User login
Association Between Ventilator Strategy and Neurocognitive Outcomes in Out-of-Hospital Cardiac Arrest Patients
Study Overview
Objective. To determine if there is an association between low tidal volume (VT) ventilation and neurocognitive outcomes in patients after out-of-hospital cardiac arrest (OHCA).
Design. Retrospective cohort study.
Setting and participants. Data was obtained from retrospective review of all adults admitted between 2008 and 2014 to one of 2 centers (A or B) with nontraumatic OHCA requiring mechanical ventilation for greater than 48 hours. The study physicians screened records primarily using chart review with secondary confirmation of the diagnosis of OHCA and eligibility criteria. Patients with an outside hospital stay greater than 24 hours, intracranial hemorrhage, use of extracorporeal membranous oxygenation (ECMO), use of airway pressure release mode of ventilation, chronic dependence on mechanical ventilation, or missing data were excluded. Of the 579 patients with OHCA, 256 (44.2%) met the inclusion criteria and were included in the main analysis. A total of 97 patients were identified as having high VT (defined as > 8 mL/kg of predicted body weight [PBW]) and were matched to 97 of the 159 patients identified as having a low VT as part of the propensity-matched subgroup analysis using 1:1 optimal caliper matching.
Main outcome measure. The primary outcome was a favorable neurocognitive outcome at hospital discharge (Cerebral Performance Category score [CPC] of 1 or 2). A CPC of 1 or 2 corresponds to normal life or life that is disabled but independent, respectively. A CPC of 3 is disabled and dependent, and a CPC of 5 is alive but brain dead. Two physicians blinded to VT and other measures of illness severity calculated the CPC via chart review. Discordant scores were resolved by consensus, and a Kappa statistic was calculated to quantify agreement between investigators. Secondary outcomes included ventilator-free days, hospital-free days, ICU-free days, shock-free days, and extrapulmonary organ failure–free days. Logistic regression with backward elimination was used to identify predictors of receiving VT ≤ 8 mL/kg PBW to be used in the propensity-matched analysis, along with relevant predictors identified from the literature. The odds ratio for the primary outcome was calculated using both logistic regression analysis and propensity-matched analysis. Other methods of sensitivity analysis (propensity quintile adjustment, inverse-probability-of-treatment weighting) were used to confirm the robustness of the initial analysis to different statistical methods. A P value of < 0.05 was considered significant.
Main results. Of the study patients, approximately half (49% in high VT, 52% in low VT) had an initial rhythm of ventricular tachycardia or ventricular fibrillation. Patients with low VT were significantly younger (mean age 59 yr vs. 66 yr), taller (mean height 177 cm vs. 165 cm), and heavier (mean weight 88 kg vs. 81 kg). There were also significantly fewer females in the low VT group (19% vs. 46%). There were no significant differences between baseline comorbidities, arrest characteristics, or illness severity between the 2 groups with the exception of significantly more patients in the low VT underwent therapeutic hypothermia (87% vs. 76%) and were admitted to hospital A (69% vs. 55%). There were no significant differences between the groups across ventilator parameters aside from tidal volume. The average VT in mL/kg PBW was 9.3 in the high VT group and 7.1 in the low VT group over the first 48 hours.
In the multivariate regression analysis, significant independent predictors of receiving high VT included height, weight, and hospital of admission. The final propensity model to predict VT included age, height, weight, sex, illness severity measures (APACHE-II score and presence of circulatory shock in the first 24 hours of admission), arrest characteristics, and respiratory characteristics (initial pH, initial PaCO2, PaO2:FiO2 ratio, and initial peak inspiratory pressure) as covariates. The use of low VT was significantly associated with a favorable neurocognitive outcome in the multivariate regression analysis (odds ratio [OR] 1.65, 95% confidence interval [CI] 1.18–2.29). This association held in both the propensity matched analysis (OR 1.68, 95% CI 1.11–2.55) as well as conditional logistic regression analysis using propensity score as a covariate (OR 1.61, 95% CI 1.13–2.28).
In the propensity-adjusted conditional logistic regression analysis, a lower VT (1 mL/kg of PBW decrease) was significantly associated with ventilator-free days (OR 1.78, 95% CI 0.39–3.16), shock-free days (OR 1.31, 95% CI 0.10–2.51), ICU-free days (OR 1.38, 95% CI 0.13–2.63), and hospital-free days (OR 1.07, 95% CI 0.04–2.09). There was a nonsignificant trend towards improved survival to hospital discharge (OR 1.23, 95% CI 0.95–1.60, P = 0.115). After propensity score adjustment, lower VT was not associated with therapeutic hypothermia (OR 0.14, 95% CI −0.19 to 0.47), and in the multivariate regression analysis there was no association between favorable neurocognitive outcome and therapeutic hypothermia (P = 0.516). While there was a significant association between lower VT and site of admission (Hospital A: OR 1.50, 95% CI 1.04–2.17 per 1 mL/kg of PBW decrease), there was no association between favorable neurocognitive outcome and hospital site of admission in the final adjusted regression analysis (P = 0.588).
Conclusion. In this retrospective cohort study, lower VT in the first 48 hours of admission following OHCA was independently associated with favorable neurocognitive outcomes as measured by the CPC score, as well as more ventilator-free, shock-free, ICU-free, and hospital-free days.
Commentary
Neurocognitive impairment following nontraumatic OHCA is common, estimated to occur in roughly half of all survivors [1]. Similar to the acute respiratory distress syndrome (ARDS), the post–cardiac arrest syndrome (PCAS) is recognized as a systemic process with multi-organ effects thought to be mediated in part by inflammatory cytokines [2]. While the beneficial role of low VT in patients with ARDS is well established, currently there are no recommendations for specific VT targets in post–cardiac arrest care, and the effect of VT on outcomes following cardiac arrest is unknown [3].
In this study, Beitler and colleagues suggest a possible association between VT and neurocognitive outcomes following OHCA. Using retrospective data drawn from 2 centers, and employing both regression analysis and propensity matching, the authors identified a significant beneficial effect of lower VT on neurocognitive outcomes in their cohort. This benefit held regardless of the statistical analytic method employed and was present even when correcting for the difference between groups in hospital admission site and use of therapeutic hypothermia in the original cohort. The authors also demonstrated a lower VT was associated with a number of secondary outcomes including fewer hospital, ICU, and ventilator days. While the statistical methods employed by the authors are robust and attempt to account for the limitations inherent to observational studies, a number of questions remain.
First, as the authors appropriately note, causality cannot be proven from a retrospective study. While the analytic methods employed by the authors serve to limit the effect of residual confounding, they do not eliminate it. Although unlikely, it is possible low VT may be a marker for an unmeasured variable that leads to more favorable neurocognitive outcomes. Further research into a possible casual association between VT and neurocognitive outcomes is needed.
The authors also suggest a number of inflammatory-related mechanisms for the association between lower VT and improved neurocognitive outcomes, which they collectively name “brain-lung communication.” While this is a physiologically attractive hypothesis in light of what is known regarding PCAS, the retrospective nature of the study prevents measurement of any inflammatory markers or cytokine levels that might strengthen this hypothesis. As it stands, further exploration of the mechanisms that might link lower VT to improved neurocognitive outcomes will be required before a more definitive statement regarding brain-lung communication can be accepted.
Although the authors identified an association between lower VT and a number of secondary outcomes, their results show there were no significant associations between lower VT and fewer days of extrapulmonary organ failure or improved survival. Given the contradictory nature of some of these secondary outcomes (such as an association with fewer shock-free days but no association with less extrapulmonary organ failure, a known consequence of hemodynamic shock), the true impact of low VT on these outcomes is unclear. While it is logical that the association between lower VT and some secondary outcomes (such as fewer ICU days and fewer ventilator-dependent days) is a result of improved neurocognitive outcomes, further work is required to elucidate the true clinical significance of these secondary outcomes.
Finally, while there was no significant difference between groups in terms of initial pH or PCO2, and these variables were included in the propensity matching analysis, both groups had mean initial PCO2 levels that were elevated (47 mm Hg and 49 mm Hg in the high and low VT groups, respectively). These values are above the physiological range (35–45 mm Hg) recommended by the 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care [3]. The authors suggest that the recommended eucapnic targets can be met in a low VT strategy by increasing the respiratory rate. However, current literature suggests that patients with ARDS exposed to higher respiratory rates may have more frequent exposure to ventilator-induced lung injury (VILI) stresses and an increased rate of lung injury [4]. While there are no clinical trials proving the benefit of a low vs. high respiratory rate strategy, current recommendations for reducing the risk of VILI include limiting the respiratory rate. It is unclear at this time if an increase in the respiratory rate would increase the incidence of VILI and negate any potential benefit provided by low VT in these patients, but this would be an important cost to account for when employing a low VT strategy.
Applications for Clinical Practice
In this study, Beitler and colleagues found that using a low VT ventilation strategy in OHCA patients was associated with improved neurocognitive outcomes. This study is primarily useful as a hypothesis generator. Further research into the effects of ventilator parameters such as VT on the inflammatory cascade, neurocognitive outcomes in other groups of patients (such as those with ARDS), and the existence of a “brain-lung communication” pathway is warranted. From a practical standpoint, evidence continues to mount that lower VT is associated with a number of beneficial effects that are not limited to patients with ARDS [5]. This study would support the current practice of many intensivists to utilize a low VT strategy unless a compelling contraindication exists, as the potential benefits are substantial and the risks minimal. However, this practice will have to be balanced with the need to avoid hypercapnia, and the elevated respiratory rates used to achieve eucapnia may have unforeseen consequences.
—Arun Jose, MD, The George Washington University, Washington, DC
1. Moulaert VR, Verbunt JA, van Heugten CM, Wade DT. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation 2009;80:297–305.
2. Peberdy MA, Andersen LW, Abbate A, et al. Inflammatory markers following resuscitation from out-of-hospital cardiac arrest – A prospective multicenter observational study. Resuscitation 2016;103:117–24.
3. Callaway CW, Soar J, Aibiki M, et al. Advanced life support chapter collaborators. Part 4: Advanced life support: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015;132:S84–S145.
4. Beitler JR, Malhotra A, Thompson BT. Ventilator-induced lung injury. Clin Chest Med 2016;37:633–46.
5. Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA 2012;
308:1651–9.
Study Overview
Objective. To determine if there is an association between low tidal volume (VT) ventilation and neurocognitive outcomes in patients after out-of-hospital cardiac arrest (OHCA).
Design. Retrospective cohort study.
Setting and participants. Data was obtained from retrospective review of all adults admitted between 2008 and 2014 to one of 2 centers (A or B) with nontraumatic OHCA requiring mechanical ventilation for greater than 48 hours. The study physicians screened records primarily using chart review with secondary confirmation of the diagnosis of OHCA and eligibility criteria. Patients with an outside hospital stay greater than 24 hours, intracranial hemorrhage, use of extracorporeal membranous oxygenation (ECMO), use of airway pressure release mode of ventilation, chronic dependence on mechanical ventilation, or missing data were excluded. Of the 579 patients with OHCA, 256 (44.2%) met the inclusion criteria and were included in the main analysis. A total of 97 patients were identified as having high VT (defined as > 8 mL/kg of predicted body weight [PBW]) and were matched to 97 of the 159 patients identified as having a low VT as part of the propensity-matched subgroup analysis using 1:1 optimal caliper matching.
Main outcome measure. The primary outcome was a favorable neurocognitive outcome at hospital discharge (Cerebral Performance Category score [CPC] of 1 or 2). A CPC of 1 or 2 corresponds to normal life or life that is disabled but independent, respectively. A CPC of 3 is disabled and dependent, and a CPC of 5 is alive but brain dead. Two physicians blinded to VT and other measures of illness severity calculated the CPC via chart review. Discordant scores were resolved by consensus, and a Kappa statistic was calculated to quantify agreement between investigators. Secondary outcomes included ventilator-free days, hospital-free days, ICU-free days, shock-free days, and extrapulmonary organ failure–free days. Logistic regression with backward elimination was used to identify predictors of receiving VT ≤ 8 mL/kg PBW to be used in the propensity-matched analysis, along with relevant predictors identified from the literature. The odds ratio for the primary outcome was calculated using both logistic regression analysis and propensity-matched analysis. Other methods of sensitivity analysis (propensity quintile adjustment, inverse-probability-of-treatment weighting) were used to confirm the robustness of the initial analysis to different statistical methods. A P value of < 0.05 was considered significant.
Main results. Of the study patients, approximately half (49% in high VT, 52% in low VT) had an initial rhythm of ventricular tachycardia or ventricular fibrillation. Patients with low VT were significantly younger (mean age 59 yr vs. 66 yr), taller (mean height 177 cm vs. 165 cm), and heavier (mean weight 88 kg vs. 81 kg). There were also significantly fewer females in the low VT group (19% vs. 46%). There were no significant differences between baseline comorbidities, arrest characteristics, or illness severity between the 2 groups with the exception of significantly more patients in the low VT underwent therapeutic hypothermia (87% vs. 76%) and were admitted to hospital A (69% vs. 55%). There were no significant differences between the groups across ventilator parameters aside from tidal volume. The average VT in mL/kg PBW was 9.3 in the high VT group and 7.1 in the low VT group over the first 48 hours.
In the multivariate regression analysis, significant independent predictors of receiving high VT included height, weight, and hospital of admission. The final propensity model to predict VT included age, height, weight, sex, illness severity measures (APACHE-II score and presence of circulatory shock in the first 24 hours of admission), arrest characteristics, and respiratory characteristics (initial pH, initial PaCO2, PaO2:FiO2 ratio, and initial peak inspiratory pressure) as covariates. The use of low VT was significantly associated with a favorable neurocognitive outcome in the multivariate regression analysis (odds ratio [OR] 1.65, 95% confidence interval [CI] 1.18–2.29). This association held in both the propensity matched analysis (OR 1.68, 95% CI 1.11–2.55) as well as conditional logistic regression analysis using propensity score as a covariate (OR 1.61, 95% CI 1.13–2.28).
In the propensity-adjusted conditional logistic regression analysis, a lower VT (1 mL/kg of PBW decrease) was significantly associated with ventilator-free days (OR 1.78, 95% CI 0.39–3.16), shock-free days (OR 1.31, 95% CI 0.10–2.51), ICU-free days (OR 1.38, 95% CI 0.13–2.63), and hospital-free days (OR 1.07, 95% CI 0.04–2.09). There was a nonsignificant trend towards improved survival to hospital discharge (OR 1.23, 95% CI 0.95–1.60, P = 0.115). After propensity score adjustment, lower VT was not associated with therapeutic hypothermia (OR 0.14, 95% CI −0.19 to 0.47), and in the multivariate regression analysis there was no association between favorable neurocognitive outcome and therapeutic hypothermia (P = 0.516). While there was a significant association between lower VT and site of admission (Hospital A: OR 1.50, 95% CI 1.04–2.17 per 1 mL/kg of PBW decrease), there was no association between favorable neurocognitive outcome and hospital site of admission in the final adjusted regression analysis (P = 0.588).
Conclusion. In this retrospective cohort study, lower VT in the first 48 hours of admission following OHCA was independently associated with favorable neurocognitive outcomes as measured by the CPC score, as well as more ventilator-free, shock-free, ICU-free, and hospital-free days.
Commentary
Neurocognitive impairment following nontraumatic OHCA is common, estimated to occur in roughly half of all survivors [1]. Similar to the acute respiratory distress syndrome (ARDS), the post–cardiac arrest syndrome (PCAS) is recognized as a systemic process with multi-organ effects thought to be mediated in part by inflammatory cytokines [2]. While the beneficial role of low VT in patients with ARDS is well established, currently there are no recommendations for specific VT targets in post–cardiac arrest care, and the effect of VT on outcomes following cardiac arrest is unknown [3].
In this study, Beitler and colleagues suggest a possible association between VT and neurocognitive outcomes following OHCA. Using retrospective data drawn from 2 centers, and employing both regression analysis and propensity matching, the authors identified a significant beneficial effect of lower VT on neurocognitive outcomes in their cohort. This benefit held regardless of the statistical analytic method employed and was present even when correcting for the difference between groups in hospital admission site and use of therapeutic hypothermia in the original cohort. The authors also demonstrated a lower VT was associated with a number of secondary outcomes including fewer hospital, ICU, and ventilator days. While the statistical methods employed by the authors are robust and attempt to account for the limitations inherent to observational studies, a number of questions remain.
First, as the authors appropriately note, causality cannot be proven from a retrospective study. While the analytic methods employed by the authors serve to limit the effect of residual confounding, they do not eliminate it. Although unlikely, it is possible low VT may be a marker for an unmeasured variable that leads to more favorable neurocognitive outcomes. Further research into a possible casual association between VT and neurocognitive outcomes is needed.
The authors also suggest a number of inflammatory-related mechanisms for the association between lower VT and improved neurocognitive outcomes, which they collectively name “brain-lung communication.” While this is a physiologically attractive hypothesis in light of what is known regarding PCAS, the retrospective nature of the study prevents measurement of any inflammatory markers or cytokine levels that might strengthen this hypothesis. As it stands, further exploration of the mechanisms that might link lower VT to improved neurocognitive outcomes will be required before a more definitive statement regarding brain-lung communication can be accepted.
Although the authors identified an association between lower VT and a number of secondary outcomes, their results show there were no significant associations between lower VT and fewer days of extrapulmonary organ failure or improved survival. Given the contradictory nature of some of these secondary outcomes (such as an association with fewer shock-free days but no association with less extrapulmonary organ failure, a known consequence of hemodynamic shock), the true impact of low VT on these outcomes is unclear. While it is logical that the association between lower VT and some secondary outcomes (such as fewer ICU days and fewer ventilator-dependent days) is a result of improved neurocognitive outcomes, further work is required to elucidate the true clinical significance of these secondary outcomes.
Finally, while there was no significant difference between groups in terms of initial pH or PCO2, and these variables were included in the propensity matching analysis, both groups had mean initial PCO2 levels that were elevated (47 mm Hg and 49 mm Hg in the high and low VT groups, respectively). These values are above the physiological range (35–45 mm Hg) recommended by the 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care [3]. The authors suggest that the recommended eucapnic targets can be met in a low VT strategy by increasing the respiratory rate. However, current literature suggests that patients with ARDS exposed to higher respiratory rates may have more frequent exposure to ventilator-induced lung injury (VILI) stresses and an increased rate of lung injury [4]. While there are no clinical trials proving the benefit of a low vs. high respiratory rate strategy, current recommendations for reducing the risk of VILI include limiting the respiratory rate. It is unclear at this time if an increase in the respiratory rate would increase the incidence of VILI and negate any potential benefit provided by low VT in these patients, but this would be an important cost to account for when employing a low VT strategy.
Applications for Clinical Practice
In this study, Beitler and colleagues found that using a low VT ventilation strategy in OHCA patients was associated with improved neurocognitive outcomes. This study is primarily useful as a hypothesis generator. Further research into the effects of ventilator parameters such as VT on the inflammatory cascade, neurocognitive outcomes in other groups of patients (such as those with ARDS), and the existence of a “brain-lung communication” pathway is warranted. From a practical standpoint, evidence continues to mount that lower VT is associated with a number of beneficial effects that are not limited to patients with ARDS [5]. This study would support the current practice of many intensivists to utilize a low VT strategy unless a compelling contraindication exists, as the potential benefits are substantial and the risks minimal. However, this practice will have to be balanced with the need to avoid hypercapnia, and the elevated respiratory rates used to achieve eucapnia may have unforeseen consequences.
—Arun Jose, MD, The George Washington University, Washington, DC
Study Overview
Objective. To determine if there is an association between low tidal volume (VT) ventilation and neurocognitive outcomes in patients after out-of-hospital cardiac arrest (OHCA).
Design. Retrospective cohort study.
Setting and participants. Data was obtained from retrospective review of all adults admitted between 2008 and 2014 to one of 2 centers (A or B) with nontraumatic OHCA requiring mechanical ventilation for greater than 48 hours. The study physicians screened records primarily using chart review with secondary confirmation of the diagnosis of OHCA and eligibility criteria. Patients with an outside hospital stay greater than 24 hours, intracranial hemorrhage, use of extracorporeal membranous oxygenation (ECMO), use of airway pressure release mode of ventilation, chronic dependence on mechanical ventilation, or missing data were excluded. Of the 579 patients with OHCA, 256 (44.2%) met the inclusion criteria and were included in the main analysis. A total of 97 patients were identified as having high VT (defined as > 8 mL/kg of predicted body weight [PBW]) and were matched to 97 of the 159 patients identified as having a low VT as part of the propensity-matched subgroup analysis using 1:1 optimal caliper matching.
Main outcome measure. The primary outcome was a favorable neurocognitive outcome at hospital discharge (Cerebral Performance Category score [CPC] of 1 or 2). A CPC of 1 or 2 corresponds to normal life or life that is disabled but independent, respectively. A CPC of 3 is disabled and dependent, and a CPC of 5 is alive but brain dead. Two physicians blinded to VT and other measures of illness severity calculated the CPC via chart review. Discordant scores were resolved by consensus, and a Kappa statistic was calculated to quantify agreement between investigators. Secondary outcomes included ventilator-free days, hospital-free days, ICU-free days, shock-free days, and extrapulmonary organ failure–free days. Logistic regression with backward elimination was used to identify predictors of receiving VT ≤ 8 mL/kg PBW to be used in the propensity-matched analysis, along with relevant predictors identified from the literature. The odds ratio for the primary outcome was calculated using both logistic regression analysis and propensity-matched analysis. Other methods of sensitivity analysis (propensity quintile adjustment, inverse-probability-of-treatment weighting) were used to confirm the robustness of the initial analysis to different statistical methods. A P value of < 0.05 was considered significant.
Main results. Of the study patients, approximately half (49% in high VT, 52% in low VT) had an initial rhythm of ventricular tachycardia or ventricular fibrillation. Patients with low VT were significantly younger (mean age 59 yr vs. 66 yr), taller (mean height 177 cm vs. 165 cm), and heavier (mean weight 88 kg vs. 81 kg). There were also significantly fewer females in the low VT group (19% vs. 46%). There were no significant differences between baseline comorbidities, arrest characteristics, or illness severity between the 2 groups with the exception of significantly more patients in the low VT underwent therapeutic hypothermia (87% vs. 76%) and were admitted to hospital A (69% vs. 55%). There were no significant differences between the groups across ventilator parameters aside from tidal volume. The average VT in mL/kg PBW was 9.3 in the high VT group and 7.1 in the low VT group over the first 48 hours.
In the multivariate regression analysis, significant independent predictors of receiving high VT included height, weight, and hospital of admission. The final propensity model to predict VT included age, height, weight, sex, illness severity measures (APACHE-II score and presence of circulatory shock in the first 24 hours of admission), arrest characteristics, and respiratory characteristics (initial pH, initial PaCO2, PaO2:FiO2 ratio, and initial peak inspiratory pressure) as covariates. The use of low VT was significantly associated with a favorable neurocognitive outcome in the multivariate regression analysis (odds ratio [OR] 1.65, 95% confidence interval [CI] 1.18–2.29). This association held in both the propensity matched analysis (OR 1.68, 95% CI 1.11–2.55) as well as conditional logistic regression analysis using propensity score as a covariate (OR 1.61, 95% CI 1.13–2.28).
In the propensity-adjusted conditional logistic regression analysis, a lower VT (1 mL/kg of PBW decrease) was significantly associated with ventilator-free days (OR 1.78, 95% CI 0.39–3.16), shock-free days (OR 1.31, 95% CI 0.10–2.51), ICU-free days (OR 1.38, 95% CI 0.13–2.63), and hospital-free days (OR 1.07, 95% CI 0.04–2.09). There was a nonsignificant trend towards improved survival to hospital discharge (OR 1.23, 95% CI 0.95–1.60, P = 0.115). After propensity score adjustment, lower VT was not associated with therapeutic hypothermia (OR 0.14, 95% CI −0.19 to 0.47), and in the multivariate regression analysis there was no association between favorable neurocognitive outcome and therapeutic hypothermia (P = 0.516). While there was a significant association between lower VT and site of admission (Hospital A: OR 1.50, 95% CI 1.04–2.17 per 1 mL/kg of PBW decrease), there was no association between favorable neurocognitive outcome and hospital site of admission in the final adjusted regression analysis (P = 0.588).
Conclusion. In this retrospective cohort study, lower VT in the first 48 hours of admission following OHCA was independently associated with favorable neurocognitive outcomes as measured by the CPC score, as well as more ventilator-free, shock-free, ICU-free, and hospital-free days.
Commentary
Neurocognitive impairment following nontraumatic OHCA is common, estimated to occur in roughly half of all survivors [1]. Similar to the acute respiratory distress syndrome (ARDS), the post–cardiac arrest syndrome (PCAS) is recognized as a systemic process with multi-organ effects thought to be mediated in part by inflammatory cytokines [2]. While the beneficial role of low VT in patients with ARDS is well established, currently there are no recommendations for specific VT targets in post–cardiac arrest care, and the effect of VT on outcomes following cardiac arrest is unknown [3].
In this study, Beitler and colleagues suggest a possible association between VT and neurocognitive outcomes following OHCA. Using retrospective data drawn from 2 centers, and employing both regression analysis and propensity matching, the authors identified a significant beneficial effect of lower VT on neurocognitive outcomes in their cohort. This benefit held regardless of the statistical analytic method employed and was present even when correcting for the difference between groups in hospital admission site and use of therapeutic hypothermia in the original cohort. The authors also demonstrated a lower VT was associated with a number of secondary outcomes including fewer hospital, ICU, and ventilator days. While the statistical methods employed by the authors are robust and attempt to account for the limitations inherent to observational studies, a number of questions remain.
First, as the authors appropriately note, causality cannot be proven from a retrospective study. While the analytic methods employed by the authors serve to limit the effect of residual confounding, they do not eliminate it. Although unlikely, it is possible low VT may be a marker for an unmeasured variable that leads to more favorable neurocognitive outcomes. Further research into a possible casual association between VT and neurocognitive outcomes is needed.
The authors also suggest a number of inflammatory-related mechanisms for the association between lower VT and improved neurocognitive outcomes, which they collectively name “brain-lung communication.” While this is a physiologically attractive hypothesis in light of what is known regarding PCAS, the retrospective nature of the study prevents measurement of any inflammatory markers or cytokine levels that might strengthen this hypothesis. As it stands, further exploration of the mechanisms that might link lower VT to improved neurocognitive outcomes will be required before a more definitive statement regarding brain-lung communication can be accepted.
Although the authors identified an association between lower VT and a number of secondary outcomes, their results show there were no significant associations between lower VT and fewer days of extrapulmonary organ failure or improved survival. Given the contradictory nature of some of these secondary outcomes (such as an association with fewer shock-free days but no association with less extrapulmonary organ failure, a known consequence of hemodynamic shock), the true impact of low VT on these outcomes is unclear. While it is logical that the association between lower VT and some secondary outcomes (such as fewer ICU days and fewer ventilator-dependent days) is a result of improved neurocognitive outcomes, further work is required to elucidate the true clinical significance of these secondary outcomes.
Finally, while there was no significant difference between groups in terms of initial pH or PCO2, and these variables were included in the propensity matching analysis, both groups had mean initial PCO2 levels that were elevated (47 mm Hg and 49 mm Hg in the high and low VT groups, respectively). These values are above the physiological range (35–45 mm Hg) recommended by the 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care [3]. The authors suggest that the recommended eucapnic targets can be met in a low VT strategy by increasing the respiratory rate. However, current literature suggests that patients with ARDS exposed to higher respiratory rates may have more frequent exposure to ventilator-induced lung injury (VILI) stresses and an increased rate of lung injury [4]. While there are no clinical trials proving the benefit of a low vs. high respiratory rate strategy, current recommendations for reducing the risk of VILI include limiting the respiratory rate. It is unclear at this time if an increase in the respiratory rate would increase the incidence of VILI and negate any potential benefit provided by low VT in these patients, but this would be an important cost to account for when employing a low VT strategy.
Applications for Clinical Practice
In this study, Beitler and colleagues found that using a low VT ventilation strategy in OHCA patients was associated with improved neurocognitive outcomes. This study is primarily useful as a hypothesis generator. Further research into the effects of ventilator parameters such as VT on the inflammatory cascade, neurocognitive outcomes in other groups of patients (such as those with ARDS), and the existence of a “brain-lung communication” pathway is warranted. From a practical standpoint, evidence continues to mount that lower VT is associated with a number of beneficial effects that are not limited to patients with ARDS [5]. This study would support the current practice of many intensivists to utilize a low VT strategy unless a compelling contraindication exists, as the potential benefits are substantial and the risks minimal. However, this practice will have to be balanced with the need to avoid hypercapnia, and the elevated respiratory rates used to achieve eucapnia may have unforeseen consequences.
—Arun Jose, MD, The George Washington University, Washington, DC
1. Moulaert VR, Verbunt JA, van Heugten CM, Wade DT. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation 2009;80:297–305.
2. Peberdy MA, Andersen LW, Abbate A, et al. Inflammatory markers following resuscitation from out-of-hospital cardiac arrest – A prospective multicenter observational study. Resuscitation 2016;103:117–24.
3. Callaway CW, Soar J, Aibiki M, et al. Advanced life support chapter collaborators. Part 4: Advanced life support: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015;132:S84–S145.
4. Beitler JR, Malhotra A, Thompson BT. Ventilator-induced lung injury. Clin Chest Med 2016;37:633–46.
5. Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA 2012;
308:1651–9.
1. Moulaert VR, Verbunt JA, van Heugten CM, Wade DT. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation 2009;80:297–305.
2. Peberdy MA, Andersen LW, Abbate A, et al. Inflammatory markers following resuscitation from out-of-hospital cardiac arrest – A prospective multicenter observational study. Resuscitation 2016;103:117–24.
3. Callaway CW, Soar J, Aibiki M, et al. Advanced life support chapter collaborators. Part 4: Advanced life support: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015;132:S84–S145.
4. Beitler JR, Malhotra A, Thompson BT. Ventilator-induced lung injury. Clin Chest Med 2016;37:633–46.
5. Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA 2012;
308:1651–9.
Use of Lay Navigation Is Associated with Reduction in Health Care Use and Medicare Costs Among Older Adults with Cancer
Study Overview
Objective. To determine the effect of navigation for older cancer patients by lay persons on health care use and Medicare costs.
Design. Observational cohort study using propensity score–matched controls.
Setting and participants. The study was conducted at the University of Alabama at Birmingham Health System Cancer Community Network, which consists of 2 academic and 10 community cancer centers across Alabama, Georgia, Florida, Mississippi and Tennessee. Participants were Medicare beneficiaries who received care at these facilities from 1 Jan 2012 to 31 Dec 2015. The patient population includes Medicare beneficiaries age 65 years or older with primary Medicare Part A and B insurance and a cancer diagnosis from 2012 to 2015, and excludes those with Medicare health maintenance organization coverage. Only patients with 1 quarter of observation prior to receiving patient navigation and those with 2 quarters of observation after initiation of navigation services were included in the sample. Propensity score matching method was used to establish a matched group of patients without patient navigation. Covariates included in the propensity score matching include age at diagnosis, race, sex, cancer acuity, phase of care, comorbidity score, cost of care, treatment with chemotherapy and emergency department (ED) and intensive care unit use at baseline.
Patients were identified to receive patient navigation through review of patient census in the ED and hospital, clinical referral, and self-referral. High-risk patients were prioritized to receive navigation; this included patients with metastatic disease, cancers that have high morbidity, chronic diseases that have high morbidity, or a history of recent acute care utilization.
Navigation program. The patient navigation program was started in 2013 as an innovation project funded by the Center for Medicare and Medicaid Services. Implementation began in March 2013 and all sites started to enroll patients for patient navigation by October 2013. Patient navigation was conducted by lay navigators who were hired from within the community. Navigators were required to have a bachelor’s degree but were not licensed clinicians such as a nurse or social worker. Patient navigators aimed to proactively identify patient needs, connect patient with resources, coordinate patient care, and empower patients to take an active role in their own care. Navigators performed distress screenings that assessed patients’ practical, information, financial, familial, emotional, spiritual and physical concerns. Assistance was given to patients at patients’ request and algorithms were used to guide frequency of contact.
Main outcome measures. The main outcome measure was Medicare costs per beneficiary per quarter; these costs include all amounts paid by Medicare for all care received but exclude Medicare Part D prescription drug costs. Other outcomes included source of costs and resource utilization defined by number of ED visits, hospitalizations, and intensive care unit admissions per quarter. The return on investment was also examined with the investment defined by salaries for the patient navigators, including fringe benefits; each navigator had a mean caseload of 152 patients per quarter. The return on investment was calculated as reduced Medicare costs of navigated patients compared with non-navigated patients multiplied by the number of patients served.
Main results. A total of 6214 matched pairs of navigated and non-navigated patients were included in the analysis. The mean age of the patients was 75 (SD ± 7) and 12% were African American. Medicare costs declined faster among those with navigation compared to the control group by $781 more per quarter per navigated patient. Inpatient and outpatient costs had the largest decline at $294 and $275 respectively. Resource use decreased in the navigated group more so than the non-navigated group, with a 6% more decrease per quarter in ED visits, 8% more decrease in hospitalization, and 11% more decrease in intensive care unit admissions. The return on investment was estimated at 1:10 with a $475,024 reduction in Medicare cost per navigator annually.
Conclusion. Navigation by lay persons among older Medicare beneficiaries with cancer is associated with a decrease in Medicare costs and resource utilization. There is substantial return on investment when considering the salaries of navigator staff against the Medicare savings associated with care navigation. Lay navigation appears to have benefits of reducing health care costs and resource use.
Commentary
The U.S. health care system is often difficult to navigate for older persons, particularly those with complex health care needs. Older adults with chronic disease, including cancer, may utilize care in multiple settings and with multiple providers and teams, making it challenging to organize and obtain needed care. In this study, the authors examined the impact of a patient navigation program on older patients with cancer and found that the use of lay navigation is associated with reduced costs and resource use for the health care system. Prior studies have examined the use of care navigation in complex chronic disease management, such as HIV infection and cancer [1,2] and have often found positive impacts on patient satisfaction, adherence to treatments, and reducing care disparities in vulnerable populations [3]. Care navigation has been performed using clinical staff, such as nursing, but with lay persons as well [4]. Lay persons offer the benefit of reduced costs, and if they are able to perform the care navigation tasks well with training, clinical staff use may not be necessary.
This study uses alternative methods to randomization to generate a balanced non-navigated control group for comparison to determine the impact of care navigation. The limitation is that the propensity score method used may balance potential confounders that are specified but unmeasured confounders were not accounted for in the analysis [5]. Another limitation is that the comparison group may not be concurrent, because non-navigated patients prior to the initiation of the navigation program were included in the control group. As care delivery often changes over time, non-concurrent comparison may introduce bias in the study. Nonetheless, the effect that is found on costs and resource utilization appear to be a strong one and is consistent with prior studies on the effects of care navigation.
Although this study spanned several clinical settings across a large geographic area, it is unclear if the program will offer similar benefits at other institutions. Additional studies that examine the impact of lay navigation on other patient outcomes such as satisfaction will be useful, as will studying the model at other institutions and in other settings to examine whether the program’s effects can be generalized.
Applications for Clinical Practice
In general, evidence suggests that patient navigation is an effective intervention for use in health care. Clinicians should consider assigning team members to help their patients with cancer navigate the health care system.
—William W. Hung, MD, MPH
1. Shacham E, López JD, Brown TM, et al. Enhancing adherence to care in the HIV care continuum: the Barrier Elimination and Care Navigation (BEACON) project evaluation. AIDS Behav 2017.
2. Ali-Faisal SF, Colella TJ, Medina-Jaudes N, Benz Scott L. The effectiveness of patient navigation to improve healthcare utilization outcomes: A meta-analysis of randomized controlled trials. Patient Educ Couns 2017;100:436–48.
3. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
4. Kim K, Choi JS, Choi E, et al. Effects of community-based health worker interventions to improve chronic disease management and care among vulnerable populations: a systematic review. Am J Public Health 2016;106:e3–e28.
5. Austin PC, Grootendorst P, Anderson GM. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: a Monte Carlo study. Stat Med 2007;26:734–53.
Study Overview
Objective. To determine the effect of navigation for older cancer patients by lay persons on health care use and Medicare costs.
Design. Observational cohort study using propensity score–matched controls.
Setting and participants. The study was conducted at the University of Alabama at Birmingham Health System Cancer Community Network, which consists of 2 academic and 10 community cancer centers across Alabama, Georgia, Florida, Mississippi and Tennessee. Participants were Medicare beneficiaries who received care at these facilities from 1 Jan 2012 to 31 Dec 2015. The patient population includes Medicare beneficiaries age 65 years or older with primary Medicare Part A and B insurance and a cancer diagnosis from 2012 to 2015, and excludes those with Medicare health maintenance organization coverage. Only patients with 1 quarter of observation prior to receiving patient navigation and those with 2 quarters of observation after initiation of navigation services were included in the sample. Propensity score matching method was used to establish a matched group of patients without patient navigation. Covariates included in the propensity score matching include age at diagnosis, race, sex, cancer acuity, phase of care, comorbidity score, cost of care, treatment with chemotherapy and emergency department (ED) and intensive care unit use at baseline.
Patients were identified to receive patient navigation through review of patient census in the ED and hospital, clinical referral, and self-referral. High-risk patients were prioritized to receive navigation; this included patients with metastatic disease, cancers that have high morbidity, chronic diseases that have high morbidity, or a history of recent acute care utilization.
Navigation program. The patient navigation program was started in 2013 as an innovation project funded by the Center for Medicare and Medicaid Services. Implementation began in March 2013 and all sites started to enroll patients for patient navigation by October 2013. Patient navigation was conducted by lay navigators who were hired from within the community. Navigators were required to have a bachelor’s degree but were not licensed clinicians such as a nurse or social worker. Patient navigators aimed to proactively identify patient needs, connect patient with resources, coordinate patient care, and empower patients to take an active role in their own care. Navigators performed distress screenings that assessed patients’ practical, information, financial, familial, emotional, spiritual and physical concerns. Assistance was given to patients at patients’ request and algorithms were used to guide frequency of contact.
Main outcome measures. The main outcome measure was Medicare costs per beneficiary per quarter; these costs include all amounts paid by Medicare for all care received but exclude Medicare Part D prescription drug costs. Other outcomes included source of costs and resource utilization defined by number of ED visits, hospitalizations, and intensive care unit admissions per quarter. The return on investment was also examined with the investment defined by salaries for the patient navigators, including fringe benefits; each navigator had a mean caseload of 152 patients per quarter. The return on investment was calculated as reduced Medicare costs of navigated patients compared with non-navigated patients multiplied by the number of patients served.
Main results. A total of 6214 matched pairs of navigated and non-navigated patients were included in the analysis. The mean age of the patients was 75 (SD ± 7) and 12% were African American. Medicare costs declined faster among those with navigation compared to the control group by $781 more per quarter per navigated patient. Inpatient and outpatient costs had the largest decline at $294 and $275 respectively. Resource use decreased in the navigated group more so than the non-navigated group, with a 6% more decrease per quarter in ED visits, 8% more decrease in hospitalization, and 11% more decrease in intensive care unit admissions. The return on investment was estimated at 1:10 with a $475,024 reduction in Medicare cost per navigator annually.
Conclusion. Navigation by lay persons among older Medicare beneficiaries with cancer is associated with a decrease in Medicare costs and resource utilization. There is substantial return on investment when considering the salaries of navigator staff against the Medicare savings associated with care navigation. Lay navigation appears to have benefits of reducing health care costs and resource use.
Commentary
The U.S. health care system is often difficult to navigate for older persons, particularly those with complex health care needs. Older adults with chronic disease, including cancer, may utilize care in multiple settings and with multiple providers and teams, making it challenging to organize and obtain needed care. In this study, the authors examined the impact of a patient navigation program on older patients with cancer and found that the use of lay navigation is associated with reduced costs and resource use for the health care system. Prior studies have examined the use of care navigation in complex chronic disease management, such as HIV infection and cancer [1,2] and have often found positive impacts on patient satisfaction, adherence to treatments, and reducing care disparities in vulnerable populations [3]. Care navigation has been performed using clinical staff, such as nursing, but with lay persons as well [4]. Lay persons offer the benefit of reduced costs, and if they are able to perform the care navigation tasks well with training, clinical staff use may not be necessary.
This study uses alternative methods to randomization to generate a balanced non-navigated control group for comparison to determine the impact of care navigation. The limitation is that the propensity score method used may balance potential confounders that are specified but unmeasured confounders were not accounted for in the analysis [5]. Another limitation is that the comparison group may not be concurrent, because non-navigated patients prior to the initiation of the navigation program were included in the control group. As care delivery often changes over time, non-concurrent comparison may introduce bias in the study. Nonetheless, the effect that is found on costs and resource utilization appear to be a strong one and is consistent with prior studies on the effects of care navigation.
Although this study spanned several clinical settings across a large geographic area, it is unclear if the program will offer similar benefits at other institutions. Additional studies that examine the impact of lay navigation on other patient outcomes such as satisfaction will be useful, as will studying the model at other institutions and in other settings to examine whether the program’s effects can be generalized.
Applications for Clinical Practice
In general, evidence suggests that patient navigation is an effective intervention for use in health care. Clinicians should consider assigning team members to help their patients with cancer navigate the health care system.
—William W. Hung, MD, MPH
Study Overview
Objective. To determine the effect of navigation for older cancer patients by lay persons on health care use and Medicare costs.
Design. Observational cohort study using propensity score–matched controls.
Setting and participants. The study was conducted at the University of Alabama at Birmingham Health System Cancer Community Network, which consists of 2 academic and 10 community cancer centers across Alabama, Georgia, Florida, Mississippi and Tennessee. Participants were Medicare beneficiaries who received care at these facilities from 1 Jan 2012 to 31 Dec 2015. The patient population includes Medicare beneficiaries age 65 years or older with primary Medicare Part A and B insurance and a cancer diagnosis from 2012 to 2015, and excludes those with Medicare health maintenance organization coverage. Only patients with 1 quarter of observation prior to receiving patient navigation and those with 2 quarters of observation after initiation of navigation services were included in the sample. Propensity score matching method was used to establish a matched group of patients without patient navigation. Covariates included in the propensity score matching include age at diagnosis, race, sex, cancer acuity, phase of care, comorbidity score, cost of care, treatment with chemotherapy and emergency department (ED) and intensive care unit use at baseline.
Patients were identified to receive patient navigation through review of patient census in the ED and hospital, clinical referral, and self-referral. High-risk patients were prioritized to receive navigation; this included patients with metastatic disease, cancers that have high morbidity, chronic diseases that have high morbidity, or a history of recent acute care utilization.
Navigation program. The patient navigation program was started in 2013 as an innovation project funded by the Center for Medicare and Medicaid Services. Implementation began in March 2013 and all sites started to enroll patients for patient navigation by October 2013. Patient navigation was conducted by lay navigators who were hired from within the community. Navigators were required to have a bachelor’s degree but were not licensed clinicians such as a nurse or social worker. Patient navigators aimed to proactively identify patient needs, connect patient with resources, coordinate patient care, and empower patients to take an active role in their own care. Navigators performed distress screenings that assessed patients’ practical, information, financial, familial, emotional, spiritual and physical concerns. Assistance was given to patients at patients’ request and algorithms were used to guide frequency of contact.
Main outcome measures. The main outcome measure was Medicare costs per beneficiary per quarter; these costs include all amounts paid by Medicare for all care received but exclude Medicare Part D prescription drug costs. Other outcomes included source of costs and resource utilization defined by number of ED visits, hospitalizations, and intensive care unit admissions per quarter. The return on investment was also examined with the investment defined by salaries for the patient navigators, including fringe benefits; each navigator had a mean caseload of 152 patients per quarter. The return on investment was calculated as reduced Medicare costs of navigated patients compared with non-navigated patients multiplied by the number of patients served.
Main results. A total of 6214 matched pairs of navigated and non-navigated patients were included in the analysis. The mean age of the patients was 75 (SD ± 7) and 12% were African American. Medicare costs declined faster among those with navigation compared to the control group by $781 more per quarter per navigated patient. Inpatient and outpatient costs had the largest decline at $294 and $275 respectively. Resource use decreased in the navigated group more so than the non-navigated group, with a 6% more decrease per quarter in ED visits, 8% more decrease in hospitalization, and 11% more decrease in intensive care unit admissions. The return on investment was estimated at 1:10 with a $475,024 reduction in Medicare cost per navigator annually.
Conclusion. Navigation by lay persons among older Medicare beneficiaries with cancer is associated with a decrease in Medicare costs and resource utilization. There is substantial return on investment when considering the salaries of navigator staff against the Medicare savings associated with care navigation. Lay navigation appears to have benefits of reducing health care costs and resource use.
Commentary
The U.S. health care system is often difficult to navigate for older persons, particularly those with complex health care needs. Older adults with chronic disease, including cancer, may utilize care in multiple settings and with multiple providers and teams, making it challenging to organize and obtain needed care. In this study, the authors examined the impact of a patient navigation program on older patients with cancer and found that the use of lay navigation is associated with reduced costs and resource use for the health care system. Prior studies have examined the use of care navigation in complex chronic disease management, such as HIV infection and cancer [1,2] and have often found positive impacts on patient satisfaction, adherence to treatments, and reducing care disparities in vulnerable populations [3]. Care navigation has been performed using clinical staff, such as nursing, but with lay persons as well [4]. Lay persons offer the benefit of reduced costs, and if they are able to perform the care navigation tasks well with training, clinical staff use may not be necessary.
This study uses alternative methods to randomization to generate a balanced non-navigated control group for comparison to determine the impact of care navigation. The limitation is that the propensity score method used may balance potential confounders that are specified but unmeasured confounders were not accounted for in the analysis [5]. Another limitation is that the comparison group may not be concurrent, because non-navigated patients prior to the initiation of the navigation program were included in the control group. As care delivery often changes over time, non-concurrent comparison may introduce bias in the study. Nonetheless, the effect that is found on costs and resource utilization appear to be a strong one and is consistent with prior studies on the effects of care navigation.
Although this study spanned several clinical settings across a large geographic area, it is unclear if the program will offer similar benefits at other institutions. Additional studies that examine the impact of lay navigation on other patient outcomes such as satisfaction will be useful, as will studying the model at other institutions and in other settings to examine whether the program’s effects can be generalized.
Applications for Clinical Practice
In general, evidence suggests that patient navigation is an effective intervention for use in health care. Clinicians should consider assigning team members to help their patients with cancer navigate the health care system.
—William W. Hung, MD, MPH
1. Shacham E, López JD, Brown TM, et al. Enhancing adherence to care in the HIV care continuum: the Barrier Elimination and Care Navigation (BEACON) project evaluation. AIDS Behav 2017.
2. Ali-Faisal SF, Colella TJ, Medina-Jaudes N, Benz Scott L. The effectiveness of patient navigation to improve healthcare utilization outcomes: A meta-analysis of randomized controlled trials. Patient Educ Couns 2017;100:436–48.
3. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
4. Kim K, Choi JS, Choi E, et al. Effects of community-based health worker interventions to improve chronic disease management and care among vulnerable populations: a systematic review. Am J Public Health 2016;106:e3–e28.
5. Austin PC, Grootendorst P, Anderson GM. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: a Monte Carlo study. Stat Med 2007;26:734–53.
1. Shacham E, López JD, Brown TM, et al. Enhancing adherence to care in the HIV care continuum: the Barrier Elimination and Care Navigation (BEACON) project evaluation. AIDS Behav 2017.
2. Ali-Faisal SF, Colella TJ, Medina-Jaudes N, Benz Scott L. The effectiveness of patient navigation to improve healthcare utilization outcomes: A meta-analysis of randomized controlled trials. Patient Educ Couns 2017;100:436–48.
3. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
4. Kim K, Choi JS, Choi E, et al. Effects of community-based health worker interventions to improve chronic disease management and care among vulnerable populations: a systematic review. Am J Public Health 2016;106:e3–e28.
5. Austin PC, Grootendorst P, Anderson GM. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: a Monte Carlo study. Stat Med 2007;26:734–53.
Vaccination does not eliminate risk for meningococcal disease in eculizumab recipients
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM MMWR
Standardization lacking in pediatric trials of atopic dermatitis
CHICAGO – There is considerable variability and poor documentation of severity assessments used for inclusion criteria and baseline severity evaluations in randomized, controlled pediatric atopic dermatitis (AD) trials, results from a systematic review showed.
“It is important for clinicians and investigators to recognize that these differences may limit our ability to reproduce trials, interpret individual studies, and compare results between studies of similar target populations for severity,” lead study author Rishi Chopra, MS, said in an interview in advance of the World Congress of Pediatric Dermatology. “Moreover, this heterogeneity should be considered when retroactively pooling results for meta-analyses of pediatric atopic dermatitis randomized, controlled trials.”
In an effort to evaluate the documentation and characterize the severity assessments used in inclusion criteria and baseline evaluations for randomized, controlled trials of pediatric AD internationally, the researchers performed a systematic review of relevant studies contained in the Cochrane Library, Embase, LILACS, GREAT, MEDLINE, and Scopus databases during 2007-2016. Inclusion criteria were RCT with a pharmacological intervention and any comparison with a control group, children, and males or females. In all, 89 studies met the inclusion/exclusion criteria. Most (70.8%) were studies of pediatric populations aged 0-17 years, and almost 17% were studies of infants aged 0-1 years. The most common target populations were mild-moderate AD (31.5%), moderate-severe AD (18.0%), or undefined (36.0%).
Mr. Chopra and his associates found that the most commonly used severity indices were Scoring AD (SCORAD) in 29.2%, Body Surface Area (BSA) in 16.9%, and global assessments in 13.4%, while the most common assessments of baseline severity were SCORAD in 43.8%, global assessments in 20.2%, Eczema Area and Severity Index in 17.9%, BSA in 14.6%, and visual itch in 13.5%. Only 85.4% of studies recorded the severity assessments used for recruiting the predefined target population and only 76.4% of studies documented baseline severity.
There was considerable heterogeneity across studies, as 16 unique assessments were used as inclusion criteria and 34 assessments were used to evaluate baseline severity. “In addition, even within an individual study, there was substantial discordance in their use as only 71.2% of studies used the same assessments for inclusion and documenting baseline disease severity,” Mr. Chopra said. “Altogether, this multidimensional lack of documentation and heterogeneity of inclusion criteria and baseline severity assessments limits our ability to assess whether the recruitment methods for patients were adequate and confirm whether the intended target population for severity was successfully enrolled.”
He acknowledged certain limitations of the study, including the fact that it may not be generalizable to nonpharmacological interventional trials or noninterventional studies. “In addition, we could only conduct an analysis for studies that provided adequate documentation of inclusion criteria and baseline severity,” Mr. Chopra said. “Thus, those studies that did not provide this information were left out. Nevertheless, across all studies, the uniformity and concordance between assessments likely are even more negatively impacted. It should also be noted that lack of documentation of assessments for inclusion criteria and baseline severity does not imply lack of their utilization. Finally, it is important to acknowledge that AD’s diverse phenotype and relapsing and remitting course may result in the unavoidable heterogeneity of severity assessment use. This may actually help to capture a broader range of disease and improve the external validity of results.”
He reported having no financial disclosures.
CHICAGO – There is considerable variability and poor documentation of severity assessments used for inclusion criteria and baseline severity evaluations in randomized, controlled pediatric atopic dermatitis (AD) trials, results from a systematic review showed.
“It is important for clinicians and investigators to recognize that these differences may limit our ability to reproduce trials, interpret individual studies, and compare results between studies of similar target populations for severity,” lead study author Rishi Chopra, MS, said in an interview in advance of the World Congress of Pediatric Dermatology. “Moreover, this heterogeneity should be considered when retroactively pooling results for meta-analyses of pediatric atopic dermatitis randomized, controlled trials.”
In an effort to evaluate the documentation and characterize the severity assessments used in inclusion criteria and baseline evaluations for randomized, controlled trials of pediatric AD internationally, the researchers performed a systematic review of relevant studies contained in the Cochrane Library, Embase, LILACS, GREAT, MEDLINE, and Scopus databases during 2007-2016. Inclusion criteria were RCT with a pharmacological intervention and any comparison with a control group, children, and males or females. In all, 89 studies met the inclusion/exclusion criteria. Most (70.8%) were studies of pediatric populations aged 0-17 years, and almost 17% were studies of infants aged 0-1 years. The most common target populations were mild-moderate AD (31.5%), moderate-severe AD (18.0%), or undefined (36.0%).
Mr. Chopra and his associates found that the most commonly used severity indices were Scoring AD (SCORAD) in 29.2%, Body Surface Area (BSA) in 16.9%, and global assessments in 13.4%, while the most common assessments of baseline severity were SCORAD in 43.8%, global assessments in 20.2%, Eczema Area and Severity Index in 17.9%, BSA in 14.6%, and visual itch in 13.5%. Only 85.4% of studies recorded the severity assessments used for recruiting the predefined target population and only 76.4% of studies documented baseline severity.
There was considerable heterogeneity across studies, as 16 unique assessments were used as inclusion criteria and 34 assessments were used to evaluate baseline severity. “In addition, even within an individual study, there was substantial discordance in their use as only 71.2% of studies used the same assessments for inclusion and documenting baseline disease severity,” Mr. Chopra said. “Altogether, this multidimensional lack of documentation and heterogeneity of inclusion criteria and baseline severity assessments limits our ability to assess whether the recruitment methods for patients were adequate and confirm whether the intended target population for severity was successfully enrolled.”
He acknowledged certain limitations of the study, including the fact that it may not be generalizable to nonpharmacological interventional trials or noninterventional studies. “In addition, we could only conduct an analysis for studies that provided adequate documentation of inclusion criteria and baseline severity,” Mr. Chopra said. “Thus, those studies that did not provide this information were left out. Nevertheless, across all studies, the uniformity and concordance between assessments likely are even more negatively impacted. It should also be noted that lack of documentation of assessments for inclusion criteria and baseline severity does not imply lack of their utilization. Finally, it is important to acknowledge that AD’s diverse phenotype and relapsing and remitting course may result in the unavoidable heterogeneity of severity assessment use. This may actually help to capture a broader range of disease and improve the external validity of results.”
He reported having no financial disclosures.
CHICAGO – There is considerable variability and poor documentation of severity assessments used for inclusion criteria and baseline severity evaluations in randomized, controlled pediatric atopic dermatitis (AD) trials, results from a systematic review showed.
“It is important for clinicians and investigators to recognize that these differences may limit our ability to reproduce trials, interpret individual studies, and compare results between studies of similar target populations for severity,” lead study author Rishi Chopra, MS, said in an interview in advance of the World Congress of Pediatric Dermatology. “Moreover, this heterogeneity should be considered when retroactively pooling results for meta-analyses of pediatric atopic dermatitis randomized, controlled trials.”
In an effort to evaluate the documentation and characterize the severity assessments used in inclusion criteria and baseline evaluations for randomized, controlled trials of pediatric AD internationally, the researchers performed a systematic review of relevant studies contained in the Cochrane Library, Embase, LILACS, GREAT, MEDLINE, and Scopus databases during 2007-2016. Inclusion criteria were RCT with a pharmacological intervention and any comparison with a control group, children, and males or females. In all, 89 studies met the inclusion/exclusion criteria. Most (70.8%) were studies of pediatric populations aged 0-17 years, and almost 17% were studies of infants aged 0-1 years. The most common target populations were mild-moderate AD (31.5%), moderate-severe AD (18.0%), or undefined (36.0%).
Mr. Chopra and his associates found that the most commonly used severity indices were Scoring AD (SCORAD) in 29.2%, Body Surface Area (BSA) in 16.9%, and global assessments in 13.4%, while the most common assessments of baseline severity were SCORAD in 43.8%, global assessments in 20.2%, Eczema Area and Severity Index in 17.9%, BSA in 14.6%, and visual itch in 13.5%. Only 85.4% of studies recorded the severity assessments used for recruiting the predefined target population and only 76.4% of studies documented baseline severity.
There was considerable heterogeneity across studies, as 16 unique assessments were used as inclusion criteria and 34 assessments were used to evaluate baseline severity. “In addition, even within an individual study, there was substantial discordance in their use as only 71.2% of studies used the same assessments for inclusion and documenting baseline disease severity,” Mr. Chopra said. “Altogether, this multidimensional lack of documentation and heterogeneity of inclusion criteria and baseline severity assessments limits our ability to assess whether the recruitment methods for patients were adequate and confirm whether the intended target population for severity was successfully enrolled.”
He acknowledged certain limitations of the study, including the fact that it may not be generalizable to nonpharmacological interventional trials or noninterventional studies. “In addition, we could only conduct an analysis for studies that provided adequate documentation of inclusion criteria and baseline severity,” Mr. Chopra said. “Thus, those studies that did not provide this information were left out. Nevertheless, across all studies, the uniformity and concordance between assessments likely are even more negatively impacted. It should also be noted that lack of documentation of assessments for inclusion criteria and baseline severity does not imply lack of their utilization. Finally, it is important to acknowledge that AD’s diverse phenotype and relapsing and remitting course may result in the unavoidable heterogeneity of severity assessment use. This may actually help to capture a broader range of disease and improve the external validity of results.”
He reported having no financial disclosures.
AT WCPD 2017
Key clinical point:
Major finding: Only 85.4% of studies recorded the severity assessments used for recruiting the predefined target population, and only 76.4% of studies documented baseline severity.
Data source: A systematic review of 89 pediatric atopic dermatitis randomized, controlled trials published during 2007-2016.
Disclosures: Mr. Chopra reported having no financial disclosures.
Subset of pediatric herpes simplex virus entails frequent episodes
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University. 
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University.
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University.
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
FROM PEDIATRIC DERMATOLOGY
Key clinical point:
Major finding: 19 of 48 (40%) patients had six or more HSV outbreaks per year, and the mean frequency of outbreaks in this study population was seven per year.
Data source: Chart review of 48 cases referred to a single pediatric dermatology clinic in a 10-year period.
Disclosures: No financial disclosures were provided for Dr. Gittler and her associates.
Eroded Plaque on the Lower Lip
The Diagnosis: Squamous Cell Carcinoma
The initial clinical presentation suggested a diagnosis of herpes simplex labialis. The patient reported no response to topical acyclovir, and because the plaque persisted, a biopsy was performed. Pathology demonstrated squamous cell carcinoma (SCC) that was moderately well differentiated and invasive (Figure).
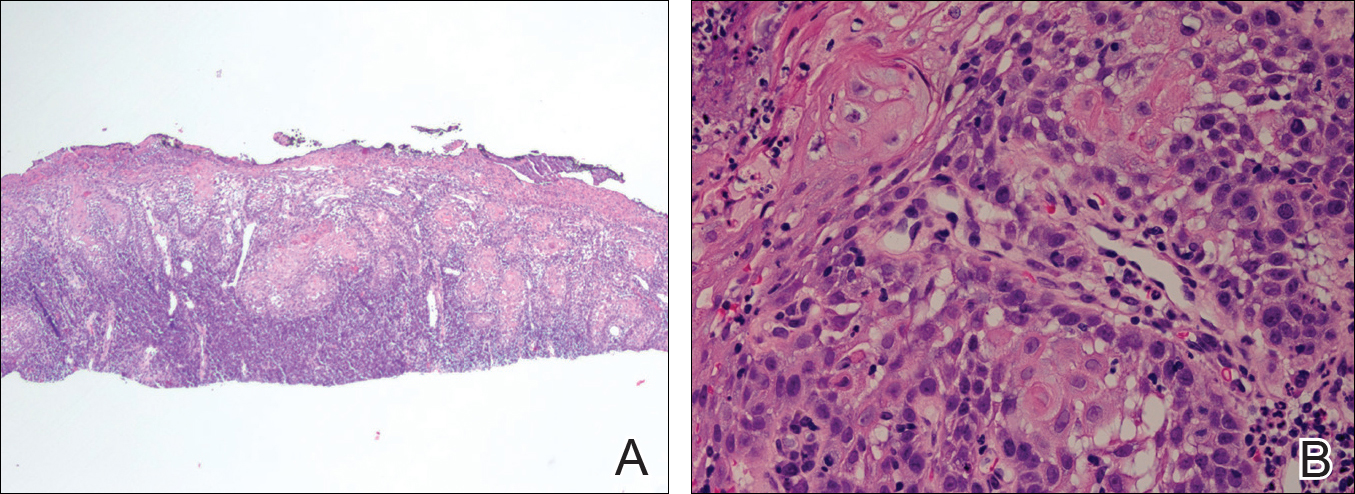
Approximately 38% of all oral SCCs in the United States occur on the lower lip and typically are solar-related cancers developing within the epidermis.1 Oral lesions initially may be asymptomatic and may not be of concern to the patient; however, it is important to recognize SCC early, as invasive lesions have the potential to metastasize. Some factors that increase the chance for the development of metastases include tumor size larger than 2 cm; location on the ear, lip, or other sites on the head and neck; and history of prior unsuccessful treatment.2 Any solitary ulcer, lump, wound, or lesion that will not heal and persists for more than 3 weeks should be regarded as cancer until proven otherwise. Although few oral SCCs are detected by clinicians at an early stage, diagnostic aids such as vital staining and molecular markers in tissues and saliva may be implemented.3 Toluidine blue is a simple, fast, and inexpensive technique that stains the nuclear material of malignant lesions, but not normal mucosa, and may be a worthwhile diagnostic adjunct to clinical inspection.4
Our patient presented with a lesion that clinically looked herpetic, though he reported no prodromal signs of tingling, burning, or pain before the occurrence of the lesion. Due to the persistence of the lesion and lack of response to treatment, a biopsy was indicated. The differential diagnoses include aphthous ulcers, which may occasionally extend on to the vermilion border of the lip and exhibit nondiagnostic histology.5 Bullous oral lichen planus is the least common variant of oral lichen planus, is unlikely to present as a solitary lesion, and is rarely seen on the lips. Histologically, the lesion demonstrated lichenoid inflammation.6 Solitary keratoacanthoma, though histologically similar to SCC, typically presents as a rapidly growing crateriform nodule without erosion or ulceration.7 The differential diagnoses are summarized in the Table.
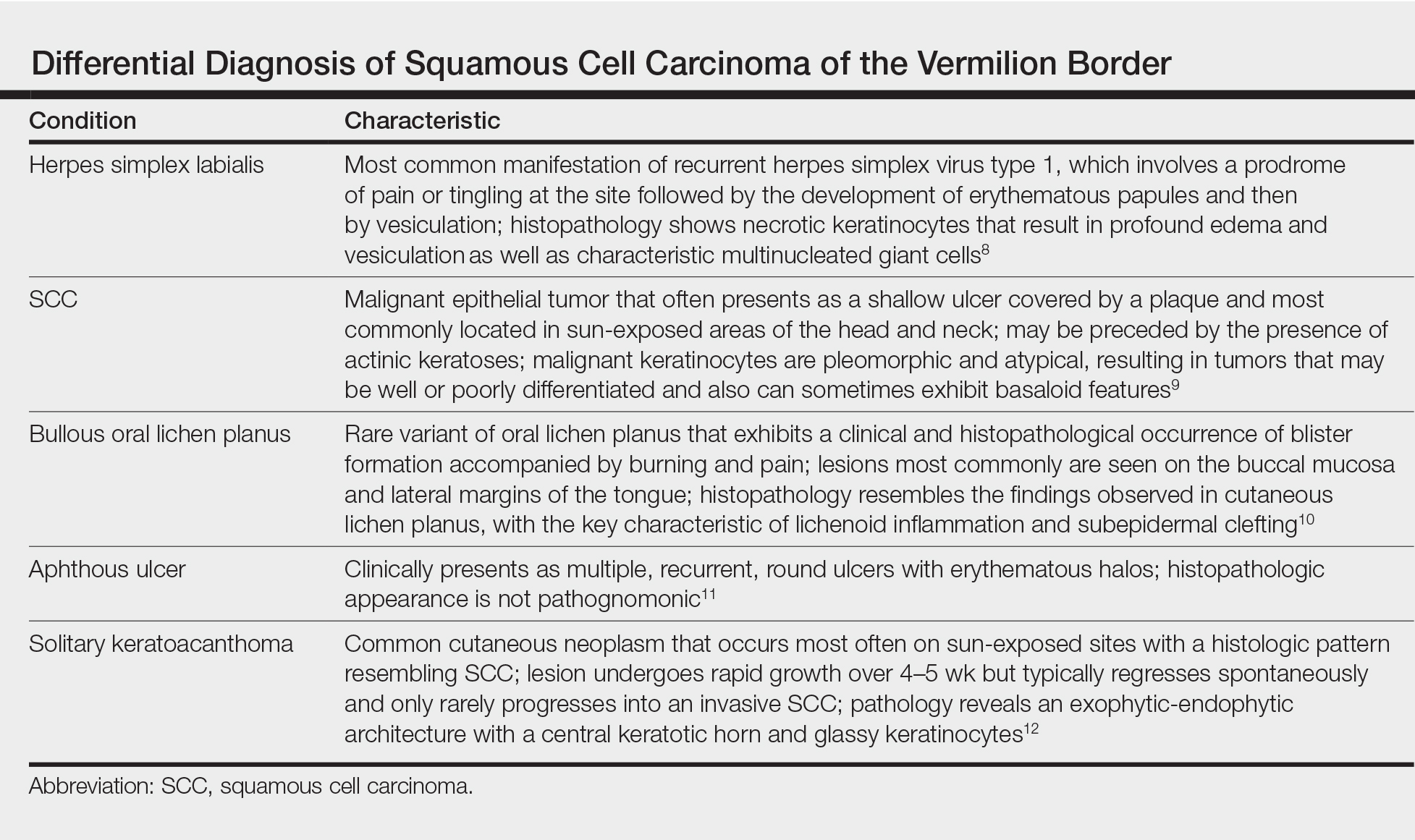
The patient underwent wide excision with repair by mucosal advancement flap. He continues to be regularly seen in the clinic for monitoring of other skin cancers and is doing well. Clinicians encountering any wound or ulcer that does not show signs of healing should be wary of underlying malignancy and be prompted to perform a biopsy.
- Fehrenbach MJ. Extraoral and intraoral clinical assessment. In: Darby ML, Walsh MM, eds. Dental Hygiene: Theory and Practice. 4th ed. St Louis, MO: Elsevier; 2014:214-233.
- Hawrot A, Alam M, Ratner D. Squamous cell carcinoma. Curr Probl Dermatol. 2003;15:91-133.
- Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45:301-308.
- Chhabra N, Chhabra S, Sapra N. Diagnostic modalities for squamous cell carcinoma: an extensive review of literature considering toluidine blue as a useful adjunct. J Oral Maxillofac Surg. 2015;14:188-200.
- Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 2003;9:1499-1505.
- Bricker SL. Oral lichen planus: a review. Semin Dermatol. 1994;13:87-90.
- Cabrijan L, Lipozencic´ J, Batinac T, et al. Differences between keratoacanthoma and squamous cell carcinoma using TGF-alpha. Coll Antropol. 2013;37:147-150.
- Douglas GD, Couch RB. A prospective study of chronic herpes simplex virus infection and recurrent herpes labialis in humans. J Immunol. 1970;104:289-295.
- Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344:976-983.
- van Tuyll van Serooskerken AM, van Marion AM, de Zwart-Storm E, et al. Lichen planus with bullous manifestation on the lip. Int J Dermatol. 2007;46(suppl 3):25-26.
- Messadi DV, Younai F. Apthous ulcers. Dermatol Ther. 2010;23:281-290.
- Ko CJ. Keratoacanthoma: facts and controversies. Clin Dermatol. 2010;28:254-261.
The Diagnosis: Squamous Cell Carcinoma
The initial clinical presentation suggested a diagnosis of herpes simplex labialis. The patient reported no response to topical acyclovir, and because the plaque persisted, a biopsy was performed. Pathology demonstrated squamous cell carcinoma (SCC) that was moderately well differentiated and invasive (Figure).
Approximately 38% of all oral SCCs in the United States occur on the lower lip and typically are solar-related cancers developing within the epidermis.1 Oral lesions initially may be asymptomatic and may not be of concern to the patient; however, it is important to recognize SCC early, as invasive lesions have the potential to metastasize. Some factors that increase the chance for the development of metastases include tumor size larger than 2 cm; location on the ear, lip, or other sites on the head and neck; and history of prior unsuccessful treatment.2 Any solitary ulcer, lump, wound, or lesion that will not heal and persists for more than 3 weeks should be regarded as cancer until proven otherwise. Although few oral SCCs are detected by clinicians at an early stage, diagnostic aids such as vital staining and molecular markers in tissues and saliva may be implemented.3 Toluidine blue is a simple, fast, and inexpensive technique that stains the nuclear material of malignant lesions, but not normal mucosa, and may be a worthwhile diagnostic adjunct to clinical inspection.4
Our patient presented with a lesion that clinically looked herpetic, though he reported no prodromal signs of tingling, burning, or pain before the occurrence of the lesion. Due to the persistence of the lesion and lack of response to treatment, a biopsy was indicated. The differential diagnoses include aphthous ulcers, which may occasionally extend on to the vermilion border of the lip and exhibit nondiagnostic histology.5 Bullous oral lichen planus is the least common variant of oral lichen planus, is unlikely to present as a solitary lesion, and is rarely seen on the lips. Histologically, the lesion demonstrated lichenoid inflammation.6 Solitary keratoacanthoma, though histologically similar to SCC, typically presents as a rapidly growing crateriform nodule without erosion or ulceration.7 The differential diagnoses are summarized in the Table.
The patient underwent wide excision with repair by mucosal advancement flap. He continues to be regularly seen in the clinic for monitoring of other skin cancers and is doing well. Clinicians encountering any wound or ulcer that does not show signs of healing should be wary of underlying malignancy and be prompted to perform a biopsy.
The Diagnosis: Squamous Cell Carcinoma
The initial clinical presentation suggested a diagnosis of herpes simplex labialis. The patient reported no response to topical acyclovir, and because the plaque persisted, a biopsy was performed. Pathology demonstrated squamous cell carcinoma (SCC) that was moderately well differentiated and invasive (Figure).
Approximately 38% of all oral SCCs in the United States occur on the lower lip and typically are solar-related cancers developing within the epidermis.1 Oral lesions initially may be asymptomatic and may not be of concern to the patient; however, it is important to recognize SCC early, as invasive lesions have the potential to metastasize. Some factors that increase the chance for the development of metastases include tumor size larger than 2 cm; location on the ear, lip, or other sites on the head and neck; and history of prior unsuccessful treatment.2 Any solitary ulcer, lump, wound, or lesion that will not heal and persists for more than 3 weeks should be regarded as cancer until proven otherwise. Although few oral SCCs are detected by clinicians at an early stage, diagnostic aids such as vital staining and molecular markers in tissues and saliva may be implemented.3 Toluidine blue is a simple, fast, and inexpensive technique that stains the nuclear material of malignant lesions, but not normal mucosa, and may be a worthwhile diagnostic adjunct to clinical inspection.4
Our patient presented with a lesion that clinically looked herpetic, though he reported no prodromal signs of tingling, burning, or pain before the occurrence of the lesion. Due to the persistence of the lesion and lack of response to treatment, a biopsy was indicated. The differential diagnoses include aphthous ulcers, which may occasionally extend on to the vermilion border of the lip and exhibit nondiagnostic histology.5 Bullous oral lichen planus is the least common variant of oral lichen planus, is unlikely to present as a solitary lesion, and is rarely seen on the lips. Histologically, the lesion demonstrated lichenoid inflammation.6 Solitary keratoacanthoma, though histologically similar to SCC, typically presents as a rapidly growing crateriform nodule without erosion or ulceration.7 The differential diagnoses are summarized in the Table.
The patient underwent wide excision with repair by mucosal advancement flap. He continues to be regularly seen in the clinic for monitoring of other skin cancers and is doing well. Clinicians encountering any wound or ulcer that does not show signs of healing should be wary of underlying malignancy and be prompted to perform a biopsy.
- Fehrenbach MJ. Extraoral and intraoral clinical assessment. In: Darby ML, Walsh MM, eds. Dental Hygiene: Theory and Practice. 4th ed. St Louis, MO: Elsevier; 2014:214-233.
- Hawrot A, Alam M, Ratner D. Squamous cell carcinoma. Curr Probl Dermatol. 2003;15:91-133.
- Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45:301-308.
- Chhabra N, Chhabra S, Sapra N. Diagnostic modalities for squamous cell carcinoma: an extensive review of literature considering toluidine blue as a useful adjunct. J Oral Maxillofac Surg. 2015;14:188-200.
- Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 2003;9:1499-1505.
- Bricker SL. Oral lichen planus: a review. Semin Dermatol. 1994;13:87-90.
- Cabrijan L, Lipozencic´ J, Batinac T, et al. Differences between keratoacanthoma and squamous cell carcinoma using TGF-alpha. Coll Antropol. 2013;37:147-150.
- Douglas GD, Couch RB. A prospective study of chronic herpes simplex virus infection and recurrent herpes labialis in humans. J Immunol. 1970;104:289-295.
- Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344:976-983.
- van Tuyll van Serooskerken AM, van Marion AM, de Zwart-Storm E, et al. Lichen planus with bullous manifestation on the lip. Int J Dermatol. 2007;46(suppl 3):25-26.
- Messadi DV, Younai F. Apthous ulcers. Dermatol Ther. 2010;23:281-290.
- Ko CJ. Keratoacanthoma: facts and controversies. Clin Dermatol. 2010;28:254-261.
- Fehrenbach MJ. Extraoral and intraoral clinical assessment. In: Darby ML, Walsh MM, eds. Dental Hygiene: Theory and Practice. 4th ed. St Louis, MO: Elsevier; 2014:214-233.
- Hawrot A, Alam M, Ratner D. Squamous cell carcinoma. Curr Probl Dermatol. 2003;15:91-133.
- Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45:301-308.
- Chhabra N, Chhabra S, Sapra N. Diagnostic modalities for squamous cell carcinoma: an extensive review of literature considering toluidine blue as a useful adjunct. J Oral Maxillofac Surg. 2015;14:188-200.
- Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 2003;9:1499-1505.
- Bricker SL. Oral lichen planus: a review. Semin Dermatol. 1994;13:87-90.
- Cabrijan L, Lipozencic´ J, Batinac T, et al. Differences between keratoacanthoma and squamous cell carcinoma using TGF-alpha. Coll Antropol. 2013;37:147-150.
- Douglas GD, Couch RB. A prospective study of chronic herpes simplex virus infection and recurrent herpes labialis in humans. J Immunol. 1970;104:289-295.
- Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344:976-983.
- van Tuyll van Serooskerken AM, van Marion AM, de Zwart-Storm E, et al. Lichen planus with bullous manifestation on the lip. Int J Dermatol. 2007;46(suppl 3):25-26.
- Messadi DV, Younai F. Apthous ulcers. Dermatol Ther. 2010;23:281-290.
- Ko CJ. Keratoacanthoma: facts and controversies. Clin Dermatol. 2010;28:254-261.

An 83-year-old man presented with a new-onset 1.2-cm eroded plaque on the vermilion border of the right lower lip that reportedly developed 2 weeks prior and was increasing in size. The plaque was moist and was composed of confluent glistening papules. Medical history was notable for the presence of both basal cell and squamous cell carcinomas.

Monthly fitusiran showed promise in small phase I hemophilia trial
and increased thrombin production, according to the results of a small phase I dose-escalation study.
Compared with baseline, levels of antithrombin dropped by 70%-89%, K. John Pasi, MB, ChB, PhD, of the Royal London Haemophilia Centre and the London School of Medicine and Dentistry and his associates reported at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine. There were no thromboembolic events during the study, and the most common adverse events were mild injection-site reactions, they added.
Patients with hemophilia typically need frequent infusions of clotting factors, creating an urgent need for new therapies. Fitusiran is an investigational RNA interference (RNAi) therapy that targets antithrombin. This multicenter, open-label, phase I study included four healthy volunteers and 25 patients with moderate or severe hemophilia A or B without inhibitors. The healthy participants received a single subcutaneous injection of fitusiran (0.03 mg/kg) or placebo. The hemophilia patients received three injections of fitusiran either once weekly (0.015, 0.045, or 0.075 mg/kg) or once monthly (0.225, 0.45, 0.9, or 1.8 mg/kg, or a fixed dose of 80 mg (N Engl J Med. 2017 July 10. doi: 10.1056/NEJMoa1616569).
The single fitusiran dose and the weekly treatment regimens both produced consistent, sustained drops in plasma antithrombin levels, which supported a longer interval between doses, the researchers said. A monthly dose of 0.225 mg/kg cut antithrombin levels by about 70%, compared with baseline (standard deviation, ±9%), while a monthly dose of 1.8 mg/kg produced about an 89% (standard deviation, ±1%) drop in antithrombin levels. The fixed 80-mg dose consistently lowered antithrombin levels by about 87%, compared with baseline. The decreases in antithrombin varied little during the weeks between doses and were associated with increased thrombin generation, regardless of whether patients had hemophilia A or B, Dr. Pasi and his associates said.
One patient stopped treatment because of severe chest pain, but the investigators ruled out thrombosis as a cause. Fitusiran targets the liver, and 36% of patients developed transient increases in liver aminotransferase levels, they noted. Most of these patients had a history of hepatitis C virus infection. An extension study (NCT02554773) is ongoing to assess longer-term safety and efficacy findings. The investigators also are studying fitusiran in patients with inhibitory alloantibodies.
Alnylam Pharmaceuticals provided funding. Dr. Pasi disclosed research funding, advisory board fees, and travel grants from Alnylam and Genzyme. Four coinvestigators also disclosed receiving support from Alnylam during the conduct of the study.
and increased thrombin production, according to the results of a small phase I dose-escalation study.
Compared with baseline, levels of antithrombin dropped by 70%-89%, K. John Pasi, MB, ChB, PhD, of the Royal London Haemophilia Centre and the London School of Medicine and Dentistry and his associates reported at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine. There were no thromboembolic events during the study, and the most common adverse events were mild injection-site reactions, they added.
Patients with hemophilia typically need frequent infusions of clotting factors, creating an urgent need for new therapies. Fitusiran is an investigational RNA interference (RNAi) therapy that targets antithrombin. This multicenter, open-label, phase I study included four healthy volunteers and 25 patients with moderate or severe hemophilia A or B without inhibitors. The healthy participants received a single subcutaneous injection of fitusiran (0.03 mg/kg) or placebo. The hemophilia patients received three injections of fitusiran either once weekly (0.015, 0.045, or 0.075 mg/kg) or once monthly (0.225, 0.45, 0.9, or 1.8 mg/kg, or a fixed dose of 80 mg (N Engl J Med. 2017 July 10. doi: 10.1056/NEJMoa1616569).
The single fitusiran dose and the weekly treatment regimens both produced consistent, sustained drops in plasma antithrombin levels, which supported a longer interval between doses, the researchers said. A monthly dose of 0.225 mg/kg cut antithrombin levels by about 70%, compared with baseline (standard deviation, ±9%), while a monthly dose of 1.8 mg/kg produced about an 89% (standard deviation, ±1%) drop in antithrombin levels. The fixed 80-mg dose consistently lowered antithrombin levels by about 87%, compared with baseline. The decreases in antithrombin varied little during the weeks between doses and were associated with increased thrombin generation, regardless of whether patients had hemophilia A or B, Dr. Pasi and his associates said.
One patient stopped treatment because of severe chest pain, but the investigators ruled out thrombosis as a cause. Fitusiran targets the liver, and 36% of patients developed transient increases in liver aminotransferase levels, they noted. Most of these patients had a history of hepatitis C virus infection. An extension study (NCT02554773) is ongoing to assess longer-term safety and efficacy findings. The investigators also are studying fitusiran in patients with inhibitory alloantibodies.
Alnylam Pharmaceuticals provided funding. Dr. Pasi disclosed research funding, advisory board fees, and travel grants from Alnylam and Genzyme. Four coinvestigators also disclosed receiving support from Alnylam during the conduct of the study.
and increased thrombin production, according to the results of a small phase I dose-escalation study.
Compared with baseline, levels of antithrombin dropped by 70%-89%, K. John Pasi, MB, ChB, PhD, of the Royal London Haemophilia Centre and the London School of Medicine and Dentistry and his associates reported at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine. There were no thromboembolic events during the study, and the most common adverse events were mild injection-site reactions, they added.
Patients with hemophilia typically need frequent infusions of clotting factors, creating an urgent need for new therapies. Fitusiran is an investigational RNA interference (RNAi) therapy that targets antithrombin. This multicenter, open-label, phase I study included four healthy volunteers and 25 patients with moderate or severe hemophilia A or B without inhibitors. The healthy participants received a single subcutaneous injection of fitusiran (0.03 mg/kg) or placebo. The hemophilia patients received three injections of fitusiran either once weekly (0.015, 0.045, or 0.075 mg/kg) or once monthly (0.225, 0.45, 0.9, or 1.8 mg/kg, or a fixed dose of 80 mg (N Engl J Med. 2017 July 10. doi: 10.1056/NEJMoa1616569).
The single fitusiran dose and the weekly treatment regimens both produced consistent, sustained drops in plasma antithrombin levels, which supported a longer interval between doses, the researchers said. A monthly dose of 0.225 mg/kg cut antithrombin levels by about 70%, compared with baseline (standard deviation, ±9%), while a monthly dose of 1.8 mg/kg produced about an 89% (standard deviation, ±1%) drop in antithrombin levels. The fixed 80-mg dose consistently lowered antithrombin levels by about 87%, compared with baseline. The decreases in antithrombin varied little during the weeks between doses and were associated with increased thrombin generation, regardless of whether patients had hemophilia A or B, Dr. Pasi and his associates said.
One patient stopped treatment because of severe chest pain, but the investigators ruled out thrombosis as a cause. Fitusiran targets the liver, and 36% of patients developed transient increases in liver aminotransferase levels, they noted. Most of these patients had a history of hepatitis C virus infection. An extension study (NCT02554773) is ongoing to assess longer-term safety and efficacy findings. The investigators also are studying fitusiran in patients with inhibitory alloantibodies.
Alnylam Pharmaceuticals provided funding. Dr. Pasi disclosed research funding, advisory board fees, and travel grants from Alnylam and Genzyme. Four coinvestigators also disclosed receiving support from Alnylam during the conduct of the study.
FROM THE 2017 ISTH CONGRESS
Key clinical point: Once-monthly subcutaneous treatment with fitusiran led to dose-dependent lowering of antithrombin levels and increased thrombin production among patients with hemophilia A or B without inhibitors.
Major finding: Compared with baseline, levels of antithrombin dropped by 70%-89%. There were no episodes of thrombosis, and the most common adverse events were injection-site reactions.
Data source: A phase I dose-escalation study.
Disclosures: Alnylam Pharmaceuticals provided funding. Dr. Pasi disclosed research funding, advisory board fees, and travel grants from Alnylam and Genzyme. Four coinvestigators also disclosed receiving support from Alnylam during the conduct of the study.
Obesity medicine: How to incorporate it into your practice
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Resources
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Resources
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Resources

Prophylactic emicizumab cut bleeds by 87% in hemophilia A with inhibitors
Once-weekly prophylactic therapy with emicizumab (ACE910) was associated an 87% lower rate of treated bleeding than no prophylaxis among patients with hemophilia A with inhibitors in the open-label, phase III HAVEN 1 trial.
After a median 24 weeks of treatment (range, 3-48 weeks), the 35 patients who were randomly assigned to prophylactic emicizumab (3.0 mg per kg for 4 weeks, followed by 1.5 mg per kg) had an annualized bleeding rate of 2.9 events, compared with an annualized rate of 23.3 events among the 18 patients who received no prophylaxis. The difference was statistically significant, reported Johannes Oldenburg, MD, PhD, and his associates at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jul 10. doi: 10.1056/NEJMoa1703068).
In addition, 63% of patients who received prophylactic emicizumab had no bleeding events, compared with only 6% of the comparison group, said Dr. Oldenburg of Universitaetsklinikum Bonn, Germany. Emicizumab also was associated with a 79% lower rate of treated bleeds, compared with the historic rate among 24 patients who previously had been on prophylactic bypassing agents (P less than .001). No patient developed detectable antidrug antibodies.
The most common adverse events were injection site reactions (15% of patients), followed by headache, upper respiratory tract infection, arthralgia, and fatigue. Four patients developed thrombotic microangiopathy or cavernous sinus thrombosis and skin necrosis, all of whom had experienced breakthrough bleeding for which they had received multiple infusions of activated prothrombin complex concentrate at doses averaging more than 100 U per kg per day.
Patients with severe hemophilia A typically require prophylactic factor VIII infusions two to three times a week, but 30% develop neutralizing antibodies against factor VIII (inhibitors), which increases care burden, costs, and complication rates.
Emicizumab is a recombinant humanized bispecific monoclonal antibody that restores the function of missing active factor VIII by bridging activated factor IX and factor X, the investigators noted. A phase I study linked once-weekly emicizumab prophylaxis to markedly lower bleeding rates without dose-limiting toxicities (N Engl J Med 2016;374:2044-53). Subsequently, the phase III HAVEN 1 study (NCT02622321) compared once-weekly subcutaneous prophylactic emicizumab with on-demand (episodic) and prophylactic use of bypassing agents (BPAs) in 109 adults and adolescents (12 years and older) with hemophilia A with inhibitors. The primary endpoint was the difference in rates of treated bleeds between the groups. Patients had a median age of 28 years, all were male, and most had severe hemophilia at baseline. They typically had more than nine bleeding events in the 6 months before enrollment, with bleeding in more than one target joint and factor VIII titers of 180 Bethesda units per mL.
HAVEN 1 was funded by F. Hoffmann-La Roche and Chugai Pharmaceutical. Dr. Oldenburg and 13 coinvestigators disclosed ties to Chugai, Roche, and other pharmaceutical companies. The remaining coinvestigator had no disclosures.
The results of this phase III trial are of great importance to patients with for hemophilia A, offering “an elegant new solution for treatment.” Although it is not clear how best to treat the infrequent events of breakthrough bleeding when administering emicizumab, it is evident that repeated high doses of activated prothrombin complex concentrate should be avoided. Also, how to integrate emicizumab prophylaxis with current schedules for the induction of immune tolerance to factor VIII remains to be seen.
Meanwhile, weekly subcutaneous emicizumab prophylaxis offer great reductions in bleeding rates and improve quality of life “for this very challenging patient group.” Additional studies already are underway to ascertain the benefit of emicizumab prophylaxis in children with hemophilia with inhibitors, and a study for patients with hemophilia A without inhibitors is planned.
“These are extraordinary times for innovation in hemophilia therapy, and the introduction of emicizumab represents a major contribution toward achieving an enhanced standard of care for this lifelong bleeding disorder.”
David Lillicrap, MD, is with the department of pathology and molecular medicine at Queen’s University, Kingston, Ontario. He reported having no relevant conflicts of interest. These comments are from his accompanying editorial (N Engl J Med. 2017 June 10. doi: 10.1056/NEJMe1707802).
The results of this phase III trial are of great importance to patients with for hemophilia A, offering “an elegant new solution for treatment.” Although it is not clear how best to treat the infrequent events of breakthrough bleeding when administering emicizumab, it is evident that repeated high doses of activated prothrombin complex concentrate should be avoided. Also, how to integrate emicizumab prophylaxis with current schedules for the induction of immune tolerance to factor VIII remains to be seen.
Meanwhile, weekly subcutaneous emicizumab prophylaxis offer great reductions in bleeding rates and improve quality of life “for this very challenging patient group.” Additional studies already are underway to ascertain the benefit of emicizumab prophylaxis in children with hemophilia with inhibitors, and a study for patients with hemophilia A without inhibitors is planned.
“These are extraordinary times for innovation in hemophilia therapy, and the introduction of emicizumab represents a major contribution toward achieving an enhanced standard of care for this lifelong bleeding disorder.”
David Lillicrap, MD, is with the department of pathology and molecular medicine at Queen’s University, Kingston, Ontario. He reported having no relevant conflicts of interest. These comments are from his accompanying editorial (N Engl J Med. 2017 June 10. doi: 10.1056/NEJMe1707802).
The results of this phase III trial are of great importance to patients with for hemophilia A, offering “an elegant new solution for treatment.” Although it is not clear how best to treat the infrequent events of breakthrough bleeding when administering emicizumab, it is evident that repeated high doses of activated prothrombin complex concentrate should be avoided. Also, how to integrate emicizumab prophylaxis with current schedules for the induction of immune tolerance to factor VIII remains to be seen.
Meanwhile, weekly subcutaneous emicizumab prophylaxis offer great reductions in bleeding rates and improve quality of life “for this very challenging patient group.” Additional studies already are underway to ascertain the benefit of emicizumab prophylaxis in children with hemophilia with inhibitors, and a study for patients with hemophilia A without inhibitors is planned.
“These are extraordinary times for innovation in hemophilia therapy, and the introduction of emicizumab represents a major contribution toward achieving an enhanced standard of care for this lifelong bleeding disorder.”
David Lillicrap, MD, is with the department of pathology and molecular medicine at Queen’s University, Kingston, Ontario. He reported having no relevant conflicts of interest. These comments are from his accompanying editorial (N Engl J Med. 2017 June 10. doi: 10.1056/NEJMe1707802).
Once-weekly prophylactic therapy with emicizumab (ACE910) was associated an 87% lower rate of treated bleeding than no prophylaxis among patients with hemophilia A with inhibitors in the open-label, phase III HAVEN 1 trial.
After a median 24 weeks of treatment (range, 3-48 weeks), the 35 patients who were randomly assigned to prophylactic emicizumab (3.0 mg per kg for 4 weeks, followed by 1.5 mg per kg) had an annualized bleeding rate of 2.9 events, compared with an annualized rate of 23.3 events among the 18 patients who received no prophylaxis. The difference was statistically significant, reported Johannes Oldenburg, MD, PhD, and his associates at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jul 10. doi: 10.1056/NEJMoa1703068).
In addition, 63% of patients who received prophylactic emicizumab had no bleeding events, compared with only 6% of the comparison group, said Dr. Oldenburg of Universitaetsklinikum Bonn, Germany. Emicizumab also was associated with a 79% lower rate of treated bleeds, compared with the historic rate among 24 patients who previously had been on prophylactic bypassing agents (P less than .001). No patient developed detectable antidrug antibodies.
The most common adverse events were injection site reactions (15% of patients), followed by headache, upper respiratory tract infection, arthralgia, and fatigue. Four patients developed thrombotic microangiopathy or cavernous sinus thrombosis and skin necrosis, all of whom had experienced breakthrough bleeding for which they had received multiple infusions of activated prothrombin complex concentrate at doses averaging more than 100 U per kg per day.
Patients with severe hemophilia A typically require prophylactic factor VIII infusions two to three times a week, but 30% develop neutralizing antibodies against factor VIII (inhibitors), which increases care burden, costs, and complication rates.
Emicizumab is a recombinant humanized bispecific monoclonal antibody that restores the function of missing active factor VIII by bridging activated factor IX and factor X, the investigators noted. A phase I study linked once-weekly emicizumab prophylaxis to markedly lower bleeding rates without dose-limiting toxicities (N Engl J Med 2016;374:2044-53). Subsequently, the phase III HAVEN 1 study (NCT02622321) compared once-weekly subcutaneous prophylactic emicizumab with on-demand (episodic) and prophylactic use of bypassing agents (BPAs) in 109 adults and adolescents (12 years and older) with hemophilia A with inhibitors. The primary endpoint was the difference in rates of treated bleeds between the groups. Patients had a median age of 28 years, all were male, and most had severe hemophilia at baseline. They typically had more than nine bleeding events in the 6 months before enrollment, with bleeding in more than one target joint and factor VIII titers of 180 Bethesda units per mL.
HAVEN 1 was funded by F. Hoffmann-La Roche and Chugai Pharmaceutical. Dr. Oldenburg and 13 coinvestigators disclosed ties to Chugai, Roche, and other pharmaceutical companies. The remaining coinvestigator had no disclosures.
Once-weekly prophylactic therapy with emicizumab (ACE910) was associated an 87% lower rate of treated bleeding than no prophylaxis among patients with hemophilia A with inhibitors in the open-label, phase III HAVEN 1 trial.
After a median 24 weeks of treatment (range, 3-48 weeks), the 35 patients who were randomly assigned to prophylactic emicizumab (3.0 mg per kg for 4 weeks, followed by 1.5 mg per kg) had an annualized bleeding rate of 2.9 events, compared with an annualized rate of 23.3 events among the 18 patients who received no prophylaxis. The difference was statistically significant, reported Johannes Oldenburg, MD, PhD, and his associates at the International Society on Thrombosis and Haemostasis congress and simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jul 10. doi: 10.1056/NEJMoa1703068).
In addition, 63% of patients who received prophylactic emicizumab had no bleeding events, compared with only 6% of the comparison group, said Dr. Oldenburg of Universitaetsklinikum Bonn, Germany. Emicizumab also was associated with a 79% lower rate of treated bleeds, compared with the historic rate among 24 patients who previously had been on prophylactic bypassing agents (P less than .001). No patient developed detectable antidrug antibodies.
The most common adverse events were injection site reactions (15% of patients), followed by headache, upper respiratory tract infection, arthralgia, and fatigue. Four patients developed thrombotic microangiopathy or cavernous sinus thrombosis and skin necrosis, all of whom had experienced breakthrough bleeding for which they had received multiple infusions of activated prothrombin complex concentrate at doses averaging more than 100 U per kg per day.
Patients with severe hemophilia A typically require prophylactic factor VIII infusions two to three times a week, but 30% develop neutralizing antibodies against factor VIII (inhibitors), which increases care burden, costs, and complication rates.
Emicizumab is a recombinant humanized bispecific monoclonal antibody that restores the function of missing active factor VIII by bridging activated factor IX and factor X, the investigators noted. A phase I study linked once-weekly emicizumab prophylaxis to markedly lower bleeding rates without dose-limiting toxicities (N Engl J Med 2016;374:2044-53). Subsequently, the phase III HAVEN 1 study (NCT02622321) compared once-weekly subcutaneous prophylactic emicizumab with on-demand (episodic) and prophylactic use of bypassing agents (BPAs) in 109 adults and adolescents (12 years and older) with hemophilia A with inhibitors. The primary endpoint was the difference in rates of treated bleeds between the groups. Patients had a median age of 28 years, all were male, and most had severe hemophilia at baseline. They typically had more than nine bleeding events in the 6 months before enrollment, with bleeding in more than one target joint and factor VIII titers of 180 Bethesda units per mL.
HAVEN 1 was funded by F. Hoffmann-La Roche and Chugai Pharmaceutical. Dr. Oldenburg and 13 coinvestigators disclosed ties to Chugai, Roche, and other pharmaceutical companies. The remaining coinvestigator had no disclosures.
From 2017 ISTH CONGRESS
Key clinical point: .
Major finding: After a median 24 weeks of treatment, the intervention group averaged 2.9 bleeds per year vs. 23.3 events in the control group.
Data source: A phase III randomized multicenter open-label trial of 109 male adolescents and adults with hemophilia A and factor VIII inhibitors.
Disclosures: HAVEN 1 was funded by F. Hoffmann-La Roche and Chugai Pharmaceutical. Dr. Oldenburg and 13 coinvestigators disclosed ties to Chugai, Roche, and other pharmaceutical companies. The remaining coinvestigator had no disclosures.
Antibody could reduce bone fractures in MM

Preclinical research suggests a targeted therapy may be able to rebuild and strengthen bone in patients with multiple myeloma (MM).
Researchers tested an antibody targeting the protein sclerostin, an important regulator of bone formation, in mouse models of MM.
The antibody prevented bone loss and even increased bone volume in the mice.
The treatment also made bones more resistant to fracture and worked synergistically with zoledronic acid.
Michelle McDonald, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia, and her colleagues reported these findings in Blood.
“Multiple myeloma is a cancer that grows in bone, and, in most patients, it is associated with widespread bone loss and recurrent bone fractures, which can be extremely painful and debilitating,” Dr McDonald said.
“The current treatment for myeloma-associated bone disease with bisphosphonate drugs prevents further bone loss, but it doesn’t fix damaged bones, so patients continue to fracture. We wanted to re-stimulate bone formation and increase bone strength and resistance to fracture.”
So the researchers tested an antibody that targets and neutralizes sclerostin. In clinical studies of osteoporosis, such antibodies have been shown to increase bone mass and reduce fracture incidence.
In the mouse models of MM, the antibody prevented further bone loss and even doubled bone volume in some of the mice.
“When we looked at the bones before and after treatment, the difference was remarkable,” Dr McDonald said. “We saw less lesions or ‘holes’ in the bones after anti-sclerostin treatment. These lesions are the primary cause of bone pain, so this is an extremely important result.”
The treatment also made the bones substantially stronger, with more than double the resistance to fracture observed in many of the tests.
The researchers then combined the antibody with the bisphosphonate zoledronic acid and observed positive results.
“Bisphosphonates work by preventing bone breakdown, so we combined zoledronic acid with the new anti-sclerostin antibody that rebuilds bone,” Dr McDonald said. “Together, the impact on bone thickness, strength, and resistance to fracture was greater than either treatment alone.”
The researchers said these findings suggest a potential new strategy for reducing fractures in patients with MM.
“[M]yelomas, like other cancers, vary from individual to individual and can therefore be difficult to target,” said study author Peter I. Croucher, PhD, of the Garvan Institute of Medical Research.
“By targeting sclerostin, we are blocking a protein that is active in every person’s bones and not something unique to a person’s cancer. Therefore, in the future, when we test this antibody in humans, we are hopeful to see a response in most, if not all, patients.”
“We are now looking towards clinical trials for this antibody and, in the future, development of this type of therapy for the clinical treatment of multiple myeloma. This therapeutic approach has the potential to transform the prognosis for myeloma patients, enhancing quality of life, and ultimately reducing mortality. It also has clinical implications for the treatment of other cancers that develop in the skeleton.” ![]()
Preclinical research suggests a targeted therapy may be able to rebuild and strengthen bone in patients with multiple myeloma (MM).
Researchers tested an antibody targeting the protein sclerostin, an important regulator of bone formation, in mouse models of MM.
The antibody prevented bone loss and even increased bone volume in the mice.
The treatment also made bones more resistant to fracture and worked synergistically with zoledronic acid.
Michelle McDonald, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia, and her colleagues reported these findings in Blood.
“Multiple myeloma is a cancer that grows in bone, and, in most patients, it is associated with widespread bone loss and recurrent bone fractures, which can be extremely painful and debilitating,” Dr McDonald said.
“The current treatment for myeloma-associated bone disease with bisphosphonate drugs prevents further bone loss, but it doesn’t fix damaged bones, so patients continue to fracture. We wanted to re-stimulate bone formation and increase bone strength and resistance to fracture.”
So the researchers tested an antibody that targets and neutralizes sclerostin. In clinical studies of osteoporosis, such antibodies have been shown to increase bone mass and reduce fracture incidence.
In the mouse models of MM, the antibody prevented further bone loss and even doubled bone volume in some of the mice.
“When we looked at the bones before and after treatment, the difference was remarkable,” Dr McDonald said. “We saw less lesions or ‘holes’ in the bones after anti-sclerostin treatment. These lesions are the primary cause of bone pain, so this is an extremely important result.”
The treatment also made the bones substantially stronger, with more than double the resistance to fracture observed in many of the tests.
The researchers then combined the antibody with the bisphosphonate zoledronic acid and observed positive results.
“Bisphosphonates work by preventing bone breakdown, so we combined zoledronic acid with the new anti-sclerostin antibody that rebuilds bone,” Dr McDonald said. “Together, the impact on bone thickness, strength, and resistance to fracture was greater than either treatment alone.”
The researchers said these findings suggest a potential new strategy for reducing fractures in patients with MM.
“[M]yelomas, like other cancers, vary from individual to individual and can therefore be difficult to target,” said study author Peter I. Croucher, PhD, of the Garvan Institute of Medical Research.
“By targeting sclerostin, we are blocking a protein that is active in every person’s bones and not something unique to a person’s cancer. Therefore, in the future, when we test this antibody in humans, we are hopeful to see a response in most, if not all, patients.”
“We are now looking towards clinical trials for this antibody and, in the future, development of this type of therapy for the clinical treatment of multiple myeloma. This therapeutic approach has the potential to transform the prognosis for myeloma patients, enhancing quality of life, and ultimately reducing mortality. It also has clinical implications for the treatment of other cancers that develop in the skeleton.” ![]()
Preclinical research suggests a targeted therapy may be able to rebuild and strengthen bone in patients with multiple myeloma (MM).
Researchers tested an antibody targeting the protein sclerostin, an important regulator of bone formation, in mouse models of MM.
The antibody prevented bone loss and even increased bone volume in the mice.
The treatment also made bones more resistant to fracture and worked synergistically with zoledronic acid.
Michelle McDonald, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia, and her colleagues reported these findings in Blood.
“Multiple myeloma is a cancer that grows in bone, and, in most patients, it is associated with widespread bone loss and recurrent bone fractures, which can be extremely painful and debilitating,” Dr McDonald said.
“The current treatment for myeloma-associated bone disease with bisphosphonate drugs prevents further bone loss, but it doesn’t fix damaged bones, so patients continue to fracture. We wanted to re-stimulate bone formation and increase bone strength and resistance to fracture.”
So the researchers tested an antibody that targets and neutralizes sclerostin. In clinical studies of osteoporosis, such antibodies have been shown to increase bone mass and reduce fracture incidence.
In the mouse models of MM, the antibody prevented further bone loss and even doubled bone volume in some of the mice.
“When we looked at the bones before and after treatment, the difference was remarkable,” Dr McDonald said. “We saw less lesions or ‘holes’ in the bones after anti-sclerostin treatment. These lesions are the primary cause of bone pain, so this is an extremely important result.”
The treatment also made the bones substantially stronger, with more than double the resistance to fracture observed in many of the tests.
The researchers then combined the antibody with the bisphosphonate zoledronic acid and observed positive results.
“Bisphosphonates work by preventing bone breakdown, so we combined zoledronic acid with the new anti-sclerostin antibody that rebuilds bone,” Dr McDonald said. “Together, the impact on bone thickness, strength, and resistance to fracture was greater than either treatment alone.”
The researchers said these findings suggest a potential new strategy for reducing fractures in patients with MM.
“[M]yelomas, like other cancers, vary from individual to individual and can therefore be difficult to target,” said study author Peter I. Croucher, PhD, of the Garvan Institute of Medical Research.
“By targeting sclerostin, we are blocking a protein that is active in every person’s bones and not something unique to a person’s cancer. Therefore, in the future, when we test this antibody in humans, we are hopeful to see a response in most, if not all, patients.”
“We are now looking towards clinical trials for this antibody and, in the future, development of this type of therapy for the clinical treatment of multiple myeloma. This therapeutic approach has the potential to transform the prognosis for myeloma patients, enhancing quality of life, and ultimately reducing mortality. It also has clinical implications for the treatment of other cancers that develop in the skeleton.” ![]()