User login
Myasthenia Gravis: 5 Things to Know
Myasthenia gravis (MG) is a rare autoimmune neurologic disorder that occurs when the transmission between nerves and muscles is disrupted. It is caused by autoantibodies against acetylcholine receptors (AChRs), which results in muscle weakness that is often fatigable and affects various muscles in the body, including those that move the eyes, eyelids, and limbs. Ocular MG affects only the muscles that move the eyes and eyelids, whereas generalized MG (gMG) affects muscles throughout the body. When MG occurs with a thymoma, it is called thymoma-associated MG and is considered a paraneoplastic disease. In severe cases of MG, patients can experience a myasthenic crisis (MC), during which respiratory muscles weaken and necessitate mechanical ventilation. Diagnosis of MG is based on clinical examination, and laboratory tests are used to confirm the diagnosis. Treatment options include cholinesterase enzyme inhibitors and immunosuppressive agents, which aim to either reduce symptoms or cause nonspecific immunosuppression, respectively, but do not target the pathogenetic autoantibodies that characterize the disease.
1. The most common age at onset of gMG is the second and third decades in women and the seventh and eighth decades in men.
MG has an annual incidence of approximately four to 30 new cases per million population. Prevalence rates range from 150 to 200 cases per million population, and they have steadily increased over the past 50 years. This increase in prevalence is probably the result of better disease recognition, aging of the population, and an increased life span in patients.
MG can occur at any age; however, onset is more common in females in the second and third decades and is more common in males in the seventh to eighth decades. Before age 40 years, the female-to-male ratio is 3:1, and after age 50 years, the female-to-male ratio is 3:2.
2. gMG commonly weakens muscles responsible for eye movement, facial expressions, and functions such as chewing, swallowing, and speaking.
gMG typically manifests as muscle weakness that worsens with repeated use. Patients often report that their function is best in the morning, with more pronounced weakness at the end of the day. Permanent muscle damage is rare, however, and maximal muscle strength is often good.
Extraocular muscles are more commonly affected, as twitch fibers in these muscles develop tension faster, have a higher frequency of synaptic firing than limb muscles, and have fewer AChRs, making them more susceptible to fatigue. Patients present asymmetrically; intermittent drooping of the upper eyelid (ptosis) and double vision (diplopia) are the most common symptoms.
Muscles innervated by the cranial nerves (bulbar muscles) are involved in 60% of patients with gMG and can lead to fatigable chewing, reduced facial expression, speech difficulties (dysarthria), and weakness of swallowing (dysphagia). Up to 15% of patients initially present with bulbar muscle involvement, including dysarthria and painless dysphagia.
3. Emotional stress can trigger an MC.
MC is a complication of MG characterized by worsening muscle weakness that results in respiratory failure and necessitates mechanical ventilation.
MC is often the result of respiratory muscle weakness but can also be due to bulbar weakness with upper airway collapse. MC can occur in 15%-20% of patients within the first 2-3 years of the disease; however, it can also be the first presentation of MG in 18%-28% of cases.
MC can be triggered by multiple causes, including emotional or physical stress. The most common precipitant is infection; other precipitants include surgery, pregnancy, perimenstrual state, certain medications, tapering of immune-modulating medications, exposure to temperature extremes, pain, and sleep deprivation. Approximately one third to one half of patients with MC may have no obvious cause.
4. High levels of anti-AChR antibodies strongly indicate MG, but normal levels do not rule it out.
All patients with a clinical history suggestive of MG should be tested for antibodies for confirmation. Most patients have anti-AChR antibodies (~85%), and those without have anti–muscle-specific kinase (MuSK antibodies) (6%) and anti–lipoprotein receptor-related protein 4 (LRP4) antibodies (2%).
The sensitivity of anti-AChR antibodies varies depending on whether the antibody is binding, modulating, or blocking the AChR. Binding antibody is the most common, and when combined with blocking antibodies, has a high sensitivity (99.6%) and is typically tested first. Higher AChR antibody titers are more specific for the diagnosis of MG than are low titers, but they do not correlate with disease severity.
For patients who do not have anti-AChR antibodies but do have clinical features of MG, anti-MuSK antibodies and anti-LRP4 antibodies are measured to increase diagnostic sensitivity. For symptomatic patients who do not have any autoantibodies (seronegative), electrodiagnostic testing that shows evidence of impaired signal transmission at the neuromuscular junction is used to confirm the diagnosis of MG.
5. Studies suggest that over 75% of seropositive MG patients show distinct thymus abnormalities.
More than 75% of patients with AChR antibody–positive MG have abnormalities in their thymus, and up to 40% of patients with a thymoma have MG. Among those with thymic pathology, thymic hyperplasia is the most common type (85%), but other thymic tumors (mainly thymoma) can be present in up to 15% of cases. Thymomas are typically noninvasive and cortical, but in some rare cases, invasive thymic carcinoma can occur.
Given this overlap in presentation, it is recommended that patients with seronegative and seropositive MG undergo chest CT or MRI for evaluation of their anterior mediastinal anatomy and to detect the presence of a thymoma. For patients with MG and a thymoma, as well as selected (nonthymomatous) patients with seropositive or seronegative MG, therapeutic thymectomy is recommended.
Myasthenia gravis (MG) is a rare autoimmune neurologic disorder that occurs when the transmission between nerves and muscles is disrupted. It is caused by autoantibodies against acetylcholine receptors (AChRs), which results in muscle weakness that is often fatigable and affects various muscles in the body, including those that move the eyes, eyelids, and limbs. Ocular MG affects only the muscles that move the eyes and eyelids, whereas generalized MG (gMG) affects muscles throughout the body. When MG occurs with a thymoma, it is called thymoma-associated MG and is considered a paraneoplastic disease. In severe cases of MG, patients can experience a myasthenic crisis (MC), during which respiratory muscles weaken and necessitate mechanical ventilation. Diagnosis of MG is based on clinical examination, and laboratory tests are used to confirm the diagnosis. Treatment options include cholinesterase enzyme inhibitors and immunosuppressive agents, which aim to either reduce symptoms or cause nonspecific immunosuppression, respectively, but do not target the pathogenetic autoantibodies that characterize the disease.
1. The most common age at onset of gMG is the second and third decades in women and the seventh and eighth decades in men.
MG has an annual incidence of approximately four to 30 new cases per million population. Prevalence rates range from 150 to 200 cases per million population, and they have steadily increased over the past 50 years. This increase in prevalence is probably the result of better disease recognition, aging of the population, and an increased life span in patients.
MG can occur at any age; however, onset is more common in females in the second and third decades and is more common in males in the seventh to eighth decades. Before age 40 years, the female-to-male ratio is 3:1, and after age 50 years, the female-to-male ratio is 3:2.
2. gMG commonly weakens muscles responsible for eye movement, facial expressions, and functions such as chewing, swallowing, and speaking.
gMG typically manifests as muscle weakness that worsens with repeated use. Patients often report that their function is best in the morning, with more pronounced weakness at the end of the day. Permanent muscle damage is rare, however, and maximal muscle strength is often good.
Extraocular muscles are more commonly affected, as twitch fibers in these muscles develop tension faster, have a higher frequency of synaptic firing than limb muscles, and have fewer AChRs, making them more susceptible to fatigue. Patients present asymmetrically; intermittent drooping of the upper eyelid (ptosis) and double vision (diplopia) are the most common symptoms.
Muscles innervated by the cranial nerves (bulbar muscles) are involved in 60% of patients with gMG and can lead to fatigable chewing, reduced facial expression, speech difficulties (dysarthria), and weakness of swallowing (dysphagia). Up to 15% of patients initially present with bulbar muscle involvement, including dysarthria and painless dysphagia.
3. Emotional stress can trigger an MC.
MC is a complication of MG characterized by worsening muscle weakness that results in respiratory failure and necessitates mechanical ventilation.
MC is often the result of respiratory muscle weakness but can also be due to bulbar weakness with upper airway collapse. MC can occur in 15%-20% of patients within the first 2-3 years of the disease; however, it can also be the first presentation of MG in 18%-28% of cases.
MC can be triggered by multiple causes, including emotional or physical stress. The most common precipitant is infection; other precipitants include surgery, pregnancy, perimenstrual state, certain medications, tapering of immune-modulating medications, exposure to temperature extremes, pain, and sleep deprivation. Approximately one third to one half of patients with MC may have no obvious cause.
4. High levels of anti-AChR antibodies strongly indicate MG, but normal levels do not rule it out.
All patients with a clinical history suggestive of MG should be tested for antibodies for confirmation. Most patients have anti-AChR antibodies (~85%), and those without have anti–muscle-specific kinase (MuSK antibodies) (6%) and anti–lipoprotein receptor-related protein 4 (LRP4) antibodies (2%).
The sensitivity of anti-AChR antibodies varies depending on whether the antibody is binding, modulating, or blocking the AChR. Binding antibody is the most common, and when combined with blocking antibodies, has a high sensitivity (99.6%) and is typically tested first. Higher AChR antibody titers are more specific for the diagnosis of MG than are low titers, but they do not correlate with disease severity.
For patients who do not have anti-AChR antibodies but do have clinical features of MG, anti-MuSK antibodies and anti-LRP4 antibodies are measured to increase diagnostic sensitivity. For symptomatic patients who do not have any autoantibodies (seronegative), electrodiagnostic testing that shows evidence of impaired signal transmission at the neuromuscular junction is used to confirm the diagnosis of MG.
5. Studies suggest that over 75% of seropositive MG patients show distinct thymus abnormalities.
More than 75% of patients with AChR antibody–positive MG have abnormalities in their thymus, and up to 40% of patients with a thymoma have MG. Among those with thymic pathology, thymic hyperplasia is the most common type (85%), but other thymic tumors (mainly thymoma) can be present in up to 15% of cases. Thymomas are typically noninvasive and cortical, but in some rare cases, invasive thymic carcinoma can occur.
Given this overlap in presentation, it is recommended that patients with seronegative and seropositive MG undergo chest CT or MRI for evaluation of their anterior mediastinal anatomy and to detect the presence of a thymoma. For patients with MG and a thymoma, as well as selected (nonthymomatous) patients with seropositive or seronegative MG, therapeutic thymectomy is recommended.
Myasthenia gravis (MG) is a rare autoimmune neurologic disorder that occurs when the transmission between nerves and muscles is disrupted. It is caused by autoantibodies against acetylcholine receptors (AChRs), which results in muscle weakness that is often fatigable and affects various muscles in the body, including those that move the eyes, eyelids, and limbs. Ocular MG affects only the muscles that move the eyes and eyelids, whereas generalized MG (gMG) affects muscles throughout the body. When MG occurs with a thymoma, it is called thymoma-associated MG and is considered a paraneoplastic disease. In severe cases of MG, patients can experience a myasthenic crisis (MC), during which respiratory muscles weaken and necessitate mechanical ventilation. Diagnosis of MG is based on clinical examination, and laboratory tests are used to confirm the diagnosis. Treatment options include cholinesterase enzyme inhibitors and immunosuppressive agents, which aim to either reduce symptoms or cause nonspecific immunosuppression, respectively, but do not target the pathogenetic autoantibodies that characterize the disease.
1. The most common age at onset of gMG is the second and third decades in women and the seventh and eighth decades in men.
MG has an annual incidence of approximately four to 30 new cases per million population. Prevalence rates range from 150 to 200 cases per million population, and they have steadily increased over the past 50 years. This increase in prevalence is probably the result of better disease recognition, aging of the population, and an increased life span in patients.
MG can occur at any age; however, onset is more common in females in the second and third decades and is more common in males in the seventh to eighth decades. Before age 40 years, the female-to-male ratio is 3:1, and after age 50 years, the female-to-male ratio is 3:2.
2. gMG commonly weakens muscles responsible for eye movement, facial expressions, and functions such as chewing, swallowing, and speaking.
gMG typically manifests as muscle weakness that worsens with repeated use. Patients often report that their function is best in the morning, with more pronounced weakness at the end of the day. Permanent muscle damage is rare, however, and maximal muscle strength is often good.
Extraocular muscles are more commonly affected, as twitch fibers in these muscles develop tension faster, have a higher frequency of synaptic firing than limb muscles, and have fewer AChRs, making them more susceptible to fatigue. Patients present asymmetrically; intermittent drooping of the upper eyelid (ptosis) and double vision (diplopia) are the most common symptoms.
Muscles innervated by the cranial nerves (bulbar muscles) are involved in 60% of patients with gMG and can lead to fatigable chewing, reduced facial expression, speech difficulties (dysarthria), and weakness of swallowing (dysphagia). Up to 15% of patients initially present with bulbar muscle involvement, including dysarthria and painless dysphagia.
3. Emotional stress can trigger an MC.
MC is a complication of MG characterized by worsening muscle weakness that results in respiratory failure and necessitates mechanical ventilation.
MC is often the result of respiratory muscle weakness but can also be due to bulbar weakness with upper airway collapse. MC can occur in 15%-20% of patients within the first 2-3 years of the disease; however, it can also be the first presentation of MG in 18%-28% of cases.
MC can be triggered by multiple causes, including emotional or physical stress. The most common precipitant is infection; other precipitants include surgery, pregnancy, perimenstrual state, certain medications, tapering of immune-modulating medications, exposure to temperature extremes, pain, and sleep deprivation. Approximately one third to one half of patients with MC may have no obvious cause.
4. High levels of anti-AChR antibodies strongly indicate MG, but normal levels do not rule it out.
All patients with a clinical history suggestive of MG should be tested for antibodies for confirmation. Most patients have anti-AChR antibodies (~85%), and those without have anti–muscle-specific kinase (MuSK antibodies) (6%) and anti–lipoprotein receptor-related protein 4 (LRP4) antibodies (2%).
The sensitivity of anti-AChR antibodies varies depending on whether the antibody is binding, modulating, or blocking the AChR. Binding antibody is the most common, and when combined with blocking antibodies, has a high sensitivity (99.6%) and is typically tested first. Higher AChR antibody titers are more specific for the diagnosis of MG than are low titers, but they do not correlate with disease severity.
For patients who do not have anti-AChR antibodies but do have clinical features of MG, anti-MuSK antibodies and anti-LRP4 antibodies are measured to increase diagnostic sensitivity. For symptomatic patients who do not have any autoantibodies (seronegative), electrodiagnostic testing that shows evidence of impaired signal transmission at the neuromuscular junction is used to confirm the diagnosis of MG.
5. Studies suggest that over 75% of seropositive MG patients show distinct thymus abnormalities.
More than 75% of patients with AChR antibody–positive MG have abnormalities in their thymus, and up to 40% of patients with a thymoma have MG. Among those with thymic pathology, thymic hyperplasia is the most common type (85%), but other thymic tumors (mainly thymoma) can be present in up to 15% of cases. Thymomas are typically noninvasive and cortical, but in some rare cases, invasive thymic carcinoma can occur.
Given this overlap in presentation, it is recommended that patients with seronegative and seropositive MG undergo chest CT or MRI for evaluation of their anterior mediastinal anatomy and to detect the presence of a thymoma. For patients with MG and a thymoma, as well as selected (nonthymomatous) patients with seropositive or seronegative MG, therapeutic thymectomy is recommended.
Is Migraine a Forerunner of Multiple Sclerosis?
WEST PALM BEACH, FLORIDA — new research suggested. Investigators found that patients with MS were more likely than controls to develop migraine shortly before disease diagnosis, suggesting the headache type is not a forerunner of MS.
“The risk [of migraine] was concentrated in the year of their first [MS] symptom, or the year prior, instead of many years before,” said lead investigator Vinicius A. Schoeps, MD, MPH, postdoctoral fellow at the University of California San Francisco.
The findings were presented at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Is MS a Migraine Trigger?
Worldwide up to 43% of patients with MS report migraine. Recent data point to a 3- to 5-year clinically symptomatic prodromal phase of MS and suggest migraine may be one of its potential constituents. However, the relationship between the two disorders remains unclear.
The investigators wanted to determine whether migraine is part of the MS prodrome because if this is the case, it could provide a potential opportunity for early intervention to delay or prevent the disease.
The team analyzed incidence cases of MS and matched controls in the Kaiser Permanente Southern California health system from 2011 to 2014. Participants took part in structured in-person interviews that included questions about migraine.
The 591 MS cases had an average age of onset at 36 years, with a similar index date for controls. Among the cases, 71% were women, 42% were White, 32% Hispanic, and 21% Black. Almost 40% of cases had obesity. These demographic data were similar in the control group.
In those with MS, 13% had a history of mononucleosis compared with 6% of controls. Epstein-Barr virus, which causes conditions such as mononucleosis, was considered a likely cause of MS.
Migraine was diagnosed before MS onset in 27% of cases and before the index date in 21% of controls (adjusted odds ratio [aOR], 1.36; P = .03). Migraine onset occurred later in cases versus controls (mean, 21 years vs 17 years; P = .008).
Migraine was also more likely to occur at the same time or 1 year prior to MS symptoms or the index date in cases versus controls (4.3% vs 1.3%; aOR, 3.54; P = .002).
“These findings suggest that migraine can be triggered by MS rather than part of the constellation of nonspecific symptoms that constitute the 3- to 5-year-long MS prodrome,” the investigators reported.
“The inflammatory setting of the first MS relapse might be actually triggering the migraine,” Dr. Shoeps said. He added that patients with MS developed migraines later in life.
“There could be a different pathological process in people who have traditional migraine at the most common age where people get their diagnosis of migraine — and have them throughout their lifetime — versus having a migraine at older age and a diagnosis of MS close to that period of time,” he said. However, he noted, the study design does not allow for this type of analysis.
Commenting on the findings, Anibal Chertcoff, MD, PhD, an assistant professor in the Multiple Sclerosis Research Centre at the University of Manitoba, Winnipeg, Manitoba, Canada, noted the study’s large population and well-balanced case and control groups are strengths of the study.
However, Dr. Chertcoff, who was not involved in the research, cautioned that the study is cross-sectional noting that he is “not convinced this is the best type of study design to provide insights into cause-and-effect relationships.”
Dr. Chertcoff added the findings are limited by their reliance on data from a single health system.
Disclosures were not provided. A grant from the National Institute of Neurologic Disorders and Stroke to an author helped support the study. Dr. Chertcoff received funding from MS Canada and the Michael Smith Foundation for Health Research and support from Novartis to attend a scientific meeting.
A version of this article appeared on Medscape.com.
WEST PALM BEACH, FLORIDA — new research suggested. Investigators found that patients with MS were more likely than controls to develop migraine shortly before disease diagnosis, suggesting the headache type is not a forerunner of MS.
“The risk [of migraine] was concentrated in the year of their first [MS] symptom, or the year prior, instead of many years before,” said lead investigator Vinicius A. Schoeps, MD, MPH, postdoctoral fellow at the University of California San Francisco.
The findings were presented at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Is MS a Migraine Trigger?
Worldwide up to 43% of patients with MS report migraine. Recent data point to a 3- to 5-year clinically symptomatic prodromal phase of MS and suggest migraine may be one of its potential constituents. However, the relationship between the two disorders remains unclear.
The investigators wanted to determine whether migraine is part of the MS prodrome because if this is the case, it could provide a potential opportunity for early intervention to delay or prevent the disease.
The team analyzed incidence cases of MS and matched controls in the Kaiser Permanente Southern California health system from 2011 to 2014. Participants took part in structured in-person interviews that included questions about migraine.
The 591 MS cases had an average age of onset at 36 years, with a similar index date for controls. Among the cases, 71% were women, 42% were White, 32% Hispanic, and 21% Black. Almost 40% of cases had obesity. These demographic data were similar in the control group.
In those with MS, 13% had a history of mononucleosis compared with 6% of controls. Epstein-Barr virus, which causes conditions such as mononucleosis, was considered a likely cause of MS.
Migraine was diagnosed before MS onset in 27% of cases and before the index date in 21% of controls (adjusted odds ratio [aOR], 1.36; P = .03). Migraine onset occurred later in cases versus controls (mean, 21 years vs 17 years; P = .008).
Migraine was also more likely to occur at the same time or 1 year prior to MS symptoms or the index date in cases versus controls (4.3% vs 1.3%; aOR, 3.54; P = .002).
“These findings suggest that migraine can be triggered by MS rather than part of the constellation of nonspecific symptoms that constitute the 3- to 5-year-long MS prodrome,” the investigators reported.
“The inflammatory setting of the first MS relapse might be actually triggering the migraine,” Dr. Shoeps said. He added that patients with MS developed migraines later in life.
“There could be a different pathological process in people who have traditional migraine at the most common age where people get their diagnosis of migraine — and have them throughout their lifetime — versus having a migraine at older age and a diagnosis of MS close to that period of time,” he said. However, he noted, the study design does not allow for this type of analysis.
Commenting on the findings, Anibal Chertcoff, MD, PhD, an assistant professor in the Multiple Sclerosis Research Centre at the University of Manitoba, Winnipeg, Manitoba, Canada, noted the study’s large population and well-balanced case and control groups are strengths of the study.
However, Dr. Chertcoff, who was not involved in the research, cautioned that the study is cross-sectional noting that he is “not convinced this is the best type of study design to provide insights into cause-and-effect relationships.”
Dr. Chertcoff added the findings are limited by their reliance on data from a single health system.
Disclosures were not provided. A grant from the National Institute of Neurologic Disorders and Stroke to an author helped support the study. Dr. Chertcoff received funding from MS Canada and the Michael Smith Foundation for Health Research and support from Novartis to attend a scientific meeting.
A version of this article appeared on Medscape.com.
WEST PALM BEACH, FLORIDA — new research suggested. Investigators found that patients with MS were more likely than controls to develop migraine shortly before disease diagnosis, suggesting the headache type is not a forerunner of MS.
“The risk [of migraine] was concentrated in the year of their first [MS] symptom, or the year prior, instead of many years before,” said lead investigator Vinicius A. Schoeps, MD, MPH, postdoctoral fellow at the University of California San Francisco.
The findings were presented at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Is MS a Migraine Trigger?
Worldwide up to 43% of patients with MS report migraine. Recent data point to a 3- to 5-year clinically symptomatic prodromal phase of MS and suggest migraine may be one of its potential constituents. However, the relationship between the two disorders remains unclear.
The investigators wanted to determine whether migraine is part of the MS prodrome because if this is the case, it could provide a potential opportunity for early intervention to delay or prevent the disease.
The team analyzed incidence cases of MS and matched controls in the Kaiser Permanente Southern California health system from 2011 to 2014. Participants took part in structured in-person interviews that included questions about migraine.
The 591 MS cases had an average age of onset at 36 years, with a similar index date for controls. Among the cases, 71% were women, 42% were White, 32% Hispanic, and 21% Black. Almost 40% of cases had obesity. These demographic data were similar in the control group.
In those with MS, 13% had a history of mononucleosis compared with 6% of controls. Epstein-Barr virus, which causes conditions such as mononucleosis, was considered a likely cause of MS.
Migraine was diagnosed before MS onset in 27% of cases and before the index date in 21% of controls (adjusted odds ratio [aOR], 1.36; P = .03). Migraine onset occurred later in cases versus controls (mean, 21 years vs 17 years; P = .008).
Migraine was also more likely to occur at the same time or 1 year prior to MS symptoms or the index date in cases versus controls (4.3% vs 1.3%; aOR, 3.54; P = .002).
“These findings suggest that migraine can be triggered by MS rather than part of the constellation of nonspecific symptoms that constitute the 3- to 5-year-long MS prodrome,” the investigators reported.
“The inflammatory setting of the first MS relapse might be actually triggering the migraine,” Dr. Shoeps said. He added that patients with MS developed migraines later in life.
“There could be a different pathological process in people who have traditional migraine at the most common age where people get their diagnosis of migraine — and have them throughout their lifetime — versus having a migraine at older age and a diagnosis of MS close to that period of time,” he said. However, he noted, the study design does not allow for this type of analysis.
Commenting on the findings, Anibal Chertcoff, MD, PhD, an assistant professor in the Multiple Sclerosis Research Centre at the University of Manitoba, Winnipeg, Manitoba, Canada, noted the study’s large population and well-balanced case and control groups are strengths of the study.
However, Dr. Chertcoff, who was not involved in the research, cautioned that the study is cross-sectional noting that he is “not convinced this is the best type of study design to provide insights into cause-and-effect relationships.”
Dr. Chertcoff added the findings are limited by their reliance on data from a single health system.
Disclosures were not provided. A grant from the National Institute of Neurologic Disorders and Stroke to an author helped support the study. Dr. Chertcoff received funding from MS Canada and the Michael Smith Foundation for Health Research and support from Novartis to attend a scientific meeting.
A version of this article appeared on Medscape.com.
FROM ACTRIMS FORUM 2024
Seizure Risk Is Nearly Double in Patients With MS
TOPLINE:
, results of a new meta-analysis of randomized controlled trials (RCTs) suggest. Those with a progressive disease phenotype are at particularly high seizure risk.
METHODOLOGY:
- The meta-analysis included 63 phase 3 RCTs with 53,535 patients.
- Most of the studies included in the meta-analysis investigated disease-modifying treatments compared with placebo or an active comparator such as interferon beta, teriflunomide, and dimethyl fumarate, in terms of relapse rate and/or disability progression.
- Researchers extracted relevant information from studies, including MS subtype (clinically isolated syndrome, relapsing-remitting, primary progressive, or secondary progressive MS), mean Expanded Disability Status Scale (EDSS) score, lesion volume on T2-hyperintense sequence, normalized brain volume, and number of seizures or epilepsy events.
- They calculated the pooled effect size of studies on the incidence rate of seizure or epilepsy as the number of events per patient-years and explored which variables influenced the pooled effect size.
TAKEAWAY:
- A total of 120 patients experienced epileptic seizure events over a median follow-up of 2 years, resulting in a pooled incidence rate of 68.0 (95% CI, 49.1-86.9) per 100,000 patient-years, which investigators noted is significantly higher than the general population rate of 34.6.
- Higher seizure incidence rates were found among patients with progressive disease courses, longer time since clinical onset, higher EDSS scores, and lower normalized brain volume; age and T2 lesion volume did not affect the pooled effect size.
- Patients treated with S1PR modulators (fingolimod, ozanimod, ponesimod, and siponimod) had more than double the risk for seizure compared with placebo or comparators (estimated incident seizure risk ratio, 2.45; P = .008).
IN PRACTICE:
“Our findings underscore epilepsy as a significant comorbidity in MS and emphasize the necessity for further research into its triggers, preventive measures and treatment strategies,” the authors wrote.
SOURCE:
The study, led by Valeria Pozzilli, Unit of Neurology, Neurophysiology and Neurobiology, Department of Medicine and Surgery, Campus Bio-Medico University, Roma, Italy, was published online in the Journal of Neurology, Neurosurgery, and Psychiatry.
LIMITATIONS:
As none of the included RCTs considered epilepsy an exclusion criterion, patients with comorbid epilepsy may have been enrolled in these studies. There was significant diversity in reporting of adverse events across studies. While this study’s statistical methodology was robust, the findings can’t be applied directly to individuals due to the risk for ecological fallacy.
DISCLOSURES:
Pozzilli had no relevant conflicts of interests. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
, results of a new meta-analysis of randomized controlled trials (RCTs) suggest. Those with a progressive disease phenotype are at particularly high seizure risk.
METHODOLOGY:
- The meta-analysis included 63 phase 3 RCTs with 53,535 patients.
- Most of the studies included in the meta-analysis investigated disease-modifying treatments compared with placebo or an active comparator such as interferon beta, teriflunomide, and dimethyl fumarate, in terms of relapse rate and/or disability progression.
- Researchers extracted relevant information from studies, including MS subtype (clinically isolated syndrome, relapsing-remitting, primary progressive, or secondary progressive MS), mean Expanded Disability Status Scale (EDSS) score, lesion volume on T2-hyperintense sequence, normalized brain volume, and number of seizures or epilepsy events.
- They calculated the pooled effect size of studies on the incidence rate of seizure or epilepsy as the number of events per patient-years and explored which variables influenced the pooled effect size.
TAKEAWAY:
- A total of 120 patients experienced epileptic seizure events over a median follow-up of 2 years, resulting in a pooled incidence rate of 68.0 (95% CI, 49.1-86.9) per 100,000 patient-years, which investigators noted is significantly higher than the general population rate of 34.6.
- Higher seizure incidence rates were found among patients with progressive disease courses, longer time since clinical onset, higher EDSS scores, and lower normalized brain volume; age and T2 lesion volume did not affect the pooled effect size.
- Patients treated with S1PR modulators (fingolimod, ozanimod, ponesimod, and siponimod) had more than double the risk for seizure compared with placebo or comparators (estimated incident seizure risk ratio, 2.45; P = .008).
IN PRACTICE:
“Our findings underscore epilepsy as a significant comorbidity in MS and emphasize the necessity for further research into its triggers, preventive measures and treatment strategies,” the authors wrote.
SOURCE:
The study, led by Valeria Pozzilli, Unit of Neurology, Neurophysiology and Neurobiology, Department of Medicine and Surgery, Campus Bio-Medico University, Roma, Italy, was published online in the Journal of Neurology, Neurosurgery, and Psychiatry.
LIMITATIONS:
As none of the included RCTs considered epilepsy an exclusion criterion, patients with comorbid epilepsy may have been enrolled in these studies. There was significant diversity in reporting of adverse events across studies. While this study’s statistical methodology was robust, the findings can’t be applied directly to individuals due to the risk for ecological fallacy.
DISCLOSURES:
Pozzilli had no relevant conflicts of interests. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
, results of a new meta-analysis of randomized controlled trials (RCTs) suggest. Those with a progressive disease phenotype are at particularly high seizure risk.
METHODOLOGY:
- The meta-analysis included 63 phase 3 RCTs with 53,535 patients.
- Most of the studies included in the meta-analysis investigated disease-modifying treatments compared with placebo or an active comparator such as interferon beta, teriflunomide, and dimethyl fumarate, in terms of relapse rate and/or disability progression.
- Researchers extracted relevant information from studies, including MS subtype (clinically isolated syndrome, relapsing-remitting, primary progressive, or secondary progressive MS), mean Expanded Disability Status Scale (EDSS) score, lesion volume on T2-hyperintense sequence, normalized brain volume, and number of seizures or epilepsy events.
- They calculated the pooled effect size of studies on the incidence rate of seizure or epilepsy as the number of events per patient-years and explored which variables influenced the pooled effect size.
TAKEAWAY:
- A total of 120 patients experienced epileptic seizure events over a median follow-up of 2 years, resulting in a pooled incidence rate of 68.0 (95% CI, 49.1-86.9) per 100,000 patient-years, which investigators noted is significantly higher than the general population rate of 34.6.
- Higher seizure incidence rates were found among patients with progressive disease courses, longer time since clinical onset, higher EDSS scores, and lower normalized brain volume; age and T2 lesion volume did not affect the pooled effect size.
- Patients treated with S1PR modulators (fingolimod, ozanimod, ponesimod, and siponimod) had more than double the risk for seizure compared with placebo or comparators (estimated incident seizure risk ratio, 2.45; P = .008).
IN PRACTICE:
“Our findings underscore epilepsy as a significant comorbidity in MS and emphasize the necessity for further research into its triggers, preventive measures and treatment strategies,” the authors wrote.
SOURCE:
The study, led by Valeria Pozzilli, Unit of Neurology, Neurophysiology and Neurobiology, Department of Medicine and Surgery, Campus Bio-Medico University, Roma, Italy, was published online in the Journal of Neurology, Neurosurgery, and Psychiatry.
LIMITATIONS:
As none of the included RCTs considered epilepsy an exclusion criterion, patients with comorbid epilepsy may have been enrolled in these studies. There was significant diversity in reporting of adverse events across studies. While this study’s statistical methodology was robust, the findings can’t be applied directly to individuals due to the risk for ecological fallacy.
DISCLOSURES:
Pozzilli had no relevant conflicts of interests. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
California Pushes to Expand the Universe of Abortion Care Providers
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Nurturing health equity in smoking cessation care
Thoracic Oncology And Chest Procedures Network
Lung Cancer Section

Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
References
1. Dresler et al. Lung Cancer. 2003.
2. J Cancer Educ. 2018;33[5].
3. Addiction. 2023.
Thoracic Oncology And Chest Procedures Network
Lung Cancer Section
Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
References
1. Dresler et al. Lung Cancer. 2003.
2. J Cancer Educ. 2018;33[5].
3. Addiction. 2023.
Thoracic Oncology And Chest Procedures Network
Lung Cancer Section
Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
References
1. Dresler et al. Lung Cancer. 2003.
2. J Cancer Educ. 2018;33[5].
3. Addiction. 2023.
The not-so-silent night: Challenges in improving sleep in inpatients with Dr. Vineet Arora
Sleep Medicine Network
Nonrespiratory Sleep Section

Q: Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
Sleep Medicine Network
Nonrespiratory Sleep Section
Q: Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
Sleep Medicine Network
Nonrespiratory Sleep Section
Q: Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
Compassionate extubation and beyond: Is there a need for more guidance in managing end-of-life in the intensive care unit?
Critical Care Network
Palliative and End-of-Life Care Section

For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
Critical Care Network
Palliative and End-of-Life Care Section
For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
Critical Care Network
Palliative and End-of-Life Care Section
For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
COVID-19 Is a Very Weird Virus
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.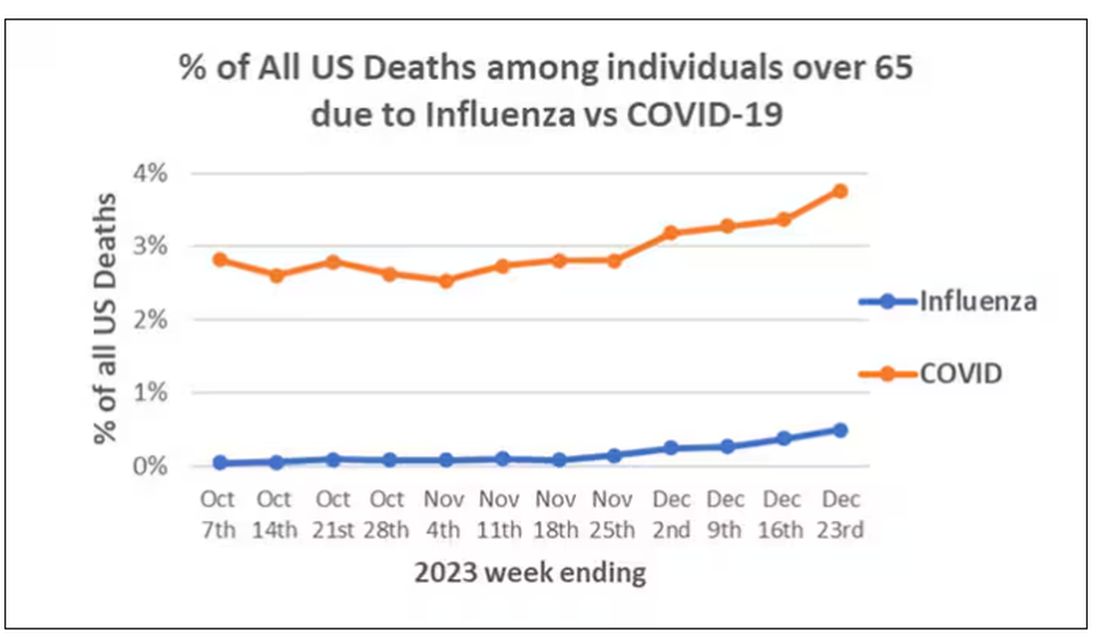
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)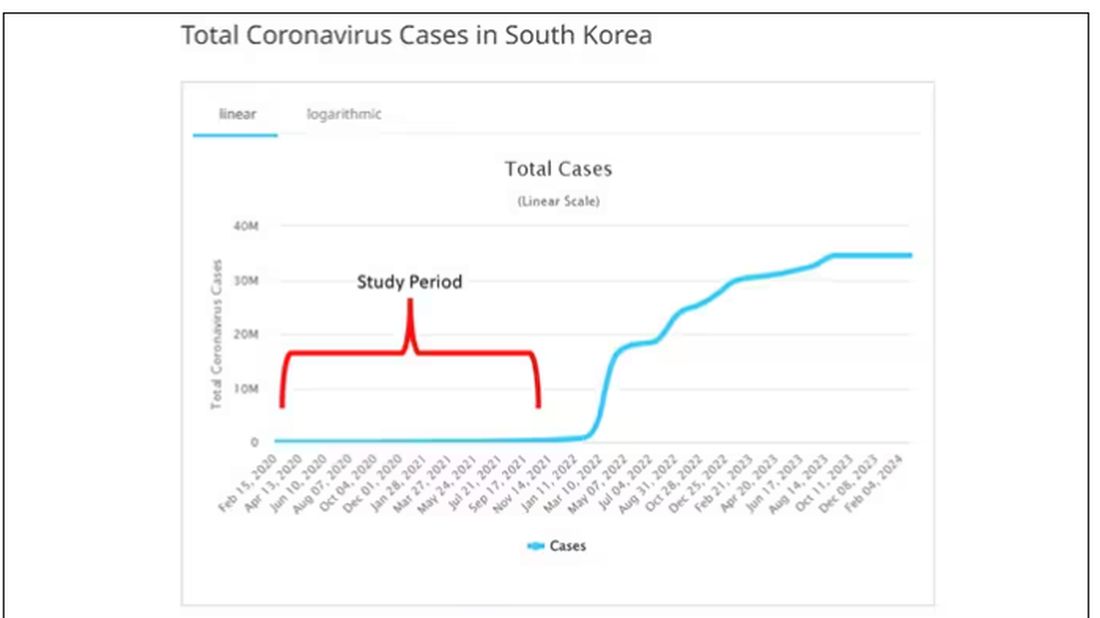
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.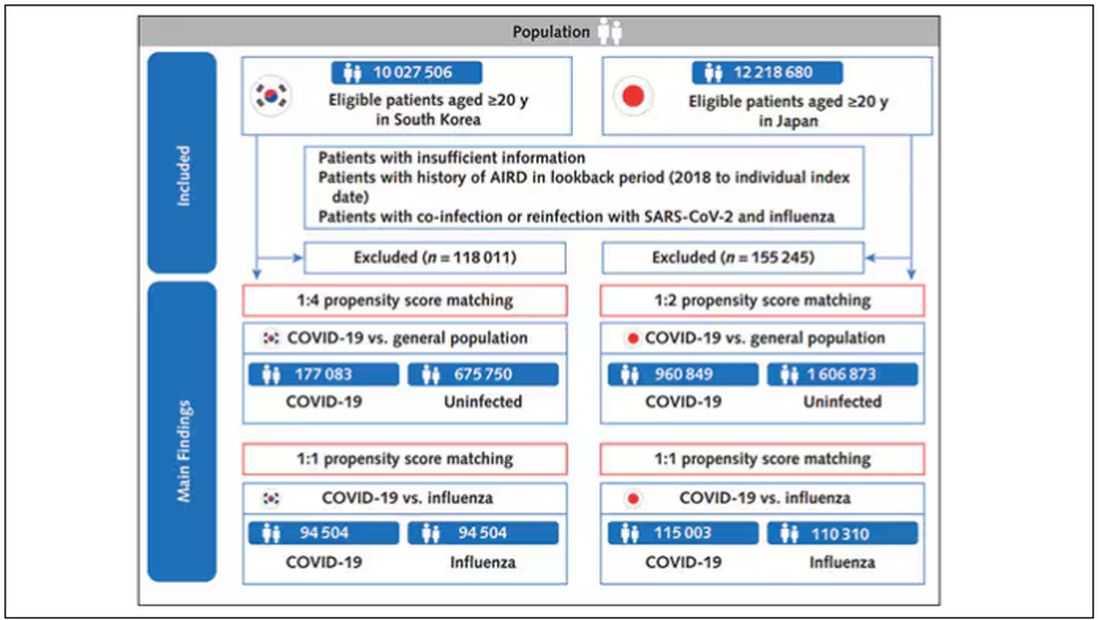
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).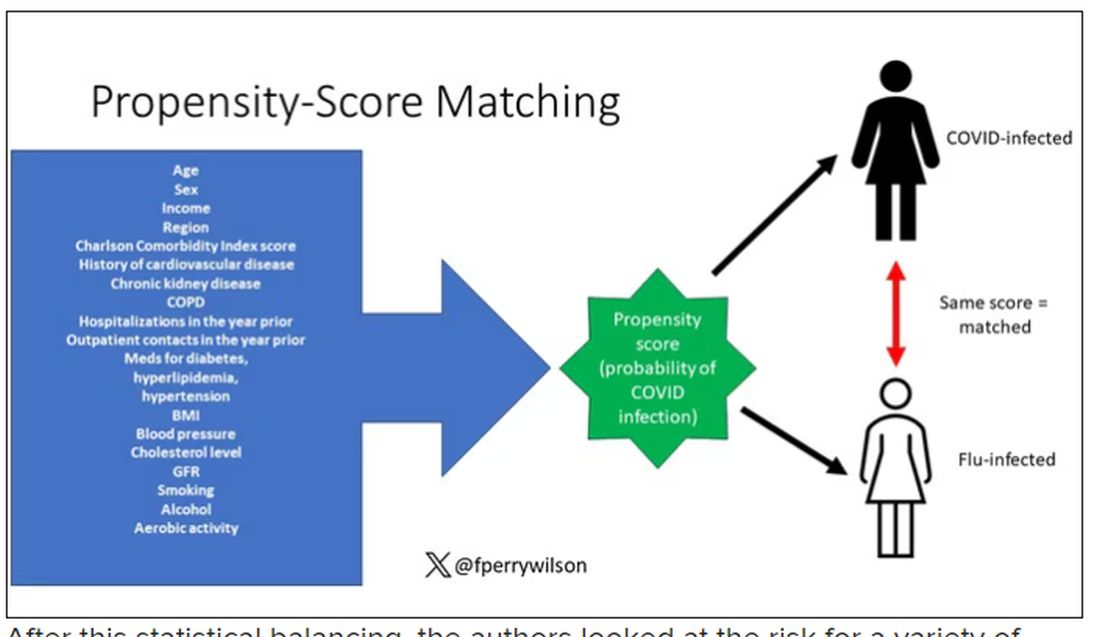
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.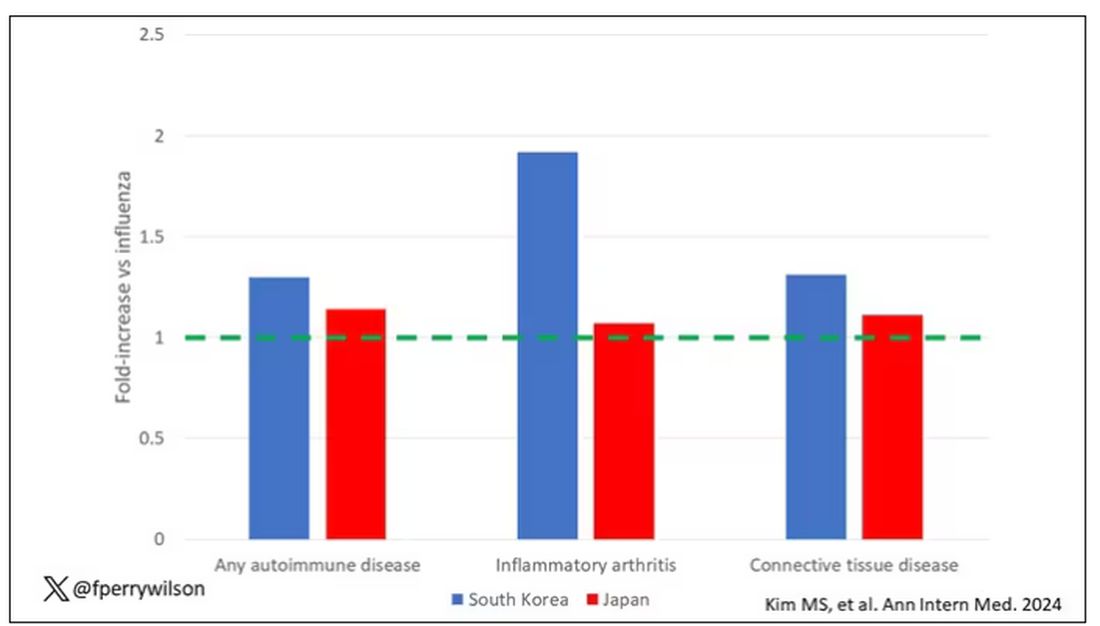
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.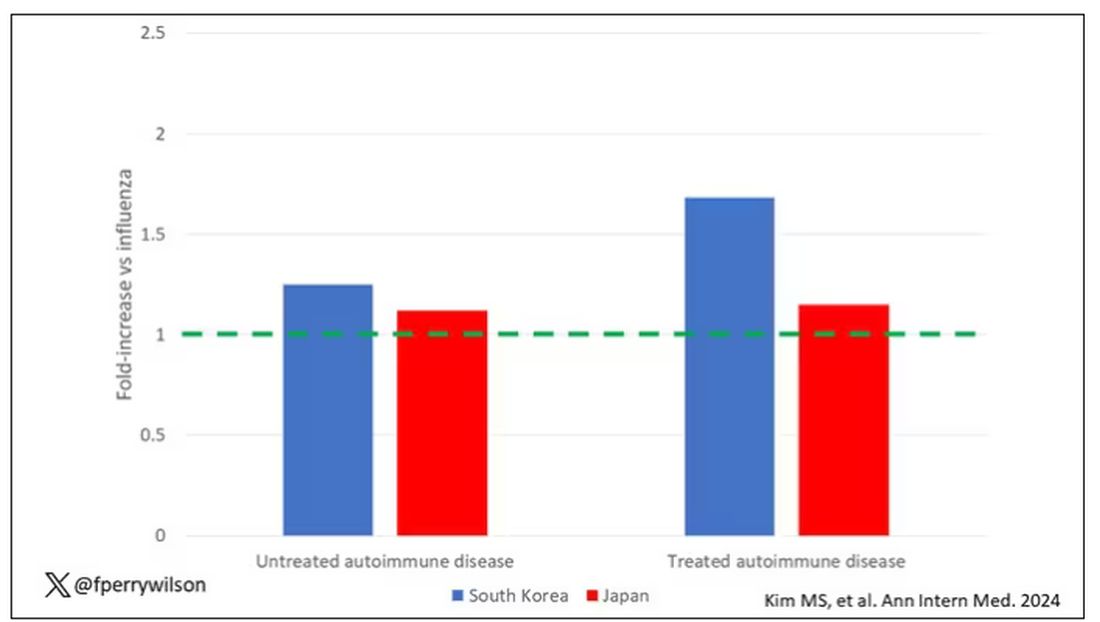
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.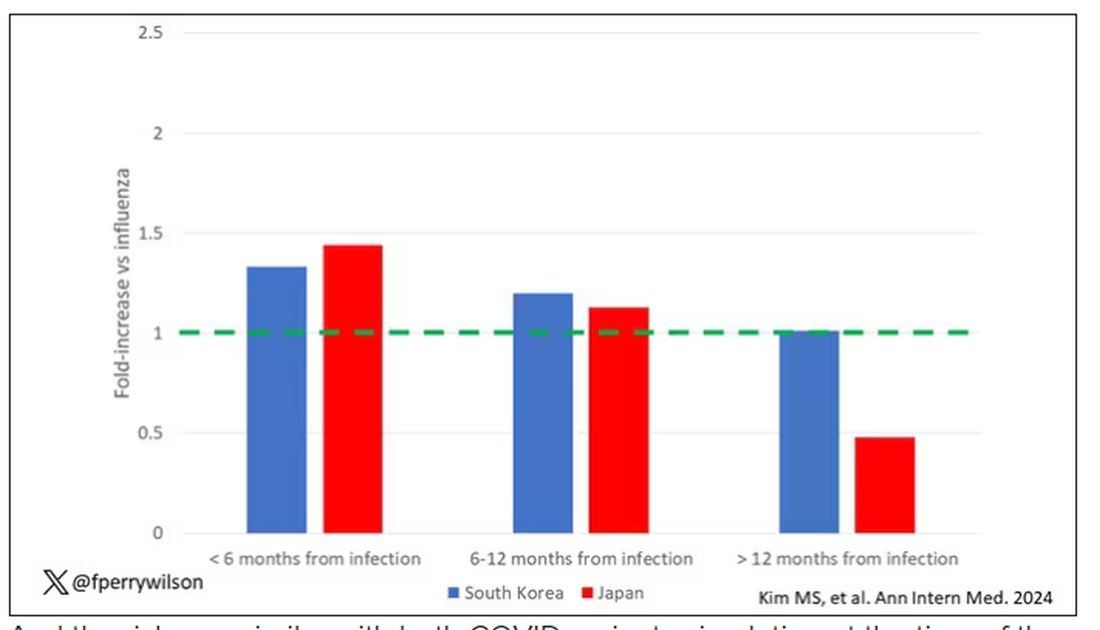
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?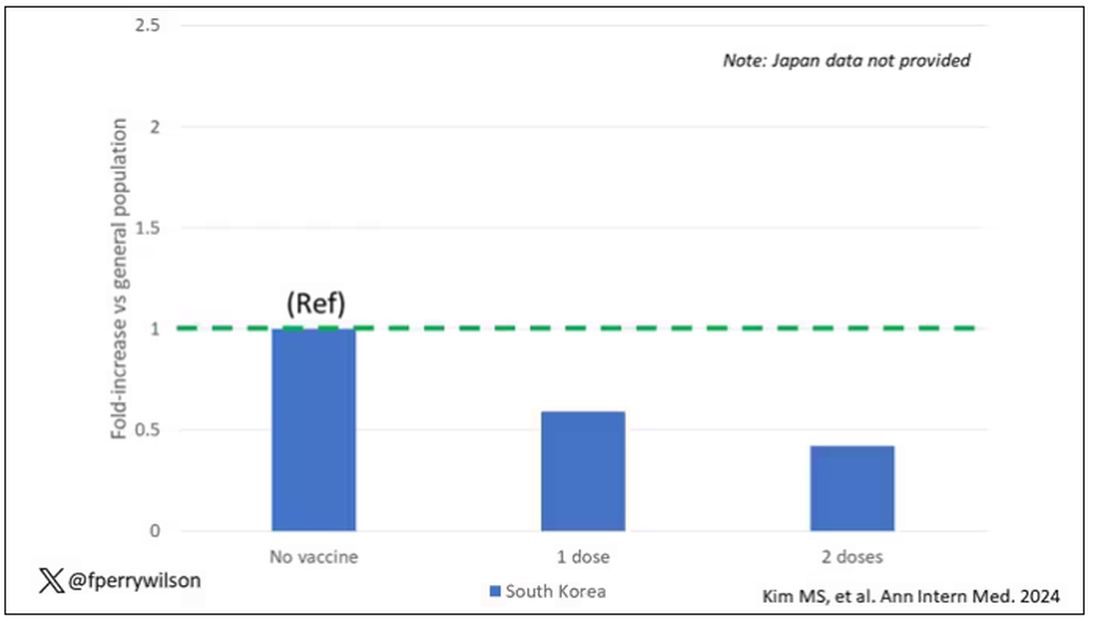
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
What’s Eating You? Carpet Beetles (Dermestidae)
Carpet beetle larvae of the family Dermestidae have been documented to cause both acute and delayed hypersensitivity reactions in susceptible individuals. These larvae have specialized horizontal rows of spear-shaped hairs called hastisetae, which detach easily into the surrounding environment and are small enough to travel by air. Exposure to hastisetae has been tied to adverse effects ranging from dermatitis to rhinoconjunctivitis and acute asthma, with treatment being mostly empiric and symptom based. Due to the pervasiveness of carpet beetles in homes, improved awareness of dermestid-induced manifestations is valuable for clinicians.
Beetles in the Dermestidae family do not bite humans but have been reported to cause skin reactions in addition to other symptoms typical of an allergic reaction. Skin contact with larval hairs (hastisetae) of these insects—known as carpet, larder, or hide beetles — may cause urticarial or edematous papules that are mistaken for papular urticaria or arthropod bites. 1 There are approximately 500 to 700 species of carpet beetles worldwide. Carpet beetles are a clinically underrecognized cause of allergic contact dermatitis given their frequent presence in homes across the world. 2 Carpet beetle larvae feed on shed skin, feathers, hair, wool, book bindings, felt, leather, wood, silk, and sometimes grains and thus can be found nearly anywhere. Most symptom-inducing exposures to Dermestidae beetles occur occupationally, such as in museum curators working hands-on with collection materials and workers handling infested materials such as wool. 3,4 In-home Dermestidae exposure may lead to symptoms, especially if regularly worn clothing and bedding materials are infested. The broad palate of dermestid members has resulted in substantial contamination of stored materials such as flour and fabric in addition to the destruction of museum collections. 5-7
The larvae of some dermestid species, most commonly of the genera Anthrenus and Dermestes, are 2 to 3 mm in length and have detachable hairlike hastisetae that shed into the surrounding environment throughout larval development (Figure 1).8 The hastisetae, located on the thoracic and abdominal segments (tergites), serve as a larval defense mechanism. When prodded, the round, hairy, wormlike larvae tense up and can raise their abdominal tergites while splaying the hastisetae out in a fanlike manner.9 Similar to porcupine quills, the hastisetae easily detach and can entrap the appendages of invertebrate predators. Hastisetae are not known to be sharp enough to puncture human skin, but friction and irritation from skin contact and superficial sticking of the hastisetae into mucous membranes and noncornified epithelium, such as in the bronchial airways, are thought to induce hypersensitivity reactions in susceptible individuals.

Additionally, hastisetae and the exoskeletons of both adult and larval dermestid beetles are composed mostly of chitin, which is highly allergenic. Chitin has been found to play a proinflammatory role in ocular inflammation, asthma, and bronchial reactivity via T helper cell (TH2)–mediated cellular interactions.10-12 Larvae shed their exoskeletons, including hastisetae, multiple times over the course of their development, which contributes to their potential allergen burden (Figure 2). Reports of positive prick and/or patch testing to larval components indicate some cases of both acute type 1 and delayed type 4 hypersensitivity reactions.4,8,13

Clinical Presentation and Diagnosis
Multiple erythematous urticarial papules, papulopustules, and papulovesicles are the typical manifestations of dermestid dermatitis.3,4,13-16 Figure 3 demonstrates several characteristic edematous papules with background erythema. Unlike the clusters seen with flea and bed bug bites, dermestid-induced lesions typically are single and scattered, with a propensity for exposed limbs and the face. Exposure to hastisetae commonly results in classic allergic symptoms including rhinitis, conjunctivitis, coughing, wheezing, sneezing, and intranasal and periocular pruritus, even in those with no personal history of atopy.17-19 Lymphadenopathy, vasculitis, and allergic alveolitis also have been reported.20 A large infestation in which many individual beetles as well as larvae can be found in 1 or more areas of the inhabited structure has been reported to cause more severe symptoms, including acute eczema, otitis externa, lymphocytic vasculitis, and allergic alveolitis, all of which resolved within 3 months of thorough deinfestation cleaning.21

Skin-prick and/or patch testing is not necessary for this clinical diagnosis of dermestid-induced allergic contact dermatitis. This diagnosis is bolstered by (but does not require a history of) repeated symptom induction upon performing certain activities (eg, handling taxidermy specimens) and/or in certain environments (eg, only at home). Because of individual differences in hypersensitivity to dermestid parts, it is not typical for all members of a household to be affected.
When there are multiple potential suspected allergens or an unknown cause for symptoms despite a detailed history, allergy testing can be useful in confirming a diagnosis and directing management. Immediate-onset type 1 hypersensitivity reactions are evaluated using skin-prick testing or serum IgE levels, whereas delayed type 4 hypersensitivity reactions can be evaluated using patch testing. Type 1 reactions tend to present with classic allergy symptoms, especially where there are abundant mast cells to degranulate in the skin and mucosa of the gastrointestinal and respiratory tracts; these symptoms range from mild wheezing, urticaria, periorbital pruritus, and sneezing to outright asthma, diarrhea, rhinoconjunctivitis, and even anaphylaxis. With these reactions, initial exposure to an antigen such as chitin in the hastisetae leads to an asymptomatic sensitization against the antigen in which its introduction leads to a TH2-skewed cellular response, which promotes B-cell production of IgE antibodies. Upon subsequent exposure to this antigen, IgE antibodies bound to mast cells will lead them to degranulate with release of histamine and other proinflammatory molecules, resulting in clinical manifestations. The skin-prick test relies on introduction of potential antigens through the epidermis into the dermis with a sharp lancet to induce IgE antibody activation and then degranulation of the patient’s mast cells, resulting in a pruritic erythematous wheal. This IgE-mediated process has been shown to occur in response to dermestid larval parts among household dust, resulting in chronic coughing, sneezing, nasal pruritus, and asthma.15,17,22
Type 4 hypersensitivity reactions are T-cell mediated and also include a sensitization phase followed by symptom manifestation upon repeat exposure; however, these reactions usually are not immediate and can take up to 72 hours after exposure to manifest.23 This is because T cells specific to the antigen do not lead a process resulting in antibodies but instead recruit numerous other TH1-polarized mediators upon re-exposure to activate cytotoxic CD8+ T cells and macrophages to attempt to neutralize the antigen. Many type 4 reactions result in mostly cutaneous manifestations, such as contact dermatitis. Patch testing involves adhering potential allergens to the skin for a time with assessments at regular intervals to evaluate the level of reaction from weakly positive to severe. At minimum, most reports of dermestid-related manifestations include a rash such as erythematous papules, and several published cases involving patch testing have yielded positive results to various preparations of larval parts.3,14,21
Management and Treatment
Prevention of dermestid exposure is difficult given the myriad materials eaten by the larvae. An insect exterminator should verify and treat a carpet beetle infestation, while a dermatologist can treat symptomatic individuals. Treatment is driven by the severity of the patient’s discomfort and is aimed at both symptomatic relief and reducing dermestid exposure moving forward. Although in certain environments it will be nearly impossible to eradicate Dermestidae, cleaning thoroughly and regularly may go far to reduce exposure and associated symptoms.
Clothing and other materials such as bedding that will have direct skin contact should be washed to remove hastisetae and be stored in airtight containers in addition to items made with animal fibers, such as wool sweaters and down blankets. Mattresses, flooring, rugs, curtains, and other amenable areas should be vacuumed thoroughly, and the vacuum bag should be placed in the trash afterward. Protective pillow and mattress covers should be used. Stuffed animals in infested areas should be thrown away if not able to be completely washed and dried. Air conditioning systems may spread larval hairs away from the site of infestation and should be cleaned as much as possible. Surfaces where beetles and larvae also are commonly seen, such as windowsills, and hidden among closet and pantry items should also be wiped clean to remove both insects and potential substrate. In one case, scraping the wood flooring and applying a thick coat of varnish in addition to removing all stuffed animals from an affected individual’s home allowed for resolution of symptoms.17
Treatment for symptoms includes topical anti-inflammatory agents and/or oral antihistamines, with improvement in symptoms typically occurring within days and resolution dependent on level of exposure moving forward.
Final Thoughts
- Gumina ME, Yan AC. Carpet beetle dermatitis mimicking bullous impetigo. Pediatr Dermatol. 2021;38:329-331. doi:10.1111/pde.14453
- Bertone MA, Leong M, Bayless KM, et al. Arthropods of the great indoors: characterizing diversity inside urban and suburban homes. PeerJ. 2016;4:E1582. doi:10.7717/peerj.1582
- Siegel S, Lee N, Rohr A, et. al. Evaluation of dermestid sensitivity in museum personnel. J Allergy Clin Immunol. 1991;87:190. doi:10.1016/0091-6749(91)91488-F
- Brito FF, Mur P, Barber D, et al. Occupational rhinoconjunctivitis and asthma in a wool worker caused by Dermestidae spp. Allergy. 2002;57:1191-1194.
- Stengaard HL, Akerlund M, Grontoft T, et al. Future pest status of an insect pest in museums, Attagenus smirnovi: distribution and food consumption in relation to climate change. J Cult Herit. 2012;13:22l-227.
- Veer V, Negi BK, Rao KM. Dermestid beetles and some other insect pests associated with stored silkworm cocoons in India, including a world list of dermestid species found attacking this commodity. J Stored Products Research. 1996;32:69-89.
- Veer V, Prasad R, Rao KM. Taxonomic and biological notes on Attagenus and Anthrenus spp. (Coleoptera: Dermestidae) found damaging stored woolen fabrics in India. J Stored Products Research. 1991;27:189-198.
- Háva J. World Catalogue of Insects. Volume 13. Dermestidae (Coleoptera). Brill; 2015.
- Ruzzier E, Kadej M, Di Giulio A, et al. Entangling the enemy: ecological, systematic, and medical implications of dermestid beetle Hastisetae. Insects. 2021;12:436. doi:10.3390/insects12050436
- Arae K, Morita H, Unno H, et al. Chitin promotes antigen-specific Th2 cell-mediated murine asthma through induction of IL-33-mediated IL-1β production by DCs. Sci Rep. 2018;8:11721.
- Brinchmann BC, Bayat M, Brøgger T, et. al. A possible role of chitin in the pathogenesis of asthma and allergy. Ann Agric Environ Med. 2011;18:7-12.
- Bucolo C, Musumeci M, Musumeci S, et al. Acidic mammalian chitinase and the eye: implications for ocular inflammatory diseases. Front Pharmacol. 2011;2:1-4.
- Hoverson K, Wohltmann WE, Pollack RJ, et al. Dermestid dermatitis in a 2-year-old girl: case report and review of the literature. Pediatr Dermatol. 2015;32:E228-E233. doi:10.1111/pde.12641
- Simon L, Boukari F, Oumarou H, et al. Anthrenus sp. and an uncommon cluster of dermatitis. Emerg Infect Dis. 2021;27:1940-1943. doi:10.3201/eid2707.203245
- Ahmed R, Moy R, Barr R, et al. Carpet beetle dermatitis. J Am Acad Dermatol. 1981;5:428-432.
- MacArthur K, Richardson V, Novoa R, et al. Carpet beetle dermatitis: a possibly under-recognized entity. Int J Dermatol. 2016;55:577-579.
- Cuesta-Herranz J, de las Heras M, Sastre J, et al. Asthma caused by Dermestidae (black carpet beetle): a new allergen in house dust. J Allergy Clin Immunol. 1997;99(1 Pt 1):147-149.
- Bernstein J, Morgan M, Ghosh D, et al. Respiratory sensitization of a worker to the warehouse beetle Trogoderma variabile: an index case report. J Allergy Clin Immunol. 2009;123:1413-1416.
- Gorgojo IE, De Las Heras M, Pastor C, et al. Allergy to Dermestidae: a new indoor allergen? [abstract] J Allergy Clin Immunol. 2015;135:AB105.
- Ruzzier E, Kadej M, Battisti A. Occurrence, ecological function and medical importance of dermestid beetle hastisetae. PeerJ. 2020;8:E8340. doi:10.7717/peerj.8340
- Ramachandran J, Hern J, Almeyda J, et al. Contact dermatitis with cervical lymphadenopathy following exposure to the hide beetle, Dermestes peruvianus. Br J Dermatol. 1997;136:943-945.
- Horster S, Prinz J, Holm N, et al. Anthrenus-dermatitis. Hautarzt. 2002;53:328-331.
- Justiz Vaillant AA, Vashisht R, Zito PM. Immediate hypersensitivity reactions. In: StatPearls. StatPearls Publishing; 2023.
Carpet beetle larvae of the family Dermestidae have been documented to cause both acute and delayed hypersensitivity reactions in susceptible individuals. These larvae have specialized horizontal rows of spear-shaped hairs called hastisetae, which detach easily into the surrounding environment and are small enough to travel by air. Exposure to hastisetae has been tied to adverse effects ranging from dermatitis to rhinoconjunctivitis and acute asthma, with treatment being mostly empiric and symptom based. Due to the pervasiveness of carpet beetles in homes, improved awareness of dermestid-induced manifestations is valuable for clinicians.
Beetles in the Dermestidae family do not bite humans but have been reported to cause skin reactions in addition to other symptoms typical of an allergic reaction. Skin contact with larval hairs (hastisetae) of these insects—known as carpet, larder, or hide beetles — may cause urticarial or edematous papules that are mistaken for papular urticaria or arthropod bites. 1 There are approximately 500 to 700 species of carpet beetles worldwide. Carpet beetles are a clinically underrecognized cause of allergic contact dermatitis given their frequent presence in homes across the world. 2 Carpet beetle larvae feed on shed skin, feathers, hair, wool, book bindings, felt, leather, wood, silk, and sometimes grains and thus can be found nearly anywhere. Most symptom-inducing exposures to Dermestidae beetles occur occupationally, such as in museum curators working hands-on with collection materials and workers handling infested materials such as wool. 3,4 In-home Dermestidae exposure may lead to symptoms, especially if regularly worn clothing and bedding materials are infested. The broad palate of dermestid members has resulted in substantial contamination of stored materials such as flour and fabric in addition to the destruction of museum collections. 5-7
The larvae of some dermestid species, most commonly of the genera Anthrenus and Dermestes, are 2 to 3 mm in length and have detachable hairlike hastisetae that shed into the surrounding environment throughout larval development (Figure 1).8 The hastisetae, located on the thoracic and abdominal segments (tergites), serve as a larval defense mechanism. When prodded, the round, hairy, wormlike larvae tense up and can raise their abdominal tergites while splaying the hastisetae out in a fanlike manner.9 Similar to porcupine quills, the hastisetae easily detach and can entrap the appendages of invertebrate predators. Hastisetae are not known to be sharp enough to puncture human skin, but friction and irritation from skin contact and superficial sticking of the hastisetae into mucous membranes and noncornified epithelium, such as in the bronchial airways, are thought to induce hypersensitivity reactions in susceptible individuals.
Additionally, hastisetae and the exoskeletons of both adult and larval dermestid beetles are composed mostly of chitin, which is highly allergenic. Chitin has been found to play a proinflammatory role in ocular inflammation, asthma, and bronchial reactivity via T helper cell (TH2)–mediated cellular interactions.10-12 Larvae shed their exoskeletons, including hastisetae, multiple times over the course of their development, which contributes to their potential allergen burden (Figure 2). Reports of positive prick and/or patch testing to larval components indicate some cases of both acute type 1 and delayed type 4 hypersensitivity reactions.4,8,13
Clinical Presentation and Diagnosis
Multiple erythematous urticarial papules, papulopustules, and papulovesicles are the typical manifestations of dermestid dermatitis.3,4,13-16 Figure 3 demonstrates several characteristic edematous papules with background erythema. Unlike the clusters seen with flea and bed bug bites, dermestid-induced lesions typically are single and scattered, with a propensity for exposed limbs and the face. Exposure to hastisetae commonly results in classic allergic symptoms including rhinitis, conjunctivitis, coughing, wheezing, sneezing, and intranasal and periocular pruritus, even in those with no personal history of atopy.17-19 Lymphadenopathy, vasculitis, and allergic alveolitis also have been reported.20 A large infestation in which many individual beetles as well as larvae can be found in 1 or more areas of the inhabited structure has been reported to cause more severe symptoms, including acute eczema, otitis externa, lymphocytic vasculitis, and allergic alveolitis, all of which resolved within 3 months of thorough deinfestation cleaning.21
Skin-prick and/or patch testing is not necessary for this clinical diagnosis of dermestid-induced allergic contact dermatitis. This diagnosis is bolstered by (but does not require a history of) repeated symptom induction upon performing certain activities (eg, handling taxidermy specimens) and/or in certain environments (eg, only at home). Because of individual differences in hypersensitivity to dermestid parts, it is not typical for all members of a household to be affected.
When there are multiple potential suspected allergens or an unknown cause for symptoms despite a detailed history, allergy testing can be useful in confirming a diagnosis and directing management. Immediate-onset type 1 hypersensitivity reactions are evaluated using skin-prick testing or serum IgE levels, whereas delayed type 4 hypersensitivity reactions can be evaluated using patch testing. Type 1 reactions tend to present with classic allergy symptoms, especially where there are abundant mast cells to degranulate in the skin and mucosa of the gastrointestinal and respiratory tracts; these symptoms range from mild wheezing, urticaria, periorbital pruritus, and sneezing to outright asthma, diarrhea, rhinoconjunctivitis, and even anaphylaxis. With these reactions, initial exposure to an antigen such as chitin in the hastisetae leads to an asymptomatic sensitization against the antigen in which its introduction leads to a TH2-skewed cellular response, which promotes B-cell production of IgE antibodies. Upon subsequent exposure to this antigen, IgE antibodies bound to mast cells will lead them to degranulate with release of histamine and other proinflammatory molecules, resulting in clinical manifestations. The skin-prick test relies on introduction of potential antigens through the epidermis into the dermis with a sharp lancet to induce IgE antibody activation and then degranulation of the patient’s mast cells, resulting in a pruritic erythematous wheal. This IgE-mediated process has been shown to occur in response to dermestid larval parts among household dust, resulting in chronic coughing, sneezing, nasal pruritus, and asthma.15,17,22
Type 4 hypersensitivity reactions are T-cell mediated and also include a sensitization phase followed by symptom manifestation upon repeat exposure; however, these reactions usually are not immediate and can take up to 72 hours after exposure to manifest.23 This is because T cells specific to the antigen do not lead a process resulting in antibodies but instead recruit numerous other TH1-polarized mediators upon re-exposure to activate cytotoxic CD8+ T cells and macrophages to attempt to neutralize the antigen. Many type 4 reactions result in mostly cutaneous manifestations, such as contact dermatitis. Patch testing involves adhering potential allergens to the skin for a time with assessments at regular intervals to evaluate the level of reaction from weakly positive to severe. At minimum, most reports of dermestid-related manifestations include a rash such as erythematous papules, and several published cases involving patch testing have yielded positive results to various preparations of larval parts.3,14,21
Management and Treatment
Prevention of dermestid exposure is difficult given the myriad materials eaten by the larvae. An insect exterminator should verify and treat a carpet beetle infestation, while a dermatologist can treat symptomatic individuals. Treatment is driven by the severity of the patient’s discomfort and is aimed at both symptomatic relief and reducing dermestid exposure moving forward. Although in certain environments it will be nearly impossible to eradicate Dermestidae, cleaning thoroughly and regularly may go far to reduce exposure and associated symptoms.
Clothing and other materials such as bedding that will have direct skin contact should be washed to remove hastisetae and be stored in airtight containers in addition to items made with animal fibers, such as wool sweaters and down blankets. Mattresses, flooring, rugs, curtains, and other amenable areas should be vacuumed thoroughly, and the vacuum bag should be placed in the trash afterward. Protective pillow and mattress covers should be used. Stuffed animals in infested areas should be thrown away if not able to be completely washed and dried. Air conditioning systems may spread larval hairs away from the site of infestation and should be cleaned as much as possible. Surfaces where beetles and larvae also are commonly seen, such as windowsills, and hidden among closet and pantry items should also be wiped clean to remove both insects and potential substrate. In one case, scraping the wood flooring and applying a thick coat of varnish in addition to removing all stuffed animals from an affected individual’s home allowed for resolution of symptoms.17
Treatment for symptoms includes topical anti-inflammatory agents and/or oral antihistamines, with improvement in symptoms typically occurring within days and resolution dependent on level of exposure moving forward.
Final Thoughts
Carpet beetle larvae of the family Dermestidae have been documented to cause both acute and delayed hypersensitivity reactions in susceptible individuals. These larvae have specialized horizontal rows of spear-shaped hairs called hastisetae, which detach easily into the surrounding environment and are small enough to travel by air. Exposure to hastisetae has been tied to adverse effects ranging from dermatitis to rhinoconjunctivitis and acute asthma, with treatment being mostly empiric and symptom based. Due to the pervasiveness of carpet beetles in homes, improved awareness of dermestid-induced manifestations is valuable for clinicians.
Beetles in the Dermestidae family do not bite humans but have been reported to cause skin reactions in addition to other symptoms typical of an allergic reaction. Skin contact with larval hairs (hastisetae) of these insects—known as carpet, larder, or hide beetles — may cause urticarial or edematous papules that are mistaken for papular urticaria or arthropod bites. 1 There are approximately 500 to 700 species of carpet beetles worldwide. Carpet beetles are a clinically underrecognized cause of allergic contact dermatitis given their frequent presence in homes across the world. 2 Carpet beetle larvae feed on shed skin, feathers, hair, wool, book bindings, felt, leather, wood, silk, and sometimes grains and thus can be found nearly anywhere. Most symptom-inducing exposures to Dermestidae beetles occur occupationally, such as in museum curators working hands-on with collection materials and workers handling infested materials such as wool. 3,4 In-home Dermestidae exposure may lead to symptoms, especially if regularly worn clothing and bedding materials are infested. The broad palate of dermestid members has resulted in substantial contamination of stored materials such as flour and fabric in addition to the destruction of museum collections. 5-7
The larvae of some dermestid species, most commonly of the genera Anthrenus and Dermestes, are 2 to 3 mm in length and have detachable hairlike hastisetae that shed into the surrounding environment throughout larval development (Figure 1).8 The hastisetae, located on the thoracic and abdominal segments (tergites), serve as a larval defense mechanism. When prodded, the round, hairy, wormlike larvae tense up and can raise their abdominal tergites while splaying the hastisetae out in a fanlike manner.9 Similar to porcupine quills, the hastisetae easily detach and can entrap the appendages of invertebrate predators. Hastisetae are not known to be sharp enough to puncture human skin, but friction and irritation from skin contact and superficial sticking of the hastisetae into mucous membranes and noncornified epithelium, such as in the bronchial airways, are thought to induce hypersensitivity reactions in susceptible individuals.
Additionally, hastisetae and the exoskeletons of both adult and larval dermestid beetles are composed mostly of chitin, which is highly allergenic. Chitin has been found to play a proinflammatory role in ocular inflammation, asthma, and bronchial reactivity via T helper cell (TH2)–mediated cellular interactions.10-12 Larvae shed their exoskeletons, including hastisetae, multiple times over the course of their development, which contributes to their potential allergen burden (Figure 2). Reports of positive prick and/or patch testing to larval components indicate some cases of both acute type 1 and delayed type 4 hypersensitivity reactions.4,8,13
Clinical Presentation and Diagnosis
Multiple erythematous urticarial papules, papulopustules, and papulovesicles are the typical manifestations of dermestid dermatitis.3,4,13-16 Figure 3 demonstrates several characteristic edematous papules with background erythema. Unlike the clusters seen with flea and bed bug bites, dermestid-induced lesions typically are single and scattered, with a propensity for exposed limbs and the face. Exposure to hastisetae commonly results in classic allergic symptoms including rhinitis, conjunctivitis, coughing, wheezing, sneezing, and intranasal and periocular pruritus, even in those with no personal history of atopy.17-19 Lymphadenopathy, vasculitis, and allergic alveolitis also have been reported.20 A large infestation in which many individual beetles as well as larvae can be found in 1 or more areas of the inhabited structure has been reported to cause more severe symptoms, including acute eczema, otitis externa, lymphocytic vasculitis, and allergic alveolitis, all of which resolved within 3 months of thorough deinfestation cleaning.21
Skin-prick and/or patch testing is not necessary for this clinical diagnosis of dermestid-induced allergic contact dermatitis. This diagnosis is bolstered by (but does not require a history of) repeated symptom induction upon performing certain activities (eg, handling taxidermy specimens) and/or in certain environments (eg, only at home). Because of individual differences in hypersensitivity to dermestid parts, it is not typical for all members of a household to be affected.
When there are multiple potential suspected allergens or an unknown cause for symptoms despite a detailed history, allergy testing can be useful in confirming a diagnosis and directing management. Immediate-onset type 1 hypersensitivity reactions are evaluated using skin-prick testing or serum IgE levels, whereas delayed type 4 hypersensitivity reactions can be evaluated using patch testing. Type 1 reactions tend to present with classic allergy symptoms, especially where there are abundant mast cells to degranulate in the skin and mucosa of the gastrointestinal and respiratory tracts; these symptoms range from mild wheezing, urticaria, periorbital pruritus, and sneezing to outright asthma, diarrhea, rhinoconjunctivitis, and even anaphylaxis. With these reactions, initial exposure to an antigen such as chitin in the hastisetae leads to an asymptomatic sensitization against the antigen in which its introduction leads to a TH2-skewed cellular response, which promotes B-cell production of IgE antibodies. Upon subsequent exposure to this antigen, IgE antibodies bound to mast cells will lead them to degranulate with release of histamine and other proinflammatory molecules, resulting in clinical manifestations. The skin-prick test relies on introduction of potential antigens through the epidermis into the dermis with a sharp lancet to induce IgE antibody activation and then degranulation of the patient’s mast cells, resulting in a pruritic erythematous wheal. This IgE-mediated process has been shown to occur in response to dermestid larval parts among household dust, resulting in chronic coughing, sneezing, nasal pruritus, and asthma.15,17,22
Type 4 hypersensitivity reactions are T-cell mediated and also include a sensitization phase followed by symptom manifestation upon repeat exposure; however, these reactions usually are not immediate and can take up to 72 hours after exposure to manifest.23 This is because T cells specific to the antigen do not lead a process resulting in antibodies but instead recruit numerous other TH1-polarized mediators upon re-exposure to activate cytotoxic CD8+ T cells and macrophages to attempt to neutralize the antigen. Many type 4 reactions result in mostly cutaneous manifestations, such as contact dermatitis. Patch testing involves adhering potential allergens to the skin for a time with assessments at regular intervals to evaluate the level of reaction from weakly positive to severe. At minimum, most reports of dermestid-related manifestations include a rash such as erythematous papules, and several published cases involving patch testing have yielded positive results to various preparations of larval parts.3,14,21
Management and Treatment
Prevention of dermestid exposure is difficult given the myriad materials eaten by the larvae. An insect exterminator should verify and treat a carpet beetle infestation, while a dermatologist can treat symptomatic individuals. Treatment is driven by the severity of the patient’s discomfort and is aimed at both symptomatic relief and reducing dermestid exposure moving forward. Although in certain environments it will be nearly impossible to eradicate Dermestidae, cleaning thoroughly and regularly may go far to reduce exposure and associated symptoms.
Clothing and other materials such as bedding that will have direct skin contact should be washed to remove hastisetae and be stored in airtight containers in addition to items made with animal fibers, such as wool sweaters and down blankets. Mattresses, flooring, rugs, curtains, and other amenable areas should be vacuumed thoroughly, and the vacuum bag should be placed in the trash afterward. Protective pillow and mattress covers should be used. Stuffed animals in infested areas should be thrown away if not able to be completely washed and dried. Air conditioning systems may spread larval hairs away from the site of infestation and should be cleaned as much as possible. Surfaces where beetles and larvae also are commonly seen, such as windowsills, and hidden among closet and pantry items should also be wiped clean to remove both insects and potential substrate. In one case, scraping the wood flooring and applying a thick coat of varnish in addition to removing all stuffed animals from an affected individual’s home allowed for resolution of symptoms.17
Treatment for symptoms includes topical anti-inflammatory agents and/or oral antihistamines, with improvement in symptoms typically occurring within days and resolution dependent on level of exposure moving forward.
Final Thoughts
- Gumina ME, Yan AC. Carpet beetle dermatitis mimicking bullous impetigo. Pediatr Dermatol. 2021;38:329-331. doi:10.1111/pde.14453
- Bertone MA, Leong M, Bayless KM, et al. Arthropods of the great indoors: characterizing diversity inside urban and suburban homes. PeerJ. 2016;4:E1582. doi:10.7717/peerj.1582
- Siegel S, Lee N, Rohr A, et. al. Evaluation of dermestid sensitivity in museum personnel. J Allergy Clin Immunol. 1991;87:190. doi:10.1016/0091-6749(91)91488-F
- Brito FF, Mur P, Barber D, et al. Occupational rhinoconjunctivitis and asthma in a wool worker caused by Dermestidae spp. Allergy. 2002;57:1191-1194.
- Stengaard HL, Akerlund M, Grontoft T, et al. Future pest status of an insect pest in museums, Attagenus smirnovi: distribution and food consumption in relation to climate change. J Cult Herit. 2012;13:22l-227.
- Veer V, Negi BK, Rao KM. Dermestid beetles and some other insect pests associated with stored silkworm cocoons in India, including a world list of dermestid species found attacking this commodity. J Stored Products Research. 1996;32:69-89.
- Veer V, Prasad R, Rao KM. Taxonomic and biological notes on Attagenus and Anthrenus spp. (Coleoptera: Dermestidae) found damaging stored woolen fabrics in India. J Stored Products Research. 1991;27:189-198.
- Háva J. World Catalogue of Insects. Volume 13. Dermestidae (Coleoptera). Brill; 2015.
- Ruzzier E, Kadej M, Di Giulio A, et al. Entangling the enemy: ecological, systematic, and medical implications of dermestid beetle Hastisetae. Insects. 2021;12:436. doi:10.3390/insects12050436
- Arae K, Morita H, Unno H, et al. Chitin promotes antigen-specific Th2 cell-mediated murine asthma through induction of IL-33-mediated IL-1β production by DCs. Sci Rep. 2018;8:11721.
- Brinchmann BC, Bayat M, Brøgger T, et. al. A possible role of chitin in the pathogenesis of asthma and allergy. Ann Agric Environ Med. 2011;18:7-12.
- Bucolo C, Musumeci M, Musumeci S, et al. Acidic mammalian chitinase and the eye: implications for ocular inflammatory diseases. Front Pharmacol. 2011;2:1-4.
- Hoverson K, Wohltmann WE, Pollack RJ, et al. Dermestid dermatitis in a 2-year-old girl: case report and review of the literature. Pediatr Dermatol. 2015;32:E228-E233. doi:10.1111/pde.12641
- Simon L, Boukari F, Oumarou H, et al. Anthrenus sp. and an uncommon cluster of dermatitis. Emerg Infect Dis. 2021;27:1940-1943. doi:10.3201/eid2707.203245
- Ahmed R, Moy R, Barr R, et al. Carpet beetle dermatitis. J Am Acad Dermatol. 1981;5:428-432.
- MacArthur K, Richardson V, Novoa R, et al. Carpet beetle dermatitis: a possibly under-recognized entity. Int J Dermatol. 2016;55:577-579.
- Cuesta-Herranz J, de las Heras M, Sastre J, et al. Asthma caused by Dermestidae (black carpet beetle): a new allergen in house dust. J Allergy Clin Immunol. 1997;99(1 Pt 1):147-149.
- Bernstein J, Morgan M, Ghosh D, et al. Respiratory sensitization of a worker to the warehouse beetle Trogoderma variabile: an index case report. J Allergy Clin Immunol. 2009;123:1413-1416.
- Gorgojo IE, De Las Heras M, Pastor C, et al. Allergy to Dermestidae: a new indoor allergen? [abstract] J Allergy Clin Immunol. 2015;135:AB105.
- Ruzzier E, Kadej M, Battisti A. Occurrence, ecological function and medical importance of dermestid beetle hastisetae. PeerJ. 2020;8:E8340. doi:10.7717/peerj.8340
- Ramachandran J, Hern J, Almeyda J, et al. Contact dermatitis with cervical lymphadenopathy following exposure to the hide beetle, Dermestes peruvianus. Br J Dermatol. 1997;136:943-945.
- Horster S, Prinz J, Holm N, et al. Anthrenus-dermatitis. Hautarzt. 2002;53:328-331.
- Justiz Vaillant AA, Vashisht R, Zito PM. Immediate hypersensitivity reactions. In: StatPearls. StatPearls Publishing; 2023.
- Gumina ME, Yan AC. Carpet beetle dermatitis mimicking bullous impetigo. Pediatr Dermatol. 2021;38:329-331. doi:10.1111/pde.14453
- Bertone MA, Leong M, Bayless KM, et al. Arthropods of the great indoors: characterizing diversity inside urban and suburban homes. PeerJ. 2016;4:E1582. doi:10.7717/peerj.1582
- Siegel S, Lee N, Rohr A, et. al. Evaluation of dermestid sensitivity in museum personnel. J Allergy Clin Immunol. 1991;87:190. doi:10.1016/0091-6749(91)91488-F
- Brito FF, Mur P, Barber D, et al. Occupational rhinoconjunctivitis and asthma in a wool worker caused by Dermestidae spp. Allergy. 2002;57:1191-1194.
- Stengaard HL, Akerlund M, Grontoft T, et al. Future pest status of an insect pest in museums, Attagenus smirnovi: distribution and food consumption in relation to climate change. J Cult Herit. 2012;13:22l-227.
- Veer V, Negi BK, Rao KM. Dermestid beetles and some other insect pests associated with stored silkworm cocoons in India, including a world list of dermestid species found attacking this commodity. J Stored Products Research. 1996;32:69-89.
- Veer V, Prasad R, Rao KM. Taxonomic and biological notes on Attagenus and Anthrenus spp. (Coleoptera: Dermestidae) found damaging stored woolen fabrics in India. J Stored Products Research. 1991;27:189-198.
- Háva J. World Catalogue of Insects. Volume 13. Dermestidae (Coleoptera). Brill; 2015.
- Ruzzier E, Kadej M, Di Giulio A, et al. Entangling the enemy: ecological, systematic, and medical implications of dermestid beetle Hastisetae. Insects. 2021;12:436. doi:10.3390/insects12050436
- Arae K, Morita H, Unno H, et al. Chitin promotes antigen-specific Th2 cell-mediated murine asthma through induction of IL-33-mediated IL-1β production by DCs. Sci Rep. 2018;8:11721.
- Brinchmann BC, Bayat M, Brøgger T, et. al. A possible role of chitin in the pathogenesis of asthma and allergy. Ann Agric Environ Med. 2011;18:7-12.
- Bucolo C, Musumeci M, Musumeci S, et al. Acidic mammalian chitinase and the eye: implications for ocular inflammatory diseases. Front Pharmacol. 2011;2:1-4.
- Hoverson K, Wohltmann WE, Pollack RJ, et al. Dermestid dermatitis in a 2-year-old girl: case report and review of the literature. Pediatr Dermatol. 2015;32:E228-E233. doi:10.1111/pde.12641
- Simon L, Boukari F, Oumarou H, et al. Anthrenus sp. and an uncommon cluster of dermatitis. Emerg Infect Dis. 2021;27:1940-1943. doi:10.3201/eid2707.203245
- Ahmed R, Moy R, Barr R, et al. Carpet beetle dermatitis. J Am Acad Dermatol. 1981;5:428-432.
- MacArthur K, Richardson V, Novoa R, et al. Carpet beetle dermatitis: a possibly under-recognized entity. Int J Dermatol. 2016;55:577-579.
- Cuesta-Herranz J, de las Heras M, Sastre J, et al. Asthma caused by Dermestidae (black carpet beetle): a new allergen in house dust. J Allergy Clin Immunol. 1997;99(1 Pt 1):147-149.
- Bernstein J, Morgan M, Ghosh D, et al. Respiratory sensitization of a worker to the warehouse beetle Trogoderma variabile: an index case report. J Allergy Clin Immunol. 2009;123:1413-1416.
- Gorgojo IE, De Las Heras M, Pastor C, et al. Allergy to Dermestidae: a new indoor allergen? [abstract] J Allergy Clin Immunol. 2015;135:AB105.
- Ruzzier E, Kadej M, Battisti A. Occurrence, ecological function and medical importance of dermestid beetle hastisetae. PeerJ. 2020;8:E8340. doi:10.7717/peerj.8340
- Ramachandran J, Hern J, Almeyda J, et al. Contact dermatitis with cervical lymphadenopathy following exposure to the hide beetle, Dermestes peruvianus. Br J Dermatol. 1997;136:943-945.
- Horster S, Prinz J, Holm N, et al. Anthrenus-dermatitis. Hautarzt. 2002;53:328-331.
- Justiz Vaillant AA, Vashisht R, Zito PM. Immediate hypersensitivity reactions. In: StatPearls. StatPearls Publishing; 2023.
Practice Points
- Given their ubiquity, dermatologists should be aware of the potential for hypersensitivity reactions to carpet beetles (Dermestidae).
- Pruritic erythematous papules, pustules, and vesicles are the most common manifestations of exposure to larval hairs.
- Treatment is symptom based, and future exposure can be greatly diminished with thorough cleaning of the patient’s environment.

Psilocybin Poison Control Calls Spike in Teens, Young Adults
Calls to US poison centers related to psilocybin more than tripled among teens and more than doubled in young adults between 2019 and 2022, new research suggests. Investigators say the increase may be linked to decriminalization efforts in US cities and states.
METHODOLOGY:
- Investigators used data from the National Poison Data System (NPDS) to identify calls involving psilocybin between January 2013 and December 2022.
- Researchers focused on calls about individuals between the ages of 13 and 25 years.
- Exposures to psilocybin were examined based on demographics, clinical effects, level of care, and medical outcome.
TAKEAWAY:
- During the entire 10-year study period, 4055 psilocybin-involved exposures were reported in the age groups studied, with 66% being single-substance exposures and close to three quarters receiving medical attention.
- Psilocybin’s most common effects were hallucinations or delusions (37% of calls), agitation (28%), tachycardia (20%), and confusion (16%).
- The number of psilocybin-related calls to poison control centers for youth were largely unchanged from 2013 to 2018 but more than tripled among adolescents (aged 13-19 years) from 2019 and 2022 and more than doubled among young adults (aged 20-25 years) between 2018 and 2022 (P < .0001).
IN PRACTICE:
The increase in poison center calls coincides with psilocybin decriminalization efforts in several states in 2019, the authors noted. However, because those efforts only legalized use in adults aged 21 years and older, the rise among younger people is concerning, they added. “As psilocybin may become more widely available, it is important for parents to be aware that psilocybin is also available in edible forms such as chocolate and gummies. And we learned from our experience with edible cannabis that young children can mistake edibles for candy,” lead author Rita Farah, PharmD, MPH, PhD, Blue Ridge Poison Center epidemiologist, said in a news release.
SOURCE:
Christopher Holstege, MD, director of UVA Health’s Blue Ridge Poison Center and chief of the Division of Medical Toxicology at the UVA School of Medicine was the senior and corresponding author of the study. It was published online on February 26 in the Journal of Adolescent Health.
LIMITATIONS:
NPDS data are not designed to assess potential risk factors leading to increases in psilocybin-related cases. Moreover, because reports to poison control centers are voluntary and don’t capture all exposures, NPDS data likely under-represent cases of hallucinogenic mushroom poisonings. Lastly, NPDS data are susceptible to reporting and misclassification biases.
DISCLOSURES:
Funding source was not disclosed. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Calls to US poison centers related to psilocybin more than tripled among teens and more than doubled in young adults between 2019 and 2022, new research suggests. Investigators say the increase may be linked to decriminalization efforts in US cities and states.
METHODOLOGY:
- Investigators used data from the National Poison Data System (NPDS) to identify calls involving psilocybin between January 2013 and December 2022.
- Researchers focused on calls about individuals between the ages of 13 and 25 years.
- Exposures to psilocybin were examined based on demographics, clinical effects, level of care, and medical outcome.
TAKEAWAY:
- During the entire 10-year study period, 4055 psilocybin-involved exposures were reported in the age groups studied, with 66% being single-substance exposures and close to three quarters receiving medical attention.
- Psilocybin’s most common effects were hallucinations or delusions (37% of calls), agitation (28%), tachycardia (20%), and confusion (16%).
- The number of psilocybin-related calls to poison control centers for youth were largely unchanged from 2013 to 2018 but more than tripled among adolescents (aged 13-19 years) from 2019 and 2022 and more than doubled among young adults (aged 20-25 years) between 2018 and 2022 (P < .0001).
IN PRACTICE:
The increase in poison center calls coincides with psilocybin decriminalization efforts in several states in 2019, the authors noted. However, because those efforts only legalized use in adults aged 21 years and older, the rise among younger people is concerning, they added. “As psilocybin may become more widely available, it is important for parents to be aware that psilocybin is also available in edible forms such as chocolate and gummies. And we learned from our experience with edible cannabis that young children can mistake edibles for candy,” lead author Rita Farah, PharmD, MPH, PhD, Blue Ridge Poison Center epidemiologist, said in a news release.
SOURCE:
Christopher Holstege, MD, director of UVA Health’s Blue Ridge Poison Center and chief of the Division of Medical Toxicology at the UVA School of Medicine was the senior and corresponding author of the study. It was published online on February 26 in the Journal of Adolescent Health.
LIMITATIONS:
NPDS data are not designed to assess potential risk factors leading to increases in psilocybin-related cases. Moreover, because reports to poison control centers are voluntary and don’t capture all exposures, NPDS data likely under-represent cases of hallucinogenic mushroom poisonings. Lastly, NPDS data are susceptible to reporting and misclassification biases.
DISCLOSURES:
Funding source was not disclosed. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Calls to US poison centers related to psilocybin more than tripled among teens and more than doubled in young adults between 2019 and 2022, new research suggests. Investigators say the increase may be linked to decriminalization efforts in US cities and states.
METHODOLOGY:
- Investigators used data from the National Poison Data System (NPDS) to identify calls involving psilocybin between January 2013 and December 2022.
- Researchers focused on calls about individuals between the ages of 13 and 25 years.
- Exposures to psilocybin were examined based on demographics, clinical effects, level of care, and medical outcome.
TAKEAWAY:
- During the entire 10-year study period, 4055 psilocybin-involved exposures were reported in the age groups studied, with 66% being single-substance exposures and close to three quarters receiving medical attention.
- Psilocybin’s most common effects were hallucinations or delusions (37% of calls), agitation (28%), tachycardia (20%), and confusion (16%).
- The number of psilocybin-related calls to poison control centers for youth were largely unchanged from 2013 to 2018 but more than tripled among adolescents (aged 13-19 years) from 2019 and 2022 and more than doubled among young adults (aged 20-25 years) between 2018 and 2022 (P < .0001).
IN PRACTICE:
The increase in poison center calls coincides with psilocybin decriminalization efforts in several states in 2019, the authors noted. However, because those efforts only legalized use in adults aged 21 years and older, the rise among younger people is concerning, they added. “As psilocybin may become more widely available, it is important for parents to be aware that psilocybin is also available in edible forms such as chocolate and gummies. And we learned from our experience with edible cannabis that young children can mistake edibles for candy,” lead author Rita Farah, PharmD, MPH, PhD, Blue Ridge Poison Center epidemiologist, said in a news release.
SOURCE:
Christopher Holstege, MD, director of UVA Health’s Blue Ridge Poison Center and chief of the Division of Medical Toxicology at the UVA School of Medicine was the senior and corresponding author of the study. It was published online on February 26 in the Journal of Adolescent Health.
LIMITATIONS:
NPDS data are not designed to assess potential risk factors leading to increases in psilocybin-related cases. Moreover, because reports to poison control centers are voluntary and don’t capture all exposures, NPDS data likely under-represent cases of hallucinogenic mushroom poisonings. Lastly, NPDS data are susceptible to reporting and misclassification biases.
DISCLOSURES:
Funding source was not disclosed. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.