User login
Beware of the latest TikTok trend: Nasal spray tans
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
DSM-5 update: What’s new?
Ahead of its official release on March 18, the new Diagnostic and Statistical Manual of Mental Disorders, which is in the form of a textbook, is already drawing some criticism.
It also includes symptom codes for suicidal behavior and nonsuicidal self-injury, clarifying modifications to criteria sets for more than 70 disorders, including autism spectrum disorder; changes in terminology for gender dysphoria; and a comprehensive review of the impact of racism and discrimination on the diagnosis and manifestations of mental disorders.
The Text Revision is a compilation of iterative changes that have been made online on a rolling basis since the DSM-5 was first published in 2013.
“The goal of the Text Revision was to allow a thorough revision of the text, not the criteria,” Paul Appelbaum, MD, chair of the APA’s DSM steering committee, told this news organization.

For the Text Revision, some 200 experts across a variety of APA working groups recommended changes to the text based on a comprehensive literature review, said Appelbaum, who is the Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law, and director of the division of law, ethics and psychiatry at Columbia University, New York.
However, there’s not a lot that’s new, in part, because there have been few therapeutic advances.
Money maker?
Allen Frances, MD, chair of the DSM-4 task force and professor and chair emeritus of psychiatry at Duke University, Durham, N.C., said the APA is publishing the Text Revision “just to make money. They’re very anxious to do anything that will increase sales and having a revision forces some people, especially in institutions, to buy the book, even though it may not have anything substantive to add to the original.”

Dr. Frances told this news organization that when the APA published the first DSM in the late 1970s, “it became an instantaneous best-seller, to everyone’s surprise.”
The APA would not comment on how many of the $170 (list price) volumes it sells or how much those sales contribute to its budget.
Dr. Appelbaum acknowledged, “at any point in time, the canonical version is the online version.” However, it’s clear from DSM-5 sales “that many people still value having a hard copy of the DSM available to them.”
Prolonged grief: Timely or overkill?
Persistent complex bereavement disorder (PCBD) was listed as a “condition for further study” in DSM-5. After a 2019 workshop aimed at getting consensus for diagnosis criteria, the APA board approved the new prolonged grief disorder in October 2020, and the APA assembly approved the new disorder in November 2020.
Given the 950,000 deaths from COVID-19 over the past 2 years, inclusion of prolonged grief disorder in the DSM-5 may arrive at just the right time.
The diagnostic criteria for PCBD include:
- The development of a persistent grief response (longer than a year for adults and 6 months for children and adolescents) characterized by one or both of the following symptoms, which have been present most days to a clinically significant degree, and have occurred nearly every day for at least the last month: intense yearning/longing for the deceased person; preoccupation with thoughts or memories of the deceased person.
- Since the death, at least three symptoms present most days to a clinically significant degree, and occurring nearly every day for at least the last month, including identity disruption, marked sense of disbelief about the death, avoidance of reminders that the person is dead, intense emotional pain related to the death, difficulty reintegrating into one’s relationships and activities after the death, emotional numbness, feeling that life is meaningless as a result of the death, and intense loneliness as a result of the death.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The duration and severity of the bereavement reaction clearly exceed expected social, cultural, or religious norms for the individual’s culture and context.
- The symptoms are not better explained by another mental disorder, such as major depressive disorder (MDD) or PTSD, and are not attributable to the physiological effects of a substance or another medical condition.
Dr. Frances said he believes creating a new diagnosis pathologizes grief. In DSM-3 and DSM-4, an exception was made under the diagnosis of MDD for individuals who had recently lost a loved one. “We wanted to have at least an opportunity for people to grieve without being stigmatized, mislabeled, and overtreated with medication.”
DSM-5 removed the bereavement exclusion. After 2 weeks, people who are grieving and have particular symptoms could receive a diagnosis of MDD, said Dr. Frances. He believes the exclusion should have been broadened to cover anyone experiencing a major loss – such as a job loss or divorce. If someone is having prolonged symptoms that interfere with functioning, they should get an MDD diagnosis.
The new disorder “doesn’t solve anything, it just adds to the confusion and stigmatization, and it’s part of a kind of creeping medical imperialization of everyday life, where everything has to have a mental disorder label,” Dr. Frances said.
However, Dr. Appelbaum countered that “the criteria for prolonged grief disorder are constructed in such a way as to make every effort to exclude people who are going through a normal grieving process.”
“Part of the purpose of the data analyses was to ensure the criteria that were adopted would, in fact, effectively distinguish between what anybody goes through, say when someone close to you dies, and this unusual prolonged grieving process without end that affects a much smaller number of people but which really can be crippling for them,” he added.
The Text Revision adds new symptom codes for suicidal behavior and nonsuicidal self-injury, which appear in the chapter, “Other Conditions That May Be a Focus of Clinical Attention,” said Dr. Appelbaum.
“Both suicidal behavior and nonsuicidal self-injury seem pretty persuasively to fall into that category – something a clinician would want to know about, pay attention to, and factor into treatment planning, although they are behaviors that cross many diagnostic categories,” he added.
Codes also provide a systematic way of ascertaining the incidence and prevalence of such behaviors, said Dr. Appelbaum.
Changes to gender terminology
The Text Revision also tweaks some terminology with respect to transgender individuals. The term “desired gender” is now “experienced gender”, the term “cross-sex medical procedure” is now “gender-affirming medical procedure”, and the terms “natal male/natal female” are now “individual assigned male/female at birth”.
Dr. Frances said that the existence of gender dysphoria as a diagnosis has been a matter of controversy ever since it was first included.
“The transgender community has had mixed feelings on whether there should be anything at all in the manual,” he said. On one hand is the argument that gender dysphoria should be removed because it’s not really a psychiatric issue.
“We seriously considered eliminating it altogether in DSM-4,” said Dr. Frances.
However, an argument in favor of keeping it was that if the diagnosis was removed, it would mean that people could not receive treatment. “There’s no right argument for this dilemma,” he said.
Dr. Frances, who has been a frequent critic of DSM-5, said he believes the manual continues to miss opportunities to tighten criteria for many diagnoses, including ADHD and autism spectrum disorder.
“There’s a consistent pattern of taking behaviors and symptoms of behaviors that are on the border with normality and expanding the definition of mental disorder and reducing the realm of normality,” he said.
That has consequences, Dr. Frances added. “When someone gets a diagnosis that they need to get, it’s the beginning of a much better future. When someone gets a diagnosis that’s a mislabel that they don’t need, it has all harms and no benefits. It’s stigmatizing, leads to too much treatment, the wrong treatment, and it’s much more harmful than helpful.”
A version of this article first appeared on Medscape.com.
Ahead of its official release on March 18, the new Diagnostic and Statistical Manual of Mental Disorders, which is in the form of a textbook, is already drawing some criticism.
It also includes symptom codes for suicidal behavior and nonsuicidal self-injury, clarifying modifications to criteria sets for more than 70 disorders, including autism spectrum disorder; changes in terminology for gender dysphoria; and a comprehensive review of the impact of racism and discrimination on the diagnosis and manifestations of mental disorders.
The Text Revision is a compilation of iterative changes that have been made online on a rolling basis since the DSM-5 was first published in 2013.
“The goal of the Text Revision was to allow a thorough revision of the text, not the criteria,” Paul Appelbaum, MD, chair of the APA’s DSM steering committee, told this news organization.
For the Text Revision, some 200 experts across a variety of APA working groups recommended changes to the text based on a comprehensive literature review, said Appelbaum, who is the Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law, and director of the division of law, ethics and psychiatry at Columbia University, New York.
However, there’s not a lot that’s new, in part, because there have been few therapeutic advances.
Money maker?
Allen Frances, MD, chair of the DSM-4 task force and professor and chair emeritus of psychiatry at Duke University, Durham, N.C., said the APA is publishing the Text Revision “just to make money. They’re very anxious to do anything that will increase sales and having a revision forces some people, especially in institutions, to buy the book, even though it may not have anything substantive to add to the original.”
Dr. Frances told this news organization that when the APA published the first DSM in the late 1970s, “it became an instantaneous best-seller, to everyone’s surprise.”
The APA would not comment on how many of the $170 (list price) volumes it sells or how much those sales contribute to its budget.
Dr. Appelbaum acknowledged, “at any point in time, the canonical version is the online version.” However, it’s clear from DSM-5 sales “that many people still value having a hard copy of the DSM available to them.”
Prolonged grief: Timely or overkill?
Persistent complex bereavement disorder (PCBD) was listed as a “condition for further study” in DSM-5. After a 2019 workshop aimed at getting consensus for diagnosis criteria, the APA board approved the new prolonged grief disorder in October 2020, and the APA assembly approved the new disorder in November 2020.
Given the 950,000 deaths from COVID-19 over the past 2 years, inclusion of prolonged grief disorder in the DSM-5 may arrive at just the right time.
The diagnostic criteria for PCBD include:
- The development of a persistent grief response (longer than a year for adults and 6 months for children and adolescents) characterized by one or both of the following symptoms, which have been present most days to a clinically significant degree, and have occurred nearly every day for at least the last month: intense yearning/longing for the deceased person; preoccupation with thoughts or memories of the deceased person.
- Since the death, at least three symptoms present most days to a clinically significant degree, and occurring nearly every day for at least the last month, including identity disruption, marked sense of disbelief about the death, avoidance of reminders that the person is dead, intense emotional pain related to the death, difficulty reintegrating into one’s relationships and activities after the death, emotional numbness, feeling that life is meaningless as a result of the death, and intense loneliness as a result of the death.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The duration and severity of the bereavement reaction clearly exceed expected social, cultural, or religious norms for the individual’s culture and context.
- The symptoms are not better explained by another mental disorder, such as major depressive disorder (MDD) or PTSD, and are not attributable to the physiological effects of a substance or another medical condition.
Dr. Frances said he believes creating a new diagnosis pathologizes grief. In DSM-3 and DSM-4, an exception was made under the diagnosis of MDD for individuals who had recently lost a loved one. “We wanted to have at least an opportunity for people to grieve without being stigmatized, mislabeled, and overtreated with medication.”
DSM-5 removed the bereavement exclusion. After 2 weeks, people who are grieving and have particular symptoms could receive a diagnosis of MDD, said Dr. Frances. He believes the exclusion should have been broadened to cover anyone experiencing a major loss – such as a job loss or divorce. If someone is having prolonged symptoms that interfere with functioning, they should get an MDD diagnosis.
The new disorder “doesn’t solve anything, it just adds to the confusion and stigmatization, and it’s part of a kind of creeping medical imperialization of everyday life, where everything has to have a mental disorder label,” Dr. Frances said.
However, Dr. Appelbaum countered that “the criteria for prolonged grief disorder are constructed in such a way as to make every effort to exclude people who are going through a normal grieving process.”
“Part of the purpose of the data analyses was to ensure the criteria that were adopted would, in fact, effectively distinguish between what anybody goes through, say when someone close to you dies, and this unusual prolonged grieving process without end that affects a much smaller number of people but which really can be crippling for them,” he added.
The Text Revision adds new symptom codes for suicidal behavior and nonsuicidal self-injury, which appear in the chapter, “Other Conditions That May Be a Focus of Clinical Attention,” said Dr. Appelbaum.
“Both suicidal behavior and nonsuicidal self-injury seem pretty persuasively to fall into that category – something a clinician would want to know about, pay attention to, and factor into treatment planning, although they are behaviors that cross many diagnostic categories,” he added.
Codes also provide a systematic way of ascertaining the incidence and prevalence of such behaviors, said Dr. Appelbaum.
Changes to gender terminology
The Text Revision also tweaks some terminology with respect to transgender individuals. The term “desired gender” is now “experienced gender”, the term “cross-sex medical procedure” is now “gender-affirming medical procedure”, and the terms “natal male/natal female” are now “individual assigned male/female at birth”.
Dr. Frances said that the existence of gender dysphoria as a diagnosis has been a matter of controversy ever since it was first included.
“The transgender community has had mixed feelings on whether there should be anything at all in the manual,” he said. On one hand is the argument that gender dysphoria should be removed because it’s not really a psychiatric issue.
“We seriously considered eliminating it altogether in DSM-4,” said Dr. Frances.
However, an argument in favor of keeping it was that if the diagnosis was removed, it would mean that people could not receive treatment. “There’s no right argument for this dilemma,” he said.
Dr. Frances, who has been a frequent critic of DSM-5, said he believes the manual continues to miss opportunities to tighten criteria for many diagnoses, including ADHD and autism spectrum disorder.
“There’s a consistent pattern of taking behaviors and symptoms of behaviors that are on the border with normality and expanding the definition of mental disorder and reducing the realm of normality,” he said.
That has consequences, Dr. Frances added. “When someone gets a diagnosis that they need to get, it’s the beginning of a much better future. When someone gets a diagnosis that’s a mislabel that they don’t need, it has all harms and no benefits. It’s stigmatizing, leads to too much treatment, the wrong treatment, and it’s much more harmful than helpful.”
A version of this article first appeared on Medscape.com.
Ahead of its official release on March 18, the new Diagnostic and Statistical Manual of Mental Disorders, which is in the form of a textbook, is already drawing some criticism.
It also includes symptom codes for suicidal behavior and nonsuicidal self-injury, clarifying modifications to criteria sets for more than 70 disorders, including autism spectrum disorder; changes in terminology for gender dysphoria; and a comprehensive review of the impact of racism and discrimination on the diagnosis and manifestations of mental disorders.
The Text Revision is a compilation of iterative changes that have been made online on a rolling basis since the DSM-5 was first published in 2013.
“The goal of the Text Revision was to allow a thorough revision of the text, not the criteria,” Paul Appelbaum, MD, chair of the APA’s DSM steering committee, told this news organization.
For the Text Revision, some 200 experts across a variety of APA working groups recommended changes to the text based on a comprehensive literature review, said Appelbaum, who is the Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law, and director of the division of law, ethics and psychiatry at Columbia University, New York.
However, there’s not a lot that’s new, in part, because there have been few therapeutic advances.
Money maker?
Allen Frances, MD, chair of the DSM-4 task force and professor and chair emeritus of psychiatry at Duke University, Durham, N.C., said the APA is publishing the Text Revision “just to make money. They’re very anxious to do anything that will increase sales and having a revision forces some people, especially in institutions, to buy the book, even though it may not have anything substantive to add to the original.”
Dr. Frances told this news organization that when the APA published the first DSM in the late 1970s, “it became an instantaneous best-seller, to everyone’s surprise.”
The APA would not comment on how many of the $170 (list price) volumes it sells or how much those sales contribute to its budget.
Dr. Appelbaum acknowledged, “at any point in time, the canonical version is the online version.” However, it’s clear from DSM-5 sales “that many people still value having a hard copy of the DSM available to them.”
Prolonged grief: Timely or overkill?
Persistent complex bereavement disorder (PCBD) was listed as a “condition for further study” in DSM-5. After a 2019 workshop aimed at getting consensus for diagnosis criteria, the APA board approved the new prolonged grief disorder in October 2020, and the APA assembly approved the new disorder in November 2020.
Given the 950,000 deaths from COVID-19 over the past 2 years, inclusion of prolonged grief disorder in the DSM-5 may arrive at just the right time.
The diagnostic criteria for PCBD include:
- The development of a persistent grief response (longer than a year for adults and 6 months for children and adolescents) characterized by one or both of the following symptoms, which have been present most days to a clinically significant degree, and have occurred nearly every day for at least the last month: intense yearning/longing for the deceased person; preoccupation with thoughts or memories of the deceased person.
- Since the death, at least three symptoms present most days to a clinically significant degree, and occurring nearly every day for at least the last month, including identity disruption, marked sense of disbelief about the death, avoidance of reminders that the person is dead, intense emotional pain related to the death, difficulty reintegrating into one’s relationships and activities after the death, emotional numbness, feeling that life is meaningless as a result of the death, and intense loneliness as a result of the death.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The duration and severity of the bereavement reaction clearly exceed expected social, cultural, or religious norms for the individual’s culture and context.
- The symptoms are not better explained by another mental disorder, such as major depressive disorder (MDD) or PTSD, and are not attributable to the physiological effects of a substance or another medical condition.
Dr. Frances said he believes creating a new diagnosis pathologizes grief. In DSM-3 and DSM-4, an exception was made under the diagnosis of MDD for individuals who had recently lost a loved one. “We wanted to have at least an opportunity for people to grieve without being stigmatized, mislabeled, and overtreated with medication.”
DSM-5 removed the bereavement exclusion. After 2 weeks, people who are grieving and have particular symptoms could receive a diagnosis of MDD, said Dr. Frances. He believes the exclusion should have been broadened to cover anyone experiencing a major loss – such as a job loss or divorce. If someone is having prolonged symptoms that interfere with functioning, they should get an MDD diagnosis.
The new disorder “doesn’t solve anything, it just adds to the confusion and stigmatization, and it’s part of a kind of creeping medical imperialization of everyday life, where everything has to have a mental disorder label,” Dr. Frances said.
However, Dr. Appelbaum countered that “the criteria for prolonged grief disorder are constructed in such a way as to make every effort to exclude people who are going through a normal grieving process.”
“Part of the purpose of the data analyses was to ensure the criteria that were adopted would, in fact, effectively distinguish between what anybody goes through, say when someone close to you dies, and this unusual prolonged grieving process without end that affects a much smaller number of people but which really can be crippling for them,” he added.
The Text Revision adds new symptom codes for suicidal behavior and nonsuicidal self-injury, which appear in the chapter, “Other Conditions That May Be a Focus of Clinical Attention,” said Dr. Appelbaum.
“Both suicidal behavior and nonsuicidal self-injury seem pretty persuasively to fall into that category – something a clinician would want to know about, pay attention to, and factor into treatment planning, although they are behaviors that cross many diagnostic categories,” he added.
Codes also provide a systematic way of ascertaining the incidence and prevalence of such behaviors, said Dr. Appelbaum.
Changes to gender terminology
The Text Revision also tweaks some terminology with respect to transgender individuals. The term “desired gender” is now “experienced gender”, the term “cross-sex medical procedure” is now “gender-affirming medical procedure”, and the terms “natal male/natal female” are now “individual assigned male/female at birth”.
Dr. Frances said that the existence of gender dysphoria as a diagnosis has been a matter of controversy ever since it was first included.
“The transgender community has had mixed feelings on whether there should be anything at all in the manual,” he said. On one hand is the argument that gender dysphoria should be removed because it’s not really a psychiatric issue.
“We seriously considered eliminating it altogether in DSM-4,” said Dr. Frances.
However, an argument in favor of keeping it was that if the diagnosis was removed, it would mean that people could not receive treatment. “There’s no right argument for this dilemma,” he said.
Dr. Frances, who has been a frequent critic of DSM-5, said he believes the manual continues to miss opportunities to tighten criteria for many diagnoses, including ADHD and autism spectrum disorder.
“There’s a consistent pattern of taking behaviors and symptoms of behaviors that are on the border with normality and expanding the definition of mental disorder and reducing the realm of normality,” he said.
That has consequences, Dr. Frances added. “When someone gets a diagnosis that they need to get, it’s the beginning of a much better future. When someone gets a diagnosis that’s a mislabel that they don’t need, it has all harms and no benefits. It’s stigmatizing, leads to too much treatment, the wrong treatment, and it’s much more harmful than helpful.”
A version of this article first appeared on Medscape.com.
COVID-19 vaccine does not affect in vitro fertilization outcomes
Getting a COVID-19 mRNA vaccine did not affect pregnancy rates for women trying to conceive with in vitro fertilization or ovarian response to treatment, findings of a new study indicate.
The study was led by Sarit Avraham, MD, with the IVF unit, department of obstetrics and gynecology, Shamir Medical Center in Tzrifi, Israel. The findings were published online in Fertility and Sterility in a preproof version.
“Women should be vaccinated for COVID-19 prior to attempting to conceive via IVF treatments, given the higher risk of severe illness in pregnant women,” the authors wrote.
Doubts arose from “the theoretical concept of the supposed similarity between the SARS-CoV-2 spike protein and the syncytin protein that is speculated to take part in the fertilization process and the formation of the placenta,” the authors wrote.
Some then assumed that the COVID vaccine might kick off an immune response that could affect implantation and pregnancy. But this study and others before it found otherwise.
Researchers included 200 vaccinated women trying to conceive with IVF treatments in the retrospective study, and compared them with 200 unvaccinated patients of similar age (average age in both groups, 36 years) who were not previously infected with COVID-19. All the women were undergoing IVF from January to April 2021 and all the vaccinated women completed two doses of the BNT162b2 (Pfizer/BioNTech) vaccine at least 2 weeks before ovarian stimulation.
Researchers compared the average number of oocytes retrieved and clinical pregnancy rates between the two groups.
No difference between groups
Two hundred patients underwent oocyte retrieval 14-68 days after receiving a COVID shot; there was no significant difference by vaccination status in the number retrieved per cycle (10.63 in the vaccinated group vs. 10.72 in the unvaccinated group; P = .93).
There was also no difference in the clinical pregnancy rates after fresh embryo transfers. The rate among 128 vaccinated patients was 32.8% versus 33.1% in the 133 unvaccinated patients (P = .96), with 42 and 44 clinical pregnancies, respectively.
A total of 113 patients (66 in the study group and 47 in the controls) underwent freeze-all cycles to preserve fertility and fertilization rates were similar between vaccinated and unvaccinated (55.43% vaccinated vs. 54.29% unvaccinated; P = .73). The average number of cryopreserved embryos was 3.59 (vaccinated) versus 3.28 (unvaccinated) (P = .80).
In a subanalysis of outcomes by age, researchers found vaccination status had no effect on number of oocytes or pregnancy rates in the 39-and-older group. That’s important because it shows the vaccine did not affect outcomes even in a population with reduced ovarian reserves, the authors wrote.
The authors noted one of the study’s limitations is that it didn’t include information about vaccination or past infection status of the male partners.
Question should be put to rest
Sarah Cross, MD, a maternal-fetal medicine specialist at the University of Minnesota, Minneapolis, said the study is the biggest she’s seen that concludes COVID vaccinations are safe and highly encouraged for women before trying to conceive, but other smaller studies have come to the same conclusion.

She pointed to research including a study from 2021 with similar findings that concluded: “Physicians and public health personnel can counsel women of reproductive age that neither previous illness with COVID-19 nor antibodies produced from vaccination to COVID-19 will cause sterility.”
She said she thinks the question of whether COVID shots are safe with IVF has been answered and the results of the latest study add proof to counter misinformation around the issue.
“The COVID-19 vaccine does not affect fertility,” she said. “I don’t know how many more [studies] we need.”
The harm is in not getting vaccinated, she said. Pregnancy significantly increases a woman’s chance of getting severe COVID, the need for hospitalization, mechanical ventilation, and risk of death.
“I personally have never had a hospitalized patient who’s been vaccinated,” Dr. Cross said. “The worst thing for the fetus is to have a critically ill mother.”
Dr. Cross, whose high-risk patients include those seeking counseling before IVF, added: “I would counsel all of them that they should absolutely get vaccinated prior to pregnancy, when they’re pregnant, whenever it is, as soon as they possibly can.”
The study authors and Dr. Cross report no relevant financial relationships.
Getting a COVID-19 mRNA vaccine did not affect pregnancy rates for women trying to conceive with in vitro fertilization or ovarian response to treatment, findings of a new study indicate.
The study was led by Sarit Avraham, MD, with the IVF unit, department of obstetrics and gynecology, Shamir Medical Center in Tzrifi, Israel. The findings were published online in Fertility and Sterility in a preproof version.
“Women should be vaccinated for COVID-19 prior to attempting to conceive via IVF treatments, given the higher risk of severe illness in pregnant women,” the authors wrote.
Doubts arose from “the theoretical concept of the supposed similarity between the SARS-CoV-2 spike protein and the syncytin protein that is speculated to take part in the fertilization process and the formation of the placenta,” the authors wrote.
Some then assumed that the COVID vaccine might kick off an immune response that could affect implantation and pregnancy. But this study and others before it found otherwise.
Researchers included 200 vaccinated women trying to conceive with IVF treatments in the retrospective study, and compared them with 200 unvaccinated patients of similar age (average age in both groups, 36 years) who were not previously infected with COVID-19. All the women were undergoing IVF from January to April 2021 and all the vaccinated women completed two doses of the BNT162b2 (Pfizer/BioNTech) vaccine at least 2 weeks before ovarian stimulation.
Researchers compared the average number of oocytes retrieved and clinical pregnancy rates between the two groups.
No difference between groups
Two hundred patients underwent oocyte retrieval 14-68 days after receiving a COVID shot; there was no significant difference by vaccination status in the number retrieved per cycle (10.63 in the vaccinated group vs. 10.72 in the unvaccinated group; P = .93).
There was also no difference in the clinical pregnancy rates after fresh embryo transfers. The rate among 128 vaccinated patients was 32.8% versus 33.1% in the 133 unvaccinated patients (P = .96), with 42 and 44 clinical pregnancies, respectively.
A total of 113 patients (66 in the study group and 47 in the controls) underwent freeze-all cycles to preserve fertility and fertilization rates were similar between vaccinated and unvaccinated (55.43% vaccinated vs. 54.29% unvaccinated; P = .73). The average number of cryopreserved embryos was 3.59 (vaccinated) versus 3.28 (unvaccinated) (P = .80).
In a subanalysis of outcomes by age, researchers found vaccination status had no effect on number of oocytes or pregnancy rates in the 39-and-older group. That’s important because it shows the vaccine did not affect outcomes even in a population with reduced ovarian reserves, the authors wrote.
The authors noted one of the study’s limitations is that it didn’t include information about vaccination or past infection status of the male partners.
Question should be put to rest
Sarah Cross, MD, a maternal-fetal medicine specialist at the University of Minnesota, Minneapolis, said the study is the biggest she’s seen that concludes COVID vaccinations are safe and highly encouraged for women before trying to conceive, but other smaller studies have come to the same conclusion.
She pointed to research including a study from 2021 with similar findings that concluded: “Physicians and public health personnel can counsel women of reproductive age that neither previous illness with COVID-19 nor antibodies produced from vaccination to COVID-19 will cause sterility.”
She said she thinks the question of whether COVID shots are safe with IVF has been answered and the results of the latest study add proof to counter misinformation around the issue.
“The COVID-19 vaccine does not affect fertility,” she said. “I don’t know how many more [studies] we need.”
The harm is in not getting vaccinated, she said. Pregnancy significantly increases a woman’s chance of getting severe COVID, the need for hospitalization, mechanical ventilation, and risk of death.
“I personally have never had a hospitalized patient who’s been vaccinated,” Dr. Cross said. “The worst thing for the fetus is to have a critically ill mother.”
Dr. Cross, whose high-risk patients include those seeking counseling before IVF, added: “I would counsel all of them that they should absolutely get vaccinated prior to pregnancy, when they’re pregnant, whenever it is, as soon as they possibly can.”
The study authors and Dr. Cross report no relevant financial relationships.
Getting a COVID-19 mRNA vaccine did not affect pregnancy rates for women trying to conceive with in vitro fertilization or ovarian response to treatment, findings of a new study indicate.
The study was led by Sarit Avraham, MD, with the IVF unit, department of obstetrics and gynecology, Shamir Medical Center in Tzrifi, Israel. The findings were published online in Fertility and Sterility in a preproof version.
“Women should be vaccinated for COVID-19 prior to attempting to conceive via IVF treatments, given the higher risk of severe illness in pregnant women,” the authors wrote.
Doubts arose from “the theoretical concept of the supposed similarity between the SARS-CoV-2 spike protein and the syncytin protein that is speculated to take part in the fertilization process and the formation of the placenta,” the authors wrote.
Some then assumed that the COVID vaccine might kick off an immune response that could affect implantation and pregnancy. But this study and others before it found otherwise.
Researchers included 200 vaccinated women trying to conceive with IVF treatments in the retrospective study, and compared them with 200 unvaccinated patients of similar age (average age in both groups, 36 years) who were not previously infected with COVID-19. All the women were undergoing IVF from January to April 2021 and all the vaccinated women completed two doses of the BNT162b2 (Pfizer/BioNTech) vaccine at least 2 weeks before ovarian stimulation.
Researchers compared the average number of oocytes retrieved and clinical pregnancy rates between the two groups.
No difference between groups
Two hundred patients underwent oocyte retrieval 14-68 days after receiving a COVID shot; there was no significant difference by vaccination status in the number retrieved per cycle (10.63 in the vaccinated group vs. 10.72 in the unvaccinated group; P = .93).
There was also no difference in the clinical pregnancy rates after fresh embryo transfers. The rate among 128 vaccinated patients was 32.8% versus 33.1% in the 133 unvaccinated patients (P = .96), with 42 and 44 clinical pregnancies, respectively.
A total of 113 patients (66 in the study group and 47 in the controls) underwent freeze-all cycles to preserve fertility and fertilization rates were similar between vaccinated and unvaccinated (55.43% vaccinated vs. 54.29% unvaccinated; P = .73). The average number of cryopreserved embryos was 3.59 (vaccinated) versus 3.28 (unvaccinated) (P = .80).
In a subanalysis of outcomes by age, researchers found vaccination status had no effect on number of oocytes or pregnancy rates in the 39-and-older group. That’s important because it shows the vaccine did not affect outcomes even in a population with reduced ovarian reserves, the authors wrote.
The authors noted one of the study’s limitations is that it didn’t include information about vaccination or past infection status of the male partners.
Question should be put to rest
Sarah Cross, MD, a maternal-fetal medicine specialist at the University of Minnesota, Minneapolis, said the study is the biggest she’s seen that concludes COVID vaccinations are safe and highly encouraged for women before trying to conceive, but other smaller studies have come to the same conclusion.
She pointed to research including a study from 2021 with similar findings that concluded: “Physicians and public health personnel can counsel women of reproductive age that neither previous illness with COVID-19 nor antibodies produced from vaccination to COVID-19 will cause sterility.”
She said she thinks the question of whether COVID shots are safe with IVF has been answered and the results of the latest study add proof to counter misinformation around the issue.
“The COVID-19 vaccine does not affect fertility,” she said. “I don’t know how many more [studies] we need.”
The harm is in not getting vaccinated, she said. Pregnancy significantly increases a woman’s chance of getting severe COVID, the need for hospitalization, mechanical ventilation, and risk of death.
“I personally have never had a hospitalized patient who’s been vaccinated,” Dr. Cross said. “The worst thing for the fetus is to have a critically ill mother.”
Dr. Cross, whose high-risk patients include those seeking counseling before IVF, added: “I would counsel all of them that they should absolutely get vaccinated prior to pregnancy, when they’re pregnant, whenever it is, as soon as they possibly can.”
The study authors and Dr. Cross report no relevant financial relationships.
FROM FERTILITY AND STERILITY
Finerenone + SGLT2 inhibitor of benefit in diabetes with CKD?
New signals of a potential additive benefit from the nonsteroidal mineralocorticoid antagonist finerenone (Kerendia) and a sodium-glucose transporter 2 inhibitor in patients with type 2 diabetes and chronic kidney disease (CKD) emerged in a follow-up report from the FIDELITY analysis, which combined data from more than 13,000 patients who received finerenone in either of the two pivotal trials with the agent.
The analysis showed that the 877 patients enrolled in either the FIDELIO DKD or FIGARO DKD trials taking an SGLT2 inhibitor at baseline had a 37% relative reduction in their urinary albumin-to-creatinine ratio (UACR), compared with placebo-treated patients after a median of 3 years on treatment.
Among the remaining 12,149 patients who did not receive an SGLT2 inhibitor, finerenone cut the average UACR by 32%, compared with placebo, said Peter Rossing, DMSc, MD, who presented the findings on Feb. 27 at the World Congress of Nephrology 2022 in Kuala Lumpur, Malaysia.
Primary endpoint results for FIDELIO-DKD and FIGARO-DKD also suggest similar additive effects of finerenone plus an SGLT2 inhibitor.
Results of the composite renal endpoint in each study – progression to kidney failure, renal death, or at least a 57% decline in estimated glomerular filtration rate (eGFR) from baseline – showed a 58% relative risk reduction in patients who received agents from both drug classes and a 20% relative risk reduction in those who only received finerenone, a between-group difference that was not significant.
For the composite cardiovascular event endpoint – cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure – the rate fell by 37%, compared with placebo, in patients who also received an SGLT2 inhibitor, and by 13%, compared with placebo, in those who received finerenone but no SGLT2 inhibitor, also a difference that was not significant.
‘A lot of interest in finerenone’ in U.S.
“The benefits of finerenone on cardiovascular and kidney outcomes were consistent, irrespective of SGLT2 inhibitor use at baseline,” concluded Dr. Rossing, professor and head of research at the Steno Diabetes Center in Copenhagen.
The new findings are a “suggestion that the two classes might be additive [in their effects], but more data are needed,” Dr. Rossing said during his presentation.
But he cautioned that in both pivotal trials randomization did not consider SGLT2 inhibitor use. All patients in the two trials were already receiving a renin-angiotensin system (RAS) inhibitor as background treatment, either an ACE inhibitor or angiotensin-receptor blocker.
The consequence of treatment with finerenone combined with an SGLT2 inhibitor is of growing importance because “an SGLT2 inhibitor is now recommended in most guidelines” for the type of patients enrolled in the two finerenone trials, explained Dr. Rossing.
He also noted that the first guideline to recommend routine use of finerenone in indicated patients appeared recently in the annual update to Standards of Medical Care in Diabetes – 2022 published by the American Diabetes Association.
The 2022 Standards states: “In patients with CKD who are at increased risk for cardiovascular events or CKD progression or are unable to use an SGLT2 inhibitor, a nonsteroidal mineralocorticoid receptor antagonist (finerenone) is recommended to reduce CKD progression and cardiovascular events.”
Results from FIDELIO-DKD, reported in the New England Journal of Medicine in 2020, and the main study, FIGARO-DKD, published in the same journal in 2021, led the Food and Drug Administration to approve finerenone in July 2021 to slow the progression of renal disease in patients with type 2 diabetes and CKD.
“My impression is that in the United States there is a lot of interest in finerenone,” Dr. Rossing said during the discussion following his presentation.
Finerenone has also been recently approved in the European Union.
‘Consistent’ benefits irrespective of SGLT2 inhibitors
“The cardiovascular and kidney benefits of finerenone were consistent irrespective of SGLT2 inhibitor use. This is definitely interesting and warrants a randomized controlled trial” to examine the relationship in a more rigorous way, commented Tejas Desai, MD, a nephrologist with the Department of Veterans Affairs, Charlotte, N.C.
That study, CONFIDENCE, is on its way, Dr. Rossing said during his talk. The randomized phase 2 trial has a planned enrollment of 800 patients with type 2 diabetes and CKD and three treatment groups: finerenone plus placebo, the SGLT2 inhibitor empagliflozin (Jardiance) plus placebo, or finerenone plus empagliflozin. The study will launch later in 2022 and has a planned completion date of late 2023.
“SGLT2 inhibitors, compared with finerenone, is where all of this is headed. We need a large trial that adjudicates the best medication to use with a RAS inhibitor,” Dr. Desai said in an interview.
The new analyses from the combined FIDELITY study expand on a previous report presented at the 2021 annual congress of the European Society of Cardiology and published in the European Heart Journal.
‘Impressive’ effect on cardiovascular events
The main findings from FIDELITY presented in those earlier reports, in 13,026 patients, showed there was a significant 14% relative reduction in the composite cardiovascular endpoint with finerenone, compared with placebo, during a median 3 years of follow-up.
The same report documented, in the total combined cohort, a significant 23% relative reduction in the composite renal endpoint in those taking finerenone compared with placebo.
“Reducing the risk of cardiovascular endpoints by a relative 14% is impressive,” and the time course showed a “relatively quick onset of action,” Dr. Desai noted.
He also characterized the enrolled patients, which included many with stage 3 or 4 CKD, as “not the sickest population of patients with CKD,” but rather “relatively healthier patients with CKD.”
Dr. Desai also downplayed the importance of the observed reduction in UACR associated with finerenone in FIDELITY.
“UACR is a surrogate marker. Results from many studies have shown improvements in UACR only to not show protection against falls in eGFR rate,” Dr. Desai said.
He was also reassured by the low incidence of hyperkalemia that led to discontinuation, which occurred in 1.7% of patients taking finerenone and in 0.6% of those taking placebo.
The types of patients enrolled in FIDELIO-DKD and FIGARO-DKD, who did not have eGFR rates below 25 mL/min per 1.73 m2, are not particularly susceptible to this adverse effect, he said, noting, “I’m not overly concerned with hyperkalemia in this CKD population.
“I’m more concerned about [hyperkalemia in] patients with CKD and an eGFR of less than 25 mL/min per 1.73 m2, but this was less than 1% of the enrolled population,” Dr. Desai observed.
FIDELIO-DKD, FIGARO-DKD, and FIDELITY were sponsored by Bayer, which markets finerenone (Kerendia). Dr. Rossing reported being a consultant for Bayer and other drug companies, and receiving research funding from AstraZeneca and Novo Nordisk. Dr. Desai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New signals of a potential additive benefit from the nonsteroidal mineralocorticoid antagonist finerenone (Kerendia) and a sodium-glucose transporter 2 inhibitor in patients with type 2 diabetes and chronic kidney disease (CKD) emerged in a follow-up report from the FIDELITY analysis, which combined data from more than 13,000 patients who received finerenone in either of the two pivotal trials with the agent.
The analysis showed that the 877 patients enrolled in either the FIDELIO DKD or FIGARO DKD trials taking an SGLT2 inhibitor at baseline had a 37% relative reduction in their urinary albumin-to-creatinine ratio (UACR), compared with placebo-treated patients after a median of 3 years on treatment.
Among the remaining 12,149 patients who did not receive an SGLT2 inhibitor, finerenone cut the average UACR by 32%, compared with placebo, said Peter Rossing, DMSc, MD, who presented the findings on Feb. 27 at the World Congress of Nephrology 2022 in Kuala Lumpur, Malaysia.
Primary endpoint results for FIDELIO-DKD and FIGARO-DKD also suggest similar additive effects of finerenone plus an SGLT2 inhibitor.
Results of the composite renal endpoint in each study – progression to kidney failure, renal death, or at least a 57% decline in estimated glomerular filtration rate (eGFR) from baseline – showed a 58% relative risk reduction in patients who received agents from both drug classes and a 20% relative risk reduction in those who only received finerenone, a between-group difference that was not significant.
For the composite cardiovascular event endpoint – cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure – the rate fell by 37%, compared with placebo, in patients who also received an SGLT2 inhibitor, and by 13%, compared with placebo, in those who received finerenone but no SGLT2 inhibitor, also a difference that was not significant.
‘A lot of interest in finerenone’ in U.S.
“The benefits of finerenone on cardiovascular and kidney outcomes were consistent, irrespective of SGLT2 inhibitor use at baseline,” concluded Dr. Rossing, professor and head of research at the Steno Diabetes Center in Copenhagen.
The new findings are a “suggestion that the two classes might be additive [in their effects], but more data are needed,” Dr. Rossing said during his presentation.
But he cautioned that in both pivotal trials randomization did not consider SGLT2 inhibitor use. All patients in the two trials were already receiving a renin-angiotensin system (RAS) inhibitor as background treatment, either an ACE inhibitor or angiotensin-receptor blocker.
The consequence of treatment with finerenone combined with an SGLT2 inhibitor is of growing importance because “an SGLT2 inhibitor is now recommended in most guidelines” for the type of patients enrolled in the two finerenone trials, explained Dr. Rossing.
He also noted that the first guideline to recommend routine use of finerenone in indicated patients appeared recently in the annual update to Standards of Medical Care in Diabetes – 2022 published by the American Diabetes Association.
The 2022 Standards states: “In patients with CKD who are at increased risk for cardiovascular events or CKD progression or are unable to use an SGLT2 inhibitor, a nonsteroidal mineralocorticoid receptor antagonist (finerenone) is recommended to reduce CKD progression and cardiovascular events.”
Results from FIDELIO-DKD, reported in the New England Journal of Medicine in 2020, and the main study, FIGARO-DKD, published in the same journal in 2021, led the Food and Drug Administration to approve finerenone in July 2021 to slow the progression of renal disease in patients with type 2 diabetes and CKD.
“My impression is that in the United States there is a lot of interest in finerenone,” Dr. Rossing said during the discussion following his presentation.
Finerenone has also been recently approved in the European Union.
‘Consistent’ benefits irrespective of SGLT2 inhibitors
“The cardiovascular and kidney benefits of finerenone were consistent irrespective of SGLT2 inhibitor use. This is definitely interesting and warrants a randomized controlled trial” to examine the relationship in a more rigorous way, commented Tejas Desai, MD, a nephrologist with the Department of Veterans Affairs, Charlotte, N.C.
That study, CONFIDENCE, is on its way, Dr. Rossing said during his talk. The randomized phase 2 trial has a planned enrollment of 800 patients with type 2 diabetes and CKD and three treatment groups: finerenone plus placebo, the SGLT2 inhibitor empagliflozin (Jardiance) plus placebo, or finerenone plus empagliflozin. The study will launch later in 2022 and has a planned completion date of late 2023.
“SGLT2 inhibitors, compared with finerenone, is where all of this is headed. We need a large trial that adjudicates the best medication to use with a RAS inhibitor,” Dr. Desai said in an interview.
The new analyses from the combined FIDELITY study expand on a previous report presented at the 2021 annual congress of the European Society of Cardiology and published in the European Heart Journal.
‘Impressive’ effect on cardiovascular events
The main findings from FIDELITY presented in those earlier reports, in 13,026 patients, showed there was a significant 14% relative reduction in the composite cardiovascular endpoint with finerenone, compared with placebo, during a median 3 years of follow-up.
The same report documented, in the total combined cohort, a significant 23% relative reduction in the composite renal endpoint in those taking finerenone compared with placebo.
“Reducing the risk of cardiovascular endpoints by a relative 14% is impressive,” and the time course showed a “relatively quick onset of action,” Dr. Desai noted.
He also characterized the enrolled patients, which included many with stage 3 or 4 CKD, as “not the sickest population of patients with CKD,” but rather “relatively healthier patients with CKD.”
Dr. Desai also downplayed the importance of the observed reduction in UACR associated with finerenone in FIDELITY.
“UACR is a surrogate marker. Results from many studies have shown improvements in UACR only to not show protection against falls in eGFR rate,” Dr. Desai said.
He was also reassured by the low incidence of hyperkalemia that led to discontinuation, which occurred in 1.7% of patients taking finerenone and in 0.6% of those taking placebo.
The types of patients enrolled in FIDELIO-DKD and FIGARO-DKD, who did not have eGFR rates below 25 mL/min per 1.73 m2, are not particularly susceptible to this adverse effect, he said, noting, “I’m not overly concerned with hyperkalemia in this CKD population.
“I’m more concerned about [hyperkalemia in] patients with CKD and an eGFR of less than 25 mL/min per 1.73 m2, but this was less than 1% of the enrolled population,” Dr. Desai observed.
FIDELIO-DKD, FIGARO-DKD, and FIDELITY were sponsored by Bayer, which markets finerenone (Kerendia). Dr. Rossing reported being a consultant for Bayer and other drug companies, and receiving research funding from AstraZeneca and Novo Nordisk. Dr. Desai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New signals of a potential additive benefit from the nonsteroidal mineralocorticoid antagonist finerenone (Kerendia) and a sodium-glucose transporter 2 inhibitor in patients with type 2 diabetes and chronic kidney disease (CKD) emerged in a follow-up report from the FIDELITY analysis, which combined data from more than 13,000 patients who received finerenone in either of the two pivotal trials with the agent.
The analysis showed that the 877 patients enrolled in either the FIDELIO DKD or FIGARO DKD trials taking an SGLT2 inhibitor at baseline had a 37% relative reduction in their urinary albumin-to-creatinine ratio (UACR), compared with placebo-treated patients after a median of 3 years on treatment.
Among the remaining 12,149 patients who did not receive an SGLT2 inhibitor, finerenone cut the average UACR by 32%, compared with placebo, said Peter Rossing, DMSc, MD, who presented the findings on Feb. 27 at the World Congress of Nephrology 2022 in Kuala Lumpur, Malaysia.
Primary endpoint results for FIDELIO-DKD and FIGARO-DKD also suggest similar additive effects of finerenone plus an SGLT2 inhibitor.
Results of the composite renal endpoint in each study – progression to kidney failure, renal death, or at least a 57% decline in estimated glomerular filtration rate (eGFR) from baseline – showed a 58% relative risk reduction in patients who received agents from both drug classes and a 20% relative risk reduction in those who only received finerenone, a between-group difference that was not significant.
For the composite cardiovascular event endpoint – cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure – the rate fell by 37%, compared with placebo, in patients who also received an SGLT2 inhibitor, and by 13%, compared with placebo, in those who received finerenone but no SGLT2 inhibitor, also a difference that was not significant.
‘A lot of interest in finerenone’ in U.S.
“The benefits of finerenone on cardiovascular and kidney outcomes were consistent, irrespective of SGLT2 inhibitor use at baseline,” concluded Dr. Rossing, professor and head of research at the Steno Diabetes Center in Copenhagen.
The new findings are a “suggestion that the two classes might be additive [in their effects], but more data are needed,” Dr. Rossing said during his presentation.
But he cautioned that in both pivotal trials randomization did not consider SGLT2 inhibitor use. All patients in the two trials were already receiving a renin-angiotensin system (RAS) inhibitor as background treatment, either an ACE inhibitor or angiotensin-receptor blocker.
The consequence of treatment with finerenone combined with an SGLT2 inhibitor is of growing importance because “an SGLT2 inhibitor is now recommended in most guidelines” for the type of patients enrolled in the two finerenone trials, explained Dr. Rossing.
He also noted that the first guideline to recommend routine use of finerenone in indicated patients appeared recently in the annual update to Standards of Medical Care in Diabetes – 2022 published by the American Diabetes Association.
The 2022 Standards states: “In patients with CKD who are at increased risk for cardiovascular events or CKD progression or are unable to use an SGLT2 inhibitor, a nonsteroidal mineralocorticoid receptor antagonist (finerenone) is recommended to reduce CKD progression and cardiovascular events.”
Results from FIDELIO-DKD, reported in the New England Journal of Medicine in 2020, and the main study, FIGARO-DKD, published in the same journal in 2021, led the Food and Drug Administration to approve finerenone in July 2021 to slow the progression of renal disease in patients with type 2 diabetes and CKD.
“My impression is that in the United States there is a lot of interest in finerenone,” Dr. Rossing said during the discussion following his presentation.
Finerenone has also been recently approved in the European Union.
‘Consistent’ benefits irrespective of SGLT2 inhibitors
“The cardiovascular and kidney benefits of finerenone were consistent irrespective of SGLT2 inhibitor use. This is definitely interesting and warrants a randomized controlled trial” to examine the relationship in a more rigorous way, commented Tejas Desai, MD, a nephrologist with the Department of Veterans Affairs, Charlotte, N.C.
That study, CONFIDENCE, is on its way, Dr. Rossing said during his talk. The randomized phase 2 trial has a planned enrollment of 800 patients with type 2 diabetes and CKD and three treatment groups: finerenone plus placebo, the SGLT2 inhibitor empagliflozin (Jardiance) plus placebo, or finerenone plus empagliflozin. The study will launch later in 2022 and has a planned completion date of late 2023.
“SGLT2 inhibitors, compared with finerenone, is where all of this is headed. We need a large trial that adjudicates the best medication to use with a RAS inhibitor,” Dr. Desai said in an interview.
The new analyses from the combined FIDELITY study expand on a previous report presented at the 2021 annual congress of the European Society of Cardiology and published in the European Heart Journal.
‘Impressive’ effect on cardiovascular events
The main findings from FIDELITY presented in those earlier reports, in 13,026 patients, showed there was a significant 14% relative reduction in the composite cardiovascular endpoint with finerenone, compared with placebo, during a median 3 years of follow-up.
The same report documented, in the total combined cohort, a significant 23% relative reduction in the composite renal endpoint in those taking finerenone compared with placebo.
“Reducing the risk of cardiovascular endpoints by a relative 14% is impressive,” and the time course showed a “relatively quick onset of action,” Dr. Desai noted.
He also characterized the enrolled patients, which included many with stage 3 or 4 CKD, as “not the sickest population of patients with CKD,” but rather “relatively healthier patients with CKD.”
Dr. Desai also downplayed the importance of the observed reduction in UACR associated with finerenone in FIDELITY.
“UACR is a surrogate marker. Results from many studies have shown improvements in UACR only to not show protection against falls in eGFR rate,” Dr. Desai said.
He was also reassured by the low incidence of hyperkalemia that led to discontinuation, which occurred in 1.7% of patients taking finerenone and in 0.6% of those taking placebo.
The types of patients enrolled in FIDELIO-DKD and FIGARO-DKD, who did not have eGFR rates below 25 mL/min per 1.73 m2, are not particularly susceptible to this adverse effect, he said, noting, “I’m not overly concerned with hyperkalemia in this CKD population.
“I’m more concerned about [hyperkalemia in] patients with CKD and an eGFR of less than 25 mL/min per 1.73 m2, but this was less than 1% of the enrolled population,” Dr. Desai observed.
FIDELIO-DKD, FIGARO-DKD, and FIDELITY were sponsored by Bayer, which markets finerenone (Kerendia). Dr. Rossing reported being a consultant for Bayer and other drug companies, and receiving research funding from AstraZeneca and Novo Nordisk. Dr. Desai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE WORLD CONGRESS OF NEPHROLOGY
Nirsevimab protects healthy infants from RSV
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Pediatric IBD increases cancer risk later in life
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK
Geriatric guideline implementation remains unrealistic in most EDs
Many emergency departments are currently unable to provide care for geriatric patients that meets best practices and guidelines recommended by several major medical organizations, but a panel discussion in 2021 at the American Academy of Emergency Medicine’s Scientific Assembly identified three areas in which realistic improvements might be achieved.
In an article published online in the Journal of Emergency Medicine, Richard D. Shih, MD, of Florida Atlantic University, Boca Raton, and colleagues synthesized the presentation and discussion of an expert panel on the topic of the GED guidelines and the current realities of patient care.
The Geriatric Emergency Department (GED) Guidelines, published in 2014 in Annals of Emergency Medicine, were endorsed by the American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association, and Society for Academic Emergency Medicine.
“With the substantial challenges in providing guideline-recommended care in EDs, this article will explore three high-impact GED clinical conditions to highlight guideline recommendations, challenges, and opportunities, and discuss realistically achievable expectations for non–GED-accredited institutions,” the authors wrote.
Geriatric patients and delirium
When delirium in older adults is not identified in the ED, the patient’s 6-month mortality rate significantly increases, but few EDs have delirium screening protocols, the authors said. Challenges included the time and money needed to educate staff, on top of multiple mandatory training requirements on other topics. Delirium screening in the clinical setting also requires personnel to conduct assessments, and time to document symptoms and screening results in medical records.
“Perhaps the highest priority challenge for delirium experts is to evaluate and publish effective delirium intervention strategies because current evidence is completely lacking for ED-based delirium prevention or treatment,” they said. In the meantime, developing outcome measures for quality improvement of delirium care will require institutional support as well as education.
Geriatric patients and falls
Approximately one third of community-dwelling adults older than 65 years suffer falls, but data suggest that fewer than half of these individuals report falls to their doctors. “Older adults who present to an ED after a fall have an approximately 30% greater risk of functional decline and depression at 6 months after the event,” the authors noted.
The GED guidelines call for a comprehensive approach to evaluating and managing falls in older adults, but many of these “are untested in the ED,” the authors said. The recommended protocol includes an initial assessment of fall risk, followed by, for those at low risk, tailored recommendations for education and the use of community resources. Additional recommendations for those at high risk of falls include multifactorial assessment of modifiable risk factors, including peripheral neuropathy, balance/gait assessment, and medication review.
However, this best practice workflow is beyond the resource capacity of most EDs, the authors noted. “When ED resources are insufficient to support best practices, the care should focus on educating patients and caregivers about the significance of a fall event, providing educational materials (e.g., [the Centers for Disease Control and Prevention’s] STEADI materials), and assessing safety with respect to mobility for immediate return to the home environment and follow-up with a PCP.”
Geriatric patients and polypharmacy
Polypharmacy is common among older adults by virtue of their greater number of illnesses and comorbid conditions, and polypharmacy also has been associated with more adverse drug reactions, the authors said. The AGS Beers Criteria identifies medications associated with adverse drug reactions, but it is not practical for use in a busy ED setting. Instead, the authors suggested a more practical approach of focusing on a smaller list of common medications that tend to cause the adverse events that may result in ED visits.
“Perhaps targeting patients on multiple (three or more) psychoactive medications, drugs that can cause hypotension, or hypoglycemics could not only be done quickly, but identify patients in whom deprescribing should be considered in the ED,” the authors wrote. Deprescribing is a complicated process, however, and may be more effective when done via the patient’s primary care provider or in a geriatric consultation.
The GED Guidelines highlighted the specific needs of the geriatric population in the ED, the authors said. Widespread implementation remains a challenge, but many organizations provide resources to help improve care of geriatric patients in the ED and beyond.
In particular, the Geriatric Emergency Care Applied Research Network and Geriatric Emergency Department Collaborative provide funding opportunities, updated and focused published reviews, and webinars (some including free continuing medical education) for the entire health care team, including hospital administrators, the authors said.
Article brings attention to clinical realities
“The reality is that the overwhelming majority of emergency departments in the United States, if not globally, are simply not equipped – operationally or financially – to meet the rigorous standards that are required to fulfill the goals of operating an accredited geriatric ED,” Robert D. Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, said in an interview.
“Drawing attention to this important gap in accreditation is critical to not only inform hospitals, health care providers and stakeholders, but the public, patients, and their families about the important work that needs to be done to better equip all EDs with the proper tools and educational approaches to more effectively care for the geriatric community,” Dr. Glatter emphasized.
“There are currently three tiers of accreditation, with level 1 being the highest,” he explained, but there are only 100 geriatric ED accreditation-certified hospitals across the United States.
“I am not surprised at all by the challenges of implementing current GED guidelines,” said Dr. Glatter. “It comes down to operational and budget considerations, which ultimately compete with many other departments and regulatory constraints in any given hospital.”
However, “the bottom line is that such guidelines are designed with patient safety in mind, making them important issues in the eyes of any hospital administrator looking to improve outcomes and reduce medicolegal risk or exposure impacting geriatric patients in the emergency department,” he noted.
Ultimately, guideline adherence “comes down to budget decisions, and where hospitals must invest their money to meet the bottom line,” said Dr. Glatter. “Making modifications to hospital infrastructure and architecture to accommodate geriatric patients may not be the top priority of hospital administrators when confronted with multiple competing interests. But, if it impacts patient safety, the decision to invest in structural and operational improvements may certainly have additional and important considerations.
“Until Medicare, or even the Joint Commission on Accreditation of Hospitals, adopts geriatric guidelines in emergency departments as a requirement for accreditation, there may not be adequate incentives in place currently to satisfy the intent of having a rigorous set of guidelines in the first place,” Dr. Glatter added.
Despite the limitations of applying the current guidelines, there are some steps hospitals can take, said Dr. Glatter. “They can institute new measures in a graded fashion, with the goal of taking the important steps to satisfy at least some components of the guidelines. Attention to details can go a long way, such as rails in bathrooms, better lighting, and treads on floors that may reduce the risk of falls in the ED itself.
“Attention to fall prevention by assessing contributors including polypharmacy, gait instability, and quality of footwear can impact risk of future ED visits. Having incentives in place by Medicare or JACO may force the hand of hospital administrators to comply with geriatric guidelines and place emphasis on compliance,” noted Dr. Glatter.
More research is needed that “looks at costs of implementing geriatric guidelines in typical community and academic EDs and how this impacts key metrics such as length of stay, effect on reimbursement per ICD-10 code, and savings, if any, realized in reduced malpractice claims related to missed diagnoses (such as delirium), injuries, (patient falls), or medical misadventures due to polypharmacy,” he said.
The article received no outside funding. The authors disclosed no relevant financial relationships. Dr. Glatter disclosed no relevant financial relationships, and serves on the advisory board of Medscape Emergency Medicine.
A version of this article first appeared on Medscape.com.
Many emergency departments are currently unable to provide care for geriatric patients that meets best practices and guidelines recommended by several major medical organizations, but a panel discussion in 2021 at the American Academy of Emergency Medicine’s Scientific Assembly identified three areas in which realistic improvements might be achieved.
In an article published online in the Journal of Emergency Medicine, Richard D. Shih, MD, of Florida Atlantic University, Boca Raton, and colleagues synthesized the presentation and discussion of an expert panel on the topic of the GED guidelines and the current realities of patient care.
The Geriatric Emergency Department (GED) Guidelines, published in 2014 in Annals of Emergency Medicine, were endorsed by the American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association, and Society for Academic Emergency Medicine.
“With the substantial challenges in providing guideline-recommended care in EDs, this article will explore three high-impact GED clinical conditions to highlight guideline recommendations, challenges, and opportunities, and discuss realistically achievable expectations for non–GED-accredited institutions,” the authors wrote.
Geriatric patients and delirium
When delirium in older adults is not identified in the ED, the patient’s 6-month mortality rate significantly increases, but few EDs have delirium screening protocols, the authors said. Challenges included the time and money needed to educate staff, on top of multiple mandatory training requirements on other topics. Delirium screening in the clinical setting also requires personnel to conduct assessments, and time to document symptoms and screening results in medical records.
“Perhaps the highest priority challenge for delirium experts is to evaluate and publish effective delirium intervention strategies because current evidence is completely lacking for ED-based delirium prevention or treatment,” they said. In the meantime, developing outcome measures for quality improvement of delirium care will require institutional support as well as education.
Geriatric patients and falls
Approximately one third of community-dwelling adults older than 65 years suffer falls, but data suggest that fewer than half of these individuals report falls to their doctors. “Older adults who present to an ED after a fall have an approximately 30% greater risk of functional decline and depression at 6 months after the event,” the authors noted.
The GED guidelines call for a comprehensive approach to evaluating and managing falls in older adults, but many of these “are untested in the ED,” the authors said. The recommended protocol includes an initial assessment of fall risk, followed by, for those at low risk, tailored recommendations for education and the use of community resources. Additional recommendations for those at high risk of falls include multifactorial assessment of modifiable risk factors, including peripheral neuropathy, balance/gait assessment, and medication review.
However, this best practice workflow is beyond the resource capacity of most EDs, the authors noted. “When ED resources are insufficient to support best practices, the care should focus on educating patients and caregivers about the significance of a fall event, providing educational materials (e.g., [the Centers for Disease Control and Prevention’s] STEADI materials), and assessing safety with respect to mobility for immediate return to the home environment and follow-up with a PCP.”
Geriatric patients and polypharmacy
Polypharmacy is common among older adults by virtue of their greater number of illnesses and comorbid conditions, and polypharmacy also has been associated with more adverse drug reactions, the authors said. The AGS Beers Criteria identifies medications associated with adverse drug reactions, but it is not practical for use in a busy ED setting. Instead, the authors suggested a more practical approach of focusing on a smaller list of common medications that tend to cause the adverse events that may result in ED visits.
“Perhaps targeting patients on multiple (three or more) psychoactive medications, drugs that can cause hypotension, or hypoglycemics could not only be done quickly, but identify patients in whom deprescribing should be considered in the ED,” the authors wrote. Deprescribing is a complicated process, however, and may be more effective when done via the patient’s primary care provider or in a geriatric consultation.
The GED Guidelines highlighted the specific needs of the geriatric population in the ED, the authors said. Widespread implementation remains a challenge, but many organizations provide resources to help improve care of geriatric patients in the ED and beyond.
In particular, the Geriatric Emergency Care Applied Research Network and Geriatric Emergency Department Collaborative provide funding opportunities, updated and focused published reviews, and webinars (some including free continuing medical education) for the entire health care team, including hospital administrators, the authors said.
Article brings attention to clinical realities
“The reality is that the overwhelming majority of emergency departments in the United States, if not globally, are simply not equipped – operationally or financially – to meet the rigorous standards that are required to fulfill the goals of operating an accredited geriatric ED,” Robert D. Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, said in an interview.
“Drawing attention to this important gap in accreditation is critical to not only inform hospitals, health care providers and stakeholders, but the public, patients, and their families about the important work that needs to be done to better equip all EDs with the proper tools and educational approaches to more effectively care for the geriatric community,” Dr. Glatter emphasized.
“There are currently three tiers of accreditation, with level 1 being the highest,” he explained, but there are only 100 geriatric ED accreditation-certified hospitals across the United States.
“I am not surprised at all by the challenges of implementing current GED guidelines,” said Dr. Glatter. “It comes down to operational and budget considerations, which ultimately compete with many other departments and regulatory constraints in any given hospital.”
However, “the bottom line is that such guidelines are designed with patient safety in mind, making them important issues in the eyes of any hospital administrator looking to improve outcomes and reduce medicolegal risk or exposure impacting geriatric patients in the emergency department,” he noted.
Ultimately, guideline adherence “comes down to budget decisions, and where hospitals must invest their money to meet the bottom line,” said Dr. Glatter. “Making modifications to hospital infrastructure and architecture to accommodate geriatric patients may not be the top priority of hospital administrators when confronted with multiple competing interests. But, if it impacts patient safety, the decision to invest in structural and operational improvements may certainly have additional and important considerations.
“Until Medicare, or even the Joint Commission on Accreditation of Hospitals, adopts geriatric guidelines in emergency departments as a requirement for accreditation, there may not be adequate incentives in place currently to satisfy the intent of having a rigorous set of guidelines in the first place,” Dr. Glatter added.
Despite the limitations of applying the current guidelines, there are some steps hospitals can take, said Dr. Glatter. “They can institute new measures in a graded fashion, with the goal of taking the important steps to satisfy at least some components of the guidelines. Attention to details can go a long way, such as rails in bathrooms, better lighting, and treads on floors that may reduce the risk of falls in the ED itself.
“Attention to fall prevention by assessing contributors including polypharmacy, gait instability, and quality of footwear can impact risk of future ED visits. Having incentives in place by Medicare or JACO may force the hand of hospital administrators to comply with geriatric guidelines and place emphasis on compliance,” noted Dr. Glatter.
More research is needed that “looks at costs of implementing geriatric guidelines in typical community and academic EDs and how this impacts key metrics such as length of stay, effect on reimbursement per ICD-10 code, and savings, if any, realized in reduced malpractice claims related to missed diagnoses (such as delirium), injuries, (patient falls), or medical misadventures due to polypharmacy,” he said.
The article received no outside funding. The authors disclosed no relevant financial relationships. Dr. Glatter disclosed no relevant financial relationships, and serves on the advisory board of Medscape Emergency Medicine.
A version of this article first appeared on Medscape.com.
Many emergency departments are currently unable to provide care for geriatric patients that meets best practices and guidelines recommended by several major medical organizations, but a panel discussion in 2021 at the American Academy of Emergency Medicine’s Scientific Assembly identified three areas in which realistic improvements might be achieved.
In an article published online in the Journal of Emergency Medicine, Richard D. Shih, MD, of Florida Atlantic University, Boca Raton, and colleagues synthesized the presentation and discussion of an expert panel on the topic of the GED guidelines and the current realities of patient care.
The Geriatric Emergency Department (GED) Guidelines, published in 2014 in Annals of Emergency Medicine, were endorsed by the American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association, and Society for Academic Emergency Medicine.
“With the substantial challenges in providing guideline-recommended care in EDs, this article will explore three high-impact GED clinical conditions to highlight guideline recommendations, challenges, and opportunities, and discuss realistically achievable expectations for non–GED-accredited institutions,” the authors wrote.
Geriatric patients and delirium
When delirium in older adults is not identified in the ED, the patient’s 6-month mortality rate significantly increases, but few EDs have delirium screening protocols, the authors said. Challenges included the time and money needed to educate staff, on top of multiple mandatory training requirements on other topics. Delirium screening in the clinical setting also requires personnel to conduct assessments, and time to document symptoms and screening results in medical records.
“Perhaps the highest priority challenge for delirium experts is to evaluate and publish effective delirium intervention strategies because current evidence is completely lacking for ED-based delirium prevention or treatment,” they said. In the meantime, developing outcome measures for quality improvement of delirium care will require institutional support as well as education.
Geriatric patients and falls
Approximately one third of community-dwelling adults older than 65 years suffer falls, but data suggest that fewer than half of these individuals report falls to their doctors. “Older adults who present to an ED after a fall have an approximately 30% greater risk of functional decline and depression at 6 months after the event,” the authors noted.
The GED guidelines call for a comprehensive approach to evaluating and managing falls in older adults, but many of these “are untested in the ED,” the authors said. The recommended protocol includes an initial assessment of fall risk, followed by, for those at low risk, tailored recommendations for education and the use of community resources. Additional recommendations for those at high risk of falls include multifactorial assessment of modifiable risk factors, including peripheral neuropathy, balance/gait assessment, and medication review.
However, this best practice workflow is beyond the resource capacity of most EDs, the authors noted. “When ED resources are insufficient to support best practices, the care should focus on educating patients and caregivers about the significance of a fall event, providing educational materials (e.g., [the Centers for Disease Control and Prevention’s] STEADI materials), and assessing safety with respect to mobility for immediate return to the home environment and follow-up with a PCP.”
Geriatric patients and polypharmacy
Polypharmacy is common among older adults by virtue of their greater number of illnesses and comorbid conditions, and polypharmacy also has been associated with more adverse drug reactions, the authors said. The AGS Beers Criteria identifies medications associated with adverse drug reactions, but it is not practical for use in a busy ED setting. Instead, the authors suggested a more practical approach of focusing on a smaller list of common medications that tend to cause the adverse events that may result in ED visits.
“Perhaps targeting patients on multiple (three or more) psychoactive medications, drugs that can cause hypotension, or hypoglycemics could not only be done quickly, but identify patients in whom deprescribing should be considered in the ED,” the authors wrote. Deprescribing is a complicated process, however, and may be more effective when done via the patient’s primary care provider or in a geriatric consultation.
The GED Guidelines highlighted the specific needs of the geriatric population in the ED, the authors said. Widespread implementation remains a challenge, but many organizations provide resources to help improve care of geriatric patients in the ED and beyond.
In particular, the Geriatric Emergency Care Applied Research Network and Geriatric Emergency Department Collaborative provide funding opportunities, updated and focused published reviews, and webinars (some including free continuing medical education) for the entire health care team, including hospital administrators, the authors said.
Article brings attention to clinical realities
“The reality is that the overwhelming majority of emergency departments in the United States, if not globally, are simply not equipped – operationally or financially – to meet the rigorous standards that are required to fulfill the goals of operating an accredited geriatric ED,” Robert D. Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, said in an interview.
“Drawing attention to this important gap in accreditation is critical to not only inform hospitals, health care providers and stakeholders, but the public, patients, and their families about the important work that needs to be done to better equip all EDs with the proper tools and educational approaches to more effectively care for the geriatric community,” Dr. Glatter emphasized.
“There are currently three tiers of accreditation, with level 1 being the highest,” he explained, but there are only 100 geriatric ED accreditation-certified hospitals across the United States.
“I am not surprised at all by the challenges of implementing current GED guidelines,” said Dr. Glatter. “It comes down to operational and budget considerations, which ultimately compete with many other departments and regulatory constraints in any given hospital.”
However, “the bottom line is that such guidelines are designed with patient safety in mind, making them important issues in the eyes of any hospital administrator looking to improve outcomes and reduce medicolegal risk or exposure impacting geriatric patients in the emergency department,” he noted.
Ultimately, guideline adherence “comes down to budget decisions, and where hospitals must invest their money to meet the bottom line,” said Dr. Glatter. “Making modifications to hospital infrastructure and architecture to accommodate geriatric patients may not be the top priority of hospital administrators when confronted with multiple competing interests. But, if it impacts patient safety, the decision to invest in structural and operational improvements may certainly have additional and important considerations.
“Until Medicare, or even the Joint Commission on Accreditation of Hospitals, adopts geriatric guidelines in emergency departments as a requirement for accreditation, there may not be adequate incentives in place currently to satisfy the intent of having a rigorous set of guidelines in the first place,” Dr. Glatter added.
Despite the limitations of applying the current guidelines, there are some steps hospitals can take, said Dr. Glatter. “They can institute new measures in a graded fashion, with the goal of taking the important steps to satisfy at least some components of the guidelines. Attention to details can go a long way, such as rails in bathrooms, better lighting, and treads on floors that may reduce the risk of falls in the ED itself.
“Attention to fall prevention by assessing contributors including polypharmacy, gait instability, and quality of footwear can impact risk of future ED visits. Having incentives in place by Medicare or JACO may force the hand of hospital administrators to comply with geriatric guidelines and place emphasis on compliance,” noted Dr. Glatter.
More research is needed that “looks at costs of implementing geriatric guidelines in typical community and academic EDs and how this impacts key metrics such as length of stay, effect on reimbursement per ICD-10 code, and savings, if any, realized in reduced malpractice claims related to missed diagnoses (such as delirium), injuries, (patient falls), or medical misadventures due to polypharmacy,” he said.
The article received no outside funding. The authors disclosed no relevant financial relationships. Dr. Glatter disclosed no relevant financial relationships, and serves on the advisory board of Medscape Emergency Medicine.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF EMERGENCY MEDICINE
Dupilumab shows histological and clinical benefit in larger eosinophilic esophagitis cohort
The late-breaking data on Part B of the LIBERTY EoE TREET study drew a standing-room-only crowd at the American Academy of Allergy, Asthma and Immunology (AAAAI) annual meeting.
EoE is a chronic, progressive, type 2 inflammatory disease resulting from esophageal build-up of eosinophils, which injures the tissue and leads to swallowing difficulties. Dupilumab, a monoclonal antibody that blocks type 2 immune responses, is currently approved to treat poorly controlled atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.
Dupilumab also showed benefits in patients with hard-to-treat EoE in a phase 3 trial (LIBERTY EoE TREET 28-week extension of Part A), reported by Medscape Medical News in October from the American College of Gastroenterology (ACG) annual meeting.
Part B enrolled 159 EoE patients 12 years or older and tested the efficacy and safety of weekly 300 mg dupilumab versus placebo injections for 24 weeks. More than half of the participants had previously tried swallowed topical corticosteroids, and about 30% were on a food elimination diet. (Generally, corticosteroids and elimination diets are about 70% effective in EoE.)
Compared with placebo, 6 months of weekly dupilumab reduced eosinophils in the esophagus and produced statistically significant and clinically meaningful improvements in the ability to swallow.
Treated participants saw a 64% reduction in disease symptoms (23.8-point improvement on the self-reported Dysphagia Symptom Questionnaire [DSQ]), compared with 41% reduction (13.9 point DSQ improvement) in the placebo group.
Histologically, dupilumab reduced peak eosinophil counts to 6 or lower in 59% of patients, whereas only 6% achieved disease remission on placebo.
On safety, dupilumab was generally well tolerated. The most common treatment adverse events were injection site reactions (occurring in about 20% of both groups) or injection site erythema (occurring in 10% of treated patients and 11.5% of placebo patients).
“These results replicate those in Part A in a larger sample size,” Marc Rothenberg, MD, PhD, director of the division of allergy and immunology at Cincinnati Children’s Hospital Medical Center, noted in a prerecorded presentation.
Based on the phase 3 data, dupilumab seems “effective for patients who may have no other options for managing their EoE,” Brian Schroer, MD, director of allergy and immunology at Akron (Ohio) Children’s Hospital, said in an interview. Dr. Schroer expects EoE cases to rise as more food allergy patients begin oral immunotherapy (OIT), where studies have shown EoE as a side effect in about 4% of patients undergoing OIT.
In a live Q&A following the prerecorded talk, Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, told attendees that data from Part B’s second arm, which tested dupilumab injections given every other week, have not yet been presented. So far, histological results in this arm look identical to those of patients who received weekly dupilumab, though symptoms “did not meet statistical significance,” he said. “I think we’re going to have much more detail about those results at some conferences to come in the spring.”
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon and Dr. Rothenberg reported numerous conflicts of interest. Dr. Schroer has received consulting fees from Sanofi and Ready, Set, Food.
A version of this article first appeared on Medscape.com.
The late-breaking data on Part B of the LIBERTY EoE TREET study drew a standing-room-only crowd at the American Academy of Allergy, Asthma and Immunology (AAAAI) annual meeting.
EoE is a chronic, progressive, type 2 inflammatory disease resulting from esophageal build-up of eosinophils, which injures the tissue and leads to swallowing difficulties. Dupilumab, a monoclonal antibody that blocks type 2 immune responses, is currently approved to treat poorly controlled atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.
Dupilumab also showed benefits in patients with hard-to-treat EoE in a phase 3 trial (LIBERTY EoE TREET 28-week extension of Part A), reported by Medscape Medical News in October from the American College of Gastroenterology (ACG) annual meeting.
Part B enrolled 159 EoE patients 12 years or older and tested the efficacy and safety of weekly 300 mg dupilumab versus placebo injections for 24 weeks. More than half of the participants had previously tried swallowed topical corticosteroids, and about 30% were on a food elimination diet. (Generally, corticosteroids and elimination diets are about 70% effective in EoE.)
Compared with placebo, 6 months of weekly dupilumab reduced eosinophils in the esophagus and produced statistically significant and clinically meaningful improvements in the ability to swallow.
Treated participants saw a 64% reduction in disease symptoms (23.8-point improvement on the self-reported Dysphagia Symptom Questionnaire [DSQ]), compared with 41% reduction (13.9 point DSQ improvement) in the placebo group.
Histologically, dupilumab reduced peak eosinophil counts to 6 or lower in 59% of patients, whereas only 6% achieved disease remission on placebo.
On safety, dupilumab was generally well tolerated. The most common treatment adverse events were injection site reactions (occurring in about 20% of both groups) or injection site erythema (occurring in 10% of treated patients and 11.5% of placebo patients).
“These results replicate those in Part A in a larger sample size,” Marc Rothenberg, MD, PhD, director of the division of allergy and immunology at Cincinnati Children’s Hospital Medical Center, noted in a prerecorded presentation.
Based on the phase 3 data, dupilumab seems “effective for patients who may have no other options for managing their EoE,” Brian Schroer, MD, director of allergy and immunology at Akron (Ohio) Children’s Hospital, said in an interview. Dr. Schroer expects EoE cases to rise as more food allergy patients begin oral immunotherapy (OIT), where studies have shown EoE as a side effect in about 4% of patients undergoing OIT.
In a live Q&A following the prerecorded talk, Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, told attendees that data from Part B’s second arm, which tested dupilumab injections given every other week, have not yet been presented. So far, histological results in this arm look identical to those of patients who received weekly dupilumab, though symptoms “did not meet statistical significance,” he said. “I think we’re going to have much more detail about those results at some conferences to come in the spring.”
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon and Dr. Rothenberg reported numerous conflicts of interest. Dr. Schroer has received consulting fees from Sanofi and Ready, Set, Food.
A version of this article first appeared on Medscape.com.
The late-breaking data on Part B of the LIBERTY EoE TREET study drew a standing-room-only crowd at the American Academy of Allergy, Asthma and Immunology (AAAAI) annual meeting.
EoE is a chronic, progressive, type 2 inflammatory disease resulting from esophageal build-up of eosinophils, which injures the tissue and leads to swallowing difficulties. Dupilumab, a monoclonal antibody that blocks type 2 immune responses, is currently approved to treat poorly controlled atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.
Dupilumab also showed benefits in patients with hard-to-treat EoE in a phase 3 trial (LIBERTY EoE TREET 28-week extension of Part A), reported by Medscape Medical News in October from the American College of Gastroenterology (ACG) annual meeting.
Part B enrolled 159 EoE patients 12 years or older and tested the efficacy and safety of weekly 300 mg dupilumab versus placebo injections for 24 weeks. More than half of the participants had previously tried swallowed topical corticosteroids, and about 30% were on a food elimination diet. (Generally, corticosteroids and elimination diets are about 70% effective in EoE.)
Compared with placebo, 6 months of weekly dupilumab reduced eosinophils in the esophagus and produced statistically significant and clinically meaningful improvements in the ability to swallow.
Treated participants saw a 64% reduction in disease symptoms (23.8-point improvement on the self-reported Dysphagia Symptom Questionnaire [DSQ]), compared with 41% reduction (13.9 point DSQ improvement) in the placebo group.
Histologically, dupilumab reduced peak eosinophil counts to 6 or lower in 59% of patients, whereas only 6% achieved disease remission on placebo.
On safety, dupilumab was generally well tolerated. The most common treatment adverse events were injection site reactions (occurring in about 20% of both groups) or injection site erythema (occurring in 10% of treated patients and 11.5% of placebo patients).
“These results replicate those in Part A in a larger sample size,” Marc Rothenberg, MD, PhD, director of the division of allergy and immunology at Cincinnati Children’s Hospital Medical Center, noted in a prerecorded presentation.
Based on the phase 3 data, dupilumab seems “effective for patients who may have no other options for managing their EoE,” Brian Schroer, MD, director of allergy and immunology at Akron (Ohio) Children’s Hospital, said in an interview. Dr. Schroer expects EoE cases to rise as more food allergy patients begin oral immunotherapy (OIT), where studies have shown EoE as a side effect in about 4% of patients undergoing OIT.
In a live Q&A following the prerecorded talk, Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, told attendees that data from Part B’s second arm, which tested dupilumab injections given every other week, have not yet been presented. So far, histological results in this arm look identical to those of patients who received weekly dupilumab, though symptoms “did not meet statistical significance,” he said. “I think we’re going to have much more detail about those results at some conferences to come in the spring.”
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon and Dr. Rothenberg reported numerous conflicts of interest. Dr. Schroer has received consulting fees from Sanofi and Ready, Set, Food.
A version of this article first appeared on Medscape.com.
REPORTING FROM AAAAI
An Academic Hospitalist–Run Outpatient Paracentesis Clinic
Cirrhosis is the most common cause of ascites in the United States. In patients with compensated cirrhosis, the 10-year probability of developing ascites is 47%. Developing ascites portends a poor prognosis. Fifteen percent of patients who receive this diagnosis die within 1 year, and 44% within 5 years.1 First-line treatment of cirrhotic ascites consists of dietary sodium restriction and diuretic therapy. Refractory ascites is defined as ascites that cannot be easily mobilized despite adhering to a dietary sodium intake of ≤ 2 g daily and daily doses of spironolactone 400 mg and furosemide 160 mg.
Patients who cannot tolerate diuretics because of complications are defined as having diuretic intractable ascites. Diuretic-induced complications include hepatic encephalopathy, renal impairment, hyponatremia, and hypo- or hyperkalemia. Because these patients are either unresponsive to or intolerant of diuretics, second-line treatments, such as regular large-volume paracentesis (LVP) or the insertion of a transjugular intrahepatic portosystemic shunt (TIPS) are needed to manage their ascites. These patients also should be considered for liver transplantation unless there is a contraindication.2
Serial LVP has been shown to be safe and effective in controlling refractory ascites.3 TIPS will decrease the need for repeated LVP in patients with refractory LVP. However, given the uncertainty as to the effect of TIPS creation on survival and the increased risk of encephalopathy, the American Association for the Study of Liver Diseases (AASLD) recommends that TIPS should be used only in those patients who cannot tolerate repeated LVP.4 Repeated LVP also has been shown to be safe and effective in controlling malignant ascites.5,6
LVP can be done in different health care settings. These include the emergency department (ED), interventional radiology suite, inpatient bed, or an outpatient paracentesis clinic. There have been various descriptions of outpatient paracentesis clinics. Reports from the United Kingdom have revealed that paracenteses in these outpatient clinics can be performed safely by nurse practitioners or a liver specialist nurse, that these clinics are highly rated by the patients, and are cost effective.7-10 Gashau and colleagues describe a clinic in Great Britain run by gastroenterology (GI) fellows using an endoscopy suite.11 A nurse practitioner outpatient paracentesis clinic in the US has been described as well.12 Grabau and colleagues present a clinic run by GI endoscopy assistants (licensed practical nurses) using a dedicated paracentesis room in the endoscopy suite.13 Cheng and colleagues describe an outpatient paracentesis clinic in a radiology department run by a single advanced practitioner with assistance from an ultrasound technologist.14 Wang and colleagues present outpatient paracenteses in an outpatient transitional care program by a physician or an advanced practitioner supervised by a physician.15 Sehgal and colleagues describe (in abstract) the creation of a hospitalist-run paracentesis clinic.16
Traditionally, at Veterans Affairs Pittsburgh Healthcare System (VAPHS) in Pennsylvania, if a patient needed LVP, they were admitted to a medicine bed. LVP is not done in the ED, and interventional radiology cannot accommodate the number of patients requiring LVP because of their caseload. The procedure was done by an attending hospitalist or medical residents under the supervision of an attending hospitalist. To improve patient flow and decrease the number of patients using inpatients beds, we created an outpatient paracentesis clinic in 2014. Here, we present the logistics of the clinic, patient demographics, the amount of ascites removed, and the time required to remove the ascites. As part of ongoing quality assurance, we keep track of any complications and report these as well.
Methods
The setting of the outpatient paracentesis clinic is a room in the VAPHS endoscopy suite. The clinic operates 1 half-day per week with up to 3 patients receiving a paracentesis. We use the existing logistics in the endoscopy suite. There are 1 or 2 registered nurses (RNs) who assist the physician performing the paracentesis. The proceduralist is an academic hospitalist who at the time is not on service with residents. The patients are referred to the clinic by the ED, hepatology clinic, palliative care, primary care physicians, or at hospital discharge. In the clinic consult, patients are required to have at least an estimated 3 L of ascites and systolic blood pressure (SBP) ≥ 90. The patients can eat and take medications the morning of the procedure except diuretics. Patients are checked in to the endoscopy suite and a peripheral IV is placed. Blood tests, such as a complete blood count and coagulation studies, are not checked routinely since the AASLD guidelines state that routine prophylactic use of fresh frozen plasma or platelets before paracentesis is not recommended because bleeding is uncommon.3 The proceduralist can order blood work at their discretion.
After the procedure, patients are brought to the recovery area of the endoscopy suite and discharged. The patients are discharged usually within 15 to 30 minutes from arriving in the recovery area after it is assured that the SBP is within 10% of their baseline. Patient follow-up in the outpatient paracentesis clinic is determined by the proceduralist. Most patients need regularly scheduled paracenteses depending on how quickly they reaccumulate ascites. If a patient does not need a regularly scheduled paracentesis, the proceduralist ensures that the appropriate outpatient clinic visit has been scheduled or requested.
Procedure
Informed consent is obtained, and a time-out is performed before each paracentesis. The patient is attached to a cardiac monitor and pulse oximetry as per the endoscopy suite protocol. The proceduralist does a point-of-care ultrasound to find the optimal site and marks the site of puncture. The skin around the marked site is prepared with 3 chlorhexidine gluconate 2%/isopropyl alcohol 70% applicators. A fenestrated drape is used to form a sterile field. The Avanos Paracentesis Kit is routinely used for LVP at VAPHS. Local anesthesia with 1% lidocaine is used with a 25-gauge × 1-inch needle. Deeper anesthesia is obtained with 1% lidocaine, using a 22-gauge × 1.5-inch needle, injecting and aspirating while advancing the needle until ascites is aspirated.
A 15-gauge 3.3-inch Caldwell cannula with an inner needle is inserted into the peritoneal cavity and ascites is aspirated into a syringe. The inner needle is then removed, and the Caldwell cannula is left in the peritoneal cavity and tubing with a roller clamp is attached to the cannula. The tubing is then attached to a 1-L vacuum suction bottle by the RN. We use the CareFusion PleurX drainage bottle. The proceduralist maintains sterility and assures the cannula remains in place. The RN changes the drainage bottles after being filled with 1 L of ascites.
We drain as much ascites as possible until drainage stops on its own. The cannula is then removed, and pressure is held with a gauze pad. An adhesive bandage is then placed over the site. Consistent with AASLD guideline, 25 g of IV albumin 25% is infused for every 3 L of albumin removed provided > 5 L of ascites is removed.3 The albumin is infused during the procedure and not after to limit the time of the procedure. A sample of ascites is sent for cell count with differential and culture.
Results
Between March 2014 and May 2020, 506 paracenteses were performed on 82 patients. The mean age was 66.4 years, and 80 of 82 patients were male. The etiology of the ascites is presented in the Table. Twelve percent of the patients had concomitant hepatocellular carcinoma. Data on the amount of ascites removed were available for all patients, but data on the amount of time it took to do the LVP were available for 392 of 506 paracenteses. The mean volume removed was 7.9 L (range, 0.2-22.9 L), and the mean time of the procedure was 33.3 minutes. The time of the procedure was the time difference between entering and leaving the procedure room. This does not include IV placement or the recovery area time.
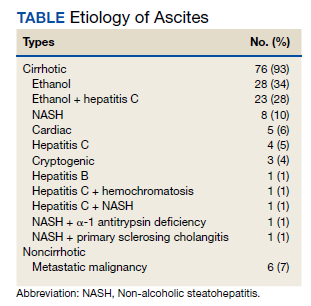
There were 5 episodes of postprocedure hypotension that required IV fluid or admission. In all these events, the patients had received the appropriate amount of IV albumin. Three patients required admission, and 1 patient required IV fluid postparacentesis on 2 occasions and then was discharged home. One abdominal wall hematoma occurred. Two patients with umbilical hernias developed incarceration after the paracentesis; both required surgical repair. There were 3 episodes of leakage at the paracentesis site; a skin adhesive was used in 2 cases, and sutures were applied in the other. There were no deaths.
Possible Infections
Ascitic fluid infection is a risk for patients needing paracentesis. Spontaneous bacterial peritonitis (SBP) is a bacterial infection of ascites in the absence of a focal contiguous source. The polymorphonuclear leukocyte (PMN) count in the ascites is ≥ 250 cells/mm3 in the presence of a single organism on culture. Culture-negative neutrocytic ascites (CNNA) is an ascitic fluid PMN count ≥ 250 cells/mm3 in the absence of culture growth obtained before the administration of antibiotics. Monomicrobial nonneutrocytic bacterascites (MNB) is an ascitic fluid PMN count < 250 cells/mm3 with growth of a single organism on culture.17 There was one occasion where a patient developed symptomatic CNNA 3 days after having a therapeutic paracentesis in the clinic at which time his ascites had a normal neutrophil count and a negative culture. He presented with abdominal pain and fever 3 days later, and a diagnostic paracentesis was done in the ED. He was treated as though he had SBP and did well.
Ascites cell count and culture are routinely sent in the clinic, and 1 case of asymptomatic SBP and 3 cases of asymptomatic ascitic fluid infection variants were diagnosed. The patient with SBP grew vancomycin-resistant Enterococcus faecium in his ascites. Two cases were CNNA. These patients were admitted to the hospital and treated with IV antibiotics. One case of MNB occurred that grew Escherichia coli. The patient refused to return to the hospital for IV antibiotics and was treated with a 5-day course of oral ciprofloxacin.
Discussion
We describe an academic hospitalist–run outpatient LVP clinic where large volumes of ascites are removed efficiently and safely. The only other description of a hospitalist-run paracentesis clinic was in abstract form.16 Without the clinic, the patients would have been admitted to the hospital to get an LVP. Based on VAPHS data from fiscal year 2021, the average cost per day of a nontelemetry medicine admission was $3394. Over 74 months, 506 admissions were prevented, which averages to 82 admissions prevented per year, an approximate annual cost savings of $278,308 in the last fiscal year alone.
Possible Complications
The complications we report are congruent with those reported in the literature. Runyon reported that the rate of an abdominal wall hematoma requiring blood transfusion was 0.9%, and the rate of an abdominal wall hematoma not requiring blood transfusion was also 0.9%.18 We had 1 patient who developed an abdominal wall hematoma (0.2% of paracenteses). This patient required 4 units of packed red blood cells. The incidence of ascitic fluid leakage after paracentesis has been reported to be between 0.4% and 2.4%.12 We had 3 episodes of leakage (0.6% of paracenteses). The Z-track technique has been purported to decrease postparacentesis leakage.2 This involves creating a pathway that is nonlinear when anesthetizing the soft tissues and inserting the paracentesis needle. The Z-track technique was not used in any of the paracenteses in our clinic.
Postparacentesis hypotension has been reported to be 0.4% to 1.8%.12,14 We report 5 episodes of hypotension (0.1% of paracenteses) of which 3 patients were admitted to the hospital. Interestingly, 4 of the 5 patients were on β-blockers. Serste and colleagues reported in a crossover trial that paracentesis-induced circulatory dysfunction (PICD) decreased from 80 to 10% when propranolol was discontinued.19 PICD is characterized by reduction of effective arterial blood volume with subsequent activation of vasoconstrictor and antinatriuretic factors that can cause rapid ascites recurrence rate, development of dilutional hyponatremia, hepatorenal syndrome, and increased mortality. IV albumin is given during LVP to prevent PICD. Discontinuing unnecessary antihypertensive medications, especially β-blockers, may mitigate postparacentesis hypotension. In a study of 515 paracenteses, De Gottardi and colleagues reported a 0.2% rate of iatrogenic percutaneous infection of ascites.20 We had 1 patient return 3 days after LVP with fever, abdominal pain, and neutrocytic ascites. His blood and ascites cultures were negative. The etiology of his infected ascites could have been either a spontaneously developed CNNA infection or an iatrogenic percutaneous infection of ascites.
Two cases of incarceration and strangulation of umbilical hernias postparacentesis that required emergent surgical intervention were unanticipated complications. Incarceration of an existing umbilical hernia postparacentesis is an uncommon but serious complication of LVP described in the past in numerous case reports but whose incidence is otherwise unknown.21-26 The fluid and pressure shifts before and after LVP are likely responsible for the hernia incarceration. When ascites is present, the umbilical hernia ring is kept patent by the pressure of the ascitic fluid, and the decrease in tension after removal of ascites may lead to decreased size of the hernia ring and trapping of contents in the hernia sac.25-27 In most reported cases, symptoms and recognition of the incarcerated hernia have occurred within 2 days of the index paracentesis procedure. Most cases were in patients who required serial paracenteses for management of ascites and had relatively regular LVPs.
In both cases, the patients had regular visits for paracentesis, and incarceration occurred 0.5 hours postprocedure, in 1 case and 6 hours in the other. Umbilical hernias are common in patients with cirrhosis, with the prevalence approaching 20%.28 The management of umbilical hernias in patients with ascites is complex and optimal guideline-based management involves elective repair when ascites is adequately controlled to prevent recurrence, with consideration of TIPS at the time of repair.3 However, patients enrolled in outpatient paracentesis clinics are unlikely to have adequate ascites control to be considered optimized for an elective repair. In addition, given the number of serial procedures that they require, it is not surprising that they may be at risk for complications that are otherwise thought to be rare. Although incarceration and strangulation of umbilical hernia is thought to be a rare complication of LVP, patients should be informed of this potential complication so that they are aware to seek medical attention should they develop signs or symptoms.
Guidelines
There are no guidelines on how much ascites can be removed and how quickly the ascites can be removed during LVP. The goal of a therapeutic paracentesis is to remove as much fluid as possible, and there are no limits on the amount that can be removed safely.1 Concerning paracentesis flow rates, Elsabaawy and colleagues showed that ascites flow rate does not correlate with PICD. They looked at 3 groups with ascites flow rates of 80 mL/min, 180 mL/min and 270 mL/min.29 We had data on the time in the procedure room in 77% of our procedures. Given our average amount of ascites removed (7.9 L) and average time in the procedure room (33.3 minutes), the average flow rate from our clinic was at least 237 mL/min (although the flow rate was likely higher because the average time from needle inserted to needle removed was < 33.3 minutes). Both the mean duration of LVP and the mean volume of ascites removed in an outpatient paracentesis clinic were reported in only 1 other study. In a study of 1100 patients, Grabau and colleagues reported the mean duration, defined as the time between when the patient entered and exited the procedure room (the same time period we reported) as 97 minutes and the mean volume of ascites removed as 8.7 L.13
The AASLD guidelines state that patients undergoing serial outpatient LVP should be tested only for cell count and differential without sending a bacterial culture. The reason given is that false positives may exceed true positives from ascites bacterial culture results in asymptomatic patients.3 Mohan and Venkataraman reported a 0.4% rate of SBP, 1.4% rate of CNNA, and 0.7% rate of MNB in asymptomatic patients undergoing LVP in an outpatient clinic.30 We had a 0.2% rate of SBP, 0.4% rate of CNNA, and 0.2% rate of MNB. Given the low rates of SBP in outpatient paracenteses clinics, we will adopt the AASLD suggestions to only send an ascites cell count and not a culture in asymptomatic patients. Noteworthy, our patient with asymptomatic SBP grew vancomycin-resistant Enterococcus faecium, which was resistant to standard SBP antibiotic therapy. However, if ascites culture was not sent, he would have been treated with antibiotics for CNNA, and if he developed symptoms, he would have had a repeat paracentesis with cell count and culture sent.
Training
In 2015, faculty at VAPHS and the University of Pittsburgh School of Medicine designed a Mastering Paracentesis for Medical Residents course based on current guidelines on the management of ascites and published procedural guides. The course is mandatory for all postgraduate year-1 internal medicine residents and begins with 2 hours of didactic and simulation-based training with an ultrasound-compatible paracentesis mannequin. In the 3 weeks following simulation-based training, residents rotate through our outpatient paracentesis clinic and perform between 1 and 3 abdominal paracentesis procedures, receiving as-needed coaching and postprocedure feedback from faculty. Since the course’s inception, more than 150 internal medicine residents have been trained in paracentesis through our clinic.
Conclusions
We present a description of a successful outpatient paracentesis clinic at our hospital run by academic hospitalists. The clinic was created to decrease the number of admissions for LVP. We were fortunate to be able to use the GI endoscopy suite and their resources as the clinic setting. To create outpatient LVP clinics at other institutions, administrative support is essential. In conclusion, we have shown that an outpatient paracentesis clinic run by academic hospitalists can safely and quickly remove large volumes of ascites.
1. Ge PS, Runyon BA. Treatment of patients with cirrhosis. N Engl J Med. 2016;375(8):767-777. doi:10.1056/NEJMra1504367
2. Wong F. Management of ascites in cirrhosis. J Gastroenterol Hepatol. 2012;27(1):11-20. doi:10.1111/j.1440-1746.2011.06925.x
3. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359
4. Boyer TD, Haskal ZJ; American Association for the Study of Liver Diseases. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension: update 2009. Hepatology. 2010;51(1):306. doi:10.1002/hep.23383
5. Harding V, Fenu E, Medani H, et al. Safety, cost-effectiveness and feasibility of daycase paracentesis in the management of malignant ascites with a focus on ovarian cancer. Br J Cancer. 2012;107(6):925-930. doi:10.1038/bjc.2012.343
6. Korpi S, Salminen VV, Piili RP, Paunu N, Luukkaala T, Lehto JT. Therapeutic procedures for malignant ascites in a palliative care outpatient clinic. J Palliat Med. 2018;21(6):836-841. doi:10.1089/jpm.2017.0616
7. Vaughan J. Developing a nurse-led paracentesis service in an ambulatory care unit. Nurs Stand. 2013;28(4):44-50. doi:10.7748/ns2013.09.28.4.44.e7751
8. Menon S, Thompson L-S, Tan M, et al. Development and cost-benefit analysis of a nurse-led paracentesis and infusion service. Gastrointestinal Nursing. 2016;14(9):32-38. doi:10.12968/gasn.2016.14.9.32
9. Hill S, Smalley JR, Laasch H-U. Developing a nurse-led, day-case, abdominal paracentesis service. Cancer Nursing Practice. 2013;12(5):14-20. doi:10.7748/cnp2013.06.12.5.14.e942
10. Tahir F, Hollywood C, Durrant D. PWE-134 Overview of efficacy and cost effectiveness of nurse led day case abdominal paracentesis service at Gloucestershire Hospital NHS Foundation Trust. Gut. 2014;63(suppl 1):A183.2-A183. doi:10.1136/gutjnl-2014-307263.394
11. Gashau W, Samra G, Gasser J, Rolland M, Sambaiah P, Shorrock C. PTH-075 “ascites clinic”: an outpatient service model for patients requiring large volume paracentesis. Gut. 2014;63(suppl 1):A242.2-A242. doi:10.1136/gutjnl-2014-307263.521
12. Gilani N, Patel N, Gerkin RD, Ramirez FC, Tharalson EE, Patel K. The safety and feasibility of large volume paracentesis performed by an experienced nurse practitioner. Ann Hepatol. 2009;8(4):359-363.
13. Grabau CM, Crago SF, Hoff LK, et al. Performance standards for therapeutic abdominal paracentesis. Hepatology. 2004;40(2):484-488. doi:10.1002/hep.20317
14. Cheng YW, Sandrasegaran K, Cheng K, et al. A dedicated paracentesis clinic decreases healthcare utilization for serial paracenteses in decompensated cirrhosis. Abdom Radiol (NY). 2018;43(8):2190-2197. doi:10.1007/s00261-017-1406-y
15. Wang J, Khan S, Wyer P, et al. The role of ultrasound-guided therapeutic paracentesis in an outpatient transitional care program: a case series. Am J Hosp Palliat Care. 2018;35(9):1256-1260. doi:10.1177/1049909118755378
16. Sehgal R, Dickerson J, Holcomb M. Creation of a hospitalist-run paracentesis clinic [abstract]. J Hosp Med. 2015;10(suppl 2).
17. Sheer TA, Runyon BA. Spontaneous bacterial peritonitis. Dig Dis. 2005;23(1):39-46. doi:10.1159/000084724
18. Runyon BA. Paracentesis of ascitic fluid. A safe procedure. Arch Intern Med. 1986;146(11):2259-2261.
19. Sersté T, Francoz C, Durand F, et al. Beta-blockers cause paracentesis-induced circulatory dysfunction in patients with cirrhosis and refractory ascites: a cross-over study. J Hepatol. 2011;55(4):794-799. doi:10.1016/j.jhep.2011.01.034
20. De Gottardi A, Thévenot T, Spahr L, et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clin Gastroenterol Hepatol. 2009;7(8):906-909. doi:10.1016/j.cgh.2009.05.004
21. Khodarahmi I, Shahid MU, Contractor S. Incarceration of umbilical hernia: a rare complication of large volume paracentesis. J Radiol Case Rep. 2015;9(9):20-25. doi:10.3941/jrcr.v9i9.2614
22. Chu KM, McCaughan GW. Iatrogenic incarceration of umbilical hernia in cirrhotic patients with ascites. Am J Gastroenterol. 1995;90(11):2058-2059.
23. Triantos CK, Kehagias I, Nikolopoulou V, Burroughs AK. Incarcerated umbilical hernia after large volume paracentesis for refractory ascites. J Gastrointestin Liver Dis. 2010;19(3):245.
24. Touze I, Asselah T, Boruchowicz A, Paris JC. Abdominal pain in a cirrhotic patient with ascites. Postgrad Med J. 1997;73(865):751-752. doi:10.1136/pgmj.73.865.751
25. Baron HC. Umbilical hernia secondary to cirrhosis of the liver. Complications of surgical correction. N Engl J Med. 1960;263:824-828. doi:10.1056/NEJM196010272631702
26. Tan HK, Chang PE. Acute abdomen secondary to incarcerated umbilical hernia after treatment of massive cirrhotic ascites. Case Reports Hepatol. 2013;2013:948172. doi:10.1155/2013/948172
27. Lemmer JH, Strodel WE, Eckhauser FE. Umbilical hernia incarceration: a complication of medical therapy of ascites. Am J Gastroenterol. 1983;78(5):295-296.
28. Belghiti J, Durand F. Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis. 1997;17(3):219-226. doi:10.1055/s-2007-1007199
29. Elsabaawy MM, Abdelhamid SR, Alsebaey A, et al. The impact of paracentesis flow rate in patients with liver cirrhosis on the development of paracentesis induced circulatory dysfunction. Clin Mol Hepatol. 2015;21(4):365-371. doi:10.3350/cmh.2015.21.4.365
30. Mohan P, Venkataraman J. Prevalence and risk factors for unsuspected spontaneous ascitic fluid infection in cirrhotics undergoing therapeutic paracentesis in an outpatient clinic. Indian J Gastroenterol. 2011;30(5):221-224. doi:10.1007/s12664-011-0131-7
Cirrhosis is the most common cause of ascites in the United States. In patients with compensated cirrhosis, the 10-year probability of developing ascites is 47%. Developing ascites portends a poor prognosis. Fifteen percent of patients who receive this diagnosis die within 1 year, and 44% within 5 years.1 First-line treatment of cirrhotic ascites consists of dietary sodium restriction and diuretic therapy. Refractory ascites is defined as ascites that cannot be easily mobilized despite adhering to a dietary sodium intake of ≤ 2 g daily and daily doses of spironolactone 400 mg and furosemide 160 mg.
Patients who cannot tolerate diuretics because of complications are defined as having diuretic intractable ascites. Diuretic-induced complications include hepatic encephalopathy, renal impairment, hyponatremia, and hypo- or hyperkalemia. Because these patients are either unresponsive to or intolerant of diuretics, second-line treatments, such as regular large-volume paracentesis (LVP) or the insertion of a transjugular intrahepatic portosystemic shunt (TIPS) are needed to manage their ascites. These patients also should be considered for liver transplantation unless there is a contraindication.2
Serial LVP has been shown to be safe and effective in controlling refractory ascites.3 TIPS will decrease the need for repeated LVP in patients with refractory LVP. However, given the uncertainty as to the effect of TIPS creation on survival and the increased risk of encephalopathy, the American Association for the Study of Liver Diseases (AASLD) recommends that TIPS should be used only in those patients who cannot tolerate repeated LVP.4 Repeated LVP also has been shown to be safe and effective in controlling malignant ascites.5,6
LVP can be done in different health care settings. These include the emergency department (ED), interventional radiology suite, inpatient bed, or an outpatient paracentesis clinic. There have been various descriptions of outpatient paracentesis clinics. Reports from the United Kingdom have revealed that paracenteses in these outpatient clinics can be performed safely by nurse practitioners or a liver specialist nurse, that these clinics are highly rated by the patients, and are cost effective.7-10 Gashau and colleagues describe a clinic in Great Britain run by gastroenterology (GI) fellows using an endoscopy suite.11 A nurse practitioner outpatient paracentesis clinic in the US has been described as well.12 Grabau and colleagues present a clinic run by GI endoscopy assistants (licensed practical nurses) using a dedicated paracentesis room in the endoscopy suite.13 Cheng and colleagues describe an outpatient paracentesis clinic in a radiology department run by a single advanced practitioner with assistance from an ultrasound technologist.14 Wang and colleagues present outpatient paracenteses in an outpatient transitional care program by a physician or an advanced practitioner supervised by a physician.15 Sehgal and colleagues describe (in abstract) the creation of a hospitalist-run paracentesis clinic.16
Traditionally, at Veterans Affairs Pittsburgh Healthcare System (VAPHS) in Pennsylvania, if a patient needed LVP, they were admitted to a medicine bed. LVP is not done in the ED, and interventional radiology cannot accommodate the number of patients requiring LVP because of their caseload. The procedure was done by an attending hospitalist or medical residents under the supervision of an attending hospitalist. To improve patient flow and decrease the number of patients using inpatients beds, we created an outpatient paracentesis clinic in 2014. Here, we present the logistics of the clinic, patient demographics, the amount of ascites removed, and the time required to remove the ascites. As part of ongoing quality assurance, we keep track of any complications and report these as well.
Methods
The setting of the outpatient paracentesis clinic is a room in the VAPHS endoscopy suite. The clinic operates 1 half-day per week with up to 3 patients receiving a paracentesis. We use the existing logistics in the endoscopy suite. There are 1 or 2 registered nurses (RNs) who assist the physician performing the paracentesis. The proceduralist is an academic hospitalist who at the time is not on service with residents. The patients are referred to the clinic by the ED, hepatology clinic, palliative care, primary care physicians, or at hospital discharge. In the clinic consult, patients are required to have at least an estimated 3 L of ascites and systolic blood pressure (SBP) ≥ 90. The patients can eat and take medications the morning of the procedure except diuretics. Patients are checked in to the endoscopy suite and a peripheral IV is placed. Blood tests, such as a complete blood count and coagulation studies, are not checked routinely since the AASLD guidelines state that routine prophylactic use of fresh frozen plasma or platelets before paracentesis is not recommended because bleeding is uncommon.3 The proceduralist can order blood work at their discretion.
After the procedure, patients are brought to the recovery area of the endoscopy suite and discharged. The patients are discharged usually within 15 to 30 minutes from arriving in the recovery area after it is assured that the SBP is within 10% of their baseline. Patient follow-up in the outpatient paracentesis clinic is determined by the proceduralist. Most patients need regularly scheduled paracenteses depending on how quickly they reaccumulate ascites. If a patient does not need a regularly scheduled paracentesis, the proceduralist ensures that the appropriate outpatient clinic visit has been scheduled or requested.
Procedure
Informed consent is obtained, and a time-out is performed before each paracentesis. The patient is attached to a cardiac monitor and pulse oximetry as per the endoscopy suite protocol. The proceduralist does a point-of-care ultrasound to find the optimal site and marks the site of puncture. The skin around the marked site is prepared with 3 chlorhexidine gluconate 2%/isopropyl alcohol 70% applicators. A fenestrated drape is used to form a sterile field. The Avanos Paracentesis Kit is routinely used for LVP at VAPHS. Local anesthesia with 1% lidocaine is used with a 25-gauge × 1-inch needle. Deeper anesthesia is obtained with 1% lidocaine, using a 22-gauge × 1.5-inch needle, injecting and aspirating while advancing the needle until ascites is aspirated.
A 15-gauge 3.3-inch Caldwell cannula with an inner needle is inserted into the peritoneal cavity and ascites is aspirated into a syringe. The inner needle is then removed, and the Caldwell cannula is left in the peritoneal cavity and tubing with a roller clamp is attached to the cannula. The tubing is then attached to a 1-L vacuum suction bottle by the RN. We use the CareFusion PleurX drainage bottle. The proceduralist maintains sterility and assures the cannula remains in place. The RN changes the drainage bottles after being filled with 1 L of ascites.
We drain as much ascites as possible until drainage stops on its own. The cannula is then removed, and pressure is held with a gauze pad. An adhesive bandage is then placed over the site. Consistent with AASLD guideline, 25 g of IV albumin 25% is infused for every 3 L of albumin removed provided > 5 L of ascites is removed.3 The albumin is infused during the procedure and not after to limit the time of the procedure. A sample of ascites is sent for cell count with differential and culture.
Results
Between March 2014 and May 2020, 506 paracenteses were performed on 82 patients. The mean age was 66.4 years, and 80 of 82 patients were male. The etiology of the ascites is presented in the Table. Twelve percent of the patients had concomitant hepatocellular carcinoma. Data on the amount of ascites removed were available for all patients, but data on the amount of time it took to do the LVP were available for 392 of 506 paracenteses. The mean volume removed was 7.9 L (range, 0.2-22.9 L), and the mean time of the procedure was 33.3 minutes. The time of the procedure was the time difference between entering and leaving the procedure room. This does not include IV placement or the recovery area time.
There were 5 episodes of postprocedure hypotension that required IV fluid or admission. In all these events, the patients had received the appropriate amount of IV albumin. Three patients required admission, and 1 patient required IV fluid postparacentesis on 2 occasions and then was discharged home. One abdominal wall hematoma occurred. Two patients with umbilical hernias developed incarceration after the paracentesis; both required surgical repair. There were 3 episodes of leakage at the paracentesis site; a skin adhesive was used in 2 cases, and sutures were applied in the other. There were no deaths.
Possible Infections
Ascitic fluid infection is a risk for patients needing paracentesis. Spontaneous bacterial peritonitis (SBP) is a bacterial infection of ascites in the absence of a focal contiguous source. The polymorphonuclear leukocyte (PMN) count in the ascites is ≥ 250 cells/mm3 in the presence of a single organism on culture. Culture-negative neutrocytic ascites (CNNA) is an ascitic fluid PMN count ≥ 250 cells/mm3 in the absence of culture growth obtained before the administration of antibiotics. Monomicrobial nonneutrocytic bacterascites (MNB) is an ascitic fluid PMN count < 250 cells/mm3 with growth of a single organism on culture.17 There was one occasion where a patient developed symptomatic CNNA 3 days after having a therapeutic paracentesis in the clinic at which time his ascites had a normal neutrophil count and a negative culture. He presented with abdominal pain and fever 3 days later, and a diagnostic paracentesis was done in the ED. He was treated as though he had SBP and did well.
Ascites cell count and culture are routinely sent in the clinic, and 1 case of asymptomatic SBP and 3 cases of asymptomatic ascitic fluid infection variants were diagnosed. The patient with SBP grew vancomycin-resistant Enterococcus faecium in his ascites. Two cases were CNNA. These patients were admitted to the hospital and treated with IV antibiotics. One case of MNB occurred that grew Escherichia coli. The patient refused to return to the hospital for IV antibiotics and was treated with a 5-day course of oral ciprofloxacin.
Discussion
We describe an academic hospitalist–run outpatient LVP clinic where large volumes of ascites are removed efficiently and safely. The only other description of a hospitalist-run paracentesis clinic was in abstract form.16 Without the clinic, the patients would have been admitted to the hospital to get an LVP. Based on VAPHS data from fiscal year 2021, the average cost per day of a nontelemetry medicine admission was $3394. Over 74 months, 506 admissions were prevented, which averages to 82 admissions prevented per year, an approximate annual cost savings of $278,308 in the last fiscal year alone.
Possible Complications
The complications we report are congruent with those reported in the literature. Runyon reported that the rate of an abdominal wall hematoma requiring blood transfusion was 0.9%, and the rate of an abdominal wall hematoma not requiring blood transfusion was also 0.9%.18 We had 1 patient who developed an abdominal wall hematoma (0.2% of paracenteses). This patient required 4 units of packed red blood cells. The incidence of ascitic fluid leakage after paracentesis has been reported to be between 0.4% and 2.4%.12 We had 3 episodes of leakage (0.6% of paracenteses). The Z-track technique has been purported to decrease postparacentesis leakage.2 This involves creating a pathway that is nonlinear when anesthetizing the soft tissues and inserting the paracentesis needle. The Z-track technique was not used in any of the paracenteses in our clinic.
Postparacentesis hypotension has been reported to be 0.4% to 1.8%.12,14 We report 5 episodes of hypotension (0.1% of paracenteses) of which 3 patients were admitted to the hospital. Interestingly, 4 of the 5 patients were on β-blockers. Serste and colleagues reported in a crossover trial that paracentesis-induced circulatory dysfunction (PICD) decreased from 80 to 10% when propranolol was discontinued.19 PICD is characterized by reduction of effective arterial blood volume with subsequent activation of vasoconstrictor and antinatriuretic factors that can cause rapid ascites recurrence rate, development of dilutional hyponatremia, hepatorenal syndrome, and increased mortality. IV albumin is given during LVP to prevent PICD. Discontinuing unnecessary antihypertensive medications, especially β-blockers, may mitigate postparacentesis hypotension. In a study of 515 paracenteses, De Gottardi and colleagues reported a 0.2% rate of iatrogenic percutaneous infection of ascites.20 We had 1 patient return 3 days after LVP with fever, abdominal pain, and neutrocytic ascites. His blood and ascites cultures were negative. The etiology of his infected ascites could have been either a spontaneously developed CNNA infection or an iatrogenic percutaneous infection of ascites.
Two cases of incarceration and strangulation of umbilical hernias postparacentesis that required emergent surgical intervention were unanticipated complications. Incarceration of an existing umbilical hernia postparacentesis is an uncommon but serious complication of LVP described in the past in numerous case reports but whose incidence is otherwise unknown.21-26 The fluid and pressure shifts before and after LVP are likely responsible for the hernia incarceration. When ascites is present, the umbilical hernia ring is kept patent by the pressure of the ascitic fluid, and the decrease in tension after removal of ascites may lead to decreased size of the hernia ring and trapping of contents in the hernia sac.25-27 In most reported cases, symptoms and recognition of the incarcerated hernia have occurred within 2 days of the index paracentesis procedure. Most cases were in patients who required serial paracenteses for management of ascites and had relatively regular LVPs.
In both cases, the patients had regular visits for paracentesis, and incarceration occurred 0.5 hours postprocedure, in 1 case and 6 hours in the other. Umbilical hernias are common in patients with cirrhosis, with the prevalence approaching 20%.28 The management of umbilical hernias in patients with ascites is complex and optimal guideline-based management involves elective repair when ascites is adequately controlled to prevent recurrence, with consideration of TIPS at the time of repair.3 However, patients enrolled in outpatient paracentesis clinics are unlikely to have adequate ascites control to be considered optimized for an elective repair. In addition, given the number of serial procedures that they require, it is not surprising that they may be at risk for complications that are otherwise thought to be rare. Although incarceration and strangulation of umbilical hernia is thought to be a rare complication of LVP, patients should be informed of this potential complication so that they are aware to seek medical attention should they develop signs or symptoms.
Guidelines
There are no guidelines on how much ascites can be removed and how quickly the ascites can be removed during LVP. The goal of a therapeutic paracentesis is to remove as much fluid as possible, and there are no limits on the amount that can be removed safely.1 Concerning paracentesis flow rates, Elsabaawy and colleagues showed that ascites flow rate does not correlate with PICD. They looked at 3 groups with ascites flow rates of 80 mL/min, 180 mL/min and 270 mL/min.29 We had data on the time in the procedure room in 77% of our procedures. Given our average amount of ascites removed (7.9 L) and average time in the procedure room (33.3 minutes), the average flow rate from our clinic was at least 237 mL/min (although the flow rate was likely higher because the average time from needle inserted to needle removed was < 33.3 minutes). Both the mean duration of LVP and the mean volume of ascites removed in an outpatient paracentesis clinic were reported in only 1 other study. In a study of 1100 patients, Grabau and colleagues reported the mean duration, defined as the time between when the patient entered and exited the procedure room (the same time period we reported) as 97 minutes and the mean volume of ascites removed as 8.7 L.13
The AASLD guidelines state that patients undergoing serial outpatient LVP should be tested only for cell count and differential without sending a bacterial culture. The reason given is that false positives may exceed true positives from ascites bacterial culture results in asymptomatic patients.3 Mohan and Venkataraman reported a 0.4% rate of SBP, 1.4% rate of CNNA, and 0.7% rate of MNB in asymptomatic patients undergoing LVP in an outpatient clinic.30 We had a 0.2% rate of SBP, 0.4% rate of CNNA, and 0.2% rate of MNB. Given the low rates of SBP in outpatient paracenteses clinics, we will adopt the AASLD suggestions to only send an ascites cell count and not a culture in asymptomatic patients. Noteworthy, our patient with asymptomatic SBP grew vancomycin-resistant Enterococcus faecium, which was resistant to standard SBP antibiotic therapy. However, if ascites culture was not sent, he would have been treated with antibiotics for CNNA, and if he developed symptoms, he would have had a repeat paracentesis with cell count and culture sent.
Training
In 2015, faculty at VAPHS and the University of Pittsburgh School of Medicine designed a Mastering Paracentesis for Medical Residents course based on current guidelines on the management of ascites and published procedural guides. The course is mandatory for all postgraduate year-1 internal medicine residents and begins with 2 hours of didactic and simulation-based training with an ultrasound-compatible paracentesis mannequin. In the 3 weeks following simulation-based training, residents rotate through our outpatient paracentesis clinic and perform between 1 and 3 abdominal paracentesis procedures, receiving as-needed coaching and postprocedure feedback from faculty. Since the course’s inception, more than 150 internal medicine residents have been trained in paracentesis through our clinic.
Conclusions
We present a description of a successful outpatient paracentesis clinic at our hospital run by academic hospitalists. The clinic was created to decrease the number of admissions for LVP. We were fortunate to be able to use the GI endoscopy suite and their resources as the clinic setting. To create outpatient LVP clinics at other institutions, administrative support is essential. In conclusion, we have shown that an outpatient paracentesis clinic run by academic hospitalists can safely and quickly remove large volumes of ascites.
Cirrhosis is the most common cause of ascites in the United States. In patients with compensated cirrhosis, the 10-year probability of developing ascites is 47%. Developing ascites portends a poor prognosis. Fifteen percent of patients who receive this diagnosis die within 1 year, and 44% within 5 years.1 First-line treatment of cirrhotic ascites consists of dietary sodium restriction and diuretic therapy. Refractory ascites is defined as ascites that cannot be easily mobilized despite adhering to a dietary sodium intake of ≤ 2 g daily and daily doses of spironolactone 400 mg and furosemide 160 mg.
Patients who cannot tolerate diuretics because of complications are defined as having diuretic intractable ascites. Diuretic-induced complications include hepatic encephalopathy, renal impairment, hyponatremia, and hypo- or hyperkalemia. Because these patients are either unresponsive to or intolerant of diuretics, second-line treatments, such as regular large-volume paracentesis (LVP) or the insertion of a transjugular intrahepatic portosystemic shunt (TIPS) are needed to manage their ascites. These patients also should be considered for liver transplantation unless there is a contraindication.2
Serial LVP has been shown to be safe and effective in controlling refractory ascites.3 TIPS will decrease the need for repeated LVP in patients with refractory LVP. However, given the uncertainty as to the effect of TIPS creation on survival and the increased risk of encephalopathy, the American Association for the Study of Liver Diseases (AASLD) recommends that TIPS should be used only in those patients who cannot tolerate repeated LVP.4 Repeated LVP also has been shown to be safe and effective in controlling malignant ascites.5,6
LVP can be done in different health care settings. These include the emergency department (ED), interventional radiology suite, inpatient bed, or an outpatient paracentesis clinic. There have been various descriptions of outpatient paracentesis clinics. Reports from the United Kingdom have revealed that paracenteses in these outpatient clinics can be performed safely by nurse practitioners or a liver specialist nurse, that these clinics are highly rated by the patients, and are cost effective.7-10 Gashau and colleagues describe a clinic in Great Britain run by gastroenterology (GI) fellows using an endoscopy suite.11 A nurse practitioner outpatient paracentesis clinic in the US has been described as well.12 Grabau and colleagues present a clinic run by GI endoscopy assistants (licensed practical nurses) using a dedicated paracentesis room in the endoscopy suite.13 Cheng and colleagues describe an outpatient paracentesis clinic in a radiology department run by a single advanced practitioner with assistance from an ultrasound technologist.14 Wang and colleagues present outpatient paracenteses in an outpatient transitional care program by a physician or an advanced practitioner supervised by a physician.15 Sehgal and colleagues describe (in abstract) the creation of a hospitalist-run paracentesis clinic.16
Traditionally, at Veterans Affairs Pittsburgh Healthcare System (VAPHS) in Pennsylvania, if a patient needed LVP, they were admitted to a medicine bed. LVP is not done in the ED, and interventional radiology cannot accommodate the number of patients requiring LVP because of their caseload. The procedure was done by an attending hospitalist or medical residents under the supervision of an attending hospitalist. To improve patient flow and decrease the number of patients using inpatients beds, we created an outpatient paracentesis clinic in 2014. Here, we present the logistics of the clinic, patient demographics, the amount of ascites removed, and the time required to remove the ascites. As part of ongoing quality assurance, we keep track of any complications and report these as well.
Methods
The setting of the outpatient paracentesis clinic is a room in the VAPHS endoscopy suite. The clinic operates 1 half-day per week with up to 3 patients receiving a paracentesis. We use the existing logistics in the endoscopy suite. There are 1 or 2 registered nurses (RNs) who assist the physician performing the paracentesis. The proceduralist is an academic hospitalist who at the time is not on service with residents. The patients are referred to the clinic by the ED, hepatology clinic, palliative care, primary care physicians, or at hospital discharge. In the clinic consult, patients are required to have at least an estimated 3 L of ascites and systolic blood pressure (SBP) ≥ 90. The patients can eat and take medications the morning of the procedure except diuretics. Patients are checked in to the endoscopy suite and a peripheral IV is placed. Blood tests, such as a complete blood count and coagulation studies, are not checked routinely since the AASLD guidelines state that routine prophylactic use of fresh frozen plasma or platelets before paracentesis is not recommended because bleeding is uncommon.3 The proceduralist can order blood work at their discretion.
After the procedure, patients are brought to the recovery area of the endoscopy suite and discharged. The patients are discharged usually within 15 to 30 minutes from arriving in the recovery area after it is assured that the SBP is within 10% of their baseline. Patient follow-up in the outpatient paracentesis clinic is determined by the proceduralist. Most patients need regularly scheduled paracenteses depending on how quickly they reaccumulate ascites. If a patient does not need a regularly scheduled paracentesis, the proceduralist ensures that the appropriate outpatient clinic visit has been scheduled or requested.
Procedure
Informed consent is obtained, and a time-out is performed before each paracentesis. The patient is attached to a cardiac monitor and pulse oximetry as per the endoscopy suite protocol. The proceduralist does a point-of-care ultrasound to find the optimal site and marks the site of puncture. The skin around the marked site is prepared with 3 chlorhexidine gluconate 2%/isopropyl alcohol 70% applicators. A fenestrated drape is used to form a sterile field. The Avanos Paracentesis Kit is routinely used for LVP at VAPHS. Local anesthesia with 1% lidocaine is used with a 25-gauge × 1-inch needle. Deeper anesthesia is obtained with 1% lidocaine, using a 22-gauge × 1.5-inch needle, injecting and aspirating while advancing the needle until ascites is aspirated.
A 15-gauge 3.3-inch Caldwell cannula with an inner needle is inserted into the peritoneal cavity and ascites is aspirated into a syringe. The inner needle is then removed, and the Caldwell cannula is left in the peritoneal cavity and tubing with a roller clamp is attached to the cannula. The tubing is then attached to a 1-L vacuum suction bottle by the RN. We use the CareFusion PleurX drainage bottle. The proceduralist maintains sterility and assures the cannula remains in place. The RN changes the drainage bottles after being filled with 1 L of ascites.
We drain as much ascites as possible until drainage stops on its own. The cannula is then removed, and pressure is held with a gauze pad. An adhesive bandage is then placed over the site. Consistent with AASLD guideline, 25 g of IV albumin 25% is infused for every 3 L of albumin removed provided > 5 L of ascites is removed.3 The albumin is infused during the procedure and not after to limit the time of the procedure. A sample of ascites is sent for cell count with differential and culture.
Results
Between March 2014 and May 2020, 506 paracenteses were performed on 82 patients. The mean age was 66.4 years, and 80 of 82 patients were male. The etiology of the ascites is presented in the Table. Twelve percent of the patients had concomitant hepatocellular carcinoma. Data on the amount of ascites removed were available for all patients, but data on the amount of time it took to do the LVP were available for 392 of 506 paracenteses. The mean volume removed was 7.9 L (range, 0.2-22.9 L), and the mean time of the procedure was 33.3 minutes. The time of the procedure was the time difference between entering and leaving the procedure room. This does not include IV placement or the recovery area time.
There were 5 episodes of postprocedure hypotension that required IV fluid or admission. In all these events, the patients had received the appropriate amount of IV albumin. Three patients required admission, and 1 patient required IV fluid postparacentesis on 2 occasions and then was discharged home. One abdominal wall hematoma occurred. Two patients with umbilical hernias developed incarceration after the paracentesis; both required surgical repair. There were 3 episodes of leakage at the paracentesis site; a skin adhesive was used in 2 cases, and sutures were applied in the other. There were no deaths.
Possible Infections
Ascitic fluid infection is a risk for patients needing paracentesis. Spontaneous bacterial peritonitis (SBP) is a bacterial infection of ascites in the absence of a focal contiguous source. The polymorphonuclear leukocyte (PMN) count in the ascites is ≥ 250 cells/mm3 in the presence of a single organism on culture. Culture-negative neutrocytic ascites (CNNA) is an ascitic fluid PMN count ≥ 250 cells/mm3 in the absence of culture growth obtained before the administration of antibiotics. Monomicrobial nonneutrocytic bacterascites (MNB) is an ascitic fluid PMN count < 250 cells/mm3 with growth of a single organism on culture.17 There was one occasion where a patient developed symptomatic CNNA 3 days after having a therapeutic paracentesis in the clinic at which time his ascites had a normal neutrophil count and a negative culture. He presented with abdominal pain and fever 3 days later, and a diagnostic paracentesis was done in the ED. He was treated as though he had SBP and did well.
Ascites cell count and culture are routinely sent in the clinic, and 1 case of asymptomatic SBP and 3 cases of asymptomatic ascitic fluid infection variants were diagnosed. The patient with SBP grew vancomycin-resistant Enterococcus faecium in his ascites. Two cases were CNNA. These patients were admitted to the hospital and treated with IV antibiotics. One case of MNB occurred that grew Escherichia coli. The patient refused to return to the hospital for IV antibiotics and was treated with a 5-day course of oral ciprofloxacin.
Discussion
We describe an academic hospitalist–run outpatient LVP clinic where large volumes of ascites are removed efficiently and safely. The only other description of a hospitalist-run paracentesis clinic was in abstract form.16 Without the clinic, the patients would have been admitted to the hospital to get an LVP. Based on VAPHS data from fiscal year 2021, the average cost per day of a nontelemetry medicine admission was $3394. Over 74 months, 506 admissions were prevented, which averages to 82 admissions prevented per year, an approximate annual cost savings of $278,308 in the last fiscal year alone.
Possible Complications
The complications we report are congruent with those reported in the literature. Runyon reported that the rate of an abdominal wall hematoma requiring blood transfusion was 0.9%, and the rate of an abdominal wall hematoma not requiring blood transfusion was also 0.9%.18 We had 1 patient who developed an abdominal wall hematoma (0.2% of paracenteses). This patient required 4 units of packed red blood cells. The incidence of ascitic fluid leakage after paracentesis has been reported to be between 0.4% and 2.4%.12 We had 3 episodes of leakage (0.6% of paracenteses). The Z-track technique has been purported to decrease postparacentesis leakage.2 This involves creating a pathway that is nonlinear when anesthetizing the soft tissues and inserting the paracentesis needle. The Z-track technique was not used in any of the paracenteses in our clinic.
Postparacentesis hypotension has been reported to be 0.4% to 1.8%.12,14 We report 5 episodes of hypotension (0.1% of paracenteses) of which 3 patients were admitted to the hospital. Interestingly, 4 of the 5 patients were on β-blockers. Serste and colleagues reported in a crossover trial that paracentesis-induced circulatory dysfunction (PICD) decreased from 80 to 10% when propranolol was discontinued.19 PICD is characterized by reduction of effective arterial blood volume with subsequent activation of vasoconstrictor and antinatriuretic factors that can cause rapid ascites recurrence rate, development of dilutional hyponatremia, hepatorenal syndrome, and increased mortality. IV albumin is given during LVP to prevent PICD. Discontinuing unnecessary antihypertensive medications, especially β-blockers, may mitigate postparacentesis hypotension. In a study of 515 paracenteses, De Gottardi and colleagues reported a 0.2% rate of iatrogenic percutaneous infection of ascites.20 We had 1 patient return 3 days after LVP with fever, abdominal pain, and neutrocytic ascites. His blood and ascites cultures were negative. The etiology of his infected ascites could have been either a spontaneously developed CNNA infection or an iatrogenic percutaneous infection of ascites.
Two cases of incarceration and strangulation of umbilical hernias postparacentesis that required emergent surgical intervention were unanticipated complications. Incarceration of an existing umbilical hernia postparacentesis is an uncommon but serious complication of LVP described in the past in numerous case reports but whose incidence is otherwise unknown.21-26 The fluid and pressure shifts before and after LVP are likely responsible for the hernia incarceration. When ascites is present, the umbilical hernia ring is kept patent by the pressure of the ascitic fluid, and the decrease in tension after removal of ascites may lead to decreased size of the hernia ring and trapping of contents in the hernia sac.25-27 In most reported cases, symptoms and recognition of the incarcerated hernia have occurred within 2 days of the index paracentesis procedure. Most cases were in patients who required serial paracenteses for management of ascites and had relatively regular LVPs.
In both cases, the patients had regular visits for paracentesis, and incarceration occurred 0.5 hours postprocedure, in 1 case and 6 hours in the other. Umbilical hernias are common in patients with cirrhosis, with the prevalence approaching 20%.28 The management of umbilical hernias in patients with ascites is complex and optimal guideline-based management involves elective repair when ascites is adequately controlled to prevent recurrence, with consideration of TIPS at the time of repair.3 However, patients enrolled in outpatient paracentesis clinics are unlikely to have adequate ascites control to be considered optimized for an elective repair. In addition, given the number of serial procedures that they require, it is not surprising that they may be at risk for complications that are otherwise thought to be rare. Although incarceration and strangulation of umbilical hernia is thought to be a rare complication of LVP, patients should be informed of this potential complication so that they are aware to seek medical attention should they develop signs or symptoms.
Guidelines
There are no guidelines on how much ascites can be removed and how quickly the ascites can be removed during LVP. The goal of a therapeutic paracentesis is to remove as much fluid as possible, and there are no limits on the amount that can be removed safely.1 Concerning paracentesis flow rates, Elsabaawy and colleagues showed that ascites flow rate does not correlate with PICD. They looked at 3 groups with ascites flow rates of 80 mL/min, 180 mL/min and 270 mL/min.29 We had data on the time in the procedure room in 77% of our procedures. Given our average amount of ascites removed (7.9 L) and average time in the procedure room (33.3 minutes), the average flow rate from our clinic was at least 237 mL/min (although the flow rate was likely higher because the average time from needle inserted to needle removed was < 33.3 minutes). Both the mean duration of LVP and the mean volume of ascites removed in an outpatient paracentesis clinic were reported in only 1 other study. In a study of 1100 patients, Grabau and colleagues reported the mean duration, defined as the time between when the patient entered and exited the procedure room (the same time period we reported) as 97 minutes and the mean volume of ascites removed as 8.7 L.13
The AASLD guidelines state that patients undergoing serial outpatient LVP should be tested only for cell count and differential without sending a bacterial culture. The reason given is that false positives may exceed true positives from ascites bacterial culture results in asymptomatic patients.3 Mohan and Venkataraman reported a 0.4% rate of SBP, 1.4% rate of CNNA, and 0.7% rate of MNB in asymptomatic patients undergoing LVP in an outpatient clinic.30 We had a 0.2% rate of SBP, 0.4% rate of CNNA, and 0.2% rate of MNB. Given the low rates of SBP in outpatient paracenteses clinics, we will adopt the AASLD suggestions to only send an ascites cell count and not a culture in asymptomatic patients. Noteworthy, our patient with asymptomatic SBP grew vancomycin-resistant Enterococcus faecium, which was resistant to standard SBP antibiotic therapy. However, if ascites culture was not sent, he would have been treated with antibiotics for CNNA, and if he developed symptoms, he would have had a repeat paracentesis with cell count and culture sent.
Training
In 2015, faculty at VAPHS and the University of Pittsburgh School of Medicine designed a Mastering Paracentesis for Medical Residents course based on current guidelines on the management of ascites and published procedural guides. The course is mandatory for all postgraduate year-1 internal medicine residents and begins with 2 hours of didactic and simulation-based training with an ultrasound-compatible paracentesis mannequin. In the 3 weeks following simulation-based training, residents rotate through our outpatient paracentesis clinic and perform between 1 and 3 abdominal paracentesis procedures, receiving as-needed coaching and postprocedure feedback from faculty. Since the course’s inception, more than 150 internal medicine residents have been trained in paracentesis through our clinic.
Conclusions
We present a description of a successful outpatient paracentesis clinic at our hospital run by academic hospitalists. The clinic was created to decrease the number of admissions for LVP. We were fortunate to be able to use the GI endoscopy suite and their resources as the clinic setting. To create outpatient LVP clinics at other institutions, administrative support is essential. In conclusion, we have shown that an outpatient paracentesis clinic run by academic hospitalists can safely and quickly remove large volumes of ascites.
1. Ge PS, Runyon BA. Treatment of patients with cirrhosis. N Engl J Med. 2016;375(8):767-777. doi:10.1056/NEJMra1504367
2. Wong F. Management of ascites in cirrhosis. J Gastroenterol Hepatol. 2012;27(1):11-20. doi:10.1111/j.1440-1746.2011.06925.x
3. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359
4. Boyer TD, Haskal ZJ; American Association for the Study of Liver Diseases. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension: update 2009. Hepatology. 2010;51(1):306. doi:10.1002/hep.23383
5. Harding V, Fenu E, Medani H, et al. Safety, cost-effectiveness and feasibility of daycase paracentesis in the management of malignant ascites with a focus on ovarian cancer. Br J Cancer. 2012;107(6):925-930. doi:10.1038/bjc.2012.343
6. Korpi S, Salminen VV, Piili RP, Paunu N, Luukkaala T, Lehto JT. Therapeutic procedures for malignant ascites in a palliative care outpatient clinic. J Palliat Med. 2018;21(6):836-841. doi:10.1089/jpm.2017.0616
7. Vaughan J. Developing a nurse-led paracentesis service in an ambulatory care unit. Nurs Stand. 2013;28(4):44-50. doi:10.7748/ns2013.09.28.4.44.e7751
8. Menon S, Thompson L-S, Tan M, et al. Development and cost-benefit analysis of a nurse-led paracentesis and infusion service. Gastrointestinal Nursing. 2016;14(9):32-38. doi:10.12968/gasn.2016.14.9.32
9. Hill S, Smalley JR, Laasch H-U. Developing a nurse-led, day-case, abdominal paracentesis service. Cancer Nursing Practice. 2013;12(5):14-20. doi:10.7748/cnp2013.06.12.5.14.e942
10. Tahir F, Hollywood C, Durrant D. PWE-134 Overview of efficacy and cost effectiveness of nurse led day case abdominal paracentesis service at Gloucestershire Hospital NHS Foundation Trust. Gut. 2014;63(suppl 1):A183.2-A183. doi:10.1136/gutjnl-2014-307263.394
11. Gashau W, Samra G, Gasser J, Rolland M, Sambaiah P, Shorrock C. PTH-075 “ascites clinic”: an outpatient service model for patients requiring large volume paracentesis. Gut. 2014;63(suppl 1):A242.2-A242. doi:10.1136/gutjnl-2014-307263.521
12. Gilani N, Patel N, Gerkin RD, Ramirez FC, Tharalson EE, Patel K. The safety and feasibility of large volume paracentesis performed by an experienced nurse practitioner. Ann Hepatol. 2009;8(4):359-363.
13. Grabau CM, Crago SF, Hoff LK, et al. Performance standards for therapeutic abdominal paracentesis. Hepatology. 2004;40(2):484-488. doi:10.1002/hep.20317
14. Cheng YW, Sandrasegaran K, Cheng K, et al. A dedicated paracentesis clinic decreases healthcare utilization for serial paracenteses in decompensated cirrhosis. Abdom Radiol (NY). 2018;43(8):2190-2197. doi:10.1007/s00261-017-1406-y
15. Wang J, Khan S, Wyer P, et al. The role of ultrasound-guided therapeutic paracentesis in an outpatient transitional care program: a case series. Am J Hosp Palliat Care. 2018;35(9):1256-1260. doi:10.1177/1049909118755378
16. Sehgal R, Dickerson J, Holcomb M. Creation of a hospitalist-run paracentesis clinic [abstract]. J Hosp Med. 2015;10(suppl 2).
17. Sheer TA, Runyon BA. Spontaneous bacterial peritonitis. Dig Dis. 2005;23(1):39-46. doi:10.1159/000084724
18. Runyon BA. Paracentesis of ascitic fluid. A safe procedure. Arch Intern Med. 1986;146(11):2259-2261.
19. Sersté T, Francoz C, Durand F, et al. Beta-blockers cause paracentesis-induced circulatory dysfunction in patients with cirrhosis and refractory ascites: a cross-over study. J Hepatol. 2011;55(4):794-799. doi:10.1016/j.jhep.2011.01.034
20. De Gottardi A, Thévenot T, Spahr L, et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clin Gastroenterol Hepatol. 2009;7(8):906-909. doi:10.1016/j.cgh.2009.05.004
21. Khodarahmi I, Shahid MU, Contractor S. Incarceration of umbilical hernia: a rare complication of large volume paracentesis. J Radiol Case Rep. 2015;9(9):20-25. doi:10.3941/jrcr.v9i9.2614
22. Chu KM, McCaughan GW. Iatrogenic incarceration of umbilical hernia in cirrhotic patients with ascites. Am J Gastroenterol. 1995;90(11):2058-2059.
23. Triantos CK, Kehagias I, Nikolopoulou V, Burroughs AK. Incarcerated umbilical hernia after large volume paracentesis for refractory ascites. J Gastrointestin Liver Dis. 2010;19(3):245.
24. Touze I, Asselah T, Boruchowicz A, Paris JC. Abdominal pain in a cirrhotic patient with ascites. Postgrad Med J. 1997;73(865):751-752. doi:10.1136/pgmj.73.865.751
25. Baron HC. Umbilical hernia secondary to cirrhosis of the liver. Complications of surgical correction. N Engl J Med. 1960;263:824-828. doi:10.1056/NEJM196010272631702
26. Tan HK, Chang PE. Acute abdomen secondary to incarcerated umbilical hernia after treatment of massive cirrhotic ascites. Case Reports Hepatol. 2013;2013:948172. doi:10.1155/2013/948172
27. Lemmer JH, Strodel WE, Eckhauser FE. Umbilical hernia incarceration: a complication of medical therapy of ascites. Am J Gastroenterol. 1983;78(5):295-296.
28. Belghiti J, Durand F. Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis. 1997;17(3):219-226. doi:10.1055/s-2007-1007199
29. Elsabaawy MM, Abdelhamid SR, Alsebaey A, et al. The impact of paracentesis flow rate in patients with liver cirrhosis on the development of paracentesis induced circulatory dysfunction. Clin Mol Hepatol. 2015;21(4):365-371. doi:10.3350/cmh.2015.21.4.365
30. Mohan P, Venkataraman J. Prevalence and risk factors for unsuspected spontaneous ascitic fluid infection in cirrhotics undergoing therapeutic paracentesis in an outpatient clinic. Indian J Gastroenterol. 2011;30(5):221-224. doi:10.1007/s12664-011-0131-7
1. Ge PS, Runyon BA. Treatment of patients with cirrhosis. N Engl J Med. 2016;375(8):767-777. doi:10.1056/NEJMra1504367
2. Wong F. Management of ascites in cirrhosis. J Gastroenterol Hepatol. 2012;27(1):11-20. doi:10.1111/j.1440-1746.2011.06925.x
3. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359
4. Boyer TD, Haskal ZJ; American Association for the Study of Liver Diseases. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension: update 2009. Hepatology. 2010;51(1):306. doi:10.1002/hep.23383
5. Harding V, Fenu E, Medani H, et al. Safety, cost-effectiveness and feasibility of daycase paracentesis in the management of malignant ascites with a focus on ovarian cancer. Br J Cancer. 2012;107(6):925-930. doi:10.1038/bjc.2012.343
6. Korpi S, Salminen VV, Piili RP, Paunu N, Luukkaala T, Lehto JT. Therapeutic procedures for malignant ascites in a palliative care outpatient clinic. J Palliat Med. 2018;21(6):836-841. doi:10.1089/jpm.2017.0616
7. Vaughan J. Developing a nurse-led paracentesis service in an ambulatory care unit. Nurs Stand. 2013;28(4):44-50. doi:10.7748/ns2013.09.28.4.44.e7751
8. Menon S, Thompson L-S, Tan M, et al. Development and cost-benefit analysis of a nurse-led paracentesis and infusion service. Gastrointestinal Nursing. 2016;14(9):32-38. doi:10.12968/gasn.2016.14.9.32
9. Hill S, Smalley JR, Laasch H-U. Developing a nurse-led, day-case, abdominal paracentesis service. Cancer Nursing Practice. 2013;12(5):14-20. doi:10.7748/cnp2013.06.12.5.14.e942
10. Tahir F, Hollywood C, Durrant D. PWE-134 Overview of efficacy and cost effectiveness of nurse led day case abdominal paracentesis service at Gloucestershire Hospital NHS Foundation Trust. Gut. 2014;63(suppl 1):A183.2-A183. doi:10.1136/gutjnl-2014-307263.394
11. Gashau W, Samra G, Gasser J, Rolland M, Sambaiah P, Shorrock C. PTH-075 “ascites clinic”: an outpatient service model for patients requiring large volume paracentesis. Gut. 2014;63(suppl 1):A242.2-A242. doi:10.1136/gutjnl-2014-307263.521
12. Gilani N, Patel N, Gerkin RD, Ramirez FC, Tharalson EE, Patel K. The safety and feasibility of large volume paracentesis performed by an experienced nurse practitioner. Ann Hepatol. 2009;8(4):359-363.
13. Grabau CM, Crago SF, Hoff LK, et al. Performance standards for therapeutic abdominal paracentesis. Hepatology. 2004;40(2):484-488. doi:10.1002/hep.20317
14. Cheng YW, Sandrasegaran K, Cheng K, et al. A dedicated paracentesis clinic decreases healthcare utilization for serial paracenteses in decompensated cirrhosis. Abdom Radiol (NY). 2018;43(8):2190-2197. doi:10.1007/s00261-017-1406-y
15. Wang J, Khan S, Wyer P, et al. The role of ultrasound-guided therapeutic paracentesis in an outpatient transitional care program: a case series. Am J Hosp Palliat Care. 2018;35(9):1256-1260. doi:10.1177/1049909118755378
16. Sehgal R, Dickerson J, Holcomb M. Creation of a hospitalist-run paracentesis clinic [abstract]. J Hosp Med. 2015;10(suppl 2).
17. Sheer TA, Runyon BA. Spontaneous bacterial peritonitis. Dig Dis. 2005;23(1):39-46. doi:10.1159/000084724
18. Runyon BA. Paracentesis of ascitic fluid. A safe procedure. Arch Intern Med. 1986;146(11):2259-2261.
19. Sersté T, Francoz C, Durand F, et al. Beta-blockers cause paracentesis-induced circulatory dysfunction in patients with cirrhosis and refractory ascites: a cross-over study. J Hepatol. 2011;55(4):794-799. doi:10.1016/j.jhep.2011.01.034
20. De Gottardi A, Thévenot T, Spahr L, et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clin Gastroenterol Hepatol. 2009;7(8):906-909. doi:10.1016/j.cgh.2009.05.004
21. Khodarahmi I, Shahid MU, Contractor S. Incarceration of umbilical hernia: a rare complication of large volume paracentesis. J Radiol Case Rep. 2015;9(9):20-25. doi:10.3941/jrcr.v9i9.2614
22. Chu KM, McCaughan GW. Iatrogenic incarceration of umbilical hernia in cirrhotic patients with ascites. Am J Gastroenterol. 1995;90(11):2058-2059.
23. Triantos CK, Kehagias I, Nikolopoulou V, Burroughs AK. Incarcerated umbilical hernia after large volume paracentesis for refractory ascites. J Gastrointestin Liver Dis. 2010;19(3):245.
24. Touze I, Asselah T, Boruchowicz A, Paris JC. Abdominal pain in a cirrhotic patient with ascites. Postgrad Med J. 1997;73(865):751-752. doi:10.1136/pgmj.73.865.751
25. Baron HC. Umbilical hernia secondary to cirrhosis of the liver. Complications of surgical correction. N Engl J Med. 1960;263:824-828. doi:10.1056/NEJM196010272631702
26. Tan HK, Chang PE. Acute abdomen secondary to incarcerated umbilical hernia after treatment of massive cirrhotic ascites. Case Reports Hepatol. 2013;2013:948172. doi:10.1155/2013/948172
27. Lemmer JH, Strodel WE, Eckhauser FE. Umbilical hernia incarceration: a complication of medical therapy of ascites. Am J Gastroenterol. 1983;78(5):295-296.
28. Belghiti J, Durand F. Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis. 1997;17(3):219-226. doi:10.1055/s-2007-1007199
29. Elsabaawy MM, Abdelhamid SR, Alsebaey A, et al. The impact of paracentesis flow rate in patients with liver cirrhosis on the development of paracentesis induced circulatory dysfunction. Clin Mol Hepatol. 2015;21(4):365-371. doi:10.3350/cmh.2015.21.4.365
30. Mohan P, Venkataraman J. Prevalence and risk factors for unsuspected spontaneous ascitic fluid infection in cirrhotics undergoing therapeutic paracentesis in an outpatient clinic. Indian J Gastroenterol. 2011;30(5):221-224. doi:10.1007/s12664-011-0131-7
Mental Health Pharmacists: Increasing Necessary Mental Health Service Delivery
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
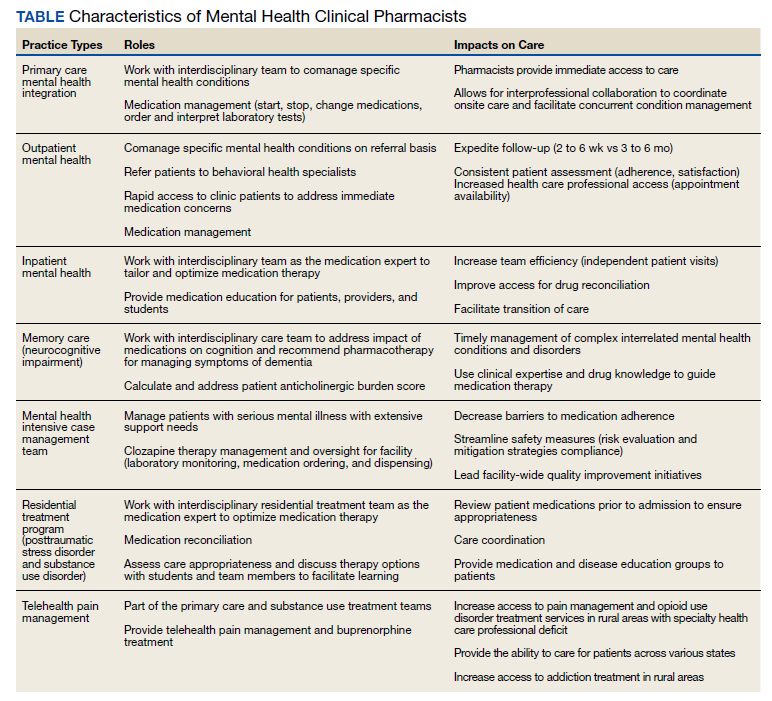
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554