User login
U.S. okay looms for third drug-coated PAD balloon
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.
The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.
The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.
So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.
So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.
So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.
The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.
The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.
The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.
The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Key clinical point:
Major finding: The primary efficacy endpoint occurred in 76% of patients in the drug-coated balloon arm and 58% of controls.
Data source: The ILLUMENATE pivotal trial, which enrolled 300 patients at 63 U.S. and European centers.
Disclosures: The ILLUMENATE pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
Thyme
Native to the western Mediterranean, Thymus vulgaris (one of approximately 300 Thymus species) is a small bush used for centuries as a spice and in medicine, particularly to treat bronchitis.1Thymus species are among the wild and cultivated species used in traditional medicine in Bosnia and Herzegovina for various indications, including skin disorders.2 Thyme essential oil is a natural compound generally recognized as safe by the Food and Drug Administration, with demonstrated antibacterial, antifungal, and antispasmodic activities.3,4 Several other biologic activities have been associated with the polyphenol-rich herb, many of which have dermatologic implications. Notably, the essential oil of thyme and thymol, a key constituent of thyme, are known to act as skin sensitizers and allergens.5
Photoprotective activity
Recently, Sun et al. showed that UVB-induced skin damage was attenuated by treating hairless mice (HR-1) with T. vulgaris, as indicated by reduced matrix metalloproteinases and elevated collagen synthesis. In cultured normal human dermal fibroblasts, the investigators found that T. vulgaris blocked UVB-induced reactive oxygen species and lactate dehydrogenase, and dose-dependently yielded increases in glutathione, NAD(P)H: quinone oxidoreductase 1, and heme oxygenase-1. Further, the botanical significantly reduced UVB-induced phosphorylation of mitogen-activated protein kinases. The investigators concluded that T. vulgaris has potential for use in preventing skin damage caused by UV radiation–induced oxidative stress.6
Thyme also was demonstrated by Cornaghi et al. in 2016 to exert a protective effect on normal human skin explants obtained from seven young healthy women that were treated 1 hour before UVB irradiation.7
In 2015, Calò et al. evaluated the protective effects of a dry extract from T. vulgaris and its primary synthetic constituent thymol against UVA- and UVB-induced oxidative and genotoxic damage in the keratinocyte cell line NCTC 2544. Both thymol and T. vulgaris suppressed reactive oxygen species production in UVA- and UVB-treated cells, but lowered malondialdehyde synthesis only in cells treated with UVA.8
Antioxidant activity
In 2007, Wei and Shibamoto reported that thyme essential oil mixed with clove oil exhibited over a 90% inhibitory effect against the formation of malondialdehyde. They speculated that the presence of thymol and eugenol might account for the strong antioxidant activity displayed by the thyme/clove leaf combination.9 The investigators previously observed antioxidant activities exhibited by volatile extracts isolated from thyme (as well as various other herbs and spices) using aldehyde/carboxylic acid as well as conjugated diene assays.10 The antioxidant activity of thyme also was demonstrated by Miura et al. using the oil stability index method.11
Antimicrobial activity
In 2011, Sienkiewicz et al. reported that the oil of T. vulgaris displayed potent activity against clinical bacterial strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas genera. In addition, thyme essential oil exhibited efficacy against tested antibiotic-resistant strains of bacteria.12 The following year, Sienkiewicz et al. assessed the antimicrobial activity of thyme essential oil against clinical multidrug-resistant strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas, finding that it potently suppressed the growth of each.13
Potential cutaneous indications: atopic dermatitis, leishmaniasis, eczema, hair growth
In 2015, Seo and Jeong showed that lavender oil, thyme oil, and a blend of the two were all effective in reducing the symptoms of atopic dermatitis in mice. The researchers suggested that developing treatments with these oils for human patients with atopic dermatitis is warranted.14
Nilforoushzadeh et al. found in 2008 that herbal extracts of T. vulgaris and Achillea millefolium (yarrow), as well as propolis hydroalcoholic extracts, were effective in treating cutaneous leishmaniasis in mice and recommended the study of these extracts alone or in combination in human trials.15
A two-arm, randomized, double-blind, placebo-controlled trial conducted by Shimelis et al. in 2012 evaluated the efficacy of a 3% thyme essential oil antifungal cream and a 10% chamomile extract cream in the treatment of eczemalike lesions. Complete healing was achieved in 10 patients (66.5%) treated with the thyme cream, compared with four patients (28.5%) in the placebo group. Although no significant differences were observed between the active chamomile group and placebo, an appreciable number of subjects improved or healed. The investigators concluded that their findings from this small study suggest that, while more research is needed, a 3% thyme essential oil cream appears to be an inexpensive and readily available option to treat mild to moderate cutaneous conditions, including fungal infections, pityriasis alba, and eczema.16
In 2013, Rastegar et al. found that the combination of herbal extracts (including thyme) and platelet-rich plasma induced significant proliferation of human dermal papilla cells by regulating extracellular signal-regulated kinase (ERK) and Akt (protein kinase B). They concluded that their findings suggest the potential for developing combination therapies intended to improve hair growth.17
Insect repellent activity
In a 2016 study by Gutiérrez et al., the essential oil of T. vulgaris was found to be effective against Pediculus humanus capitis (head lice) adults and eggs. The researchers concluded that T. vulgaris achieves a strong knockdown and mortality rate in adult head lice and toxicity in the eggs after 21 minutes of application at a low concentration.18
In a small 1999 study by Barnard of the repellency to Aedes aegypti and Anopheles albimanus of various concentrations and combinations of five essential oils (Bourbon geranium, cedarwood, clove, peppermint, and thyme) applied to human skin, thyme and clove oils were found to be the most effective mosquito repellents. The author noted that thyme oil (as well as clove and peppermint oils) can irritate the skin and the odor of thyme and clove oils, at concentrations of 25%, or more were deemed unacceptable by the two participants in the study.19
Three years later, Choi et al. found that the essential oil of T. vulgaris also repelled adult mosquitoes (Culex pipiens pallens) on hairless mice and displayed potent repellent activity.20
Melanoma
In 2005, Carrera et al. reported a case of long-term complete remission of cutaneous melanoma metastases in a 73-year-old white woman who consumed a dried thyme herbal tea and thyme topical applications in compresses.4 An association between thyme and melanoma has not been reported in the subsequent literature.
Conclusion
Thyme has a long history of culinary and medical uses. Its antimicrobial and antioxidant activity are well documented. While there is reason to consider the potential applications of thyme for dermatologic conditions, much more research is necessary to determine its viability for such purposes.
References
1. An Illustrated Guide to 101 Medicinal Herbs: Their History, Use, Recommended Dosages, and Cautions (Loveland, Colo.: Interweave Press, 1998, pp. 198-9).
2. J Ethnopharmacol. 2010 Aug 19;131(1):33-55.
3. J Food Sci. 2014 May;79(5):M903-10.
4. J Am Acad Dermatol. 2005 Apr;52(4):713-5.
5. Nat Neurosci. 2006 May;9(5):628-35.
6. J Cell Mol Med. 2016 Sep 19. doi: 10.1111/jcmm.12968. [Epub ahead of print]
7. Cells Tissues Organs. 2016;201(3):180-92.
8. Mutat Res Genet Toxicol Environ Mutagen. 2015 Sep;791:30-7.
9. Cutan Ocul Toxicol. 2007;26(3):227-33.
10. J Agric Food Chem. 2002 Aug 14;50(17):4947-52.
11. J Agric Food Chem. 2002 Mar 27;50(7):1845-51.
12. Med Chem. 2011 Nov;7(6):674-89.
13. Microb Drug Resist. 2012 Apr;18(2):137-48.
14. J Korean Acad Nurs. 2015 Jun;45(3):367-77.
15. J Vector Borne Dis. 2008 Dec;45(4):301-6.
16. Int J Dermatol. 2012 Jul;51(7):790-5.
17. J Cosmet Dermatol. 2013 Jun;12(2):116-22.
18. Parasitol Res. 2016 Feb;115(2):633-41.
19. J Med Entomol. 1999 Sep;36(5):625-9.
20. J Am Mosq Control Assoc. 2002 Dec;18(4):348-51.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Native to the western Mediterranean, Thymus vulgaris (one of approximately 300 Thymus species) is a small bush used for centuries as a spice and in medicine, particularly to treat bronchitis.1Thymus species are among the wild and cultivated species used in traditional medicine in Bosnia and Herzegovina for various indications, including skin disorders.2 Thyme essential oil is a natural compound generally recognized as safe by the Food and Drug Administration, with demonstrated antibacterial, antifungal, and antispasmodic activities.3,4 Several other biologic activities have been associated with the polyphenol-rich herb, many of which have dermatologic implications. Notably, the essential oil of thyme and thymol, a key constituent of thyme, are known to act as skin sensitizers and allergens.5
Photoprotective activity
Recently, Sun et al. showed that UVB-induced skin damage was attenuated by treating hairless mice (HR-1) with T. vulgaris, as indicated by reduced matrix metalloproteinases and elevated collagen synthesis. In cultured normal human dermal fibroblasts, the investigators found that T. vulgaris blocked UVB-induced reactive oxygen species and lactate dehydrogenase, and dose-dependently yielded increases in glutathione, NAD(P)H: quinone oxidoreductase 1, and heme oxygenase-1. Further, the botanical significantly reduced UVB-induced phosphorylation of mitogen-activated protein kinases. The investigators concluded that T. vulgaris has potential for use in preventing skin damage caused by UV radiation–induced oxidative stress.6
Thyme also was demonstrated by Cornaghi et al. in 2016 to exert a protective effect on normal human skin explants obtained from seven young healthy women that were treated 1 hour before UVB irradiation.7
In 2015, Calò et al. evaluated the protective effects of a dry extract from T. vulgaris and its primary synthetic constituent thymol against UVA- and UVB-induced oxidative and genotoxic damage in the keratinocyte cell line NCTC 2544. Both thymol and T. vulgaris suppressed reactive oxygen species production in UVA- and UVB-treated cells, but lowered malondialdehyde synthesis only in cells treated with UVA.8
Antioxidant activity
In 2007, Wei and Shibamoto reported that thyme essential oil mixed with clove oil exhibited over a 90% inhibitory effect against the formation of malondialdehyde. They speculated that the presence of thymol and eugenol might account for the strong antioxidant activity displayed by the thyme/clove leaf combination.9 The investigators previously observed antioxidant activities exhibited by volatile extracts isolated from thyme (as well as various other herbs and spices) using aldehyde/carboxylic acid as well as conjugated diene assays.10 The antioxidant activity of thyme also was demonstrated by Miura et al. using the oil stability index method.11
Antimicrobial activity
In 2011, Sienkiewicz et al. reported that the oil of T. vulgaris displayed potent activity against clinical bacterial strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas genera. In addition, thyme essential oil exhibited efficacy against tested antibiotic-resistant strains of bacteria.12 The following year, Sienkiewicz et al. assessed the antimicrobial activity of thyme essential oil against clinical multidrug-resistant strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas, finding that it potently suppressed the growth of each.13
Potential cutaneous indications: atopic dermatitis, leishmaniasis, eczema, hair growth
In 2015, Seo and Jeong showed that lavender oil, thyme oil, and a blend of the two were all effective in reducing the symptoms of atopic dermatitis in mice. The researchers suggested that developing treatments with these oils for human patients with atopic dermatitis is warranted.14
Nilforoushzadeh et al. found in 2008 that herbal extracts of T. vulgaris and Achillea millefolium (yarrow), as well as propolis hydroalcoholic extracts, were effective in treating cutaneous leishmaniasis in mice and recommended the study of these extracts alone or in combination in human trials.15
A two-arm, randomized, double-blind, placebo-controlled trial conducted by Shimelis et al. in 2012 evaluated the efficacy of a 3% thyme essential oil antifungal cream and a 10% chamomile extract cream in the treatment of eczemalike lesions. Complete healing was achieved in 10 patients (66.5%) treated with the thyme cream, compared with four patients (28.5%) in the placebo group. Although no significant differences were observed between the active chamomile group and placebo, an appreciable number of subjects improved or healed. The investigators concluded that their findings from this small study suggest that, while more research is needed, a 3% thyme essential oil cream appears to be an inexpensive and readily available option to treat mild to moderate cutaneous conditions, including fungal infections, pityriasis alba, and eczema.16
In 2013, Rastegar et al. found that the combination of herbal extracts (including thyme) and platelet-rich plasma induced significant proliferation of human dermal papilla cells by regulating extracellular signal-regulated kinase (ERK) and Akt (protein kinase B). They concluded that their findings suggest the potential for developing combination therapies intended to improve hair growth.17
Insect repellent activity
In a 2016 study by Gutiérrez et al., the essential oil of T. vulgaris was found to be effective against Pediculus humanus capitis (head lice) adults and eggs. The researchers concluded that T. vulgaris achieves a strong knockdown and mortality rate in adult head lice and toxicity in the eggs after 21 minutes of application at a low concentration.18
In a small 1999 study by Barnard of the repellency to Aedes aegypti and Anopheles albimanus of various concentrations and combinations of five essential oils (Bourbon geranium, cedarwood, clove, peppermint, and thyme) applied to human skin, thyme and clove oils were found to be the most effective mosquito repellents. The author noted that thyme oil (as well as clove and peppermint oils) can irritate the skin and the odor of thyme and clove oils, at concentrations of 25%, or more were deemed unacceptable by the two participants in the study.19
Three years later, Choi et al. found that the essential oil of T. vulgaris also repelled adult mosquitoes (Culex pipiens pallens) on hairless mice and displayed potent repellent activity.20
Melanoma
In 2005, Carrera et al. reported a case of long-term complete remission of cutaneous melanoma metastases in a 73-year-old white woman who consumed a dried thyme herbal tea and thyme topical applications in compresses.4 An association between thyme and melanoma has not been reported in the subsequent literature.
Conclusion
Thyme has a long history of culinary and medical uses. Its antimicrobial and antioxidant activity are well documented. While there is reason to consider the potential applications of thyme for dermatologic conditions, much more research is necessary to determine its viability for such purposes.
References
1. An Illustrated Guide to 101 Medicinal Herbs: Their History, Use, Recommended Dosages, and Cautions (Loveland, Colo.: Interweave Press, 1998, pp. 198-9).
2. J Ethnopharmacol. 2010 Aug 19;131(1):33-55.
3. J Food Sci. 2014 May;79(5):M903-10.
4. J Am Acad Dermatol. 2005 Apr;52(4):713-5.
5. Nat Neurosci. 2006 May;9(5):628-35.
6. J Cell Mol Med. 2016 Sep 19. doi: 10.1111/jcmm.12968. [Epub ahead of print]
7. Cells Tissues Organs. 2016;201(3):180-92.
8. Mutat Res Genet Toxicol Environ Mutagen. 2015 Sep;791:30-7.
9. Cutan Ocul Toxicol. 2007;26(3):227-33.
10. J Agric Food Chem. 2002 Aug 14;50(17):4947-52.
11. J Agric Food Chem. 2002 Mar 27;50(7):1845-51.
12. Med Chem. 2011 Nov;7(6):674-89.
13. Microb Drug Resist. 2012 Apr;18(2):137-48.
14. J Korean Acad Nurs. 2015 Jun;45(3):367-77.
15. J Vector Borne Dis. 2008 Dec;45(4):301-6.
16. Int J Dermatol. 2012 Jul;51(7):790-5.
17. J Cosmet Dermatol. 2013 Jun;12(2):116-22.
18. Parasitol Res. 2016 Feb;115(2):633-41.
19. J Med Entomol. 1999 Sep;36(5):625-9.
20. J Am Mosq Control Assoc. 2002 Dec;18(4):348-51.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Native to the western Mediterranean, Thymus vulgaris (one of approximately 300 Thymus species) is a small bush used for centuries as a spice and in medicine, particularly to treat bronchitis.1Thymus species are among the wild and cultivated species used in traditional medicine in Bosnia and Herzegovina for various indications, including skin disorders.2 Thyme essential oil is a natural compound generally recognized as safe by the Food and Drug Administration, with demonstrated antibacterial, antifungal, and antispasmodic activities.3,4 Several other biologic activities have been associated with the polyphenol-rich herb, many of which have dermatologic implications. Notably, the essential oil of thyme and thymol, a key constituent of thyme, are known to act as skin sensitizers and allergens.5
Photoprotective activity
Recently, Sun et al. showed that UVB-induced skin damage was attenuated by treating hairless mice (HR-1) with T. vulgaris, as indicated by reduced matrix metalloproteinases and elevated collagen synthesis. In cultured normal human dermal fibroblasts, the investigators found that T. vulgaris blocked UVB-induced reactive oxygen species and lactate dehydrogenase, and dose-dependently yielded increases in glutathione, NAD(P)H: quinone oxidoreductase 1, and heme oxygenase-1. Further, the botanical significantly reduced UVB-induced phosphorylation of mitogen-activated protein kinases. The investigators concluded that T. vulgaris has potential for use in preventing skin damage caused by UV radiation–induced oxidative stress.6
Thyme also was demonstrated by Cornaghi et al. in 2016 to exert a protective effect on normal human skin explants obtained from seven young healthy women that were treated 1 hour before UVB irradiation.7
In 2015, Calò et al. evaluated the protective effects of a dry extract from T. vulgaris and its primary synthetic constituent thymol against UVA- and UVB-induced oxidative and genotoxic damage in the keratinocyte cell line NCTC 2544. Both thymol and T. vulgaris suppressed reactive oxygen species production in UVA- and UVB-treated cells, but lowered malondialdehyde synthesis only in cells treated with UVA.8
Antioxidant activity
In 2007, Wei and Shibamoto reported that thyme essential oil mixed with clove oil exhibited over a 90% inhibitory effect against the formation of malondialdehyde. They speculated that the presence of thymol and eugenol might account for the strong antioxidant activity displayed by the thyme/clove leaf combination.9 The investigators previously observed antioxidant activities exhibited by volatile extracts isolated from thyme (as well as various other herbs and spices) using aldehyde/carboxylic acid as well as conjugated diene assays.10 The antioxidant activity of thyme also was demonstrated by Miura et al. using the oil stability index method.11
Antimicrobial activity
In 2011, Sienkiewicz et al. reported that the oil of T. vulgaris displayed potent activity against clinical bacterial strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas genera. In addition, thyme essential oil exhibited efficacy against tested antibiotic-resistant strains of bacteria.12 The following year, Sienkiewicz et al. assessed the antimicrobial activity of thyme essential oil against clinical multidrug-resistant strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas, finding that it potently suppressed the growth of each.13
Potential cutaneous indications: atopic dermatitis, leishmaniasis, eczema, hair growth
In 2015, Seo and Jeong showed that lavender oil, thyme oil, and a blend of the two were all effective in reducing the symptoms of atopic dermatitis in mice. The researchers suggested that developing treatments with these oils for human patients with atopic dermatitis is warranted.14
Nilforoushzadeh et al. found in 2008 that herbal extracts of T. vulgaris and Achillea millefolium (yarrow), as well as propolis hydroalcoholic extracts, were effective in treating cutaneous leishmaniasis in mice and recommended the study of these extracts alone or in combination in human trials.15
A two-arm, randomized, double-blind, placebo-controlled trial conducted by Shimelis et al. in 2012 evaluated the efficacy of a 3% thyme essential oil antifungal cream and a 10% chamomile extract cream in the treatment of eczemalike lesions. Complete healing was achieved in 10 patients (66.5%) treated with the thyme cream, compared with four patients (28.5%) in the placebo group. Although no significant differences were observed between the active chamomile group and placebo, an appreciable number of subjects improved or healed. The investigators concluded that their findings from this small study suggest that, while more research is needed, a 3% thyme essential oil cream appears to be an inexpensive and readily available option to treat mild to moderate cutaneous conditions, including fungal infections, pityriasis alba, and eczema.16
In 2013, Rastegar et al. found that the combination of herbal extracts (including thyme) and platelet-rich plasma induced significant proliferation of human dermal papilla cells by regulating extracellular signal-regulated kinase (ERK) and Akt (protein kinase B). They concluded that their findings suggest the potential for developing combination therapies intended to improve hair growth.17
Insect repellent activity
In a 2016 study by Gutiérrez et al., the essential oil of T. vulgaris was found to be effective against Pediculus humanus capitis (head lice) adults and eggs. The researchers concluded that T. vulgaris achieves a strong knockdown and mortality rate in adult head lice and toxicity in the eggs after 21 minutes of application at a low concentration.18
In a small 1999 study by Barnard of the repellency to Aedes aegypti and Anopheles albimanus of various concentrations and combinations of five essential oils (Bourbon geranium, cedarwood, clove, peppermint, and thyme) applied to human skin, thyme and clove oils were found to be the most effective mosquito repellents. The author noted that thyme oil (as well as clove and peppermint oils) can irritate the skin and the odor of thyme and clove oils, at concentrations of 25%, or more were deemed unacceptable by the two participants in the study.19
Three years later, Choi et al. found that the essential oil of T. vulgaris also repelled adult mosquitoes (Culex pipiens pallens) on hairless mice and displayed potent repellent activity.20
Melanoma
In 2005, Carrera et al. reported a case of long-term complete remission of cutaneous melanoma metastases in a 73-year-old white woman who consumed a dried thyme herbal tea and thyme topical applications in compresses.4 An association between thyme and melanoma has not been reported in the subsequent literature.
Conclusion
Thyme has a long history of culinary and medical uses. Its antimicrobial and antioxidant activity are well documented. While there is reason to consider the potential applications of thyme for dermatologic conditions, much more research is necessary to determine its viability for such purposes.
References
1. An Illustrated Guide to 101 Medicinal Herbs: Their History, Use, Recommended Dosages, and Cautions (Loveland, Colo.: Interweave Press, 1998, pp. 198-9).
2. J Ethnopharmacol. 2010 Aug 19;131(1):33-55.
3. J Food Sci. 2014 May;79(5):M903-10.
4. J Am Acad Dermatol. 2005 Apr;52(4):713-5.
5. Nat Neurosci. 2006 May;9(5):628-35.
6. J Cell Mol Med. 2016 Sep 19. doi: 10.1111/jcmm.12968. [Epub ahead of print]
7. Cells Tissues Organs. 2016;201(3):180-92.
8. Mutat Res Genet Toxicol Environ Mutagen. 2015 Sep;791:30-7.
9. Cutan Ocul Toxicol. 2007;26(3):227-33.
10. J Agric Food Chem. 2002 Aug 14;50(17):4947-52.
11. J Agric Food Chem. 2002 Mar 27;50(7):1845-51.
12. Med Chem. 2011 Nov;7(6):674-89.
13. Microb Drug Resist. 2012 Apr;18(2):137-48.
14. J Korean Acad Nurs. 2015 Jun;45(3):367-77.
15. J Vector Borne Dis. 2008 Dec;45(4):301-6.
16. Int J Dermatol. 2012 Jul;51(7):790-5.
17. J Cosmet Dermatol. 2013 Jun;12(2):116-22.
18. Parasitol Res. 2016 Feb;115(2):633-41.
19. J Med Entomol. 1999 Sep;36(5):625-9.
20. J Am Mosq Control Assoc. 2002 Dec;18(4):348-51.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.

Sofosbuvir, daclatasvir combo best treatment for HCV cryoglobulinemia vasculitis
WASHINGTON – A combined regimen of sofosbuvir and daclatasvir is the best option to treat patients with hepatitis C virus infections experiencing cryoglobulinemia vasculitis, according to the findings of a new study presented at the annual meeting of the American College of Rheumatology.
“The HCV cryoglobulinemia vasculitis is a very important vasculitis because it represents 5% of chronically infected HCV patients in the world,” explained David Saadoun, MD, of Sorbonne Universities, Paris. “It’s sometimes a life-threatening vasculitis because patients may develop inflammation [so] there’s a need for very active and well-tolerated treatment.”
The primary endpoint – complete response to treatment at the end of the regimen – was achieved in 91% of subjects by the end of 24 weeks. Furthermore, 50% of patients experienced complete immunological response, defined as the complete clearance of cryoglobulin, within 24 weeks. At 12 weeks, average cryoglobulin levels decreased from 0.36 ± 0.12 to 0.10 ± 0.08 g/L, (P = .019), while average aminotransferase levels decreased from 57.6 ± 7.1 to 20.4 ± 2.0 IU/mL, (P less than .01).
But perhaps most significant, according to Dr. Saadoun, is that less than 5% of subjects required any additional treatment via immunosuppressants, such as steroids or rituximab. Average HCV viral loads dropped from 5.6 to 1.18 IU/mL at week 4 (P less than .01), with similarly sustained results through to week 12, indicating good virological responses. No serious adverse events were reported by any subjects throughout the trial period.
“The limitation is that there are quite a few patients, because it is only 35 patients this time, [and] that it’s a prospective, open-label study with no comparators,” Dr. Saadoun explained, adding that, in terms of further research, “[any] new study would focus on the way to avoid rituximab and steroid use in these patients, and to also have more patients treated with this regimen.”
No funding source was disclosed for this study. Dr. Saadoun did not report any relevant financial disclosures.
WASHINGTON – A combined regimen of sofosbuvir and daclatasvir is the best option to treat patients with hepatitis C virus infections experiencing cryoglobulinemia vasculitis, according to the findings of a new study presented at the annual meeting of the American College of Rheumatology.
“The HCV cryoglobulinemia vasculitis is a very important vasculitis because it represents 5% of chronically infected HCV patients in the world,” explained David Saadoun, MD, of Sorbonne Universities, Paris. “It’s sometimes a life-threatening vasculitis because patients may develop inflammation [so] there’s a need for very active and well-tolerated treatment.”
The primary endpoint – complete response to treatment at the end of the regimen – was achieved in 91% of subjects by the end of 24 weeks. Furthermore, 50% of patients experienced complete immunological response, defined as the complete clearance of cryoglobulin, within 24 weeks. At 12 weeks, average cryoglobulin levels decreased from 0.36 ± 0.12 to 0.10 ± 0.08 g/L, (P = .019), while average aminotransferase levels decreased from 57.6 ± 7.1 to 20.4 ± 2.0 IU/mL, (P less than .01).
But perhaps most significant, according to Dr. Saadoun, is that less than 5% of subjects required any additional treatment via immunosuppressants, such as steroids or rituximab. Average HCV viral loads dropped from 5.6 to 1.18 IU/mL at week 4 (P less than .01), with similarly sustained results through to week 12, indicating good virological responses. No serious adverse events were reported by any subjects throughout the trial period.
“The limitation is that there are quite a few patients, because it is only 35 patients this time, [and] that it’s a prospective, open-label study with no comparators,” Dr. Saadoun explained, adding that, in terms of further research, “[any] new study would focus on the way to avoid rituximab and steroid use in these patients, and to also have more patients treated with this regimen.”
No funding source was disclosed for this study. Dr. Saadoun did not report any relevant financial disclosures.
WASHINGTON – A combined regimen of sofosbuvir and daclatasvir is the best option to treat patients with hepatitis C virus infections experiencing cryoglobulinemia vasculitis, according to the findings of a new study presented at the annual meeting of the American College of Rheumatology.
“The HCV cryoglobulinemia vasculitis is a very important vasculitis because it represents 5% of chronically infected HCV patients in the world,” explained David Saadoun, MD, of Sorbonne Universities, Paris. “It’s sometimes a life-threatening vasculitis because patients may develop inflammation [so] there’s a need for very active and well-tolerated treatment.”
The primary endpoint – complete response to treatment at the end of the regimen – was achieved in 91% of subjects by the end of 24 weeks. Furthermore, 50% of patients experienced complete immunological response, defined as the complete clearance of cryoglobulin, within 24 weeks. At 12 weeks, average cryoglobulin levels decreased from 0.36 ± 0.12 to 0.10 ± 0.08 g/L, (P = .019), while average aminotransferase levels decreased from 57.6 ± 7.1 to 20.4 ± 2.0 IU/mL, (P less than .01).
But perhaps most significant, according to Dr. Saadoun, is that less than 5% of subjects required any additional treatment via immunosuppressants, such as steroids or rituximab. Average HCV viral loads dropped from 5.6 to 1.18 IU/mL at week 4 (P less than .01), with similarly sustained results through to week 12, indicating good virological responses. No serious adverse events were reported by any subjects throughout the trial period.
“The limitation is that there are quite a few patients, because it is only 35 patients this time, [and] that it’s a prospective, open-label study with no comparators,” Dr. Saadoun explained, adding that, in terms of further research, “[any] new study would focus on the way to avoid rituximab and steroid use in these patients, and to also have more patients treated with this regimen.”
No funding source was disclosed for this study. Dr. Saadoun did not report any relevant financial disclosures.
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: Of 35 patients, 32 (91%) achieved complete clinical response in 6 months, with less than 5% requiring the use of additional immunosuppressants and none experiencing serious adverse events.
Data source: A prospective, open-label study of 35 patients with cryoglobulinemia vasculitis brought on by HCV infection.
Disclosures: Dr. Saadoun did not report any relevant financial disclosures.
Fecal calprotectin tops CRP as Crohn’s marker
Stool calprotectin correlates with severity of small-bowel Crohn’s disease, as measured against balloon-assisted enteroscopy and computed tomography enterography, according to a review reported in the January issue of Clinical Gastroenterology and Hepatology of 89 patients at Toho University in Chiba, Japan.
Although the correlation was moderate, the findings suggest that fecal calprotectin (FC), with additional work, might turn out to be a good biomarker for tracking small-bowel Crohn’s disease (CD) and its response to tumor necrosis factor blockers. “Currently, it is not widely accepted that FC relates to disease activity in patients with small-intestinal CD,” said investigators led by Tsunetaka Arai of Toho University’s division of gastroenterology and hepatology (Clin Gastroenterol Hepatol. 2016 Aug 23. doi: 10.1016/j.cgh.2016.08.015).
Gastroenterologists need a decent biomarker for small-bowel Crohn’s because old-school endoscopy falls short. Adhesions and strictures block endoscopes, and sometimes scopes simply can’t reach the disease site.
Balloon-assisted enteroscopy (BAE) and computed tomography enterography (CTE) have emerged in recent years as alternatives, but, even so, the need persists for a noninvasive and inexpensive biomarker that’s better than the current standard of C-reactive protein (CRP), which can be thrown off by systemic inflammation, among other problems. The Toho investigators “believe that FC could be a relevant surrogate marker of disease activity in small-bowel CD.” Stool calprotectin paralleled disease activity in their study, while “neither the CDAI [CD activity index] score nor serum CRP showed similar correlation,” they said.
However, elevations in FC – a calcium- and zinc-binding protein released when neutrophils, monocytes, and macrophages inflame the intestinal mucosa – was independent of CD location, which signals the need for further investigation.
Meanwhile, the decent correlation between FC and CTE in the study “should [also] mean that” they could be used together to reliably define mucosal healing. CTE on its own “showed good correlation” with BAE; a CTE score/segment less than 2 [was] associated with endoscopic mucosal healing” on BAE, the investigators said.
The study subjects were an average of 32 years old, and had CD for 9 years; most were men. They had highly active disease at their first endoscopy (average CDAI of 120 points), and an average CRP of 1.09 mg/dL. Twenty-seven patients (30.3%) had small-bowel CD, 50 (56.2%) had ileocolonic CD, and 12 (13.5%) had colonic CD.
They all had endoscopic exams, BAE, and FC stool testing; those with strictures (17) went on to CTE; CTE detected every lesion despite the strictures.
The authors had no conflicts of interest.
Stool calprotectin correlates with severity of small-bowel Crohn’s disease, as measured against balloon-assisted enteroscopy and computed tomography enterography, according to a review reported in the January issue of Clinical Gastroenterology and Hepatology of 89 patients at Toho University in Chiba, Japan.
Although the correlation was moderate, the findings suggest that fecal calprotectin (FC), with additional work, might turn out to be a good biomarker for tracking small-bowel Crohn’s disease (CD) and its response to tumor necrosis factor blockers. “Currently, it is not widely accepted that FC relates to disease activity in patients with small-intestinal CD,” said investigators led by Tsunetaka Arai of Toho University’s division of gastroenterology and hepatology (Clin Gastroenterol Hepatol. 2016 Aug 23. doi: 10.1016/j.cgh.2016.08.015).
Gastroenterologists need a decent biomarker for small-bowel Crohn’s because old-school endoscopy falls short. Adhesions and strictures block endoscopes, and sometimes scopes simply can’t reach the disease site.
Balloon-assisted enteroscopy (BAE) and computed tomography enterography (CTE) have emerged in recent years as alternatives, but, even so, the need persists for a noninvasive and inexpensive biomarker that’s better than the current standard of C-reactive protein (CRP), which can be thrown off by systemic inflammation, among other problems. The Toho investigators “believe that FC could be a relevant surrogate marker of disease activity in small-bowel CD.” Stool calprotectin paralleled disease activity in their study, while “neither the CDAI [CD activity index] score nor serum CRP showed similar correlation,” they said.
However, elevations in FC – a calcium- and zinc-binding protein released when neutrophils, monocytes, and macrophages inflame the intestinal mucosa – was independent of CD location, which signals the need for further investigation.
Meanwhile, the decent correlation between FC and CTE in the study “should [also] mean that” they could be used together to reliably define mucosal healing. CTE on its own “showed good correlation” with BAE; a CTE score/segment less than 2 [was] associated with endoscopic mucosal healing” on BAE, the investigators said.
The study subjects were an average of 32 years old, and had CD for 9 years; most were men. They had highly active disease at their first endoscopy (average CDAI of 120 points), and an average CRP of 1.09 mg/dL. Twenty-seven patients (30.3%) had small-bowel CD, 50 (56.2%) had ileocolonic CD, and 12 (13.5%) had colonic CD.
They all had endoscopic exams, BAE, and FC stool testing; those with strictures (17) went on to CTE; CTE detected every lesion despite the strictures.
The authors had no conflicts of interest.
Stool calprotectin correlates with severity of small-bowel Crohn’s disease, as measured against balloon-assisted enteroscopy and computed tomography enterography, according to a review reported in the January issue of Clinical Gastroenterology and Hepatology of 89 patients at Toho University in Chiba, Japan.
Although the correlation was moderate, the findings suggest that fecal calprotectin (FC), with additional work, might turn out to be a good biomarker for tracking small-bowel Crohn’s disease (CD) and its response to tumor necrosis factor blockers. “Currently, it is not widely accepted that FC relates to disease activity in patients with small-intestinal CD,” said investigators led by Tsunetaka Arai of Toho University’s division of gastroenterology and hepatology (Clin Gastroenterol Hepatol. 2016 Aug 23. doi: 10.1016/j.cgh.2016.08.015).
Gastroenterologists need a decent biomarker for small-bowel Crohn’s because old-school endoscopy falls short. Adhesions and strictures block endoscopes, and sometimes scopes simply can’t reach the disease site.
Balloon-assisted enteroscopy (BAE) and computed tomography enterography (CTE) have emerged in recent years as alternatives, but, even so, the need persists for a noninvasive and inexpensive biomarker that’s better than the current standard of C-reactive protein (CRP), which can be thrown off by systemic inflammation, among other problems. The Toho investigators “believe that FC could be a relevant surrogate marker of disease activity in small-bowel CD.” Stool calprotectin paralleled disease activity in their study, while “neither the CDAI [CD activity index] score nor serum CRP showed similar correlation,” they said.
However, elevations in FC – a calcium- and zinc-binding protein released when neutrophils, monocytes, and macrophages inflame the intestinal mucosa – was independent of CD location, which signals the need for further investigation.
Meanwhile, the decent correlation between FC and CTE in the study “should [also] mean that” they could be used together to reliably define mucosal healing. CTE on its own “showed good correlation” with BAE; a CTE score/segment less than 2 [was] associated with endoscopic mucosal healing” on BAE, the investigators said.
The study subjects were an average of 32 years old, and had CD for 9 years; most were men. They had highly active disease at their first endoscopy (average CDAI of 120 points), and an average CRP of 1.09 mg/dL. Twenty-seven patients (30.3%) had small-bowel CD, 50 (56.2%) had ileocolonic CD, and 12 (13.5%) had colonic CD.
They all had endoscopic exams, BAE, and FC stool testing; those with strictures (17) went on to CTE; CTE detected every lesion despite the strictures.
The authors had no conflicts of interest.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point:
Major finding: A fecal calprotectin cutoff of 215 mcg/g identified mucosal healing with 82.8% sensitivity, 71.4% specificity, and an AUC of 0.81.
Data source: Review of 89 Crohn’s patients
Disclosures: The investigators had no conflicts of interest.
PrEP adoption lagging behind awareness in high-risk population
NEW ORLEANS – Awareness about preexposure prophylaxis (PrEP) is steadily increasing among men who have sex with men at high risk for HIV infection, but that increased knowledge did not translate into greater willingness to take the daily pill nor did it increase engagement in high-risk behaviors.
Using questions from the National HIV Behavioral Surveillance System (NHBS), investigators surveyed men who have sex with men in urban settings in 3-year cycles. Awareness about HIV PrEP, once-daily emtricitabine/tenofovir (Truvada) increased from 21% in 2008 to 28% in 2011 to 46% in 2014.
The increase from 2011 to 2014 was statistically significant (P less than .001). The Food and Drug Administration approved the preventive regimen in 2012.
Increased knowledge did not translate to greater willingness to take the daily pill – which has held steady at about 60% of over time.
The number of men who self-reported as HIV negative and sexually active in the previous 12 months included in the survey varied from 421 in 2008, to 461 in 2011, to 451 in 2014.
For people at elevated risk for HIV infection, PrEP also represents an opportunity to take greater control over behavior, according to a recent review (Curr Opin HIV AIDS. 2016;11:3-9). “When you get people in for counseling or condoms, you give them a sense of control,” said Dr. Krotchko of Denver Health Medical Center.
Most survey respondents said they anticipated they would use condoms just as frequently as before if taking PrEP (82%, 78%, and 78%, in 2008, 2011, and 2014, respectively). Similarly, the majority of respondents anticipated having the same number of sexual partners if taking PrEP (92%, 85%, and 89%). These differences were not statistically significant.
The findings indicate availability of HIV PrEP is not increasing unhealthy behaviors, as some may fear. “Riskier behavior while on PrEP has not been borne out by the literature,” Dr. Krotchko said.
Strengths of the study include directly targeting a high-risk population and identifying those with high-risk behaviors who could benefit from use of HIV PrEP. Self-reported anticipated changes may not reflect future behavior in all cases, a potential limitation, Dr. Krotchko pointed out.
The NHBS survey is funded by the Centers for Disease Control and Prevention. IDWeek 2016 comprises the combined meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
NEW ORLEANS – Awareness about preexposure prophylaxis (PrEP) is steadily increasing among men who have sex with men at high risk for HIV infection, but that increased knowledge did not translate into greater willingness to take the daily pill nor did it increase engagement in high-risk behaviors.
Using questions from the National HIV Behavioral Surveillance System (NHBS), investigators surveyed men who have sex with men in urban settings in 3-year cycles. Awareness about HIV PrEP, once-daily emtricitabine/tenofovir (Truvada) increased from 21% in 2008 to 28% in 2011 to 46% in 2014.
The increase from 2011 to 2014 was statistically significant (P less than .001). The Food and Drug Administration approved the preventive regimen in 2012.
Increased knowledge did not translate to greater willingness to take the daily pill – which has held steady at about 60% of over time.
The number of men who self-reported as HIV negative and sexually active in the previous 12 months included in the survey varied from 421 in 2008, to 461 in 2011, to 451 in 2014.
For people at elevated risk for HIV infection, PrEP also represents an opportunity to take greater control over behavior, according to a recent review (Curr Opin HIV AIDS. 2016;11:3-9). “When you get people in for counseling or condoms, you give them a sense of control,” said Dr. Krotchko of Denver Health Medical Center.
Most survey respondents said they anticipated they would use condoms just as frequently as before if taking PrEP (82%, 78%, and 78%, in 2008, 2011, and 2014, respectively). Similarly, the majority of respondents anticipated having the same number of sexual partners if taking PrEP (92%, 85%, and 89%). These differences were not statistically significant.
The findings indicate availability of HIV PrEP is not increasing unhealthy behaviors, as some may fear. “Riskier behavior while on PrEP has not been borne out by the literature,” Dr. Krotchko said.
Strengths of the study include directly targeting a high-risk population and identifying those with high-risk behaviors who could benefit from use of HIV PrEP. Self-reported anticipated changes may not reflect future behavior in all cases, a potential limitation, Dr. Krotchko pointed out.
The NHBS survey is funded by the Centers for Disease Control and Prevention. IDWeek 2016 comprises the combined meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
NEW ORLEANS – Awareness about preexposure prophylaxis (PrEP) is steadily increasing among men who have sex with men at high risk for HIV infection, but that increased knowledge did not translate into greater willingness to take the daily pill nor did it increase engagement in high-risk behaviors.
Using questions from the National HIV Behavioral Surveillance System (NHBS), investigators surveyed men who have sex with men in urban settings in 3-year cycles. Awareness about HIV PrEP, once-daily emtricitabine/tenofovir (Truvada) increased from 21% in 2008 to 28% in 2011 to 46% in 2014.
The increase from 2011 to 2014 was statistically significant (P less than .001). The Food and Drug Administration approved the preventive regimen in 2012.
Increased knowledge did not translate to greater willingness to take the daily pill – which has held steady at about 60% of over time.
The number of men who self-reported as HIV negative and sexually active in the previous 12 months included in the survey varied from 421 in 2008, to 461 in 2011, to 451 in 2014.
For people at elevated risk for HIV infection, PrEP also represents an opportunity to take greater control over behavior, according to a recent review (Curr Opin HIV AIDS. 2016;11:3-9). “When you get people in for counseling or condoms, you give them a sense of control,” said Dr. Krotchko of Denver Health Medical Center.
Most survey respondents said they anticipated they would use condoms just as frequently as before if taking PrEP (82%, 78%, and 78%, in 2008, 2011, and 2014, respectively). Similarly, the majority of respondents anticipated having the same number of sexual partners if taking PrEP (92%, 85%, and 89%). These differences were not statistically significant.
The findings indicate availability of HIV PrEP is not increasing unhealthy behaviors, as some may fear. “Riskier behavior while on PrEP has not been borne out by the literature,” Dr. Krotchko said.
Strengths of the study include directly targeting a high-risk population and identifying those with high-risk behaviors who could benefit from use of HIV PrEP. Self-reported anticipated changes may not reflect future behavior in all cases, a potential limitation, Dr. Krotchko pointed out.
The NHBS survey is funded by the Centers for Disease Control and Prevention. IDWeek 2016 comprises the combined meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
AT IDWEEK 2016
Key clinical point: Adoption and use of HIV PrEP continues to lag behind studies showing its effectiveness in the high-risk population of men who have sex with men.
Major finding: Despite increasing awareness, willingness to use HIV PrEP among MSM remained steady at about 60% over time in a series of national behavioral health surveys.
Data source: The National HIV Behavioral Surveillance System.
Disclosures: Dr. Krotchko had no relevant disclosures.
Thank You to Our 2016 Peer Reviewers
The editors of Emergency Medicine acknowledge the help of the journal’s editorial board members, other emergency physicians, and colleagues in other specialties who reviewed manuscripts in 2016. On behalf of our readers, who are the beneficiaries of your efforts, we thank you.
Alfred Z. Abuhamad, MD
Department of Obstetrics and Gynecology
Eastern Virginia Medical School
John E. Arbo, MD
Division of Emergency Medicine and Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
David P. Calfee, MD
Division of Infectious Diseases
Weill Cornell Medical College, Cornell University
Richard M. Cantor, MD, FAAP, FACEP
Emergency Department, Pediatrics
Upstate Medical University
Wallace A. Carter, MD, FACEP
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Sunday Clark, ScD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Theodore R. Delbridge, MD
Department of Emergency
Medicine East Carolina University, Brody School of Medicine
Joseph J. Fins, MD
Division of Medical Ethics Internal Medicine
Weill Cornell Medical College, Cornell University
Ron W. Flenner, MD
Department of Internal Medicine
Eastern Virginia Medical School
E. John Gallagher, MD
Department of Emergency Medicine
Albert Einstein College of Medicine
Marianne Gausche-Hill, MD
Department of Emergency Medicine
Harbor-UCLA Medical Center
Keith D. Hentel, MD
Department of Radiology
Weill Cornell Medical College, Cornell University
Barry J. Knapp, MD
Department of Emergency Medicine
Eastern Virginia Medical School
Richard I. Lapin, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Anthony C. Mustalish, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Lewis S. Nelson, MD
Department of Emergency Medicine
Rutgers New Jersey Medical School
Debra Perina, MD
Department of Emergency Medicine
University of Virginia, Charlottesville
Constance Peterson, MA
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Shari L. Platt, MD, FAAP
Division of Pediatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Rama B. Rao, MD
Division of Toxicology
Weill Cornell Medical College, Cornell University
Earl J. Reisdorff, MD
Executive Director
American Board of Emergency Medicine
Thomas M. Scalea, MD, FACS, FCCM
Program in Trauma
University of Maryland School of Medicine
Edward J. Schenk, MD
Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
Christopher K. Schott, MD, MS
Department of Emergency Medicine and Critical Care Medicine
University of Pittsburgh
Adam J Singer, MD
Department of Emergency Medicine
Stony Brook University and Medical Center
Sarah A. Stahmer, MD, FACEP
Division of Emergency Medicine
Duke University Medical Center
Michael E. Stern, MD
Division of Geriatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Susan Stone, MD
Emergency Medicine/Palliative Care
University of California, Los Angeles
Todd Taylor, MD
Department of Emergency Medicine
Emory University School of Medicine
The editors of Emergency Medicine acknowledge the help of the journal’s editorial board members, other emergency physicians, and colleagues in other specialties who reviewed manuscripts in 2016. On behalf of our readers, who are the beneficiaries of your efforts, we thank you.
Alfred Z. Abuhamad, MD
Department of Obstetrics and Gynecology
Eastern Virginia Medical School
John E. Arbo, MD
Division of Emergency Medicine and Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
David P. Calfee, MD
Division of Infectious Diseases
Weill Cornell Medical College, Cornell University
Richard M. Cantor, MD, FAAP, FACEP
Emergency Department, Pediatrics
Upstate Medical University
Wallace A. Carter, MD, FACEP
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Sunday Clark, ScD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Theodore R. Delbridge, MD
Department of Emergency
Medicine East Carolina University, Brody School of Medicine
Joseph J. Fins, MD
Division of Medical Ethics Internal Medicine
Weill Cornell Medical College, Cornell University
Ron W. Flenner, MD
Department of Internal Medicine
Eastern Virginia Medical School
E. John Gallagher, MD
Department of Emergency Medicine
Albert Einstein College of Medicine
Marianne Gausche-Hill, MD
Department of Emergency Medicine
Harbor-UCLA Medical Center
Keith D. Hentel, MD
Department of Radiology
Weill Cornell Medical College, Cornell University
Barry J. Knapp, MD
Department of Emergency Medicine
Eastern Virginia Medical School
Richard I. Lapin, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Anthony C. Mustalish, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Lewis S. Nelson, MD
Department of Emergency Medicine
Rutgers New Jersey Medical School
Debra Perina, MD
Department of Emergency Medicine
University of Virginia, Charlottesville
Constance Peterson, MA
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Shari L. Platt, MD, FAAP
Division of Pediatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Rama B. Rao, MD
Division of Toxicology
Weill Cornell Medical College, Cornell University
Earl J. Reisdorff, MD
Executive Director
American Board of Emergency Medicine
Thomas M. Scalea, MD, FACS, FCCM
Program in Trauma
University of Maryland School of Medicine
Edward J. Schenk, MD
Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
Christopher K. Schott, MD, MS
Department of Emergency Medicine and Critical Care Medicine
University of Pittsburgh
Adam J Singer, MD
Department of Emergency Medicine
Stony Brook University and Medical Center
Sarah A. Stahmer, MD, FACEP
Division of Emergency Medicine
Duke University Medical Center
Michael E. Stern, MD
Division of Geriatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Susan Stone, MD
Emergency Medicine/Palliative Care
University of California, Los Angeles
Todd Taylor, MD
Department of Emergency Medicine
Emory University School of Medicine
The editors of Emergency Medicine acknowledge the help of the journal’s editorial board members, other emergency physicians, and colleagues in other specialties who reviewed manuscripts in 2016. On behalf of our readers, who are the beneficiaries of your efforts, we thank you.
Alfred Z. Abuhamad, MD
Department of Obstetrics and Gynecology
Eastern Virginia Medical School
John E. Arbo, MD
Division of Emergency Medicine and Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
David P. Calfee, MD
Division of Infectious Diseases
Weill Cornell Medical College, Cornell University
Richard M. Cantor, MD, FAAP, FACEP
Emergency Department, Pediatrics
Upstate Medical University
Wallace A. Carter, MD, FACEP
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Sunday Clark, ScD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Theodore R. Delbridge, MD
Department of Emergency
Medicine East Carolina University, Brody School of Medicine
Joseph J. Fins, MD
Division of Medical Ethics Internal Medicine
Weill Cornell Medical College, Cornell University
Ron W. Flenner, MD
Department of Internal Medicine
Eastern Virginia Medical School
E. John Gallagher, MD
Department of Emergency Medicine
Albert Einstein College of Medicine
Marianne Gausche-Hill, MD
Department of Emergency Medicine
Harbor-UCLA Medical Center
Keith D. Hentel, MD
Department of Radiology
Weill Cornell Medical College, Cornell University
Barry J. Knapp, MD
Department of Emergency Medicine
Eastern Virginia Medical School
Richard I. Lapin, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Anthony C. Mustalish, MD
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Lewis S. Nelson, MD
Department of Emergency Medicine
Rutgers New Jersey Medical School
Debra Perina, MD
Department of Emergency Medicine
University of Virginia, Charlottesville
Constance Peterson, MA
Department of Emergency Medicine
Weill Cornell Medical College, Cornell University
Shari L. Platt, MD, FAAP
Division of Pediatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Rama B. Rao, MD
Division of Toxicology
Weill Cornell Medical College, Cornell University
Earl J. Reisdorff, MD
Executive Director
American Board of Emergency Medicine
Thomas M. Scalea, MD, FACS, FCCM
Program in Trauma
University of Maryland School of Medicine
Edward J. Schenk, MD
Pulmonary Critical Care Medicine
Weill Cornell Medical College, Cornell University
Christopher K. Schott, MD, MS
Department of Emergency Medicine and Critical Care Medicine
University of Pittsburgh
Adam J Singer, MD
Department of Emergency Medicine
Stony Brook University and Medical Center
Sarah A. Stahmer, MD, FACEP
Division of Emergency Medicine
Duke University Medical Center
Michael E. Stern, MD
Division of Geriatric Emergency Medicine
Weill Cornell Medical College, Cornell University
Susan Stone, MD
Emergency Medicine/Palliative Care
University of California, Los Angeles
Todd Taylor, MD
Department of Emergency Medicine
Emory University School of Medicine

Screening tool spots teens headed for substance-dependent adulthood
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
EXPERT ANALYSIS FROM THE ECNP CONGRESS
Ocular rosacea remains a stubborn foe
Few skin disorders have the power to devastate lives like ocular rosacea, a painful condition that disrupts vision and can lead to blindness, according to ophthalmologist Edward Wladis, MD.
“Patients really suffer from this diagnosis,” said Dr. Wladis, who practices in Slingerlands, N.Y.
Charles Slonim, MD, an ophthalmologist who practices in Tampa, Fla., put it this way: “We control the condition more than 50 percent of the time, but frequently patients go into periods of remission only to have a recurrence or exacerbation of their ocular rosacea.”
Dr. Wladis coauthored a 2013 report that examined treatments for ocular rosacea, which noted that estimates of the proportion of people with rosacea in the United States who develop ocular rosacea vary, ranging from 58% to 72% (US Ophthalmic Review, 2013;6[2]:86-8).
“Ocular rosacea is one of the subtypes of this disease of cutaneous inflammation,” Dr. Wladis said. “Once the skin becomes so severely inflamed, the glands that lubricate the eye become damaged, and the tear film evaporates rapidly. As a result, patients complain of the effects of a dry ocular surface, and they suffer from blurred vision, tearing, pain, and problems with glare.”
Dr. Slonim suggests that dermatologists refer rosacea patients to an ophthalmologist if they present with any eye symptom, such as dryness, burning, or itching, foreign body sensation in one or both eyes, or chronic redness of either the eyes or the eyelid margins. “They should be seen should be seen by an ophthalmologist to rule out ocular rosacea,” he said. “The ophthalmologist’s ability to look at the eye and eyelids under high magnification – a slit lamp examination – gives us an advantage in the diagnosis of ocular rosacea.”
If these patients do have ocular rosacea, their prognosis is unclear. “Unfortunately, many of our treatments haven’t been carefully vetted,” Dr. Wladis said.
He tends to begin with simpler treatments to heal the ocular surface, such as artificial tears and plugs in the tear drainage ducts to keep tears from leaving the eye quickly. Eyelid scrubs and warm compresses can also be helpful, he said, along with suggestions about lifestyle modifications to avoid the triggers that may exacerbate rosacea.
If those treatments fail, antibiotics are an option.
A 2015 Cochrane Review of studies of rosacea treatments suggested that for treating ocular rosacea, cyclosporine 0.05% ophthalmic emulsion “appeared to be more effective than artificial tears” (Cochrane Database Syst Rev. 2015 Apr 28;[3]:CD003262). And a 2015 study of 38 patients with ocular rosacea concluded that topical cyclosporine was significantly more effective in relieving symptoms and in the treatment of eyelid signs, compared with oral doxycycline (Int J Ophthalmol. 2015 Jun 18;8[3]:544-9).
Antibiotics seem to improve the eyelid’s health, “although some studies have documented that the cornea often doesn’t benefit from antibiotics, and patients’ visual acuity may not improve,” Dr. Wladis said.
Ophthalmologists also may prescribe nonsteroidal and steroidal anti-inflammatory drops, Dr. Slonim added, although “the use of topical ophthalmic steroids do carry the risk of secondary glaucoma with increased intraocular pressures.”
There are even more alternatives. “Dietary modification with omega-3 fatty acids appears to benefit the quality of the tear film,” Dr. Wladis said, referring to the results of a prospective, placebo-controlled, double-blind, randomized trial of patients with dry eye (Int J Ophthalmol. 2013 Dec 18;[6]:811-6). “Intraductal meibomian gland probing and intense pulsed light therapy have both been shown to improve ocular surface–related quality of life, although these treatments are relatively invasive and can rapidly become quite expensive for the patient.”
What’s on the horizon? Researchers have “started to unlock the mysteries of rosacea at the cellular level,” Dr. Wladis said. “Our efforts have recently focused on the cellular changes in the skin of rosacea patients. Using several methods, we assayed the activation of a wide variety of signals within the cells of the skin of these patients and found a consistent elevation of two specific signals.”
The researchers were especially pleased, he said, “that these signals appear to be activated in the outer layers of the skin, meaning that a topical preparation could be developed to selectively suppress these cell signals to turn off the disease without interfering with normal skin structure and function and without the side effects of oral or intravenous medications.”
His team is now working on a topical medication. “Ideally,” he noted, “future clinicians will be able to shift their focus from nonspecific therapies like antibiotics and steroids to really powerful, meaningful cellular therapeutics.”
Dr. Slonim reported no relevant disclosures. Dr. Wladis shares a provisional patent for the use of topical kinase inhibitors in the management of rosacea and recently co-started a biotechnology company called Praxis Biotechnology that aims to develop and test therapies for the condition. He serves as a consultant for both Bausch & Lomb and Valeant Pharmaceuticals.
Few skin disorders have the power to devastate lives like ocular rosacea, a painful condition that disrupts vision and can lead to blindness, according to ophthalmologist Edward Wladis, MD.
“Patients really suffer from this diagnosis,” said Dr. Wladis, who practices in Slingerlands, N.Y.
Charles Slonim, MD, an ophthalmologist who practices in Tampa, Fla., put it this way: “We control the condition more than 50 percent of the time, but frequently patients go into periods of remission only to have a recurrence or exacerbation of their ocular rosacea.”
Dr. Wladis coauthored a 2013 report that examined treatments for ocular rosacea, which noted that estimates of the proportion of people with rosacea in the United States who develop ocular rosacea vary, ranging from 58% to 72% (US Ophthalmic Review, 2013;6[2]:86-8).
“Ocular rosacea is one of the subtypes of this disease of cutaneous inflammation,” Dr. Wladis said. “Once the skin becomes so severely inflamed, the glands that lubricate the eye become damaged, and the tear film evaporates rapidly. As a result, patients complain of the effects of a dry ocular surface, and they suffer from blurred vision, tearing, pain, and problems with glare.”
Dr. Slonim suggests that dermatologists refer rosacea patients to an ophthalmologist if they present with any eye symptom, such as dryness, burning, or itching, foreign body sensation in one or both eyes, or chronic redness of either the eyes or the eyelid margins. “They should be seen should be seen by an ophthalmologist to rule out ocular rosacea,” he said. “The ophthalmologist’s ability to look at the eye and eyelids under high magnification – a slit lamp examination – gives us an advantage in the diagnosis of ocular rosacea.”
If these patients do have ocular rosacea, their prognosis is unclear. “Unfortunately, many of our treatments haven’t been carefully vetted,” Dr. Wladis said.
He tends to begin with simpler treatments to heal the ocular surface, such as artificial tears and plugs in the tear drainage ducts to keep tears from leaving the eye quickly. Eyelid scrubs and warm compresses can also be helpful, he said, along with suggestions about lifestyle modifications to avoid the triggers that may exacerbate rosacea.
If those treatments fail, antibiotics are an option.
A 2015 Cochrane Review of studies of rosacea treatments suggested that for treating ocular rosacea, cyclosporine 0.05% ophthalmic emulsion “appeared to be more effective than artificial tears” (Cochrane Database Syst Rev. 2015 Apr 28;[3]:CD003262). And a 2015 study of 38 patients with ocular rosacea concluded that topical cyclosporine was significantly more effective in relieving symptoms and in the treatment of eyelid signs, compared with oral doxycycline (Int J Ophthalmol. 2015 Jun 18;8[3]:544-9).
Antibiotics seem to improve the eyelid’s health, “although some studies have documented that the cornea often doesn’t benefit from antibiotics, and patients’ visual acuity may not improve,” Dr. Wladis said.
Ophthalmologists also may prescribe nonsteroidal and steroidal anti-inflammatory drops, Dr. Slonim added, although “the use of topical ophthalmic steroids do carry the risk of secondary glaucoma with increased intraocular pressures.”
There are even more alternatives. “Dietary modification with omega-3 fatty acids appears to benefit the quality of the tear film,” Dr. Wladis said, referring to the results of a prospective, placebo-controlled, double-blind, randomized trial of patients with dry eye (Int J Ophthalmol. 2013 Dec 18;[6]:811-6). “Intraductal meibomian gland probing and intense pulsed light therapy have both been shown to improve ocular surface–related quality of life, although these treatments are relatively invasive and can rapidly become quite expensive for the patient.”
What’s on the horizon? Researchers have “started to unlock the mysteries of rosacea at the cellular level,” Dr. Wladis said. “Our efforts have recently focused on the cellular changes in the skin of rosacea patients. Using several methods, we assayed the activation of a wide variety of signals within the cells of the skin of these patients and found a consistent elevation of two specific signals.”
The researchers were especially pleased, he said, “that these signals appear to be activated in the outer layers of the skin, meaning that a topical preparation could be developed to selectively suppress these cell signals to turn off the disease without interfering with normal skin structure and function and without the side effects of oral or intravenous medications.”
His team is now working on a topical medication. “Ideally,” he noted, “future clinicians will be able to shift their focus from nonspecific therapies like antibiotics and steroids to really powerful, meaningful cellular therapeutics.”
Dr. Slonim reported no relevant disclosures. Dr. Wladis shares a provisional patent for the use of topical kinase inhibitors in the management of rosacea and recently co-started a biotechnology company called Praxis Biotechnology that aims to develop and test therapies for the condition. He serves as a consultant for both Bausch & Lomb and Valeant Pharmaceuticals.
Few skin disorders have the power to devastate lives like ocular rosacea, a painful condition that disrupts vision and can lead to blindness, according to ophthalmologist Edward Wladis, MD.
“Patients really suffer from this diagnosis,” said Dr. Wladis, who practices in Slingerlands, N.Y.
Charles Slonim, MD, an ophthalmologist who practices in Tampa, Fla., put it this way: “We control the condition more than 50 percent of the time, but frequently patients go into periods of remission only to have a recurrence or exacerbation of their ocular rosacea.”
Dr. Wladis coauthored a 2013 report that examined treatments for ocular rosacea, which noted that estimates of the proportion of people with rosacea in the United States who develop ocular rosacea vary, ranging from 58% to 72% (US Ophthalmic Review, 2013;6[2]:86-8).
“Ocular rosacea is one of the subtypes of this disease of cutaneous inflammation,” Dr. Wladis said. “Once the skin becomes so severely inflamed, the glands that lubricate the eye become damaged, and the tear film evaporates rapidly. As a result, patients complain of the effects of a dry ocular surface, and they suffer from blurred vision, tearing, pain, and problems with glare.”
Dr. Slonim suggests that dermatologists refer rosacea patients to an ophthalmologist if they present with any eye symptom, such as dryness, burning, or itching, foreign body sensation in one or both eyes, or chronic redness of either the eyes or the eyelid margins. “They should be seen should be seen by an ophthalmologist to rule out ocular rosacea,” he said. “The ophthalmologist’s ability to look at the eye and eyelids under high magnification – a slit lamp examination – gives us an advantage in the diagnosis of ocular rosacea.”
If these patients do have ocular rosacea, their prognosis is unclear. “Unfortunately, many of our treatments haven’t been carefully vetted,” Dr. Wladis said.
He tends to begin with simpler treatments to heal the ocular surface, such as artificial tears and plugs in the tear drainage ducts to keep tears from leaving the eye quickly. Eyelid scrubs and warm compresses can also be helpful, he said, along with suggestions about lifestyle modifications to avoid the triggers that may exacerbate rosacea.
If those treatments fail, antibiotics are an option.
A 2015 Cochrane Review of studies of rosacea treatments suggested that for treating ocular rosacea, cyclosporine 0.05% ophthalmic emulsion “appeared to be more effective than artificial tears” (Cochrane Database Syst Rev. 2015 Apr 28;[3]:CD003262). And a 2015 study of 38 patients with ocular rosacea concluded that topical cyclosporine was significantly more effective in relieving symptoms and in the treatment of eyelid signs, compared with oral doxycycline (Int J Ophthalmol. 2015 Jun 18;8[3]:544-9).
Antibiotics seem to improve the eyelid’s health, “although some studies have documented that the cornea often doesn’t benefit from antibiotics, and patients’ visual acuity may not improve,” Dr. Wladis said.
Ophthalmologists also may prescribe nonsteroidal and steroidal anti-inflammatory drops, Dr. Slonim added, although “the use of topical ophthalmic steroids do carry the risk of secondary glaucoma with increased intraocular pressures.”
There are even more alternatives. “Dietary modification with omega-3 fatty acids appears to benefit the quality of the tear film,” Dr. Wladis said, referring to the results of a prospective, placebo-controlled, double-blind, randomized trial of patients with dry eye (Int J Ophthalmol. 2013 Dec 18;[6]:811-6). “Intraductal meibomian gland probing and intense pulsed light therapy have both been shown to improve ocular surface–related quality of life, although these treatments are relatively invasive and can rapidly become quite expensive for the patient.”
What’s on the horizon? Researchers have “started to unlock the mysteries of rosacea at the cellular level,” Dr. Wladis said. “Our efforts have recently focused on the cellular changes in the skin of rosacea patients. Using several methods, we assayed the activation of a wide variety of signals within the cells of the skin of these patients and found a consistent elevation of two specific signals.”
The researchers were especially pleased, he said, “that these signals appear to be activated in the outer layers of the skin, meaning that a topical preparation could be developed to selectively suppress these cell signals to turn off the disease without interfering with normal skin structure and function and without the side effects of oral or intravenous medications.”
His team is now working on a topical medication. “Ideally,” he noted, “future clinicians will be able to shift their focus from nonspecific therapies like antibiotics and steroids to really powerful, meaningful cellular therapeutics.”
Dr. Slonim reported no relevant disclosures. Dr. Wladis shares a provisional patent for the use of topical kinase inhibitors in the management of rosacea and recently co-started a biotechnology company called Praxis Biotechnology that aims to develop and test therapies for the condition. He serves as a consultant for both Bausch & Lomb and Valeant Pharmaceuticals.

Emergency Imaging: Facial Trauma After a Fall
An 89-year-old man presented to the ED with facial trauma due to a mechanical fall after losing his balance on uneven pavement and hitting the right side of his face. Physical examination revealed an ecchymosis inferior to the right eye and tenderness to palpation at the right maxilla and bilateral nasolabial folds. Maxillofacial computed tomography (CT) was ordered for further evaluation; representative images are presented above (Figure 1a and 1b).

What is the diagnosis?
Answer
A noncontrast CT of the maxillofacial bones demonstrated acute fractures through the bilateral pterygoid plates (white arrows, Figure 2a). The fractures extended through the medial and lateral walls of the bilateral maxillary sinuses (red arrows, Figure 2a), and propagated to the frontal processes of the maxilla (red arrows, Figure 2b), extending toward the alveolar process, indicating involvement of the anterolateral margin of the nasal fossa. The full extent of the fracture is best seen on a 3D-reconstructed image (red arrows, Figure 3). Additional images (not presented here) confirmed no fracture involvement of the orbital floors, nasal bones, or zygomatic arches. Expected posttraumatic hemorrhage was appreciated within the maxillary sinuses (white asterisks, Figure 2a).

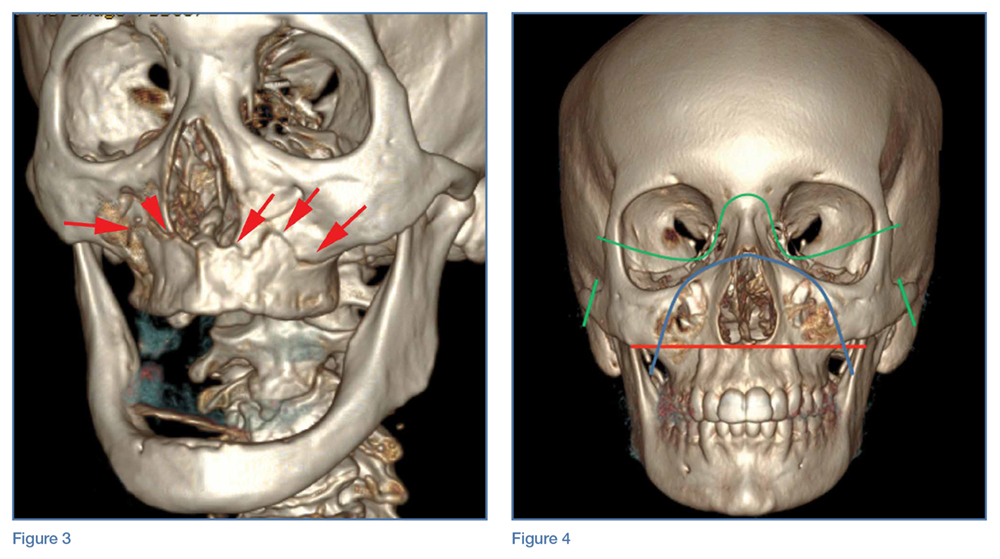
Le Fort Fractures
The findings described above are characteristic of a Le Fort I fracture pattern. Initially described in 1901 by René Le Fort, a French surgeon, the Le Fort classification system details somewhat predictable midface fracture patterns resulting in various degrees of craniofacial disassociation.1 Using weights that were dropped on cadaveric heads, Le Fort discovered that the pterygoid plates must be disrupted in order for the midface facial bones to separate from the skull base. As such, when diagnosing a Le Fort fracture, fracture of the pterygoid plate must be present, regardless of the fracture type (Le Fort I, II, and III).2
Le Fort I Fracture. This fracture pattern (red line, Figure 4) is referred to as a “floating palate” and involves separation of the hard palate from the skull base via fracture extension from the pterygoid plates into the maxillary sinus walls, as demonstrated in this case. The key distinguisher of the Le Fort I pattern is involvement of the anterolateral margin of the nasal fossa.2
Le Fort II Fracture. This fracture pattern (blue line, Figure 4) describes a “floating maxilla” wherein the pterygoid plate fractures are met with a pyramidal-type fracture pattern of the midface. The maxillary teeth form the base of the pyramid, and the fracture extends superiorly through the infraorbital rims bilaterally and toward the nasofrontal suture.2,3 Le Fort II fractures result in the maxilla floating freely from the rest of the midface and skull base.
Le Fort III Fracture. This fracture pattern (green lines, Figure 4) describes a “floating face” with complete craniofacial disjunction resulting from fracture of the pterygoid plates, nasofrontal suture, maxillofrontal suture, orbital wall, and zygomatic arch/zygomaticofrontal suture.2,3
It is important to note that midface trauma represents a complex spectrum of injuries, and Le Fort fractures only account for a small percentage of facial bone fractures that present through Level 1 trauma centers.2 Le Fort fracture patterns can coexist with other fracture patterns and also can be seen in combination with each other. For example, one side of the face may demonstrate a Le Fort II pattern while the other side concurrently demonstrates a Le Fort III pattern. Though not robust enough for complete description of and surgical planning for facial fractures, this classification system is a succinct and well-accepted means of describing major fracture planes.
1. Le Fort R. Etude experimentale sur les fractures de la machoire superieure. Rev Chir. 1901;23:208-227, 360-379, 479-507.
2. Rhea JT, Novelline RA. How to simplify the CT diagnosis of Le Fort fractures. AJR Am J Roentgenol. 2005;184(5):1700-1705.
3. Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-793.
An 89-year-old man presented to the ED with facial trauma due to a mechanical fall after losing his balance on uneven pavement and hitting the right side of his face. Physical examination revealed an ecchymosis inferior to the right eye and tenderness to palpation at the right maxilla and bilateral nasolabial folds. Maxillofacial computed tomography (CT) was ordered for further evaluation; representative images are presented above (Figure 1a and 1b).
What is the diagnosis?
Answer
A noncontrast CT of the maxillofacial bones demonstrated acute fractures through the bilateral pterygoid plates (white arrows, Figure 2a). The fractures extended through the medial and lateral walls of the bilateral maxillary sinuses (red arrows, Figure 2a), and propagated to the frontal processes of the maxilla (red arrows, Figure 2b), extending toward the alveolar process, indicating involvement of the anterolateral margin of the nasal fossa. The full extent of the fracture is best seen on a 3D-reconstructed image (red arrows, Figure 3). Additional images (not presented here) confirmed no fracture involvement of the orbital floors, nasal bones, or zygomatic arches. Expected posttraumatic hemorrhage was appreciated within the maxillary sinuses (white asterisks, Figure 2a).
Le Fort Fractures
The findings described above are characteristic of a Le Fort I fracture pattern. Initially described in 1901 by René Le Fort, a French surgeon, the Le Fort classification system details somewhat predictable midface fracture patterns resulting in various degrees of craniofacial disassociation.1 Using weights that were dropped on cadaveric heads, Le Fort discovered that the pterygoid plates must be disrupted in order for the midface facial bones to separate from the skull base. As such, when diagnosing a Le Fort fracture, fracture of the pterygoid plate must be present, regardless of the fracture type (Le Fort I, II, and III).2
Le Fort I Fracture. This fracture pattern (red line, Figure 4) is referred to as a “floating palate” and involves separation of the hard palate from the skull base via fracture extension from the pterygoid plates into the maxillary sinus walls, as demonstrated in this case. The key distinguisher of the Le Fort I pattern is involvement of the anterolateral margin of the nasal fossa.2
Le Fort II Fracture. This fracture pattern (blue line, Figure 4) describes a “floating maxilla” wherein the pterygoid plate fractures are met with a pyramidal-type fracture pattern of the midface. The maxillary teeth form the base of the pyramid, and the fracture extends superiorly through the infraorbital rims bilaterally and toward the nasofrontal suture.2,3 Le Fort II fractures result in the maxilla floating freely from the rest of the midface and skull base.
Le Fort III Fracture. This fracture pattern (green lines, Figure 4) describes a “floating face” with complete craniofacial disjunction resulting from fracture of the pterygoid plates, nasofrontal suture, maxillofrontal suture, orbital wall, and zygomatic arch/zygomaticofrontal suture.2,3
It is important to note that midface trauma represents a complex spectrum of injuries, and Le Fort fractures only account for a small percentage of facial bone fractures that present through Level 1 trauma centers.2 Le Fort fracture patterns can coexist with other fracture patterns and also can be seen in combination with each other. For example, one side of the face may demonstrate a Le Fort II pattern while the other side concurrently demonstrates a Le Fort III pattern. Though not robust enough for complete description of and surgical planning for facial fractures, this classification system is a succinct and well-accepted means of describing major fracture planes.
An 89-year-old man presented to the ED with facial trauma due to a mechanical fall after losing his balance on uneven pavement and hitting the right side of his face. Physical examination revealed an ecchymosis inferior to the right eye and tenderness to palpation at the right maxilla and bilateral nasolabial folds. Maxillofacial computed tomography (CT) was ordered for further evaluation; representative images are presented above (Figure 1a and 1b).
What is the diagnosis?
Answer
A noncontrast CT of the maxillofacial bones demonstrated acute fractures through the bilateral pterygoid plates (white arrows, Figure 2a). The fractures extended through the medial and lateral walls of the bilateral maxillary sinuses (red arrows, Figure 2a), and propagated to the frontal processes of the maxilla (red arrows, Figure 2b), extending toward the alveolar process, indicating involvement of the anterolateral margin of the nasal fossa. The full extent of the fracture is best seen on a 3D-reconstructed image (red arrows, Figure 3). Additional images (not presented here) confirmed no fracture involvement of the orbital floors, nasal bones, or zygomatic arches. Expected posttraumatic hemorrhage was appreciated within the maxillary sinuses (white asterisks, Figure 2a).
Le Fort Fractures
The findings described above are characteristic of a Le Fort I fracture pattern. Initially described in 1901 by René Le Fort, a French surgeon, the Le Fort classification system details somewhat predictable midface fracture patterns resulting in various degrees of craniofacial disassociation.1 Using weights that were dropped on cadaveric heads, Le Fort discovered that the pterygoid plates must be disrupted in order for the midface facial bones to separate from the skull base. As such, when diagnosing a Le Fort fracture, fracture of the pterygoid plate must be present, regardless of the fracture type (Le Fort I, II, and III).2
Le Fort I Fracture. This fracture pattern (red line, Figure 4) is referred to as a “floating palate” and involves separation of the hard palate from the skull base via fracture extension from the pterygoid plates into the maxillary sinus walls, as demonstrated in this case. The key distinguisher of the Le Fort I pattern is involvement of the anterolateral margin of the nasal fossa.2
Le Fort II Fracture. This fracture pattern (blue line, Figure 4) describes a “floating maxilla” wherein the pterygoid plate fractures are met with a pyramidal-type fracture pattern of the midface. The maxillary teeth form the base of the pyramid, and the fracture extends superiorly through the infraorbital rims bilaterally and toward the nasofrontal suture.2,3 Le Fort II fractures result in the maxilla floating freely from the rest of the midface and skull base.
Le Fort III Fracture. This fracture pattern (green lines, Figure 4) describes a “floating face” with complete craniofacial disjunction resulting from fracture of the pterygoid plates, nasofrontal suture, maxillofrontal suture, orbital wall, and zygomatic arch/zygomaticofrontal suture.2,3
It is important to note that midface trauma represents a complex spectrum of injuries, and Le Fort fractures only account for a small percentage of facial bone fractures that present through Level 1 trauma centers.2 Le Fort fracture patterns can coexist with other fracture patterns and also can be seen in combination with each other. For example, one side of the face may demonstrate a Le Fort II pattern while the other side concurrently demonstrates a Le Fort III pattern. Though not robust enough for complete description of and surgical planning for facial fractures, this classification system is a succinct and well-accepted means of describing major fracture planes.
1. Le Fort R. Etude experimentale sur les fractures de la machoire superieure. Rev Chir. 1901;23:208-227, 360-379, 479-507.
2. Rhea JT, Novelline RA. How to simplify the CT diagnosis of Le Fort fractures. AJR Am J Roentgenol. 2005;184(5):1700-1705.
3. Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-793.
1. Le Fort R. Etude experimentale sur les fractures de la machoire superieure. Rev Chir. 1901;23:208-227, 360-379, 479-507.
2. Rhea JT, Novelline RA. How to simplify the CT diagnosis of Le Fort fractures. AJR Am J Roentgenol. 2005;184(5):1700-1705.
3. Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-793.

First EDition: Retail Clinics and Rate of ED Visits, more
Retail Clinics Have Not Decreased the Rate of Low-Acuity ED Visits
BY JEFF BAUER
The number of retail clinics—those located in pharmacies, supermarkets, and other retail settings—in the United States increased from 130 in 2006 to nearly 1,400 in 2012. However, this proliferation of retail clinics has not lead to a meaningful reduction in low-acuity ED visits, according to a recent observational study published in Annals of Emergency Medicine.1
Using information from the Healthcare Cost and Utilization Project State Emergency Department Databases, which include data on more than 2,000 EDs in 23 states from 2006 through 2013, researchers looked at the association between retail clinic penetration and the rate of treat-and-release ED visits for 11 low-acuity conditions (allergic rhinitis, bronchitis, conjunctivitis, other eye conditions, influenza, otitis externa, otitis media, pharyngitis, upper respiratory infections/sinusitis, urinary tract infections, and viral infections).
Retail clinic penetration was defined as the percentage of an ED’s catchment area (areas that accounted for up to 75% of patients who visited for low-acuity conditions) that overlapped with the 10-minute-drive radius of a retail clinic. The results were calculated as a rate ratio, which reflected the change in the rate of low-acuity ED visits associated with an ED having no retail clinic penetration to having approximately the average penetration rate within 2012. Results were controlled for the number of urgent care centers that were present in each ED catchment area, but only for hospital-associated urgent care centers, as there are no reliable data to identify all urgent care centers.
Retail clinic penetration more than doubled during the study period. Overall, increased retail clinic penetration was not associated with a change in the rate of low-acuity ED visits. Among patients with private insurance, there was a small reduction (0.3% per calendar quarter) in ED visits for low-acuity conditions, but this translated into an estimated 17 fewer ED visits by privately insured patients over 1 year for the average ED, assuming the retail clinic penetration rate increased by 40% in that year.
In an accompanying editorial,2 Jesse M. Pines, MD, suggests that visits to retail clinics may be mostly “new-use” visits, meaning many individuals who would not have otherwise received treatment seek care in a retail clinic because such clinics are available. Dr Pines proposed three reasons retail clinics may create new-use visits: they meet unmet demands for care; motivations for seeking care differ in EDs and retail clinics; and people who are more likely to use EDs for low-acuity conditions do so because they have limited access to other types of care, including retail clinics.
1. Martsolf G, Fingar KR, Coffey R, et al. Association between the opening of retail clinics and low-acuity emergency department visits. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.08.462.
2. Pines JM. Why retail clinics do not substitute for emergency department visits and what this means for value-based care. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.09.047.
Hypotension During Transport to ED Drives Mortality in Traumatic Brain Injury
MITCHEL L. ZOLER
FRONTLINE MEDICAL NEWS
The severity and duration of hypotension in traumatic brain injury (TBI) patients during emergency medical service (EMS) transport to an ED has a tight and essentially linear relationship to mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure (BP) was <90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with TBI leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should be completed by the end of 2017, said Dr Spaite, professor of emergency medicine at the University of Arizona in Tucson.Results from prior studies have clearly linked prehospital hypotension with worse survival in TBI patients. Until now, however, there was no appreciation of the fact that not all hypotensive episodes are equal, and that both the severity of hypotension and its duration incrementally contribute to mortality as the “dose” of hypotension a patient experiences increases. In large part, this is because prehospital hypotension has been recorded simply as a dichotomous, yes/no condition.
The innovation introduced by Dr Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI. Their calculations were limited to patients with EMS records of at least two BP measurements during prehospital transport. These data allowed Spaite et al to utilize both the extent to which systolic BP dropped below 90 mm Hg and the amount of time systolic BP was below this threshold to better define the total hypotension exposure each patient received.
This meant that a patient with a TBI and a systolic BP of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a systolic BP of 85 mm Hg for 10 minutes and a patient with a systolic BP of 80 mm Hg for 5 minutes.
The analysis by Spaite et al also adjusted the relationship of total hypotensive severity and duration and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension severity and duration and mortality, Dr Spaite said.
The EPIC-TBI enrolled TBI patients aged 10 years or older during 2007 to 2014 through participation of dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two BP measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising BP via intravenous (IV) fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the implementation of the third edition of the TBI guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension severity and duration each patient experienced, he noted.
“What’s remarkable is that the single prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr Spaite said.
1. Spaite DW. Presentation at: American Heart Association Scientific Sessions 2016. November 12-16, 2016; New Orleans, LA.
Fluid Administration in Sepsis Did Not Increase Need for Dialysis
M. Alexander Otto
FRONTLINE MEDICAL NEWS
Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Texas.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio [OR], 0.915; 95% confidence interval [CI], 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L of fluid had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).
These findings come from a quality improvement project the hospital launched after researchers there realized that the benchmark Surviving Sepsis Campaign guidelines were not being met. The patients in the study had a systolic BP below 90 mm Hg or lactate level of at least 4 mmol/L. The guidelines would have called for these patients to receive 30 mL/kg of crystalloid fluids within 3 hours of presentation, but only 28 patients (17%) met that mark.
“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received ≥30 mL/kg of fluid resuscitation, while 28% received ≥20 mL/kg of IV fluid resuscitation. It turned out that staff in the ED—where most of the patients were treated in the critical first 6 hours—were concerned about fluid overload and putting patients into respiratory, heart, or renal failure, Dr Jahoor said. The team found no difference in mortality rates when patients received 30 mL/kg—just over 2 L in a patient weighing 70 kg—vs 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27% and 32%, respectively.
There also were no increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter.’ You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” she said.
1. Jahoor A, Delmas T, Giri B, et al. Fluid resuscitation of at least 1 liter in septic patients decreases the need for renal replacement therapy without increasing the risk of acute congestive heart failure or acute respiratory failure. Chest. 2016;150(4_S):349A. doi:10.1016/j.chest.2016.08.362.
Survey: Antibiotic Shortages Are the New Norm
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Antibiotic shortages reported by the Emerging Infections Network (EIN) in 2011 persist in 2016, according to a Web-based follow-up survey of infectious disease physicians.
Of 701 network members who responded to the EIN survey in early 2016, 70% reported needing to modify their antimicrobial choice because of a shortage in the past 2 years. They did so by using broader-spectrum agents (75% of respondents), more costly agents (58%), less effective second-line agents (45%), and more toxic agents (37%), Adi Gundlapalli, MD, PhD, reported at an annual scientific meeting on infectious diseases.
In addition, 73% of respondents reported that the shortages affected patient care or outcomes, reported Dr Gundlapalli of the University of Utah, Salt Lake City.
The percentage of respondents reporting adverse patient outcomes related to shortages increased from 2011 to 2016 (51% vs 73%), he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In the 2016 survey, the top 10 antimicrobials reported as being in short supply over the past 2 years were piperacillin-tazobactam, ampicillin-sulbactam, meropenem, cefotaxime, cefepime, trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, imipenem, acyclovir, and amikacin. Trimethoprim-sulfamethoxazole and acyclovir were in short supply in 2011 and 2016.
According to respondents, the most common ways they learned about drug shortages were from hospital notification (76%), from a colleague (56%), from a pharmacy that contacted them regarding a prescription for the agent (53%), or from the US Food and Drug Administration (FDA) Web site or another Web site (23%). The most common ways of learning about a shortage changed—from notification after trying to prescribe a drug in 2011, to proactive hospital/system (local) notification in 2016; 71% of respondents said that communications in 2016 were sufficient.
Most respondents (83%) reported that guidelines for dealing with shortages had been developed by an antimicrobial stewardship program (ASP) at their institution.
“This, I think, is one of the highlight results,” said Dr Gundlapalli, who is also a staff physician at the VA Salt Lake City Health System. “In 2011, we had no specific question or comments received about [ASPs], and here in 2016, 83% of respondents’ institutions had developed guidelines related to drug shortages.”
Respondents also had the opportunity to submit free-text responses, and among the themes that emerged was concern regarding toxicity and adverse outcomes associated with increased use of aminoglycosides because of the shortage of piperacillin-tazobactam. Another was the shortage of meropenem, which led one ASP to “institute restrictions on its use, which have continued,” he said.
“Another theme was ‘simpler agents seem more likely to be in shortage,’ ” Dr Gundlapalli said, noting ampicillin-sulbactam in 2016 and penicillin G procaine as examples.
“And then, of course, the other theme across the board...was our new asset,” he said, explaining that some respondents commented on the value of ASP pharmacists and programs to help with drug shortage issues.
The overall theme of this follow-up survey, in the context of prior surveys in 2001 and 2011, is that antibiotic shortages are the “new normal—a way of life,” Dr Gundlapalli said.
“The concerns do persist, and we feel there is further work to be done here,” he said. He specifically noted that there is a need to inform and educate fellows and colleagues in hospitals, increase awareness generally, improve communication strategies, and conduct detailed studies on adverse effects and outcomes.
“And now, since ASPs are very pervasive...maybe it’s time to formalize and delineate the role of ASPs in antimicrobial shortages,” he said.
Donald Graham, MD, one of the study’s coauthors, said he believes the problem is in part the result of economics, and in part because of “the higher standards that the FDA imposes upon these manufacturing concerns.” These drugs often are low-profit items, and it is not always in the financial best interest of a pharmaceutical company to upgrade their facilities.
1. Gundlapalli A. Presentation at: IDWeek 2016. October 26-30, 2016. New Orleans, LA.
Hospitalizations for Opioid Poisoning Tripled in Preschool Children
Richard Franki
FRONTLINE MEDICAL NEWS
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1 to 19 years, according to data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1 to 19 years, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Connecticut.
The greatest change occurred among the youngest children, as the number of those aged 1 to 4 years rose from 133 in 1997 to 421 in 2012—an increase of 217%. For those aged 15 to 19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators,
The increase in hospitalizations for prescription opioid poisoning in children aged 10 to 14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-old children did not meet the criteria for statistical reliability and were not included in the analysis, Dr Gaither and her associates said.
1. Gaither JR, Leventhal JM, Ryan SA, Camenga DR. National trends in hospitalizations for opioid poisonings among children and adolescents, 1997 to 2012. JAMA Pediatr. 2016 Oct 31. Epub ahead of print. doi:10.1001/jamapediatrics.2016.2154.
Pelvic Fracture Pattern Predicts the Need for Hemorrhage Control
Doug Brunk
FRONTLINE MEDICAL NEWS
Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage-control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma (AAST). They identified three main force patterns: lateral compression, anterior posterior compression, and vertical shear.
“They were able to show that certain pelvic fractures were associated with soft-tissue injury and pelvic hemorrhage,” said Dr Costantini, of the division of trauma, surgical critical care, burns and acute care surgery at the University of California, San Diego. “Since then, several single-center studies have been conducted in an attempt to correlate fracture pattern with the risk of pelvic hemorrhage. A majority of these studies evaluated angiogram [and embolization] as the endpoint for hemorrhage control. Modern trauma care has evolved to include multiple modalities to control hemorrhage, which include pelvic external fixator placement, pelvic angiography and embolization, preperitoneal pelvic packing, and the use of the REBOA [Resuscitative Endovascular Balloon Occlusion of the Aorta] catheter as an adjunct to hemorrhage control.”
In a recently published study, Dr Costantini and his associates found wide variability in the use of pelvic hemorrhage-control methods.1 “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level 1 trauma centers over a 2-year period.2 Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over age 18 years, blunt mechanism of injury, and shock on admission defined as “...systolic blood pressure <90 mm Hg or heart rate >120 beats per minute or base deficit <-5.”1 Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr Costantini said. Next, they used univariate and multivariate logistic regression analyses to examine predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the 2-year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic BP was 93 mm Hg, their mean HR was 117 beats/min, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian vs auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage-control intervention, those who did received more transfusion of packed red blood cells (13 vs 7 units, respectively; P < .01) and fresh frozen plasma (10 U vs 5 U; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage-control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (OR, 109.43; P < .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
1. Costantini TW, Coimbra R, Holcomb JB, et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J Trauma Acute Care Surg. 2016;80(5):717-723; discussion 723-725. doi:10.1097/TA.0000000000001034.2. Costantini TW. Presentation at: 75th Annual Meeting of American Association for the Surgery of Trauma (AAST) and Clinical Congress of Acute Care Surgery. September 14-17, 2016. Waikoloa, Hawaii.
Retail Clinics Have Not Decreased the Rate of Low-Acuity ED Visits
BY JEFF BAUER
The number of retail clinics—those located in pharmacies, supermarkets, and other retail settings—in the United States increased from 130 in 2006 to nearly 1,400 in 2012. However, this proliferation of retail clinics has not lead to a meaningful reduction in low-acuity ED visits, according to a recent observational study published in Annals of Emergency Medicine.1
Using information from the Healthcare Cost and Utilization Project State Emergency Department Databases, which include data on more than 2,000 EDs in 23 states from 2006 through 2013, researchers looked at the association between retail clinic penetration and the rate of treat-and-release ED visits for 11 low-acuity conditions (allergic rhinitis, bronchitis, conjunctivitis, other eye conditions, influenza, otitis externa, otitis media, pharyngitis, upper respiratory infections/sinusitis, urinary tract infections, and viral infections).
Retail clinic penetration was defined as the percentage of an ED’s catchment area (areas that accounted for up to 75% of patients who visited for low-acuity conditions) that overlapped with the 10-minute-drive radius of a retail clinic. The results were calculated as a rate ratio, which reflected the change in the rate of low-acuity ED visits associated with an ED having no retail clinic penetration to having approximately the average penetration rate within 2012. Results were controlled for the number of urgent care centers that were present in each ED catchment area, but only for hospital-associated urgent care centers, as there are no reliable data to identify all urgent care centers.
Retail clinic penetration more than doubled during the study period. Overall, increased retail clinic penetration was not associated with a change in the rate of low-acuity ED visits. Among patients with private insurance, there was a small reduction (0.3% per calendar quarter) in ED visits for low-acuity conditions, but this translated into an estimated 17 fewer ED visits by privately insured patients over 1 year for the average ED, assuming the retail clinic penetration rate increased by 40% in that year.
In an accompanying editorial,2 Jesse M. Pines, MD, suggests that visits to retail clinics may be mostly “new-use” visits, meaning many individuals who would not have otherwise received treatment seek care in a retail clinic because such clinics are available. Dr Pines proposed three reasons retail clinics may create new-use visits: they meet unmet demands for care; motivations for seeking care differ in EDs and retail clinics; and people who are more likely to use EDs for low-acuity conditions do so because they have limited access to other types of care, including retail clinics.
1. Martsolf G, Fingar KR, Coffey R, et al. Association between the opening of retail clinics and low-acuity emergency department visits. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.08.462.
2. Pines JM. Why retail clinics do not substitute for emergency department visits and what this means for value-based care. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.09.047.
Hypotension During Transport to ED Drives Mortality in Traumatic Brain Injury
MITCHEL L. ZOLER
FRONTLINE MEDICAL NEWS
The severity and duration of hypotension in traumatic brain injury (TBI) patients during emergency medical service (EMS) transport to an ED has a tight and essentially linear relationship to mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure (BP) was <90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with TBI leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should be completed by the end of 2017, said Dr Spaite, professor of emergency medicine at the University of Arizona in Tucson.Results from prior studies have clearly linked prehospital hypotension with worse survival in TBI patients. Until now, however, there was no appreciation of the fact that not all hypotensive episodes are equal, and that both the severity of hypotension and its duration incrementally contribute to mortality as the “dose” of hypotension a patient experiences increases. In large part, this is because prehospital hypotension has been recorded simply as a dichotomous, yes/no condition.
The innovation introduced by Dr Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI. Their calculations were limited to patients with EMS records of at least two BP measurements during prehospital transport. These data allowed Spaite et al to utilize both the extent to which systolic BP dropped below 90 mm Hg and the amount of time systolic BP was below this threshold to better define the total hypotension exposure each patient received.
This meant that a patient with a TBI and a systolic BP of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a systolic BP of 85 mm Hg for 10 minutes and a patient with a systolic BP of 80 mm Hg for 5 minutes.
The analysis by Spaite et al also adjusted the relationship of total hypotensive severity and duration and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension severity and duration and mortality, Dr Spaite said.
The EPIC-TBI enrolled TBI patients aged 10 years or older during 2007 to 2014 through participation of dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two BP measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising BP via intravenous (IV) fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the implementation of the third edition of the TBI guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension severity and duration each patient experienced, he noted.
“What’s remarkable is that the single prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr Spaite said.
1. Spaite DW. Presentation at: American Heart Association Scientific Sessions 2016. November 12-16, 2016; New Orleans, LA.
Fluid Administration in Sepsis Did Not Increase Need for Dialysis
M. Alexander Otto
FRONTLINE MEDICAL NEWS
Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Texas.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio [OR], 0.915; 95% confidence interval [CI], 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L of fluid had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).
These findings come from a quality improvement project the hospital launched after researchers there realized that the benchmark Surviving Sepsis Campaign guidelines were not being met. The patients in the study had a systolic BP below 90 mm Hg or lactate level of at least 4 mmol/L. The guidelines would have called for these patients to receive 30 mL/kg of crystalloid fluids within 3 hours of presentation, but only 28 patients (17%) met that mark.
“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received ≥30 mL/kg of fluid resuscitation, while 28% received ≥20 mL/kg of IV fluid resuscitation. It turned out that staff in the ED—where most of the patients were treated in the critical first 6 hours—were concerned about fluid overload and putting patients into respiratory, heart, or renal failure, Dr Jahoor said. The team found no difference in mortality rates when patients received 30 mL/kg—just over 2 L in a patient weighing 70 kg—vs 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27% and 32%, respectively.
There also were no increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter.’ You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” she said.
1. Jahoor A, Delmas T, Giri B, et al. Fluid resuscitation of at least 1 liter in septic patients decreases the need for renal replacement therapy without increasing the risk of acute congestive heart failure or acute respiratory failure. Chest. 2016;150(4_S):349A. doi:10.1016/j.chest.2016.08.362.
Survey: Antibiotic Shortages Are the New Norm
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Antibiotic shortages reported by the Emerging Infections Network (EIN) in 2011 persist in 2016, according to a Web-based follow-up survey of infectious disease physicians.
Of 701 network members who responded to the EIN survey in early 2016, 70% reported needing to modify their antimicrobial choice because of a shortage in the past 2 years. They did so by using broader-spectrum agents (75% of respondents), more costly agents (58%), less effective second-line agents (45%), and more toxic agents (37%), Adi Gundlapalli, MD, PhD, reported at an annual scientific meeting on infectious diseases.
In addition, 73% of respondents reported that the shortages affected patient care or outcomes, reported Dr Gundlapalli of the University of Utah, Salt Lake City.
The percentage of respondents reporting adverse patient outcomes related to shortages increased from 2011 to 2016 (51% vs 73%), he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In the 2016 survey, the top 10 antimicrobials reported as being in short supply over the past 2 years were piperacillin-tazobactam, ampicillin-sulbactam, meropenem, cefotaxime, cefepime, trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, imipenem, acyclovir, and amikacin. Trimethoprim-sulfamethoxazole and acyclovir were in short supply in 2011 and 2016.
According to respondents, the most common ways they learned about drug shortages were from hospital notification (76%), from a colleague (56%), from a pharmacy that contacted them regarding a prescription for the agent (53%), or from the US Food and Drug Administration (FDA) Web site or another Web site (23%). The most common ways of learning about a shortage changed—from notification after trying to prescribe a drug in 2011, to proactive hospital/system (local) notification in 2016; 71% of respondents said that communications in 2016 were sufficient.
Most respondents (83%) reported that guidelines for dealing with shortages had been developed by an antimicrobial stewardship program (ASP) at their institution.
“This, I think, is one of the highlight results,” said Dr Gundlapalli, who is also a staff physician at the VA Salt Lake City Health System. “In 2011, we had no specific question or comments received about [ASPs], and here in 2016, 83% of respondents’ institutions had developed guidelines related to drug shortages.”
Respondents also had the opportunity to submit free-text responses, and among the themes that emerged was concern regarding toxicity and adverse outcomes associated with increased use of aminoglycosides because of the shortage of piperacillin-tazobactam. Another was the shortage of meropenem, which led one ASP to “institute restrictions on its use, which have continued,” he said.
“Another theme was ‘simpler agents seem more likely to be in shortage,’ ” Dr Gundlapalli said, noting ampicillin-sulbactam in 2016 and penicillin G procaine as examples.
“And then, of course, the other theme across the board...was our new asset,” he said, explaining that some respondents commented on the value of ASP pharmacists and programs to help with drug shortage issues.
The overall theme of this follow-up survey, in the context of prior surveys in 2001 and 2011, is that antibiotic shortages are the “new normal—a way of life,” Dr Gundlapalli said.
“The concerns do persist, and we feel there is further work to be done here,” he said. He specifically noted that there is a need to inform and educate fellows and colleagues in hospitals, increase awareness generally, improve communication strategies, and conduct detailed studies on adverse effects and outcomes.
“And now, since ASPs are very pervasive...maybe it’s time to formalize and delineate the role of ASPs in antimicrobial shortages,” he said.
Donald Graham, MD, one of the study’s coauthors, said he believes the problem is in part the result of economics, and in part because of “the higher standards that the FDA imposes upon these manufacturing concerns.” These drugs often are low-profit items, and it is not always in the financial best interest of a pharmaceutical company to upgrade their facilities.
1. Gundlapalli A. Presentation at: IDWeek 2016. October 26-30, 2016. New Orleans, LA.
Hospitalizations for Opioid Poisoning Tripled in Preschool Children
Richard Franki
FRONTLINE MEDICAL NEWS
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1 to 19 years, according to data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1 to 19 years, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Connecticut.
The greatest change occurred among the youngest children, as the number of those aged 1 to 4 years rose from 133 in 1997 to 421 in 2012—an increase of 217%. For those aged 15 to 19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators,
The increase in hospitalizations for prescription opioid poisoning in children aged 10 to 14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-old children did not meet the criteria for statistical reliability and were not included in the analysis, Dr Gaither and her associates said.
1. Gaither JR, Leventhal JM, Ryan SA, Camenga DR. National trends in hospitalizations for opioid poisonings among children and adolescents, 1997 to 2012. JAMA Pediatr. 2016 Oct 31. Epub ahead of print. doi:10.1001/jamapediatrics.2016.2154.
Pelvic Fracture Pattern Predicts the Need for Hemorrhage Control
Doug Brunk
FRONTLINE MEDICAL NEWS
Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage-control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma (AAST). They identified three main force patterns: lateral compression, anterior posterior compression, and vertical shear.
“They were able to show that certain pelvic fractures were associated with soft-tissue injury and pelvic hemorrhage,” said Dr Costantini, of the division of trauma, surgical critical care, burns and acute care surgery at the University of California, San Diego. “Since then, several single-center studies have been conducted in an attempt to correlate fracture pattern with the risk of pelvic hemorrhage. A majority of these studies evaluated angiogram [and embolization] as the endpoint for hemorrhage control. Modern trauma care has evolved to include multiple modalities to control hemorrhage, which include pelvic external fixator placement, pelvic angiography and embolization, preperitoneal pelvic packing, and the use of the REBOA [Resuscitative Endovascular Balloon Occlusion of the Aorta] catheter as an adjunct to hemorrhage control.”
In a recently published study, Dr Costantini and his associates found wide variability in the use of pelvic hemorrhage-control methods.1 “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level 1 trauma centers over a 2-year period.2 Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over age 18 years, blunt mechanism of injury, and shock on admission defined as “...systolic blood pressure <90 mm Hg or heart rate >120 beats per minute or base deficit <-5.”1 Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr Costantini said. Next, they used univariate and multivariate logistic regression analyses to examine predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the 2-year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic BP was 93 mm Hg, their mean HR was 117 beats/min, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian vs auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage-control intervention, those who did received more transfusion of packed red blood cells (13 vs 7 units, respectively; P < .01) and fresh frozen plasma (10 U vs 5 U; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage-control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (OR, 109.43; P < .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
1. Costantini TW, Coimbra R, Holcomb JB, et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J Trauma Acute Care Surg. 2016;80(5):717-723; discussion 723-725. doi:10.1097/TA.0000000000001034.2. Costantini TW. Presentation at: 75th Annual Meeting of American Association for the Surgery of Trauma (AAST) and Clinical Congress of Acute Care Surgery. September 14-17, 2016. Waikoloa, Hawaii.
Retail Clinics Have Not Decreased the Rate of Low-Acuity ED Visits
BY JEFF BAUER
The number of retail clinics—those located in pharmacies, supermarkets, and other retail settings—in the United States increased from 130 in 2006 to nearly 1,400 in 2012. However, this proliferation of retail clinics has not lead to a meaningful reduction in low-acuity ED visits, according to a recent observational study published in Annals of Emergency Medicine.1
Using information from the Healthcare Cost and Utilization Project State Emergency Department Databases, which include data on more than 2,000 EDs in 23 states from 2006 through 2013, researchers looked at the association between retail clinic penetration and the rate of treat-and-release ED visits for 11 low-acuity conditions (allergic rhinitis, bronchitis, conjunctivitis, other eye conditions, influenza, otitis externa, otitis media, pharyngitis, upper respiratory infections/sinusitis, urinary tract infections, and viral infections).
Retail clinic penetration was defined as the percentage of an ED’s catchment area (areas that accounted for up to 75% of patients who visited for low-acuity conditions) that overlapped with the 10-minute-drive radius of a retail clinic. The results were calculated as a rate ratio, which reflected the change in the rate of low-acuity ED visits associated with an ED having no retail clinic penetration to having approximately the average penetration rate within 2012. Results were controlled for the number of urgent care centers that were present in each ED catchment area, but only for hospital-associated urgent care centers, as there are no reliable data to identify all urgent care centers.
Retail clinic penetration more than doubled during the study period. Overall, increased retail clinic penetration was not associated with a change in the rate of low-acuity ED visits. Among patients with private insurance, there was a small reduction (0.3% per calendar quarter) in ED visits for low-acuity conditions, but this translated into an estimated 17 fewer ED visits by privately insured patients over 1 year for the average ED, assuming the retail clinic penetration rate increased by 40% in that year.
In an accompanying editorial,2 Jesse M. Pines, MD, suggests that visits to retail clinics may be mostly “new-use” visits, meaning many individuals who would not have otherwise received treatment seek care in a retail clinic because such clinics are available. Dr Pines proposed three reasons retail clinics may create new-use visits: they meet unmet demands for care; motivations for seeking care differ in EDs and retail clinics; and people who are more likely to use EDs for low-acuity conditions do so because they have limited access to other types of care, including retail clinics.
1. Martsolf G, Fingar KR, Coffey R, et al. Association between the opening of retail clinics and low-acuity emergency department visits. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.08.462.
2. Pines JM. Why retail clinics do not substitute for emergency department visits and what this means for value-based care. Ann Emerg Med. 2016. In press. http://dx.doi.org/10.1016/j.annemergmed.2016.09.047.
Hypotension During Transport to ED Drives Mortality in Traumatic Brain Injury
MITCHEL L. ZOLER
FRONTLINE MEDICAL NEWS
The severity and duration of hypotension in traumatic brain injury (TBI) patients during emergency medical service (EMS) transport to an ED has a tight and essentially linear relationship to mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure (BP) was <90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with TBI leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should be completed by the end of 2017, said Dr Spaite, professor of emergency medicine at the University of Arizona in Tucson.Results from prior studies have clearly linked prehospital hypotension with worse survival in TBI patients. Until now, however, there was no appreciation of the fact that not all hypotensive episodes are equal, and that both the severity of hypotension and its duration incrementally contribute to mortality as the “dose” of hypotension a patient experiences increases. In large part, this is because prehospital hypotension has been recorded simply as a dichotomous, yes/no condition.
The innovation introduced by Dr Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI. Their calculations were limited to patients with EMS records of at least two BP measurements during prehospital transport. These data allowed Spaite et al to utilize both the extent to which systolic BP dropped below 90 mm Hg and the amount of time systolic BP was below this threshold to better define the total hypotension exposure each patient received.
This meant that a patient with a TBI and a systolic BP of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a systolic BP of 85 mm Hg for 10 minutes and a patient with a systolic BP of 80 mm Hg for 5 minutes.
The analysis by Spaite et al also adjusted the relationship of total hypotensive severity and duration and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension severity and duration and mortality, Dr Spaite said.
The EPIC-TBI enrolled TBI patients aged 10 years or older during 2007 to 2014 through participation of dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two BP measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising BP via intravenous (IV) fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the implementation of the third edition of the TBI guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension severity and duration each patient experienced, he noted.
“What’s remarkable is that the single prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr Spaite said.
1. Spaite DW. Presentation at: American Heart Association Scientific Sessions 2016. November 12-16, 2016; New Orleans, LA.
Fluid Administration in Sepsis Did Not Increase Need for Dialysis
M. Alexander Otto
FRONTLINE MEDICAL NEWS
Fluid administration of at least 1 L did not increase the incidence of acute respiratory or heart failure in severe sepsis, and actually seemed to decrease the need for dialysis in a review of 164 patients at Scott and White Memorial Hospital in Temple, Texas.
For every 1 mL of fluid administered per kilogram of body weight, the likelihood of dialysis decreased by 8.5% (odds ratio [OR], 0.915; 95% confidence interval [CI], 0.854-0.980; P = .0111), with no increase in heart or respiratory failure on univariate analysis. The 126 patients (77%) who received at least 1 L of fluid had a 68% reduction in the need for dialysis (OR, 0.32; CI, 0.117-0.890; P = .0288).
These findings come from a quality improvement project the hospital launched after researchers there realized that the benchmark Surviving Sepsis Campaign guidelines were not being met. The patients in the study had a systolic BP below 90 mm Hg or lactate level of at least 4 mmol/L. The guidelines would have called for these patients to receive 30 mL/kg of crystalloid fluids within 3 hours of presentation, but only 28 patients (17%) met that mark.
“The No. 1 reason we weren’t meeting benchmarks was fluid administration,” explained lead investigator Aruna Jahoor, MD, a pulmonary critical care and sleep medicine fellow at Texas Tech University Health Sciences Center.
Seventeen percent of patients received ≥30 mL/kg of fluid resuscitation, while 28% received ≥20 mL/kg of IV fluid resuscitation. It turned out that staff in the ED—where most of the patients were treated in the critical first 6 hours—were concerned about fluid overload and putting patients into respiratory, heart, or renal failure, Dr Jahoor said. The team found no difference in mortality rates when patients received 30 mL/kg—just over 2 L in a patient weighing 70 kg—vs 20 mL/kg or 1 L. The patients’ in-hospital mortality rate and 28-day mortality rate were 27% and 32%, respectively.
There also were no increased rates of heart failure, acute respiratory failure, or mechanical ventilation when patients received at least 1 L of fluid. “There were [also] lower rates of dialysis, which indicated that we weren’t overloading patients. Even when we looked at fluid as a continuous variable, we still didn’t see” complications, Dr Jahoor said.
The findings should be reassuring to treating physicians. “When you have pushback against 30-mL/kg administration, you can say ‘well, at least let’s give a liter.’ You don’t have to worry as much about some of the complications you are citing,’ ” she said.
For very obese patients, “it can get a little uncomfortable to be given” enough fluid to meet the 30-mL/kg goal, “but you can give at least a liter” without having to worry too much, she said. The patients in the study were treated from 2010 to 2013; normal saline was the most common resuscitation fluid. The hospital has since added the 30-mL/kg fluid resuscitation to its sepsis admission orders, and compliance has increased significantly.
A multivariate analysis is in the works to control for confounders. “We will probably [still] see you are not having increased rates of congestive heart or respiratory failure, or needing dialysis,” Dr Jahoor said. The protective effect against dialysis might drop out, “but I am hoping it doesn’t,” she said.
1. Jahoor A, Delmas T, Giri B, et al. Fluid resuscitation of at least 1 liter in septic patients decreases the need for renal replacement therapy without increasing the risk of acute congestive heart failure or acute respiratory failure. Chest. 2016;150(4_S):349A. doi:10.1016/j.chest.2016.08.362.
Survey: Antibiotic Shortages Are the New Norm
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Antibiotic shortages reported by the Emerging Infections Network (EIN) in 2011 persist in 2016, according to a Web-based follow-up survey of infectious disease physicians.
Of 701 network members who responded to the EIN survey in early 2016, 70% reported needing to modify their antimicrobial choice because of a shortage in the past 2 years. They did so by using broader-spectrum agents (75% of respondents), more costly agents (58%), less effective second-line agents (45%), and more toxic agents (37%), Adi Gundlapalli, MD, PhD, reported at an annual scientific meeting on infectious diseases.
In addition, 73% of respondents reported that the shortages affected patient care or outcomes, reported Dr Gundlapalli of the University of Utah, Salt Lake City.
The percentage of respondents reporting adverse patient outcomes related to shortages increased from 2011 to 2016 (51% vs 73%), he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In the 2016 survey, the top 10 antimicrobials reported as being in short supply over the past 2 years were piperacillin-tazobactam, ampicillin-sulbactam, meropenem, cefotaxime, cefepime, trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, imipenem, acyclovir, and amikacin. Trimethoprim-sulfamethoxazole and acyclovir were in short supply in 2011 and 2016.
According to respondents, the most common ways they learned about drug shortages were from hospital notification (76%), from a colleague (56%), from a pharmacy that contacted them regarding a prescription for the agent (53%), or from the US Food and Drug Administration (FDA) Web site or another Web site (23%). The most common ways of learning about a shortage changed—from notification after trying to prescribe a drug in 2011, to proactive hospital/system (local) notification in 2016; 71% of respondents said that communications in 2016 were sufficient.
Most respondents (83%) reported that guidelines for dealing with shortages had been developed by an antimicrobial stewardship program (ASP) at their institution.
“This, I think, is one of the highlight results,” said Dr Gundlapalli, who is also a staff physician at the VA Salt Lake City Health System. “In 2011, we had no specific question or comments received about [ASPs], and here in 2016, 83% of respondents’ institutions had developed guidelines related to drug shortages.”
Respondents also had the opportunity to submit free-text responses, and among the themes that emerged was concern regarding toxicity and adverse outcomes associated with increased use of aminoglycosides because of the shortage of piperacillin-tazobactam. Another was the shortage of meropenem, which led one ASP to “institute restrictions on its use, which have continued,” he said.
“Another theme was ‘simpler agents seem more likely to be in shortage,’ ” Dr Gundlapalli said, noting ampicillin-sulbactam in 2016 and penicillin G procaine as examples.
“And then, of course, the other theme across the board...was our new asset,” he said, explaining that some respondents commented on the value of ASP pharmacists and programs to help with drug shortage issues.
The overall theme of this follow-up survey, in the context of prior surveys in 2001 and 2011, is that antibiotic shortages are the “new normal—a way of life,” Dr Gundlapalli said.
“The concerns do persist, and we feel there is further work to be done here,” he said. He specifically noted that there is a need to inform and educate fellows and colleagues in hospitals, increase awareness generally, improve communication strategies, and conduct detailed studies on adverse effects and outcomes.
“And now, since ASPs are very pervasive...maybe it’s time to formalize and delineate the role of ASPs in antimicrobial shortages,” he said.
Donald Graham, MD, one of the study’s coauthors, said he believes the problem is in part the result of economics, and in part because of “the higher standards that the FDA imposes upon these manufacturing concerns.” These drugs often are low-profit items, and it is not always in the financial best interest of a pharmaceutical company to upgrade their facilities.
1. Gundlapalli A. Presentation at: IDWeek 2016. October 26-30, 2016. New Orleans, LA.
Hospitalizations for Opioid Poisoning Tripled in Preschool Children
Richard Franki
FRONTLINE MEDICAL NEWS
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1 to 19 years, according to data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1 to 19 years, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Connecticut.
The greatest change occurred among the youngest children, as the number of those aged 1 to 4 years rose from 133 in 1997 to 421 in 2012—an increase of 217%. For those aged 15 to 19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators,
The increase in hospitalizations for prescription opioid poisoning in children aged 10 to 14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-old children did not meet the criteria for statistical reliability and were not included in the analysis, Dr Gaither and her associates said.
1. Gaither JR, Leventhal JM, Ryan SA, Camenga DR. National trends in hospitalizations for opioid poisonings among children and adolescents, 1997 to 2012. JAMA Pediatr. 2016 Oct 31. Epub ahead of print. doi:10.1001/jamapediatrics.2016.2154.
Pelvic Fracture Pattern Predicts the Need for Hemorrhage Control
Doug Brunk
FRONTLINE MEDICAL NEWS
Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage-control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma (AAST). They identified three main force patterns: lateral compression, anterior posterior compression, and vertical shear.
“They were able to show that certain pelvic fractures were associated with soft-tissue injury and pelvic hemorrhage,” said Dr Costantini, of the division of trauma, surgical critical care, burns and acute care surgery at the University of California, San Diego. “Since then, several single-center studies have been conducted in an attempt to correlate fracture pattern with the risk of pelvic hemorrhage. A majority of these studies evaluated angiogram [and embolization] as the endpoint for hemorrhage control. Modern trauma care has evolved to include multiple modalities to control hemorrhage, which include pelvic external fixator placement, pelvic angiography and embolization, preperitoneal pelvic packing, and the use of the REBOA [Resuscitative Endovascular Balloon Occlusion of the Aorta] catheter as an adjunct to hemorrhage control.”
In a recently published study, Dr Costantini and his associates found wide variability in the use of pelvic hemorrhage-control methods.1 “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level 1 trauma centers over a 2-year period.2 Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over age 18 years, blunt mechanism of injury, and shock on admission defined as “...systolic blood pressure <90 mm Hg or heart rate >120 beats per minute or base deficit <-5.”1 Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr Costantini said. Next, they used univariate and multivariate logistic regression analyses to examine predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the 2-year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic BP was 93 mm Hg, their mean HR was 117 beats/min, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian vs auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage-control intervention, those who did received more transfusion of packed red blood cells (13 vs 7 units, respectively; P < .01) and fresh frozen plasma (10 U vs 5 U; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage-control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (OR, 109.43; P < .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
1. Costantini TW, Coimbra R, Holcomb JB, et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J Trauma Acute Care Surg. 2016;80(5):717-723; discussion 723-725. doi:10.1097/TA.0000000000001034.2. Costantini TW. Presentation at: 75th Annual Meeting of American Association for the Surgery of Trauma (AAST) and Clinical Congress of Acute Care Surgery. September 14-17, 2016. Waikoloa, Hawaii.
