User login
Aging HIV patients face comorbidities and hospitalizations
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
Provider recommendation key to boosting teen HPV vaccines
Human papilloma virus (HPV) vaccination coverage of at least one dose significantly increased in U.S. adolescents from 56.1% in 2015 to 75.4% in 2020, according to the National Immunization Survey–Teen (NIS-Teen).
The telephone survey, conducted among the parents or guardians of children ages 13-17, found a faster increase in coverage among males than females: 4.7 percentage points annually versus 2.7 percentage points annually. With yearly overall survey samples ranging from 21,875 to 17,970, these coverage differences between males and females narrowed over the 5 years of the survey period.
The difference between coverage among males and females decreased from 13 to 3 percentage points. Traditionally, parents of boys have been less likely to vaccinate their sons against HPV.
Despite the increase in uptake, however, in 2020 about 25% of adolescents had not received at least one dose of HPV vaccine. “Targeted strategies are needed to increase coverage and narrow down inequalities,” Peng-jun Lu, MD, PhD, of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention in Atlanta, and colleagues wrote in Pediatrics.
In other NIS-Teen findings:
- Coverage in 2020 was 73.7% for males and 76.8% for females (P < .05).
- Coverage rose to 80.7% for those with a provider recommendation but was only 51.7% for those without one (P < .05).
- The rate was 80.3% for those with a well-child visit at age 11-12 years and 64.8% for those without (P < .05).
- In multivariable logistic regression, the main characteristics independently associated with a higher likelihood of vaccination included a provider recommendation, age 16-17 years, and being non-Hispanic Black, Hispanic, American Indian, or Alaskan Native.
- Other predictors of vaccination included having Medicaid insurance and having a mother who was widowed, divorced, or separated, or had no more than a high school education.
- Also predictive was having two or more provider contacts in the past 12 months, a well-child visit at age 11-12 years, and one or two vaccine providers (P < .05).
- Coverage among adolescents living in non-metropolitan statistical areas was significantly lower than those living in MSA principal cities in all years assessed (P < .05).
Provider recommendation remains significant and has historically been highly associated with HPV vaccination. In the 2012 NIS-Teen, for example, 15% of parents not intending to have their daughters vaccinated in the next 12 months cited the lack of a provider recommendation.
“To increase HPV vaccination coverage and further reduce HPV-related morbidity and mortality, providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives the HPV vaccine and other needed vaccines,” Dr. Lu and associates wrote. But 18.5% of parents in the survey received no provider recommendation.
“Of note, we found that teenagers who had mothers with more education or who live in more rural communities had a lower likelihood of receiving vaccination against HPV,” Dr. Lu told this news organization. “Further research should be conducted to better understand these findings.”
According to Margaret E. Thew, DNP, FNP-BC, director of adolescent medicine at the Medical College of Wisconsin in Milwaukee, several studies have highlighted resistance to the vaccine among better-educated parents. “Parents with higher education associate the HPV vaccine with sexual activity and consequently refuse,” said Ms. Thew, who was not involved in the NIS-Teen study. “They mistakenly assume that their children are not sexually active and they lack the understanding that HPV is one of the biggest causes of oral cancer.”

The increased uptake among males was encouraging, said Ms. Thew.
Sharing her perspective on the survey-based study but not involved in it, Melissa B. Gilkey, PhD, associate professor of health behavior at the University of North Carolina in Chapel Hill, said the study is important for characterizing national trends in HPV vaccination coverage using high-quality data. “The almost 20-percentage-point jump in HPV vaccination coverage from 2015 to 2020 speaks to the hard work of primary care doctors and nurses, health departments, the CDC, and other government agencies, and public health researchers,” she told this news organization. “We’ve long understood how critical primary care is, but these data are a powerful reminder that if we want to increase HPV vaccination rates, we need to be supporting primary care doctors and nurses.”
Dr. Gilkey added that effective interventions are available to help primary care teams recommend the HPV vaccine and address parents’ vaccination concerns effectively. “However, there remains an urgent need to roll out these interventions nationally.”
This is especially true in the context of the COVID-19 pandemic, which has disrupted well-child visits and led to a decline in HPV vaccination coverage, she said. “We can’t afford to lose our hard-won gains in HPV vaccination coverage, so supporting provider recommendations and well-child visits is more important now than ever.”
According to Dr. Lu, providers should routinely recommend the vaccine and highlight the importance of vaccination in preventing HPV-related cancers. “Additionally, health care providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives HPV vaccine and other needed vaccines.”
This study had no external funding. The authors had no potential conflicts of interest to disclose. Dr. Gilkey is co-principal investigator of a CDC-funded study evaluating a model for improving HPV vaccine coverage in primary care settings. Ms. Thew disclosed no potential conflicts of interest.
Human papilloma virus (HPV) vaccination coverage of at least one dose significantly increased in U.S. adolescents from 56.1% in 2015 to 75.4% in 2020, according to the National Immunization Survey–Teen (NIS-Teen).
The telephone survey, conducted among the parents or guardians of children ages 13-17, found a faster increase in coverage among males than females: 4.7 percentage points annually versus 2.7 percentage points annually. With yearly overall survey samples ranging from 21,875 to 17,970, these coverage differences between males and females narrowed over the 5 years of the survey period.
The difference between coverage among males and females decreased from 13 to 3 percentage points. Traditionally, parents of boys have been less likely to vaccinate their sons against HPV.
Despite the increase in uptake, however, in 2020 about 25% of adolescents had not received at least one dose of HPV vaccine. “Targeted strategies are needed to increase coverage and narrow down inequalities,” Peng-jun Lu, MD, PhD, of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention in Atlanta, and colleagues wrote in Pediatrics.
In other NIS-Teen findings:
- Coverage in 2020 was 73.7% for males and 76.8% for females (P < .05).
- Coverage rose to 80.7% for those with a provider recommendation but was only 51.7% for those without one (P < .05).
- The rate was 80.3% for those with a well-child visit at age 11-12 years and 64.8% for those without (P < .05).
- In multivariable logistic regression, the main characteristics independently associated with a higher likelihood of vaccination included a provider recommendation, age 16-17 years, and being non-Hispanic Black, Hispanic, American Indian, or Alaskan Native.
- Other predictors of vaccination included having Medicaid insurance and having a mother who was widowed, divorced, or separated, or had no more than a high school education.
- Also predictive was having two or more provider contacts in the past 12 months, a well-child visit at age 11-12 years, and one or two vaccine providers (P < .05).
- Coverage among adolescents living in non-metropolitan statistical areas was significantly lower than those living in MSA principal cities in all years assessed (P < .05).
Provider recommendation remains significant and has historically been highly associated with HPV vaccination. In the 2012 NIS-Teen, for example, 15% of parents not intending to have their daughters vaccinated in the next 12 months cited the lack of a provider recommendation.
“To increase HPV vaccination coverage and further reduce HPV-related morbidity and mortality, providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives the HPV vaccine and other needed vaccines,” Dr. Lu and associates wrote. But 18.5% of parents in the survey received no provider recommendation.
“Of note, we found that teenagers who had mothers with more education or who live in more rural communities had a lower likelihood of receiving vaccination against HPV,” Dr. Lu told this news organization. “Further research should be conducted to better understand these findings.”
According to Margaret E. Thew, DNP, FNP-BC, director of adolescent medicine at the Medical College of Wisconsin in Milwaukee, several studies have highlighted resistance to the vaccine among better-educated parents. “Parents with higher education associate the HPV vaccine with sexual activity and consequently refuse,” said Ms. Thew, who was not involved in the NIS-Teen study. “They mistakenly assume that their children are not sexually active and they lack the understanding that HPV is one of the biggest causes of oral cancer.”
The increased uptake among males was encouraging, said Ms. Thew.
Sharing her perspective on the survey-based study but not involved in it, Melissa B. Gilkey, PhD, associate professor of health behavior at the University of North Carolina in Chapel Hill, said the study is important for characterizing national trends in HPV vaccination coverage using high-quality data. “The almost 20-percentage-point jump in HPV vaccination coverage from 2015 to 2020 speaks to the hard work of primary care doctors and nurses, health departments, the CDC, and other government agencies, and public health researchers,” she told this news organization. “We’ve long understood how critical primary care is, but these data are a powerful reminder that if we want to increase HPV vaccination rates, we need to be supporting primary care doctors and nurses.”
Dr. Gilkey added that effective interventions are available to help primary care teams recommend the HPV vaccine and address parents’ vaccination concerns effectively. “However, there remains an urgent need to roll out these interventions nationally.”
This is especially true in the context of the COVID-19 pandemic, which has disrupted well-child visits and led to a decline in HPV vaccination coverage, she said. “We can’t afford to lose our hard-won gains in HPV vaccination coverage, so supporting provider recommendations and well-child visits is more important now than ever.”
According to Dr. Lu, providers should routinely recommend the vaccine and highlight the importance of vaccination in preventing HPV-related cancers. “Additionally, health care providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives HPV vaccine and other needed vaccines.”
This study had no external funding. The authors had no potential conflicts of interest to disclose. Dr. Gilkey is co-principal investigator of a CDC-funded study evaluating a model for improving HPV vaccine coverage in primary care settings. Ms. Thew disclosed no potential conflicts of interest.
Human papilloma virus (HPV) vaccination coverage of at least one dose significantly increased in U.S. adolescents from 56.1% in 2015 to 75.4% in 2020, according to the National Immunization Survey–Teen (NIS-Teen).
The telephone survey, conducted among the parents or guardians of children ages 13-17, found a faster increase in coverage among males than females: 4.7 percentage points annually versus 2.7 percentage points annually. With yearly overall survey samples ranging from 21,875 to 17,970, these coverage differences between males and females narrowed over the 5 years of the survey period.
The difference between coverage among males and females decreased from 13 to 3 percentage points. Traditionally, parents of boys have been less likely to vaccinate their sons against HPV.
Despite the increase in uptake, however, in 2020 about 25% of adolescents had not received at least one dose of HPV vaccine. “Targeted strategies are needed to increase coverage and narrow down inequalities,” Peng-jun Lu, MD, PhD, of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention in Atlanta, and colleagues wrote in Pediatrics.
In other NIS-Teen findings:
- Coverage in 2020 was 73.7% for males and 76.8% for females (P < .05).
- Coverage rose to 80.7% for those with a provider recommendation but was only 51.7% for those without one (P < .05).
- The rate was 80.3% for those with a well-child visit at age 11-12 years and 64.8% for those without (P < .05).
- In multivariable logistic regression, the main characteristics independently associated with a higher likelihood of vaccination included a provider recommendation, age 16-17 years, and being non-Hispanic Black, Hispanic, American Indian, or Alaskan Native.
- Other predictors of vaccination included having Medicaid insurance and having a mother who was widowed, divorced, or separated, or had no more than a high school education.
- Also predictive was having two or more provider contacts in the past 12 months, a well-child visit at age 11-12 years, and one or two vaccine providers (P < .05).
- Coverage among adolescents living in non-metropolitan statistical areas was significantly lower than those living in MSA principal cities in all years assessed (P < .05).
Provider recommendation remains significant and has historically been highly associated with HPV vaccination. In the 2012 NIS-Teen, for example, 15% of parents not intending to have their daughters vaccinated in the next 12 months cited the lack of a provider recommendation.
“To increase HPV vaccination coverage and further reduce HPV-related morbidity and mortality, providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives the HPV vaccine and other needed vaccines,” Dr. Lu and associates wrote. But 18.5% of parents in the survey received no provider recommendation.
“Of note, we found that teenagers who had mothers with more education or who live in more rural communities had a lower likelihood of receiving vaccination against HPV,” Dr. Lu told this news organization. “Further research should be conducted to better understand these findings.”
According to Margaret E. Thew, DNP, FNP-BC, director of adolescent medicine at the Medical College of Wisconsin in Milwaukee, several studies have highlighted resistance to the vaccine among better-educated parents. “Parents with higher education associate the HPV vaccine with sexual activity and consequently refuse,” said Ms. Thew, who was not involved in the NIS-Teen study. “They mistakenly assume that their children are not sexually active and they lack the understanding that HPV is one of the biggest causes of oral cancer.”
The increased uptake among males was encouraging, said Ms. Thew.
Sharing her perspective on the survey-based study but not involved in it, Melissa B. Gilkey, PhD, associate professor of health behavior at the University of North Carolina in Chapel Hill, said the study is important for characterizing national trends in HPV vaccination coverage using high-quality data. “The almost 20-percentage-point jump in HPV vaccination coverage from 2015 to 2020 speaks to the hard work of primary care doctors and nurses, health departments, the CDC, and other government agencies, and public health researchers,” she told this news organization. “We’ve long understood how critical primary care is, but these data are a powerful reminder that if we want to increase HPV vaccination rates, we need to be supporting primary care doctors and nurses.”
Dr. Gilkey added that effective interventions are available to help primary care teams recommend the HPV vaccine and address parents’ vaccination concerns effectively. “However, there remains an urgent need to roll out these interventions nationally.”
This is especially true in the context of the COVID-19 pandemic, which has disrupted well-child visits and led to a decline in HPV vaccination coverage, she said. “We can’t afford to lose our hard-won gains in HPV vaccination coverage, so supporting provider recommendations and well-child visits is more important now than ever.”
According to Dr. Lu, providers should routinely recommend the vaccine and highlight the importance of vaccination in preventing HPV-related cancers. “Additionally, health care providers, parents, and adolescents should use every health care visit as a chance to review vaccination histories and ensure that every adolescent receives HPV vaccine and other needed vaccines.”
This study had no external funding. The authors had no potential conflicts of interest to disclose. Dr. Gilkey is co-principal investigator of a CDC-funded study evaluating a model for improving HPV vaccine coverage in primary care settings. Ms. Thew disclosed no potential conflicts of interest.
FROM PEDIATRICS
Children and COVID: Vaccines now available to all ages
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.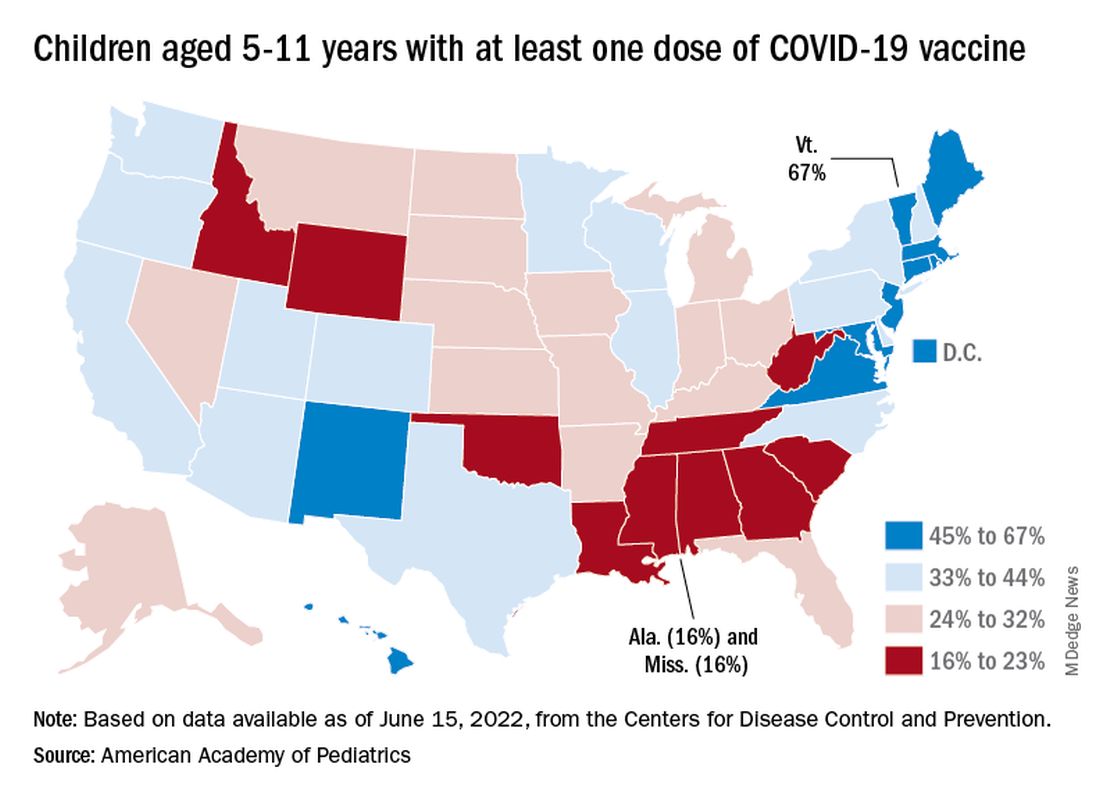
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.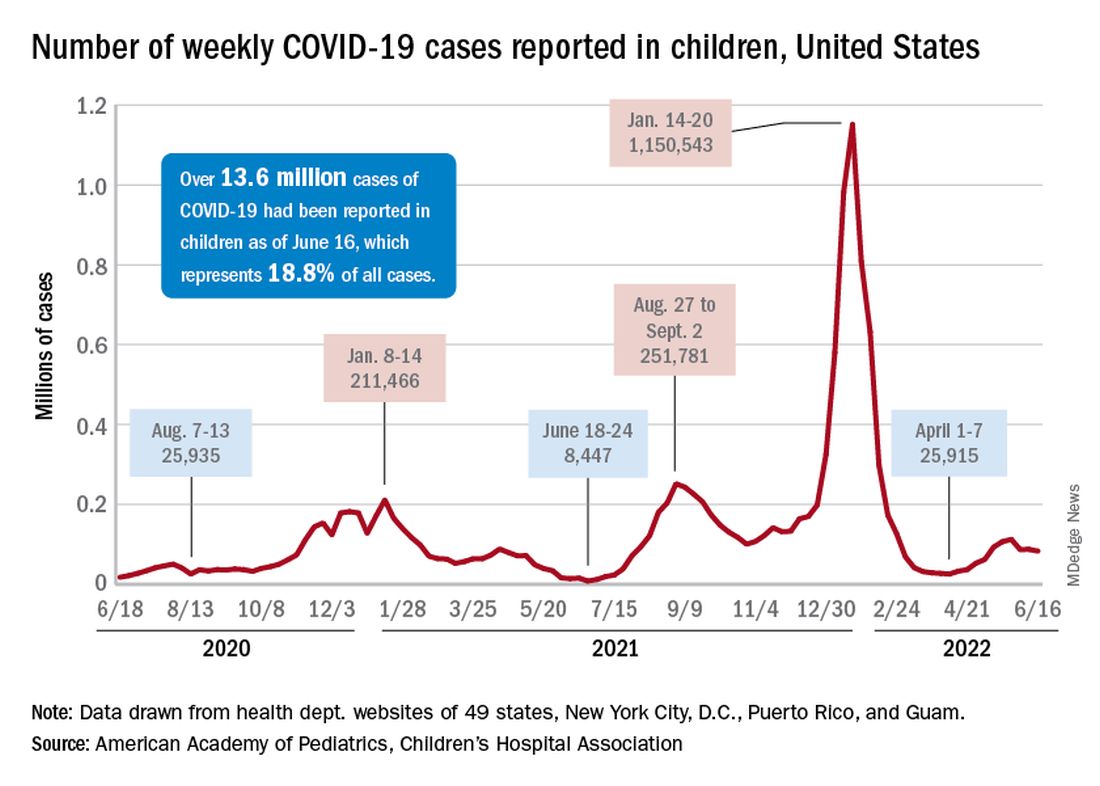
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
Postherpetic Pink, Smooth, Annular Convalescing Plaques
The Diagnosis: Granuloma Annulare
A biopsy of a lesion on the right flank demonstrated granulomatous inflammation and interstitial mucin (Figure), characteristic of granuloma annulare (GA).1,2 Granuloma annulare is a relatively common skin disorder with an unknown etiology. It typically presents as smooth, annular, erythematous plaques.1 The most common variants of GA are localized, generalized, and subcutaneous. Our case demonstrated Wolf isotopic response, an unrelated skin disease that forms at the same location as a previously healed skin lesion.2 It is important to be aware of this phenomenon so that it is not confused with a recurrence of herpes zoster virus (HZV).
Although relatively infrequent, GA is the most common isotopic response following HZV infections.3-5 Other postherpetic isotopic eruptions include cutaneous malignancies, lichen planus, sarcoidosis, morphea, reactive perforating collagenosis, psoriasis, and infections, among others.3,5,6 The time between HZV infection and GA can be variable, ranging from a few weeks to many years apart.3
Oftentimes GA will spontaneously resolve within 2 years; however, recurrence is common.7-9 There currently are no standard treatment guidelines. The most promising treatment options include intralesional or topical glucocorticoids for localized GA as well as phototherapy or hydroxychloroquine for widespread disease.8,10

Annular elastolytic giant cell granuloma (also called actinic granuloma) is a rare idiopathic inflammatory skin disease. It is characterized by erythematous annular papules or plaques mainly found on sun-exposed skin, such as the backs of the hands, forearms, or face.11,12 Therefore, based on the distribution of our patient’s lesions, annular elastolytic giant cell granuloma was an unlikely diagnosis. Furthermore, it is not a known postherpetic isotopic reaction. Annular elastolytic giant cell granuloma can appear histologically similar to GA. Differentiating histologic features include a nonpalisading granuloma as well as the absence of mucin and necrobiosis.12
Annular lichen planus is a long-recognized but uncommon clinical variant of lichen planus that typically presents as pruritic, purple, annular plaques on the penis, scrotum, or intertriginous areas.13 The violaceous coloring is more characteristic of lichen planus. Histology is helpful in differentiating from GA.
Nummular eczema presents as scattered, welldefined, pruritic, erythematous, coin-shaped, coin-sized plaques in patients with diffusely dry skin.14 The scaling and serous crusting as well as more prominent pruritus help distinguish it from GA. The appearance of nummular eczema is quite characteristic; therefore, a biopsy typically is unnecessary for diagnosis. However, a potassium hydroxide wet mount examination of a skin scraping should be performed if tinea corporis also is suspected.
Superficial erythema annulare centrifugum classically presents as an annular or arciform pruritic lesion with an advancing outer erythematous edge with an inner rim of scale that most commonly occurs on the lower extremities. 15 The presence of pruritus and trailing scale helps distinguish this lesion from GA. Histologically, there are epidermal changes of hyperplasia, spongiosis, and parakeratosis, as well as lymphohistiocytic infiltrate surrounding the superficial dermal vessels.16
We report this case to highlight GA as the most common postherpetic isotopic response. It should be on the differential diagnosis when a patient presents with erythematous, smooth, annular plaques occurring in the distribution of a resolved case of HZV.
- Piette EW, Rosenbach M. Granuloma annulare: clinical and histologic variants, epidemiology, and genetics. J Am Acad Dermatol. 2016;75:457-465.
- . Wolf R, Brenner S, Ruocco V, et al. Isotopic response. Int J Dermatol. 1995;34:341-348.
- Kapoor R, Piris A, Saavedra AP, et al. Wolf isotopic response manifesting as postherpetic granuloma annulare: a case series. Arch Pathol Lab Med. 2013;137:255-258.
- Ezra N, Ahdout J, Haley JC, et al. Granuloma annulare in a zoster scar of a patient with multiple myeloma. Cutis. 2011;87:240-244.
- Noh TW, Park SH, Kang YS, et al. Morphea developing at the site of healed herpes zoster. Ann Dermatol. 2011;23:242-245.
- Ruocco V, Ruocco E, Ghersetich I, et al. Isotopic response after herpesvirus infection: an update. J Am Acad Dermatol. 2002;46:90-94.
- Sparrow G, Abell E. Granuloma annulare and necrobiosis lipoidica treated by jet injector. Br J Dermatol. 1975;93:85-89.
- Piette EW, Rosenbach M. Granuloma annulare: pathogenesis, disease associations and triggers, and therapeutic options. J Am Acad Dermatol. 2016;75:467-479.
- Thornsberry LA, English JC. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. Am J Clin Dermatol. 2013;14:279-290.
- Rubin CB, Rosenbach M. Granuloma annulare: a retrospective series of 133 patients. Cutis. 2019;103:102-106.
- Stein JA, Fangman B, Strober B. Actinic granuloma. Dermatol Online J. 2007;13:19.
- Mistry AM, Patel R, Mistry M, et al. Annular elastolytic giant cell granuloma. Cureus. 2020;12:E11456.
- Reich HL, Nguyen JT, James WD. Annular lichen planus: a case series of 20 patients. J Am Acad Dermatol. 2004;50:595-599.
- Leung AKC, Lam JM, Leong KF, et al. Nummular eczema: an updated review. Recent Pat Inflamm Allergy Drug Discov. 2020;14:146-155.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Coronel-Pérez IM, Morillo-Andújar M. Erythema annulare centrifugum responding to natural ultraviolet light [in Spanish]. Actas Dermosifiliogr. 2010;101:177-178.
The Diagnosis: Granuloma Annulare
A biopsy of a lesion on the right flank demonstrated granulomatous inflammation and interstitial mucin (Figure), characteristic of granuloma annulare (GA).1,2 Granuloma annulare is a relatively common skin disorder with an unknown etiology. It typically presents as smooth, annular, erythematous plaques.1 The most common variants of GA are localized, generalized, and subcutaneous. Our case demonstrated Wolf isotopic response, an unrelated skin disease that forms at the same location as a previously healed skin lesion.2 It is important to be aware of this phenomenon so that it is not confused with a recurrence of herpes zoster virus (HZV).
Although relatively infrequent, GA is the most common isotopic response following HZV infections.3-5 Other postherpetic isotopic eruptions include cutaneous malignancies, lichen planus, sarcoidosis, morphea, reactive perforating collagenosis, psoriasis, and infections, among others.3,5,6 The time between HZV infection and GA can be variable, ranging from a few weeks to many years apart.3
Oftentimes GA will spontaneously resolve within 2 years; however, recurrence is common.7-9 There currently are no standard treatment guidelines. The most promising treatment options include intralesional or topical glucocorticoids for localized GA as well as phototherapy or hydroxychloroquine for widespread disease.8,10
Annular elastolytic giant cell granuloma (also called actinic granuloma) is a rare idiopathic inflammatory skin disease. It is characterized by erythematous annular papules or plaques mainly found on sun-exposed skin, such as the backs of the hands, forearms, or face.11,12 Therefore, based on the distribution of our patient’s lesions, annular elastolytic giant cell granuloma was an unlikely diagnosis. Furthermore, it is not a known postherpetic isotopic reaction. Annular elastolytic giant cell granuloma can appear histologically similar to GA. Differentiating histologic features include a nonpalisading granuloma as well as the absence of mucin and necrobiosis.12
Annular lichen planus is a long-recognized but uncommon clinical variant of lichen planus that typically presents as pruritic, purple, annular plaques on the penis, scrotum, or intertriginous areas.13 The violaceous coloring is more characteristic of lichen planus. Histology is helpful in differentiating from GA.
Nummular eczema presents as scattered, welldefined, pruritic, erythematous, coin-shaped, coin-sized plaques in patients with diffusely dry skin.14 The scaling and serous crusting as well as more prominent pruritus help distinguish it from GA. The appearance of nummular eczema is quite characteristic; therefore, a biopsy typically is unnecessary for diagnosis. However, a potassium hydroxide wet mount examination of a skin scraping should be performed if tinea corporis also is suspected.
Superficial erythema annulare centrifugum classically presents as an annular or arciform pruritic lesion with an advancing outer erythematous edge with an inner rim of scale that most commonly occurs on the lower extremities. 15 The presence of pruritus and trailing scale helps distinguish this lesion from GA. Histologically, there are epidermal changes of hyperplasia, spongiosis, and parakeratosis, as well as lymphohistiocytic infiltrate surrounding the superficial dermal vessels.16
We report this case to highlight GA as the most common postherpetic isotopic response. It should be on the differential diagnosis when a patient presents with erythematous, smooth, annular plaques occurring in the distribution of a resolved case of HZV.
The Diagnosis: Granuloma Annulare
A biopsy of a lesion on the right flank demonstrated granulomatous inflammation and interstitial mucin (Figure), characteristic of granuloma annulare (GA).1,2 Granuloma annulare is a relatively common skin disorder with an unknown etiology. It typically presents as smooth, annular, erythematous plaques.1 The most common variants of GA are localized, generalized, and subcutaneous. Our case demonstrated Wolf isotopic response, an unrelated skin disease that forms at the same location as a previously healed skin lesion.2 It is important to be aware of this phenomenon so that it is not confused with a recurrence of herpes zoster virus (HZV).
Although relatively infrequent, GA is the most common isotopic response following HZV infections.3-5 Other postherpetic isotopic eruptions include cutaneous malignancies, lichen planus, sarcoidosis, morphea, reactive perforating collagenosis, psoriasis, and infections, among others.3,5,6 The time between HZV infection and GA can be variable, ranging from a few weeks to many years apart.3
Oftentimes GA will spontaneously resolve within 2 years; however, recurrence is common.7-9 There currently are no standard treatment guidelines. The most promising treatment options include intralesional or topical glucocorticoids for localized GA as well as phototherapy or hydroxychloroquine for widespread disease.8,10
Annular elastolytic giant cell granuloma (also called actinic granuloma) is a rare idiopathic inflammatory skin disease. It is characterized by erythematous annular papules or plaques mainly found on sun-exposed skin, such as the backs of the hands, forearms, or face.11,12 Therefore, based on the distribution of our patient’s lesions, annular elastolytic giant cell granuloma was an unlikely diagnosis. Furthermore, it is not a known postherpetic isotopic reaction. Annular elastolytic giant cell granuloma can appear histologically similar to GA. Differentiating histologic features include a nonpalisading granuloma as well as the absence of mucin and necrobiosis.12
Annular lichen planus is a long-recognized but uncommon clinical variant of lichen planus that typically presents as pruritic, purple, annular plaques on the penis, scrotum, or intertriginous areas.13 The violaceous coloring is more characteristic of lichen planus. Histology is helpful in differentiating from GA.
Nummular eczema presents as scattered, welldefined, pruritic, erythematous, coin-shaped, coin-sized plaques in patients with diffusely dry skin.14 The scaling and serous crusting as well as more prominent pruritus help distinguish it from GA. The appearance of nummular eczema is quite characteristic; therefore, a biopsy typically is unnecessary for diagnosis. However, a potassium hydroxide wet mount examination of a skin scraping should be performed if tinea corporis also is suspected.
Superficial erythema annulare centrifugum classically presents as an annular or arciform pruritic lesion with an advancing outer erythematous edge with an inner rim of scale that most commonly occurs on the lower extremities. 15 The presence of pruritus and trailing scale helps distinguish this lesion from GA. Histologically, there are epidermal changes of hyperplasia, spongiosis, and parakeratosis, as well as lymphohistiocytic infiltrate surrounding the superficial dermal vessels.16
We report this case to highlight GA as the most common postherpetic isotopic response. It should be on the differential diagnosis when a patient presents with erythematous, smooth, annular plaques occurring in the distribution of a resolved case of HZV.
- Piette EW, Rosenbach M. Granuloma annulare: clinical and histologic variants, epidemiology, and genetics. J Am Acad Dermatol. 2016;75:457-465.
- . Wolf R, Brenner S, Ruocco V, et al. Isotopic response. Int J Dermatol. 1995;34:341-348.
- Kapoor R, Piris A, Saavedra AP, et al. Wolf isotopic response manifesting as postherpetic granuloma annulare: a case series. Arch Pathol Lab Med. 2013;137:255-258.
- Ezra N, Ahdout J, Haley JC, et al. Granuloma annulare in a zoster scar of a patient with multiple myeloma. Cutis. 2011;87:240-244.
- Noh TW, Park SH, Kang YS, et al. Morphea developing at the site of healed herpes zoster. Ann Dermatol. 2011;23:242-245.
- Ruocco V, Ruocco E, Ghersetich I, et al. Isotopic response after herpesvirus infection: an update. J Am Acad Dermatol. 2002;46:90-94.
- Sparrow G, Abell E. Granuloma annulare and necrobiosis lipoidica treated by jet injector. Br J Dermatol. 1975;93:85-89.
- Piette EW, Rosenbach M. Granuloma annulare: pathogenesis, disease associations and triggers, and therapeutic options. J Am Acad Dermatol. 2016;75:467-479.
- Thornsberry LA, English JC. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. Am J Clin Dermatol. 2013;14:279-290.
- Rubin CB, Rosenbach M. Granuloma annulare: a retrospective series of 133 patients. Cutis. 2019;103:102-106.
- Stein JA, Fangman B, Strober B. Actinic granuloma. Dermatol Online J. 2007;13:19.
- Mistry AM, Patel R, Mistry M, et al. Annular elastolytic giant cell granuloma. Cureus. 2020;12:E11456.
- Reich HL, Nguyen JT, James WD. Annular lichen planus: a case series of 20 patients. J Am Acad Dermatol. 2004;50:595-599.
- Leung AKC, Lam JM, Leong KF, et al. Nummular eczema: an updated review. Recent Pat Inflamm Allergy Drug Discov. 2020;14:146-155.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Coronel-Pérez IM, Morillo-Andújar M. Erythema annulare centrifugum responding to natural ultraviolet light [in Spanish]. Actas Dermosifiliogr. 2010;101:177-178.
- Piette EW, Rosenbach M. Granuloma annulare: clinical and histologic variants, epidemiology, and genetics. J Am Acad Dermatol. 2016;75:457-465.
- . Wolf R, Brenner S, Ruocco V, et al. Isotopic response. Int J Dermatol. 1995;34:341-348.
- Kapoor R, Piris A, Saavedra AP, et al. Wolf isotopic response manifesting as postherpetic granuloma annulare: a case series. Arch Pathol Lab Med. 2013;137:255-258.
- Ezra N, Ahdout J, Haley JC, et al. Granuloma annulare in a zoster scar of a patient with multiple myeloma. Cutis. 2011;87:240-244.
- Noh TW, Park SH, Kang YS, et al. Morphea developing at the site of healed herpes zoster. Ann Dermatol. 2011;23:242-245.
- Ruocco V, Ruocco E, Ghersetich I, et al. Isotopic response after herpesvirus infection: an update. J Am Acad Dermatol. 2002;46:90-94.
- Sparrow G, Abell E. Granuloma annulare and necrobiosis lipoidica treated by jet injector. Br J Dermatol. 1975;93:85-89.
- Piette EW, Rosenbach M. Granuloma annulare: pathogenesis, disease associations and triggers, and therapeutic options. J Am Acad Dermatol. 2016;75:467-479.
- Thornsberry LA, English JC. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. Am J Clin Dermatol. 2013;14:279-290.
- Rubin CB, Rosenbach M. Granuloma annulare: a retrospective series of 133 patients. Cutis. 2019;103:102-106.
- Stein JA, Fangman B, Strober B. Actinic granuloma. Dermatol Online J. 2007;13:19.
- Mistry AM, Patel R, Mistry M, et al. Annular elastolytic giant cell granuloma. Cureus. 2020;12:E11456.
- Reich HL, Nguyen JT, James WD. Annular lichen planus: a case series of 20 patients. J Am Acad Dermatol. 2004;50:595-599.
- Leung AKC, Lam JM, Leong KF, et al. Nummular eczema: an updated review. Recent Pat Inflamm Allergy Drug Discov. 2020;14:146-155.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Coronel-Pérez IM, Morillo-Andújar M. Erythema annulare centrifugum responding to natural ultraviolet light [in Spanish]. Actas Dermosifiliogr. 2010;101:177-178.
An 82-year-old man presented with painful, pink, smooth, annular convalescing plaques on the right back, flank, and abdomen in a zosteriform distribution involving the T10/11 dermatome. He had a history of hypertension and type 2 diabetes mellitus, and 12 months prior to presentation he had an outbreak of herpes zoster virus in the same distribution that was treated with valacyclovir 1000 mg 3 times daily for 7 days. Over the following month he noticed a resolution of blisters and crusting as they morphed into the current lesions.

Precision medicine vs. antibiotic resistance
Diversity is an omnipresent element in clinical practice: in the genome, in the environment, in patients’ lifestyles and habits. Precision medicine addresses the variability of the individual to improve diagnosis and treatment. It is increasingly used in specialties such as oncology, neurology, and cardiology. A personalized approach has many objectives, including to optimize treatment, minimize the risk of adverse effects, facilitate early diagnosis, and determine predisposition to disease. Genomic technologies, such as massive sequencing techniques, and tools such as CRISPR-Cas9 are key to the future of personalized medicine.
Jesús Oteo Iglesias, MD, PhD, a specialist in microbiology and director of Spain’s National Center for Microbiology, spoke at the Spanish Association of Infectious Diseases and Clinical Microbiology’s recent conference. He discussed various precision medicine projects aimed at reinforcing the fight against antibiotic resistance.
Infectious diseases are complex because the diversity of the pathogenic microorganism combines with the patient’s own diversity, which influences the interaction between the two, said Dr. Oteo. Thus, the antibiogram and targeted antibiotic treatments (which are chosen according to the species, sensitivity to antimicrobials, type of infection, and patient characteristics) have been established applications of precision medicine for decades. However, multiple tools could further strengthen personalized medicine against multiresistant pathogens.
Therapeutic drug monitoring, in which multiple pharmacokinetic and pharmacodynamic factors are considered, is a strategy with great potential to increase the effectiveness of antibiotics and minimize toxicity. Owing to its costs and the need for trained staff, this tool would be especially indicated in the treatment of patients with more complex conditions, such as those suffering from obesity, complex infections, or infections with multiresistant bacteria, as well as those in critical condition. Multiple computer programs are available to help determine the dosage of antibiotics by estimating drug exposure and to provide recommendations. However, clinical trials are needed to assess the pros and cons of applying therapeutic monitoring for types of antibiotics other than those for which a given type is already used (for example, aminoglycosides and glycopeptides).
One technology that could help in antibiotic use optimization programs is microneedle-based biosensors, which could be implanted in the skin for real-time antibiotic monitoring. This tool “could be the first step in establishing automated antibiotic administration systems, with infusion pumps and feedback systems, like those already used in diabetes for insulin administration,” said Dr. Oteo.
Artificial intelligence could also be a valuable technology for optimization programs. “We should go a step further in the implementation of artificial intelligence through clinical decision support systems,” said Dr. Oteo. This technology would guide the administration of antimicrobials using data extracted from the electronic medical record. However, there are great challenges to overcome in creating these tools, such as the risk of entering erroneous data; the difficulty in entering complex data, such as data relevant to antibiotic resistance; and the variability at the geographic and institutional levels.
Genomics is also a tool with great potential for identifying bacteria’s degree of resistance to antibiotics by studying mutations in chromosomal and acquired genes. A proof-of-concept study evaluated the sensitivity of different Pseudomonas aeruginosa strains to several antibiotics by analyzing genome sequences associated with resistance, said Dr. Otero. The researchers found that this system was effective at predicting the sensitivity of bacteria from genomic data.
In the United States, the PATRIC bioinformatics center, which is financed by the National Institute of Allergy and Infectious Diseases, works with automated learning models to predict the antimicrobial resistance of different species of bacteria, including Staphylococcus aureus, Streptococcus pneumoniae, and Mycobacterium tuberculosis. These models, which work with genomic data associated with antibiotic resistance phenotypes, are able to identify resistance without prior knowledge of the underlying mechanisms.
Another factor to consider with regard to the use of precision medicine for infectious diseases is the microbiota. Dr. Oteo explained that the pathogenic microorganism interacts not only with the host but also with its microbiota, “which can be diverse, is manifold, and can be very different, depending on the circumstances. These interactions can be translated into ecological and evolutionary pressures that may have clinical significance.” One of the best-known examples is the possibility that a beta-lactamase–producing bacterium benefits other bacteria around it by secreting these enzymes. Furthermore, some known forms of bacterial interaction (such as plasmid transfer) are directly related to antibiotic resistance. Metagenomics, which involves the genetic study of communities of microbes, could provide more information for predicting and avoiding infections by multiresistant pathogens by monitoring the microbiome.
The CRISPR-Cas9 gene editing tool could also be an ally in the fight against antibiotic resistance by eliminating resistance genes and thus making bacteria sensitive to certain antibiotics. Several published preliminary studies indicate that this is possible in vitro. The main challenge for the clinical application of CRISPR is in introducing it into the target microbial population. Use of conjugative plasmids and bacteriophages could perhaps be an option for overcoming this obstacle in the future.
Exploiting the possibilities of precision medicine through use of the most innovative tools in addressing antibiotic resistance is a great challenge, said Dr. Oteo, but the situation demands it, and it is necessary to take small steps to achieve this goal.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
Diversity is an omnipresent element in clinical practice: in the genome, in the environment, in patients’ lifestyles and habits. Precision medicine addresses the variability of the individual to improve diagnosis and treatment. It is increasingly used in specialties such as oncology, neurology, and cardiology. A personalized approach has many objectives, including to optimize treatment, minimize the risk of adverse effects, facilitate early diagnosis, and determine predisposition to disease. Genomic technologies, such as massive sequencing techniques, and tools such as CRISPR-Cas9 are key to the future of personalized medicine.
Jesús Oteo Iglesias, MD, PhD, a specialist in microbiology and director of Spain’s National Center for Microbiology, spoke at the Spanish Association of Infectious Diseases and Clinical Microbiology’s recent conference. He discussed various precision medicine projects aimed at reinforcing the fight against antibiotic resistance.
Infectious diseases are complex because the diversity of the pathogenic microorganism combines with the patient’s own diversity, which influences the interaction between the two, said Dr. Oteo. Thus, the antibiogram and targeted antibiotic treatments (which are chosen according to the species, sensitivity to antimicrobials, type of infection, and patient characteristics) have been established applications of precision medicine for decades. However, multiple tools could further strengthen personalized medicine against multiresistant pathogens.
Therapeutic drug monitoring, in which multiple pharmacokinetic and pharmacodynamic factors are considered, is a strategy with great potential to increase the effectiveness of antibiotics and minimize toxicity. Owing to its costs and the need for trained staff, this tool would be especially indicated in the treatment of patients with more complex conditions, such as those suffering from obesity, complex infections, or infections with multiresistant bacteria, as well as those in critical condition. Multiple computer programs are available to help determine the dosage of antibiotics by estimating drug exposure and to provide recommendations. However, clinical trials are needed to assess the pros and cons of applying therapeutic monitoring for types of antibiotics other than those for which a given type is already used (for example, aminoglycosides and glycopeptides).
One technology that could help in antibiotic use optimization programs is microneedle-based biosensors, which could be implanted in the skin for real-time antibiotic monitoring. This tool “could be the first step in establishing automated antibiotic administration systems, with infusion pumps and feedback systems, like those already used in diabetes for insulin administration,” said Dr. Oteo.
Artificial intelligence could also be a valuable technology for optimization programs. “We should go a step further in the implementation of artificial intelligence through clinical decision support systems,” said Dr. Oteo. This technology would guide the administration of antimicrobials using data extracted from the electronic medical record. However, there are great challenges to overcome in creating these tools, such as the risk of entering erroneous data; the difficulty in entering complex data, such as data relevant to antibiotic resistance; and the variability at the geographic and institutional levels.
Genomics is also a tool with great potential for identifying bacteria’s degree of resistance to antibiotics by studying mutations in chromosomal and acquired genes. A proof-of-concept study evaluated the sensitivity of different Pseudomonas aeruginosa strains to several antibiotics by analyzing genome sequences associated with resistance, said Dr. Otero. The researchers found that this system was effective at predicting the sensitivity of bacteria from genomic data.
In the United States, the PATRIC bioinformatics center, which is financed by the National Institute of Allergy and Infectious Diseases, works with automated learning models to predict the antimicrobial resistance of different species of bacteria, including Staphylococcus aureus, Streptococcus pneumoniae, and Mycobacterium tuberculosis. These models, which work with genomic data associated with antibiotic resistance phenotypes, are able to identify resistance without prior knowledge of the underlying mechanisms.
Another factor to consider with regard to the use of precision medicine for infectious diseases is the microbiota. Dr. Oteo explained that the pathogenic microorganism interacts not only with the host but also with its microbiota, “which can be diverse, is manifold, and can be very different, depending on the circumstances. These interactions can be translated into ecological and evolutionary pressures that may have clinical significance.” One of the best-known examples is the possibility that a beta-lactamase–producing bacterium benefits other bacteria around it by secreting these enzymes. Furthermore, some known forms of bacterial interaction (such as plasmid transfer) are directly related to antibiotic resistance. Metagenomics, which involves the genetic study of communities of microbes, could provide more information for predicting and avoiding infections by multiresistant pathogens by monitoring the microbiome.
The CRISPR-Cas9 gene editing tool could also be an ally in the fight against antibiotic resistance by eliminating resistance genes and thus making bacteria sensitive to certain antibiotics. Several published preliminary studies indicate that this is possible in vitro. The main challenge for the clinical application of CRISPR is in introducing it into the target microbial population. Use of conjugative plasmids and bacteriophages could perhaps be an option for overcoming this obstacle in the future.
Exploiting the possibilities of precision medicine through use of the most innovative tools in addressing antibiotic resistance is a great challenge, said Dr. Oteo, but the situation demands it, and it is necessary to take small steps to achieve this goal.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
Diversity is an omnipresent element in clinical practice: in the genome, in the environment, in patients’ lifestyles and habits. Precision medicine addresses the variability of the individual to improve diagnosis and treatment. It is increasingly used in specialties such as oncology, neurology, and cardiology. A personalized approach has many objectives, including to optimize treatment, minimize the risk of adverse effects, facilitate early diagnosis, and determine predisposition to disease. Genomic technologies, such as massive sequencing techniques, and tools such as CRISPR-Cas9 are key to the future of personalized medicine.
Jesús Oteo Iglesias, MD, PhD, a specialist in microbiology and director of Spain’s National Center for Microbiology, spoke at the Spanish Association of Infectious Diseases and Clinical Microbiology’s recent conference. He discussed various precision medicine projects aimed at reinforcing the fight against antibiotic resistance.
Infectious diseases are complex because the diversity of the pathogenic microorganism combines with the patient’s own diversity, which influences the interaction between the two, said Dr. Oteo. Thus, the antibiogram and targeted antibiotic treatments (which are chosen according to the species, sensitivity to antimicrobials, type of infection, and patient characteristics) have been established applications of precision medicine for decades. However, multiple tools could further strengthen personalized medicine against multiresistant pathogens.
Therapeutic drug monitoring, in which multiple pharmacokinetic and pharmacodynamic factors are considered, is a strategy with great potential to increase the effectiveness of antibiotics and minimize toxicity. Owing to its costs and the need for trained staff, this tool would be especially indicated in the treatment of patients with more complex conditions, such as those suffering from obesity, complex infections, or infections with multiresistant bacteria, as well as those in critical condition. Multiple computer programs are available to help determine the dosage of antibiotics by estimating drug exposure and to provide recommendations. However, clinical trials are needed to assess the pros and cons of applying therapeutic monitoring for types of antibiotics other than those for which a given type is already used (for example, aminoglycosides and glycopeptides).
One technology that could help in antibiotic use optimization programs is microneedle-based biosensors, which could be implanted in the skin for real-time antibiotic monitoring. This tool “could be the first step in establishing automated antibiotic administration systems, with infusion pumps and feedback systems, like those already used in diabetes for insulin administration,” said Dr. Oteo.
Artificial intelligence could also be a valuable technology for optimization programs. “We should go a step further in the implementation of artificial intelligence through clinical decision support systems,” said Dr. Oteo. This technology would guide the administration of antimicrobials using data extracted from the electronic medical record. However, there are great challenges to overcome in creating these tools, such as the risk of entering erroneous data; the difficulty in entering complex data, such as data relevant to antibiotic resistance; and the variability at the geographic and institutional levels.
Genomics is also a tool with great potential for identifying bacteria’s degree of resistance to antibiotics by studying mutations in chromosomal and acquired genes. A proof-of-concept study evaluated the sensitivity of different Pseudomonas aeruginosa strains to several antibiotics by analyzing genome sequences associated with resistance, said Dr. Otero. The researchers found that this system was effective at predicting the sensitivity of bacteria from genomic data.
In the United States, the PATRIC bioinformatics center, which is financed by the National Institute of Allergy and Infectious Diseases, works with automated learning models to predict the antimicrobial resistance of different species of bacteria, including Staphylococcus aureus, Streptococcus pneumoniae, and Mycobacterium tuberculosis. These models, which work with genomic data associated with antibiotic resistance phenotypes, are able to identify resistance without prior knowledge of the underlying mechanisms.
Another factor to consider with regard to the use of precision medicine for infectious diseases is the microbiota. Dr. Oteo explained that the pathogenic microorganism interacts not only with the host but also with its microbiota, “which can be diverse, is manifold, and can be very different, depending on the circumstances. These interactions can be translated into ecological and evolutionary pressures that may have clinical significance.” One of the best-known examples is the possibility that a beta-lactamase–producing bacterium benefits other bacteria around it by secreting these enzymes. Furthermore, some known forms of bacterial interaction (such as plasmid transfer) are directly related to antibiotic resistance. Metagenomics, which involves the genetic study of communities of microbes, could provide more information for predicting and avoiding infections by multiresistant pathogens by monitoring the microbiome.
The CRISPR-Cas9 gene editing tool could also be an ally in the fight against antibiotic resistance by eliminating resistance genes and thus making bacteria sensitive to certain antibiotics. Several published preliminary studies indicate that this is possible in vitro. The main challenge for the clinical application of CRISPR is in introducing it into the target microbial population. Use of conjugative plasmids and bacteriophages could perhaps be an option for overcoming this obstacle in the future.
Exploiting the possibilities of precision medicine through use of the most innovative tools in addressing antibiotic resistance is a great challenge, said Dr. Oteo, but the situation demands it, and it is necessary to take small steps to achieve this goal.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
New treatment reduces risk of anal cancer in people with HIV
It all began with the question, “Has your butt been getting enough attention?”
Though that may seem unorthodox, it led researchers to discovering a treatment that may help prevent anal cancer in people with HIV/AIDS. It’s still featured on their study’s website, with this further explanation: “You get your viral load checked, your T-cell count checked, but what about your anus? Did you know that half of HIV+ men have cell changes in their anus caused by HPV?”
The Anal Cancer/HSIL Outcomes Research (ANCHOR) study, led by Joel Palefsky, MD, was published in The New England Journal of Medicine. Dr. Palefsky, an infectious disease expert at the University of California, San Francisco, and his team set out to determine whether a treatment that prevents cervical cancer in people with human papillomavirus (HPV) would benefit people with HIV/AIDS. The new treatment reduced the likelihood of anal cancer by more than 50%.
The team worked over 7 years, during which time they tested 4,459 men, women, transgender, and nonbinary individuals at 25 sites across the United States. The participants were sorted into two groups: Some received treatment for high-grade squamous intraepithelial lesions (HSILs), and some did not but were monitored for signs of disease. These included individuals over 35 who were living with HIV/AIDS and who were found to have patches of abnormal cells in their rectal lining.
HSILs are the cells gynecologists look for in performing a pap smear. They are precancerous cells commonly found in the cervix of persons with HPV. Finding HSILs during a gynecologic examination alerts clinicians to potential problems.
HSILs can also be found in the anal tract of men and women with HIV. Dr. Palefsky therefore hypothesized that, as with HPV and cervical cancer, these anal HSILs may be a precursor of anal cancer.
The scientists decided to treat these cells the same way they would treat them if found in the cervix and to see whether that reduced the risk of cancer. Doctors used lidocaine to numb the area, then removed the HSILs with an electric probe. The team then assessed whether the treatment prevented people from getting cancer.
It turns out that in many cases, it did. The study concluded after 30 of the participants developed anal cancer. Of those, 21 patients had not received HSIL treatment, compared with nine who did receive the treatment. The treatment resulted in a 57% reduction in the rate of anal cancer among patients who received treatment for their HSILs.
These results are encouraging, said Aasma Shaukat, MD, director of outcomes research in the Division of Gastroenterology and Hepatology at NYU Langone Health. Dr. Shaukat was not involved with the study. She believes it’s going to cause ripples across the field.
“The study is likely to change guidelines in favor of active and early treatment for HSIL and away from watchful waiting in individuals living with HIV to reduce the risk of developing anal squamous cell carcinoma, akin to removing polyps during colonoscopy to progression to and incidence of colorectal cancer,” she said in an email interview.
Treatments for this group of patients are more important now than ever. Since the beginning of the AIDS epidemic in the 1980s, the number of people with HIV has increased, Dr. Palefsky detailed in a press conference announcing the ANCHOR results. That’s partially because of new transmissions and partially owing to the fact that new treatments make it possible for people with HIV to live long, healthy lives. So as more people with HIV move into their sunset years, there are more people at risk for developing cancer, which is a disease associated with aging. Anal cancer sits at the intersection of risk for aging people who have HIV.
Any defense we have against the risk of cancer in this growing demographic is a good thing, says Hanna K. Sanoff, MD, a gastrointestinal oncologist at the Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, who was also not involved in the study. Although it’s not ready to be applied in doctors’ offices now, it could be a tool in the future. “Anything we can do to try and decrease the chance of precancerous lesions progressing to a real invasive cancer is of great importance. This kind of prevention work is critical to helping minimize the burden of cancer on our communities,” Dr. Sanoff said in an interview.
The study was funded by the National Cancer Institute of the National Institutes of Health and was conducted through the NCI-supported AIDS Malignancy Consortium. Dr. Shaukat and Dr. Sanoff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It all began with the question, “Has your butt been getting enough attention?”
Though that may seem unorthodox, it led researchers to discovering a treatment that may help prevent anal cancer in people with HIV/AIDS. It’s still featured on their study’s website, with this further explanation: “You get your viral load checked, your T-cell count checked, but what about your anus? Did you know that half of HIV+ men have cell changes in their anus caused by HPV?”
The Anal Cancer/HSIL Outcomes Research (ANCHOR) study, led by Joel Palefsky, MD, was published in The New England Journal of Medicine. Dr. Palefsky, an infectious disease expert at the University of California, San Francisco, and his team set out to determine whether a treatment that prevents cervical cancer in people with human papillomavirus (HPV) would benefit people with HIV/AIDS. The new treatment reduced the likelihood of anal cancer by more than 50%.
The team worked over 7 years, during which time they tested 4,459 men, women, transgender, and nonbinary individuals at 25 sites across the United States. The participants were sorted into two groups: Some received treatment for high-grade squamous intraepithelial lesions (HSILs), and some did not but were monitored for signs of disease. These included individuals over 35 who were living with HIV/AIDS and who were found to have patches of abnormal cells in their rectal lining.
HSILs are the cells gynecologists look for in performing a pap smear. They are precancerous cells commonly found in the cervix of persons with HPV. Finding HSILs during a gynecologic examination alerts clinicians to potential problems.
HSILs can also be found in the anal tract of men and women with HIV. Dr. Palefsky therefore hypothesized that, as with HPV and cervical cancer, these anal HSILs may be a precursor of anal cancer.
The scientists decided to treat these cells the same way they would treat them if found in the cervix and to see whether that reduced the risk of cancer. Doctors used lidocaine to numb the area, then removed the HSILs with an electric probe. The team then assessed whether the treatment prevented people from getting cancer.
It turns out that in many cases, it did. The study concluded after 30 of the participants developed anal cancer. Of those, 21 patients had not received HSIL treatment, compared with nine who did receive the treatment. The treatment resulted in a 57% reduction in the rate of anal cancer among patients who received treatment for their HSILs.
These results are encouraging, said Aasma Shaukat, MD, director of outcomes research in the Division of Gastroenterology and Hepatology at NYU Langone Health. Dr. Shaukat was not involved with the study. She believes it’s going to cause ripples across the field.
“The study is likely to change guidelines in favor of active and early treatment for HSIL and away from watchful waiting in individuals living with HIV to reduce the risk of developing anal squamous cell carcinoma, akin to removing polyps during colonoscopy to progression to and incidence of colorectal cancer,” she said in an email interview.
Treatments for this group of patients are more important now than ever. Since the beginning of the AIDS epidemic in the 1980s, the number of people with HIV has increased, Dr. Palefsky detailed in a press conference announcing the ANCHOR results. That’s partially because of new transmissions and partially owing to the fact that new treatments make it possible for people with HIV to live long, healthy lives. So as more people with HIV move into their sunset years, there are more people at risk for developing cancer, which is a disease associated with aging. Anal cancer sits at the intersection of risk for aging people who have HIV.
Any defense we have against the risk of cancer in this growing demographic is a good thing, says Hanna K. Sanoff, MD, a gastrointestinal oncologist at the Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, who was also not involved in the study. Although it’s not ready to be applied in doctors’ offices now, it could be a tool in the future. “Anything we can do to try and decrease the chance of precancerous lesions progressing to a real invasive cancer is of great importance. This kind of prevention work is critical to helping minimize the burden of cancer on our communities,” Dr. Sanoff said in an interview.
The study was funded by the National Cancer Institute of the National Institutes of Health and was conducted through the NCI-supported AIDS Malignancy Consortium. Dr. Shaukat and Dr. Sanoff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It all began with the question, “Has your butt been getting enough attention?”
Though that may seem unorthodox, it led researchers to discovering a treatment that may help prevent anal cancer in people with HIV/AIDS. It’s still featured on their study’s website, with this further explanation: “You get your viral load checked, your T-cell count checked, but what about your anus? Did you know that half of HIV+ men have cell changes in their anus caused by HPV?”
The Anal Cancer/HSIL Outcomes Research (ANCHOR) study, led by Joel Palefsky, MD, was published in The New England Journal of Medicine. Dr. Palefsky, an infectious disease expert at the University of California, San Francisco, and his team set out to determine whether a treatment that prevents cervical cancer in people with human papillomavirus (HPV) would benefit people with HIV/AIDS. The new treatment reduced the likelihood of anal cancer by more than 50%.
The team worked over 7 years, during which time they tested 4,459 men, women, transgender, and nonbinary individuals at 25 sites across the United States. The participants were sorted into two groups: Some received treatment for high-grade squamous intraepithelial lesions (HSILs), and some did not but were monitored for signs of disease. These included individuals over 35 who were living with HIV/AIDS and who were found to have patches of abnormal cells in their rectal lining.
HSILs are the cells gynecologists look for in performing a pap smear. They are precancerous cells commonly found in the cervix of persons with HPV. Finding HSILs during a gynecologic examination alerts clinicians to potential problems.
HSILs can also be found in the anal tract of men and women with HIV. Dr. Palefsky therefore hypothesized that, as with HPV and cervical cancer, these anal HSILs may be a precursor of anal cancer.
The scientists decided to treat these cells the same way they would treat them if found in the cervix and to see whether that reduced the risk of cancer. Doctors used lidocaine to numb the area, then removed the HSILs with an electric probe. The team then assessed whether the treatment prevented people from getting cancer.
It turns out that in many cases, it did. The study concluded after 30 of the participants developed anal cancer. Of those, 21 patients had not received HSIL treatment, compared with nine who did receive the treatment. The treatment resulted in a 57% reduction in the rate of anal cancer among patients who received treatment for their HSILs.
These results are encouraging, said Aasma Shaukat, MD, director of outcomes research in the Division of Gastroenterology and Hepatology at NYU Langone Health. Dr. Shaukat was not involved with the study. She believes it’s going to cause ripples across the field.
“The study is likely to change guidelines in favor of active and early treatment for HSIL and away from watchful waiting in individuals living with HIV to reduce the risk of developing anal squamous cell carcinoma, akin to removing polyps during colonoscopy to progression to and incidence of colorectal cancer,” she said in an email interview.
Treatments for this group of patients are more important now than ever. Since the beginning of the AIDS epidemic in the 1980s, the number of people with HIV has increased, Dr. Palefsky detailed in a press conference announcing the ANCHOR results. That’s partially because of new transmissions and partially owing to the fact that new treatments make it possible for people with HIV to live long, healthy lives. So as more people with HIV move into their sunset years, there are more people at risk for developing cancer, which is a disease associated with aging. Anal cancer sits at the intersection of risk for aging people who have HIV.
Any defense we have against the risk of cancer in this growing demographic is a good thing, says Hanna K. Sanoff, MD, a gastrointestinal oncologist at the Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, who was also not involved in the study. Although it’s not ready to be applied in doctors’ offices now, it could be a tool in the future. “Anything we can do to try and decrease the chance of precancerous lesions progressing to a real invasive cancer is of great importance. This kind of prevention work is critical to helping minimize the burden of cancer on our communities,” Dr. Sanoff said in an interview.
The study was funded by the National Cancer Institute of the National Institutes of Health and was conducted through the NCI-supported AIDS Malignancy Consortium. Dr. Shaukat and Dr. Sanoff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Disturbed sleep drives poor PrEP adherence in young Black sexual-minority men
Young Black sexual-minority men (YBSMM) who experience sleep disturbance at least 3-4 times a week are much more likely to miss HIV pre-exposure prophylaxis (PrEP) doses than those who rarely report sleep disturbance, according to a new study published online in the journal AIDS and Behavior.
Sleep disturbance, poor cognitive processing, and memory function deficits go hand in hand, especially among people living with HIV.
Data have suggested that poor sleep might be an important factor in common neurocognitive complaints and overall health outcomes, especially among older adults with HIV. But few studies have examined the role that sleep quality might play in driving health behaviors around prevention and PrEP adherence, especially among YBSMM, who are at highest risk for acquiring new HIV infections.
Commonly cited reasons for suboptimal HIV prevention efforts within this population often include stigma, mistrust of the medical system, and a lack of culturally appropriate care.
“We make a lot of assumptions about young people and their brains and their ability to remember things, namely [that] they should be better than older adults at remembering to take medications,” lead study investigator Jade Pagkas-Bather, MD, an infectious disease specialist at University of Chicago Medicine, told this news organization.
“In reality, many young people are not used to taking medications, [especially] for a disease that they do not have.”
Too many pills, too little sleep
The researchers examined data collected from participants in the Neighborhoods and Networks Cohort Study, Chicago, which looked at the role of social, contextual, network, and geospatial factors influencing HIV prevention and care in HIV-negative, cisgender YBSMM between 2018 and 2019.
The investigators included 70 YBSMM participants who reported current PrEP use in the analysis. All were between the ages of 16 and 24 years, self-identified as African American or Black, were assigned male at birth, and reported at least one sexual encounter with a man or transgender woman in the previous 12 months.
Sleep was measured using the Patient Health Questionnaire-9 (PHQ-9) which includes a question on frequency of sleep disturbance (that is, trouble falling asleep, staying asleep, or sleeping too much) categorized as follows: less than 1 day (rarely or none of the time), 1-2 days (some or a little of the time), 3-4 days (occasionally or a moderate amount of time), or 5-7 days (all of the time).
Almost half (47.1%) of participants self-reported some or moderate sleep disturbance, with 8.6% having sleep disturbance all of the time.
“One of the main findings was that poor sleep and having too many pills impacts people’s ability to remember to take their PrEP or is associated with missing PrEP doses,” explained Dr. Pagkas-Bather.
In adjusted models, YBSMM who reported moderate sleep disturbances cited having too many pills to take as the reason for missing or forgetting PrEP doses (adjusted odds ratio, 7.59; 95% confidence interval, 1.05-54.57), compared with peers who did not have sleep issues.
Depression was likewise an important factor. Participants who reported experiencing sleep disturbance all of the time and missing PrEP doses were also highly likely to be depressed (aOR, 11.30; 95% CI, 1.19-107.53).
“The PHQ-9 is a widely accepted measure looking at depression – and sleep as one symptom of depression,” explained Brooke Genkin Rogers, Ph.D., M.P.H., a research scientist and assistant professor of psychiatry and human behavior at the Warren Alpert Medical School of Brown University, Providence, R.I.
Dr. Rogers, who was not involved in the study, noted, “Sleep disturbance is a sign of poor physical or mental health, particularly in an otherwise younger, healthier population.” But Dr. Rogers also had questions about sleep duration (that is, too short or too long) and whether or not it also played a role in poor adherence, information that was not pursued within the study.
“As a clinician, I see quite a few people who are young Black sexual minority men who are on PrEP, or on the converse side, people living with HIV and taking medications for HIV treatment. I would posit a guess that it’s not that people are necessarily sleeping too much, but there are other sorts of factors that interfere with being able to get 8 hours of sleep a night,” explained Dr. Pagkas-Bather.
They include structural issues like greater exposure to housing instability and neighborhood safety.
However, Dr. Pagkas-Bather pointed to an even more critical factor influencing PrEP usage and adherence, one that she refers to as “Trickle Up HIV Care.”
“We can’t just come up with interventions, drugs, and studies and say, we have all of these options, anyone who wants them, come and get them,” she said. “We really need to work very hard at educating and encouraging populations who have no high-level need for prevention and treatment.”
As a clinician who works closely with the YBSMM population, Dr. Pagkas-Bather also shared that her patients have told her that they’ve asked for PrEP and have had providers turn them down because they weren’t comfortable prescribing PrEP or made assumptions about the kind of people who are on PrEP.
“There are sometimes assumptions made about Black men and sexual promiscuity. And the data doesn’t bear that out. It’s not that Black men are having more sex than White men or any other man; it’s that the prevalence of HIV in the Black community is higher overall relative to the population,” noted Dr. Pagkas-Bather.
“We need a nuanced approach to examining these issues ... to take a look at multiple levels of influence on folks’ health and HIV risk,” said Dr. Rogers.
Both clinicians acknowledged that creative solutions have not been exhausted.
“There’s a lot of opportunity if we sit down with communities and share in decisions around HIV treatment and prevention ... if we tap into the wealth and knowledge of the Black communities to prevent HIV,” concluded Dr. Pagkas-Bather.
Dr. Pagkas-Bather reports that she is a Gilead Sciences HIV Research Scholar awardee. Dr. Rogers reports receiving a scientific research grant from Gilead Sciences.
A version of this article first appeared on Medscape.com.
Young Black sexual-minority men (YBSMM) who experience sleep disturbance at least 3-4 times a week are much more likely to miss HIV pre-exposure prophylaxis (PrEP) doses than those who rarely report sleep disturbance, according to a new study published online in the journal AIDS and Behavior.
Sleep disturbance, poor cognitive processing, and memory function deficits go hand in hand, especially among people living with HIV.
Data have suggested that poor sleep might be an important factor in common neurocognitive complaints and overall health outcomes, especially among older adults with HIV. But few studies have examined the role that sleep quality might play in driving health behaviors around prevention and PrEP adherence, especially among YBSMM, who are at highest risk for acquiring new HIV infections.
Commonly cited reasons for suboptimal HIV prevention efforts within this population often include stigma, mistrust of the medical system, and a lack of culturally appropriate care.
“We make a lot of assumptions about young people and their brains and their ability to remember things, namely [that] they should be better than older adults at remembering to take medications,” lead study investigator Jade Pagkas-Bather, MD, an infectious disease specialist at University of Chicago Medicine, told this news organization.
“In reality, many young people are not used to taking medications, [especially] for a disease that they do not have.”
Too many pills, too little sleep
The researchers examined data collected from participants in the Neighborhoods and Networks Cohort Study, Chicago, which looked at the role of social, contextual, network, and geospatial factors influencing HIV prevention and care in HIV-negative, cisgender YBSMM between 2018 and 2019.
The investigators included 70 YBSMM participants who reported current PrEP use in the analysis. All were between the ages of 16 and 24 years, self-identified as African American or Black, were assigned male at birth, and reported at least one sexual encounter with a man or transgender woman in the previous 12 months.
Sleep was measured using the Patient Health Questionnaire-9 (PHQ-9) which includes a question on frequency of sleep disturbance (that is, trouble falling asleep, staying asleep, or sleeping too much) categorized as follows: less than 1 day (rarely or none of the time), 1-2 days (some or a little of the time), 3-4 days (occasionally or a moderate amount of time), or 5-7 days (all of the time).
Almost half (47.1%) of participants self-reported some or moderate sleep disturbance, with 8.6% having sleep disturbance all of the time.
“One of the main findings was that poor sleep and having too many pills impacts people’s ability to remember to take their PrEP or is associated with missing PrEP doses,” explained Dr. Pagkas-Bather.
In adjusted models, YBSMM who reported moderate sleep disturbances cited having too many pills to take as the reason for missing or forgetting PrEP doses (adjusted odds ratio, 7.59; 95% confidence interval, 1.05-54.57), compared with peers who did not have sleep issues.
Depression was likewise an important factor. Participants who reported experiencing sleep disturbance all of the time and missing PrEP doses were also highly likely to be depressed (aOR, 11.30; 95% CI, 1.19-107.53).
“The PHQ-9 is a widely accepted measure looking at depression – and sleep as one symptom of depression,” explained Brooke Genkin Rogers, Ph.D., M.P.H., a research scientist and assistant professor of psychiatry and human behavior at the Warren Alpert Medical School of Brown University, Providence, R.I.
Dr. Rogers, who was not involved in the study, noted, “Sleep disturbance is a sign of poor physical or mental health, particularly in an otherwise younger, healthier population.” But Dr. Rogers also had questions about sleep duration (that is, too short or too long) and whether or not it also played a role in poor adherence, information that was not pursued within the study.
“As a clinician, I see quite a few people who are young Black sexual minority men who are on PrEP, or on the converse side, people living with HIV and taking medications for HIV treatment. I would posit a guess that it’s not that people are necessarily sleeping too much, but there are other sorts of factors that interfere with being able to get 8 hours of sleep a night,” explained Dr. Pagkas-Bather.
They include structural issues like greater exposure to housing instability and neighborhood safety.
However, Dr. Pagkas-Bather pointed to an even more critical factor influencing PrEP usage and adherence, one that she refers to as “Trickle Up HIV Care.”
“We can’t just come up with interventions, drugs, and studies and say, we have all of these options, anyone who wants them, come and get them,” she said. “We really need to work very hard at educating and encouraging populations who have no high-level need for prevention and treatment.”
As a clinician who works closely with the YBSMM population, Dr. Pagkas-Bather also shared that her patients have told her that they’ve asked for PrEP and have had providers turn them down because they weren’t comfortable prescribing PrEP or made assumptions about the kind of people who are on PrEP.
“There are sometimes assumptions made about Black men and sexual promiscuity. And the data doesn’t bear that out. It’s not that Black men are having more sex than White men or any other man; it’s that the prevalence of HIV in the Black community is higher overall relative to the population,” noted Dr. Pagkas-Bather.
“We need a nuanced approach to examining these issues ... to take a look at multiple levels of influence on folks’ health and HIV risk,” said Dr. Rogers.
Both clinicians acknowledged that creative solutions have not been exhausted.
“There’s a lot of opportunity if we sit down with communities and share in decisions around HIV treatment and prevention ... if we tap into the wealth and knowledge of the Black communities to prevent HIV,” concluded Dr. Pagkas-Bather.
Dr. Pagkas-Bather reports that she is a Gilead Sciences HIV Research Scholar awardee. Dr. Rogers reports receiving a scientific research grant from Gilead Sciences.
A version of this article first appeared on Medscape.com.
Young Black sexual-minority men (YBSMM) who experience sleep disturbance at least 3-4 times a week are much more likely to miss HIV pre-exposure prophylaxis (PrEP) doses than those who rarely report sleep disturbance, according to a new study published online in the journal AIDS and Behavior.
Sleep disturbance, poor cognitive processing, and memory function deficits go hand in hand, especially among people living with HIV.
Data have suggested that poor sleep might be an important factor in common neurocognitive complaints and overall health outcomes, especially among older adults with HIV. But few studies have examined the role that sleep quality might play in driving health behaviors around prevention and PrEP adherence, especially among YBSMM, who are at highest risk for acquiring new HIV infections.
Commonly cited reasons for suboptimal HIV prevention efforts within this population often include stigma, mistrust of the medical system, and a lack of culturally appropriate care.
“We make a lot of assumptions about young people and their brains and their ability to remember things, namely [that] they should be better than older adults at remembering to take medications,” lead study investigator Jade Pagkas-Bather, MD, an infectious disease specialist at University of Chicago Medicine, told this news organization.
“In reality, many young people are not used to taking medications, [especially] for a disease that they do not have.”
Too many pills, too little sleep
The researchers examined data collected from participants in the Neighborhoods and Networks Cohort Study, Chicago, which looked at the role of social, contextual, network, and geospatial factors influencing HIV prevention and care in HIV-negative, cisgender YBSMM between 2018 and 2019.
The investigators included 70 YBSMM participants who reported current PrEP use in the analysis. All were between the ages of 16 and 24 years, self-identified as African American or Black, were assigned male at birth, and reported at least one sexual encounter with a man or transgender woman in the previous 12 months.
Sleep was measured using the Patient Health Questionnaire-9 (PHQ-9) which includes a question on frequency of sleep disturbance (that is, trouble falling asleep, staying asleep, or sleeping too much) categorized as follows: less than 1 day (rarely or none of the time), 1-2 days (some or a little of the time), 3-4 days (occasionally or a moderate amount of time), or 5-7 days (all of the time).
Almost half (47.1%) of participants self-reported some or moderate sleep disturbance, with 8.6% having sleep disturbance all of the time.
“One of the main findings was that poor sleep and having too many pills impacts people’s ability to remember to take their PrEP or is associated with missing PrEP doses,” explained Dr. Pagkas-Bather.
In adjusted models, YBSMM who reported moderate sleep disturbances cited having too many pills to take as the reason for missing or forgetting PrEP doses (adjusted odds ratio, 7.59; 95% confidence interval, 1.05-54.57), compared with peers who did not have sleep issues.
Depression was likewise an important factor. Participants who reported experiencing sleep disturbance all of the time and missing PrEP doses were also highly likely to be depressed (aOR, 11.30; 95% CI, 1.19-107.53).
“The PHQ-9 is a widely accepted measure looking at depression – and sleep as one symptom of depression,” explained Brooke Genkin Rogers, Ph.D., M.P.H., a research scientist and assistant professor of psychiatry and human behavior at the Warren Alpert Medical School of Brown University, Providence, R.I.
Dr. Rogers, who was not involved in the study, noted, “Sleep disturbance is a sign of poor physical or mental health, particularly in an otherwise younger, healthier population.” But Dr. Rogers also had questions about sleep duration (that is, too short or too long) and whether or not it also played a role in poor adherence, information that was not pursued within the study.
“As a clinician, I see quite a few people who are young Black sexual minority men who are on PrEP, or on the converse side, people living with HIV and taking medications for HIV treatment. I would posit a guess that it’s not that people are necessarily sleeping too much, but there are other sorts of factors that interfere with being able to get 8 hours of sleep a night,” explained Dr. Pagkas-Bather.
They include structural issues like greater exposure to housing instability and neighborhood safety.
However, Dr. Pagkas-Bather pointed to an even more critical factor influencing PrEP usage and adherence, one that she refers to as “Trickle Up HIV Care.”
“We can’t just come up with interventions, drugs, and studies and say, we have all of these options, anyone who wants them, come and get them,” she said. “We really need to work very hard at educating and encouraging populations who have no high-level need for prevention and treatment.”
As a clinician who works closely with the YBSMM population, Dr. Pagkas-Bather also shared that her patients have told her that they’ve asked for PrEP and have had providers turn them down because they weren’t comfortable prescribing PrEP or made assumptions about the kind of people who are on PrEP.
“There are sometimes assumptions made about Black men and sexual promiscuity. And the data doesn’t bear that out. It’s not that Black men are having more sex than White men or any other man; it’s that the prevalence of HIV in the Black community is higher overall relative to the population,” noted Dr. Pagkas-Bather.
“We need a nuanced approach to examining these issues ... to take a look at multiple levels of influence on folks’ health and HIV risk,” said Dr. Rogers.
Both clinicians acknowledged that creative solutions have not been exhausted.
“There’s a lot of opportunity if we sit down with communities and share in decisions around HIV treatment and prevention ... if we tap into the wealth and knowledge of the Black communities to prevent HIV,” concluded Dr. Pagkas-Bather.
Dr. Pagkas-Bather reports that she is a Gilead Sciences HIV Research Scholar awardee. Dr. Rogers reports receiving a scientific research grant from Gilead Sciences.
A version of this article first appeared on Medscape.com.
Doc’s misdiagnosis causes former firefighter to lose leg from flesh-eating bacterial infection
, as a story in the Pensacola News Journal indicates.
In September 2016, the former firefighter visited a hospital-affiliated urgent care center after he developed an ache and a blue discoloration in his right leg. Prior to this, the story says, he had been “exposed to the waters of Pensacola Bay,” which might have caused the infection.
At the urgent care center, he was examined by a primary care physician, who diagnosed him with an ankle sprain. Instructed to ice and elevate his leg, the former firefighter was given crutches and sent home.
The following day, still in pain, he visited a local podiatrist, who “immediately suspected ... [the patient] was suffering from an ongoing aggressive bacterial infection.” The podiatrist then arranged for the patient to be seen at a nearby hospital emergency department. There, doctors diagnosed a “necrotizing bacterial infection that need[ed] to be aggressively treated with antibodies and the removal of dead tissue.”
But despite their best efforts to control the infection and remove the necrotized tissue, the doctors eventually had to amputate the patient’s right leg above the knee.
The former firefighter and his wife then sued the primary care physician and the hospital where the physician worked.
After an 8-day civil trial, the jury awarded the plaintiff and his wife $6,805,071 and $787,371, respectively.
“What happened to [my clients] should never have happened,” said the attorney representing the plaintiffs.
The hospital declined to comment to the Pensacola News Journal about the case.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
, as a story in the Pensacola News Journal indicates.
In September 2016, the former firefighter visited a hospital-affiliated urgent care center after he developed an ache and a blue discoloration in his right leg. Prior to this, the story says, he had been “exposed to the waters of Pensacola Bay,” which might have caused the infection.
At the urgent care center, he was examined by a primary care physician, who diagnosed him with an ankle sprain. Instructed to ice and elevate his leg, the former firefighter was given crutches and sent home.
The following day, still in pain, he visited a local podiatrist, who “immediately suspected ... [the patient] was suffering from an ongoing aggressive bacterial infection.” The podiatrist then arranged for the patient to be seen at a nearby hospital emergency department. There, doctors diagnosed a “necrotizing bacterial infection that need[ed] to be aggressively treated with antibodies and the removal of dead tissue.”
But despite their best efforts to control the infection and remove the necrotized tissue, the doctors eventually had to amputate the patient’s right leg above the knee.
The former firefighter and his wife then sued the primary care physician and the hospital where the physician worked.
After an 8-day civil trial, the jury awarded the plaintiff and his wife $6,805,071 and $787,371, respectively.
“What happened to [my clients] should never have happened,” said the attorney representing the plaintiffs.
The hospital declined to comment to the Pensacola News Journal about the case.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
, as a story in the Pensacola News Journal indicates.
In September 2016, the former firefighter visited a hospital-affiliated urgent care center after he developed an ache and a blue discoloration in his right leg. Prior to this, the story says, he had been “exposed to the waters of Pensacola Bay,” which might have caused the infection.
At the urgent care center, he was examined by a primary care physician, who diagnosed him with an ankle sprain. Instructed to ice and elevate his leg, the former firefighter was given crutches and sent home.
The following day, still in pain, he visited a local podiatrist, who “immediately suspected ... [the patient] was suffering from an ongoing aggressive bacterial infection.” The podiatrist then arranged for the patient to be seen at a nearby hospital emergency department. There, doctors diagnosed a “necrotizing bacterial infection that need[ed] to be aggressively treated with antibodies and the removal of dead tissue.”
But despite their best efforts to control the infection and remove the necrotized tissue, the doctors eventually had to amputate the patient’s right leg above the knee.
The former firefighter and his wife then sued the primary care physician and the hospital where the physician worked.
After an 8-day civil trial, the jury awarded the plaintiff and his wife $6,805,071 and $787,371, respectively.
“What happened to [my clients] should never have happened,” said the attorney representing the plaintiffs.
The hospital declined to comment to the Pensacola News Journal about the case.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
FDA authorizes COVID vaccines in kids as young as 6 months
, one of the final steps in a long-awaited authorization process to extend protection to the youngest of Americans.
The agency’s move comes after a closely watched FDA advisory group vote earlier this week, which resulted in a unanimous vote in favor of the FDA authorizing both vaccines in this age group.
“The FDA’s evaluation and analysis of the safety, effectiveness, and manufacturing data of these vaccines was rigorous and comprehensive, supporting the EUAs,” the agency said in a news release.
The data show that the “known and potential benefits” of the vaccines outweigh any potential risks, the agency said.
The Moderna vaccine is authorized as a two-dose primary series in children 6 months to 17 years of age. The Pfizer vaccine is now authorized as a three-dose primary series in children 6 months up to 4 years of age. Pfizer’s vaccine was already authorized in children 5 years old and older.
Now all eyes are on the Centers for Disease Control and Prevention, which is expected to decide on the final regulatory hurdle at a meeting June 18. The CDC’s Advisory Committee on Immunization Practices has scheduled a vote on whether to give the vaccines the green light.
If ACIP gives the OK, CDC Director Rochelle Walensky, MD, MPH, is expected to issue recommendations for use shortly thereafter.
Following these final regulatory steps, parents could start bringing their children to pediatricians, family doctors, or local pharmacies for vaccination as early as June 20.
A version of this article first appeared on WebMD.com.
, one of the final steps in a long-awaited authorization process to extend protection to the youngest of Americans.
The agency’s move comes after a closely watched FDA advisory group vote earlier this week, which resulted in a unanimous vote in favor of the FDA authorizing both vaccines in this age group.
“The FDA’s evaluation and analysis of the safety, effectiveness, and manufacturing data of these vaccines was rigorous and comprehensive, supporting the EUAs,” the agency said in a news release.
The data show that the “known and potential benefits” of the vaccines outweigh any potential risks, the agency said.
The Moderna vaccine is authorized as a two-dose primary series in children 6 months to 17 years of age. The Pfizer vaccine is now authorized as a three-dose primary series in children 6 months up to 4 years of age. Pfizer’s vaccine was already authorized in children 5 years old and older.
Now all eyes are on the Centers for Disease Control and Prevention, which is expected to decide on the final regulatory hurdle at a meeting June 18. The CDC’s Advisory Committee on Immunization Practices has scheduled a vote on whether to give the vaccines the green light.
If ACIP gives the OK, CDC Director Rochelle Walensky, MD, MPH, is expected to issue recommendations for use shortly thereafter.
Following these final regulatory steps, parents could start bringing their children to pediatricians, family doctors, or local pharmacies for vaccination as early as June 20.
A version of this article first appeared on WebMD.com.
, one of the final steps in a long-awaited authorization process to extend protection to the youngest of Americans.
The agency’s move comes after a closely watched FDA advisory group vote earlier this week, which resulted in a unanimous vote in favor of the FDA authorizing both vaccines in this age group.
“The FDA’s evaluation and analysis of the safety, effectiveness, and manufacturing data of these vaccines was rigorous and comprehensive, supporting the EUAs,” the agency said in a news release.
The data show that the “known and potential benefits” of the vaccines outweigh any potential risks, the agency said.
The Moderna vaccine is authorized as a two-dose primary series in children 6 months to 17 years of age. The Pfizer vaccine is now authorized as a three-dose primary series in children 6 months up to 4 years of age. Pfizer’s vaccine was already authorized in children 5 years old and older.
Now all eyes are on the Centers for Disease Control and Prevention, which is expected to decide on the final regulatory hurdle at a meeting June 18. The CDC’s Advisory Committee on Immunization Practices has scheduled a vote on whether to give the vaccines the green light.
If ACIP gives the OK, CDC Director Rochelle Walensky, MD, MPH, is expected to issue recommendations for use shortly thereafter.
Following these final regulatory steps, parents could start bringing their children to pediatricians, family doctors, or local pharmacies for vaccination as early as June 20.
A version of this article first appeared on WebMD.com.
Past COVID-19 infection could play role in childhood hepatitis
There may be a link between the recent unexplained cases of hepatitis in children and prior coronavirus infections, according to new research from Israel.
The study involves five children in Israel who had mild cases of COVID-19 who went on to develop hepatitis; two of these children required liver transplants. But clinicians are cautious about drawing conclusions from such a small study.
“All you can say is that these five cases seem to have proximity to COVID-19, and COVID-19 may be able to cause pediatric liver complications,” said Nancy Reau, MD, section chief of hepatology at Rush University in Chicago. She was not involved with the study.
While COVID-19 could be one explanation for these hepatitis cases, it is also possible that the two are unrelated, said William Balistreri, MD, director emeritus of the Pediatric Liver Care Center at Cincinnati Children’s Hospital Medical Center. He also is unaffiliated with the study.
Hepatitis is rare in children, and between 30% and 50% of these pediatric cases have no known cause, according to the CDC.
Since April 2022, children with hepatitis of an unexplained cause have garnered global attention. The United Kingdom now has 240 confirmed cases, the United States is investigating 290 cases, and Israel has reported 12 cases to the World Health Organization. Many investigators think that these liver problems could be related to adenovirus – a common infection in children that normally causes cold or flu-like symptoms – because more than half of global cases tested for the virus have been positive, according to the WHO. About 12% of children with unexplained hepatitis have tested positive for SARS-CoV-2, the virus that causes COVID-19, but investigators are considering the possibility that some cases may be related to prior infections.
The study documents five patients, 3-months to 13 years old, with prior coronavirus infection who later developed hepatitis. All were treated at Schneider Children’s Medical Hospital in Petah Tikva, Israel, during 2021. The paper was published in the Journal of Pediatric Gastroenterology and Nutrition. Two patients, a 3-month-old and 5-month-old, needed liver transplants. The other three patients (two 8-year-olds and a 13-year-old) were treated with steroids. None of the five children had received any vaccinations against COVID-19. The time between COVID-19 infection and liver problems ranged from 21 to 130 days.
“It took time to be convinced that this could be COVID-related,” said senior study author Orith Waisbourd-Zinman, MD, director of pediatric liver disease service at Schneider Children’s Medical Hospital. “It’s something that wasn’t described.”
Sudden-onset hepatitis after COVID-19 has been recorded in adults, and the virus has been associated with multisystem inflammatory syndrome in children (MIS-C). The condition causes inflammation through the body, including the heart, lungs, and kidneys.
“We know that COVID can be mischievous, and children are no more exempt from that than adults,” Dr. Reau said.
Liver samples taken from these five patients did not test positive for COVID-19, similar to how liver samples have tested negative for adenovirus in more recent hepatitis cases around the world. Dr. Waisbourd-Zinman suggested that in these patients, hepatitis may have been brought on by an inflammatory response that was triggered by the virus.
Still, there are notable differences between these five cases and current cases internationally. These five children became sick during the period of December 2020 to September 2021, whereas all current counted cases in the United Kingdom occurred after January 2022. The first cases in the United States took place in October 2021. It could be that there were similar hepatitis cases before that were not identified, Dr. Reau said.
The ages of the Israeli children with hepatitis also differ from the cases seen globally. More than three-fourths of these reported hepatitis cases occurred in children under 5, the WHO reports, though affected individuals have been as young as 1-month-old up to 16 years old. In the United Kingdom, which accounts for about a third of cases reported to the WHO, most children with unexplained hepatitis have been between 3 and 5 years old.
More research is needed to tease out any relationship between prior COVID-19 infection and liver inflammation, Dr. Balistreri said.
“I’m not sure what to make of any of it yet. We know that SARS-CoV-2 can alter immune responses ... so it wouldn’t surprise me,” if COVID-19 and these hepatitis cases were linked, he said. “It’s just that we need more information.”
A version of this article first appeared on WebMD.com.
There may be a link between the recent unexplained cases of hepatitis in children and prior coronavirus infections, according to new research from Israel.
The study involves five children in Israel who had mild cases of COVID-19 who went on to develop hepatitis; two of these children required liver transplants. But clinicians are cautious about drawing conclusions from such a small study.
“All you can say is that these five cases seem to have proximity to COVID-19, and COVID-19 may be able to cause pediatric liver complications,” said Nancy Reau, MD, section chief of hepatology at Rush University in Chicago. She was not involved with the study.
While COVID-19 could be one explanation for these hepatitis cases, it is also possible that the two are unrelated, said William Balistreri, MD, director emeritus of the Pediatric Liver Care Center at Cincinnati Children’s Hospital Medical Center. He also is unaffiliated with the study.
Hepatitis is rare in children, and between 30% and 50% of these pediatric cases have no known cause, according to the CDC.
Since April 2022, children with hepatitis of an unexplained cause have garnered global attention. The United Kingdom now has 240 confirmed cases, the United States is investigating 290 cases, and Israel has reported 12 cases to the World Health Organization. Many investigators think that these liver problems could be related to adenovirus – a common infection in children that normally causes cold or flu-like symptoms – because more than half of global cases tested for the virus have been positive, according to the WHO. About 12% of children with unexplained hepatitis have tested positive for SARS-CoV-2, the virus that causes COVID-19, but investigators are considering the possibility that some cases may be related to prior infections.
The study documents five patients, 3-months to 13 years old, with prior coronavirus infection who later developed hepatitis. All were treated at Schneider Children’s Medical Hospital in Petah Tikva, Israel, during 2021. The paper was published in the Journal of Pediatric Gastroenterology and Nutrition. Two patients, a 3-month-old and 5-month-old, needed liver transplants. The other three patients (two 8-year-olds and a 13-year-old) were treated with steroids. None of the five children had received any vaccinations against COVID-19. The time between COVID-19 infection and liver problems ranged from 21 to 130 days.
“It took time to be convinced that this could be COVID-related,” said senior study author Orith Waisbourd-Zinman, MD, director of pediatric liver disease service at Schneider Children’s Medical Hospital. “It’s something that wasn’t described.”
Sudden-onset hepatitis after COVID-19 has been recorded in adults, and the virus has been associated with multisystem inflammatory syndrome in children (MIS-C). The condition causes inflammation through the body, including the heart, lungs, and kidneys.
“We know that COVID can be mischievous, and children are no more exempt from that than adults,” Dr. Reau said.
Liver samples taken from these five patients did not test positive for COVID-19, similar to how liver samples have tested negative for adenovirus in more recent hepatitis cases around the world. Dr. Waisbourd-Zinman suggested that in these patients, hepatitis may have been brought on by an inflammatory response that was triggered by the virus.
Still, there are notable differences between these five cases and current cases internationally. These five children became sick during the period of December 2020 to September 2021, whereas all current counted cases in the United Kingdom occurred after January 2022. The first cases in the United States took place in October 2021. It could be that there were similar hepatitis cases before that were not identified, Dr. Reau said.
The ages of the Israeli children with hepatitis also differ from the cases seen globally. More than three-fourths of these reported hepatitis cases occurred in children under 5, the WHO reports, though affected individuals have been as young as 1-month-old up to 16 years old. In the United Kingdom, which accounts for about a third of cases reported to the WHO, most children with unexplained hepatitis have been between 3 and 5 years old.
More research is needed to tease out any relationship between prior COVID-19 infection and liver inflammation, Dr. Balistreri said.
“I’m not sure what to make of any of it yet. We know that SARS-CoV-2 can alter immune responses ... so it wouldn’t surprise me,” if COVID-19 and these hepatitis cases were linked, he said. “It’s just that we need more information.”
A version of this article first appeared on WebMD.com.
There may be a link between the recent unexplained cases of hepatitis in children and prior coronavirus infections, according to new research from Israel.
The study involves five children in Israel who had mild cases of COVID-19 who went on to develop hepatitis; two of these children required liver transplants. But clinicians are cautious about drawing conclusions from such a small study.
“All you can say is that these five cases seem to have proximity to COVID-19, and COVID-19 may be able to cause pediatric liver complications,” said Nancy Reau, MD, section chief of hepatology at Rush University in Chicago. She was not involved with the study.
While COVID-19 could be one explanation for these hepatitis cases, it is also possible that the two are unrelated, said William Balistreri, MD, director emeritus of the Pediatric Liver Care Center at Cincinnati Children’s Hospital Medical Center. He also is unaffiliated with the study.
Hepatitis is rare in children, and between 30% and 50% of these pediatric cases have no known cause, according to the CDC.
Since April 2022, children with hepatitis of an unexplained cause have garnered global attention. The United Kingdom now has 240 confirmed cases, the United States is investigating 290 cases, and Israel has reported 12 cases to the World Health Organization. Many investigators think that these liver problems could be related to adenovirus – a common infection in children that normally causes cold or flu-like symptoms – because more than half of global cases tested for the virus have been positive, according to the WHO. About 12% of children with unexplained hepatitis have tested positive for SARS-CoV-2, the virus that causes COVID-19, but investigators are considering the possibility that some cases may be related to prior infections.
The study documents five patients, 3-months to 13 years old, with prior coronavirus infection who later developed hepatitis. All were treated at Schneider Children’s Medical Hospital in Petah Tikva, Israel, during 2021. The paper was published in the Journal of Pediatric Gastroenterology and Nutrition. Two patients, a 3-month-old and 5-month-old, needed liver transplants. The other three patients (two 8-year-olds and a 13-year-old) were treated with steroids. None of the five children had received any vaccinations against COVID-19. The time between COVID-19 infection and liver problems ranged from 21 to 130 days.
“It took time to be convinced that this could be COVID-related,” said senior study author Orith Waisbourd-Zinman, MD, director of pediatric liver disease service at Schneider Children’s Medical Hospital. “It’s something that wasn’t described.”
Sudden-onset hepatitis after COVID-19 has been recorded in adults, and the virus has been associated with multisystem inflammatory syndrome in children (MIS-C). The condition causes inflammation through the body, including the heart, lungs, and kidneys.
“We know that COVID can be mischievous, and children are no more exempt from that than adults,” Dr. Reau said.
Liver samples taken from these five patients did not test positive for COVID-19, similar to how liver samples have tested negative for adenovirus in more recent hepatitis cases around the world. Dr. Waisbourd-Zinman suggested that in these patients, hepatitis may have been brought on by an inflammatory response that was triggered by the virus.
Still, there are notable differences between these five cases and current cases internationally. These five children became sick during the period of December 2020 to September 2021, whereas all current counted cases in the United Kingdom occurred after January 2022. The first cases in the United States took place in October 2021. It could be that there were similar hepatitis cases before that were not identified, Dr. Reau said.
The ages of the Israeli children with hepatitis also differ from the cases seen globally. More than three-fourths of these reported hepatitis cases occurred in children under 5, the WHO reports, though affected individuals have been as young as 1-month-old up to 16 years old. In the United Kingdom, which accounts for about a third of cases reported to the WHO, most children with unexplained hepatitis have been between 3 and 5 years old.
More research is needed to tease out any relationship between prior COVID-19 infection and liver inflammation, Dr. Balistreri said.
“I’m not sure what to make of any of it yet. We know that SARS-CoV-2 can alter immune responses ... so it wouldn’t surprise me,” if COVID-19 and these hepatitis cases were linked, he said. “It’s just that we need more information.”
A version of this article first appeared on WebMD.com.