User login
COVID-19 Is a Very Weird Virus
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.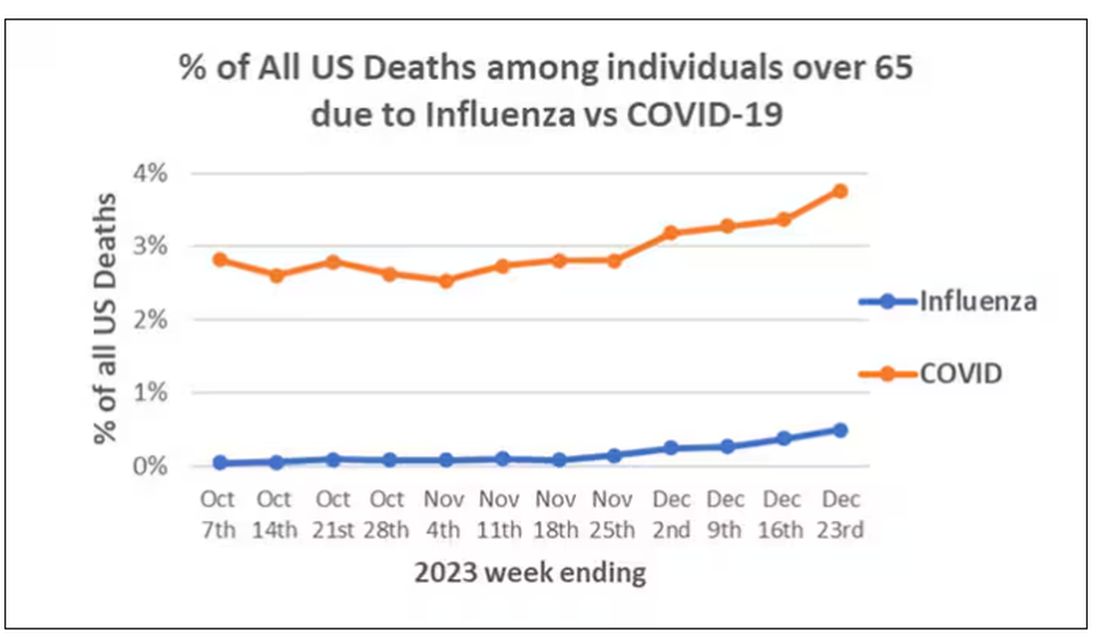
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)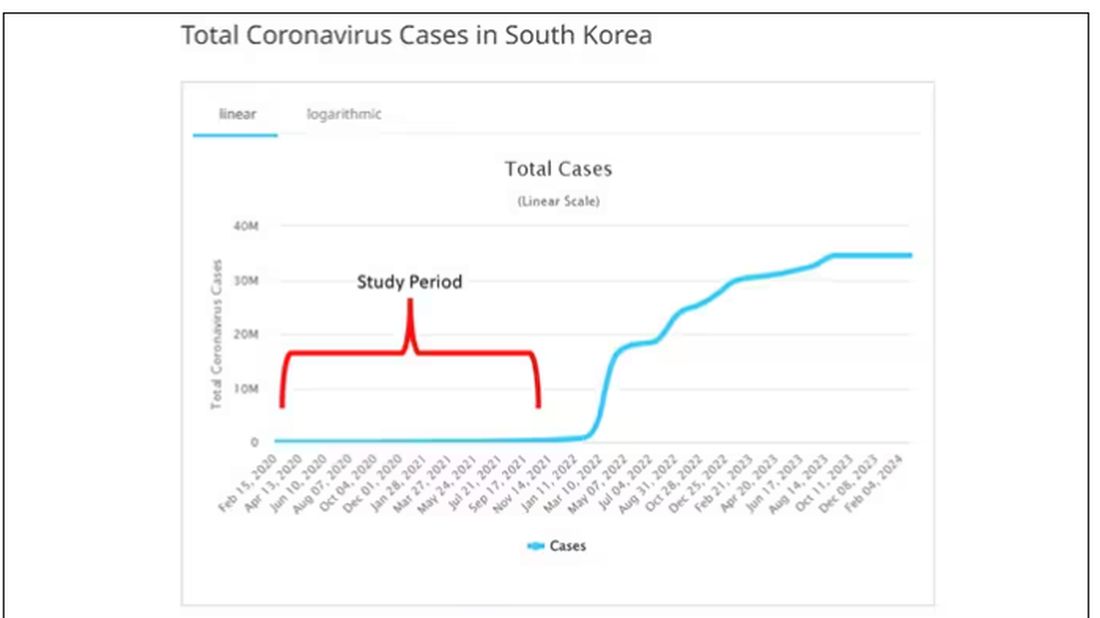
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.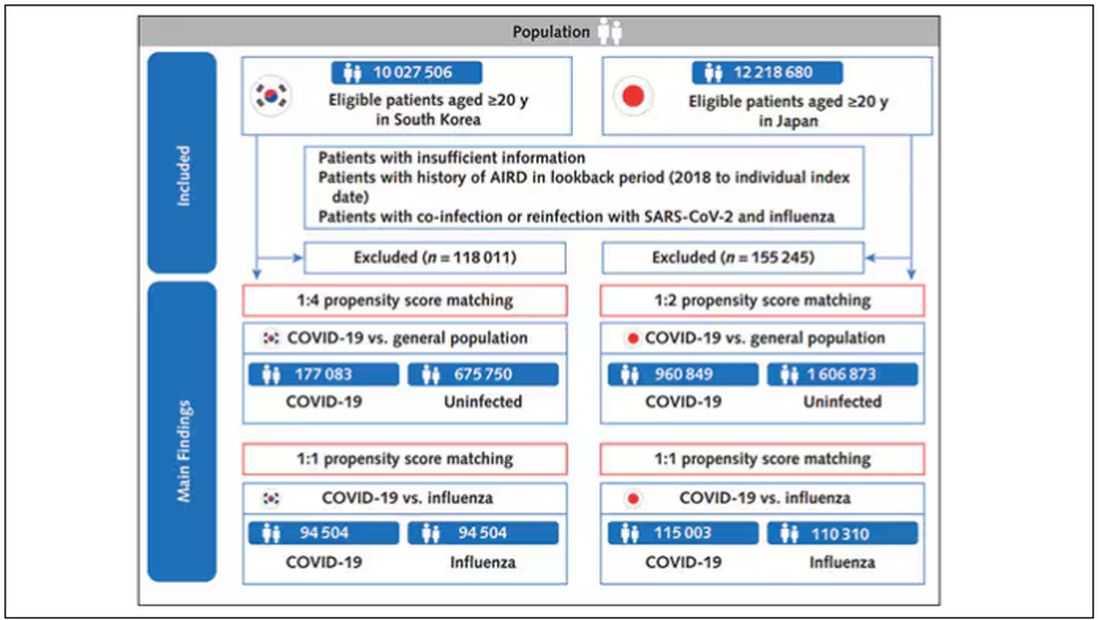
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).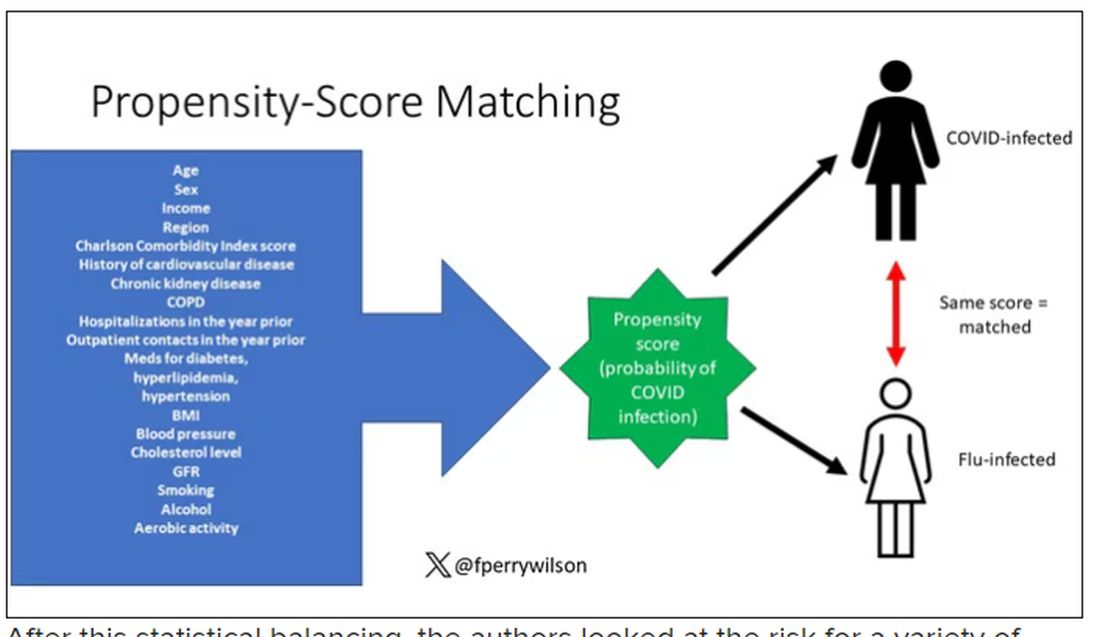
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.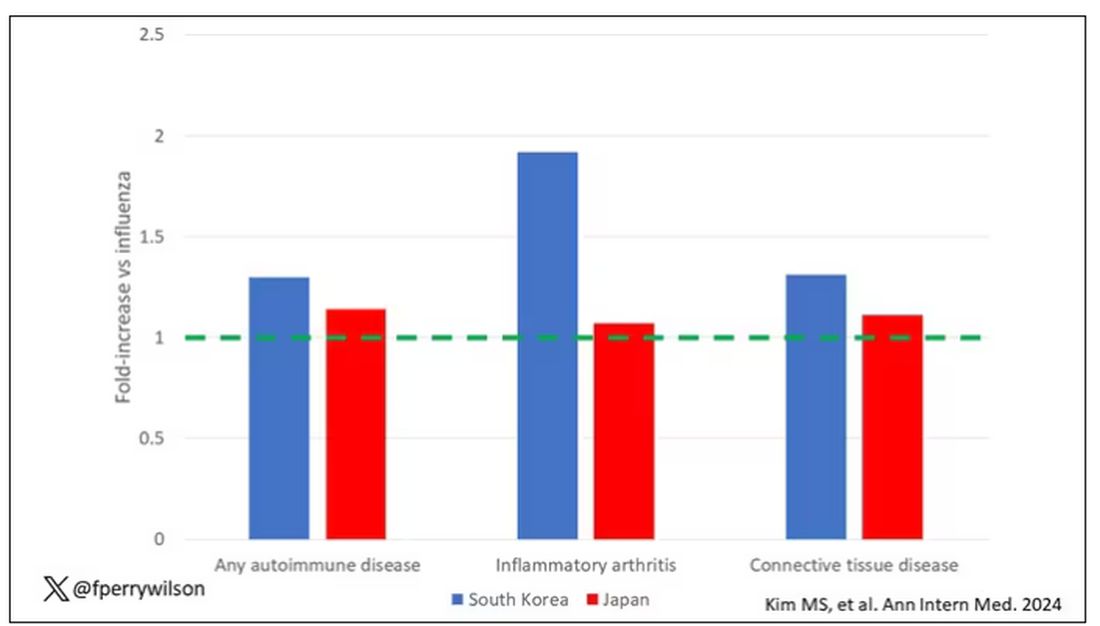
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.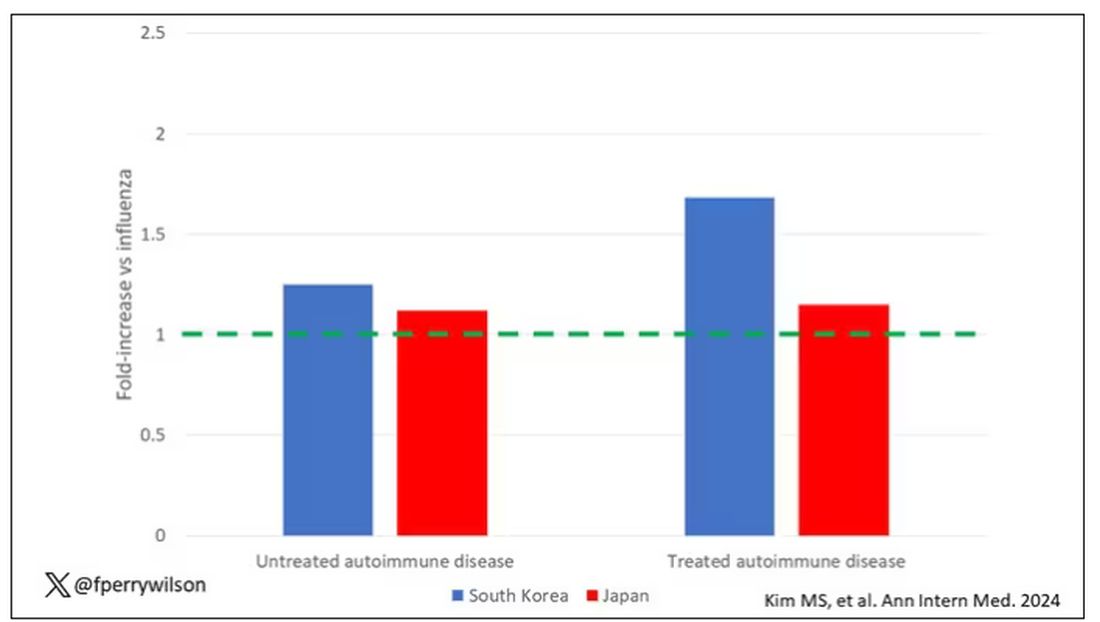
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.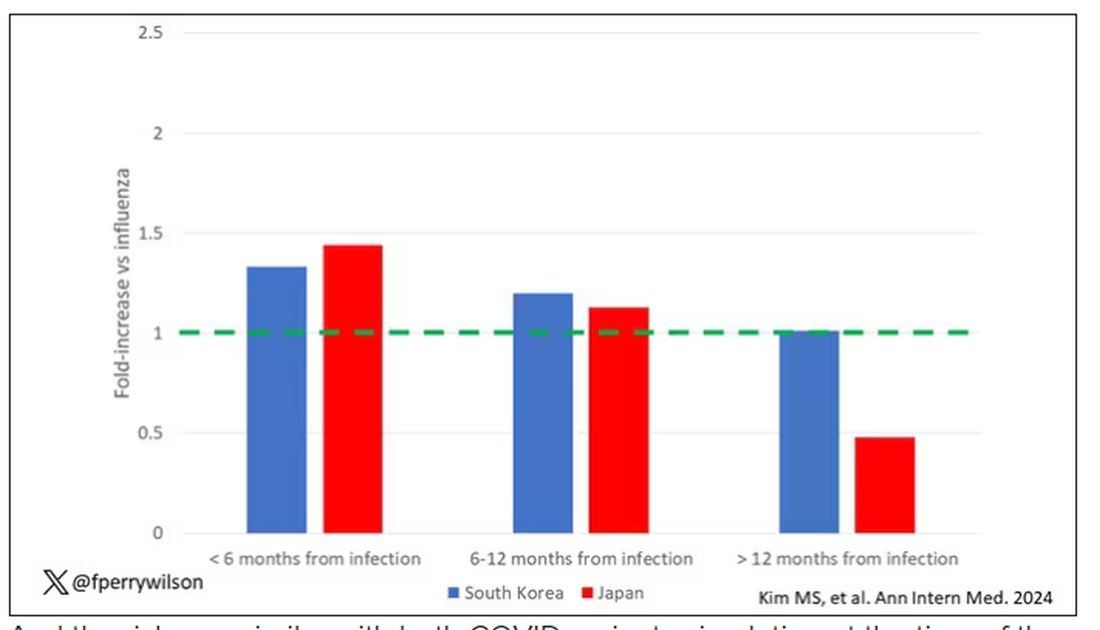
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?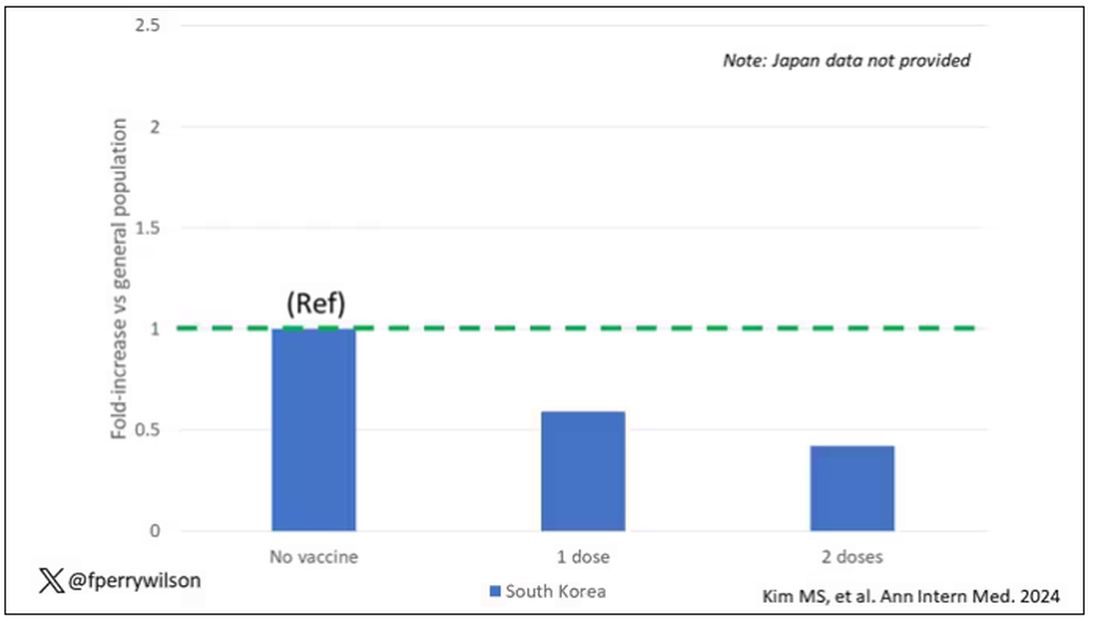
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Effect of Metformin Across Renal Function States in Diabetes
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.
Mixing Paxlovid With Specific Immunosuppressants Risks Serious Adverse Reactions
The Pharmacovigilance Risk Assessment Committee (PRAC) of the European Medicines Agency (EMA) has issued a reminder to healthcare professionals regarding the potential serious adverse reactions associated with Paxlovid when administered in combination with specific immunosuppressants.
These immunosuppressants, encompassing calcineurin inhibitors (tacrolimus and ciclosporin) and mTOR inhibitors (everolimus and sirolimus), possess a narrow safe dosage range. They are recognized for their role in diminishing the activity of the immune system and are typically prescribed for autoimmune conditions and organ transplant recipients.
The highlighted risk arises due to drug-drug interactions, which can compromise the body’s ability to eliminate these medicines effectively.
Paxlovid, also known as nirmatrelvir with ritonavir, is an antiviral medication used to treat COVID-19 in adults who do not require supplemental oxygen and who are at an increased risk of progressing to severe COVID-19. It should be administered as soon as possible after a diagnosis of COVID-19 has been made and within 5 days of symptom onset.
Conditional marketing authorization for Paxlovid was granted across the European Union (EU) on January 28, 2022, and subsequently transitioned to full marketing authorization on February 24, 2023.
Developed by Pfizer, Paxlovid exhibited an 89% reduction in the risk for hospitalization or death among unvaccinated individuals in a phase 2-3 clinical trial. This led the National Institutes of Health to prioritize Paxlovid over other COVID-19 treatments. Subsequent real-world studies have affirmed its effectiveness, even among the vaccinated.
When combining Paxlovid with tacrolimus, ciclosporin, everolimus, or sirolimus, healthcare professionals need to actively monitor their blood levels. This proactive approach is essential to mitigate the risk for drug-drug interactions and potential serious reactions. They should collaborate with a multidisciplinary team of specialists to navigate the complexities of administering these medications concurrently.
Further, Paxlovid must not be coadministered with medications highly reliant on CYP3A liver enzymes for elimination, such as the immunosuppressant voclosporin. When administered together, there is a risk for these drugs interfering with each other’s metabolism, potentially leading to altered blood levels, reduced effectiveness, or an increased risk for adverse reactions.
After a thorough review, PRAC has highlighted potential serious adverse reactions, including fatal cases, due to drug interactions between Paxlovid and specified immunosuppressants. Thus, it issued a direct healthcare professional communication (DHPC) to emphasize the recognized risk for these interactions, as previously outlined in Paxlovid’s product information.
The DHPC for Paxlovid will undergo further evaluation by EMA’s Committee for Medicinal Products for Human Use and, upon adoption, will be disseminated to healthcare professionals. The communication plan will include publication on the DHPCs page and in national registers across EU Member States.
A version of this article appeared on Medscape.com.
The Pharmacovigilance Risk Assessment Committee (PRAC) of the European Medicines Agency (EMA) has issued a reminder to healthcare professionals regarding the potential serious adverse reactions associated with Paxlovid when administered in combination with specific immunosuppressants.
These immunosuppressants, encompassing calcineurin inhibitors (tacrolimus and ciclosporin) and mTOR inhibitors (everolimus and sirolimus), possess a narrow safe dosage range. They are recognized for their role in diminishing the activity of the immune system and are typically prescribed for autoimmune conditions and organ transplant recipients.
The highlighted risk arises due to drug-drug interactions, which can compromise the body’s ability to eliminate these medicines effectively.
Paxlovid, also known as nirmatrelvir with ritonavir, is an antiviral medication used to treat COVID-19 in adults who do not require supplemental oxygen and who are at an increased risk of progressing to severe COVID-19. It should be administered as soon as possible after a diagnosis of COVID-19 has been made and within 5 days of symptom onset.
Conditional marketing authorization for Paxlovid was granted across the European Union (EU) on January 28, 2022, and subsequently transitioned to full marketing authorization on February 24, 2023.
Developed by Pfizer, Paxlovid exhibited an 89% reduction in the risk for hospitalization or death among unvaccinated individuals in a phase 2-3 clinical trial. This led the National Institutes of Health to prioritize Paxlovid over other COVID-19 treatments. Subsequent real-world studies have affirmed its effectiveness, even among the vaccinated.
When combining Paxlovid with tacrolimus, ciclosporin, everolimus, or sirolimus, healthcare professionals need to actively monitor their blood levels. This proactive approach is essential to mitigate the risk for drug-drug interactions and potential serious reactions. They should collaborate with a multidisciplinary team of specialists to navigate the complexities of administering these medications concurrently.
Further, Paxlovid must not be coadministered with medications highly reliant on CYP3A liver enzymes for elimination, such as the immunosuppressant voclosporin. When administered together, there is a risk for these drugs interfering with each other’s metabolism, potentially leading to altered blood levels, reduced effectiveness, or an increased risk for adverse reactions.
After a thorough review, PRAC has highlighted potential serious adverse reactions, including fatal cases, due to drug interactions between Paxlovid and specified immunosuppressants. Thus, it issued a direct healthcare professional communication (DHPC) to emphasize the recognized risk for these interactions, as previously outlined in Paxlovid’s product information.
The DHPC for Paxlovid will undergo further evaluation by EMA’s Committee for Medicinal Products for Human Use and, upon adoption, will be disseminated to healthcare professionals. The communication plan will include publication on the DHPCs page and in national registers across EU Member States.
A version of this article appeared on Medscape.com.
The Pharmacovigilance Risk Assessment Committee (PRAC) of the European Medicines Agency (EMA) has issued a reminder to healthcare professionals regarding the potential serious adverse reactions associated with Paxlovid when administered in combination with specific immunosuppressants.
These immunosuppressants, encompassing calcineurin inhibitors (tacrolimus and ciclosporin) and mTOR inhibitors (everolimus and sirolimus), possess a narrow safe dosage range. They are recognized for their role in diminishing the activity of the immune system and are typically prescribed for autoimmune conditions and organ transplant recipients.
The highlighted risk arises due to drug-drug interactions, which can compromise the body’s ability to eliminate these medicines effectively.
Paxlovid, also known as nirmatrelvir with ritonavir, is an antiviral medication used to treat COVID-19 in adults who do not require supplemental oxygen and who are at an increased risk of progressing to severe COVID-19. It should be administered as soon as possible after a diagnosis of COVID-19 has been made and within 5 days of symptom onset.
Conditional marketing authorization for Paxlovid was granted across the European Union (EU) on January 28, 2022, and subsequently transitioned to full marketing authorization on February 24, 2023.
Developed by Pfizer, Paxlovid exhibited an 89% reduction in the risk for hospitalization or death among unvaccinated individuals in a phase 2-3 clinical trial. This led the National Institutes of Health to prioritize Paxlovid over other COVID-19 treatments. Subsequent real-world studies have affirmed its effectiveness, even among the vaccinated.
When combining Paxlovid with tacrolimus, ciclosporin, everolimus, or sirolimus, healthcare professionals need to actively monitor their blood levels. This proactive approach is essential to mitigate the risk for drug-drug interactions and potential serious reactions. They should collaborate with a multidisciplinary team of specialists to navigate the complexities of administering these medications concurrently.
Further, Paxlovid must not be coadministered with medications highly reliant on CYP3A liver enzymes for elimination, such as the immunosuppressant voclosporin. When administered together, there is a risk for these drugs interfering with each other’s metabolism, potentially leading to altered blood levels, reduced effectiveness, or an increased risk for adverse reactions.
After a thorough review, PRAC has highlighted potential serious adverse reactions, including fatal cases, due to drug interactions between Paxlovid and specified immunosuppressants. Thus, it issued a direct healthcare professional communication (DHPC) to emphasize the recognized risk for these interactions, as previously outlined in Paxlovid’s product information.
The DHPC for Paxlovid will undergo further evaluation by EMA’s Committee for Medicinal Products for Human Use and, upon adoption, will be disseminated to healthcare professionals. The communication plan will include publication on the DHPCs page and in national registers across EU Member States.
A version of this article appeared on Medscape.com.
My Kidney Is Fine, Can’t You Cystatin C?
Clinicians usually measure renal function by using surrogate markers because directly measuring glomerular filtration rate (GFR) is not routinely feasible in a clinical setting.1,2 Creatinine (Cr) and cystatin C (CysC) are the 2 main surrogate molecules used to estimate GFR.3
Creatine is a molecule nonenzymatically converted into Cr, weighing only 113 Da in skeletal muscles.4 It is then filtered at the glomeruli and secreted at the proximal tubules of the kidneys. However, serum Cr (sCr) levels are affected by several factors, including age, biological sex, liver function, diet, and muscle mass.5 Historically, sCr levels also are affected by race.5 In an early study of factors affecting accurate GFR, researchers reported that self-identified African American patients had a 16% higher GFR than those who did not when using Cr.6 Despite this, the inclusion of Cr on a basic metabolic panel has allowed automatic reporting of an estimated GFR using sCr (eGFRCr) to be readily available.7

In comparison to Cr, CysC is an endogenous protein weighing 13 kDa produced by all nucleated cells.8,9 CysC is filtered by the kidney at the glomeruli and completely reabsorbed and catabolized by epithelial cells at the proximal tubule.9 Since production is not dependent on skeletal muscle, there are fewer physiological impacts on serum concentration of CysC. Levels of CysC may be elevated by factors shown in the Table.
Estimating Glomerular Filtration Rates
Multiple equations were developed to mitigate the impact of extraneous factors on the accuracy of an eGFRCr. The first widely used equation that included a variable adjustment for race was the Modification of Diet in Renal Disease study, presented in 2006.10 The equation increased the accuracy of eGFRCr further by adjusting for sex and age. It was followed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation in 2009, which was more accurate at higher GFR levels.11
CysC was simultaneously studied as an alternative to Cr with multiple equation iterations shown to be viable in various populations as early as 2003.12-15 However, it was not until 2012 that an equation for the use of CysC was offered for widespread use as an alternative to Cr alongside further refinement of the CKD-EPI equation for Cr.16 A new formula was presented in 2021 to use both sCr and serum CysC levels to obtain a more accurate estimation of GFR.17 Research continues its effort to accurately estimate GFR for diagnosing kidney disease and assessing comorbidities relating to decreased kidney function.3
All historical equations attempted to mitigate the potential impact of race on sCr level when calculating eGFRCr by assigning a separate variable for African American patients. As an unintended adverse effect, these equations may have led to discrimination by having a different equation for African American patients.18 Moreover, these Cr-based equations remain less accurate in patients with varied muscle mass, such as older patients, bodybuilders, athletes, and individuals with varied extremes of daily protein intake.1,8,9,19 Several medications can also directly affect Cr clearance, reducing its ability to act as a surrogate for kidney function.1 In this case report, we discuss an African American patient with high muscle mass and protein intake who was initially diagnosed with kidney disease based on an elevated Cr and found to be misdiagnosed based on the use of CysC for a more accurate GFR estimation.
Case Presentation

A 35-year-old African American man serving in the military and recently diagnosed with HIV was referred to a nephrology clinic for further evaluation of an acute elevation in sCr. Before treatment for HIV, a brief record review showed a baseline Cr of about 1.3 mg/dL, with an eGFRCr of 75 mL/min/1.73 m2.20 In the same month, the patient was prescribed bictegravir/emtricitabine/tenofovir alafenamide, an HIV drug with nephrotoxic potential.21 The patient's total viral load remained low, and CD4 count remained > 500 after initiation of the HIV treatment. He was in his normal state of health and had no known contributory history before his HIV diagnosis. Cr readings peaked at 1.83 mg/dL after starting the HIV treatment and remained elevated to 1.73 mg/dL over the next few months, corresponding to CKD stage 3A. Because bictegravir/emtricitabine/tenofovir alafenamide is cleared by the kidneys and has a nephrotoxic profile, the clinical care team considered dosage adjustment or a medication switch given his observed elevated eGFRCr based on the CKD-EPI 2021 equation for Cr alone. It was also noted that the patient had a similar Cr spike to 1.83 mg/dL in 2018 without any identifiable renal insult or symptoms (Figure).
Diagnostic Evaluation
The primary care team ordered a renal ultrasound and referred the patient to the nephrology clinic. The nephrologist ordered the following laboratory studies: urine microalbumin to Cr ratio, basic metabolic panel (BMP), comprehensive metabolic panel (CMP), urinalysis, urine protein, urine Cr, parathyroid hormone level, hemoglobin A1c, complement component 3/4 panels, antinuclear and antineutrophil cytoplasmic antibodies titers, glomerular basement membrane antibody titer, urine light chains, serum protein electrophoresis, κ/λ ratio, viral hepatitis panel, and rapid plasma reagin testing. Much of this laboratory evaluation served to rule out any secondary causes of kidney disease, including autoimmune disease, monoclonal or polyclonal gammopathies, diabetic nephropathy or glomerulosclerosis, and nephrotic or nephritic syndromes.
All laboratory studies returned within normal limits; no proteinuria was discovered on urinalysis, and no abnormalities were visualized on renal ultrasound. Bictegravir/emtricitabine/tenofovir alafenamide nephrotoxicity was highest among the differential diagnoses due to the timing of Cr elevation coinciding with the initiation of the medications. The patient's CysC level was 0.85 mg/dL with a calculated eGFRCys of 125 mL/min/1.73 m2. The calculated sCR and serum cystatin C (eGFRCr-Cys) using the new 2021 equation and when adjusting for body surface area placed his eGFR at 92 mL/min/1.73 m2.20
The patient’s eGFRCys reassured the care team that the patient’s renal function was not acutely or chronically impacted by bictegravir/emtricitabine/tenofovir alafenamide, resulting in avoidance of unnecessary dosage adjustment or discontinuation of the HIV treatment. The patient reported a chronic habit of protein and creatine supplementation and bodybuilding, which likely further compounded the discrepancy between eGFRCr and eGFRCys and explained his previous elevation in Cr in 2018.
Follow-up
The patient underwent serial monitoring that revealed a stable Cr and unremarkable eGFR, ruling out CKD. There has been no evidence of worsening kidney disease to date, and the patient remained on his initial HIV regimen.
Discussion
This case shows the importance of using CysC as an alternative or confirmatory marker compared with sCr to estimate GFR in patients with high muscle mass and/or high creatine intake, such as many in the US Department of Defense (DoD) and US Department of Veterans Affairs (VA) patient populations. In the presented case, recorded Cr levels climbed from baseline Cr with the initiation of bictegravir/emtricitabine/tenofovir alafenamide. This raised the concern that HIV treatment was leading to the development of kidney damage.22
Diagnosis of kidney disease as opposed to the normal decline of eGFR with age in individuals without intrinsic CKD requires GFR ≥ 60 mL/min/1.73 m2 with kidney damage (proteinuria or radiological abnormalities, etc) or GFR < 135 to 140 mL/min/1.73 m2 minus the patient’s age in years.23 The patient’s Cr peak at 1.83 mg/dL in 2018 led to an inappropriate diagnosis of kidney disease stage 3a based on an eGFRCr (2021 equation) of 52 mL/min/1.73 m2 when not corrected for body surface area.20 However, using the new 2021 equation using both Cr and CysC, the patient’s eGFRCr-Cys was 92 mL/min/1.73 m2 after a correction for body surface area.
The 2009 CKD-EPI recommended the calculation of eGFR based on SCr concentration using age, sex, and race while the 2021 CKD-EPI recommended the exclusion of race.3 Both equations are less accurate in African American patients, individuals taking medications that interfere with Cr secretion and assay, and patients taking creatine supplements, high daily protein intake, or with high muscle mass.7 These settings result in a decreased eGFRCr without corresponding eGFRCys changes. Using SCr and CysC together, the eGFRCr-Cys yields improved concordance to measured GFR across race groups compared to GFR estimation based on Cr alone, which can avoid unnecessary expensive diagnostic workup, inappropriate kidney disease diagnosis, incorrect dosing of drugs, and accurately represent the military readiness of patients. Interestingly, in African American patients with recently diagnosed HIV, CKD-EPI using both Cr and CysC without race inclusion led to only a 2.9% overestimation of GFR and was the only equation with no statistically significant bias compared with measured GFR.24
A March 2023 case involving an otherwise healthy 26-year-old male active-duty US Navy member with a history of excessive protein supplement intake and intense exercise < 24 hours before laboratory work was diagnosed with CKD after a measured Cr of 16 mg/dL and an eGFRCr of 4 mL/min/1.73 m2 without any other evidence of kidney disease. His CysC remained within normal limits, resulting in a normal eGFRCys of 121 mL/min/1.73 m2, indicating no CKD. His Cr and eGFR recovered 10 days after his clinic visit and cessation of his supplement intake. These findings may not be uncommon given that 65% of active-duty military use protein supplements and 38% use other performance-enhancing supplements, such as creatine, according to a study.25
Unfortunately, the BMP/CMP traditionally used at VA centers use the eGFRCr equation, and it is unknown how many primary care practitioners recognize the limitations of these metabolic panels on accurate estimation of kidney function. However, in 2022 an expert panel including VA physicians recommended the immediate use of eGFRCr-Cys or eGFRCys for confirmatory testing and potentially screening of CKD.26 A small number of VAs have since adopted this recommendation, which should lead to fewer misdiagnoses among US military members as clinicians should now have access to more accurate measurements of GFR.
The VA spends about $18 billion (excluding dialysis) for care for 1.1 to 2.5 million VA patients with CKD.27 The majority of these diagnoses were undoubtedly made using the eGFRCr equation, raising the question of how many may be misdiagnosed. Assessment with CysC is currently relatively expensive, but it will likely become more affordable as the use of CysC as a confirmatory test increases.5 The cost of a sCr test is about $2.50, while CysC costs about $10.60, with variation from laboratory to laboratory.28 By comparison, a renal ultrasound costs $99 to $140 for uninsured patients.29 Furthermore, the cost of CysC testing is likely to trend downward as more facilities adopt the use of CysC measurements, which can be run on the same analytical equipment currently used for Cr measurements. Currently, most laboratories do not have established assays to use in-house and thus require CysC to be sent out to a laboratory, which increases result time and makes Cr a more attractive option. As more laboratories adopt assays for CysC, the cost of reagents will further decrease.
Given such considerations, confirmation testing of kidney function with CysC in specific patient populations with decreased eGFRCr without other features of CKD can offer great medical and financial benefits. A 2023 KDIGO report noted that many individuals may be mistakenly diagnosed with CKD when using eGFRCr.3 KDIGO noted that a 2013 meta-analysis of 90,000 individuals found that with a Cr-based eGFR of 45 to 59 mL/min/1.73 m2 (42%) had a CysC-based eGFR of ≥ 60 mL/min/1.73 m2. An eGFRCr of 45 to 59 represents 54% of all patients with CKD, amounting to millions of people (including current and former military personnel).3,29-31 Correcting a misdiagnosis of CKD would bring significant relief to patients and save millions in health care spending.
Conclusions
In patients who meet CKD criteria using eGFRCr but without other features of CKD, we recommend using confirmatory CysC levels and the eGFRCr-Cys equation. This will align care with the KDIGO guidelines and could be a cost-effective step toward improving military patient care. Further work in this area should focus on determining the knowledge gaps in primary care practitioners’ understanding of the limits of eGFRCr, the potential mitigation of concomitant CysC testing in equivocal CKD cases, and the cost-effectiveness and increased utilization of CysC.
1. Gabriel R. Time to scrap creatinine clearance? Br Med J (Clin Res Ed). 1986;293(6555):1119-1120. doi:10.1136/bmj.293.6555.1119
2. Swan SK. The search continues—an ideal marker of GFR. Clin Chem. 1997;43(6):913-914.doi:10.1093/clinchem/43.6.913 3. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1).
4. Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80(3):1107-1213. doi:10.1152/physrev.2000.80.3.1107
5. Ferguson TW, Komenda P, Tangri N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr Opin Nephrol Hypertens. 2015;24(3):295-300. doi:10.1097/mnh.0000000000000115
6. Levey AS, Titan SM, Powe NR, Coresh J, Inker LA. Kidney disease, race, and GFR estimation. Clin J Am Soc Nephrol. 2020;15(8):1203-1212. doi:10.2215/cjn.12791019
7. Shlipak MG, Tummalapalli SL, Boulware LE, et al; Conference Participants. The case for early identification and intervention of chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) controversies conference. Kidney Int. 2021;99(1):34-47. doi:10.1016/j.kint.2020.10.012
8. O’Riordan SE, Webb MC, Stowe HJ, et al. Cystatin C improves the detection of mild renal dysfunction in older patients. Ann Clin Biochem. 2003;40(pt 6):648-655. doi:10.1258/000456303770367243
9. Stevens LA, Schmid CH, Greene T, et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 2009;75(6):652-660. doi:10.1038/ki.2008.638
10. Levey AS, Coresh J, Greene T, et al; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247-254. doi:10.7326/0003-4819-145-4-200608150-00004
11. Levey AS, Stevens LA, Schmid CH, et al; Chronic Kidney Disease Epidemiology Collaboration. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612. doi:10.7326/0003-4819-150-9-200905050-00006
12. Pöge U, Gerhardt T, Stoffel-Wagner B, Klehr HU, Sauerbruch T, Woitas RP. Calculation of glomerular filtration rate based on cystatin C in cirrhotic patients. Nephrol Dial Transplant. 2006;21(3):660-664. doi:10.1093/ndt/gfi305
13. Larsson A, Malm J, Grubb A, Hansson LO. Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand J Clin Lab Invest. 2004;64(1):25-30. doi:10.1080/00365510410003723.
14. Macisaac RJ, Tsalamandris C, Thomas MC, et al. Estimating glomerular filtration rate in diabetes: a comparison of cystatin-C- and creatinine-based methods. Diabetologia. 2006;49(7):1686-1689. doi:10.1007/s00125-006-0275-7
15. Rule AD, Bergstralh EJ, Slezak JM, Bergert J, Larson TS. Glomerular filtration rate estimated by cystatin C among different clinical presentations. Kidney Int. 2006;69(2):399-405. doi:10.1038/sj.ki.5000073
16. Inker LA, Schmid CH, Tighiouart H, et al; Chronic Kidney Disease Epidemiology Collaboration Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20-29. doi:10.1056/NEJMoa1114248
17. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
18. Inker LA, Eneanya ND, Coresh J, et al; Chronic Kidney Disease Epidemiology Collaboration. New creatinine- and cystatin C–Based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737-1749. doi:10.1056/NEJMoa2102953
19. Oterdoom LH, Gansevoort RT, Schouten JP, de Jong PE, Gans ROB, Bakker SJL. Urinary creatinine excretion, an indirect measure of muscle mass, is an independent predictor of cardiovascular disease and mortality in the general population. Atherosclerosis. 2009;207(2):534-540. doi.10.1016/j.atherosclerosis.2009.05.010
20. National Kidney Foundation Inc. eGFR calculator. Accessed October 20, 2023. https://www.kidney.org/professionals/kdoqi/gfr_calculator
21. Ueaphongsukkit T, Gatechompol S, Avihingsanon A, et al. Tenofovir alafenamide nephrotoxicity: a case report and literature review. AIDS Res Ther. 2021;18(1):53. doi:10.1186/s12981-021-00380-w
22. D’Agati V, Appel GB. Renal pathology of human immunodeficiency virus infection. Semin Nephrol. 1998;18(4):406-421.
23. Glassock RJ, Winearls C. Ageing and the glomerular filtration rate: truths and consequences. Trans Am Clin Climatol Assoc. 2009;120:419-428.
24. Seape T, Gounden V, van Deventer HE, Candy GP, George JA. Cystatin C- and creatinine-based equations in the assessment of renal function in HIV-positive patients prior to commencing highly active antiretroviral therapy. Ann Clin Biochem. 2016;53(pt 1):58-66. doi:10.1177/0004563215579695
25. Tobin TW, Thurlow JS, Yuan CM. A healthy active duty soldier with an elevated serum creatinine. Mil Med. 2023;188(3-4):e866-e869. doi:10.1093/milmed/usab163
26. Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Am J Kidney Dis. 2022;79(2):268-288.e1. doi:10.1053/j.ajkd.2021.08.003
27. Saran R, Pearson A, Tilea A, et al; VA-REINS Steering Committee; VA Advisory Board. Burden and cost of caring for us veterans with CKD: initial findings from the VA Renal Information System (VA-REINS). Am J Kidney Dis. 2021;77(3):397-405. doi:10.1053/j.ajkd.2020.07.013
28. Zoler ML. Nephrologists make the case for cystatin C-based eGFR. Accessed October 20, 2023. https://www.medscape.com/viewarticle/951335#vp_2
29. Versaw N. How much does an ultrasound cost? Updated February 2022. Accessed October 20, 2023. https://www.compare.com/health/healthcare-resources/how-much-does-an-ultrasound-cost
30. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165-180. doi:10.1016/S0140-6736(11)60178-5
31. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
Clinicians usually measure renal function by using surrogate markers because directly measuring glomerular filtration rate (GFR) is not routinely feasible in a clinical setting.1,2 Creatinine (Cr) and cystatin C (CysC) are the 2 main surrogate molecules used to estimate GFR.3
Creatine is a molecule nonenzymatically converted into Cr, weighing only 113 Da in skeletal muscles.4 It is then filtered at the glomeruli and secreted at the proximal tubules of the kidneys. However, serum Cr (sCr) levels are affected by several factors, including age, biological sex, liver function, diet, and muscle mass.5 Historically, sCr levels also are affected by race.5 In an early study of factors affecting accurate GFR, researchers reported that self-identified African American patients had a 16% higher GFR than those who did not when using Cr.6 Despite this, the inclusion of Cr on a basic metabolic panel has allowed automatic reporting of an estimated GFR using sCr (eGFRCr) to be readily available.7
In comparison to Cr, CysC is an endogenous protein weighing 13 kDa produced by all nucleated cells.8,9 CysC is filtered by the kidney at the glomeruli and completely reabsorbed and catabolized by epithelial cells at the proximal tubule.9 Since production is not dependent on skeletal muscle, there are fewer physiological impacts on serum concentration of CysC. Levels of CysC may be elevated by factors shown in the Table.
Estimating Glomerular Filtration Rates
Multiple equations were developed to mitigate the impact of extraneous factors on the accuracy of an eGFRCr. The first widely used equation that included a variable adjustment for race was the Modification of Diet in Renal Disease study, presented in 2006.10 The equation increased the accuracy of eGFRCr further by adjusting for sex and age. It was followed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation in 2009, which was more accurate at higher GFR levels.11
CysC was simultaneously studied as an alternative to Cr with multiple equation iterations shown to be viable in various populations as early as 2003.12-15 However, it was not until 2012 that an equation for the use of CysC was offered for widespread use as an alternative to Cr alongside further refinement of the CKD-EPI equation for Cr.16 A new formula was presented in 2021 to use both sCr and serum CysC levels to obtain a more accurate estimation of GFR.17 Research continues its effort to accurately estimate GFR for diagnosing kidney disease and assessing comorbidities relating to decreased kidney function.3
All historical equations attempted to mitigate the potential impact of race on sCr level when calculating eGFRCr by assigning a separate variable for African American patients. As an unintended adverse effect, these equations may have led to discrimination by having a different equation for African American patients.18 Moreover, these Cr-based equations remain less accurate in patients with varied muscle mass, such as older patients, bodybuilders, athletes, and individuals with varied extremes of daily protein intake.1,8,9,19 Several medications can also directly affect Cr clearance, reducing its ability to act as a surrogate for kidney function.1 In this case report, we discuss an African American patient with high muscle mass and protein intake who was initially diagnosed with kidney disease based on an elevated Cr and found to be misdiagnosed based on the use of CysC for a more accurate GFR estimation.
Case Presentation
A 35-year-old African American man serving in the military and recently diagnosed with HIV was referred to a nephrology clinic for further evaluation of an acute elevation in sCr. Before treatment for HIV, a brief record review showed a baseline Cr of about 1.3 mg/dL, with an eGFRCr of 75 mL/min/1.73 m2.20 In the same month, the patient was prescribed bictegravir/emtricitabine/tenofovir alafenamide, an HIV drug with nephrotoxic potential.21 The patient's total viral load remained low, and CD4 count remained > 500 after initiation of the HIV treatment. He was in his normal state of health and had no known contributory history before his HIV diagnosis. Cr readings peaked at 1.83 mg/dL after starting the HIV treatment and remained elevated to 1.73 mg/dL over the next few months, corresponding to CKD stage 3A. Because bictegravir/emtricitabine/tenofovir alafenamide is cleared by the kidneys and has a nephrotoxic profile, the clinical care team considered dosage adjustment or a medication switch given his observed elevated eGFRCr based on the CKD-EPI 2021 equation for Cr alone. It was also noted that the patient had a similar Cr spike to 1.83 mg/dL in 2018 without any identifiable renal insult or symptoms (Figure).
Diagnostic Evaluation
The primary care team ordered a renal ultrasound and referred the patient to the nephrology clinic. The nephrologist ordered the following laboratory studies: urine microalbumin to Cr ratio, basic metabolic panel (BMP), comprehensive metabolic panel (CMP), urinalysis, urine protein, urine Cr, parathyroid hormone level, hemoglobin A1c, complement component 3/4 panels, antinuclear and antineutrophil cytoplasmic antibodies titers, glomerular basement membrane antibody titer, urine light chains, serum protein electrophoresis, κ/λ ratio, viral hepatitis panel, and rapid plasma reagin testing. Much of this laboratory evaluation served to rule out any secondary causes of kidney disease, including autoimmune disease, monoclonal or polyclonal gammopathies, diabetic nephropathy or glomerulosclerosis, and nephrotic or nephritic syndromes.
All laboratory studies returned within normal limits; no proteinuria was discovered on urinalysis, and no abnormalities were visualized on renal ultrasound. Bictegravir/emtricitabine/tenofovir alafenamide nephrotoxicity was highest among the differential diagnoses due to the timing of Cr elevation coinciding with the initiation of the medications. The patient's CysC level was 0.85 mg/dL with a calculated eGFRCys of 125 mL/min/1.73 m2. The calculated sCR and serum cystatin C (eGFRCr-Cys) using the new 2021 equation and when adjusting for body surface area placed his eGFR at 92 mL/min/1.73 m2.20
The patient’s eGFRCys reassured the care team that the patient’s renal function was not acutely or chronically impacted by bictegravir/emtricitabine/tenofovir alafenamide, resulting in avoidance of unnecessary dosage adjustment or discontinuation of the HIV treatment. The patient reported a chronic habit of protein and creatine supplementation and bodybuilding, which likely further compounded the discrepancy between eGFRCr and eGFRCys and explained his previous elevation in Cr in 2018.
Follow-up
The patient underwent serial monitoring that revealed a stable Cr and unremarkable eGFR, ruling out CKD. There has been no evidence of worsening kidney disease to date, and the patient remained on his initial HIV regimen.
Discussion
This case shows the importance of using CysC as an alternative or confirmatory marker compared with sCr to estimate GFR in patients with high muscle mass and/or high creatine intake, such as many in the US Department of Defense (DoD) and US Department of Veterans Affairs (VA) patient populations. In the presented case, recorded Cr levels climbed from baseline Cr with the initiation of bictegravir/emtricitabine/tenofovir alafenamide. This raised the concern that HIV treatment was leading to the development of kidney damage.22
Diagnosis of kidney disease as opposed to the normal decline of eGFR with age in individuals without intrinsic CKD requires GFR ≥ 60 mL/min/1.73 m2 with kidney damage (proteinuria or radiological abnormalities, etc) or GFR < 135 to 140 mL/min/1.73 m2 minus the patient’s age in years.23 The patient’s Cr peak at 1.83 mg/dL in 2018 led to an inappropriate diagnosis of kidney disease stage 3a based on an eGFRCr (2021 equation) of 52 mL/min/1.73 m2 when not corrected for body surface area.20 However, using the new 2021 equation using both Cr and CysC, the patient’s eGFRCr-Cys was 92 mL/min/1.73 m2 after a correction for body surface area.
The 2009 CKD-EPI recommended the calculation of eGFR based on SCr concentration using age, sex, and race while the 2021 CKD-EPI recommended the exclusion of race.3 Both equations are less accurate in African American patients, individuals taking medications that interfere with Cr secretion and assay, and patients taking creatine supplements, high daily protein intake, or with high muscle mass.7 These settings result in a decreased eGFRCr without corresponding eGFRCys changes. Using SCr and CysC together, the eGFRCr-Cys yields improved concordance to measured GFR across race groups compared to GFR estimation based on Cr alone, which can avoid unnecessary expensive diagnostic workup, inappropriate kidney disease diagnosis, incorrect dosing of drugs, and accurately represent the military readiness of patients. Interestingly, in African American patients with recently diagnosed HIV, CKD-EPI using both Cr and CysC without race inclusion led to only a 2.9% overestimation of GFR and was the only equation with no statistically significant bias compared with measured GFR.24
A March 2023 case involving an otherwise healthy 26-year-old male active-duty US Navy member with a history of excessive protein supplement intake and intense exercise < 24 hours before laboratory work was diagnosed with CKD after a measured Cr of 16 mg/dL and an eGFRCr of 4 mL/min/1.73 m2 without any other evidence of kidney disease. His CysC remained within normal limits, resulting in a normal eGFRCys of 121 mL/min/1.73 m2, indicating no CKD. His Cr and eGFR recovered 10 days after his clinic visit and cessation of his supplement intake. These findings may not be uncommon given that 65% of active-duty military use protein supplements and 38% use other performance-enhancing supplements, such as creatine, according to a study.25
Unfortunately, the BMP/CMP traditionally used at VA centers use the eGFRCr equation, and it is unknown how many primary care practitioners recognize the limitations of these metabolic panels on accurate estimation of kidney function. However, in 2022 an expert panel including VA physicians recommended the immediate use of eGFRCr-Cys or eGFRCys for confirmatory testing and potentially screening of CKD.26 A small number of VAs have since adopted this recommendation, which should lead to fewer misdiagnoses among US military members as clinicians should now have access to more accurate measurements of GFR.
The VA spends about $18 billion (excluding dialysis) for care for 1.1 to 2.5 million VA patients with CKD.27 The majority of these diagnoses were undoubtedly made using the eGFRCr equation, raising the question of how many may be misdiagnosed. Assessment with CysC is currently relatively expensive, but it will likely become more affordable as the use of CysC as a confirmatory test increases.5 The cost of a sCr test is about $2.50, while CysC costs about $10.60, with variation from laboratory to laboratory.28 By comparison, a renal ultrasound costs $99 to $140 for uninsured patients.29 Furthermore, the cost of CysC testing is likely to trend downward as more facilities adopt the use of CysC measurements, which can be run on the same analytical equipment currently used for Cr measurements. Currently, most laboratories do not have established assays to use in-house and thus require CysC to be sent out to a laboratory, which increases result time and makes Cr a more attractive option. As more laboratories adopt assays for CysC, the cost of reagents will further decrease.
Given such considerations, confirmation testing of kidney function with CysC in specific patient populations with decreased eGFRCr without other features of CKD can offer great medical and financial benefits. A 2023 KDIGO report noted that many individuals may be mistakenly diagnosed with CKD when using eGFRCr.3 KDIGO noted that a 2013 meta-analysis of 90,000 individuals found that with a Cr-based eGFR of 45 to 59 mL/min/1.73 m2 (42%) had a CysC-based eGFR of ≥ 60 mL/min/1.73 m2. An eGFRCr of 45 to 59 represents 54% of all patients with CKD, amounting to millions of people (including current and former military personnel).3,29-31 Correcting a misdiagnosis of CKD would bring significant relief to patients and save millions in health care spending.
Conclusions
In patients who meet CKD criteria using eGFRCr but without other features of CKD, we recommend using confirmatory CysC levels and the eGFRCr-Cys equation. This will align care with the KDIGO guidelines and could be a cost-effective step toward improving military patient care. Further work in this area should focus on determining the knowledge gaps in primary care practitioners’ understanding of the limits of eGFRCr, the potential mitigation of concomitant CysC testing in equivocal CKD cases, and the cost-effectiveness and increased utilization of CysC.
Clinicians usually measure renal function by using surrogate markers because directly measuring glomerular filtration rate (GFR) is not routinely feasible in a clinical setting.1,2 Creatinine (Cr) and cystatin C (CysC) are the 2 main surrogate molecules used to estimate GFR.3
Creatine is a molecule nonenzymatically converted into Cr, weighing only 113 Da in skeletal muscles.4 It is then filtered at the glomeruli and secreted at the proximal tubules of the kidneys. However, serum Cr (sCr) levels are affected by several factors, including age, biological sex, liver function, diet, and muscle mass.5 Historically, sCr levels also are affected by race.5 In an early study of factors affecting accurate GFR, researchers reported that self-identified African American patients had a 16% higher GFR than those who did not when using Cr.6 Despite this, the inclusion of Cr on a basic metabolic panel has allowed automatic reporting of an estimated GFR using sCr (eGFRCr) to be readily available.7
In comparison to Cr, CysC is an endogenous protein weighing 13 kDa produced by all nucleated cells.8,9 CysC is filtered by the kidney at the glomeruli and completely reabsorbed and catabolized by epithelial cells at the proximal tubule.9 Since production is not dependent on skeletal muscle, there are fewer physiological impacts on serum concentration of CysC. Levels of CysC may be elevated by factors shown in the Table.
Estimating Glomerular Filtration Rates
Multiple equations were developed to mitigate the impact of extraneous factors on the accuracy of an eGFRCr. The first widely used equation that included a variable adjustment for race was the Modification of Diet in Renal Disease study, presented in 2006.10 The equation increased the accuracy of eGFRCr further by adjusting for sex and age. It was followed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation in 2009, which was more accurate at higher GFR levels.11
CysC was simultaneously studied as an alternative to Cr with multiple equation iterations shown to be viable in various populations as early as 2003.12-15 However, it was not until 2012 that an equation for the use of CysC was offered for widespread use as an alternative to Cr alongside further refinement of the CKD-EPI equation for Cr.16 A new formula was presented in 2021 to use both sCr and serum CysC levels to obtain a more accurate estimation of GFR.17 Research continues its effort to accurately estimate GFR for diagnosing kidney disease and assessing comorbidities relating to decreased kidney function.3
All historical equations attempted to mitigate the potential impact of race on sCr level when calculating eGFRCr by assigning a separate variable for African American patients. As an unintended adverse effect, these equations may have led to discrimination by having a different equation for African American patients.18 Moreover, these Cr-based equations remain less accurate in patients with varied muscle mass, such as older patients, bodybuilders, athletes, and individuals with varied extremes of daily protein intake.1,8,9,19 Several medications can also directly affect Cr clearance, reducing its ability to act as a surrogate for kidney function.1 In this case report, we discuss an African American patient with high muscle mass and protein intake who was initially diagnosed with kidney disease based on an elevated Cr and found to be misdiagnosed based on the use of CysC for a more accurate GFR estimation.
Case Presentation
A 35-year-old African American man serving in the military and recently diagnosed with HIV was referred to a nephrology clinic for further evaluation of an acute elevation in sCr. Before treatment for HIV, a brief record review showed a baseline Cr of about 1.3 mg/dL, with an eGFRCr of 75 mL/min/1.73 m2.20 In the same month, the patient was prescribed bictegravir/emtricitabine/tenofovir alafenamide, an HIV drug with nephrotoxic potential.21 The patient's total viral load remained low, and CD4 count remained > 500 after initiation of the HIV treatment. He was in his normal state of health and had no known contributory history before his HIV diagnosis. Cr readings peaked at 1.83 mg/dL after starting the HIV treatment and remained elevated to 1.73 mg/dL over the next few months, corresponding to CKD stage 3A. Because bictegravir/emtricitabine/tenofovir alafenamide is cleared by the kidneys and has a nephrotoxic profile, the clinical care team considered dosage adjustment or a medication switch given his observed elevated eGFRCr based on the CKD-EPI 2021 equation for Cr alone. It was also noted that the patient had a similar Cr spike to 1.83 mg/dL in 2018 without any identifiable renal insult or symptoms (Figure).
Diagnostic Evaluation
The primary care team ordered a renal ultrasound and referred the patient to the nephrology clinic. The nephrologist ordered the following laboratory studies: urine microalbumin to Cr ratio, basic metabolic panel (BMP), comprehensive metabolic panel (CMP), urinalysis, urine protein, urine Cr, parathyroid hormone level, hemoglobin A1c, complement component 3/4 panels, antinuclear and antineutrophil cytoplasmic antibodies titers, glomerular basement membrane antibody titer, urine light chains, serum protein electrophoresis, κ/λ ratio, viral hepatitis panel, and rapid plasma reagin testing. Much of this laboratory evaluation served to rule out any secondary causes of kidney disease, including autoimmune disease, monoclonal or polyclonal gammopathies, diabetic nephropathy or glomerulosclerosis, and nephrotic or nephritic syndromes.
All laboratory studies returned within normal limits; no proteinuria was discovered on urinalysis, and no abnormalities were visualized on renal ultrasound. Bictegravir/emtricitabine/tenofovir alafenamide nephrotoxicity was highest among the differential diagnoses due to the timing of Cr elevation coinciding with the initiation of the medications. The patient's CysC level was 0.85 mg/dL with a calculated eGFRCys of 125 mL/min/1.73 m2. The calculated sCR and serum cystatin C (eGFRCr-Cys) using the new 2021 equation and when adjusting for body surface area placed his eGFR at 92 mL/min/1.73 m2.20
The patient’s eGFRCys reassured the care team that the patient’s renal function was not acutely or chronically impacted by bictegravir/emtricitabine/tenofovir alafenamide, resulting in avoidance of unnecessary dosage adjustment or discontinuation of the HIV treatment. The patient reported a chronic habit of protein and creatine supplementation and bodybuilding, which likely further compounded the discrepancy between eGFRCr and eGFRCys and explained his previous elevation in Cr in 2018.
Follow-up
The patient underwent serial monitoring that revealed a stable Cr and unremarkable eGFR, ruling out CKD. There has been no evidence of worsening kidney disease to date, and the patient remained on his initial HIV regimen.
Discussion
This case shows the importance of using CysC as an alternative or confirmatory marker compared with sCr to estimate GFR in patients with high muscle mass and/or high creatine intake, such as many in the US Department of Defense (DoD) and US Department of Veterans Affairs (VA) patient populations. In the presented case, recorded Cr levels climbed from baseline Cr with the initiation of bictegravir/emtricitabine/tenofovir alafenamide. This raised the concern that HIV treatment was leading to the development of kidney damage.22
Diagnosis of kidney disease as opposed to the normal decline of eGFR with age in individuals without intrinsic CKD requires GFR ≥ 60 mL/min/1.73 m2 with kidney damage (proteinuria or radiological abnormalities, etc) or GFR < 135 to 140 mL/min/1.73 m2 minus the patient’s age in years.23 The patient’s Cr peak at 1.83 mg/dL in 2018 led to an inappropriate diagnosis of kidney disease stage 3a based on an eGFRCr (2021 equation) of 52 mL/min/1.73 m2 when not corrected for body surface area.20 However, using the new 2021 equation using both Cr and CysC, the patient’s eGFRCr-Cys was 92 mL/min/1.73 m2 after a correction for body surface area.
The 2009 CKD-EPI recommended the calculation of eGFR based on SCr concentration using age, sex, and race while the 2021 CKD-EPI recommended the exclusion of race.3 Both equations are less accurate in African American patients, individuals taking medications that interfere with Cr secretion and assay, and patients taking creatine supplements, high daily protein intake, or with high muscle mass.7 These settings result in a decreased eGFRCr without corresponding eGFRCys changes. Using SCr and CysC together, the eGFRCr-Cys yields improved concordance to measured GFR across race groups compared to GFR estimation based on Cr alone, which can avoid unnecessary expensive diagnostic workup, inappropriate kidney disease diagnosis, incorrect dosing of drugs, and accurately represent the military readiness of patients. Interestingly, in African American patients with recently diagnosed HIV, CKD-EPI using both Cr and CysC without race inclusion led to only a 2.9% overestimation of GFR and was the only equation with no statistically significant bias compared with measured GFR.24
A March 2023 case involving an otherwise healthy 26-year-old male active-duty US Navy member with a history of excessive protein supplement intake and intense exercise < 24 hours before laboratory work was diagnosed with CKD after a measured Cr of 16 mg/dL and an eGFRCr of 4 mL/min/1.73 m2 without any other evidence of kidney disease. His CysC remained within normal limits, resulting in a normal eGFRCys of 121 mL/min/1.73 m2, indicating no CKD. His Cr and eGFR recovered 10 days after his clinic visit and cessation of his supplement intake. These findings may not be uncommon given that 65% of active-duty military use protein supplements and 38% use other performance-enhancing supplements, such as creatine, according to a study.25
Unfortunately, the BMP/CMP traditionally used at VA centers use the eGFRCr equation, and it is unknown how many primary care practitioners recognize the limitations of these metabolic panels on accurate estimation of kidney function. However, in 2022 an expert panel including VA physicians recommended the immediate use of eGFRCr-Cys or eGFRCys for confirmatory testing and potentially screening of CKD.26 A small number of VAs have since adopted this recommendation, which should lead to fewer misdiagnoses among US military members as clinicians should now have access to more accurate measurements of GFR.
The VA spends about $18 billion (excluding dialysis) for care for 1.1 to 2.5 million VA patients with CKD.27 The majority of these diagnoses were undoubtedly made using the eGFRCr equation, raising the question of how many may be misdiagnosed. Assessment with CysC is currently relatively expensive, but it will likely become more affordable as the use of CysC as a confirmatory test increases.5 The cost of a sCr test is about $2.50, while CysC costs about $10.60, with variation from laboratory to laboratory.28 By comparison, a renal ultrasound costs $99 to $140 for uninsured patients.29 Furthermore, the cost of CysC testing is likely to trend downward as more facilities adopt the use of CysC measurements, which can be run on the same analytical equipment currently used for Cr measurements. Currently, most laboratories do not have established assays to use in-house and thus require CysC to be sent out to a laboratory, which increases result time and makes Cr a more attractive option. As more laboratories adopt assays for CysC, the cost of reagents will further decrease.
Given such considerations, confirmation testing of kidney function with CysC in specific patient populations with decreased eGFRCr without other features of CKD can offer great medical and financial benefits. A 2023 KDIGO report noted that many individuals may be mistakenly diagnosed with CKD when using eGFRCr.3 KDIGO noted that a 2013 meta-analysis of 90,000 individuals found that with a Cr-based eGFR of 45 to 59 mL/min/1.73 m2 (42%) had a CysC-based eGFR of ≥ 60 mL/min/1.73 m2. An eGFRCr of 45 to 59 represents 54% of all patients with CKD, amounting to millions of people (including current and former military personnel).3,29-31 Correcting a misdiagnosis of CKD would bring significant relief to patients and save millions in health care spending.
Conclusions
In patients who meet CKD criteria using eGFRCr but without other features of CKD, we recommend using confirmatory CysC levels and the eGFRCr-Cys equation. This will align care with the KDIGO guidelines and could be a cost-effective step toward improving military patient care. Further work in this area should focus on determining the knowledge gaps in primary care practitioners’ understanding of the limits of eGFRCr, the potential mitigation of concomitant CysC testing in equivocal CKD cases, and the cost-effectiveness and increased utilization of CysC.
1. Gabriel R. Time to scrap creatinine clearance? Br Med J (Clin Res Ed). 1986;293(6555):1119-1120. doi:10.1136/bmj.293.6555.1119
2. Swan SK. The search continues—an ideal marker of GFR. Clin Chem. 1997;43(6):913-914.doi:10.1093/clinchem/43.6.913 3. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1).
4. Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80(3):1107-1213. doi:10.1152/physrev.2000.80.3.1107
5. Ferguson TW, Komenda P, Tangri N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr Opin Nephrol Hypertens. 2015;24(3):295-300. doi:10.1097/mnh.0000000000000115
6. Levey AS, Titan SM, Powe NR, Coresh J, Inker LA. Kidney disease, race, and GFR estimation. Clin J Am Soc Nephrol. 2020;15(8):1203-1212. doi:10.2215/cjn.12791019
7. Shlipak MG, Tummalapalli SL, Boulware LE, et al; Conference Participants. The case for early identification and intervention of chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) controversies conference. Kidney Int. 2021;99(1):34-47. doi:10.1016/j.kint.2020.10.012
8. O’Riordan SE, Webb MC, Stowe HJ, et al. Cystatin C improves the detection of mild renal dysfunction in older patients. Ann Clin Biochem. 2003;40(pt 6):648-655. doi:10.1258/000456303770367243
9. Stevens LA, Schmid CH, Greene T, et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 2009;75(6):652-660. doi:10.1038/ki.2008.638
10. Levey AS, Coresh J, Greene T, et al; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247-254. doi:10.7326/0003-4819-145-4-200608150-00004
11. Levey AS, Stevens LA, Schmid CH, et al; Chronic Kidney Disease Epidemiology Collaboration. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612. doi:10.7326/0003-4819-150-9-200905050-00006
12. Pöge U, Gerhardt T, Stoffel-Wagner B, Klehr HU, Sauerbruch T, Woitas RP. Calculation of glomerular filtration rate based on cystatin C in cirrhotic patients. Nephrol Dial Transplant. 2006;21(3):660-664. doi:10.1093/ndt/gfi305
13. Larsson A, Malm J, Grubb A, Hansson LO. Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand J Clin Lab Invest. 2004;64(1):25-30. doi:10.1080/00365510410003723.
14. Macisaac RJ, Tsalamandris C, Thomas MC, et al. Estimating glomerular filtration rate in diabetes: a comparison of cystatin-C- and creatinine-based methods. Diabetologia. 2006;49(7):1686-1689. doi:10.1007/s00125-006-0275-7
15. Rule AD, Bergstralh EJ, Slezak JM, Bergert J, Larson TS. Glomerular filtration rate estimated by cystatin C among different clinical presentations. Kidney Int. 2006;69(2):399-405. doi:10.1038/sj.ki.5000073
16. Inker LA, Schmid CH, Tighiouart H, et al; Chronic Kidney Disease Epidemiology Collaboration Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20-29. doi:10.1056/NEJMoa1114248
17. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
18. Inker LA, Eneanya ND, Coresh J, et al; Chronic Kidney Disease Epidemiology Collaboration. New creatinine- and cystatin C–Based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737-1749. doi:10.1056/NEJMoa2102953
19. Oterdoom LH, Gansevoort RT, Schouten JP, de Jong PE, Gans ROB, Bakker SJL. Urinary creatinine excretion, an indirect measure of muscle mass, is an independent predictor of cardiovascular disease and mortality in the general population. Atherosclerosis. 2009;207(2):534-540. doi.10.1016/j.atherosclerosis.2009.05.010
20. National Kidney Foundation Inc. eGFR calculator. Accessed October 20, 2023. https://www.kidney.org/professionals/kdoqi/gfr_calculator
21. Ueaphongsukkit T, Gatechompol S, Avihingsanon A, et al. Tenofovir alafenamide nephrotoxicity: a case report and literature review. AIDS Res Ther. 2021;18(1):53. doi:10.1186/s12981-021-00380-w
22. D’Agati V, Appel GB. Renal pathology of human immunodeficiency virus infection. Semin Nephrol. 1998;18(4):406-421.
23. Glassock RJ, Winearls C. Ageing and the glomerular filtration rate: truths and consequences. Trans Am Clin Climatol Assoc. 2009;120:419-428.
24. Seape T, Gounden V, van Deventer HE, Candy GP, George JA. Cystatin C- and creatinine-based equations in the assessment of renal function in HIV-positive patients prior to commencing highly active antiretroviral therapy. Ann Clin Biochem. 2016;53(pt 1):58-66. doi:10.1177/0004563215579695
25. Tobin TW, Thurlow JS, Yuan CM. A healthy active duty soldier with an elevated serum creatinine. Mil Med. 2023;188(3-4):e866-e869. doi:10.1093/milmed/usab163
26. Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Am J Kidney Dis. 2022;79(2):268-288.e1. doi:10.1053/j.ajkd.2021.08.003
27. Saran R, Pearson A, Tilea A, et al; VA-REINS Steering Committee; VA Advisory Board. Burden and cost of caring for us veterans with CKD: initial findings from the VA Renal Information System (VA-REINS). Am J Kidney Dis. 2021;77(3):397-405. doi:10.1053/j.ajkd.2020.07.013
28. Zoler ML. Nephrologists make the case for cystatin C-based eGFR. Accessed October 20, 2023. https://www.medscape.com/viewarticle/951335#vp_2
29. Versaw N. How much does an ultrasound cost? Updated February 2022. Accessed October 20, 2023. https://www.compare.com/health/healthcare-resources/how-much-does-an-ultrasound-cost
30. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165-180. doi:10.1016/S0140-6736(11)60178-5
31. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
1. Gabriel R. Time to scrap creatinine clearance? Br Med J (Clin Res Ed). 1986;293(6555):1119-1120. doi:10.1136/bmj.293.6555.1119
2. Swan SK. The search continues—an ideal marker of GFR. Clin Chem. 1997;43(6):913-914.doi:10.1093/clinchem/43.6.913 3. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1).
4. Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80(3):1107-1213. doi:10.1152/physrev.2000.80.3.1107
5. Ferguson TW, Komenda P, Tangri N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr Opin Nephrol Hypertens. 2015;24(3):295-300. doi:10.1097/mnh.0000000000000115
6. Levey AS, Titan SM, Powe NR, Coresh J, Inker LA. Kidney disease, race, and GFR estimation. Clin J Am Soc Nephrol. 2020;15(8):1203-1212. doi:10.2215/cjn.12791019
7. Shlipak MG, Tummalapalli SL, Boulware LE, et al; Conference Participants. The case for early identification and intervention of chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) controversies conference. Kidney Int. 2021;99(1):34-47. doi:10.1016/j.kint.2020.10.012
8. O’Riordan SE, Webb MC, Stowe HJ, et al. Cystatin C improves the detection of mild renal dysfunction in older patients. Ann Clin Biochem. 2003;40(pt 6):648-655. doi:10.1258/000456303770367243
9. Stevens LA, Schmid CH, Greene T, et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 2009;75(6):652-660. doi:10.1038/ki.2008.638
10. Levey AS, Coresh J, Greene T, et al; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247-254. doi:10.7326/0003-4819-145-4-200608150-00004
11. Levey AS, Stevens LA, Schmid CH, et al; Chronic Kidney Disease Epidemiology Collaboration. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612. doi:10.7326/0003-4819-150-9-200905050-00006
12. Pöge U, Gerhardt T, Stoffel-Wagner B, Klehr HU, Sauerbruch T, Woitas RP. Calculation of glomerular filtration rate based on cystatin C in cirrhotic patients. Nephrol Dial Transplant. 2006;21(3):660-664. doi:10.1093/ndt/gfi305
13. Larsson A, Malm J, Grubb A, Hansson LO. Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand J Clin Lab Invest. 2004;64(1):25-30. doi:10.1080/00365510410003723.
14. Macisaac RJ, Tsalamandris C, Thomas MC, et al. Estimating glomerular filtration rate in diabetes: a comparison of cystatin-C- and creatinine-based methods. Diabetologia. 2006;49(7):1686-1689. doi:10.1007/s00125-006-0275-7
15. Rule AD, Bergstralh EJ, Slezak JM, Bergert J, Larson TS. Glomerular filtration rate estimated by cystatin C among different clinical presentations. Kidney Int. 2006;69(2):399-405. doi:10.1038/sj.ki.5000073
16. Inker LA, Schmid CH, Tighiouart H, et al; Chronic Kidney Disease Epidemiology Collaboration Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20-29. doi:10.1056/NEJMoa1114248
17. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
18. Inker LA, Eneanya ND, Coresh J, et al; Chronic Kidney Disease Epidemiology Collaboration. New creatinine- and cystatin C–Based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737-1749. doi:10.1056/NEJMoa2102953
19. Oterdoom LH, Gansevoort RT, Schouten JP, de Jong PE, Gans ROB, Bakker SJL. Urinary creatinine excretion, an indirect measure of muscle mass, is an independent predictor of cardiovascular disease and mortality in the general population. Atherosclerosis. 2009;207(2):534-540. doi.10.1016/j.atherosclerosis.2009.05.010
20. National Kidney Foundation Inc. eGFR calculator. Accessed October 20, 2023. https://www.kidney.org/professionals/kdoqi/gfr_calculator
21. Ueaphongsukkit T, Gatechompol S, Avihingsanon A, et al. Tenofovir alafenamide nephrotoxicity: a case report and literature review. AIDS Res Ther. 2021;18(1):53. doi:10.1186/s12981-021-00380-w
22. D’Agati V, Appel GB. Renal pathology of human immunodeficiency virus infection. Semin Nephrol. 1998;18(4):406-421.
23. Glassock RJ, Winearls C. Ageing and the glomerular filtration rate: truths and consequences. Trans Am Clin Climatol Assoc. 2009;120:419-428.
24. Seape T, Gounden V, van Deventer HE, Candy GP, George JA. Cystatin C- and creatinine-based equations in the assessment of renal function in HIV-positive patients prior to commencing highly active antiretroviral therapy. Ann Clin Biochem. 2016;53(pt 1):58-66. doi:10.1177/0004563215579695
25. Tobin TW, Thurlow JS, Yuan CM. A healthy active duty soldier with an elevated serum creatinine. Mil Med. 2023;188(3-4):e866-e869. doi:10.1093/milmed/usab163
26. Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Am J Kidney Dis. 2022;79(2):268-288.e1. doi:10.1053/j.ajkd.2021.08.003
27. Saran R, Pearson A, Tilea A, et al; VA-REINS Steering Committee; VA Advisory Board. Burden and cost of caring for us veterans with CKD: initial findings from the VA Renal Information System (VA-REINS). Am J Kidney Dis. 2021;77(3):397-405. doi:10.1053/j.ajkd.2020.07.013
28. Zoler ML. Nephrologists make the case for cystatin C-based eGFR. Accessed October 20, 2023. https://www.medscape.com/viewarticle/951335#vp_2
29. Versaw N. How much does an ultrasound cost? Updated February 2022. Accessed October 20, 2023. https://www.compare.com/health/healthcare-resources/how-much-does-an-ultrasound-cost
30. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165-180. doi:10.1016/S0140-6736(11)60178-5
31. Shlipak MG, Matsushita K, Ärnlöv J, et al; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. doi:10.1056/NEJMoa1214234
Sodium vs Potassium for Lowering Blood Pressure?
A pair of dueling editorials in the journal Hypertension debate whether our focus should be on sodium or its often neglected partner, potassium.
A meta-analysis of 85 trials showed a consistent and linear. It may also depend on where you live and whether your concern is treating individuals or implementing effective food policy.
The Case for Sodium Restriction
Stephen Juraschek, MD, PhD, of the Beth Israel Deaconess Medical Center, Boston, Massachusetts, co-author of one editorial, told me in a zoom interview that he believes his side of the debate clearly has the stronger argument. Of the two cations in question, there has been infinitely more ink spilled about sodium.
Studies such as INTERSALT, the DASH diet, and TOHP may be the most well-known, but there are many, many intervention studies of sodium restriction’s effect on blood pressure. A meta-analysis of 85 trials of showed a consistent and linear relationship between sodium reduction and blood pressure. In contrast, the evidence base for potassium is more limited and less consistent. There are half as many trials with potassium, and its ability to lower blood pressure may depend on how much sodium is present in the diet.
An outlier in the sodium restriction evidence base is the PURE study, which suggested that extreme sodium restriction could increase cardiovascular mortality, but the trial suffered from two potential issues. First, it used a single spot urine specimen to measure sodium rather than the generally accepted more accurate 24-hour urine collection. A reanalysis of the TOHP study using a spot urine rather than a 24-hour urine collection changed the relationship between sodium intake and mortality and possibly explained the U-shaped association observed in PURE. Second, PURE was an observational cohort and was prone to confounding, or in this case, reverse causation. Why did people who consumed very little salt have an increased risk for cardiovascular disease? It is very possible that people with a high risk for cardiovascular disease were told to consume less salt to begin with. Hence B led to A rather than A leading to B.
The debate on sodium restriction has been bitter at times. Opposing camps formed, and people took sides in the “salt wars.” A group of researchers, termed the Jackson 6, met and decided to end the controversy by running a randomized trial in US prisons (having discounted the options of long-term care homes and military bases). They detailed their plan in an editorial in Hypertension. The study never came to fruition for two reasons: the obvious ethical problems of experimenting on prisoners and the revelation of undisclosed salt industry funding.
More recent studies have mercifully been more conventional. The SSaSS study, a randomized controlled trial of a salt substitute, provided the cardiovascular outcomes data that many were waiting for. And CARDIA-SSBP, a cross-over randomized trial recently presented at the American Heart Association meeting, showed that reducing dietary sodium was on par with medication when it came to lowering blood pressure.
For Dr. Juraschek, the evidence is clear: “If you were going to choose one, I would say the weight of the evidence is still really heavily on the sodium side.”
The Case for Potassium Supplementation
The evidence for salt restriction notwithstanding, Swapnil Hiremath, MD, MPH, from the University of Ottawa, Ontario, Canada, argued in his editorial that potassium supplementation has gotten short shrift. Though he admits the studies for potassium supplementation have been smaller and sometimes rely on observational evidence, the evidence is there. In the distal convoluted tubule, the sodium chloride cotransporter (NCC), aka the potassium switch, is turned on by low potassium levels and leads to sodium reabsorption by the kidney even in settings of high sodium intake (Figure). To nonnephrologists, renal physiology may be a black box. But if you quickly brush up on the mechanism of action of thiazide diuretics, the preceding descriptor will make more sense.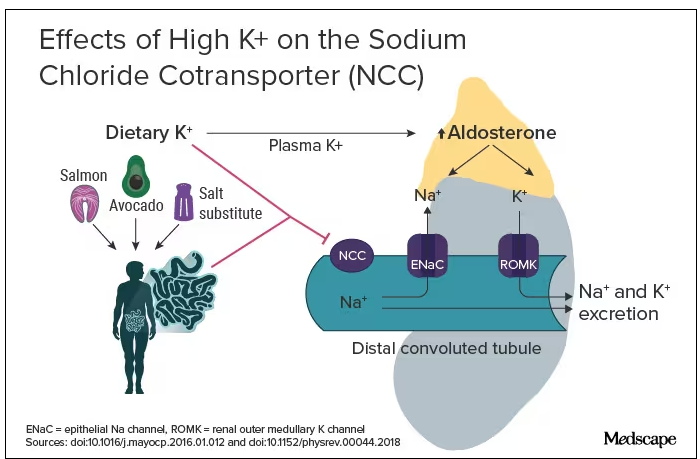
Dr. Hiremath points out that the DASH diet study also got patients to increase their potassium intake by eating more fruits and vegetables. Furthermore, the SSaSS study tested a salt substitute that was 25% potassium (and 75% sodium).
How much blood pressure lowering is due to sodium restriction vs potassium supplementation is a complex question because lowering sodium intake will invariably lead to more potassium intake. “It’s very hard to untangle the relationship,” Dr. Hiremath said in an interview. “It’s sort of synergistic but it’s not completely additive. It’s not as if you add four and four and get eight.” But he maintains there is more evidence regarding the benefit of potassium supplementation than many realize.
Realistic Diets and Taste Issues
“We know that increasing potassium, decreasing sodium is useful. The question is how do we do that?” says Dr. Hiremath. Should we encourage fruit and vegetable consumption in a healthy diet, give potassium supplements, or encourage the use of low-sodium salt substitutes?
Recommending a healthier diet with more fruits and vegetables is a no-brainer. But getting people to do it is hard. In a world where fruit is more expensive than junk food is, economic realities may drive food choice regardless of our best efforts. The 4700 mg of potassium in the DASH eating plan is the equivalent of eleven bananas daily; although not impossible, it would require a substantive shift in eating patterns for most people.
Given that we prescribe iron, vitamin B12, calcium, and vitamin D to patients who need them, why not potassium tablets to help with blood pressure? Granted, there are concerns about inducing hyperkalemia. Also, why not just prescribe a proven anti-hypertensive, such as ramipril, which has the added benefit of helping with renal protection or cardiac remodeling? Dr. Hiremath points out that patients are far less reluctant to take dietary supplements. Medication is something you take when sick. A supplement is seen as “natural” and “healthy” and might be more attractive to people resistant to prescription meds.
Another drawback of oral potassium supplementation is taste. In a Consumer Reports taste test, potassium chloride fared poorly. It was bitter and had a metallic aftertaste. At least one tester wouldn’t ever consume it again. Potassium citrate is slightly more palpable.
Salt substitutes, like the 75:25 ratio of sodium to potassium used in SSaSS, may be as high as you can go for potassium in any low-sodium salt alternative. If you go any higher than that, the taste will just turn people off, suggests Dr. Hiremath.
But SsaSS, which was done in China, may not be relevant to North America. In China, most sodium is added during cooking at home, and the consumption of processed foods is low. For the typical North American, roughly three quarters of the sodium eaten is added to their food by someone else; only about 15% is added during cooking at home or at the dinner table. If you aren’t someone who cooks, buying a salt substitute is probably not going to have much impact.
Given that reality, Dr. Juraschek thinks we need to target the sodium in processed foods. “There’s just so much sodium in so many products,” he says. “When you think about public policy, it’s most expeditious for there to be more regulation about how much is added to our food supply vs trying to get people to consume eight to 12 servings of fruit.”
No Salt War Here
Despite their different editorial takes, Dr. Hiremath and Dr. Juraschek largely agree on the broad strokes of the problem. This isn’t X (or Twitter) after all. Potassium supplementation may be useful in some parts of the world but may not address the underlying problem in countries where processed foods are the source of most dietary sodium.
The CARDIA-SSBP trial showed that a very low–sodium diet had the same blood pressure–lowering effect as a first-line antihypertensive, but most people will not be able to limit themselves to 500 mg of dietary sodium per day. In CARDIA-SSBP, just as in DASH, participants were provided with meals from study kitchens. They were not just told to eat less salt, which would almost certainly have failed.
“We should aim for stuff that is practical and doable rather than aim for stuff that cannot be done,” according to Dr. Hiremath. Whether that should be salt substitutes or policy change may depend on which part of the planet you live on.
One recent positive change may herald the beginning of a policy change, at least in the United States. In March 2023, the US Food and Drug Administration proposed a rule change to allow salt substitutes to be labeled as salt. This would make it easier for food manufacturers to swap out sodium chloride for a low-sodium alternative and reduce the amount of sodium in the US diet without having a large impact on taste and consumer uptake. Both Dr. Hiremath and Dr. Juraschek agree that it may not be enough on its own but that it’s a start.
Christopher Labos is a cardiologist with a degree in epidemiology. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally, he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal, and is host of the award-winning podcast The Body of Evidence.
A version of this article appeared on Medscape.com.
A pair of dueling editorials in the journal Hypertension debate whether our focus should be on sodium or its often neglected partner, potassium.
A meta-analysis of 85 trials showed a consistent and linear. It may also depend on where you live and whether your concern is treating individuals or implementing effective food policy.
The Case for Sodium Restriction
Stephen Juraschek, MD, PhD, of the Beth Israel Deaconess Medical Center, Boston, Massachusetts, co-author of one editorial, told me in a zoom interview that he believes his side of the debate clearly has the stronger argument. Of the two cations in question, there has been infinitely more ink spilled about sodium.
Studies such as INTERSALT, the DASH diet, and TOHP may be the most well-known, but there are many, many intervention studies of sodium restriction’s effect on blood pressure. A meta-analysis of 85 trials of showed a consistent and linear relationship between sodium reduction and blood pressure. In contrast, the evidence base for potassium is more limited and less consistent. There are half as many trials with potassium, and its ability to lower blood pressure may depend on how much sodium is present in the diet.
An outlier in the sodium restriction evidence base is the PURE study, which suggested that extreme sodium restriction could increase cardiovascular mortality, but the trial suffered from two potential issues. First, it used a single spot urine specimen to measure sodium rather than the generally accepted more accurate 24-hour urine collection. A reanalysis of the TOHP study using a spot urine rather than a 24-hour urine collection changed the relationship between sodium intake and mortality and possibly explained the U-shaped association observed in PURE. Second, PURE was an observational cohort and was prone to confounding, or in this case, reverse causation. Why did people who consumed very little salt have an increased risk for cardiovascular disease? It is very possible that people with a high risk for cardiovascular disease were told to consume less salt to begin with. Hence B led to A rather than A leading to B.
The debate on sodium restriction has been bitter at times. Opposing camps formed, and people took sides in the “salt wars.” A group of researchers, termed the Jackson 6, met and decided to end the controversy by running a randomized trial in US prisons (having discounted the options of long-term care homes and military bases). They detailed their plan in an editorial in Hypertension. The study never came to fruition for two reasons: the obvious ethical problems of experimenting on prisoners and the revelation of undisclosed salt industry funding.
More recent studies have mercifully been more conventional. The SSaSS study, a randomized controlled trial of a salt substitute, provided the cardiovascular outcomes data that many were waiting for. And CARDIA-SSBP, a cross-over randomized trial recently presented at the American Heart Association meeting, showed that reducing dietary sodium was on par with medication when it came to lowering blood pressure.
For Dr. Juraschek, the evidence is clear: “If you were going to choose one, I would say the weight of the evidence is still really heavily on the sodium side.”
The Case for Potassium Supplementation
The evidence for salt restriction notwithstanding, Swapnil Hiremath, MD, MPH, from the University of Ottawa, Ontario, Canada, argued in his editorial that potassium supplementation has gotten short shrift. Though he admits the studies for potassium supplementation have been smaller and sometimes rely on observational evidence, the evidence is there. In the distal convoluted tubule, the sodium chloride cotransporter (NCC), aka the potassium switch, is turned on by low potassium levels and leads to sodium reabsorption by the kidney even in settings of high sodium intake (Figure). To nonnephrologists, renal physiology may be a black box. But if you quickly brush up on the mechanism of action of thiazide diuretics, the preceding descriptor will make more sense.
Dr. Hiremath points out that the DASH diet study also got patients to increase their potassium intake by eating more fruits and vegetables. Furthermore, the SSaSS study tested a salt substitute that was 25% potassium (and 75% sodium).
How much blood pressure lowering is due to sodium restriction vs potassium supplementation is a complex question because lowering sodium intake will invariably lead to more potassium intake. “It’s very hard to untangle the relationship,” Dr. Hiremath said in an interview. “It’s sort of synergistic but it’s not completely additive. It’s not as if you add four and four and get eight.” But he maintains there is more evidence regarding the benefit of potassium supplementation than many realize.
Realistic Diets and Taste Issues
“We know that increasing potassium, decreasing sodium is useful. The question is how do we do that?” says Dr. Hiremath. Should we encourage fruit and vegetable consumption in a healthy diet, give potassium supplements, or encourage the use of low-sodium salt substitutes?
Recommending a healthier diet with more fruits and vegetables is a no-brainer. But getting people to do it is hard. In a world where fruit is more expensive than junk food is, economic realities may drive food choice regardless of our best efforts. The 4700 mg of potassium in the DASH eating plan is the equivalent of eleven bananas daily; although not impossible, it would require a substantive shift in eating patterns for most people.
Given that we prescribe iron, vitamin B12, calcium, and vitamin D to patients who need them, why not potassium tablets to help with blood pressure? Granted, there are concerns about inducing hyperkalemia. Also, why not just prescribe a proven anti-hypertensive, such as ramipril, which has the added benefit of helping with renal protection or cardiac remodeling? Dr. Hiremath points out that patients are far less reluctant to take dietary supplements. Medication is something you take when sick. A supplement is seen as “natural” and “healthy” and might be more attractive to people resistant to prescription meds.
Another drawback of oral potassium supplementation is taste. In a Consumer Reports taste test, potassium chloride fared poorly. It was bitter and had a metallic aftertaste. At least one tester wouldn’t ever consume it again. Potassium citrate is slightly more palpable.
Salt substitutes, like the 75:25 ratio of sodium to potassium used in SSaSS, may be as high as you can go for potassium in any low-sodium salt alternative. If you go any higher than that, the taste will just turn people off, suggests Dr. Hiremath.
But SsaSS, which was done in China, may not be relevant to North America. In China, most sodium is added during cooking at home, and the consumption of processed foods is low. For the typical North American, roughly three quarters of the sodium eaten is added to their food by someone else; only about 15% is added during cooking at home or at the dinner table. If you aren’t someone who cooks, buying a salt substitute is probably not going to have much impact.
Given that reality, Dr. Juraschek thinks we need to target the sodium in processed foods. “There’s just so much sodium in so many products,” he says. “When you think about public policy, it’s most expeditious for there to be more regulation about how much is added to our food supply vs trying to get people to consume eight to 12 servings of fruit.”
No Salt War Here
Despite their different editorial takes, Dr. Hiremath and Dr. Juraschek largely agree on the broad strokes of the problem. This isn’t X (or Twitter) after all. Potassium supplementation may be useful in some parts of the world but may not address the underlying problem in countries where processed foods are the source of most dietary sodium.
The CARDIA-SSBP trial showed that a very low–sodium diet had the same blood pressure–lowering effect as a first-line antihypertensive, but most people will not be able to limit themselves to 500 mg of dietary sodium per day. In CARDIA-SSBP, just as in DASH, participants were provided with meals from study kitchens. They were not just told to eat less salt, which would almost certainly have failed.
“We should aim for stuff that is practical and doable rather than aim for stuff that cannot be done,” according to Dr. Hiremath. Whether that should be salt substitutes or policy change may depend on which part of the planet you live on.
One recent positive change may herald the beginning of a policy change, at least in the United States. In March 2023, the US Food and Drug Administration proposed a rule change to allow salt substitutes to be labeled as salt. This would make it easier for food manufacturers to swap out sodium chloride for a low-sodium alternative and reduce the amount of sodium in the US diet without having a large impact on taste and consumer uptake. Both Dr. Hiremath and Dr. Juraschek agree that it may not be enough on its own but that it’s a start.
Christopher Labos is a cardiologist with a degree in epidemiology. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally, he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal, and is host of the award-winning podcast The Body of Evidence.
A version of this article appeared on Medscape.com.
A pair of dueling editorials in the journal Hypertension debate whether our focus should be on sodium or its often neglected partner, potassium.
A meta-analysis of 85 trials showed a consistent and linear. It may also depend on where you live and whether your concern is treating individuals or implementing effective food policy.
The Case for Sodium Restriction
Stephen Juraschek, MD, PhD, of the Beth Israel Deaconess Medical Center, Boston, Massachusetts, co-author of one editorial, told me in a zoom interview that he believes his side of the debate clearly has the stronger argument. Of the two cations in question, there has been infinitely more ink spilled about sodium.
Studies such as INTERSALT, the DASH diet, and TOHP may be the most well-known, but there are many, many intervention studies of sodium restriction’s effect on blood pressure. A meta-analysis of 85 trials of showed a consistent and linear relationship between sodium reduction and blood pressure. In contrast, the evidence base for potassium is more limited and less consistent. There are half as many trials with potassium, and its ability to lower blood pressure may depend on how much sodium is present in the diet.
An outlier in the sodium restriction evidence base is the PURE study, which suggested that extreme sodium restriction could increase cardiovascular mortality, but the trial suffered from two potential issues. First, it used a single spot urine specimen to measure sodium rather than the generally accepted more accurate 24-hour urine collection. A reanalysis of the TOHP study using a spot urine rather than a 24-hour urine collection changed the relationship between sodium intake and mortality and possibly explained the U-shaped association observed in PURE. Second, PURE was an observational cohort and was prone to confounding, or in this case, reverse causation. Why did people who consumed very little salt have an increased risk for cardiovascular disease? It is very possible that people with a high risk for cardiovascular disease were told to consume less salt to begin with. Hence B led to A rather than A leading to B.
The debate on sodium restriction has been bitter at times. Opposing camps formed, and people took sides in the “salt wars.” A group of researchers, termed the Jackson 6, met and decided to end the controversy by running a randomized trial in US prisons (having discounted the options of long-term care homes and military bases). They detailed their plan in an editorial in Hypertension. The study never came to fruition for two reasons: the obvious ethical problems of experimenting on prisoners and the revelation of undisclosed salt industry funding.
More recent studies have mercifully been more conventional. The SSaSS study, a randomized controlled trial of a salt substitute, provided the cardiovascular outcomes data that many were waiting for. And CARDIA-SSBP, a cross-over randomized trial recently presented at the American Heart Association meeting, showed that reducing dietary sodium was on par with medication when it came to lowering blood pressure.
For Dr. Juraschek, the evidence is clear: “If you were going to choose one, I would say the weight of the evidence is still really heavily on the sodium side.”
The Case for Potassium Supplementation
The evidence for salt restriction notwithstanding, Swapnil Hiremath, MD, MPH, from the University of Ottawa, Ontario, Canada, argued in his editorial that potassium supplementation has gotten short shrift. Though he admits the studies for potassium supplementation have been smaller and sometimes rely on observational evidence, the evidence is there. In the distal convoluted tubule, the sodium chloride cotransporter (NCC), aka the potassium switch, is turned on by low potassium levels and leads to sodium reabsorption by the kidney even in settings of high sodium intake (Figure). To nonnephrologists, renal physiology may be a black box. But if you quickly brush up on the mechanism of action of thiazide diuretics, the preceding descriptor will make more sense.
Dr. Hiremath points out that the DASH diet study also got patients to increase their potassium intake by eating more fruits and vegetables. Furthermore, the SSaSS study tested a salt substitute that was 25% potassium (and 75% sodium).
How much blood pressure lowering is due to sodium restriction vs potassium supplementation is a complex question because lowering sodium intake will invariably lead to more potassium intake. “It’s very hard to untangle the relationship,” Dr. Hiremath said in an interview. “It’s sort of synergistic but it’s not completely additive. It’s not as if you add four and four and get eight.” But he maintains there is more evidence regarding the benefit of potassium supplementation than many realize.
Realistic Diets and Taste Issues
“We know that increasing potassium, decreasing sodium is useful. The question is how do we do that?” says Dr. Hiremath. Should we encourage fruit and vegetable consumption in a healthy diet, give potassium supplements, or encourage the use of low-sodium salt substitutes?
Recommending a healthier diet with more fruits and vegetables is a no-brainer. But getting people to do it is hard. In a world where fruit is more expensive than junk food is, economic realities may drive food choice regardless of our best efforts. The 4700 mg of potassium in the DASH eating plan is the equivalent of eleven bananas daily; although not impossible, it would require a substantive shift in eating patterns for most people.
Given that we prescribe iron, vitamin B12, calcium, and vitamin D to patients who need them, why not potassium tablets to help with blood pressure? Granted, there are concerns about inducing hyperkalemia. Also, why not just prescribe a proven anti-hypertensive, such as ramipril, which has the added benefit of helping with renal protection or cardiac remodeling? Dr. Hiremath points out that patients are far less reluctant to take dietary supplements. Medication is something you take when sick. A supplement is seen as “natural” and “healthy” and might be more attractive to people resistant to prescription meds.
Another drawback of oral potassium supplementation is taste. In a Consumer Reports taste test, potassium chloride fared poorly. It was bitter and had a metallic aftertaste. At least one tester wouldn’t ever consume it again. Potassium citrate is slightly more palpable.
Salt substitutes, like the 75:25 ratio of sodium to potassium used in SSaSS, may be as high as you can go for potassium in any low-sodium salt alternative. If you go any higher than that, the taste will just turn people off, suggests Dr. Hiremath.
But SsaSS, which was done in China, may not be relevant to North America. In China, most sodium is added during cooking at home, and the consumption of processed foods is low. For the typical North American, roughly three quarters of the sodium eaten is added to their food by someone else; only about 15% is added during cooking at home or at the dinner table. If you aren’t someone who cooks, buying a salt substitute is probably not going to have much impact.
Given that reality, Dr. Juraschek thinks we need to target the sodium in processed foods. “There’s just so much sodium in so many products,” he says. “When you think about public policy, it’s most expeditious for there to be more regulation about how much is added to our food supply vs trying to get people to consume eight to 12 servings of fruit.”
No Salt War Here
Despite their different editorial takes, Dr. Hiremath and Dr. Juraschek largely agree on the broad strokes of the problem. This isn’t X (or Twitter) after all. Potassium supplementation may be useful in some parts of the world but may not address the underlying problem in countries where processed foods are the source of most dietary sodium.
The CARDIA-SSBP trial showed that a very low–sodium diet had the same blood pressure–lowering effect as a first-line antihypertensive, but most people will not be able to limit themselves to 500 mg of dietary sodium per day. In CARDIA-SSBP, just as in DASH, participants were provided with meals from study kitchens. They were not just told to eat less salt, which would almost certainly have failed.
“We should aim for stuff that is practical and doable rather than aim for stuff that cannot be done,” according to Dr. Hiremath. Whether that should be salt substitutes or policy change may depend on which part of the planet you live on.
One recent positive change may herald the beginning of a policy change, at least in the United States. In March 2023, the US Food and Drug Administration proposed a rule change to allow salt substitutes to be labeled as salt. This would make it easier for food manufacturers to swap out sodium chloride for a low-sodium alternative and reduce the amount of sodium in the US diet without having a large impact on taste and consumer uptake. Both Dr. Hiremath and Dr. Juraschek agree that it may not be enough on its own but that it’s a start.
Christopher Labos is a cardiologist with a degree in epidemiology. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally, he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal, and is host of the award-winning podcast The Body of Evidence.
A version of this article appeared on Medscape.com.
Insulin Resistance Doesn’t Affect Finerenone’s Efficacy
TOPLINE:
In patients with chronic kidney disease (CKD) and type 2 diabetes, baseline insulin resistance was associated with increased cardiovascular (CV) but not kidney risk and did not affect the efficacy of finerenone.
METHODOLOGY:
- Insulin resistance is implicated in CV disease in patients with CKD, but its role in CKD progression is less clear.
- This post hoc analysis of FIDELITY, a pooled analysis of the and trials, randomly assigned patients with type 2 diabetes and CKD (who received optimized renin-angiotensin system blockade) to receive finerenone (10 mg or 20 mg) once daily or placebo and followed them for a median of 3 years.
- An estimated glucose disposal rate (eGDR), a measure of insulin resistance, was calculated for 12,964 patients (median age, 65 years), using waist circumference, hypertension status, and glycated hemoglobin.
- Outcomes included a CV composite (time to CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and a kidney composite (time to renal failure, a sustained decrease ≥ 57% in the initial estimated glomerular filtration rate, or renal death).
TAKEAWAY:
- The median eGDR was 4.1 mg/kg/min. The 50% of patients with a lower eGDR were considered insulin resistant, whereas the remaining half with a higher eGDR were considered insulin sensitive.
- The incidence rate of CV outcomes was higher among patients with insulin resistance in both the finerenone group (incidence rate per 100 patient-years, 5.18 vs 3.47 among insulin-sensitive patients) and the placebo group (6.34 vs 3.76), but eGDR showed no association with kidney outcomes.
- The efficacy of finerenone vs placebo on CV (Wald test P = .063) and kidney outcomes (Wald test P = .51) did not change significantly across the range of baseline eGDR values.
- The incidences of treatment-emergent adverse events and severe adverse events with finerenone were similar between the insulin-resistant and insulin-sensitive subgroups.
IN PRACTICE:
“The efficacy and safety of finerenone were not modified by baseline insulin resistance. A higher risk of CV — but not kidney outcomes was observed in patients with CKD and T2D with greater insulin resistance,” the authors wrote.
SOURCE:
This study was led by Thomas Ebert of the Medical Department III — Endocrinology, Nephrology, Rheumatology, University of Leipzig Medical Center, Leipzig, Germany, and published online in Diabetes Care.
LIMITATIONS:
This study was not adequately powered to evaluate the statistical significance of the association of eGDR with CV and kidney outcomes and was hypothesis-generating. Further studies are needed to examine whether the effects of insulin resistance differ between individuals with diabetes vs those with advanced CKD with or without diabetes.
DISCLOSURES:
The FIDELIO-DKD and FIGARO-DKD trials were conducted and sponsored by Bayer AG. Three authors declared being full-time employees of Bayer. Several authors declared receiving personal fees, consulting fees, grants, or research support from; holding patents with; or having ownership interests in various pharmaceutical companies, including Bayer.
A version of this article appeared on Medscape.com.
TOPLINE:
In patients with chronic kidney disease (CKD) and type 2 diabetes, baseline insulin resistance was associated with increased cardiovascular (CV) but not kidney risk and did not affect the efficacy of finerenone.
METHODOLOGY:
- Insulin resistance is implicated in CV disease in patients with CKD, but its role in CKD progression is less clear.
- This post hoc analysis of FIDELITY, a pooled analysis of the and trials, randomly assigned patients with type 2 diabetes and CKD (who received optimized renin-angiotensin system blockade) to receive finerenone (10 mg or 20 mg) once daily or placebo and followed them for a median of 3 years.
- An estimated glucose disposal rate (eGDR), a measure of insulin resistance, was calculated for 12,964 patients (median age, 65 years), using waist circumference, hypertension status, and glycated hemoglobin.
- Outcomes included a CV composite (time to CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and a kidney composite (time to renal failure, a sustained decrease ≥ 57% in the initial estimated glomerular filtration rate, or renal death).
TAKEAWAY:
- The median eGDR was 4.1 mg/kg/min. The 50% of patients with a lower eGDR were considered insulin resistant, whereas the remaining half with a higher eGDR were considered insulin sensitive.
- The incidence rate of CV outcomes was higher among patients with insulin resistance in both the finerenone group (incidence rate per 100 patient-years, 5.18 vs 3.47 among insulin-sensitive patients) and the placebo group (6.34 vs 3.76), but eGDR showed no association with kidney outcomes.
- The efficacy of finerenone vs placebo on CV (Wald test P = .063) and kidney outcomes (Wald test P = .51) did not change significantly across the range of baseline eGDR values.
- The incidences of treatment-emergent adverse events and severe adverse events with finerenone were similar between the insulin-resistant and insulin-sensitive subgroups.
IN PRACTICE:
“The efficacy and safety of finerenone were not modified by baseline insulin resistance. A higher risk of CV — but not kidney outcomes was observed in patients with CKD and T2D with greater insulin resistance,” the authors wrote.
SOURCE:
This study was led by Thomas Ebert of the Medical Department III — Endocrinology, Nephrology, Rheumatology, University of Leipzig Medical Center, Leipzig, Germany, and published online in Diabetes Care.
LIMITATIONS:
This study was not adequately powered to evaluate the statistical significance of the association of eGDR with CV and kidney outcomes and was hypothesis-generating. Further studies are needed to examine whether the effects of insulin resistance differ between individuals with diabetes vs those with advanced CKD with or without diabetes.
DISCLOSURES:
The FIDELIO-DKD and FIGARO-DKD trials were conducted and sponsored by Bayer AG. Three authors declared being full-time employees of Bayer. Several authors declared receiving personal fees, consulting fees, grants, or research support from; holding patents with; or having ownership interests in various pharmaceutical companies, including Bayer.
A version of this article appeared on Medscape.com.
TOPLINE:
In patients with chronic kidney disease (CKD) and type 2 diabetes, baseline insulin resistance was associated with increased cardiovascular (CV) but not kidney risk and did not affect the efficacy of finerenone.
METHODOLOGY:
- Insulin resistance is implicated in CV disease in patients with CKD, but its role in CKD progression is less clear.
- This post hoc analysis of FIDELITY, a pooled analysis of the and trials, randomly assigned patients with type 2 diabetes and CKD (who received optimized renin-angiotensin system blockade) to receive finerenone (10 mg or 20 mg) once daily or placebo and followed them for a median of 3 years.
- An estimated glucose disposal rate (eGDR), a measure of insulin resistance, was calculated for 12,964 patients (median age, 65 years), using waist circumference, hypertension status, and glycated hemoglobin.
- Outcomes included a CV composite (time to CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and a kidney composite (time to renal failure, a sustained decrease ≥ 57% in the initial estimated glomerular filtration rate, or renal death).
TAKEAWAY:
- The median eGDR was 4.1 mg/kg/min. The 50% of patients with a lower eGDR were considered insulin resistant, whereas the remaining half with a higher eGDR were considered insulin sensitive.
- The incidence rate of CV outcomes was higher among patients with insulin resistance in both the finerenone group (incidence rate per 100 patient-years, 5.18 vs 3.47 among insulin-sensitive patients) and the placebo group (6.34 vs 3.76), but eGDR showed no association with kidney outcomes.
- The efficacy of finerenone vs placebo on CV (Wald test P = .063) and kidney outcomes (Wald test P = .51) did not change significantly across the range of baseline eGDR values.
- The incidences of treatment-emergent adverse events and severe adverse events with finerenone were similar between the insulin-resistant and insulin-sensitive subgroups.
IN PRACTICE:
“The efficacy and safety of finerenone were not modified by baseline insulin resistance. A higher risk of CV — but not kidney outcomes was observed in patients with CKD and T2D with greater insulin resistance,” the authors wrote.
SOURCE:
This study was led by Thomas Ebert of the Medical Department III — Endocrinology, Nephrology, Rheumatology, University of Leipzig Medical Center, Leipzig, Germany, and published online in Diabetes Care.
LIMITATIONS:
This study was not adequately powered to evaluate the statistical significance of the association of eGDR with CV and kidney outcomes and was hypothesis-generating. Further studies are needed to examine whether the effects of insulin resistance differ between individuals with diabetes vs those with advanced CKD with or without diabetes.
DISCLOSURES:
The FIDELIO-DKD and FIGARO-DKD trials were conducted and sponsored by Bayer AG. Three authors declared being full-time employees of Bayer. Several authors declared receiving personal fees, consulting fees, grants, or research support from; holding patents with; or having ownership interests in various pharmaceutical companies, including Bayer.
A version of this article appeared on Medscape.com.
High Salt Intake Linked to Increased Risk for Kidney Disease
People who habitually add salt to their meals at the table may unknowingly be risking their kidneys, according to a study utilizing UK Biobank data. Chronic salt additions are associated with an elevated risk of developing chronic kidney disease (CKD), as revealed by researchers led by Rui Tang, a doctoral candidate in epidemiology at Tulane University in New Orleans, Louisiana. The study was published in JAMA Network Open.
Large Study Sample
In a population-based cohort study comprising over 460,000 UK Biobank participants aged 37-73 years, the researchers explored the association between adding table salt to food and increased CKD risk.
Participants indicated how often they added salt to their meals: Never or rarely, sometimes, often, or always. The follow-up period exceeded a decade, and median duration was 11.8 years. During this time, approximately 22,000 new CKD cases were documented. Data analysis revealed a significantly higher CKD risk among those who frequently added salt.
The extent of risk elevation varied with the frequency of salt additions. Even occasional salters had a 7% higher risk than those who never or rarely added salt. For frequent salters, the risk increased by 12%, and for those who always added salt, it rose to 29%. These results were adjusted for age and gender.
Worse Overall Health
The research group noted that individuals who frequently added salt were generally less healthy, adopting an unhealthier lifestyle and having lower socioeconomic status. They exhibited higher body mass index (BMI), were more likely to smoke, had diabetes or cardiovascular diseases, and had reduced estimated glomerular filtration rate (eGFR) at the beginning of the study. Moreover, their Townsend Deprivation Index, indicating material deprivation, was higher.
Considering these factors, the researchers adjusted the results not only for age and gender but also for ethnicity, Townsend Deprivation Index, eGFR, BMI, smoking status, alcohol consumption, physical activity, elevated cholesterol levels, diabetes, cardiovascular diseases, hypertension, infectious diseases, immune system disorders, and the use of nephrotoxic medications.
Association Persists
Even after accounting for these factors, a significant, albeit attenuated, association between salt additions and CKD risk remained. The risk increased by 2% for occasional salters, 5% for frequent salters, and 6% for those who always added salt.
The research group concluded that adding salt to meals could be associated with an increased risk for CKD in the general population. However, they highlighted several limitations that should be considered when interpreting the study results.
Reducing Salt
Primarily, self-reported frequency of salt addition doesn’t precisely reflect actual salt consumption. While earlier studies validated the accuracy of this variable, the researchers acknowledged the possibility that frequent salt addition may merely be a marker for an unhealthy lifestyle.
Nevertheless, the authors speculated that reducing the frequency of salt additions to meals could contribute to lowering CKD risk in the general population. They suggested validating their results in post hoc analyses or follow-up studies from clinical trials.
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
People who habitually add salt to their meals at the table may unknowingly be risking their kidneys, according to a study utilizing UK Biobank data. Chronic salt additions are associated with an elevated risk of developing chronic kidney disease (CKD), as revealed by researchers led by Rui Tang, a doctoral candidate in epidemiology at Tulane University in New Orleans, Louisiana. The study was published in JAMA Network Open.
Large Study Sample
In a population-based cohort study comprising over 460,000 UK Biobank participants aged 37-73 years, the researchers explored the association between adding table salt to food and increased CKD risk.
Participants indicated how often they added salt to their meals: Never or rarely, sometimes, often, or always. The follow-up period exceeded a decade, and median duration was 11.8 years. During this time, approximately 22,000 new CKD cases were documented. Data analysis revealed a significantly higher CKD risk among those who frequently added salt.
The extent of risk elevation varied with the frequency of salt additions. Even occasional salters had a 7% higher risk than those who never or rarely added salt. For frequent salters, the risk increased by 12%, and for those who always added salt, it rose to 29%. These results were adjusted for age and gender.
Worse Overall Health
The research group noted that individuals who frequently added salt were generally less healthy, adopting an unhealthier lifestyle and having lower socioeconomic status. They exhibited higher body mass index (BMI), were more likely to smoke, had diabetes or cardiovascular diseases, and had reduced estimated glomerular filtration rate (eGFR) at the beginning of the study. Moreover, their Townsend Deprivation Index, indicating material deprivation, was higher.
Considering these factors, the researchers adjusted the results not only for age and gender but also for ethnicity, Townsend Deprivation Index, eGFR, BMI, smoking status, alcohol consumption, physical activity, elevated cholesterol levels, diabetes, cardiovascular diseases, hypertension, infectious diseases, immune system disorders, and the use of nephrotoxic medications.
Association Persists
Even after accounting for these factors, a significant, albeit attenuated, association between salt additions and CKD risk remained. The risk increased by 2% for occasional salters, 5% for frequent salters, and 6% for those who always added salt.
The research group concluded that adding salt to meals could be associated with an increased risk for CKD in the general population. However, they highlighted several limitations that should be considered when interpreting the study results.
Reducing Salt
Primarily, self-reported frequency of salt addition doesn’t precisely reflect actual salt consumption. While earlier studies validated the accuracy of this variable, the researchers acknowledged the possibility that frequent salt addition may merely be a marker for an unhealthy lifestyle.
Nevertheless, the authors speculated that reducing the frequency of salt additions to meals could contribute to lowering CKD risk in the general population. They suggested validating their results in post hoc analyses or follow-up studies from clinical trials.
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
People who habitually add salt to their meals at the table may unknowingly be risking their kidneys, according to a study utilizing UK Biobank data. Chronic salt additions are associated with an elevated risk of developing chronic kidney disease (CKD), as revealed by researchers led by Rui Tang, a doctoral candidate in epidemiology at Tulane University in New Orleans, Louisiana. The study was published in JAMA Network Open.
Large Study Sample
In a population-based cohort study comprising over 460,000 UK Biobank participants aged 37-73 years, the researchers explored the association between adding table salt to food and increased CKD risk.
Participants indicated how often they added salt to their meals: Never or rarely, sometimes, often, or always. The follow-up period exceeded a decade, and median duration was 11.8 years. During this time, approximately 22,000 new CKD cases were documented. Data analysis revealed a significantly higher CKD risk among those who frequently added salt.
The extent of risk elevation varied with the frequency of salt additions. Even occasional salters had a 7% higher risk than those who never or rarely added salt. For frequent salters, the risk increased by 12%, and for those who always added salt, it rose to 29%. These results were adjusted for age and gender.
Worse Overall Health
The research group noted that individuals who frequently added salt were generally less healthy, adopting an unhealthier lifestyle and having lower socioeconomic status. They exhibited higher body mass index (BMI), were more likely to smoke, had diabetes or cardiovascular diseases, and had reduced estimated glomerular filtration rate (eGFR) at the beginning of the study. Moreover, their Townsend Deprivation Index, indicating material deprivation, was higher.
Considering these factors, the researchers adjusted the results not only for age and gender but also for ethnicity, Townsend Deprivation Index, eGFR, BMI, smoking status, alcohol consumption, physical activity, elevated cholesterol levels, diabetes, cardiovascular diseases, hypertension, infectious diseases, immune system disorders, and the use of nephrotoxic medications.
Association Persists
Even after accounting for these factors, a significant, albeit attenuated, association between salt additions and CKD risk remained. The risk increased by 2% for occasional salters, 5% for frequent salters, and 6% for those who always added salt.
The research group concluded that adding salt to meals could be associated with an increased risk for CKD in the general population. However, they highlighted several limitations that should be considered when interpreting the study results.
Reducing Salt
Primarily, self-reported frequency of salt addition doesn’t precisely reflect actual salt consumption. While earlier studies validated the accuracy of this variable, the researchers acknowledged the possibility that frequent salt addition may merely be a marker for an unhealthy lifestyle.
Nevertheless, the authors speculated that reducing the frequency of salt additions to meals could contribute to lowering CKD risk in the general population. They suggested validating their results in post hoc analyses or follow-up studies from clinical trials.
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
Hypocalcemia Risk Warning Added to Osteoporosis Drug
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
EHR Tool Enhances Primary Aldosteronism Screening in Hypertensive Patients
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Primary aldosteronism (PA) is a frequently overlooked yet common cause of secondary hypertension, presenting significant risk for cardiovascular morbidity and mortality.
But fewer than 4% of at-risk patients receive the recommended screening for PA, leaving a substantial gap in early detection and management, according to Adina F. Turcu, MD, MS, associate professor in endocrinology and internal medicine at University of Michigan Health in Ann Arbor.
In response to this clinical challenge, Dr. Turcu and her colleagues developed a best-practice advisory (BPA) to identify patients who were at risk for PA and embedded it into electronic health record at University of Michigan ambulatory clinics. Her team found that use of the tool led to increased rates of screening for PA, particularly among primary care physicians.
Over a 15-month period, Dr. Turcu and her colleagues tested the BPA through a quality improvement study, identifying 14,603 unique candidates for PA screening, with a mean age of 65.5 years and a diverse representation of ethnic backgrounds.
Notably, 48.1% of these candidates had treatment-resistant hypertension, 43.5% exhibited hypokalemia, 10.5% were younger than 35 years, and 3.1% had adrenal nodules. Of these candidates, 14.0% received orders for PA screening, with 70.5% completing the recommended screening within the system, and 17.4% receiving positive screening results.
The study, conducted over 6 months in 2023, targeted adults with hypertension and at least one of the following: Those who took four or more antihypertensive medications, exhibited hypokalemia, were younger than age 35 years, or had adrenal nodules. Patients previously tested for PA were excluded from the analysis.
The noninterruptive BPA was triggered during outpatient visits with clinicians who specialized in hypertension. The advisory would then offer an order set for PA screening and provide a link to interpretation guidance for results. Clinicians had the option to use, ignore, or decline the BPA.
“Although we were hoping for broader uptake of this EHR-embedded BPA, we were delighted to see an increase in PA screening rates to 14% of identified candidates as compared to an average of less than 3% in retrospective studies of similar populations, including in our own institution prior to implementing this BPA,” Dr. Turcu told this news organization.
Physician specialty played a crucial role in the utilization of the BPA. Internists and family medicine physicians accounted for the majority of screening orders, placing 40.0% and 28.1% of these, respectively. Family practitioners and internists predominantly used the embedded order set (80.3% and 68.9%, respectively).
“Hypertension often gets treated rather than screening for [causes of] secondary hypertension prior to treatment,” said Kaniksha Desai, MD, clinical associate professor and endocrinology quality director at Stanford University School of Medicine, Stanford, California, who was not involved in the research. But “primary hyperaldosteronism is a condition that can be treated surgically and has increased long term cardiovascular consequences if not identified. While guidelines recommend screening at-risk patients, this often can get lost in translation in clinical practice due to many factors, including time constraints and volume of patients.”
Patients who did vs did not undergo screening were more likely to be women, Black, and younger than age 35 years. Additionally, the likelihood of screening was higher among patients with obesity and dyslipidemia, whereas it was lower in those with chronic kidney disease and established cardiovascular complications.
According to Dr. Turcu, the findings from this study suggest that noninterruptive BPAs, especially when integrated into primary care workflows, hold promise as effective tools for PA screening.
When coupled with artificial intelligence to optimize detection yield, these refined BPAs could significantly contribute to personalized care for hypertension, the investigators said.
“Considering that in the United States almost one in two adults has hypertension, such automatized tools become instrumental to busy clinicians, particularly those in primary care,” Dr. Turcu said. “Our results indicate a promising opportunity to meaningfully improve PA awareness and enhance its diagnosis.”
Dr. Turcu reported receiving grants from the National Heart, Lung, and Blood Institute and Doris Duke Foundation, served as an investigator in a CinCor Pharma clinical trial, and received financial support to her institution during the conduct of the study. Dr. Desai reported no relevant financial disclosures.
A version of this article appeared on Medscape.com.
Why Is Kidney Disease So Often Missed?
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.