User login
Severe Salt Restriction May Not Benefit Heart Failure
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
FROM THE EUROPEAN JOURNAL OF CLINICAL INVESTIGATION
Meat Alternatives May Benefit the Heart
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Does An Elevated Lp(a) Call for Low-dose Aspirin?
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Facial Temperature Can Reveal Age and Disease
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those. 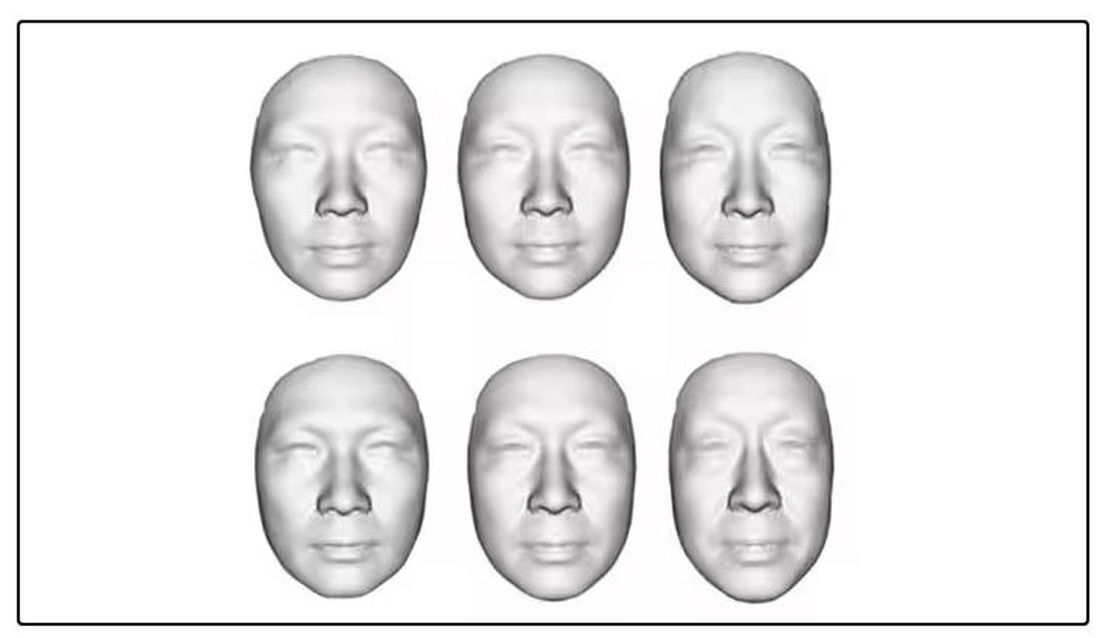
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.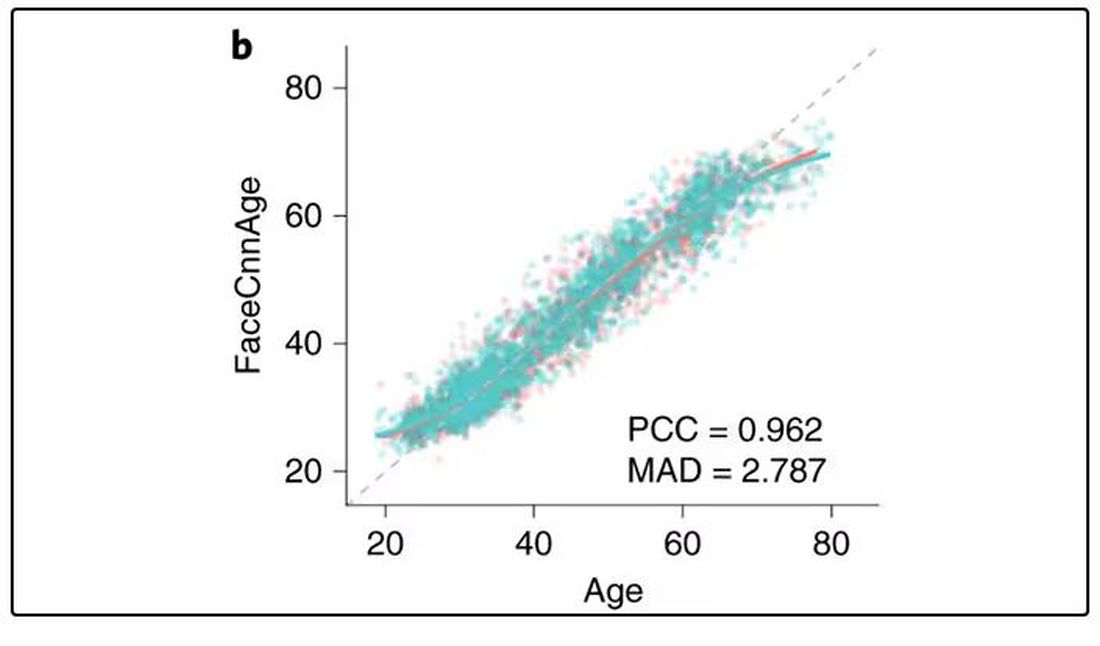
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally. 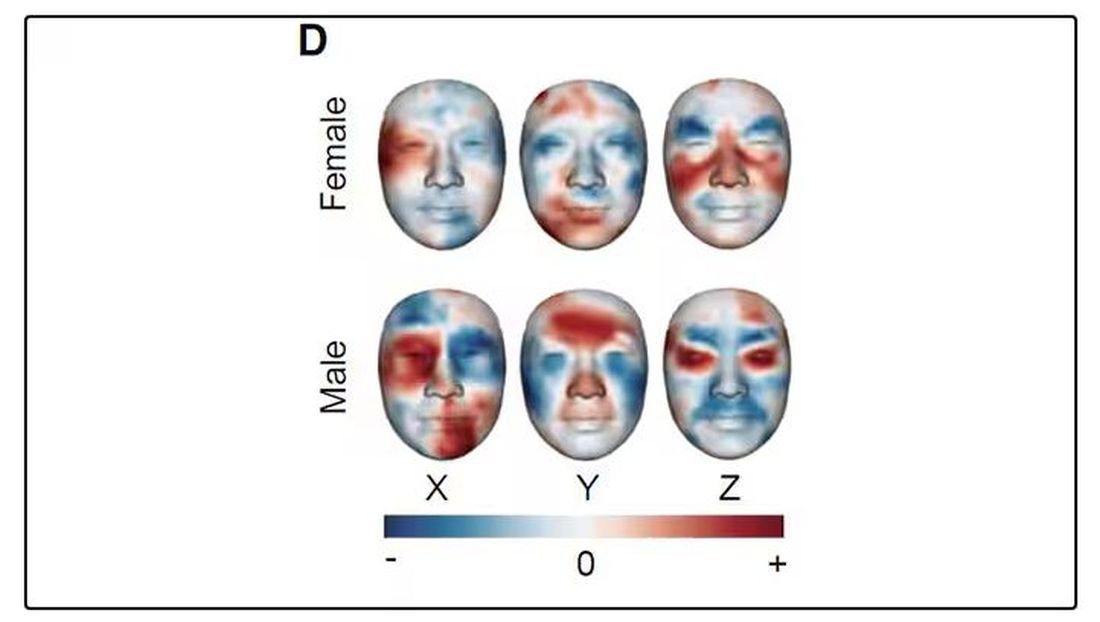
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.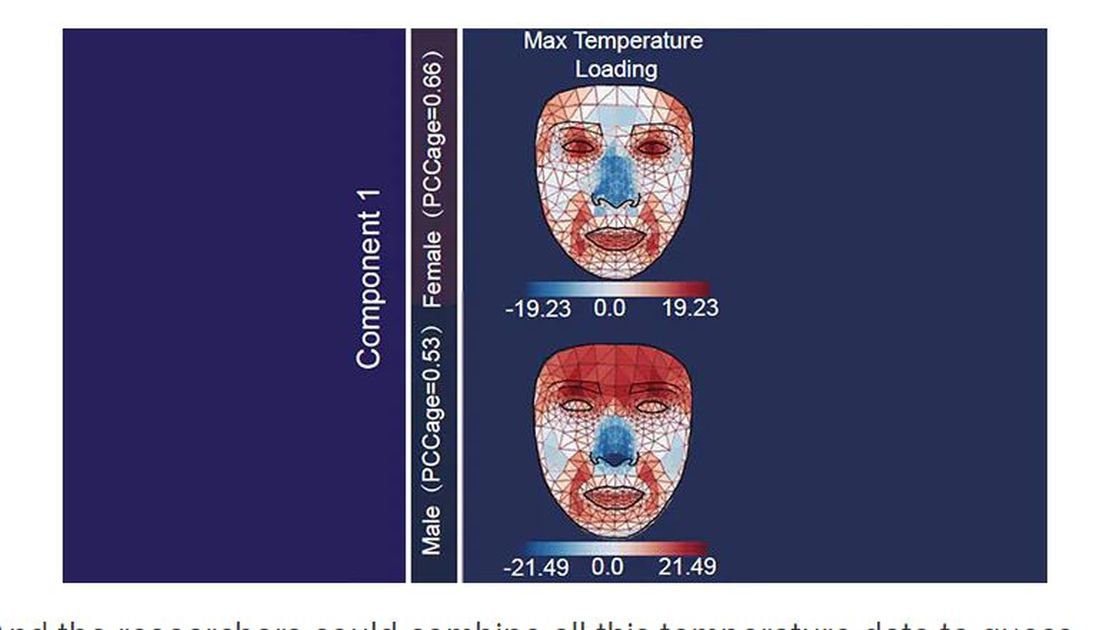
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.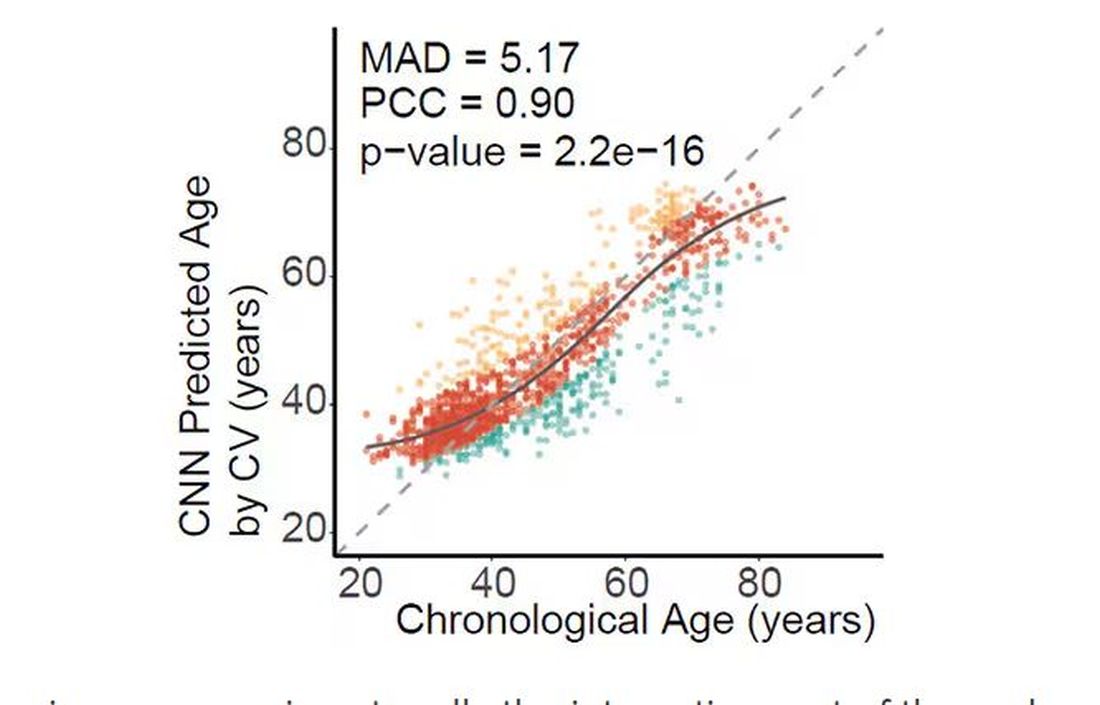
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.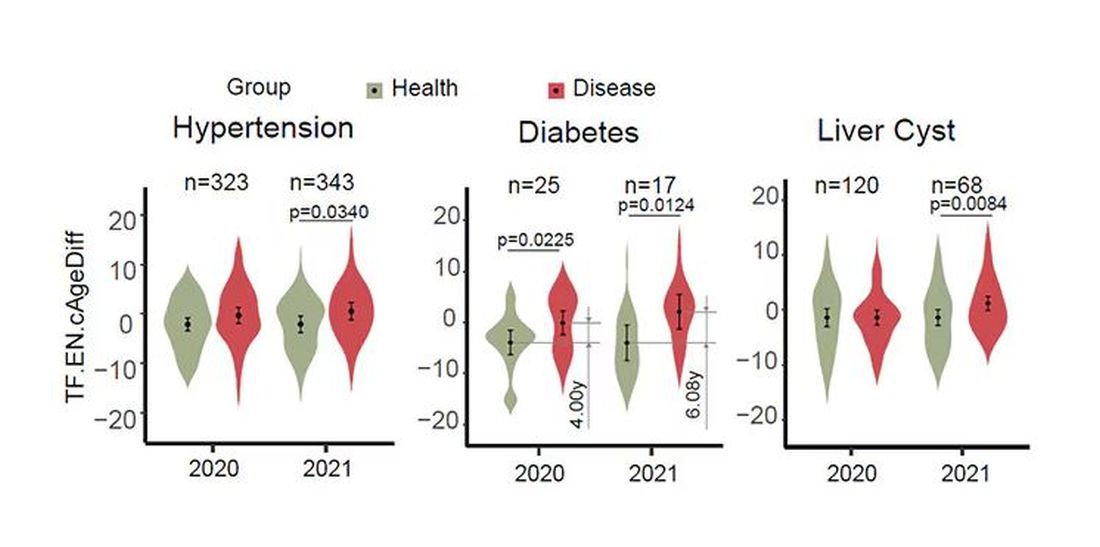
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.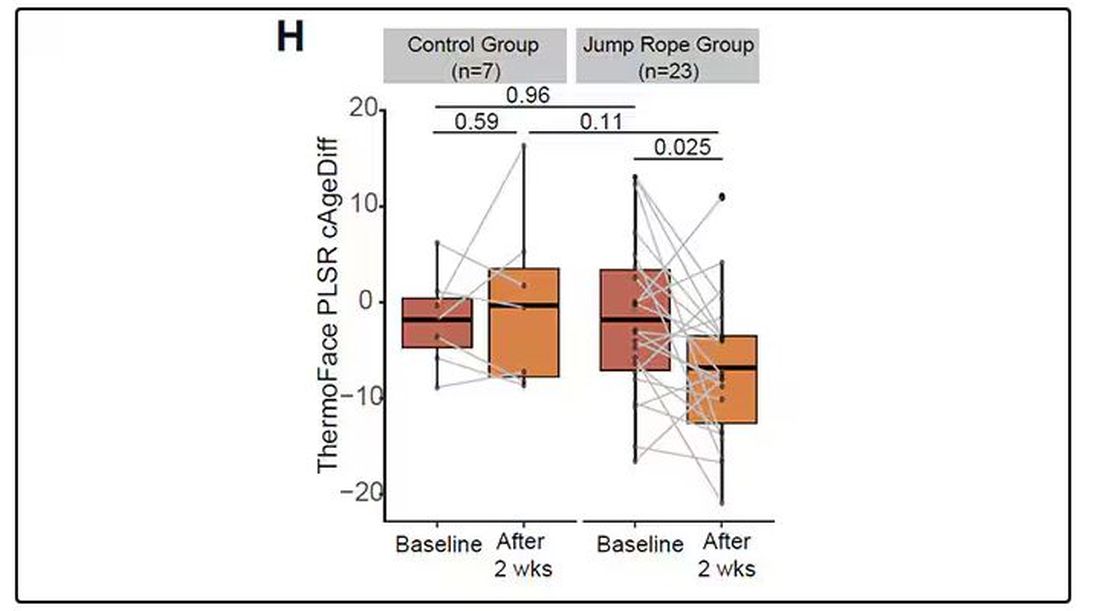
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those.
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally.
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those.
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally.
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Does Semaglutide Reduce Inflammation?
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.
Top reads from the CHEST journal portfolio
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.

– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.

– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.

– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.
– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.
– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.
– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.
– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.
– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.
– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Cardiovascular Health Becoming a Major Risk Factor for Dementia
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
FROM THE LANCET PUBLIC HEALTH
Similar Outcomes With Labetalol, Nifedipine for Chronic Hypertension in Pregnancy
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
- The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
- Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
- There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
- The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
- Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
- There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
- The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
- Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
- There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.
FROM OBSTETRICS & GYNECOLOGY
New Insight Into CVD, Stroke Risk in Migraine
SAN DIEGO – Researchers are unraveling the complex relationship between cardiovascular (CV)- and stroke-related outcomes in migraine with, and without, aura.
“We confirmed that aura increases the risk for these cerebrovascular and cardiovascular outcomes in people with migraine and that there’s an increased risk of these MACE events in men with migraine,” said study investigator Gina Dumkrieger, PhD, principal data science analyst and assistant professor of neurology, Mayo Clinic, Phoenix, Arizona.
The findings were presented at the annual meeting of the American Headache Society.
Few Data on Migraine and Stroke Risk
The extent to which migraine increases the risk for stroke CV outcomes has not been extensively studied.
“We’re trying to find out whether migraine-related factors make it more likely that you’re going to have one of these events,” said Dr. Dumkrieger. “Knowing a particular factor increases the risk is something patients and medical providers would want to know.”
Using Mayo Clinic electronic health records, which cover all three sites (Florida, Minnesota, and Arizona), researchers identified individuals with migraine using diagnostic codes. They also looked at data on sex, race, and the presence of aura.
They investigated whether a history of MACE risk factors — including atrial fibrillation, diabetes, hyperlipidemia, hypertension, and tobacco use — affected risk and the potential interaction of aura with these risk factors.
MACE events included cerebral infarction, intracerebral hemorrhage, and acute myocardial infarction.
The analysis included 130,126 participants (80% women, 95% White individuals). Of these, 6% experienced a MACE event, and 94% did not.
“We confirmed that aura does increase the risk for a MACE event, and all of the known risk factors that we included were also significant,” said Dr. Dumkrieger.
Odds ratios (ORs) were 3.82 for atrial fibrillation, 3.11 for hypertension, and 3.06 for hyperlipidemia.
It was surprising, said Dr. Dumkrieger, that male sex was tied to an increased risk for a MACE event (OR, 1.40). “This is not something that was known before,” she said.
The link between migraine and ischemic stroke, particularly with aura, was stronger in women — particularly young women.
Investigators also found an interaction between male sex and aura, when it comes to MACE outcomes, said Dr. Dumkrieger. “Males in general are at higher risk, and people with aura are at higher risk. Males with aura are also at higher risk, but maybe not as much as you would think they would be. It’s not a purely additive thing. This is something we need to look into more,” she said.
The study also revealed an interaction between aura and hypertension as well as aura and tobacco use, but here too, it was not an additive risk, said Dr. Dumkrieger. However, she added, the presence of aura does not moderate the risk for hyperlipidemia, diabetes, or atrial fibrillation.
The research also showed a significant interaction between male sex and Black race which was additive. “There’s apparently increased risk if you are male and Black or African American that’s greater than what you would expect. We should be especially concerned about these individuals,” she said.
Unanswered Questions
The current analysis is part of a larger study that will more closely examine these relationships. “We want to learn, for example, why aura moderates some of the risk factors but not others,” said Dr. Dumkrieger.
The researchers also plan to investigate other migraine features, including headache frequency, and headache sensations such as pulsating or throbbing.
Dr. Dumkrieger was an investigator of another study, also presented at the AHS meeting, that’s investigating the role of migraine-specific features and imaging results in the complex interrelationship between migraine and MACE risk.
That study, which also used the Mayo Clinic electronic health record data, included 60,454 migraine patients diagnosed with migraine after 2010.
Researchers divided participants into those with a MACE outcome (1107) and those without such an outcome (59,347) after at least 2 years of follow-up. They created a propensity cohort of individuals matched for age and risk factors for MACE outcome.
The final cohort consisted of 575 patients with and 652 patients without MACE outcome.
One of the most interesting early results from this study was that those with a MACE outcome had significantly more white matter hyperintensities than those with no MACE outcome, at 64% versus 51%, respectively.
This and other findings need to be validated in a different cohort with an electronic health records database from another institution. In future, the team plans to focus on identifying specific migraine features and medications and their relative contributions to MACE risk in migraine patients.
Yet another study featured at the AHS meeting confirmed the increased risk for stroke among migraine patients using a large database with over 410,000 subjects.
Results showed stroke was more than three times more common in those with a migraine diagnosis than in those without (risk ratio, [RR] 3.23; P < .001). The RR for hemorrhagic stroke (3.15) was comparable with that of ischemic stroke (3.20).
The overall stroke RR for chronic migraine versus controls without migraine was 3.68 (P < .001). The RR for migraine with aura versus migraine without aura was 1.37 (P < .001).
Useful Data
Commenting on the research, Juliana VanderPluym, MD, a headache specialist at the Mayo Clinic, Phoenix, Arizona, described this new information as “very useful.”
The fact that there are more white matter lesions on MRI scans in migraine patients with MACE needs further exploration, said Dr. VanderPluym.
“Understanding how much of that relates to migraine, how much relates to other comorbid conditions, and what this all means together, is very important, particularly because MACE can be life-threatening and life-altering,” she added.
Learning how migraine medications may impact MACE risk is also something that needs to be examined in greater depth, she said. “I would think that migraines that are controlled might have a different risk for MACE than uncontrolled migraine,” she said.
The investigators reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO – Researchers are unraveling the complex relationship between cardiovascular (CV)- and stroke-related outcomes in migraine with, and without, aura.
“We confirmed that aura increases the risk for these cerebrovascular and cardiovascular outcomes in people with migraine and that there’s an increased risk of these MACE events in men with migraine,” said study investigator Gina Dumkrieger, PhD, principal data science analyst and assistant professor of neurology, Mayo Clinic, Phoenix, Arizona.
The findings were presented at the annual meeting of the American Headache Society.
Few Data on Migraine and Stroke Risk
The extent to which migraine increases the risk for stroke CV outcomes has not been extensively studied.
“We’re trying to find out whether migraine-related factors make it more likely that you’re going to have one of these events,” said Dr. Dumkrieger. “Knowing a particular factor increases the risk is something patients and medical providers would want to know.”
Using Mayo Clinic electronic health records, which cover all three sites (Florida, Minnesota, and Arizona), researchers identified individuals with migraine using diagnostic codes. They also looked at data on sex, race, and the presence of aura.
They investigated whether a history of MACE risk factors — including atrial fibrillation, diabetes, hyperlipidemia, hypertension, and tobacco use — affected risk and the potential interaction of aura with these risk factors.
MACE events included cerebral infarction, intracerebral hemorrhage, and acute myocardial infarction.
The analysis included 130,126 participants (80% women, 95% White individuals). Of these, 6% experienced a MACE event, and 94% did not.
“We confirmed that aura does increase the risk for a MACE event, and all of the known risk factors that we included were also significant,” said Dr. Dumkrieger.
Odds ratios (ORs) were 3.82 for atrial fibrillation, 3.11 for hypertension, and 3.06 for hyperlipidemia.
It was surprising, said Dr. Dumkrieger, that male sex was tied to an increased risk for a MACE event (OR, 1.40). “This is not something that was known before,” she said.
The link between migraine and ischemic stroke, particularly with aura, was stronger in women — particularly young women.
Investigators also found an interaction between male sex and aura, when it comes to MACE outcomes, said Dr. Dumkrieger. “Males in general are at higher risk, and people with aura are at higher risk. Males with aura are also at higher risk, but maybe not as much as you would think they would be. It’s not a purely additive thing. This is something we need to look into more,” she said.
The study also revealed an interaction between aura and hypertension as well as aura and tobacco use, but here too, it was not an additive risk, said Dr. Dumkrieger. However, she added, the presence of aura does not moderate the risk for hyperlipidemia, diabetes, or atrial fibrillation.
The research also showed a significant interaction between male sex and Black race which was additive. “There’s apparently increased risk if you are male and Black or African American that’s greater than what you would expect. We should be especially concerned about these individuals,” she said.
Unanswered Questions
The current analysis is part of a larger study that will more closely examine these relationships. “We want to learn, for example, why aura moderates some of the risk factors but not others,” said Dr. Dumkrieger.
The researchers also plan to investigate other migraine features, including headache frequency, and headache sensations such as pulsating or throbbing.
Dr. Dumkrieger was an investigator of another study, also presented at the AHS meeting, that’s investigating the role of migraine-specific features and imaging results in the complex interrelationship between migraine and MACE risk.
That study, which also used the Mayo Clinic electronic health record data, included 60,454 migraine patients diagnosed with migraine after 2010.
Researchers divided participants into those with a MACE outcome (1107) and those without such an outcome (59,347) after at least 2 years of follow-up. They created a propensity cohort of individuals matched for age and risk factors for MACE outcome.
The final cohort consisted of 575 patients with and 652 patients without MACE outcome.
One of the most interesting early results from this study was that those with a MACE outcome had significantly more white matter hyperintensities than those with no MACE outcome, at 64% versus 51%, respectively.
This and other findings need to be validated in a different cohort with an electronic health records database from another institution. In future, the team plans to focus on identifying specific migraine features and medications and their relative contributions to MACE risk in migraine patients.
Yet another study featured at the AHS meeting confirmed the increased risk for stroke among migraine patients using a large database with over 410,000 subjects.
Results showed stroke was more than three times more common in those with a migraine diagnosis than in those without (risk ratio, [RR] 3.23; P < .001). The RR for hemorrhagic stroke (3.15) was comparable with that of ischemic stroke (3.20).
The overall stroke RR for chronic migraine versus controls without migraine was 3.68 (P < .001). The RR for migraine with aura versus migraine without aura was 1.37 (P < .001).
Useful Data
Commenting on the research, Juliana VanderPluym, MD, a headache specialist at the Mayo Clinic, Phoenix, Arizona, described this new information as “very useful.”
The fact that there are more white matter lesions on MRI scans in migraine patients with MACE needs further exploration, said Dr. VanderPluym.
“Understanding how much of that relates to migraine, how much relates to other comorbid conditions, and what this all means together, is very important, particularly because MACE can be life-threatening and life-altering,” she added.
Learning how migraine medications may impact MACE risk is also something that needs to be examined in greater depth, she said. “I would think that migraines that are controlled might have a different risk for MACE than uncontrolled migraine,” she said.
The investigators reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN DIEGO – Researchers are unraveling the complex relationship between cardiovascular (CV)- and stroke-related outcomes in migraine with, and without, aura.
“We confirmed that aura increases the risk for these cerebrovascular and cardiovascular outcomes in people with migraine and that there’s an increased risk of these MACE events in men with migraine,” said study investigator Gina Dumkrieger, PhD, principal data science analyst and assistant professor of neurology, Mayo Clinic, Phoenix, Arizona.
The findings were presented at the annual meeting of the American Headache Society.
Few Data on Migraine and Stroke Risk
The extent to which migraine increases the risk for stroke CV outcomes has not been extensively studied.
“We’re trying to find out whether migraine-related factors make it more likely that you’re going to have one of these events,” said Dr. Dumkrieger. “Knowing a particular factor increases the risk is something patients and medical providers would want to know.”
Using Mayo Clinic electronic health records, which cover all three sites (Florida, Minnesota, and Arizona), researchers identified individuals with migraine using diagnostic codes. They also looked at data on sex, race, and the presence of aura.
They investigated whether a history of MACE risk factors — including atrial fibrillation, diabetes, hyperlipidemia, hypertension, and tobacco use — affected risk and the potential interaction of aura with these risk factors.
MACE events included cerebral infarction, intracerebral hemorrhage, and acute myocardial infarction.
The analysis included 130,126 participants (80% women, 95% White individuals). Of these, 6% experienced a MACE event, and 94% did not.
“We confirmed that aura does increase the risk for a MACE event, and all of the known risk factors that we included were also significant,” said Dr. Dumkrieger.
Odds ratios (ORs) were 3.82 for atrial fibrillation, 3.11 for hypertension, and 3.06 for hyperlipidemia.
It was surprising, said Dr. Dumkrieger, that male sex was tied to an increased risk for a MACE event (OR, 1.40). “This is not something that was known before,” she said.
The link between migraine and ischemic stroke, particularly with aura, was stronger in women — particularly young women.
Investigators also found an interaction between male sex and aura, when it comes to MACE outcomes, said Dr. Dumkrieger. “Males in general are at higher risk, and people with aura are at higher risk. Males with aura are also at higher risk, but maybe not as much as you would think they would be. It’s not a purely additive thing. This is something we need to look into more,” she said.
The study also revealed an interaction between aura and hypertension as well as aura and tobacco use, but here too, it was not an additive risk, said Dr. Dumkrieger. However, she added, the presence of aura does not moderate the risk for hyperlipidemia, diabetes, or atrial fibrillation.
The research also showed a significant interaction between male sex and Black race which was additive. “There’s apparently increased risk if you are male and Black or African American that’s greater than what you would expect. We should be especially concerned about these individuals,” she said.
Unanswered Questions
The current analysis is part of a larger study that will more closely examine these relationships. “We want to learn, for example, why aura moderates some of the risk factors but not others,” said Dr. Dumkrieger.
The researchers also plan to investigate other migraine features, including headache frequency, and headache sensations such as pulsating or throbbing.
Dr. Dumkrieger was an investigator of another study, also presented at the AHS meeting, that’s investigating the role of migraine-specific features and imaging results in the complex interrelationship between migraine and MACE risk.
That study, which also used the Mayo Clinic electronic health record data, included 60,454 migraine patients diagnosed with migraine after 2010.
Researchers divided participants into those with a MACE outcome (1107) and those without such an outcome (59,347) after at least 2 years of follow-up. They created a propensity cohort of individuals matched for age and risk factors for MACE outcome.
The final cohort consisted of 575 patients with and 652 patients without MACE outcome.
One of the most interesting early results from this study was that those with a MACE outcome had significantly more white matter hyperintensities than those with no MACE outcome, at 64% versus 51%, respectively.
This and other findings need to be validated in a different cohort with an electronic health records database from another institution. In future, the team plans to focus on identifying specific migraine features and medications and their relative contributions to MACE risk in migraine patients.
Yet another study featured at the AHS meeting confirmed the increased risk for stroke among migraine patients using a large database with over 410,000 subjects.
Results showed stroke was more than three times more common in those with a migraine diagnosis than in those without (risk ratio, [RR] 3.23; P < .001). The RR for hemorrhagic stroke (3.15) was comparable with that of ischemic stroke (3.20).
The overall stroke RR for chronic migraine versus controls without migraine was 3.68 (P < .001). The RR for migraine with aura versus migraine without aura was 1.37 (P < .001).
Useful Data
Commenting on the research, Juliana VanderPluym, MD, a headache specialist at the Mayo Clinic, Phoenix, Arizona, described this new information as “very useful.”
The fact that there are more white matter lesions on MRI scans in migraine patients with MACE needs further exploration, said Dr. VanderPluym.
“Understanding how much of that relates to migraine, how much relates to other comorbid conditions, and what this all means together, is very important, particularly because MACE can be life-threatening and life-altering,” she added.
Learning how migraine medications may impact MACE risk is also something that needs to be examined in greater depth, she said. “I would think that migraines that are controlled might have a different risk for MACE than uncontrolled migraine,” she said.
The investigators reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM AHS 2024
Novel PCSK9 Drives High-Risk Patients to Target LDL
LYON, France – Lerodalcibep, a novel, third-generation anti-proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, helps high-risk patients already receiving maximally tolerated statins to achieve guideline lipid targets, reported investigators.
In the randomized, placebo-controlled LIBerate-CVD trial of more than 900 patients, lerodalcibep led to reductions from baseline in low-density lipoprotein (LDL) cholesterol levels of more than 60%.
“We believe that lerodalcibep offers a novel, effective alternative to current PCSK9 inhibitors for patients with cardiovascular disease or at very high risk for cardiovascular disease,” said Evan Stein, MD, PhD, chief scientific officer and cofounder of LIB Therapeutics in Chicago, who presented the findings at the European Atherosclerosis Society (EAS) 2024.
Moreover, it leads to “substantial additional LDL cholesterol reductions on top of existing oral agents” and allows more than 90% of patients to achieve the latest European Society of Cardiology (ESC) guideline targets, he said.
Lerodalcibep has “tolerability and safety similar to placebo,” Dr. Stein said, and requires only “a small monthly injection, which takes about 12 seconds.”
“The drug doesn’t require refrigeration” and is “stable, so far, over 9 months,” he reported.
The latest data “confirm the efficacy of lerodalcibep,” said Giuseppe Danilo Norata, PhD, from the Department of Pharmacological and Biomolecular Sciences at the University of Milan, Milan, Italy, who was not involved in the study.
The LDL cholesterol reduction in this phase 3 trial is “in line with what was observed in LIBerate-FH,” and the high proportion of patients achieving their LDL cholesterol target is “impressive,” he added.
Effective and Well Tolerated
The safety results are “suggestive of a drug that is well tolerated, with injection-site reactions being the only remarkable adverse event increased in the treatment group,” Dr. Norata reported.
Only a “limited number” of patients developed neutralizing antidrug antibodies, which did not affect the efficacy of lerodalcibep. However, “given that the therapy is expected to be administered for years,” a longer analysis is needed to exclude the concern that a small percentage of neutralizing antidrug antibodies could reduce the efficacy, he said.
If approved, lerodalcibep could end up as a first-line option in the treatment pathway for high-risk cardiovascular disease because the efficacy “is similar to that of other injectable PCSK9 inhibitors,” he said, adding that its position in the market will “largely depend on the price.”
As the mechanism of action is similar to that of other monoclonal antibodies, “there is no pharmacological rationale to use it after another PSCK9 inhibitor,” he explained.
Lerodalcibep is a small recombinant fusion protein that combines a PCSK9-binding domain with human serum albumin.
The binding domain blocks the interaction between PCSK9 and the LDL cholesterol receptor, and the albumin linkage increases the half-life to 12-15 days, allowing low-volume injections to be given every 4 weeks.
A prior phase 2 study suggested that lerodalcibep substantially decreases LDL cholesterol levels in patients already taking maximally tolerated statins. The 300-mg dose was associated with an average reduction from baseline in LDL cholesterol levels of 77% over 12 weeks, whereas free PCSK9 levels decreased by 88%.
The current phase 3 study enrolled individuals at 65 centers in 100 countries who had or were at a very high risk for cardiovascular disease and who had an LDL cholesterol level of ≥ 1.8 mmol/L despite being on maximally tolerated statins.
Study participants were randomized in a 2:1 ratio to receive monthly subcutaneous lerodalcibep (n = 614) or placebo (n = 308) for 52 weeks and were assessed for the co-primary endpoints of the percentage change in LDL cholesterol levels from baseline to week 52 and the mean of levels at weeks 50 and 52.
The mean age was similar in the lerodalcibep and placebo groups (63.3 vs 64.5 years), as were the proportion of female (30% vs 30%) and White (80% vs 79%) participants.
The vast majority of participants in the lerodalcibep and placebo groups had a documented cardiovascular event (85.3% vs 86.4%) and were receiving secondary prevention, and 87% and 82%, respectively, were receiving a statin (any dose).
In a modified intention-to-treat analysis, the mean placebo-adjusted reduction in LDL cholesterol levels from baseline with lerodalcibep was 62% at week 52 (P < .0001), and the mean of levels at weeks 50 and 52 was 69.4% (P < .0001).
Similar results were seen in a per protocol analysis and an intention-to-treat analysis with imputation, which is a US Food and Drug Administration measure introduced in 2021 that assumes patients who discontinue the study treatment have an outcome similar to that in the placebo patients.
Moreover, 98.2% of patients in the lerodalcibep group achieved the ESC and European Atherosclerosis Society recommended reduction in LDL cholesterol levels of ≥ 50%, whereas only 8.8% in the placebo group did.
Hitting the LDL Cholesterol Target
More patients in the lerodalcibep group than in the placebo group achieved the LDL cholesterol target of < 1.4 mmol/L (95.3% vs 18.5%), and more patients in the lerodalcibep group achieved both that target and the ≥ 50% target (94.5% and 6.8%).
Lerodalcibep was also associated with significant reductions from baseline in levels of non–high-density lipoprotein (HDL) cholesterol, apolipoprotein B, very LDL cholesterol, and triglycerides, as well as an increase in HDL cholesterol levels (P < .0001 for all).
In terms of safety, lerodalcibep was associated with an adverse event rate leading to withdrawal similar to that seen with placebo (4.2% vs 3.6%), and 15.9% and 14.8% of patients, respectively, experienced at least one serious adverse event.
In-stent restenosis occurred more often in the lerodalcibep group than in the placebo group (5.4% vs 2.0%).
The study drug was associated with low levels of transient and sporadic antidrug antibodies and a low rate of neutralizing antidrug antibodies (0.9%), which were not associated with restenosis, a reduction in free PCSK9 levels, or the ability of lerodalcibep to lower LDL cholesterol levels.
A version of this article first appeared on Medscape.com.
LYON, France – Lerodalcibep, a novel, third-generation anti-proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, helps high-risk patients already receiving maximally tolerated statins to achieve guideline lipid targets, reported investigators.
In the randomized, placebo-controlled LIBerate-CVD trial of more than 900 patients, lerodalcibep led to reductions from baseline in low-density lipoprotein (LDL) cholesterol levels of more than 60%.
“We believe that lerodalcibep offers a novel, effective alternative to current PCSK9 inhibitors for patients with cardiovascular disease or at very high risk for cardiovascular disease,” said Evan Stein, MD, PhD, chief scientific officer and cofounder of LIB Therapeutics in Chicago, who presented the findings at the European Atherosclerosis Society (EAS) 2024.
Moreover, it leads to “substantial additional LDL cholesterol reductions on top of existing oral agents” and allows more than 90% of patients to achieve the latest European Society of Cardiology (ESC) guideline targets, he said.
Lerodalcibep has “tolerability and safety similar to placebo,” Dr. Stein said, and requires only “a small monthly injection, which takes about 12 seconds.”
“The drug doesn’t require refrigeration” and is “stable, so far, over 9 months,” he reported.
The latest data “confirm the efficacy of lerodalcibep,” said Giuseppe Danilo Norata, PhD, from the Department of Pharmacological and Biomolecular Sciences at the University of Milan, Milan, Italy, who was not involved in the study.
The LDL cholesterol reduction in this phase 3 trial is “in line with what was observed in LIBerate-FH,” and the high proportion of patients achieving their LDL cholesterol target is “impressive,” he added.
Effective and Well Tolerated
The safety results are “suggestive of a drug that is well tolerated, with injection-site reactions being the only remarkable adverse event increased in the treatment group,” Dr. Norata reported.
Only a “limited number” of patients developed neutralizing antidrug antibodies, which did not affect the efficacy of lerodalcibep. However, “given that the therapy is expected to be administered for years,” a longer analysis is needed to exclude the concern that a small percentage of neutralizing antidrug antibodies could reduce the efficacy, he said.
If approved, lerodalcibep could end up as a first-line option in the treatment pathway for high-risk cardiovascular disease because the efficacy “is similar to that of other injectable PCSK9 inhibitors,” he said, adding that its position in the market will “largely depend on the price.”
As the mechanism of action is similar to that of other monoclonal antibodies, “there is no pharmacological rationale to use it after another PSCK9 inhibitor,” he explained.
Lerodalcibep is a small recombinant fusion protein that combines a PCSK9-binding domain with human serum albumin.
The binding domain blocks the interaction between PCSK9 and the LDL cholesterol receptor, and the albumin linkage increases the half-life to 12-15 days, allowing low-volume injections to be given every 4 weeks.
A prior phase 2 study suggested that lerodalcibep substantially decreases LDL cholesterol levels in patients already taking maximally tolerated statins. The 300-mg dose was associated with an average reduction from baseline in LDL cholesterol levels of 77% over 12 weeks, whereas free PCSK9 levels decreased by 88%.
The current phase 3 study enrolled individuals at 65 centers in 100 countries who had or were at a very high risk for cardiovascular disease and who had an LDL cholesterol level of ≥ 1.8 mmol/L despite being on maximally tolerated statins.
Study participants were randomized in a 2:1 ratio to receive monthly subcutaneous lerodalcibep (n = 614) or placebo (n = 308) for 52 weeks and were assessed for the co-primary endpoints of the percentage change in LDL cholesterol levels from baseline to week 52 and the mean of levels at weeks 50 and 52.
The mean age was similar in the lerodalcibep and placebo groups (63.3 vs 64.5 years), as were the proportion of female (30% vs 30%) and White (80% vs 79%) participants.
The vast majority of participants in the lerodalcibep and placebo groups had a documented cardiovascular event (85.3% vs 86.4%) and were receiving secondary prevention, and 87% and 82%, respectively, were receiving a statin (any dose).
In a modified intention-to-treat analysis, the mean placebo-adjusted reduction in LDL cholesterol levels from baseline with lerodalcibep was 62% at week 52 (P < .0001), and the mean of levels at weeks 50 and 52 was 69.4% (P < .0001).
Similar results were seen in a per protocol analysis and an intention-to-treat analysis with imputation, which is a US Food and Drug Administration measure introduced in 2021 that assumes patients who discontinue the study treatment have an outcome similar to that in the placebo patients.
Moreover, 98.2% of patients in the lerodalcibep group achieved the ESC and European Atherosclerosis Society recommended reduction in LDL cholesterol levels of ≥ 50%, whereas only 8.8% in the placebo group did.
Hitting the LDL Cholesterol Target
More patients in the lerodalcibep group than in the placebo group achieved the LDL cholesterol target of < 1.4 mmol/L (95.3% vs 18.5%), and more patients in the lerodalcibep group achieved both that target and the ≥ 50% target (94.5% and 6.8%).
Lerodalcibep was also associated with significant reductions from baseline in levels of non–high-density lipoprotein (HDL) cholesterol, apolipoprotein B, very LDL cholesterol, and triglycerides, as well as an increase in HDL cholesterol levels (P < .0001 for all).
In terms of safety, lerodalcibep was associated with an adverse event rate leading to withdrawal similar to that seen with placebo (4.2% vs 3.6%), and 15.9% and 14.8% of patients, respectively, experienced at least one serious adverse event.
In-stent restenosis occurred more often in the lerodalcibep group than in the placebo group (5.4% vs 2.0%).
The study drug was associated with low levels of transient and sporadic antidrug antibodies and a low rate of neutralizing antidrug antibodies (0.9%), which were not associated with restenosis, a reduction in free PCSK9 levels, or the ability of lerodalcibep to lower LDL cholesterol levels.
A version of this article first appeared on Medscape.com.
LYON, France – Lerodalcibep, a novel, third-generation anti-proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, helps high-risk patients already receiving maximally tolerated statins to achieve guideline lipid targets, reported investigators.
In the randomized, placebo-controlled LIBerate-CVD trial of more than 900 patients, lerodalcibep led to reductions from baseline in low-density lipoprotein (LDL) cholesterol levels of more than 60%.
“We believe that lerodalcibep offers a novel, effective alternative to current PCSK9 inhibitors for patients with cardiovascular disease or at very high risk for cardiovascular disease,” said Evan Stein, MD, PhD, chief scientific officer and cofounder of LIB Therapeutics in Chicago, who presented the findings at the European Atherosclerosis Society (EAS) 2024.
Moreover, it leads to “substantial additional LDL cholesterol reductions on top of existing oral agents” and allows more than 90% of patients to achieve the latest European Society of Cardiology (ESC) guideline targets, he said.
Lerodalcibep has “tolerability and safety similar to placebo,” Dr. Stein said, and requires only “a small monthly injection, which takes about 12 seconds.”
“The drug doesn’t require refrigeration” and is “stable, so far, over 9 months,” he reported.
The latest data “confirm the efficacy of lerodalcibep,” said Giuseppe Danilo Norata, PhD, from the Department of Pharmacological and Biomolecular Sciences at the University of Milan, Milan, Italy, who was not involved in the study.
The LDL cholesterol reduction in this phase 3 trial is “in line with what was observed in LIBerate-FH,” and the high proportion of patients achieving their LDL cholesterol target is “impressive,” he added.
Effective and Well Tolerated
The safety results are “suggestive of a drug that is well tolerated, with injection-site reactions being the only remarkable adverse event increased in the treatment group,” Dr. Norata reported.
Only a “limited number” of patients developed neutralizing antidrug antibodies, which did not affect the efficacy of lerodalcibep. However, “given that the therapy is expected to be administered for years,” a longer analysis is needed to exclude the concern that a small percentage of neutralizing antidrug antibodies could reduce the efficacy, he said.
If approved, lerodalcibep could end up as a first-line option in the treatment pathway for high-risk cardiovascular disease because the efficacy “is similar to that of other injectable PCSK9 inhibitors,” he said, adding that its position in the market will “largely depend on the price.”
As the mechanism of action is similar to that of other monoclonal antibodies, “there is no pharmacological rationale to use it after another PSCK9 inhibitor,” he explained.
Lerodalcibep is a small recombinant fusion protein that combines a PCSK9-binding domain with human serum albumin.
The binding domain blocks the interaction between PCSK9 and the LDL cholesterol receptor, and the albumin linkage increases the half-life to 12-15 days, allowing low-volume injections to be given every 4 weeks.
A prior phase 2 study suggested that lerodalcibep substantially decreases LDL cholesterol levels in patients already taking maximally tolerated statins. The 300-mg dose was associated with an average reduction from baseline in LDL cholesterol levels of 77% over 12 weeks, whereas free PCSK9 levels decreased by 88%.
The current phase 3 study enrolled individuals at 65 centers in 100 countries who had or were at a very high risk for cardiovascular disease and who had an LDL cholesterol level of ≥ 1.8 mmol/L despite being on maximally tolerated statins.
Study participants were randomized in a 2:1 ratio to receive monthly subcutaneous lerodalcibep (n = 614) or placebo (n = 308) for 52 weeks and were assessed for the co-primary endpoints of the percentage change in LDL cholesterol levels from baseline to week 52 and the mean of levels at weeks 50 and 52.
The mean age was similar in the lerodalcibep and placebo groups (63.3 vs 64.5 years), as were the proportion of female (30% vs 30%) and White (80% vs 79%) participants.
The vast majority of participants in the lerodalcibep and placebo groups had a documented cardiovascular event (85.3% vs 86.4%) and were receiving secondary prevention, and 87% and 82%, respectively, were receiving a statin (any dose).
In a modified intention-to-treat analysis, the mean placebo-adjusted reduction in LDL cholesterol levels from baseline with lerodalcibep was 62% at week 52 (P < .0001), and the mean of levels at weeks 50 and 52 was 69.4% (P < .0001).
Similar results were seen in a per protocol analysis and an intention-to-treat analysis with imputation, which is a US Food and Drug Administration measure introduced in 2021 that assumes patients who discontinue the study treatment have an outcome similar to that in the placebo patients.
Moreover, 98.2% of patients in the lerodalcibep group achieved the ESC and European Atherosclerosis Society recommended reduction in LDL cholesterol levels of ≥ 50%, whereas only 8.8% in the placebo group did.
Hitting the LDL Cholesterol Target
More patients in the lerodalcibep group than in the placebo group achieved the LDL cholesterol target of < 1.4 mmol/L (95.3% vs 18.5%), and more patients in the lerodalcibep group achieved both that target and the ≥ 50% target (94.5% and 6.8%).
Lerodalcibep was also associated with significant reductions from baseline in levels of non–high-density lipoprotein (HDL) cholesterol, apolipoprotein B, very LDL cholesterol, and triglycerides, as well as an increase in HDL cholesterol levels (P < .0001 for all).
In terms of safety, lerodalcibep was associated with an adverse event rate leading to withdrawal similar to that seen with placebo (4.2% vs 3.6%), and 15.9% and 14.8% of patients, respectively, experienced at least one serious adverse event.
In-stent restenosis occurred more often in the lerodalcibep group than in the placebo group (5.4% vs 2.0%).
The study drug was associated with low levels of transient and sporadic antidrug antibodies and a low rate of neutralizing antidrug antibodies (0.9%), which were not associated with restenosis, a reduction in free PCSK9 levels, or the ability of lerodalcibep to lower LDL cholesterol levels.
A version of this article first appeared on Medscape.com.
FROM EAS 2024