User login
Cesarean delivery reduces some risks, raises others
Cesarean deliveries may reduce a woman’s risk for urinary incontinence and pelvic organ prolapse but may raise her risk of complications with future pregnancies, based on data from a literature review including nearly 30,000,000 women.
Rates of cesarean delivery in 2016, often without medical indication, were approximately 25%, 32%, and 41% in Western Europe, North America, and South America, respectively, wrote Oonagh E. Keag, MD, of the Royal Infirmary of Edinburgh and colleagues in a study published in PLOS Medicine.
The researchers reviewed data from 79 observational studies and 1 randomized, controlled trial for a study population of 29,928,274 individuals.
Overall, women who had cesarean deliveries had a significantly lower risk of urinary incontinence (odds ratio, 0.56) and pelvic organ prolapse (OR, 0.29), compared with women who had vaginal deliveries.
No significant association appeared between type of delivery and risk of perinatal death, but women with a history of cesarean delivery were significantly more likely to experience miscarriage or stillbirth on a subsequent pregnancy, as well as placenta previa, placenta accreta, and placental abruption.
In addition, children born via cesarean delivery were significantly more likely than those born via vaginal delivery to have asthma at age 12 years (OR, 1.21) and to be obese up to age 5 years (OR, 1.59).
The findings were limited by the observational nature of most of the data, which does not imply causation, the researchers said. In addition, the study was not designed for subanalysis of elective vs. emergency cesarean delivery.
Although women will attach varying degrees of significance to the risks and benefits associated with cesarean delivery, “it is imperative that clinicians take care to ensure that women are made aware of any risk that they are likely to attach significance to,” the researchers said. “Women and clinicians thus should be aware of both the short- and long-term risks and benefits of cesarean delivery and discuss these when deciding on mode of delivery,” they noted.
The researchers had no financial conflicts to disclose.
SOURCE: Keag OE et al. PLoS Med. 2018 Jan 23. 15(1):e1002494.
As health care practitioners, ob.gyns. must continually evaluate potential consequences of a management strategy to our patients’ health and well-being. This is especially true when determining the best method of delivery – vaginal or cesarean section – because our approach can affect not only the mother but also the baby.
It is well known that vaginal deliveries can be associated with long-term complications for women, including pelvic floor disorders (that is, prolapse), pelvic injury, and incontinence. For women who have undergone a cesarean section, the uterine scars caused by the surgery can lead to increased risk for placenta previa or, more seriously, placenta accreta, as well as possible miscarriage or stillbirth.
Because the best possible care must also be informed care, every ob.gyn. should conduct periodic reviews of the scientific literature. Research continually advances our knowledge and our practice. For example, the recent work on the use of statins to prevent preeclampsia is an area of intense interest. Although we’ve known about hypertensive disorders of pregnancy for many years, management and prevention strategies are adequate at best. This new and exciting line of research has the potential to solve a conundrum we’ve grappled with for centuries.
The study by Keag et al. analyzes the findings from observational studies on the risks and benefits of cesarean versus vaginal delivery, within certain limitations. The study authors found that cesarean deliveries are associated with lower risk of urinary incontinence and pelvic prolapse, but higher risk of placenta previa, miscarriage, and stillbirth. Additionally, the authors reported that babies delivered by cesarean section had a higher risk of developing asthma and obesity.
Although the results of the study are not surprising, the findings reinforce the idea that ob.gyns must make decisions on a case-by-case basis and on obstetrical indications. We cannot use a set of possible complications as a reason to choose one delivery route over another. Every patient is unique. Every circumstance is unique. Every delivery requires us to make an informed decision to achieve the best possible outcome. Otherwise, we run the great risk of doing a disservice to our patients and their families.
E. Albert Reece, MD , PhD, MBA, specializes in maternal-fetal medicine and is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He has no relevant financial disclosures.
As health care practitioners, ob.gyns. must continually evaluate potential consequences of a management strategy to our patients’ health and well-being. This is especially true when determining the best method of delivery – vaginal or cesarean section – because our approach can affect not only the mother but also the baby.
It is well known that vaginal deliveries can be associated with long-term complications for women, including pelvic floor disorders (that is, prolapse), pelvic injury, and incontinence. For women who have undergone a cesarean section, the uterine scars caused by the surgery can lead to increased risk for placenta previa or, more seriously, placenta accreta, as well as possible miscarriage or stillbirth.
Because the best possible care must also be informed care, every ob.gyn. should conduct periodic reviews of the scientific literature. Research continually advances our knowledge and our practice. For example, the recent work on the use of statins to prevent preeclampsia is an area of intense interest. Although we’ve known about hypertensive disorders of pregnancy for many years, management and prevention strategies are adequate at best. This new and exciting line of research has the potential to solve a conundrum we’ve grappled with for centuries.
The study by Keag et al. analyzes the findings from observational studies on the risks and benefits of cesarean versus vaginal delivery, within certain limitations. The study authors found that cesarean deliveries are associated with lower risk of urinary incontinence and pelvic prolapse, but higher risk of placenta previa, miscarriage, and stillbirth. Additionally, the authors reported that babies delivered by cesarean section had a higher risk of developing asthma and obesity.
Although the results of the study are not surprising, the findings reinforce the idea that ob.gyns must make decisions on a case-by-case basis and on obstetrical indications. We cannot use a set of possible complications as a reason to choose one delivery route over another. Every patient is unique. Every circumstance is unique. Every delivery requires us to make an informed decision to achieve the best possible outcome. Otherwise, we run the great risk of doing a disservice to our patients and their families.
E. Albert Reece, MD , PhD, MBA, specializes in maternal-fetal medicine and is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He has no relevant financial disclosures.
As health care practitioners, ob.gyns. must continually evaluate potential consequences of a management strategy to our patients’ health and well-being. This is especially true when determining the best method of delivery – vaginal or cesarean section – because our approach can affect not only the mother but also the baby.
It is well known that vaginal deliveries can be associated with long-term complications for women, including pelvic floor disorders (that is, prolapse), pelvic injury, and incontinence. For women who have undergone a cesarean section, the uterine scars caused by the surgery can lead to increased risk for placenta previa or, more seriously, placenta accreta, as well as possible miscarriage or stillbirth.
Because the best possible care must also be informed care, every ob.gyn. should conduct periodic reviews of the scientific literature. Research continually advances our knowledge and our practice. For example, the recent work on the use of statins to prevent preeclampsia is an area of intense interest. Although we’ve known about hypertensive disorders of pregnancy for many years, management and prevention strategies are adequate at best. This new and exciting line of research has the potential to solve a conundrum we’ve grappled with for centuries.
The study by Keag et al. analyzes the findings from observational studies on the risks and benefits of cesarean versus vaginal delivery, within certain limitations. The study authors found that cesarean deliveries are associated with lower risk of urinary incontinence and pelvic prolapse, but higher risk of placenta previa, miscarriage, and stillbirth. Additionally, the authors reported that babies delivered by cesarean section had a higher risk of developing asthma and obesity.
Although the results of the study are not surprising, the findings reinforce the idea that ob.gyns must make decisions on a case-by-case basis and on obstetrical indications. We cannot use a set of possible complications as a reason to choose one delivery route over another. Every patient is unique. Every circumstance is unique. Every delivery requires us to make an informed decision to achieve the best possible outcome. Otherwise, we run the great risk of doing a disservice to our patients and their families.
E. Albert Reece, MD , PhD, MBA, specializes in maternal-fetal medicine and is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He has no relevant financial disclosures.
Cesarean deliveries may reduce a woman’s risk for urinary incontinence and pelvic organ prolapse but may raise her risk of complications with future pregnancies, based on data from a literature review including nearly 30,000,000 women.
Rates of cesarean delivery in 2016, often without medical indication, were approximately 25%, 32%, and 41% in Western Europe, North America, and South America, respectively, wrote Oonagh E. Keag, MD, of the Royal Infirmary of Edinburgh and colleagues in a study published in PLOS Medicine.
The researchers reviewed data from 79 observational studies and 1 randomized, controlled trial for a study population of 29,928,274 individuals.
Overall, women who had cesarean deliveries had a significantly lower risk of urinary incontinence (odds ratio, 0.56) and pelvic organ prolapse (OR, 0.29), compared with women who had vaginal deliveries.
No significant association appeared between type of delivery and risk of perinatal death, but women with a history of cesarean delivery were significantly more likely to experience miscarriage or stillbirth on a subsequent pregnancy, as well as placenta previa, placenta accreta, and placental abruption.
In addition, children born via cesarean delivery were significantly more likely than those born via vaginal delivery to have asthma at age 12 years (OR, 1.21) and to be obese up to age 5 years (OR, 1.59).
The findings were limited by the observational nature of most of the data, which does not imply causation, the researchers said. In addition, the study was not designed for subanalysis of elective vs. emergency cesarean delivery.
Although women will attach varying degrees of significance to the risks and benefits associated with cesarean delivery, “it is imperative that clinicians take care to ensure that women are made aware of any risk that they are likely to attach significance to,” the researchers said. “Women and clinicians thus should be aware of both the short- and long-term risks and benefits of cesarean delivery and discuss these when deciding on mode of delivery,” they noted.
The researchers had no financial conflicts to disclose.
SOURCE: Keag OE et al. PLoS Med. 2018 Jan 23. 15(1):e1002494.
Cesarean deliveries may reduce a woman’s risk for urinary incontinence and pelvic organ prolapse but may raise her risk of complications with future pregnancies, based on data from a literature review including nearly 30,000,000 women.
Rates of cesarean delivery in 2016, often without medical indication, were approximately 25%, 32%, and 41% in Western Europe, North America, and South America, respectively, wrote Oonagh E. Keag, MD, of the Royal Infirmary of Edinburgh and colleagues in a study published in PLOS Medicine.
The researchers reviewed data from 79 observational studies and 1 randomized, controlled trial for a study population of 29,928,274 individuals.
Overall, women who had cesarean deliveries had a significantly lower risk of urinary incontinence (odds ratio, 0.56) and pelvic organ prolapse (OR, 0.29), compared with women who had vaginal deliveries.
No significant association appeared between type of delivery and risk of perinatal death, but women with a history of cesarean delivery were significantly more likely to experience miscarriage or stillbirth on a subsequent pregnancy, as well as placenta previa, placenta accreta, and placental abruption.
In addition, children born via cesarean delivery were significantly more likely than those born via vaginal delivery to have asthma at age 12 years (OR, 1.21) and to be obese up to age 5 years (OR, 1.59).
The findings were limited by the observational nature of most of the data, which does not imply causation, the researchers said. In addition, the study was not designed for subanalysis of elective vs. emergency cesarean delivery.
Although women will attach varying degrees of significance to the risks and benefits associated with cesarean delivery, “it is imperative that clinicians take care to ensure that women are made aware of any risk that they are likely to attach significance to,” the researchers said. “Women and clinicians thus should be aware of both the short- and long-term risks and benefits of cesarean delivery and discuss these when deciding on mode of delivery,” they noted.
The researchers had no financial conflicts to disclose.
SOURCE: Keag OE et al. PLoS Med. 2018 Jan 23. 15(1):e1002494.
FROM PLOS MEDICINE
Key clinical point: Cesarean delivery was associated with a reduced risk for incontinence and prolapse.
Major finding: Urinary incontinence and pelvic organ prolapse were less likely after cesarean vs. vaginal deliveries (OR, 0.56 and 0.29, respectively).
Study details: The data come from a review of 80 studies.
Disclosures: The researchers had no financial conflicts to disclose.
Source: Keag OE et al. PLoS Med. 2018 Jan 23. 15(1):e1002494.
Protocols to reduce opioid use and shorten length of stay
While originally pioneered by European anesthesiologists and surgeons in Europe in the 1990s, enhanced recovery after surgery (ERAS) programs, also known as enhanced recovery protocols or fast-track surgery, have now gained popularity across the surgical spectrum within the United States. The goal of these programs is to utilize multidisciplinary and multimodal interventions to minimize the physiologic changes associated with surgery and thereby enhance the perioperative experience – reduced morbidity and mortality, shorter length of stay, less postoperative opioid use, and faster resumption to normal activity, at a decreased cost of care.

1. Enhanced patient education, including managing expectations.
2. Decreased perioperative fasting periods.
3. Blood volume and temperature maintenance intraoperatively.
4. Postoperative mobilization early and often.
5. Multimodal pain relief and nausea/vomiting prophylaxis.
6. Use of postoperative drains and catheters only as long as required.
Today, I have asked Kirsten Sasaki, MD, to discuss some of these ERAS concepts. I have asked Dr. Sasaki to especially focus on decreasing opioid utilization. For a thorough discussion on ERAS recommendations using an evidence-based approach, one can review two excellent papers by Nelson et al. (Gynecol Oncol. 2016 Feb;140[2]:313-22; Gynecol Oncol. 2016 Feb;140[2]:323-32).
Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston. Dr. Sasaki then went on to become our second fellow at the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and Society of Reproductive Surgeons at Advocate Lutheran General Hospital, Park Ridge, Ill. As a Fellow, Dr. Sasaki was recognized for her excellent teaching and research capabilities. Ultimately, however, it was her tremendous surgical skills and surgical sense that led me to invite her to join my practice in 2014.
Dr. Miller is a clinical associate professor at the University of Illinois in Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago and the director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. He has no disclosures relevant to this Master Class.
While originally pioneered by European anesthesiologists and surgeons in Europe in the 1990s, enhanced recovery after surgery (ERAS) programs, also known as enhanced recovery protocols or fast-track surgery, have now gained popularity across the surgical spectrum within the United States. The goal of these programs is to utilize multidisciplinary and multimodal interventions to minimize the physiologic changes associated with surgery and thereby enhance the perioperative experience – reduced morbidity and mortality, shorter length of stay, less postoperative opioid use, and faster resumption to normal activity, at a decreased cost of care.
1. Enhanced patient education, including managing expectations.
2. Decreased perioperative fasting periods.
3. Blood volume and temperature maintenance intraoperatively.
4. Postoperative mobilization early and often.
5. Multimodal pain relief and nausea/vomiting prophylaxis.
6. Use of postoperative drains and catheters only as long as required.
Today, I have asked Kirsten Sasaki, MD, to discuss some of these ERAS concepts. I have asked Dr. Sasaki to especially focus on decreasing opioid utilization. For a thorough discussion on ERAS recommendations using an evidence-based approach, one can review two excellent papers by Nelson et al. (Gynecol Oncol. 2016 Feb;140[2]:313-22; Gynecol Oncol. 2016 Feb;140[2]:323-32).
Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston. Dr. Sasaki then went on to become our second fellow at the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and Society of Reproductive Surgeons at Advocate Lutheran General Hospital, Park Ridge, Ill. As a Fellow, Dr. Sasaki was recognized for her excellent teaching and research capabilities. Ultimately, however, it was her tremendous surgical skills and surgical sense that led me to invite her to join my practice in 2014.
Dr. Miller is a clinical associate professor at the University of Illinois in Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago and the director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. He has no disclosures relevant to this Master Class.
While originally pioneered by European anesthesiologists and surgeons in Europe in the 1990s, enhanced recovery after surgery (ERAS) programs, also known as enhanced recovery protocols or fast-track surgery, have now gained popularity across the surgical spectrum within the United States. The goal of these programs is to utilize multidisciplinary and multimodal interventions to minimize the physiologic changes associated with surgery and thereby enhance the perioperative experience – reduced morbidity and mortality, shorter length of stay, less postoperative opioid use, and faster resumption to normal activity, at a decreased cost of care.
1. Enhanced patient education, including managing expectations.
2. Decreased perioperative fasting periods.
3. Blood volume and temperature maintenance intraoperatively.
4. Postoperative mobilization early and often.
5. Multimodal pain relief and nausea/vomiting prophylaxis.
6. Use of postoperative drains and catheters only as long as required.
Today, I have asked Kirsten Sasaki, MD, to discuss some of these ERAS concepts. I have asked Dr. Sasaki to especially focus on decreasing opioid utilization. For a thorough discussion on ERAS recommendations using an evidence-based approach, one can review two excellent papers by Nelson et al. (Gynecol Oncol. 2016 Feb;140[2]:313-22; Gynecol Oncol. 2016 Feb;140[2]:323-32).
Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston. Dr. Sasaki then went on to become our second fellow at the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and Society of Reproductive Surgeons at Advocate Lutheran General Hospital, Park Ridge, Ill. As a Fellow, Dr. Sasaki was recognized for her excellent teaching and research capabilities. Ultimately, however, it was her tremendous surgical skills and surgical sense that led me to invite her to join my practice in 2014.
Dr. Miller is a clinical associate professor at the University of Illinois in Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago and the director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. He has no disclosures relevant to this Master Class.

Supportive oncodermatology: Cancer advances spawn new subspecialty
Not too long ago at the Dana-Farber/Brigham and Women’s Cancer Center in Boston, a woman with widely metastatic melanoma, who had been planning her own funeral, was surprised when she had a phenomenal response to immunotherapy.
She was shocked to learn that her cancer was almost completely gone after 12 weeks, but she was stunned when she developed a rash that made her oncologist think she needed to stop treatment.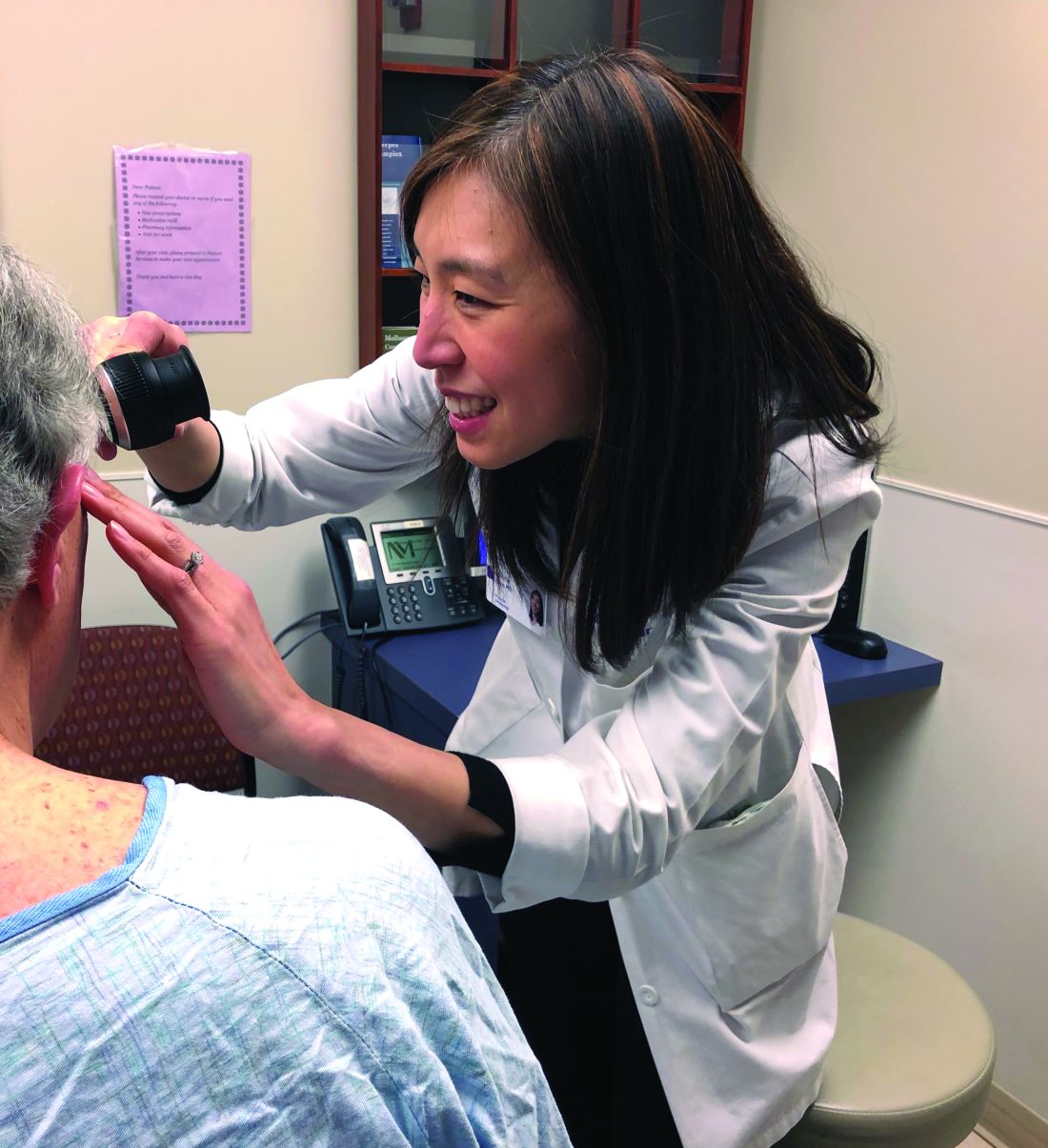
With traditional cytotoxic chemotherapies, there were a few well-defined skin side effects that oncologists were comfortable managing on their own with steroids or by reducing or stopping treatment for a bit.
But over the last decade, new cancer options have become available, most notably immunotherapies and targeted biologics, which are keeping some people alive longer but also causing cutaneous side effects that have never been seen before in oncology and are being reported frequently.
An urgent need

Currently in the United States, there’s only a handful of dedicated supportive oncodermatology services, which can be found at major academic cancer centers such as Dana-Farber/Brigham and Women’s, but the residents and fellows being trained at these centers are starting to fan out across the country and set up new services.
One day, it’s likely that every major cancer institution will have “a toxicities team with expert dermatologists,” said Dr. LeBoeuf, who launched the supportive oncodermatology program at Dana-Farber in 2014 and who now runs it with a team of dermatologists and clinics every week. Dr. LeBoeuf is a leader in the field, like the other dermatologists interviewed for this story.
With all the new treatments and with even more on the way, “there’s an urgent need for dermatologists to be involved in care of cancer patients,” Dr. LeBoeuf said.
The problem
Immunotherapies like the PD-1 blocking agents pembrolizumab (Keytruda) and nivolumab (Opdivo) – both used for an ever-expanding list of tumors – amp up the immune system to fight cancer, but they also tend to cause adverse events that mimic autoimmune diseases such as lupus, psoriasis, lichen planus, and vitiligo. Dermatologists are familiar with those problems and how to manage them, but oncologists generally are not.
Meanwhile, the many targeted therapies approved over the past decade interfere with specific molecules needed for tumor growth, but they also are associated with a wide range of skin, hair, and nail side effects that include skin growths, itching, paronychia, and more.
Agents that target vascular endothelial growth factors, such as sorafenib (Nexavar) and bevacizumab (Avastin), can trigger a painful hand-foot skin reaction that’s different from the hand-foot syndrome reported with older cytotoxic agents.
Epidermal growth factor receptor (EGFR) inhibitors, such as erlotinib (Tarceva) or gefitinib (Iressa), often cause miserable acne-like eruptions, but that can mean the drug is working.
It’s hard for oncologists to know what’s life-threatening and what isn’t; that’s where dermatologists come in.
A solution

When problems come up, oncologists and patients need answers right away, she said. There’s no time to wait a month or two for a dermatology appointment to find out whether, for instance, a new mouth ulcer is a minor inconvenience or the first sign of Stevens-Johnson syndrome, and the last thing an exhausted cancer patient needs is to be told to go to yet another clinic for a dermatology consult.
For supportive oncodermatology, that means being where the patients are: in the cancer centers. “Our clinic is situated on the same cancer floor as all the other oncology clinics,” which means easy access for both patients and oncologists, Dr. Choi said. “They just come down the hall.”
Build it, and they will come
The Stanford (Calif.) Cancer Center is a good example of what happens once a supportive oncodermatology service is up and running.
The program there was the brainchild of dermatologist Bernice Kwong, MD, who helped launch it in 2012 with 2 half-day outpatient clinics per week.
“Once people knew we were there seeing patients, we needed to expand it to 3 half days, and within 6 months, we knew we had to be” in the cancer center daily, she said. “The oncologists felt we were helping them keep their patients on treatment longer; they didn’t have to stop therapy to sort out a rash.”
Currently, the clinic sees about 15 to 20 patients a day, but “we have more need than that,” said Dr. Kwong, who is trying to recruit more dermatologists to help.
“The need is huge. There’s so much room for growth,” she noted, but first, “you need the oncologists to be on board.”
Dermatologist Adam Friedman, MD, director of supportive oncodermatology at the George Washington University Cancer Center, Washington, says his program is on the other end of the growth curve since it was only launched in the spring of 2017. Only about 80 patients have been treated so far, and there’s one dedicated clinic day a month, although he is on call for urgent cases, as is the case for many of the other dermatologists interviewed for this story.
Dr. Friedman expects business will pick up soon once word gets out, just like at Dana-Farber/Brigham and Women’s, Stanford, and elsewhere. “The places with the greatest need are going to have these services first, and then you’ll see them pop up elsewhere. I think we are going to see more,” he said.
The birth of supportive oncodermatology
Dermatologist Mario Lacouture, MD, director of the oncodermatology program at Memorial Sloan Kettering Cancer Center, New York, is considered by many oncodermatologists to be the father of the field.
He started the very first program in 2005 at Northwestern University, Chicago, followed by the program at Sloan Kettering a few years later. He has helped train many of the leaders in the field and coined the phrase “supportive oncodermatology” as the senior author in the field’s seminal paper, published in 2011 (J Am Acad Dermatol. 2011 Sep;65[3]:624-35). That article, in turn, inspired at least a few young dermatologists to make supportive oncodermatology their career choice. Dr. Lacouture speaks regularly at oncology and dermatology meetings to raise awareness about how dermatologists can improve cancer care.
Cancer survivors were also a concern. “Cancer treatment has improved so much that people are living longer, but the majority of survivors have either temporary or permanent cutaneous problems that would benefit from dermatologic care. However, the oncology community and patients are usually not aware that there are things we can do to help,” Dr. Lacouture said.
The message seems to have gotten out, however, among the hundreds of oncologists affiliated with Sloan Kettering. Dr. Lacouture needs a team of supportive oncodermatologists to meet the demand, with walk-in clinics every day and round-the-clock call.
He anticipates a day when visiting a supportive oncodermatologist will be routine, even before the start of cancer treatment, just as people visit a dentist before bone marrow transplants or radiation treatment to the head and neck. The idea would be to prevent cutaneous toxicity, something Dr. Lacouture and his team are already doing at Sloan Kettering. In time, supportive oncodermatology “is something that is going to be instituted early on” in treatment, he said.
“It’s important for dermatologists to reach out to their local oncologists; they will see there are many, many cancer patients and survivors who would benefit immensely from their care,” he said.
Dr. Lacouture is a consultant for Galderma, Janssen, and Johnson & Johnson. The other dermatologists interviewed for this story had no relevant industry disclosures. La Roche-Posay, a subsidiary of L’Oreal, is helping fund the supportive oncodermatology program at George Washington University. The company is interested in using cosmetics to camouflage cancer treatment skin lesions, Dr. Friedman said. Dr. Friedman is a member of the Dermatology News advisory board.
aotto@frontlinemedcom.com
Not too long ago at the Dana-Farber/Brigham and Women’s Cancer Center in Boston, a woman with widely metastatic melanoma, who had been planning her own funeral, was surprised when she had a phenomenal response to immunotherapy.
She was shocked to learn that her cancer was almost completely gone after 12 weeks, but she was stunned when she developed a rash that made her oncologist think she needed to stop treatment.
With traditional cytotoxic chemotherapies, there were a few well-defined skin side effects that oncologists were comfortable managing on their own with steroids or by reducing or stopping treatment for a bit.
But over the last decade, new cancer options have become available, most notably immunotherapies and targeted biologics, which are keeping some people alive longer but also causing cutaneous side effects that have never been seen before in oncology and are being reported frequently.
An urgent need
Currently in the United States, there’s only a handful of dedicated supportive oncodermatology services, which can be found at major academic cancer centers such as Dana-Farber/Brigham and Women’s, but the residents and fellows being trained at these centers are starting to fan out across the country and set up new services.
One day, it’s likely that every major cancer institution will have “a toxicities team with expert dermatologists,” said Dr. LeBoeuf, who launched the supportive oncodermatology program at Dana-Farber in 2014 and who now runs it with a team of dermatologists and clinics every week. Dr. LeBoeuf is a leader in the field, like the other dermatologists interviewed for this story.
With all the new treatments and with even more on the way, “there’s an urgent need for dermatologists to be involved in care of cancer patients,” Dr. LeBoeuf said.
The problem
Immunotherapies like the PD-1 blocking agents pembrolizumab (Keytruda) and nivolumab (Opdivo) – both used for an ever-expanding list of tumors – amp up the immune system to fight cancer, but they also tend to cause adverse events that mimic autoimmune diseases such as lupus, psoriasis, lichen planus, and vitiligo. Dermatologists are familiar with those problems and how to manage them, but oncologists generally are not.
Meanwhile, the many targeted therapies approved over the past decade interfere with specific molecules needed for tumor growth, but they also are associated with a wide range of skin, hair, and nail side effects that include skin growths, itching, paronychia, and more.
Agents that target vascular endothelial growth factors, such as sorafenib (Nexavar) and bevacizumab (Avastin), can trigger a painful hand-foot skin reaction that’s different from the hand-foot syndrome reported with older cytotoxic agents.
Epidermal growth factor receptor (EGFR) inhibitors, such as erlotinib (Tarceva) or gefitinib (Iressa), often cause miserable acne-like eruptions, but that can mean the drug is working.
It’s hard for oncologists to know what’s life-threatening and what isn’t; that’s where dermatologists come in.
A solution
When problems come up, oncologists and patients need answers right away, she said. There’s no time to wait a month or two for a dermatology appointment to find out whether, for instance, a new mouth ulcer is a minor inconvenience or the first sign of Stevens-Johnson syndrome, and the last thing an exhausted cancer patient needs is to be told to go to yet another clinic for a dermatology consult.
For supportive oncodermatology, that means being where the patients are: in the cancer centers. “Our clinic is situated on the same cancer floor as all the other oncology clinics,” which means easy access for both patients and oncologists, Dr. Choi said. “They just come down the hall.”
Build it, and they will come
The Stanford (Calif.) Cancer Center is a good example of what happens once a supportive oncodermatology service is up and running.
The program there was the brainchild of dermatologist Bernice Kwong, MD, who helped launch it in 2012 with 2 half-day outpatient clinics per week.
“Once people knew we were there seeing patients, we needed to expand it to 3 half days, and within 6 months, we knew we had to be” in the cancer center daily, she said. “The oncologists felt we were helping them keep their patients on treatment longer; they didn’t have to stop therapy to sort out a rash.”
Currently, the clinic sees about 15 to 20 patients a day, but “we have more need than that,” said Dr. Kwong, who is trying to recruit more dermatologists to help.
“The need is huge. There’s so much room for growth,” she noted, but first, “you need the oncologists to be on board.”
Dermatologist Adam Friedman, MD, director of supportive oncodermatology at the George Washington University Cancer Center, Washington, says his program is on the other end of the growth curve since it was only launched in the spring of 2017. Only about 80 patients have been treated so far, and there’s one dedicated clinic day a month, although he is on call for urgent cases, as is the case for many of the other dermatologists interviewed for this story.
Dr. Friedman expects business will pick up soon once word gets out, just like at Dana-Farber/Brigham and Women’s, Stanford, and elsewhere. “The places with the greatest need are going to have these services first, and then you’ll see them pop up elsewhere. I think we are going to see more,” he said.
The birth of supportive oncodermatology
Dermatologist Mario Lacouture, MD, director of the oncodermatology program at Memorial Sloan Kettering Cancer Center, New York, is considered by many oncodermatologists to be the father of the field.
He started the very first program in 2005 at Northwestern University, Chicago, followed by the program at Sloan Kettering a few years later. He has helped train many of the leaders in the field and coined the phrase “supportive oncodermatology” as the senior author in the field’s seminal paper, published in 2011 (J Am Acad Dermatol. 2011 Sep;65[3]:624-35). That article, in turn, inspired at least a few young dermatologists to make supportive oncodermatology their career choice. Dr. Lacouture speaks regularly at oncology and dermatology meetings to raise awareness about how dermatologists can improve cancer care.
Cancer survivors were also a concern. “Cancer treatment has improved so much that people are living longer, but the majority of survivors have either temporary or permanent cutaneous problems that would benefit from dermatologic care. However, the oncology community and patients are usually not aware that there are things we can do to help,” Dr. Lacouture said.
The message seems to have gotten out, however, among the hundreds of oncologists affiliated with Sloan Kettering. Dr. Lacouture needs a team of supportive oncodermatologists to meet the demand, with walk-in clinics every day and round-the-clock call.
He anticipates a day when visiting a supportive oncodermatologist will be routine, even before the start of cancer treatment, just as people visit a dentist before bone marrow transplants or radiation treatment to the head and neck. The idea would be to prevent cutaneous toxicity, something Dr. Lacouture and his team are already doing at Sloan Kettering. In time, supportive oncodermatology “is something that is going to be instituted early on” in treatment, he said.
“It’s important for dermatologists to reach out to their local oncologists; they will see there are many, many cancer patients and survivors who would benefit immensely from their care,” he said.
Dr. Lacouture is a consultant for Galderma, Janssen, and Johnson & Johnson. The other dermatologists interviewed for this story had no relevant industry disclosures. La Roche-Posay, a subsidiary of L’Oreal, is helping fund the supportive oncodermatology program at George Washington University. The company is interested in using cosmetics to camouflage cancer treatment skin lesions, Dr. Friedman said. Dr. Friedman is a member of the Dermatology News advisory board.
aotto@frontlinemedcom.com
Not too long ago at the Dana-Farber/Brigham and Women’s Cancer Center in Boston, a woman with widely metastatic melanoma, who had been planning her own funeral, was surprised when she had a phenomenal response to immunotherapy.
She was shocked to learn that her cancer was almost completely gone after 12 weeks, but she was stunned when she developed a rash that made her oncologist think she needed to stop treatment.
With traditional cytotoxic chemotherapies, there were a few well-defined skin side effects that oncologists were comfortable managing on their own with steroids or by reducing or stopping treatment for a bit.
But over the last decade, new cancer options have become available, most notably immunotherapies and targeted biologics, which are keeping some people alive longer but also causing cutaneous side effects that have never been seen before in oncology and are being reported frequently.
An urgent need
Currently in the United States, there’s only a handful of dedicated supportive oncodermatology services, which can be found at major academic cancer centers such as Dana-Farber/Brigham and Women’s, but the residents and fellows being trained at these centers are starting to fan out across the country and set up new services.
One day, it’s likely that every major cancer institution will have “a toxicities team with expert dermatologists,” said Dr. LeBoeuf, who launched the supportive oncodermatology program at Dana-Farber in 2014 and who now runs it with a team of dermatologists and clinics every week. Dr. LeBoeuf is a leader in the field, like the other dermatologists interviewed for this story.
With all the new treatments and with even more on the way, “there’s an urgent need for dermatologists to be involved in care of cancer patients,” Dr. LeBoeuf said.
The problem
Immunotherapies like the PD-1 blocking agents pembrolizumab (Keytruda) and nivolumab (Opdivo) – both used for an ever-expanding list of tumors – amp up the immune system to fight cancer, but they also tend to cause adverse events that mimic autoimmune diseases such as lupus, psoriasis, lichen planus, and vitiligo. Dermatologists are familiar with those problems and how to manage them, but oncologists generally are not.
Meanwhile, the many targeted therapies approved over the past decade interfere with specific molecules needed for tumor growth, but they also are associated with a wide range of skin, hair, and nail side effects that include skin growths, itching, paronychia, and more.
Agents that target vascular endothelial growth factors, such as sorafenib (Nexavar) and bevacizumab (Avastin), can trigger a painful hand-foot skin reaction that’s different from the hand-foot syndrome reported with older cytotoxic agents.
Epidermal growth factor receptor (EGFR) inhibitors, such as erlotinib (Tarceva) or gefitinib (Iressa), often cause miserable acne-like eruptions, but that can mean the drug is working.
It’s hard for oncologists to know what’s life-threatening and what isn’t; that’s where dermatologists come in.
A solution
When problems come up, oncologists and patients need answers right away, she said. There’s no time to wait a month or two for a dermatology appointment to find out whether, for instance, a new mouth ulcer is a minor inconvenience or the first sign of Stevens-Johnson syndrome, and the last thing an exhausted cancer patient needs is to be told to go to yet another clinic for a dermatology consult.
For supportive oncodermatology, that means being where the patients are: in the cancer centers. “Our clinic is situated on the same cancer floor as all the other oncology clinics,” which means easy access for both patients and oncologists, Dr. Choi said. “They just come down the hall.”
Build it, and they will come
The Stanford (Calif.) Cancer Center is a good example of what happens once a supportive oncodermatology service is up and running.
The program there was the brainchild of dermatologist Bernice Kwong, MD, who helped launch it in 2012 with 2 half-day outpatient clinics per week.
“Once people knew we were there seeing patients, we needed to expand it to 3 half days, and within 6 months, we knew we had to be” in the cancer center daily, she said. “The oncologists felt we were helping them keep their patients on treatment longer; they didn’t have to stop therapy to sort out a rash.”
Currently, the clinic sees about 15 to 20 patients a day, but “we have more need than that,” said Dr. Kwong, who is trying to recruit more dermatologists to help.
“The need is huge. There’s so much room for growth,” she noted, but first, “you need the oncologists to be on board.”
Dermatologist Adam Friedman, MD, director of supportive oncodermatology at the George Washington University Cancer Center, Washington, says his program is on the other end of the growth curve since it was only launched in the spring of 2017. Only about 80 patients have been treated so far, and there’s one dedicated clinic day a month, although he is on call for urgent cases, as is the case for many of the other dermatologists interviewed for this story.
Dr. Friedman expects business will pick up soon once word gets out, just like at Dana-Farber/Brigham and Women’s, Stanford, and elsewhere. “The places with the greatest need are going to have these services first, and then you’ll see them pop up elsewhere. I think we are going to see more,” he said.
The birth of supportive oncodermatology
Dermatologist Mario Lacouture, MD, director of the oncodermatology program at Memorial Sloan Kettering Cancer Center, New York, is considered by many oncodermatologists to be the father of the field.
He started the very first program in 2005 at Northwestern University, Chicago, followed by the program at Sloan Kettering a few years later. He has helped train many of the leaders in the field and coined the phrase “supportive oncodermatology” as the senior author in the field’s seminal paper, published in 2011 (J Am Acad Dermatol. 2011 Sep;65[3]:624-35). That article, in turn, inspired at least a few young dermatologists to make supportive oncodermatology their career choice. Dr. Lacouture speaks regularly at oncology and dermatology meetings to raise awareness about how dermatologists can improve cancer care.
Cancer survivors were also a concern. “Cancer treatment has improved so much that people are living longer, but the majority of survivors have either temporary or permanent cutaneous problems that would benefit from dermatologic care. However, the oncology community and patients are usually not aware that there are things we can do to help,” Dr. Lacouture said.
The message seems to have gotten out, however, among the hundreds of oncologists affiliated with Sloan Kettering. Dr. Lacouture needs a team of supportive oncodermatologists to meet the demand, with walk-in clinics every day and round-the-clock call.
He anticipates a day when visiting a supportive oncodermatologist will be routine, even before the start of cancer treatment, just as people visit a dentist before bone marrow transplants or radiation treatment to the head and neck. The idea would be to prevent cutaneous toxicity, something Dr. Lacouture and his team are already doing at Sloan Kettering. In time, supportive oncodermatology “is something that is going to be instituted early on” in treatment, he said.
“It’s important for dermatologists to reach out to their local oncologists; they will see there are many, many cancer patients and survivors who would benefit immensely from their care,” he said.
Dr. Lacouture is a consultant for Galderma, Janssen, and Johnson & Johnson. The other dermatologists interviewed for this story had no relevant industry disclosures. La Roche-Posay, a subsidiary of L’Oreal, is helping fund the supportive oncodermatology program at George Washington University. The company is interested in using cosmetics to camouflage cancer treatment skin lesions, Dr. Friedman said. Dr. Friedman is a member of the Dermatology News advisory board.
aotto@frontlinemedcom.com
Almost 40% of pediatric residents experience burnout, study finds
, according to two Pediatrics articles highlighted by editor in chief Lewis R. First, MD, MS.
The studies investigated the prevalence and effects of burnout among pediatric residents, and all health care providers, working in intensive care units. They were among those published in 2017 that Dr. First deemed potentially practice changing – ones whose clinical implications may have immediate relevance in your daily work.
“There are a variety of ways to overcome burnout and promote our resiliency that starts with our ability to find joy in caring for children and our lifelong learning” through professional development sessions and academic journals, according to Dr. First, professor and chair of pediatrics at the University of Vermont in Burlington. He also serves as chief of pediatrics at the University of Vermont Children’s Hospital. He spoke at the 2017 annual meeting of the American Academy of Pediatrics and in later interviews.
High prevalence of burnout
The study by Baer et al. found that almost two in five pediatric residents experience burnout, often accompanied by poorer care of patients (Pediatrics. 2017. doi: 10.1542/peds.2016-2163). Using a 7-point Likert scale ranging from “never” to “every day,” 258 residents from 11 different residency programs filled out an anonymous Web-based survey on how often they felt emotional exhaustion (“I feel burnout from my work”) and depersonalization (“I’ve become more callous toward people since I took this job”). 
Of the 258 respondents, 39% had burnout, defined as answering affirmatively to either of the above questions with at least “weekly.” Most of the respondents were female, white, and married or in a long-term relationship without children, but the burnout rates did not vary across gender, race/ethnicity, relationship or parental status, or among different characteristics of the residency program and schedule. Higher burnout rates did occur among those feeling sleep deprived.
Those with burnout also had substantially higher odds of providing lower-quality care. Residents with burnout were seven times more likely to make treatment or medication errors not related to inadequate knowledge or experience, six times more likely to feel guilty about how they had treated a patient, more than four times more likely to report having little emotional reaction to a patient’s death, and four times more likely to discharge a patient earlier to make service more manageable. Burned-out residents had more than nine times greater odds of paying “little attention to the social or personal impact of an illness on a patient,” the study showed.
Burnout symptoms and solutions
Symptoms of potential burnout, Dr. First said in an interview, include emotional exhaustion, feeling a loss of meaning in work, feelings of ineffectiveness, a tendency to view people as objects instead of human beings, increasingly poor communication, and poor interpersonal and clinical skills and behaviors.

Other research also has found burnout linked to doctors’ errors, self-reported negative attitudes toward patients, and less time spent with patients, she said. “Thus physicians should be on the lookout for burnout within themselves as well as in their colleagues and medical trainees.”
Both Dr. Baer and Dr. First noted the importance of organizational leadership in preventing burnout.
The Association of Medical School Pediatric Department Chairs is sharing a toolbox of strategies that they have found effective for reducing burnout and developing wellness among physicians, Dr. First said in the interview.
“Some of those suggestions include personal attention to wellness via good nutrition, exercise, mindfulness for emotional self-regulation, and developing supportive relationships,” he noted. In addition to organizational mindfulness programs and ones that foster work-life integration and social activities, prevention programs should “create wellness and resilience, and a sense of pride and meaning in the work that is being done.”
Drs. First also pointed to ways of addressing triggers of burnout:
- Reduce the burden of bureaucratic tasks.
- Examine how many hours physicians spend at home or work at home.
- Improve efficiency, such as in EHR use.
- Provide individuals time to discuss stressors and ways to resolve them collaboratively with peers and leadership.
Burnout risk in the NICU
Similar interventions may help with burnout in neonatal ICUs (NICUs), the focus of the second study Dr. First discussed. Tawfik et al. surveyed 2,760 personnel from 41 NICUs in the United States to learn the prevalence of burnout and how it was associated with NICU organization (Pediatrics. 2017. doi: 10.1542/peds.2016-4134).
Among the 1,934 providers who replied (a response rate of 70%), 27% had burnout; at individual NICUs, burnout prevalence varied from 8% to 43%. The majority of respondents (72%) were registered nurses, followed by respiratory therapists, physicians, neonatal nurse practitioners, and others. The highest burnout rates occurred in NICUs with higher average daily admissions and higher average occupancy – and those using EHRs.
“Don’t assume that just because you use the EHR every day means you know how best to use this tool to improve your efficiency and effectiveness in generating and deriving information on your patients,” Dr. First said in the interview. He encouraged physicians to find out what resources their institutions might offer to help, such as EHR hospital teams or office support who can look at providers’ EHR usage, and show them shortcuts and time-savers to improve efficiency based on their usage patterns.
“Nursing burnout was more sensitive to the setting than physician burnout, especially in regard to average daily admissions, late transfer numbers, nursing hours per patient day, and mortality per 1,000 infants,” Dr. First noted.
Interestingly, burnout prevalence was not associated with the proportion of high-risk patients seen in the NICUs, the number of attending physicians in the unit, or whether the institution was a teaching hospital or not, he said.
Dr. First listed strategies to reduce burnout risk in NICUs that the study authors also described: expressing thankfulness each day, focusing on positive events at the start or end of each day, performing random acts of kindness for colleagues and staff, and encouraging providers to identify the strengths in one another.
Addressing burnout requires efforts from everyone
“Given the potential effects of burnout on patient care and professionalism and physician wellness, it is important for physicians to speak up if they have concerns about burnout in their colleagues,” Dr. Baer said in the interview.
Burnout is common, she said, occurring in more than half of physicians at some point in time, so a doctor experiencing it is almost certainly not alone among colleagues.
“Physicians can work together and with their leadership to prevent and mitigate the effects of burnout by promoting personal and professional wellness, effective teamwork, and reducing the administrative burdens that impact time spent directly with patients and have been demonstrated to contribute to physician burnout,” Dr. Baer noted.
She also pointed to the need to address it in medical education, given the downstream risks of burnout on the next generation of physicians.
“Medical schools and residency and fellowship programs should address the risks and signs of burnout, as medical students and trainees are likely seeing signs of burnout in some of their physician teachers and mentors,” Dr. Baer said in the interview.
Some burnout among providers may be inevitable at times, but it’s important to continue looking for ways to combat it.
“We need to do more to remind each other of why we chose our profession, and how good it makes us feel to strive to make a difference in our patients and families each and every day,” Dr. First said in the interview.
Dr. First reported having no disclosures and no external funding. The residents’ study by Baer et al. was funded by the Boston Children’s Hospital’s Fred Lovejoy Resident Research Award and a grant from the Health Resources and Services Administration. The NICU study by Tamfik et al. was funded by the National Institutes of Health, grants from the National Institute of Child Health and Human Development, and the Jackson Vaughan Critical Care Research Fund. The authors of both studies had no relevant financial disclosures.
, according to two Pediatrics articles highlighted by editor in chief Lewis R. First, MD, MS.
The studies investigated the prevalence and effects of burnout among pediatric residents, and all health care providers, working in intensive care units. They were among those published in 2017 that Dr. First deemed potentially practice changing – ones whose clinical implications may have immediate relevance in your daily work.
“There are a variety of ways to overcome burnout and promote our resiliency that starts with our ability to find joy in caring for children and our lifelong learning” through professional development sessions and academic journals, according to Dr. First, professor and chair of pediatrics at the University of Vermont in Burlington. He also serves as chief of pediatrics at the University of Vermont Children’s Hospital. He spoke at the 2017 annual meeting of the American Academy of Pediatrics and in later interviews.
High prevalence of burnout
The study by Baer et al. found that almost two in five pediatric residents experience burnout, often accompanied by poorer care of patients (Pediatrics. 2017. doi: 10.1542/peds.2016-2163). Using a 7-point Likert scale ranging from “never” to “every day,” 258 residents from 11 different residency programs filled out an anonymous Web-based survey on how often they felt emotional exhaustion (“I feel burnout from my work”) and depersonalization (“I’ve become more callous toward people since I took this job”).
Of the 258 respondents, 39% had burnout, defined as answering affirmatively to either of the above questions with at least “weekly.” Most of the respondents were female, white, and married or in a long-term relationship without children, but the burnout rates did not vary across gender, race/ethnicity, relationship or parental status, or among different characteristics of the residency program and schedule. Higher burnout rates did occur among those feeling sleep deprived.
Those with burnout also had substantially higher odds of providing lower-quality care. Residents with burnout were seven times more likely to make treatment or medication errors not related to inadequate knowledge or experience, six times more likely to feel guilty about how they had treated a patient, more than four times more likely to report having little emotional reaction to a patient’s death, and four times more likely to discharge a patient earlier to make service more manageable. Burned-out residents had more than nine times greater odds of paying “little attention to the social or personal impact of an illness on a patient,” the study showed.
Burnout symptoms and solutions
Symptoms of potential burnout, Dr. First said in an interview, include emotional exhaustion, feeling a loss of meaning in work, feelings of ineffectiveness, a tendency to view people as objects instead of human beings, increasingly poor communication, and poor interpersonal and clinical skills and behaviors.
Other research also has found burnout linked to doctors’ errors, self-reported negative attitudes toward patients, and less time spent with patients, she said. “Thus physicians should be on the lookout for burnout within themselves as well as in their colleagues and medical trainees.”
Both Dr. Baer and Dr. First noted the importance of organizational leadership in preventing burnout.
The Association of Medical School Pediatric Department Chairs is sharing a toolbox of strategies that they have found effective for reducing burnout and developing wellness among physicians, Dr. First said in the interview.
“Some of those suggestions include personal attention to wellness via good nutrition, exercise, mindfulness for emotional self-regulation, and developing supportive relationships,” he noted. In addition to organizational mindfulness programs and ones that foster work-life integration and social activities, prevention programs should “create wellness and resilience, and a sense of pride and meaning in the work that is being done.”
Drs. First also pointed to ways of addressing triggers of burnout:
- Reduce the burden of bureaucratic tasks.
- Examine how many hours physicians spend at home or work at home.
- Improve efficiency, such as in EHR use.
- Provide individuals time to discuss stressors and ways to resolve them collaboratively with peers and leadership.
Burnout risk in the NICU
Similar interventions may help with burnout in neonatal ICUs (NICUs), the focus of the second study Dr. First discussed. Tawfik et al. surveyed 2,760 personnel from 41 NICUs in the United States to learn the prevalence of burnout and how it was associated with NICU organization (Pediatrics. 2017. doi: 10.1542/peds.2016-4134).
Among the 1,934 providers who replied (a response rate of 70%), 27% had burnout; at individual NICUs, burnout prevalence varied from 8% to 43%. The majority of respondents (72%) were registered nurses, followed by respiratory therapists, physicians, neonatal nurse practitioners, and others. The highest burnout rates occurred in NICUs with higher average daily admissions and higher average occupancy – and those using EHRs.
“Don’t assume that just because you use the EHR every day means you know how best to use this tool to improve your efficiency and effectiveness in generating and deriving information on your patients,” Dr. First said in the interview. He encouraged physicians to find out what resources their institutions might offer to help, such as EHR hospital teams or office support who can look at providers’ EHR usage, and show them shortcuts and time-savers to improve efficiency based on their usage patterns.
“Nursing burnout was more sensitive to the setting than physician burnout, especially in regard to average daily admissions, late transfer numbers, nursing hours per patient day, and mortality per 1,000 infants,” Dr. First noted.
Interestingly, burnout prevalence was not associated with the proportion of high-risk patients seen in the NICUs, the number of attending physicians in the unit, or whether the institution was a teaching hospital or not, he said.
Dr. First listed strategies to reduce burnout risk in NICUs that the study authors also described: expressing thankfulness each day, focusing on positive events at the start or end of each day, performing random acts of kindness for colleagues and staff, and encouraging providers to identify the strengths in one another.
Addressing burnout requires efforts from everyone
“Given the potential effects of burnout on patient care and professionalism and physician wellness, it is important for physicians to speak up if they have concerns about burnout in their colleagues,” Dr. Baer said in the interview.
Burnout is common, she said, occurring in more than half of physicians at some point in time, so a doctor experiencing it is almost certainly not alone among colleagues.
“Physicians can work together and with their leadership to prevent and mitigate the effects of burnout by promoting personal and professional wellness, effective teamwork, and reducing the administrative burdens that impact time spent directly with patients and have been demonstrated to contribute to physician burnout,” Dr. Baer noted.
She also pointed to the need to address it in medical education, given the downstream risks of burnout on the next generation of physicians.
“Medical schools and residency and fellowship programs should address the risks and signs of burnout, as medical students and trainees are likely seeing signs of burnout in some of their physician teachers and mentors,” Dr. Baer said in the interview.
Some burnout among providers may be inevitable at times, but it’s important to continue looking for ways to combat it.
“We need to do more to remind each other of why we chose our profession, and how good it makes us feel to strive to make a difference in our patients and families each and every day,” Dr. First said in the interview.
Dr. First reported having no disclosures and no external funding. The residents’ study by Baer et al. was funded by the Boston Children’s Hospital’s Fred Lovejoy Resident Research Award and a grant from the Health Resources and Services Administration. The NICU study by Tamfik et al. was funded by the National Institutes of Health, grants from the National Institute of Child Health and Human Development, and the Jackson Vaughan Critical Care Research Fund. The authors of both studies had no relevant financial disclosures.
, according to two Pediatrics articles highlighted by editor in chief Lewis R. First, MD, MS.
The studies investigated the prevalence and effects of burnout among pediatric residents, and all health care providers, working in intensive care units. They were among those published in 2017 that Dr. First deemed potentially practice changing – ones whose clinical implications may have immediate relevance in your daily work.
“There are a variety of ways to overcome burnout and promote our resiliency that starts with our ability to find joy in caring for children and our lifelong learning” through professional development sessions and academic journals, according to Dr. First, professor and chair of pediatrics at the University of Vermont in Burlington. He also serves as chief of pediatrics at the University of Vermont Children’s Hospital. He spoke at the 2017 annual meeting of the American Academy of Pediatrics and in later interviews.
High prevalence of burnout
The study by Baer et al. found that almost two in five pediatric residents experience burnout, often accompanied by poorer care of patients (Pediatrics. 2017. doi: 10.1542/peds.2016-2163). Using a 7-point Likert scale ranging from “never” to “every day,” 258 residents from 11 different residency programs filled out an anonymous Web-based survey on how often they felt emotional exhaustion (“I feel burnout from my work”) and depersonalization (“I’ve become more callous toward people since I took this job”).
Of the 258 respondents, 39% had burnout, defined as answering affirmatively to either of the above questions with at least “weekly.” Most of the respondents were female, white, and married or in a long-term relationship without children, but the burnout rates did not vary across gender, race/ethnicity, relationship or parental status, or among different characteristics of the residency program and schedule. Higher burnout rates did occur among those feeling sleep deprived.
Those with burnout also had substantially higher odds of providing lower-quality care. Residents with burnout were seven times more likely to make treatment or medication errors not related to inadequate knowledge or experience, six times more likely to feel guilty about how they had treated a patient, more than four times more likely to report having little emotional reaction to a patient’s death, and four times more likely to discharge a patient earlier to make service more manageable. Burned-out residents had more than nine times greater odds of paying “little attention to the social or personal impact of an illness on a patient,” the study showed.
Burnout symptoms and solutions
Symptoms of potential burnout, Dr. First said in an interview, include emotional exhaustion, feeling a loss of meaning in work, feelings of ineffectiveness, a tendency to view people as objects instead of human beings, increasingly poor communication, and poor interpersonal and clinical skills and behaviors.
Other research also has found burnout linked to doctors’ errors, self-reported negative attitudes toward patients, and less time spent with patients, she said. “Thus physicians should be on the lookout for burnout within themselves as well as in their colleagues and medical trainees.”
Both Dr. Baer and Dr. First noted the importance of organizational leadership in preventing burnout.
The Association of Medical School Pediatric Department Chairs is sharing a toolbox of strategies that they have found effective for reducing burnout and developing wellness among physicians, Dr. First said in the interview.
“Some of those suggestions include personal attention to wellness via good nutrition, exercise, mindfulness for emotional self-regulation, and developing supportive relationships,” he noted. In addition to organizational mindfulness programs and ones that foster work-life integration and social activities, prevention programs should “create wellness and resilience, and a sense of pride and meaning in the work that is being done.”
Drs. First also pointed to ways of addressing triggers of burnout:
- Reduce the burden of bureaucratic tasks.
- Examine how many hours physicians spend at home or work at home.
- Improve efficiency, such as in EHR use.
- Provide individuals time to discuss stressors and ways to resolve them collaboratively with peers and leadership.
Burnout risk in the NICU
Similar interventions may help with burnout in neonatal ICUs (NICUs), the focus of the second study Dr. First discussed. Tawfik et al. surveyed 2,760 personnel from 41 NICUs in the United States to learn the prevalence of burnout and how it was associated with NICU organization (Pediatrics. 2017. doi: 10.1542/peds.2016-4134).
Among the 1,934 providers who replied (a response rate of 70%), 27% had burnout; at individual NICUs, burnout prevalence varied from 8% to 43%. The majority of respondents (72%) were registered nurses, followed by respiratory therapists, physicians, neonatal nurse practitioners, and others. The highest burnout rates occurred in NICUs with higher average daily admissions and higher average occupancy – and those using EHRs.
“Don’t assume that just because you use the EHR every day means you know how best to use this tool to improve your efficiency and effectiveness in generating and deriving information on your patients,” Dr. First said in the interview. He encouraged physicians to find out what resources their institutions might offer to help, such as EHR hospital teams or office support who can look at providers’ EHR usage, and show them shortcuts and time-savers to improve efficiency based on their usage patterns.
“Nursing burnout was more sensitive to the setting than physician burnout, especially in regard to average daily admissions, late transfer numbers, nursing hours per patient day, and mortality per 1,000 infants,” Dr. First noted.
Interestingly, burnout prevalence was not associated with the proportion of high-risk patients seen in the NICUs, the number of attending physicians in the unit, or whether the institution was a teaching hospital or not, he said.
Dr. First listed strategies to reduce burnout risk in NICUs that the study authors also described: expressing thankfulness each day, focusing on positive events at the start or end of each day, performing random acts of kindness for colleagues and staff, and encouraging providers to identify the strengths in one another.
Addressing burnout requires efforts from everyone
“Given the potential effects of burnout on patient care and professionalism and physician wellness, it is important for physicians to speak up if they have concerns about burnout in their colleagues,” Dr. Baer said in the interview.
Burnout is common, she said, occurring in more than half of physicians at some point in time, so a doctor experiencing it is almost certainly not alone among colleagues.
“Physicians can work together and with their leadership to prevent and mitigate the effects of burnout by promoting personal and professional wellness, effective teamwork, and reducing the administrative burdens that impact time spent directly with patients and have been demonstrated to contribute to physician burnout,” Dr. Baer noted.
She also pointed to the need to address it in medical education, given the downstream risks of burnout on the next generation of physicians.
“Medical schools and residency and fellowship programs should address the risks and signs of burnout, as medical students and trainees are likely seeing signs of burnout in some of their physician teachers and mentors,” Dr. Baer said in the interview.
Some burnout among providers may be inevitable at times, but it’s important to continue looking for ways to combat it.
“We need to do more to remind each other of why we chose our profession, and how good it makes us feel to strive to make a difference in our patients and families each and every day,” Dr. First said in the interview.
Dr. First reported having no disclosures and no external funding. The residents’ study by Baer et al. was funded by the Boston Children’s Hospital’s Fred Lovejoy Resident Research Award and a grant from the Health Resources and Services Administration. The NICU study by Tamfik et al. was funded by the National Institutes of Health, grants from the National Institute of Child Health and Human Development, and the Jackson Vaughan Critical Care Research Fund. The authors of both studies had no relevant financial disclosures.

Gastrografin offers an alternative to surgery for SBO
LAKE BUENA VISTA, FLA. – Gastrografin significantly decreased the need for an operation in small bowel obstruction (SBO) patients, even among patients who had never undergone abdominal surgery, according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“Small bowel obstruction is a common clinical problem in the United States, with 15 out of 100 admissions for abdominal pain related to SBO,” said Morgan Collom, DO, surgical resident at Medical City Fort Worth (Tex.). “Many studies conclude that [operative exploration] is not needed and it is feasible to perform nonoperative conservative management, yet still argue that small obstruction in a virgin abdomen patient should undergo mandatory exploration to avoid missing a diagnosis of malignancy.”
Investigators studied 601 SBO patients admitted to one of 14 institutions included in an EAST database between February 2015 and December 2016 for this prospective study.
Of those included, 500 had previous abdominal surgery and the others had never had surgery. Gastrografin (Bracco Diagnostics) was used to treat their bowel obstruction.
Those with previous abdominal surgery were more likely to be over age 65 years (48% vs. 36%), be female (50% vs. 25%), have a history of cancer (42.6% vs. 18.8%), and have a prior admission of SBO (41.2% vs 8.9%), according to Dr. Collom.
Among patients who previously had surgery, operative exploration was 50% less likely (odds ratio = .51, P = .04) than among those who had never had surgery. In a comparison of patients with and without previous surgery, introducing Gastrografin evened out the likelihood for an operation (OR = .17 and .21, respectively). Overall, those who received Gastrografin were 86% less likely to undergo bowel exploration(OR = .14, P less than .01).
Of the 36 NAS patients treated with Gastrografin, 33 underwent successful, nonoperative therapy, and 3 underwent a therapeutic laparotomy for a malignancy.
During a question-and-answer session, audience members called to attention the issue of the database used, which does not review complications or recurrences after 30 days or any missed abnormalities, indicating that some malignancies may have developed after the therapy.
Dr. Collom acknowledged the limitation and agreed that the next study would need to address this.
The investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: EAST Scientific Assembly abstract No. 24.
LAKE BUENA VISTA, FLA. – Gastrografin significantly decreased the need for an operation in small bowel obstruction (SBO) patients, even among patients who had never undergone abdominal surgery, according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“Small bowel obstruction is a common clinical problem in the United States, with 15 out of 100 admissions for abdominal pain related to SBO,” said Morgan Collom, DO, surgical resident at Medical City Fort Worth (Tex.). “Many studies conclude that [operative exploration] is not needed and it is feasible to perform nonoperative conservative management, yet still argue that small obstruction in a virgin abdomen patient should undergo mandatory exploration to avoid missing a diagnosis of malignancy.”
Investigators studied 601 SBO patients admitted to one of 14 institutions included in an EAST database between February 2015 and December 2016 for this prospective study.
Of those included, 500 had previous abdominal surgery and the others had never had surgery. Gastrografin (Bracco Diagnostics) was used to treat their bowel obstruction.
Those with previous abdominal surgery were more likely to be over age 65 years (48% vs. 36%), be female (50% vs. 25%), have a history of cancer (42.6% vs. 18.8%), and have a prior admission of SBO (41.2% vs 8.9%), according to Dr. Collom.
Among patients who previously had surgery, operative exploration was 50% less likely (odds ratio = .51, P = .04) than among those who had never had surgery. In a comparison of patients with and without previous surgery, introducing Gastrografin evened out the likelihood for an operation (OR = .17 and .21, respectively). Overall, those who received Gastrografin were 86% less likely to undergo bowel exploration(OR = .14, P less than .01).
Of the 36 NAS patients treated with Gastrografin, 33 underwent successful, nonoperative therapy, and 3 underwent a therapeutic laparotomy for a malignancy.
During a question-and-answer session, audience members called to attention the issue of the database used, which does not review complications or recurrences after 30 days or any missed abnormalities, indicating that some malignancies may have developed after the therapy.
Dr. Collom acknowledged the limitation and agreed that the next study would need to address this.
The investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: EAST Scientific Assembly abstract No. 24.
LAKE BUENA VISTA, FLA. – Gastrografin significantly decreased the need for an operation in small bowel obstruction (SBO) patients, even among patients who had never undergone abdominal surgery, according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“Small bowel obstruction is a common clinical problem in the United States, with 15 out of 100 admissions for abdominal pain related to SBO,” said Morgan Collom, DO, surgical resident at Medical City Fort Worth (Tex.). “Many studies conclude that [operative exploration] is not needed and it is feasible to perform nonoperative conservative management, yet still argue that small obstruction in a virgin abdomen patient should undergo mandatory exploration to avoid missing a diagnosis of malignancy.”
Investigators studied 601 SBO patients admitted to one of 14 institutions included in an EAST database between February 2015 and December 2016 for this prospective study.
Of those included, 500 had previous abdominal surgery and the others had never had surgery. Gastrografin (Bracco Diagnostics) was used to treat their bowel obstruction.
Those with previous abdominal surgery were more likely to be over age 65 years (48% vs. 36%), be female (50% vs. 25%), have a history of cancer (42.6% vs. 18.8%), and have a prior admission of SBO (41.2% vs 8.9%), according to Dr. Collom.
Among patients who previously had surgery, operative exploration was 50% less likely (odds ratio = .51, P = .04) than among those who had never had surgery. In a comparison of patients with and without previous surgery, introducing Gastrografin evened out the likelihood for an operation (OR = .17 and .21, respectively). Overall, those who received Gastrografin were 86% less likely to undergo bowel exploration(OR = .14, P less than .01).
Of the 36 NAS patients treated with Gastrografin, 33 underwent successful, nonoperative therapy, and 3 underwent a therapeutic laparotomy for a malignancy.
During a question-and-answer session, audience members called to attention the issue of the database used, which does not review complications or recurrences after 30 days or any missed abnormalities, indicating that some malignancies may have developed after the therapy.
Dr. Collom acknowledged the limitation and agreed that the next study would need to address this.
The investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: EAST Scientific Assembly abstract No. 24.
REPORTING FROM EAST 2018
Key clinical point: Gastrografin is an effective alternative to operative exploration in small bowel obstruction patients with or without a history of surgical intervention.
Major finding: Treatment with Gastrografin (Bracco Diagnostics) reduced the risk of operative exploration for patients with small bowel obstruction (OR = .14, P less than .01).
Data source: Prospective, observational study of 601 small bowel obstruction patients seen at 14 institutions between February 2015 and December 2016.
Disclosures: The investigators reported no relevant financial disclosures.
Source: Collom et al. EAST Scientific Assembly, abstract 24.
PPIs, certain antibiotics increase risk of hospital onset C. difficile infection
The use of proton pump inhibitors increased the odds of a patient having hospital-onset Clostridium difficile infection (HO CDI) as did the use of third- and fourth-generation cephalosporins, carbapenems, and piperacillin/tazobactam, according to the results of a retrospective database study of more than 1 million patients at 150 U.S. hospitals.
PPIs increased the odds of HO CDI by 44% (P less than .001), whereas the use of H2 antagonists increased the odds ratio for HO CDI to a lesser, but still significant, extent (13% increase, P less than .001), according to the report published online in Clinical Infectious Diseases.
Overall, the odds of HO CDI were significantly higher in patients taking carbapenems, third- and fourth-generation cephalosporins, metronidazole, and piperacillin/tazobactam, as well as patients on multiple antibiotics. However, treatment with tetracyclines, macrolides, or clindamycin significantly reduced the odds of HO CDI.
The combination of PPIs with fluoroquinolones, third-generation cephalosporins, fourth-generation cephalosporins, clindamycin, or carbapenems did not significantly alter the odds of HO CDI, which was in contrast with a previous meta-analysis (Am J Gastroenterol. 2012;107[7]:1011-9).
In addition to the drug associations, the odds of a patient having HO CDI increased by 0.5% for each year in age. The odds of CDI in women was 1.2 times as likely as in men, and admission from a long-term care facility, the presence of the comorbidities of diabetes, Crohn’s disease or ulcerative colitis, as well as days in the ICU and antibiotic days of therapy all significantly increased the odds of a patient having HO CDI. (Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112).
“The results support the need for stewardship practices around both high-risk antibiotics and medications that alter gastric acid regulation. Furthermore, the impact of deprescribing acid suppression therapy coupled with antibiotic stewardship could greatly reduce the incidence of HO CDI,” the researchers concluded.
The authors reported that they had no conflicts or funding source for this work.
SOURCE: Watson, T. et al. Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112.
The use of proton pump inhibitors increased the odds of a patient having hospital-onset Clostridium difficile infection (HO CDI) as did the use of third- and fourth-generation cephalosporins, carbapenems, and piperacillin/tazobactam, according to the results of a retrospective database study of more than 1 million patients at 150 U.S. hospitals.
PPIs increased the odds of HO CDI by 44% (P less than .001), whereas the use of H2 antagonists increased the odds ratio for HO CDI to a lesser, but still significant, extent (13% increase, P less than .001), according to the report published online in Clinical Infectious Diseases.
Overall, the odds of HO CDI were significantly higher in patients taking carbapenems, third- and fourth-generation cephalosporins, metronidazole, and piperacillin/tazobactam, as well as patients on multiple antibiotics. However, treatment with tetracyclines, macrolides, or clindamycin significantly reduced the odds of HO CDI.
The combination of PPIs with fluoroquinolones, third-generation cephalosporins, fourth-generation cephalosporins, clindamycin, or carbapenems did not significantly alter the odds of HO CDI, which was in contrast with a previous meta-analysis (Am J Gastroenterol. 2012;107[7]:1011-9).
In addition to the drug associations, the odds of a patient having HO CDI increased by 0.5% for each year in age. The odds of CDI in women was 1.2 times as likely as in men, and admission from a long-term care facility, the presence of the comorbidities of diabetes, Crohn’s disease or ulcerative colitis, as well as days in the ICU and antibiotic days of therapy all significantly increased the odds of a patient having HO CDI. (Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112).
“The results support the need for stewardship practices around both high-risk antibiotics and medications that alter gastric acid regulation. Furthermore, the impact of deprescribing acid suppression therapy coupled with antibiotic stewardship could greatly reduce the incidence of HO CDI,” the researchers concluded.
The authors reported that they had no conflicts or funding source for this work.
SOURCE: Watson, T. et al. Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112.
The use of proton pump inhibitors increased the odds of a patient having hospital-onset Clostridium difficile infection (HO CDI) as did the use of third- and fourth-generation cephalosporins, carbapenems, and piperacillin/tazobactam, according to the results of a retrospective database study of more than 1 million patients at 150 U.S. hospitals.
PPIs increased the odds of HO CDI by 44% (P less than .001), whereas the use of H2 antagonists increased the odds ratio for HO CDI to a lesser, but still significant, extent (13% increase, P less than .001), according to the report published online in Clinical Infectious Diseases.
Overall, the odds of HO CDI were significantly higher in patients taking carbapenems, third- and fourth-generation cephalosporins, metronidazole, and piperacillin/tazobactam, as well as patients on multiple antibiotics. However, treatment with tetracyclines, macrolides, or clindamycin significantly reduced the odds of HO CDI.
The combination of PPIs with fluoroquinolones, third-generation cephalosporins, fourth-generation cephalosporins, clindamycin, or carbapenems did not significantly alter the odds of HO CDI, which was in contrast with a previous meta-analysis (Am J Gastroenterol. 2012;107[7]:1011-9).
In addition to the drug associations, the odds of a patient having HO CDI increased by 0.5% for each year in age. The odds of CDI in women was 1.2 times as likely as in men, and admission from a long-term care facility, the presence of the comorbidities of diabetes, Crohn’s disease or ulcerative colitis, as well as days in the ICU and antibiotic days of therapy all significantly increased the odds of a patient having HO CDI. (Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112).
“The results support the need for stewardship practices around both high-risk antibiotics and medications that alter gastric acid regulation. Furthermore, the impact of deprescribing acid suppression therapy coupled with antibiotic stewardship could greatly reduce the incidence of HO CDI,” the researchers concluded.
The authors reported that they had no conflicts or funding source for this work.
SOURCE: Watson, T. et al. Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112.
FROM CLINICAL INFECTIOUS DISEASES
Key clinical point: Proper stewardship of PPIs, antibiotics might lower risk of hospital-onset C. difficile infection.
Major finding: Patients taking PPIs had a 44% increased risk of developing hospital-onset C. difficile infection.
Study details: Retrospective database study of more than 1 million patients at 150 U.S. hospitals.
Disclosures: The authors reported that they had no conflicts or funding source for this work.
Source: Watson, T. et al. Clin Infect Dis. 2017 Dec. 20. doi: 10.1093/cid/cix1112.
Shortened PTSD therapy still effective in active duty military personnel
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
FROM JAMA
CHIP gets a 6-year extension in stopgap budget
The legislation did not address two Affordable Care Act provisions that have been bandied about in this years’ budget debacle – delaying the “Cadillac tax” on high-valued employer health insurance plans and the medical device tax.
The short-term funding bill (H.R. 195) passed the Senate by an 81-18 vote and the House by a 266-150 vote after a 3-day shutdown of the federal government driven primarily by partisan disagreement over immigration policy.
CHIP funding had expired at the end of September 2017. The 6-year reauthorization period is the longest since the program was created in 1997. The Senate Finance Committee passed a bill reauthorizing CHIP for 5 years in October 2017, but the Senate did not take any action.
Although he voted for the 6-year extension, Sen. Ben Cardin (D-Md.) said that Congress was going only for a temporary extension rather than making CHIP a permanent program.
“I wish it were permanent,” Sen. Cardin said on the Senate floor. “Rather than putting another deadline on the program, we should try to make this permanent.”
Sen. Cardin also said the bill did nothing to extend funding to community health centers, where many children covered by CHIP get their medical treatments.
The legislation did not address two Affordable Care Act provisions that have been bandied about in this years’ budget debacle – delaying the “Cadillac tax” on high-valued employer health insurance plans and the medical device tax.
The short-term funding bill (H.R. 195) passed the Senate by an 81-18 vote and the House by a 266-150 vote after a 3-day shutdown of the federal government driven primarily by partisan disagreement over immigration policy.
CHIP funding had expired at the end of September 2017. The 6-year reauthorization period is the longest since the program was created in 1997. The Senate Finance Committee passed a bill reauthorizing CHIP for 5 years in October 2017, but the Senate did not take any action.
Although he voted for the 6-year extension, Sen. Ben Cardin (D-Md.) said that Congress was going only for a temporary extension rather than making CHIP a permanent program.
“I wish it were permanent,” Sen. Cardin said on the Senate floor. “Rather than putting another deadline on the program, we should try to make this permanent.”
Sen. Cardin also said the bill did nothing to extend funding to community health centers, where many children covered by CHIP get their medical treatments.
The legislation did not address two Affordable Care Act provisions that have been bandied about in this years’ budget debacle – delaying the “Cadillac tax” on high-valued employer health insurance plans and the medical device tax.
The short-term funding bill (H.R. 195) passed the Senate by an 81-18 vote and the House by a 266-150 vote after a 3-day shutdown of the federal government driven primarily by partisan disagreement over immigration policy.
CHIP funding had expired at the end of September 2017. The 6-year reauthorization period is the longest since the program was created in 1997. The Senate Finance Committee passed a bill reauthorizing CHIP for 5 years in October 2017, but the Senate did not take any action.
Although he voted for the 6-year extension, Sen. Ben Cardin (D-Md.) said that Congress was going only for a temporary extension rather than making CHIP a permanent program.
“I wish it were permanent,” Sen. Cardin said on the Senate floor. “Rather than putting another deadline on the program, we should try to make this permanent.”
Sen. Cardin also said the bill did nothing to extend funding to community health centers, where many children covered by CHIP get their medical treatments.
Introducing our daily medical news podcast!
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Get your daily dose of medical news right here every weekday. MDEdge Medical News Briefing serves up the latest clinical research and socioeconomic news that impacts your practice, all in less than 3 minutes.
In today's news: Flu update, a blood test for cancer, malpractice premiums on the move, and more!
Check back again tomorrow for another quick infusion of medical news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Get your daily dose of medical news right here every weekday. MDEdge Medical News Briefing serves up the latest clinical research and socioeconomic news that impacts your practice, all in less than 3 minutes.
In today's news: Flu update, a blood test for cancer, malpractice premiums on the move, and more!
Check back again tomorrow for another quick infusion of medical news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Get your daily dose of medical news right here every weekday. MDEdge Medical News Briefing serves up the latest clinical research and socioeconomic news that impacts your practice, all in less than 3 minutes.
In today's news: Flu update, a blood test for cancer, malpractice premiums on the move, and more!
Check back again tomorrow for another quick infusion of medical news.

Asymptomatic carotid in-stent restenosis? Think medical management
CHICAGO – with a carotid in-stent restenosis in excess of 70%, Jayer Chung, MD, asserted at a symposium on vascular surgery sponsored by Northwestern University.
That, in his view, makes medical management the clear preferred strategy.
A growing body of evidence, mainly from nested cohorts within randomized controlled trials, indicates that the late ipsilateral stroke rate associated with post–carotid endarterectomy restenosis (CEA) is much higher than that for carotid in-stent restenosis (C-ISR). In a recent meta-analysis of nine randomized trials, the difference in risk was more than 10-fold, with a 9.2% stroke rate at a mean of 37 months of follow-up in patients with post-CEA restenosis, compared with a 0.8% rate with 50 months of follow-up in patients with C-ISR (Eur J Vasc Endovasc Surg. 2017 Jun;53[6]:766-75).
“These pathologies behave very, very differently,” Dr. Chung observed. “The C-ISR lesions tend to be less embologenic.”
C-ISR is an uncommon event. Extrapolating from the landmark CREST (Carotid Revascularization Endarterectomy versus Stenting Trial) and other randomized trials, about 6% of patients who undergo percutaneous carotid stenting will be develop C-ISR within 2 years. But since the proportion of all carotid revascularizations that are done by carotid stent angioplasty has steadily increased over the past 15 years as the frequency of CEA has dropped, C-ISR is a problem that vascular specialists will continue to encounter on a regular basis.
Symptomatic C-ISR warrants reintervention; broad agreement exists on that. But there is a paucity of data to guide treatment decisions regarding asymptomatic yet angiographically severe C-ISR. Indeed, Dr. Chung was lead author of the only retrospective study of the natural history of untreated C-ISR, as opposed to carefully selected cohorts from randomized trials involving highly experienced operators. This study was a retrospective review of 59 patients with 75 C-ISRs of at least 50% seen at a single Veterans Affairs medical center over a 13-year period. Three-quarters of the ISRs were asymptomatic.
Forty of the 79 C-ISRs underwent percutaneous intervention at the physician’s discretion. Those patients did not differ from the observation-only group in age, comorbid conditions, type of original stent, or clopidogrel use. Reintervention was safe: There was one stent thrombosis resulting in stroke and death within 30 days in the reintervention group and no 30-day strokes in the observation-only group. During a mean 2.6 years of follow-up, the composite rate of death, stroke, or MI was low and not statistically significantly different between the two groups. Indeed, during up to 13 years of follow-up only one patient with untreated C-ISR experienced an ipsilateral stroke, as did two patients in the percutaneous intervention group (J Vasc Surg. 2016 Nov;64[5]:1286-94).
Dr. Chung does the math
According to data from the National Inpatient Sample, vascular surgeons do an average of 15 carotid angioplasty and stenting procedures per year. If 6% of those stents develop in-stent restenosis, and with a number needed to treat with revascularization of 25 to prevent 1 stroke, Dr. Chung estimated that hypothetically it would take the typical vascular surgeon 27 years to prevent one stroke due to C-ISR.
“That’s a very long time to prevent one stroke, in my opinion,” he said.
How his study has affected his own practice
Dr. Chung now intervenes only for symptomatic C-ISRs, and only after an affected patient is on optimal medical therapy, including a statin and dual-antiplatelet therapy.
“I try to do an open procedure if possible, especially if the restenosis is above C-2. The ones I tend to do percutaneously are the post-irradiation stenoses or those with excessive scarring, and I use a cerebral protection device,” the surgeon explained.
He emphasized, however, that the final word on the appropriate management of C-ISRs isn’t in yet. A standardized definition of C-ISR is needed, as are multicenter prospective registries of medically managed patients as well as those undergoing various forms of reintervention. And a pathologic study is warranted to confirm the hypothesis that the histopathology of post-CEA and post-stent restenosis – and hence the natural history – is markedly different.
Dr. Chung reported having no financial conflicts regarding his presentation.
CHICAGO – with a carotid in-stent restenosis in excess of 70%, Jayer Chung, MD, asserted at a symposium on vascular surgery sponsored by Northwestern University.
That, in his view, makes medical management the clear preferred strategy.
A growing body of evidence, mainly from nested cohorts within randomized controlled trials, indicates that the late ipsilateral stroke rate associated with post–carotid endarterectomy restenosis (CEA) is much higher than that for carotid in-stent restenosis (C-ISR). In a recent meta-analysis of nine randomized trials, the difference in risk was more than 10-fold, with a 9.2% stroke rate at a mean of 37 months of follow-up in patients with post-CEA restenosis, compared with a 0.8% rate with 50 months of follow-up in patients with C-ISR (Eur J Vasc Endovasc Surg. 2017 Jun;53[6]:766-75).
“These pathologies behave very, very differently,” Dr. Chung observed. “The C-ISR lesions tend to be less embologenic.”
C-ISR is an uncommon event. Extrapolating from the landmark CREST (Carotid Revascularization Endarterectomy versus Stenting Trial) and other randomized trials, about 6% of patients who undergo percutaneous carotid stenting will be develop C-ISR within 2 years. But since the proportion of all carotid revascularizations that are done by carotid stent angioplasty has steadily increased over the past 15 years as the frequency of CEA has dropped, C-ISR is a problem that vascular specialists will continue to encounter on a regular basis.
Symptomatic C-ISR warrants reintervention; broad agreement exists on that. But there is a paucity of data to guide treatment decisions regarding asymptomatic yet angiographically severe C-ISR. Indeed, Dr. Chung was lead author of the only retrospective study of the natural history of untreated C-ISR, as opposed to carefully selected cohorts from randomized trials involving highly experienced operators. This study was a retrospective review of 59 patients with 75 C-ISRs of at least 50% seen at a single Veterans Affairs medical center over a 13-year period. Three-quarters of the ISRs were asymptomatic.
Forty of the 79 C-ISRs underwent percutaneous intervention at the physician’s discretion. Those patients did not differ from the observation-only group in age, comorbid conditions, type of original stent, or clopidogrel use. Reintervention was safe: There was one stent thrombosis resulting in stroke and death within 30 days in the reintervention group and no 30-day strokes in the observation-only group. During a mean 2.6 years of follow-up, the composite rate of death, stroke, or MI was low and not statistically significantly different between the two groups. Indeed, during up to 13 years of follow-up only one patient with untreated C-ISR experienced an ipsilateral stroke, as did two patients in the percutaneous intervention group (J Vasc Surg. 2016 Nov;64[5]:1286-94).
Dr. Chung does the math
According to data from the National Inpatient Sample, vascular surgeons do an average of 15 carotid angioplasty and stenting procedures per year. If 6% of those stents develop in-stent restenosis, and with a number needed to treat with revascularization of 25 to prevent 1 stroke, Dr. Chung estimated that hypothetically it would take the typical vascular surgeon 27 years to prevent one stroke due to C-ISR.
“That’s a very long time to prevent one stroke, in my opinion,” he said.
How his study has affected his own practice
Dr. Chung now intervenes only for symptomatic C-ISRs, and only after an affected patient is on optimal medical therapy, including a statin and dual-antiplatelet therapy.
“I try to do an open procedure if possible, especially if the restenosis is above C-2. The ones I tend to do percutaneously are the post-irradiation stenoses or those with excessive scarring, and I use a cerebral protection device,” the surgeon explained.
He emphasized, however, that the final word on the appropriate management of C-ISRs isn’t in yet. A standardized definition of C-ISR is needed, as are multicenter prospective registries of medically managed patients as well as those undergoing various forms of reintervention. And a pathologic study is warranted to confirm the hypothesis that the histopathology of post-CEA and post-stent restenosis – and hence the natural history – is markedly different.
Dr. Chung reported having no financial conflicts regarding his presentation.
CHICAGO – with a carotid in-stent restenosis in excess of 70%, Jayer Chung, MD, asserted at a symposium on vascular surgery sponsored by Northwestern University.
That, in his view, makes medical management the clear preferred strategy.
A growing body of evidence, mainly from nested cohorts within randomized controlled trials, indicates that the late ipsilateral stroke rate associated with post–carotid endarterectomy restenosis (CEA) is much higher than that for carotid in-stent restenosis (C-ISR). In a recent meta-analysis of nine randomized trials, the difference in risk was more than 10-fold, with a 9.2% stroke rate at a mean of 37 months of follow-up in patients with post-CEA restenosis, compared with a 0.8% rate with 50 months of follow-up in patients with C-ISR (Eur J Vasc Endovasc Surg. 2017 Jun;53[6]:766-75).
“These pathologies behave very, very differently,” Dr. Chung observed. “The C-ISR lesions tend to be less embologenic.”
C-ISR is an uncommon event. Extrapolating from the landmark CREST (Carotid Revascularization Endarterectomy versus Stenting Trial) and other randomized trials, about 6% of patients who undergo percutaneous carotid stenting will be develop C-ISR within 2 years. But since the proportion of all carotid revascularizations that are done by carotid stent angioplasty has steadily increased over the past 15 years as the frequency of CEA has dropped, C-ISR is a problem that vascular specialists will continue to encounter on a regular basis.
Symptomatic C-ISR warrants reintervention; broad agreement exists on that. But there is a paucity of data to guide treatment decisions regarding asymptomatic yet angiographically severe C-ISR. Indeed, Dr. Chung was lead author of the only retrospective study of the natural history of untreated C-ISR, as opposed to carefully selected cohorts from randomized trials involving highly experienced operators. This study was a retrospective review of 59 patients with 75 C-ISRs of at least 50% seen at a single Veterans Affairs medical center over a 13-year period. Three-quarters of the ISRs were asymptomatic.
Forty of the 79 C-ISRs underwent percutaneous intervention at the physician’s discretion. Those patients did not differ from the observation-only group in age, comorbid conditions, type of original stent, or clopidogrel use. Reintervention was safe: There was one stent thrombosis resulting in stroke and death within 30 days in the reintervention group and no 30-day strokes in the observation-only group. During a mean 2.6 years of follow-up, the composite rate of death, stroke, or MI was low and not statistically significantly different between the two groups. Indeed, during up to 13 years of follow-up only one patient with untreated C-ISR experienced an ipsilateral stroke, as did two patients in the percutaneous intervention group (J Vasc Surg. 2016 Nov;64[5]:1286-94).
Dr. Chung does the math
According to data from the National Inpatient Sample, vascular surgeons do an average of 15 carotid angioplasty and stenting procedures per year. If 6% of those stents develop in-stent restenosis, and with a number needed to treat with revascularization of 25 to prevent 1 stroke, Dr. Chung estimated that hypothetically it would take the typical vascular surgeon 27 years to prevent one stroke due to C-ISR.
“That’s a very long time to prevent one stroke, in my opinion,” he said.
How his study has affected his own practice
Dr. Chung now intervenes only for symptomatic C-ISRs, and only after an affected patient is on optimal medical therapy, including a statin and dual-antiplatelet therapy.
“I try to do an open procedure if possible, especially if the restenosis is above C-2. The ones I tend to do percutaneously are the post-irradiation stenoses or those with excessive scarring, and I use a cerebral protection device,” the surgeon explained.
He emphasized, however, that the final word on the appropriate management of C-ISRs isn’t in yet. A standardized definition of C-ISR is needed, as are multicenter prospective registries of medically managed patients as well as those undergoing various forms of reintervention. And a pathologic study is warranted to confirm the hypothesis that the histopathology of post-CEA and post-stent restenosis – and hence the natural history – is markedly different.
Dr. Chung reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE NORTHWESTERN VASCULAR SYMPOSIUM