society’s arm that conducts quality improvement programs for hospitalist teams. In addition to being a past president of SHM’s board of directors, he is the course director for the SHM Leadership Academies.
“Now more than ever, SHM has an opportunity to superserve hospitalists and the patients they serve, and I couldn’t be more excited to lead the society into its next chapter,” Dr. Howell said. “Supported by a dedicated member base and innovative staff, I am confident that SHM will continue on its successful path forward and will provide its members with the products, services, and tools that hospitalists need to improve patient care and adapt to the constantly evolving environment.”
In addition to serving in various capacities at SHM, Dr. Howell has served as a professor of medicine in the department of medicine at Johns Hopkins University, Baltimore. He has held multiple titles within the Johns Hopkins medical institutions, including chief of the division of hospital medicine at Johns Hopkins Bayview, section chief of hospital medicine for Johns Hopkins Community Physicians, deputy director of hospital operations for the department of medicine at Johns Hopkins Bayview Medical Center, and chief medical officer of operations at Johns Hopkins Bayview. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and oversaw nearly 200 physicians and clinical staff providing patient care in three hospitals. Along with his role as SHM CEO, he will remain a member of the adjunct faculty at Johns Hopkins University.
More recently, Dr. Howell served as chief medical officer for the Baltimore Convention Center Field Hospital, a fully functional, 250-bed hospital created to care for patients in the Baltimore metropolitan area who were suffering from complications from COVID-19.
Dr. Howell received his electrical engineering degree from the University of Maryland, College Park, which has proven instrumental in his mastery of managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput and patient outcomes.
The nationwide search process that led to Dr. Howell’s appointment was led by a CEO Search Committee, which included members of the SHM board of directors and was assisted by the executive search firm Spencer Stuart.
Dr. Howell succeeds Laurence Wellikson, MD, MHM, who helped in founding the Society of Hospital Medicine, its first and only CEO since 2000 prior to Dr. Howell’s appointment.
The Society of Hospital Medicine officially welcomed Eric E. Howell, MD, MHM, as chief executive officer on July 1, 2020. Dr. Howell reports to the Society of Hospital Medicine board of directors and is tasked with ensuring that SHM continues to serve the evolving needs and interests of its members while overseeing the organization’s strategic direction.
“The SHM board of directors is excited to work with Dr. Howell to navigate the future of SHM and of the hospital medicine specialty,” said Danielle Scheurer, MD, MSCR, SFHM, SHM president and chair of the CEO Search Committee. “With his extensive knowledge of the health care landscape and of SHM, Dr. Howell embodies the society’s dedication to empowering hospitalists to be positive change agents in their institutions and in the health care system as a whole.”
Prior to his current role, Dr. Howell served as chief operating officer of SHM for 2 years; in that role, he led senior management’s planning and defined organizational goals to drive growth. As the senior physician adviser to SHM’s Center for Quality Improvement for 5 years, he consulted for the society’s arm that conducts quality improvement programs for hospitalist teams. In addition to being a past president of SHM’s board of directors, he is the course director for the SHM Leadership Academies.
“Now more than ever, SHM has an opportunity to superserve hospitalists and the patients they serve, and I couldn’t be more excited to lead the society into its next chapter,” Dr. Howell said. “Supported by a dedicated member base and innovative staff, I am confident that SHM will continue on its successful path forward and will provide its members with the products, services, and tools that hospitalists need to improve patient care and adapt to the constantly evolving environment.”
In addition to serving in various capacities at SHM, Dr. Howell has served as a professor of medicine in the department of medicine at Johns Hopkins University, Baltimore. He has held multiple titles within the Johns Hopkins medical institutions, including chief of the division of hospital medicine at Johns Hopkins Bayview, section chief of hospital medicine for Johns Hopkins Community Physicians, deputy director of hospital operations for the department of medicine at Johns Hopkins Bayview Medical Center, and chief medical officer of operations at Johns Hopkins Bayview. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and oversaw nearly 200 physicians and clinical staff providing patient care in three hospitals. Along with his role as SHM CEO, he will remain a member of the adjunct faculty at Johns Hopkins University.
More recently, Dr. Howell served as chief medical officer for the Baltimore Convention Center Field Hospital, a fully functional, 250-bed hospital created to care for patients in the Baltimore metropolitan area who were suffering from complications from COVID-19.
Dr. Howell received his electrical engineering degree from the University of Maryland, College Park, which has proven instrumental in his mastery of managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput and patient outcomes.
The nationwide search process that led to Dr. Howell’s appointment was led by a CEO Search Committee, which included members of the SHM board of directors and was assisted by the executive search firm Spencer Stuart.
Dr. Howell succeeds Laurence Wellikson, MD, MHM, who helped in founding the Society of Hospital Medicine, its first and only CEO since 2000 prior to Dr. Howell’s appointment.
The Society of Hospital Medicine officially welcomed Eric E. Howell, MD, MHM, as chief executive officer on July 1, 2020. Dr. Howell reports to the Society of Hospital Medicine board of directors and is tasked with ensuring that SHM continues to serve the evolving needs and interests of its members while overseeing the organization’s strategic direction.
“The SHM board of directors is excited to work with Dr. Howell to navigate the future of SHM and of the hospital medicine specialty,” said Danielle Scheurer, MD, MSCR, SFHM, SHM president and chair of the CEO Search Committee. “With his extensive knowledge of the health care landscape and of SHM, Dr. Howell embodies the society’s dedication to empowering hospitalists to be positive change agents in their institutions and in the health care system as a whole.”
Prior to his current role, Dr. Howell served as chief operating officer of SHM for 2 years; in that role, he led senior management’s planning and defined organizational goals to drive growth. As the senior physician adviser to SHM’s Center for Quality Improvement for 5 years, he consulted for the society’s arm that conducts quality improvement programs for hospitalist teams. In addition to being a past president of SHM’s board of directors, he is the course director for the SHM Leadership Academies.
“Now more than ever, SHM has an opportunity to superserve hospitalists and the patients they serve, and I couldn’t be more excited to lead the society into its next chapter,” Dr. Howell said. “Supported by a dedicated member base and innovative staff, I am confident that SHM will continue on its successful path forward and will provide its members with the products, services, and tools that hospitalists need to improve patient care and adapt to the constantly evolving environment.”
In addition to serving in various capacities at SHM, Dr. Howell has served as a professor of medicine in the department of medicine at Johns Hopkins University, Baltimore. He has held multiple titles within the Johns Hopkins medical institutions, including chief of the division of hospital medicine at Johns Hopkins Bayview, section chief of hospital medicine for Johns Hopkins Community Physicians, deputy director of hospital operations for the department of medicine at Johns Hopkins Bayview Medical Center, and chief medical officer of operations at Johns Hopkins Bayview. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and oversaw nearly 200 physicians and clinical staff providing patient care in three hospitals. Along with his role as SHM CEO, he will remain a member of the adjunct faculty at Johns Hopkins University.
More recently, Dr. Howell served as chief medical officer for the Baltimore Convention Center Field Hospital, a fully functional, 250-bed hospital created to care for patients in the Baltimore metropolitan area who were suffering from complications from COVID-19.
Dr. Howell received his electrical engineering degree from the University of Maryland, College Park, which has proven instrumental in his mastery of managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput and patient outcomes.
The nationwide search process that led to Dr. Howell’s appointment was led by a CEO Search Committee, which included members of the SHM board of directors and was assisted by the executive search firm Spencer Stuart.
Dr. Howell succeeds Laurence Wellikson, MD, MHM, who helped in founding the Society of Hospital Medicine, its first and only CEO since 2000 prior to Dr. Howell’s appointment.
One-year mortality after dialysis initiation nearly double prior estimates
Background: The United States Renal Data System registry estimates that approximately 30% of patients die within 1 year of initiating hemodialysis.
Study design: Retrospective, observational analysis.
Setting: The Health and Retirement Study is a nationally representative survey of Medicare beneficiaries during 1998-2014. Medicare claims were linked to mortality data from the National Death Index.
Synopsis: Among 391 patients who initiated dialysis, 22.5%, 44.2%, and 54.5% died within 30 days, 6 months, and 1 year, respectively. After multivariate adjustment, 1-year mortality was higher among those who initiated dialysis while inpatients (hazard ratio, 2.17; 62.2%), had any activity of daily living dependence prior to dialysis (HR, 1.88; 73.0%), or had more than four comorbidities (HR, 1.5; 59.9%).
Bottom line: Medicare beneficiaries may have significantly higher mortality after initiating dialysis than prior data suggest.
Citation: Wachterman MW et al. One-year mortality after dialysis initiation among older adults. JAMA Intern Med. 2019 Apr 22. doi: 10.1001/jamainternmed.2019.0125.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.
Background: The United States Renal Data System registry estimates that approximately 30% of patients die within 1 year of initiating hemodialysis.
Study design: Retrospective, observational analysis.
Setting: The Health and Retirement Study is a nationally representative survey of Medicare beneficiaries during 1998-2014. Medicare claims were linked to mortality data from the National Death Index.
Synopsis: Among 391 patients who initiated dialysis, 22.5%, 44.2%, and 54.5% died within 30 days, 6 months, and 1 year, respectively. After multivariate adjustment, 1-year mortality was higher among those who initiated dialysis while inpatients (hazard ratio, 2.17; 62.2%), had any activity of daily living dependence prior to dialysis (HR, 1.88; 73.0%), or had more than four comorbidities (HR, 1.5; 59.9%).
Bottom line: Medicare beneficiaries may have significantly higher mortality after initiating dialysis than prior data suggest.
Citation: Wachterman MW et al. One-year mortality after dialysis initiation among older adults. JAMA Intern Med. 2019 Apr 22. doi: 10.1001/jamainternmed.2019.0125.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.
Background: The United States Renal Data System registry estimates that approximately 30% of patients die within 1 year of initiating hemodialysis.
Study design: Retrospective, observational analysis.
Setting: The Health and Retirement Study is a nationally representative survey of Medicare beneficiaries during 1998-2014. Medicare claims were linked to mortality data from the National Death Index.
Synopsis: Among 391 patients who initiated dialysis, 22.5%, 44.2%, and 54.5% died within 30 days, 6 months, and 1 year, respectively. After multivariate adjustment, 1-year mortality was higher among those who initiated dialysis while inpatients (hazard ratio, 2.17; 62.2%), had any activity of daily living dependence prior to dialysis (HR, 1.88; 73.0%), or had more than four comorbidities (HR, 1.5; 59.9%).
Bottom line: Medicare beneficiaries may have significantly higher mortality after initiating dialysis than prior data suggest.
Citation: Wachterman MW et al. One-year mortality after dialysis initiation among older adults. JAMA Intern Med. 2019 Apr 22. doi: 10.1001/jamainternmed.2019.0125.
Dr. Lublin is a hospitalist at the University of Colorado at Denver, Aurora.