User login
New ustekinumab response predictor in Crohn’s called ‘brilliant’
SAN ANTONIO – The probability of achieving clinical remission of Crohn’s disease in response to ustekinumab can now be readily estimated by using a clinical prediction tool, Parambir S. Dulai, MBBS, announced at the annual meeting of the American College of Gastroenterology.

This new clinical decision support tool also provides individualized stratification of the rapidity with which symptoms will be reduced in response to the anti-interleukin-12/23 biologic, added Dr. Dulai, a gastroenterologist at the University of California, San Diego.
He and his coinvestigators developed the prediction tool through analysis of detailed data on 781 patients with active Crohn’s disease treated with ustekinumab (Stelara) during both the induction and maintenance portions of the phase 3 UNITI randomized trials conducted in the biologic’s development program. The researchers identified a series of baseline features associated with clinical remission as defined by a Crohn’s Disease Activity Index (CDAI) score below 150 by week 16 of treatment. Through statistical manipulation, they transformed the data into a predictive model and then went one step further by turning the model into a decision support tool with points given for the individual predictive variables (see graphic).
Patients with 5 or more total points were categorized as having a high probability of week-16 clinical remission. Patients with 0 or 1 point were deemed low probability, and a score of 2-4 indicated an intermediate likelihood of clinical remission.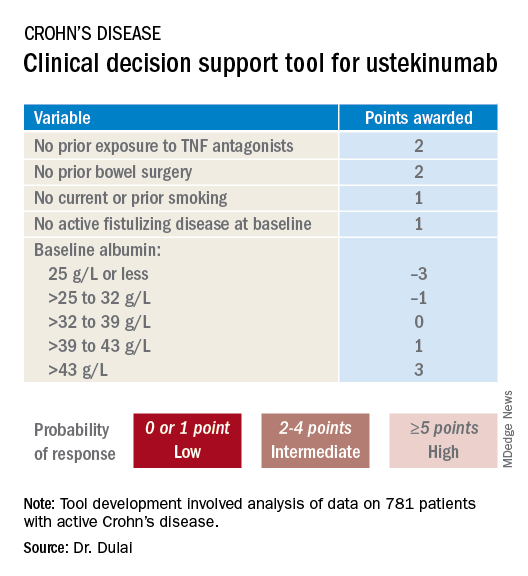
Next, the investigators applied their new clinical decision support tool to the 781 ustekinumab-treated patients included in the derivation analysis. The tool performed well: The high-probability group had a 57% clinical remission rate, significantly better than the 34% rate in the intermediate-probability group, which in turn was significantly better than the 21% rate of clinical remission in the group with a baseline score of 0 or 1.
In addition, onset of treatment benefit was significantly faster in the group having a score of 5 or more. They had a significantly higher clinical remission rate than the intermediate- and low-probability groups at all scheduled assessments, which were conducted at weeks 3, 6, 8, and 16. Indeed, by week 3 the high-probability group experienced a mean 69-point drop from baseline in CDAI and a 94-point drop by week 8, as compared with week-8 reductions of 54 and 40 points in the intermediate- and low-probability groups, respectively.
In an exploratory analysis involving the 122 patients who underwent week-8 endoscopy, endoscopic remission was documented in 12% of patients whose baseline scores placed them in the high-probability group, 10% in the intermediate group, and 8% of those in the low-probability group.
The high-probability group had significantly higher ustekinumab trough concentrations than did the intermediate- and low-probability groups when measured at weeks 3, 6, 8, and 16.
An external validation study conducted in a large cohort of Crohn’s disease patients seen in routine clinical practice has recently been completed, with the results now being analyzed, according to Dr. Dulai.
Miguel Requeiro, MD, chairman of gastroenterology and hepatology at the Cleveland Clinic, rose from the audience to declare the creation of the decision support tool to be “brilliant work.” He asked if it has changed clinical practice for Dr. Dulai and his coworkers.
“We’ve begun doing two things differently,” Dr. Dulai replied. “First, we’ve built a similar model for vedolizumab and Crohn’s. That means we can use both tools together to discriminate between a patient who should get vedolizumab versus ustekinumab because the variables and their weighting differ between the two. And the other thing we’ve been able to do is argue with payers for positioning of the treatments when we have evidence to support that we can use them earlier in the treatment course to optimize outcomes.”
Another audience member, David T. Rubin, MD, also praised the decision support tool as “brilliant” and “definitely needed.”
“Thank you for hitting the sweet spot of what we’ve all been waiting for,” added Dr. Rubin, professor of medicine and codirector of the Digestive Diseases Center at the University of Chicago.
Dr. Dulai reported receiving a research grant for the project from Janssen, which markets ustekinumab.
SAN ANTONIO – The probability of achieving clinical remission of Crohn’s disease in response to ustekinumab can now be readily estimated by using a clinical prediction tool, Parambir S. Dulai, MBBS, announced at the annual meeting of the American College of Gastroenterology.
This new clinical decision support tool also provides individualized stratification of the rapidity with which symptoms will be reduced in response to the anti-interleukin-12/23 biologic, added Dr. Dulai, a gastroenterologist at the University of California, San Diego.
He and his coinvestigators developed the prediction tool through analysis of detailed data on 781 patients with active Crohn’s disease treated with ustekinumab (Stelara) during both the induction and maintenance portions of the phase 3 UNITI randomized trials conducted in the biologic’s development program. The researchers identified a series of baseline features associated with clinical remission as defined by a Crohn’s Disease Activity Index (CDAI) score below 150 by week 16 of treatment. Through statistical manipulation, they transformed the data into a predictive model and then went one step further by turning the model into a decision support tool with points given for the individual predictive variables (see graphic).
Patients with 5 or more total points were categorized as having a high probability of week-16 clinical remission. Patients with 0 or 1 point were deemed low probability, and a score of 2-4 indicated an intermediate likelihood of clinical remission.
Next, the investigators applied their new clinical decision support tool to the 781 ustekinumab-treated patients included in the derivation analysis. The tool performed well: The high-probability group had a 57% clinical remission rate, significantly better than the 34% rate in the intermediate-probability group, which in turn was significantly better than the 21% rate of clinical remission in the group with a baseline score of 0 or 1.
In addition, onset of treatment benefit was significantly faster in the group having a score of 5 or more. They had a significantly higher clinical remission rate than the intermediate- and low-probability groups at all scheduled assessments, which were conducted at weeks 3, 6, 8, and 16. Indeed, by week 3 the high-probability group experienced a mean 69-point drop from baseline in CDAI and a 94-point drop by week 8, as compared with week-8 reductions of 54 and 40 points in the intermediate- and low-probability groups, respectively.
In an exploratory analysis involving the 122 patients who underwent week-8 endoscopy, endoscopic remission was documented in 12% of patients whose baseline scores placed them in the high-probability group, 10% in the intermediate group, and 8% of those in the low-probability group.
The high-probability group had significantly higher ustekinumab trough concentrations than did the intermediate- and low-probability groups when measured at weeks 3, 6, 8, and 16.
An external validation study conducted in a large cohort of Crohn’s disease patients seen in routine clinical practice has recently been completed, with the results now being analyzed, according to Dr. Dulai.
Miguel Requeiro, MD, chairman of gastroenterology and hepatology at the Cleveland Clinic, rose from the audience to declare the creation of the decision support tool to be “brilliant work.” He asked if it has changed clinical practice for Dr. Dulai and his coworkers.
“We’ve begun doing two things differently,” Dr. Dulai replied. “First, we’ve built a similar model for vedolizumab and Crohn’s. That means we can use both tools together to discriminate between a patient who should get vedolizumab versus ustekinumab because the variables and their weighting differ between the two. And the other thing we’ve been able to do is argue with payers for positioning of the treatments when we have evidence to support that we can use them earlier in the treatment course to optimize outcomes.”
Another audience member, David T. Rubin, MD, also praised the decision support tool as “brilliant” and “definitely needed.”
“Thank you for hitting the sweet spot of what we’ve all been waiting for,” added Dr. Rubin, professor of medicine and codirector of the Digestive Diseases Center at the University of Chicago.
Dr. Dulai reported receiving a research grant for the project from Janssen, which markets ustekinumab.
SAN ANTONIO – The probability of achieving clinical remission of Crohn’s disease in response to ustekinumab can now be readily estimated by using a clinical prediction tool, Parambir S. Dulai, MBBS, announced at the annual meeting of the American College of Gastroenterology.
This new clinical decision support tool also provides individualized stratification of the rapidity with which symptoms will be reduced in response to the anti-interleukin-12/23 biologic, added Dr. Dulai, a gastroenterologist at the University of California, San Diego.
He and his coinvestigators developed the prediction tool through analysis of detailed data on 781 patients with active Crohn’s disease treated with ustekinumab (Stelara) during both the induction and maintenance portions of the phase 3 UNITI randomized trials conducted in the biologic’s development program. The researchers identified a series of baseline features associated with clinical remission as defined by a Crohn’s Disease Activity Index (CDAI) score below 150 by week 16 of treatment. Through statistical manipulation, they transformed the data into a predictive model and then went one step further by turning the model into a decision support tool with points given for the individual predictive variables (see graphic).
Patients with 5 or more total points were categorized as having a high probability of week-16 clinical remission. Patients with 0 or 1 point were deemed low probability, and a score of 2-4 indicated an intermediate likelihood of clinical remission.
Next, the investigators applied their new clinical decision support tool to the 781 ustekinumab-treated patients included in the derivation analysis. The tool performed well: The high-probability group had a 57% clinical remission rate, significantly better than the 34% rate in the intermediate-probability group, which in turn was significantly better than the 21% rate of clinical remission in the group with a baseline score of 0 or 1.
In addition, onset of treatment benefit was significantly faster in the group having a score of 5 or more. They had a significantly higher clinical remission rate than the intermediate- and low-probability groups at all scheduled assessments, which were conducted at weeks 3, 6, 8, and 16. Indeed, by week 3 the high-probability group experienced a mean 69-point drop from baseline in CDAI and a 94-point drop by week 8, as compared with week-8 reductions of 54 and 40 points in the intermediate- and low-probability groups, respectively.
In an exploratory analysis involving the 122 patients who underwent week-8 endoscopy, endoscopic remission was documented in 12% of patients whose baseline scores placed them in the high-probability group, 10% in the intermediate group, and 8% of those in the low-probability group.
The high-probability group had significantly higher ustekinumab trough concentrations than did the intermediate- and low-probability groups when measured at weeks 3, 6, 8, and 16.
An external validation study conducted in a large cohort of Crohn’s disease patients seen in routine clinical practice has recently been completed, with the results now being analyzed, according to Dr. Dulai.
Miguel Requeiro, MD, chairman of gastroenterology and hepatology at the Cleveland Clinic, rose from the audience to declare the creation of the decision support tool to be “brilliant work.” He asked if it has changed clinical practice for Dr. Dulai and his coworkers.
“We’ve begun doing two things differently,” Dr. Dulai replied. “First, we’ve built a similar model for vedolizumab and Crohn’s. That means we can use both tools together to discriminate between a patient who should get vedolizumab versus ustekinumab because the variables and their weighting differ between the two. And the other thing we’ve been able to do is argue with payers for positioning of the treatments when we have evidence to support that we can use them earlier in the treatment course to optimize outcomes.”
Another audience member, David T. Rubin, MD, also praised the decision support tool as “brilliant” and “definitely needed.”
“Thank you for hitting the sweet spot of what we’ve all been waiting for,” added Dr. Rubin, professor of medicine and codirector of the Digestive Diseases Center at the University of Chicago.
Dr. Dulai reported receiving a research grant for the project from Janssen, which markets ustekinumab.
REPORTING FROM ACG 2019
Societies dig in to EXCEL trial controversy
Thoracic surgery societies on both sides of the Atlantic have released new statements on a continuing controversy dogging the EXCEL trial, one that has fueled a highly public war of words over how the study was conducted, interpreted, and reported by its investigators.

In a statement dated Dec. 19, 2019, the European Association for Cardio-Thoracic Surgery (EACTS) offered new details on why it withdrew its endorsement of the 2018 EACTS-European Society of Cardiology (ESC) clinical guidelines section covering left-main coronary artery disease.
That part of the guideline had relied in part on 3-year outcomes from EXCEL, which were published in the New England Journal of Medicine in 2016 (2016 Dec 8;375[23]:2223-35) and are central to the ongoing dispute. The trial, in essence, was a comparison of percutaneous coronary intervention (PCI) and coronary bypass surgery (CABG) in left-main disease. In that report, PCI was noninferior to CABG with respect to the composite endpoint of death, stroke, or myocardial infarction at 3 years in patients with left-main disease and low or intermediate anatomical complexity.
The new statement, signed by the society’s secretary general Domenico Pagano, MD, also calls for a new EACTS-ESC evidence review and development of updated recommendations for left-main disease “as a matter of urgency.”
For its part, the ESC had earlier declared its continuing support for the full guideline but hinted that might change pending further details on EXCEL yet to be made public.
The EACTS statement follows the society’s earlier announcement that it would pull support of the guideline section on left-main disease in response to a Dec. 9, 2019, news report from BBC Newsnight that was critical of the EXCEL trial’s methodology and reporting.
The news story made a number of allegations regarding the interpretation and reporting of EXCEL based largely on unpublished data it had obtained through unofficial channels.
Key among them was that reanalysis of myocardial infarction outcomes using the Third Universal Definition of MI, rather than the primarily enzymatic definition on which the reported outcomes were based, substantially raised the MI count in the PCI group, compared with those who had CABG.
The data for that alternative analysis, which had not been publicly reported, seemed to recast the published EXCEL primary outcome from one of parity for PCI and CABG in left-main disease to one that significantly favored CABG, noted the BBC Newsnight story.
Also, the news story claimed that EXCEL investigators had promised to publicly release the trial’s data based on the Third Universal Definition of MI, but had not done so, and had not adequately heeded concerns raised by its Data Safety Monitoring Board (DSMB) over signs of an apparently increased mortality risk from PCI.
Another society weighs in
The unreported data and other issues have led the American Association for Thoracic Surgery (AATS) to issue a statement acknowledging the possibility of misguided treatment recommendations, and therefore patient care, stemming from incomplete reporting of EXCEL.
If there are serious concerns about the “presentation or interpretation” of clinical trials, “then the best way forward is the public release of all trial data for an independent analysis to confirm that the original trial conclusions are valid,” says the statement, signed by AATS president Vaughn A. Starnes, MD, and secretary David R. Jones, MD.
“The AATS agrees with others that all of the data should be made publicly available for analysis and interpretation, as a way to resolve the current controversy around the EXCEL trial, in order to provide patients with the best possible counsel and informed consent,” it states.
The BBC Newsnight story “raised legitimate questions regarding what data was/was not presented to the other EXCEL investigators and to [the] ESC/EACTS guideline committee, and what, when, and to whom were safety warnings raised by the DSMB,” David Taggart, MD, PhD, wrote in an email interview.
“Until these issues are resolved, both EACTS and AATS have expressed concerns about what has happened and, most importantly, the potential implications for patient safety. This stance underpins their sincerity that patient safety, genuine informed consent, and scientific integrity are amongst their highest priorities. Consequently they have my complete support,” said Dr. Taggart, of the University of Oxford (England) a former EXCEL trialist who has been among the most vocal critics of how the EXCEL leadership has interpreted and reported the trial’s outcomes.
“Personally, I do not feel that the current controversy over the EXCEL trial will be resolved until there is full and independent reanalysis of its data. I feel that this would be absolutely crucial in reassuring our patients, the wider medical community, and the general public of the validity of current recommendations.”
An EXCEL principal investigator and prominent public voice for the trial, Gregg W. Stone, MD, of Icahn School of Medicine at Mount Sinai, New York, has not responded to requests for comment on the new society statements.
Point-counterpoint
As previously reported, allegations about EXCEL in news reports and the sometimes fiery public debate led the trialists to release a long and wide-ranging public communique that forcefully disputes the charges. Among them, that they were either remiss or willfully deceptive in not reporting an analysis based on the Third Universal Definition of MI.
In response, Dr. Taggart provided a toughly worded statement that disputes the EXCEL leadership’s missive nearly point by point. It variously describes the assertions as “simplistic,” seemingly “illogical,” “disingenuous,” and “factually completely incorrect,” among other terms.
The document provides Dr. Taggart’s perspective on how MI was defined and interpreted while he was an active member of the EXCEL trial’s leadership, and alleged shortfalls in how outcomes were interpreted and reported.
In it, Taggart also wonders whether or not EXCEL leadership had possibly been aware of a tilt favoring CABG in the analysis based on Third Universal Definition of MI but “decided to suppress it,” and also whether the trial’s sponsor, Abbott Vascular, had influenced the trial’s conduct.
Despite the EXCEL leadership’s communique, “my profound concerns remain the same and, in my opinion, the very long rebuttal response by the EXCEL investigators does not adequately respond to the core issues,” Dr. Taggart writes.
He withdrew his name as an author on the trial’s 5-year outcomes publication, Dr. Taggart says, because “I believed, and still do, that the final interpretation of the actual data in the [New England Journal of Medicine] manuscript did not appropriately reflect its clinical reality, and especially with regards to mortality, and would therefore have potential to do real harm to patients.”
Dr. Taggart has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.
Thoracic surgery societies on both sides of the Atlantic have released new statements on a continuing controversy dogging the EXCEL trial, one that has fueled a highly public war of words over how the study was conducted, interpreted, and reported by its investigators.
In a statement dated Dec. 19, 2019, the European Association for Cardio-Thoracic Surgery (EACTS) offered new details on why it withdrew its endorsement of the 2018 EACTS-European Society of Cardiology (ESC) clinical guidelines section covering left-main coronary artery disease.
That part of the guideline had relied in part on 3-year outcomes from EXCEL, which were published in the New England Journal of Medicine in 2016 (2016 Dec 8;375[23]:2223-35) and are central to the ongoing dispute. The trial, in essence, was a comparison of percutaneous coronary intervention (PCI) and coronary bypass surgery (CABG) in left-main disease. In that report, PCI was noninferior to CABG with respect to the composite endpoint of death, stroke, or myocardial infarction at 3 years in patients with left-main disease and low or intermediate anatomical complexity.
The new statement, signed by the society’s secretary general Domenico Pagano, MD, also calls for a new EACTS-ESC evidence review and development of updated recommendations for left-main disease “as a matter of urgency.”
For its part, the ESC had earlier declared its continuing support for the full guideline but hinted that might change pending further details on EXCEL yet to be made public.
The EACTS statement follows the society’s earlier announcement that it would pull support of the guideline section on left-main disease in response to a Dec. 9, 2019, news report from BBC Newsnight that was critical of the EXCEL trial’s methodology and reporting.
The news story made a number of allegations regarding the interpretation and reporting of EXCEL based largely on unpublished data it had obtained through unofficial channels.
Key among them was that reanalysis of myocardial infarction outcomes using the Third Universal Definition of MI, rather than the primarily enzymatic definition on which the reported outcomes were based, substantially raised the MI count in the PCI group, compared with those who had CABG.
The data for that alternative analysis, which had not been publicly reported, seemed to recast the published EXCEL primary outcome from one of parity for PCI and CABG in left-main disease to one that significantly favored CABG, noted the BBC Newsnight story.
Also, the news story claimed that EXCEL investigators had promised to publicly release the trial’s data based on the Third Universal Definition of MI, but had not done so, and had not adequately heeded concerns raised by its Data Safety Monitoring Board (DSMB) over signs of an apparently increased mortality risk from PCI.
Another society weighs in
The unreported data and other issues have led the American Association for Thoracic Surgery (AATS) to issue a statement acknowledging the possibility of misguided treatment recommendations, and therefore patient care, stemming from incomplete reporting of EXCEL.
If there are serious concerns about the “presentation or interpretation” of clinical trials, “then the best way forward is the public release of all trial data for an independent analysis to confirm that the original trial conclusions are valid,” says the statement, signed by AATS president Vaughn A. Starnes, MD, and secretary David R. Jones, MD.
“The AATS agrees with others that all of the data should be made publicly available for analysis and interpretation, as a way to resolve the current controversy around the EXCEL trial, in order to provide patients with the best possible counsel and informed consent,” it states.
The BBC Newsnight story “raised legitimate questions regarding what data was/was not presented to the other EXCEL investigators and to [the] ESC/EACTS guideline committee, and what, when, and to whom were safety warnings raised by the DSMB,” David Taggart, MD, PhD, wrote in an email interview.
“Until these issues are resolved, both EACTS and AATS have expressed concerns about what has happened and, most importantly, the potential implications for patient safety. This stance underpins their sincerity that patient safety, genuine informed consent, and scientific integrity are amongst their highest priorities. Consequently they have my complete support,” said Dr. Taggart, of the University of Oxford (England) a former EXCEL trialist who has been among the most vocal critics of how the EXCEL leadership has interpreted and reported the trial’s outcomes.
“Personally, I do not feel that the current controversy over the EXCEL trial will be resolved until there is full and independent reanalysis of its data. I feel that this would be absolutely crucial in reassuring our patients, the wider medical community, and the general public of the validity of current recommendations.”
An EXCEL principal investigator and prominent public voice for the trial, Gregg W. Stone, MD, of Icahn School of Medicine at Mount Sinai, New York, has not responded to requests for comment on the new society statements.
Point-counterpoint
As previously reported, allegations about EXCEL in news reports and the sometimes fiery public debate led the trialists to release a long and wide-ranging public communique that forcefully disputes the charges. Among them, that they were either remiss or willfully deceptive in not reporting an analysis based on the Third Universal Definition of MI.
In response, Dr. Taggart provided a toughly worded statement that disputes the EXCEL leadership’s missive nearly point by point. It variously describes the assertions as “simplistic,” seemingly “illogical,” “disingenuous,” and “factually completely incorrect,” among other terms.
The document provides Dr. Taggart’s perspective on how MI was defined and interpreted while he was an active member of the EXCEL trial’s leadership, and alleged shortfalls in how outcomes were interpreted and reported.
In it, Taggart also wonders whether or not EXCEL leadership had possibly been aware of a tilt favoring CABG in the analysis based on Third Universal Definition of MI but “decided to suppress it,” and also whether the trial’s sponsor, Abbott Vascular, had influenced the trial’s conduct.
Despite the EXCEL leadership’s communique, “my profound concerns remain the same and, in my opinion, the very long rebuttal response by the EXCEL investigators does not adequately respond to the core issues,” Dr. Taggart writes.
He withdrew his name as an author on the trial’s 5-year outcomes publication, Dr. Taggart says, because “I believed, and still do, that the final interpretation of the actual data in the [New England Journal of Medicine] manuscript did not appropriately reflect its clinical reality, and especially with regards to mortality, and would therefore have potential to do real harm to patients.”
Dr. Taggart has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.
Thoracic surgery societies on both sides of the Atlantic have released new statements on a continuing controversy dogging the EXCEL trial, one that has fueled a highly public war of words over how the study was conducted, interpreted, and reported by its investigators.
In a statement dated Dec. 19, 2019, the European Association for Cardio-Thoracic Surgery (EACTS) offered new details on why it withdrew its endorsement of the 2018 EACTS-European Society of Cardiology (ESC) clinical guidelines section covering left-main coronary artery disease.
That part of the guideline had relied in part on 3-year outcomes from EXCEL, which were published in the New England Journal of Medicine in 2016 (2016 Dec 8;375[23]:2223-35) and are central to the ongoing dispute. The trial, in essence, was a comparison of percutaneous coronary intervention (PCI) and coronary bypass surgery (CABG) in left-main disease. In that report, PCI was noninferior to CABG with respect to the composite endpoint of death, stroke, or myocardial infarction at 3 years in patients with left-main disease and low or intermediate anatomical complexity.
The new statement, signed by the society’s secretary general Domenico Pagano, MD, also calls for a new EACTS-ESC evidence review and development of updated recommendations for left-main disease “as a matter of urgency.”
For its part, the ESC had earlier declared its continuing support for the full guideline but hinted that might change pending further details on EXCEL yet to be made public.
The EACTS statement follows the society’s earlier announcement that it would pull support of the guideline section on left-main disease in response to a Dec. 9, 2019, news report from BBC Newsnight that was critical of the EXCEL trial’s methodology and reporting.
The news story made a number of allegations regarding the interpretation and reporting of EXCEL based largely on unpublished data it had obtained through unofficial channels.
Key among them was that reanalysis of myocardial infarction outcomes using the Third Universal Definition of MI, rather than the primarily enzymatic definition on which the reported outcomes were based, substantially raised the MI count in the PCI group, compared with those who had CABG.
The data for that alternative analysis, which had not been publicly reported, seemed to recast the published EXCEL primary outcome from one of parity for PCI and CABG in left-main disease to one that significantly favored CABG, noted the BBC Newsnight story.
Also, the news story claimed that EXCEL investigators had promised to publicly release the trial’s data based on the Third Universal Definition of MI, but had not done so, and had not adequately heeded concerns raised by its Data Safety Monitoring Board (DSMB) over signs of an apparently increased mortality risk from PCI.
Another society weighs in
The unreported data and other issues have led the American Association for Thoracic Surgery (AATS) to issue a statement acknowledging the possibility of misguided treatment recommendations, and therefore patient care, stemming from incomplete reporting of EXCEL.
If there are serious concerns about the “presentation or interpretation” of clinical trials, “then the best way forward is the public release of all trial data for an independent analysis to confirm that the original trial conclusions are valid,” says the statement, signed by AATS president Vaughn A. Starnes, MD, and secretary David R. Jones, MD.
“The AATS agrees with others that all of the data should be made publicly available for analysis and interpretation, as a way to resolve the current controversy around the EXCEL trial, in order to provide patients with the best possible counsel and informed consent,” it states.
The BBC Newsnight story “raised legitimate questions regarding what data was/was not presented to the other EXCEL investigators and to [the] ESC/EACTS guideline committee, and what, when, and to whom were safety warnings raised by the DSMB,” David Taggart, MD, PhD, wrote in an email interview.
“Until these issues are resolved, both EACTS and AATS have expressed concerns about what has happened and, most importantly, the potential implications for patient safety. This stance underpins their sincerity that patient safety, genuine informed consent, and scientific integrity are amongst their highest priorities. Consequently they have my complete support,” said Dr. Taggart, of the University of Oxford (England) a former EXCEL trialist who has been among the most vocal critics of how the EXCEL leadership has interpreted and reported the trial’s outcomes.
“Personally, I do not feel that the current controversy over the EXCEL trial will be resolved until there is full and independent reanalysis of its data. I feel that this would be absolutely crucial in reassuring our patients, the wider medical community, and the general public of the validity of current recommendations.”
An EXCEL principal investigator and prominent public voice for the trial, Gregg W. Stone, MD, of Icahn School of Medicine at Mount Sinai, New York, has not responded to requests for comment on the new society statements.
Point-counterpoint
As previously reported, allegations about EXCEL in news reports and the sometimes fiery public debate led the trialists to release a long and wide-ranging public communique that forcefully disputes the charges. Among them, that they were either remiss or willfully deceptive in not reporting an analysis based on the Third Universal Definition of MI.
In response, Dr. Taggart provided a toughly worded statement that disputes the EXCEL leadership’s missive nearly point by point. It variously describes the assertions as “simplistic,” seemingly “illogical,” “disingenuous,” and “factually completely incorrect,” among other terms.
The document provides Dr. Taggart’s perspective on how MI was defined and interpreted while he was an active member of the EXCEL trial’s leadership, and alleged shortfalls in how outcomes were interpreted and reported.
In it, Taggart also wonders whether or not EXCEL leadership had possibly been aware of a tilt favoring CABG in the analysis based on Third Universal Definition of MI but “decided to suppress it,” and also whether the trial’s sponsor, Abbott Vascular, had influenced the trial’s conduct.
Despite the EXCEL leadership’s communique, “my profound concerns remain the same and, in my opinion, the very long rebuttal response by the EXCEL investigators does not adequately respond to the core issues,” Dr. Taggart writes.
He withdrew his name as an author on the trial’s 5-year outcomes publication, Dr. Taggart says, because “I believed, and still do, that the final interpretation of the actual data in the [New England Journal of Medicine] manuscript did not appropriately reflect its clinical reality, and especially with regards to mortality, and would therefore have potential to do real harm to patients.”
Dr. Taggart has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.
Psychiatrists urged to look beyond the ‘monoamine island’
Now that 2019 has passed us by, it is a time for reflection for most of us. We can think about the state of our important relationships, perhaps the growth of our children or other loved ones, the trajectory of our practices, and ideas for the future. Most commonly, I would wager, we likely think about how we might do things differently in the new year.

Applying this lens to our chosen profession, the practice of clinical psychiatry, I hope 2020 brings real, or at least, incremental change. Our profession has evolved markedly over the last several decades, from psychoanalysis to the psychopharmacology revolution, to a now largely multimodal approach. Our treatment of psychiatric illness has evolved and, for the most part, improved the lives of millions across the country and around the world.
However, in so doing, we have, perhaps inadvertently, or maybe out of necessity, found ourselves on an allegorical island that we, as clinical, everyday psychiatrists defend to the death. Surrounded by an ocean of psychiatric disorders, illnesses, and symptomatology, we wave our prescription pads (or e-pads), like wands, hoping to calm the torrents of the psychiatric sea with yet another prescription. However, I’m not writing this to bemoan modern psychopharmacology, for it has saved and improved lives and led to a fruitful practice and livelihood for me and most of my colleagues. As the torrents of illness continue to flare around us, I’m not advocating that we put down our wands and become strictly therapists. What I am advocating for is the use of different wands, as it were.
Our chosen wand is undoubtedly largely composed of monoamine-based remedies – most involving the holy trinity of serotonin, dopamine, and norepinephrine. As we stand on our island, trying to quell hurricane-force winds, shark-infested waters, or a tidal wave, we wave the same wand – hoping that a dash of monoamine will slow down winds, scare away sharks, and reduce the destructive capacity of water.
We, more than those in any other medical profession, use the same basic treatments for heterogeneous disorders, whose true underlying physiology, despite important progress over the years, remains elusive and only partly understood. We see improvement and even resolution sometimes, but, for the most part, our treatments keep our patients going, so they can continue to sail, just avoiding being capsized by the psychiatric torrents beneath the surface. When the torrents flare, we wave the same wand again, hoping that another dash of monoamine modulation, this time, maybe in a new wrapper, or with a new name, will keep the ocean calm for a bit longer. Now, this has worked for decades to keep many ships from being capsized and our island still largely habitable, but this strategy is akin to building a shelter out of twigs and leaves and grasses, and never advancing to permanent construction techniques, and just replacing broken branches and leaves that will, undoubtedly, break again.
As we stand on our island, I say, we use the branches, leaves, and twigs to build a bridge to another island, and, there, we can make new wands.
In 2020, the materials for these new wands are readily available, but we have to be willing to trust these new wands, and yet not completely discard the old wands we have used for so long. These new wands are the nonmonoamine-based treatments, which have shown remarkable efficacy and safety in patients across the country and the world. We must accept that we, as a species, are remarkably complex creatures, and the disorders we try to treat have their origins in the most complex part of our being: the brain. Therefore, considering the complexity, it is only reasonable to think that there is more to our illnesses than modulating monoamines.
In 2020, I challenge every day, clinical psychiatrists to embrace these new treatments and wave these new wands. As someone who has been fortunate enough to prescribe ketamine infusion and nasal sprays in the clinic, I can say we must gravitate toward these new treatments when clinically appropriate. While ketamine treatment is no panacea, its use, and the adoption of other nonmonoamine-based treatments, hopefully will fuel the development, use, and perhaps, most importantly, novel thinking about new biological treatment of psychiatric illness.
Dr. Shroff is board-certified in psychiatry in sleep medicine, and practices in Smyrna, Ga. He is a fellow of the American Psychiatric Association.
Now that 2019 has passed us by, it is a time for reflection for most of us. We can think about the state of our important relationships, perhaps the growth of our children or other loved ones, the trajectory of our practices, and ideas for the future. Most commonly, I would wager, we likely think about how we might do things differently in the new year.
Applying this lens to our chosen profession, the practice of clinical psychiatry, I hope 2020 brings real, or at least, incremental change. Our profession has evolved markedly over the last several decades, from psychoanalysis to the psychopharmacology revolution, to a now largely multimodal approach. Our treatment of psychiatric illness has evolved and, for the most part, improved the lives of millions across the country and around the world.
However, in so doing, we have, perhaps inadvertently, or maybe out of necessity, found ourselves on an allegorical island that we, as clinical, everyday psychiatrists defend to the death. Surrounded by an ocean of psychiatric disorders, illnesses, and symptomatology, we wave our prescription pads (or e-pads), like wands, hoping to calm the torrents of the psychiatric sea with yet another prescription. However, I’m not writing this to bemoan modern psychopharmacology, for it has saved and improved lives and led to a fruitful practice and livelihood for me and most of my colleagues. As the torrents of illness continue to flare around us, I’m not advocating that we put down our wands and become strictly therapists. What I am advocating for is the use of different wands, as it were.
Our chosen wand is undoubtedly largely composed of monoamine-based remedies – most involving the holy trinity of serotonin, dopamine, and norepinephrine. As we stand on our island, trying to quell hurricane-force winds, shark-infested waters, or a tidal wave, we wave the same wand – hoping that a dash of monoamine will slow down winds, scare away sharks, and reduce the destructive capacity of water.
We, more than those in any other medical profession, use the same basic treatments for heterogeneous disorders, whose true underlying physiology, despite important progress over the years, remains elusive and only partly understood. We see improvement and even resolution sometimes, but, for the most part, our treatments keep our patients going, so they can continue to sail, just avoiding being capsized by the psychiatric torrents beneath the surface. When the torrents flare, we wave the same wand again, hoping that another dash of monoamine modulation, this time, maybe in a new wrapper, or with a new name, will keep the ocean calm for a bit longer. Now, this has worked for decades to keep many ships from being capsized and our island still largely habitable, but this strategy is akin to building a shelter out of twigs and leaves and grasses, and never advancing to permanent construction techniques, and just replacing broken branches and leaves that will, undoubtedly, break again.
As we stand on our island, I say, we use the branches, leaves, and twigs to build a bridge to another island, and, there, we can make new wands.
In 2020, the materials for these new wands are readily available, but we have to be willing to trust these new wands, and yet not completely discard the old wands we have used for so long. These new wands are the nonmonoamine-based treatments, which have shown remarkable efficacy and safety in patients across the country and the world. We must accept that we, as a species, are remarkably complex creatures, and the disorders we try to treat have their origins in the most complex part of our being: the brain. Therefore, considering the complexity, it is only reasonable to think that there is more to our illnesses than modulating monoamines.
In 2020, I challenge every day, clinical psychiatrists to embrace these new treatments and wave these new wands. As someone who has been fortunate enough to prescribe ketamine infusion and nasal sprays in the clinic, I can say we must gravitate toward these new treatments when clinically appropriate. While ketamine treatment is no panacea, its use, and the adoption of other nonmonoamine-based treatments, hopefully will fuel the development, use, and perhaps, most importantly, novel thinking about new biological treatment of psychiatric illness.
Dr. Shroff is board-certified in psychiatry in sleep medicine, and practices in Smyrna, Ga. He is a fellow of the American Psychiatric Association.
Now that 2019 has passed us by, it is a time for reflection for most of us. We can think about the state of our important relationships, perhaps the growth of our children or other loved ones, the trajectory of our practices, and ideas for the future. Most commonly, I would wager, we likely think about how we might do things differently in the new year.
Applying this lens to our chosen profession, the practice of clinical psychiatry, I hope 2020 brings real, or at least, incremental change. Our profession has evolved markedly over the last several decades, from psychoanalysis to the psychopharmacology revolution, to a now largely multimodal approach. Our treatment of psychiatric illness has evolved and, for the most part, improved the lives of millions across the country and around the world.
However, in so doing, we have, perhaps inadvertently, or maybe out of necessity, found ourselves on an allegorical island that we, as clinical, everyday psychiatrists defend to the death. Surrounded by an ocean of psychiatric disorders, illnesses, and symptomatology, we wave our prescription pads (or e-pads), like wands, hoping to calm the torrents of the psychiatric sea with yet another prescription. However, I’m not writing this to bemoan modern psychopharmacology, for it has saved and improved lives and led to a fruitful practice and livelihood for me and most of my colleagues. As the torrents of illness continue to flare around us, I’m not advocating that we put down our wands and become strictly therapists. What I am advocating for is the use of different wands, as it were.
Our chosen wand is undoubtedly largely composed of monoamine-based remedies – most involving the holy trinity of serotonin, dopamine, and norepinephrine. As we stand on our island, trying to quell hurricane-force winds, shark-infested waters, or a tidal wave, we wave the same wand – hoping that a dash of monoamine will slow down winds, scare away sharks, and reduce the destructive capacity of water.
We, more than those in any other medical profession, use the same basic treatments for heterogeneous disorders, whose true underlying physiology, despite important progress over the years, remains elusive and only partly understood. We see improvement and even resolution sometimes, but, for the most part, our treatments keep our patients going, so they can continue to sail, just avoiding being capsized by the psychiatric torrents beneath the surface. When the torrents flare, we wave the same wand again, hoping that another dash of monoamine modulation, this time, maybe in a new wrapper, or with a new name, will keep the ocean calm for a bit longer. Now, this has worked for decades to keep many ships from being capsized and our island still largely habitable, but this strategy is akin to building a shelter out of twigs and leaves and grasses, and never advancing to permanent construction techniques, and just replacing broken branches and leaves that will, undoubtedly, break again.
As we stand on our island, I say, we use the branches, leaves, and twigs to build a bridge to another island, and, there, we can make new wands.
In 2020, the materials for these new wands are readily available, but we have to be willing to trust these new wands, and yet not completely discard the old wands we have used for so long. These new wands are the nonmonoamine-based treatments, which have shown remarkable efficacy and safety in patients across the country and the world. We must accept that we, as a species, are remarkably complex creatures, and the disorders we try to treat have their origins in the most complex part of our being: the brain. Therefore, considering the complexity, it is only reasonable to think that there is more to our illnesses than modulating monoamines.
In 2020, I challenge every day, clinical psychiatrists to embrace these new treatments and wave these new wands. As someone who has been fortunate enough to prescribe ketamine infusion and nasal sprays in the clinic, I can say we must gravitate toward these new treatments when clinically appropriate. While ketamine treatment is no panacea, its use, and the adoption of other nonmonoamine-based treatments, hopefully will fuel the development, use, and perhaps, most importantly, novel thinking about new biological treatment of psychiatric illness.
Dr. Shroff is board-certified in psychiatry in sleep medicine, and practices in Smyrna, Ga. He is a fellow of the American Psychiatric Association.
Study simplifies bladder cancer molecular subtypes
Muscle-invasive bladder cancer (MIBC) can be divided into six molecular classes that may eventually guide clinical decision making, according to an international consensus group.
The six classes are based on a variety of disease factors, including immune and stromal cell infiltration, oncogenic mechanisms, histologic features, and clinical characteristics, reported lead author Aurélie Kamoun, PhD, of Ligue Nationale Contre le Cancer in Paris, and colleagues.
Although several molecular classification systems for MIBC have been previously published, subtypes have varied widely, the investigators explained in European Urology.
“This diversity has impeded transferring subtypes into clinical practice and highlights that establishing a single consensus set of molecular subtypes would facilitate achieving such a transfer,” the investigators wrote.
In order to reach a consensus, the investigators drew data from the six previously published classification systems, including 1,750 transcriptomic profiles from 16 published datasets and 2 additional patient populations.
Using a network-based approach, the investigators identified consensus classes that reconciled differences between the previously published systems. This process revealed a core set of 1,084 consensus samples, from which the investigators built a single-sample transcriptomic classifier. This free tool is now available online at https://github.com/cit-bioinfo/consensusMIBC.
The six consensus molecular classes (with prevalence among samples) are basal/squamous (35%), luminal papillary (24%), luminal unstable (15%), luminal nonspecified (8%), stroma rich (15%), and neuroendocrine like (3%).
The investigators described a number of disease characteristics that correlate with each molecular class, from the genomic to the clinical level. For example, basal/squamous tumors were associated with TP53 mutations and immune infiltration involving natural killer cells and cytotoxic lymphocytes.
Similar conclusions were described at the clinical level.
Consensus class predicted overall survival, with neuroendocrine-like tumors having the worst prognosis relative to luminal papillary tumors (hazard ratio, 2.34; P less than .03).
The investigators also highlighted some possible treatment implications related to subtype. For example, patients with basal/squamous or luminal nonspecified tumors derived benefit from neoadjuvant chemotherapy. Similarly, patients with luminal nonspecified, luminal unstable, or neuroendocrine-like tumors were more likely to respond when given atezolizumab.
“We expect that this consensus classification will help the development of MIBC precision medicine by providing a robust framework to connect clinical findings to molecular contexts and to identify clinically relevant biomarkers for patient management,” Dr. Kamoun and coauthors concluded.
The investigators reported relationships with Bayer, Astellas, Genentech, and others.
SOURCE: Kamoun A et al. Eur Urol. 2019 Sep 26. doi: 10.1016/j.eururo.2019.09.006.
Muscle-invasive bladder cancer (MIBC) can be divided into six molecular classes that may eventually guide clinical decision making, according to an international consensus group.
The six classes are based on a variety of disease factors, including immune and stromal cell infiltration, oncogenic mechanisms, histologic features, and clinical characteristics, reported lead author Aurélie Kamoun, PhD, of Ligue Nationale Contre le Cancer in Paris, and colleagues.
Although several molecular classification systems for MIBC have been previously published, subtypes have varied widely, the investigators explained in European Urology.
“This diversity has impeded transferring subtypes into clinical practice and highlights that establishing a single consensus set of molecular subtypes would facilitate achieving such a transfer,” the investigators wrote.
In order to reach a consensus, the investigators drew data from the six previously published classification systems, including 1,750 transcriptomic profiles from 16 published datasets and 2 additional patient populations.
Using a network-based approach, the investigators identified consensus classes that reconciled differences between the previously published systems. This process revealed a core set of 1,084 consensus samples, from which the investigators built a single-sample transcriptomic classifier. This free tool is now available online at https://github.com/cit-bioinfo/consensusMIBC.
The six consensus molecular classes (with prevalence among samples) are basal/squamous (35%), luminal papillary (24%), luminal unstable (15%), luminal nonspecified (8%), stroma rich (15%), and neuroendocrine like (3%).
The investigators described a number of disease characteristics that correlate with each molecular class, from the genomic to the clinical level. For example, basal/squamous tumors were associated with TP53 mutations and immune infiltration involving natural killer cells and cytotoxic lymphocytes.
Similar conclusions were described at the clinical level.
Consensus class predicted overall survival, with neuroendocrine-like tumors having the worst prognosis relative to luminal papillary tumors (hazard ratio, 2.34; P less than .03).
The investigators also highlighted some possible treatment implications related to subtype. For example, patients with basal/squamous or luminal nonspecified tumors derived benefit from neoadjuvant chemotherapy. Similarly, patients with luminal nonspecified, luminal unstable, or neuroendocrine-like tumors were more likely to respond when given atezolizumab.
“We expect that this consensus classification will help the development of MIBC precision medicine by providing a robust framework to connect clinical findings to molecular contexts and to identify clinically relevant biomarkers for patient management,” Dr. Kamoun and coauthors concluded.
The investigators reported relationships with Bayer, Astellas, Genentech, and others.
SOURCE: Kamoun A et al. Eur Urol. 2019 Sep 26. doi: 10.1016/j.eururo.2019.09.006.
Muscle-invasive bladder cancer (MIBC) can be divided into six molecular classes that may eventually guide clinical decision making, according to an international consensus group.
The six classes are based on a variety of disease factors, including immune and stromal cell infiltration, oncogenic mechanisms, histologic features, and clinical characteristics, reported lead author Aurélie Kamoun, PhD, of Ligue Nationale Contre le Cancer in Paris, and colleagues.
Although several molecular classification systems for MIBC have been previously published, subtypes have varied widely, the investigators explained in European Urology.
“This diversity has impeded transferring subtypes into clinical practice and highlights that establishing a single consensus set of molecular subtypes would facilitate achieving such a transfer,” the investigators wrote.
In order to reach a consensus, the investigators drew data from the six previously published classification systems, including 1,750 transcriptomic profiles from 16 published datasets and 2 additional patient populations.
Using a network-based approach, the investigators identified consensus classes that reconciled differences between the previously published systems. This process revealed a core set of 1,084 consensus samples, from which the investigators built a single-sample transcriptomic classifier. This free tool is now available online at https://github.com/cit-bioinfo/consensusMIBC.
The six consensus molecular classes (with prevalence among samples) are basal/squamous (35%), luminal papillary (24%), luminal unstable (15%), luminal nonspecified (8%), stroma rich (15%), and neuroendocrine like (3%).
The investigators described a number of disease characteristics that correlate with each molecular class, from the genomic to the clinical level. For example, basal/squamous tumors were associated with TP53 mutations and immune infiltration involving natural killer cells and cytotoxic lymphocytes.
Similar conclusions were described at the clinical level.
Consensus class predicted overall survival, with neuroendocrine-like tumors having the worst prognosis relative to luminal papillary tumors (hazard ratio, 2.34; P less than .03).
The investigators also highlighted some possible treatment implications related to subtype. For example, patients with basal/squamous or luminal nonspecified tumors derived benefit from neoadjuvant chemotherapy. Similarly, patients with luminal nonspecified, luminal unstable, or neuroendocrine-like tumors were more likely to respond when given atezolizumab.
“We expect that this consensus classification will help the development of MIBC precision medicine by providing a robust framework to connect clinical findings to molecular contexts and to identify clinically relevant biomarkers for patient management,” Dr. Kamoun and coauthors concluded.
The investigators reported relationships with Bayer, Astellas, Genentech, and others.
SOURCE: Kamoun A et al. Eur Urol. 2019 Sep 26. doi: 10.1016/j.eururo.2019.09.006.
FROM EUROPEAN UROLOGY
Aligning scheduling and satisfaction
Research reveals counterintuitive results
Hospitalist work schedules have been the subject of much reporting – and recent research. Studies have shown that control over work hours and schedule flexibility are predictors of clinicians’ career satisfaction and burnout, factors linked to quality of patient care and retention.

Starting in January 2017, an academic hospital medicine group at the University of Colorado at Denver, Aurora, undertook a scheduling redesign using improvement methodology, combined with purchased scheduling software. Tyler Anstett, DO, a hospitalist and assistant professor at the university, and colleagues presented the results in an abstract published during the SHM 2019 annual conference last March.
“We wrote this abstract as a report of the work that we did over several years in our hospital medicine group to improve hospitalist satisfaction with their schedules,” said Dr. Anstett. “We identified that, despite not following the traditional seven-on, seven-off model and 100% fulfillment of individual schedule requests, the majority of clinicians were dissatisfied with the scheduling process and their overall clinical schedules. Further, building these complex, individualized schedules resulted in a heavy administrative burden. We strove to provide better alignment of schedule satisfaction and the administrative burden of incorporating individualized schedule requests.”
Prior to January 2017, service stretches had ranged from 5 to 9 days, and there were few limits on time-off requests.
“Through sequential interventions, we standardized service stretches to 7 days (Tuesday-Monday), introduced a limited number of guaranteed 7-day time-off requests (Tuesday-Monday), and added a limited number of nonguaranteed 3-day flexible time-off requests,” according to the authors. “This simplification improved the automation of the scheduling software, which increased the schedule release lead time to an average of 16 weeks. Further, despite standardizing service stretches to 7 days and limiting time-off requests, physicians surveyed reported improved satisfaction with both their scheduling process (34% of participants ‘satisfied’ in 2017 to 67% in 2018) and their overall clinical schedules (50% of participants ‘satisfied’ in 2017 to 75% in 2018).”So counterintuitively, creating individualized schedules may not result in improved satisfaction and likely results in heavy administrative burden, Dr. Anstett said. “Standardization of schedule creation with allowance of a ‘free-market’ system, allowing clinicians to self-individualize their schedules may also result in less administrative burden and improved satisfaction.”
Reference
1. Anstett T et al. K.I.S.S. (Keep It Simple … Schedules): How Standardization and Simplification Can Improve Scheduling and Physician Satisfaction. SHM 2019, Abstract 112. Accessed June 4, 2019.
Research reveals counterintuitive results
Research reveals counterintuitive results
Hospitalist work schedules have been the subject of much reporting – and recent research. Studies have shown that control over work hours and schedule flexibility are predictors of clinicians’ career satisfaction and burnout, factors linked to quality of patient care and retention.
Starting in January 2017, an academic hospital medicine group at the University of Colorado at Denver, Aurora, undertook a scheduling redesign using improvement methodology, combined with purchased scheduling software. Tyler Anstett, DO, a hospitalist and assistant professor at the university, and colleagues presented the results in an abstract published during the SHM 2019 annual conference last March.
“We wrote this abstract as a report of the work that we did over several years in our hospital medicine group to improve hospitalist satisfaction with their schedules,” said Dr. Anstett. “We identified that, despite not following the traditional seven-on, seven-off model and 100% fulfillment of individual schedule requests, the majority of clinicians were dissatisfied with the scheduling process and their overall clinical schedules. Further, building these complex, individualized schedules resulted in a heavy administrative burden. We strove to provide better alignment of schedule satisfaction and the administrative burden of incorporating individualized schedule requests.”
Prior to January 2017, service stretches had ranged from 5 to 9 days, and there were few limits on time-off requests.
“Through sequential interventions, we standardized service stretches to 7 days (Tuesday-Monday), introduced a limited number of guaranteed 7-day time-off requests (Tuesday-Monday), and added a limited number of nonguaranteed 3-day flexible time-off requests,” according to the authors. “This simplification improved the automation of the scheduling software, which increased the schedule release lead time to an average of 16 weeks. Further, despite standardizing service stretches to 7 days and limiting time-off requests, physicians surveyed reported improved satisfaction with both their scheduling process (34% of participants ‘satisfied’ in 2017 to 67% in 2018) and their overall clinical schedules (50% of participants ‘satisfied’ in 2017 to 75% in 2018).”So counterintuitively, creating individualized schedules may not result in improved satisfaction and likely results in heavy administrative burden, Dr. Anstett said. “Standardization of schedule creation with allowance of a ‘free-market’ system, allowing clinicians to self-individualize their schedules may also result in less administrative burden and improved satisfaction.”
Reference
1. Anstett T et al. K.I.S.S. (Keep It Simple … Schedules): How Standardization and Simplification Can Improve Scheduling and Physician Satisfaction. SHM 2019, Abstract 112. Accessed June 4, 2019.
Hospitalist work schedules have been the subject of much reporting – and recent research. Studies have shown that control over work hours and schedule flexibility are predictors of clinicians’ career satisfaction and burnout, factors linked to quality of patient care and retention.
Starting in January 2017, an academic hospital medicine group at the University of Colorado at Denver, Aurora, undertook a scheduling redesign using improvement methodology, combined with purchased scheduling software. Tyler Anstett, DO, a hospitalist and assistant professor at the university, and colleagues presented the results in an abstract published during the SHM 2019 annual conference last March.
“We wrote this abstract as a report of the work that we did over several years in our hospital medicine group to improve hospitalist satisfaction with their schedules,” said Dr. Anstett. “We identified that, despite not following the traditional seven-on, seven-off model and 100% fulfillment of individual schedule requests, the majority of clinicians were dissatisfied with the scheduling process and their overall clinical schedules. Further, building these complex, individualized schedules resulted in a heavy administrative burden. We strove to provide better alignment of schedule satisfaction and the administrative burden of incorporating individualized schedule requests.”
Prior to January 2017, service stretches had ranged from 5 to 9 days, and there were few limits on time-off requests.
“Through sequential interventions, we standardized service stretches to 7 days (Tuesday-Monday), introduced a limited number of guaranteed 7-day time-off requests (Tuesday-Monday), and added a limited number of nonguaranteed 3-day flexible time-off requests,” according to the authors. “This simplification improved the automation of the scheduling software, which increased the schedule release lead time to an average of 16 weeks. Further, despite standardizing service stretches to 7 days and limiting time-off requests, physicians surveyed reported improved satisfaction with both their scheduling process (34% of participants ‘satisfied’ in 2017 to 67% in 2018) and their overall clinical schedules (50% of participants ‘satisfied’ in 2017 to 75% in 2018).”So counterintuitively, creating individualized schedules may not result in improved satisfaction and likely results in heavy administrative burden, Dr. Anstett said. “Standardization of schedule creation with allowance of a ‘free-market’ system, allowing clinicians to self-individualize their schedules may also result in less administrative burden and improved satisfaction.”
Reference
1. Anstett T et al. K.I.S.S. (Keep It Simple … Schedules): How Standardization and Simplification Can Improve Scheduling and Physician Satisfaction. SHM 2019, Abstract 112. Accessed June 4, 2019.
Top AGA Community patient cases
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. In case you missed it, here are the most popular clinical discussions shared in the forum recently:
1. Possible congestive heart failure, tuberculosis (http://ow.ly/QdmG30pZqqo) – Join the GI community in discussing the echocardiogram results of a Holocaust survivor with a history of diabetes, hypothyroidism, benign prostate hyperplasia and hypercholesterolemia, and whose daughter was recently found to be QuantiFERON Gold positive.
2. Recurrent diarrhea in Behcet’s disease patient (http://ow.ly/YX6L30pZqws) – A 42-year-old patient diagnosed with Behcet’s disease at age 13 presented with recurrent diarrhea; a colonoscopy revealed terminal ileal and cecal ulcerations.
3. Gastroparesis patient unable to take anti-emetics (http://ow.ly/E5jD30pZqw4) – Help your colleague address a tricky patient with prolonged QT and gastroparesis.
Access these clinical cases and more discussions at https://community.gastro.org/discussions.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. In case you missed it, here are the most popular clinical discussions shared in the forum recently:
1. Possible congestive heart failure, tuberculosis (http://ow.ly/QdmG30pZqqo) – Join the GI community in discussing the echocardiogram results of a Holocaust survivor with a history of diabetes, hypothyroidism, benign prostate hyperplasia and hypercholesterolemia, and whose daughter was recently found to be QuantiFERON Gold positive.
2. Recurrent diarrhea in Behcet’s disease patient (http://ow.ly/YX6L30pZqws) – A 42-year-old patient diagnosed with Behcet’s disease at age 13 presented with recurrent diarrhea; a colonoscopy revealed terminal ileal and cecal ulcerations.
3. Gastroparesis patient unable to take anti-emetics (http://ow.ly/E5jD30pZqw4) – Help your colleague address a tricky patient with prolonged QT and gastroparesis.
Access these clinical cases and more discussions at https://community.gastro.org/discussions.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. In case you missed it, here are the most popular clinical discussions shared in the forum recently:
1. Possible congestive heart failure, tuberculosis (http://ow.ly/QdmG30pZqqo) – Join the GI community in discussing the echocardiogram results of a Holocaust survivor with a history of diabetes, hypothyroidism, benign prostate hyperplasia and hypercholesterolemia, and whose daughter was recently found to be QuantiFERON Gold positive.
2. Recurrent diarrhea in Behcet’s disease patient (http://ow.ly/YX6L30pZqws) – A 42-year-old patient diagnosed with Behcet’s disease at age 13 presented with recurrent diarrhea; a colonoscopy revealed terminal ileal and cecal ulcerations.
3. Gastroparesis patient unable to take anti-emetics (http://ow.ly/E5jD30pZqw4) – Help your colleague address a tricky patient with prolonged QT and gastroparesis.
Access these clinical cases and more discussions at https://community.gastro.org/discussions.
Simple ways to create your legacy
Creating a legacy of giving is easier than you think. As the new year begins, take some time to start creating your legacy while supporting the AGA Research Foundation. Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission continues even after your lifetime.
Here are two ideas to help you get started.
Name the AGA Research Foundation as a beneficiary. This arrangement is one of the most tax-smart ways to support the AGA Research Foundation after your lifetime. When you leave retirement plan assets to us, we bypass any taxes and receive the full amount.
Include the AGA Research Foundation in your will or living trust. This gift can be made by including as little as one sentence in your will or living trust. Plus, your gift can be modified throughout your lifetime as circumstances change.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact Harmony Excellent at 301-272-1602 or hexcellent@gastro.org.
Creating a legacy of giving is easier than you think. As the new year begins, take some time to start creating your legacy while supporting the AGA Research Foundation. Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission continues even after your lifetime.
Here are two ideas to help you get started.
Name the AGA Research Foundation as a beneficiary. This arrangement is one of the most tax-smart ways to support the AGA Research Foundation after your lifetime. When you leave retirement plan assets to us, we bypass any taxes and receive the full amount.
Include the AGA Research Foundation in your will or living trust. This gift can be made by including as little as one sentence in your will or living trust. Plus, your gift can be modified throughout your lifetime as circumstances change.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact Harmony Excellent at 301-272-1602 or hexcellent@gastro.org.
Creating a legacy of giving is easier than you think. As the new year begins, take some time to start creating your legacy while supporting the AGA Research Foundation. Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission continues even after your lifetime.
Here are two ideas to help you get started.
Name the AGA Research Foundation as a beneficiary. This arrangement is one of the most tax-smart ways to support the AGA Research Foundation after your lifetime. When you leave retirement plan assets to us, we bypass any taxes and receive the full amount.
Include the AGA Research Foundation in your will or living trust. This gift can be made by including as little as one sentence in your will or living trust. Plus, your gift can be modified throughout your lifetime as circumstances change.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact Harmony Excellent at 301-272-1602 or hexcellent@gastro.org.
Talk to your patients about the current state of prebiotics
Bridgette Wilson, PhD, RD, postdoctoral research associate in nutritional sciences, and Kevin Whelan, PhD, RD, professor of dietetics, King’s College London, England, share talking points to help your patients understand what is currently known about the use of prebiotics for GI disorders.
Explaining prebiotics for GI disorders
Different prebiotic supplements have different effects on gut symptoms. For example, lower doses of noninulin type fructans (e.g., beta-galacto-oligosaccharides [GOS], pectin, partially hydrolyzed guar gum) are likely to be better tolerated in patients with functional gut symptoms, including irritable bowel syndrome (IBS).
Though prebiotic-containing foods are thought to benefit gut health in general, some prebiotics are FODMAPs that have been associated with symptoms in IBS patients. Individual patients on restrictive diets should systematically introduce prebiotic foods to identify the type and quantity they can tolerate.

Prebiotic supplementation of more than 10 g/d may soften stools and increase bowel movements in patients with defecation difficulty or constipation.
Prebiotic supplementation may worsen symptoms in Crohn’s disease but is well tolerated in ulcerative colitis, although there is no effect on disease activity.
These tips are from “The current state of prebiotics,” the third article of a four-part CME series on prebiotics. This activity is supported by an educational grant from GlaxoSmithKline. Part one, “Prebiotics 101,” and part two, “Diet vs. Prebiotics,” are available through AGA University (agau.gastro.org).
AGA also has educational materials for patients on probiotics, which can be accessed at www.gastro.org/probiotics in English and Spanish.
ginews@gastro.org
Bridgette Wilson, PhD, RD, postdoctoral research associate in nutritional sciences, and Kevin Whelan, PhD, RD, professor of dietetics, King’s College London, England, share talking points to help your patients understand what is currently known about the use of prebiotics for GI disorders.
Explaining prebiotics for GI disorders
Different prebiotic supplements have different effects on gut symptoms. For example, lower doses of noninulin type fructans (e.g., beta-galacto-oligosaccharides [GOS], pectin, partially hydrolyzed guar gum) are likely to be better tolerated in patients with functional gut symptoms, including irritable bowel syndrome (IBS).
Though prebiotic-containing foods are thought to benefit gut health in general, some prebiotics are FODMAPs that have been associated with symptoms in IBS patients. Individual patients on restrictive diets should systematically introduce prebiotic foods to identify the type and quantity they can tolerate.
Prebiotic supplementation of more than 10 g/d may soften stools and increase bowel movements in patients with defecation difficulty or constipation.
Prebiotic supplementation may worsen symptoms in Crohn’s disease but is well tolerated in ulcerative colitis, although there is no effect on disease activity.
These tips are from “The current state of prebiotics,” the third article of a four-part CME series on prebiotics. This activity is supported by an educational grant from GlaxoSmithKline. Part one, “Prebiotics 101,” and part two, “Diet vs. Prebiotics,” are available through AGA University (agau.gastro.org).
AGA also has educational materials for patients on probiotics, which can be accessed at www.gastro.org/probiotics in English and Spanish.
ginews@gastro.org
Bridgette Wilson, PhD, RD, postdoctoral research associate in nutritional sciences, and Kevin Whelan, PhD, RD, professor of dietetics, King’s College London, England, share talking points to help your patients understand what is currently known about the use of prebiotics for GI disorders.
Explaining prebiotics for GI disorders
Different prebiotic supplements have different effects on gut symptoms. For example, lower doses of noninulin type fructans (e.g., beta-galacto-oligosaccharides [GOS], pectin, partially hydrolyzed guar gum) are likely to be better tolerated in patients with functional gut symptoms, including irritable bowel syndrome (IBS).
Though prebiotic-containing foods are thought to benefit gut health in general, some prebiotics are FODMAPs that have been associated with symptoms in IBS patients. Individual patients on restrictive diets should systematically introduce prebiotic foods to identify the type and quantity they can tolerate.
Prebiotic supplementation of more than 10 g/d may soften stools and increase bowel movements in patients with defecation difficulty or constipation.
Prebiotic supplementation may worsen symptoms in Crohn’s disease but is well tolerated in ulcerative colitis, although there is no effect on disease activity.
These tips are from “The current state of prebiotics,” the third article of a four-part CME series on prebiotics. This activity is supported by an educational grant from GlaxoSmithKline. Part one, “Prebiotics 101,” and part two, “Diet vs. Prebiotics,” are available through AGA University (agau.gastro.org).
AGA also has educational materials for patients on probiotics, which can be accessed at www.gastro.org/probiotics in English and Spanish.
ginews@gastro.org
Step Therapy National Day of Advocacy
AGA and 17 other specialty physician and patient advocacy organizations partnered with the Digestive Disease National Coalition (DDNC) on an advocacy day focused on the need for step therapy reform.
We met with congressional offices to seek support for patient protection guardrails in step therapy and to encourage co-sponsorship of the Safe Step Act. This bipartisan legislation would create a clear process for a patient or physician to request an exception to a step therapy protocol. It also would require insurers to grant exemptions to step therapy in the following situations:
- Patient already tried and failed on a required treatment
- Delayed treatment will cause irreversible damage
- Required treatment will cause harm to the patient
- Required treatment will prevent a patient from working or fulling daily activities
- Patient is stable on their current treatment
AGA representatives and patient advocates met with the congressional offices of these legislators who serve on key committees that have jurisdiction over this issue.
Sen. Chris Van Hollen, D-Md
Sen. Tim Scott, R-S.C.
Sen. Thom Tillis, R-N.C.
Sen. Lamar Alexander, R-N.C.
Rep. Alma Adams, D-N.C.
Rep. Mark Walker, R-N.C.
Rep. Tim Walberg, R-Mich
A special thanks to AGA members who contacted your legislators online. A combination of 344 tweets and emails were sent urging federal legislators to support the Safe Step Act.
Sharing is caring
Legislators and their staff are always asking us for real-life examples from constituents about step therapy burdens to humanize the issue. Contact AGA staff at agaadvocacy@gastro.org to share your story.
AGA and 17 other specialty physician and patient advocacy organizations partnered with the Digestive Disease National Coalition (DDNC) on an advocacy day focused on the need for step therapy reform.
We met with congressional offices to seek support for patient protection guardrails in step therapy and to encourage co-sponsorship of the Safe Step Act. This bipartisan legislation would create a clear process for a patient or physician to request an exception to a step therapy protocol. It also would require insurers to grant exemptions to step therapy in the following situations:
- Patient already tried and failed on a required treatment
- Delayed treatment will cause irreversible damage
- Required treatment will cause harm to the patient
- Required treatment will prevent a patient from working or fulling daily activities
- Patient is stable on their current treatment
AGA representatives and patient advocates met with the congressional offices of these legislators who serve on key committees that have jurisdiction over this issue.
Sen. Chris Van Hollen, D-Md
Sen. Tim Scott, R-S.C.
Sen. Thom Tillis, R-N.C.
Sen. Lamar Alexander, R-N.C.
Rep. Alma Adams, D-N.C.
Rep. Mark Walker, R-N.C.
Rep. Tim Walberg, R-Mich
A special thanks to AGA members who contacted your legislators online. A combination of 344 tweets and emails were sent urging federal legislators to support the Safe Step Act.
Sharing is caring
Legislators and their staff are always asking us for real-life examples from constituents about step therapy burdens to humanize the issue. Contact AGA staff at agaadvocacy@gastro.org to share your story.
AGA and 17 other specialty physician and patient advocacy organizations partnered with the Digestive Disease National Coalition (DDNC) on an advocacy day focused on the need for step therapy reform.
We met with congressional offices to seek support for patient protection guardrails in step therapy and to encourage co-sponsorship of the Safe Step Act. This bipartisan legislation would create a clear process for a patient or physician to request an exception to a step therapy protocol. It also would require insurers to grant exemptions to step therapy in the following situations:
- Patient already tried and failed on a required treatment
- Delayed treatment will cause irreversible damage
- Required treatment will cause harm to the patient
- Required treatment will prevent a patient from working or fulling daily activities
- Patient is stable on their current treatment
AGA representatives and patient advocates met with the congressional offices of these legislators who serve on key committees that have jurisdiction over this issue.
Sen. Chris Van Hollen, D-Md
Sen. Tim Scott, R-S.C.
Sen. Thom Tillis, R-N.C.
Sen. Lamar Alexander, R-N.C.
Rep. Alma Adams, D-N.C.
Rep. Mark Walker, R-N.C.
Rep. Tim Walberg, R-Mich
A special thanks to AGA members who contacted your legislators online. A combination of 344 tweets and emails were sent urging federal legislators to support the Safe Step Act.
Sharing is caring
Legislators and their staff are always asking us for real-life examples from constituents about step therapy burdens to humanize the issue. Contact AGA staff at agaadvocacy@gastro.org to share your story.
GI societies advise FDA on duodenoscope reprocessing
AGA, ACG, ASGE and SAGES were represented by three physicians who made oral remarks to the panel: Michael Kochman, MD, AGAF, Wilmott Professor of Medicine and Surgery at the University of Pennsylvania; Bret Petersen, MD, FASGE, professor of medicine and advanced endoscopist at the Mayo Clinic in Rochester, Minn. and Danielle Walsh, MD, associate professor of surgery at East Carolina University.

The GI societies over-arching goal is to ensure patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
The panel discussed the adequacy/margin of safety for high-level disinfection, as well as the challenges and benefits of sterilization for routine for duodenoscope reprocessing. The panel’s consensus was that cleaning is the most important step in duodenoscope reprocessing. The panel noted that in properly cleaned duodenoscopes, high-level disinfection is appropriate; however, panel members acknowledged that reports indicate that duodenoscopes are not properly cleaned. The panel also discussed the challenges of implementing sterilization of duodenoscopes, such as potential decreased patient access to endoscopic retrograde cholangiopancreatography (ERCP) and increased costs.
On behalf of the GI societies, Dr. Kochman and Dr. Petersen proposed several overarching principles for the future evolution of our clinical practices focusing on patient safety and outcomes:
We encourage embracing multiple solutions, using a measured step-wise approach to the transition with both iterative and novel devices and processes.
We encourage data-based solutions addressing real-world efficacy while incorporating ongoing surveillance of processes and performance to ensure that early trouble signals are detected.
We believe that device or reprocessing transitions can be incorporated over the lifecycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology.
We accept minimizing extensive premarket studies, while expecting vigilant post-market surveillance, for technologies or device changes made exclusively with intent to convert to conceptually more safe designs without significant changes in mechanism or function.
We support the addition of durability testing for devices undergoing both standard reprocessing and, in particular, those undergoing sterilization.
Our societies are prepared to support and participate in continued discussion regarding:
Mandatory servicing and inspections.
Mandatory device retirement for reusable devices.
Assessment of the role and standards for third-party inspection and repair.
Our societies strongly support the importance and oversight of succinct, practical, reproducible, user-friendly guidance in manufacturers’ instructions for use (IFUs), which should incorporate post-market validation studies and updates.
We recommend that devices that incorporate programmable features (AERs, washers, sterilizers) should have lock-down mechanisms in place to prevent both user and manufacturer from deviating from the FDA-cleared IFU parameters for the device.
Our societies, as well as numerous guidelines, include high-level disinfection as a currently acceptable option for endoscope reprocessing, assuming use of enhanced washing and drying standards of practice.
Finally, we support the FDA in its efforts to convey to companies the necessary endpoints and goals for performance and expectations relative to post-market review and development of new data to ensure efficacy in the community.
Our societies appreciated this opportunity to comment on the complex and critical topic at hand. Our over-arching goal as physicians remains that of ensuring patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
ginews@gastro.org
AGA, ACG, ASGE and SAGES were represented by three physicians who made oral remarks to the panel: Michael Kochman, MD, AGAF, Wilmott Professor of Medicine and Surgery at the University of Pennsylvania; Bret Petersen, MD, FASGE, professor of medicine and advanced endoscopist at the Mayo Clinic in Rochester, Minn. and Danielle Walsh, MD, associate professor of surgery at East Carolina University.
The GI societies over-arching goal is to ensure patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
The panel discussed the adequacy/margin of safety for high-level disinfection, as well as the challenges and benefits of sterilization for routine for duodenoscope reprocessing. The panel’s consensus was that cleaning is the most important step in duodenoscope reprocessing. The panel noted that in properly cleaned duodenoscopes, high-level disinfection is appropriate; however, panel members acknowledged that reports indicate that duodenoscopes are not properly cleaned. The panel also discussed the challenges of implementing sterilization of duodenoscopes, such as potential decreased patient access to endoscopic retrograde cholangiopancreatography (ERCP) and increased costs.
On behalf of the GI societies, Dr. Kochman and Dr. Petersen proposed several overarching principles for the future evolution of our clinical practices focusing on patient safety and outcomes:
We encourage embracing multiple solutions, using a measured step-wise approach to the transition with both iterative and novel devices and processes.
We encourage data-based solutions addressing real-world efficacy while incorporating ongoing surveillance of processes and performance to ensure that early trouble signals are detected.
We believe that device or reprocessing transitions can be incorporated over the lifecycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology.
We accept minimizing extensive premarket studies, while expecting vigilant post-market surveillance, for technologies or device changes made exclusively with intent to convert to conceptually more safe designs without significant changes in mechanism or function.
We support the addition of durability testing for devices undergoing both standard reprocessing and, in particular, those undergoing sterilization.
Our societies are prepared to support and participate in continued discussion regarding:
Mandatory servicing and inspections.
Mandatory device retirement for reusable devices.
Assessment of the role and standards for third-party inspection and repair.
Our societies strongly support the importance and oversight of succinct, practical, reproducible, user-friendly guidance in manufacturers’ instructions for use (IFUs), which should incorporate post-market validation studies and updates.
We recommend that devices that incorporate programmable features (AERs, washers, sterilizers) should have lock-down mechanisms in place to prevent both user and manufacturer from deviating from the FDA-cleared IFU parameters for the device.
Our societies, as well as numerous guidelines, include high-level disinfection as a currently acceptable option for endoscope reprocessing, assuming use of enhanced washing and drying standards of practice.
Finally, we support the FDA in its efforts to convey to companies the necessary endpoints and goals for performance and expectations relative to post-market review and development of new data to ensure efficacy in the community.
Our societies appreciated this opportunity to comment on the complex and critical topic at hand. Our over-arching goal as physicians remains that of ensuring patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
ginews@gastro.org
AGA, ACG, ASGE and SAGES were represented by three physicians who made oral remarks to the panel: Michael Kochman, MD, AGAF, Wilmott Professor of Medicine and Surgery at the University of Pennsylvania; Bret Petersen, MD, FASGE, professor of medicine and advanced endoscopist at the Mayo Clinic in Rochester, Minn. and Danielle Walsh, MD, associate professor of surgery at East Carolina University.
The GI societies over-arching goal is to ensure patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
The panel discussed the adequacy/margin of safety for high-level disinfection, as well as the challenges and benefits of sterilization for routine for duodenoscope reprocessing. The panel’s consensus was that cleaning is the most important step in duodenoscope reprocessing. The panel noted that in properly cleaned duodenoscopes, high-level disinfection is appropriate; however, panel members acknowledged that reports indicate that duodenoscopes are not properly cleaned. The panel also discussed the challenges of implementing sterilization of duodenoscopes, such as potential decreased patient access to endoscopic retrograde cholangiopancreatography (ERCP) and increased costs.
On behalf of the GI societies, Dr. Kochman and Dr. Petersen proposed several overarching principles for the future evolution of our clinical practices focusing on patient safety and outcomes:
We encourage embracing multiple solutions, using a measured step-wise approach to the transition with both iterative and novel devices and processes.
We encourage data-based solutions addressing real-world efficacy while incorporating ongoing surveillance of processes and performance to ensure that early trouble signals are detected.
We believe that device or reprocessing transitions can be incorporated over the lifecycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology.
We accept minimizing extensive premarket studies, while expecting vigilant post-market surveillance, for technologies or device changes made exclusively with intent to convert to conceptually more safe designs without significant changes in mechanism or function.
We support the addition of durability testing for devices undergoing both standard reprocessing and, in particular, those undergoing sterilization.
Our societies are prepared to support and participate in continued discussion regarding:
Mandatory servicing and inspections.
Mandatory device retirement for reusable devices.
Assessment of the role and standards for third-party inspection and repair.
Our societies strongly support the importance and oversight of succinct, practical, reproducible, user-friendly guidance in manufacturers’ instructions for use (IFUs), which should incorporate post-market validation studies and updates.
We recommend that devices that incorporate programmable features (AERs, washers, sterilizers) should have lock-down mechanisms in place to prevent both user and manufacturer from deviating from the FDA-cleared IFU parameters for the device.
Our societies, as well as numerous guidelines, include high-level disinfection as a currently acceptable option for endoscope reprocessing, assuming use of enhanced washing and drying standards of practice.
Finally, we support the FDA in its efforts to convey to companies the necessary endpoints and goals for performance and expectations relative to post-market review and development of new data to ensure efficacy in the community.
Our societies appreciated this opportunity to comment on the complex and critical topic at hand. Our over-arching goal as physicians remains that of ensuring patient safety and ready access to clinically indicated procedures employing duodenoscopes and other elevator-channel endoscopes.
ginews@gastro.org