User login
Gender-affirming surgeries nearly tripled between 2016 and 2019: Study
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).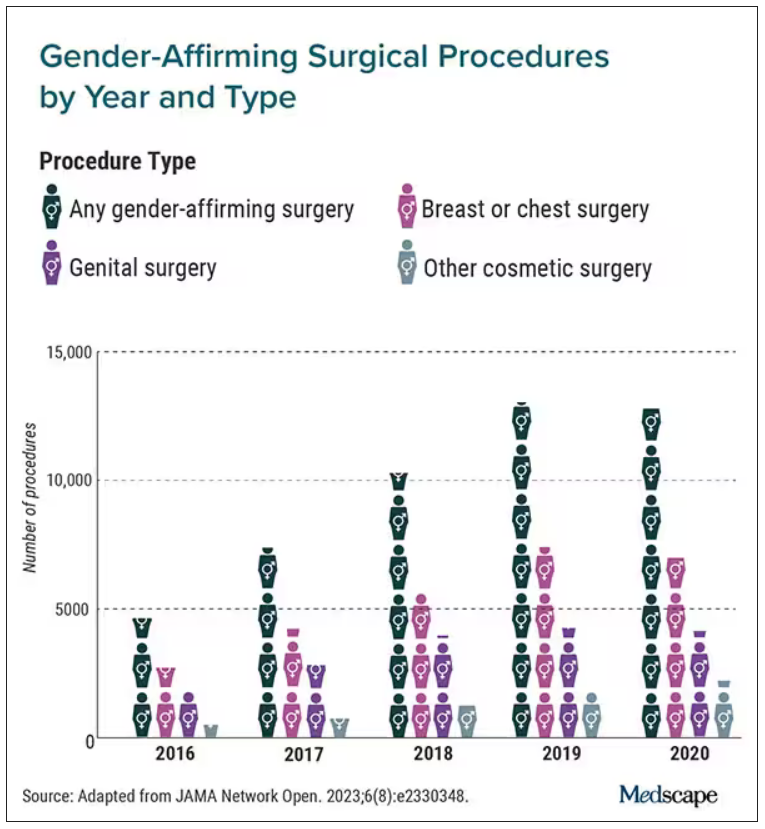
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
High-intensity interval training before major surgery may boost postoperative outcomes
TOPLINE:
It cuts the risk of postoperative complications and may shorten hospital length of stay and improve postoperative quality of life.
METHODOLOGY:
Evidence suggests CRF – which improves physical and cognitive function and is associated with a reduction in cardiovascular risk – can be enhanced before major surgeries, but reported postoperative outcomes in previous reviews have been inconsistent.
In the study, HIIT involved repeated aerobic high-intensity exercise intervals at about 80% of maximum heart rate, followed by active recovery.
The meta-analysis included 12 studies with 832 patients (mean age, 67) that compared preoperative HIIT – supervised at hospitals, gyms, or community or physical therapy centers, or unsupervised at home – with standard care for patients slated for major surgery, including liver, lung, colorectal, urologic, and mixed major abdominal operations.
The primary outcome was change in CRF by peak VO2 or 6-minute walk test; other endpoints included change in endurance time and postoperative outcomes.
TAKEAWAY:
Preoperative HIIT (median total, 160 minutes; range, 80-240 minutes; intense exercise during 6-40 sessions) was associated with an increase in peak oxygen consumption (VO2 peak) by 2.59 mL/kg/min (95% confidence interval, 1.52-3.65 mL/kg/min; P < .001), compared with standard care, which represents about a 10% increase in CRF.
In eight studies that involved 770 patients, there was moderate evidence that preoperative HIIT cut the odds ratio for postoperative complications by more than half (OR, 0.44; 95% CI, 0.32-0.60; P < .001); there was a similar apparent benefit in an analysis that was limited to patients who were slated for abdominal surgery (OR, 0.45; 95% CI, 0.29-0.68; P < .001).
An analysis that was limited to studies that reported hospital length of stay showed a clinically relevant but nonsignificant 3-day reduction among patients in the HIIT groups.
Most quality of life assessments did not show post-HIIT improvements; some showed a significant benefit 6 weeks after surgery.
IN PRACTICE:
The results suggest preoperative HIIT may improve postoperative outcomes. By extension, it could be cost-effective and “should be included in prehabilitation programs,” the report states.
SOURCE:
The study was carried out by Kari Clifford, PhD, Otago Medical School, University of Otago, Dunedin, New Zealand, and colleagues. It was published online June 30, 2023, in JAMA Network Open.
LIMITATIONS:
Included studies were heterogeneous in methodology; for example, HIIT definitions and protocols varied across almost every study. Data reporting was incomplete, the samples sizes in the studies were limited, and patients could not be blinded to their intervention. The patients could not be stratified on the basis of frailty. There were limited HIIT data from patients who underwent orthopedic surgeries.
DISCLOSURES:
The study received funding from the University of Otago. The authors reported no conflicts.
A version of this article first appeared on Medscape.com.
TOPLINE:
It cuts the risk of postoperative complications and may shorten hospital length of stay and improve postoperative quality of life.
METHODOLOGY:
Evidence suggests CRF – which improves physical and cognitive function and is associated with a reduction in cardiovascular risk – can be enhanced before major surgeries, but reported postoperative outcomes in previous reviews have been inconsistent.
In the study, HIIT involved repeated aerobic high-intensity exercise intervals at about 80% of maximum heart rate, followed by active recovery.
The meta-analysis included 12 studies with 832 patients (mean age, 67) that compared preoperative HIIT – supervised at hospitals, gyms, or community or physical therapy centers, or unsupervised at home – with standard care for patients slated for major surgery, including liver, lung, colorectal, urologic, and mixed major abdominal operations.
The primary outcome was change in CRF by peak VO2 or 6-minute walk test; other endpoints included change in endurance time and postoperative outcomes.
TAKEAWAY:
Preoperative HIIT (median total, 160 minutes; range, 80-240 minutes; intense exercise during 6-40 sessions) was associated with an increase in peak oxygen consumption (VO2 peak) by 2.59 mL/kg/min (95% confidence interval, 1.52-3.65 mL/kg/min; P < .001), compared with standard care, which represents about a 10% increase in CRF.
In eight studies that involved 770 patients, there was moderate evidence that preoperative HIIT cut the odds ratio for postoperative complications by more than half (OR, 0.44; 95% CI, 0.32-0.60; P < .001); there was a similar apparent benefit in an analysis that was limited to patients who were slated for abdominal surgery (OR, 0.45; 95% CI, 0.29-0.68; P < .001).
An analysis that was limited to studies that reported hospital length of stay showed a clinically relevant but nonsignificant 3-day reduction among patients in the HIIT groups.
Most quality of life assessments did not show post-HIIT improvements; some showed a significant benefit 6 weeks after surgery.
IN PRACTICE:
The results suggest preoperative HIIT may improve postoperative outcomes. By extension, it could be cost-effective and “should be included in prehabilitation programs,” the report states.
SOURCE:
The study was carried out by Kari Clifford, PhD, Otago Medical School, University of Otago, Dunedin, New Zealand, and colleagues. It was published online June 30, 2023, in JAMA Network Open.
LIMITATIONS:
Included studies were heterogeneous in methodology; for example, HIIT definitions and protocols varied across almost every study. Data reporting was incomplete, the samples sizes in the studies were limited, and patients could not be blinded to their intervention. The patients could not be stratified on the basis of frailty. There were limited HIIT data from patients who underwent orthopedic surgeries.
DISCLOSURES:
The study received funding from the University of Otago. The authors reported no conflicts.
A version of this article first appeared on Medscape.com.
TOPLINE:
It cuts the risk of postoperative complications and may shorten hospital length of stay and improve postoperative quality of life.
METHODOLOGY:
Evidence suggests CRF – which improves physical and cognitive function and is associated with a reduction in cardiovascular risk – can be enhanced before major surgeries, but reported postoperative outcomes in previous reviews have been inconsistent.
In the study, HIIT involved repeated aerobic high-intensity exercise intervals at about 80% of maximum heart rate, followed by active recovery.
The meta-analysis included 12 studies with 832 patients (mean age, 67) that compared preoperative HIIT – supervised at hospitals, gyms, or community or physical therapy centers, or unsupervised at home – with standard care for patients slated for major surgery, including liver, lung, colorectal, urologic, and mixed major abdominal operations.
The primary outcome was change in CRF by peak VO2 or 6-minute walk test; other endpoints included change in endurance time and postoperative outcomes.
TAKEAWAY:
Preoperative HIIT (median total, 160 minutes; range, 80-240 minutes; intense exercise during 6-40 sessions) was associated with an increase in peak oxygen consumption (VO2 peak) by 2.59 mL/kg/min (95% confidence interval, 1.52-3.65 mL/kg/min; P < .001), compared with standard care, which represents about a 10% increase in CRF.
In eight studies that involved 770 patients, there was moderate evidence that preoperative HIIT cut the odds ratio for postoperative complications by more than half (OR, 0.44; 95% CI, 0.32-0.60; P < .001); there was a similar apparent benefit in an analysis that was limited to patients who were slated for abdominal surgery (OR, 0.45; 95% CI, 0.29-0.68; P < .001).
An analysis that was limited to studies that reported hospital length of stay showed a clinically relevant but nonsignificant 3-day reduction among patients in the HIIT groups.
Most quality of life assessments did not show post-HIIT improvements; some showed a significant benefit 6 weeks after surgery.
IN PRACTICE:
The results suggest preoperative HIIT may improve postoperative outcomes. By extension, it could be cost-effective and “should be included in prehabilitation programs,” the report states.
SOURCE:
The study was carried out by Kari Clifford, PhD, Otago Medical School, University of Otago, Dunedin, New Zealand, and colleagues. It was published online June 30, 2023, in JAMA Network Open.
LIMITATIONS:
Included studies were heterogeneous in methodology; for example, HIIT definitions and protocols varied across almost every study. Data reporting was incomplete, the samples sizes in the studies were limited, and patients could not be blinded to their intervention. The patients could not be stratified on the basis of frailty. There were limited HIIT data from patients who underwent orthopedic surgeries.
DISCLOSURES:
The study received funding from the University of Otago. The authors reported no conflicts.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Mortality post perioperative CPR climbs with patient frailty
And the frailer that patients were going into surgery, according to their scores on an established frailty index, the greater their adjusted mortality risk at 30 days and the likelier they were to be discharged to a location other than their home.
The findings are based on more than 3,000 patients in an American College of Surgeons (ACS) quality improvement registry who underwent CPR at noncardiac surgery, about one-fourth of whom scored a least 40 on the revised Risk Analysis Index (RAI). The frailty index accounts for the patient’s comorbidities, cognition, functional and nutritional status, and other factors as predictors of postoperative mortality risk.
Such CPR for perioperative cardiac arrest “should not be considered futile just because a patient is frail, but neither should cardiac arrest be considered as ‘reversible’ in this population, as previously thought,” lead author Matthew B. Allen, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
“We know that patients who are frail have higher risk of complications and mortality after surgery, and recent studies have demonstrated that frailty is associated with very poor outcomes following CPR in nonsurgical settings,” said Dr. Allen, an attending physician in the department of anesthesiology, perioperative, and pain medicine at his center.
Although cardiac arrest is typically regarded as being “more reversible” in the setting of surgery and anesthesia than elsewhere in the hospital, he observed, there’s very little data on whether that is indeed the case for frail patients.
The current analysis provides “a heretofore absent base of evidence to guide decision-making regarding CPR in patients with frailty who undergo surgery,” states the report, published in JAMA Network Open.
The 3,058 patients in the analysis, from the ACS National Surgical Quality Improvement database, received CPR for cardiac arrest during or soon after noncardiac surgery. Their mean age was 71 and 44% were women.
Their RAI scores ranged from 14 to 71 and averaged 37.7; one-fourth of the patients had scores of 40 or higher, the study’s threshold for identifying patients as “frail.”
Overall in the cohort, more cardiac arrests occurred during surgeries that entailed low-to-moderate physiologic stress (an Operative Stress Score of 1 to 3) than in the setting of emergency surgery: 67.9% vs. 39.1%, respectively.
During emergency surgeries, a greater proportion of frail than nonfrail patients experienced cardiac arrest, 42% and 38%, respectively. The same relationship was observed during low-to-moderate stress surgeries: 76.6% of frail patients and 64.8% of nonfrail patients. General anesthesia was used in about 93% of procedures for both frail and nonfrail patients, the report states.
The primary endpoint, 30-day mortality, was 58.6% overall, 67.4% in frail patients, and 55.6% for nonfrail patients. Frailty and mortality were positively associated, with an adjusted odds ratio (AOR) of 1.35 (95% confidence interval [CI], 1.11-1.65, P = .003) in multivariate analysis.
Of the cohort’s 1,164 patients who had been admitted from home and survived to discharge, 38.6% were discharged to a destination other than home; the corresponding rates for frail and nonfrail patients were 59.3% and 33.9%, respectively. Frailty and nonhome discharge were positively correlated with an AOR of 1.85 (95% CI, 1.31-2.62, P < .001).
“There is no such thing as a low-risk procedure in patients who are frail,” Dr. Allen said in an interview. “Frail patients should be medically optimized prior to undergoing surgery and anesthesia, and plans should be tailored to patients’ vulnerabilities to reduce the risk of complications and facilitate rapid recognition and treatment when they occur.”
Moreover, he said, management of clinical decompensation in the perioperative period should be a part of the shared decision-making process “to establish a plan aligned with the patients’ priorities whenever possible.”
The current study quantifies risk associated with frailty in the surgical setting, and “this quantification can help providers, patients, and insurers better grasp the growing frailty problem,” Balachundhar Subramaniam, MD, MPH, of Harvard Medical School, Boston, said in an interview.
Universal screening for frailty is “a must in all surgical patients” to help identify those who are high-risk and reduce their chances for perioperative adverse events, said Dr. Subramaniam, who was not involved in the study.
“Prehabilitation with education, nutrition, physical fitness, and psychological support offer the best chance of significantly reducing poor outcomes” in frail patients, he said, along with “continuous education” in the care of frail patients.
University of Colorado surgeon Joseph Cleveland, MD, not part of the current study, said that it “provides a framework for counseling patients” regarding their do-not-resuscitate status.
“We can counsel patients with frailty with this information,” he said, “that if their heart should stop or go into in irregular rhythm, their chances of surviving are not greater than 50% and they have a more than 50% chance of not being discharged home.”
Dr. Allen reported receiving a clinical translational starter grant from Brigham and Women’s Hospital Department of Anesthesiology; disclosures for the other authors are in the original article. Dr. Subramaniam disclosed research funding from Masimo and Merck and serving as an education consultant for Masimo. Dr. Cleveland reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
And the frailer that patients were going into surgery, according to their scores on an established frailty index, the greater their adjusted mortality risk at 30 days and the likelier they were to be discharged to a location other than their home.
The findings are based on more than 3,000 patients in an American College of Surgeons (ACS) quality improvement registry who underwent CPR at noncardiac surgery, about one-fourth of whom scored a least 40 on the revised Risk Analysis Index (RAI). The frailty index accounts for the patient’s comorbidities, cognition, functional and nutritional status, and other factors as predictors of postoperative mortality risk.
Such CPR for perioperative cardiac arrest “should not be considered futile just because a patient is frail, but neither should cardiac arrest be considered as ‘reversible’ in this population, as previously thought,” lead author Matthew B. Allen, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
“We know that patients who are frail have higher risk of complications and mortality after surgery, and recent studies have demonstrated that frailty is associated with very poor outcomes following CPR in nonsurgical settings,” said Dr. Allen, an attending physician in the department of anesthesiology, perioperative, and pain medicine at his center.
Although cardiac arrest is typically regarded as being “more reversible” in the setting of surgery and anesthesia than elsewhere in the hospital, he observed, there’s very little data on whether that is indeed the case for frail patients.
The current analysis provides “a heretofore absent base of evidence to guide decision-making regarding CPR in patients with frailty who undergo surgery,” states the report, published in JAMA Network Open.
The 3,058 patients in the analysis, from the ACS National Surgical Quality Improvement database, received CPR for cardiac arrest during or soon after noncardiac surgery. Their mean age was 71 and 44% were women.
Their RAI scores ranged from 14 to 71 and averaged 37.7; one-fourth of the patients had scores of 40 or higher, the study’s threshold for identifying patients as “frail.”
Overall in the cohort, more cardiac arrests occurred during surgeries that entailed low-to-moderate physiologic stress (an Operative Stress Score of 1 to 3) than in the setting of emergency surgery: 67.9% vs. 39.1%, respectively.
During emergency surgeries, a greater proportion of frail than nonfrail patients experienced cardiac arrest, 42% and 38%, respectively. The same relationship was observed during low-to-moderate stress surgeries: 76.6% of frail patients and 64.8% of nonfrail patients. General anesthesia was used in about 93% of procedures for both frail and nonfrail patients, the report states.
The primary endpoint, 30-day mortality, was 58.6% overall, 67.4% in frail patients, and 55.6% for nonfrail patients. Frailty and mortality were positively associated, with an adjusted odds ratio (AOR) of 1.35 (95% confidence interval [CI], 1.11-1.65, P = .003) in multivariate analysis.
Of the cohort’s 1,164 patients who had been admitted from home and survived to discharge, 38.6% were discharged to a destination other than home; the corresponding rates for frail and nonfrail patients were 59.3% and 33.9%, respectively. Frailty and nonhome discharge were positively correlated with an AOR of 1.85 (95% CI, 1.31-2.62, P < .001).
“There is no such thing as a low-risk procedure in patients who are frail,” Dr. Allen said in an interview. “Frail patients should be medically optimized prior to undergoing surgery and anesthesia, and plans should be tailored to patients’ vulnerabilities to reduce the risk of complications and facilitate rapid recognition and treatment when they occur.”
Moreover, he said, management of clinical decompensation in the perioperative period should be a part of the shared decision-making process “to establish a plan aligned with the patients’ priorities whenever possible.”
The current study quantifies risk associated with frailty in the surgical setting, and “this quantification can help providers, patients, and insurers better grasp the growing frailty problem,” Balachundhar Subramaniam, MD, MPH, of Harvard Medical School, Boston, said in an interview.
Universal screening for frailty is “a must in all surgical patients” to help identify those who are high-risk and reduce their chances for perioperative adverse events, said Dr. Subramaniam, who was not involved in the study.
“Prehabilitation with education, nutrition, physical fitness, and psychological support offer the best chance of significantly reducing poor outcomes” in frail patients, he said, along with “continuous education” in the care of frail patients.
University of Colorado surgeon Joseph Cleveland, MD, not part of the current study, said that it “provides a framework for counseling patients” regarding their do-not-resuscitate status.
“We can counsel patients with frailty with this information,” he said, “that if their heart should stop or go into in irregular rhythm, their chances of surviving are not greater than 50% and they have a more than 50% chance of not being discharged home.”
Dr. Allen reported receiving a clinical translational starter grant from Brigham and Women’s Hospital Department of Anesthesiology; disclosures for the other authors are in the original article. Dr. Subramaniam disclosed research funding from Masimo and Merck and serving as an education consultant for Masimo. Dr. Cleveland reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
And the frailer that patients were going into surgery, according to their scores on an established frailty index, the greater their adjusted mortality risk at 30 days and the likelier they were to be discharged to a location other than their home.
The findings are based on more than 3,000 patients in an American College of Surgeons (ACS) quality improvement registry who underwent CPR at noncardiac surgery, about one-fourth of whom scored a least 40 on the revised Risk Analysis Index (RAI). The frailty index accounts for the patient’s comorbidities, cognition, functional and nutritional status, and other factors as predictors of postoperative mortality risk.
Such CPR for perioperative cardiac arrest “should not be considered futile just because a patient is frail, but neither should cardiac arrest be considered as ‘reversible’ in this population, as previously thought,” lead author Matthew B. Allen, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
“We know that patients who are frail have higher risk of complications and mortality after surgery, and recent studies have demonstrated that frailty is associated with very poor outcomes following CPR in nonsurgical settings,” said Dr. Allen, an attending physician in the department of anesthesiology, perioperative, and pain medicine at his center.
Although cardiac arrest is typically regarded as being “more reversible” in the setting of surgery and anesthesia than elsewhere in the hospital, he observed, there’s very little data on whether that is indeed the case for frail patients.
The current analysis provides “a heretofore absent base of evidence to guide decision-making regarding CPR in patients with frailty who undergo surgery,” states the report, published in JAMA Network Open.
The 3,058 patients in the analysis, from the ACS National Surgical Quality Improvement database, received CPR for cardiac arrest during or soon after noncardiac surgery. Their mean age was 71 and 44% were women.
Their RAI scores ranged from 14 to 71 and averaged 37.7; one-fourth of the patients had scores of 40 or higher, the study’s threshold for identifying patients as “frail.”
Overall in the cohort, more cardiac arrests occurred during surgeries that entailed low-to-moderate physiologic stress (an Operative Stress Score of 1 to 3) than in the setting of emergency surgery: 67.9% vs. 39.1%, respectively.
During emergency surgeries, a greater proportion of frail than nonfrail patients experienced cardiac arrest, 42% and 38%, respectively. The same relationship was observed during low-to-moderate stress surgeries: 76.6% of frail patients and 64.8% of nonfrail patients. General anesthesia was used in about 93% of procedures for both frail and nonfrail patients, the report states.
The primary endpoint, 30-day mortality, was 58.6% overall, 67.4% in frail patients, and 55.6% for nonfrail patients. Frailty and mortality were positively associated, with an adjusted odds ratio (AOR) of 1.35 (95% confidence interval [CI], 1.11-1.65, P = .003) in multivariate analysis.
Of the cohort’s 1,164 patients who had been admitted from home and survived to discharge, 38.6% were discharged to a destination other than home; the corresponding rates for frail and nonfrail patients were 59.3% and 33.9%, respectively. Frailty and nonhome discharge were positively correlated with an AOR of 1.85 (95% CI, 1.31-2.62, P < .001).
“There is no such thing as a low-risk procedure in patients who are frail,” Dr. Allen said in an interview. “Frail patients should be medically optimized prior to undergoing surgery and anesthesia, and plans should be tailored to patients’ vulnerabilities to reduce the risk of complications and facilitate rapid recognition and treatment when they occur.”
Moreover, he said, management of clinical decompensation in the perioperative period should be a part of the shared decision-making process “to establish a plan aligned with the patients’ priorities whenever possible.”
The current study quantifies risk associated with frailty in the surgical setting, and “this quantification can help providers, patients, and insurers better grasp the growing frailty problem,” Balachundhar Subramaniam, MD, MPH, of Harvard Medical School, Boston, said in an interview.
Universal screening for frailty is “a must in all surgical patients” to help identify those who are high-risk and reduce their chances for perioperative adverse events, said Dr. Subramaniam, who was not involved in the study.
“Prehabilitation with education, nutrition, physical fitness, and psychological support offer the best chance of significantly reducing poor outcomes” in frail patients, he said, along with “continuous education” in the care of frail patients.
University of Colorado surgeon Joseph Cleveland, MD, not part of the current study, said that it “provides a framework for counseling patients” regarding their do-not-resuscitate status.
“We can counsel patients with frailty with this information,” he said, “that if their heart should stop or go into in irregular rhythm, their chances of surviving are not greater than 50% and they have a more than 50% chance of not being discharged home.”
Dr. Allen reported receiving a clinical translational starter grant from Brigham and Women’s Hospital Department of Anesthesiology; disclosures for the other authors are in the original article. Dr. Subramaniam disclosed research funding from Masimo and Merck and serving as an education consultant for Masimo. Dr. Cleveland reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Hold Ozempic before surgery to optimize patient safety?
Semaglutide and related drugs for weight loss have co-opted bariatric medicine in recent months. They have also raised serious questions for hospital-based clinicians who wonder whether the drugs may pose risks to surgery patients undergoing anesthesia.
at this point. Official guidance on best practices has not yet caught up to surging popularity of this and other glucagon-like peptide-1 (GLP-1) agonists for weight loss.
Ozempic is indicated for treating type 2 diabetes but also is prescribed off-label for weight loss. Other GLP-1 agents from Novo Nordisk, Wegovy (semaglutide) and Saxenda (liraglutide) injections, are Food and Drug Administration–approved for weight loss. These medications work by decreasing hunger and lowering how much people eat. Semaglutide also is available as a once-daily tablet for type 2 diabetes (Rybelsus).
The American Society of Anesthesiologists (ASA) has been working on guidance on the drugs. “It’s a really hot issue now. We are getting emails from our members looking for guidance,” ASA president Michael Champeau, MD, said in an interview.
But despite the interest in how the medications might affect surgery patients and interact with anesthesia, relatively little evidence exists in the literature beyond case studies. So the society is not issuing official recommendations at this point.
“We’re going to just be calling it ‘guidance’ for right now because of the paucity of the scientific literature,” said Dr. Champeau, adjunct clinical professor of anesthesiology, perioperative, and pain medicine at Stanford (Calif.) University. “It’s probably not going to have words like ‘must; it will probably have words like ‘should’ or ‘should consider.’ “
The ASA guidance could be out in written form soon, Dr. Champeau added.
Meanwhile, whether physicians should advise stopping these medications 24 hours, 48 hours, or up to 2 weeks before surgery remains unknown.
In search of some consensus, John Shields, MD, an orthopedic surgeon at Atrium Health Wake Forest Baptist Davie Medical Center in Bermuda Run, N.C., asked colleagues on #MedTwitter: “Anyone have guidelines for ozempic around time of surgery? – holding med? – how long NPO?”
Because a full stomach can interfere with anesthesia, clinicians often advise people to stop eating and drinking 12-24 hours before elective procedures (NPO). In the case of once-weekly GLP-1 injections, which can slow gastric emptying, the optimal timeframe remains an open question. The main concern is aspiration, where a patient actively vomits while under anesthesia or their stomach contents passively come back up.
Dr. Shields’ Twitter post garnered significant reaction and comments. Within 4 days, the post was retweeted 30 times and received 72 replies and comments. Dr. Shields noted the general consensus was to hold semaglutide for 1-2 weeks before a procedure. Other suggestions included recommending a liquid diet only for 24-48 hours before surgery, recommending an NPO protocol 24-36 hours in advance, or adjusting the weekly injection so the last dose is taken 5-6 days before surgery.
Anesthesiologist Cliff Gevirtz, MD, has encountered only a few surgical patients so far taking a GLP-1 for weight loss. “And thankfully no aspiration,” added Dr. Gevirtz, clinical director of office-based ambulatory anesthesia services at Somnia Anesthesia in Harrison, N.Y.
To minimize risk, some physicians will perform an ultrasound scan to assess the contents of the stomach. If surgery is elective in a patient with a full stomach, the procedure can get postponed. Another option is to proceed with the case but treat the patient as anesthesiologists approach an emergency procedure. To be safe, many will treat the case as if the patient has a full stomach.
Dr. Gevirtz said he would treat the patient as a ‘full stomach’ and perform a rapid sequence induction with cricoid pressure. He would then extubate the patient once laryngeal reflexes return.
A rapid-sequence induction involves giving the medicine that makes a patient go to sleep, giving another medicine that paralyzes them quickly, then inserting a breathing tube – all within about 30 seconds. Cricoid pressure involves pushing on the neck during intubation to try to seal off the top of the esophagus and again minimize the chances of food coming back up.
Giving metoclopramide 30 minutes before surgery is another option, Dr. Gevirtz said. Metoclopramide can hasten the emptying of stomach contents. Administration in advance is important because waiting for the drug to work can prolong time in the operating room.
Is holding semaglutide before surgery a relevant clinical question? “Yes, very much so,” said Ronnie Fass, MD, division director of gastroenterology and hepatology and the medical director of the Digestive Health Center at The MetroHealth System in Cleveland.
Dr. Fass recommended different strategies based on the semaglutide indication. Currently, clinicians at MetroHealth instruct patients to discontinue diabetic medications the day of surgery. For those who take semaglutide for diabetes, and because the medication is taken once a week, “there is growing discussion among surgeons that the medication should not be stopped prior to surgery. This is to ensure that patients’ diabetes is well controlled before and during surgery,” Dr. Fass said.
In patients taking semaglutide for weight loss only, “there is no clear answer at this point,” he said.
Dr. Fass said the question is complicated by the fact that the medication is taken once a week. “It brings up important questions about the use of the medication during surgery, which may increase the likelihood of side effects in general and for certain types of surgery. Personally, if a patient is taking [semaglutide] for weight loss only, I would consider stopping the medication before surgery.”
The ASA was able to act quickly because it already had an expert task force review how long people should fast before surgery last year – before the explosion in popularity of the GLP-1 agonists.
Although it is still a work in progress, Dr. Champeau offered “a peek” at the recommendations. “The guidance is going to look at how far in advance the drugs should be stopped, rather than looking at making people fast even longer” before surgery, he said. “There’s just no data on that latter question.”
A version of this article originally appeared on Medscape.com.
Semaglutide and related drugs for weight loss have co-opted bariatric medicine in recent months. They have also raised serious questions for hospital-based clinicians who wonder whether the drugs may pose risks to surgery patients undergoing anesthesia.
at this point. Official guidance on best practices has not yet caught up to surging popularity of this and other glucagon-like peptide-1 (GLP-1) agonists for weight loss.
Ozempic is indicated for treating type 2 diabetes but also is prescribed off-label for weight loss. Other GLP-1 agents from Novo Nordisk, Wegovy (semaglutide) and Saxenda (liraglutide) injections, are Food and Drug Administration–approved for weight loss. These medications work by decreasing hunger and lowering how much people eat. Semaglutide also is available as a once-daily tablet for type 2 diabetes (Rybelsus).
The American Society of Anesthesiologists (ASA) has been working on guidance on the drugs. “It’s a really hot issue now. We are getting emails from our members looking for guidance,” ASA president Michael Champeau, MD, said in an interview.
But despite the interest in how the medications might affect surgery patients and interact with anesthesia, relatively little evidence exists in the literature beyond case studies. So the society is not issuing official recommendations at this point.
“We’re going to just be calling it ‘guidance’ for right now because of the paucity of the scientific literature,” said Dr. Champeau, adjunct clinical professor of anesthesiology, perioperative, and pain medicine at Stanford (Calif.) University. “It’s probably not going to have words like ‘must; it will probably have words like ‘should’ or ‘should consider.’ “
The ASA guidance could be out in written form soon, Dr. Champeau added.
Meanwhile, whether physicians should advise stopping these medications 24 hours, 48 hours, or up to 2 weeks before surgery remains unknown.
In search of some consensus, John Shields, MD, an orthopedic surgeon at Atrium Health Wake Forest Baptist Davie Medical Center in Bermuda Run, N.C., asked colleagues on #MedTwitter: “Anyone have guidelines for ozempic around time of surgery? – holding med? – how long NPO?”
Because a full stomach can interfere with anesthesia, clinicians often advise people to stop eating and drinking 12-24 hours before elective procedures (NPO). In the case of once-weekly GLP-1 injections, which can slow gastric emptying, the optimal timeframe remains an open question. The main concern is aspiration, where a patient actively vomits while under anesthesia or their stomach contents passively come back up.
Dr. Shields’ Twitter post garnered significant reaction and comments. Within 4 days, the post was retweeted 30 times and received 72 replies and comments. Dr. Shields noted the general consensus was to hold semaglutide for 1-2 weeks before a procedure. Other suggestions included recommending a liquid diet only for 24-48 hours before surgery, recommending an NPO protocol 24-36 hours in advance, or adjusting the weekly injection so the last dose is taken 5-6 days before surgery.
Anesthesiologist Cliff Gevirtz, MD, has encountered only a few surgical patients so far taking a GLP-1 for weight loss. “And thankfully no aspiration,” added Dr. Gevirtz, clinical director of office-based ambulatory anesthesia services at Somnia Anesthesia in Harrison, N.Y.
To minimize risk, some physicians will perform an ultrasound scan to assess the contents of the stomach. If surgery is elective in a patient with a full stomach, the procedure can get postponed. Another option is to proceed with the case but treat the patient as anesthesiologists approach an emergency procedure. To be safe, many will treat the case as if the patient has a full stomach.
Dr. Gevirtz said he would treat the patient as a ‘full stomach’ and perform a rapid sequence induction with cricoid pressure. He would then extubate the patient once laryngeal reflexes return.
A rapid-sequence induction involves giving the medicine that makes a patient go to sleep, giving another medicine that paralyzes them quickly, then inserting a breathing tube – all within about 30 seconds. Cricoid pressure involves pushing on the neck during intubation to try to seal off the top of the esophagus and again minimize the chances of food coming back up.
Giving metoclopramide 30 minutes before surgery is another option, Dr. Gevirtz said. Metoclopramide can hasten the emptying of stomach contents. Administration in advance is important because waiting for the drug to work can prolong time in the operating room.
Is holding semaglutide before surgery a relevant clinical question? “Yes, very much so,” said Ronnie Fass, MD, division director of gastroenterology and hepatology and the medical director of the Digestive Health Center at The MetroHealth System in Cleveland.
Dr. Fass recommended different strategies based on the semaglutide indication. Currently, clinicians at MetroHealth instruct patients to discontinue diabetic medications the day of surgery. For those who take semaglutide for diabetes, and because the medication is taken once a week, “there is growing discussion among surgeons that the medication should not be stopped prior to surgery. This is to ensure that patients’ diabetes is well controlled before and during surgery,” Dr. Fass said.
In patients taking semaglutide for weight loss only, “there is no clear answer at this point,” he said.
Dr. Fass said the question is complicated by the fact that the medication is taken once a week. “It brings up important questions about the use of the medication during surgery, which may increase the likelihood of side effects in general and for certain types of surgery. Personally, if a patient is taking [semaglutide] for weight loss only, I would consider stopping the medication before surgery.”
The ASA was able to act quickly because it already had an expert task force review how long people should fast before surgery last year – before the explosion in popularity of the GLP-1 agonists.
Although it is still a work in progress, Dr. Champeau offered “a peek” at the recommendations. “The guidance is going to look at how far in advance the drugs should be stopped, rather than looking at making people fast even longer” before surgery, he said. “There’s just no data on that latter question.”
A version of this article originally appeared on Medscape.com.
Semaglutide and related drugs for weight loss have co-opted bariatric medicine in recent months. They have also raised serious questions for hospital-based clinicians who wonder whether the drugs may pose risks to surgery patients undergoing anesthesia.
at this point. Official guidance on best practices has not yet caught up to surging popularity of this and other glucagon-like peptide-1 (GLP-1) agonists for weight loss.
Ozempic is indicated for treating type 2 diabetes but also is prescribed off-label for weight loss. Other GLP-1 agents from Novo Nordisk, Wegovy (semaglutide) and Saxenda (liraglutide) injections, are Food and Drug Administration–approved for weight loss. These medications work by decreasing hunger and lowering how much people eat. Semaglutide also is available as a once-daily tablet for type 2 diabetes (Rybelsus).
The American Society of Anesthesiologists (ASA) has been working on guidance on the drugs. “It’s a really hot issue now. We are getting emails from our members looking for guidance,” ASA president Michael Champeau, MD, said in an interview.
But despite the interest in how the medications might affect surgery patients and interact with anesthesia, relatively little evidence exists in the literature beyond case studies. So the society is not issuing official recommendations at this point.
“We’re going to just be calling it ‘guidance’ for right now because of the paucity of the scientific literature,” said Dr. Champeau, adjunct clinical professor of anesthesiology, perioperative, and pain medicine at Stanford (Calif.) University. “It’s probably not going to have words like ‘must; it will probably have words like ‘should’ or ‘should consider.’ “
The ASA guidance could be out in written form soon, Dr. Champeau added.
Meanwhile, whether physicians should advise stopping these medications 24 hours, 48 hours, or up to 2 weeks before surgery remains unknown.
In search of some consensus, John Shields, MD, an orthopedic surgeon at Atrium Health Wake Forest Baptist Davie Medical Center in Bermuda Run, N.C., asked colleagues on #MedTwitter: “Anyone have guidelines for ozempic around time of surgery? – holding med? – how long NPO?”
Because a full stomach can interfere with anesthesia, clinicians often advise people to stop eating and drinking 12-24 hours before elective procedures (NPO). In the case of once-weekly GLP-1 injections, which can slow gastric emptying, the optimal timeframe remains an open question. The main concern is aspiration, where a patient actively vomits while under anesthesia or their stomach contents passively come back up.
Dr. Shields’ Twitter post garnered significant reaction and comments. Within 4 days, the post was retweeted 30 times and received 72 replies and comments. Dr. Shields noted the general consensus was to hold semaglutide for 1-2 weeks before a procedure. Other suggestions included recommending a liquid diet only for 24-48 hours before surgery, recommending an NPO protocol 24-36 hours in advance, or adjusting the weekly injection so the last dose is taken 5-6 days before surgery.
Anesthesiologist Cliff Gevirtz, MD, has encountered only a few surgical patients so far taking a GLP-1 for weight loss. “And thankfully no aspiration,” added Dr. Gevirtz, clinical director of office-based ambulatory anesthesia services at Somnia Anesthesia in Harrison, N.Y.
To minimize risk, some physicians will perform an ultrasound scan to assess the contents of the stomach. If surgery is elective in a patient with a full stomach, the procedure can get postponed. Another option is to proceed with the case but treat the patient as anesthesiologists approach an emergency procedure. To be safe, many will treat the case as if the patient has a full stomach.
Dr. Gevirtz said he would treat the patient as a ‘full stomach’ and perform a rapid sequence induction with cricoid pressure. He would then extubate the patient once laryngeal reflexes return.
A rapid-sequence induction involves giving the medicine that makes a patient go to sleep, giving another medicine that paralyzes them quickly, then inserting a breathing tube – all within about 30 seconds. Cricoid pressure involves pushing on the neck during intubation to try to seal off the top of the esophagus and again minimize the chances of food coming back up.
Giving metoclopramide 30 minutes before surgery is another option, Dr. Gevirtz said. Metoclopramide can hasten the emptying of stomach contents. Administration in advance is important because waiting for the drug to work can prolong time in the operating room.
Is holding semaglutide before surgery a relevant clinical question? “Yes, very much so,” said Ronnie Fass, MD, division director of gastroenterology and hepatology and the medical director of the Digestive Health Center at The MetroHealth System in Cleveland.
Dr. Fass recommended different strategies based on the semaglutide indication. Currently, clinicians at MetroHealth instruct patients to discontinue diabetic medications the day of surgery. For those who take semaglutide for diabetes, and because the medication is taken once a week, “there is growing discussion among surgeons that the medication should not be stopped prior to surgery. This is to ensure that patients’ diabetes is well controlled before and during surgery,” Dr. Fass said.
In patients taking semaglutide for weight loss only, “there is no clear answer at this point,” he said.
Dr. Fass said the question is complicated by the fact that the medication is taken once a week. “It brings up important questions about the use of the medication during surgery, which may increase the likelihood of side effects in general and for certain types of surgery. Personally, if a patient is taking [semaglutide] for weight loss only, I would consider stopping the medication before surgery.”
The ASA was able to act quickly because it already had an expert task force review how long people should fast before surgery last year – before the explosion in popularity of the GLP-1 agonists.
Although it is still a work in progress, Dr. Champeau offered “a peek” at the recommendations. “The guidance is going to look at how far in advance the drugs should be stopped, rather than looking at making people fast even longer” before surgery, he said. “There’s just no data on that latter question.”
A version of this article originally appeared on Medscape.com.
A doctor must go to extremes to save a choking victim
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.
Some time ago I was invited to join a bipartisan congressional task force on valley fever, also known as coccidioidomycosis. A large and diverse crowd attended the task force’s first meeting in Bakersfield, Calif. – a meeting for everyone: the medical profession, the public, it even included veterinarians.
The whole thing was a resounding success. Francis Collins was there, the just-retired director of the NIH. Tom Frieden, then-director of the Centers for Disease Control and Prevention was there, as were several congresspeople and also my college roommate, a retired Navy medical corps captain. I was enjoying it.
Afterward, we had a banquet dinner at a restaurant in downtown Bakersfield. One of the people there was a woman I knew well – her husband was a physician friend. The restaurant served steak and salmon, and this woman made the mistake of ordering the steak.
Not long after the entrees were served, I heard a commotion at the table just behind me. I turned around and saw that woman in distress. A piece of steak had wedged in her trachea and she couldn’t breathe.
Almost immediately, the chef showed up. I don’t know how he got there. The chef at this restaurant was a big guy. I mean, probably 6 feet, 5 inches tall and 275 pounds. He tried the Heimlich maneuver. It didn’t work.
At that point, I jumped up. I thought, “Well, maybe I know how to do this better than him.” Probably not, actually. I tried and couldn’t make it work either. So I knew we were going to have to do something.
Paul Krogstad, my friend and research partner who is a pediatric infectious disease physician, stepped up and tried to put his finger in her throat and dig it out. He couldn’t get it. The patient had lost consciousness.
So, I’m thinking, okay, there’s really only one choice. You have to get an airway surgically.
I said, “We have to put her down on the floor.” And then I said, “Knife!”
I was looking at the steak knives on the table and they weren’t to my liking for doing a procedure. My college roommate – the retired Navy man – whipped out this very good pocketknife.
I had never done this in my life.
While I was making the incision, somebody gave Paul a ballpoint pen and he broke it into pieces to make a tracheostomy tube. Once I’d made the little incision, I put the tube in. She wasn’t breathing, but she still had a pulse.
I leaned forward and blew into the tube and inflated her lungs. I could see her lungs balloon up. It was a nice feeling, because I knew I was clearly in the right place.
I can’t quite explain it, but while I was doing this, I was enormously calm and totally focused. I knew there was a crowd of people around me, all looking at me, but I wasn’t conscious of that.
It was really just the four of us: Paul and Tom and me and our patient. Those were the only people that I was really cognizant of. Paul and Tom were not panic stricken at all. I remember somebody shouting, “We have to start CPR!” and Frieden said, “No. We don’t.”
Moments later, she woke up, sat up, coughed, and shot the piece of steak across the room.
She was breathing on her own, but we still taped that tube into place. Somebody had already summoned an ambulance; they were there not very long after we completed this procedure. I got in the ambulance with her and we rode over to the emergency room at Mercy Truxtun.
She was stable and doing okay. I sat with her until a thoracic surgeon showed up. He checked out the situation and decided we didn’t need that tube and took it out. I didn’t want to take that out until I had a surgeon there who could do a formal tracheostomy.
They kept her in the hospital for 3 or 4 days. Now, this woman had always had difficulties swallowing, so steak may not have been the best choice. She still had trouble swallowing afterward but recovered.
I’ve known her and her husband a long time, so it was certainly rewarding to be able to provide this service. Years later, though, when her husband died, I spoke at his funeral. When she was speaking to the gathering, she said, “And oh, by the way, Royce, thanks for saving my life.”
That surprised me. I didn’t think we were going to go there.
I’d never tried to practice medicine “at the roadside” before. But that’s part of the career.
Royce Johnson, MD, is the chief of the division of infectious disease among other leadership positions at Kern Medical in Bakersfield, Calif., and the medical director of the Valley Fever Institute.
A version of this article first appeared on Medscape.com.
Appendicitis more often missed in patients who are Black
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
FROM JAMA SURGERY
Key factors predict gallbladder cancer on routine cholecystectomy
The study covered in this summary was published on researchsquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
Why this matters
- More than 60% of gallbladder cancers are diagnosed incidentally following cholecystectomy for benign reasons.
- Identifying predictors allows surgeons to send high-risk individuals for oncologic evaluation beforehand and to prepare for intraoperative frozen pathology and more appropriate surgery, including extended cholecystectomy and lymph node dissection.
Study design
- The investigators analyzed 403,443 cholecystectomies in the American College of Surgeons’ NSQIP database from 2007 to 2017.
- They used multivariable logistic regression to identify risk factors for gallbladder cancers.
- Patients undergoing cholecystectomy for suspected or confirmed gallbladder cancer were excluded.
Key results
- The incidence of gallbladder cancer was 0.11% (441 of 403,443 patients).
- Preoperative factors significantly associated with gallbladder cancer included age older than 60 years (odds ratio [OR], 6.51), female sex (OR, 1.75), weight loss (OR, 2.58), and elevated alkaline phosphatase level (OR, 1.67).
- Starting with or converting to an open approach – both potential indicators of more complex disease – were associated with seven times’ higher odds of gallbladder cancer (OR, 7.33; P < .001), as were longer operative times (127 minutes vs. 70.7 minutes; P < .001).
Limitations
- There is a risk of selection bias regarding which patients were included in the database.
- Presenting symptoms, preoperative imaging findings, and pathologic staging were not available.
- The database did not record the reasons for choosing open surgery rather than laparoscopic surgery or for converting to an open approach.
Disclosures
- There was no funding for the work, and the investigators did not disclose any relevant financial relationships.
This is a summary of a preprint research study, “Gallbladder Cancer Incidentally Found at Cholecystectomy: Perioperative Risk Factors,” led by Elizabeth Olecki of Penn State University, State College. The study has not been peer reviewed. The full text can be found at researchsquare.com. A version of this article first appeared on Medscape.com.
The study covered in this summary was published on researchsquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
Why this matters
- More than 60% of gallbladder cancers are diagnosed incidentally following cholecystectomy for benign reasons.
- Identifying predictors allows surgeons to send high-risk individuals for oncologic evaluation beforehand and to prepare for intraoperative frozen pathology and more appropriate surgery, including extended cholecystectomy and lymph node dissection.
Study design
- The investigators analyzed 403,443 cholecystectomies in the American College of Surgeons’ NSQIP database from 2007 to 2017.
- They used multivariable logistic regression to identify risk factors for gallbladder cancers.
- Patients undergoing cholecystectomy for suspected or confirmed gallbladder cancer were excluded.
Key results
- The incidence of gallbladder cancer was 0.11% (441 of 403,443 patients).
- Preoperative factors significantly associated with gallbladder cancer included age older than 60 years (odds ratio [OR], 6.51), female sex (OR, 1.75), weight loss (OR, 2.58), and elevated alkaline phosphatase level (OR, 1.67).
- Starting with or converting to an open approach – both potential indicators of more complex disease – were associated with seven times’ higher odds of gallbladder cancer (OR, 7.33; P < .001), as were longer operative times (127 minutes vs. 70.7 minutes; P < .001).
Limitations
- There is a risk of selection bias regarding which patients were included in the database.
- Presenting symptoms, preoperative imaging findings, and pathologic staging were not available.
- The database did not record the reasons for choosing open surgery rather than laparoscopic surgery or for converting to an open approach.
Disclosures
- There was no funding for the work, and the investigators did not disclose any relevant financial relationships.
This is a summary of a preprint research study, “Gallbladder Cancer Incidentally Found at Cholecystectomy: Perioperative Risk Factors,” led by Elizabeth Olecki of Penn State University, State College. The study has not been peer reviewed. The full text can be found at researchsquare.com. A version of this article first appeared on Medscape.com.
The study covered in this summary was published on researchsquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
Why this matters
- More than 60% of gallbladder cancers are diagnosed incidentally following cholecystectomy for benign reasons.
- Identifying predictors allows surgeons to send high-risk individuals for oncologic evaluation beforehand and to prepare for intraoperative frozen pathology and more appropriate surgery, including extended cholecystectomy and lymph node dissection.
Study design
- The investigators analyzed 403,443 cholecystectomies in the American College of Surgeons’ NSQIP database from 2007 to 2017.
- They used multivariable logistic regression to identify risk factors for gallbladder cancers.
- Patients undergoing cholecystectomy for suspected or confirmed gallbladder cancer were excluded.
Key results
- The incidence of gallbladder cancer was 0.11% (441 of 403,443 patients).
- Preoperative factors significantly associated with gallbladder cancer included age older than 60 years (odds ratio [OR], 6.51), female sex (OR, 1.75), weight loss (OR, 2.58), and elevated alkaline phosphatase level (OR, 1.67).
- Starting with or converting to an open approach – both potential indicators of more complex disease – were associated with seven times’ higher odds of gallbladder cancer (OR, 7.33; P < .001), as were longer operative times (127 minutes vs. 70.7 minutes; P < .001).
Limitations
- There is a risk of selection bias regarding which patients were included in the database.
- Presenting symptoms, preoperative imaging findings, and pathologic staging were not available.
- The database did not record the reasons for choosing open surgery rather than laparoscopic surgery or for converting to an open approach.
Disclosures
- There was no funding for the work, and the investigators did not disclose any relevant financial relationships.
This is a summary of a preprint research study, “Gallbladder Cancer Incidentally Found at Cholecystectomy: Perioperative Risk Factors,” led by Elizabeth Olecki of Penn State University, State College. The study has not been peer reviewed. The full text can be found at researchsquare.com. A version of this article first appeared on Medscape.com.
A patient named ‘Settle’ decides to sue instead
On Nov. 1, 2020, Dallas Settle went to Plateau Medical Center, Oak Hill, W.Va., complaining of pain that was later described in court documents as being “in his right mid-abdomen migrating to his right lower abdomen.” Following a CT scan, Mr. Settle was diagnosed with diverticulitis resulting in pneumoperitoneum, which is the presence of air or other gas in the abdominal cavity. The patient, it was decided, required surgery to correct the problem, but Plateau Medical Center didn’t have the staff to perform the procedure.
Mr. Settle was then transferred to another West Virginia hospital, Charleston Area Medical Center (CAMC). Here, he was evaluated by doctors in the facility’s General Division, who initiated treatment with IV fluids and opiate analgesics. He was then placed under the care of a trauma surgeon, who initially decided to treat the patient nonoperatively. If that approach failed, the surgeon believed, Mr. Settle would probably require a laparotomy, bowel resection, and ostomy.
Another surgical team performed an exploratory laparotomy the following day. The team determined that Mr. Settle was suffering from a ruptured appendicitis and allegedly performed an appendectomy. But Mr. Settle’s condition continued to deteriorate the following day.
Another CT scan followed. It revealed various problems – multiple fluid collections, an ileus, distended loops of the patient’s small bowel, a left renal cyst, subcentimeter mesenteric, and retroperitoneal adenopathy. Additional CT scans conducted 4 days later indicated other problems, including fluid collections in the patient’s right- and left-lower quadrants.
Over the next few days, doctors performed further exploratory laparotomies. Finally, on Nov. 22, Mr. Settle was transferred out of the intensive care unit in preparation for his discharge the following day.
His pain continued to worsen, however, and he was readmitted to CAMC a day later. At this point, an examination revealed that his surgical incisions had become infected.
Worse news was on the horizon. On Nov. 28, the trauma surgeon who had first agreed to treat Mr. Settle informed him that, despite claims to the contrary, his appendix hadn’t been removed.
Eventually, Mr. Settle was referred to the Cleveland Clinic, where at press time he was still being treated.
Mr. Settle has hired the firm Calwell Luce diTrapano to sue CAMC, accusing it of medical malpractice, medical negligence, and other lapses in the standard of care. In his complaint, he accused the hospital and its staff of breaching their duty of care “by negligently and improperly treating him” and by failing “to exercise the degree of care, skill, and learning required and expected of reasonable health care providers.”
His suit seeks not only compensatory damages and other relief but also punitive damages.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article originally appeared on Medscape.com.
On Nov. 1, 2020, Dallas Settle went to Plateau Medical Center, Oak Hill, W.Va., complaining of pain that was later described in court documents as being “in his right mid-abdomen migrating to his right lower abdomen.” Following a CT scan, Mr. Settle was diagnosed with diverticulitis resulting in pneumoperitoneum, which is the presence of air or other gas in the abdominal cavity. The patient, it was decided, required surgery to correct the problem, but Plateau Medical Center didn’t have the staff to perform the procedure.
Mr. Settle was then transferred to another West Virginia hospital, Charleston Area Medical Center (CAMC). Here, he was evaluated by doctors in the facility’s General Division, who initiated treatment with IV fluids and opiate analgesics. He was then placed under the care of a trauma surgeon, who initially decided to treat the patient nonoperatively. If that approach failed, the surgeon believed, Mr. Settle would probably require a laparotomy, bowel resection, and ostomy.
Another surgical team performed an exploratory laparotomy the following day. The team determined that Mr. Settle was suffering from a ruptured appendicitis and allegedly performed an appendectomy. But Mr. Settle’s condition continued to deteriorate the following day.
Another CT scan followed. It revealed various problems – multiple fluid collections, an ileus, distended loops of the patient’s small bowel, a left renal cyst, subcentimeter mesenteric, and retroperitoneal adenopathy. Additional CT scans conducted 4 days later indicated other problems, including fluid collections in the patient’s right- and left-lower quadrants.
Over the next few days, doctors performed further exploratory laparotomies. Finally, on Nov. 22, Mr. Settle was transferred out of the intensive care unit in preparation for his discharge the following day.
His pain continued to worsen, however, and he was readmitted to CAMC a day later. At this point, an examination revealed that his surgical incisions had become infected.
Worse news was on the horizon. On Nov. 28, the trauma surgeon who had first agreed to treat Mr. Settle informed him that, despite claims to the contrary, his appendix hadn’t been removed.
Eventually, Mr. Settle was referred to the Cleveland Clinic, where at press time he was still being treated.
Mr. Settle has hired the firm Calwell Luce diTrapano to sue CAMC, accusing it of medical malpractice, medical negligence, and other lapses in the standard of care. In his complaint, he accused the hospital and its staff of breaching their duty of care “by negligently and improperly treating him” and by failing “to exercise the degree of care, skill, and learning required and expected of reasonable health care providers.”
His suit seeks not only compensatory damages and other relief but also punitive damages.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article originally appeared on Medscape.com.
On Nov. 1, 2020, Dallas Settle went to Plateau Medical Center, Oak Hill, W.Va., complaining of pain that was later described in court documents as being “in his right mid-abdomen migrating to his right lower abdomen.” Following a CT scan, Mr. Settle was diagnosed with diverticulitis resulting in pneumoperitoneum, which is the presence of air or other gas in the abdominal cavity. The patient, it was decided, required surgery to correct the problem, but Plateau Medical Center didn’t have the staff to perform the procedure.
Mr. Settle was then transferred to another West Virginia hospital, Charleston Area Medical Center (CAMC). Here, he was evaluated by doctors in the facility’s General Division, who initiated treatment with IV fluids and opiate analgesics. He was then placed under the care of a trauma surgeon, who initially decided to treat the patient nonoperatively. If that approach failed, the surgeon believed, Mr. Settle would probably require a laparotomy, bowel resection, and ostomy.
Another surgical team performed an exploratory laparotomy the following day. The team determined that Mr. Settle was suffering from a ruptured appendicitis and allegedly performed an appendectomy. But Mr. Settle’s condition continued to deteriorate the following day.
Another CT scan followed. It revealed various problems – multiple fluid collections, an ileus, distended loops of the patient’s small bowel, a left renal cyst, subcentimeter mesenteric, and retroperitoneal adenopathy. Additional CT scans conducted 4 days later indicated other problems, including fluid collections in the patient’s right- and left-lower quadrants.
Over the next few days, doctors performed further exploratory laparotomies. Finally, on Nov. 22, Mr. Settle was transferred out of the intensive care unit in preparation for his discharge the following day.
His pain continued to worsen, however, and he was readmitted to CAMC a day later. At this point, an examination revealed that his surgical incisions had become infected.
Worse news was on the horizon. On Nov. 28, the trauma surgeon who had first agreed to treat Mr. Settle informed him that, despite claims to the contrary, his appendix hadn’t been removed.
Eventually, Mr. Settle was referred to the Cleveland Clinic, where at press time he was still being treated.
Mr. Settle has hired the firm Calwell Luce diTrapano to sue CAMC, accusing it of medical malpractice, medical negligence, and other lapses in the standard of care. In his complaint, he accused the hospital and its staff of breaching their duty of care “by negligently and improperly treating him” and by failing “to exercise the degree of care, skill, and learning required and expected of reasonable health care providers.”
His suit seeks not only compensatory damages and other relief but also punitive damages.
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article originally appeared on Medscape.com.
‘Game changer’: Thyroid cancer recurrence no higher with lobectomy
Patients with intermediate-risk papillary thyroid cancer and lymph node metastasis show no significant increase in tumor recurrence when undergoing lobectomy compared with a total thyroidectomy, new research shows.
“Results of this cohort study suggest that patients with ipsilateral clinical lateral neck metastasis (cN1b) papillary thyroid cancer who underwent lobectomy exhibited recurrence-free survival rates similar to those who underwent total thyroidectomy after controlling for major prognostic factors,” the authors conclude in the study published online in JAMA Surgery.
“These findings suggest that cN1b alone should not be an absolute indication for total thyroidectomy,” they note.
The study, involving the largest cohort to date to compare patients with intermediate-risk papillary thyroid cancer treated with lobectomy versus total thyroidectomy, “challenged the current guidelines and pushed the boundary of limited surgical treatment even further,” say Michelle B. Mulder, MD, and Quan-Yang Duh, MD, of the department of surgery, University of California, San Francisco, in an accompanying editorial.
“It can be a game changer if confirmed by future prospective and multicenter studies,” they add.
Guidelines still recommend total thyroidectomy with subsequent RAI
While lower-intensity treatment options, with a lower risk of complications, have gained favor in the treatment of low-risk papillary thyroid cancer, guidelines still recommend the consideration of total thyroidectomy and subsequent radioactive iodine ablation (RAI) for intermediate-risk cancers because of the higher chance of recurrence, particularly among those with clinically positive nodes.
However, data on the superiority of a total thyroidectomy, with or without RAI, versus lobectomy is inconsistent, prompting first author Siyuan Xu, MD, of the department of head and neck surgical oncology, National Cancer Center, Beijing, and colleagues to compare the risk of recurrence with the two approaches.
For the study, patients with intermediate-risk papillary thyroid cancer treated at the Chinese Academy of Medical Sciences Cancer Hospital in Beijing between January 2000 and December 2017, who had a lobectomy or total thyroidectomy, were paired 1:1 in a propensity score matching analysis.
Other than treatment type, the 265 pairs of patients were matched based on all other potential prognostic factors, including age, sex, primary tumor size, minor extrathyroidal extension, multifocality, number of lymph node metastases, and lymph node ratio.
Participants were a mean age of 37 years and 66% were female.
With a median follow-up of 60 months in the lobectomy group and 58 months in the total thyroidectomy group, structural recurrences occurred in 7.9% (21) and 6.4% (17) of patients, respectively, which was not significantly different.
The primary endpoint, 5-year rate of recurrence-free survival, was also not significantly different between the lobectomy (92.3%) and total thyroidectomy groups (93.7%) (adjusted hazard ratio, 1.10; P = .77).
In a further stratified analysis of patients treated with total thyroidectomy along with RAI (n = 75), the lack of a significant difference in recurrence-free survival versus lobectomy remained (aHR, 0.59; P = .46).
The results were similar in unadjusted as well as adjusted analyses, and a power analysis indicated that the study had a 90% power to detect a more than 4.9% difference in recurrence-free survival.
“Given the lower complication rate of lobectomy, a maximal 4.9% recurrence-free survival difference is acceptable, which enhances the reliability of the study results,” the authors say.
They conclude that “our findings call into question whether cN1b alone [ipsilateral clinical lateral neck metastasis papillary thyroid cancer] should be an absolute determinant for deciding the optimal extent of thyroid surgery for papillary thyroid cancer.”
With total thyroidectomy, RAI can be given
An important argument in favor of total thyroidectomy is that with the complete resection of thyroid tissue, RAI ablation can then be used for postoperative detection of residual or metastatic disease, as well as for treatment, the authors note.
Indeed, a study using the Surveillance, Epidemiology, and End Results (SEER) database showed RAI ablation is associated with a 29% reduction in the risk of death in patients with intermediate-risk papillary thyroid cancer, with a hazard risk of 0.71.
However, conflicting data from Memorial Sloan-Kettering Cancer Center, New York, suggests no significant benefit with total thyroidectomy and RAI ablation.
The current study’s analysis of patients treated with RAI, though limited in size, supports the latter study’s findings, the authors note.
“When we performed further stratified analyses in patients treated with total thyroidectomy plus RAI ablation and their counterparts, no significant difference was found, which conformed with [the] result from the whole cohort.”
“Certainly, the stratified comparison did not have enough power to examine the effect of RAI ablation on tumor recurrence subject to the limitation of sample size and case selection [and] further study is needed on this topic,” they write.
Some limitations warrant cautious interpretation
In their editorial, Dr. Mulder and Dr. Duh note that while some previous studies have shown similar outcomes relating to tumor size, thyroid hormone suppression therapy, and multifocality, “few have addressed lateral neck involvement.”
They suggest cautious interpretation, however, due to limitations, acknowledged by the authors, including the single-center nature of the study.
“Appropriate propensity matching may mitigate selection bias but cannot eliminate it entirely and their findings may not be replicated in other institutions by other surgeons,” they note.
Other limitations include that changes in clinical practice and patient selection were likely over the course of the study because of significant changes in American Thyroid Association (ATA) guidelines between 2009 and 2017, and characteristics including molecular genetic testing, which could have influenced final results, were not taken into consideration.
Furthermore, for patients with intermediate-risk cancer, modifications in postoperative follow-up are necessary following lobectomy versus total thyroidectomy; “the role of radioiodine is limited and the levels of thyroglobulin more complicated to interpret,” they note.
The study and editorial authors had no disclosures to report.
A version of this article first appeared on Medscape.com.
Patients with intermediate-risk papillary thyroid cancer and lymph node metastasis show no significant increase in tumor recurrence when undergoing lobectomy compared with a total thyroidectomy, new research shows.
“Results of this cohort study suggest that patients with ipsilateral clinical lateral neck metastasis (cN1b) papillary thyroid cancer who underwent lobectomy exhibited recurrence-free survival rates similar to those who underwent total thyroidectomy after controlling for major prognostic factors,” the authors conclude in the study published online in JAMA Surgery.
“These findings suggest that cN1b alone should not be an absolute indication for total thyroidectomy,” they note.
The study, involving the largest cohort to date to compare patients with intermediate-risk papillary thyroid cancer treated with lobectomy versus total thyroidectomy, “challenged the current guidelines and pushed the boundary of limited surgical treatment even further,” say Michelle B. Mulder, MD, and Quan-Yang Duh, MD, of the department of surgery, University of California, San Francisco, in an accompanying editorial.
“It can be a game changer if confirmed by future prospective and multicenter studies,” they add.
Guidelines still recommend total thyroidectomy with subsequent RAI
While lower-intensity treatment options, with a lower risk of complications, have gained favor in the treatment of low-risk papillary thyroid cancer, guidelines still recommend the consideration of total thyroidectomy and subsequent radioactive iodine ablation (RAI) for intermediate-risk cancers because of the higher chance of recurrence, particularly among those with clinically positive nodes.
However, data on the superiority of a total thyroidectomy, with or without RAI, versus lobectomy is inconsistent, prompting first author Siyuan Xu, MD, of the department of head and neck surgical oncology, National Cancer Center, Beijing, and colleagues to compare the risk of recurrence with the two approaches.
For the study, patients with intermediate-risk papillary thyroid cancer treated at the Chinese Academy of Medical Sciences Cancer Hospital in Beijing between January 2000 and December 2017, who had a lobectomy or total thyroidectomy, were paired 1:1 in a propensity score matching analysis.
Other than treatment type, the 265 pairs of patients were matched based on all other potential prognostic factors, including age, sex, primary tumor size, minor extrathyroidal extension, multifocality, number of lymph node metastases, and lymph node ratio.
Participants were a mean age of 37 years and 66% were female.
With a median follow-up of 60 months in the lobectomy group and 58 months in the total thyroidectomy group, structural recurrences occurred in 7.9% (21) and 6.4% (17) of patients, respectively, which was not significantly different.
The primary endpoint, 5-year rate of recurrence-free survival, was also not significantly different between the lobectomy (92.3%) and total thyroidectomy groups (93.7%) (adjusted hazard ratio, 1.10; P = .77).
In a further stratified analysis of patients treated with total thyroidectomy along with RAI (n = 75), the lack of a significant difference in recurrence-free survival versus lobectomy remained (aHR, 0.59; P = .46).
The results were similar in unadjusted as well as adjusted analyses, and a power analysis indicated that the study had a 90% power to detect a more than 4.9% difference in recurrence-free survival.
“Given the lower complication rate of lobectomy, a maximal 4.9% recurrence-free survival difference is acceptable, which enhances the reliability of the study results,” the authors say.
They conclude that “our findings call into question whether cN1b alone [ipsilateral clinical lateral neck metastasis papillary thyroid cancer] should be an absolute determinant for deciding the optimal extent of thyroid surgery for papillary thyroid cancer.”
With total thyroidectomy, RAI can be given
An important argument in favor of total thyroidectomy is that with the complete resection of thyroid tissue, RAI ablation can then be used for postoperative detection of residual or metastatic disease, as well as for treatment, the authors note.
Indeed, a study using the Surveillance, Epidemiology, and End Results (SEER) database showed RAI ablation is associated with a 29% reduction in the risk of death in patients with intermediate-risk papillary thyroid cancer, with a hazard risk of 0.71.
However, conflicting data from Memorial Sloan-Kettering Cancer Center, New York, suggests no significant benefit with total thyroidectomy and RAI ablation.
The current study’s analysis of patients treated with RAI, though limited in size, supports the latter study’s findings, the authors note.
“When we performed further stratified analyses in patients treated with total thyroidectomy plus RAI ablation and their counterparts, no significant difference was found, which conformed with [the] result from the whole cohort.”
“Certainly, the stratified comparison did not have enough power to examine the effect of RAI ablation on tumor recurrence subject to the limitation of sample size and case selection [and] further study is needed on this topic,” they write.
Some limitations warrant cautious interpretation
In their editorial, Dr. Mulder and Dr. Duh note that while some previous studies have shown similar outcomes relating to tumor size, thyroid hormone suppression therapy, and multifocality, “few have addressed lateral neck involvement.”
They suggest cautious interpretation, however, due to limitations, acknowledged by the authors, including the single-center nature of the study.
“Appropriate propensity matching may mitigate selection bias but cannot eliminate it entirely and their findings may not be replicated in other institutions by other surgeons,” they note.
Other limitations include that changes in clinical practice and patient selection were likely over the course of the study because of significant changes in American Thyroid Association (ATA) guidelines between 2009 and 2017, and characteristics including molecular genetic testing, which could have influenced final results, were not taken into consideration.
Furthermore, for patients with intermediate-risk cancer, modifications in postoperative follow-up are necessary following lobectomy versus total thyroidectomy; “the role of radioiodine is limited and the levels of thyroglobulin more complicated to interpret,” they note.
The study and editorial authors had no disclosures to report.
A version of this article first appeared on Medscape.com.
Patients with intermediate-risk papillary thyroid cancer and lymph node metastasis show no significant increase in tumor recurrence when undergoing lobectomy compared with a total thyroidectomy, new research shows.
“Results of this cohort study suggest that patients with ipsilateral clinical lateral neck metastasis (cN1b) papillary thyroid cancer who underwent lobectomy exhibited recurrence-free survival rates similar to those who underwent total thyroidectomy after controlling for major prognostic factors,” the authors conclude in the study published online in JAMA Surgery.
“These findings suggest that cN1b alone should not be an absolute indication for total thyroidectomy,” they note.
The study, involving the largest cohort to date to compare patients with intermediate-risk papillary thyroid cancer treated with lobectomy versus total thyroidectomy, “challenged the current guidelines and pushed the boundary of limited surgical treatment even further,” say Michelle B. Mulder, MD, and Quan-Yang Duh, MD, of the department of surgery, University of California, San Francisco, in an accompanying editorial.
“It can be a game changer if confirmed by future prospective and multicenter studies,” they add.
Guidelines still recommend total thyroidectomy with subsequent RAI
While lower-intensity treatment options, with a lower risk of complications, have gained favor in the treatment of low-risk papillary thyroid cancer, guidelines still recommend the consideration of total thyroidectomy and subsequent radioactive iodine ablation (RAI) for intermediate-risk cancers because of the higher chance of recurrence, particularly among those with clinically positive nodes.
However, data on the superiority of a total thyroidectomy, with or without RAI, versus lobectomy is inconsistent, prompting first author Siyuan Xu, MD, of the department of head and neck surgical oncology, National Cancer Center, Beijing, and colleagues to compare the risk of recurrence with the two approaches.
For the study, patients with intermediate-risk papillary thyroid cancer treated at the Chinese Academy of Medical Sciences Cancer Hospital in Beijing between January 2000 and December 2017, who had a lobectomy or total thyroidectomy, were paired 1:1 in a propensity score matching analysis.
Other than treatment type, the 265 pairs of patients were matched based on all other potential prognostic factors, including age, sex, primary tumor size, minor extrathyroidal extension, multifocality, number of lymph node metastases, and lymph node ratio.
Participants were a mean age of 37 years and 66% were female.
With a median follow-up of 60 months in the lobectomy group and 58 months in the total thyroidectomy group, structural recurrences occurred in 7.9% (21) and 6.4% (17) of patients, respectively, which was not significantly different.
The primary endpoint, 5-year rate of recurrence-free survival, was also not significantly different between the lobectomy (92.3%) and total thyroidectomy groups (93.7%) (adjusted hazard ratio, 1.10; P = .77).
In a further stratified analysis of patients treated with total thyroidectomy along with RAI (n = 75), the lack of a significant difference in recurrence-free survival versus lobectomy remained (aHR, 0.59; P = .46).
The results were similar in unadjusted as well as adjusted analyses, and a power analysis indicated that the study had a 90% power to detect a more than 4.9% difference in recurrence-free survival.
“Given the lower complication rate of lobectomy, a maximal 4.9% recurrence-free survival difference is acceptable, which enhances the reliability of the study results,” the authors say.
They conclude that “our findings call into question whether cN1b alone [ipsilateral clinical lateral neck metastasis papillary thyroid cancer] should be an absolute determinant for deciding the optimal extent of thyroid surgery for papillary thyroid cancer.”
With total thyroidectomy, RAI can be given
An important argument in favor of total thyroidectomy is that with the complete resection of thyroid tissue, RAI ablation can then be used for postoperative detection of residual or metastatic disease, as well as for treatment, the authors note.
Indeed, a study using the Surveillance, Epidemiology, and End Results (SEER) database showed RAI ablation is associated with a 29% reduction in the risk of death in patients with intermediate-risk papillary thyroid cancer, with a hazard risk of 0.71.
However, conflicting data from Memorial Sloan-Kettering Cancer Center, New York, suggests no significant benefit with total thyroidectomy and RAI ablation.
The current study’s analysis of patients treated with RAI, though limited in size, supports the latter study’s findings, the authors note.
“When we performed further stratified analyses in patients treated with total thyroidectomy plus RAI ablation and their counterparts, no significant difference was found, which conformed with [the] result from the whole cohort.”
“Certainly, the stratified comparison did not have enough power to examine the effect of RAI ablation on tumor recurrence subject to the limitation of sample size and case selection [and] further study is needed on this topic,” they write.
Some limitations warrant cautious interpretation
In their editorial, Dr. Mulder and Dr. Duh note that while some previous studies have shown similar outcomes relating to tumor size, thyroid hormone suppression therapy, and multifocality, “few have addressed lateral neck involvement.”
They suggest cautious interpretation, however, due to limitations, acknowledged by the authors, including the single-center nature of the study.
“Appropriate propensity matching may mitigate selection bias but cannot eliminate it entirely and their findings may not be replicated in other institutions by other surgeons,” they note.
Other limitations include that changes in clinical practice and patient selection were likely over the course of the study because of significant changes in American Thyroid Association (ATA) guidelines between 2009 and 2017, and characteristics including molecular genetic testing, which could have influenced final results, were not taken into consideration.
Furthermore, for patients with intermediate-risk cancer, modifications in postoperative follow-up are necessary following lobectomy versus total thyroidectomy; “the role of radioiodine is limited and the levels of thyroglobulin more complicated to interpret,” they note.
The study and editorial authors had no disclosures to report.
A version of this article first appeared on Medscape.com.
FROM JAMA SURGERY
Surgical site dressing turns blue when it needs changing
Surgical site infections are one of the top causes of postoperative morbidity and death worldwide, but there is little agreement and much debate over the most effective wound dressing to improve outcomes and reduce the health care burden.
Recent clinical trials have indicated that transparent, semiocclusive films have advantages over gauze held by adhesive tape.
But current transparent film bandages may become dislodged during activities such as showering, say authors of a pilot study published in the Journal of Wound Care. Patients may not realize the bandage has been disrupted, which can lead to infection.
.
“Clinicians, patients, and caregivers are alerted to the loss of dressing integrity and can replace the dressing when any portion of the perimeter changes to a blue [color],” the authors explain. “In addition, the dressing turns blue when the central pad is saturated with fluid, allowing the patient or provider to change the dressing.”
DSD is indicated for wounds that have low levels of exudate.
Two transparent film dressings compared
Researchers recruited 20 patients from the general population in Pittsburgh, for a small pilot study to test DSD against a comparator film dressing (3M Tegaderm + Pad). The volunteers received “a small stipend,” according to the paper.
A 1.5-centimeter incision was made in both forearms of each volunteer. The forearms were randomized regarding which got which bandage. Both bandages have been cleared by the U.S. Food and Drug Administration as nonsignificant-risk devices.
Volunteers were instructed to wear the dressing and continue their typical activities of daily living.
The average age of the volunteers was 52 years (range, 20-80 years). Among the 20 volunteers, 11 reported no comorbidities, and 45% reported at least one comorbidity.
Most of the volunteers favored DSD over the comparator in a postoperative survey – 75% to 25%, according to the report.
The wear time between the two transparent dressings across all subjects was 1.4 days. There was no difference in wear time, logged by the volunteers, between the two groups.
There were no infectious complications, the paper states.
The maker, DrySee (Houston), which holds three patents on the product, supported the research with an unrestricted grant.
DrySee CEO Brad Greer told this news organization, “With DrySee, you know when to change your dressing. All other dressings look the same wet, saturated, or dry.”
He said the study confirms what they have seen in practice, adding that the product is unique.
“No one else in the world has this technology,” Mr. Greer said.
Surgeons want to see more data
Heather Evans, MD, a general surgeon with the Medical University of South Carolina, MUSC Health, Charleston, who was not involved with the study, praised the color-indicator design and said she liked the bandage’s narrow indication for low-exudate wounds.
She said in an interview, “It’s a lot to put on a layperson to suddenly know how to take care of wounds when you leave the hospital.”
Giving them the confidence that their wound is safe if the blue doesn’t appear “is a really cool concept,” she said.
She said that, although the volunteers included some elderly people and people with conditions such as diabetes that could affect wound healing, the bandage needs to be tested with a bigger trial to see if it is effective outside controlled conditions.
She also said that some occlusive dressings will be more durable and stay on days longer than DSD or the comparator, which may affect the choice for some.
“The average length of dressing time in this study was less than 2 days,” she pointed out.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health Bedford, who was not involved with the study, agreed that any surgical or wound dressing, including transparent films, can become dislodged, and said, “This type of product has promise but this is a small pilot study. I would want to see results from a trial of actual surgical patients to see if this type of dressing did indeed decrease post-op infections compared to standard dressing materials.”
Not all are convinced either that there is a need to be filled or that DSD will be the right solution.
Therese Duane, MD, a general surgeon with Texas Health Harris Methodist Fort Worth, who was not part of the study, said in an interview that she “has no issues with the current products.”
She added that more information is needed before considering DSD a better solution, including animal studies and use “on very sick patients.”
“Twenty volunteers with cuts on their arm is barely a start for comparison,” she said.
The authors, led by Kristy Breisinger, a research analyst with the SerenaGroup Research Foundation in Cambridge, Mass., acknowledged the limitations, including the small sample size and that the trial was conducted at only one institution. Additionally, the analysis is based on descriptive statistics.
They write that the trial design was chosen “to simulate a real-world setting that is not always achievable in animal studies.”
The research was sponsored by an unrestricted grant from the maker of DSD, DrySee Inc., in Houston.
Mr. Greer is DrySee’s CEO. The authors and Dr. Duane, Dr. Rickert, and Dr. Evans declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surgical site infections are one of the top causes of postoperative morbidity and death worldwide, but there is little agreement and much debate over the most effective wound dressing to improve outcomes and reduce the health care burden.
Recent clinical trials have indicated that transparent, semiocclusive films have advantages over gauze held by adhesive tape.
But current transparent film bandages may become dislodged during activities such as showering, say authors of a pilot study published in the Journal of Wound Care. Patients may not realize the bandage has been disrupted, which can lead to infection.
.
“Clinicians, patients, and caregivers are alerted to the loss of dressing integrity and can replace the dressing when any portion of the perimeter changes to a blue [color],” the authors explain. “In addition, the dressing turns blue when the central pad is saturated with fluid, allowing the patient or provider to change the dressing.”
DSD is indicated for wounds that have low levels of exudate.
Two transparent film dressings compared
Researchers recruited 20 patients from the general population in Pittsburgh, for a small pilot study to test DSD against a comparator film dressing (3M Tegaderm + Pad). The volunteers received “a small stipend,” according to the paper.
A 1.5-centimeter incision was made in both forearms of each volunteer. The forearms were randomized regarding which got which bandage. Both bandages have been cleared by the U.S. Food and Drug Administration as nonsignificant-risk devices.
Volunteers were instructed to wear the dressing and continue their typical activities of daily living.
The average age of the volunteers was 52 years (range, 20-80 years). Among the 20 volunteers, 11 reported no comorbidities, and 45% reported at least one comorbidity.
Most of the volunteers favored DSD over the comparator in a postoperative survey – 75% to 25%, according to the report.
The wear time between the two transparent dressings across all subjects was 1.4 days. There was no difference in wear time, logged by the volunteers, between the two groups.
There were no infectious complications, the paper states.
The maker, DrySee (Houston), which holds three patents on the product, supported the research with an unrestricted grant.
DrySee CEO Brad Greer told this news organization, “With DrySee, you know when to change your dressing. All other dressings look the same wet, saturated, or dry.”
He said the study confirms what they have seen in practice, adding that the product is unique.
“No one else in the world has this technology,” Mr. Greer said.
Surgeons want to see more data
Heather Evans, MD, a general surgeon with the Medical University of South Carolina, MUSC Health, Charleston, who was not involved with the study, praised the color-indicator design and said she liked the bandage’s narrow indication for low-exudate wounds.
She said in an interview, “It’s a lot to put on a layperson to suddenly know how to take care of wounds when you leave the hospital.”
Giving them the confidence that their wound is safe if the blue doesn’t appear “is a really cool concept,” she said.
She said that, although the volunteers included some elderly people and people with conditions such as diabetes that could affect wound healing, the bandage needs to be tested with a bigger trial to see if it is effective outside controlled conditions.
She also said that some occlusive dressings will be more durable and stay on days longer than DSD or the comparator, which may affect the choice for some.
“The average length of dressing time in this study was less than 2 days,” she pointed out.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health Bedford, who was not involved with the study, agreed that any surgical or wound dressing, including transparent films, can become dislodged, and said, “This type of product has promise but this is a small pilot study. I would want to see results from a trial of actual surgical patients to see if this type of dressing did indeed decrease post-op infections compared to standard dressing materials.”
Not all are convinced either that there is a need to be filled or that DSD will be the right solution.
Therese Duane, MD, a general surgeon with Texas Health Harris Methodist Fort Worth, who was not part of the study, said in an interview that she “has no issues with the current products.”
She added that more information is needed before considering DSD a better solution, including animal studies and use “on very sick patients.”
“Twenty volunteers with cuts on their arm is barely a start for comparison,” she said.
The authors, led by Kristy Breisinger, a research analyst with the SerenaGroup Research Foundation in Cambridge, Mass., acknowledged the limitations, including the small sample size and that the trial was conducted at only one institution. Additionally, the analysis is based on descriptive statistics.
They write that the trial design was chosen “to simulate a real-world setting that is not always achievable in animal studies.”
The research was sponsored by an unrestricted grant from the maker of DSD, DrySee Inc., in Houston.
Mr. Greer is DrySee’s CEO. The authors and Dr. Duane, Dr. Rickert, and Dr. Evans declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surgical site infections are one of the top causes of postoperative morbidity and death worldwide, but there is little agreement and much debate over the most effective wound dressing to improve outcomes and reduce the health care burden.
Recent clinical trials have indicated that transparent, semiocclusive films have advantages over gauze held by adhesive tape.
But current transparent film bandages may become dislodged during activities such as showering, say authors of a pilot study published in the Journal of Wound Care. Patients may not realize the bandage has been disrupted, which can lead to infection.
.
“Clinicians, patients, and caregivers are alerted to the loss of dressing integrity and can replace the dressing when any portion of the perimeter changes to a blue [color],” the authors explain. “In addition, the dressing turns blue when the central pad is saturated with fluid, allowing the patient or provider to change the dressing.”
DSD is indicated for wounds that have low levels of exudate.
Two transparent film dressings compared
Researchers recruited 20 patients from the general population in Pittsburgh, for a small pilot study to test DSD against a comparator film dressing (3M Tegaderm + Pad). The volunteers received “a small stipend,” according to the paper.
A 1.5-centimeter incision was made in both forearms of each volunteer. The forearms were randomized regarding which got which bandage. Both bandages have been cleared by the U.S. Food and Drug Administration as nonsignificant-risk devices.
Volunteers were instructed to wear the dressing and continue their typical activities of daily living.
The average age of the volunteers was 52 years (range, 20-80 years). Among the 20 volunteers, 11 reported no comorbidities, and 45% reported at least one comorbidity.
Most of the volunteers favored DSD over the comparator in a postoperative survey – 75% to 25%, according to the report.
The wear time between the two transparent dressings across all subjects was 1.4 days. There was no difference in wear time, logged by the volunteers, between the two groups.
There were no infectious complications, the paper states.
The maker, DrySee (Houston), which holds three patents on the product, supported the research with an unrestricted grant.
DrySee CEO Brad Greer told this news organization, “With DrySee, you know when to change your dressing. All other dressings look the same wet, saturated, or dry.”
He said the study confirms what they have seen in practice, adding that the product is unique.
“No one else in the world has this technology,” Mr. Greer said.
Surgeons want to see more data
Heather Evans, MD, a general surgeon with the Medical University of South Carolina, MUSC Health, Charleston, who was not involved with the study, praised the color-indicator design and said she liked the bandage’s narrow indication for low-exudate wounds.
She said in an interview, “It’s a lot to put on a layperson to suddenly know how to take care of wounds when you leave the hospital.”
Giving them the confidence that their wound is safe if the blue doesn’t appear “is a really cool concept,” she said.
She said that, although the volunteers included some elderly people and people with conditions such as diabetes that could affect wound healing, the bandage needs to be tested with a bigger trial to see if it is effective outside controlled conditions.
She also said that some occlusive dressings will be more durable and stay on days longer than DSD or the comparator, which may affect the choice for some.
“The average length of dressing time in this study was less than 2 days,” she pointed out.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health Bedford, who was not involved with the study, agreed that any surgical or wound dressing, including transparent films, can become dislodged, and said, “This type of product has promise but this is a small pilot study. I would want to see results from a trial of actual surgical patients to see if this type of dressing did indeed decrease post-op infections compared to standard dressing materials.”
Not all are convinced either that there is a need to be filled or that DSD will be the right solution.
Therese Duane, MD, a general surgeon with Texas Health Harris Methodist Fort Worth, who was not part of the study, said in an interview that she “has no issues with the current products.”
She added that more information is needed before considering DSD a better solution, including animal studies and use “on very sick patients.”
“Twenty volunteers with cuts on their arm is barely a start for comparison,” she said.
The authors, led by Kristy Breisinger, a research analyst with the SerenaGroup Research Foundation in Cambridge, Mass., acknowledged the limitations, including the small sample size and that the trial was conducted at only one institution. Additionally, the analysis is based on descriptive statistics.
They write that the trial design was chosen “to simulate a real-world setting that is not always achievable in animal studies.”
The research was sponsored by an unrestricted grant from the maker of DSD, DrySee Inc., in Houston.
Mr. Greer is DrySee’s CEO. The authors and Dr. Duane, Dr. Rickert, and Dr. Evans declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF WOUND CARE