User login
App for MS aims to capture elusive signals of progression

At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
FROM MSVirtual2020
Satralizumab reduces risk of severe NMOSD relapse
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.

NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
FROM MSVirtual2020
Cardiovascular risk factors linked to brain atrophy in MS
The presence of cardiovascular risk factors in patients with multiple sclerosis (MS) is associated with a greater degree of brain atrophy even in young patients who are unlikely to have small vessel disease, a new study has shown.
The results were presented by Raffaello Bonacchi, MD, Vita-Salute San Raffaele University, Milan, Italy, at at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020. .
“Our results suggest that even low levels of exposure to cardiovascular risk factors are important in MS and might affect brain atrophy—and therefore long-term disability—even in young patients,” Dr. Bonacchi said.
“It is not only smoking,” he added. “Other cardiovascular risk factors also appear to be implicated. We found a synergistic effect of the different risk factors.”
These are only preliminary data and need to be confirmed in other studies,” he said, “but it does suggest that MS neurologists need to pay attention to comprehensive care—not just MS disease activity.
“They also need to be discussing lifestyle with their patients, evaluating their cardiovascular risk factors, and giving advice on stopping smoking, lowering blood pressure, cholesterol, etc.”
Brain changes
Dr. Bonacchi explained that previous studies have suggested a relationship between cardiovascular risk factors and changes on magnetic resonance imaging (MRI) and clinical outcomes in patients with MS that may be mediated by small vessel disease and/or inflammation.
“Small vessel disease is widespread in the population over 50 years of age, but in this study we wanted to look at the impact of cardiovascular risk factors in younger patients with MS who are not likely to have much small vessel disease to try and see whether there is still a relationship with brain atrophy or white/gray matter lesions,” he said.
Previous studies have not set an age limit for examining this relationship and they have also assessed the presence versus absence of cardiovascular risk factors, without attempting to grade the strength of exposure, he noted.
For the current study, the researchers examined several cardiovascular risk factors and in addition to just being present or absent. They also graded each risk factor as being stringent or not depending on a certain threshold.
For example, smoking was defined as a threshold of 5 pack-years (smoking 5 cigarettes a day for 20 years or 20 cigarettes a day for 5 years). And the more stringent definition was 10 pack-years.
For hypertension, the stringent definition was consistently high blood pressure levels and use of antihypertensive medication, with similar definitions used for cholesterol and diabetes.
This was a cross-sectional observational study in 124 patients with MS and 95 healthy controls. The researchers examined MRI scans and neurological exams and investigated whether the amount of cardiovascular risk factors a patient was exposed to was associated with degree of brain atrophy and white matter/gray matter volume. Results were adjusted for age, sex, disease duration, phenotype (relapsing-remitting versus progressive MS) and treatment.
Results showed no significant difference if patients were exposed to at least one classical risk factor versus no risk factors. But if a patient had at least two classical risk factors, significant differences were found in gray matter, white matter, and total brain volume.
Patients with MS and no risk factors had a mean brain volume of 1524 mL versus 1481 mL in those with at least two risk factors, a difference that was significant (P = 0.003). Mean gray matter volume was 856 mL in MS patients without cardiovascular risk factors and 836 mL in those with at least two risk factors (P = 0.01) Mean white matter volume was 668 mL in MS patients without cardiovascular risk factors and 845 mL in those with at least two risk factors (P = 0.03).
“This is one of the first studies to have graded degrees of risk factors and we found one stringent risk factor was associated with the same effects on brain atrophy as two less stringent risk factors,” Dr. Bonacchi reported.
Healthy controls showed no differences in any of the brain volume outcomes in those with or without cardiovascular risk factors.
“As our population was under aged 50 years, who are unlikely to have much small vessel disease, our results suggest that the influence of cardiovascular risk factors on brain atrophy in MS is not just mediated through small vessel disease and is probably also mediated by increased inflammation,” Dr. Bonacchi suggested.
Impact of CV risk factors
Commenting on the study, Dalia Rotstein, MD, assistant professor, department of neurology, University of Toronto, Ontario, Canada, session cochair, said: “This is an interesting study that captures the impact of cardiovascular risk factors on various measures of brain atrophy in MS.”
The cohort was quite young, under age 50, and the effect on brain atrophy was increased with more severe cardiovascular risk factors, she noted.
“The investigators compared these effects to a population of healthy controls and did not observe as substantial an effect in controls. However, they were likely underpowered for the analysis in the healthy controls because of a relatively small number of subjects with cardiovascular risk factors in this group,” Dr. Rotstein noted.
“More research is needed to determine whether the observed relationship is unique to MS and whether treating cardiovascular risk factors may help protect against neurodegeneration in MS,” she added.
Dr. Bonacchi has reported no relevant financial relationships. Dr. Rotstein has reported acting as a consultant for Roche, Alexion, Novartis, EMD Serono, and Sanofi Aventis.
SOURCE: Bonacchi R. et al. MSVirtual2020. Session PS04.05.
This article originally appeared on Medscape.com .
The presence of cardiovascular risk factors in patients with multiple sclerosis (MS) is associated with a greater degree of brain atrophy even in young patients who are unlikely to have small vessel disease, a new study has shown.
The results were presented by Raffaello Bonacchi, MD, Vita-Salute San Raffaele University, Milan, Italy, at at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020. .
“Our results suggest that even low levels of exposure to cardiovascular risk factors are important in MS and might affect brain atrophy—and therefore long-term disability—even in young patients,” Dr. Bonacchi said.
“It is not only smoking,” he added. “Other cardiovascular risk factors also appear to be implicated. We found a synergistic effect of the different risk factors.”
These are only preliminary data and need to be confirmed in other studies,” he said, “but it does suggest that MS neurologists need to pay attention to comprehensive care—not just MS disease activity.
“They also need to be discussing lifestyle with their patients, evaluating their cardiovascular risk factors, and giving advice on stopping smoking, lowering blood pressure, cholesterol, etc.”
Brain changes
Dr. Bonacchi explained that previous studies have suggested a relationship between cardiovascular risk factors and changes on magnetic resonance imaging (MRI) and clinical outcomes in patients with MS that may be mediated by small vessel disease and/or inflammation.
“Small vessel disease is widespread in the population over 50 years of age, but in this study we wanted to look at the impact of cardiovascular risk factors in younger patients with MS who are not likely to have much small vessel disease to try and see whether there is still a relationship with brain atrophy or white/gray matter lesions,” he said.
Previous studies have not set an age limit for examining this relationship and they have also assessed the presence versus absence of cardiovascular risk factors, without attempting to grade the strength of exposure, he noted.
For the current study, the researchers examined several cardiovascular risk factors and in addition to just being present or absent. They also graded each risk factor as being stringent or not depending on a certain threshold.
For example, smoking was defined as a threshold of 5 pack-years (smoking 5 cigarettes a day for 20 years or 20 cigarettes a day for 5 years). And the more stringent definition was 10 pack-years.
For hypertension, the stringent definition was consistently high blood pressure levels and use of antihypertensive medication, with similar definitions used for cholesterol and diabetes.
This was a cross-sectional observational study in 124 patients with MS and 95 healthy controls. The researchers examined MRI scans and neurological exams and investigated whether the amount of cardiovascular risk factors a patient was exposed to was associated with degree of brain atrophy and white matter/gray matter volume. Results were adjusted for age, sex, disease duration, phenotype (relapsing-remitting versus progressive MS) and treatment.
Results showed no significant difference if patients were exposed to at least one classical risk factor versus no risk factors. But if a patient had at least two classical risk factors, significant differences were found in gray matter, white matter, and total brain volume.
Patients with MS and no risk factors had a mean brain volume of 1524 mL versus 1481 mL in those with at least two risk factors, a difference that was significant (P = 0.003). Mean gray matter volume was 856 mL in MS patients without cardiovascular risk factors and 836 mL in those with at least two risk factors (P = 0.01) Mean white matter volume was 668 mL in MS patients without cardiovascular risk factors and 845 mL in those with at least two risk factors (P = 0.03).
“This is one of the first studies to have graded degrees of risk factors and we found one stringent risk factor was associated with the same effects on brain atrophy as two less stringent risk factors,” Dr. Bonacchi reported.
Healthy controls showed no differences in any of the brain volume outcomes in those with or without cardiovascular risk factors.
“As our population was under aged 50 years, who are unlikely to have much small vessel disease, our results suggest that the influence of cardiovascular risk factors on brain atrophy in MS is not just mediated through small vessel disease and is probably also mediated by increased inflammation,” Dr. Bonacchi suggested.
Impact of CV risk factors
Commenting on the study, Dalia Rotstein, MD, assistant professor, department of neurology, University of Toronto, Ontario, Canada, session cochair, said: “This is an interesting study that captures the impact of cardiovascular risk factors on various measures of brain atrophy in MS.”
The cohort was quite young, under age 50, and the effect on brain atrophy was increased with more severe cardiovascular risk factors, she noted.
“The investigators compared these effects to a population of healthy controls and did not observe as substantial an effect in controls. However, they were likely underpowered for the analysis in the healthy controls because of a relatively small number of subjects with cardiovascular risk factors in this group,” Dr. Rotstein noted.
“More research is needed to determine whether the observed relationship is unique to MS and whether treating cardiovascular risk factors may help protect against neurodegeneration in MS,” she added.
Dr. Bonacchi has reported no relevant financial relationships. Dr. Rotstein has reported acting as a consultant for Roche, Alexion, Novartis, EMD Serono, and Sanofi Aventis.
SOURCE: Bonacchi R. et al. MSVirtual2020. Session PS04.05.
This article originally appeared on Medscape.com .
The presence of cardiovascular risk factors in patients with multiple sclerosis (MS) is associated with a greater degree of brain atrophy even in young patients who are unlikely to have small vessel disease, a new study has shown.
The results were presented by Raffaello Bonacchi, MD, Vita-Salute San Raffaele University, Milan, Italy, at at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020. .
“Our results suggest that even low levels of exposure to cardiovascular risk factors are important in MS and might affect brain atrophy—and therefore long-term disability—even in young patients,” Dr. Bonacchi said.
“It is not only smoking,” he added. “Other cardiovascular risk factors also appear to be implicated. We found a synergistic effect of the different risk factors.”
These are only preliminary data and need to be confirmed in other studies,” he said, “but it does suggest that MS neurologists need to pay attention to comprehensive care—not just MS disease activity.
“They also need to be discussing lifestyle with their patients, evaluating their cardiovascular risk factors, and giving advice on stopping smoking, lowering blood pressure, cholesterol, etc.”
Brain changes
Dr. Bonacchi explained that previous studies have suggested a relationship between cardiovascular risk factors and changes on magnetic resonance imaging (MRI) and clinical outcomes in patients with MS that may be mediated by small vessel disease and/or inflammation.
“Small vessel disease is widespread in the population over 50 years of age, but in this study we wanted to look at the impact of cardiovascular risk factors in younger patients with MS who are not likely to have much small vessel disease to try and see whether there is still a relationship with brain atrophy or white/gray matter lesions,” he said.
Previous studies have not set an age limit for examining this relationship and they have also assessed the presence versus absence of cardiovascular risk factors, without attempting to grade the strength of exposure, he noted.
For the current study, the researchers examined several cardiovascular risk factors and in addition to just being present or absent. They also graded each risk factor as being stringent or not depending on a certain threshold.
For example, smoking was defined as a threshold of 5 pack-years (smoking 5 cigarettes a day for 20 years or 20 cigarettes a day for 5 years). And the more stringent definition was 10 pack-years.
For hypertension, the stringent definition was consistently high blood pressure levels and use of antihypertensive medication, with similar definitions used for cholesterol and diabetes.
This was a cross-sectional observational study in 124 patients with MS and 95 healthy controls. The researchers examined MRI scans and neurological exams and investigated whether the amount of cardiovascular risk factors a patient was exposed to was associated with degree of brain atrophy and white matter/gray matter volume. Results were adjusted for age, sex, disease duration, phenotype (relapsing-remitting versus progressive MS) and treatment.
Results showed no significant difference if patients were exposed to at least one classical risk factor versus no risk factors. But if a patient had at least two classical risk factors, significant differences were found in gray matter, white matter, and total brain volume.
Patients with MS and no risk factors had a mean brain volume of 1524 mL versus 1481 mL in those with at least two risk factors, a difference that was significant (P = 0.003). Mean gray matter volume was 856 mL in MS patients without cardiovascular risk factors and 836 mL in those with at least two risk factors (P = 0.01) Mean white matter volume was 668 mL in MS patients without cardiovascular risk factors and 845 mL in those with at least two risk factors (P = 0.03).
“This is one of the first studies to have graded degrees of risk factors and we found one stringent risk factor was associated with the same effects on brain atrophy as two less stringent risk factors,” Dr. Bonacchi reported.
Healthy controls showed no differences in any of the brain volume outcomes in those with or without cardiovascular risk factors.
“As our population was under aged 50 years, who are unlikely to have much small vessel disease, our results suggest that the influence of cardiovascular risk factors on brain atrophy in MS is not just mediated through small vessel disease and is probably also mediated by increased inflammation,” Dr. Bonacchi suggested.
Impact of CV risk factors
Commenting on the study, Dalia Rotstein, MD, assistant professor, department of neurology, University of Toronto, Ontario, Canada, session cochair, said: “This is an interesting study that captures the impact of cardiovascular risk factors on various measures of brain atrophy in MS.”
The cohort was quite young, under age 50, and the effect on brain atrophy was increased with more severe cardiovascular risk factors, she noted.
“The investigators compared these effects to a population of healthy controls and did not observe as substantial an effect in controls. However, they were likely underpowered for the analysis in the healthy controls because of a relatively small number of subjects with cardiovascular risk factors in this group,” Dr. Rotstein noted.
“More research is needed to determine whether the observed relationship is unique to MS and whether treating cardiovascular risk factors may help protect against neurodegeneration in MS,” she added.
Dr. Bonacchi has reported no relevant financial relationships. Dr. Rotstein has reported acting as a consultant for Roche, Alexion, Novartis, EMD Serono, and Sanofi Aventis.
SOURCE: Bonacchi R. et al. MSVirtual2020. Session PS04.05.
This article originally appeared on Medscape.com .
FROM MSVirtual2020
Lessons for patients with MS and COVID-19
Two important lessons about managing patients with multiple sclerosis (MS) and COVID-19 have emerged from a hospital clinic in Madrid that managed COVID-infected patients with MS through the peak of the pandemic: Combined polymeric chain reaction and serology testing helped avoid disease reactivation in asymptomatic carriers during the pandemic peak, although after the peak PCR alone proved just as effective; and
Virginia Meca-Lallana, MD, a neurologist and coordinator of the demyelinating diseases unit at the Hospital of the University of the Princess in Madrid, and colleagues presented their findings in two posters at the Joint European Committee for Treatment and Research in Multiple Sclerosis-Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“MS treatments don’t seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors,” Dr. Meca-Lallana said in an interview. “MS treatments prevent the patients’ disability, and it is very important not to stop them if it isn’t necessary.”
The results arose from a multidisciplinary safety protocol involving neurology, microbiology, and preventive medicine that the University of Princess physicians developed to keep MS stable in patients diagnosed with SARS-CoV-2.
The researchers obtained 152 PCR nasopharyngeal swabs and 140 serology tests in 90 patients with MS over 3 months before starting a variety of MS treatments: Natalizumab (96 tests), ocrelizumab (36), rituximab (3), methylprednisolone (7), cladribine (4), and dimethyl fumarate (3). The protocol identified 7 asymptomatic carriers—7.8% of the total population—5 of whom had positive immunoglobulin M and G serology. The study also confirmed 5 patients with positive IgM+IgG serology post-infection, but no COVID-19 reactivations were detected after implementation of the protocol.
“The safety protocol reached its objective of avoiding disease reactivation and clinical activation in asymptomatic carriers,” Dr. Meca-Lallana said.
The second poster she presented reported on the real-world experience with SARS-CoV-2 in the MS unit at her hospital. The observational, prospective study included 41 cases, 38 of which were relapsing-remitting MS and the remainder progressive MS. The patients had MS for an average of 9 years.
“We need more patients to draw more robust conclusions, but in our patients, MS treatments seem safe in this situation,” Dr. Meca-Lallana said. “We did not discontinue treatments, and after our first results, we only delayed treatments in patients with any additional comorbidity or when coming to the hospital was not safe.”
A total of 39 patients were taking disease-modifying therapies (DMTs): 46.3% with oral agents, 39% with monoclonal antibodies, and 10% with injectable agents; 27 patients were previously treated with other DMTs. The median Expanded Disability Status Scale (EDSS) was 2.5, and 11 patients had clinical activity the previous year. Eighteen cases were confirmed by PCR or serology, or both, and 23 were diagnosed clinically.
Among the patients with MS and COVID-19, 17% were admitted to the hospital. Six patients had pneumonia, but none required admission to the intensive care unit, and no deaths occurred. Three patients had other comorbidities. Admitted patients tended to be older and had higher EDSS scores, although the difference was not statistically significant. MS worsened in 7 patients, and 10 patients stopped or paused DMTs because of the infection.
“Multiple sclerosis is a weakening illness,” Dr. Meca-Lallana said. “MS treatments do not seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors.”
The SARS-CoV-2 infection does not seem to result in a more aggressive form of the disease in MS patients, and selective immunosuppression may improve their outcomes, she noted.
“MS treatments avoid the patient’s disability,” the investigator added, “and it is very important not to stop them if it isn’t necessary.”
Dr. Meca-Lallana had no relevant financial disclosures.
Two important lessons about managing patients with multiple sclerosis (MS) and COVID-19 have emerged from a hospital clinic in Madrid that managed COVID-infected patients with MS through the peak of the pandemic: Combined polymeric chain reaction and serology testing helped avoid disease reactivation in asymptomatic carriers during the pandemic peak, although after the peak PCR alone proved just as effective; and
Virginia Meca-Lallana, MD, a neurologist and coordinator of the demyelinating diseases unit at the Hospital of the University of the Princess in Madrid, and colleagues presented their findings in two posters at the Joint European Committee for Treatment and Research in Multiple Sclerosis-Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“MS treatments don’t seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors,” Dr. Meca-Lallana said in an interview. “MS treatments prevent the patients’ disability, and it is very important not to stop them if it isn’t necessary.”
The results arose from a multidisciplinary safety protocol involving neurology, microbiology, and preventive medicine that the University of Princess physicians developed to keep MS stable in patients diagnosed with SARS-CoV-2.
The researchers obtained 152 PCR nasopharyngeal swabs and 140 serology tests in 90 patients with MS over 3 months before starting a variety of MS treatments: Natalizumab (96 tests), ocrelizumab (36), rituximab (3), methylprednisolone (7), cladribine (4), and dimethyl fumarate (3). The protocol identified 7 asymptomatic carriers—7.8% of the total population—5 of whom had positive immunoglobulin M and G serology. The study also confirmed 5 patients with positive IgM+IgG serology post-infection, but no COVID-19 reactivations were detected after implementation of the protocol.
“The safety protocol reached its objective of avoiding disease reactivation and clinical activation in asymptomatic carriers,” Dr. Meca-Lallana said.
The second poster she presented reported on the real-world experience with SARS-CoV-2 in the MS unit at her hospital. The observational, prospective study included 41 cases, 38 of which were relapsing-remitting MS and the remainder progressive MS. The patients had MS for an average of 9 years.
“We need more patients to draw more robust conclusions, but in our patients, MS treatments seem safe in this situation,” Dr. Meca-Lallana said. “We did not discontinue treatments, and after our first results, we only delayed treatments in patients with any additional comorbidity or when coming to the hospital was not safe.”
A total of 39 patients were taking disease-modifying therapies (DMTs): 46.3% with oral agents, 39% with monoclonal antibodies, and 10% with injectable agents; 27 patients were previously treated with other DMTs. The median Expanded Disability Status Scale (EDSS) was 2.5, and 11 patients had clinical activity the previous year. Eighteen cases were confirmed by PCR or serology, or both, and 23 were diagnosed clinically.
Among the patients with MS and COVID-19, 17% were admitted to the hospital. Six patients had pneumonia, but none required admission to the intensive care unit, and no deaths occurred. Three patients had other comorbidities. Admitted patients tended to be older and had higher EDSS scores, although the difference was not statistically significant. MS worsened in 7 patients, and 10 patients stopped or paused DMTs because of the infection.
“Multiple sclerosis is a weakening illness,” Dr. Meca-Lallana said. “MS treatments do not seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors.”
The SARS-CoV-2 infection does not seem to result in a more aggressive form of the disease in MS patients, and selective immunosuppression may improve their outcomes, she noted.
“MS treatments avoid the patient’s disability,” the investigator added, “and it is very important not to stop them if it isn’t necessary.”
Dr. Meca-Lallana had no relevant financial disclosures.
Two important lessons about managing patients with multiple sclerosis (MS) and COVID-19 have emerged from a hospital clinic in Madrid that managed COVID-infected patients with MS through the peak of the pandemic: Combined polymeric chain reaction and serology testing helped avoid disease reactivation in asymptomatic carriers during the pandemic peak, although after the peak PCR alone proved just as effective; and
Virginia Meca-Lallana, MD, a neurologist and coordinator of the demyelinating diseases unit at the Hospital of the University of the Princess in Madrid, and colleagues presented their findings in two posters at the Joint European Committee for Treatment and Research in Multiple Sclerosis-Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
“MS treatments don’t seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors,” Dr. Meca-Lallana said in an interview. “MS treatments prevent the patients’ disability, and it is very important not to stop them if it isn’t necessary.”
The results arose from a multidisciplinary safety protocol involving neurology, microbiology, and preventive medicine that the University of Princess physicians developed to keep MS stable in patients diagnosed with SARS-CoV-2.
The researchers obtained 152 PCR nasopharyngeal swabs and 140 serology tests in 90 patients with MS over 3 months before starting a variety of MS treatments: Natalizumab (96 tests), ocrelizumab (36), rituximab (3), methylprednisolone (7), cladribine (4), and dimethyl fumarate (3). The protocol identified 7 asymptomatic carriers—7.8% of the total population—5 of whom had positive immunoglobulin M and G serology. The study also confirmed 5 patients with positive IgM+IgG serology post-infection, but no COVID-19 reactivations were detected after implementation of the protocol.
“The safety protocol reached its objective of avoiding disease reactivation and clinical activation in asymptomatic carriers,” Dr. Meca-Lallana said.
The second poster she presented reported on the real-world experience with SARS-CoV-2 in the MS unit at her hospital. The observational, prospective study included 41 cases, 38 of which were relapsing-remitting MS and the remainder progressive MS. The patients had MS for an average of 9 years.
“We need more patients to draw more robust conclusions, but in our patients, MS treatments seem safe in this situation,” Dr. Meca-Lallana said. “We did not discontinue treatments, and after our first results, we only delayed treatments in patients with any additional comorbidity or when coming to the hospital was not safe.”
A total of 39 patients were taking disease-modifying therapies (DMTs): 46.3% with oral agents, 39% with monoclonal antibodies, and 10% with injectable agents; 27 patients were previously treated with other DMTs. The median Expanded Disability Status Scale (EDSS) was 2.5, and 11 patients had clinical activity the previous year. Eighteen cases were confirmed by PCR or serology, or both, and 23 were diagnosed clinically.
Among the patients with MS and COVID-19, 17% were admitted to the hospital. Six patients had pneumonia, but none required admission to the intensive care unit, and no deaths occurred. Three patients had other comorbidities. Admitted patients tended to be older and had higher EDSS scores, although the difference was not statistically significant. MS worsened in 7 patients, and 10 patients stopped or paused DMTs because of the infection.
“Multiple sclerosis is a weakening illness,” Dr. Meca-Lallana said. “MS treatments do not seem to make the prognosis of COVID-19 worse, but it is very important to evaluate other risk factors.”
The SARS-CoV-2 infection does not seem to result in a more aggressive form of the disease in MS patients, and selective immunosuppression may improve their outcomes, she noted.
“MS treatments avoid the patient’s disability,” the investigator added, “and it is very important not to stop them if it isn’t necessary.”
Dr. Meca-Lallana had no relevant financial disclosures.
FROM MSVirtual2020
Increasing hepatitis C treatment may curb hepatocellular carcinoma
Widespread treatment of hepatitis C virus significantly reduced the risk of hepatocellular carcinoma, based on 18 years of data from patients in Veterans Health Administration hospitals.
Although eradication of hepatitis C virus (HCV) infections has been shown to reduce the risk of hepatocellular carcinoma (HCC), effective direct-acting antiviral therapies available since 2013 appear underused in the United States, with a 14% cure rate for HCV patients as of 2016, wrote Lauren A. Beste, MD, of Veterans Affairs Puget Sound Health Care System, Seattle, and colleagues.
However, “the Veterans Health Administration, the largest integrated health care system in the U.S., provides unrestricted access to HCV treatments and approximately 85% of its case load has achieved cure,” the researchers said.
In a letter published in JAMA, the researchers identified all patients in the VHA diagnosed with HCC based on electronic health records for each year between 2002 and 2018. HCV infection was based on any history of detectable viral load, and HCV cure was defined as a negative viral load at least 12 weeks following completion of antiviral treatment, the researchers said.
“We categorized patients into 3 groups as of the time of HCC diagnosis: HCC/HCV viremic (latest HCV RNA before HCC diagnosis was positive), HCC/HCV cured (HCV eradicated before HCC diagnosis), and HCC/non-HCV (no positive lifetime HCV RNA),” they explained.
The sum of HCC/HCV viremic plus HCC/HCV cured made up the HCC/HCV total. Overall, the incidence of HCC/HCV total increased from 2000 to 2015, peaked at 31.0 per 100,000 patients in 2015, and decreased to 21.8 per 100,000 in 2018 after the introduction of viral eradication efforts from 2014 to 2016.
HCV treatment shows value despite lack of causality
Although the study could not prove causality, “the timing of HCV eradication and declining HCC incidence, lack of decline in non–HCV-related HCC, and prior studies demonstrating that HCV eradication reduces HCC risk, provide indirect evidence that this decline may be related to widespread HCV treatment,” the researchers said.
The findings were limited by several factors including the observational study design, use of the International Classification of Diseases to define HCC, use of a VA population that might limit generalizability, and lack of data on the severity of disease prior to treatment, the researchers noted. However, “HCC incidence trends should continue to be monitored closely because patients cured of HCV may have yet to experience the full potential of risk reduction,” and the study results support large-scale campaigns to eliminate HCV as well as monitoring for HCC and HCV patients who achieve disease eradication, they concluded.
The study was supported in part by grants from the National Institutes of Health/National Cancer Institute and the Veterans Affairs Clinical Science Research and Development. The researchers had no financial conflicts to disclose.
SOURCE: Beste LA et al. JAMA. 2020 Sep 8;324(10):1003-5.
Widespread treatment of hepatitis C virus significantly reduced the risk of hepatocellular carcinoma, based on 18 years of data from patients in Veterans Health Administration hospitals.
Although eradication of hepatitis C virus (HCV) infections has been shown to reduce the risk of hepatocellular carcinoma (HCC), effective direct-acting antiviral therapies available since 2013 appear underused in the United States, with a 14% cure rate for HCV patients as of 2016, wrote Lauren A. Beste, MD, of Veterans Affairs Puget Sound Health Care System, Seattle, and colleagues.
However, “the Veterans Health Administration, the largest integrated health care system in the U.S., provides unrestricted access to HCV treatments and approximately 85% of its case load has achieved cure,” the researchers said.
In a letter published in JAMA, the researchers identified all patients in the VHA diagnosed with HCC based on electronic health records for each year between 2002 and 2018. HCV infection was based on any history of detectable viral load, and HCV cure was defined as a negative viral load at least 12 weeks following completion of antiviral treatment, the researchers said.
“We categorized patients into 3 groups as of the time of HCC diagnosis: HCC/HCV viremic (latest HCV RNA before HCC diagnosis was positive), HCC/HCV cured (HCV eradicated before HCC diagnosis), and HCC/non-HCV (no positive lifetime HCV RNA),” they explained.
The sum of HCC/HCV viremic plus HCC/HCV cured made up the HCC/HCV total. Overall, the incidence of HCC/HCV total increased from 2000 to 2015, peaked at 31.0 per 100,000 patients in 2015, and decreased to 21.8 per 100,000 in 2018 after the introduction of viral eradication efforts from 2014 to 2016.
HCV treatment shows value despite lack of causality
Although the study could not prove causality, “the timing of HCV eradication and declining HCC incidence, lack of decline in non–HCV-related HCC, and prior studies demonstrating that HCV eradication reduces HCC risk, provide indirect evidence that this decline may be related to widespread HCV treatment,” the researchers said.
The findings were limited by several factors including the observational study design, use of the International Classification of Diseases to define HCC, use of a VA population that might limit generalizability, and lack of data on the severity of disease prior to treatment, the researchers noted. However, “HCC incidence trends should continue to be monitored closely because patients cured of HCV may have yet to experience the full potential of risk reduction,” and the study results support large-scale campaigns to eliminate HCV as well as monitoring for HCC and HCV patients who achieve disease eradication, they concluded.
The study was supported in part by grants from the National Institutes of Health/National Cancer Institute and the Veterans Affairs Clinical Science Research and Development. The researchers had no financial conflicts to disclose.
SOURCE: Beste LA et al. JAMA. 2020 Sep 8;324(10):1003-5.
Widespread treatment of hepatitis C virus significantly reduced the risk of hepatocellular carcinoma, based on 18 years of data from patients in Veterans Health Administration hospitals.
Although eradication of hepatitis C virus (HCV) infections has been shown to reduce the risk of hepatocellular carcinoma (HCC), effective direct-acting antiviral therapies available since 2013 appear underused in the United States, with a 14% cure rate for HCV patients as of 2016, wrote Lauren A. Beste, MD, of Veterans Affairs Puget Sound Health Care System, Seattle, and colleagues.
However, “the Veterans Health Administration, the largest integrated health care system in the U.S., provides unrestricted access to HCV treatments and approximately 85% of its case load has achieved cure,” the researchers said.
In a letter published in JAMA, the researchers identified all patients in the VHA diagnosed with HCC based on electronic health records for each year between 2002 and 2018. HCV infection was based on any history of detectable viral load, and HCV cure was defined as a negative viral load at least 12 weeks following completion of antiviral treatment, the researchers said.
“We categorized patients into 3 groups as of the time of HCC diagnosis: HCC/HCV viremic (latest HCV RNA before HCC diagnosis was positive), HCC/HCV cured (HCV eradicated before HCC diagnosis), and HCC/non-HCV (no positive lifetime HCV RNA),” they explained.
The sum of HCC/HCV viremic plus HCC/HCV cured made up the HCC/HCV total. Overall, the incidence of HCC/HCV total increased from 2000 to 2015, peaked at 31.0 per 100,000 patients in 2015, and decreased to 21.8 per 100,000 in 2018 after the introduction of viral eradication efforts from 2014 to 2016.
HCV treatment shows value despite lack of causality
Although the study could not prove causality, “the timing of HCV eradication and declining HCC incidence, lack of decline in non–HCV-related HCC, and prior studies demonstrating that HCV eradication reduces HCC risk, provide indirect evidence that this decline may be related to widespread HCV treatment,” the researchers said.
The findings were limited by several factors including the observational study design, use of the International Classification of Diseases to define HCC, use of a VA population that might limit generalizability, and lack of data on the severity of disease prior to treatment, the researchers noted. However, “HCC incidence trends should continue to be monitored closely because patients cured of HCV may have yet to experience the full potential of risk reduction,” and the study results support large-scale campaigns to eliminate HCV as well as monitoring for HCC and HCV patients who achieve disease eradication, they concluded.
The study was supported in part by grants from the National Institutes of Health/National Cancer Institute and the Veterans Affairs Clinical Science Research and Development. The researchers had no financial conflicts to disclose.
SOURCE: Beste LA et al. JAMA. 2020 Sep 8;324(10):1003-5.
FROM JAMA
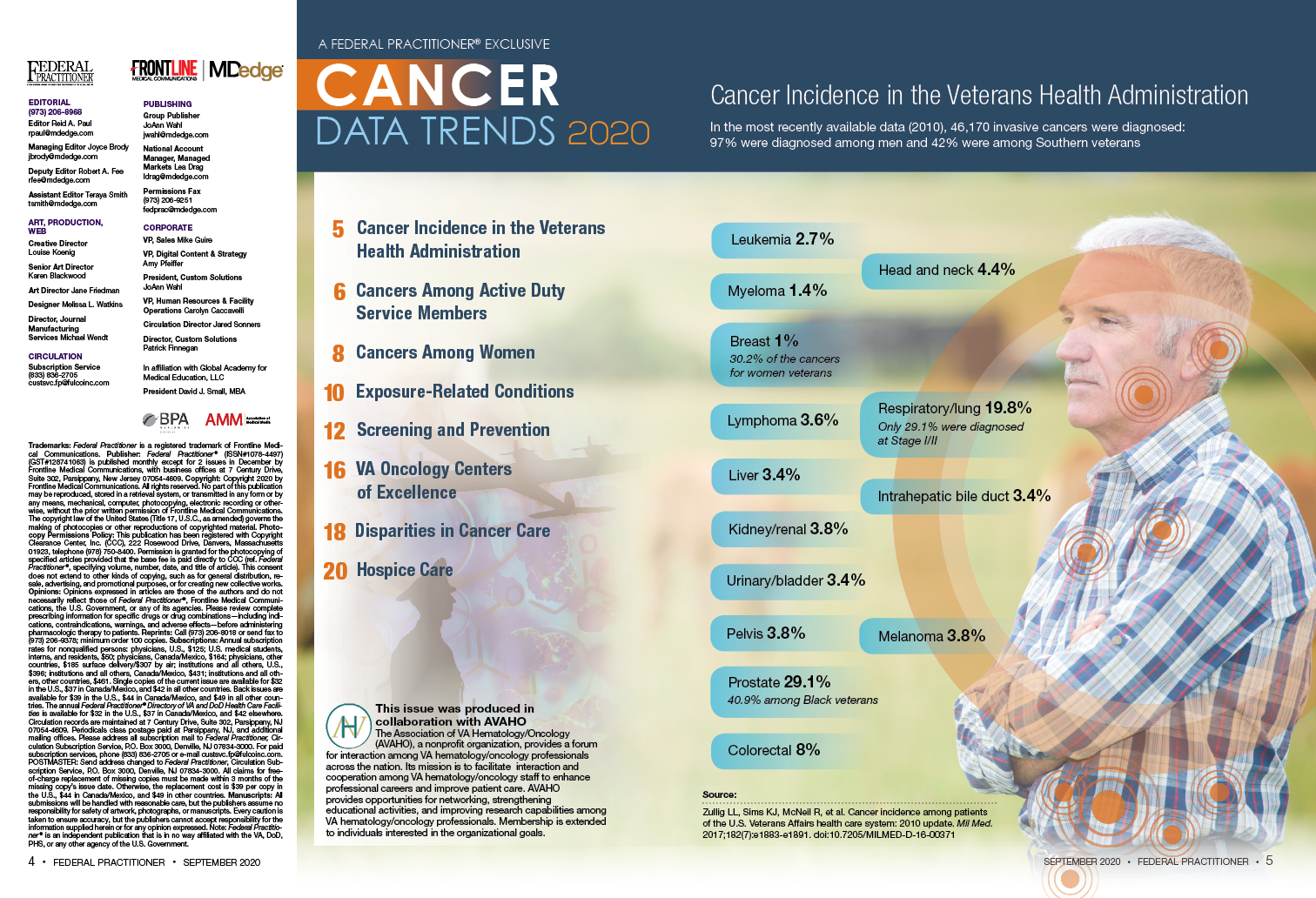
2020 Cancer Data Trends



Exposure to DMT may delay disability accumulation in primary progressive MS
Reducing the delay to treatment initiation, as well as treating younger patients, might improve long-term disability outcomes, according to a new study.
“To optimize treatment decision-making in primary progressive MS, further profiling of the best candidates for treatment is needed,” said the researchers. The study was presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Ocrelizumab remains the only treatment available for patients with primary progressive MS. In clinical trials, other drugs have failed to reduce disability progression in this population. Mattia Fonderico, a doctoral student and research assistant at the University of Florence (Italy), and colleagues reviewed data from the Italian MS Registry to examine whether DMT affects the attainment of given disability outcomes.
Patients with longer exposure were younger at baseline
Patients eligible for inclusion in the study had primary progressive MS, at least three evaluations using the Expanded Disability Status Scale (EDSS), and 3 years’ follow-up. The investigators defined the baseline for untreated patients as the first EDSS evaluation. For treated patients, the baseline was the date of DMT initiation.
Using multivariable Cox regression models, Ms. Fonderico and colleagues examined the effect of DMT on the risk of reaching EDSS scores of 6 (i.e., requirement for intermittent or unilateral constant walking assistance) and 7 (i.e., restriction to a wheelchair) as a dichotomous variable and as a time-dependent covariate. The researchers adjusted the data for age at baseline, sex, first EDSS score, symptoms at onset, annualized visit rate, and annualized relapse rate. They compared outcomes with an as-treated analysis and chose cohorts with similar baseline characteristics using propensity-score matching. In addition, Ms. Fonderico and colleagues also analyzed quartiles of DMT exposure.
The investigators included 1,214 patients (671 women) in their analysis. The population’s mean age at baseline was 48.7 years, and its mean EDSS score was 4.1. A total of 626 patients (52%) received DMT during follow-up. Approximately 57% of DMTs were platform therapies, and 43% were high-efficacy therapies.
Mean follow-up duration was 11.6 years. By the end of follow-up, 994 patients (82%) reached an EDSS score of 6, and 539 (44%) reached an EDSS score of 7. Multivariable Cox regression models indicated that DMT, analyzed as a dichotomous variable, did not affect the risk of reaching EDSS 6 (adjusted hazard ratio, 1.1) or EDSS 7 (aHR, 0.93). Longer DMT exposure, however, significantly reduced the risk of reaching EDSS 7 (aHR, 0.73).
Compared with patients with shorter exposure to DMT, patients in the highest quartile of DMT exposure were younger at baseline (mean age, 44.1 years) and initiated DMT closer to disease onset (mean time to DMT initiation was 6.8 years). The propensity score matching analysis confirmed these findings.
The investigators did not consider MRI variables, which Ms. Fonderico acknowledged was a weakness of the study. In addition, they did not analyze the effect of superimposed relapses.
A new perspective on primary progressive MS?
These results suggest that primary progressive MS behaves like relapsing-remitting MS, said Gavin Giovannoni, MD, PhD, chair of neurology at Queen Mary University of London. That is, they suggest that primary progressive MS “is modifiable by a DMT and that the earlier you treat, the better the outcome.” The results also indicate that neurologists commonly prescribe DMT off label in Italy, he added.
A weakness of the study is that it was not randomized. Furthermore, “EDSS [evaluations] tend not be done properly in routine clinical practice,” said Dr. Giovannoni. Still, the study raises an important question for future research. “Why have we missed the treatment effect in previous trials?” asked Dr. Giovannoni. Whether previous trials were too short or underpowered could be investigated, he added.
Study funding was not reported. Ms. Fonderico had no relevant disclosures. Dr. Giovannoni had no relevant disclosures.
Reducing the delay to treatment initiation, as well as treating younger patients, might improve long-term disability outcomes, according to a new study.
“To optimize treatment decision-making in primary progressive MS, further profiling of the best candidates for treatment is needed,” said the researchers. The study was presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Ocrelizumab remains the only treatment available for patients with primary progressive MS. In clinical trials, other drugs have failed to reduce disability progression in this population. Mattia Fonderico, a doctoral student and research assistant at the University of Florence (Italy), and colleagues reviewed data from the Italian MS Registry to examine whether DMT affects the attainment of given disability outcomes.
Patients with longer exposure were younger at baseline
Patients eligible for inclusion in the study had primary progressive MS, at least three evaluations using the Expanded Disability Status Scale (EDSS), and 3 years’ follow-up. The investigators defined the baseline for untreated patients as the first EDSS evaluation. For treated patients, the baseline was the date of DMT initiation.
Using multivariable Cox regression models, Ms. Fonderico and colleagues examined the effect of DMT on the risk of reaching EDSS scores of 6 (i.e., requirement for intermittent or unilateral constant walking assistance) and 7 (i.e., restriction to a wheelchair) as a dichotomous variable and as a time-dependent covariate. The researchers adjusted the data for age at baseline, sex, first EDSS score, symptoms at onset, annualized visit rate, and annualized relapse rate. They compared outcomes with an as-treated analysis and chose cohorts with similar baseline characteristics using propensity-score matching. In addition, Ms. Fonderico and colleagues also analyzed quartiles of DMT exposure.
The investigators included 1,214 patients (671 women) in their analysis. The population’s mean age at baseline was 48.7 years, and its mean EDSS score was 4.1. A total of 626 patients (52%) received DMT during follow-up. Approximately 57% of DMTs were platform therapies, and 43% were high-efficacy therapies.
Mean follow-up duration was 11.6 years. By the end of follow-up, 994 patients (82%) reached an EDSS score of 6, and 539 (44%) reached an EDSS score of 7. Multivariable Cox regression models indicated that DMT, analyzed as a dichotomous variable, did not affect the risk of reaching EDSS 6 (adjusted hazard ratio, 1.1) or EDSS 7 (aHR, 0.93). Longer DMT exposure, however, significantly reduced the risk of reaching EDSS 7 (aHR, 0.73).
Compared with patients with shorter exposure to DMT, patients in the highest quartile of DMT exposure were younger at baseline (mean age, 44.1 years) and initiated DMT closer to disease onset (mean time to DMT initiation was 6.8 years). The propensity score matching analysis confirmed these findings.
The investigators did not consider MRI variables, which Ms. Fonderico acknowledged was a weakness of the study. In addition, they did not analyze the effect of superimposed relapses.
A new perspective on primary progressive MS?
These results suggest that primary progressive MS behaves like relapsing-remitting MS, said Gavin Giovannoni, MD, PhD, chair of neurology at Queen Mary University of London. That is, they suggest that primary progressive MS “is modifiable by a DMT and that the earlier you treat, the better the outcome.” The results also indicate that neurologists commonly prescribe DMT off label in Italy, he added.
A weakness of the study is that it was not randomized. Furthermore, “EDSS [evaluations] tend not be done properly in routine clinical practice,” said Dr. Giovannoni. Still, the study raises an important question for future research. “Why have we missed the treatment effect in previous trials?” asked Dr. Giovannoni. Whether previous trials were too short or underpowered could be investigated, he added.
Study funding was not reported. Ms. Fonderico had no relevant disclosures. Dr. Giovannoni had no relevant disclosures.
Reducing the delay to treatment initiation, as well as treating younger patients, might improve long-term disability outcomes, according to a new study.
“To optimize treatment decision-making in primary progressive MS, further profiling of the best candidates for treatment is needed,” said the researchers. The study was presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Ocrelizumab remains the only treatment available for patients with primary progressive MS. In clinical trials, other drugs have failed to reduce disability progression in this population. Mattia Fonderico, a doctoral student and research assistant at the University of Florence (Italy), and colleagues reviewed data from the Italian MS Registry to examine whether DMT affects the attainment of given disability outcomes.
Patients with longer exposure were younger at baseline
Patients eligible for inclusion in the study had primary progressive MS, at least three evaluations using the Expanded Disability Status Scale (EDSS), and 3 years’ follow-up. The investigators defined the baseline for untreated patients as the first EDSS evaluation. For treated patients, the baseline was the date of DMT initiation.
Using multivariable Cox regression models, Ms. Fonderico and colleagues examined the effect of DMT on the risk of reaching EDSS scores of 6 (i.e., requirement for intermittent or unilateral constant walking assistance) and 7 (i.e., restriction to a wheelchair) as a dichotomous variable and as a time-dependent covariate. The researchers adjusted the data for age at baseline, sex, first EDSS score, symptoms at onset, annualized visit rate, and annualized relapse rate. They compared outcomes with an as-treated analysis and chose cohorts with similar baseline characteristics using propensity-score matching. In addition, Ms. Fonderico and colleagues also analyzed quartiles of DMT exposure.
The investigators included 1,214 patients (671 women) in their analysis. The population’s mean age at baseline was 48.7 years, and its mean EDSS score was 4.1. A total of 626 patients (52%) received DMT during follow-up. Approximately 57% of DMTs were platform therapies, and 43% were high-efficacy therapies.
Mean follow-up duration was 11.6 years. By the end of follow-up, 994 patients (82%) reached an EDSS score of 6, and 539 (44%) reached an EDSS score of 7. Multivariable Cox regression models indicated that DMT, analyzed as a dichotomous variable, did not affect the risk of reaching EDSS 6 (adjusted hazard ratio, 1.1) or EDSS 7 (aHR, 0.93). Longer DMT exposure, however, significantly reduced the risk of reaching EDSS 7 (aHR, 0.73).
Compared with patients with shorter exposure to DMT, patients in the highest quartile of DMT exposure were younger at baseline (mean age, 44.1 years) and initiated DMT closer to disease onset (mean time to DMT initiation was 6.8 years). The propensity score matching analysis confirmed these findings.
The investigators did not consider MRI variables, which Ms. Fonderico acknowledged was a weakness of the study. In addition, they did not analyze the effect of superimposed relapses.
A new perspective on primary progressive MS?
These results suggest that primary progressive MS behaves like relapsing-remitting MS, said Gavin Giovannoni, MD, PhD, chair of neurology at Queen Mary University of London. That is, they suggest that primary progressive MS “is modifiable by a DMT and that the earlier you treat, the better the outcome.” The results also indicate that neurologists commonly prescribe DMT off label in Italy, he added.
A weakness of the study is that it was not randomized. Furthermore, “EDSS [evaluations] tend not be done properly in routine clinical practice,” said Dr. Giovannoni. Still, the study raises an important question for future research. “Why have we missed the treatment effect in previous trials?” asked Dr. Giovannoni. Whether previous trials were too short or underpowered could be investigated, he added.
Study funding was not reported. Ms. Fonderico had no relevant disclosures. Dr. Giovannoni had no relevant disclosures.
FROM MSVirtual 2020
Disparities seen in COVID-19–related avoidance of care
In the early weeks and months of the COVID-19 pandemic, many people were trying to avoid the coronavirus by staying away from emergency rooms and medical offices. But how many people is “many”?
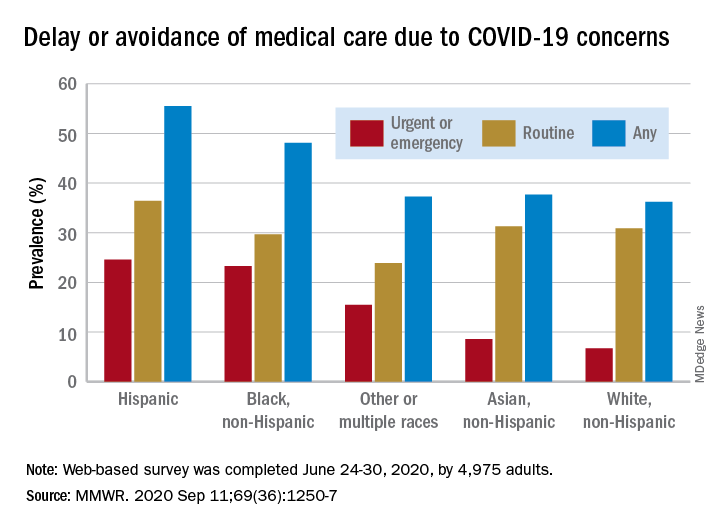
Turns out almost 41% of Americans delayed or avoided some form of medical care because of concerns about COVID-19, according to the results of a survey conducted June 24-30 by commercial survey company Qualtrics.
More specifically, the avoidance looks like this: 31.5% of the 4,975 adult respondents had avoided routine care and 12.0% had avoided urgent or emergency care, Mark E. Czeisler and associates said in the Morbidity and Mortality Weekly Report. The two categories were not mutually exclusive since respondents could select both routine care and urgent/emergency care.
There were, however, a number of significant disparities hidden among those numbers for the overall population. Blacks and Hispanics, with respective prevalences of 23.3% and 24.6%, were significantly more likely to delay or avoid urgent/emergency care than were Whites (6.7%), said Mr. Czeisler, a graduate student at Monash University, Melbourne, and associates.
Those differences “are especially concerning given increased COVID-19–associated mortality among Black adults and Hispanic adults,” they noted, adding that “age-adjusted COVID-19 hospitalization rates are approximately five times higher among Black persons and four times higher among Hispanic persons than” among Whites.
Other significant disparities in urgent/emergency care avoidance included the following:
- Unpaid caregivers for adults (29.8%) vs. noncaregivers (5.4%).
- Adults with two or more underlying conditions (22.7%) vs. those without such conditions (8.2%).
- Those with a disability (22.8%) vs. those without (8.9%).
- Those with health insurance (12.4%) vs. those without (7.8%).
The highest prevalence for all types of COVID-19–related delay and avoidance came from the adult caregivers (64.3%), followed by those with a disability (60.3%) and adults aged 18-24 years (57.2%). The lowest prevalence numbers were for adults with health insurance (24.8%) and those who were not caregivers for adults (32.2%), Mr. Czeisler and associates reported.
These reports of delayed and avoided care “might reflect adherence to community mitigation efforts such as stay-at-home orders, temporary closures of health facilities, or additional factors. However, if routine care avoidance were to be sustained, adults could miss opportunities for management of chronic conditions, receipt of routine vaccinations, or early detection of new conditions, which might worsen outcomes,” they wrote.
SOURCE: Czeisler ME et al. MMWR. 2020 Sep 11;69(36):1250-7.
In the early weeks and months of the COVID-19 pandemic, many people were trying to avoid the coronavirus by staying away from emergency rooms and medical offices. But how many people is “many”?
Turns out almost 41% of Americans delayed or avoided some form of medical care because of concerns about COVID-19, according to the results of a survey conducted June 24-30 by commercial survey company Qualtrics.
More specifically, the avoidance looks like this: 31.5% of the 4,975 adult respondents had avoided routine care and 12.0% had avoided urgent or emergency care, Mark E. Czeisler and associates said in the Morbidity and Mortality Weekly Report. The two categories were not mutually exclusive since respondents could select both routine care and urgent/emergency care.
There were, however, a number of significant disparities hidden among those numbers for the overall population. Blacks and Hispanics, with respective prevalences of 23.3% and 24.6%, were significantly more likely to delay or avoid urgent/emergency care than were Whites (6.7%), said Mr. Czeisler, a graduate student at Monash University, Melbourne, and associates.
Those differences “are especially concerning given increased COVID-19–associated mortality among Black adults and Hispanic adults,” they noted, adding that “age-adjusted COVID-19 hospitalization rates are approximately five times higher among Black persons and four times higher among Hispanic persons than” among Whites.
Other significant disparities in urgent/emergency care avoidance included the following:
- Unpaid caregivers for adults (29.8%) vs. noncaregivers (5.4%).
- Adults with two or more underlying conditions (22.7%) vs. those without such conditions (8.2%).
- Those with a disability (22.8%) vs. those without (8.9%).
- Those with health insurance (12.4%) vs. those without (7.8%).
The highest prevalence for all types of COVID-19–related delay and avoidance came from the adult caregivers (64.3%), followed by those with a disability (60.3%) and adults aged 18-24 years (57.2%). The lowest prevalence numbers were for adults with health insurance (24.8%) and those who were not caregivers for adults (32.2%), Mr. Czeisler and associates reported.
These reports of delayed and avoided care “might reflect adherence to community mitigation efforts such as stay-at-home orders, temporary closures of health facilities, or additional factors. However, if routine care avoidance were to be sustained, adults could miss opportunities for management of chronic conditions, receipt of routine vaccinations, or early detection of new conditions, which might worsen outcomes,” they wrote.
SOURCE: Czeisler ME et al. MMWR. 2020 Sep 11;69(36):1250-7.
In the early weeks and months of the COVID-19 pandemic, many people were trying to avoid the coronavirus by staying away from emergency rooms and medical offices. But how many people is “many”?
Turns out almost 41% of Americans delayed or avoided some form of medical care because of concerns about COVID-19, according to the results of a survey conducted June 24-30 by commercial survey company Qualtrics.
More specifically, the avoidance looks like this: 31.5% of the 4,975 adult respondents had avoided routine care and 12.0% had avoided urgent or emergency care, Mark E. Czeisler and associates said in the Morbidity and Mortality Weekly Report. The two categories were not mutually exclusive since respondents could select both routine care and urgent/emergency care.
There were, however, a number of significant disparities hidden among those numbers for the overall population. Blacks and Hispanics, with respective prevalences of 23.3% and 24.6%, were significantly more likely to delay or avoid urgent/emergency care than were Whites (6.7%), said Mr. Czeisler, a graduate student at Monash University, Melbourne, and associates.
Those differences “are especially concerning given increased COVID-19–associated mortality among Black adults and Hispanic adults,” they noted, adding that “age-adjusted COVID-19 hospitalization rates are approximately five times higher among Black persons and four times higher among Hispanic persons than” among Whites.
Other significant disparities in urgent/emergency care avoidance included the following:
- Unpaid caregivers for adults (29.8%) vs. noncaregivers (5.4%).
- Adults with two or more underlying conditions (22.7%) vs. those without such conditions (8.2%).
- Those with a disability (22.8%) vs. those without (8.9%).
- Those with health insurance (12.4%) vs. those without (7.8%).
The highest prevalence for all types of COVID-19–related delay and avoidance came from the adult caregivers (64.3%), followed by those with a disability (60.3%) and adults aged 18-24 years (57.2%). The lowest prevalence numbers were for adults with health insurance (24.8%) and those who were not caregivers for adults (32.2%), Mr. Czeisler and associates reported.
These reports of delayed and avoided care “might reflect adherence to community mitigation efforts such as stay-at-home orders, temporary closures of health facilities, or additional factors. However, if routine care avoidance were to be sustained, adults could miss opportunities for management of chronic conditions, receipt of routine vaccinations, or early detection of new conditions, which might worsen outcomes,” they wrote.
SOURCE: Czeisler ME et al. MMWR. 2020 Sep 11;69(36):1250-7.
New billing code for added COVID practice expense
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.
In MS, serious adverse effects are more common in rituximab versus ocrelizumab
, a new postmarketing analysis finds, and AE-related deaths were not unusual. Serious AEs, and those linked to death, were more common in the rituximab group, although the reported infection rate was higher in the ocrelizumab group.
The analysis, published Aug. 21 in the Multiple Sclerosis Journal, highlights the importance of monitoring patients for infections and encouraging them to do the same, the authors said.
“This report points out the impact of treatments in terms of unrecognized or underappreciated complications,” said Mark Gudesblatt, MD, medical director of the Comprehensive MS Care Center at South Shore Neurologic Associates in Patchogue, N.Y., who reviewed the study findings. “These medications have a significant downside.”
Lead author Natalia Gonzalez Caldito, MD, of the University of Texas Southwestern Medical Center, Dallas, and colleagues analyzed AEs for the drugs in the Food and Drug Administration’s Adverse Event Reporting System. They only included cases in which the drugs were solely used to treat MS and were indicated as the cause of the AEs.
Rituximab (Rituxan) and ocrelizumab (Ocrevus) are both monoclonal antibodies. Rituximab is not FDA approved for MS but is used off label; ocrelizumab is approved for the relapsing forms of MS and primary progressive MS.
The researchers found 623 AE reports and 1,466 total AEs for rituximab and 7,948 and 23,613, respectively, for ocrelizumab. The average ages for the groups were 48.76 versus 43.89, respectively, (P < .001), and 71% in each group were women.
Among total AEs, serious AEs were more common in the rituximab group versus the ocrelizumab group (64.8% vs. 56.3%, respectively, P < .001). Adverse events that caused death were also more common in the rituximab group versus the ocrelizumab group (5.75% vs. 2.11%, P < .001).
Infections and infestations were more common in the ocrelizumab group than the rituximab group (21.93% vs. 11.05%, respectively, P < .001). However, certain AEs were more common in the rituximab group than the ocrelizumab group: Those in the blood and lymphatic system category (2.86% vs. 0.91%, respectively, P < .001), and those in the neoplasms category (4.02% vs. 1.28%, P < .001, respectively).
Researchers found a highly strong association between rituximab and a rare side effects – ear pruritus (itching, 0.8%). They also identified signals for infusion-related reaction (4.82%), throat irritation (4.01%) and throat tightness (1.44%), malignant melanoma (0.8%), breast cancer (1.77%) and neutropenia (2.57%).
Among the ocrelizumab AEs, researchers found the strongest association with oral herpes (2.21%), and they found other signals for herpes zoster (2.89%), urinary tract infection (10.52%), nasopharyngitis (9.79%), infusion-related reaction (4.76%), throat irritation (3.08%), and notably MS relapses (4.1%).
“Additional pharmacovigilance studies are needed to explore and further characterize these findings,” the researchers wrote. “Furthermore, these observations suggest that the AE profile of other second-generation anti-CD20 [monoclonal antibodies] may also differ from those of rituximab and ocrelizumab.”
Dr. Gudesblatt praised the analysis and said the findings make sense. “Use of B-cell–depleting agents lead to accumulative immune deficiency in routine care, which leads to higher rates of infection,” he said. He added that, “in the clinical trials for ocrelizumab, patients with IgG and IgM deficiency were excluded, but there is no advisement to exclude such patients in real care. The rates of infection in those patients with MS who have preexisting immune deficiencies and who are treated with these agents are unknown.”
The prospect of AEs is especially worrisome, he said, since “this information is only short term. Who knows what effect the prolonged use of unopposed B-cell depletion will have on infections in the long run?”
Neurologist Mitchell Wallin, MD, MPH, of George Washington University, Washington, and the University of Maryland, Baltimore County, said in an interview that the analysis is rigorous and especially useful because it includes a wider array of subjects – including those who are older and sicker – than took part in earlier clinical trials. “It’s really important to look at this real-world evidence,” he said, “and basically put this in the back of your head when you follow up with your patients.”
No study funding was reported. The corresponding author reported various disclosures. Dr. Gudesblatt and Dr. Wallin reported no disclosures.
SOURCE: Gonzalez Caldito N et al. Mult Scler J. 2020 Aug 21. doi: 10.1177/1352458520949986.
, a new postmarketing analysis finds, and AE-related deaths were not unusual. Serious AEs, and those linked to death, were more common in the rituximab group, although the reported infection rate was higher in the ocrelizumab group.
The analysis, published Aug. 21 in the Multiple Sclerosis Journal, highlights the importance of monitoring patients for infections and encouraging them to do the same, the authors said.
“This report points out the impact of treatments in terms of unrecognized or underappreciated complications,” said Mark Gudesblatt, MD, medical director of the Comprehensive MS Care Center at South Shore Neurologic Associates in Patchogue, N.Y., who reviewed the study findings. “These medications have a significant downside.”
Lead author Natalia Gonzalez Caldito, MD, of the University of Texas Southwestern Medical Center, Dallas, and colleagues analyzed AEs for the drugs in the Food and Drug Administration’s Adverse Event Reporting System. They only included cases in which the drugs were solely used to treat MS and were indicated as the cause of the AEs.
Rituximab (Rituxan) and ocrelizumab (Ocrevus) are both monoclonal antibodies. Rituximab is not FDA approved for MS but is used off label; ocrelizumab is approved for the relapsing forms of MS and primary progressive MS.
The researchers found 623 AE reports and 1,466 total AEs for rituximab and 7,948 and 23,613, respectively, for ocrelizumab. The average ages for the groups were 48.76 versus 43.89, respectively, (P < .001), and 71% in each group were women.
Among total AEs, serious AEs were more common in the rituximab group versus the ocrelizumab group (64.8% vs. 56.3%, respectively, P < .001). Adverse events that caused death were also more common in the rituximab group versus the ocrelizumab group (5.75% vs. 2.11%, P < .001).
Infections and infestations were more common in the ocrelizumab group than the rituximab group (21.93% vs. 11.05%, respectively, P < .001). However, certain AEs were more common in the rituximab group than the ocrelizumab group: Those in the blood and lymphatic system category (2.86% vs. 0.91%, respectively, P < .001), and those in the neoplasms category (4.02% vs. 1.28%, P < .001, respectively).
Researchers found a highly strong association between rituximab and a rare side effects – ear pruritus (itching, 0.8%). They also identified signals for infusion-related reaction (4.82%), throat irritation (4.01%) and throat tightness (1.44%), malignant melanoma (0.8%), breast cancer (1.77%) and neutropenia (2.57%).
Among the ocrelizumab AEs, researchers found the strongest association with oral herpes (2.21%), and they found other signals for herpes zoster (2.89%), urinary tract infection (10.52%), nasopharyngitis (9.79%), infusion-related reaction (4.76%), throat irritation (3.08%), and notably MS relapses (4.1%).
“Additional pharmacovigilance studies are needed to explore and further characterize these findings,” the researchers wrote. “Furthermore, these observations suggest that the AE profile of other second-generation anti-CD20 [monoclonal antibodies] may also differ from those of rituximab and ocrelizumab.”
Dr. Gudesblatt praised the analysis and said the findings make sense. “Use of B-cell–depleting agents lead to accumulative immune deficiency in routine care, which leads to higher rates of infection,” he said. He added that, “in the clinical trials for ocrelizumab, patients with IgG and IgM deficiency were excluded, but there is no advisement to exclude such patients in real care. The rates of infection in those patients with MS who have preexisting immune deficiencies and who are treated with these agents are unknown.”
The prospect of AEs is especially worrisome, he said, since “this information is only short term. Who knows what effect the prolonged use of unopposed B-cell depletion will have on infections in the long run?”
Neurologist Mitchell Wallin, MD, MPH, of George Washington University, Washington, and the University of Maryland, Baltimore County, said in an interview that the analysis is rigorous and especially useful because it includes a wider array of subjects – including those who are older and sicker – than took part in earlier clinical trials. “It’s really important to look at this real-world evidence,” he said, “and basically put this in the back of your head when you follow up with your patients.”
No study funding was reported. The corresponding author reported various disclosures. Dr. Gudesblatt and Dr. Wallin reported no disclosures.
SOURCE: Gonzalez Caldito N et al. Mult Scler J. 2020 Aug 21. doi: 10.1177/1352458520949986.
, a new postmarketing analysis finds, and AE-related deaths were not unusual. Serious AEs, and those linked to death, were more common in the rituximab group, although the reported infection rate was higher in the ocrelizumab group.
The analysis, published Aug. 21 in the Multiple Sclerosis Journal, highlights the importance of monitoring patients for infections and encouraging them to do the same, the authors said.
“This report points out the impact of treatments in terms of unrecognized or underappreciated complications,” said Mark Gudesblatt, MD, medical director of the Comprehensive MS Care Center at South Shore Neurologic Associates in Patchogue, N.Y., who reviewed the study findings. “These medications have a significant downside.”
Lead author Natalia Gonzalez Caldito, MD, of the University of Texas Southwestern Medical Center, Dallas, and colleagues analyzed AEs for the drugs in the Food and Drug Administration’s Adverse Event Reporting System. They only included cases in which the drugs were solely used to treat MS and were indicated as the cause of the AEs.
Rituximab (Rituxan) and ocrelizumab (Ocrevus) are both monoclonal antibodies. Rituximab is not FDA approved for MS but is used off label; ocrelizumab is approved for the relapsing forms of MS and primary progressive MS.
The researchers found 623 AE reports and 1,466 total AEs for rituximab and 7,948 and 23,613, respectively, for ocrelizumab. The average ages for the groups were 48.76 versus 43.89, respectively, (P < .001), and 71% in each group were women.
Among total AEs, serious AEs were more common in the rituximab group versus the ocrelizumab group (64.8% vs. 56.3%, respectively, P < .001). Adverse events that caused death were also more common in the rituximab group versus the ocrelizumab group (5.75% vs. 2.11%, P < .001).
Infections and infestations were more common in the ocrelizumab group than the rituximab group (21.93% vs. 11.05%, respectively, P < .001). However, certain AEs were more common in the rituximab group than the ocrelizumab group: Those in the blood and lymphatic system category (2.86% vs. 0.91%, respectively, P < .001), and those in the neoplasms category (4.02% vs. 1.28%, P < .001, respectively).
Researchers found a highly strong association between rituximab and a rare side effects – ear pruritus (itching, 0.8%). They also identified signals for infusion-related reaction (4.82%), throat irritation (4.01%) and throat tightness (1.44%), malignant melanoma (0.8%), breast cancer (1.77%) and neutropenia (2.57%).
Among the ocrelizumab AEs, researchers found the strongest association with oral herpes (2.21%), and they found other signals for herpes zoster (2.89%), urinary tract infection (10.52%), nasopharyngitis (9.79%), infusion-related reaction (4.76%), throat irritation (3.08%), and notably MS relapses (4.1%).
“Additional pharmacovigilance studies are needed to explore and further characterize these findings,” the researchers wrote. “Furthermore, these observations suggest that the AE profile of other second-generation anti-CD20 [monoclonal antibodies] may also differ from those of rituximab and ocrelizumab.”
Dr. Gudesblatt praised the analysis and said the findings make sense. “Use of B-cell–depleting agents lead to accumulative immune deficiency in routine care, which leads to higher rates of infection,” he said. He added that, “in the clinical trials for ocrelizumab, patients with IgG and IgM deficiency were excluded, but there is no advisement to exclude such patients in real care. The rates of infection in those patients with MS who have preexisting immune deficiencies and who are treated with these agents are unknown.”
The prospect of AEs is especially worrisome, he said, since “this information is only short term. Who knows what effect the prolonged use of unopposed B-cell depletion will have on infections in the long run?”
Neurologist Mitchell Wallin, MD, MPH, of George Washington University, Washington, and the University of Maryland, Baltimore County, said in an interview that the analysis is rigorous and especially useful because it includes a wider array of subjects – including those who are older and sicker – than took part in earlier clinical trials. “It’s really important to look at this real-world evidence,” he said, “and basically put this in the back of your head when you follow up with your patients.”
No study funding was reported. The corresponding author reported various disclosures. Dr. Gudesblatt and Dr. Wallin reported no disclosures.
SOURCE: Gonzalez Caldito N et al. Mult Scler J. 2020 Aug 21. doi: 10.1177/1352458520949986.
FROM MULTIPLE SCLEROSIS JOURNAL