User login
Emerging therapies in Duchenne and facioscapulohumeral muscular dystrophy
“There have been so many breakthroughs recently on the side of genetically targeted treatment [for muscular dystrophy] that supports muscle better,” said John F. Brandsema, MD, a child neurologist and section head at Children’s Hospital of Philadelphia, in an interview with Neurology Reviews 2023 Rare Neurological Disease Special Report. “We’re starting to see clinical response to some things that have been in trials – after decades of banging our heads on the wall trying new therapies, only to see them fail. I think it’s about reframing Duchenne muscular dystrophy [DMD] and facioscapulohumeral muscular dystrophy [FSHD] as treatable by target therapy because previously, they were treated with supportive care.”
DMD: Current and emerging therapies

DMD is caused by a mutation in the dystrophin gene on the X chromosome that inhibits production of dystrophin, a protein that shields muscles from injury during contraction. Dystrophin deficiency prevents muscle recovery, resulting in muscle-cell death and, ultimately, loss of function due to muscle degeneration.
FDA-approved exon-skipping therapies. Treatment modalities for what has historically been an incurable, lifespan-shortening disease involved supportive care that addresses symptoms, not the underlying cause. Consequently, many patients with DMD live only into their 20s and 30s. The tide began to turn in 2016, however, when the U.S. Food and Drug Administration granted accelerated approval for eteplirsen, an exon 51–skipping treatment that was the first RNA-based therapy for DMD to target the underlying cause. Additional exon-skipping therapies followed, including casimersen, which skips exon 45, and golodirsen and viltolarsen, which skip exon 53.
AOC 1044: Novel exon-skipping. In April 2023, the FDA granted orphan-drug designation to the experimental drug antibody oligonucleotide conjugate (AOC) 1044 that skips exon 44. A small interfering RNA (siRNA), AOC 1044 works in patients who have a mutation amenable to exon 44 skipping (a disease type known as DMD44) by delivering phosphorodiamidate morpholino to skeletal muscle and heart tissue that skips exon 44. The process allows for dystrophin production, thereby preventing degradation of muscle tissue.
The orphan drug status of AOC 1044 made it available to the population of patients enrolled in the EXPLORE44 Phase 1/2 trial. However, studies demonstrating effectiveness of the drug – with the hope of, ultimately, providing widespread access to AOC 1044 – are still underway. In one of those studies, investigators expect to enroll approximately 40 healthy volunteers and 24 DMD44 patients 7-27 years of age.3 The study will evaluate the effects of exon skipping and dystrophin protein levels in participants who have DMD44.
Delandistrogene moxeparvovec. Oct. 27, 2021, marked the inception of the phase 3 Multinational, Randomized, Double-Blind, Placebo-Controlled Systemic Gene Delivery Study to Evaluate the Safety and Efficacy of SRP-9001 in Subjects With Duchenne Muscular Dystrophy (EMBARK). The trial is evaluating the safety and efficacy of the gene-therapy agent delandistrogene moxeparvovec in ambulatory boys who were 4 to less than 8 years of age at randomization. The 126 boys enrolled in the trial met the criteria of (1) a diagnosis of DMD confirmed by documented clinical findings and previous genetic testing and (2) a pathogenic frameshift mutation stop codon located between exons 18 and 79 (inclusive), except for a mutation fully contained within exon 45.
Additional inclusion criteria were (1) the ability to cooperate with motor-assessment testing and (2) receiving a steady daily dose of oral corticosteroid for 12 weeks or longer prior to screening, and (3) the expectation of maintaining the study dosage throughout screening. Boys who had previously received gene therapy, investigational medication, or any treatment that could have amplified dystrophin expression within the time limit specified by the protocol were ineligible to participate. Boys were excluded from the study if they presented with any other illness, medical condition, or need for chronic drug treatment.
Exon-skipping therapies in trials. Various biotech and pharmaceutical companies have initiated clinical trials to explore the potential of additional exon-skipping therapies for the DMD population:
ENTR-601-44 is another exon 44–skipping therapy in the pipeline.
On Aug. 22, 2023, the FDA approved delandistrogene moxeparvovec-rokl, a recombinant gene therapy utilizing an adenovirus vector. The product is indicated for ambulatory patients with DMD 4-5 years of age who have a confirmed mutation of the dystrophin gene.
Dyne Therapeutics is actively recruiting participants to investigate Dyne 251, its exon 51–skipping therapy.
Trials are in the works by BioMarin Pharmaceutical for its next-generation peptide-conjugated phosphorodiamidate morpholino oligomers (PPMO) for skipping exon 51.
Despite the prospects of such therapy, therapeutic targeting of exon 44 addresses only patients with DMD44, who account for approximately 10% of the DMD population. Disease involving the most prevalent site of a dystrophin gene mutation, exon 51, affects 13% of the DMD population. This leaves the majority of patients with DMD without gene therapy. Yet Dr. Brandsema is optimistic nevertheless.
“We were just failing over and over again with DMD treatment, but there is some hope now,” Dr. Brandsema said. “Also, FSHD is right on the cusp of having new therapies approaching.”
FSHD: Emerging therapies
The third more common type of muscular dystrophy is not a life-threatening condition. FSHD affects approximately 4 of every 100,000 people.1 An autosomal-dominant condition, FSHD is ultimately caused by inappropriate expression of the DUX4 protein product – a consequence of a complex genetic activity involving DUX4, its chromosomal locus, and the number of repeats of a microsatellite called D4Z4.4 The disease usually starts in proximal regions of the face (that is, surrounding the eyes and mouth), before spreading to muscular groups of the limbs – most prominently, muscles of the scapulae and humeri. Symptoms usually appear in these places initially, but the condition can affect any part of the body. Fifty percent of FSHD patients experience loss of high-frequency hearing and present with retinovasculopathy. Like DMD, FSHD varies in severity, with some forms presenting at birth.
AOC 1020-CS1 is an example of a new FSHD treatment under investigation. The phase 1/2 FORTITUDE trial is a randomized, double-blind, placebo-controlled study exploring the safety, tolerability, pharmacokinetics, pharmacodynamics, and potential efficacy of single- and multiple-dose AOC 1020-CS1 therapy in FSHD.5 The trial began in April 2023; estimated completion date is September 2025.
As with many rare diseases, however, following patients and capturing data that fully narrate their story remains challenging in both DMD and FSHD. Although clinical trials undoubtedly offer hope of expanding treatment options and additional insights into disease-state management, the often insidious, complex nature of some rare diseases, such as DMD and FSHD, presents some limitations.
“Patients are hard to measure,” Dr. Brandsema explained, “because they’re so variable at baseline in history and progress in a different [slower] way than timelines are set up in our system to study drugs.”
Neonatal screening and early diagnosis: Imperative for improving outcomes
Neonatal screening helps with early detection and treatment. Prompt diagnosis does not necessarily prolong a DMD patient’s life, but it can enhance their quality of life.

DNA diagnostics. A critical component of the path to treatment is DNA diagnostics. According to Barry J. Byrne, MD, PhD, chief medical advisor of the Muscular Dystrophy Association, the Human Genome Project conducted by the National Institutes of Health helped make DNA tests affordable; such tests run about $800 today. However, given continuous advancements in sequencing, Dr. Byrne said that whole-exome sequencing for $100 is within reach.
In terms of accessibility, some nations – Canada is an example – include testing as part of national health care services. In the United States, coverage for testing varies by health insurance plan. In addition, some plans have favored rapid diagnostic testing, and the overall cost is often individualized to the patient.
Early diagnosis and supportive care. Early diagnosis can certainly help improve DMD patients’ quality of life; supportive care provides some benefit. Dr. Byrne stressed the importance of managing extraskeletal clinical manifestations in this patient population. A critical area is initiating cardiovascular treatment immediately following diagnosis, even if the patient does not exhibit cardiovascular symptoms.
“Cardiac manifestations are actually the cause of mortality in DMD, and most boys with DMD should begin cardiovascular treatment shortly after diagnosis,” Dr. Byrne told Neurology Reviews 2023 Rare Neurological Disease Special Report. “The message to neurologists is that these patients can benefit from early cardiovascular treatment because we can prevent the complications of DMD-related heart failure until much later in life.”
Historically, clinicians used echocardiography as the mainstay tool to assess cardiovascular function; however, more and more clinicians are turning to magnetic resonance imaging for such investigation. Dr. Byrne, a cardiologist, explained that magnetic resonance imaging identifies cardiovascular dysfunction at earlier stages than echocardiography can. In addition, although DMD patients frequently experience fatigue, Dr. Byrne cautions neurologists that fatigue is usually related to muscle weakness, not necessarily heart failure.
DMD therapies carry a hefty price
Right now, the projected price range of AOC 1044 is $3.2 million to $3.4 million. Akin to the case with onasemnogene abeparvovec-xioi (Zolgensma) for spinal muscular atrophy, the world’s first gene therapy and first seven-figure drug, the manufacturer of AOC 1044 based pricing on the anticipated cost of treating a DMD44 patient throughout the lifespan, according to Dr. Byrne.
Delandistrogene moxeparvovec might come with an even higher price tag. A cost-effectiveness analysis study priced the therapy at $5 million. In a presentation to investors, the manufacturer projected the price in the range of $5 million to $13 million.6,7
‘It takes a village’: Comprehensive care requires a multidisciplinary team
Dr. Brandsema and Dr. Byrne agree: Optimizing outcomes requires ongoing coordinated and collaborative efforts of an interdisciplinary team of health care providers for the duration of DMD and FSHD patients’ lifespan.
A neurologist by training, Dr. Brandsema recognizes the importance of interdisciplinary collaboration in caring for patients with DMD, given the multiorgan manifestations of the disease.
“We have some hope with DMD, and FSHD is right on the cusp of having new therapies approaching ... It is important to recognize that interdisciplinary follow-up and optimized standard of care are important after dosing.”
“I think many patients living with neurological disorders have multiple providers they rely on for care,” Dr. Byrne said, “but cardiovascular and pulmonary care are important because both are affected in the case of DMD – not so much in FSHD.”
Ultimately, advancements in therapy and care give patients living with these disorders, and their caregivers, a renewed sense of hope – hope that their life will be improved by breakthrough therapies that have been approved or will arrive soon.
Dr. Brandsema discloses he is a consultant for Alexion, Audentes, AveXis/Novartis, Biogen, Cytokinetics, Dyne, Edgewise, Fibrogen, Genentech/Roche, Janssen, Marathon, Momenta, NS Pharma, PTC Therapeutics, Sarepta, Scholar Rock, Takeda, and WaVe. He is a speaker for AveXis and Biogen, a medical advisory council member for Cure SMA, and a site investigator for clinical trials with Alexion, Astellas, AveXis/Novartis, Biogen, Catabasis, CSL Behring, Cytokinetics, Fibrogen, Genentech/Roche, Ionis, Lilly, Janssen, Pfizer, PTC Therapeutics, Sarepta, Scholar Rock, Summit, and WaVe. Dr. Byrne has no relevant financial disclosures.
References
1. Centers for Disease Control and Prevention. What is muscular dystrophy? Updated Nov. 21, 2022. Accessed Sept. 3, 2023. https://www.cdc.gov/ncbddd/musculardystrophy/facts.html.
2. FDA approves first gene therapy for treatment of certain patients with Duchenne muscular dystrophy. U.S. Food and Drug Administration. Press release. June 22, 2023. Accessed Sept. 3, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-gene-therapy-treatment-certain-patients-duchenne-muscular-dystrophy.
3. Study of AOC 1044 in healthy adult volunteers and participants with Duchenne muscular dystrophy (DMD) mutations amenable to exon 44 skipping (EXPLORE44). ClinicalTrials.gov Identifier: NCT05670730. Updated April 4, 2023. Accessed Sep. 3, 2023. https://www.clinicaltrials.gov/study/NCT05670730?cond=DMD&intr=AOC%201044&rank=1.
4. Statland JM, Tawil R. Facioscapulohumeral muscular dystrophy. Continuum (Minneap. Minn). 2016;22(6, Muscle and Neuromuscular Junction Disorders):1916-31. doi: 10.1212/CON.0000000000000399.
5. Phase 1/2 study of AOC 1020 in adults with facioscapulohumeral muscular dystrophy (FSHD) (FORTITUDE). ClinicalTrials.gov Identifier: NCT05747924. Updated Aug. 9, 2023. Accessed Sept. 3, 2023. https://clinicaltrials.gov/study/NCT05747924?term=fORTITUDE&cond=Facioscapulohumeral%20Muscular%20Dystrophy&rank=1.
6. Klimchak AC, Sedita LE, Rodino-Klapac LR, et al. Assessing the value of delandistrogene moxeparvovec (SRP-9001) gene therapy in patients with Duchenne muscular dystrophy in the United States. J Mark Access Health Policy. 2023;11(1):2216518. doi: 10.1080/20016689.2023.2216518.
7. Ingram D. [Investor relations presentation.] Sarepta Therapeutics website. June 22, 2023. Accessed Sept. 3, 2023. https://investorrelations.sarepta.com/static-files/7216948c-f688-4024-922e-39761bc7a984.
“There have been so many breakthroughs recently on the side of genetically targeted treatment [for muscular dystrophy] that supports muscle better,” said John F. Brandsema, MD, a child neurologist and section head at Children’s Hospital of Philadelphia, in an interview with Neurology Reviews 2023 Rare Neurological Disease Special Report. “We’re starting to see clinical response to some things that have been in trials – after decades of banging our heads on the wall trying new therapies, only to see them fail. I think it’s about reframing Duchenne muscular dystrophy [DMD] and facioscapulohumeral muscular dystrophy [FSHD] as treatable by target therapy because previously, they were treated with supportive care.”
DMD: Current and emerging therapies
DMD is caused by a mutation in the dystrophin gene on the X chromosome that inhibits production of dystrophin, a protein that shields muscles from injury during contraction. Dystrophin deficiency prevents muscle recovery, resulting in muscle-cell death and, ultimately, loss of function due to muscle degeneration.
FDA-approved exon-skipping therapies. Treatment modalities for what has historically been an incurable, lifespan-shortening disease involved supportive care that addresses symptoms, not the underlying cause. Consequently, many patients with DMD live only into their 20s and 30s. The tide began to turn in 2016, however, when the U.S. Food and Drug Administration granted accelerated approval for eteplirsen, an exon 51–skipping treatment that was the first RNA-based therapy for DMD to target the underlying cause. Additional exon-skipping therapies followed, including casimersen, which skips exon 45, and golodirsen and viltolarsen, which skip exon 53.
AOC 1044: Novel exon-skipping. In April 2023, the FDA granted orphan-drug designation to the experimental drug antibody oligonucleotide conjugate (AOC) 1044 that skips exon 44. A small interfering RNA (siRNA), AOC 1044 works in patients who have a mutation amenable to exon 44 skipping (a disease type known as DMD44) by delivering phosphorodiamidate morpholino to skeletal muscle and heart tissue that skips exon 44. The process allows for dystrophin production, thereby preventing degradation of muscle tissue.
The orphan drug status of AOC 1044 made it available to the population of patients enrolled in the EXPLORE44 Phase 1/2 trial. However, studies demonstrating effectiveness of the drug – with the hope of, ultimately, providing widespread access to AOC 1044 – are still underway. In one of those studies, investigators expect to enroll approximately 40 healthy volunteers and 24 DMD44 patients 7-27 years of age.3 The study will evaluate the effects of exon skipping and dystrophin protein levels in participants who have DMD44.
Delandistrogene moxeparvovec. Oct. 27, 2021, marked the inception of the phase 3 Multinational, Randomized, Double-Blind, Placebo-Controlled Systemic Gene Delivery Study to Evaluate the Safety and Efficacy of SRP-9001 in Subjects With Duchenne Muscular Dystrophy (EMBARK). The trial is evaluating the safety and efficacy of the gene-therapy agent delandistrogene moxeparvovec in ambulatory boys who were 4 to less than 8 years of age at randomization. The 126 boys enrolled in the trial met the criteria of (1) a diagnosis of DMD confirmed by documented clinical findings and previous genetic testing and (2) a pathogenic frameshift mutation stop codon located between exons 18 and 79 (inclusive), except for a mutation fully contained within exon 45.
Additional inclusion criteria were (1) the ability to cooperate with motor-assessment testing and (2) receiving a steady daily dose of oral corticosteroid for 12 weeks or longer prior to screening, and (3) the expectation of maintaining the study dosage throughout screening. Boys who had previously received gene therapy, investigational medication, or any treatment that could have amplified dystrophin expression within the time limit specified by the protocol were ineligible to participate. Boys were excluded from the study if they presented with any other illness, medical condition, or need for chronic drug treatment.
Exon-skipping therapies in trials. Various biotech and pharmaceutical companies have initiated clinical trials to explore the potential of additional exon-skipping therapies for the DMD population:
ENTR-601-44 is another exon 44–skipping therapy in the pipeline.
On Aug. 22, 2023, the FDA approved delandistrogene moxeparvovec-rokl, a recombinant gene therapy utilizing an adenovirus vector. The product is indicated for ambulatory patients with DMD 4-5 years of age who have a confirmed mutation of the dystrophin gene.
Dyne Therapeutics is actively recruiting participants to investigate Dyne 251, its exon 51–skipping therapy.
Trials are in the works by BioMarin Pharmaceutical for its next-generation peptide-conjugated phosphorodiamidate morpholino oligomers (PPMO) for skipping exon 51.
Despite the prospects of such therapy, therapeutic targeting of exon 44 addresses only patients with DMD44, who account for approximately 10% of the DMD population. Disease involving the most prevalent site of a dystrophin gene mutation, exon 51, affects 13% of the DMD population. This leaves the majority of patients with DMD without gene therapy. Yet Dr. Brandsema is optimistic nevertheless.
“We were just failing over and over again with DMD treatment, but there is some hope now,” Dr. Brandsema said. “Also, FSHD is right on the cusp of having new therapies approaching.”
FSHD: Emerging therapies
The third more common type of muscular dystrophy is not a life-threatening condition. FSHD affects approximately 4 of every 100,000 people.1 An autosomal-dominant condition, FSHD is ultimately caused by inappropriate expression of the DUX4 protein product – a consequence of a complex genetic activity involving DUX4, its chromosomal locus, and the number of repeats of a microsatellite called D4Z4.4 The disease usually starts in proximal regions of the face (that is, surrounding the eyes and mouth), before spreading to muscular groups of the limbs – most prominently, muscles of the scapulae and humeri. Symptoms usually appear in these places initially, but the condition can affect any part of the body. Fifty percent of FSHD patients experience loss of high-frequency hearing and present with retinovasculopathy. Like DMD, FSHD varies in severity, with some forms presenting at birth.
AOC 1020-CS1 is an example of a new FSHD treatment under investigation. The phase 1/2 FORTITUDE trial is a randomized, double-blind, placebo-controlled study exploring the safety, tolerability, pharmacokinetics, pharmacodynamics, and potential efficacy of single- and multiple-dose AOC 1020-CS1 therapy in FSHD.5 The trial began in April 2023; estimated completion date is September 2025.
As with many rare diseases, however, following patients and capturing data that fully narrate their story remains challenging in both DMD and FSHD. Although clinical trials undoubtedly offer hope of expanding treatment options and additional insights into disease-state management, the often insidious, complex nature of some rare diseases, such as DMD and FSHD, presents some limitations.
“Patients are hard to measure,” Dr. Brandsema explained, “because they’re so variable at baseline in history and progress in a different [slower] way than timelines are set up in our system to study drugs.”
Neonatal screening and early diagnosis: Imperative for improving outcomes
Neonatal screening helps with early detection and treatment. Prompt diagnosis does not necessarily prolong a DMD patient’s life, but it can enhance their quality of life.
DNA diagnostics. A critical component of the path to treatment is DNA diagnostics. According to Barry J. Byrne, MD, PhD, chief medical advisor of the Muscular Dystrophy Association, the Human Genome Project conducted by the National Institutes of Health helped make DNA tests affordable; such tests run about $800 today. However, given continuous advancements in sequencing, Dr. Byrne said that whole-exome sequencing for $100 is within reach.
In terms of accessibility, some nations – Canada is an example – include testing as part of national health care services. In the United States, coverage for testing varies by health insurance plan. In addition, some plans have favored rapid diagnostic testing, and the overall cost is often individualized to the patient.
Early diagnosis and supportive care. Early diagnosis can certainly help improve DMD patients’ quality of life; supportive care provides some benefit. Dr. Byrne stressed the importance of managing extraskeletal clinical manifestations in this patient population. A critical area is initiating cardiovascular treatment immediately following diagnosis, even if the patient does not exhibit cardiovascular symptoms.
“Cardiac manifestations are actually the cause of mortality in DMD, and most boys with DMD should begin cardiovascular treatment shortly after diagnosis,” Dr. Byrne told Neurology Reviews 2023 Rare Neurological Disease Special Report. “The message to neurologists is that these patients can benefit from early cardiovascular treatment because we can prevent the complications of DMD-related heart failure until much later in life.”
Historically, clinicians used echocardiography as the mainstay tool to assess cardiovascular function; however, more and more clinicians are turning to magnetic resonance imaging for such investigation. Dr. Byrne, a cardiologist, explained that magnetic resonance imaging identifies cardiovascular dysfunction at earlier stages than echocardiography can. In addition, although DMD patients frequently experience fatigue, Dr. Byrne cautions neurologists that fatigue is usually related to muscle weakness, not necessarily heart failure.
DMD therapies carry a hefty price
Right now, the projected price range of AOC 1044 is $3.2 million to $3.4 million. Akin to the case with onasemnogene abeparvovec-xioi (Zolgensma) for spinal muscular atrophy, the world’s first gene therapy and first seven-figure drug, the manufacturer of AOC 1044 based pricing on the anticipated cost of treating a DMD44 patient throughout the lifespan, according to Dr. Byrne.
Delandistrogene moxeparvovec might come with an even higher price tag. A cost-effectiveness analysis study priced the therapy at $5 million. In a presentation to investors, the manufacturer projected the price in the range of $5 million to $13 million.6,7
‘It takes a village’: Comprehensive care requires a multidisciplinary team
Dr. Brandsema and Dr. Byrne agree: Optimizing outcomes requires ongoing coordinated and collaborative efforts of an interdisciplinary team of health care providers for the duration of DMD and FSHD patients’ lifespan.
A neurologist by training, Dr. Brandsema recognizes the importance of interdisciplinary collaboration in caring for patients with DMD, given the multiorgan manifestations of the disease.
“We have some hope with DMD, and FSHD is right on the cusp of having new therapies approaching ... It is important to recognize that interdisciplinary follow-up and optimized standard of care are important after dosing.”
“I think many patients living with neurological disorders have multiple providers they rely on for care,” Dr. Byrne said, “but cardiovascular and pulmonary care are important because both are affected in the case of DMD – not so much in FSHD.”
Ultimately, advancements in therapy and care give patients living with these disorders, and their caregivers, a renewed sense of hope – hope that their life will be improved by breakthrough therapies that have been approved or will arrive soon.
Dr. Brandsema discloses he is a consultant for Alexion, Audentes, AveXis/Novartis, Biogen, Cytokinetics, Dyne, Edgewise, Fibrogen, Genentech/Roche, Janssen, Marathon, Momenta, NS Pharma, PTC Therapeutics, Sarepta, Scholar Rock, Takeda, and WaVe. He is a speaker for AveXis and Biogen, a medical advisory council member for Cure SMA, and a site investigator for clinical trials with Alexion, Astellas, AveXis/Novartis, Biogen, Catabasis, CSL Behring, Cytokinetics, Fibrogen, Genentech/Roche, Ionis, Lilly, Janssen, Pfizer, PTC Therapeutics, Sarepta, Scholar Rock, Summit, and WaVe. Dr. Byrne has no relevant financial disclosures.
References
1. Centers for Disease Control and Prevention. What is muscular dystrophy? Updated Nov. 21, 2022. Accessed Sept. 3, 2023. https://www.cdc.gov/ncbddd/musculardystrophy/facts.html.
2. FDA approves first gene therapy for treatment of certain patients with Duchenne muscular dystrophy. U.S. Food and Drug Administration. Press release. June 22, 2023. Accessed Sept. 3, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-gene-therapy-treatment-certain-patients-duchenne-muscular-dystrophy.
3. Study of AOC 1044 in healthy adult volunteers and participants with Duchenne muscular dystrophy (DMD) mutations amenable to exon 44 skipping (EXPLORE44). ClinicalTrials.gov Identifier: NCT05670730. Updated April 4, 2023. Accessed Sep. 3, 2023. https://www.clinicaltrials.gov/study/NCT05670730?cond=DMD&intr=AOC%201044&rank=1.
4. Statland JM, Tawil R. Facioscapulohumeral muscular dystrophy. Continuum (Minneap. Minn). 2016;22(6, Muscle and Neuromuscular Junction Disorders):1916-31. doi: 10.1212/CON.0000000000000399.
5. Phase 1/2 study of AOC 1020 in adults with facioscapulohumeral muscular dystrophy (FSHD) (FORTITUDE). ClinicalTrials.gov Identifier: NCT05747924. Updated Aug. 9, 2023. Accessed Sept. 3, 2023. https://clinicaltrials.gov/study/NCT05747924?term=fORTITUDE&cond=Facioscapulohumeral%20Muscular%20Dystrophy&rank=1.
6. Klimchak AC, Sedita LE, Rodino-Klapac LR, et al. Assessing the value of delandistrogene moxeparvovec (SRP-9001) gene therapy in patients with Duchenne muscular dystrophy in the United States. J Mark Access Health Policy. 2023;11(1):2216518. doi: 10.1080/20016689.2023.2216518.
7. Ingram D. [Investor relations presentation.] Sarepta Therapeutics website. June 22, 2023. Accessed Sept. 3, 2023. https://investorrelations.sarepta.com/static-files/7216948c-f688-4024-922e-39761bc7a984.
“There have been so many breakthroughs recently on the side of genetically targeted treatment [for muscular dystrophy] that supports muscle better,” said John F. Brandsema, MD, a child neurologist and section head at Children’s Hospital of Philadelphia, in an interview with Neurology Reviews 2023 Rare Neurological Disease Special Report. “We’re starting to see clinical response to some things that have been in trials – after decades of banging our heads on the wall trying new therapies, only to see them fail. I think it’s about reframing Duchenne muscular dystrophy [DMD] and facioscapulohumeral muscular dystrophy [FSHD] as treatable by target therapy because previously, they were treated with supportive care.”
DMD: Current and emerging therapies
DMD is caused by a mutation in the dystrophin gene on the X chromosome that inhibits production of dystrophin, a protein that shields muscles from injury during contraction. Dystrophin deficiency prevents muscle recovery, resulting in muscle-cell death and, ultimately, loss of function due to muscle degeneration.
FDA-approved exon-skipping therapies. Treatment modalities for what has historically been an incurable, lifespan-shortening disease involved supportive care that addresses symptoms, not the underlying cause. Consequently, many patients with DMD live only into their 20s and 30s. The tide began to turn in 2016, however, when the U.S. Food and Drug Administration granted accelerated approval for eteplirsen, an exon 51–skipping treatment that was the first RNA-based therapy for DMD to target the underlying cause. Additional exon-skipping therapies followed, including casimersen, which skips exon 45, and golodirsen and viltolarsen, which skip exon 53.
AOC 1044: Novel exon-skipping. In April 2023, the FDA granted orphan-drug designation to the experimental drug antibody oligonucleotide conjugate (AOC) 1044 that skips exon 44. A small interfering RNA (siRNA), AOC 1044 works in patients who have a mutation amenable to exon 44 skipping (a disease type known as DMD44) by delivering phosphorodiamidate morpholino to skeletal muscle and heart tissue that skips exon 44. The process allows for dystrophin production, thereby preventing degradation of muscle tissue.
The orphan drug status of AOC 1044 made it available to the population of patients enrolled in the EXPLORE44 Phase 1/2 trial. However, studies demonstrating effectiveness of the drug – with the hope of, ultimately, providing widespread access to AOC 1044 – are still underway. In one of those studies, investigators expect to enroll approximately 40 healthy volunteers and 24 DMD44 patients 7-27 years of age.3 The study will evaluate the effects of exon skipping and dystrophin protein levels in participants who have DMD44.
Delandistrogene moxeparvovec. Oct. 27, 2021, marked the inception of the phase 3 Multinational, Randomized, Double-Blind, Placebo-Controlled Systemic Gene Delivery Study to Evaluate the Safety and Efficacy of SRP-9001 in Subjects With Duchenne Muscular Dystrophy (EMBARK). The trial is evaluating the safety and efficacy of the gene-therapy agent delandistrogene moxeparvovec in ambulatory boys who were 4 to less than 8 years of age at randomization. The 126 boys enrolled in the trial met the criteria of (1) a diagnosis of DMD confirmed by documented clinical findings and previous genetic testing and (2) a pathogenic frameshift mutation stop codon located between exons 18 and 79 (inclusive), except for a mutation fully contained within exon 45.
Additional inclusion criteria were (1) the ability to cooperate with motor-assessment testing and (2) receiving a steady daily dose of oral corticosteroid for 12 weeks or longer prior to screening, and (3) the expectation of maintaining the study dosage throughout screening. Boys who had previously received gene therapy, investigational medication, or any treatment that could have amplified dystrophin expression within the time limit specified by the protocol were ineligible to participate. Boys were excluded from the study if they presented with any other illness, medical condition, or need for chronic drug treatment.
Exon-skipping therapies in trials. Various biotech and pharmaceutical companies have initiated clinical trials to explore the potential of additional exon-skipping therapies for the DMD population:
ENTR-601-44 is another exon 44–skipping therapy in the pipeline.
On Aug. 22, 2023, the FDA approved delandistrogene moxeparvovec-rokl, a recombinant gene therapy utilizing an adenovirus vector. The product is indicated for ambulatory patients with DMD 4-5 years of age who have a confirmed mutation of the dystrophin gene.
Dyne Therapeutics is actively recruiting participants to investigate Dyne 251, its exon 51–skipping therapy.
Trials are in the works by BioMarin Pharmaceutical for its next-generation peptide-conjugated phosphorodiamidate morpholino oligomers (PPMO) for skipping exon 51.
Despite the prospects of such therapy, therapeutic targeting of exon 44 addresses only patients with DMD44, who account for approximately 10% of the DMD population. Disease involving the most prevalent site of a dystrophin gene mutation, exon 51, affects 13% of the DMD population. This leaves the majority of patients with DMD without gene therapy. Yet Dr. Brandsema is optimistic nevertheless.
“We were just failing over and over again with DMD treatment, but there is some hope now,” Dr. Brandsema said. “Also, FSHD is right on the cusp of having new therapies approaching.”
FSHD: Emerging therapies
The third more common type of muscular dystrophy is not a life-threatening condition. FSHD affects approximately 4 of every 100,000 people.1 An autosomal-dominant condition, FSHD is ultimately caused by inappropriate expression of the DUX4 protein product – a consequence of a complex genetic activity involving DUX4, its chromosomal locus, and the number of repeats of a microsatellite called D4Z4.4 The disease usually starts in proximal regions of the face (that is, surrounding the eyes and mouth), before spreading to muscular groups of the limbs – most prominently, muscles of the scapulae and humeri. Symptoms usually appear in these places initially, but the condition can affect any part of the body. Fifty percent of FSHD patients experience loss of high-frequency hearing and present with retinovasculopathy. Like DMD, FSHD varies in severity, with some forms presenting at birth.
AOC 1020-CS1 is an example of a new FSHD treatment under investigation. The phase 1/2 FORTITUDE trial is a randomized, double-blind, placebo-controlled study exploring the safety, tolerability, pharmacokinetics, pharmacodynamics, and potential efficacy of single- and multiple-dose AOC 1020-CS1 therapy in FSHD.5 The trial began in April 2023; estimated completion date is September 2025.
As with many rare diseases, however, following patients and capturing data that fully narrate their story remains challenging in both DMD and FSHD. Although clinical trials undoubtedly offer hope of expanding treatment options and additional insights into disease-state management, the often insidious, complex nature of some rare diseases, such as DMD and FSHD, presents some limitations.
“Patients are hard to measure,” Dr. Brandsema explained, “because they’re so variable at baseline in history and progress in a different [slower] way than timelines are set up in our system to study drugs.”
Neonatal screening and early diagnosis: Imperative for improving outcomes
Neonatal screening helps with early detection and treatment. Prompt diagnosis does not necessarily prolong a DMD patient’s life, but it can enhance their quality of life.
DNA diagnostics. A critical component of the path to treatment is DNA diagnostics. According to Barry J. Byrne, MD, PhD, chief medical advisor of the Muscular Dystrophy Association, the Human Genome Project conducted by the National Institutes of Health helped make DNA tests affordable; such tests run about $800 today. However, given continuous advancements in sequencing, Dr. Byrne said that whole-exome sequencing for $100 is within reach.
In terms of accessibility, some nations – Canada is an example – include testing as part of national health care services. In the United States, coverage for testing varies by health insurance plan. In addition, some plans have favored rapid diagnostic testing, and the overall cost is often individualized to the patient.
Early diagnosis and supportive care. Early diagnosis can certainly help improve DMD patients’ quality of life; supportive care provides some benefit. Dr. Byrne stressed the importance of managing extraskeletal clinical manifestations in this patient population. A critical area is initiating cardiovascular treatment immediately following diagnosis, even if the patient does not exhibit cardiovascular symptoms.
“Cardiac manifestations are actually the cause of mortality in DMD, and most boys with DMD should begin cardiovascular treatment shortly after diagnosis,” Dr. Byrne told Neurology Reviews 2023 Rare Neurological Disease Special Report. “The message to neurologists is that these patients can benefit from early cardiovascular treatment because we can prevent the complications of DMD-related heart failure until much later in life.”
Historically, clinicians used echocardiography as the mainstay tool to assess cardiovascular function; however, more and more clinicians are turning to magnetic resonance imaging for such investigation. Dr. Byrne, a cardiologist, explained that magnetic resonance imaging identifies cardiovascular dysfunction at earlier stages than echocardiography can. In addition, although DMD patients frequently experience fatigue, Dr. Byrne cautions neurologists that fatigue is usually related to muscle weakness, not necessarily heart failure.
DMD therapies carry a hefty price
Right now, the projected price range of AOC 1044 is $3.2 million to $3.4 million. Akin to the case with onasemnogene abeparvovec-xioi (Zolgensma) for spinal muscular atrophy, the world’s first gene therapy and first seven-figure drug, the manufacturer of AOC 1044 based pricing on the anticipated cost of treating a DMD44 patient throughout the lifespan, according to Dr. Byrne.
Delandistrogene moxeparvovec might come with an even higher price tag. A cost-effectiveness analysis study priced the therapy at $5 million. In a presentation to investors, the manufacturer projected the price in the range of $5 million to $13 million.6,7
‘It takes a village’: Comprehensive care requires a multidisciplinary team
Dr. Brandsema and Dr. Byrne agree: Optimizing outcomes requires ongoing coordinated and collaborative efforts of an interdisciplinary team of health care providers for the duration of DMD and FSHD patients’ lifespan.
A neurologist by training, Dr. Brandsema recognizes the importance of interdisciplinary collaboration in caring for patients with DMD, given the multiorgan manifestations of the disease.
“We have some hope with DMD, and FSHD is right on the cusp of having new therapies approaching ... It is important to recognize that interdisciplinary follow-up and optimized standard of care are important after dosing.”
“I think many patients living with neurological disorders have multiple providers they rely on for care,” Dr. Byrne said, “but cardiovascular and pulmonary care are important because both are affected in the case of DMD – not so much in FSHD.”
Ultimately, advancements in therapy and care give patients living with these disorders, and their caregivers, a renewed sense of hope – hope that their life will be improved by breakthrough therapies that have been approved or will arrive soon.
Dr. Brandsema discloses he is a consultant for Alexion, Audentes, AveXis/Novartis, Biogen, Cytokinetics, Dyne, Edgewise, Fibrogen, Genentech/Roche, Janssen, Marathon, Momenta, NS Pharma, PTC Therapeutics, Sarepta, Scholar Rock, Takeda, and WaVe. He is a speaker for AveXis and Biogen, a medical advisory council member for Cure SMA, and a site investigator for clinical trials with Alexion, Astellas, AveXis/Novartis, Biogen, Catabasis, CSL Behring, Cytokinetics, Fibrogen, Genentech/Roche, Ionis, Lilly, Janssen, Pfizer, PTC Therapeutics, Sarepta, Scholar Rock, Summit, and WaVe. Dr. Byrne has no relevant financial disclosures.
References
1. Centers for Disease Control and Prevention. What is muscular dystrophy? Updated Nov. 21, 2022. Accessed Sept. 3, 2023. https://www.cdc.gov/ncbddd/musculardystrophy/facts.html.
2. FDA approves first gene therapy for treatment of certain patients with Duchenne muscular dystrophy. U.S. Food and Drug Administration. Press release. June 22, 2023. Accessed Sept. 3, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-gene-therapy-treatment-certain-patients-duchenne-muscular-dystrophy.
3. Study of AOC 1044 in healthy adult volunteers and participants with Duchenne muscular dystrophy (DMD) mutations amenable to exon 44 skipping (EXPLORE44). ClinicalTrials.gov Identifier: NCT05670730. Updated April 4, 2023. Accessed Sep. 3, 2023. https://www.clinicaltrials.gov/study/NCT05670730?cond=DMD&intr=AOC%201044&rank=1.
4. Statland JM, Tawil R. Facioscapulohumeral muscular dystrophy. Continuum (Minneap. Minn). 2016;22(6, Muscle and Neuromuscular Junction Disorders):1916-31. doi: 10.1212/CON.0000000000000399.
5. Phase 1/2 study of AOC 1020 in adults with facioscapulohumeral muscular dystrophy (FSHD) (FORTITUDE). ClinicalTrials.gov Identifier: NCT05747924. Updated Aug. 9, 2023. Accessed Sept. 3, 2023. https://clinicaltrials.gov/study/NCT05747924?term=fORTITUDE&cond=Facioscapulohumeral%20Muscular%20Dystrophy&rank=1.
6. Klimchak AC, Sedita LE, Rodino-Klapac LR, et al. Assessing the value of delandistrogene moxeparvovec (SRP-9001) gene therapy in patients with Duchenne muscular dystrophy in the United States. J Mark Access Health Policy. 2023;11(1):2216518. doi: 10.1080/20016689.2023.2216518.
7. Ingram D. [Investor relations presentation.] Sarepta Therapeutics website. June 22, 2023. Accessed Sept. 3, 2023. https://investorrelations.sarepta.com/static-files/7216948c-f688-4024-922e-39761bc7a984.

CPAP in overlap syndrome: Unveiling the evidence
Sleep Medicine Network
Respiratory-Related Sleep Disorders Section
The overlap syndrome (OS), which refers to the co-occurrence of OSA and COPD, was first described by Flenley in 1985 (Flenley DC. Clin Chest Med. 1985;6[4]:651). Over the years, numerous studies have demonstrated an increased risk of hospitalization and mortality in patients with OS (Brennan M, et al. 2022;1-10). Despite these findings, limited evidence exists regarding the optimal treatment approach for individuals with OS.

CPAP therapy has demonstrated various physiologic advantages for patients with OS (Srivali N, et al. Sleep Med. 2023;108:55-60), which contribute to diminished dyspnea symptoms, lowered pro-inflammatory markers, improved arterial blood gases, increased 6-minute walk distance, enhanced FEV1, and decreased mean pulmonary artery pressure (Suri TM, et al. FASEB BioAdv. 2021;3[9]:683-93). CPAP therapy in patients with OS has been linked to a reduction in COPD exacerbations (Voulgaris A, et al. Clin Respir Jour. 2023; 17[3]:165), fewer COPD-related hospitalizations (Marin JM, et al. Am J Respir Crit Care Med. 2010;182[3]:325-31), decreased cardiovascular events (Kendzerska T, et al. Ann ATS. 2019;16[1]:71), and an overall decline in mortality rates (Machado ML, et al. Eur Respir J. 2010;35[1]:132-7).
It is important to acknowledge that, as of now, no randomized clinical trial has specifically addressed the treatment of OS, leaving recommendations largely reliant on observational studies. Conversely, recent guidelines have proposed the utilization of high-intensity noninvasive ventilation (NIV) for hypercapnic patients with COPD. Thus, extensive research is warranted to characterize distinct sleep-related breathing disorders within the OS population and to investigate the effects of CPAP in comparison to other NIV modalities on patients with overlap syndrome.
Solmaz Ehteshami-Afshar, MD
Kirat Gill, MD, Section Member-at-Large
Sleep Medicine Network
Respiratory-Related Sleep Disorders Section
The overlap syndrome (OS), which refers to the co-occurrence of OSA and COPD, was first described by Flenley in 1985 (Flenley DC. Clin Chest Med. 1985;6[4]:651). Over the years, numerous studies have demonstrated an increased risk of hospitalization and mortality in patients with OS (Brennan M, et al. 2022;1-10). Despite these findings, limited evidence exists regarding the optimal treatment approach for individuals with OS.
CPAP therapy has demonstrated various physiologic advantages for patients with OS (Srivali N, et al. Sleep Med. 2023;108:55-60), which contribute to diminished dyspnea symptoms, lowered pro-inflammatory markers, improved arterial blood gases, increased 6-minute walk distance, enhanced FEV1, and decreased mean pulmonary artery pressure (Suri TM, et al. FASEB BioAdv. 2021;3[9]:683-93). CPAP therapy in patients with OS has been linked to a reduction in COPD exacerbations (Voulgaris A, et al. Clin Respir Jour. 2023; 17[3]:165), fewer COPD-related hospitalizations (Marin JM, et al. Am J Respir Crit Care Med. 2010;182[3]:325-31), decreased cardiovascular events (Kendzerska T, et al. Ann ATS. 2019;16[1]:71), and an overall decline in mortality rates (Machado ML, et al. Eur Respir J. 2010;35[1]:132-7).
It is important to acknowledge that, as of now, no randomized clinical trial has specifically addressed the treatment of OS, leaving recommendations largely reliant on observational studies. Conversely, recent guidelines have proposed the utilization of high-intensity noninvasive ventilation (NIV) for hypercapnic patients with COPD. Thus, extensive research is warranted to characterize distinct sleep-related breathing disorders within the OS population and to investigate the effects of CPAP in comparison to other NIV modalities on patients with overlap syndrome.
Solmaz Ehteshami-Afshar, MD
Kirat Gill, MD, Section Member-at-Large
Sleep Medicine Network
Respiratory-Related Sleep Disorders Section
The overlap syndrome (OS), which refers to the co-occurrence of OSA and COPD, was first described by Flenley in 1985 (Flenley DC. Clin Chest Med. 1985;6[4]:651). Over the years, numerous studies have demonstrated an increased risk of hospitalization and mortality in patients with OS (Brennan M, et al. 2022;1-10). Despite these findings, limited evidence exists regarding the optimal treatment approach for individuals with OS.
CPAP therapy has demonstrated various physiologic advantages for patients with OS (Srivali N, et al. Sleep Med. 2023;108:55-60), which contribute to diminished dyspnea symptoms, lowered pro-inflammatory markers, improved arterial blood gases, increased 6-minute walk distance, enhanced FEV1, and decreased mean pulmonary artery pressure (Suri TM, et al. FASEB BioAdv. 2021;3[9]:683-93). CPAP therapy in patients with OS has been linked to a reduction in COPD exacerbations (Voulgaris A, et al. Clin Respir Jour. 2023; 17[3]:165), fewer COPD-related hospitalizations (Marin JM, et al. Am J Respir Crit Care Med. 2010;182[3]:325-31), decreased cardiovascular events (Kendzerska T, et al. Ann ATS. 2019;16[1]:71), and an overall decline in mortality rates (Machado ML, et al. Eur Respir J. 2010;35[1]:132-7).
It is important to acknowledge that, as of now, no randomized clinical trial has specifically addressed the treatment of OS, leaving recommendations largely reliant on observational studies. Conversely, recent guidelines have proposed the utilization of high-intensity noninvasive ventilation (NIV) for hypercapnic patients with COPD. Thus, extensive research is warranted to characterize distinct sleep-related breathing disorders within the OS population and to investigate the effects of CPAP in comparison to other NIV modalities on patients with overlap syndrome.
Solmaz Ehteshami-Afshar, MD
Kirat Gill, MD, Section Member-at-Large
Use of 6-minute walk distance as a clinical trial outcome in interstitial lung disease
Diffuse Lung & Transplant Network
Pulmonary Physiology & Rehabilitation Section
Pulmonary arterial hypertension (PH) and more recently interstitial lung disease (ILD) trials use the 6-minute walk test (6MWT) as a primary outcome due to its ability to conveniently capture a patient’s functional capacity and quality of life. However, interpreting the 6MWT in complex and diverse diseases, such as ILD, presents significant challenges.
A recent article (Harari, et al. Eur Respir Rev. 2022 Aug 23;31(165):220087. doi: 10.1183/16000617.0087-2022) advocates for further research to determine the optimal use of the 6MWT as a clinical endpoint in ILD trials. A decline in 6MWT can represent progression of ILD; ILD-related PH; or musculoskeletal, hematologic, or cardiac etiologies related to the underlying cause of ILD.
To enhance sensitivity, the authors endorse the inclusion of additional parameters in the analysis, possibly as a composite outcome. This would involve integrating the oxygen desaturation profile, dyspnea scores, and heart rate recovery with changes in the 6MWT-distance. They propose this composite measure could serve as a primary endpoint when the study intervention’s impact on clinical performance – either improvement or stabilization of ILD or ILD-related PH – is clearly defined. The prognostic significance of these additional parameters in patients with ILD, however, requires further investigation.
Inter-test reliability requires a standardized 6MWT, as previously proposed for this population (Lancaster, et al. Contemporary Clin Trials. 2021;Nov 25,2020). The standardized test protocol that includes continuous pulse oximetry and heart rate measurement, oxygen titration, and end of test guidelines, will reduce variability and boost reproducibility.
In light of recent advancements in the affordability, convenience, and portability of oxygen consumption (VO2) gas analyzers, we believe that incorporating V
Ruchicka Sangani, MD, Section Fellow-in-Training
Saqib Baig, MD, Section Member-at-Large
Diffuse Lung & Transplant Network
Pulmonary Physiology & Rehabilitation Section
Pulmonary arterial hypertension (PH) and more recently interstitial lung disease (ILD) trials use the 6-minute walk test (6MWT) as a primary outcome due to its ability to conveniently capture a patient’s functional capacity and quality of life. However, interpreting the 6MWT in complex and diverse diseases, such as ILD, presents significant challenges.
A recent article (Harari, et al. Eur Respir Rev. 2022 Aug 23;31(165):220087. doi: 10.1183/16000617.0087-2022) advocates for further research to determine the optimal use of the 6MWT as a clinical endpoint in ILD trials. A decline in 6MWT can represent progression of ILD; ILD-related PH; or musculoskeletal, hematologic, or cardiac etiologies related to the underlying cause of ILD.
To enhance sensitivity, the authors endorse the inclusion of additional parameters in the analysis, possibly as a composite outcome. This would involve integrating the oxygen desaturation profile, dyspnea scores, and heart rate recovery with changes in the 6MWT-distance. They propose this composite measure could serve as a primary endpoint when the study intervention’s impact on clinical performance – either improvement or stabilization of ILD or ILD-related PH – is clearly defined. The prognostic significance of these additional parameters in patients with ILD, however, requires further investigation.
Inter-test reliability requires a standardized 6MWT, as previously proposed for this population (Lancaster, et al. Contemporary Clin Trials. 2021;Nov 25,2020). The standardized test protocol that includes continuous pulse oximetry and heart rate measurement, oxygen titration, and end of test guidelines, will reduce variability and boost reproducibility.
In light of recent advancements in the affordability, convenience, and portability of oxygen consumption (VO2) gas analyzers, we believe that incorporating V
Ruchicka Sangani, MD, Section Fellow-in-Training
Saqib Baig, MD, Section Member-at-Large
Diffuse Lung & Transplant Network
Pulmonary Physiology & Rehabilitation Section
Pulmonary arterial hypertension (PH) and more recently interstitial lung disease (ILD) trials use the 6-minute walk test (6MWT) as a primary outcome due to its ability to conveniently capture a patient’s functional capacity and quality of life. However, interpreting the 6MWT in complex and diverse diseases, such as ILD, presents significant challenges.
A recent article (Harari, et al. Eur Respir Rev. 2022 Aug 23;31(165):220087. doi: 10.1183/16000617.0087-2022) advocates for further research to determine the optimal use of the 6MWT as a clinical endpoint in ILD trials. A decline in 6MWT can represent progression of ILD; ILD-related PH; or musculoskeletal, hematologic, or cardiac etiologies related to the underlying cause of ILD.
To enhance sensitivity, the authors endorse the inclusion of additional parameters in the analysis, possibly as a composite outcome. This would involve integrating the oxygen desaturation profile, dyspnea scores, and heart rate recovery with changes in the 6MWT-distance. They propose this composite measure could serve as a primary endpoint when the study intervention’s impact on clinical performance – either improvement or stabilization of ILD or ILD-related PH – is clearly defined. The prognostic significance of these additional parameters in patients with ILD, however, requires further investigation.
Inter-test reliability requires a standardized 6MWT, as previously proposed for this population (Lancaster, et al. Contemporary Clin Trials. 2021;Nov 25,2020). The standardized test protocol that includes continuous pulse oximetry and heart rate measurement, oxygen titration, and end of test guidelines, will reduce variability and boost reproducibility.
In light of recent advancements in the affordability, convenience, and portability of oxygen consumption (VO2) gas analyzers, we believe that incorporating V
Ruchicka Sangani, MD, Section Fellow-in-Training
Saqib Baig, MD, Section Member-at-Large
Now we have MERCY
Critical Care Network
Sepsis/Shock Section
Beta-lactam antibiotics, including penicillin, carbapenems, and cephalosporins, exhibit time-dependent bacterial eradication. Prolonged infusions are thought to enhance the duration of effective bactericidal antibiotic exposure, decreasing the emergence of drug resistance due to reduced bacterial regrowth between doses – which may lead to cost savings by reducing drug acquisition costs and shortening hospital stays (Lodise TP Jr, et al. Clin Infect Dis. 2007;44[3]:357-63).
The best evidence for these benefits comes from observational studies and meta-analyses. The Defining Antibiotic Levels in Intensive Care Unit Patients (DALI) study emphasized the correlation between achieving target concentrations of beta-lactam antibiotics in critically ill patients and positive clinical outcomes for bloodstream infections but not for lung or intra-abdominal infections (Roberts JA, et al. Clin Infect Dis. 2014;58[8]:1072-83). A meta-analysis of 29 studies suggested that prolonged infusion of piperacillin-tazobactam was associated with a mortality benefit compared with intermittent infusions, but prolonged infusions of cephalosporins or carbapenems resulted in comparable outcomes without mortality benefit (Teo J, et al. Int J Antimicrob Agents. 2014;43[5]:403-11).
MERCY was a multinational, randomized controlled trial investigating the efficacy of continuous vs intermittent administration of meropenem in critically ill patients with sepsis. The primary outcome, a composite of mortality and emergence of resistant bacteria at day 28, showed no significant difference between continuous and intermittent administration (47% vs. 49%). Secondary outcomes and adverse events also did not display significant differences, suggesting that continuous meropenem did not improve outcomes compared with intermittent administration (Monti G, et al. JAMA. 2023;330[2]:141-51).
MERCY adds to the existing body of evidence suggesting that prolonged and intermittent infusion strategies for meropenem are at least equivalent in efficacy. Therefore, the strategy chosen can depend on other individualized factors.
The views expressed are those of the authors and do not reflect the official policy or position of the U.S. Navy, Department of Defense, or the US Government.

Meredith L. Olsen, MD, Section Member-at-Large
Casey Cable, MD, FCCP, Section Member-at-Large
Kathryn Pendleton, MD, FCCP, Section Vice-Chair
Critical Care Network
Sepsis/Shock Section
Beta-lactam antibiotics, including penicillin, carbapenems, and cephalosporins, exhibit time-dependent bacterial eradication. Prolonged infusions are thought to enhance the duration of effective bactericidal antibiotic exposure, decreasing the emergence of drug resistance due to reduced bacterial regrowth between doses – which may lead to cost savings by reducing drug acquisition costs and shortening hospital stays (Lodise TP Jr, et al. Clin Infect Dis. 2007;44[3]:357-63).
The best evidence for these benefits comes from observational studies and meta-analyses. The Defining Antibiotic Levels in Intensive Care Unit Patients (DALI) study emphasized the correlation between achieving target concentrations of beta-lactam antibiotics in critically ill patients and positive clinical outcomes for bloodstream infections but not for lung or intra-abdominal infections (Roberts JA, et al. Clin Infect Dis. 2014;58[8]:1072-83). A meta-analysis of 29 studies suggested that prolonged infusion of piperacillin-tazobactam was associated with a mortality benefit compared with intermittent infusions, but prolonged infusions of cephalosporins or carbapenems resulted in comparable outcomes without mortality benefit (Teo J, et al. Int J Antimicrob Agents. 2014;43[5]:403-11).
MERCY was a multinational, randomized controlled trial investigating the efficacy of continuous vs intermittent administration of meropenem in critically ill patients with sepsis. The primary outcome, a composite of mortality and emergence of resistant bacteria at day 28, showed no significant difference between continuous and intermittent administration (47% vs. 49%). Secondary outcomes and adverse events also did not display significant differences, suggesting that continuous meropenem did not improve outcomes compared with intermittent administration (Monti G, et al. JAMA. 2023;330[2]:141-51).
MERCY adds to the existing body of evidence suggesting that prolonged and intermittent infusion strategies for meropenem are at least equivalent in efficacy. Therefore, the strategy chosen can depend on other individualized factors.
The views expressed are those of the authors and do not reflect the official policy or position of the U.S. Navy, Department of Defense, or the US Government.
Meredith L. Olsen, MD, Section Member-at-Large
Casey Cable, MD, FCCP, Section Member-at-Large
Kathryn Pendleton, MD, FCCP, Section Vice-Chair
Critical Care Network
Sepsis/Shock Section
Beta-lactam antibiotics, including penicillin, carbapenems, and cephalosporins, exhibit time-dependent bacterial eradication. Prolonged infusions are thought to enhance the duration of effective bactericidal antibiotic exposure, decreasing the emergence of drug resistance due to reduced bacterial regrowth between doses – which may lead to cost savings by reducing drug acquisition costs and shortening hospital stays (Lodise TP Jr, et al. Clin Infect Dis. 2007;44[3]:357-63).
The best evidence for these benefits comes from observational studies and meta-analyses. The Defining Antibiotic Levels in Intensive Care Unit Patients (DALI) study emphasized the correlation between achieving target concentrations of beta-lactam antibiotics in critically ill patients and positive clinical outcomes for bloodstream infections but not for lung or intra-abdominal infections (Roberts JA, et al. Clin Infect Dis. 2014;58[8]:1072-83). A meta-analysis of 29 studies suggested that prolonged infusion of piperacillin-tazobactam was associated with a mortality benefit compared with intermittent infusions, but prolonged infusions of cephalosporins or carbapenems resulted in comparable outcomes without mortality benefit (Teo J, et al. Int J Antimicrob Agents. 2014;43[5]:403-11).
MERCY was a multinational, randomized controlled trial investigating the efficacy of continuous vs intermittent administration of meropenem in critically ill patients with sepsis. The primary outcome, a composite of mortality and emergence of resistant bacteria at day 28, showed no significant difference between continuous and intermittent administration (47% vs. 49%). Secondary outcomes and adverse events also did not display significant differences, suggesting that continuous meropenem did not improve outcomes compared with intermittent administration (Monti G, et al. JAMA. 2023;330[2]:141-51).
MERCY adds to the existing body of evidence suggesting that prolonged and intermittent infusion strategies for meropenem are at least equivalent in efficacy. Therefore, the strategy chosen can depend on other individualized factors.
The views expressed are those of the authors and do not reflect the official policy or position of the U.S. Navy, Department of Defense, or the US Government.
Meredith L. Olsen, MD, Section Member-at-Large
Casey Cable, MD, FCCP, Section Member-at-Large
Kathryn Pendleton, MD, FCCP, Section Vice-Chair
Have you asked your patients: What is your ideal outpatient gynecology experience?
There has been increasing awareness of a need for creating a more patient-centered experience with outpatient gynecology; however, very little data exist about what interventions are important to patients. Given social media’s ease of use and ability for widespread access to a diverse group of users, it has the potential to be a powerful tool for qualitative research questions without the difficulties of cost, transportation, transcription, etc. required of a focus group. Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of “likes” that, at scale, can provide a reliable measure of public support or engagement for a particular concept.1 Particularly for topics that are controversial or novel, X (formerly Twitter, and referred to as Twitter intermittently throughout this article based on the time the study was conducted), with 300 million monthly users,2 has become a popular tool for general and health care ̶ focused content and sentiment analysis.3,4 This study presents a qualitative analysis of themes from a crowdsourced request on Twitter to design the ideal outpatient gynecologic experience that subsequently went “viral”.5,6
When asked to design the optimized outpatient gynecology experience, social media users expressed:
- hospitality, comfort, and pain control as frequent themes
- preserving privacy and acknowledgement of voluntary nulliparity as frequent themes
- a desire for diverse imagery and representation related to race, LGBTQIA+ themes, age, and weight/body type within the office setting
- a call for a sense of psychological safety within gynecology
Why the need for our research question on patient-centered gyn care
While the body of literature on patient-centered health care has grown rapidly in recent years, a patient-centered outpatient gynecology experience has not yet been described in the medical literature.
Patient-centered office design, driven by cultural sensitivity, has been shown in other studies to be both appreciated by established patients and a viable business strategy to attract new patients.7 Topics such as pain control, trauma-informed care in gynecologyclinics,8 and diverse representation in patient materials and illustrations9 have been popular topics in medicine and in the lay press. Our primary aim in our research was to utilize feedback from the question posed to quantify and rank patient-centered interventions in a gynecology office. These themes and others that emerged in our analysis were used to suggest b
What we asked social media users. The survey query to social media users, “I have the opportunity to design my office from scratch. I’m asking women: How would you design/optimize a visit to the gynecologist’s office?” was crowd-sourced via Twitter on December 5, 2021.5 Given a robust response to the query, it provided an opportunity for a qualitative research study exploring social media users’ perspectives on optimizing outpatient gynecologic care, although the original question was not planned for research utilization.
What we found
By December 27, 2021, the original tweet had earned 9,411 likes; 2,143 retweets; and 3,400 replies. Of this group, we analyzed 131 tweets, all of which had 100 or greater likes on Twitter at the time of the review. The majority of analyzed tweets earned between 100 ̶ 500 likes (75/131; 57.3%), while 22.9% (30/131) had 501 ̶ 1,000 likes, 11.5% (15/131) had >2,000 likes, and 8.4% (11/131) had 1,001 ̶ 1,999 likes.
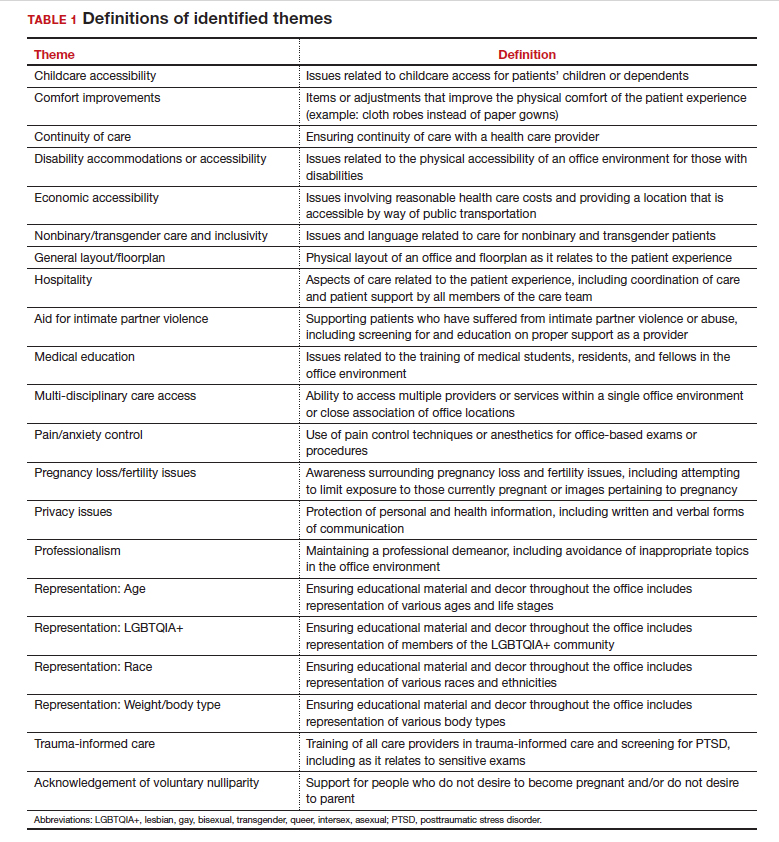
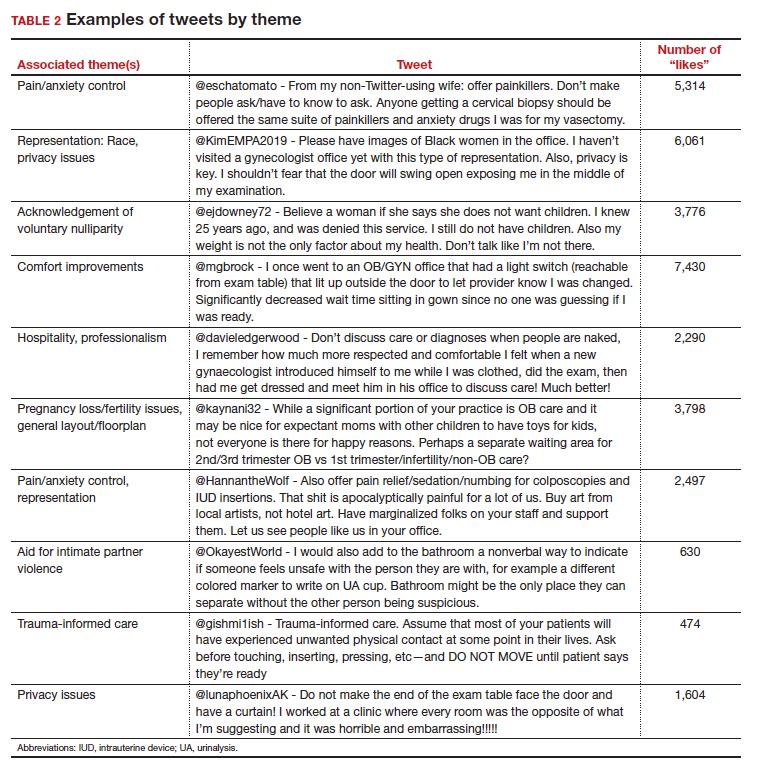
Identified themes within the tweets analyzed included: medical education, comfort improvements, continuity of care, disability accommodations/accessibility, economic accessibility, nonbinary/transgender care and inclusivity, general layout/floorplan, hospitality, aid for intimate partner violence, childcare accessibility, multi-disciplinary care access, pain/anxiety control, sensitivity toward pregnancy loss/fertility issues, privacy issues, professionalism, representation (subdivided into race, LGBTQIA+, age, and weight/body type), trauma-informed care, and acknowledgement of voluntary nulliparity/support for reproductive choices (TABLE 1). TABLE 2 lists examples of popular tweets by selected themes.
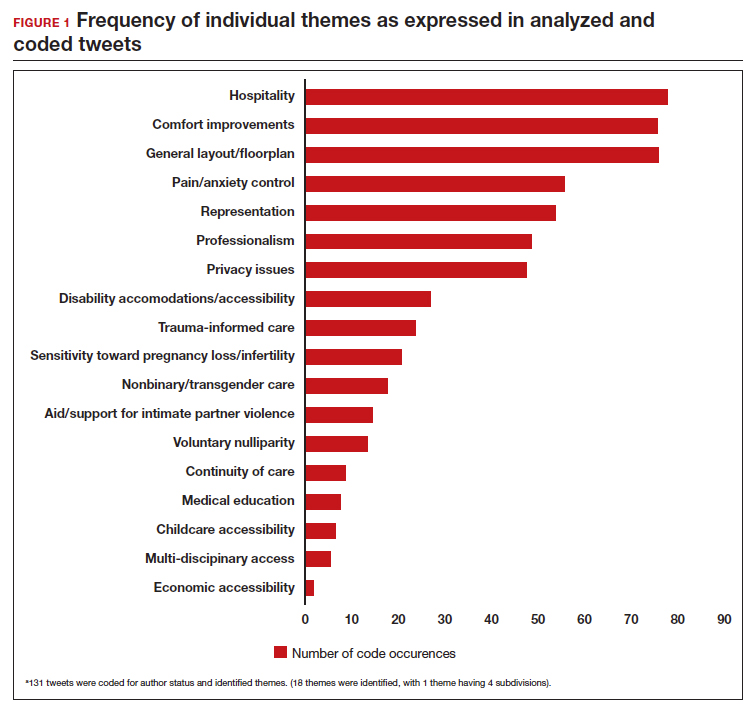
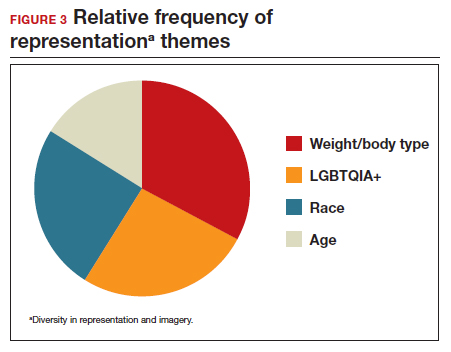
Frequent themes. The most frequently occurring themes within the 131 analyzed tweets (FIGURE 1) were:
- hospitality (77 occurrences)
- comfort improvements (75 occurrences)
- general layout/floorplan (75 occurrences)
- pain/anxiety control (55 occurrences)
- representation (53 occurrences).
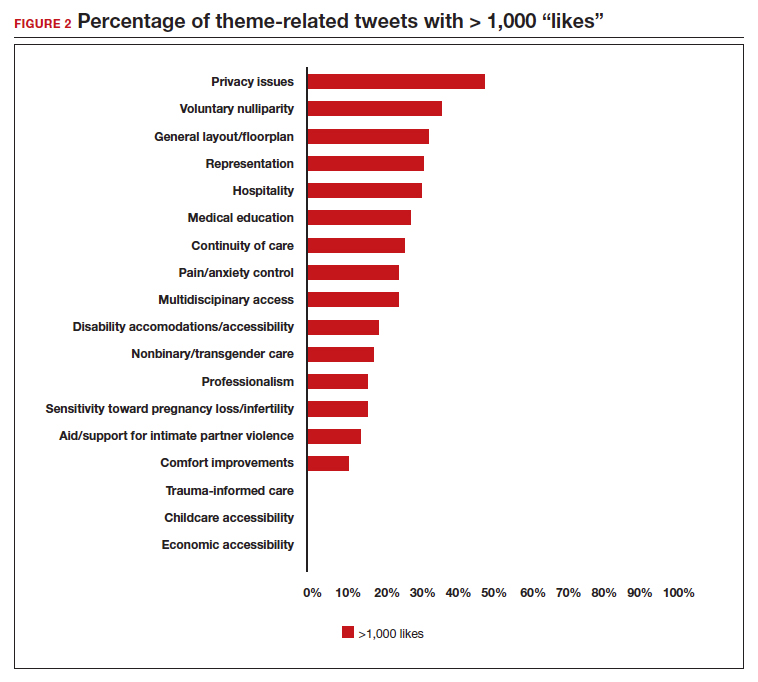
Popular themes. Defined as those with more than 1,000 likes at the time of analysis (FIGURE 2), the most popular themes included:
- privacy issues (48.5% of related tweets with >1,000 likes)
- voluntary nulliparity (37.0% of related tweets with >1,000 likes)
- general layout/floorplan (33.4% of related tweets with >1,000 likes)
- representation (32.1% of related tweets with >1,000 likes)
- hospitality (31.3% of related tweets with >1,000 likes).
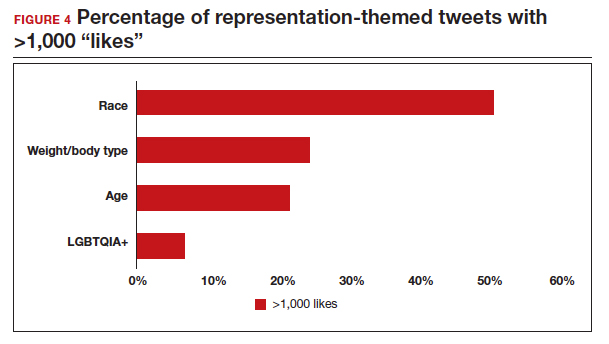
A sub-analysis of themes related to specific types of representation—race, LGBTQIA+, age, and weight/body type was performed. Tweets related to diverse weight/body type representation occurred most frequently (19 code occurrences; FIGURE 3). Similarly, tweets related to the representation of diverse races and the LGBTQIA+ community each comprised 26% of the total representation-based tweets. In terms of popularity as described above, 51.4% of tweets describing racial representation earned >1,000 likes (FIGURE 4).
Tweet demographics. Seven (7/131; 5.3%) of the tweet authors were verified Twitter users and 35 (35/131; 26.7%) authors reported working in the health care field within their Twitter profile description.
Continue to: Implementing our feedback can enhance patient experience and care...
Implementing our feedback can enhance patient experience and care
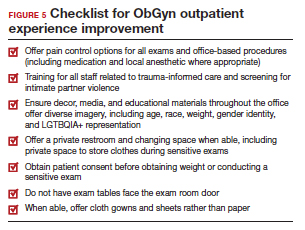
Our study provides a unique view of the patient perspective through analyzed crowdsourced public opinion via Twitter. To our knowledge, an optimized patient-centered outpatient gynecology experience has not previously been described in the medical literature. Optimizing the found domains of hospitality, comfort measures, pain and anxiety control, privacy, and diverse representationin the outpatient gynecologic experience within the outpatient care setting may ultimately result in improved patient satisfaction, patient well-being, and adherence to care through maximizing patient-centered care. We created a checklist of suggestions, including offering analgesics during office-based procedures and tailoring the floorplan to maximize privacy (FIGURE 5), for improving the outpatient gynecology experience based on our findings.
Prior data on patient satisfaction and outcomes
Improving patient satisfaction with health care is a priority for both clinicians and hospital systems. Prior studies have revealed only variable associations between patient satisfaction, safety, and clinical outcomes. One study involving the analysis of clinical and operational data from 171 hospitals found that hospital size, surgical volume, and low mortality rates were associated with higher patient satisfaction, while favorable surgical outcomes did not consistently correlate with higher Hospital Consumer Assessment of Healthcare Provers and Systems (HCAHPS) scores.10 Smaller, lower-volume hospitals earned higher satisfaction scores related to cleanliness, quietness, and receiving help measures.10 It has also been shown that the strongest predictors of patient satisfaction with the hospital childbirth experience included items related to staff communication, compassion, empathy, and respect.11 These data suggest that patient satisfaction is likely more significantly impacted by factors other than patient safety and effectiveness, and this was supported by the findings of our analysis. The growing body of literature associating a sense of psychological and physical safety within the health care system and improved patient outcomes and experience suggests that the data gathered from public commentary such as that presented here is extremely important for galvanizing change within the US health care system.
In one systematic review, the relationship between patient-centered care and clinical outcomes was mixed, although generally the association was positive.12 Additionally, patient-centered care was often associated with increased patient satisfaction and well-being. Some studies suggest that patient well-being and satisfaction also may be associated with improved adherence and self-management behaviors.12,13 Overall, optimizing patient-centered care may lead to improved patient satisfaction and potentially improved clinical outcomes.
Additionally, increasing diverse representation in patient materials and illustrations may help to improve the patient experience. Louie and colleagues found that dark skin tones were represented in only 4.5% of 4,146 images from anatomy texts analyzed in 2018.14 Similarly, a photogrammetric analysis of medical images utilized in New England Journal of Medicine found that only 18% of images depicted non-white skin.15 More recent efforts to create a royalty-free digital gallery of images reflecting bodies with diverse skin tones, body shapes, body hair, and age as well as transgender and nonbinary people have been discussed in the lay press.9 Based on our findings, social media users value and are actively seeking diversity in representation and imagery during their outpatient gynecology experience.
Opportunities for future study
Our research utilized social media as a diverse and accessible source of information; however, there are significant opportunities to refine the methodologic approach to answering the fundamental question of creating the patient-centered gynecologic experience. This type of study has not yet been conducted; however, the richness of the information from this current analysis could be informative to survey creation. Future research on this subject outside of social media could bolster the generalizability of our conclusions and the ability to report on qualitative findings in the setting of known patient demographics.
Social media remains a powerful tool as evidenced by this study, and continued use and observation of trending themes among patients is essential. The influence of social media will remain important for answering questions in gynecology and beyond.
Our work is strengthened by social media’s low threshold for use and the ability for widespread access to a diverse group of users. Additionally, social media allows for many responses to be collected in a timely manner, giving strength to the abstracted themes. The constant production of data by X users and their accessibility provide the opportunity for greater geographic coverage in those surveyed.4 Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of likes and retweets that may provide a reliable measure of public support or engagement.1
Future studies should examine ways to implement the suggested improvements to the office setting in a cost-effective manner and follow both subjective patient-reported outcomes as well as objective data after implementation, as these changes may have implications for much broader public health crises, such as maternal morbidity and mortality.
Study limitations. Our study is limited by the inherent biases and confounders associated with utilizing data derived from social media. Specifically, not all patients who seek outpatient gynecologic care utilize social media and/or X; using a “like” as a surrogate for endorsement of an idea by an identified party limits the generalizability of the data.
The initial Twitter query specified, “I’m asking women”, which may have altered the intended study population, influenced the analysis, and affected the representativeness of the sample through utilizing non ̶inclusive language. While non-binary/transgender care and inclusivity emerged as a theme discussed with the tweets, it is unclear if this represents an independent theme or rather a reaction to the non–inclusive language within the original tweet. ●
The data abstracted was analyzed with Dedoose1 software using a convenience sample and a mixed-methods analysis. Utilizing X (formerly Twitter and referred here as such given the time the study was conducted) for crowdsourcing functions similarly to an open survey. In the absence of similar analyses, a modified Checklist for Reporting Results of Internet E-Surveys (CHERRIES) checklist was utilized to organize our approach.2
This analysis was comprised of information freely available in the public domain, and the study was classified as IRB exempt. Ethical considerations were made for the fact that this is open access information and participants can reasonably expect their responses to be viewed by the public.3 As this question was not originally intended for research purposes, there was not a formalized development, recruitment, or consent process. The survey was not advertised beyond the original posting on Twitter, and the organic interest that it generated online. No incentives were offered to participants, and all participation was voluntary. There is no mechanism on Twitter for respondents to edit their response, although responses can be deleted. Unique visitors or viewers beyond posted impressions in response to the original tweet could not be determined.
Twitter thread responses were reviewed, and all completed and posted responses to the original Twitter query with 100 or greater “likes” were included in the analysis. These tweets were abstracted from Twitter between December 17, 2021, and December 27, 2021. At the time of tweet abstraction, engagement metrics, including the numbers of likes, retweets, and replies, were recorded. Additionally, author characteristics were abstracted, including author verification status and association with health care, as described in their Twitter profile. Definition of an individual associated with health care was broad and included physicians, advanced practice providers, nurses, first responders, and allied health professionals.
A total of 131 tweets met inclusion criteria and were uploaded for analysis using Dedoose qualitative analytic software.1 Two authors independently utilized a qualitative analysis to code the isolated tweets and identify thematic patterns among them. Uploaded tweets were additionally coded based on ranges of likes: 100-500; 501-1,000; 1,001-1,999; and >2,000. Tweets were coded for author verification status and whether or not the author was associated with the health care field. Themes were identified and defined during the coding process and were shared between the two authors. A total of 18 themes were identified, with 1 theme having 4 subdivisions. Interrater reliability testing was performed using Dedoose1 software and resulted with a pooled Cohen’s Kappa of 0.63, indicating “good” agreement between authors, which is an adequate level of agreement per the Dedoose software guidelines.
References
1. Dedoose website. Accessed July 28, 2022. https://www .dedoose.com/
2. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet e-surveys (CHERRIES) [published correction appears in J Med Internet Res. 2012;14:e8. doi:10.2196/jmir.2042]. J Med Internet Res. 2004;6:e34. doi:10.2196/jmir.6.3.e34
3. Townsend L, Wallace C. Social media research: a guide to ethics [University of Glasgow Information for the Media website]. Accessed March 2, 2023. https://www.gla.ac.uk /media/Media_487729_smxx.pdf
- Garvey MD, Samuel J, Pelaez A. Would you please like my tweet?! An artificially intelligent, generative probabilistic, and econometric based system design for popularity-driven tweet content generation. Decis Support Syst. 2021;144:113497. doi: 10.1016/j.dss.2021.113497
- Twitter Revenue and Usage Statistics (2023). Business of apps. Published August 10, 2023. Accessed September 19, 2023. https://www.businessofapps.com/data/twitter-statistics/
- Doan AE, Bogen KW, Higgins E. A content analysis of twitter backlash to Georgia’s abortion ban. Sex Reprod Healthc. 2022;31:100689. doi:10.1016/j.srhc.2021.100689
- Roberts H, Sadler J, Chapman L. The value of Twitter data for determining the emotional responses of people to urban green spaces: a case study and critical evaluation. Urban Stud. 2019;56:818-835. doi: 10.1177/0042098017748544
- Stewart R [@stuboo]. I have the opportunity to design my office from scratch. I’m asking women. How would you design/optimize a visit to the gynecologist’s office? problems frustrations solutions No detail is too small. If I’ve ever had a tweet worthy of virality, it’s this one. RT. Twitter. Published December 5, 2021. Accessed March 1, 2023. https://twitter .com/stuboo/status/1467522852664532994
- A gynecologist asked Twitter how he should redesign his office. The answers he got were about deeper health care issues. Fortune. Accessed March 2, 2023. https://fortune .com/2021/12/07/gynecologist-twitter-question/
- Anderson GD, Nelson-Becker C, Hannigan EV, et al. A patientcentered health care delivery system by a university obstetrics and gynecology department. Obstet Gynecol. 2005;105:205210. doi:10.1097/01.AOG.0000146288.28195.27
- Ades V, Wu SX, Rabinowitz E, et al. An integrated, traumainformed care model for female survivors of sexual violence: the engage, motivate, protect, organize, self-worth, educate, respect (EMPOWER) clinic. Obstet Gynecol. 2019;133:803809. doi:10.1097/AOG.0000000000003186
- Gordon D. Health equity comes to medical illustrations with launch of new image library. Forbes. Accessed March 2023. https://www.forbes.com/sites/debgordon/2022/05/11 /health-equity-comes-to-medical-illustrations-with-launch -of-new-image-library/
- Kennedy GD, Tevis SE, Kent KC. Is there a relationship between patient satisfaction and favorable outcomes? Ann Surg. 2014;260:592-600. doi:10.1097/SLA.0000000000000932
- Gregory KD, Korst LM, Saeb S, et al. Childbirth-specific patient-reported outcomes as predictors of hospital satisfaction. Am J Obstet Gynecol. 2019;220:201.e1-201.e19. doi:10.1016/j.ajog.2018.10.093
- Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70:351-379. doi:10.1177/1077558712465774
- Kahn KL, Schneider EC, Malin JL, et al. Patient-centered experiences in breast cancer: predicting long-term adherence to tamoxifen use. Med Care. 2007;45:431-439. doi:10.1097/01 .mlr.0000257193.10760.7
- Louie P, Wilkes R. Representations of race and skin tone in medical textbook imagery. Soc Sci Med. 2018;202:38-42. doi:10.1016/j.socscimed.2018.02.023
- Massie JP, Cho DY, Kneib CJ, et al. A picture of modern medicine: race and visual representation in medical literature. J Natl Med Assoc. 2021;113:88-94. doi:10.1016/j.jnma.2020.07.013
There has been increasing awareness of a need for creating a more patient-centered experience with outpatient gynecology; however, very little data exist about what interventions are important to patients. Given social media’s ease of use and ability for widespread access to a diverse group of users, it has the potential to be a powerful tool for qualitative research questions without the difficulties of cost, transportation, transcription, etc. required of a focus group. Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of “likes” that, at scale, can provide a reliable measure of public support or engagement for a particular concept.1 Particularly for topics that are controversial or novel, X (formerly Twitter, and referred to as Twitter intermittently throughout this article based on the time the study was conducted), with 300 million monthly users,2 has become a popular tool for general and health care ̶ focused content and sentiment analysis.3,4 This study presents a qualitative analysis of themes from a crowdsourced request on Twitter to design the ideal outpatient gynecologic experience that subsequently went “viral”.5,6
When asked to design the optimized outpatient gynecology experience, social media users expressed:
- hospitality, comfort, and pain control as frequent themes
- preserving privacy and acknowledgement of voluntary nulliparity as frequent themes
- a desire for diverse imagery and representation related to race, LGBTQIA+ themes, age, and weight/body type within the office setting
- a call for a sense of psychological safety within gynecology
Why the need for our research question on patient-centered gyn care
While the body of literature on patient-centered health care has grown rapidly in recent years, a patient-centered outpatient gynecology experience has not yet been described in the medical literature.
Patient-centered office design, driven by cultural sensitivity, has been shown in other studies to be both appreciated by established patients and a viable business strategy to attract new patients.7 Topics such as pain control, trauma-informed care in gynecologyclinics,8 and diverse representation in patient materials and illustrations9 have been popular topics in medicine and in the lay press. Our primary aim in our research was to utilize feedback from the question posed to quantify and rank patient-centered interventions in a gynecology office. These themes and others that emerged in our analysis were used to suggest b
What we asked social media users. The survey query to social media users, “I have the opportunity to design my office from scratch. I’m asking women: How would you design/optimize a visit to the gynecologist’s office?” was crowd-sourced via Twitter on December 5, 2021.5 Given a robust response to the query, it provided an opportunity for a qualitative research study exploring social media users’ perspectives on optimizing outpatient gynecologic care, although the original question was not planned for research utilization.
What we found
By December 27, 2021, the original tweet had earned 9,411 likes; 2,143 retweets; and 3,400 replies. Of this group, we analyzed 131 tweets, all of which had 100 or greater likes on Twitter at the time of the review. The majority of analyzed tweets earned between 100 ̶ 500 likes (75/131; 57.3%), while 22.9% (30/131) had 501 ̶ 1,000 likes, 11.5% (15/131) had >2,000 likes, and 8.4% (11/131) had 1,001 ̶ 1,999 likes.
Identified themes within the tweets analyzed included: medical education, comfort improvements, continuity of care, disability accommodations/accessibility, economic accessibility, nonbinary/transgender care and inclusivity, general layout/floorplan, hospitality, aid for intimate partner violence, childcare accessibility, multi-disciplinary care access, pain/anxiety control, sensitivity toward pregnancy loss/fertility issues, privacy issues, professionalism, representation (subdivided into race, LGBTQIA+, age, and weight/body type), trauma-informed care, and acknowledgement of voluntary nulliparity/support for reproductive choices (TABLE 1). TABLE 2 lists examples of popular tweets by selected themes.
Frequent themes. The most frequently occurring themes within the 131 analyzed tweets (FIGURE 1) were:
- hospitality (77 occurrences)
- comfort improvements (75 occurrences)
- general layout/floorplan (75 occurrences)
- pain/anxiety control (55 occurrences)
- representation (53 occurrences).
Popular themes. Defined as those with more than 1,000 likes at the time of analysis (FIGURE 2), the most popular themes included:
- privacy issues (48.5% of related tweets with >1,000 likes)
- voluntary nulliparity (37.0% of related tweets with >1,000 likes)
- general layout/floorplan (33.4% of related tweets with >1,000 likes)
- representation (32.1% of related tweets with >1,000 likes)
- hospitality (31.3% of related tweets with >1,000 likes).
A sub-analysis of themes related to specific types of representation—race, LGBTQIA+, age, and weight/body type was performed. Tweets related to diverse weight/body type representation occurred most frequently (19 code occurrences; FIGURE 3). Similarly, tweets related to the representation of diverse races and the LGBTQIA+ community each comprised 26% of the total representation-based tweets. In terms of popularity as described above, 51.4% of tweets describing racial representation earned >1,000 likes (FIGURE 4).
Tweet demographics. Seven (7/131; 5.3%) of the tweet authors were verified Twitter users and 35 (35/131; 26.7%) authors reported working in the health care field within their Twitter profile description.
Continue to: Implementing our feedback can enhance patient experience and care...
Implementing our feedback can enhance patient experience and care
Our study provides a unique view of the patient perspective through analyzed crowdsourced public opinion via Twitter. To our knowledge, an optimized patient-centered outpatient gynecology experience has not previously been described in the medical literature. Optimizing the found domains of hospitality, comfort measures, pain and anxiety control, privacy, and diverse representationin the outpatient gynecologic experience within the outpatient care setting may ultimately result in improved patient satisfaction, patient well-being, and adherence to care through maximizing patient-centered care. We created a checklist of suggestions, including offering analgesics during office-based procedures and tailoring the floorplan to maximize privacy (FIGURE 5), for improving the outpatient gynecology experience based on our findings.
Prior data on patient satisfaction and outcomes
Improving patient satisfaction with health care is a priority for both clinicians and hospital systems. Prior studies have revealed only variable associations between patient satisfaction, safety, and clinical outcomes. One study involving the analysis of clinical and operational data from 171 hospitals found that hospital size, surgical volume, and low mortality rates were associated with higher patient satisfaction, while favorable surgical outcomes did not consistently correlate with higher Hospital Consumer Assessment of Healthcare Provers and Systems (HCAHPS) scores.10 Smaller, lower-volume hospitals earned higher satisfaction scores related to cleanliness, quietness, and receiving help measures.10 It has also been shown that the strongest predictors of patient satisfaction with the hospital childbirth experience included items related to staff communication, compassion, empathy, and respect.11 These data suggest that patient satisfaction is likely more significantly impacted by factors other than patient safety and effectiveness, and this was supported by the findings of our analysis. The growing body of literature associating a sense of psychological and physical safety within the health care system and improved patient outcomes and experience suggests that the data gathered from public commentary such as that presented here is extremely important for galvanizing change within the US health care system.
In one systematic review, the relationship between patient-centered care and clinical outcomes was mixed, although generally the association was positive.12 Additionally, patient-centered care was often associated with increased patient satisfaction and well-being. Some studies suggest that patient well-being and satisfaction also may be associated with improved adherence and self-management behaviors.12,13 Overall, optimizing patient-centered care may lead to improved patient satisfaction and potentially improved clinical outcomes.
Additionally, increasing diverse representation in patient materials and illustrations may help to improve the patient experience. Louie and colleagues found that dark skin tones were represented in only 4.5% of 4,146 images from anatomy texts analyzed in 2018.14 Similarly, a photogrammetric analysis of medical images utilized in New England Journal of Medicine found that only 18% of images depicted non-white skin.15 More recent efforts to create a royalty-free digital gallery of images reflecting bodies with diverse skin tones, body shapes, body hair, and age as well as transgender and nonbinary people have been discussed in the lay press.9 Based on our findings, social media users value and are actively seeking diversity in representation and imagery during their outpatient gynecology experience.
Opportunities for future study
Our research utilized social media as a diverse and accessible source of information; however, there are significant opportunities to refine the methodologic approach to answering the fundamental question of creating the patient-centered gynecologic experience. This type of study has not yet been conducted; however, the richness of the information from this current analysis could be informative to survey creation. Future research on this subject outside of social media could bolster the generalizability of our conclusions and the ability to report on qualitative findings in the setting of known patient demographics.
Social media remains a powerful tool as evidenced by this study, and continued use and observation of trending themes among patients is essential. The influence of social media will remain important for answering questions in gynecology and beyond.
Our work is strengthened by social media’s low threshold for use and the ability for widespread access to a diverse group of users. Additionally, social media allows for many responses to be collected in a timely manner, giving strength to the abstracted themes. The constant production of data by X users and their accessibility provide the opportunity for greater geographic coverage in those surveyed.4 Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of likes and retweets that may provide a reliable measure of public support or engagement.1
Future studies should examine ways to implement the suggested improvements to the office setting in a cost-effective manner and follow both subjective patient-reported outcomes as well as objective data after implementation, as these changes may have implications for much broader public health crises, such as maternal morbidity and mortality.
Study limitations. Our study is limited by the inherent biases and confounders associated with utilizing data derived from social media. Specifically, not all patients who seek outpatient gynecologic care utilize social media and/or X; using a “like” as a surrogate for endorsement of an idea by an identified party limits the generalizability of the data.
The initial Twitter query specified, “I’m asking women”, which may have altered the intended study population, influenced the analysis, and affected the representativeness of the sample through utilizing non ̶inclusive language. While non-binary/transgender care and inclusivity emerged as a theme discussed with the tweets, it is unclear if this represents an independent theme or rather a reaction to the non–inclusive language within the original tweet. ●
The data abstracted was analyzed with Dedoose1 software using a convenience sample and a mixed-methods analysis. Utilizing X (formerly Twitter and referred here as such given the time the study was conducted) for crowdsourcing functions similarly to an open survey. In the absence of similar analyses, a modified Checklist for Reporting Results of Internet E-Surveys (CHERRIES) checklist was utilized to organize our approach.2
This analysis was comprised of information freely available in the public domain, and the study was classified as IRB exempt. Ethical considerations were made for the fact that this is open access information and participants can reasonably expect their responses to be viewed by the public.3 As this question was not originally intended for research purposes, there was not a formalized development, recruitment, or consent process. The survey was not advertised beyond the original posting on Twitter, and the organic interest that it generated online. No incentives were offered to participants, and all participation was voluntary. There is no mechanism on Twitter for respondents to edit their response, although responses can be deleted. Unique visitors or viewers beyond posted impressions in response to the original tweet could not be determined.
Twitter thread responses were reviewed, and all completed and posted responses to the original Twitter query with 100 or greater “likes” were included in the analysis. These tweets were abstracted from Twitter between December 17, 2021, and December 27, 2021. At the time of tweet abstraction, engagement metrics, including the numbers of likes, retweets, and replies, were recorded. Additionally, author characteristics were abstracted, including author verification status and association with health care, as described in their Twitter profile. Definition of an individual associated with health care was broad and included physicians, advanced practice providers, nurses, first responders, and allied health professionals.
A total of 131 tweets met inclusion criteria and were uploaded for analysis using Dedoose qualitative analytic software.1 Two authors independently utilized a qualitative analysis to code the isolated tweets and identify thematic patterns among them. Uploaded tweets were additionally coded based on ranges of likes: 100-500; 501-1,000; 1,001-1,999; and >2,000. Tweets were coded for author verification status and whether or not the author was associated with the health care field. Themes were identified and defined during the coding process and were shared between the two authors. A total of 18 themes were identified, with 1 theme having 4 subdivisions. Interrater reliability testing was performed using Dedoose1 software and resulted with a pooled Cohen’s Kappa of 0.63, indicating “good” agreement between authors, which is an adequate level of agreement per the Dedoose software guidelines.
References
1. Dedoose website. Accessed July 28, 2022. https://www .dedoose.com/
2. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet e-surveys (CHERRIES) [published correction appears in J Med Internet Res. 2012;14:e8. doi:10.2196/jmir.2042]. J Med Internet Res. 2004;6:e34. doi:10.2196/jmir.6.3.e34
3. Townsend L, Wallace C. Social media research: a guide to ethics [University of Glasgow Information for the Media website]. Accessed March 2, 2023. https://www.gla.ac.uk /media/Media_487729_smxx.pdf
There has been increasing awareness of a need for creating a more patient-centered experience with outpatient gynecology; however, very little data exist about what interventions are important to patients. Given social media’s ease of use and ability for widespread access to a diverse group of users, it has the potential to be a powerful tool for qualitative research questions without the difficulties of cost, transportation, transcription, etc. required of a focus group. Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of “likes” that, at scale, can provide a reliable measure of public support or engagement for a particular concept.1 Particularly for topics that are controversial or novel, X (formerly Twitter, and referred to as Twitter intermittently throughout this article based on the time the study was conducted), with 300 million monthly users,2 has become a popular tool for general and health care ̶ focused content and sentiment analysis.3,4 This study presents a qualitative analysis of themes from a crowdsourced request on Twitter to design the ideal outpatient gynecologic experience that subsequently went “viral”.5,6
When asked to design the optimized outpatient gynecology experience, social media users expressed:
- hospitality, comfort, and pain control as frequent themes
- preserving privacy and acknowledgement of voluntary nulliparity as frequent themes
- a desire for diverse imagery and representation related to race, LGBTQIA+ themes, age, and weight/body type within the office setting
- a call for a sense of psychological safety within gynecology
Why the need for our research question on patient-centered gyn care
While the body of literature on patient-centered health care has grown rapidly in recent years, a patient-centered outpatient gynecology experience has not yet been described in the medical literature.
Patient-centered office design, driven by cultural sensitivity, has been shown in other studies to be both appreciated by established patients and a viable business strategy to attract new patients.7 Topics such as pain control, trauma-informed care in gynecologyclinics,8 and diverse representation in patient materials and illustrations9 have been popular topics in medicine and in the lay press. Our primary aim in our research was to utilize feedback from the question posed to quantify and rank patient-centered interventions in a gynecology office. These themes and others that emerged in our analysis were used to suggest b
What we asked social media users. The survey query to social media users, “I have the opportunity to design my office from scratch. I’m asking women: How would you design/optimize a visit to the gynecologist’s office?” was crowd-sourced via Twitter on December 5, 2021.5 Given a robust response to the query, it provided an opportunity for a qualitative research study exploring social media users’ perspectives on optimizing outpatient gynecologic care, although the original question was not planned for research utilization.
What we found
By December 27, 2021, the original tweet had earned 9,411 likes; 2,143 retweets; and 3,400 replies. Of this group, we analyzed 131 tweets, all of which had 100 or greater likes on Twitter at the time of the review. The majority of analyzed tweets earned between 100 ̶ 500 likes (75/131; 57.3%), while 22.9% (30/131) had 501 ̶ 1,000 likes, 11.5% (15/131) had >2,000 likes, and 8.4% (11/131) had 1,001 ̶ 1,999 likes.
Identified themes within the tweets analyzed included: medical education, comfort improvements, continuity of care, disability accommodations/accessibility, economic accessibility, nonbinary/transgender care and inclusivity, general layout/floorplan, hospitality, aid for intimate partner violence, childcare accessibility, multi-disciplinary care access, pain/anxiety control, sensitivity toward pregnancy loss/fertility issues, privacy issues, professionalism, representation (subdivided into race, LGBTQIA+, age, and weight/body type), trauma-informed care, and acknowledgement of voluntary nulliparity/support for reproductive choices (TABLE 1). TABLE 2 lists examples of popular tweets by selected themes.
Frequent themes. The most frequently occurring themes within the 131 analyzed tweets (FIGURE 1) were:
- hospitality (77 occurrences)
- comfort improvements (75 occurrences)
- general layout/floorplan (75 occurrences)
- pain/anxiety control (55 occurrences)
- representation (53 occurrences).
Popular themes. Defined as those with more than 1,000 likes at the time of analysis (FIGURE 2), the most popular themes included:
- privacy issues (48.5% of related tweets with >1,000 likes)
- voluntary nulliparity (37.0% of related tweets with >1,000 likes)
- general layout/floorplan (33.4% of related tweets with >1,000 likes)
- representation (32.1% of related tweets with >1,000 likes)
- hospitality (31.3% of related tweets with >1,000 likes).
A sub-analysis of themes related to specific types of representation—race, LGBTQIA+, age, and weight/body type was performed. Tweets related to diverse weight/body type representation occurred most frequently (19 code occurrences; FIGURE 3). Similarly, tweets related to the representation of diverse races and the LGBTQIA+ community each comprised 26% of the total representation-based tweets. In terms of popularity as described above, 51.4% of tweets describing racial representation earned >1,000 likes (FIGURE 4).
Tweet demographics. Seven (7/131; 5.3%) of the tweet authors were verified Twitter users and 35 (35/131; 26.7%) authors reported working in the health care field within their Twitter profile description.
Continue to: Implementing our feedback can enhance patient experience and care...
Implementing our feedback can enhance patient experience and care
Our study provides a unique view of the patient perspective through analyzed crowdsourced public opinion via Twitter. To our knowledge, an optimized patient-centered outpatient gynecology experience has not previously been described in the medical literature. Optimizing the found domains of hospitality, comfort measures, pain and anxiety control, privacy, and diverse representationin the outpatient gynecologic experience within the outpatient care setting may ultimately result in improved patient satisfaction, patient well-being, and adherence to care through maximizing patient-centered care. We created a checklist of suggestions, including offering analgesics during office-based procedures and tailoring the floorplan to maximize privacy (FIGURE 5), for improving the outpatient gynecology experience based on our findings.
Prior data on patient satisfaction and outcomes
Improving patient satisfaction with health care is a priority for both clinicians and hospital systems. Prior studies have revealed only variable associations between patient satisfaction, safety, and clinical outcomes. One study involving the analysis of clinical and operational data from 171 hospitals found that hospital size, surgical volume, and low mortality rates were associated with higher patient satisfaction, while favorable surgical outcomes did not consistently correlate with higher Hospital Consumer Assessment of Healthcare Provers and Systems (HCAHPS) scores.10 Smaller, lower-volume hospitals earned higher satisfaction scores related to cleanliness, quietness, and receiving help measures.10 It has also been shown that the strongest predictors of patient satisfaction with the hospital childbirth experience included items related to staff communication, compassion, empathy, and respect.11 These data suggest that patient satisfaction is likely more significantly impacted by factors other than patient safety and effectiveness, and this was supported by the findings of our analysis. The growing body of literature associating a sense of psychological and physical safety within the health care system and improved patient outcomes and experience suggests that the data gathered from public commentary such as that presented here is extremely important for galvanizing change within the US health care system.
In one systematic review, the relationship between patient-centered care and clinical outcomes was mixed, although generally the association was positive.12 Additionally, patient-centered care was often associated with increased patient satisfaction and well-being. Some studies suggest that patient well-being and satisfaction also may be associated with improved adherence and self-management behaviors.12,13 Overall, optimizing patient-centered care may lead to improved patient satisfaction and potentially improved clinical outcomes.
Additionally, increasing diverse representation in patient materials and illustrations may help to improve the patient experience. Louie and colleagues found that dark skin tones were represented in only 4.5% of 4,146 images from anatomy texts analyzed in 2018.14 Similarly, a photogrammetric analysis of medical images utilized in New England Journal of Medicine found that only 18% of images depicted non-white skin.15 More recent efforts to create a royalty-free digital gallery of images reflecting bodies with diverse skin tones, body shapes, body hair, and age as well as transgender and nonbinary people have been discussed in the lay press.9 Based on our findings, social media users value and are actively seeking diversity in representation and imagery during their outpatient gynecology experience.
Opportunities for future study
Our research utilized social media as a diverse and accessible source of information; however, there are significant opportunities to refine the methodologic approach to answering the fundamental question of creating the patient-centered gynecologic experience. This type of study has not yet been conducted; however, the richness of the information from this current analysis could be informative to survey creation. Future research on this subject outside of social media could bolster the generalizability of our conclusions and the ability to report on qualitative findings in the setting of known patient demographics.
Social media remains a powerful tool as evidenced by this study, and continued use and observation of trending themes among patients is essential. The influence of social media will remain important for answering questions in gynecology and beyond.
Our work is strengthened by social media’s low threshold for use and the ability for widespread access to a diverse group of users. Additionally, social media allows for many responses to be collected in a timely manner, giving strength to the abstracted themes. The constant production of data by X users and their accessibility provide the opportunity for greater geographic coverage in those surveyed.4 Crowdsourced public opinion also has the advantage of producing qualitative metrics in the form of likes and retweets that may provide a reliable measure of public support or engagement.1
Future studies should examine ways to implement the suggested improvements to the office setting in a cost-effective manner and follow both subjective patient-reported outcomes as well as objective data after implementation, as these changes may have implications for much broader public health crises, such as maternal morbidity and mortality.
Study limitations. Our study is limited by the inherent biases and confounders associated with utilizing data derived from social media. Specifically, not all patients who seek outpatient gynecologic care utilize social media and/or X; using a “like” as a surrogate for endorsement of an idea by an identified party limits the generalizability of the data.
The initial Twitter query specified, “I’m asking women”, which may have altered the intended study population, influenced the analysis, and affected the representativeness of the sample through utilizing non ̶inclusive language. While non-binary/transgender care and inclusivity emerged as a theme discussed with the tweets, it is unclear if this represents an independent theme or rather a reaction to the non–inclusive language within the original tweet. ●
The data abstracted was analyzed with Dedoose1 software using a convenience sample and a mixed-methods analysis. Utilizing X (formerly Twitter and referred here as such given the time the study was conducted) for crowdsourcing functions similarly to an open survey. In the absence of similar analyses, a modified Checklist for Reporting Results of Internet E-Surveys (CHERRIES) checklist was utilized to organize our approach.2
This analysis was comprised of information freely available in the public domain, and the study was classified as IRB exempt. Ethical considerations were made for the fact that this is open access information and participants can reasonably expect their responses to be viewed by the public.3 As this question was not originally intended for research purposes, there was not a formalized development, recruitment, or consent process. The survey was not advertised beyond the original posting on Twitter, and the organic interest that it generated online. No incentives were offered to participants, and all participation was voluntary. There is no mechanism on Twitter for respondents to edit their response, although responses can be deleted. Unique visitors or viewers beyond posted impressions in response to the original tweet could not be determined.
Twitter thread responses were reviewed, and all completed and posted responses to the original Twitter query with 100 or greater “likes” were included in the analysis. These tweets were abstracted from Twitter between December 17, 2021, and December 27, 2021. At the time of tweet abstraction, engagement metrics, including the numbers of likes, retweets, and replies, were recorded. Additionally, author characteristics were abstracted, including author verification status and association with health care, as described in their Twitter profile. Definition of an individual associated with health care was broad and included physicians, advanced practice providers, nurses, first responders, and allied health professionals.
A total of 131 tweets met inclusion criteria and were uploaded for analysis using Dedoose qualitative analytic software.1 Two authors independently utilized a qualitative analysis to code the isolated tweets and identify thematic patterns among them. Uploaded tweets were additionally coded based on ranges of likes: 100-500; 501-1,000; 1,001-1,999; and >2,000. Tweets were coded for author verification status and whether or not the author was associated with the health care field. Themes were identified and defined during the coding process and were shared between the two authors. A total of 18 themes were identified, with 1 theme having 4 subdivisions. Interrater reliability testing was performed using Dedoose1 software and resulted with a pooled Cohen’s Kappa of 0.63, indicating “good” agreement between authors, which is an adequate level of agreement per the Dedoose software guidelines.
References
1. Dedoose website. Accessed July 28, 2022. https://www .dedoose.com/
2. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet e-surveys (CHERRIES) [published correction appears in J Med Internet Res. 2012;14:e8. doi:10.2196/jmir.2042]. J Med Internet Res. 2004;6:e34. doi:10.2196/jmir.6.3.e34
3. Townsend L, Wallace C. Social media research: a guide to ethics [University of Glasgow Information for the Media website]. Accessed March 2, 2023. https://www.gla.ac.uk /media/Media_487729_smxx.pdf
- Garvey MD, Samuel J, Pelaez A. Would you please like my tweet?! An artificially intelligent, generative probabilistic, and econometric based system design for popularity-driven tweet content generation. Decis Support Syst. 2021;144:113497. doi: 10.1016/j.dss.2021.113497
- Twitter Revenue and Usage Statistics (2023). Business of apps. Published August 10, 2023. Accessed September 19, 2023. https://www.businessofapps.com/data/twitter-statistics/
- Doan AE, Bogen KW, Higgins E. A content analysis of twitter backlash to Georgia’s abortion ban. Sex Reprod Healthc. 2022;31:100689. doi:10.1016/j.srhc.2021.100689
- Roberts H, Sadler J, Chapman L. The value of Twitter data for determining the emotional responses of people to urban green spaces: a case study and critical evaluation. Urban Stud. 2019;56:818-835. doi: 10.1177/0042098017748544
- Stewart R [@stuboo]. I have the opportunity to design my office from scratch. I’m asking women. How would you design/optimize a visit to the gynecologist’s office? problems frustrations solutions No detail is too small. If I’ve ever had a tweet worthy of virality, it’s this one. RT. Twitter. Published December 5, 2021. Accessed March 1, 2023. https://twitter .com/stuboo/status/1467522852664532994
- A gynecologist asked Twitter how he should redesign his office. The answers he got were about deeper health care issues. Fortune. Accessed March 2, 2023. https://fortune .com/2021/12/07/gynecologist-twitter-question/
- Anderson GD, Nelson-Becker C, Hannigan EV, et al. A patientcentered health care delivery system by a university obstetrics and gynecology department. Obstet Gynecol. 2005;105:205210. doi:10.1097/01.AOG.0000146288.28195.27
- Ades V, Wu SX, Rabinowitz E, et al. An integrated, traumainformed care model for female survivors of sexual violence: the engage, motivate, protect, organize, self-worth, educate, respect (EMPOWER) clinic. Obstet Gynecol. 2019;133:803809. doi:10.1097/AOG.0000000000003186
- Gordon D. Health equity comes to medical illustrations with launch of new image library. Forbes. Accessed March 2023. https://www.forbes.com/sites/debgordon/2022/05/11 /health-equity-comes-to-medical-illustrations-with-launch -of-new-image-library/
- Kennedy GD, Tevis SE, Kent KC. Is there a relationship between patient satisfaction and favorable outcomes? Ann Surg. 2014;260:592-600. doi:10.1097/SLA.0000000000000932
- Gregory KD, Korst LM, Saeb S, et al. Childbirth-specific patient-reported outcomes as predictors of hospital satisfaction. Am J Obstet Gynecol. 2019;220:201.e1-201.e19. doi:10.1016/j.ajog.2018.10.093
- Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70:351-379. doi:10.1177/1077558712465774
- Kahn KL, Schneider EC, Malin JL, et al. Patient-centered experiences in breast cancer: predicting long-term adherence to tamoxifen use. Med Care. 2007;45:431-439. doi:10.1097/01 .mlr.0000257193.10760.7
- Louie P, Wilkes R. Representations of race and skin tone in medical textbook imagery. Soc Sci Med. 2018;202:38-42. doi:10.1016/j.socscimed.2018.02.023
- Massie JP, Cho DY, Kneib CJ, et al. A picture of modern medicine: race and visual representation in medical literature. J Natl Med Assoc. 2021;113:88-94. doi:10.1016/j.jnma.2020.07.013
- Garvey MD, Samuel J, Pelaez A. Would you please like my tweet?! An artificially intelligent, generative probabilistic, and econometric based system design for popularity-driven tweet content generation. Decis Support Syst. 2021;144:113497. doi: 10.1016/j.dss.2021.113497
- Twitter Revenue and Usage Statistics (2023). Business of apps. Published August 10, 2023. Accessed September 19, 2023. https://www.businessofapps.com/data/twitter-statistics/
- Doan AE, Bogen KW, Higgins E. A content analysis of twitter backlash to Georgia’s abortion ban. Sex Reprod Healthc. 2022;31:100689. doi:10.1016/j.srhc.2021.100689
- Roberts H, Sadler J, Chapman L. The value of Twitter data for determining the emotional responses of people to urban green spaces: a case study and critical evaluation. Urban Stud. 2019;56:818-835. doi: 10.1177/0042098017748544
- Stewart R [@stuboo]. I have the opportunity to design my office from scratch. I’m asking women. How would you design/optimize a visit to the gynecologist’s office? problems frustrations solutions No detail is too small. If I’ve ever had a tweet worthy of virality, it’s this one. RT. Twitter. Published December 5, 2021. Accessed March 1, 2023. https://twitter .com/stuboo/status/1467522852664532994
- A gynecologist asked Twitter how he should redesign his office. The answers he got were about deeper health care issues. Fortune. Accessed March 2, 2023. https://fortune .com/2021/12/07/gynecologist-twitter-question/
- Anderson GD, Nelson-Becker C, Hannigan EV, et al. A patientcentered health care delivery system by a university obstetrics and gynecology department. Obstet Gynecol. 2005;105:205210. doi:10.1097/01.AOG.0000146288.28195.27
- Ades V, Wu SX, Rabinowitz E, et al. An integrated, traumainformed care model for female survivors of sexual violence: the engage, motivate, protect, organize, self-worth, educate, respect (EMPOWER) clinic. Obstet Gynecol. 2019;133:803809. doi:10.1097/AOG.0000000000003186
- Gordon D. Health equity comes to medical illustrations with launch of new image library. Forbes. Accessed March 2023. https://www.forbes.com/sites/debgordon/2022/05/11 /health-equity-comes-to-medical-illustrations-with-launch -of-new-image-library/
- Kennedy GD, Tevis SE, Kent KC. Is there a relationship between patient satisfaction and favorable outcomes? Ann Surg. 2014;260:592-600. doi:10.1097/SLA.0000000000000932
- Gregory KD, Korst LM, Saeb S, et al. Childbirth-specific patient-reported outcomes as predictors of hospital satisfaction. Am J Obstet Gynecol. 2019;220:201.e1-201.e19. doi:10.1016/j.ajog.2018.10.093
- Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70:351-379. doi:10.1177/1077558712465774
- Kahn KL, Schneider EC, Malin JL, et al. Patient-centered experiences in breast cancer: predicting long-term adherence to tamoxifen use. Med Care. 2007;45:431-439. doi:10.1097/01 .mlr.0000257193.10760.7
- Louie P, Wilkes R. Representations of race and skin tone in medical textbook imagery. Soc Sci Med. 2018;202:38-42. doi:10.1016/j.socscimed.2018.02.023
- Massie JP, Cho DY, Kneib CJ, et al. A picture of modern medicine: race and visual representation in medical literature. J Natl Med Assoc. 2021;113:88-94. doi:10.1016/j.jnma.2020.07.013
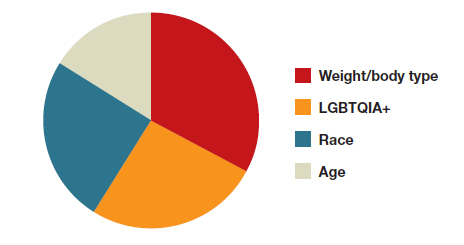
In-hospital mortality increased in COPD patients with acute exacerbations and high serum phosphate levels
found significantly higher in-hospital mortality among AECOPD patients with high serum phosphate levels. The finding, according to Siqi Li et al. in a preproof HELIYON article, suggests that hyperphosphatemia may be a high-risk factor for AECOPD-related in-hospital mortality.
Phosphorus is key to several physiological processes, among them energy metabolism, bone mineralization, membrane transport, and intracellular signaling. Li et al. pointed out that in patients with multiple diseases, hyperphosphatemia is associated with increased mortality. In the development of COPD specifically, acute exacerbations have been shown in several recent studies to be an important adverse event conferring heightened mortality risk. Despite many efforts, AECOPD mortality rates remain high, making identification of potential factors, Li et al. stated, crucial for improving outcomes in high-risk patients.
The electronic Intensive Care Unit Collaborative Research Database (eICU-CRD) holds data associated with over 200,000 patient stays, providing a large sample size for research studies. To determine the relationship between serum phosphate and in-hospital mortality in AECOPD patients, investigators analyzed data from a total of 1,199 AECOPD patients (mean age, 68 years; ~55% female) enrolled in eICU-CRD and divided them into three groups according to serum phosphate level tertiles: lowest tertile (serum phosphate ≤ 3.0 mg/dL, n = 445), median tertile (serum phosphate > 3.0 mg/dL and ≤ 4.0 mg/dL, n = 378), and highest tertile (serum phosphate > 4.0 mg/dL, n = 376). The Li et al. study’s primary outcome was all-cause in-hospital mortality, defined as survival to hospital discharge. Secondary outcomes included length of stay (LOS) in the intensive care unit (ICU), LOS in the hospital, and all-cause ICU mortality.
The Li et al. analysis of patient characteristics showed that patients in the highest tertile of serum phosphate had significantly higher body mass index (BMI) (P < .001), lower temperature (P < .001), lower heart rate (P < .001), lower mean arterial blood pressure (P = .011), higher creatinine (P < .001), higher potassium (P < .001), higher sequential organ failure assessment (SOFA) (P < .001), higher acute physiology and chronic health evaluation (APACHE IV) (P < .001), and higher ICU mortality (P < .001). Also, patients with higher serum phosphate levels were more likely to receive renal replacement therapy (RRT) (P < .001) and vasoactive drugs (P = .003) than those in the lower serum phosphate group. Such differences were also observed for age (P = .021), calcium level (P = .023), sodium level (P = .039), hypertension (P = .014), coronary artery disease (P = .004), diabetes (P = .017), and chronic kidney disease (P < .001). No significant differences were observed for gender, respiration rate, SpO2, white blood cell count, hemoglobin, platelets, cirrhosis, stroke, ventilation, LOS in ICU, and LOS in hospital (P > .05).
A univariate logistic regression analysis performed to determine the relationship between serum phosphate level and risk of in-hospital mortality revealed that higher serum phosphate level correlated with increased in-hospital mortality (odds ratio, 1.30; 95% confidence interval, 1.16-1.46; P < .001).
Li et al. posited that several mechanisms may explain increased mortality at higher serum phosphate levels in AECOPD patients: increased serum phosphate induces vascular calcification and endothelial dysfunction, leading to organ dysfunction; hyperphosphatemia causes oxidative stress, cell apoptosis, and inflammation, all of which are involved in the pathogenesis of AECOPD, and a higher phosphate diet exacerbates aging and lung emphysema phenotypes; restriction of phosphate intake and absorption relieves these phenotypes and alveolar destruction, which might contribute to the development of AECOPD.
Li et al. concluded: “Reducing serum phosphate levels may be a therapeutic strategy to improve prognosis of AECOPD patients.”
“This large retrospective analysis on eICU database in the U.S. revealed elevated serum phosphate levels with increased in-hospital mortality among patients experiencing acute exacerbation of COPD,” commented Dharani Narendra, MD, assistant professor in medicine, at Baylor College of Medicine, Houston. “This association, previously observed in various chronic conditions including COPD, particularly in men, is now noted to apply to both genders, irrespective of chronic kidney disease. The study also hints at potential mechanisms for elevated phosphate levels, such as inflammation, oxidative stress, and cell apoptosis in AECOPD, as well as a high-phosphate diet.”
She told this news organization also, “It remains imperative to ascertain whether treating hyperphosphatemia or implementing dietary phosphate restrictions can reduce mortality or prevent AECOPD episodes. These demand additional clinical trials to establish a definitive cause-and-effect relationship and to guide potential treatment and prevention strategies.”
Noting study limitations, Li et al. stated that many variables, such as smoking, exacerbation frequency, severity, PH, PaO2, PaCO2, and lactate, were not included in this study owing to more than 20% missing values.
This work was supported by the National Natural Science Foundation of China, Scientific Research Fund of Hunan Provincial Education Department, Hunan Provincial Natural Science Foundation, and Special fund for rehabilitation medicine of the National Clinical Research Center for Geriatric Disorders Clinical Research Fund. The authors declare no competing interests.
found significantly higher in-hospital mortality among AECOPD patients with high serum phosphate levels. The finding, according to Siqi Li et al. in a preproof HELIYON article, suggests that hyperphosphatemia may be a high-risk factor for AECOPD-related in-hospital mortality.
Phosphorus is key to several physiological processes, among them energy metabolism, bone mineralization, membrane transport, and intracellular signaling. Li et al. pointed out that in patients with multiple diseases, hyperphosphatemia is associated with increased mortality. In the development of COPD specifically, acute exacerbations have been shown in several recent studies to be an important adverse event conferring heightened mortality risk. Despite many efforts, AECOPD mortality rates remain high, making identification of potential factors, Li et al. stated, crucial for improving outcomes in high-risk patients.
The electronic Intensive Care Unit Collaborative Research Database (eICU-CRD) holds data associated with over 200,000 patient stays, providing a large sample size for research studies. To determine the relationship between serum phosphate and in-hospital mortality in AECOPD patients, investigators analyzed data from a total of 1,199 AECOPD patients (mean age, 68 years; ~55% female) enrolled in eICU-CRD and divided them into three groups according to serum phosphate level tertiles: lowest tertile (serum phosphate ≤ 3.0 mg/dL, n = 445), median tertile (serum phosphate > 3.0 mg/dL and ≤ 4.0 mg/dL, n = 378), and highest tertile (serum phosphate > 4.0 mg/dL, n = 376). The Li et al. study’s primary outcome was all-cause in-hospital mortality, defined as survival to hospital discharge. Secondary outcomes included length of stay (LOS) in the intensive care unit (ICU), LOS in the hospital, and all-cause ICU mortality.
The Li et al. analysis of patient characteristics showed that patients in the highest tertile of serum phosphate had significantly higher body mass index (BMI) (P < .001), lower temperature (P < .001), lower heart rate (P < .001), lower mean arterial blood pressure (P = .011), higher creatinine (P < .001), higher potassium (P < .001), higher sequential organ failure assessment (SOFA) (P < .001), higher acute physiology and chronic health evaluation (APACHE IV) (P < .001), and higher ICU mortality (P < .001). Also, patients with higher serum phosphate levels were more likely to receive renal replacement therapy (RRT) (P < .001) and vasoactive drugs (P = .003) than those in the lower serum phosphate group. Such differences were also observed for age (P = .021), calcium level (P = .023), sodium level (P = .039), hypertension (P = .014), coronary artery disease (P = .004), diabetes (P = .017), and chronic kidney disease (P < .001). No significant differences were observed for gender, respiration rate, SpO2, white blood cell count, hemoglobin, platelets, cirrhosis, stroke, ventilation, LOS in ICU, and LOS in hospital (P > .05).
A univariate logistic regression analysis performed to determine the relationship between serum phosphate level and risk of in-hospital mortality revealed that higher serum phosphate level correlated with increased in-hospital mortality (odds ratio, 1.30; 95% confidence interval, 1.16-1.46; P < .001).
Li et al. posited that several mechanisms may explain increased mortality at higher serum phosphate levels in AECOPD patients: increased serum phosphate induces vascular calcification and endothelial dysfunction, leading to organ dysfunction; hyperphosphatemia causes oxidative stress, cell apoptosis, and inflammation, all of which are involved in the pathogenesis of AECOPD, and a higher phosphate diet exacerbates aging and lung emphysema phenotypes; restriction of phosphate intake and absorption relieves these phenotypes and alveolar destruction, which might contribute to the development of AECOPD.
Li et al. concluded: “Reducing serum phosphate levels may be a therapeutic strategy to improve prognosis of AECOPD patients.”
“This large retrospective analysis on eICU database in the U.S. revealed elevated serum phosphate levels with increased in-hospital mortality among patients experiencing acute exacerbation of COPD,” commented Dharani Narendra, MD, assistant professor in medicine, at Baylor College of Medicine, Houston. “This association, previously observed in various chronic conditions including COPD, particularly in men, is now noted to apply to both genders, irrespective of chronic kidney disease. The study also hints at potential mechanisms for elevated phosphate levels, such as inflammation, oxidative stress, and cell apoptosis in AECOPD, as well as a high-phosphate diet.”
She told this news organization also, “It remains imperative to ascertain whether treating hyperphosphatemia or implementing dietary phosphate restrictions can reduce mortality or prevent AECOPD episodes. These demand additional clinical trials to establish a definitive cause-and-effect relationship and to guide potential treatment and prevention strategies.”
Noting study limitations, Li et al. stated that many variables, such as smoking, exacerbation frequency, severity, PH, PaO2, PaCO2, and lactate, were not included in this study owing to more than 20% missing values.
This work was supported by the National Natural Science Foundation of China, Scientific Research Fund of Hunan Provincial Education Department, Hunan Provincial Natural Science Foundation, and Special fund for rehabilitation medicine of the National Clinical Research Center for Geriatric Disorders Clinical Research Fund. The authors declare no competing interests.
found significantly higher in-hospital mortality among AECOPD patients with high serum phosphate levels. The finding, according to Siqi Li et al. in a preproof HELIYON article, suggests that hyperphosphatemia may be a high-risk factor for AECOPD-related in-hospital mortality.
Phosphorus is key to several physiological processes, among them energy metabolism, bone mineralization, membrane transport, and intracellular signaling. Li et al. pointed out that in patients with multiple diseases, hyperphosphatemia is associated with increased mortality. In the development of COPD specifically, acute exacerbations have been shown in several recent studies to be an important adverse event conferring heightened mortality risk. Despite many efforts, AECOPD mortality rates remain high, making identification of potential factors, Li et al. stated, crucial for improving outcomes in high-risk patients.
The electronic Intensive Care Unit Collaborative Research Database (eICU-CRD) holds data associated with over 200,000 patient stays, providing a large sample size for research studies. To determine the relationship between serum phosphate and in-hospital mortality in AECOPD patients, investigators analyzed data from a total of 1,199 AECOPD patients (mean age, 68 years; ~55% female) enrolled in eICU-CRD and divided them into three groups according to serum phosphate level tertiles: lowest tertile (serum phosphate ≤ 3.0 mg/dL, n = 445), median tertile (serum phosphate > 3.0 mg/dL and ≤ 4.0 mg/dL, n = 378), and highest tertile (serum phosphate > 4.0 mg/dL, n = 376). The Li et al. study’s primary outcome was all-cause in-hospital mortality, defined as survival to hospital discharge. Secondary outcomes included length of stay (LOS) in the intensive care unit (ICU), LOS in the hospital, and all-cause ICU mortality.
The Li et al. analysis of patient characteristics showed that patients in the highest tertile of serum phosphate had significantly higher body mass index (BMI) (P < .001), lower temperature (P < .001), lower heart rate (P < .001), lower mean arterial blood pressure (P = .011), higher creatinine (P < .001), higher potassium (P < .001), higher sequential organ failure assessment (SOFA) (P < .001), higher acute physiology and chronic health evaluation (APACHE IV) (P < .001), and higher ICU mortality (P < .001). Also, patients with higher serum phosphate levels were more likely to receive renal replacement therapy (RRT) (P < .001) and vasoactive drugs (P = .003) than those in the lower serum phosphate group. Such differences were also observed for age (P = .021), calcium level (P = .023), sodium level (P = .039), hypertension (P = .014), coronary artery disease (P = .004), diabetes (P = .017), and chronic kidney disease (P < .001). No significant differences were observed for gender, respiration rate, SpO2, white blood cell count, hemoglobin, platelets, cirrhosis, stroke, ventilation, LOS in ICU, and LOS in hospital (P > .05).
A univariate logistic regression analysis performed to determine the relationship between serum phosphate level and risk of in-hospital mortality revealed that higher serum phosphate level correlated with increased in-hospital mortality (odds ratio, 1.30; 95% confidence interval, 1.16-1.46; P < .001).
Li et al. posited that several mechanisms may explain increased mortality at higher serum phosphate levels in AECOPD patients: increased serum phosphate induces vascular calcification and endothelial dysfunction, leading to organ dysfunction; hyperphosphatemia causes oxidative stress, cell apoptosis, and inflammation, all of which are involved in the pathogenesis of AECOPD, and a higher phosphate diet exacerbates aging and lung emphysema phenotypes; restriction of phosphate intake and absorption relieves these phenotypes and alveolar destruction, which might contribute to the development of AECOPD.
Li et al. concluded: “Reducing serum phosphate levels may be a therapeutic strategy to improve prognosis of AECOPD patients.”
“This large retrospective analysis on eICU database in the U.S. revealed elevated serum phosphate levels with increased in-hospital mortality among patients experiencing acute exacerbation of COPD,” commented Dharani Narendra, MD, assistant professor in medicine, at Baylor College of Medicine, Houston. “This association, previously observed in various chronic conditions including COPD, particularly in men, is now noted to apply to both genders, irrespective of chronic kidney disease. The study also hints at potential mechanisms for elevated phosphate levels, such as inflammation, oxidative stress, and cell apoptosis in AECOPD, as well as a high-phosphate diet.”
She told this news organization also, “It remains imperative to ascertain whether treating hyperphosphatemia or implementing dietary phosphate restrictions can reduce mortality or prevent AECOPD episodes. These demand additional clinical trials to establish a definitive cause-and-effect relationship and to guide potential treatment and prevention strategies.”
Noting study limitations, Li et al. stated that many variables, such as smoking, exacerbation frequency, severity, PH, PaO2, PaCO2, and lactate, were not included in this study owing to more than 20% missing values.
This work was supported by the National Natural Science Foundation of China, Scientific Research Fund of Hunan Provincial Education Department, Hunan Provincial Natural Science Foundation, and Special fund for rehabilitation medicine of the National Clinical Research Center for Geriatric Disorders Clinical Research Fund. The authors declare no competing interests.
FROM HELIYON
Home oxygen therapy: What does the data show?
Inhalers, nebulizers, antibiotics, and steroids – these are some of the most common tools in our pulmonary arsenal that we deploy on a daily basis. But, there is no treatment more fundamental to a pulmonary practitioner than oxygen. So how is it that something that naturally occurs and comprises 21% of ambient air has become so medicalized?
It is difficult (perhaps impossible) to find a pulmonologist or a hospitalist who has not included the phrase “obtain ambulatory saturation to qualify the patient for home oxygen” in at least one of their progress notes on a daily basis. Chronic obstructive pulmonary disease (COPD) is the most common reason for the prescription of long-term oxygen therapy (LTOT), a large industry tightly regulated by the Centers for Medicare & Medicaid Services (CMS).
The evidence for the use of LTOT in patients with COPD dates back to two seminal papers published in 1980 and 1981. The British Medical Research Council Working Party conducted the BMRC trial, in which 87 patients with a Pa
Another study published around the same time, the Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease (NOTT) trial (Ann Intern Med. 1980;93[3]:391-8) directly compared continuous 24-hour to nocturnal home oxygen therapy in patients with COPD and severe hypoxemia with a Pa
Afterward, it became universally accepted dogma that patients with COPD and severe hypoxemia stood to substantially benefit from LTOT. For years, it was the only therapy associated with a mortality reduction. The LOTT study (Albert RK, et al. N Engl J Med. 2016;375[17]:1617-27) included 768 patients with stable COPD and a resting or nocturnal Sp
The INOX (Lacasse Y, et al. N Engl J Med. 2020;383[12]:1129-38) trial, in which 243 patients with oxygen saturation less than 90% for at least 30% of the night were assigned to receive nocturnal vs sham oxygen, found similar results. There was no difference in the composite outcome of all-cause mortality and progression to 24-7 oxygen requirement (according to the criteria originally defined by NOTT). A 2022 systematic review and meta-analysis including six studies designed to assess the role of LTOT in patients with COPD and moderate desaturation, including LOTT and INOX, found no benefit to providing LTOT (Lacasse Y, et al. Lancet Respir Med. 2022;10[11]:1029-37).
Based on these studies, a resting Sp
COPD management has changed significantly in the 40 years since NOTT was published. In the early 1980s, standard of care included an inhaled beta-agonist and oral theophylline. We now prescribe a regimen of modern-day inhaler combinations, which can lead to a mortality benefit in the correct population. Additionally, rates of smoking are markedly lower now than they were in 1980. In the Minnesota Heart Survey, the prevalence of being an ever-smoking man or woman in 1980 compared with 2009 dropped from 71.6% and 54.7% to 44.2% and 39.6%, respectively (Filion KB, et al. Am J Public Health. 2012;102[4]:705-13). Treatment of common comorbid conditions has also dramatically improved.
A report containing all fee-for-service data published in 2021 by CMS reported oxygen therapy accounted for 9.8% of all DME costs covered by CMS and totaled approximately $800,000,000 (Centers for Medicare & Medicaid Services. FFS Data. 2021. This represents a significant financial burden to our health system and government.
Two of the eligible groups per CMS (those with isolated ambulatory or nocturnal hypoxemia) do not benefit from LTOT in RCTs. The other two groups are eligible based on trial data from a small number of patients who were studied more than 40 years ago. These facts raise serious questions about the cost-efficacy of LTOT.
So where does this leave us?
There are significant barriers to repeating large randomized oxygen trials. Due to broad inclusion criteria for LTOT by CMS, there are undoubtedly many people prescribed LTOT for whom there is minimal to no benefit. Patients often feel restricted in their mobility and may feel isolated being tethered to medical equipment. It is good practice to think about LTOT the same way we do any other therapy we provide - as a medicine with associated risks, benefits, and costs.
Despite its ubiquity, oxygen remains an important therapeutic tool. Still, choosing wisely means recognizing that not all patients who qualify for LTOT by CMS criteria will benefit.
Drs. Kreisel and Sonti are with the Division of Pulmonary, Critical Care, and Sleep Medicine, MedStar Georgetown University Hospital, Washington, DC.
Inhalers, nebulizers, antibiotics, and steroids – these are some of the most common tools in our pulmonary arsenal that we deploy on a daily basis. But, there is no treatment more fundamental to a pulmonary practitioner than oxygen. So how is it that something that naturally occurs and comprises 21% of ambient air has become so medicalized?
It is difficult (perhaps impossible) to find a pulmonologist or a hospitalist who has not included the phrase “obtain ambulatory saturation to qualify the patient for home oxygen” in at least one of their progress notes on a daily basis. Chronic obstructive pulmonary disease (COPD) is the most common reason for the prescription of long-term oxygen therapy (LTOT), a large industry tightly regulated by the Centers for Medicare & Medicaid Services (CMS).
The evidence for the use of LTOT in patients with COPD dates back to two seminal papers published in 1980 and 1981. The British Medical Research Council Working Party conducted the BMRC trial, in which 87 patients with a Pa
Another study published around the same time, the Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease (NOTT) trial (Ann Intern Med. 1980;93[3]:391-8) directly compared continuous 24-hour to nocturnal home oxygen therapy in patients with COPD and severe hypoxemia with a Pa
Afterward, it became universally accepted dogma that patients with COPD and severe hypoxemia stood to substantially benefit from LTOT. For years, it was the only therapy associated with a mortality reduction. The LOTT study (Albert RK, et al. N Engl J Med. 2016;375[17]:1617-27) included 768 patients with stable COPD and a resting or nocturnal Sp
The INOX (Lacasse Y, et al. N Engl J Med. 2020;383[12]:1129-38) trial, in which 243 patients with oxygen saturation less than 90% for at least 30% of the night were assigned to receive nocturnal vs sham oxygen, found similar results. There was no difference in the composite outcome of all-cause mortality and progression to 24-7 oxygen requirement (according to the criteria originally defined by NOTT). A 2022 systematic review and meta-analysis including six studies designed to assess the role of LTOT in patients with COPD and moderate desaturation, including LOTT and INOX, found no benefit to providing LTOT (Lacasse Y, et al. Lancet Respir Med. 2022;10[11]:1029-37).
Based on these studies, a resting Sp
COPD management has changed significantly in the 40 years since NOTT was published. In the early 1980s, standard of care included an inhaled beta-agonist and oral theophylline. We now prescribe a regimen of modern-day inhaler combinations, which can lead to a mortality benefit in the correct population. Additionally, rates of smoking are markedly lower now than they were in 1980. In the Minnesota Heart Survey, the prevalence of being an ever-smoking man or woman in 1980 compared with 2009 dropped from 71.6% and 54.7% to 44.2% and 39.6%, respectively (Filion KB, et al. Am J Public Health. 2012;102[4]:705-13). Treatment of common comorbid conditions has also dramatically improved.
A report containing all fee-for-service data published in 2021 by CMS reported oxygen therapy accounted for 9.8% of all DME costs covered by CMS and totaled approximately $800,000,000 (Centers for Medicare & Medicaid Services. FFS Data. 2021. This represents a significant financial burden to our health system and government.
Two of the eligible groups per CMS (those with isolated ambulatory or nocturnal hypoxemia) do not benefit from LTOT in RCTs. The other two groups are eligible based on trial data from a small number of patients who were studied more than 40 years ago. These facts raise serious questions about the cost-efficacy of LTOT.
So where does this leave us?
There are significant barriers to repeating large randomized oxygen trials. Due to broad inclusion criteria for LTOT by CMS, there are undoubtedly many people prescribed LTOT for whom there is minimal to no benefit. Patients often feel restricted in their mobility and may feel isolated being tethered to medical equipment. It is good practice to think about LTOT the same way we do any other therapy we provide - as a medicine with associated risks, benefits, and costs.
Despite its ubiquity, oxygen remains an important therapeutic tool. Still, choosing wisely means recognizing that not all patients who qualify for LTOT by CMS criteria will benefit.
Drs. Kreisel and Sonti are with the Division of Pulmonary, Critical Care, and Sleep Medicine, MedStar Georgetown University Hospital, Washington, DC.
Inhalers, nebulizers, antibiotics, and steroids – these are some of the most common tools in our pulmonary arsenal that we deploy on a daily basis. But, there is no treatment more fundamental to a pulmonary practitioner than oxygen. So how is it that something that naturally occurs and comprises 21% of ambient air has become so medicalized?
It is difficult (perhaps impossible) to find a pulmonologist or a hospitalist who has not included the phrase “obtain ambulatory saturation to qualify the patient for home oxygen” in at least one of their progress notes on a daily basis. Chronic obstructive pulmonary disease (COPD) is the most common reason for the prescription of long-term oxygen therapy (LTOT), a large industry tightly regulated by the Centers for Medicare & Medicaid Services (CMS).
The evidence for the use of LTOT in patients with COPD dates back to two seminal papers published in 1980 and 1981. The British Medical Research Council Working Party conducted the BMRC trial, in which 87 patients with a Pa
Another study published around the same time, the Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease (NOTT) trial (Ann Intern Med. 1980;93[3]:391-8) directly compared continuous 24-hour to nocturnal home oxygen therapy in patients with COPD and severe hypoxemia with a Pa
Afterward, it became universally accepted dogma that patients with COPD and severe hypoxemia stood to substantially benefit from LTOT. For years, it was the only therapy associated with a mortality reduction. The LOTT study (Albert RK, et al. N Engl J Med. 2016;375[17]:1617-27) included 768 patients with stable COPD and a resting or nocturnal Sp
The INOX (Lacasse Y, et al. N Engl J Med. 2020;383[12]:1129-38) trial, in which 243 patients with oxygen saturation less than 90% for at least 30% of the night were assigned to receive nocturnal vs sham oxygen, found similar results. There was no difference in the composite outcome of all-cause mortality and progression to 24-7 oxygen requirement (according to the criteria originally defined by NOTT). A 2022 systematic review and meta-analysis including six studies designed to assess the role of LTOT in patients with COPD and moderate desaturation, including LOTT and INOX, found no benefit to providing LTOT (Lacasse Y, et al. Lancet Respir Med. 2022;10[11]:1029-37).
Based on these studies, a resting Sp
COPD management has changed significantly in the 40 years since NOTT was published. In the early 1980s, standard of care included an inhaled beta-agonist and oral theophylline. We now prescribe a regimen of modern-day inhaler combinations, which can lead to a mortality benefit in the correct population. Additionally, rates of smoking are markedly lower now than they were in 1980. In the Minnesota Heart Survey, the prevalence of being an ever-smoking man or woman in 1980 compared with 2009 dropped from 71.6% and 54.7% to 44.2% and 39.6%, respectively (Filion KB, et al. Am J Public Health. 2012;102[4]:705-13). Treatment of common comorbid conditions has also dramatically improved.
A report containing all fee-for-service data published in 2021 by CMS reported oxygen therapy accounted for 9.8% of all DME costs covered by CMS and totaled approximately $800,000,000 (Centers for Medicare & Medicaid Services. FFS Data. 2021. This represents a significant financial burden to our health system and government.
Two of the eligible groups per CMS (those with isolated ambulatory or nocturnal hypoxemia) do not benefit from LTOT in RCTs. The other two groups are eligible based on trial data from a small number of patients who were studied more than 40 years ago. These facts raise serious questions about the cost-efficacy of LTOT.
So where does this leave us?
There are significant barriers to repeating large randomized oxygen trials. Due to broad inclusion criteria for LTOT by CMS, there are undoubtedly many people prescribed LTOT for whom there is minimal to no benefit. Patients often feel restricted in their mobility and may feel isolated being tethered to medical equipment. It is good practice to think about LTOT the same way we do any other therapy we provide - as a medicine with associated risks, benefits, and costs.
Despite its ubiquity, oxygen remains an important therapeutic tool. Still, choosing wisely means recognizing that not all patients who qualify for LTOT by CMS criteria will benefit.
Drs. Kreisel and Sonti are with the Division of Pulmonary, Critical Care, and Sleep Medicine, MedStar Georgetown University Hospital, Washington, DC.
Wastewater can signal upswing in flu, RSV
according to new research reported at an annual scientific meeting on infectious diseases.
The analysis of wastewater in Calgary (Alta.) found a “positive correlation” between positivity rates for these three viruses in wastewater and weekly laboratory-confirmed clinical cases and test positivity rates, study investigator Kristine Du, with Cumming School of Medicine, University of Calgary, told this news organization.
Wastewater monitoring of viral activity has become an established tool for COVID-19 pandemic monitoring, providing a leading indicator to cases and hospitalizations. However, less is known about its potential for monitoring endemic respiratory viruses.
The new study shows that wastewater-based surveillance is a “robust and adaptable” tool for community-level surveillance of seasonal respiratory viruses – “one that can complement health care clinical testing because it’s independent from testing biases, and we can actually correlate our cases very well with it,” Ms. Du said during a preconference media briefing.
Tracking community trends
For the study, Ms. Du and colleagues assessed the occurrence of influenza A, influenza B, and RSV RNA in all three wastewater treatment plants in Calgary between March 2022 and April 2023 and its correlation with clinical disease.
They found that viral signals in Calgary’s wastewater for influenza A and B and RSV correlated significantly with weekly confirmed clinical cases in Calgary residents.
Influenza A peaked in Calgary’s wastewater between November and December 2022; influenza B peaked between February and April 2023; and RSV between November 2022 and February 2023.
“Wastewater gives us unbiased, objective, and comprehensive data. It can be used in addition to other testing for assessing the community burden that disease may have, and it is complementary to clinical testing,” Ms. Du said.
Their team, Ms. Du said, is continuing to proactively monitor wastewater for influenza and RSV, as well as other agents of “pandemic potential to make sure we know what could affect humans – and make sure everyone is aware of that.”
Commenting on the research, briefing moderator Belinda Ostrowsky, MD, MPH, Albert Einstein College of Medicine, New York, said, “Wastewater surveillance illustrates how understanding community levels of viral trends can identify hotspots, inform local public health decision-making, and prepare clinicians and hospitals for potential outreach. This topic is particularly timely as we head into the flu and RSV season.”
The study had no commercial funding. Ms. Du and Dr. Ostrowsky report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new research reported at an annual scientific meeting on infectious diseases.
The analysis of wastewater in Calgary (Alta.) found a “positive correlation” between positivity rates for these three viruses in wastewater and weekly laboratory-confirmed clinical cases and test positivity rates, study investigator Kristine Du, with Cumming School of Medicine, University of Calgary, told this news organization.
Wastewater monitoring of viral activity has become an established tool for COVID-19 pandemic monitoring, providing a leading indicator to cases and hospitalizations. However, less is known about its potential for monitoring endemic respiratory viruses.
The new study shows that wastewater-based surveillance is a “robust and adaptable” tool for community-level surveillance of seasonal respiratory viruses – “one that can complement health care clinical testing because it’s independent from testing biases, and we can actually correlate our cases very well with it,” Ms. Du said during a preconference media briefing.
Tracking community trends
For the study, Ms. Du and colleagues assessed the occurrence of influenza A, influenza B, and RSV RNA in all three wastewater treatment plants in Calgary between March 2022 and April 2023 and its correlation with clinical disease.
They found that viral signals in Calgary’s wastewater for influenza A and B and RSV correlated significantly with weekly confirmed clinical cases in Calgary residents.
Influenza A peaked in Calgary’s wastewater between November and December 2022; influenza B peaked between February and April 2023; and RSV between November 2022 and February 2023.
“Wastewater gives us unbiased, objective, and comprehensive data. It can be used in addition to other testing for assessing the community burden that disease may have, and it is complementary to clinical testing,” Ms. Du said.
Their team, Ms. Du said, is continuing to proactively monitor wastewater for influenza and RSV, as well as other agents of “pandemic potential to make sure we know what could affect humans – and make sure everyone is aware of that.”
Commenting on the research, briefing moderator Belinda Ostrowsky, MD, MPH, Albert Einstein College of Medicine, New York, said, “Wastewater surveillance illustrates how understanding community levels of viral trends can identify hotspots, inform local public health decision-making, and prepare clinicians and hospitals for potential outreach. This topic is particularly timely as we head into the flu and RSV season.”
The study had no commercial funding. Ms. Du and Dr. Ostrowsky report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new research reported at an annual scientific meeting on infectious diseases.
The analysis of wastewater in Calgary (Alta.) found a “positive correlation” between positivity rates for these three viruses in wastewater and weekly laboratory-confirmed clinical cases and test positivity rates, study investigator Kristine Du, with Cumming School of Medicine, University of Calgary, told this news organization.
Wastewater monitoring of viral activity has become an established tool for COVID-19 pandemic monitoring, providing a leading indicator to cases and hospitalizations. However, less is known about its potential for monitoring endemic respiratory viruses.
The new study shows that wastewater-based surveillance is a “robust and adaptable” tool for community-level surveillance of seasonal respiratory viruses – “one that can complement health care clinical testing because it’s independent from testing biases, and we can actually correlate our cases very well with it,” Ms. Du said during a preconference media briefing.
Tracking community trends
For the study, Ms. Du and colleagues assessed the occurrence of influenza A, influenza B, and RSV RNA in all three wastewater treatment plants in Calgary between March 2022 and April 2023 and its correlation with clinical disease.
They found that viral signals in Calgary’s wastewater for influenza A and B and RSV correlated significantly with weekly confirmed clinical cases in Calgary residents.
Influenza A peaked in Calgary’s wastewater between November and December 2022; influenza B peaked between February and April 2023; and RSV between November 2022 and February 2023.
“Wastewater gives us unbiased, objective, and comprehensive data. It can be used in addition to other testing for assessing the community burden that disease may have, and it is complementary to clinical testing,” Ms. Du said.
Their team, Ms. Du said, is continuing to proactively monitor wastewater for influenza and RSV, as well as other agents of “pandemic potential to make sure we know what could affect humans – and make sure everyone is aware of that.”
Commenting on the research, briefing moderator Belinda Ostrowsky, MD, MPH, Albert Einstein College of Medicine, New York, said, “Wastewater surveillance illustrates how understanding community levels of viral trends can identify hotspots, inform local public health decision-making, and prepare clinicians and hospitals for potential outreach. This topic is particularly timely as we head into the flu and RSV season.”
The study had no commercial funding. Ms. Du and Dr. Ostrowsky report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM IDWEEK 2023
Highlights of the 2024 Medicare Physician Fee Schedule proposed rule
The suggested Medicare Physician Fee Schedule for calendar year (CY) 2024 was announced by the Centers for Medicare & Medicaid Services (CMS) in July 2023. Physicians who specialize in pulmonary, critical care, and sleep medicine will be impacted by a number of policy and payment changes. Additionally, keep in mind that this is the proposed rule. Following are some of the key points for our readers:
1. The conversion factor that CMS is suggesting for 2024 is $32.75, which represents a $1.14 (–3.34%) reduction. The current conversion factor is $33.89. This is specifically meant to lower total Medicare spending.
2. It is forecast that pulmonary specialists will experience an estimated 1.09% reduction in Medicare reimbursements if the proposed changes are approved. Medicare reimbursements for critical care specialists will be reduced by 2.51%, and sleep medicine specialists will be seeing a 0.75% increase.
3. Interestingly, CMS is proposing a Healthcare Common Procedure Coding System (HCPCS) code G2211 that will have a distinct add-on payment starting on January 1, 2024. With the help of this add-on code, the resource costs of evaluation and management visits for primary care and long-term treatment of difficult patients will be more accurately recognized. In general, it will be used as an additional payment for outpatient office visits in recognition of the potential expenditures that doctors may face when treating a patient’s single, significant, or complex chronic condition over time. Payment for this add-on code would have a redistributive impact on all other CY 2024 payments, which are still lower than what was previously predicted for this policy in CY 2021 under the Medicare Physician Fee Schedule, which was not implemented at the request of various surgical specialties.
4. As you all are aware, split (or shared) E/M visits in hospitals and other institutional settings are those that are provided in part by doctors and in part by other practitioners of the same specialty but billed under a single provider. Thankfully CMS is recommending delaying the application of the “substantive portion” definition of more than 50% of the total period to at least December 31, 2024. Instead, they are going to keep the present definition of the “substantive portion” for CY 2024, which permits use of either more than half of the visit’s total time or one of the three major components (history, exam, or MDM) to determine who bills the visit. Please remember that Critical Care services (99291/99292) may also be shared or split; however, in this case, billing is based only on time.
5. According to CMS’s current regulatory stance, teaching physicians have to be physically present to charge for services involving residents at the end of the COVID-19 Public Health Emergency. Congress, on the other hand, stepped in and passed legislation to expand Medicare coverage of a number of telehealth services. In accordance with the expanded telehealth policies adopted by Congress, CMS is recommending that teaching physicians be permitted to employ audio/video real-time communications technology when the resident physician provides telehealth services to Medicare beneficiaries for CY 2024.
The CMS’s document is fairly comprehensive, so please visit this link for more information
The suggested Medicare Physician Fee Schedule for calendar year (CY) 2024 was announced by the Centers for Medicare & Medicaid Services (CMS) in July 2023. Physicians who specialize in pulmonary, critical care, and sleep medicine will be impacted by a number of policy and payment changes. Additionally, keep in mind that this is the proposed rule. Following are some of the key points for our readers:
1. The conversion factor that CMS is suggesting for 2024 is $32.75, which represents a $1.14 (–3.34%) reduction. The current conversion factor is $33.89. This is specifically meant to lower total Medicare spending.
2. It is forecast that pulmonary specialists will experience an estimated 1.09% reduction in Medicare reimbursements if the proposed changes are approved. Medicare reimbursements for critical care specialists will be reduced by 2.51%, and sleep medicine specialists will be seeing a 0.75% increase.
3. Interestingly, CMS is proposing a Healthcare Common Procedure Coding System (HCPCS) code G2211 that will have a distinct add-on payment starting on January 1, 2024. With the help of this add-on code, the resource costs of evaluation and management visits for primary care and long-term treatment of difficult patients will be more accurately recognized. In general, it will be used as an additional payment for outpatient office visits in recognition of the potential expenditures that doctors may face when treating a patient’s single, significant, or complex chronic condition over time. Payment for this add-on code would have a redistributive impact on all other CY 2024 payments, which are still lower than what was previously predicted for this policy in CY 2021 under the Medicare Physician Fee Schedule, which was not implemented at the request of various surgical specialties.
4. As you all are aware, split (or shared) E/M visits in hospitals and other institutional settings are those that are provided in part by doctors and in part by other practitioners of the same specialty but billed under a single provider. Thankfully CMS is recommending delaying the application of the “substantive portion” definition of more than 50% of the total period to at least December 31, 2024. Instead, they are going to keep the present definition of the “substantive portion” for CY 2024, which permits use of either more than half of the visit’s total time or one of the three major components (history, exam, or MDM) to determine who bills the visit. Please remember that Critical Care services (99291/99292) may also be shared or split; however, in this case, billing is based only on time.
5. According to CMS’s current regulatory stance, teaching physicians have to be physically present to charge for services involving residents at the end of the COVID-19 Public Health Emergency. Congress, on the other hand, stepped in and passed legislation to expand Medicare coverage of a number of telehealth services. In accordance with the expanded telehealth policies adopted by Congress, CMS is recommending that teaching physicians be permitted to employ audio/video real-time communications technology when the resident physician provides telehealth services to Medicare beneficiaries for CY 2024.
The CMS’s document is fairly comprehensive, so please visit this link for more information
The suggested Medicare Physician Fee Schedule for calendar year (CY) 2024 was announced by the Centers for Medicare & Medicaid Services (CMS) in July 2023. Physicians who specialize in pulmonary, critical care, and sleep medicine will be impacted by a number of policy and payment changes. Additionally, keep in mind that this is the proposed rule. Following are some of the key points for our readers:
1. The conversion factor that CMS is suggesting for 2024 is $32.75, which represents a $1.14 (–3.34%) reduction. The current conversion factor is $33.89. This is specifically meant to lower total Medicare spending.
2. It is forecast that pulmonary specialists will experience an estimated 1.09% reduction in Medicare reimbursements if the proposed changes are approved. Medicare reimbursements for critical care specialists will be reduced by 2.51%, and sleep medicine specialists will be seeing a 0.75% increase.
3. Interestingly, CMS is proposing a Healthcare Common Procedure Coding System (HCPCS) code G2211 that will have a distinct add-on payment starting on January 1, 2024. With the help of this add-on code, the resource costs of evaluation and management visits for primary care and long-term treatment of difficult patients will be more accurately recognized. In general, it will be used as an additional payment for outpatient office visits in recognition of the potential expenditures that doctors may face when treating a patient’s single, significant, or complex chronic condition over time. Payment for this add-on code would have a redistributive impact on all other CY 2024 payments, which are still lower than what was previously predicted for this policy in CY 2021 under the Medicare Physician Fee Schedule, which was not implemented at the request of various surgical specialties.
4. As you all are aware, split (or shared) E/M visits in hospitals and other institutional settings are those that are provided in part by doctors and in part by other practitioners of the same specialty but billed under a single provider. Thankfully CMS is recommending delaying the application of the “substantive portion” definition of more than 50% of the total period to at least December 31, 2024. Instead, they are going to keep the present definition of the “substantive portion” for CY 2024, which permits use of either more than half of the visit’s total time or one of the three major components (history, exam, or MDM) to determine who bills the visit. Please remember that Critical Care services (99291/99292) may also be shared or split; however, in this case, billing is based only on time.
5. According to CMS’s current regulatory stance, teaching physicians have to be physically present to charge for services involving residents at the end of the COVID-19 Public Health Emergency. Congress, on the other hand, stepped in and passed legislation to expand Medicare coverage of a number of telehealth services. In accordance with the expanded telehealth policies adopted by Congress, CMS is recommending that teaching physicians be permitted to employ audio/video real-time communications technology when the resident physician provides telehealth services to Medicare beneficiaries for CY 2024.
The CMS’s document is fairly comprehensive, so please visit this link for more information
Pragmatic solutions to ‘catastrophic’ global stroke burden
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
FROM THE LANCET NEUROLOGY