User login
Pregnancy increases risk for symptomatic kidney stones
Pregnancy increases the risk for first-time symptomatic kidney stone formation which peaks close to the time of delivery but can persist even a year later, a population-based, case-controlled study suggests.
“We suspected the risk of a kidney stone event would be high during pregnancy, but we were surprised that the risk remained high for up to a year after delivery,” senior author Andrew Rule, MD, a nephrologist at Mayo Clinic, Rochester, Minn, said in a statement from his institution.
“[So] while most kidney stones that form during pregnancy are detected early by painful passage, some may remain stable in the kidney undetected for a longer period before dislodging and [again] resulting in a painful passage,” he added.
The study was published online April 15, 2021, in the American Journal of Kidney Diseases by Charat Thongprayoon, MD, also of the Mayo Clinic, and colleagues.
“The results of this study indicate that prenatal counseling regarding kidney stones may be warranted, especially for women with other risk factors for kidney stones, such as obesity,” he noted.
First-time stone formers
The observational study included 945 first-time symptomatic kidney stone formers aged between 15 and 45 years who were compared with 1,890 age-matched female controls from the Rochester Epidemiology Project. The latter is a medical record linkage system for almost all medical care administered in Olmsted County in Minnesota.
Compared with nonpregnant women, the odds of a symptomatic kidney stone forming in a pregnant woman was similar in the first trimester (odds ratio, 0.92; P = .8), began to increase during the second trimester (OR, 2.00; P = .007), further increased during the third trimester (OR, 2.69; P = .001), and peaked at 0-3 months after delivery (OR, 3.53; P < .001). The risk returned to baseline by 1 year after delivery.
These associations persisted after adjustment for age and race or for diabetes, hypertension, and obesity. These results did not significantly differ by age, race, time period, or number of prior pregnancies.
The risk of a pregnant woman developing a symptomatic kidney stone was higher in women with obesity, compared with those of normal weight (P = .01).
And compared with women who had not been pregnant before, one prior pregnancy also increased the risk of having a symptomatic kidney stone by approximately 30% (OR, 1.29; P = .03), although two or more prior pregnancies did not significantly increase symptomatic kidney stone risk.
Thus, “it can be inferred that the odds of a symptomatic kidney stone peak around the time of delivery,” the authors emphasized. “The odds of a first-time symptomatic kidney stone then decreased over time and were fully attenuated and no longer statistically significant by 12 months after delivery.”
Dr. Thongprayoon said there are several physiologic reasons why pregnancy might contribute to kidney stone formation.
During pregnancy, ureteral compression and ureteral relaxation caused by elevated progesterone levels can cause urinary stasis.
Furthermore, increased urinary calcium excretion and elevated urine pH during pregnancy can promote calcium phosphate stone formation. It is noteworthy that almost all pregnant, first-time stone formers had calcium phosphate stones.
“During pregnancy, a kidney stone may contribute to serious complications,” Dr. Thongprayoon explained.
General dietary recommendations for preventing kidney stones include drinking abundant fluids and consuming a low-salt diet.
The study was supported by the Mayo Clinic O’Brien Urology Research Center and a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pregnancy increases the risk for first-time symptomatic kidney stone formation which peaks close to the time of delivery but can persist even a year later, a population-based, case-controlled study suggests.
“We suspected the risk of a kidney stone event would be high during pregnancy, but we were surprised that the risk remained high for up to a year after delivery,” senior author Andrew Rule, MD, a nephrologist at Mayo Clinic, Rochester, Minn, said in a statement from his institution.
“[So] while most kidney stones that form during pregnancy are detected early by painful passage, some may remain stable in the kidney undetected for a longer period before dislodging and [again] resulting in a painful passage,” he added.
The study was published online April 15, 2021, in the American Journal of Kidney Diseases by Charat Thongprayoon, MD, also of the Mayo Clinic, and colleagues.
“The results of this study indicate that prenatal counseling regarding kidney stones may be warranted, especially for women with other risk factors for kidney stones, such as obesity,” he noted.
First-time stone formers
The observational study included 945 first-time symptomatic kidney stone formers aged between 15 and 45 years who were compared with 1,890 age-matched female controls from the Rochester Epidemiology Project. The latter is a medical record linkage system for almost all medical care administered in Olmsted County in Minnesota.
Compared with nonpregnant women, the odds of a symptomatic kidney stone forming in a pregnant woman was similar in the first trimester (odds ratio, 0.92; P = .8), began to increase during the second trimester (OR, 2.00; P = .007), further increased during the third trimester (OR, 2.69; P = .001), and peaked at 0-3 months after delivery (OR, 3.53; P < .001). The risk returned to baseline by 1 year after delivery.
These associations persisted after adjustment for age and race or for diabetes, hypertension, and obesity. These results did not significantly differ by age, race, time period, or number of prior pregnancies.
The risk of a pregnant woman developing a symptomatic kidney stone was higher in women with obesity, compared with those of normal weight (P = .01).
And compared with women who had not been pregnant before, one prior pregnancy also increased the risk of having a symptomatic kidney stone by approximately 30% (OR, 1.29; P = .03), although two or more prior pregnancies did not significantly increase symptomatic kidney stone risk.
Thus, “it can be inferred that the odds of a symptomatic kidney stone peak around the time of delivery,” the authors emphasized. “The odds of a first-time symptomatic kidney stone then decreased over time and were fully attenuated and no longer statistically significant by 12 months after delivery.”
Dr. Thongprayoon said there are several physiologic reasons why pregnancy might contribute to kidney stone formation.
During pregnancy, ureteral compression and ureteral relaxation caused by elevated progesterone levels can cause urinary stasis.
Furthermore, increased urinary calcium excretion and elevated urine pH during pregnancy can promote calcium phosphate stone formation. It is noteworthy that almost all pregnant, first-time stone formers had calcium phosphate stones.
“During pregnancy, a kidney stone may contribute to serious complications,” Dr. Thongprayoon explained.
General dietary recommendations for preventing kidney stones include drinking abundant fluids and consuming a low-salt diet.
The study was supported by the Mayo Clinic O’Brien Urology Research Center and a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pregnancy increases the risk for first-time symptomatic kidney stone formation which peaks close to the time of delivery but can persist even a year later, a population-based, case-controlled study suggests.
“We suspected the risk of a kidney stone event would be high during pregnancy, but we were surprised that the risk remained high for up to a year after delivery,” senior author Andrew Rule, MD, a nephrologist at Mayo Clinic, Rochester, Minn, said in a statement from his institution.
“[So] while most kidney stones that form during pregnancy are detected early by painful passage, some may remain stable in the kidney undetected for a longer period before dislodging and [again] resulting in a painful passage,” he added.
The study was published online April 15, 2021, in the American Journal of Kidney Diseases by Charat Thongprayoon, MD, also of the Mayo Clinic, and colleagues.
“The results of this study indicate that prenatal counseling regarding kidney stones may be warranted, especially for women with other risk factors for kidney stones, such as obesity,” he noted.
First-time stone formers
The observational study included 945 first-time symptomatic kidney stone formers aged between 15 and 45 years who were compared with 1,890 age-matched female controls from the Rochester Epidemiology Project. The latter is a medical record linkage system for almost all medical care administered in Olmsted County in Minnesota.
Compared with nonpregnant women, the odds of a symptomatic kidney stone forming in a pregnant woman was similar in the first trimester (odds ratio, 0.92; P = .8), began to increase during the second trimester (OR, 2.00; P = .007), further increased during the third trimester (OR, 2.69; P = .001), and peaked at 0-3 months after delivery (OR, 3.53; P < .001). The risk returned to baseline by 1 year after delivery.
These associations persisted after adjustment for age and race or for diabetes, hypertension, and obesity. These results did not significantly differ by age, race, time period, or number of prior pregnancies.
The risk of a pregnant woman developing a symptomatic kidney stone was higher in women with obesity, compared with those of normal weight (P = .01).
And compared with women who had not been pregnant before, one prior pregnancy also increased the risk of having a symptomatic kidney stone by approximately 30% (OR, 1.29; P = .03), although two or more prior pregnancies did not significantly increase symptomatic kidney stone risk.
Thus, “it can be inferred that the odds of a symptomatic kidney stone peak around the time of delivery,” the authors emphasized. “The odds of a first-time symptomatic kidney stone then decreased over time and were fully attenuated and no longer statistically significant by 12 months after delivery.”
Dr. Thongprayoon said there are several physiologic reasons why pregnancy might contribute to kidney stone formation.
During pregnancy, ureteral compression and ureteral relaxation caused by elevated progesterone levels can cause urinary stasis.
Furthermore, increased urinary calcium excretion and elevated urine pH during pregnancy can promote calcium phosphate stone formation. It is noteworthy that almost all pregnant, first-time stone formers had calcium phosphate stones.
“During pregnancy, a kidney stone may contribute to serious complications,” Dr. Thongprayoon explained.
General dietary recommendations for preventing kidney stones include drinking abundant fluids and consuming a low-salt diet.
The study was supported by the Mayo Clinic O’Brien Urology Research Center and a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
IV drug users: The new face of candidemia
Background: Intravenous drug use is an increasingly common risk factor for candidemia as the opioid crisis worsens. This study quantifies this change and characterizes the changing epidemiology of candidemia.

Study design: A cross-sectional study.
Setting: Health departments in nine states.
Synopsis: IV drug users typically have a very distinctive phenotype among all patients with candidemia: They are younger (35 vs. 63 years), are more likely to be homeless, are not black, are smokers; they have hepatitis C, have no malignancies, have polymicrobial bacteremia, and have acquired the infection outside of the hospital. They are much less likely to die of the infection (8.6% vs 27.5%), compared with the non-IV drug users. In four states, the proportion of candidemia associated with IV drug use more than doubled, from 7% to 15% during 2014-2017, representing a possible shift in the epidemiology of candidemia.
The study did not quantify or address complications that many hospitalists see, such as endocarditis, endophthalmitis, and osteomyelitis. The study looked at only nine states, so results may not be generalizable. Nevertheless, the robust analysis suggests an alarming, increasing trend.
Bottom line: As the opioid crisis worsens, hospitalists should consider candidemia in hospitalized IV drug users and should evaluate patients with candidemia for IV drug use.
Citation: Zhang AY et al. The changing epidemiology of candidemia in the United States: Injection drug use as an increasingly common risk factor – Active surveillance in selected sites, United States, 2014-2017. Clin Infect Dis. 2019 Nov 2. doi: 10.1093/cid/ciz1061.
Dr. Raghavan is assistant professor in the division of hospital medicine, Loyola University Medical Center, Maywood, Ill.
Background: Intravenous drug use is an increasingly common risk factor for candidemia as the opioid crisis worsens. This study quantifies this change and characterizes the changing epidemiology of candidemia.
Study design: A cross-sectional study.
Setting: Health departments in nine states.
Synopsis: IV drug users typically have a very distinctive phenotype among all patients with candidemia: They are younger (35 vs. 63 years), are more likely to be homeless, are not black, are smokers; they have hepatitis C, have no malignancies, have polymicrobial bacteremia, and have acquired the infection outside of the hospital. They are much less likely to die of the infection (8.6% vs 27.5%), compared with the non-IV drug users. In four states, the proportion of candidemia associated with IV drug use more than doubled, from 7% to 15% during 2014-2017, representing a possible shift in the epidemiology of candidemia.
The study did not quantify or address complications that many hospitalists see, such as endocarditis, endophthalmitis, and osteomyelitis. The study looked at only nine states, so results may not be generalizable. Nevertheless, the robust analysis suggests an alarming, increasing trend.
Bottom line: As the opioid crisis worsens, hospitalists should consider candidemia in hospitalized IV drug users and should evaluate patients with candidemia for IV drug use.
Citation: Zhang AY et al. The changing epidemiology of candidemia in the United States: Injection drug use as an increasingly common risk factor – Active surveillance in selected sites, United States, 2014-2017. Clin Infect Dis. 2019 Nov 2. doi: 10.1093/cid/ciz1061.
Dr. Raghavan is assistant professor in the division of hospital medicine, Loyola University Medical Center, Maywood, Ill.
Background: Intravenous drug use is an increasingly common risk factor for candidemia as the opioid crisis worsens. This study quantifies this change and characterizes the changing epidemiology of candidemia.
Study design: A cross-sectional study.
Setting: Health departments in nine states.
Synopsis: IV drug users typically have a very distinctive phenotype among all patients with candidemia: They are younger (35 vs. 63 years), are more likely to be homeless, are not black, are smokers; they have hepatitis C, have no malignancies, have polymicrobial bacteremia, and have acquired the infection outside of the hospital. They are much less likely to die of the infection (8.6% vs 27.5%), compared with the non-IV drug users. In four states, the proportion of candidemia associated with IV drug use more than doubled, from 7% to 15% during 2014-2017, representing a possible shift in the epidemiology of candidemia.
The study did not quantify or address complications that many hospitalists see, such as endocarditis, endophthalmitis, and osteomyelitis. The study looked at only nine states, so results may not be generalizable. Nevertheless, the robust analysis suggests an alarming, increasing trend.
Bottom line: As the opioid crisis worsens, hospitalists should consider candidemia in hospitalized IV drug users and should evaluate patients with candidemia for IV drug use.
Citation: Zhang AY et al. The changing epidemiology of candidemia in the United States: Injection drug use as an increasingly common risk factor – Active surveillance in selected sites, United States, 2014-2017. Clin Infect Dis. 2019 Nov 2. doi: 10.1093/cid/ciz1061.
Dr. Raghavan is assistant professor in the division of hospital medicine, Loyola University Medical Center, Maywood, Ill.
Pfizer developing pill to treat COVID-19 symptoms
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
Some MS treatments may heighten COVID risk
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.

Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.
Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.
Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
FROM AAN 2021

VNS plus rehab is a powerful poststroke combination
according to preliminary results of a randomized clinical trial at the 2021 annual meeting of the American Academy of Neurology.

“We believe that vagus nerve stimulation combined with rehabilitation is an acceptable and effective intervention for improving upper-limb impairment and function in people with moderate to severe arm weakness a long time VNS-REHAB pivotal study is a randomized, blinded, controlled trial of 108 people who had upper-extremity weakness after having a stroke at least 9 months before enrollment. The average for the group was 3 years post stroke after ischemic stroke,” said Jesse Dawson, MD, a professor at the University of Glasgow.
The Fifty-three patients were assigned active VNS followed by 6 weeks of in-clinic rehabilitation and then 90 days of home-based rehab. At in-clinic rehab, the therapist initiated a 5-second burst of VNS stimulation during each movement. In home-base treatment, the device was activated by a magnet.
Fifty-five patients were assigned sham VNS. After 90 days, the sham group crossed over to receive VNS for 6 weeks and then 90 days of home exercise. This crossover group was the focus of the data Dr. Dawson presented at AAN 2021. The overall trial results have been published in the Lancet.
“The hypothesis is based on the knowledge that the VNS stimulates the release of proneuroplastic neuromodulators norepinephrine and acetylcholine,” Dr. Dawson said. “By pairing VNS with task-specific movement, we hypothesize that we will increase task-specific neuroplasticity.”
The main study showed “a statistically significant difference across all primary and secondary endpoints at all time points in favor of rehabilitation paired with VNS,” Dr. Dawson said. The primary outcome was improvement in Fugl-Meyer Upper Extremity (FMA-UE) outcome, with the active VNS group having a significantly higher percentage of responders. For example, 47% of the active VNS patients had a greater than 6-point response on FMA-UE improvement versus 27% of the sham group (P = .010).
When the sham group crossed over to active VNS, the improvement in arm function matched that of the treatment group in the main study, Dr. Dawson said. “If you look at specifically what happened after they completed the control phase, there was a further small increase in Fugl-Meyer score, but, more importantly between 20% and 35% achieved a clinically important response on the Fugl-Meyer assessment or the Wolf Motor Function Test, giving a number need to treat ranging from three to five,” he said.
Dr. Dawson said that data on adverse events was presented in the Lancet publication. “These were observed at expected frequencies,” he said.
In an interview, he explained the significance of reporting the number to treat. “The number needed to treat helps give an idea of how many times you need to do something to achieve the desired outcome. So for VNS paired with rehab versus rehab alone, you need to treat four people to get one extra clinically important response, compared with just doing therapy.”
The next steps for his group’s research, he said, “will be to try and explore whether we can predict who responds best, and we would like to see if people with other types of stroke benefit.”

In providing comment on the study, Andreas Luft, MD, a professor at the University Hospital Zürich, noted that the FME-UE score improvements reported “are significant and meaningful. ... However, they may also be achieved by increasing the intensity of training. Many medical systems offer their patients high rehabilitation intensities and achieve similar improvements. Whether VNS can further boost higher-intensity training ‘beyond its limits’ is probable but remains to be demonstrated.”
Dr. Luft noted the study advances the knowledge of combining a therapeutic approach with training. “More such approaches are necessary to increase the therapeutic instrumentation of neurorehabilitation,” he said.
Dr. Dawson reported a financial relationship with MicroTransponder. His coauthors reported relationships with MicroTransponder, SanBio, Fujifilm Toyoma Chemical, Medtronic, TRCare, SAEBO, Allergan/AbbVie, Ipsen, Merz, Ottobock/Hangar Orthopedics, Parker Hannifin, Revance Therapeutics, ReWallk, and Sword Health. Three coauthors are employees of MicroTransponder. Dr. Luft has no relevant relationships to disclose.
according to preliminary results of a randomized clinical trial at the 2021 annual meeting of the American Academy of Neurology.
“We believe that vagus nerve stimulation combined with rehabilitation is an acceptable and effective intervention for improving upper-limb impairment and function in people with moderate to severe arm weakness a long time VNS-REHAB pivotal study is a randomized, blinded, controlled trial of 108 people who had upper-extremity weakness after having a stroke at least 9 months before enrollment. The average for the group was 3 years post stroke after ischemic stroke,” said Jesse Dawson, MD, a professor at the University of Glasgow.
The Fifty-three patients were assigned active VNS followed by 6 weeks of in-clinic rehabilitation and then 90 days of home-based rehab. At in-clinic rehab, the therapist initiated a 5-second burst of VNS stimulation during each movement. In home-base treatment, the device was activated by a magnet.
Fifty-five patients were assigned sham VNS. After 90 days, the sham group crossed over to receive VNS for 6 weeks and then 90 days of home exercise. This crossover group was the focus of the data Dr. Dawson presented at AAN 2021. The overall trial results have been published in the Lancet.
“The hypothesis is based on the knowledge that the VNS stimulates the release of proneuroplastic neuromodulators norepinephrine and acetylcholine,” Dr. Dawson said. “By pairing VNS with task-specific movement, we hypothesize that we will increase task-specific neuroplasticity.”
The main study showed “a statistically significant difference across all primary and secondary endpoints at all time points in favor of rehabilitation paired with VNS,” Dr. Dawson said. The primary outcome was improvement in Fugl-Meyer Upper Extremity (FMA-UE) outcome, with the active VNS group having a significantly higher percentage of responders. For example, 47% of the active VNS patients had a greater than 6-point response on FMA-UE improvement versus 27% of the sham group (P = .010).
When the sham group crossed over to active VNS, the improvement in arm function matched that of the treatment group in the main study, Dr. Dawson said. “If you look at specifically what happened after they completed the control phase, there was a further small increase in Fugl-Meyer score, but, more importantly between 20% and 35% achieved a clinically important response on the Fugl-Meyer assessment or the Wolf Motor Function Test, giving a number need to treat ranging from three to five,” he said.
Dr. Dawson said that data on adverse events was presented in the Lancet publication. “These were observed at expected frequencies,” he said.
In an interview, he explained the significance of reporting the number to treat. “The number needed to treat helps give an idea of how many times you need to do something to achieve the desired outcome. So for VNS paired with rehab versus rehab alone, you need to treat four people to get one extra clinically important response, compared with just doing therapy.”
The next steps for his group’s research, he said, “will be to try and explore whether we can predict who responds best, and we would like to see if people with other types of stroke benefit.”
In providing comment on the study, Andreas Luft, MD, a professor at the University Hospital Zürich, noted that the FME-UE score improvements reported “are significant and meaningful. ... However, they may also be achieved by increasing the intensity of training. Many medical systems offer their patients high rehabilitation intensities and achieve similar improvements. Whether VNS can further boost higher-intensity training ‘beyond its limits’ is probable but remains to be demonstrated.”
Dr. Luft noted the study advances the knowledge of combining a therapeutic approach with training. “More such approaches are necessary to increase the therapeutic instrumentation of neurorehabilitation,” he said.
Dr. Dawson reported a financial relationship with MicroTransponder. His coauthors reported relationships with MicroTransponder, SanBio, Fujifilm Toyoma Chemical, Medtronic, TRCare, SAEBO, Allergan/AbbVie, Ipsen, Merz, Ottobock/Hangar Orthopedics, Parker Hannifin, Revance Therapeutics, ReWallk, and Sword Health. Three coauthors are employees of MicroTransponder. Dr. Luft has no relevant relationships to disclose.
according to preliminary results of a randomized clinical trial at the 2021 annual meeting of the American Academy of Neurology.
“We believe that vagus nerve stimulation combined with rehabilitation is an acceptable and effective intervention for improving upper-limb impairment and function in people with moderate to severe arm weakness a long time VNS-REHAB pivotal study is a randomized, blinded, controlled trial of 108 people who had upper-extremity weakness after having a stroke at least 9 months before enrollment. The average for the group was 3 years post stroke after ischemic stroke,” said Jesse Dawson, MD, a professor at the University of Glasgow.
The Fifty-three patients were assigned active VNS followed by 6 weeks of in-clinic rehabilitation and then 90 days of home-based rehab. At in-clinic rehab, the therapist initiated a 5-second burst of VNS stimulation during each movement. In home-base treatment, the device was activated by a magnet.
Fifty-five patients were assigned sham VNS. After 90 days, the sham group crossed over to receive VNS for 6 weeks and then 90 days of home exercise. This crossover group was the focus of the data Dr. Dawson presented at AAN 2021. The overall trial results have been published in the Lancet.
“The hypothesis is based on the knowledge that the VNS stimulates the release of proneuroplastic neuromodulators norepinephrine and acetylcholine,” Dr. Dawson said. “By pairing VNS with task-specific movement, we hypothesize that we will increase task-specific neuroplasticity.”
The main study showed “a statistically significant difference across all primary and secondary endpoints at all time points in favor of rehabilitation paired with VNS,” Dr. Dawson said. The primary outcome was improvement in Fugl-Meyer Upper Extremity (FMA-UE) outcome, with the active VNS group having a significantly higher percentage of responders. For example, 47% of the active VNS patients had a greater than 6-point response on FMA-UE improvement versus 27% of the sham group (P = .010).
When the sham group crossed over to active VNS, the improvement in arm function matched that of the treatment group in the main study, Dr. Dawson said. “If you look at specifically what happened after they completed the control phase, there was a further small increase in Fugl-Meyer score, but, more importantly between 20% and 35% achieved a clinically important response on the Fugl-Meyer assessment or the Wolf Motor Function Test, giving a number need to treat ranging from three to five,” he said.
Dr. Dawson said that data on adverse events was presented in the Lancet publication. “These were observed at expected frequencies,” he said.
In an interview, he explained the significance of reporting the number to treat. “The number needed to treat helps give an idea of how many times you need to do something to achieve the desired outcome. So for VNS paired with rehab versus rehab alone, you need to treat four people to get one extra clinically important response, compared with just doing therapy.”
The next steps for his group’s research, he said, “will be to try and explore whether we can predict who responds best, and we would like to see if people with other types of stroke benefit.”
In providing comment on the study, Andreas Luft, MD, a professor at the University Hospital Zürich, noted that the FME-UE score improvements reported “are significant and meaningful. ... However, they may also be achieved by increasing the intensity of training. Many medical systems offer their patients high rehabilitation intensities and achieve similar improvements. Whether VNS can further boost higher-intensity training ‘beyond its limits’ is probable but remains to be demonstrated.”
Dr. Luft noted the study advances the knowledge of combining a therapeutic approach with training. “More such approaches are necessary to increase the therapeutic instrumentation of neurorehabilitation,” he said.
Dr. Dawson reported a financial relationship with MicroTransponder. His coauthors reported relationships with MicroTransponder, SanBio, Fujifilm Toyoma Chemical, Medtronic, TRCare, SAEBO, Allergan/AbbVie, Ipsen, Merz, Ottobock/Hangar Orthopedics, Parker Hannifin, Revance Therapeutics, ReWallk, and Sword Health. Three coauthors are employees of MicroTransponder. Dr. Luft has no relevant relationships to disclose.
FROM AAN 2021
Head to Toe: Recommendations for Physician Head and Shoe Coverings to Limit COVID-19 Transmission
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
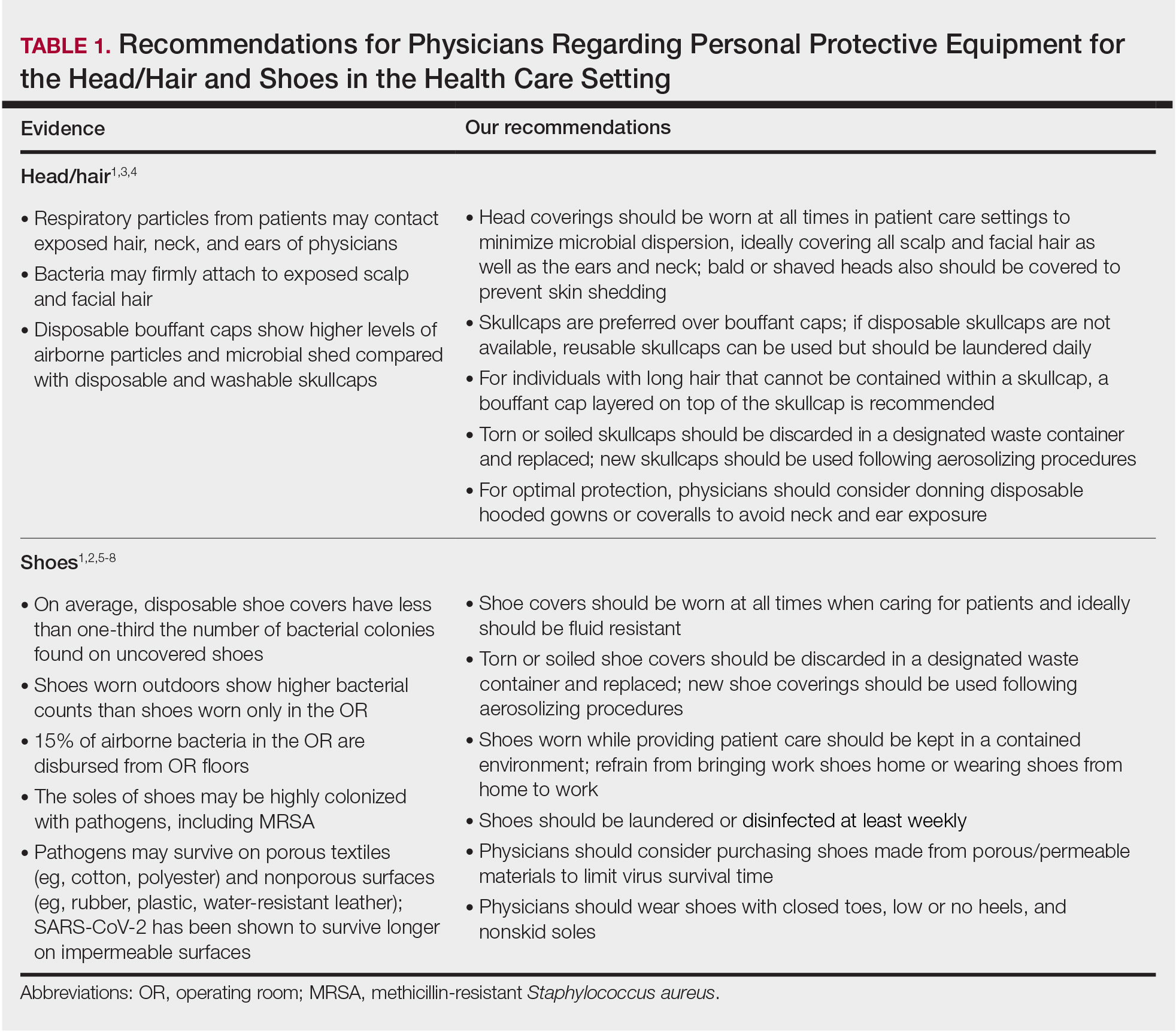
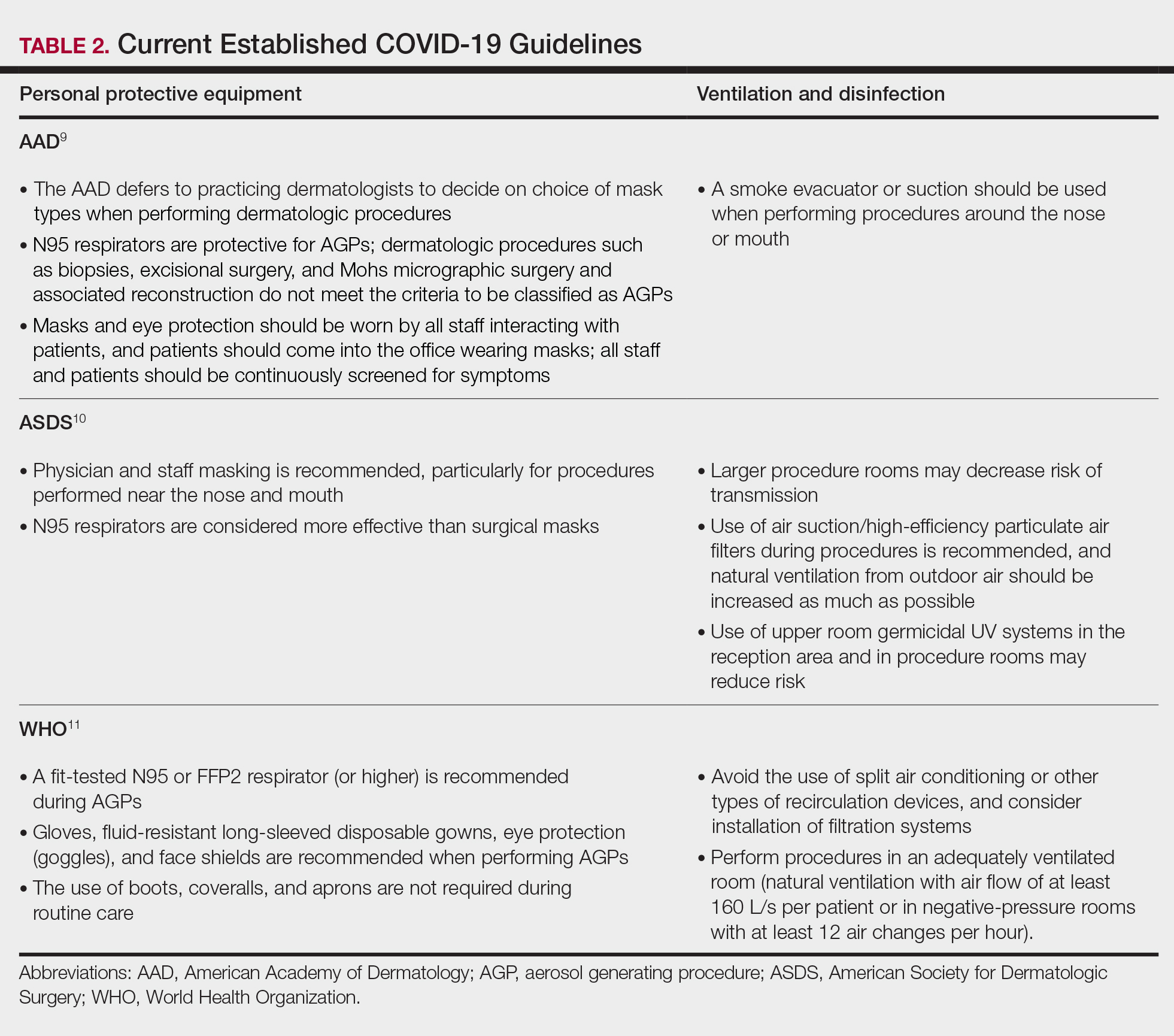
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Practice Points
- Consistent use of personal protective equipment, including masks, face shields, goggles, and gloves, may limit transmission of SARS-CoV-2.
- Hair and shoes also may transmit SARS-CoV-2, but recommendations for hair and shoe coverings to prevent SARS-CoV-2 are lacking.
Long-Distance Dermatology: Lessons From an Interview on Remote Practice During a Pandemic and Beyond
For the US health care system, the year 2020 was one of great change as well as extreme pain and hardship: some physical, but much emotional and financial. Dermatologists nationwide have not been sheltered from the winds of change. Yet as with most great challenges, one also can discern great change for the better if you look for it. One area of major growth in the wake of the COVID-19 pandemic is the expansion of telehealth, specifically teledermatology.
Prior to the pandemic, teledermatology was in a phase of modest expansion.1 Since the start of the pandemic, however, the adoption of telemedicine services in the United States has been beyond exponential. Before the pandemic, an estimated 15,000 Medicare recipients received telehealth services on a weekly basis. Yet by the end of April 2020, only 3 months after the first reported case of COVID-19 in the United States, nearly 1.3 million Medicare beneficiaries were utilizing telehealth services on a weekly basis.2 The Centers for Medicare & Medicaid Services has recognized the vast increase in need and responded with the addition of 144 new telehealth services covered by Medicare in the last year. In December 2020, the Centers for Medicare & Medicaid Services moved to make many of the previously provisional policies permanent, expanding long-term coverage for telehealth services,2 and use of teledermatology has expanded in parallel. Although the impetus for this change was simple necessity, the benefits of expanded teledermatology are likely to drive its continued incorporation into our daily practices.
Kevin Wright, MD, is a staff dermatologist at the Naval Medical Center San Diego (San Diego, California) and an Associate Professor of Dermatology at the Uniformed Services University of the Health Sciences (Bethesda, Maryland). In this interview, we discussed his experience incorporating a teledermatology component into his postresidency practice, the pros and cons of teledermatology practice, and ways that residents can prepare for a future in teledermatology.
Would you start by briefly describing your work model now?
My primary job is a Monday-through-Friday classic dermatology clinic job. On the weekends or days off, I see asynchronous and synchronous teledermatology through a specialized platform. On weekends, I tend to see anywhere between 20 and 40 patients in about a 6-hour period with breaks in between.
What does a typical “weekend” day of work look like?
In general, I’ll wake up early before my family and spend maybe an hour working. Oftentimes, that will be in my truck parked down by the beach, where I will go for a run or surf before logging on. If I have 40 visits scheduled that day, I can spend a few hours, message most of them, clarify some aspects of the visit, then go and have breakfast with my family before logging back on and completing the encounters.
Is most of your interaction with patients asynchronous, messaging back and forth to take history?
A few states require a phone call, so those are synchronous, and every Medicaid patient requires a video call. I do synchronous visits with all of my isotretinoin patients at first. It’s a mixed bag, but a lot of my visits are done entirely asynchronously.
What attracted you to this model?
During residency, I always felt that many of the ways we saw patients seemed extraordinarily inefficient. My best example of this is isotretinoin follow-ups. Before this year, most of my colleagues were uncomfortable with virtual isotretinoin follow-ups or thought it was a ridiculous idea. Frankly, I never shared this sentiment. Once I had my own board certification, I knew I was going to pursue teledermatology, because seeing kids take a half day off of school to come in for a 10-minute isotretinoin appointment (that’s mainly just a conversation about sports) just didn’t make sense to me. So I knew I wanted to pursue this idea, I just didn’t know exactly how. One day I was approached by a close friend and mentor of mine who had just purchased a teledermatology platform. She asked me if I would like to moonlight once I graduated and I jumped at the opportunity.
What steps did you take prior to graduating to help prepare you to practice teledermatology?
The most important thing I did—and the most important thing I think for third-year residents to do—is to set myself up for success by starting the US Drug Enforcement Administration (DEA) licensure and certification process. Once you have a DEA number, you can apply for Medicare and Medicaid. The nice thing about Medicare is you can start billing immediately after you apply, which is important. The reimbursement isn’t as high, but they pay faster, which allows you to start seeing patients through teledermatology right away. In a pinch, you could see all Medicare patients and make a living until you’ve completed the rest of the process. Once you have a Medicare and Medicaid number, you can apply for credentialing through private payers. However, the Medicare process takes 3 months, and private-payers credentialing takes about 90 days as well. That’s a lot of time! Before finishing residency, I recommend you make sure you have an unrestricted DEA license and you apply for Medicare/Medicaid credentials. Then, when you’re looking at future employment, you can start getting state licenses almost immediately in whatever states you anticipate needing them.
What are the top 3 benefits of incorporating teledermatology into your practice?
Accessibility is one huge benefit. If you’re practicing in a rural area, you’re basically giving [patients] back their time. Teledermatology takes patients much less time, and they get the same level of care. That’s a big selling point. Your patients will be very happy and loyal because of that.
The other thing I never would have foreseen before starting teledermatology is the amazing follow-up you can get. I think many dermatology residents will agree that there are those patients where you think, “Wow, I wish I could see them back. I wonder how they did,” but you never see them again. That’s not the case with teledermatology. I have a running list of all my interesting cases, and I’ll just shoot them a message 2 or 4 weeks later and at their convenience, they can submit a quick photo. I get that excellent feedback, and that’s huge to me for my own personal education and growth.
The third would be experience. I have 24 state medical licenses, and I see patients of all varieties: all socioeconomic backgrounds and skin types and many with severe skin conditions never managed before by a specialist. That, frankly, has increased my comfort level for seeing patients of all types. It forces me to expand my utilization of certain therapies because some people can’t afford 95% of medications we prescribe commonly. I find that challenge very rewarding. It’s something I’m not sure you can achieve by just practicing within your bubble. Inevitably you are going to see a certain type of patient that your hospital or practice attracts by merit of its geography or catchment area. Teledermatology allows you to see the full spectrum of dermatology.
What are the biggest cons to incorporating teledermatology into your practice?
To start off, some patients have boundary issues. Every 200 patients or so, I’ll have someone who submits a visit at 11:30
The second is reimbursement. In other practice models I can bill more in half the time by seeing a patient in person, doing a skin screening and a few biopsies. I believe there’s always a role for teledermatology in any practice, but ultimately dermatologists are pragmatic people who need to be smart about time management. At some point, it becomes difficult to pay the bills if reimbursement is lacking. That’s one of the bigger downsides to teledermatology. We still need to figure out how to reimburse to incentivize what’s best for the patient.
Could you talk more about the effect on work-life balance?
I think the things that make teledermatology appealing are the same things that could end up disrupting your work-life balance. On the positive side, you can vacation in Hawaii, work for 2 hours each morning, and pay for the whole thing. That’s very appealing to me! The downside is that there are always patients in the queue. In some sense, your waiting room is always half-full, 24/7. Mentally, you have to become comfortable with that, and you have to develop boundaries. I have very specific times I do teledermatology and then I log off. This helps me establish boundaries and creates balance.
You touched on it earlier regarding isotretinoin visits, but what other facets of practice do you think are particularly well-suited to teledermatology?
There are a few that I’ve incorporated into my practice quite aggressively. Almost all acne is going to go to a teledermatology visit. That’s in large part due to payer parity. For the most part, you make the same doing an acne visit online as you will doing it in person. Your patients will be getting the same level of care, better follow-up, and you’ll make the same amount of money. Another thing I do as a patient courtesy is wound checks postsurgery or post-Mohs [micrographic surgery]. There is a huge benefit there to seeing your patients because you can identify infections early, answer simple questions, and reduce in-person clinic visits. That’s a win.
What are visit types you feel are not well-suited to teledermatology or that you approach with more caution?
This will be different for everyone to some degree. I think practitioners need to be alert and use their best judgement when approaching any new patient or new concern. Pigmented lesions certainly give me pause. Although the technology is getting better every day, I believe there is still a gap between seeing a photo of a lesion and seeing a pigmented lesion in person, being able to get up close and examine it dermoscopically. Teledermoscopy, however, is an emerging business model as well, and it will be interesting to see what role this can play as it gets incorporated.
You mentioned having medical licenses in several states. Can you describe the process you went through to obtain these licenses?
It’s a painful process. I started realizing this was something I wanted to incorporate after residency, so I started looking into applying for medical licenses early. Teledermatology companies often will reimburse you and help you to get licenses. I was lucky enough to get assistance, which was essential because it is an onerous process. If you can work that into your contract during negotiations that would be ideal. Not everyone will be as lucky as I was, though. If that doesn’t pertain to you, pick a few states that have larger populations around you, where you know that they have a lot of need and start applying there. Be aware that medical licensure takes about 6 months. Having this started around mid–third year is important.
Employers want someone they can use right away, so I found it very beneficial to approach an employer and be able to explain to them tangibly where you are in the process. For example, “I’ve got my DEA license, Medicare, Medicaid number, and I have licensure in your state and all the surrounding states.” You then have a leg to stand on with your negotiating. If you do the legwork and can then negotiate a higher percentage, you’ll make up the licensure fees in a half day of work. It’s an investment toward your professional career.
Any final thoughts?
I think that insurers are very interested in teledermatology because there’s a potential for huge cost savings. As the dust settles with COVID-19 and we see how telemedicine has changed medicine in general, I really think that payers are going to be more aggressive about requiring teledermatology from their dermatologists. I think residents need to anticipate that teledermatology will be some part of their practice in the future and should start planning now to be prepared for this brave new world going forward.
- Yim KM, Florek AG, Oh DH, et al. Teledermatology in the United States: an update in a dynamic era. Telemed J E Health. 2018;24:691-697.
- Shatzkes MM, Borha EL. Permanent expansion of Medicare telehealth services. The National Law Review website. Published December 7, 2020. Accessed April 13, 2021. https://www.natlawreview.com/article/permanent-expansion-medicare-telehealth-services
For the US health care system, the year 2020 was one of great change as well as extreme pain and hardship: some physical, but much emotional and financial. Dermatologists nationwide have not been sheltered from the winds of change. Yet as with most great challenges, one also can discern great change for the better if you look for it. One area of major growth in the wake of the COVID-19 pandemic is the expansion of telehealth, specifically teledermatology.
Prior to the pandemic, teledermatology was in a phase of modest expansion.1 Since the start of the pandemic, however, the adoption of telemedicine services in the United States has been beyond exponential. Before the pandemic, an estimated 15,000 Medicare recipients received telehealth services on a weekly basis. Yet by the end of April 2020, only 3 months after the first reported case of COVID-19 in the United States, nearly 1.3 million Medicare beneficiaries were utilizing telehealth services on a weekly basis.2 The Centers for Medicare & Medicaid Services has recognized the vast increase in need and responded with the addition of 144 new telehealth services covered by Medicare in the last year. In December 2020, the Centers for Medicare & Medicaid Services moved to make many of the previously provisional policies permanent, expanding long-term coverage for telehealth services,2 and use of teledermatology has expanded in parallel. Although the impetus for this change was simple necessity, the benefits of expanded teledermatology are likely to drive its continued incorporation into our daily practices.
Kevin Wright, MD, is a staff dermatologist at the Naval Medical Center San Diego (San Diego, California) and an Associate Professor of Dermatology at the Uniformed Services University of the Health Sciences (Bethesda, Maryland). In this interview, we discussed his experience incorporating a teledermatology component into his postresidency practice, the pros and cons of teledermatology practice, and ways that residents can prepare for a future in teledermatology.
Would you start by briefly describing your work model now?
My primary job is a Monday-through-Friday classic dermatology clinic job. On the weekends or days off, I see asynchronous and synchronous teledermatology through a specialized platform. On weekends, I tend to see anywhere between 20 and 40 patients in about a 6-hour period with breaks in between.
What does a typical “weekend” day of work look like?
In general, I’ll wake up early before my family and spend maybe an hour working. Oftentimes, that will be in my truck parked down by the beach, where I will go for a run or surf before logging on. If I have 40 visits scheduled that day, I can spend a few hours, message most of them, clarify some aspects of the visit, then go and have breakfast with my family before logging back on and completing the encounters.
Is most of your interaction with patients asynchronous, messaging back and forth to take history?
A few states require a phone call, so those are synchronous, and every Medicaid patient requires a video call. I do synchronous visits with all of my isotretinoin patients at first. It’s a mixed bag, but a lot of my visits are done entirely asynchronously.
What attracted you to this model?
During residency, I always felt that many of the ways we saw patients seemed extraordinarily inefficient. My best example of this is isotretinoin follow-ups. Before this year, most of my colleagues were uncomfortable with virtual isotretinoin follow-ups or thought it was a ridiculous idea. Frankly, I never shared this sentiment. Once I had my own board certification, I knew I was going to pursue teledermatology, because seeing kids take a half day off of school to come in for a 10-minute isotretinoin appointment (that’s mainly just a conversation about sports) just didn’t make sense to me. So I knew I wanted to pursue this idea, I just didn’t know exactly how. One day I was approached by a close friend and mentor of mine who had just purchased a teledermatology platform. She asked me if I would like to moonlight once I graduated and I jumped at the opportunity.
What steps did you take prior to graduating to help prepare you to practice teledermatology?
The most important thing I did—and the most important thing I think for third-year residents to do—is to set myself up for success by starting the US Drug Enforcement Administration (DEA) licensure and certification process. Once you have a DEA number, you can apply for Medicare and Medicaid. The nice thing about Medicare is you can start billing immediately after you apply, which is important. The reimbursement isn’t as high, but they pay faster, which allows you to start seeing patients through teledermatology right away. In a pinch, you could see all Medicare patients and make a living until you’ve completed the rest of the process. Once you have a Medicare and Medicaid number, you can apply for credentialing through private payers. However, the Medicare process takes 3 months, and private-payers credentialing takes about 90 days as well. That’s a lot of time! Before finishing residency, I recommend you make sure you have an unrestricted DEA license and you apply for Medicare/Medicaid credentials. Then, when you’re looking at future employment, you can start getting state licenses almost immediately in whatever states you anticipate needing them.
What are the top 3 benefits of incorporating teledermatology into your practice?
Accessibility is one huge benefit. If you’re practicing in a rural area, you’re basically giving [patients] back their time. Teledermatology takes patients much less time, and they get the same level of care. That’s a big selling point. Your patients will be very happy and loyal because of that.
The other thing I never would have foreseen before starting teledermatology is the amazing follow-up you can get. I think many dermatology residents will agree that there are those patients where you think, “Wow, I wish I could see them back. I wonder how they did,” but you never see them again. That’s not the case with teledermatology. I have a running list of all my interesting cases, and I’ll just shoot them a message 2 or 4 weeks later and at their convenience, they can submit a quick photo. I get that excellent feedback, and that’s huge to me for my own personal education and growth.
The third would be experience. I have 24 state medical licenses, and I see patients of all varieties: all socioeconomic backgrounds and skin types and many with severe skin conditions never managed before by a specialist. That, frankly, has increased my comfort level for seeing patients of all types. It forces me to expand my utilization of certain therapies because some people can’t afford 95% of medications we prescribe commonly. I find that challenge very rewarding. It’s something I’m not sure you can achieve by just practicing within your bubble. Inevitably you are going to see a certain type of patient that your hospital or practice attracts by merit of its geography or catchment area. Teledermatology allows you to see the full spectrum of dermatology.
What are the biggest cons to incorporating teledermatology into your practice?
To start off, some patients have boundary issues. Every 200 patients or so, I’ll have someone who submits a visit at 11:30
The second is reimbursement. In other practice models I can bill more in half the time by seeing a patient in person, doing a skin screening and a few biopsies. I believe there’s always a role for teledermatology in any practice, but ultimately dermatologists are pragmatic people who need to be smart about time management. At some point, it becomes difficult to pay the bills if reimbursement is lacking. That’s one of the bigger downsides to teledermatology. We still need to figure out how to reimburse to incentivize what’s best for the patient.
Could you talk more about the effect on work-life balance?
I think the things that make teledermatology appealing are the same things that could end up disrupting your work-life balance. On the positive side, you can vacation in Hawaii, work for 2 hours each morning, and pay for the whole thing. That’s very appealing to me! The downside is that there are always patients in the queue. In some sense, your waiting room is always half-full, 24/7. Mentally, you have to become comfortable with that, and you have to develop boundaries. I have very specific times I do teledermatology and then I log off. This helps me establish boundaries and creates balance.
You touched on it earlier regarding isotretinoin visits, but what other facets of practice do you think are particularly well-suited to teledermatology?
There are a few that I’ve incorporated into my practice quite aggressively. Almost all acne is going to go to a teledermatology visit. That’s in large part due to payer parity. For the most part, you make the same doing an acne visit online as you will doing it in person. Your patients will be getting the same level of care, better follow-up, and you’ll make the same amount of money. Another thing I do as a patient courtesy is wound checks postsurgery or post-Mohs [micrographic surgery]. There is a huge benefit there to seeing your patients because you can identify infections early, answer simple questions, and reduce in-person clinic visits. That’s a win.
What are visit types you feel are not well-suited to teledermatology or that you approach with more caution?
This will be different for everyone to some degree. I think practitioners need to be alert and use their best judgement when approaching any new patient or new concern. Pigmented lesions certainly give me pause. Although the technology is getting better every day, I believe there is still a gap between seeing a photo of a lesion and seeing a pigmented lesion in person, being able to get up close and examine it dermoscopically. Teledermoscopy, however, is an emerging business model as well, and it will be interesting to see what role this can play as it gets incorporated.
You mentioned having medical licenses in several states. Can you describe the process you went through to obtain these licenses?
It’s a painful process. I started realizing this was something I wanted to incorporate after residency, so I started looking into applying for medical licenses early. Teledermatology companies often will reimburse you and help you to get licenses. I was lucky enough to get assistance, which was essential because it is an onerous process. If you can work that into your contract during negotiations that would be ideal. Not everyone will be as lucky as I was, though. If that doesn’t pertain to you, pick a few states that have larger populations around you, where you know that they have a lot of need and start applying there. Be aware that medical licensure takes about 6 months. Having this started around mid–third year is important.
Employers want someone they can use right away, so I found it very beneficial to approach an employer and be able to explain to them tangibly where you are in the process. For example, “I’ve got my DEA license, Medicare, Medicaid number, and I have licensure in your state and all the surrounding states.” You then have a leg to stand on with your negotiating. If you do the legwork and can then negotiate a higher percentage, you’ll make up the licensure fees in a half day of work. It’s an investment toward your professional career.
Any final thoughts?
I think that insurers are very interested in teledermatology because there’s a potential for huge cost savings. As the dust settles with COVID-19 and we see how telemedicine has changed medicine in general, I really think that payers are going to be more aggressive about requiring teledermatology from their dermatologists. I think residents need to anticipate that teledermatology will be some part of their practice in the future and should start planning now to be prepared for this brave new world going forward.
For the US health care system, the year 2020 was one of great change as well as extreme pain and hardship: some physical, but much emotional and financial. Dermatologists nationwide have not been sheltered from the winds of change. Yet as with most great challenges, one also can discern great change for the better if you look for it. One area of major growth in the wake of the COVID-19 pandemic is the expansion of telehealth, specifically teledermatology.
Prior to the pandemic, teledermatology was in a phase of modest expansion.1 Since the start of the pandemic, however, the adoption of telemedicine services in the United States has been beyond exponential. Before the pandemic, an estimated 15,000 Medicare recipients received telehealth services on a weekly basis. Yet by the end of April 2020, only 3 months after the first reported case of COVID-19 in the United States, nearly 1.3 million Medicare beneficiaries were utilizing telehealth services on a weekly basis.2 The Centers for Medicare & Medicaid Services has recognized the vast increase in need and responded with the addition of 144 new telehealth services covered by Medicare in the last year. In December 2020, the Centers for Medicare & Medicaid Services moved to make many of the previously provisional policies permanent, expanding long-term coverage for telehealth services,2 and use of teledermatology has expanded in parallel. Although the impetus for this change was simple necessity, the benefits of expanded teledermatology are likely to drive its continued incorporation into our daily practices.
Kevin Wright, MD, is a staff dermatologist at the Naval Medical Center San Diego (San Diego, California) and an Associate Professor of Dermatology at the Uniformed Services University of the Health Sciences (Bethesda, Maryland). In this interview, we discussed his experience incorporating a teledermatology component into his postresidency practice, the pros and cons of teledermatology practice, and ways that residents can prepare for a future in teledermatology.
Would you start by briefly describing your work model now?
My primary job is a Monday-through-Friday classic dermatology clinic job. On the weekends or days off, I see asynchronous and synchronous teledermatology through a specialized platform. On weekends, I tend to see anywhere between 20 and 40 patients in about a 6-hour period with breaks in between.
What does a typical “weekend” day of work look like?
In general, I’ll wake up early before my family and spend maybe an hour working. Oftentimes, that will be in my truck parked down by the beach, where I will go for a run or surf before logging on. If I have 40 visits scheduled that day, I can spend a few hours, message most of them, clarify some aspects of the visit, then go and have breakfast with my family before logging back on and completing the encounters.
Is most of your interaction with patients asynchronous, messaging back and forth to take history?
A few states require a phone call, so those are synchronous, and every Medicaid patient requires a video call. I do synchronous visits with all of my isotretinoin patients at first. It’s a mixed bag, but a lot of my visits are done entirely asynchronously.
What attracted you to this model?
During residency, I always felt that many of the ways we saw patients seemed extraordinarily inefficient. My best example of this is isotretinoin follow-ups. Before this year, most of my colleagues were uncomfortable with virtual isotretinoin follow-ups or thought it was a ridiculous idea. Frankly, I never shared this sentiment. Once I had my own board certification, I knew I was going to pursue teledermatology, because seeing kids take a half day off of school to come in for a 10-minute isotretinoin appointment (that’s mainly just a conversation about sports) just didn’t make sense to me. So I knew I wanted to pursue this idea, I just didn’t know exactly how. One day I was approached by a close friend and mentor of mine who had just purchased a teledermatology platform. She asked me if I would like to moonlight once I graduated and I jumped at the opportunity.
What steps did you take prior to graduating to help prepare you to practice teledermatology?
The most important thing I did—and the most important thing I think for third-year residents to do—is to set myself up for success by starting the US Drug Enforcement Administration (DEA) licensure and certification process. Once you have a DEA number, you can apply for Medicare and Medicaid. The nice thing about Medicare is you can start billing immediately after you apply, which is important. The reimbursement isn’t as high, but they pay faster, which allows you to start seeing patients through teledermatology right away. In a pinch, you could see all Medicare patients and make a living until you’ve completed the rest of the process. Once you have a Medicare and Medicaid number, you can apply for credentialing through private payers. However, the Medicare process takes 3 months, and private-payers credentialing takes about 90 days as well. That’s a lot of time! Before finishing residency, I recommend you make sure you have an unrestricted DEA license and you apply for Medicare/Medicaid credentials. Then, when you’re looking at future employment, you can start getting state licenses almost immediately in whatever states you anticipate needing them.
What are the top 3 benefits of incorporating teledermatology into your practice?
Accessibility is one huge benefit. If you’re practicing in a rural area, you’re basically giving [patients] back their time. Teledermatology takes patients much less time, and they get the same level of care. That’s a big selling point. Your patients will be very happy and loyal because of that.
The other thing I never would have foreseen before starting teledermatology is the amazing follow-up you can get. I think many dermatology residents will agree that there are those patients where you think, “Wow, I wish I could see them back. I wonder how they did,” but you never see them again. That’s not the case with teledermatology. I have a running list of all my interesting cases, and I’ll just shoot them a message 2 or 4 weeks later and at their convenience, they can submit a quick photo. I get that excellent feedback, and that’s huge to me for my own personal education and growth.
The third would be experience. I have 24 state medical licenses, and I see patients of all varieties: all socioeconomic backgrounds and skin types and many with severe skin conditions never managed before by a specialist. That, frankly, has increased my comfort level for seeing patients of all types. It forces me to expand my utilization of certain therapies because some people can’t afford 95% of medications we prescribe commonly. I find that challenge very rewarding. It’s something I’m not sure you can achieve by just practicing within your bubble. Inevitably you are going to see a certain type of patient that your hospital or practice attracts by merit of its geography or catchment area. Teledermatology allows you to see the full spectrum of dermatology.
What are the biggest cons to incorporating teledermatology into your practice?
To start off, some patients have boundary issues. Every 200 patients or so, I’ll have someone who submits a visit at 11:30
The second is reimbursement. In other practice models I can bill more in half the time by seeing a patient in person, doing a skin screening and a few biopsies. I believe there’s always a role for teledermatology in any practice, but ultimately dermatologists are pragmatic people who need to be smart about time management. At some point, it becomes difficult to pay the bills if reimbursement is lacking. That’s one of the bigger downsides to teledermatology. We still need to figure out how to reimburse to incentivize what’s best for the patient.
Could you talk more about the effect on work-life balance?
I think the things that make teledermatology appealing are the same things that could end up disrupting your work-life balance. On the positive side, you can vacation in Hawaii, work for 2 hours each morning, and pay for the whole thing. That’s very appealing to me! The downside is that there are always patients in the queue. In some sense, your waiting room is always half-full, 24/7. Mentally, you have to become comfortable with that, and you have to develop boundaries. I have very specific times I do teledermatology and then I log off. This helps me establish boundaries and creates balance.
You touched on it earlier regarding isotretinoin visits, but what other facets of practice do you think are particularly well-suited to teledermatology?
There are a few that I’ve incorporated into my practice quite aggressively. Almost all acne is going to go to a teledermatology visit. That’s in large part due to payer parity. For the most part, you make the same doing an acne visit online as you will doing it in person. Your patients will be getting the same level of care, better follow-up, and you’ll make the same amount of money. Another thing I do as a patient courtesy is wound checks postsurgery or post-Mohs [micrographic surgery]. There is a huge benefit there to seeing your patients because you can identify infections early, answer simple questions, and reduce in-person clinic visits. That’s a win.
What are visit types you feel are not well-suited to teledermatology or that you approach with more caution?
This will be different for everyone to some degree. I think practitioners need to be alert and use their best judgement when approaching any new patient or new concern. Pigmented lesions certainly give me pause. Although the technology is getting better every day, I believe there is still a gap between seeing a photo of a lesion and seeing a pigmented lesion in person, being able to get up close and examine it dermoscopically. Teledermoscopy, however, is an emerging business model as well, and it will be interesting to see what role this can play as it gets incorporated.
You mentioned having medical licenses in several states. Can you describe the process you went through to obtain these licenses?
It’s a painful process. I started realizing this was something I wanted to incorporate after residency, so I started looking into applying for medical licenses early. Teledermatology companies often will reimburse you and help you to get licenses. I was lucky enough to get assistance, which was essential because it is an onerous process. If you can work that into your contract during negotiations that would be ideal. Not everyone will be as lucky as I was, though. If that doesn’t pertain to you, pick a few states that have larger populations around you, where you know that they have a lot of need and start applying there. Be aware that medical licensure takes about 6 months. Having this started around mid–third year is important.
Employers want someone they can use right away, so I found it very beneficial to approach an employer and be able to explain to them tangibly where you are in the process. For example, “I’ve got my DEA license, Medicare, Medicaid number, and I have licensure in your state and all the surrounding states.” You then have a leg to stand on with your negotiating. If you do the legwork and can then negotiate a higher percentage, you’ll make up the licensure fees in a half day of work. It’s an investment toward your professional career.
Any final thoughts?
I think that insurers are very interested in teledermatology because there’s a potential for huge cost savings. As the dust settles with COVID-19 and we see how telemedicine has changed medicine in general, I really think that payers are going to be more aggressive about requiring teledermatology from their dermatologists. I think residents need to anticipate that teledermatology will be some part of their practice in the future and should start planning now to be prepared for this brave new world going forward.
- Yim KM, Florek AG, Oh DH, et al. Teledermatology in the United States: an update in a dynamic era. Telemed J E Health. 2018;24:691-697.
- Shatzkes MM, Borha EL. Permanent expansion of Medicare telehealth services. The National Law Review website. Published December 7, 2020. Accessed April 13, 2021. https://www.natlawreview.com/article/permanent-expansion-medicare-telehealth-services
- Yim KM, Florek AG, Oh DH, et al. Teledermatology in the United States: an update in a dynamic era. Telemed J E Health. 2018;24:691-697.
- Shatzkes MM, Borha EL. Permanent expansion of Medicare telehealth services. The National Law Review website. Published December 7, 2020. Accessed April 13, 2021. https://www.natlawreview.com/article/permanent-expansion-medicare-telehealth-services
Resident Pearl
- One result of the COVID-19 pandemic is the aggressive adoption of teledermatology across the United States. Graduating residents should be preparing for a scope of practice that incorporates teledermatology.

Diagnostic tests may miss invasive aspergillosis in children
Key clinical point: The small number of invasive aspergillosis cases may contribute to the low specificity of several tests in children after stem cell transplants and should be interpreted with caution.
Major finding: The sensitivity and specificity for probable invasive aspergillosis and potential invasive fungal disease was 80% and 55% for (1→3)-β-D-glucan (BDG); 40% and 100% for galactomannan; and 60% (and 95% (95% CI: 75–100%) for Aspergillus-specific real-time PCR.
Study details: The data come from 404 blood samples taken from 26 pediatric patients who underwent allogeneic hematopoietic stem cell transplantation between April 2016 and March 2018 at a single center.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Springer J et al. J Fungi (Basel). 2021 Mar 22. doi: 10.3390/jof7030238.
Key clinical point: The small number of invasive aspergillosis cases may contribute to the low specificity of several tests in children after stem cell transplants and should be interpreted with caution.
Major finding: The sensitivity and specificity for probable invasive aspergillosis and potential invasive fungal disease was 80% and 55% for (1→3)-β-D-glucan (BDG); 40% and 100% for galactomannan; and 60% (and 95% (95% CI: 75–100%) for Aspergillus-specific real-time PCR.
Study details: The data come from 404 blood samples taken from 26 pediatric patients who underwent allogeneic hematopoietic stem cell transplantation between April 2016 and March 2018 at a single center.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Springer J et al. J Fungi (Basel). 2021 Mar 22. doi: 10.3390/jof7030238.
Key clinical point: The small number of invasive aspergillosis cases may contribute to the low specificity of several tests in children after stem cell transplants and should be interpreted with caution.
Major finding: The sensitivity and specificity for probable invasive aspergillosis and potential invasive fungal disease was 80% and 55% for (1→3)-β-D-glucan (BDG); 40% and 100% for galactomannan; and 60% (and 95% (95% CI: 75–100%) for Aspergillus-specific real-time PCR.
Study details: The data come from 404 blood samples taken from 26 pediatric patients who underwent allogeneic hematopoietic stem cell transplantation between April 2016 and March 2018 at a single center.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Springer J et al. J Fungi (Basel). 2021 Mar 22. doi: 10.3390/jof7030238.
Coinfections raise mortality rates in COVID-19 patients
Key clinical point: Patients with severe COVID-19 and secondary coinfections had higher mortality rates and longer hospital stays compared to patients without secondary infections.
Major finding: The overall mortality rate was approximately 50%, but 83.14% of the patients with fungal or bacterial isolation died. The risk of death was significantly higher in patients with bacterial and fungal coinfections (odds ratios 11.28 and 5.97, respectively).
Study details: The data come from an analysis of 212 severely ill patients with COVID-19; 89 of these had fungal or bacterial secondary coinfections.
Disclosures: The study was supported by the Fundação de Amparo a Pesquisa do Estado de Minas Gerais - FAPEMIG and the Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq and Brazilian Ministry of Health. The researchers had no financial conflicts to disclose.
Source: Silva DL et al. J Hosp Infect. 2021 Apr 11. doi: 10.1016/j.jhin.2021.04.001.
Key clinical point: Patients with severe COVID-19 and secondary coinfections had higher mortality rates and longer hospital stays compared to patients without secondary infections.
Major finding: The overall mortality rate was approximately 50%, but 83.14% of the patients with fungal or bacterial isolation died. The risk of death was significantly higher in patients with bacterial and fungal coinfections (odds ratios 11.28 and 5.97, respectively).
Study details: The data come from an analysis of 212 severely ill patients with COVID-19; 89 of these had fungal or bacterial secondary coinfections.
Disclosures: The study was supported by the Fundação de Amparo a Pesquisa do Estado de Minas Gerais - FAPEMIG and the Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq and Brazilian Ministry of Health. The researchers had no financial conflicts to disclose.
Source: Silva DL et al. J Hosp Infect. 2021 Apr 11. doi: 10.1016/j.jhin.2021.04.001.
Key clinical point: Patients with severe COVID-19 and secondary coinfections had higher mortality rates and longer hospital stays compared to patients without secondary infections.
Major finding: The overall mortality rate was approximately 50%, but 83.14% of the patients with fungal or bacterial isolation died. The risk of death was significantly higher in patients with bacterial and fungal coinfections (odds ratios 11.28 and 5.97, respectively).
Study details: The data come from an analysis of 212 severely ill patients with COVID-19; 89 of these had fungal or bacterial secondary coinfections.
Disclosures: The study was supported by the Fundação de Amparo a Pesquisa do Estado de Minas Gerais - FAPEMIG and the Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq and Brazilian Ministry of Health. The researchers had no financial conflicts to disclose.
Source: Silva DL et al. J Hosp Infect. 2021 Apr 11. doi: 10.1016/j.jhin.2021.04.001.
Posaconazole posts strong results against invasive fungal infections in cancer patients
Key clinical point: Triazole antifungal agents, as well as amphotericin B and caspofungin, reduced rates of invasive fungal infections in patients with hematological malginancies; notably, posaconazole also was more effective at reducing all-cause mortality and adverse events compared with other triazoles.
Major finding: Posaconazole was superior to fluconazole (odds ratio 0.30), itraconazole (OR 0.40), and amphotericin B (OR 4.97) in reducing the incidence of both suspected and confirmed invasive fungal infections.
Study details: The data come from a meta-analysis of 35 studies including 37 randomized, controlled trials of the effectiveness of triazoles, polyene, and echinocandin antifungals for infection control in patients with hematological malignancies.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Zeng H et al. BMC Cancer. 2021 Apr 14. doi: 10.1186/s12885-021-07973-8.
Key clinical point: Triazole antifungal agents, as well as amphotericin B and caspofungin, reduced rates of invasive fungal infections in patients with hematological malginancies; notably, posaconazole also was more effective at reducing all-cause mortality and adverse events compared with other triazoles.
Major finding: Posaconazole was superior to fluconazole (odds ratio 0.30), itraconazole (OR 0.40), and amphotericin B (OR 4.97) in reducing the incidence of both suspected and confirmed invasive fungal infections.
Study details: The data come from a meta-analysis of 35 studies including 37 randomized, controlled trials of the effectiveness of triazoles, polyene, and echinocandin antifungals for infection control in patients with hematological malignancies.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Zeng H et al. BMC Cancer. 2021 Apr 14. doi: 10.1186/s12885-021-07973-8.
Key clinical point: Triazole antifungal agents, as well as amphotericin B and caspofungin, reduced rates of invasive fungal infections in patients with hematological malginancies; notably, posaconazole also was more effective at reducing all-cause mortality and adverse events compared with other triazoles.
Major finding: Posaconazole was superior to fluconazole (odds ratio 0.30), itraconazole (OR 0.40), and amphotericin B (OR 4.97) in reducing the incidence of both suspected and confirmed invasive fungal infections.
Study details: The data come from a meta-analysis of 35 studies including 37 randomized, controlled trials of the effectiveness of triazoles, polyene, and echinocandin antifungals for infection control in patients with hematological malignancies.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Zeng H et al. BMC Cancer. 2021 Apr 14. doi: 10.1186/s12885-021-07973-8.