User login
Is vertical transmission of SARS-CoV-2 possible? Is that the right question?
Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS CoV-2? eLife. 2020;9:e58716.
EXPERT COMMENTARY
Maternal infection with the novel SARS-CoV-2 virus has been associated with severe maternal morbidity and mortality causing adverse pregnancy outcomes, such as preterm birth and, potentially, stillbirth, with vertical transmission of the virus to the fetus possible.1,2
Uniquely, maternal physiology supports both pro- and anti-inflammatory states within pregnancy—a system that not only must protect the mother but also must tolerate a semi-allogenic fetus. Studies demonstrate that the first and third trimesters are pro-inflammatory, while the second trimester is thought to be anti-inflammatory.3 Since the discovery of the SARS-CoV-2 virus, the question surrounding vertical transmission (infectivity from mother to fetus via the placenta) has occupied the imagination of physicians, scientists, and pregnant women. Importantly, the virus is transmitted to human cells via the ACE2 (angiotensin-converting enzyme 2) receptor, which aids in viral cell attachment. ACE2 receptors are expressed in placental stromal cells, perivascular cells of decidua, cytotrophoblast and syncytiotrophoblast,4 as well as blood vessel endothelium and vascular smooth muscle from both primary and secondary villi.
Details of the study
In their recent study, Pique-Regi and colleagues used single-cell RNA sequencing data to investigate whether the receptors responsible for SARS-CoV-2 infection are expressed in the human placenta.5 Their findings suggest that TMPRSS2 is present in insufficient quantity in the placenta to make vertical transmission possible and/or clinically relevant. Thus, despite the presence of ACE2 receptors in placental tissue, without the enzymatic assistance of a helper protein like TMPRSS2 (transmembrane protease, serine 2), vertical transmission is highly unlikely. The researchers found that there was negligible co-transcription for ACE2 and TMPRSS2 in the placenta and that placental tissue lacks the mRNA necessary to produce the enzyme; they concluded that the likelihood of vertical transmission to the fetus was therefore unlikely.
As a caveat to their research, the authors noted that:
- transcription levels do not always correlate with protein expression
- it is possible that a noncanonical cell-entry mediator facilitates entry
- individuals with complications related to the renin-angiotensin-aldosterone system (such as hypertensive disease) may have alterations to the expression of ACE2.
Study strengths and limitations
Methods for this study reveal that the researchers examined 32 placentas, all taken in the third trimester (32.9-39.1 weeks), with a median gestational age of 36.9 weeks. Notably, 81.3% of placentas were from Black women, 6.2% from White women, and 12.5% from Other women. The median maternal age was 25 years, median body mass index was 27.8 kg/m2, and 84.4% of women were multiparous. While this sample was not representative of race, gestational age, or parity, it is difficult to know whether those selection biases would have changed the researchers' findings.
The question regarding vertical transmission is one not answered solely on the basis of RNA sequencing data. Clinically, we know that neonates of mothers infected with SARS-CoV-2 have been born with immunoglobulin M antibodies, indicating antenatal exposure to the virus.6,7 In addition, infants have tested positive immediately after birth for coronavirus disease 2019 (COVID-19) via nasopharyngeal swab and amniotic fluid, and there are ample cases of histologic and polymerase chain reaction evidence of placental infection.8,9 We also know that inflammatory damage to the placenta could possibly break down the placental barrier.10
The destruction that SARS-CoV-2 often leaves in its wake is devastating for the maternal-fetal dyad. The effects of maternal infection on the placenta—where additional research is needed—can be profound, causing profuse endothelial damage, vascular malperfusion, thrombi, and infarcts, all of which can be lethal to some developing fetuses.
While the study by Pique-Regi and colleagues is an important contribution to the literature, it does not satisfactorily answer the question regarding vertical transmission. More research is needed, especially regarding maternal infection in the first and second trimesters, on the effects on placental vasculature (and timing of infection in each trimester), the potential breakdown of the maternal-fetal barrier, and, most important, the clinical courses and outcomes in both mother and infant.
JANE VAN DIS, MD
- Khalil A, Kalafat E, Benlioglu C, et al. SARS-CoV-2 infection in pregnancy: a systematic review and meta-analysis of clinical features and pregnancy outcomes. EClinical Medicine. 2020;25:100446.
- Khalil A, von Dadelszen P, Draycott T, et al. Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. JAMA. 2020;324:705-706.
- Liu H, Wang LL, Zhao SJ, et al. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J Reprod Immunol. 2020;139;103122.
- Li M, Chen L, Zhang J, et al. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS One. 2020;15:e0230295.
- Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? eLife. 2020;9:e58716.
- Zeng H, Xu C, Fan J, et al. Antibodies in infants born to mothers with COVID-19 pneumonia. JAMA. 2020;323:1848-1849.
- Dong L, Tian J, He S, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020;323:1846-1848.
- Kotlyar A, Grechukhina O, Chen A, et al. Vertical transmission of COVID-19: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;S0002-9378(20)30823-1.
- Richtmann R, Torloni MR, Oyamada Otani AR, et al. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: a case series. Case Rep Womens Health. 2020;e00243.
- Wang C, Zhou YH, Yang HX, et al. Intrauterine vertical transmission of SARS-CoV-2: what we know so far. Ultrasound Obstet Gynecol. 2020;55:724-725.
Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS CoV-2? eLife. 2020;9:e58716.
EXPERT COMMENTARY
Maternal infection with the novel SARS-CoV-2 virus has been associated with severe maternal morbidity and mortality causing adverse pregnancy outcomes, such as preterm birth and, potentially, stillbirth, with vertical transmission of the virus to the fetus possible.1,2
Uniquely, maternal physiology supports both pro- and anti-inflammatory states within pregnancy—a system that not only must protect the mother but also must tolerate a semi-allogenic fetus. Studies demonstrate that the first and third trimesters are pro-inflammatory, while the second trimester is thought to be anti-inflammatory.3 Since the discovery of the SARS-CoV-2 virus, the question surrounding vertical transmission (infectivity from mother to fetus via the placenta) has occupied the imagination of physicians, scientists, and pregnant women. Importantly, the virus is transmitted to human cells via the ACE2 (angiotensin-converting enzyme 2) receptor, which aids in viral cell attachment. ACE2 receptors are expressed in placental stromal cells, perivascular cells of decidua, cytotrophoblast and syncytiotrophoblast,4 as well as blood vessel endothelium and vascular smooth muscle from both primary and secondary villi.
Details of the study
In their recent study, Pique-Regi and colleagues used single-cell RNA sequencing data to investigate whether the receptors responsible for SARS-CoV-2 infection are expressed in the human placenta.5 Their findings suggest that TMPRSS2 is present in insufficient quantity in the placenta to make vertical transmission possible and/or clinically relevant. Thus, despite the presence of ACE2 receptors in placental tissue, without the enzymatic assistance of a helper protein like TMPRSS2 (transmembrane protease, serine 2), vertical transmission is highly unlikely. The researchers found that there was negligible co-transcription for ACE2 and TMPRSS2 in the placenta and that placental tissue lacks the mRNA necessary to produce the enzyme; they concluded that the likelihood of vertical transmission to the fetus was therefore unlikely.
As a caveat to their research, the authors noted that:
- transcription levels do not always correlate with protein expression
- it is possible that a noncanonical cell-entry mediator facilitates entry
- individuals with complications related to the renin-angiotensin-aldosterone system (such as hypertensive disease) may have alterations to the expression of ACE2.
Study strengths and limitations
Methods for this study reveal that the researchers examined 32 placentas, all taken in the third trimester (32.9-39.1 weeks), with a median gestational age of 36.9 weeks. Notably, 81.3% of placentas were from Black women, 6.2% from White women, and 12.5% from Other women. The median maternal age was 25 years, median body mass index was 27.8 kg/m2, and 84.4% of women were multiparous. While this sample was not representative of race, gestational age, or parity, it is difficult to know whether those selection biases would have changed the researchers' findings.
The question regarding vertical transmission is one not answered solely on the basis of RNA sequencing data. Clinically, we know that neonates of mothers infected with SARS-CoV-2 have been born with immunoglobulin M antibodies, indicating antenatal exposure to the virus.6,7 In addition, infants have tested positive immediately after birth for coronavirus disease 2019 (COVID-19) via nasopharyngeal swab and amniotic fluid, and there are ample cases of histologic and polymerase chain reaction evidence of placental infection.8,9 We also know that inflammatory damage to the placenta could possibly break down the placental barrier.10
The destruction that SARS-CoV-2 often leaves in its wake is devastating for the maternal-fetal dyad. The effects of maternal infection on the placenta—where additional research is needed—can be profound, causing profuse endothelial damage, vascular malperfusion, thrombi, and infarcts, all of which can be lethal to some developing fetuses.
While the study by Pique-Regi and colleagues is an important contribution to the literature, it does not satisfactorily answer the question regarding vertical transmission. More research is needed, especially regarding maternal infection in the first and second trimesters, on the effects on placental vasculature (and timing of infection in each trimester), the potential breakdown of the maternal-fetal barrier, and, most important, the clinical courses and outcomes in both mother and infant.
JANE VAN DIS, MD
Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS CoV-2? eLife. 2020;9:e58716.
EXPERT COMMENTARY
Maternal infection with the novel SARS-CoV-2 virus has been associated with severe maternal morbidity and mortality causing adverse pregnancy outcomes, such as preterm birth and, potentially, stillbirth, with vertical transmission of the virus to the fetus possible.1,2
Uniquely, maternal physiology supports both pro- and anti-inflammatory states within pregnancy—a system that not only must protect the mother but also must tolerate a semi-allogenic fetus. Studies demonstrate that the first and third trimesters are pro-inflammatory, while the second trimester is thought to be anti-inflammatory.3 Since the discovery of the SARS-CoV-2 virus, the question surrounding vertical transmission (infectivity from mother to fetus via the placenta) has occupied the imagination of physicians, scientists, and pregnant women. Importantly, the virus is transmitted to human cells via the ACE2 (angiotensin-converting enzyme 2) receptor, which aids in viral cell attachment. ACE2 receptors are expressed in placental stromal cells, perivascular cells of decidua, cytotrophoblast and syncytiotrophoblast,4 as well as blood vessel endothelium and vascular smooth muscle from both primary and secondary villi.
Details of the study
In their recent study, Pique-Regi and colleagues used single-cell RNA sequencing data to investigate whether the receptors responsible for SARS-CoV-2 infection are expressed in the human placenta.5 Their findings suggest that TMPRSS2 is present in insufficient quantity in the placenta to make vertical transmission possible and/or clinically relevant. Thus, despite the presence of ACE2 receptors in placental tissue, without the enzymatic assistance of a helper protein like TMPRSS2 (transmembrane protease, serine 2), vertical transmission is highly unlikely. The researchers found that there was negligible co-transcription for ACE2 and TMPRSS2 in the placenta and that placental tissue lacks the mRNA necessary to produce the enzyme; they concluded that the likelihood of vertical transmission to the fetus was therefore unlikely.
As a caveat to their research, the authors noted that:
- transcription levels do not always correlate with protein expression
- it is possible that a noncanonical cell-entry mediator facilitates entry
- individuals with complications related to the renin-angiotensin-aldosterone system (such as hypertensive disease) may have alterations to the expression of ACE2.
Study strengths and limitations
Methods for this study reveal that the researchers examined 32 placentas, all taken in the third trimester (32.9-39.1 weeks), with a median gestational age of 36.9 weeks. Notably, 81.3% of placentas were from Black women, 6.2% from White women, and 12.5% from Other women. The median maternal age was 25 years, median body mass index was 27.8 kg/m2, and 84.4% of women were multiparous. While this sample was not representative of race, gestational age, or parity, it is difficult to know whether those selection biases would have changed the researchers' findings.
The question regarding vertical transmission is one not answered solely on the basis of RNA sequencing data. Clinically, we know that neonates of mothers infected with SARS-CoV-2 have been born with immunoglobulin M antibodies, indicating antenatal exposure to the virus.6,7 In addition, infants have tested positive immediately after birth for coronavirus disease 2019 (COVID-19) via nasopharyngeal swab and amniotic fluid, and there are ample cases of histologic and polymerase chain reaction evidence of placental infection.8,9 We also know that inflammatory damage to the placenta could possibly break down the placental barrier.10
The destruction that SARS-CoV-2 often leaves in its wake is devastating for the maternal-fetal dyad. The effects of maternal infection on the placenta—where additional research is needed—can be profound, causing profuse endothelial damage, vascular malperfusion, thrombi, and infarcts, all of which can be lethal to some developing fetuses.
While the study by Pique-Regi and colleagues is an important contribution to the literature, it does not satisfactorily answer the question regarding vertical transmission. More research is needed, especially regarding maternal infection in the first and second trimesters, on the effects on placental vasculature (and timing of infection in each trimester), the potential breakdown of the maternal-fetal barrier, and, most important, the clinical courses and outcomes in both mother and infant.
JANE VAN DIS, MD
- Khalil A, Kalafat E, Benlioglu C, et al. SARS-CoV-2 infection in pregnancy: a systematic review and meta-analysis of clinical features and pregnancy outcomes. EClinical Medicine. 2020;25:100446.
- Khalil A, von Dadelszen P, Draycott T, et al. Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. JAMA. 2020;324:705-706.
- Liu H, Wang LL, Zhao SJ, et al. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J Reprod Immunol. 2020;139;103122.
- Li M, Chen L, Zhang J, et al. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS One. 2020;15:e0230295.
- Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? eLife. 2020;9:e58716.
- Zeng H, Xu C, Fan J, et al. Antibodies in infants born to mothers with COVID-19 pneumonia. JAMA. 2020;323:1848-1849.
- Dong L, Tian J, He S, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020;323:1846-1848.
- Kotlyar A, Grechukhina O, Chen A, et al. Vertical transmission of COVID-19: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;S0002-9378(20)30823-1.
- Richtmann R, Torloni MR, Oyamada Otani AR, et al. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: a case series. Case Rep Womens Health. 2020;e00243.
- Wang C, Zhou YH, Yang HX, et al. Intrauterine vertical transmission of SARS-CoV-2: what we know so far. Ultrasound Obstet Gynecol. 2020;55:724-725.
- Khalil A, Kalafat E, Benlioglu C, et al. SARS-CoV-2 infection in pregnancy: a systematic review and meta-analysis of clinical features and pregnancy outcomes. EClinical Medicine. 2020;25:100446.
- Khalil A, von Dadelszen P, Draycott T, et al. Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. JAMA. 2020;324:705-706.
- Liu H, Wang LL, Zhao SJ, et al. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J Reprod Immunol. 2020;139;103122.
- Li M, Chen L, Zhang J, et al. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS One. 2020;15:e0230295.
- Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? eLife. 2020;9:e58716.
- Zeng H, Xu C, Fan J, et al. Antibodies in infants born to mothers with COVID-19 pneumonia. JAMA. 2020;323:1848-1849.
- Dong L, Tian J, He S, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020;323:1846-1848.
- Kotlyar A, Grechukhina O, Chen A, et al. Vertical transmission of COVID-19: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;S0002-9378(20)30823-1.
- Richtmann R, Torloni MR, Oyamada Otani AR, et al. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: a case series. Case Rep Womens Health. 2020;e00243.
- Wang C, Zhou YH, Yang HX, et al. Intrauterine vertical transmission of SARS-CoV-2: what we know so far. Ultrasound Obstet Gynecol. 2020;55:724-725.
Watch for nonsuicidal self-injury in girls with ADHD, comorbidities
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
FROM ECNP 2020
AGA addresses postendoscopy esophageal adenocarcinoma
The American Gastroenterological Association has published a clinical practice update that characterizes postendoscopy esophageal adenocarcinoma (EAC) and offers recommendations to improve endoscopic detection of dysplastic and neoplastic lesions in patients with Barrett’s esophagus.
While emerging technologies may improve detection rates in the future, short-term progress will depend on human expertise, reported lead author Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and colleagues.
Writing in Gastroenterology, Dr. Wani and colleagues noted that EAC incidence has increased sevenfold over the past 4 decades, and 40% of patients with EAC have advanced disease at diagnosis, with a “dismal” 5-year survival rate.
Attempts to catch EAC earlier through Barrett’s esophagus surveillance endoscopy have been generally fallen short, the investigators added. They discussed a variety of obstacles to success, including divergence from recommended screening timelines, nonadherence to the Seattle biopsy protocol, sampling errors, and variability of dysplastic tissue interpretation between pathologists.
“Even in the face of suboptimal impact of current strategies on population-based EAC mortality, medical societies consistently recommend [Barrett’s esophagus] screening and surveillance,” the investigators wrote. “In this context, similar to postcolonoscopy colorectal cancer, the concept of missed EAC is gaining importance in endoscopic Barrett’s esophagus screening and surveillance.”
In the present update, the investigators first aimed to standardize definitions of postendoscopy and interval EAC.
“We propose that postendoscopy EAC be defined as EAC and/or [Barrett’s esophagus]–related high-grade dysplasia identified within a finite time period (typically 1 year) following a nondiagnostic endoscopy,” the investigators wrote. “Interval EAC may be defined as EAC or [Barrett’s esophagus]–related high-grade dysplasia diagnosed after a negative screening or surveillance endoscopy before the date of the next recommended test.”
The latter definition, the investigators noted, was written with acknowledgment of emerging, noninvasive, nonendoscopic screening tools.
Next, Dr. Wani and colleagues dove deeper into the incidence of postendoscopy EAC in the Barrett’s esophagus population. Across multiple cohort studies and meta-analyses, incidence within 1 year of screening endoscopy ranged widely, from 3% to 25%. Data from Barrett’s esophagus patients undergoing endoscopic eradication therapy suggest that incidence of postendoscopy EAC may be greatest within 1-2 years of complete eradication of intestinal metaplasia; one meta-analysis involving 22 studies reported that the risk of EAC was 92% higher within the first year of eradication, compared with subsequent years.
“These data support that high-grade dysplasia/EAC identified within 1 year after complete eradication of intestinal metaplasia likely represents missed and/or incompletely treated prevalent disease rather than recurrent or incident neoplasia,” the investigators wrote.
In support of this conclusion, Dr. Wani and colleagues drew upon data from colorectal cancer screening programs, which suggest that 89% of postcolonoscopy colorectal cancers “may be avoidable, attributable to technical endoscopic factors, compromised decision-making, and administrative factors.”
Regulatory agencies measure quality of colorectal cancer screening programs with adenoma detection rate, which has been shown to correlate inversely with colorectal cancer and mortality; but no analogous measure has been established for Barrett’s esophagus screening. Candidate quality markers include neoplasia detection rate and dysplasia detection rate, though more work is needed to confirm their reliability.
“While easier to measure, compared to postendoscopy EAC rates, neoplasia detection rate remains a surrogate endoscopy quality marker in Barrett’s esophagus surveillance, while postendoscopy EAC rates serve as a true outcome measure that matters clinically,” the investigators wrote.
Dr. Wani and colleagues proposed four clinical strategies that may immediately improve quality of Barrett’s esophagus screening.
- First, they recommended “assiduous identification and photo-documentation of esophageal landmarks” coupled with lesion descriptions that adhere to Prague and Paris classification schemes, along with resection or referral upon identification.
- Second, they called for consistent use of high-definition white-light endoscopy and virtual chromoendoscopy.
- Third, they suggested that endoscopists “spend adequate time for inspection,” with biopsies taken in accordance with the Seattle protocol.
- Fourth, Dr. Wani and colleagues suggested that all practices conducting Barrett’s esophagus screening and surveillance establish continuously active quality control programs.
The investigators concluded the clinical practice update with a discussion of future directions.
“Prospective trials are needed to evaluate the impact of better dissemination of guidelines and quality indicators, improved endoscopic dysplasia detection using interactive web-based educational tools, advanced imaging techniques with artificial intelligence, and improved sampling modalities that reduce sampling errors,” they wrote. “Finally, increased emphasis is needed on improving training in both the cognitive and procedural aspects of [Barrett’s esophagus] endoscopy through structured educational programs among trainees and practicing endoscopists.”
The study was supported by the University of Colorado department of medicine’s Outstanding Early Scholars Program. The investigators disclosed relationships with Medtronic, Boston Scientific, Ironwood, and others.
SOURCE: Wani S et al. Gastroenterology. 2020 Jul 13. doi: 10.1053/j.gastro.2020.06.089.
The American Gastroenterological Association has published a clinical practice update that characterizes postendoscopy esophageal adenocarcinoma (EAC) and offers recommendations to improve endoscopic detection of dysplastic and neoplastic lesions in patients with Barrett’s esophagus.
While emerging technologies may improve detection rates in the future, short-term progress will depend on human expertise, reported lead author Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and colleagues.
Writing in Gastroenterology, Dr. Wani and colleagues noted that EAC incidence has increased sevenfold over the past 4 decades, and 40% of patients with EAC have advanced disease at diagnosis, with a “dismal” 5-year survival rate.
Attempts to catch EAC earlier through Barrett’s esophagus surveillance endoscopy have been generally fallen short, the investigators added. They discussed a variety of obstacles to success, including divergence from recommended screening timelines, nonadherence to the Seattle biopsy protocol, sampling errors, and variability of dysplastic tissue interpretation between pathologists.
“Even in the face of suboptimal impact of current strategies on population-based EAC mortality, medical societies consistently recommend [Barrett’s esophagus] screening and surveillance,” the investigators wrote. “In this context, similar to postcolonoscopy colorectal cancer, the concept of missed EAC is gaining importance in endoscopic Barrett’s esophagus screening and surveillance.”
In the present update, the investigators first aimed to standardize definitions of postendoscopy and interval EAC.
“We propose that postendoscopy EAC be defined as EAC and/or [Barrett’s esophagus]–related high-grade dysplasia identified within a finite time period (typically 1 year) following a nondiagnostic endoscopy,” the investigators wrote. “Interval EAC may be defined as EAC or [Barrett’s esophagus]–related high-grade dysplasia diagnosed after a negative screening or surveillance endoscopy before the date of the next recommended test.”
The latter definition, the investigators noted, was written with acknowledgment of emerging, noninvasive, nonendoscopic screening tools.
Next, Dr. Wani and colleagues dove deeper into the incidence of postendoscopy EAC in the Barrett’s esophagus population. Across multiple cohort studies and meta-analyses, incidence within 1 year of screening endoscopy ranged widely, from 3% to 25%. Data from Barrett’s esophagus patients undergoing endoscopic eradication therapy suggest that incidence of postendoscopy EAC may be greatest within 1-2 years of complete eradication of intestinal metaplasia; one meta-analysis involving 22 studies reported that the risk of EAC was 92% higher within the first year of eradication, compared with subsequent years.
“These data support that high-grade dysplasia/EAC identified within 1 year after complete eradication of intestinal metaplasia likely represents missed and/or incompletely treated prevalent disease rather than recurrent or incident neoplasia,” the investigators wrote.
In support of this conclusion, Dr. Wani and colleagues drew upon data from colorectal cancer screening programs, which suggest that 89% of postcolonoscopy colorectal cancers “may be avoidable, attributable to technical endoscopic factors, compromised decision-making, and administrative factors.”
Regulatory agencies measure quality of colorectal cancer screening programs with adenoma detection rate, which has been shown to correlate inversely with colorectal cancer and mortality; but no analogous measure has been established for Barrett’s esophagus screening. Candidate quality markers include neoplasia detection rate and dysplasia detection rate, though more work is needed to confirm their reliability.
“While easier to measure, compared to postendoscopy EAC rates, neoplasia detection rate remains a surrogate endoscopy quality marker in Barrett’s esophagus surveillance, while postendoscopy EAC rates serve as a true outcome measure that matters clinically,” the investigators wrote.
Dr. Wani and colleagues proposed four clinical strategies that may immediately improve quality of Barrett’s esophagus screening.
- First, they recommended “assiduous identification and photo-documentation of esophageal landmarks” coupled with lesion descriptions that adhere to Prague and Paris classification schemes, along with resection or referral upon identification.
- Second, they called for consistent use of high-definition white-light endoscopy and virtual chromoendoscopy.
- Third, they suggested that endoscopists “spend adequate time for inspection,” with biopsies taken in accordance with the Seattle protocol.
- Fourth, Dr. Wani and colleagues suggested that all practices conducting Barrett’s esophagus screening and surveillance establish continuously active quality control programs.
The investigators concluded the clinical practice update with a discussion of future directions.
“Prospective trials are needed to evaluate the impact of better dissemination of guidelines and quality indicators, improved endoscopic dysplasia detection using interactive web-based educational tools, advanced imaging techniques with artificial intelligence, and improved sampling modalities that reduce sampling errors,” they wrote. “Finally, increased emphasis is needed on improving training in both the cognitive and procedural aspects of [Barrett’s esophagus] endoscopy through structured educational programs among trainees and practicing endoscopists.”
The study was supported by the University of Colorado department of medicine’s Outstanding Early Scholars Program. The investigators disclosed relationships with Medtronic, Boston Scientific, Ironwood, and others.
SOURCE: Wani S et al. Gastroenterology. 2020 Jul 13. doi: 10.1053/j.gastro.2020.06.089.
The American Gastroenterological Association has published a clinical practice update that characterizes postendoscopy esophageal adenocarcinoma (EAC) and offers recommendations to improve endoscopic detection of dysplastic and neoplastic lesions in patients with Barrett’s esophagus.
While emerging technologies may improve detection rates in the future, short-term progress will depend on human expertise, reported lead author Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and colleagues.
Writing in Gastroenterology, Dr. Wani and colleagues noted that EAC incidence has increased sevenfold over the past 4 decades, and 40% of patients with EAC have advanced disease at diagnosis, with a “dismal” 5-year survival rate.
Attempts to catch EAC earlier through Barrett’s esophagus surveillance endoscopy have been generally fallen short, the investigators added. They discussed a variety of obstacles to success, including divergence from recommended screening timelines, nonadherence to the Seattle biopsy protocol, sampling errors, and variability of dysplastic tissue interpretation between pathologists.
“Even in the face of suboptimal impact of current strategies on population-based EAC mortality, medical societies consistently recommend [Barrett’s esophagus] screening and surveillance,” the investigators wrote. “In this context, similar to postcolonoscopy colorectal cancer, the concept of missed EAC is gaining importance in endoscopic Barrett’s esophagus screening and surveillance.”
In the present update, the investigators first aimed to standardize definitions of postendoscopy and interval EAC.
“We propose that postendoscopy EAC be defined as EAC and/or [Barrett’s esophagus]–related high-grade dysplasia identified within a finite time period (typically 1 year) following a nondiagnostic endoscopy,” the investigators wrote. “Interval EAC may be defined as EAC or [Barrett’s esophagus]–related high-grade dysplasia diagnosed after a negative screening or surveillance endoscopy before the date of the next recommended test.”
The latter definition, the investigators noted, was written with acknowledgment of emerging, noninvasive, nonendoscopic screening tools.
Next, Dr. Wani and colleagues dove deeper into the incidence of postendoscopy EAC in the Barrett’s esophagus population. Across multiple cohort studies and meta-analyses, incidence within 1 year of screening endoscopy ranged widely, from 3% to 25%. Data from Barrett’s esophagus patients undergoing endoscopic eradication therapy suggest that incidence of postendoscopy EAC may be greatest within 1-2 years of complete eradication of intestinal metaplasia; one meta-analysis involving 22 studies reported that the risk of EAC was 92% higher within the first year of eradication, compared with subsequent years.
“These data support that high-grade dysplasia/EAC identified within 1 year after complete eradication of intestinal metaplasia likely represents missed and/or incompletely treated prevalent disease rather than recurrent or incident neoplasia,” the investigators wrote.
In support of this conclusion, Dr. Wani and colleagues drew upon data from colorectal cancer screening programs, which suggest that 89% of postcolonoscopy colorectal cancers “may be avoidable, attributable to technical endoscopic factors, compromised decision-making, and administrative factors.”
Regulatory agencies measure quality of colorectal cancer screening programs with adenoma detection rate, which has been shown to correlate inversely with colorectal cancer and mortality; but no analogous measure has been established for Barrett’s esophagus screening. Candidate quality markers include neoplasia detection rate and dysplasia detection rate, though more work is needed to confirm their reliability.
“While easier to measure, compared to postendoscopy EAC rates, neoplasia detection rate remains a surrogate endoscopy quality marker in Barrett’s esophagus surveillance, while postendoscopy EAC rates serve as a true outcome measure that matters clinically,” the investigators wrote.
Dr. Wani and colleagues proposed four clinical strategies that may immediately improve quality of Barrett’s esophagus screening.
- First, they recommended “assiduous identification and photo-documentation of esophageal landmarks” coupled with lesion descriptions that adhere to Prague and Paris classification schemes, along with resection or referral upon identification.
- Second, they called for consistent use of high-definition white-light endoscopy and virtual chromoendoscopy.
- Third, they suggested that endoscopists “spend adequate time for inspection,” with biopsies taken in accordance with the Seattle protocol.
- Fourth, Dr. Wani and colleagues suggested that all practices conducting Barrett’s esophagus screening and surveillance establish continuously active quality control programs.
The investigators concluded the clinical practice update with a discussion of future directions.
“Prospective trials are needed to evaluate the impact of better dissemination of guidelines and quality indicators, improved endoscopic dysplasia detection using interactive web-based educational tools, advanced imaging techniques with artificial intelligence, and improved sampling modalities that reduce sampling errors,” they wrote. “Finally, increased emphasis is needed on improving training in both the cognitive and procedural aspects of [Barrett’s esophagus] endoscopy through structured educational programs among trainees and practicing endoscopists.”
The study was supported by the University of Colorado department of medicine’s Outstanding Early Scholars Program. The investigators disclosed relationships with Medtronic, Boston Scientific, Ironwood, and others.
SOURCE: Wani S et al. Gastroenterology. 2020 Jul 13. doi: 10.1053/j.gastro.2020.06.089.
FROM GASTROENTEROLOGY
FOLFOXIRI tops doublets as bevacizumab backbone for mCRC
investigators reported in the Journal of Clinical Oncology.
In analyzing data from five clinical trials, the investigators found a 4.4-month increase in median overall survival and an 11.6% increase in estimated 5-year overall survival with FOLFOXIRI versus doublets. The trade-off was a higher incidence of grade 3-4 adverse events with FOLFOXIRI.
FOLFOXIRI plus bevacizumab is already included among first-line options in most clinical guidelines and recommendations, but there was no “proper estimation of the magnitude of the overall survival benefit” because trials had other primary endpoints, according to study author Chiara Cremolini, MD, PhD, of University of Pisa (Italy), and colleagues.
“To fully appreciate the cost/benefit balance of this option,” the investigators wanted to see how the numbers played out when overall survival was the primary endpoint, so they pooled individual patient data from the CHARTA, OLIVIA, STEAM, TRIBE, and TRIBE2 trials.
Patient characteristics and treatment
The analysis included 1,697 patients. The median age was 61 years (range, 53-67 years).
About 99% of patients had an Eastern Cooperative Oncology Group performance score of 0 or 1. About 20% had left-sided RAS and BRAF wild-type tumors because of the increased use of anti–epidermal growth factor receptor antibodies as first-line therapy for that indication in recent years.
In all, 846 patients were randomized to FOLFOXIRI plus bevacizumab and 851 to bevacizumab with doublets: 69.9% to FOLFOX (leucovorin, fluorouracil, and oxaliplatin) and 30.1% to FOLFIRI (fluorouracil, leucovorin, and irinotecan).
The duration of induction in all five trials ranged from 4 to 6 months. It was followed by maintenance with a fluoropyrimidine (fluorouracil and leucovorin or capecitabine) plus bevacizumab.
Efficacy and safety
At a median follow-up of 39.9 months, the median overall survival was 28.9 months in the FOLFOXIRI group and 24.5 months in the doublet group (P < .001). The estimated 5-year overall survival rate was 22.3% and 10.7%, respectively.
The median progression-free survival was 12.2 months in the FOLFOXIRI group and 9.9 months in the doublet group (P < .001).
The objective response rate was higher with FOLFOXIRI (64.5% vs. 53.6%, P < .001), as was R0 resection rate (16.4% vs. 11.8%, P = .007).
The FOLFOXIRI group also had a higher incidence of grade 3-4 adverse events, including neutropenia (45.8% vs. 21.5%; P < .001), febrile neutropenia (6.3% vs. 3.7%; P = .019), nausea (5.5% vs. 3.0%; P = .016), mucositis (5.1% vs. 2.9%; P = .024), and diarrhea (17.8% vs. 8.4%; P < .001).
Even so, FOLFOXIRI plus bevacizumab was not associated with a significant increase in toxic deaths (2.3% vs. 1.4%; P = .277).
Patient selection is ‘critical’
Based on their findings, the investigators said the best candidates for first-line FOLFOXIRI plus bevacizumab may be younger patients with an ECOG performance status of 0 or 1 and right-sided and/or RAS-mutated tumors not exposed to a previous oxaliplatin-based adjuvant regimen.
FOLFOXIRI plus bevacizumab did not provide any additional benefit in patients with BRAF-mutant tumors, so the combination shouldn’t be the first choice in this group, the investigators wrote. “FOLFOX plus bevacizumab seems the preferable upfront option.”
For left-sided RAS and BRAF wild-type tumors, a chemotherapy doublet with an anti–epidermal growth factor receptor remains the preferred option, according to the investigators.
“The study does support the use of FOLFOXIRI and bevacizumab as a valuable first-line option, but patient selection is critical because there is a toxicity cost; this efficacy versus toxicity will constantly be a seesaw for us,” commented Aparna Parikh, MD, of Massachusetts General Hospital in Boston, when the study was presented at the American Society of Clinical Oncology annual meeting earlier this year.
There was no external funding for this analysis. Three of the original five trials were sponsored by Roche. The study authors had numerous industry ties. Among others, Dr. Cremolini is a consultant for and reported honoraria and travel expenses from Roche. One author was a Genentech employee. Dr. Parikh disclosed relationships with Lilly, Genentech, and other companies.
SOURCE: Cremolini C et al. J Clin Oncol. 2020 Aug 20. doi: 10.1200/JCO.20.01225.
investigators reported in the Journal of Clinical Oncology.
In analyzing data from five clinical trials, the investigators found a 4.4-month increase in median overall survival and an 11.6% increase in estimated 5-year overall survival with FOLFOXIRI versus doublets. The trade-off was a higher incidence of grade 3-4 adverse events with FOLFOXIRI.
FOLFOXIRI plus bevacizumab is already included among first-line options in most clinical guidelines and recommendations, but there was no “proper estimation of the magnitude of the overall survival benefit” because trials had other primary endpoints, according to study author Chiara Cremolini, MD, PhD, of University of Pisa (Italy), and colleagues.
“To fully appreciate the cost/benefit balance of this option,” the investigators wanted to see how the numbers played out when overall survival was the primary endpoint, so they pooled individual patient data from the CHARTA, OLIVIA, STEAM, TRIBE, and TRIBE2 trials.
Patient characteristics and treatment
The analysis included 1,697 patients. The median age was 61 years (range, 53-67 years).
About 99% of patients had an Eastern Cooperative Oncology Group performance score of 0 or 1. About 20% had left-sided RAS and BRAF wild-type tumors because of the increased use of anti–epidermal growth factor receptor antibodies as first-line therapy for that indication in recent years.
In all, 846 patients were randomized to FOLFOXIRI plus bevacizumab and 851 to bevacizumab with doublets: 69.9% to FOLFOX (leucovorin, fluorouracil, and oxaliplatin) and 30.1% to FOLFIRI (fluorouracil, leucovorin, and irinotecan).
The duration of induction in all five trials ranged from 4 to 6 months. It was followed by maintenance with a fluoropyrimidine (fluorouracil and leucovorin or capecitabine) plus bevacizumab.
Efficacy and safety
At a median follow-up of 39.9 months, the median overall survival was 28.9 months in the FOLFOXIRI group and 24.5 months in the doublet group (P < .001). The estimated 5-year overall survival rate was 22.3% and 10.7%, respectively.
The median progression-free survival was 12.2 months in the FOLFOXIRI group and 9.9 months in the doublet group (P < .001).
The objective response rate was higher with FOLFOXIRI (64.5% vs. 53.6%, P < .001), as was R0 resection rate (16.4% vs. 11.8%, P = .007).
The FOLFOXIRI group also had a higher incidence of grade 3-4 adverse events, including neutropenia (45.8% vs. 21.5%; P < .001), febrile neutropenia (6.3% vs. 3.7%; P = .019), nausea (5.5% vs. 3.0%; P = .016), mucositis (5.1% vs. 2.9%; P = .024), and diarrhea (17.8% vs. 8.4%; P < .001).
Even so, FOLFOXIRI plus bevacizumab was not associated with a significant increase in toxic deaths (2.3% vs. 1.4%; P = .277).
Patient selection is ‘critical’
Based on their findings, the investigators said the best candidates for first-line FOLFOXIRI plus bevacizumab may be younger patients with an ECOG performance status of 0 or 1 and right-sided and/or RAS-mutated tumors not exposed to a previous oxaliplatin-based adjuvant regimen.
FOLFOXIRI plus bevacizumab did not provide any additional benefit in patients with BRAF-mutant tumors, so the combination shouldn’t be the first choice in this group, the investigators wrote. “FOLFOX plus bevacizumab seems the preferable upfront option.”
For left-sided RAS and BRAF wild-type tumors, a chemotherapy doublet with an anti–epidermal growth factor receptor remains the preferred option, according to the investigators.
“The study does support the use of FOLFOXIRI and bevacizumab as a valuable first-line option, but patient selection is critical because there is a toxicity cost; this efficacy versus toxicity will constantly be a seesaw for us,” commented Aparna Parikh, MD, of Massachusetts General Hospital in Boston, when the study was presented at the American Society of Clinical Oncology annual meeting earlier this year.
There was no external funding for this analysis. Three of the original five trials were sponsored by Roche. The study authors had numerous industry ties. Among others, Dr. Cremolini is a consultant for and reported honoraria and travel expenses from Roche. One author was a Genentech employee. Dr. Parikh disclosed relationships with Lilly, Genentech, and other companies.
SOURCE: Cremolini C et al. J Clin Oncol. 2020 Aug 20. doi: 10.1200/JCO.20.01225.
investigators reported in the Journal of Clinical Oncology.
In analyzing data from five clinical trials, the investigators found a 4.4-month increase in median overall survival and an 11.6% increase in estimated 5-year overall survival with FOLFOXIRI versus doublets. The trade-off was a higher incidence of grade 3-4 adverse events with FOLFOXIRI.
FOLFOXIRI plus bevacizumab is already included among first-line options in most clinical guidelines and recommendations, but there was no “proper estimation of the magnitude of the overall survival benefit” because trials had other primary endpoints, according to study author Chiara Cremolini, MD, PhD, of University of Pisa (Italy), and colleagues.
“To fully appreciate the cost/benefit balance of this option,” the investigators wanted to see how the numbers played out when overall survival was the primary endpoint, so they pooled individual patient data from the CHARTA, OLIVIA, STEAM, TRIBE, and TRIBE2 trials.
Patient characteristics and treatment
The analysis included 1,697 patients. The median age was 61 years (range, 53-67 years).
About 99% of patients had an Eastern Cooperative Oncology Group performance score of 0 or 1. About 20% had left-sided RAS and BRAF wild-type tumors because of the increased use of anti–epidermal growth factor receptor antibodies as first-line therapy for that indication in recent years.
In all, 846 patients were randomized to FOLFOXIRI plus bevacizumab and 851 to bevacizumab with doublets: 69.9% to FOLFOX (leucovorin, fluorouracil, and oxaliplatin) and 30.1% to FOLFIRI (fluorouracil, leucovorin, and irinotecan).
The duration of induction in all five trials ranged from 4 to 6 months. It was followed by maintenance with a fluoropyrimidine (fluorouracil and leucovorin or capecitabine) plus bevacizumab.
Efficacy and safety
At a median follow-up of 39.9 months, the median overall survival was 28.9 months in the FOLFOXIRI group and 24.5 months in the doublet group (P < .001). The estimated 5-year overall survival rate was 22.3% and 10.7%, respectively.
The median progression-free survival was 12.2 months in the FOLFOXIRI group and 9.9 months in the doublet group (P < .001).
The objective response rate was higher with FOLFOXIRI (64.5% vs. 53.6%, P < .001), as was R0 resection rate (16.4% vs. 11.8%, P = .007).
The FOLFOXIRI group also had a higher incidence of grade 3-4 adverse events, including neutropenia (45.8% vs. 21.5%; P < .001), febrile neutropenia (6.3% vs. 3.7%; P = .019), nausea (5.5% vs. 3.0%; P = .016), mucositis (5.1% vs. 2.9%; P = .024), and diarrhea (17.8% vs. 8.4%; P < .001).
Even so, FOLFOXIRI plus bevacizumab was not associated with a significant increase in toxic deaths (2.3% vs. 1.4%; P = .277).
Patient selection is ‘critical’
Based on their findings, the investigators said the best candidates for first-line FOLFOXIRI plus bevacizumab may be younger patients with an ECOG performance status of 0 or 1 and right-sided and/or RAS-mutated tumors not exposed to a previous oxaliplatin-based adjuvant regimen.
FOLFOXIRI plus bevacizumab did not provide any additional benefit in patients with BRAF-mutant tumors, so the combination shouldn’t be the first choice in this group, the investigators wrote. “FOLFOX plus bevacizumab seems the preferable upfront option.”
For left-sided RAS and BRAF wild-type tumors, a chemotherapy doublet with an anti–epidermal growth factor receptor remains the preferred option, according to the investigators.
“The study does support the use of FOLFOXIRI and bevacizumab as a valuable first-line option, but patient selection is critical because there is a toxicity cost; this efficacy versus toxicity will constantly be a seesaw for us,” commented Aparna Parikh, MD, of Massachusetts General Hospital in Boston, when the study was presented at the American Society of Clinical Oncology annual meeting earlier this year.
There was no external funding for this analysis. Three of the original five trials were sponsored by Roche. The study authors had numerous industry ties. Among others, Dr. Cremolini is a consultant for and reported honoraria and travel expenses from Roche. One author was a Genentech employee. Dr. Parikh disclosed relationships with Lilly, Genentech, and other companies.
SOURCE: Cremolini C et al. J Clin Oncol. 2020 Aug 20. doi: 10.1200/JCO.20.01225.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Exorcising your ghosts
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.

If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.
If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.
If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.

For lower-risk MDS, treat ‘what bugs patients most’
Clinicians who treat patients with lower-risk myelodysplastic syndrome should focus on “what bugs patients most,” with therapeutic goals reflecting and respecting the patients’ goals, a specialist in MDS recommended.
“There’s an uncomfortable truth in treating lower-risk MDS: No treatment that we have has ever been demonstrated in a prospective trial to prolong survival in lower-risk MDS, so in the end, what we’re doing is trying to improve transfusion needs and to improve quality of life,” said Michael A. Sekeres, MD, MS, from the Cleveland Clinic.
Dr. Sekeres described optimal therapy for patients with lower-risk MDS in an online presentation during the virtual American Society of Hematology Meeting on Hematologic Malignancies.
He acknowledged that the definition of MDS as “a heterogeneous clonal hematopoietic disorder derived from an abnormal multipotent progenitor cell, characterized by a hyperproliferative bone marrow, dysplasia of the cellular elements, and ineffective hematopoiesis” can be confusing even for hematologists well versed in the disorder.
An easier-to-grasp explanation, he said, is that “MDS is considered a cancer, and like other cancers it has a clonal origin, involves the abnormal growth of cells that exceeds the growth of other cells around them and don’t know when to stop growing, and it takes over normal tissue, so that the normal tissues – in this case the hematopoietic precursors in the bone marrow – don’t function normally, resulting in cytopenias.”
‘Mild displeasure syndrome’
Approximately 95% of patients with MDS have a discrete genetic abnormality, but only one driver mutation, in the gene SF3B1, is considered to be a lower-risk abnormality, with a more favorable prognosis.
Treatment options for patients with lower-risk MDS, defined as an International Prognostic Scoring System score of 1 or less, or a Revised IPSS score of 3.5 or less, will depend on the patients’ transfusion needs and quality of life.
Patients with no transfusion requirements and a generally good quality of life may be followed by observation alone, with blood counts every 1 to 6 months depending on clinical presentation.
“We have some folks coming in who really don’t have very bad blood counts and have a good quality of life,” Dr. Sekeres said. “Those folks we would consider to have a very good risk type of MDS, which one of my patients referred to once as ‘mild displeasure syndrome.’ It was a displeasure to him to have to fight the traffic to come into Cleveland to see me every month, or 2 months, or 6 months, but beyond that we didn’t have to treat his MDS.”
Isolated cytopenias
Patients with isolated anemia, with hemoglobin less than 10 g/dL and/or transfusion dependence, and who are symptomatic should be started on an erythopoiesis-stimulating agent (ESA), either recombinant humanized erythropoietin or darbepoetin, or the erythroid-maturing agent luspatercept (Reblozyl).
The probability of a response to ESAs in this populations ranges from about 15% to 35%, with patients who have low baseline serum erythropoietin and no or few transfusions most likely to respond.
“On the other hand, patients who come into our clinic who are already dependent on red blood cell transfusions and have a sky-high [erythropoietin] level in the hundreds or even thousands have a very low likelihood of responding to exogenously administered ESAs,” he said.
Patients with no response to ESAs or luspatercept or a loss of response suggestive of disease progression should undergo repeat bone marrow biopsy. Patients who develop deletion 5q should be started on lenalidomide (Revlimid). In these patients, next-generation sequencing may also reveal targetable abnormalities.
For patients with isolated thrombocytopenia, thrombopoietin agonists such as romiplostim or eltrombopag may help to reduce platelet transfusion requirements and clinically significant bleeding events, but these agents come with a very important caveat: in addition to promoting platelet production, thrombopoietin receptor agonists can promote the growth of blasts, which could in turn promote the transformation of MDS to acute myeloid leukemia.
“This is an off-label use of romiplostim for the treatment of MDS with thrombocytopenia, and this drug should never, never, never be given to a patient who has excess blasts at baseline MDS; the same is true of its cousin eltrombopag.” Dr. Sekeres said.
Multlineage dysplasia
Patients with multilineage dysplasia can have good responses to hypomethylating agents, either azacitidine 75 mg/m2 IV or subcutaneously for 3 days every 4 weeks, or decitabine 20 mg/m2 IV for 3 days every 4 weeks.
“Another approach to treating patients with multilineage dysplasia is to consider the use of antithymocyte globulin; in other words, treat these patients as if they have aplastic anemia, because there are some types of MDS in which immune-mediated destruction of bone marrow plays a role,” Dr. Sekeres said.
“This is particularly appealing in patients who have a hyperplastic marrow, or those who have other autoimmune conditions that are going on that may indicate a broader autoimmune process that’s involved in the bone marrow,” he added.
Patients treated with antithymocyte globulin require hospitalization with discharge on steroids for 1 month to prevent serum sickness in response to the treatment, and maintenance on low-dose cyclosporine.
“In MDS, unfortunately, our understanding of the biology of the disease far exceeds what we can do about it, but we’re starting to catch up,” Dr. Sekeres said.
No funding source for the presentation was disclosed. Dr. Sekeres disclosed serving on advisory boards for Celegene/Bristol-Myers Squibb, Takeda/Millenium, and Pfizer.
Clinicians who treat patients with lower-risk myelodysplastic syndrome should focus on “what bugs patients most,” with therapeutic goals reflecting and respecting the patients’ goals, a specialist in MDS recommended.
“There’s an uncomfortable truth in treating lower-risk MDS: No treatment that we have has ever been demonstrated in a prospective trial to prolong survival in lower-risk MDS, so in the end, what we’re doing is trying to improve transfusion needs and to improve quality of life,” said Michael A. Sekeres, MD, MS, from the Cleveland Clinic.
Dr. Sekeres described optimal therapy for patients with lower-risk MDS in an online presentation during the virtual American Society of Hematology Meeting on Hematologic Malignancies.
He acknowledged that the definition of MDS as “a heterogeneous clonal hematopoietic disorder derived from an abnormal multipotent progenitor cell, characterized by a hyperproliferative bone marrow, dysplasia of the cellular elements, and ineffective hematopoiesis” can be confusing even for hematologists well versed in the disorder.
An easier-to-grasp explanation, he said, is that “MDS is considered a cancer, and like other cancers it has a clonal origin, involves the abnormal growth of cells that exceeds the growth of other cells around them and don’t know when to stop growing, and it takes over normal tissue, so that the normal tissues – in this case the hematopoietic precursors in the bone marrow – don’t function normally, resulting in cytopenias.”
‘Mild displeasure syndrome’
Approximately 95% of patients with MDS have a discrete genetic abnormality, but only one driver mutation, in the gene SF3B1, is considered to be a lower-risk abnormality, with a more favorable prognosis.
Treatment options for patients with lower-risk MDS, defined as an International Prognostic Scoring System score of 1 or less, or a Revised IPSS score of 3.5 or less, will depend on the patients’ transfusion needs and quality of life.
Patients with no transfusion requirements and a generally good quality of life may be followed by observation alone, with blood counts every 1 to 6 months depending on clinical presentation.
“We have some folks coming in who really don’t have very bad blood counts and have a good quality of life,” Dr. Sekeres said. “Those folks we would consider to have a very good risk type of MDS, which one of my patients referred to once as ‘mild displeasure syndrome.’ It was a displeasure to him to have to fight the traffic to come into Cleveland to see me every month, or 2 months, or 6 months, but beyond that we didn’t have to treat his MDS.”
Isolated cytopenias
Patients with isolated anemia, with hemoglobin less than 10 g/dL and/or transfusion dependence, and who are symptomatic should be started on an erythopoiesis-stimulating agent (ESA), either recombinant humanized erythropoietin or darbepoetin, or the erythroid-maturing agent luspatercept (Reblozyl).
The probability of a response to ESAs in this populations ranges from about 15% to 35%, with patients who have low baseline serum erythropoietin and no or few transfusions most likely to respond.
“On the other hand, patients who come into our clinic who are already dependent on red blood cell transfusions and have a sky-high [erythropoietin] level in the hundreds or even thousands have a very low likelihood of responding to exogenously administered ESAs,” he said.
Patients with no response to ESAs or luspatercept or a loss of response suggestive of disease progression should undergo repeat bone marrow biopsy. Patients who develop deletion 5q should be started on lenalidomide (Revlimid). In these patients, next-generation sequencing may also reveal targetable abnormalities.
For patients with isolated thrombocytopenia, thrombopoietin agonists such as romiplostim or eltrombopag may help to reduce platelet transfusion requirements and clinically significant bleeding events, but these agents come with a very important caveat: in addition to promoting platelet production, thrombopoietin receptor agonists can promote the growth of blasts, which could in turn promote the transformation of MDS to acute myeloid leukemia.
“This is an off-label use of romiplostim for the treatment of MDS with thrombocytopenia, and this drug should never, never, never be given to a patient who has excess blasts at baseline MDS; the same is true of its cousin eltrombopag.” Dr. Sekeres said.
Multlineage dysplasia
Patients with multilineage dysplasia can have good responses to hypomethylating agents, either azacitidine 75 mg/m2 IV or subcutaneously for 3 days every 4 weeks, or decitabine 20 mg/m2 IV for 3 days every 4 weeks.
“Another approach to treating patients with multilineage dysplasia is to consider the use of antithymocyte globulin; in other words, treat these patients as if they have aplastic anemia, because there are some types of MDS in which immune-mediated destruction of bone marrow plays a role,” Dr. Sekeres said.
“This is particularly appealing in patients who have a hyperplastic marrow, or those who have other autoimmune conditions that are going on that may indicate a broader autoimmune process that’s involved in the bone marrow,” he added.
Patients treated with antithymocyte globulin require hospitalization with discharge on steroids for 1 month to prevent serum sickness in response to the treatment, and maintenance on low-dose cyclosporine.
“In MDS, unfortunately, our understanding of the biology of the disease far exceeds what we can do about it, but we’re starting to catch up,” Dr. Sekeres said.
No funding source for the presentation was disclosed. Dr. Sekeres disclosed serving on advisory boards for Celegene/Bristol-Myers Squibb, Takeda/Millenium, and Pfizer.
Clinicians who treat patients with lower-risk myelodysplastic syndrome should focus on “what bugs patients most,” with therapeutic goals reflecting and respecting the patients’ goals, a specialist in MDS recommended.
“There’s an uncomfortable truth in treating lower-risk MDS: No treatment that we have has ever been demonstrated in a prospective trial to prolong survival in lower-risk MDS, so in the end, what we’re doing is trying to improve transfusion needs and to improve quality of life,” said Michael A. Sekeres, MD, MS, from the Cleveland Clinic.
Dr. Sekeres described optimal therapy for patients with lower-risk MDS in an online presentation during the virtual American Society of Hematology Meeting on Hematologic Malignancies.
He acknowledged that the definition of MDS as “a heterogeneous clonal hematopoietic disorder derived from an abnormal multipotent progenitor cell, characterized by a hyperproliferative bone marrow, dysplasia of the cellular elements, and ineffective hematopoiesis” can be confusing even for hematologists well versed in the disorder.
An easier-to-grasp explanation, he said, is that “MDS is considered a cancer, and like other cancers it has a clonal origin, involves the abnormal growth of cells that exceeds the growth of other cells around them and don’t know when to stop growing, and it takes over normal tissue, so that the normal tissues – in this case the hematopoietic precursors in the bone marrow – don’t function normally, resulting in cytopenias.”
‘Mild displeasure syndrome’
Approximately 95% of patients with MDS have a discrete genetic abnormality, but only one driver mutation, in the gene SF3B1, is considered to be a lower-risk abnormality, with a more favorable prognosis.
Treatment options for patients with lower-risk MDS, defined as an International Prognostic Scoring System score of 1 or less, or a Revised IPSS score of 3.5 or less, will depend on the patients’ transfusion needs and quality of life.
Patients with no transfusion requirements and a generally good quality of life may be followed by observation alone, with blood counts every 1 to 6 months depending on clinical presentation.
“We have some folks coming in who really don’t have very bad blood counts and have a good quality of life,” Dr. Sekeres said. “Those folks we would consider to have a very good risk type of MDS, which one of my patients referred to once as ‘mild displeasure syndrome.’ It was a displeasure to him to have to fight the traffic to come into Cleveland to see me every month, or 2 months, or 6 months, but beyond that we didn’t have to treat his MDS.”
Isolated cytopenias
Patients with isolated anemia, with hemoglobin less than 10 g/dL and/or transfusion dependence, and who are symptomatic should be started on an erythopoiesis-stimulating agent (ESA), either recombinant humanized erythropoietin or darbepoetin, or the erythroid-maturing agent luspatercept (Reblozyl).
The probability of a response to ESAs in this populations ranges from about 15% to 35%, with patients who have low baseline serum erythropoietin and no or few transfusions most likely to respond.
“On the other hand, patients who come into our clinic who are already dependent on red blood cell transfusions and have a sky-high [erythropoietin] level in the hundreds or even thousands have a very low likelihood of responding to exogenously administered ESAs,” he said.
Patients with no response to ESAs or luspatercept or a loss of response suggestive of disease progression should undergo repeat bone marrow biopsy. Patients who develop deletion 5q should be started on lenalidomide (Revlimid). In these patients, next-generation sequencing may also reveal targetable abnormalities.
For patients with isolated thrombocytopenia, thrombopoietin agonists such as romiplostim or eltrombopag may help to reduce platelet transfusion requirements and clinically significant bleeding events, but these agents come with a very important caveat: in addition to promoting platelet production, thrombopoietin receptor agonists can promote the growth of blasts, which could in turn promote the transformation of MDS to acute myeloid leukemia.
“This is an off-label use of romiplostim for the treatment of MDS with thrombocytopenia, and this drug should never, never, never be given to a patient who has excess blasts at baseline MDS; the same is true of its cousin eltrombopag.” Dr. Sekeres said.
Multlineage dysplasia
Patients with multilineage dysplasia can have good responses to hypomethylating agents, either azacitidine 75 mg/m2 IV or subcutaneously for 3 days every 4 weeks, or decitabine 20 mg/m2 IV for 3 days every 4 weeks.
“Another approach to treating patients with multilineage dysplasia is to consider the use of antithymocyte globulin; in other words, treat these patients as if they have aplastic anemia, because there are some types of MDS in which immune-mediated destruction of bone marrow plays a role,” Dr. Sekeres said.
“This is particularly appealing in patients who have a hyperplastic marrow, or those who have other autoimmune conditions that are going on that may indicate a broader autoimmune process that’s involved in the bone marrow,” he added.
Patients treated with antithymocyte globulin require hospitalization with discharge on steroids for 1 month to prevent serum sickness in response to the treatment, and maintenance on low-dose cyclosporine.
“In MDS, unfortunately, our understanding of the biology of the disease far exceeds what we can do about it, but we’re starting to catch up,” Dr. Sekeres said.
No funding source for the presentation was disclosed. Dr. Sekeres disclosed serving on advisory boards for Celegene/Bristol-Myers Squibb, Takeda/Millenium, and Pfizer.
FROM ASH HEMATOLOGIC MALIGNANCIES 2020
Studying in Dermatology Residency
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
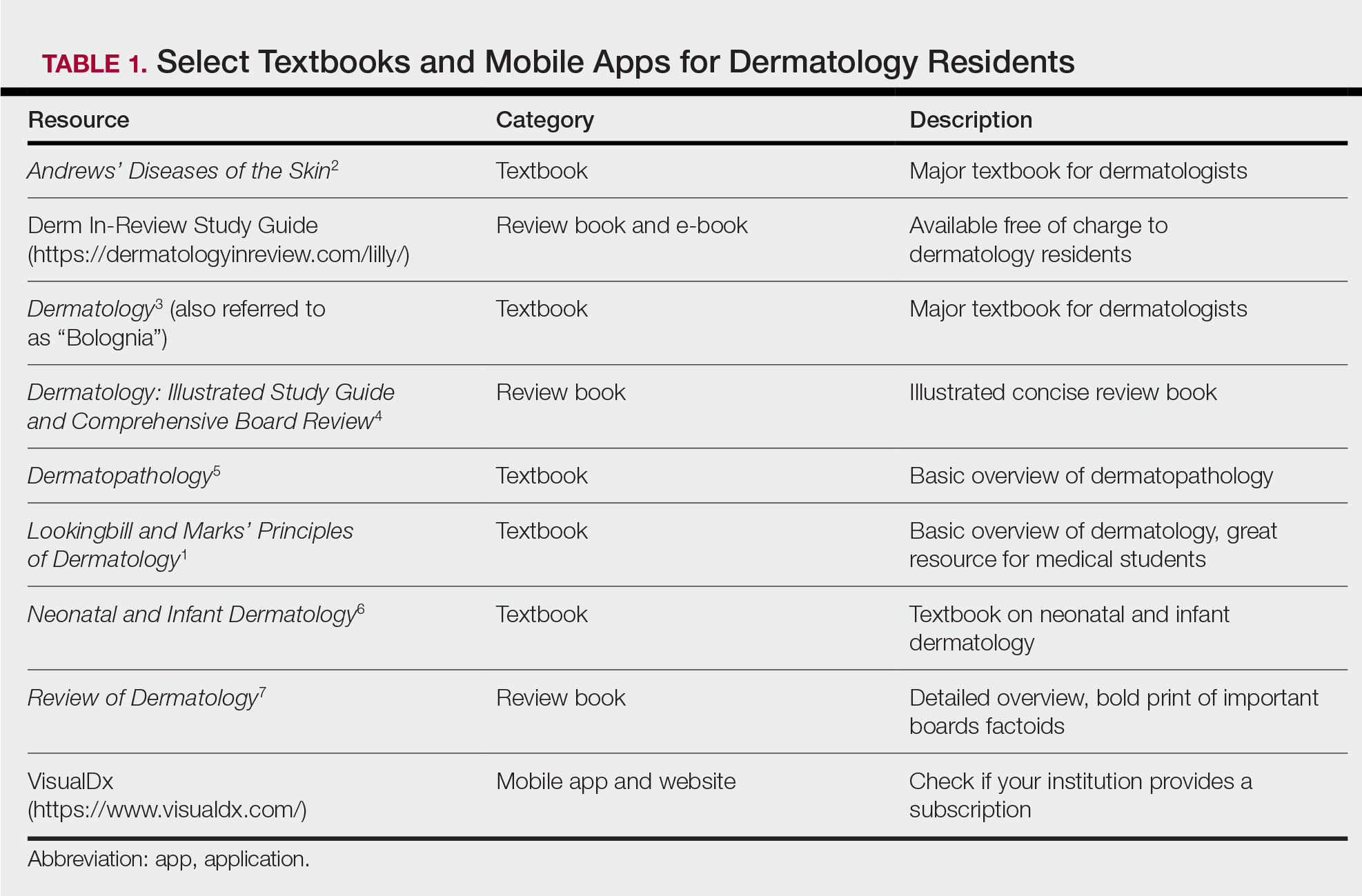
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
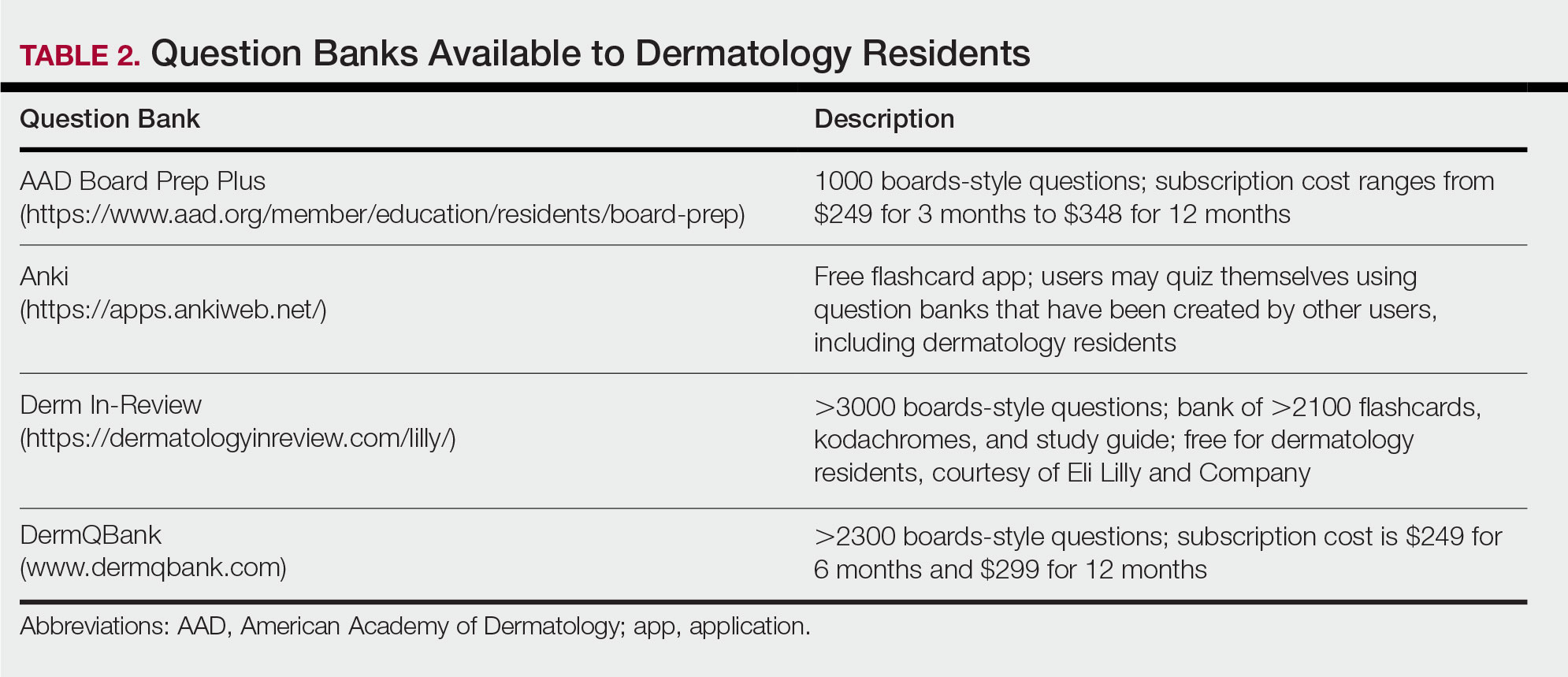
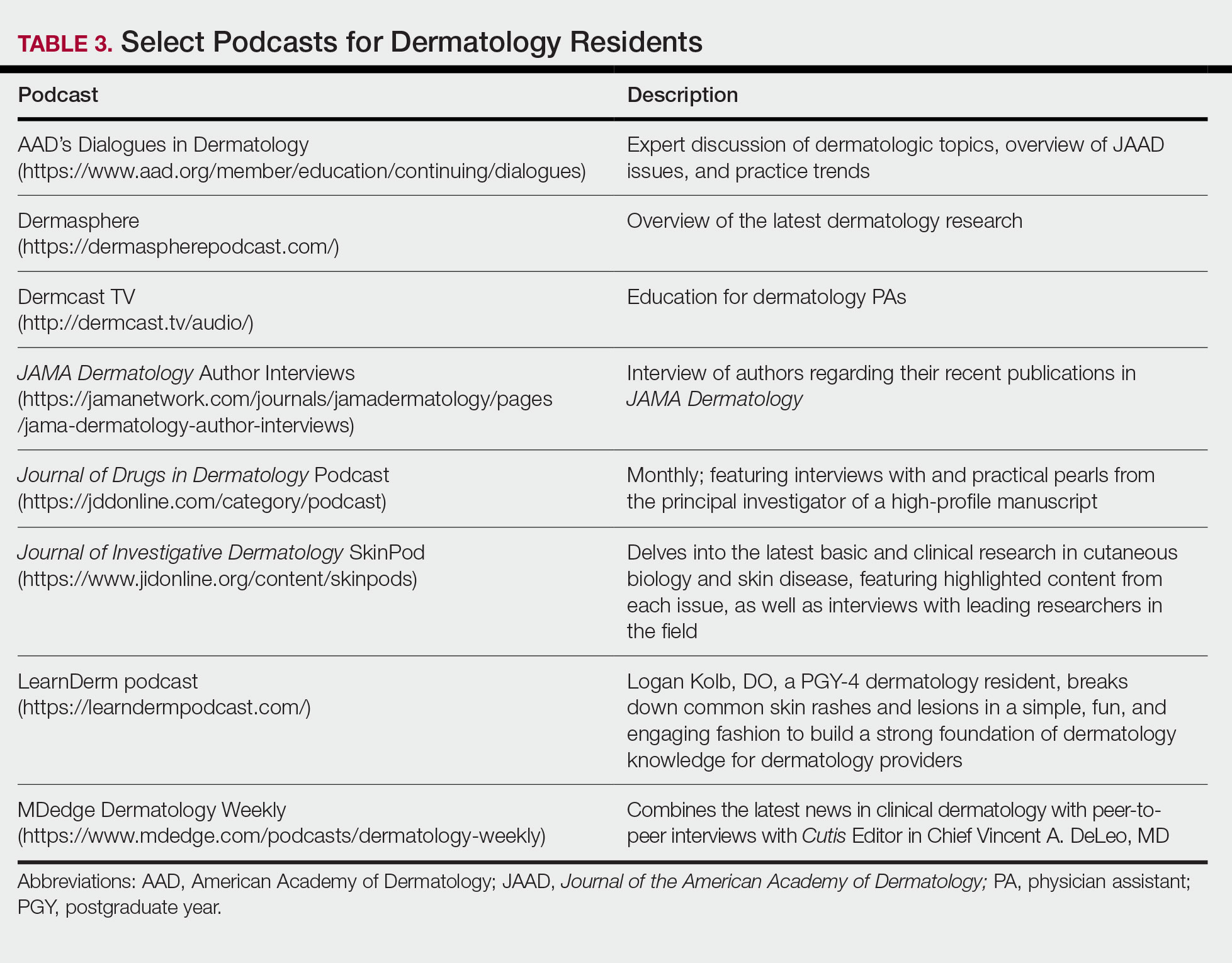
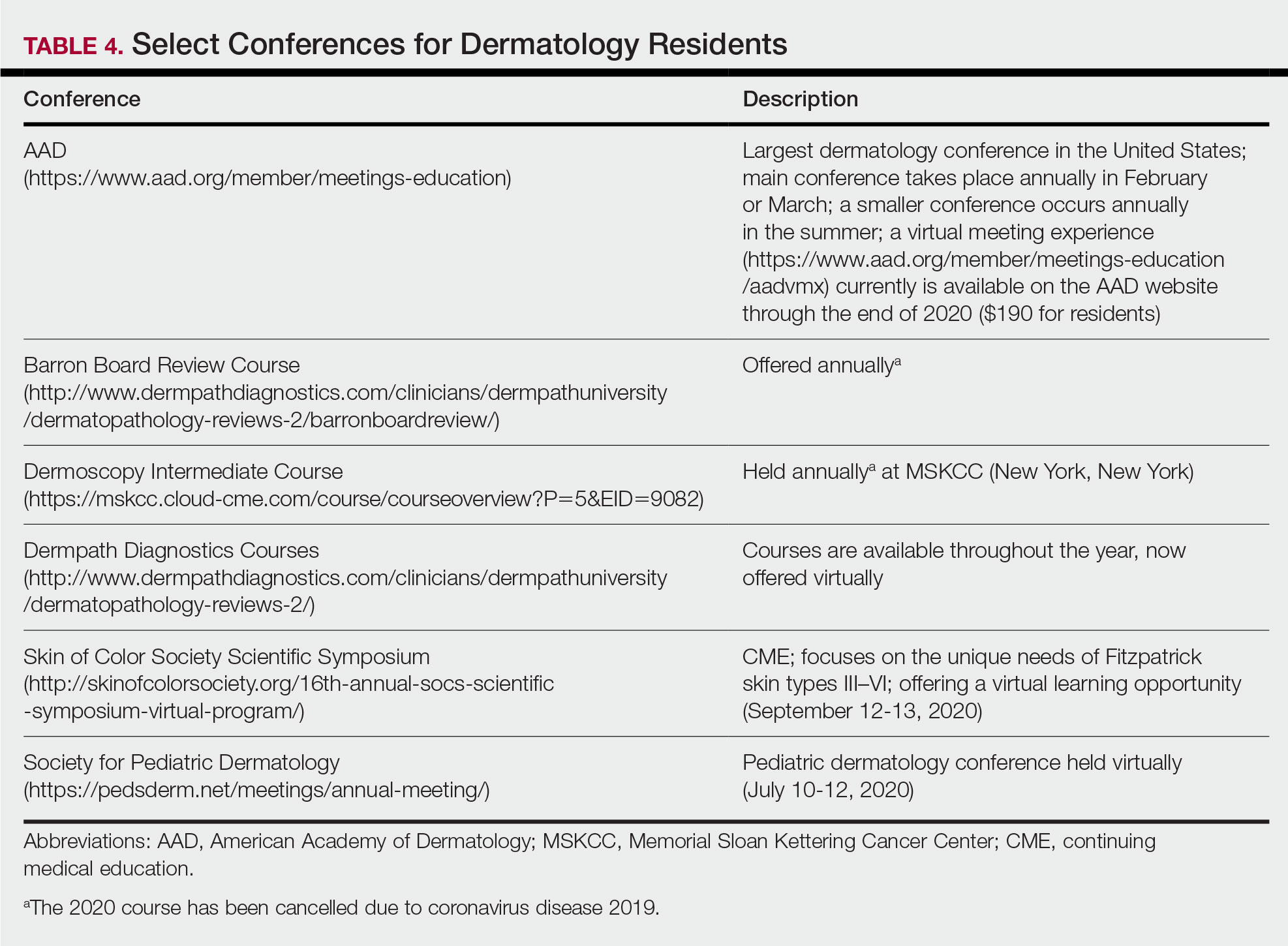
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
Resident Pearls
- Independent study is a large component of dermatology residency.
- Consistent habits and a tailored approach will support optimal learning for each dermatology resident.
- The beginning of residency is a good time to explore a variety of resources to see what works best. Toward the end of residency, as studying becomes more targeted, residents may benefit from sticking to the resources with which they are most comfortable.

Dystrophic Calcinosis Cutis: Treatment With Intravenous Sodium Thiosulfate
To the Editor:
Severe dystrophic calcinosis cutis is a debilitating disease with no universally accepted therapeutic options. This case demonstrates the benefit of intravenous (IV) sodium thiosulfate in alleviating the calcified lesions as well as the associated pain and disability. This application of IV sodium thiosulfate with a favorable outcome is new and should be considered for the treatment of generalized dystrophic calcinosis cutis, especially when topical, procedural, or surgical options are not feasible.
A 54-year-old woman with a history of well-controlled dermatomyositis and systemic lupus erythematosus presented with diffuse, hard, calcified lesions on the legs, arms, clavicular region, and neck that had slowly progressed over at least a 10-year period (Figure 1). The lesions were consistent with dystrophic calcinosis cutis. The patient was started on 12.5 g of IV sodium thiosulfate 3 times weekly infused over 30 minutes. Drastic diminution of the cutaneous calcification was observed at 3-month follow-up (Figure 2). She reported decreased pain and burning as well as increased overall functionality and improved sleep. The patient completed 8 months of therapy, but the treatment was stopped secondary to suspicion of a lupuslike flare, and the lesions recurred with more widespread involvement, including the trunk, tendons, bony prominences, and supraclavicular soft tissue. The patient reported burning pain and pruritus that resulted in impairment of daily activities such as getting dressed. Sodium thiosulfate was restarted once weekly, which again resulted in reduction of the dystrophic calcinosis cutis.
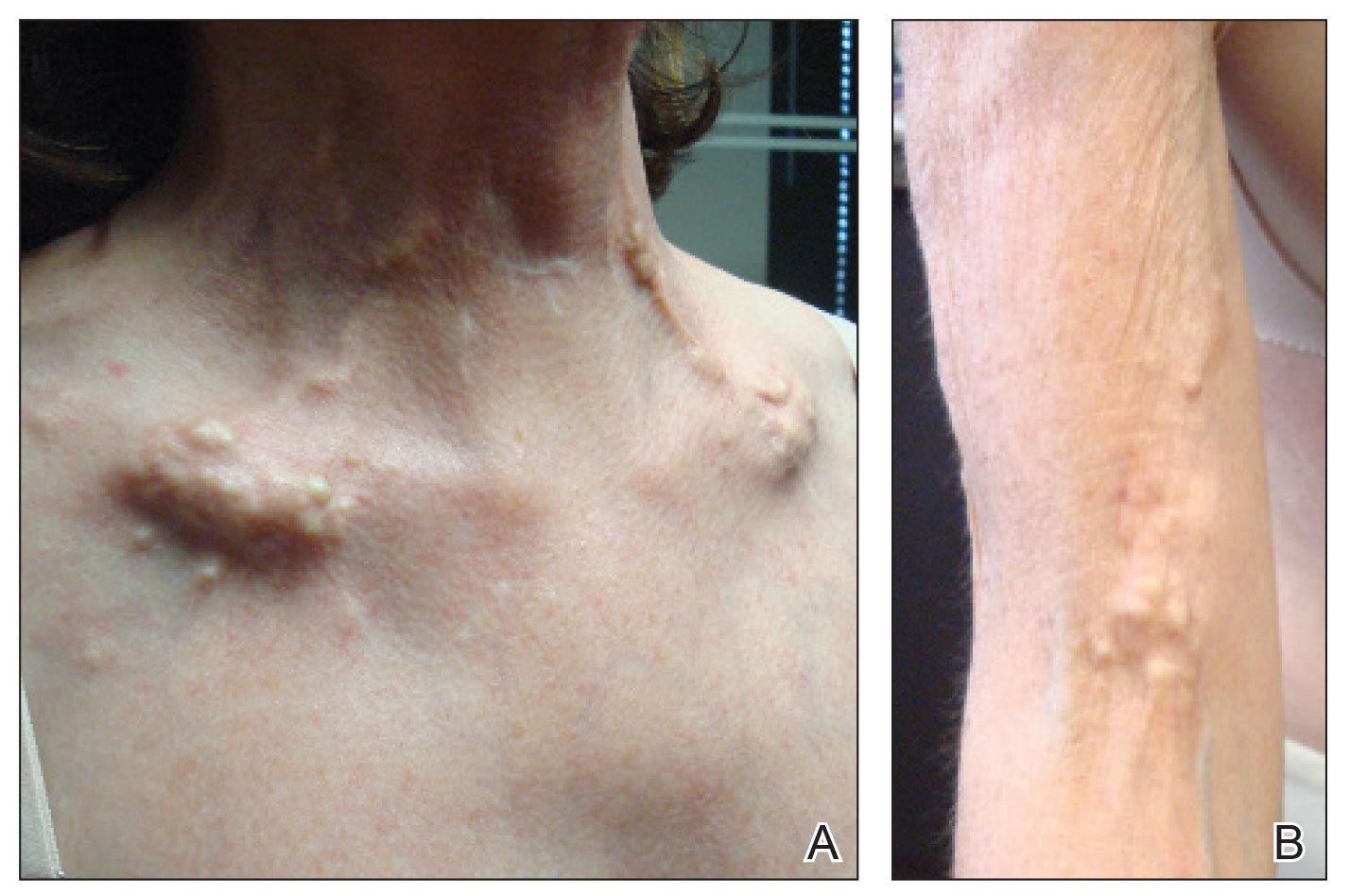
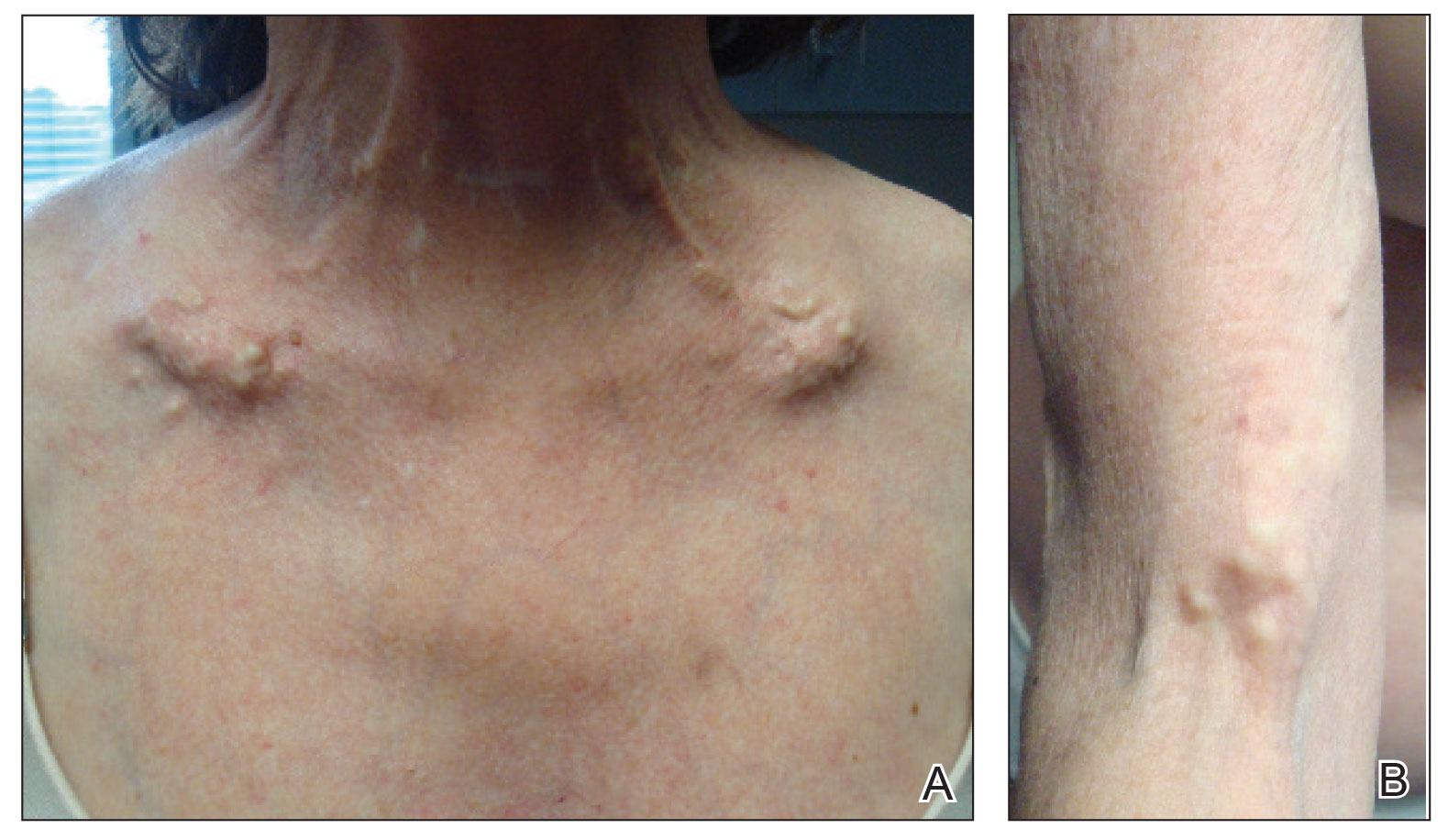
Dystrophic calcinosis cutis is a debilitating disease that results in considerable morbidity and pain with major implications on quality of life. The pathophysiology is unclear; calcium and phosphate serum levels generally are normal. A proposed mechanism is that chronic inflammation causes tissue damage and defective collagen synthesis, resulting in a distorted architecture that facilitates calcium deposition in the skin and subcutaneous tissues.1 Dystrophic calcinosis cutis most commonly is associated with systemic sclerosis and dermatomyositis but also can be seen in systemic lupus erythematosus, panniculitis, and other connective tissue diseases. It also can occur with skin neoplasms, collagen and elastin disorders, porphyria cutanea tarda, and pancreatic panniculitis.1 Progression of dystrophic calcinosis cutis usually is independent of the associated disease status.
Treatment is based on anecdotal evidence from case reports, as there is no universally accepted pharmacologic or procedural intervention available for dystrophic calcinosis cutis. Medications that have been reported to be helpful to varying degrees include diltiazem, colchicine, minocycline, IV immunoglobulin, ceftriaxone, aluminum hydroxide, probenecid, alendronic acid, etidronate disodium, warfarin, intralesional corticosteroids, and sodium thiosulfate. Procedural interventions also have been reported, such as surgical excision, extracorporeal shock wave lithotripsy, and CO2 and erbium: YAG lasers.1 Surgical excision of dystrophic calcinosis cutis is widely implemented but outcomes are poor. Moreover, in patients with widely diffuse calcinosis, targeted procedural therapy is impractical.
Intravenous sodium thiosulfate has been widely used for the treatment of calciphylaxis secondary to end-stage renal failure and tumoral calcinosis.2 It also has been reported to be effective in iatrogenic calcinosis cutis secondary to extravasation of calcium-containing solutions in a patient with T-cell acute lymphoblastic leukemia.3 However, reports of its use in treating dystrophic calcinosis cutis are limited. Intravenous sodium thiosulfate—10 g 3 times weekly for 2 weeks, followed by 15 g twice weekly for the next 3 months—was used with abatacept for treatment of dystrophic calcinosis cutis in a patient with juvenile dermatomyositis.4 Other formulations of sodium thiosulfate have been reported to result in clearance of calcified lesions, including a topical application compounded in zinc oxide5 and intradermal injection at the base of a nodule.6 We used 12.5 g over 30 minutes 3 times weekly; however, the dose can be increased to 25 g over 60 minutes if 3 to 4 treatments are tolerated, with nausea being the only notable side effect. Its mechanism of action in treating dystrophic calcinosis cutis is unclear, but it likely is due to its ability to chelate and dissolve calcium deposits. Topical and intradermal therapy is impractical for widespread, dystrophic calcinosis cutis as in our patient.
Our case highlights the successful use of IV sodium thiosulfate as a stand-alone treatment modality for generalized dystrophic calcinosis cutis in an adult patient. Both our patient and a child in a previously reported case who received the same treatment4 had dermatomyositis, but we suspect IV sodium thiosulfate also may be effective for dystrophic calcinosis cutis associated with other diseases. Sodium thiosulfate should be considered as a treatment for patients who experience tremendous pain and disability. It is safe, inexpensive, and easy to administer and is especially helpful in patients for whom topical, intradermal, or procedural therapy is not possible.
- Gutierrez A Jr, Wetter DA. Calcinosis cutis in autoimmune connective tissue diseases. Dermatol Ther. 2012;25:195-206.
- Mageau A, Guigonis V, Ratzimbasafy V, et al. Intravenous sodium thiosulfate for treating tumoral calcinosis associated with systemic disorders: report of four cases. Joint Bone Spine. 2017;84:341-344.
Raffaella C, Annapaola C, Tullio I, et al. Successful treatment of severe iatrogenic calcinosis cutis with intravenous sodium thiosulfate in a child affected by T-acute lymphoblastic leukemia. Pediatr Dermatol. 2009;26:311-315. - Arabshahi B, Silverman RA, Jones OY, et al. Abatacept and sodium thiosulfate for treatment of recalcitrant juvenile dermatomyositis complicated by ulceration and calcinosis. J Pediatrics. 2012;160:520-522.
- Bair B, Fivenson D. A novel treatment for ulcerative calcinosis cutis. J Drugs Dermatol. 2011;10:1042-1044.
- Smith GP. Intradermal sodium thiosulfate for exophytic calcinosis cutis of connective tissue disease. J Am Acad Dermatol. 2013;69:E146-E147.
To the Editor:
Severe dystrophic calcinosis cutis is a debilitating disease with no universally accepted therapeutic options. This case demonstrates the benefit of intravenous (IV) sodium thiosulfate in alleviating the calcified lesions as well as the associated pain and disability. This application of IV sodium thiosulfate with a favorable outcome is new and should be considered for the treatment of generalized dystrophic calcinosis cutis, especially when topical, procedural, or surgical options are not feasible.
A 54-year-old woman with a history of well-controlled dermatomyositis and systemic lupus erythematosus presented with diffuse, hard, calcified lesions on the legs, arms, clavicular region, and neck that had slowly progressed over at least a 10-year period (Figure 1). The lesions were consistent with dystrophic calcinosis cutis. The patient was started on 12.5 g of IV sodium thiosulfate 3 times weekly infused over 30 minutes. Drastic diminution of the cutaneous calcification was observed at 3-month follow-up (Figure 2). She reported decreased pain and burning as well as increased overall functionality and improved sleep. The patient completed 8 months of therapy, but the treatment was stopped secondary to suspicion of a lupuslike flare, and the lesions recurred with more widespread involvement, including the trunk, tendons, bony prominences, and supraclavicular soft tissue. The patient reported burning pain and pruritus that resulted in impairment of daily activities such as getting dressed. Sodium thiosulfate was restarted once weekly, which again resulted in reduction of the dystrophic calcinosis cutis.
Dystrophic calcinosis cutis is a debilitating disease that results in considerable morbidity and pain with major implications on quality of life. The pathophysiology is unclear; calcium and phosphate serum levels generally are normal. A proposed mechanism is that chronic inflammation causes tissue damage and defective collagen synthesis, resulting in a distorted architecture that facilitates calcium deposition in the skin and subcutaneous tissues.1 Dystrophic calcinosis cutis most commonly is associated with systemic sclerosis and dermatomyositis but also can be seen in systemic lupus erythematosus, panniculitis, and other connective tissue diseases. It also can occur with skin neoplasms, collagen and elastin disorders, porphyria cutanea tarda, and pancreatic panniculitis.1 Progression of dystrophic calcinosis cutis usually is independent of the associated disease status.
Treatment is based on anecdotal evidence from case reports, as there is no universally accepted pharmacologic or procedural intervention available for dystrophic calcinosis cutis. Medications that have been reported to be helpful to varying degrees include diltiazem, colchicine, minocycline, IV immunoglobulin, ceftriaxone, aluminum hydroxide, probenecid, alendronic acid, etidronate disodium, warfarin, intralesional corticosteroids, and sodium thiosulfate. Procedural interventions also have been reported, such as surgical excision, extracorporeal shock wave lithotripsy, and CO2 and erbium: YAG lasers.1 Surgical excision of dystrophic calcinosis cutis is widely implemented but outcomes are poor. Moreover, in patients with widely diffuse calcinosis, targeted procedural therapy is impractical.
Intravenous sodium thiosulfate has been widely used for the treatment of calciphylaxis secondary to end-stage renal failure and tumoral calcinosis.2 It also has been reported to be effective in iatrogenic calcinosis cutis secondary to extravasation of calcium-containing solutions in a patient with T-cell acute lymphoblastic leukemia.3 However, reports of its use in treating dystrophic calcinosis cutis are limited. Intravenous sodium thiosulfate—10 g 3 times weekly for 2 weeks, followed by 15 g twice weekly for the next 3 months—was used with abatacept for treatment of dystrophic calcinosis cutis in a patient with juvenile dermatomyositis.4 Other formulations of sodium thiosulfate have been reported to result in clearance of calcified lesions, including a topical application compounded in zinc oxide5 and intradermal injection at the base of a nodule.6 We used 12.5 g over 30 minutes 3 times weekly; however, the dose can be increased to 25 g over 60 minutes if 3 to 4 treatments are tolerated, with nausea being the only notable side effect. Its mechanism of action in treating dystrophic calcinosis cutis is unclear, but it likely is due to its ability to chelate and dissolve calcium deposits. Topical and intradermal therapy is impractical for widespread, dystrophic calcinosis cutis as in our patient.
Our case highlights the successful use of IV sodium thiosulfate as a stand-alone treatment modality for generalized dystrophic calcinosis cutis in an adult patient. Both our patient and a child in a previously reported case who received the same treatment4 had dermatomyositis, but we suspect IV sodium thiosulfate also may be effective for dystrophic calcinosis cutis associated with other diseases. Sodium thiosulfate should be considered as a treatment for patients who experience tremendous pain and disability. It is safe, inexpensive, and easy to administer and is especially helpful in patients for whom topical, intradermal, or procedural therapy is not possible.
To the Editor:
Severe dystrophic calcinosis cutis is a debilitating disease with no universally accepted therapeutic options. This case demonstrates the benefit of intravenous (IV) sodium thiosulfate in alleviating the calcified lesions as well as the associated pain and disability. This application of IV sodium thiosulfate with a favorable outcome is new and should be considered for the treatment of generalized dystrophic calcinosis cutis, especially when topical, procedural, or surgical options are not feasible.
A 54-year-old woman with a history of well-controlled dermatomyositis and systemic lupus erythematosus presented with diffuse, hard, calcified lesions on the legs, arms, clavicular region, and neck that had slowly progressed over at least a 10-year period (Figure 1). The lesions were consistent with dystrophic calcinosis cutis. The patient was started on 12.5 g of IV sodium thiosulfate 3 times weekly infused over 30 minutes. Drastic diminution of the cutaneous calcification was observed at 3-month follow-up (Figure 2). She reported decreased pain and burning as well as increased overall functionality and improved sleep. The patient completed 8 months of therapy, but the treatment was stopped secondary to suspicion of a lupuslike flare, and the lesions recurred with more widespread involvement, including the trunk, tendons, bony prominences, and supraclavicular soft tissue. The patient reported burning pain and pruritus that resulted in impairment of daily activities such as getting dressed. Sodium thiosulfate was restarted once weekly, which again resulted in reduction of the dystrophic calcinosis cutis.
Dystrophic calcinosis cutis is a debilitating disease that results in considerable morbidity and pain with major implications on quality of life. The pathophysiology is unclear; calcium and phosphate serum levels generally are normal. A proposed mechanism is that chronic inflammation causes tissue damage and defective collagen synthesis, resulting in a distorted architecture that facilitates calcium deposition in the skin and subcutaneous tissues.1 Dystrophic calcinosis cutis most commonly is associated with systemic sclerosis and dermatomyositis but also can be seen in systemic lupus erythematosus, panniculitis, and other connective tissue diseases. It also can occur with skin neoplasms, collagen and elastin disorders, porphyria cutanea tarda, and pancreatic panniculitis.1 Progression of dystrophic calcinosis cutis usually is independent of the associated disease status.
Treatment is based on anecdotal evidence from case reports, as there is no universally accepted pharmacologic or procedural intervention available for dystrophic calcinosis cutis. Medications that have been reported to be helpful to varying degrees include diltiazem, colchicine, minocycline, IV immunoglobulin, ceftriaxone, aluminum hydroxide, probenecid, alendronic acid, etidronate disodium, warfarin, intralesional corticosteroids, and sodium thiosulfate. Procedural interventions also have been reported, such as surgical excision, extracorporeal shock wave lithotripsy, and CO2 and erbium: YAG lasers.1 Surgical excision of dystrophic calcinosis cutis is widely implemented but outcomes are poor. Moreover, in patients with widely diffuse calcinosis, targeted procedural therapy is impractical.
Intravenous sodium thiosulfate has been widely used for the treatment of calciphylaxis secondary to end-stage renal failure and tumoral calcinosis.2 It also has been reported to be effective in iatrogenic calcinosis cutis secondary to extravasation of calcium-containing solutions in a patient with T-cell acute lymphoblastic leukemia.3 However, reports of its use in treating dystrophic calcinosis cutis are limited. Intravenous sodium thiosulfate—10 g 3 times weekly for 2 weeks, followed by 15 g twice weekly for the next 3 months—was used with abatacept for treatment of dystrophic calcinosis cutis in a patient with juvenile dermatomyositis.4 Other formulations of sodium thiosulfate have been reported to result in clearance of calcified lesions, including a topical application compounded in zinc oxide5 and intradermal injection at the base of a nodule.6 We used 12.5 g over 30 minutes 3 times weekly; however, the dose can be increased to 25 g over 60 minutes if 3 to 4 treatments are tolerated, with nausea being the only notable side effect. Its mechanism of action in treating dystrophic calcinosis cutis is unclear, but it likely is due to its ability to chelate and dissolve calcium deposits. Topical and intradermal therapy is impractical for widespread, dystrophic calcinosis cutis as in our patient.
Our case highlights the successful use of IV sodium thiosulfate as a stand-alone treatment modality for generalized dystrophic calcinosis cutis in an adult patient. Both our patient and a child in a previously reported case who received the same treatment4 had dermatomyositis, but we suspect IV sodium thiosulfate also may be effective for dystrophic calcinosis cutis associated with other diseases. Sodium thiosulfate should be considered as a treatment for patients who experience tremendous pain and disability. It is safe, inexpensive, and easy to administer and is especially helpful in patients for whom topical, intradermal, or procedural therapy is not possible.
- Gutierrez A Jr, Wetter DA. Calcinosis cutis in autoimmune connective tissue diseases. Dermatol Ther. 2012;25:195-206.
- Mageau A, Guigonis V, Ratzimbasafy V, et al. Intravenous sodium thiosulfate for treating tumoral calcinosis associated with systemic disorders: report of four cases. Joint Bone Spine. 2017;84:341-344.
Raffaella C, Annapaola C, Tullio I, et al. Successful treatment of severe iatrogenic calcinosis cutis with intravenous sodium thiosulfate in a child affected by T-acute lymphoblastic leukemia. Pediatr Dermatol. 2009;26:311-315. - Arabshahi B, Silverman RA, Jones OY, et al. Abatacept and sodium thiosulfate for treatment of recalcitrant juvenile dermatomyositis complicated by ulceration and calcinosis. J Pediatrics. 2012;160:520-522.
- Bair B, Fivenson D. A novel treatment for ulcerative calcinosis cutis. J Drugs Dermatol. 2011;10:1042-1044.
- Smith GP. Intradermal sodium thiosulfate for exophytic calcinosis cutis of connective tissue disease. J Am Acad Dermatol. 2013;69:E146-E147.
- Gutierrez A Jr, Wetter DA. Calcinosis cutis in autoimmune connective tissue diseases. Dermatol Ther. 2012;25:195-206.
- Mageau A, Guigonis V, Ratzimbasafy V, et al. Intravenous sodium thiosulfate for treating tumoral calcinosis associated with systemic disorders: report of four cases. Joint Bone Spine. 2017;84:341-344.
Raffaella C, Annapaola C, Tullio I, et al. Successful treatment of severe iatrogenic calcinosis cutis with intravenous sodium thiosulfate in a child affected by T-acute lymphoblastic leukemia. Pediatr Dermatol. 2009;26:311-315. - Arabshahi B, Silverman RA, Jones OY, et al. Abatacept and sodium thiosulfate for treatment of recalcitrant juvenile dermatomyositis complicated by ulceration and calcinosis. J Pediatrics. 2012;160:520-522.
- Bair B, Fivenson D. A novel treatment for ulcerative calcinosis cutis. J Drugs Dermatol. 2011;10:1042-1044.
- Smith GP. Intradermal sodium thiosulfate for exophytic calcinosis cutis of connective tissue disease. J Am Acad Dermatol. 2013;69:E146-E147.
Practice Points
- Dystrophic calcinosis cutis is a potentially debilitating condition with limited effective therapies.
- Consider intravenous sodium thiosulfate in patients with diffuse and severe dystrophic calcinosis cutis.

Novel calculator predicts cancer risk in patients with CVD
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.

She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.
She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.
She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
FROM ESC CONGRESS 2020
Physician income drops, burnout spikes globally in pandemic
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
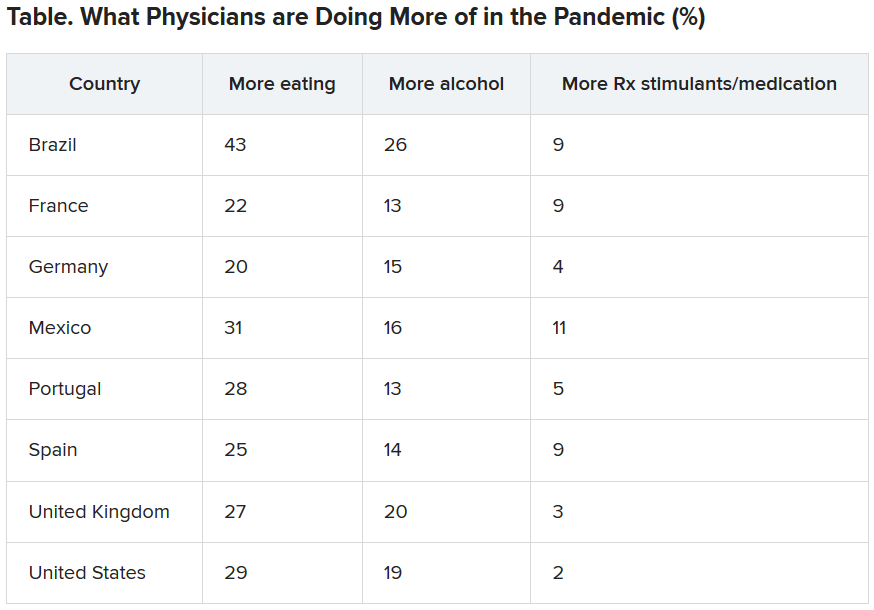
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.