User login
Increased variability in A1c and FPG is a risk factor for severe hypoglycemia
Key clinical point: In patients with type 2 diabetes (T2D), increased visit-to-visit variability in glycated hemoglobin (A1c) and fasting plasma glucose (FPG) was associated with a higher risk for severe hypoglycemia; however, FPG variability better predicted severe hypoglycemic events than A1c variability.
Major finding: Each standard deviation (SD) increase in the variability in A1c and FPG significantly increased the risk for hypoglycemia requiring any third-party assistance (adjusted hazard ratio [aHR] 1.10 and aHR 1.40, respectively; both P < .01) and hypoglycemia requiring medical assistance (aHR 1.11 and aHR 1.46, respectively; both P < .01). However, FPG variability better predicted severe hypoglycemic events than A1c variability (P < .01).
Study details: Findings are from a post hoc analysis of the ACCORD trial including patients with T2D and a high risk for cardiovascular disease, of which 10,052 and 10,068 patients were included in A1c and FPG variability analyses, respectively.
Disclosures: This study was partly supported by the National Science Foundation of China project. The authors declared no conflicts of interest.
Source: Long C et al. Association of long-term visit-to-visit variability of HbA1c and fasting glycemia with hypoglycemia in type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2022;13:975468 (Aug 11). Doi: 10.3389/fendo.2022.975468
Key clinical point: In patients with type 2 diabetes (T2D), increased visit-to-visit variability in glycated hemoglobin (A1c) and fasting plasma glucose (FPG) was associated with a higher risk for severe hypoglycemia; however, FPG variability better predicted severe hypoglycemic events than A1c variability.
Major finding: Each standard deviation (SD) increase in the variability in A1c and FPG significantly increased the risk for hypoglycemia requiring any third-party assistance (adjusted hazard ratio [aHR] 1.10 and aHR 1.40, respectively; both P < .01) and hypoglycemia requiring medical assistance (aHR 1.11 and aHR 1.46, respectively; both P < .01). However, FPG variability better predicted severe hypoglycemic events than A1c variability (P < .01).
Study details: Findings are from a post hoc analysis of the ACCORD trial including patients with T2D and a high risk for cardiovascular disease, of which 10,052 and 10,068 patients were included in A1c and FPG variability analyses, respectively.
Disclosures: This study was partly supported by the National Science Foundation of China project. The authors declared no conflicts of interest.
Source: Long C et al. Association of long-term visit-to-visit variability of HbA1c and fasting glycemia with hypoglycemia in type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2022;13:975468 (Aug 11). Doi: 10.3389/fendo.2022.975468
Key clinical point: In patients with type 2 diabetes (T2D), increased visit-to-visit variability in glycated hemoglobin (A1c) and fasting plasma glucose (FPG) was associated with a higher risk for severe hypoglycemia; however, FPG variability better predicted severe hypoglycemic events than A1c variability.
Major finding: Each standard deviation (SD) increase in the variability in A1c and FPG significantly increased the risk for hypoglycemia requiring any third-party assistance (adjusted hazard ratio [aHR] 1.10 and aHR 1.40, respectively; both P < .01) and hypoglycemia requiring medical assistance (aHR 1.11 and aHR 1.46, respectively; both P < .01). However, FPG variability better predicted severe hypoglycemic events than A1c variability (P < .01).
Study details: Findings are from a post hoc analysis of the ACCORD trial including patients with T2D and a high risk for cardiovascular disease, of which 10,052 and 10,068 patients were included in A1c and FPG variability analyses, respectively.
Disclosures: This study was partly supported by the National Science Foundation of China project. The authors declared no conflicts of interest.
Source: Long C et al. Association of long-term visit-to-visit variability of HbA1c and fasting glycemia with hypoglycemia in type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2022;13:975468 (Aug 11). Doi: 10.3389/fendo.2022.975468
SGLT2i vs DPP4i tied with reduced mortality and HF readmission risk in T2D patients with HF
Key clinical point: Sodium-glucose cotransporter-2 inhibitor (SGLT2i) vs dipeptidyl peptidase-4 inhibitor (DPP4i) use at discharge was associated with a lower risk for 1-year all-cause mortality and heart failure (HF) readmission in hospitalized patients with HF and type 2 diabetes (T2D) in a superaged society.
Major finding: Overall, 71.91% of patients were ≥75 years old. SGLT2i vs DPP4i significantly reduced the risk for 1-year all-cause mortality (adjusted hazard ratio [aHR] 0.70; 95% CI 0.56-0.89) and HF readmission (aHRk 0.52; 95% CI 0.45-0.61), with findings being similar among very elderly patients (age, ≥75 years).
Study details: Findings are from a retrospective study including patients hospitalized with the first episode of acute HF and T2D, of which 2101 patients with T2D receiving SGLT2i were propensity score-matched with 2101 of those receiving DPP4i.
Disclosures: This work was supported by Labor Research Grants from the Ministry of Health, Labour, and Welfare of Japan. The authors declared no conflicts of interest.
Source: Nakai M et al. Contemporary use of SGLT2 inhibitors in heart failure patients with diabetes mellitus: A comparison of DPP4 inhibitors in a nationwide electric health database of the superaged society. Cardiovasc Diabetol. 2022;21:157 (Aug 13). Doi: 10.1186/s12933-022-01586-6
Key clinical point: Sodium-glucose cotransporter-2 inhibitor (SGLT2i) vs dipeptidyl peptidase-4 inhibitor (DPP4i) use at discharge was associated with a lower risk for 1-year all-cause mortality and heart failure (HF) readmission in hospitalized patients with HF and type 2 diabetes (T2D) in a superaged society.
Major finding: Overall, 71.91% of patients were ≥75 years old. SGLT2i vs DPP4i significantly reduced the risk for 1-year all-cause mortality (adjusted hazard ratio [aHR] 0.70; 95% CI 0.56-0.89) and HF readmission (aHRk 0.52; 95% CI 0.45-0.61), with findings being similar among very elderly patients (age, ≥75 years).
Study details: Findings are from a retrospective study including patients hospitalized with the first episode of acute HF and T2D, of which 2101 patients with T2D receiving SGLT2i were propensity score-matched with 2101 of those receiving DPP4i.
Disclosures: This work was supported by Labor Research Grants from the Ministry of Health, Labour, and Welfare of Japan. The authors declared no conflicts of interest.
Source: Nakai M et al. Contemporary use of SGLT2 inhibitors in heart failure patients with diabetes mellitus: A comparison of DPP4 inhibitors in a nationwide electric health database of the superaged society. Cardiovasc Diabetol. 2022;21:157 (Aug 13). Doi: 10.1186/s12933-022-01586-6
Key clinical point: Sodium-glucose cotransporter-2 inhibitor (SGLT2i) vs dipeptidyl peptidase-4 inhibitor (DPP4i) use at discharge was associated with a lower risk for 1-year all-cause mortality and heart failure (HF) readmission in hospitalized patients with HF and type 2 diabetes (T2D) in a superaged society.
Major finding: Overall, 71.91% of patients were ≥75 years old. SGLT2i vs DPP4i significantly reduced the risk for 1-year all-cause mortality (adjusted hazard ratio [aHR] 0.70; 95% CI 0.56-0.89) and HF readmission (aHRk 0.52; 95% CI 0.45-0.61), with findings being similar among very elderly patients (age, ≥75 years).
Study details: Findings are from a retrospective study including patients hospitalized with the first episode of acute HF and T2D, of which 2101 patients with T2D receiving SGLT2i were propensity score-matched with 2101 of those receiving DPP4i.
Disclosures: This work was supported by Labor Research Grants from the Ministry of Health, Labour, and Welfare of Japan. The authors declared no conflicts of interest.
Source: Nakai M et al. Contemporary use of SGLT2 inhibitors in heart failure patients with diabetes mellitus: A comparison of DPP4 inhibitors in a nationwide electric health database of the superaged society. Cardiovasc Diabetol. 2022;21:157 (Aug 13). Doi: 10.1186/s12933-022-01586-6
Effect of DPP4 inhibitors on glycemic variability in T2D
Key clinical point: Dipeptidyl peptidase-4 (DPP4) inhibitors were more effective than other oral antidiabetic drugs (OAD) in reducing glycemic variability in patients with type 2 diabetes (T2D) receiving no concurrent insulin treatment.
Major finding: The mean amplitude of glycemic excursions reduced significantly in patients receiving DPP4 inhibitors vs other OAD (mean difference [MD] −0.69 mmol/L; P < .001), insulin secretagogues (MD −0.92 mmol/L; P < .001), non-secretagogues (MD −0.43 mmol/L; P = .02), sulfonylureas (MD −0.91 mmol/L; P < .001), and sodium-glucose cotransporter-2 inhibitors (MD −0.67 mmol/L; P = .03).
Study details: The data come from a meta-analysis of 14 randomized controlled trials including 855 patients with T2D.
Disclosures: This study was funded by MSD China Holding Co. Ltd. Four authors declared being employees of MSD China, and one author declared being an employee of Merck Sharp & Dohme LLC.
Source: Chai S et al. Influence of dipeptidyl peptidase-4 inhibitors on glycemic variability in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Front Endocrinol (Lausanne). 2022;13:935039 (Aug 9). Doi: 10.3389/fendo.2022.935039
Key clinical point: Dipeptidyl peptidase-4 (DPP4) inhibitors were more effective than other oral antidiabetic drugs (OAD) in reducing glycemic variability in patients with type 2 diabetes (T2D) receiving no concurrent insulin treatment.
Major finding: The mean amplitude of glycemic excursions reduced significantly in patients receiving DPP4 inhibitors vs other OAD (mean difference [MD] −0.69 mmol/L; P < .001), insulin secretagogues (MD −0.92 mmol/L; P < .001), non-secretagogues (MD −0.43 mmol/L; P = .02), sulfonylureas (MD −0.91 mmol/L; P < .001), and sodium-glucose cotransporter-2 inhibitors (MD −0.67 mmol/L; P = .03).
Study details: The data come from a meta-analysis of 14 randomized controlled trials including 855 patients with T2D.
Disclosures: This study was funded by MSD China Holding Co. Ltd. Four authors declared being employees of MSD China, and one author declared being an employee of Merck Sharp & Dohme LLC.
Source: Chai S et al. Influence of dipeptidyl peptidase-4 inhibitors on glycemic variability in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Front Endocrinol (Lausanne). 2022;13:935039 (Aug 9). Doi: 10.3389/fendo.2022.935039
Key clinical point: Dipeptidyl peptidase-4 (DPP4) inhibitors were more effective than other oral antidiabetic drugs (OAD) in reducing glycemic variability in patients with type 2 diabetes (T2D) receiving no concurrent insulin treatment.
Major finding: The mean amplitude of glycemic excursions reduced significantly in patients receiving DPP4 inhibitors vs other OAD (mean difference [MD] −0.69 mmol/L; P < .001), insulin secretagogues (MD −0.92 mmol/L; P < .001), non-secretagogues (MD −0.43 mmol/L; P = .02), sulfonylureas (MD −0.91 mmol/L; P < .001), and sodium-glucose cotransporter-2 inhibitors (MD −0.67 mmol/L; P = .03).
Study details: The data come from a meta-analysis of 14 randomized controlled trials including 855 patients with T2D.
Disclosures: This study was funded by MSD China Holding Co. Ltd. Four authors declared being employees of MSD China, and one author declared being an employee of Merck Sharp & Dohme LLC.
Source: Chai S et al. Influence of dipeptidyl peptidase-4 inhibitors on glycemic variability in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Front Endocrinol (Lausanne). 2022;13:935039 (Aug 9). Doi: 10.3389/fendo.2022.935039
No effect of SGLT-2 inhibitors on cardiac autonomic neuropathy indices in T2D
Key clinical point: Sodium-glucose cotransporter-2 (SGLT-2) inhibitors did not have any significant beneficial effects on cardiac autonomic neuropathy (CAN) indices in patients with type 2 diabetes (T2D).
Major finding: SGLT-2 inhibitors had no significant effect on the low-frequency-to-high-frequency ratio (mean difference [MD] −0.11; P = .36), change in standard deviation of all 5-minute mean normal RR intervals (MD −2.83; P = .23), and change in the square root of the mean of the sum of the squares of differences between adjacent RR intervals (MD −0.14; P = .94).
Study details: Findings are from a meta-analysis of four randomized controlled trials including 247 patients with T2D who were randomly assigned to receive SGLT-2 inhibitors or placebo/active comparator.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Patoulias D et al. Effect of SGLT-2 inhibitors on cardiac autonomic function in type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. Acta Diabetol. 2022 (Aug 19). Doi: 10.1007/s00592-022-01958-0
Key clinical point: Sodium-glucose cotransporter-2 (SGLT-2) inhibitors did not have any significant beneficial effects on cardiac autonomic neuropathy (CAN) indices in patients with type 2 diabetes (T2D).
Major finding: SGLT-2 inhibitors had no significant effect on the low-frequency-to-high-frequency ratio (mean difference [MD] −0.11; P = .36), change in standard deviation of all 5-minute mean normal RR intervals (MD −2.83; P = .23), and change in the square root of the mean of the sum of the squares of differences between adjacent RR intervals (MD −0.14; P = .94).
Study details: Findings are from a meta-analysis of four randomized controlled trials including 247 patients with T2D who were randomly assigned to receive SGLT-2 inhibitors or placebo/active comparator.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Patoulias D et al. Effect of SGLT-2 inhibitors on cardiac autonomic function in type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. Acta Diabetol. 2022 (Aug 19). Doi: 10.1007/s00592-022-01958-0
Key clinical point: Sodium-glucose cotransporter-2 (SGLT-2) inhibitors did not have any significant beneficial effects on cardiac autonomic neuropathy (CAN) indices in patients with type 2 diabetes (T2D).
Major finding: SGLT-2 inhibitors had no significant effect on the low-frequency-to-high-frequency ratio (mean difference [MD] −0.11; P = .36), change in standard deviation of all 5-minute mean normal RR intervals (MD −2.83; P = .23), and change in the square root of the mean of the sum of the squares of differences between adjacent RR intervals (MD −0.14; P = .94).
Study details: Findings are from a meta-analysis of four randomized controlled trials including 247 patients with T2D who were randomly assigned to receive SGLT-2 inhibitors or placebo/active comparator.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Patoulias D et al. Effect of SGLT-2 inhibitors on cardiac autonomic function in type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. Acta Diabetol. 2022 (Aug 19). Doi: 10.1007/s00592-022-01958-0
Treatment advancement with iGlarLixi as effective as BI+RAI in real world in T2D
Key clinical point: In patients with type 2 diabetes (T2D) advancing from basal insulin (BI) therapy, a once-daily insulin glargine 100 U/mL and lixisenatide (iGlarLixi) injection regimen showed similar glycemic control to multiple injections with BI plus rapid-acting insulin (RAI), without weight gain.
Major finding: At 6 months, the mean reduction in glycated hemoglobin with iGlarLixi was noninferior to BI+RAI (mean difference [MD] 0.1%; 1-sided P = .0032), with weight gain being significantly lower with iGlarLixi vs BI+RAI (MD −0.8 kg; 2-sided P = .0069). The incidence of hypoglycemia was similar between the treatment groups.
Study details: Findings are from a retrospective study that used propensity score matching to evaluate therapy advancement with iGlarLixi (n = 814) or BI+RAI (n = 814) in patients with T2D on BI therapy.
Disclosures: This study was funded by Sanofi, Paris, France. Some authors declared receiving honoraria for speaking or consulting or research support or serving as advisory board members or speakers for various sources, including Sanofi. Three authors reported being employees of Sanofi.
Source: McCrimmon RJ et al. iGlarLixi versus basal plus rapid-acting insulin in adults with type 2 diabetes advancing from basal insulin therapy: The SoliSimplify real-world study. Diabetes Obes Metab. 2022 (Aug 19). Doi: 10.1111/dom.14844
Key clinical point: In patients with type 2 diabetes (T2D) advancing from basal insulin (BI) therapy, a once-daily insulin glargine 100 U/mL and lixisenatide (iGlarLixi) injection regimen showed similar glycemic control to multiple injections with BI plus rapid-acting insulin (RAI), without weight gain.
Major finding: At 6 months, the mean reduction in glycated hemoglobin with iGlarLixi was noninferior to BI+RAI (mean difference [MD] 0.1%; 1-sided P = .0032), with weight gain being significantly lower with iGlarLixi vs BI+RAI (MD −0.8 kg; 2-sided P = .0069). The incidence of hypoglycemia was similar between the treatment groups.
Study details: Findings are from a retrospective study that used propensity score matching to evaluate therapy advancement with iGlarLixi (n = 814) or BI+RAI (n = 814) in patients with T2D on BI therapy.
Disclosures: This study was funded by Sanofi, Paris, France. Some authors declared receiving honoraria for speaking or consulting or research support or serving as advisory board members or speakers for various sources, including Sanofi. Three authors reported being employees of Sanofi.
Source: McCrimmon RJ et al. iGlarLixi versus basal plus rapid-acting insulin in adults with type 2 diabetes advancing from basal insulin therapy: The SoliSimplify real-world study. Diabetes Obes Metab. 2022 (Aug 19). Doi: 10.1111/dom.14844
Key clinical point: In patients with type 2 diabetes (T2D) advancing from basal insulin (BI) therapy, a once-daily insulin glargine 100 U/mL and lixisenatide (iGlarLixi) injection regimen showed similar glycemic control to multiple injections with BI plus rapid-acting insulin (RAI), without weight gain.
Major finding: At 6 months, the mean reduction in glycated hemoglobin with iGlarLixi was noninferior to BI+RAI (mean difference [MD] 0.1%; 1-sided P = .0032), with weight gain being significantly lower with iGlarLixi vs BI+RAI (MD −0.8 kg; 2-sided P = .0069). The incidence of hypoglycemia was similar between the treatment groups.
Study details: Findings are from a retrospective study that used propensity score matching to evaluate therapy advancement with iGlarLixi (n = 814) or BI+RAI (n = 814) in patients with T2D on BI therapy.
Disclosures: This study was funded by Sanofi, Paris, France. Some authors declared receiving honoraria for speaking or consulting or research support or serving as advisory board members or speakers for various sources, including Sanofi. Three authors reported being employees of Sanofi.
Source: McCrimmon RJ et al. iGlarLixi versus basal plus rapid-acting insulin in adults with type 2 diabetes advancing from basal insulin therapy: The SoliSimplify real-world study. Diabetes Obes Metab. 2022 (Aug 19). Doi: 10.1111/dom.14844
Dapagliflozin prevents kidney function decline in T2D
Key clinical point: Dapagliflozin significantly reduced kidney function decline in patients with type 2 diabetes (T2D) and a high cardiovascular disease (CVD) risk across all Kidney Disease: Improving Global Outcomes (KDIGO) risk categories, including those with low baseline end-stage kidney disease (ESKD) risk
Major finding: Dapagliflozin vs placebo led to a significant reduction in kidney-specific composite outcome across all KDIGO risk categories (Pinteraction = .97), including those with low baseline kidney disease risk (hazard ratio 0.54; P < .001), with the risk for estimated glomerular filtration rate (eGFR) reductions by ≥30%, ≥40%, ≥50%, and ≥57% being significantly lower with dapagliflozin vs placebo (all P < .05).
Study details: Findings are from a post hoc analysis of the DECLARE-TIMI 58 trial including 16,842 patients with T2D at high CVD risk and low (n = 10,958), moderate (n = 4243), high (n = 1403), and very high (n = 238) ESKD risk according to KDIGO risk categories.
Disclosures: The DECLARE-TIMI 58 trial was funded by AstraZeneca and Bristol-Myers Squibb. Some authors reported receiving research funding, grant support, honoraria, personal fees, or consultancy fees or serving as advisory board members for various resources.
Source: Mosenzon O et al. Dapagliflozin and prevention of kidney disease among patients with type 2 diabetes--Post hoc analyses from the DECLARE-TIMI 58 trial. Diabetes Care. 2022 (Aug 23). Doi: 10.2337/dc22-0382
Key clinical point: Dapagliflozin significantly reduced kidney function decline in patients with type 2 diabetes (T2D) and a high cardiovascular disease (CVD) risk across all Kidney Disease: Improving Global Outcomes (KDIGO) risk categories, including those with low baseline end-stage kidney disease (ESKD) risk
Major finding: Dapagliflozin vs placebo led to a significant reduction in kidney-specific composite outcome across all KDIGO risk categories (Pinteraction = .97), including those with low baseline kidney disease risk (hazard ratio 0.54; P < .001), with the risk for estimated glomerular filtration rate (eGFR) reductions by ≥30%, ≥40%, ≥50%, and ≥57% being significantly lower with dapagliflozin vs placebo (all P < .05).
Study details: Findings are from a post hoc analysis of the DECLARE-TIMI 58 trial including 16,842 patients with T2D at high CVD risk and low (n = 10,958), moderate (n = 4243), high (n = 1403), and very high (n = 238) ESKD risk according to KDIGO risk categories.
Disclosures: The DECLARE-TIMI 58 trial was funded by AstraZeneca and Bristol-Myers Squibb. Some authors reported receiving research funding, grant support, honoraria, personal fees, or consultancy fees or serving as advisory board members for various resources.
Source: Mosenzon O et al. Dapagliflozin and prevention of kidney disease among patients with type 2 diabetes--Post hoc analyses from the DECLARE-TIMI 58 trial. Diabetes Care. 2022 (Aug 23). Doi: 10.2337/dc22-0382
Key clinical point: Dapagliflozin significantly reduced kidney function decline in patients with type 2 diabetes (T2D) and a high cardiovascular disease (CVD) risk across all Kidney Disease: Improving Global Outcomes (KDIGO) risk categories, including those with low baseline end-stage kidney disease (ESKD) risk
Major finding: Dapagliflozin vs placebo led to a significant reduction in kidney-specific composite outcome across all KDIGO risk categories (Pinteraction = .97), including those with low baseline kidney disease risk (hazard ratio 0.54; P < .001), with the risk for estimated glomerular filtration rate (eGFR) reductions by ≥30%, ≥40%, ≥50%, and ≥57% being significantly lower with dapagliflozin vs placebo (all P < .05).
Study details: Findings are from a post hoc analysis of the DECLARE-TIMI 58 trial including 16,842 patients with T2D at high CVD risk and low (n = 10,958), moderate (n = 4243), high (n = 1403), and very high (n = 238) ESKD risk according to KDIGO risk categories.
Disclosures: The DECLARE-TIMI 58 trial was funded by AstraZeneca and Bristol-Myers Squibb. Some authors reported receiving research funding, grant support, honoraria, personal fees, or consultancy fees or serving as advisory board members for various resources.
Source: Mosenzon O et al. Dapagliflozin and prevention of kidney disease among patients with type 2 diabetes--Post hoc analyses from the DECLARE-TIMI 58 trial. Diabetes Care. 2022 (Aug 23). Doi: 10.2337/dc22-0382
New-onset AF raises the risk for CVD, CKD, and mortality in T2D
Key clinical point: Patients with type 2 diabetes (T2D) and new-onset atrial fibrillation (AF) are at a higher risk for subsequent atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), chronic kidney disease (CKD), all-cause mortality, and cardiovascular disease (CVD) mortality compared with those with T2D and without new-onset AF.
Major finding: Among patients with T2D, those with vs without incident AF had a higher risk for ASCVD (adjusted hazard ratio [aHR] 1.85; 95% CI 1.59-2.16), HF (aHR 4.40; 95% CI 3.67-5.28), CKD (aHR 1.68; 95% CI 1.41-2.01), all-cause mortality (aHR 2.91; 95% CI 2.53-3.34), and CVD mortality (aHR 3.75; 95% CI 2.93-4.80).
Study details: This study included 16,551 patients with T2D and without CVD and CKD, of which 1394 developed AF during follow-up.
Disclosures: This study did not receive any funding. No potential conflicts of interest were reported.
Source: Geng T et al. Associations of new-onset atrial fibrillation with risks of cardiovascular disease, chronic kidney disease, and mortality among patients with type 2 diabetes. Diabetes Care. 2022 (Aug 19). Doi: 10.2337/dc22-0717
Key clinical point: Patients with type 2 diabetes (T2D) and new-onset atrial fibrillation (AF) are at a higher risk for subsequent atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), chronic kidney disease (CKD), all-cause mortality, and cardiovascular disease (CVD) mortality compared with those with T2D and without new-onset AF.
Major finding: Among patients with T2D, those with vs without incident AF had a higher risk for ASCVD (adjusted hazard ratio [aHR] 1.85; 95% CI 1.59-2.16), HF (aHR 4.40; 95% CI 3.67-5.28), CKD (aHR 1.68; 95% CI 1.41-2.01), all-cause mortality (aHR 2.91; 95% CI 2.53-3.34), and CVD mortality (aHR 3.75; 95% CI 2.93-4.80).
Study details: This study included 16,551 patients with T2D and without CVD and CKD, of which 1394 developed AF during follow-up.
Disclosures: This study did not receive any funding. No potential conflicts of interest were reported.
Source: Geng T et al. Associations of new-onset atrial fibrillation with risks of cardiovascular disease, chronic kidney disease, and mortality among patients with type 2 diabetes. Diabetes Care. 2022 (Aug 19). Doi: 10.2337/dc22-0717
Key clinical point: Patients with type 2 diabetes (T2D) and new-onset atrial fibrillation (AF) are at a higher risk for subsequent atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), chronic kidney disease (CKD), all-cause mortality, and cardiovascular disease (CVD) mortality compared with those with T2D and without new-onset AF.
Major finding: Among patients with T2D, those with vs without incident AF had a higher risk for ASCVD (adjusted hazard ratio [aHR] 1.85; 95% CI 1.59-2.16), HF (aHR 4.40; 95% CI 3.67-5.28), CKD (aHR 1.68; 95% CI 1.41-2.01), all-cause mortality (aHR 2.91; 95% CI 2.53-3.34), and CVD mortality (aHR 3.75; 95% CI 2.93-4.80).
Study details: This study included 16,551 patients with T2D and without CVD and CKD, of which 1394 developed AF during follow-up.
Disclosures: This study did not receive any funding. No potential conflicts of interest were reported.
Source: Geng T et al. Associations of new-onset atrial fibrillation with risks of cardiovascular disease, chronic kidney disease, and mortality among patients with type 2 diabetes. Diabetes Care. 2022 (Aug 19). Doi: 10.2337/dc22-0717
Canagliflozin reduces total CV burden in T2D patients with CKD
Key clinical point: Canagliflozin reduced not only the risk for the first cardiovascular (CV) events but also subsequent CV events in patients with type 2 diabetes and chronic kidney disease (CKD), with absolute benefits being greater for total CV events.
Major finding: Canagliflozin reduced the risk for the first (hazard ratio 0.74; P < .001) and total (incidence rate ratio 0.71; P < .001) CV events by 26% and 29%, respectively, with the absolute risk difference per 1000 patients treated over 2.5 years being −44 (95% CI −67 to −21) and −73 (95% CI −114 to −33) for the first and total CV events, respectively.
Study details: This was a post hoc analysis of the CREDENCE trial including patients with type 2 diabetes (T2D; glycated hemoglobin 6.5%-12.0%) and CKD who were randomly assigned to receive canagliflozin or placebo.
Disclosures: The CREDENCE trial was sponsored by Janssen Research & Development, LLC. Some authors reported serving as advisory board members, speakers, or consultants, or receiving honoraria, research support, consulting, travel, or scientific presentation fees from various sources, including Janssen.
Source: Li JW et al. Effect of canagliflozin on total cardiovascular burden in patients with diabetes and chronic kidney disease: A post hoc analysis from the CREDENCE trial. J Am Heart Assoc. 2022;11(16):e025045 (Aug 5). Doi: 10.1161/JAHA.121.025045
Key clinical point: Canagliflozin reduced not only the risk for the first cardiovascular (CV) events but also subsequent CV events in patients with type 2 diabetes and chronic kidney disease (CKD), with absolute benefits being greater for total CV events.
Major finding: Canagliflozin reduced the risk for the first (hazard ratio 0.74; P < .001) and total (incidence rate ratio 0.71; P < .001) CV events by 26% and 29%, respectively, with the absolute risk difference per 1000 patients treated over 2.5 years being −44 (95% CI −67 to −21) and −73 (95% CI −114 to −33) for the first and total CV events, respectively.
Study details: This was a post hoc analysis of the CREDENCE trial including patients with type 2 diabetes (T2D; glycated hemoglobin 6.5%-12.0%) and CKD who were randomly assigned to receive canagliflozin or placebo.
Disclosures: The CREDENCE trial was sponsored by Janssen Research & Development, LLC. Some authors reported serving as advisory board members, speakers, or consultants, or receiving honoraria, research support, consulting, travel, or scientific presentation fees from various sources, including Janssen.
Source: Li JW et al. Effect of canagliflozin on total cardiovascular burden in patients with diabetes and chronic kidney disease: A post hoc analysis from the CREDENCE trial. J Am Heart Assoc. 2022;11(16):e025045 (Aug 5). Doi: 10.1161/JAHA.121.025045
Key clinical point: Canagliflozin reduced not only the risk for the first cardiovascular (CV) events but also subsequent CV events in patients with type 2 diabetes and chronic kidney disease (CKD), with absolute benefits being greater for total CV events.
Major finding: Canagliflozin reduced the risk for the first (hazard ratio 0.74; P < .001) and total (incidence rate ratio 0.71; P < .001) CV events by 26% and 29%, respectively, with the absolute risk difference per 1000 patients treated over 2.5 years being −44 (95% CI −67 to −21) and −73 (95% CI −114 to −33) for the first and total CV events, respectively.
Study details: This was a post hoc analysis of the CREDENCE trial including patients with type 2 diabetes (T2D; glycated hemoglobin 6.5%-12.0%) and CKD who were randomly assigned to receive canagliflozin or placebo.
Disclosures: The CREDENCE trial was sponsored by Janssen Research & Development, LLC. Some authors reported serving as advisory board members, speakers, or consultants, or receiving honoraria, research support, consulting, travel, or scientific presentation fees from various sources, including Janssen.
Source: Li JW et al. Effect of canagliflozin on total cardiovascular burden in patients with diabetes and chronic kidney disease: A post hoc analysis from the CREDENCE trial. J Am Heart Assoc. 2022;11(16):e025045 (Aug 5). Doi: 10.1161/JAHA.121.025045
Even small changes can make endoscopy more sustainable: Study
Moving recycling bins and providing education to staff led to a reduction in the carbon footprint at a Portuguese hospital’s endoscopy unit, according to a study published in Gut.
“Sustainable endoscopy regarding waste handling was achievable and sustained over time, did not compromise productivity, and may be cost-effective for stakeholders,” wrote João A Cunha Neves, MD, MMSc, of Algarve University Hospital Centre in Portimão, Portugal, and his colleagues.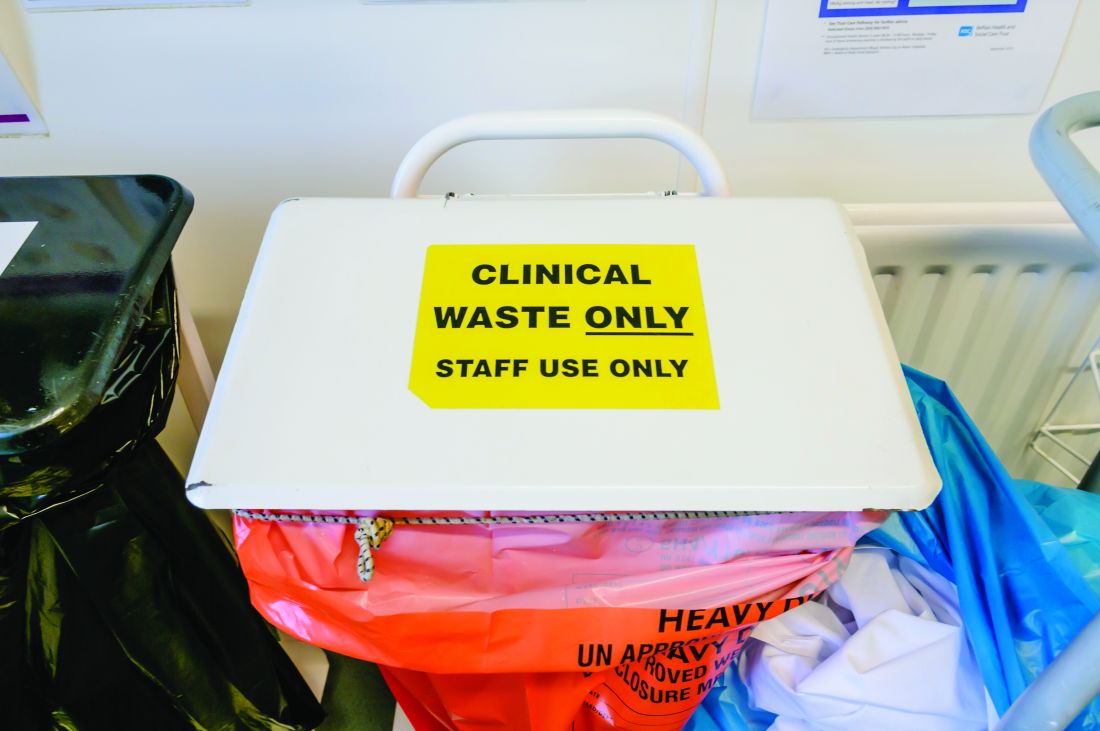
Although other work has shown that several of the strategies for reducing endoscopic waste are ‘easy wins,’ the authors noted that “lack of awareness by most endoscopy staff regarding the expenses and correct categorisation of endoscopic waste is the primary barrier to recycling in many endoscopy units.”
The four-stage prospective study took place at the Portimão endoscopy unit of Algarve University Hospital Centre in Portugal. It began with a 4-week audit that involved weighing regulated medical waste (“material fully contaminated with blood or body fluids or containing infectious agents”) and landfill waste (nonrecyclable material that isn’t fully contaminated). The researchers excluded from the analysis all waste from sharps containers, pre- and postprocedure activities, and endoscope reprocessing.
The second stage was one week of medical, nursing, and auxiliary team education about handling waste, in part based on observations collected during the first stage. Each endoscopy generates an estimated 1.5 kg of plastic waste, but recycling bins often are not available for the 0.3 kg of waste that’s recyclable. During the second stage, recycling bins were placed in endoscopy rooms while regulated medical waste and landfill bins were moved elsewhere.
The final two stages involved weighing both types of waste 1 month after the training and then 4 months after the training. For their calculations, the researchers assumed that 1 kg of landfill waste equated to 1 kg of carbon dioxide and 1 kg of regulated medical waste equated to 3 kg of carbon dioxide.
At the third stage, mean total waste fell by 12.9%, albeit not statistically significantly (P = .16), while the 41.4% regulated medical waste reduction was significant (P = .01). Landfill waste had increased 12.3% and both paper (0 to 1.2 kg) and plastic (0 to 2.1 kg) recycling waste increased. Mean endoscopy load had not significantly changed (46.2 vs. 44.5). Overall carbon dioxide was reduced by 31.6%, from 109.7 kg of carbon dioxide to 74.9 kg (P = .018), equating to an annual decrease of 1,665.6 kg. At four months postintervention, these effects remained.
“In both assessment periods, total waste produced by diagnostic standard endoscopic procedures was similar, but both regulated medical waste and overall carbon footprint were reduced,” the authors reported.
In a four-question assessment of the intervention with staff, “the entire team agreed that the study did not interfere with the daily work routine and was helpful in raising awareness about waste sorting within the unit,” the authors reported. The staff “also acknowledged that recycling waste allowed for more sustainable activity within the endoscopy unit, and that the achievements of the study were to be maintained in the future.”
How feasible is change?
The authors noted that health care accounts for 4.4% of the world’s carbon footprint and that endoscopy is the third largest generator of hospital medical waste, primarily because of single-use consumables. However, 71% of that health care carbon footprint comes from supply chain issues, particularly transportation, John I. Allen, MD, MBA, a retired clinical professor of medicine at the University Michigan, Ann Arbor, said in an interview. “Facility emissions add 17% and heating/cooling add 12%,” he said. “So, the actual footprint of endoscopy is quite small.”

Reducing single-use equipment and disposables by a third is a small overall impact considering the “labor-intensive education and monitoring system,” said Dr. Allen, who was not involved in the study. “That said, this paper and numerous others remind us of small steps that we can take – mostly to raise awareness about new technologies and more sustainable processes that are available or should be studied – to help transition us from the current [terrible] state to a more climate-friendly style of practice and life.”
One of the study’s limitations was the lack of a cost-benefit or impact analysis, according to Dr. Allen. Climate policies claiming to have local impact can be problematic when they “ignore both externalities and the actual wider impact on gas or temperature mitigation,” he added.
But he noted that “many health care systems are already implementing new ways of working with temperature- and carbon-mitigation in mind,” such as his own institution’s pledge to become carbon-neutral within a year. One step on that path has included transitioning more than 30% of their clinic visits to virtual visits, “thus saving [literally] millions of miles in travel and altering our parking construction plans,” Dr. Allen said.
“Reduction in climate impact will come from new ways to manufacture endoscopes, less reliance on single-use equipment, and increasing use of materials that encourage recycling,” Dr. Allen said. “In order to achieve meaningful climate impact, we need research into what current regulations and processes are necessary to protect patients and staff from infection transmission while creating an environmentally favorable workflow.”
Where does making a difference begin?
Another limitation was simply the small size of the department itself, which limits how much impact the intervention can have, but the study also showed the feasibility of getting buy-in from a department to make meaningful changes, according to Bishr Omary, MD, PhD, professor of medicine at Rutgers University’s Robert Wood Johnson Medical School, Piscataway, N.J. He was not involved in the study.
“Culture is an important aspect of this, but that’s where education comes in,” Dr. Omary said in an interview. “Leadership has to try to encourage and incentivize different units, not just endoscopy, but other surgery, too. I think the most effective approach is going to be top-down, where hospitals and health systems buy into this.”
One challenge to that buy-in is that climate change has become political, said Linda Anh B. Nguyen, MD, clinical professor of medicine and vice chief of clinical operations in Stanford (Calif.) University’s division of gastroenterology and hepatology.
“There may be resistance to implementation by those who do not see the value of reducing waste,” Dr. Nguyen, who was not involved in this study, said in an interview. “Successful implementation requires a culture change and reducing the physical barriers to make waste reduction easier. Having an advocate for the program embedded within the endoscopy unit will help with implementation.”
One of the advantages of the intervention in this study, Dr. Nguyen said, was its relative ease of implementation.
“The next step would be identifying which of the items that go into landfill can be replaced with reusable products,” Dr. Nguyen added.
Dr. Omary pointed to Practice Greenhealth as an example of an organization working toward the goal of climate change mitigation through a wide range of initiatives, including ones he has written about. The responsibility for reducing carbon footprints should be shared among individuals, institutions, and systems, Dr. Omary said, adding that individuals’ travel, such as to medical meetings, is a major contributor to greenhouse gas emissions.
A forthcoming publication from the four major gastroenterology medical organizations will outline additional ways gastroenterology can address climate change mitigation, Dr. Omary noted.
Dr. Nguyen said that gastroenterologists, as well as the entire health care industry, have a responsibility to combat climate change through waste reduction and that it can be done without sacrificing individual patient safety.
“Climate change must be at the forefront of our priorities for present and future generations,” Dr. Nguyen said. “We need to leave this world better than when we entered.”
But much of that change must especially occur at levels far higher than individual physicians or institutions, Dr. Allen said.
“Major responsibility for altering gastroenterology practices in order to mitigate climate change must originate in regulatory agencies and the manufacturers of our equipment,” Dr. Allen said. “Regulations must be based on demonstrated positive impact that is cost-effective for practices and health care systems.”
The research did not use external funding, and the authors reported no financial disclosures or conflicts of interests. Dr. Allen has consulted for Topography Health, OSHI Health, and Lynxmd. Dr. Nguyen has consulted for Alnylam, Ardelyx, Eli Lilly, Evoke Pharma, Ironwood, Pendulum, Phathom, Neurogastx, Sanofi, and Takeda; has served on the advisory board of Gemelli Biotech; and has received grants from Bold Health and Vanda. Dr. Omary had no disclosures.
Moving recycling bins and providing education to staff led to a reduction in the carbon footprint at a Portuguese hospital’s endoscopy unit, according to a study published in Gut.
“Sustainable endoscopy regarding waste handling was achievable and sustained over time, did not compromise productivity, and may be cost-effective for stakeholders,” wrote João A Cunha Neves, MD, MMSc, of Algarve University Hospital Centre in Portimão, Portugal, and his colleagues.
Although other work has shown that several of the strategies for reducing endoscopic waste are ‘easy wins,’ the authors noted that “lack of awareness by most endoscopy staff regarding the expenses and correct categorisation of endoscopic waste is the primary barrier to recycling in many endoscopy units.”
The four-stage prospective study took place at the Portimão endoscopy unit of Algarve University Hospital Centre in Portugal. It began with a 4-week audit that involved weighing regulated medical waste (“material fully contaminated with blood or body fluids or containing infectious agents”) and landfill waste (nonrecyclable material that isn’t fully contaminated). The researchers excluded from the analysis all waste from sharps containers, pre- and postprocedure activities, and endoscope reprocessing.
The second stage was one week of medical, nursing, and auxiliary team education about handling waste, in part based on observations collected during the first stage. Each endoscopy generates an estimated 1.5 kg of plastic waste, but recycling bins often are not available for the 0.3 kg of waste that’s recyclable. During the second stage, recycling bins were placed in endoscopy rooms while regulated medical waste and landfill bins were moved elsewhere.
The final two stages involved weighing both types of waste 1 month after the training and then 4 months after the training. For their calculations, the researchers assumed that 1 kg of landfill waste equated to 1 kg of carbon dioxide and 1 kg of regulated medical waste equated to 3 kg of carbon dioxide.
At the third stage, mean total waste fell by 12.9%, albeit not statistically significantly (P = .16), while the 41.4% regulated medical waste reduction was significant (P = .01). Landfill waste had increased 12.3% and both paper (0 to 1.2 kg) and plastic (0 to 2.1 kg) recycling waste increased. Mean endoscopy load had not significantly changed (46.2 vs. 44.5). Overall carbon dioxide was reduced by 31.6%, from 109.7 kg of carbon dioxide to 74.9 kg (P = .018), equating to an annual decrease of 1,665.6 kg. At four months postintervention, these effects remained.
“In both assessment periods, total waste produced by diagnostic standard endoscopic procedures was similar, but both regulated medical waste and overall carbon footprint were reduced,” the authors reported.
In a four-question assessment of the intervention with staff, “the entire team agreed that the study did not interfere with the daily work routine and was helpful in raising awareness about waste sorting within the unit,” the authors reported. The staff “also acknowledged that recycling waste allowed for more sustainable activity within the endoscopy unit, and that the achievements of the study were to be maintained in the future.”
How feasible is change?
The authors noted that health care accounts for 4.4% of the world’s carbon footprint and that endoscopy is the third largest generator of hospital medical waste, primarily because of single-use consumables. However, 71% of that health care carbon footprint comes from supply chain issues, particularly transportation, John I. Allen, MD, MBA, a retired clinical professor of medicine at the University Michigan, Ann Arbor, said in an interview. “Facility emissions add 17% and heating/cooling add 12%,” he said. “So, the actual footprint of endoscopy is quite small.”
Reducing single-use equipment and disposables by a third is a small overall impact considering the “labor-intensive education and monitoring system,” said Dr. Allen, who was not involved in the study. “That said, this paper and numerous others remind us of small steps that we can take – mostly to raise awareness about new technologies and more sustainable processes that are available or should be studied – to help transition us from the current [terrible] state to a more climate-friendly style of practice and life.”
One of the study’s limitations was the lack of a cost-benefit or impact analysis, according to Dr. Allen. Climate policies claiming to have local impact can be problematic when they “ignore both externalities and the actual wider impact on gas or temperature mitigation,” he added.
But he noted that “many health care systems are already implementing new ways of working with temperature- and carbon-mitigation in mind,” such as his own institution’s pledge to become carbon-neutral within a year. One step on that path has included transitioning more than 30% of their clinic visits to virtual visits, “thus saving [literally] millions of miles in travel and altering our parking construction plans,” Dr. Allen said.
“Reduction in climate impact will come from new ways to manufacture endoscopes, less reliance on single-use equipment, and increasing use of materials that encourage recycling,” Dr. Allen said. “In order to achieve meaningful climate impact, we need research into what current regulations and processes are necessary to protect patients and staff from infection transmission while creating an environmentally favorable workflow.”
Where does making a difference begin?
Another limitation was simply the small size of the department itself, which limits how much impact the intervention can have, but the study also showed the feasibility of getting buy-in from a department to make meaningful changes, according to Bishr Omary, MD, PhD, professor of medicine at Rutgers University’s Robert Wood Johnson Medical School, Piscataway, N.J. He was not involved in the study.
“Culture is an important aspect of this, but that’s where education comes in,” Dr. Omary said in an interview. “Leadership has to try to encourage and incentivize different units, not just endoscopy, but other surgery, too. I think the most effective approach is going to be top-down, where hospitals and health systems buy into this.”
One challenge to that buy-in is that climate change has become political, said Linda Anh B. Nguyen, MD, clinical professor of medicine and vice chief of clinical operations in Stanford (Calif.) University’s division of gastroenterology and hepatology.
“There may be resistance to implementation by those who do not see the value of reducing waste,” Dr. Nguyen, who was not involved in this study, said in an interview. “Successful implementation requires a culture change and reducing the physical barriers to make waste reduction easier. Having an advocate for the program embedded within the endoscopy unit will help with implementation.”
One of the advantages of the intervention in this study, Dr. Nguyen said, was its relative ease of implementation.
“The next step would be identifying which of the items that go into landfill can be replaced with reusable products,” Dr. Nguyen added.
Dr. Omary pointed to Practice Greenhealth as an example of an organization working toward the goal of climate change mitigation through a wide range of initiatives, including ones he has written about. The responsibility for reducing carbon footprints should be shared among individuals, institutions, and systems, Dr. Omary said, adding that individuals’ travel, such as to medical meetings, is a major contributor to greenhouse gas emissions.
A forthcoming publication from the four major gastroenterology medical organizations will outline additional ways gastroenterology can address climate change mitigation, Dr. Omary noted.
Dr. Nguyen said that gastroenterologists, as well as the entire health care industry, have a responsibility to combat climate change through waste reduction and that it can be done without sacrificing individual patient safety.
“Climate change must be at the forefront of our priorities for present and future generations,” Dr. Nguyen said. “We need to leave this world better than when we entered.”
But much of that change must especially occur at levels far higher than individual physicians or institutions, Dr. Allen said.
“Major responsibility for altering gastroenterology practices in order to mitigate climate change must originate in regulatory agencies and the manufacturers of our equipment,” Dr. Allen said. “Regulations must be based on demonstrated positive impact that is cost-effective for practices and health care systems.”
The research did not use external funding, and the authors reported no financial disclosures or conflicts of interests. Dr. Allen has consulted for Topography Health, OSHI Health, and Lynxmd. Dr. Nguyen has consulted for Alnylam, Ardelyx, Eli Lilly, Evoke Pharma, Ironwood, Pendulum, Phathom, Neurogastx, Sanofi, and Takeda; has served on the advisory board of Gemelli Biotech; and has received grants from Bold Health and Vanda. Dr. Omary had no disclosures.
Moving recycling bins and providing education to staff led to a reduction in the carbon footprint at a Portuguese hospital’s endoscopy unit, according to a study published in Gut.
“Sustainable endoscopy regarding waste handling was achievable and sustained over time, did not compromise productivity, and may be cost-effective for stakeholders,” wrote João A Cunha Neves, MD, MMSc, of Algarve University Hospital Centre in Portimão, Portugal, and his colleagues.
Although other work has shown that several of the strategies for reducing endoscopic waste are ‘easy wins,’ the authors noted that “lack of awareness by most endoscopy staff regarding the expenses and correct categorisation of endoscopic waste is the primary barrier to recycling in many endoscopy units.”
The four-stage prospective study took place at the Portimão endoscopy unit of Algarve University Hospital Centre in Portugal. It began with a 4-week audit that involved weighing regulated medical waste (“material fully contaminated with blood or body fluids or containing infectious agents”) and landfill waste (nonrecyclable material that isn’t fully contaminated). The researchers excluded from the analysis all waste from sharps containers, pre- and postprocedure activities, and endoscope reprocessing.
The second stage was one week of medical, nursing, and auxiliary team education about handling waste, in part based on observations collected during the first stage. Each endoscopy generates an estimated 1.5 kg of plastic waste, but recycling bins often are not available for the 0.3 kg of waste that’s recyclable. During the second stage, recycling bins were placed in endoscopy rooms while regulated medical waste and landfill bins were moved elsewhere.
The final two stages involved weighing both types of waste 1 month after the training and then 4 months after the training. For their calculations, the researchers assumed that 1 kg of landfill waste equated to 1 kg of carbon dioxide and 1 kg of regulated medical waste equated to 3 kg of carbon dioxide.
At the third stage, mean total waste fell by 12.9%, albeit not statistically significantly (P = .16), while the 41.4% regulated medical waste reduction was significant (P = .01). Landfill waste had increased 12.3% and both paper (0 to 1.2 kg) and plastic (0 to 2.1 kg) recycling waste increased. Mean endoscopy load had not significantly changed (46.2 vs. 44.5). Overall carbon dioxide was reduced by 31.6%, from 109.7 kg of carbon dioxide to 74.9 kg (P = .018), equating to an annual decrease of 1,665.6 kg. At four months postintervention, these effects remained.
“In both assessment periods, total waste produced by diagnostic standard endoscopic procedures was similar, but both regulated medical waste and overall carbon footprint were reduced,” the authors reported.
In a four-question assessment of the intervention with staff, “the entire team agreed that the study did not interfere with the daily work routine and was helpful in raising awareness about waste sorting within the unit,” the authors reported. The staff “also acknowledged that recycling waste allowed for more sustainable activity within the endoscopy unit, and that the achievements of the study were to be maintained in the future.”
How feasible is change?
The authors noted that health care accounts for 4.4% of the world’s carbon footprint and that endoscopy is the third largest generator of hospital medical waste, primarily because of single-use consumables. However, 71% of that health care carbon footprint comes from supply chain issues, particularly transportation, John I. Allen, MD, MBA, a retired clinical professor of medicine at the University Michigan, Ann Arbor, said in an interview. “Facility emissions add 17% and heating/cooling add 12%,” he said. “So, the actual footprint of endoscopy is quite small.”
Reducing single-use equipment and disposables by a third is a small overall impact considering the “labor-intensive education and monitoring system,” said Dr. Allen, who was not involved in the study. “That said, this paper and numerous others remind us of small steps that we can take – mostly to raise awareness about new technologies and more sustainable processes that are available or should be studied – to help transition us from the current [terrible] state to a more climate-friendly style of practice and life.”
One of the study’s limitations was the lack of a cost-benefit or impact analysis, according to Dr. Allen. Climate policies claiming to have local impact can be problematic when they “ignore both externalities and the actual wider impact on gas or temperature mitigation,” he added.
But he noted that “many health care systems are already implementing new ways of working with temperature- and carbon-mitigation in mind,” such as his own institution’s pledge to become carbon-neutral within a year. One step on that path has included transitioning more than 30% of their clinic visits to virtual visits, “thus saving [literally] millions of miles in travel and altering our parking construction plans,” Dr. Allen said.
“Reduction in climate impact will come from new ways to manufacture endoscopes, less reliance on single-use equipment, and increasing use of materials that encourage recycling,” Dr. Allen said. “In order to achieve meaningful climate impact, we need research into what current regulations and processes are necessary to protect patients and staff from infection transmission while creating an environmentally favorable workflow.”
Where does making a difference begin?
Another limitation was simply the small size of the department itself, which limits how much impact the intervention can have, but the study also showed the feasibility of getting buy-in from a department to make meaningful changes, according to Bishr Omary, MD, PhD, professor of medicine at Rutgers University’s Robert Wood Johnson Medical School, Piscataway, N.J. He was not involved in the study.
“Culture is an important aspect of this, but that’s where education comes in,” Dr. Omary said in an interview. “Leadership has to try to encourage and incentivize different units, not just endoscopy, but other surgery, too. I think the most effective approach is going to be top-down, where hospitals and health systems buy into this.”
One challenge to that buy-in is that climate change has become political, said Linda Anh B. Nguyen, MD, clinical professor of medicine and vice chief of clinical operations in Stanford (Calif.) University’s division of gastroenterology and hepatology.
“There may be resistance to implementation by those who do not see the value of reducing waste,” Dr. Nguyen, who was not involved in this study, said in an interview. “Successful implementation requires a culture change and reducing the physical barriers to make waste reduction easier. Having an advocate for the program embedded within the endoscopy unit will help with implementation.”
One of the advantages of the intervention in this study, Dr. Nguyen said, was its relative ease of implementation.
“The next step would be identifying which of the items that go into landfill can be replaced with reusable products,” Dr. Nguyen added.
Dr. Omary pointed to Practice Greenhealth as an example of an organization working toward the goal of climate change mitigation through a wide range of initiatives, including ones he has written about. The responsibility for reducing carbon footprints should be shared among individuals, institutions, and systems, Dr. Omary said, adding that individuals’ travel, such as to medical meetings, is a major contributor to greenhouse gas emissions.
A forthcoming publication from the four major gastroenterology medical organizations will outline additional ways gastroenterology can address climate change mitigation, Dr. Omary noted.
Dr. Nguyen said that gastroenterologists, as well as the entire health care industry, have a responsibility to combat climate change through waste reduction and that it can be done without sacrificing individual patient safety.
“Climate change must be at the forefront of our priorities for present and future generations,” Dr. Nguyen said. “We need to leave this world better than when we entered.”
But much of that change must especially occur at levels far higher than individual physicians or institutions, Dr. Allen said.
“Major responsibility for altering gastroenterology practices in order to mitigate climate change must originate in regulatory agencies and the manufacturers of our equipment,” Dr. Allen said. “Regulations must be based on demonstrated positive impact that is cost-effective for practices and health care systems.”
The research did not use external funding, and the authors reported no financial disclosures or conflicts of interests. Dr. Allen has consulted for Topography Health, OSHI Health, and Lynxmd. Dr. Nguyen has consulted for Alnylam, Ardelyx, Eli Lilly, Evoke Pharma, Ironwood, Pendulum, Phathom, Neurogastx, Sanofi, and Takeda; has served on the advisory board of Gemelli Biotech; and has received grants from Bold Health and Vanda. Dr. Omary had no disclosures.
FROM GUT
EHR: A progress report
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.

The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.
The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.
The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
