User login
Population health can improve postdischarge care
With the United States spending the most per capita on health care among industrialized nations but having the worst aggregate health outcomes, there’s a stark need for improvement, according to an expert at HM20 Virtual, hosted by the Society of Hospital Medicine.

Broadening the focus beyond the four walls of the hospital can bring better results while also saving money, said Adam Myers, MD, chief of population health at Cleveland Clinic. Dr. Myers described the way his health system has begun to pay more careful attention to the needs of specific kinds of patients and tailoring posthospitalization care accordingly, with in-person and virtual home visits, and postdischarge clinics.
With an increasing attention to value, health care organizations have to change their structure or risk going the way of the Choluteca Bridge in Honduras, Dr. Myers said. The Choluteca Bridge was built to be hurricane proof, but was nonetheless rendered useless in 1998 after Hurricane Mitch shifted the very course of the river beneath it.
Similarly, the way health care is delivered often does not meet the needs of the population.
“Our national system has been focused almost entirely on inpatient care,” Dr. Myers said. “A lot of the transition in care is outside of facilities and outside the walls of our inpatient settings.”
Instead, he said a focus on population health – understanding and tending to the needs of people rather than just treating them when they show up at clinics – should involve more outpatient care that is less centralized, fees based on outcomes and patient experience rather than simply volume of services, team approaches rather than single-provider care, and a general attention to preserving health rather than treating sickness.
At Cleveland Clinic, care teams try to understand not just the care that is medically necessary, but what is wanted and justified, as well as how to deliver that care safely, reliably, and affordably with outcomes that patients and families desire.
The results are striking. After increasing the number of ambulatory patient “touches” for those with chronic disease, inpatient care – disliked by patients and costly to health centers – decreased. From the first quarter of 2018, outpatient visits increased 9%, while inpatient visits dropped 7.4%, Dr. Myers said.
“As we managed patients more effectively on an outpatient basis, their need for inpatient care diminished,” he said. “It works.”
Cleveland Clinic has also made changes designed to reduce costly readmissions, using virtual visits, house calls, time reserved for team meetings to identify patients with gaps in their care, and attention to nonmedical determinants of health, such as assessing fall risk at home and addressing lack of nutritious food options in a community.
The health system has seen a 28% reduction in the cost of care attributed to house calls, 12% cost reduction attributed to better care coordination, and a 49% decrease in hospital days for “superutilizers” of the ED, Dr. Myers said.
Postdischarge clinics – where patients can be seen for the first few visits after hospitalization – have also been valuable for many health systems, because they are closely in tune with what happened during the inpatient stay. These clinics are staffed by hospitalists, interns, residents, or ambulatory clinicians. Dr. Myers said hospitalists tend to have an improved perspective after working in a discharge clinic, with more concern about a patient’s needs once they leave the hospital bed.
“Those hospitalists that I know who have participated in programs like this start to act a bit more like primary care physicians,” he said.
In a Q&A session after Dr. Myers’ presentation, he discussed how hospitalists can affect the many layers of health care policy, factors that often overlap with population health.
He noted that medical care accounts for only about 20% of patient outcomes – the rest involve social and environmental factors.
“I don’t know about you , but I’m not satisfied only impacting 20% of health outcomes,” he said. First, physicians need to understand what is happening in their communities, and the health policies that are preventing improvement. Then, build partnerships to help fix these problems. He pointed to lead poisoning as an example.
“If you think about it, lead poisoning is a social housing problem that shows up as a health care issue. Unless we are getting out into the community and mitigating the root problem, we will have to treat it over and over again,” he said.
Dr. Myers reported no relevant financial disclosures.
With the United States spending the most per capita on health care among industrialized nations but having the worst aggregate health outcomes, there’s a stark need for improvement, according to an expert at HM20 Virtual, hosted by the Society of Hospital Medicine.
Broadening the focus beyond the four walls of the hospital can bring better results while also saving money, said Adam Myers, MD, chief of population health at Cleveland Clinic. Dr. Myers described the way his health system has begun to pay more careful attention to the needs of specific kinds of patients and tailoring posthospitalization care accordingly, with in-person and virtual home visits, and postdischarge clinics.
With an increasing attention to value, health care organizations have to change their structure or risk going the way of the Choluteca Bridge in Honduras, Dr. Myers said. The Choluteca Bridge was built to be hurricane proof, but was nonetheless rendered useless in 1998 after Hurricane Mitch shifted the very course of the river beneath it.
Similarly, the way health care is delivered often does not meet the needs of the population.
“Our national system has been focused almost entirely on inpatient care,” Dr. Myers said. “A lot of the transition in care is outside of facilities and outside the walls of our inpatient settings.”
Instead, he said a focus on population health – understanding and tending to the needs of people rather than just treating them when they show up at clinics – should involve more outpatient care that is less centralized, fees based on outcomes and patient experience rather than simply volume of services, team approaches rather than single-provider care, and a general attention to preserving health rather than treating sickness.
At Cleveland Clinic, care teams try to understand not just the care that is medically necessary, but what is wanted and justified, as well as how to deliver that care safely, reliably, and affordably with outcomes that patients and families desire.
The results are striking. After increasing the number of ambulatory patient “touches” for those with chronic disease, inpatient care – disliked by patients and costly to health centers – decreased. From the first quarter of 2018, outpatient visits increased 9%, while inpatient visits dropped 7.4%, Dr. Myers said.
“As we managed patients more effectively on an outpatient basis, their need for inpatient care diminished,” he said. “It works.”
Cleveland Clinic has also made changes designed to reduce costly readmissions, using virtual visits, house calls, time reserved for team meetings to identify patients with gaps in their care, and attention to nonmedical determinants of health, such as assessing fall risk at home and addressing lack of nutritious food options in a community.
The health system has seen a 28% reduction in the cost of care attributed to house calls, 12% cost reduction attributed to better care coordination, and a 49% decrease in hospital days for “superutilizers” of the ED, Dr. Myers said.
Postdischarge clinics – where patients can be seen for the first few visits after hospitalization – have also been valuable for many health systems, because they are closely in tune with what happened during the inpatient stay. These clinics are staffed by hospitalists, interns, residents, or ambulatory clinicians. Dr. Myers said hospitalists tend to have an improved perspective after working in a discharge clinic, with more concern about a patient’s needs once they leave the hospital bed.
“Those hospitalists that I know who have participated in programs like this start to act a bit more like primary care physicians,” he said.
In a Q&A session after Dr. Myers’ presentation, he discussed how hospitalists can affect the many layers of health care policy, factors that often overlap with population health.
He noted that medical care accounts for only about 20% of patient outcomes – the rest involve social and environmental factors.
“I don’t know about you , but I’m not satisfied only impacting 20% of health outcomes,” he said. First, physicians need to understand what is happening in their communities, and the health policies that are preventing improvement. Then, build partnerships to help fix these problems. He pointed to lead poisoning as an example.
“If you think about it, lead poisoning is a social housing problem that shows up as a health care issue. Unless we are getting out into the community and mitigating the root problem, we will have to treat it over and over again,” he said.
Dr. Myers reported no relevant financial disclosures.
With the United States spending the most per capita on health care among industrialized nations but having the worst aggregate health outcomes, there’s a stark need for improvement, according to an expert at HM20 Virtual, hosted by the Society of Hospital Medicine.
Broadening the focus beyond the four walls of the hospital can bring better results while also saving money, said Adam Myers, MD, chief of population health at Cleveland Clinic. Dr. Myers described the way his health system has begun to pay more careful attention to the needs of specific kinds of patients and tailoring posthospitalization care accordingly, with in-person and virtual home visits, and postdischarge clinics.
With an increasing attention to value, health care organizations have to change their structure or risk going the way of the Choluteca Bridge in Honduras, Dr. Myers said. The Choluteca Bridge was built to be hurricane proof, but was nonetheless rendered useless in 1998 after Hurricane Mitch shifted the very course of the river beneath it.
Similarly, the way health care is delivered often does not meet the needs of the population.
“Our national system has been focused almost entirely on inpatient care,” Dr. Myers said. “A lot of the transition in care is outside of facilities and outside the walls of our inpatient settings.”
Instead, he said a focus on population health – understanding and tending to the needs of people rather than just treating them when they show up at clinics – should involve more outpatient care that is less centralized, fees based on outcomes and patient experience rather than simply volume of services, team approaches rather than single-provider care, and a general attention to preserving health rather than treating sickness.
At Cleveland Clinic, care teams try to understand not just the care that is medically necessary, but what is wanted and justified, as well as how to deliver that care safely, reliably, and affordably with outcomes that patients and families desire.
The results are striking. After increasing the number of ambulatory patient “touches” for those with chronic disease, inpatient care – disliked by patients and costly to health centers – decreased. From the first quarter of 2018, outpatient visits increased 9%, while inpatient visits dropped 7.4%, Dr. Myers said.
“As we managed patients more effectively on an outpatient basis, their need for inpatient care diminished,” he said. “It works.”
Cleveland Clinic has also made changes designed to reduce costly readmissions, using virtual visits, house calls, time reserved for team meetings to identify patients with gaps in their care, and attention to nonmedical determinants of health, such as assessing fall risk at home and addressing lack of nutritious food options in a community.
The health system has seen a 28% reduction in the cost of care attributed to house calls, 12% cost reduction attributed to better care coordination, and a 49% decrease in hospital days for “superutilizers” of the ED, Dr. Myers said.
Postdischarge clinics – where patients can be seen for the first few visits after hospitalization – have also been valuable for many health systems, because they are closely in tune with what happened during the inpatient stay. These clinics are staffed by hospitalists, interns, residents, or ambulatory clinicians. Dr. Myers said hospitalists tend to have an improved perspective after working in a discharge clinic, with more concern about a patient’s needs once they leave the hospital bed.
“Those hospitalists that I know who have participated in programs like this start to act a bit more like primary care physicians,” he said.
In a Q&A session after Dr. Myers’ presentation, he discussed how hospitalists can affect the many layers of health care policy, factors that often overlap with population health.
He noted that medical care accounts for only about 20% of patient outcomes – the rest involve social and environmental factors.
“I don’t know about you , but I’m not satisfied only impacting 20% of health outcomes,” he said. First, physicians need to understand what is happening in their communities, and the health policies that are preventing improvement. Then, build partnerships to help fix these problems. He pointed to lead poisoning as an example.
“If you think about it, lead poisoning is a social housing problem that shows up as a health care issue. Unless we are getting out into the community and mitigating the root problem, we will have to treat it over and over again,” he said.
Dr. Myers reported no relevant financial disclosures.
How to get a position as a physician leader
The best ways to start
It’s been said that physicians tend to fall into leadership roles. Few physicians set out to become leaders, and then one day they realize that they desire to be a leader and an agent for change.
They may be rotating through the chairmanship of a clinical department or the management of a small practice and decide they like the work. In a large organization, doctors get assigned to committees, or specialists agree to run a new service line for a while, and it changes their lives.
Some physicians have a natural aptitude for managerial work. Often, colleagues tell them they are a good fit, but they may still have some reservations. In any case, it’s good to do a bit of soul-searching before taking the leap.
1. Weigh the pluses and minuses of a leadership role
When you stand at the precipice of a totally new career in physician leadership, it’s worthwhile to step back and consider the pluses and minuses of the work.
One plus is that there may be fewer work hours than on the clinical side, but being a physician leader is by no means a 9-to-5 job. In a large organization, a physician on the executive team can be on administrative call – dealing with institutional crises on off-hours – for a length of time. Board and strategic planning retreats tend to occur on weekends, and you may need to attend frequent dinner meetings.
Another plus is that the pay is pretty good. In 2016, physician leaders in large organizations earned an average of $350,000 a year, according to a survey by Cejka Executive Search and the American Association for Physician Leadership (AAPL).1
On the minus side, an executive probably won’t be as beloved as a clinician serving a host of grateful patients. And you will not have the kind of job security that most clinicians have. There may be frequent turnover among health care executives because of change of top leadership, pressure for more profitability, or a host of other reasons.
2. Try on different roles
To decide whether you want to make a career of being a physician leader, it’s useful to try out several different jobs. Volunteer for committees or take on a special project if it’s possible to do so in your organization.
You can also volunteer for posts outside the organization, such as joining the board of your local cancer or heart association or helping them out on a committee. You might volunteer for Little League or a school or civic organization. Your choices are wide open. The goal is to get a feel for directing an organization and whether that fits your lifestyle.
Also, talk to current physician leaders. Contact a cross-section of people, including those who are unhappy with their jobs and those who had to struggle with their new roles. This will give you some good perspective into whether the work is right for you, as well as tips on how to cope.
3. Find a mentor
This is also a good time to find a mentor for your new calling. Choose a seasoned physician leader who can help you over the long haul – someone who can get you up to speed and then advise you during crucial junctures in your career.
Good mentors should be willing to spend the time with you, have your best interests in mind, and be willing to provide honest assessments. They can also help you find opportunities for further learning and professional growth.
Some organizations assign mentors to physicians they want to develop for leadership roles. You can also choose specific mentors to help you in areas where you think you need more work, such as finance, quality improvement, or information systems.
Choose a path
There are many different paths you can take as a physician leader. In large organizations in particular, there are more leadership jobs open to physicians than ever before.
Jobs open to physicians can be found in the areas of clinical quality and safety, population health, managed care, and information technology. You can even look beyond these traditional roles to jobs that don’t usually attract physicians, such as in strategy, innovation, patient experience, and fundraising. In these roles, you are often expected to continue doing some clinical work.
Physician leaders now tend to have more influence than in the past. According to the Cejka-AAPL survey, 61% of physician executives said they had more strategic input currently than in the previous year.
A roster of potential physician leader jobs
1. Executive-level roles
Vice president for medical affairs. This is the traditional role for the physician executive, which involves acting as a liaison with the organization’s physicians. These officers oversee quality of care as well as hiring, training, and performance evaluation of physicians on staff.
Chief medical officer (CMO). This is now the typical term for the highest medical role in the organization. The CMO is part of the C-suite team and participates in governance, strategic planning, and business operation decisions. CMOs may be responsible for supporting value-based strategies and making sure that those strategies are efficient and medically necessary.
Physician-in-chief. This is a new term for the hospital’s top physician, who works with the senior leadership team to maintain standards of care and customer service. The physician-in-chief may also oversee operational efficiency and support organizational transformation.
Chief clinical officer (CCO). CCOs oversee patient engagement and clinical quality outcomes. They may lead initiatives to reduce waste and improve care quality, and they can be involved in implementation of electronic health records (EHRs) and data integration. They may also assist in medical staff development, clinical integration, and physician partnerships.
2. Quality, safety, and research roles
Chief patient safety officer (CPSO). CPSOs oversee the hospital or health system’s patient safety initiatives. Their goal is to reduce medical errors and near-misses.
Chief quality officer (CQO). CQOs are responsible for collecting quality data and supporting patient safety efforts. They advise on quality initiatives and hold clinicians accountable for meeting specific quality indicators. They may also be involved in developing a culture of continuous improvement in the organization.
Chief research officer (CRO). CROs oversee the organization’s research activities, including clinical trials, internal investigator-initiated research programs, and sponsored studies.
3. Technology
Chief medical information officer (CMIO). The CMIO is the information technology (IT) department’s liaison with the clinical staff, working on selection and improvement of EHR systems. The CMIO finds new ways for EHRs to improve healthcare delivery in the organization.
Chief health information officer (CHIO). CHIOs deal with EHR implementation and health informatics. They may report to the chief information officer, the chief operations officer, or another C-suite executive, and they manage health informatics, telehealth, business and clinical intelligence, and predictive analytics initiatives.
Chief technology officer (CTO). CTOs oversee the organization’s technology capabilities. They are responsible for leading the IT team and contributing to the organization’s strategic plan.
4. Jobs not usually for physicians
There are other leadership positions that may not traditionally appeal to physicians but could be worth considering:
Chief experience officer (CXO). This involves evaluating and improving the inpatient experience. CXOs work with physicians and staff on their performance in this area.
Chief innovation officer (CIO). CIOs keep up with industry trends, market disruptions, and new opportunities, and support policy innovations and training initiatives.
Chief transformation officer (CTO). CTOs are responsible for carrying out major changes in the organization. They are supposed to act as role models for change.
5. Salaries for selected physician executives
In addition to placing the average salary for a physician leader at $350,000, the 2016 Cejka-AAPL survey pinpointed average salaries for specific types of physician leaders. Chief medical officers earned $388,000, chief patient safety officers and chief quality officers $375,000, and chief medical information officers $372,500, the survey found.
Several emerging physician leader roles – physician-in-chief, chief strategy officer, chief transformation officer, chief innovation officer, and chief integration officer – earned on average $499,000 a year, according to the survey.
Those jobs provided even higher salaries than the $437,500 reported by Cejka-AAPL for physician CEOs. In comparison, a CEO at a medical group with fewer than 200 physicians had an average salary of $438,500 in 2018, according to SullivanCotter, a health care workforce strategy company.2
Some types of physician leaders have seen unusually high pay raises recently. From 2013 to 2016, the average salary for CMIOs rose 18%, and physician leaders working at the corporate level in a health system saw median compensation rise 67%, the Cejka-AAPL survey found.
Moving ahead
For physician leaders, moving up the ladder often means reinventing yourself. If you’re leaving clinical practice, be sure to develop a solid CV for your new role so that if your leadership position doesn’t work out, you are able to find an appropriate new position.
According to a 2003 assessment, CMOs typically lasted 18-24 months on the job.3
Expect to make mistakes and try to learn from them. If necessary, move on to the next job. There is always a market for seasoned physician executives who took a few punches, learned something from the experience, and found something new.
Start to network
One way to navigate the challenges of a new role is to have a strong network, a group of colleagues and mentors who can help you figure out your path forward. They can serve as sounding boards and contacts for new jobs in an industry that is constantly changing.
A well-functioning network takes constant maintenance.
You can find people for your network by attending a variety of different meetings that physician leaders and other healthcare executives attend. Make a point of keeping their contact information on file and periodically reaching out to them.
Learn in a dyad
Some healthcare organizations assign physician leaders to dyads, where they are matched with nonphysicians who have skills that the physician lacks, such as finance, data management, or organizational politics.
Dyads are less effective when the nonphysician has all the authority and the physician is basically a figurehead. But in an effective dyad, both partners share authority and they can teach skills to each other. While the physician in the dyad brings clinical insight, the nonphysician can provide managerial know-how.
Seek out coaching
There may be points in your leadership career when you become aware of areas where you need improvement. You may have gotten negative feedback on communication skills or political sensitivity. Consider hiring an executive coach; coaches provide concentrated sessions over limited periods of time.
Coaches can also help you prepare for the future. They can help you find ways to promote yourself for new projects or create a network of allies. They also can help you establish yourself as a thought leader in a particular field through writing and speaking engagements.
Some organizations provide in-house coaches. It is worthwhile to take advantage of this benefit. If you need to find a coach on your own, ask mentors or people in your network for recommendations.
Getting to the top
It can take years to rise to the level of the corporate C-suite or even to CEO of a large organization. At the top levels of management, you often have to cut back substantially on clinical work or even give it up entirely.
Becoming CEO of a hospital can be a logical fit for physicians. A physician CEO can relate to doctors on staff, who are a key constituency, and understands what clinical care is all about. However, physician CEOs also need to have a large degree of knowledge about finance, strategy, crisis management, quality improvement, and other nonclinical considerations, not to mention good people skills.
Physicians on boards
Some physicians would rather sit on the board of trustees than take the reins of CEO. Board membership allows you to continue practicing while still having a great deal of influence over the organization. Some physicians hold board seats for many years and enjoy a great deal of respect as the go-to person on clinical care.
Physicians are increasingly serving on the boards of hospitals and health systems. Trustees welcome physicians because they want more input from clinicians in decision-making. They tend to choose physicians who already have executive duties, such as having been a department head.
Which new skills should you learn?
Physician executives often put off learning business and management skills until after being appointed to a leadership position. Even then, they may prefer to take courses focused on a particular topic rather than earn a degree such as master of business administration (MBA).
Learning on the job
A number of executive skills can be learned on the job, such as dealing with quality measures, utilization, billing and coding, disease management, committees, and interpreting data. If you are not in a dyad model, you can ask someone knowledgeable in one of these skills to take you through the steps.
Many physicians could benefit from finance and business courses in order to learn some of the budgetary, accounting, and operational skills required to perform the job optimally.
In a survey of healthcare CEOs, only 30% said their most senior physician leader had a business or medical management degree, and only 21% required a degree.4
Taking classes
Physician executives who want to brush up on a particular topic can “mix and match,” taking short, focused classes on the particular topic whenever they feel the need. In addition to resources offered by SHM, courses are available from organizations such as the AAPL, American Hospital Association, the Medical Group Management Association, or the Healthcare Information and Management Systems Society, to name a few examples.
Pursuing degree programs
Degree programs like MBA, master of public health (MPH), and master of health care administration (MHA) are popular with many physician executives because they get a full overview of needed skills and the potential to earn more money with their new credentials. Physician leaders with an MBA earned 13% more in 2016 than did those with no MBA, according to the Cejka-AAPL survey.
Getting a master’s degree, however, takes time and money. For example, an MBA can cost $20,000 to as much as $100,000.5 MBA, MHA, and MPH degrees take 2 years to complete, while a master of medical management (MMM) and a physician-executive MBA – focusing specifically on what physician leaders need to learn – take 1 year.
Many part-time degree programs are available for those with full-time jobs. You can find them at nearby universities as well as far-off institutions. Much of the coursework is done online, but some on-site work is usually required. You’ll find that working directly with others enriches the learning experience and helps you build your network of colleagues.
Straight MBA or other degree?
In general, degree programs cover finance, communication, strategy, information systems, marketing, organizational behavior, operational management, and quality improvement. Straight MBA programs don’t focus on healthcare, but some physician executives still prefer this route, especially if it involves degrees from prestigious business schools.
MHA, MMM, physician-executive MBA, and other degree programs focused on healthcare are popular with many physicians on the executive track. The MPH is less business-oriented but may be preferable to some because of its focus on population-based health, which fits well with decision-making on health insurance and value-based care.
Conclusion
Physicians need to prepare for leadership because these roles are very different from clinical work. It’s easy to stumble and lose direction without mentors, a network of helpful colleagues, and at least some education in business principles.
Finding a mentor should start early in your new career. A seasoned physician executive can help you understand your options and point out your strengths and shortcomings. Beyond that, concentrated work with an executive coach can help you improve your skills and choose from among the many executive roles that are now available.
You can learn many skills on the job through dyads and other relationships with more seasoned colleagues, or take short classes on particular skills that need to be learned or sharpened. Many physician executives go a step further and get a master’s degree, such as an MBA, MHA, or MMM. This involves a year or two of study, but much of it can be done online.
This article is excerpted from the Medscape Physician Business Academy course “How to become an effective leader.” You can find more information on the course at www.medscape.com/courses/business/100018.
References
1. Cejka Executive Search. 2016 Physician Leadership Compensation Survey results released. Cejka and the American Association for Physician Leadership. Nov 3, 2016.
2. Knowles M. Salaries on upswing for physician executives. Becker’s Hospital Review. Sept 25, 2018.
3. Birrer RB. Becoming a physician executive. Health Progress: Journal of the Catholic Health Association of the United States. Jan-Feb 2003.
4. Witt/Kieffer. Transformation of physician executives: New accountability for quality, performance, integration. Fall 2010.
5. Jurica J. Does an executive salary stand up to a clinical salary? Vital Physician Executive. 2016.
The best ways to start
It’s been said that physicians tend to fall into leadership roles. Few physicians set out to become leaders, and then one day they realize that they desire to be a leader and an agent for change.
They may be rotating through the chairmanship of a clinical department or the management of a small practice and decide they like the work. In a large organization, doctors get assigned to committees, or specialists agree to run a new service line for a while, and it changes their lives.
Some physicians have a natural aptitude for managerial work. Often, colleagues tell them they are a good fit, but they may still have some reservations. In any case, it’s good to do a bit of soul-searching before taking the leap.
1. Weigh the pluses and minuses of a leadership role
When you stand at the precipice of a totally new career in physician leadership, it’s worthwhile to step back and consider the pluses and minuses of the work.
One plus is that there may be fewer work hours than on the clinical side, but being a physician leader is by no means a 9-to-5 job. In a large organization, a physician on the executive team can be on administrative call – dealing with institutional crises on off-hours – for a length of time. Board and strategic planning retreats tend to occur on weekends, and you may need to attend frequent dinner meetings.
Another plus is that the pay is pretty good. In 2016, physician leaders in large organizations earned an average of $350,000 a year, according to a survey by Cejka Executive Search and the American Association for Physician Leadership (AAPL).1
On the minus side, an executive probably won’t be as beloved as a clinician serving a host of grateful patients. And you will not have the kind of job security that most clinicians have. There may be frequent turnover among health care executives because of change of top leadership, pressure for more profitability, or a host of other reasons.
2. Try on different roles
To decide whether you want to make a career of being a physician leader, it’s useful to try out several different jobs. Volunteer for committees or take on a special project if it’s possible to do so in your organization.
You can also volunteer for posts outside the organization, such as joining the board of your local cancer or heart association or helping them out on a committee. You might volunteer for Little League or a school or civic organization. Your choices are wide open. The goal is to get a feel for directing an organization and whether that fits your lifestyle.
Also, talk to current physician leaders. Contact a cross-section of people, including those who are unhappy with their jobs and those who had to struggle with their new roles. This will give you some good perspective into whether the work is right for you, as well as tips on how to cope.
3. Find a mentor
This is also a good time to find a mentor for your new calling. Choose a seasoned physician leader who can help you over the long haul – someone who can get you up to speed and then advise you during crucial junctures in your career.
Good mentors should be willing to spend the time with you, have your best interests in mind, and be willing to provide honest assessments. They can also help you find opportunities for further learning and professional growth.
Some organizations assign mentors to physicians they want to develop for leadership roles. You can also choose specific mentors to help you in areas where you think you need more work, such as finance, quality improvement, or information systems.
Choose a path
There are many different paths you can take as a physician leader. In large organizations in particular, there are more leadership jobs open to physicians than ever before.
Jobs open to physicians can be found in the areas of clinical quality and safety, population health, managed care, and information technology. You can even look beyond these traditional roles to jobs that don’t usually attract physicians, such as in strategy, innovation, patient experience, and fundraising. In these roles, you are often expected to continue doing some clinical work.
Physician leaders now tend to have more influence than in the past. According to the Cejka-AAPL survey, 61% of physician executives said they had more strategic input currently than in the previous year.
A roster of potential physician leader jobs
1. Executive-level roles
Vice president for medical affairs. This is the traditional role for the physician executive, which involves acting as a liaison with the organization’s physicians. These officers oversee quality of care as well as hiring, training, and performance evaluation of physicians on staff.
Chief medical officer (CMO). This is now the typical term for the highest medical role in the organization. The CMO is part of the C-suite team and participates in governance, strategic planning, and business operation decisions. CMOs may be responsible for supporting value-based strategies and making sure that those strategies are efficient and medically necessary.
Physician-in-chief. This is a new term for the hospital’s top physician, who works with the senior leadership team to maintain standards of care and customer service. The physician-in-chief may also oversee operational efficiency and support organizational transformation.
Chief clinical officer (CCO). CCOs oversee patient engagement and clinical quality outcomes. They may lead initiatives to reduce waste and improve care quality, and they can be involved in implementation of electronic health records (EHRs) and data integration. They may also assist in medical staff development, clinical integration, and physician partnerships.
2. Quality, safety, and research roles
Chief patient safety officer (CPSO). CPSOs oversee the hospital or health system’s patient safety initiatives. Their goal is to reduce medical errors and near-misses.
Chief quality officer (CQO). CQOs are responsible for collecting quality data and supporting patient safety efforts. They advise on quality initiatives and hold clinicians accountable for meeting specific quality indicators. They may also be involved in developing a culture of continuous improvement in the organization.
Chief research officer (CRO). CROs oversee the organization’s research activities, including clinical trials, internal investigator-initiated research programs, and sponsored studies.
3. Technology
Chief medical information officer (CMIO). The CMIO is the information technology (IT) department’s liaison with the clinical staff, working on selection and improvement of EHR systems. The CMIO finds new ways for EHRs to improve healthcare delivery in the organization.
Chief health information officer (CHIO). CHIOs deal with EHR implementation and health informatics. They may report to the chief information officer, the chief operations officer, or another C-suite executive, and they manage health informatics, telehealth, business and clinical intelligence, and predictive analytics initiatives.
Chief technology officer (CTO). CTOs oversee the organization’s technology capabilities. They are responsible for leading the IT team and contributing to the organization’s strategic plan.
4. Jobs not usually for physicians
There are other leadership positions that may not traditionally appeal to physicians but could be worth considering:
Chief experience officer (CXO). This involves evaluating and improving the inpatient experience. CXOs work with physicians and staff on their performance in this area.
Chief innovation officer (CIO). CIOs keep up with industry trends, market disruptions, and new opportunities, and support policy innovations and training initiatives.
Chief transformation officer (CTO). CTOs are responsible for carrying out major changes in the organization. They are supposed to act as role models for change.
5. Salaries for selected physician executives
In addition to placing the average salary for a physician leader at $350,000, the 2016 Cejka-AAPL survey pinpointed average salaries for specific types of physician leaders. Chief medical officers earned $388,000, chief patient safety officers and chief quality officers $375,000, and chief medical information officers $372,500, the survey found.
Several emerging physician leader roles – physician-in-chief, chief strategy officer, chief transformation officer, chief innovation officer, and chief integration officer – earned on average $499,000 a year, according to the survey.
Those jobs provided even higher salaries than the $437,500 reported by Cejka-AAPL for physician CEOs. In comparison, a CEO at a medical group with fewer than 200 physicians had an average salary of $438,500 in 2018, according to SullivanCotter, a health care workforce strategy company.2
Some types of physician leaders have seen unusually high pay raises recently. From 2013 to 2016, the average salary for CMIOs rose 18%, and physician leaders working at the corporate level in a health system saw median compensation rise 67%, the Cejka-AAPL survey found.
Moving ahead
For physician leaders, moving up the ladder often means reinventing yourself. If you’re leaving clinical practice, be sure to develop a solid CV for your new role so that if your leadership position doesn’t work out, you are able to find an appropriate new position.
According to a 2003 assessment, CMOs typically lasted 18-24 months on the job.3
Expect to make mistakes and try to learn from them. If necessary, move on to the next job. There is always a market for seasoned physician executives who took a few punches, learned something from the experience, and found something new.
Start to network
One way to navigate the challenges of a new role is to have a strong network, a group of colleagues and mentors who can help you figure out your path forward. They can serve as sounding boards and contacts for new jobs in an industry that is constantly changing.
A well-functioning network takes constant maintenance.
You can find people for your network by attending a variety of different meetings that physician leaders and other healthcare executives attend. Make a point of keeping their contact information on file and periodically reaching out to them.
Learn in a dyad
Some healthcare organizations assign physician leaders to dyads, where they are matched with nonphysicians who have skills that the physician lacks, such as finance, data management, or organizational politics.
Dyads are less effective when the nonphysician has all the authority and the physician is basically a figurehead. But in an effective dyad, both partners share authority and they can teach skills to each other. While the physician in the dyad brings clinical insight, the nonphysician can provide managerial know-how.
Seek out coaching
There may be points in your leadership career when you become aware of areas where you need improvement. You may have gotten negative feedback on communication skills or political sensitivity. Consider hiring an executive coach; coaches provide concentrated sessions over limited periods of time.
Coaches can also help you prepare for the future. They can help you find ways to promote yourself for new projects or create a network of allies. They also can help you establish yourself as a thought leader in a particular field through writing and speaking engagements.
Some organizations provide in-house coaches. It is worthwhile to take advantage of this benefit. If you need to find a coach on your own, ask mentors or people in your network for recommendations.
Getting to the top
It can take years to rise to the level of the corporate C-suite or even to CEO of a large organization. At the top levels of management, you often have to cut back substantially on clinical work or even give it up entirely.
Becoming CEO of a hospital can be a logical fit for physicians. A physician CEO can relate to doctors on staff, who are a key constituency, and understands what clinical care is all about. However, physician CEOs also need to have a large degree of knowledge about finance, strategy, crisis management, quality improvement, and other nonclinical considerations, not to mention good people skills.
Physicians on boards
Some physicians would rather sit on the board of trustees than take the reins of CEO. Board membership allows you to continue practicing while still having a great deal of influence over the organization. Some physicians hold board seats for many years and enjoy a great deal of respect as the go-to person on clinical care.
Physicians are increasingly serving on the boards of hospitals and health systems. Trustees welcome physicians because they want more input from clinicians in decision-making. They tend to choose physicians who already have executive duties, such as having been a department head.
Which new skills should you learn?
Physician executives often put off learning business and management skills until after being appointed to a leadership position. Even then, they may prefer to take courses focused on a particular topic rather than earn a degree such as master of business administration (MBA).
Learning on the job
A number of executive skills can be learned on the job, such as dealing with quality measures, utilization, billing and coding, disease management, committees, and interpreting data. If you are not in a dyad model, you can ask someone knowledgeable in one of these skills to take you through the steps.
Many physicians could benefit from finance and business courses in order to learn some of the budgetary, accounting, and operational skills required to perform the job optimally.
In a survey of healthcare CEOs, only 30% said their most senior physician leader had a business or medical management degree, and only 21% required a degree.4
Taking classes
Physician executives who want to brush up on a particular topic can “mix and match,” taking short, focused classes on the particular topic whenever they feel the need. In addition to resources offered by SHM, courses are available from organizations such as the AAPL, American Hospital Association, the Medical Group Management Association, or the Healthcare Information and Management Systems Society, to name a few examples.
Pursuing degree programs
Degree programs like MBA, master of public health (MPH), and master of health care administration (MHA) are popular with many physician executives because they get a full overview of needed skills and the potential to earn more money with their new credentials. Physician leaders with an MBA earned 13% more in 2016 than did those with no MBA, according to the Cejka-AAPL survey.
Getting a master’s degree, however, takes time and money. For example, an MBA can cost $20,000 to as much as $100,000.5 MBA, MHA, and MPH degrees take 2 years to complete, while a master of medical management (MMM) and a physician-executive MBA – focusing specifically on what physician leaders need to learn – take 1 year.
Many part-time degree programs are available for those with full-time jobs. You can find them at nearby universities as well as far-off institutions. Much of the coursework is done online, but some on-site work is usually required. You’ll find that working directly with others enriches the learning experience and helps you build your network of colleagues.
Straight MBA or other degree?
In general, degree programs cover finance, communication, strategy, information systems, marketing, organizational behavior, operational management, and quality improvement. Straight MBA programs don’t focus on healthcare, but some physician executives still prefer this route, especially if it involves degrees from prestigious business schools.
MHA, MMM, physician-executive MBA, and other degree programs focused on healthcare are popular with many physicians on the executive track. The MPH is less business-oriented but may be preferable to some because of its focus on population-based health, which fits well with decision-making on health insurance and value-based care.
Conclusion
Physicians need to prepare for leadership because these roles are very different from clinical work. It’s easy to stumble and lose direction without mentors, a network of helpful colleagues, and at least some education in business principles.
Finding a mentor should start early in your new career. A seasoned physician executive can help you understand your options and point out your strengths and shortcomings. Beyond that, concentrated work with an executive coach can help you improve your skills and choose from among the many executive roles that are now available.
You can learn many skills on the job through dyads and other relationships with more seasoned colleagues, or take short classes on particular skills that need to be learned or sharpened. Many physician executives go a step further and get a master’s degree, such as an MBA, MHA, or MMM. This involves a year or two of study, but much of it can be done online.
This article is excerpted from the Medscape Physician Business Academy course “How to become an effective leader.” You can find more information on the course at www.medscape.com/courses/business/100018.
References
1. Cejka Executive Search. 2016 Physician Leadership Compensation Survey results released. Cejka and the American Association for Physician Leadership. Nov 3, 2016.
2. Knowles M. Salaries on upswing for physician executives. Becker’s Hospital Review. Sept 25, 2018.
3. Birrer RB. Becoming a physician executive. Health Progress: Journal of the Catholic Health Association of the United States. Jan-Feb 2003.
4. Witt/Kieffer. Transformation of physician executives: New accountability for quality, performance, integration. Fall 2010.
5. Jurica J. Does an executive salary stand up to a clinical salary? Vital Physician Executive. 2016.
The best ways to start
It’s been said that physicians tend to fall into leadership roles. Few physicians set out to become leaders, and then one day they realize that they desire to be a leader and an agent for change.
They may be rotating through the chairmanship of a clinical department or the management of a small practice and decide they like the work. In a large organization, doctors get assigned to committees, or specialists agree to run a new service line for a while, and it changes their lives.
Some physicians have a natural aptitude for managerial work. Often, colleagues tell them they are a good fit, but they may still have some reservations. In any case, it’s good to do a bit of soul-searching before taking the leap.
1. Weigh the pluses and minuses of a leadership role
When you stand at the precipice of a totally new career in physician leadership, it’s worthwhile to step back and consider the pluses and minuses of the work.
One plus is that there may be fewer work hours than on the clinical side, but being a physician leader is by no means a 9-to-5 job. In a large organization, a physician on the executive team can be on administrative call – dealing with institutional crises on off-hours – for a length of time. Board and strategic planning retreats tend to occur on weekends, and you may need to attend frequent dinner meetings.
Another plus is that the pay is pretty good. In 2016, physician leaders in large organizations earned an average of $350,000 a year, according to a survey by Cejka Executive Search and the American Association for Physician Leadership (AAPL).1
On the minus side, an executive probably won’t be as beloved as a clinician serving a host of grateful patients. And you will not have the kind of job security that most clinicians have. There may be frequent turnover among health care executives because of change of top leadership, pressure for more profitability, or a host of other reasons.
2. Try on different roles
To decide whether you want to make a career of being a physician leader, it’s useful to try out several different jobs. Volunteer for committees or take on a special project if it’s possible to do so in your organization.
You can also volunteer for posts outside the organization, such as joining the board of your local cancer or heart association or helping them out on a committee. You might volunteer for Little League or a school or civic organization. Your choices are wide open. The goal is to get a feel for directing an organization and whether that fits your lifestyle.
Also, talk to current physician leaders. Contact a cross-section of people, including those who are unhappy with their jobs and those who had to struggle with their new roles. This will give you some good perspective into whether the work is right for you, as well as tips on how to cope.
3. Find a mentor
This is also a good time to find a mentor for your new calling. Choose a seasoned physician leader who can help you over the long haul – someone who can get you up to speed and then advise you during crucial junctures in your career.
Good mentors should be willing to spend the time with you, have your best interests in mind, and be willing to provide honest assessments. They can also help you find opportunities for further learning and professional growth.
Some organizations assign mentors to physicians they want to develop for leadership roles. You can also choose specific mentors to help you in areas where you think you need more work, such as finance, quality improvement, or information systems.
Choose a path
There are many different paths you can take as a physician leader. In large organizations in particular, there are more leadership jobs open to physicians than ever before.
Jobs open to physicians can be found in the areas of clinical quality and safety, population health, managed care, and information technology. You can even look beyond these traditional roles to jobs that don’t usually attract physicians, such as in strategy, innovation, patient experience, and fundraising. In these roles, you are often expected to continue doing some clinical work.
Physician leaders now tend to have more influence than in the past. According to the Cejka-AAPL survey, 61% of physician executives said they had more strategic input currently than in the previous year.
A roster of potential physician leader jobs
1. Executive-level roles
Vice president for medical affairs. This is the traditional role for the physician executive, which involves acting as a liaison with the organization’s physicians. These officers oversee quality of care as well as hiring, training, and performance evaluation of physicians on staff.
Chief medical officer (CMO). This is now the typical term for the highest medical role in the organization. The CMO is part of the C-suite team and participates in governance, strategic planning, and business operation decisions. CMOs may be responsible for supporting value-based strategies and making sure that those strategies are efficient and medically necessary.
Physician-in-chief. This is a new term for the hospital’s top physician, who works with the senior leadership team to maintain standards of care and customer service. The physician-in-chief may also oversee operational efficiency and support organizational transformation.
Chief clinical officer (CCO). CCOs oversee patient engagement and clinical quality outcomes. They may lead initiatives to reduce waste and improve care quality, and they can be involved in implementation of electronic health records (EHRs) and data integration. They may also assist in medical staff development, clinical integration, and physician partnerships.
2. Quality, safety, and research roles
Chief patient safety officer (CPSO). CPSOs oversee the hospital or health system’s patient safety initiatives. Their goal is to reduce medical errors and near-misses.
Chief quality officer (CQO). CQOs are responsible for collecting quality data and supporting patient safety efforts. They advise on quality initiatives and hold clinicians accountable for meeting specific quality indicators. They may also be involved in developing a culture of continuous improvement in the organization.
Chief research officer (CRO). CROs oversee the organization’s research activities, including clinical trials, internal investigator-initiated research programs, and sponsored studies.
3. Technology
Chief medical information officer (CMIO). The CMIO is the information technology (IT) department’s liaison with the clinical staff, working on selection and improvement of EHR systems. The CMIO finds new ways for EHRs to improve healthcare delivery in the organization.
Chief health information officer (CHIO). CHIOs deal with EHR implementation and health informatics. They may report to the chief information officer, the chief operations officer, or another C-suite executive, and they manage health informatics, telehealth, business and clinical intelligence, and predictive analytics initiatives.
Chief technology officer (CTO). CTOs oversee the organization’s technology capabilities. They are responsible for leading the IT team and contributing to the organization’s strategic plan.
4. Jobs not usually for physicians
There are other leadership positions that may not traditionally appeal to physicians but could be worth considering:
Chief experience officer (CXO). This involves evaluating and improving the inpatient experience. CXOs work with physicians and staff on their performance in this area.
Chief innovation officer (CIO). CIOs keep up with industry trends, market disruptions, and new opportunities, and support policy innovations and training initiatives.
Chief transformation officer (CTO). CTOs are responsible for carrying out major changes in the organization. They are supposed to act as role models for change.
5. Salaries for selected physician executives
In addition to placing the average salary for a physician leader at $350,000, the 2016 Cejka-AAPL survey pinpointed average salaries for specific types of physician leaders. Chief medical officers earned $388,000, chief patient safety officers and chief quality officers $375,000, and chief medical information officers $372,500, the survey found.
Several emerging physician leader roles – physician-in-chief, chief strategy officer, chief transformation officer, chief innovation officer, and chief integration officer – earned on average $499,000 a year, according to the survey.
Those jobs provided even higher salaries than the $437,500 reported by Cejka-AAPL for physician CEOs. In comparison, a CEO at a medical group with fewer than 200 physicians had an average salary of $438,500 in 2018, according to SullivanCotter, a health care workforce strategy company.2
Some types of physician leaders have seen unusually high pay raises recently. From 2013 to 2016, the average salary for CMIOs rose 18%, and physician leaders working at the corporate level in a health system saw median compensation rise 67%, the Cejka-AAPL survey found.
Moving ahead
For physician leaders, moving up the ladder often means reinventing yourself. If you’re leaving clinical practice, be sure to develop a solid CV for your new role so that if your leadership position doesn’t work out, you are able to find an appropriate new position.
According to a 2003 assessment, CMOs typically lasted 18-24 months on the job.3
Expect to make mistakes and try to learn from them. If necessary, move on to the next job. There is always a market for seasoned physician executives who took a few punches, learned something from the experience, and found something new.
Start to network
One way to navigate the challenges of a new role is to have a strong network, a group of colleagues and mentors who can help you figure out your path forward. They can serve as sounding boards and contacts for new jobs in an industry that is constantly changing.
A well-functioning network takes constant maintenance.
You can find people for your network by attending a variety of different meetings that physician leaders and other healthcare executives attend. Make a point of keeping their contact information on file and periodically reaching out to them.
Learn in a dyad
Some healthcare organizations assign physician leaders to dyads, where they are matched with nonphysicians who have skills that the physician lacks, such as finance, data management, or organizational politics.
Dyads are less effective when the nonphysician has all the authority and the physician is basically a figurehead. But in an effective dyad, both partners share authority and they can teach skills to each other. While the physician in the dyad brings clinical insight, the nonphysician can provide managerial know-how.
Seek out coaching
There may be points in your leadership career when you become aware of areas where you need improvement. You may have gotten negative feedback on communication skills or political sensitivity. Consider hiring an executive coach; coaches provide concentrated sessions over limited periods of time.
Coaches can also help you prepare for the future. They can help you find ways to promote yourself for new projects or create a network of allies. They also can help you establish yourself as a thought leader in a particular field through writing and speaking engagements.
Some organizations provide in-house coaches. It is worthwhile to take advantage of this benefit. If you need to find a coach on your own, ask mentors or people in your network for recommendations.
Getting to the top
It can take years to rise to the level of the corporate C-suite or even to CEO of a large organization. At the top levels of management, you often have to cut back substantially on clinical work or even give it up entirely.
Becoming CEO of a hospital can be a logical fit for physicians. A physician CEO can relate to doctors on staff, who are a key constituency, and understands what clinical care is all about. However, physician CEOs also need to have a large degree of knowledge about finance, strategy, crisis management, quality improvement, and other nonclinical considerations, not to mention good people skills.
Physicians on boards
Some physicians would rather sit on the board of trustees than take the reins of CEO. Board membership allows you to continue practicing while still having a great deal of influence over the organization. Some physicians hold board seats for many years and enjoy a great deal of respect as the go-to person on clinical care.
Physicians are increasingly serving on the boards of hospitals and health systems. Trustees welcome physicians because they want more input from clinicians in decision-making. They tend to choose physicians who already have executive duties, such as having been a department head.
Which new skills should you learn?
Physician executives often put off learning business and management skills until after being appointed to a leadership position. Even then, they may prefer to take courses focused on a particular topic rather than earn a degree such as master of business administration (MBA).
Learning on the job
A number of executive skills can be learned on the job, such as dealing with quality measures, utilization, billing and coding, disease management, committees, and interpreting data. If you are not in a dyad model, you can ask someone knowledgeable in one of these skills to take you through the steps.
Many physicians could benefit from finance and business courses in order to learn some of the budgetary, accounting, and operational skills required to perform the job optimally.
In a survey of healthcare CEOs, only 30% said their most senior physician leader had a business or medical management degree, and only 21% required a degree.4
Taking classes
Physician executives who want to brush up on a particular topic can “mix and match,” taking short, focused classes on the particular topic whenever they feel the need. In addition to resources offered by SHM, courses are available from organizations such as the AAPL, American Hospital Association, the Medical Group Management Association, or the Healthcare Information and Management Systems Society, to name a few examples.
Pursuing degree programs
Degree programs like MBA, master of public health (MPH), and master of health care administration (MHA) are popular with many physician executives because they get a full overview of needed skills and the potential to earn more money with their new credentials. Physician leaders with an MBA earned 13% more in 2016 than did those with no MBA, according to the Cejka-AAPL survey.
Getting a master’s degree, however, takes time and money. For example, an MBA can cost $20,000 to as much as $100,000.5 MBA, MHA, and MPH degrees take 2 years to complete, while a master of medical management (MMM) and a physician-executive MBA – focusing specifically on what physician leaders need to learn – take 1 year.
Many part-time degree programs are available for those with full-time jobs. You can find them at nearby universities as well as far-off institutions. Much of the coursework is done online, but some on-site work is usually required. You’ll find that working directly with others enriches the learning experience and helps you build your network of colleagues.
Straight MBA or other degree?
In general, degree programs cover finance, communication, strategy, information systems, marketing, organizational behavior, operational management, and quality improvement. Straight MBA programs don’t focus on healthcare, but some physician executives still prefer this route, especially if it involves degrees from prestigious business schools.
MHA, MMM, physician-executive MBA, and other degree programs focused on healthcare are popular with many physicians on the executive track. The MPH is less business-oriented but may be preferable to some because of its focus on population-based health, which fits well with decision-making on health insurance and value-based care.
Conclusion
Physicians need to prepare for leadership because these roles are very different from clinical work. It’s easy to stumble and lose direction without mentors, a network of helpful colleagues, and at least some education in business principles.
Finding a mentor should start early in your new career. A seasoned physician executive can help you understand your options and point out your strengths and shortcomings. Beyond that, concentrated work with an executive coach can help you improve your skills and choose from among the many executive roles that are now available.
You can learn many skills on the job through dyads and other relationships with more seasoned colleagues, or take short classes on particular skills that need to be learned or sharpened. Many physician executives go a step further and get a master’s degree, such as an MBA, MHA, or MMM. This involves a year or two of study, but much of it can be done online.
This article is excerpted from the Medscape Physician Business Academy course “How to become an effective leader.” You can find more information on the course at www.medscape.com/courses/business/100018.
References
1. Cejka Executive Search. 2016 Physician Leadership Compensation Survey results released. Cejka and the American Association for Physician Leadership. Nov 3, 2016.
2. Knowles M. Salaries on upswing for physician executives. Becker’s Hospital Review. Sept 25, 2018.
3. Birrer RB. Becoming a physician executive. Health Progress: Journal of the Catholic Health Association of the United States. Jan-Feb 2003.
4. Witt/Kieffer. Transformation of physician executives: New accountability for quality, performance, integration. Fall 2010.
5. Jurica J. Does an executive salary stand up to a clinical salary? Vital Physician Executive. 2016.
More evidence links gum disease and dementia risk
especially in those with severe gum inflammation and edentulism, new research suggests.
Over a 20-year period, investigators prospectively followed more than 8,000 individuals aged around 63 years who did not have cognitive impairment or dementia at baseline, grouping them based on the extent and severity of their periodontal disease and number of lost teeth.
Results showed that 14% of participants with healthy gums and all their teeth at baseline developed dementia, compared with 18% of those with mild periodontal disease and 22% who had severe periodontal disease. The highest percentage (23%) of participants who developed dementia was found in those who were edentulous.
After accounting for comorbidities that might affect dementia risk, edentulous participants had a 20% higher risk for developing MCI or dementia, compared with the healthy group.
Because the study was observational, “we don’t have knowledge of causality so we cannot state that if you treat periodontal disease you can prevent or treat dementia,” said lead author Ryan T. Demmer, PhD, MPH, associate professor, division of epidemiology and community health, University of Minnesota, Minneapolis. However, “the take-home message from this paper is that it further supports the possibility that oral infections could be a risk factor for dementia.”
The study was published online July 29 in Neurology.
The ARIC trial
Prior studies have “described the interrelation of tooth loss or periodontal disease and cognitive outcomes, although many reports were cross-sectional or case-control … and often lacked robust confounder adjustment,” the investigators noted. Additionally, lack of longitudinal data impedes the “potential for baseline periodontal status to predict incident MCI.”
To explore the associations between periodontal status and incident MCI and dementia, the researchers studied participants in the ARIC study, a community-based longitudinal cohort consisting of 15,792 predominantly Black and White participants aged 45-64 years. The current analysis included 8,275 individuals (55% women; 21% black; mean age, 63 years) who at baseline did not meet criteria for dementia or MCI.
A full-mouth periodontal examination was conducted at baseline and participants were categorized according to the severity and extent of gingival inflammation and tooth attachment loss based on the Periodontal Profile Class (PPC) seven-category model. Potential confounding variables included age, race, education level, physical activity, smoking status, oral hygiene and access to care, plasma lipid levels, APOE genotype, body mass index, blood pressure, type 2 diabetes, and heart failure.
Based on PPC categorization, 22% of the patients had healthy gums, 12% had mild periodontal disease, 8% had a high gingival inflammation index, and 12% had posterior disease (with 6% having severe disease). In addition, 9% had tooth loss, 11% had severe tooth loss, and 20% were edentulous.
Infection hypothesis
Results showed that participants with worse periodontal status were more likely to have risk factors for vascular disease and dementia, such as smoking, hypertension, diabetes, and coronary heart disease. During median follow-up of 18.4 years, 19% of participants overall (n = 1,569) developed dementia, translating into 11.8 cases per 1,000 person-years. There were notable differences between the PPC categories in rates of incident dementia, with edentulous participants at twice the risk for developing dementia, compared with those who had healthy gums.
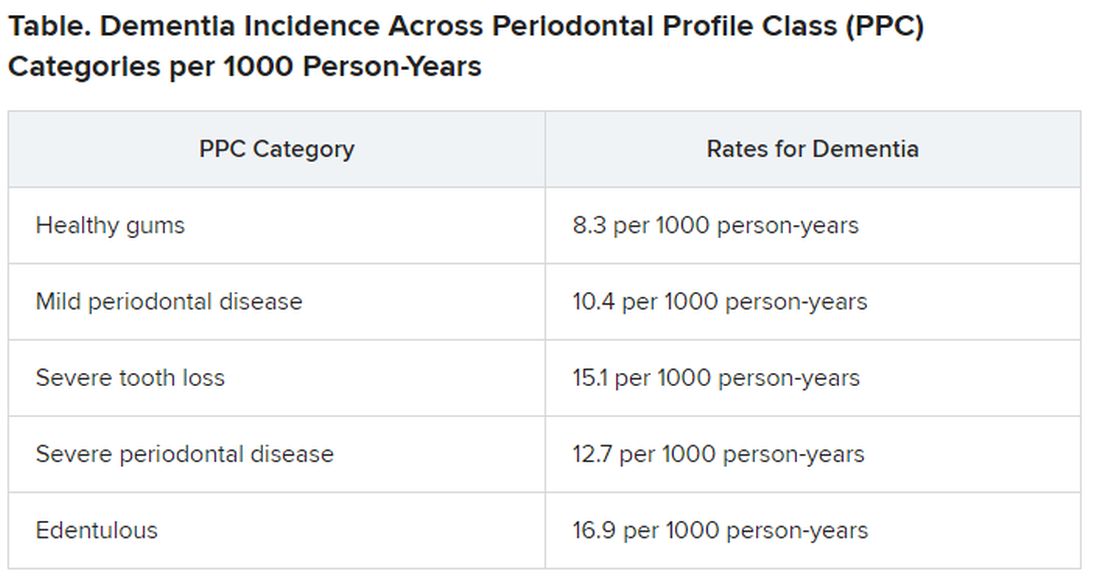
For participants with severe PPC, including severe tooth loss and severe disease, the multivariable-adjusted hazard ratio for incident dementia was 1.22 (95% confidence interval, 1.01-1.47) versus those who were periodontally healthy. For participants with edentulism, the HR was 1.21 (95% CI, 0.99-1.48). The adjusted risk ratios for the combined dementia/MCI outcome among participants with mild to intermediate PPC, severe PPC, or edentulism versus the periodontal healthy group were 1.22 (95% CI, 1.00-1.48), 1.15 (95% CI, 0.88-1.51), and 1.90 (95% CI, 1.40-2.58), respectively.
These findings were most pronounced among younger (median age at dental exam, younger than 62) versus older (62 years and older) participants (P = .02). Severe disease or total tooth loss were associated with an approximately 20% greater dementia incidence during the follow-up period, compared with healthy gums.
The investigators noted that the findings were “generally consistent” when considering the combined outcome of MCI and dementia. However, they noted that the association between edentulism and MCI was “markedly stronger,” with an approximate 100% increase in MCI or MCI plus dementia.
The association between periodontal disease and MCI or dementia “is rooted in the infection hypothesis, meaning adverse microbial exposures in the mucosal surfaces of the mouth, especially the subgingival space,” Dr. Demmer said. “One notion is that there could somehow be a direct infection of the brain with oral organisms, which posits that the oral organism could travel to the brain, colonize there, and cause damage that impairs cognition.”
Another possible mechanism is that chronic systemic inflammation in response to oral infections can eventually lead to vascular disease which, in turn, is a known risk factor for future dementia, he noted.
“Brush and floss”
Commenting on the research findings, James M. Noble, MD, associate professor of neurology, Taub Institute for Research on Alzheimer’s and the Aging Brain, Columbia University, New York, called the study “well characterized both by whole-mouth assessments and cognitive assessments performed in a standardized manner.” Moreover, “the study was sufficiently sized to allow for exploration of age and suggests that oral health may be a more important factor earlier in the course of aging, in late adulthood,” said Dr. Noble, who was not involved with the research.
The study also “makes an important contribution to this field through a rigorously followed cohort and robust design for both periodontal predictor and cognitive outcome assessments,” he said, noting that, “as always, the take-home message is ‘brush and floss.’
“Although we don’t know if treating periodontal disease can help treat dementia, this study suggests that we have to pay attention to good oral hygiene and make referrals to dentists when appropriate,” Dr. Demmer added.
The ARIC trial is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute. Dr. Demmer, the study coauthors, and Dr. Noble have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
especially in those with severe gum inflammation and edentulism, new research suggests.
Over a 20-year period, investigators prospectively followed more than 8,000 individuals aged around 63 years who did not have cognitive impairment or dementia at baseline, grouping them based on the extent and severity of their periodontal disease and number of lost teeth.
Results showed that 14% of participants with healthy gums and all their teeth at baseline developed dementia, compared with 18% of those with mild periodontal disease and 22% who had severe periodontal disease. The highest percentage (23%) of participants who developed dementia was found in those who were edentulous.
After accounting for comorbidities that might affect dementia risk, edentulous participants had a 20% higher risk for developing MCI or dementia, compared with the healthy group.
Because the study was observational, “we don’t have knowledge of causality so we cannot state that if you treat periodontal disease you can prevent or treat dementia,” said lead author Ryan T. Demmer, PhD, MPH, associate professor, division of epidemiology and community health, University of Minnesota, Minneapolis. However, “the take-home message from this paper is that it further supports the possibility that oral infections could be a risk factor for dementia.”
The study was published online July 29 in Neurology.
The ARIC trial
Prior studies have “described the interrelation of tooth loss or periodontal disease and cognitive outcomes, although many reports were cross-sectional or case-control … and often lacked robust confounder adjustment,” the investigators noted. Additionally, lack of longitudinal data impedes the “potential for baseline periodontal status to predict incident MCI.”
To explore the associations between periodontal status and incident MCI and dementia, the researchers studied participants in the ARIC study, a community-based longitudinal cohort consisting of 15,792 predominantly Black and White participants aged 45-64 years. The current analysis included 8,275 individuals (55% women; 21% black; mean age, 63 years) who at baseline did not meet criteria for dementia or MCI.
A full-mouth periodontal examination was conducted at baseline and participants were categorized according to the severity and extent of gingival inflammation and tooth attachment loss based on the Periodontal Profile Class (PPC) seven-category model. Potential confounding variables included age, race, education level, physical activity, smoking status, oral hygiene and access to care, plasma lipid levels, APOE genotype, body mass index, blood pressure, type 2 diabetes, and heart failure.
Based on PPC categorization, 22% of the patients had healthy gums, 12% had mild periodontal disease, 8% had a high gingival inflammation index, and 12% had posterior disease (with 6% having severe disease). In addition, 9% had tooth loss, 11% had severe tooth loss, and 20% were edentulous.
Infection hypothesis
Results showed that participants with worse periodontal status were more likely to have risk factors for vascular disease and dementia, such as smoking, hypertension, diabetes, and coronary heart disease. During median follow-up of 18.4 years, 19% of participants overall (n = 1,569) developed dementia, translating into 11.8 cases per 1,000 person-years. There were notable differences between the PPC categories in rates of incident dementia, with edentulous participants at twice the risk for developing dementia, compared with those who had healthy gums.
For participants with severe PPC, including severe tooth loss and severe disease, the multivariable-adjusted hazard ratio for incident dementia was 1.22 (95% confidence interval, 1.01-1.47) versus those who were periodontally healthy. For participants with edentulism, the HR was 1.21 (95% CI, 0.99-1.48). The adjusted risk ratios for the combined dementia/MCI outcome among participants with mild to intermediate PPC, severe PPC, or edentulism versus the periodontal healthy group were 1.22 (95% CI, 1.00-1.48), 1.15 (95% CI, 0.88-1.51), and 1.90 (95% CI, 1.40-2.58), respectively.
These findings were most pronounced among younger (median age at dental exam, younger than 62) versus older (62 years and older) participants (P = .02). Severe disease or total tooth loss were associated with an approximately 20% greater dementia incidence during the follow-up period, compared with healthy gums.
The investigators noted that the findings were “generally consistent” when considering the combined outcome of MCI and dementia. However, they noted that the association between edentulism and MCI was “markedly stronger,” with an approximate 100% increase in MCI or MCI plus dementia.
The association between periodontal disease and MCI or dementia “is rooted in the infection hypothesis, meaning adverse microbial exposures in the mucosal surfaces of the mouth, especially the subgingival space,” Dr. Demmer said. “One notion is that there could somehow be a direct infection of the brain with oral organisms, which posits that the oral organism could travel to the brain, colonize there, and cause damage that impairs cognition.”
Another possible mechanism is that chronic systemic inflammation in response to oral infections can eventually lead to vascular disease which, in turn, is a known risk factor for future dementia, he noted.
“Brush and floss”
Commenting on the research findings, James M. Noble, MD, associate professor of neurology, Taub Institute for Research on Alzheimer’s and the Aging Brain, Columbia University, New York, called the study “well characterized both by whole-mouth assessments and cognitive assessments performed in a standardized manner.” Moreover, “the study was sufficiently sized to allow for exploration of age and suggests that oral health may be a more important factor earlier in the course of aging, in late adulthood,” said Dr. Noble, who was not involved with the research.
The study also “makes an important contribution to this field through a rigorously followed cohort and robust design for both periodontal predictor and cognitive outcome assessments,” he said, noting that, “as always, the take-home message is ‘brush and floss.’
“Although we don’t know if treating periodontal disease can help treat dementia, this study suggests that we have to pay attention to good oral hygiene and make referrals to dentists when appropriate,” Dr. Demmer added.
The ARIC trial is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute. Dr. Demmer, the study coauthors, and Dr. Noble have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
especially in those with severe gum inflammation and edentulism, new research suggests.
Over a 20-year period, investigators prospectively followed more than 8,000 individuals aged around 63 years who did not have cognitive impairment or dementia at baseline, grouping them based on the extent and severity of their periodontal disease and number of lost teeth.
Results showed that 14% of participants with healthy gums and all their teeth at baseline developed dementia, compared with 18% of those with mild periodontal disease and 22% who had severe periodontal disease. The highest percentage (23%) of participants who developed dementia was found in those who were edentulous.
After accounting for comorbidities that might affect dementia risk, edentulous participants had a 20% higher risk for developing MCI or dementia, compared with the healthy group.
Because the study was observational, “we don’t have knowledge of causality so we cannot state that if you treat periodontal disease you can prevent or treat dementia,” said lead author Ryan T. Demmer, PhD, MPH, associate professor, division of epidemiology and community health, University of Minnesota, Minneapolis. However, “the take-home message from this paper is that it further supports the possibility that oral infections could be a risk factor for dementia.”
The study was published online July 29 in Neurology.
The ARIC trial
Prior studies have “described the interrelation of tooth loss or periodontal disease and cognitive outcomes, although many reports were cross-sectional or case-control … and often lacked robust confounder adjustment,” the investigators noted. Additionally, lack of longitudinal data impedes the “potential for baseline periodontal status to predict incident MCI.”
To explore the associations between periodontal status and incident MCI and dementia, the researchers studied participants in the ARIC study, a community-based longitudinal cohort consisting of 15,792 predominantly Black and White participants aged 45-64 years. The current analysis included 8,275 individuals (55% women; 21% black; mean age, 63 years) who at baseline did not meet criteria for dementia or MCI.
A full-mouth periodontal examination was conducted at baseline and participants were categorized according to the severity and extent of gingival inflammation and tooth attachment loss based on the Periodontal Profile Class (PPC) seven-category model. Potential confounding variables included age, race, education level, physical activity, smoking status, oral hygiene and access to care, plasma lipid levels, APOE genotype, body mass index, blood pressure, type 2 diabetes, and heart failure.
Based on PPC categorization, 22% of the patients had healthy gums, 12% had mild periodontal disease, 8% had a high gingival inflammation index, and 12% had posterior disease (with 6% having severe disease). In addition, 9% had tooth loss, 11% had severe tooth loss, and 20% were edentulous.
Infection hypothesis
Results showed that participants with worse periodontal status were more likely to have risk factors for vascular disease and dementia, such as smoking, hypertension, diabetes, and coronary heart disease. During median follow-up of 18.4 years, 19% of participants overall (n = 1,569) developed dementia, translating into 11.8 cases per 1,000 person-years. There were notable differences between the PPC categories in rates of incident dementia, with edentulous participants at twice the risk for developing dementia, compared with those who had healthy gums.
For participants with severe PPC, including severe tooth loss and severe disease, the multivariable-adjusted hazard ratio for incident dementia was 1.22 (95% confidence interval, 1.01-1.47) versus those who were periodontally healthy. For participants with edentulism, the HR was 1.21 (95% CI, 0.99-1.48). The adjusted risk ratios for the combined dementia/MCI outcome among participants with mild to intermediate PPC, severe PPC, or edentulism versus the periodontal healthy group were 1.22 (95% CI, 1.00-1.48), 1.15 (95% CI, 0.88-1.51), and 1.90 (95% CI, 1.40-2.58), respectively.
These findings were most pronounced among younger (median age at dental exam, younger than 62) versus older (62 years and older) participants (P = .02). Severe disease or total tooth loss were associated with an approximately 20% greater dementia incidence during the follow-up period, compared with healthy gums.
The investigators noted that the findings were “generally consistent” when considering the combined outcome of MCI and dementia. However, they noted that the association between edentulism and MCI was “markedly stronger,” with an approximate 100% increase in MCI or MCI plus dementia.
The association between periodontal disease and MCI or dementia “is rooted in the infection hypothesis, meaning adverse microbial exposures in the mucosal surfaces of the mouth, especially the subgingival space,” Dr. Demmer said. “One notion is that there could somehow be a direct infection of the brain with oral organisms, which posits that the oral organism could travel to the brain, colonize there, and cause damage that impairs cognition.”
Another possible mechanism is that chronic systemic inflammation in response to oral infections can eventually lead to vascular disease which, in turn, is a known risk factor for future dementia, he noted.
“Brush and floss”
Commenting on the research findings, James M. Noble, MD, associate professor of neurology, Taub Institute for Research on Alzheimer’s and the Aging Brain, Columbia University, New York, called the study “well characterized both by whole-mouth assessments and cognitive assessments performed in a standardized manner.” Moreover, “the study was sufficiently sized to allow for exploration of age and suggests that oral health may be a more important factor earlier in the course of aging, in late adulthood,” said Dr. Noble, who was not involved with the research.
The study also “makes an important contribution to this field through a rigorously followed cohort and robust design for both periodontal predictor and cognitive outcome assessments,” he said, noting that, “as always, the take-home message is ‘brush and floss.’
“Although we don’t know if treating periodontal disease can help treat dementia, this study suggests that we have to pay attention to good oral hygiene and make referrals to dentists when appropriate,” Dr. Demmer added.
The ARIC trial is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute. Dr. Demmer, the study coauthors, and Dr. Noble have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Managing acute pain in inpatients on OUD therapy
“This is something we’re going to see more frequently, and many of us already have,” Theresa E. Vettese, MD, said at HM20 Virtual, hosted by the Society of Hospital Medicine.
The drastic drop in prescriptions for opioid pain medications in the last several years hasn’t curtailed the current opioid epidemic. Instead, the epidemic has to a great extent morphed into expanded use of illicit heroin and fentanyl, noted Dr. Vettese, an internist, hospitalist, and palliative care physician at Emory University and Grady Memorial Hospital in Atlanta.
Mythbusting
Treatment of acute pain in hospitalized patients on opioid agonist therapy for opioid use disorder (OUD) is actually pretty straightforward once a few common myths have been dispelled, she said.
One of these myths –common among both physicians and patients in treatment for OUD – is that prescribing opioids for management of acute pain will place such patients at risk for OUD relapse.
“In fact, the data really strongly suggest this is not the case,” Dr. Vettese said. “It will not worsen addiction. But if we don’t aggressively treat these patients’ acute pain, it puts them at higher risk for bad outcomes.”
Another myth – this one not uncommon among hospital pharmacy departments – is that only physicians with a special certification can prescribe methadone for inpatients.
“The federal laws are clear: Any physician who has a DEA license can prescribe methadone in the hospital acute care setting, not only for pain management, but also for treatment of opioid withdrawal. You can’t prescribe it in the outpatient setting for opioid withdrawal – that has to be dispensed through a federally regulated methadone outpatient treatment program. But in the hospital, we can feel safe that we can do so. You may need to educate your pharmacist about this,” she said.
Hospitalists also can prescribe buprenorphine in the acute care inpatient setting, both for pain and treatment of opioid withdrawal, without need for a DEA waiver.
“It’s useful to get some skills in using buprenorphine in the inpatient setting. You don’t need an X waiver, but I encourage everyone to do the X-waiver training because it’s a terrific educational session. It’s 8 hours for physicians and well worth it,” Dr. Vettese noted.
By federal law the inpatient physician also can prescribe 3 days of buprenorphine at discharge to get the patient to an outpatient provider.
Misconceptions also abound about NSAIDs as a nonopioid component of acute pain management in hospitalized patients. They actually are extremely effective for the treatment of musculoskeletal, orthopedic, procedural, migraine, and some types of cancer pain. The number needed to treat (NNT) for postoperative pain relief for ibuprofen or celecoxib is 2.5, and when used in conjunction with acetaminophen at 325 mg every 4 hours, that NNT drops to 1.5, similar to the NNT of 1.7 for oxycodone at 15 mg. It should be noted, however, that the bar defining effective pain relief in randomized studies is set rather low: A 50% greater reduction in pain than achieved with placebo.
Many hospitalists would like to use NSAIDs more often, but they’re leery of the associated risks of GI bleeding, ischemic cardiovascular events, and worsening kidney function. Dr. Vettese offered several risk-mitigation strategies to increase the use of NSAIDs as opioid-sparing agents for acute pain management.
She has changed her own clinical practice with regard to using NSAIDs in patients with chronic kidney disease in response to a 2019 systematic review by investigators at the University of Ottawa.
“This was a game changer for me because in this review, low-dose NSAIDs were safe in that they didn’t significantly increase the risk of worsening kidney failure even in patients with stage 3 chronic kidney disease. So this has expanded my use of NSAIDs in this population through stage 3 CKD. With a creatinine clearance below 30, however, kidney failure worsened rapidly, so I don’t do it in patients with CKD stage 4,” Dr. Vettese said.
Gastroenterologists categorize patients as being at high risk of GI bleeding related to NSAID use if they have a history of a complicated ulcer or they have at least three of the following risk factors: Age above 65 years, history of an uncomplicated ulcer, being on high-dose NSAID therapy, or concurrent use of aspirin, glucocorticoids, or anticoagulants. Patients are considered at moderate risk if they have one or two of the risk factors, and low risk if they have none. Dr. Vettese said that, while NSAIDs clearly should be avoided in the high-risk group, moderate-risk patients are a different matter.
“Many avoid the use of NSAIDs with moderate risk, but I think we can expand their use if we use the right NSAID and we use protective strategies,” Dr. Vettese said.
Celecoxib is the safest drug in terms of upper GI bleeding risk, but ibuprofen is close. They are associated with a 2.2-fold increased risk of bleeding when compared with risk in patients not on an NSAID. Naproxen or indeomethacin use carries a fourfold to fivefold increased risk.
“Celecoxib with a proton pump inhibitor is safest, followed by celecoxib alone, followed by ibuprofen with a proton pump inhibitor. So I advocate using NSAIDs more frequently in people who are at moderate risk by using them with a PPI,” she said.
There is persuasive evidence of increased cardiovascular risk in association with even short-duration NSAIDs, as the drugs are utilized in the treatment of acute pain in hospitalized patients. That being said, Dr. Vettese believes hospitalists can use these drugs safely in more patients by following a thoughtful cardiovascular risk-mitigation strategy developed by Italian investigators.
Communicating about pain management
“Communication is always the key to effective pain management in every situation,” Dr. Vettese emphasized.
“I talk to the patient about the goals of effective pain management. I’ll discourage the use of the 1-10 pain scale, and instead, I’ll be honest about expectations, saying, ‘You have a problem that will cause acute pain, and it’s unlikely that I will be able to completely relieve your pain. The goal is to improve your function so that you can get up and go the bathroom by yourself, and so that you can sleep for a few hours. That’s how we’re going to measure the efficacy of our pain-management program.’ ”
She explains to the patient that she’ll be using nonopioid medications and nondrug therapies along with oral opioid pain medications, which are less risky than IV opioids. She offers reassurance that this treatment strategy won’t cause an OUD relapse. She lets the patient know up-front that the opioids will be tapered as the acute pain improves.
For the patient who comes into the hospital on buprenorphine for OUD, she immediately checks with the state prescription drug monitoring program to make sure everything is above board and there’s no indication of doctor shopping for prescriptions. For in-hospital acute pain, it’s safe and effective to continue the outpatient dose. On an outpatient basis, however, the drug is given once daily. On that dosing schedule both the euphoric effect as well as the analgesic effect are lost, so for acute pain management in the hospital it’s recommended to split the dose into twice- or thrice-daily doses to achieve an analgesic effect.
Oral NSAIDs are part of the treatment strategy whenever possible. For severe acute pain, Dr. Vettese will prescribe an immediate-release opioid having a high affinity to the mu opioid receptor, such as oral hydromorphone, on an as-needed basis. The drug has onset of effect in 30 minutes, peak effect in 1 hour, and a duration of effect of 4-6 hours, although she recommends going with 4 hours to provide adequate analgesia.
“These patients will require much higher doses than the patients who are opioid naive,” she advised.
For the patient with acute pain who is admitted while on methadone for OUD, it’s important to call the outpatient treatment program to verify the dosage.
“You can split the dose of methadone to try to get better analgesia, although I can tell you that patients who are treated with methadone for OUD frequently don’t want to do that. And if they don’t want to, then I don’t,” the hospitalist said.
As with the patient on buprenorphine for OUD, she’ll use additional oral immediate-release opioids as needed for acute severe pain in a patient on methadone for medication-assisted OUD treatment.
Dr. Vettese reported having no financial conflicts regarding her presentation.
“This is something we’re going to see more frequently, and many of us already have,” Theresa E. Vettese, MD, said at HM20 Virtual, hosted by the Society of Hospital Medicine.
The drastic drop in prescriptions for opioid pain medications in the last several years hasn’t curtailed the current opioid epidemic. Instead, the epidemic has to a great extent morphed into expanded use of illicit heroin and fentanyl, noted Dr. Vettese, an internist, hospitalist, and palliative care physician at Emory University and Grady Memorial Hospital in Atlanta.
Mythbusting
Treatment of acute pain in hospitalized patients on opioid agonist therapy for opioid use disorder (OUD) is actually pretty straightforward once a few common myths have been dispelled, she said.
One of these myths –common among both physicians and patients in treatment for OUD – is that prescribing opioids for management of acute pain will place such patients at risk for OUD relapse.
“In fact, the data really strongly suggest this is not the case,” Dr. Vettese said. “It will not worsen addiction. But if we don’t aggressively treat these patients’ acute pain, it puts them at higher risk for bad outcomes.”
Another myth – this one not uncommon among hospital pharmacy departments – is that only physicians with a special certification can prescribe methadone for inpatients.
“The federal laws are clear: Any physician who has a DEA license can prescribe methadone in the hospital acute care setting, not only for pain management, but also for treatment of opioid withdrawal. You can’t prescribe it in the outpatient setting for opioid withdrawal – that has to be dispensed through a federally regulated methadone outpatient treatment program. But in the hospital, we can feel safe that we can do so. You may need to educate your pharmacist about this,” she said.
Hospitalists also can prescribe buprenorphine in the acute care inpatient setting, both for pain and treatment of opioid withdrawal, without need for a DEA waiver.
“It’s useful to get some skills in using buprenorphine in the inpatient setting. You don’t need an X waiver, but I encourage everyone to do the X-waiver training because it’s a terrific educational session. It’s 8 hours for physicians and well worth it,” Dr. Vettese noted.
By federal law the inpatient physician also can prescribe 3 days of buprenorphine at discharge to get the patient to an outpatient provider.
Misconceptions also abound about NSAIDs as a nonopioid component of acute pain management in hospitalized patients. They actually are extremely effective for the treatment of musculoskeletal, orthopedic, procedural, migraine, and some types of cancer pain. The number needed to treat (NNT) for postoperative pain relief for ibuprofen or celecoxib is 2.5, and when used in conjunction with acetaminophen at 325 mg every 4 hours, that NNT drops to 1.5, similar to the NNT of 1.7 for oxycodone at 15 mg. It should be noted, however, that the bar defining effective pain relief in randomized studies is set rather low: A 50% greater reduction in pain than achieved with placebo.
Many hospitalists would like to use NSAIDs more often, but they’re leery of the associated risks of GI bleeding, ischemic cardiovascular events, and worsening kidney function. Dr. Vettese offered several risk-mitigation strategies to increase the use of NSAIDs as opioid-sparing agents for acute pain management.
She has changed her own clinical practice with regard to using NSAIDs in patients with chronic kidney disease in response to a 2019 systematic review by investigators at the University of Ottawa.
“This was a game changer for me because in this review, low-dose NSAIDs were safe in that they didn’t significantly increase the risk of worsening kidney failure even in patients with stage 3 chronic kidney disease. So this has expanded my use of NSAIDs in this population through stage 3 CKD. With a creatinine clearance below 30, however, kidney failure worsened rapidly, so I don’t do it in patients with CKD stage 4,” Dr. Vettese said.
Gastroenterologists categorize patients as being at high risk of GI bleeding related to NSAID use if they have a history of a complicated ulcer or they have at least three of the following risk factors: Age above 65 years, history of an uncomplicated ulcer, being on high-dose NSAID therapy, or concurrent use of aspirin, glucocorticoids, or anticoagulants. Patients are considered at moderate risk if they have one or two of the risk factors, and low risk if they have none. Dr. Vettese said that, while NSAIDs clearly should be avoided in the high-risk group, moderate-risk patients are a different matter.
“Many avoid the use of NSAIDs with moderate risk, but I think we can expand their use if we use the right NSAID and we use protective strategies,” Dr. Vettese said.
Celecoxib is the safest drug in terms of upper GI bleeding risk, but ibuprofen is close. They are associated with a 2.2-fold increased risk of bleeding when compared with risk in patients not on an NSAID. Naproxen or indeomethacin use carries a fourfold to fivefold increased risk.
“Celecoxib with a proton pump inhibitor is safest, followed by celecoxib alone, followed by ibuprofen with a proton pump inhibitor. So I advocate using NSAIDs more frequently in people who are at moderate risk by using them with a PPI,” she said.
There is persuasive evidence of increased cardiovascular risk in association with even short-duration NSAIDs, as the drugs are utilized in the treatment of acute pain in hospitalized patients. That being said, Dr. Vettese believes hospitalists can use these drugs safely in more patients by following a thoughtful cardiovascular risk-mitigation strategy developed by Italian investigators.
Communicating about pain management
“Communication is always the key to effective pain management in every situation,” Dr. Vettese emphasized.
“I talk to the patient about the goals of effective pain management. I’ll discourage the use of the 1-10 pain scale, and instead, I’ll be honest about expectations, saying, ‘You have a problem that will cause acute pain, and it’s unlikely that I will be able to completely relieve your pain. The goal is to improve your function so that you can get up and go the bathroom by yourself, and so that you can sleep for a few hours. That’s how we’re going to measure the efficacy of our pain-management program.’ ”
She explains to the patient that she’ll be using nonopioid medications and nondrug therapies along with oral opioid pain medications, which are less risky than IV opioids. She offers reassurance that this treatment strategy won’t cause an OUD relapse. She lets the patient know up-front that the opioids will be tapered as the acute pain improves.
For the patient who comes into the hospital on buprenorphine for OUD, she immediately checks with the state prescription drug monitoring program to make sure everything is above board and there’s no indication of doctor shopping for prescriptions. For in-hospital acute pain, it’s safe and effective to continue the outpatient dose. On an outpatient basis, however, the drug is given once daily. On that dosing schedule both the euphoric effect as well as the analgesic effect are lost, so for acute pain management in the hospital it’s recommended to split the dose into twice- or thrice-daily doses to achieve an analgesic effect.
Oral NSAIDs are part of the treatment strategy whenever possible. For severe acute pain, Dr. Vettese will prescribe an immediate-release opioid having a high affinity to the mu opioid receptor, such as oral hydromorphone, on an as-needed basis. The drug has onset of effect in 30 minutes, peak effect in 1 hour, and a duration of effect of 4-6 hours, although she recommends going with 4 hours to provide adequate analgesia.
“These patients will require much higher doses than the patients who are opioid naive,” she advised.
For the patient with acute pain who is admitted while on methadone for OUD, it’s important to call the outpatient treatment program to verify the dosage.
“You can split the dose of methadone to try to get better analgesia, although I can tell you that patients who are treated with methadone for OUD frequently don’t want to do that. And if they don’t want to, then I don’t,” the hospitalist said.
As with the patient on buprenorphine for OUD, she’ll use additional oral immediate-release opioids as needed for acute severe pain in a patient on methadone for medication-assisted OUD treatment.
Dr. Vettese reported having no financial conflicts regarding her presentation.
“This is something we’re going to see more frequently, and many of us already have,” Theresa E. Vettese, MD, said at HM20 Virtual, hosted by the Society of Hospital Medicine.
The drastic drop in prescriptions for opioid pain medications in the last several years hasn’t curtailed the current opioid epidemic. Instead, the epidemic has to a great extent morphed into expanded use of illicit heroin and fentanyl, noted Dr. Vettese, an internist, hospitalist, and palliative care physician at Emory University and Grady Memorial Hospital in Atlanta.
Mythbusting
Treatment of acute pain in hospitalized patients on opioid agonist therapy for opioid use disorder (OUD) is actually pretty straightforward once a few common myths have been dispelled, she said.
One of these myths –common among both physicians and patients in treatment for OUD – is that prescribing opioids for management of acute pain will place such patients at risk for OUD relapse.
“In fact, the data really strongly suggest this is not the case,” Dr. Vettese said. “It will not worsen addiction. But if we don’t aggressively treat these patients’ acute pain, it puts them at higher risk for bad outcomes.”
Another myth – this one not uncommon among hospital pharmacy departments – is that only physicians with a special certification can prescribe methadone for inpatients.
“The federal laws are clear: Any physician who has a DEA license can prescribe methadone in the hospital acute care setting, not only for pain management, but also for treatment of opioid withdrawal. You can’t prescribe it in the outpatient setting for opioid withdrawal – that has to be dispensed through a federally regulated methadone outpatient treatment program. But in the hospital, we can feel safe that we can do so. You may need to educate your pharmacist about this,” she said.
Hospitalists also can prescribe buprenorphine in the acute care inpatient setting, both for pain and treatment of opioid withdrawal, without need for a DEA waiver.
“It’s useful to get some skills in using buprenorphine in the inpatient setting. You don’t need an X waiver, but I encourage everyone to do the X-waiver training because it’s a terrific educational session. It’s 8 hours for physicians and well worth it,” Dr. Vettese noted.
By federal law the inpatient physician also can prescribe 3 days of buprenorphine at discharge to get the patient to an outpatient provider.
Misconceptions also abound about NSAIDs as a nonopioid component of acute pain management in hospitalized patients. They actually are extremely effective for the treatment of musculoskeletal, orthopedic, procedural, migraine, and some types of cancer pain. The number needed to treat (NNT) for postoperative pain relief for ibuprofen or celecoxib is 2.5, and when used in conjunction with acetaminophen at 325 mg every 4 hours, that NNT drops to 1.5, similar to the NNT of 1.7 for oxycodone at 15 mg. It should be noted, however, that the bar defining effective pain relief in randomized studies is set rather low: A 50% greater reduction in pain than achieved with placebo.
Many hospitalists would like to use NSAIDs more often, but they’re leery of the associated risks of GI bleeding, ischemic cardiovascular events, and worsening kidney function. Dr. Vettese offered several risk-mitigation strategies to increase the use of NSAIDs as opioid-sparing agents for acute pain management.
She has changed her own clinical practice with regard to using NSAIDs in patients with chronic kidney disease in response to a 2019 systematic review by investigators at the University of Ottawa.
“This was a game changer for me because in this review, low-dose NSAIDs were safe in that they didn’t significantly increase the risk of worsening kidney failure even in patients with stage 3 chronic kidney disease. So this has expanded my use of NSAIDs in this population through stage 3 CKD. With a creatinine clearance below 30, however, kidney failure worsened rapidly, so I don’t do it in patients with CKD stage 4,” Dr. Vettese said.
Gastroenterologists categorize patients as being at high risk of GI bleeding related to NSAID use if they have a history of a complicated ulcer or they have at least three of the following risk factors: Age above 65 years, history of an uncomplicated ulcer, being on high-dose NSAID therapy, or concurrent use of aspirin, glucocorticoids, or anticoagulants. Patients are considered at moderate risk if they have one or two of the risk factors, and low risk if they have none. Dr. Vettese said that, while NSAIDs clearly should be avoided in the high-risk group, moderate-risk patients are a different matter.
“Many avoid the use of NSAIDs with moderate risk, but I think we can expand their use if we use the right NSAID and we use protective strategies,” Dr. Vettese said.
Celecoxib is the safest drug in terms of upper GI bleeding risk, but ibuprofen is close. They are associated with a 2.2-fold increased risk of bleeding when compared with risk in patients not on an NSAID. Naproxen or indeomethacin use carries a fourfold to fivefold increased risk.
“Celecoxib with a proton pump inhibitor is safest, followed by celecoxib alone, followed by ibuprofen with a proton pump inhibitor. So I advocate using NSAIDs more frequently in people who are at moderate risk by using them with a PPI,” she said.
There is persuasive evidence of increased cardiovascular risk in association with even short-duration NSAIDs, as the drugs are utilized in the treatment of acute pain in hospitalized patients. That being said, Dr. Vettese believes hospitalists can use these drugs safely in more patients by following a thoughtful cardiovascular risk-mitigation strategy developed by Italian investigators.
Communicating about pain management
“Communication is always the key to effective pain management in every situation,” Dr. Vettese emphasized.
“I talk to the patient about the goals of effective pain management. I’ll discourage the use of the 1-10 pain scale, and instead, I’ll be honest about expectations, saying, ‘You have a problem that will cause acute pain, and it’s unlikely that I will be able to completely relieve your pain. The goal is to improve your function so that you can get up and go the bathroom by yourself, and so that you can sleep for a few hours. That’s how we’re going to measure the efficacy of our pain-management program.’ ”
She explains to the patient that she’ll be using nonopioid medications and nondrug therapies along with oral opioid pain medications, which are less risky than IV opioids. She offers reassurance that this treatment strategy won’t cause an OUD relapse. She lets the patient know up-front that the opioids will be tapered as the acute pain improves.
For the patient who comes into the hospital on buprenorphine for OUD, she immediately checks with the state prescription drug monitoring program to make sure everything is above board and there’s no indication of doctor shopping for prescriptions. For in-hospital acute pain, it’s safe and effective to continue the outpatient dose. On an outpatient basis, however, the drug is given once daily. On that dosing schedule both the euphoric effect as well as the analgesic effect are lost, so for acute pain management in the hospital it’s recommended to split the dose into twice- or thrice-daily doses to achieve an analgesic effect.
Oral NSAIDs are part of the treatment strategy whenever possible. For severe acute pain, Dr. Vettese will prescribe an immediate-release opioid having a high affinity to the mu opioid receptor, such as oral hydromorphone, on an as-needed basis. The drug has onset of effect in 30 minutes, peak effect in 1 hour, and a duration of effect of 4-6 hours, although she recommends going with 4 hours to provide adequate analgesia.
“These patients will require much higher doses than the patients who are opioid naive,” she advised.
For the patient with acute pain who is admitted while on methadone for OUD, it’s important to call the outpatient treatment program to verify the dosage.
“You can split the dose of methadone to try to get better analgesia, although I can tell you that patients who are treated with methadone for OUD frequently don’t want to do that. And if they don’t want to, then I don’t,” the hospitalist said.
As with the patient on buprenorphine for OUD, she’ll use additional oral immediate-release opioids as needed for acute severe pain in a patient on methadone for medication-assisted OUD treatment.
Dr. Vettese reported having no financial conflicts regarding her presentation.
FROM HM20 VIRTUAL
Biologic responses to metal implants: Dermatologic implications
Hypersensitivity to implantable devices, albeit rare, is a growing problem. according to a report on biological responses to metal implants released by the Food and Drug Administration in September 2019. Large controlled studies are lacking, and the FDA has initiated extensive postmarketing reviews of certain metal implants in response to safety concerns. Further research is needed on the composition of these implants, the diverse spectrum of metals used, the physical environment in which they are implanted, and the immune response associated with implants.

Local and systemic type IV hypersensitivity reactions can result from exposure to metal ions, which are thought to act as haptens and bind to proteins. The hapten-protein complex acts as the antigen for the T cell. Additionally, both acute and chronic inflammatory responses secondary to wound healing and foreign body reactions can occur. Neutrophils and macrophages elicit a tissue response, which can cause aseptic infection, loosening of joints, and tissue damage. Furthermore, corrosion of metal implants can lead to release of metal ions, which can have genotoxic and carcinogenic effects.
Clinical and subclinical effects of implantable devices depend on the device itself, the composition of the device, the tissue type, and an individual’s immune characteristics. Metal debris released from implants can activate innate and adaptive immune responses through a variety of different mechanisms, depending on the implant type and in what tissues the implant is placed. In the case of orthopedic implants, the most common implants, osteoclasts can sense metal and induce proinflammatory cytokines, which can result in corrosion and uptake of metal particles. Metal devices used in the central nervous system, such as intracerebral electrodes, can cause inflammatory responses leading to tissue encapsulation of electrodes. Corrosion of electrodes and release of metal ions can also impede ion channels in the CNS, blocking critical neuron-signaling pathways. Inflammatory reactions surrounding cardiac and vascular implants containing metal activate coagulation cascades, resulting in endothelial injury and activation of thrombi.
Despite the commonly used term “metal allergy” that delineates a type IV hypersensitivity reaction, reports in the literature supports the existence of both innate and adaptive immune responses to metal implanted in tissues. The recommended terminology is “adverse reactions to metal debris.” The clinical presentation may not be straightforward or easily attributed to the implant. Diagnostic tools are limited and may not detect a causal relationship.

Clinical symptoms can range from local rashes and pruritus to cardiac damage, depression, vertigo, and neurologic symptoms; autoimmune/autoinflammatory reactions including chronic fatigue and autoimmune-like systemic symptoms, such as joint pain, headaches, and hair loss, have also been reported in association with implants containing metal. In addition to pruritus, dermatologic manifestations can include erythema, edema, papules, vesicles, as well as systemic hypersensitivity reactions. Typically, cutaneous reactions usually present within 2 days to 24 months of implantation and may be considered surgical-site infections. Although these reactions can be treated with topical or oral corticosteroids, removal of the device is frequently needed for complete clearance.
In clinical practice, it has been frustrating that potential adverse reactions to metal implants are often overlooked because they are thought to be so rare. There are case series documenting metal implant hypersensitivity, but the actual prevalence of hypersensitivity or autoinflammatory reactions is not known. Testing methods are often inaccurate; therefore, identification of at-risk individuals and management of symptomatic patients with implants is important.
The 2016 American Contact Dermatitis Society guidelines do not recommend preimplantation patch testing unless there is a suspected metal allergy. However, patch testing cannot identify the extent of corrosion, autoinflammatory reactions, and foreign body reactions that can occur.
We must keep an open mind in patients who have implanted devices and have unusual or otherwise undefined symptoms. Often, the symptoms do not directly correspond to the site of implantation and the only way to discern whether the implant is the cause and to treat symptoms is removal of the implanted device.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
References
Food and Drug Administration. Biological Responses to Metal Implants. 2019 Sep. https://www.fda.gov/media/131150/download.
Atwater AR, Reeder M. Cutis. 2020 Feb;105(2):68-70.
Schalock PC et al. Dermatitis. Sep-Oct 2016;27(5):241-7.
Hypersensitivity to implantable devices, albeit rare, is a growing problem. according to a report on biological responses to metal implants released by the Food and Drug Administration in September 2019. Large controlled studies are lacking, and the FDA has initiated extensive postmarketing reviews of certain metal implants in response to safety concerns. Further research is needed on the composition of these implants, the diverse spectrum of metals used, the physical environment in which they are implanted, and the immune response associated with implants.
Local and systemic type IV hypersensitivity reactions can result from exposure to metal ions, which are thought to act as haptens and bind to proteins. The hapten-protein complex acts as the antigen for the T cell. Additionally, both acute and chronic inflammatory responses secondary to wound healing and foreign body reactions can occur. Neutrophils and macrophages elicit a tissue response, which can cause aseptic infection, loosening of joints, and tissue damage. Furthermore, corrosion of metal implants can lead to release of metal ions, which can have genotoxic and carcinogenic effects.
Clinical and subclinical effects of implantable devices depend on the device itself, the composition of the device, the tissue type, and an individual’s immune characteristics. Metal debris released from implants can activate innate and adaptive immune responses through a variety of different mechanisms, depending on the implant type and in what tissues the implant is placed. In the case of orthopedic implants, the most common implants, osteoclasts can sense metal and induce proinflammatory cytokines, which can result in corrosion and uptake of metal particles. Metal devices used in the central nervous system, such as intracerebral electrodes, can cause inflammatory responses leading to tissue encapsulation of electrodes. Corrosion of electrodes and release of metal ions can also impede ion channels in the CNS, blocking critical neuron-signaling pathways. Inflammatory reactions surrounding cardiac and vascular implants containing metal activate coagulation cascades, resulting in endothelial injury and activation of thrombi.
Despite the commonly used term “metal allergy” that delineates a type IV hypersensitivity reaction, reports in the literature supports the existence of both innate and adaptive immune responses to metal implanted in tissues. The recommended terminology is “adverse reactions to metal debris.” The clinical presentation may not be straightforward or easily attributed to the implant. Diagnostic tools are limited and may not detect a causal relationship.
Clinical symptoms can range from local rashes and pruritus to cardiac damage, depression, vertigo, and neurologic symptoms; autoimmune/autoinflammatory reactions including chronic fatigue and autoimmune-like systemic symptoms, such as joint pain, headaches, and hair loss, have also been reported in association with implants containing metal. In addition to pruritus, dermatologic manifestations can include erythema, edema, papules, vesicles, as well as systemic hypersensitivity reactions. Typically, cutaneous reactions usually present within 2 days to 24 months of implantation and may be considered surgical-site infections. Although these reactions can be treated with topical or oral corticosteroids, removal of the device is frequently needed for complete clearance.
In clinical practice, it has been frustrating that potential adverse reactions to metal implants are often overlooked because they are thought to be so rare. There are case series documenting metal implant hypersensitivity, but the actual prevalence of hypersensitivity or autoinflammatory reactions is not known. Testing methods are often inaccurate; therefore, identification of at-risk individuals and management of symptomatic patients with implants is important.
The 2016 American Contact Dermatitis Society guidelines do not recommend preimplantation patch testing unless there is a suspected metal allergy. However, patch testing cannot identify the extent of corrosion, autoinflammatory reactions, and foreign body reactions that can occur.
We must keep an open mind in patients who have implanted devices and have unusual or otherwise undefined symptoms. Often, the symptoms do not directly correspond to the site of implantation and the only way to discern whether the implant is the cause and to treat symptoms is removal of the implanted device.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
References
Food and Drug Administration. Biological Responses to Metal Implants. 2019 Sep. https://www.fda.gov/media/131150/download.
Atwater AR, Reeder M. Cutis. 2020 Feb;105(2):68-70.
Schalock PC et al. Dermatitis. Sep-Oct 2016;27(5):241-7.
Hypersensitivity to implantable devices, albeit rare, is a growing problem. according to a report on biological responses to metal implants released by the Food and Drug Administration in September 2019. Large controlled studies are lacking, and the FDA has initiated extensive postmarketing reviews of certain metal implants in response to safety concerns. Further research is needed on the composition of these implants, the diverse spectrum of metals used, the physical environment in which they are implanted, and the immune response associated with implants.
Local and systemic type IV hypersensitivity reactions can result from exposure to metal ions, which are thought to act as haptens and bind to proteins. The hapten-protein complex acts as the antigen for the T cell. Additionally, both acute and chronic inflammatory responses secondary to wound healing and foreign body reactions can occur. Neutrophils and macrophages elicit a tissue response, which can cause aseptic infection, loosening of joints, and tissue damage. Furthermore, corrosion of metal implants can lead to release of metal ions, which can have genotoxic and carcinogenic effects.
Clinical and subclinical effects of implantable devices depend on the device itself, the composition of the device, the tissue type, and an individual’s immune characteristics. Metal debris released from implants can activate innate and adaptive immune responses through a variety of different mechanisms, depending on the implant type and in what tissues the implant is placed. In the case of orthopedic implants, the most common implants, osteoclasts can sense metal and induce proinflammatory cytokines, which can result in corrosion and uptake of metal particles. Metal devices used in the central nervous system, such as intracerebral electrodes, can cause inflammatory responses leading to tissue encapsulation of electrodes. Corrosion of electrodes and release of metal ions can also impede ion channels in the CNS, blocking critical neuron-signaling pathways. Inflammatory reactions surrounding cardiac and vascular implants containing metal activate coagulation cascades, resulting in endothelial injury and activation of thrombi.
Despite the commonly used term “metal allergy” that delineates a type IV hypersensitivity reaction, reports in the literature supports the existence of both innate and adaptive immune responses to metal implanted in tissues. The recommended terminology is “adverse reactions to metal debris.” The clinical presentation may not be straightforward or easily attributed to the implant. Diagnostic tools are limited and may not detect a causal relationship.
Clinical symptoms can range from local rashes and pruritus to cardiac damage, depression, vertigo, and neurologic symptoms; autoimmune/autoinflammatory reactions including chronic fatigue and autoimmune-like systemic symptoms, such as joint pain, headaches, and hair loss, have also been reported in association with implants containing metal. In addition to pruritus, dermatologic manifestations can include erythema, edema, papules, vesicles, as well as systemic hypersensitivity reactions. Typically, cutaneous reactions usually present within 2 days to 24 months of implantation and may be considered surgical-site infections. Although these reactions can be treated with topical or oral corticosteroids, removal of the device is frequently needed for complete clearance.
In clinical practice, it has been frustrating that potential adverse reactions to metal implants are often overlooked because they are thought to be so rare. There are case series documenting metal implant hypersensitivity, but the actual prevalence of hypersensitivity or autoinflammatory reactions is not known. Testing methods are often inaccurate; therefore, identification of at-risk individuals and management of symptomatic patients with implants is important.
The 2016 American Contact Dermatitis Society guidelines do not recommend preimplantation patch testing unless there is a suspected metal allergy. However, patch testing cannot identify the extent of corrosion, autoinflammatory reactions, and foreign body reactions that can occur.
We must keep an open mind in patients who have implanted devices and have unusual or otherwise undefined symptoms. Often, the symptoms do not directly correspond to the site of implantation and the only way to discern whether the implant is the cause and to treat symptoms is removal of the implanted device.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
References
Food and Drug Administration. Biological Responses to Metal Implants. 2019 Sep. https://www.fda.gov/media/131150/download.
Atwater AR, Reeder M. Cutis. 2020 Feb;105(2):68-70.
Schalock PC et al. Dermatitis. Sep-Oct 2016;27(5):241-7.
FDA approves ofatumumab (Kesimpta) for relapsing forms of MS
including relapsing-remitting MS, active secondary progressive MS, and clinically isolated syndrome, Novartis announced in a press release. This is the first FDA approval of a self-administered, targeted B-cell therapy for these conditions, and is delivered via an autoinjector pen.
“This approval is wonderful news for patients with relapsing multiple sclerosis,” Stephen Hauser, MD, director of the Weill Institute for Neurosciences at the University of California, San Francisco, said in the press release. “Through its favorable safety profile and well-tolerated monthly injection regimen, patients can self-administer the treatment at home, avoiding visits to the infusion center,” he noted.
Dr. Hauser is cochair of the steering committee for the phase 3 ASCLEPIOS I and II studies that were part of the basis for the FDA’s approval.
Bruce Bebo, PhD, executive vice president of research at the National MS Society, said because response to disease-modifying treatments varies among individuals with MS, it’s important to have a range of treatment options available with differing mechanisms of action. “We are pleased to have an additional option approved for the treatment of relapsing forms of MS,” he said.
Twin studies
Formerly known as OMB157, ofatumumab is a precisely-dosed anti-CD20 monoclonal antibody administered subcutaneously via once-monthly injection. However, Novartis noted that initial doses are given at weeks 0, 1, and 2 – with the first injection occurring with a health care professional present.
The drug “is thought to work by binding to a distinct epitope on the CD20 molecule inducing potent B-cell lysis and depletion,” the manufacturer noted.
As previously reported, results for the ACLEPIOS I and II studies were presented at the 2019 Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), with additional results presented at the 2020 Virtual Annual Meeting of the Consortium of Multiple Sclerosis Centers. In addition, the findings were published in the New England Journal of Medicine.
The twin, identically designed phase 3 studies assessed the safety and efficacy of the drug at a monthly subcutaneous dose of 20 mg versus once daily teriflunomide 14-mg oral tablets. Together, the studies included 1,882 adult patients at more than 350 sites in 37 countries.
Results showed that the study drug reduced the annualized relapse rate (ARR) by 51% in the first study and by 59% in the second versus teriflunomide (P < .001 in both studies), meeting the primary endpoint. Both studies also showed significant reductions of gadolinium-enhancing (Gd+) T1 lesions (by 98% and 94%, respectively) and new or enlarging T2 lesions (by 82% and 85%).
The most commonly observed treatment-related adverse events for ofatumumab were upper respiratory tract infection, headache, and injection-related reactions.
Although the FDA first approved ofatumumab in 2009 for treating chronic lymphocytic leukemia (CLL), it was administered as a high-dose intravenous infusion by a healthcare provider. “This is a different dosing regimen and route of administration than was previously approved for the CLL indication,” the company noted.
The drug is expected to be available in the United States in September.
A version of this article originally appeared on Medscape.com.
including relapsing-remitting MS, active secondary progressive MS, and clinically isolated syndrome, Novartis announced in a press release. This is the first FDA approval of a self-administered, targeted B-cell therapy for these conditions, and is delivered via an autoinjector pen.
“This approval is wonderful news for patients with relapsing multiple sclerosis,” Stephen Hauser, MD, director of the Weill Institute for Neurosciences at the University of California, San Francisco, said in the press release. “Through its favorable safety profile and well-tolerated monthly injection regimen, patients can self-administer the treatment at home, avoiding visits to the infusion center,” he noted.
Dr. Hauser is cochair of the steering committee for the phase 3 ASCLEPIOS I and II studies that were part of the basis for the FDA’s approval.
Bruce Bebo, PhD, executive vice president of research at the National MS Society, said because response to disease-modifying treatments varies among individuals with MS, it’s important to have a range of treatment options available with differing mechanisms of action. “We are pleased to have an additional option approved for the treatment of relapsing forms of MS,” he said.
Twin studies
Formerly known as OMB157, ofatumumab is a precisely-dosed anti-CD20 monoclonal antibody administered subcutaneously via once-monthly injection. However, Novartis noted that initial doses are given at weeks 0, 1, and 2 – with the first injection occurring with a health care professional present.
The drug “is thought to work by binding to a distinct epitope on the CD20 molecule inducing potent B-cell lysis and depletion,” the manufacturer noted.
As previously reported, results for the ACLEPIOS I and II studies were presented at the 2019 Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), with additional results presented at the 2020 Virtual Annual Meeting of the Consortium of Multiple Sclerosis Centers. In addition, the findings were published in the New England Journal of Medicine.
The twin, identically designed phase 3 studies assessed the safety and efficacy of the drug at a monthly subcutaneous dose of 20 mg versus once daily teriflunomide 14-mg oral tablets. Together, the studies included 1,882 adult patients at more than 350 sites in 37 countries.
Results showed that the study drug reduced the annualized relapse rate (ARR) by 51% in the first study and by 59% in the second versus teriflunomide (P < .001 in both studies), meeting the primary endpoint. Both studies also showed significant reductions of gadolinium-enhancing (Gd+) T1 lesions (by 98% and 94%, respectively) and new or enlarging T2 lesions (by 82% and 85%).
The most commonly observed treatment-related adverse events for ofatumumab were upper respiratory tract infection, headache, and injection-related reactions.
Although the FDA first approved ofatumumab in 2009 for treating chronic lymphocytic leukemia (CLL), it was administered as a high-dose intravenous infusion by a healthcare provider. “This is a different dosing regimen and route of administration than was previously approved for the CLL indication,” the company noted.
The drug is expected to be available in the United States in September.
A version of this article originally appeared on Medscape.com.
including relapsing-remitting MS, active secondary progressive MS, and clinically isolated syndrome, Novartis announced in a press release. This is the first FDA approval of a self-administered, targeted B-cell therapy for these conditions, and is delivered via an autoinjector pen.
“This approval is wonderful news for patients with relapsing multiple sclerosis,” Stephen Hauser, MD, director of the Weill Institute for Neurosciences at the University of California, San Francisco, said in the press release. “Through its favorable safety profile and well-tolerated monthly injection regimen, patients can self-administer the treatment at home, avoiding visits to the infusion center,” he noted.
Dr. Hauser is cochair of the steering committee for the phase 3 ASCLEPIOS I and II studies that were part of the basis for the FDA’s approval.
Bruce Bebo, PhD, executive vice president of research at the National MS Society, said because response to disease-modifying treatments varies among individuals with MS, it’s important to have a range of treatment options available with differing mechanisms of action. “We are pleased to have an additional option approved for the treatment of relapsing forms of MS,” he said.
Twin studies
Formerly known as OMB157, ofatumumab is a precisely-dosed anti-CD20 monoclonal antibody administered subcutaneously via once-monthly injection. However, Novartis noted that initial doses are given at weeks 0, 1, and 2 – with the first injection occurring with a health care professional present.
The drug “is thought to work by binding to a distinct epitope on the CD20 molecule inducing potent B-cell lysis and depletion,” the manufacturer noted.
As previously reported, results for the ACLEPIOS I and II studies were presented at the 2019 Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), with additional results presented at the 2020 Virtual Annual Meeting of the Consortium of Multiple Sclerosis Centers. In addition, the findings were published in the New England Journal of Medicine.
The twin, identically designed phase 3 studies assessed the safety and efficacy of the drug at a monthly subcutaneous dose of 20 mg versus once daily teriflunomide 14-mg oral tablets. Together, the studies included 1,882 adult patients at more than 350 sites in 37 countries.
Results showed that the study drug reduced the annualized relapse rate (ARR) by 51% in the first study and by 59% in the second versus teriflunomide (P < .001 in both studies), meeting the primary endpoint. Both studies also showed significant reductions of gadolinium-enhancing (Gd+) T1 lesions (by 98% and 94%, respectively) and new or enlarging T2 lesions (by 82% and 85%).
The most commonly observed treatment-related adverse events for ofatumumab were upper respiratory tract infection, headache, and injection-related reactions.
Although the FDA first approved ofatumumab in 2009 for treating chronic lymphocytic leukemia (CLL), it was administered as a high-dose intravenous infusion by a healthcare provider. “This is a different dosing regimen and route of administration than was previously approved for the CLL indication,” the company noted.
The drug is expected to be available in the United States in September.
A version of this article originally appeared on Medscape.com.
NBA star Mason Plumlee on COVID and life inside the Orlando ‘bubble’
Editor’s Note: This transcript from the August 20 episode of the Blood & Cancer podcast has been edited for clarity. Click this link to listen to the full episode.
David Henry, MD: Welcome to this Blood & Cancer podcast. I’m your host, Dr. David Henry. This podcast airs on Thursday morning each week. This interview and others are archived with show notes from our residents at Pennsylvania Hospital at this link.
Each week we interview key opinion leaders involved in various aspects of blood and cancer. Mason was a first round pick in the NBA, a gold medalist for the U.S. men’s national team, and NBA All-Rookie first team honoree. He’s one of the top playmaking forwards in the country, if not the world, in my opinion. In his four-year college career at Duke University, he helped lead the Blue Devils to a National Collegiate Athletic Association (NCAA) championship and twice earned All-America first team academic honors at Duke. So he’s not just a basketball star, but an academic star as well. Mason, thanks so much for taking some time out from the bubble in Florida to talk with us today.
Mason Plumlee: Thanks for having me on. I’m happy to be here.
Henry: Beginning in March, the NBA didn’t know what to do about the COVID pandemic but finally decided to put you professional players in a ‘bubble.’ What did you have to go through to get there? You, your teammates, coaches, trainers, etc. And what’s the ongoing plan to be sure you continue to be safe?
Plumlee: Back to when the season shut down in March, the NBA shut down the practice facilities at the same time. Most people went home. I went back to Indiana. And then, as the idea of this bubble came up and the NBA formalized a plan to start the season again, players started to go back to market. I went back to Denver and was working out there.
About two weeks before we were scheduled to arrive in Orlando, they started testing us every other day. They used the deep nasal swab as well as the throat swab. But they were also taking two to three blood tests in that time period. You needed a certain number of consecutive negative tests before they would allow you to fly on the team plane down to Orlando. So there was an incredible amount of testing in the market. Once you got to Orlando, you went into a 48-hour quarantine. You had to have two negative tests with 48 hours between them before you could leave your hotel room.
Since then, it’s been quite strict down here. And although it’s annoying in a lot of ways, I think it’s one of the reasons our league has been able to pull this off. We’ve had no positive tests within the bubble and we are tested every day. A company called BioReference Laboratories has a setup in one of the meeting rooms here, and it’s like clockwork—we go in, we get our tests. One of my teammates missed a test and they made him stay in his room until he could get another test and get the results, so he missed a game because of that.
Henry: During this bubble time, no one has tested positive—players, coaches, staff?
Plumlee: Correct.
Henry: That’s incredible, and it’s allowed those of us who want to watch the NBA and those of you who are in it professionally to continue the sport. It must be a real nuisance for you and your family and friends, because no one can visit you, right?
Plumlee: Right. There’s no visitation. We had one false positive. It was our media relations person and the actions they took when that positive test came in -- they quarantined him in his room and interviewed everybody he had talked to; they tested anyone who had any interaction with him and those people had to go into quarantine. They’re on top of things down here. In addition to the testing, we each have a pulse oximeter and a thermometer, and we use these to check in everyday on an app. So, they’re getting all the insight they need. After the first round of the playoffs, they’re going to open the bubble to friends and family, but those friends and family will be subject to all the same protocols that we were coming in and once they’re here as well.
Henry: I’m sure you’ve heard about the Broadway star [Nick Cordero] who was healthy and suddenly got sick, lost a leg, and then lost his life. There have been some heart attacks that surprised us. Have your colleagues—players, coaches, etc.—been worried? Or are they thinking, what’s the big deal? Has the sense of how serious this is permeated through this sport?
Plumlee: The NBA is one of the groups that has heightened the understanding and awareness of this by shutting down. I think a lot of people were moving forward as is, and then, when the NBA decided to cancel the season, it let the world know, look, this is to be taken seriously.
Henry: A couple of players did test positive early on.
Plumlee: Exactly. A couple of people tested positive. I think at the outset, the unknown is always scarier. As we’ve learned more about the virus, the guys have become more comfortable. You know, I tested positive back in March. At the time, a loss of taste and smell was not a reported symptom.
Henry: And you had that?
Plumlee: I did have that, but I didn’t know what to think. More research has come out and we have a better understanding of that. I think most of the players are comfortable with the virus. We’re at a time in our lives where we’re healthy, we’re active, and we should be able to fight it off. We know the numbers for our age group. Even still, I think nobody wants to get it. Nobody wants to have to go through it. So why chance it?
Henry: Hats off to you and your sport. Other sports such as Major League Baseball haven’t been quite so successful. Of course, they’re wrestling with the players testing positive, and this has stopped games this season.
I was looking over your background prior to the interview and learned that your mother and father have been involved in the medical arena. Can you tell us about that and how it’s rubbed off on you?
Plumlee: Definitely. My mom is a pharmacist, so I spent a lot of time as a kid going to see her at work. And my dad is general counsel for an orthopedic company. My hometown is Warsaw, Ind. Some people refer to it as the “Orthopedic Capital of the World.” Zimmer Biomet is headquartered there. DePuy Synthes is there. Medtronic has offices there, as well as a lot of cottage businesses that support the orthopedic industry. In my hometown, the rock star was Dane Miller, who founded Biomet. I have no formal education in medicine or health care, but I’ve seen the impact of it. From my parents and some cousins, uncles who are doctors and surgeons, it’s been interesting to see their work and learn about what’s the latest and greatest in health care.
Henry: What’s so nice about you in particular is, with that background of interests from your family and your celebrity and accomplishments in professional basketball, you have used that to explore and promote ways to make progress in health care and help others who are less fortunate. For example, you’re involved in a telehealth platform for all-in-one practice management; affordable telehealth for pediatrics; health benefits for small businesses; prior authorization—if you can help with prior authorization, we will be in the stands for you at every game because it’s the bane of our existence; radiotherapy; and probably from mom’s background, pharmacy benefit management. Pick any of those you’d like to talk about, and tell us about your involvement and how it’s going.
Plumlee: My ticket into the arena is investment. Nobody’s calling me, asking for my expertise. But a lot of these visionary founders need financial support, and that’s where I get involved. Then also, with the celebrity angle from being an athlete, sometimes you can open doors for a start-up founder that they may not be able to open themselves.
I’m happy to speak about any of those companies. I am excited about the relaxed regulation that’s come from the pandemic; not that it’s like the Wild West out here, but I think it has allowed companies to implement solutions or think about problems in a way that they couldn’t before the pandemic. Take the prior authorization play, for example, and a company called Banjo Health, with one of my favorite founders, a guy named Saar Mahna. Medicare mandates that you turn around prior authorizations within three days. This company has an artificial intelligence and machine-learning play on prior authorizations that can deliver on that.
So efficiencies, things that increase access or affordability, better outcomes, those are the things that attract me. I lean on other people for the due diligence. The pediatric play that you referenced is a company called Blueberry Pediatrics. You have a monthly subscription for $15 that can be reimbursed by Medicaid. They send two devices to your home—an otoscope and an oximeter. The company is live in Florida right now, and it’s diverting a ton of emergency room (ER) visits. From home, for $15 a month, a mom has an otoscope and an oximeter, and she can chat or video conference with a pediatrician. There’s no additional fee. So that’s saving everyone time and saving the system money. Those are the kinds of things I’m attracted to.
Henry: You’ve touched on a couple of hot button issues for us. In oncology, unfortunately, most of our patients have pain. I am mystified every time I try to get a narcotic or a strong painkiller for a patient on a Friday night and I’m told it requires prior authorization and they’ll open up again on Monday. Well, that’s insane. These patients need something right away. So if you have a special interest in helping all of us with prior authorization, the artificial intelligence is a no brainer. If this kind of computer algorithm could happen overnight, that would be wonderful.
You mentioned the ER. Many people go to the ER as a default. They don’t know what else to do. In the COVID era, we’re trying to dial that down because we want to be able to see the sickest and have the non-sick get care elsewhere. If this particular person or people don’t know what to do, they go to the ER, it costs money, takes a lot of time, and others who may be sick are diverted from care. Families worry terribly about their children, so a device for mom and access to a pediatrician for $15 a month is another wonderful idea. These are both very interesting. Another company is in the pharmacy benefit management (PBM) space. Anything you could say about how that works?
Plumlee: I can give an overview of how I look at this as an investor in the PBM space. Three companies control about 75% of a multibillion dollar market. Several initiatives have been pursued politically to provide transparent pricing between these PBMs and pharmaceutical companies, and a lot of people are pointing fingers, but ultimately, drug prices just keep going up. Everybody knows it.
A couple of start-up founders are really set on bringing a competitive marketplace back to the pharmacy benefit manager. As an investor, when you see three people controlling a market, and you have small or medium PBMs that depend on aggregators to get competitive pricing with those big three, you get interested. It’s an interesting industry. My feeling is that somebody is going to disrupt it and bring competition back to that space. Ultimately, drug prices will come down because it’s not sustainable. The insurance companies just accommodate whatever the drug pricing is. If the drug prices go up, your premiums go up. I think these new companies will be level-setting.
Henry: In my world of oncology, we’re just a little more than halfway through 2020 and we’ve had five, six, seven new drugs approved. They all will be very expensive. One of the nicer things that’s happening and may help to tamp this down involves biosimilars. When you go to CVS or Rite Aid, you go down the aspirin aisle and see the generics, and they’re identical to the brand name aspirin. Well, these very complex molecules we used to treat cancer are antibodies or proteins, and they’re made in nature’s factories called cells. They’re not identical to the brand name drugs, but they’re called biosimilars. They work exactly the same as the branded drugs with exactly the same safety–our U.S. FDA has done a nice job of vetting that, to be sure. X, Y, Z Company has copied the brand drug after the patent expires. They were hoping for about a 30% discount in price but we’re seeing more like 15%. Nothing’s ever easy. So you make a very good point. This is not sustainable and the competition will be wonderful to tamp down these prices.
Plumlee: My hope is that those biosimilars and generics get placement in these formularies because the formularies are what’s valuable to the drug manufacturers. But they have to accommodate what the Big Three want in the PBM space. To me, making things affordable and accessible is what a lot of these startups are trying to do. And hopefully they will win.
Henry: What have you been going through, in terms of COVID? Have you recovered fully? Have your taste and smell returned, and you’re back to normal?
Plumlee: I’m all good. It caught me off guard but the symptoms weren’t too intense. For me, it was less than a flu, but more than a cold. And I’m all good today.
Henry: We’re so glad and wish you the best of luck.
Dr. Henry is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia and the host of the Blood & Cancer podcast. He has no relevant financial conflicts.
Mr. Plumlee is a board advisor to both Formsense and the Prysm Institute and a board observer with Voiceitt.
Editor’s Note: This transcript from the August 20 episode of the Blood & Cancer podcast has been edited for clarity. Click this link to listen to the full episode.
David Henry, MD: Welcome to this Blood & Cancer podcast. I’m your host, Dr. David Henry. This podcast airs on Thursday morning each week. This interview and others are archived with show notes from our residents at Pennsylvania Hospital at this link.
Each week we interview key opinion leaders involved in various aspects of blood and cancer. Mason was a first round pick in the NBA, a gold medalist for the U.S. men’s national team, and NBA All-Rookie first team honoree. He’s one of the top playmaking forwards in the country, if not the world, in my opinion. In his four-year college career at Duke University, he helped lead the Blue Devils to a National Collegiate Athletic Association (NCAA) championship and twice earned All-America first team academic honors at Duke. So he’s not just a basketball star, but an academic star as well. Mason, thanks so much for taking some time out from the bubble in Florida to talk with us today.
Mason Plumlee: Thanks for having me on. I’m happy to be here.
Henry: Beginning in March, the NBA didn’t know what to do about the COVID pandemic but finally decided to put you professional players in a ‘bubble.’ What did you have to go through to get there? You, your teammates, coaches, trainers, etc. And what’s the ongoing plan to be sure you continue to be safe?
Plumlee: Back to when the season shut down in March, the NBA shut down the practice facilities at the same time. Most people went home. I went back to Indiana. And then, as the idea of this bubble came up and the NBA formalized a plan to start the season again, players started to go back to market. I went back to Denver and was working out there.
About two weeks before we were scheduled to arrive in Orlando, they started testing us every other day. They used the deep nasal swab as well as the throat swab. But they were also taking two to three blood tests in that time period. You needed a certain number of consecutive negative tests before they would allow you to fly on the team plane down to Orlando. So there was an incredible amount of testing in the market. Once you got to Orlando, you went into a 48-hour quarantine. You had to have two negative tests with 48 hours between them before you could leave your hotel room.
Since then, it’s been quite strict down here. And although it’s annoying in a lot of ways, I think it’s one of the reasons our league has been able to pull this off. We’ve had no positive tests within the bubble and we are tested every day. A company called BioReference Laboratories has a setup in one of the meeting rooms here, and it’s like clockwork—we go in, we get our tests. One of my teammates missed a test and they made him stay in his room until he could get another test and get the results, so he missed a game because of that.
Henry: During this bubble time, no one has tested positive—players, coaches, staff?
Plumlee: Correct.
Henry: That’s incredible, and it’s allowed those of us who want to watch the NBA and those of you who are in it professionally to continue the sport. It must be a real nuisance for you and your family and friends, because no one can visit you, right?
Plumlee: Right. There’s no visitation. We had one false positive. It was our media relations person and the actions they took when that positive test came in -- they quarantined him in his room and interviewed everybody he had talked to; they tested anyone who had any interaction with him and those people had to go into quarantine. They’re on top of things down here. In addition to the testing, we each have a pulse oximeter and a thermometer, and we use these to check in everyday on an app. So, they’re getting all the insight they need. After the first round of the playoffs, they’re going to open the bubble to friends and family, but those friends and family will be subject to all the same protocols that we were coming in and once they’re here as well.
Henry: I’m sure you’ve heard about the Broadway star [Nick Cordero] who was healthy and suddenly got sick, lost a leg, and then lost his life. There have been some heart attacks that surprised us. Have your colleagues—players, coaches, etc.—been worried? Or are they thinking, what’s the big deal? Has the sense of how serious this is permeated through this sport?
Plumlee: The NBA is one of the groups that has heightened the understanding and awareness of this by shutting down. I think a lot of people were moving forward as is, and then, when the NBA decided to cancel the season, it let the world know, look, this is to be taken seriously.
Henry: A couple of players did test positive early on.
Plumlee: Exactly. A couple of people tested positive. I think at the outset, the unknown is always scarier. As we’ve learned more about the virus, the guys have become more comfortable. You know, I tested positive back in March. At the time, a loss of taste and smell was not a reported symptom.
Henry: And you had that?
Plumlee: I did have that, but I didn’t know what to think. More research has come out and we have a better understanding of that. I think most of the players are comfortable with the virus. We’re at a time in our lives where we’re healthy, we’re active, and we should be able to fight it off. We know the numbers for our age group. Even still, I think nobody wants to get it. Nobody wants to have to go through it. So why chance it?
Henry: Hats off to you and your sport. Other sports such as Major League Baseball haven’t been quite so successful. Of course, they’re wrestling with the players testing positive, and this has stopped games this season.
I was looking over your background prior to the interview and learned that your mother and father have been involved in the medical arena. Can you tell us about that and how it’s rubbed off on you?
Plumlee: Definitely. My mom is a pharmacist, so I spent a lot of time as a kid going to see her at work. And my dad is general counsel for an orthopedic company. My hometown is Warsaw, Ind. Some people refer to it as the “Orthopedic Capital of the World.” Zimmer Biomet is headquartered there. DePuy Synthes is there. Medtronic has offices there, as well as a lot of cottage businesses that support the orthopedic industry. In my hometown, the rock star was Dane Miller, who founded Biomet. I have no formal education in medicine or health care, but I’ve seen the impact of it. From my parents and some cousins, uncles who are doctors and surgeons, it’s been interesting to see their work and learn about what’s the latest and greatest in health care.
Henry: What’s so nice about you in particular is, with that background of interests from your family and your celebrity and accomplishments in professional basketball, you have used that to explore and promote ways to make progress in health care and help others who are less fortunate. For example, you’re involved in a telehealth platform for all-in-one practice management; affordable telehealth for pediatrics; health benefits for small businesses; prior authorization—if you can help with prior authorization, we will be in the stands for you at every game because it’s the bane of our existence; radiotherapy; and probably from mom’s background, pharmacy benefit management. Pick any of those you’d like to talk about, and tell us about your involvement and how it’s going.
Plumlee: My ticket into the arena is investment. Nobody’s calling me, asking for my expertise. But a lot of these visionary founders need financial support, and that’s where I get involved. Then also, with the celebrity angle from being an athlete, sometimes you can open doors for a start-up founder that they may not be able to open themselves.
I’m happy to speak about any of those companies. I am excited about the relaxed regulation that’s come from the pandemic; not that it’s like the Wild West out here, but I think it has allowed companies to implement solutions or think about problems in a way that they couldn’t before the pandemic. Take the prior authorization play, for example, and a company called Banjo Health, with one of my favorite founders, a guy named Saar Mahna. Medicare mandates that you turn around prior authorizations within three days. This company has an artificial intelligence and machine-learning play on prior authorizations that can deliver on that.
So efficiencies, things that increase access or affordability, better outcomes, those are the things that attract me. I lean on other people for the due diligence. The pediatric play that you referenced is a company called Blueberry Pediatrics. You have a monthly subscription for $15 that can be reimbursed by Medicaid. They send two devices to your home—an otoscope and an oximeter. The company is live in Florida right now, and it’s diverting a ton of emergency room (ER) visits. From home, for $15 a month, a mom has an otoscope and an oximeter, and she can chat or video conference with a pediatrician. There’s no additional fee. So that’s saving everyone time and saving the system money. Those are the kinds of things I’m attracted to.
Henry: You’ve touched on a couple of hot button issues for us. In oncology, unfortunately, most of our patients have pain. I am mystified every time I try to get a narcotic or a strong painkiller for a patient on a Friday night and I’m told it requires prior authorization and they’ll open up again on Monday. Well, that’s insane. These patients need something right away. So if you have a special interest in helping all of us with prior authorization, the artificial intelligence is a no brainer. If this kind of computer algorithm could happen overnight, that would be wonderful.
You mentioned the ER. Many people go to the ER as a default. They don’t know what else to do. In the COVID era, we’re trying to dial that down because we want to be able to see the sickest and have the non-sick get care elsewhere. If this particular person or people don’t know what to do, they go to the ER, it costs money, takes a lot of time, and others who may be sick are diverted from care. Families worry terribly about their children, so a device for mom and access to a pediatrician for $15 a month is another wonderful idea. These are both very interesting. Another company is in the pharmacy benefit management (PBM) space. Anything you could say about how that works?
Plumlee: I can give an overview of how I look at this as an investor in the PBM space. Three companies control about 75% of a multibillion dollar market. Several initiatives have been pursued politically to provide transparent pricing between these PBMs and pharmaceutical companies, and a lot of people are pointing fingers, but ultimately, drug prices just keep going up. Everybody knows it.
A couple of start-up founders are really set on bringing a competitive marketplace back to the pharmacy benefit manager. As an investor, when you see three people controlling a market, and you have small or medium PBMs that depend on aggregators to get competitive pricing with those big three, you get interested. It’s an interesting industry. My feeling is that somebody is going to disrupt it and bring competition back to that space. Ultimately, drug prices will come down because it’s not sustainable. The insurance companies just accommodate whatever the drug pricing is. If the drug prices go up, your premiums go up. I think these new companies will be level-setting.
Henry: In my world of oncology, we’re just a little more than halfway through 2020 and we’ve had five, six, seven new drugs approved. They all will be very expensive. One of the nicer things that’s happening and may help to tamp this down involves biosimilars. When you go to CVS or Rite Aid, you go down the aspirin aisle and see the generics, and they’re identical to the brand name aspirin. Well, these very complex molecules we used to treat cancer are antibodies or proteins, and they’re made in nature’s factories called cells. They’re not identical to the brand name drugs, but they’re called biosimilars. They work exactly the same as the branded drugs with exactly the same safety–our U.S. FDA has done a nice job of vetting that, to be sure. X, Y, Z Company has copied the brand drug after the patent expires. They were hoping for about a 30% discount in price but we’re seeing more like 15%. Nothing’s ever easy. So you make a very good point. This is not sustainable and the competition will be wonderful to tamp down these prices.
Plumlee: My hope is that those biosimilars and generics get placement in these formularies because the formularies are what’s valuable to the drug manufacturers. But they have to accommodate what the Big Three want in the PBM space. To me, making things affordable and accessible is what a lot of these startups are trying to do. And hopefully they will win.
Henry: What have you been going through, in terms of COVID? Have you recovered fully? Have your taste and smell returned, and you’re back to normal?
Plumlee: I’m all good. It caught me off guard but the symptoms weren’t too intense. For me, it was less than a flu, but more than a cold. And I’m all good today.
Henry: We’re so glad and wish you the best of luck.
Dr. Henry is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia and the host of the Blood & Cancer podcast. He has no relevant financial conflicts.
Mr. Plumlee is a board advisor to both Formsense and the Prysm Institute and a board observer with Voiceitt.
Editor’s Note: This transcript from the August 20 episode of the Blood & Cancer podcast has been edited for clarity. Click this link to listen to the full episode.
David Henry, MD: Welcome to this Blood & Cancer podcast. I’m your host, Dr. David Henry. This podcast airs on Thursday morning each week. This interview and others are archived with show notes from our residents at Pennsylvania Hospital at this link.
Each week we interview key opinion leaders involved in various aspects of blood and cancer. Mason was a first round pick in the NBA, a gold medalist for the U.S. men’s national team, and NBA All-Rookie first team honoree. He’s one of the top playmaking forwards in the country, if not the world, in my opinion. In his four-year college career at Duke University, he helped lead the Blue Devils to a National Collegiate Athletic Association (NCAA) championship and twice earned All-America first team academic honors at Duke. So he’s not just a basketball star, but an academic star as well. Mason, thanks so much for taking some time out from the bubble in Florida to talk with us today.
Mason Plumlee: Thanks for having me on. I’m happy to be here.
Henry: Beginning in March, the NBA didn’t know what to do about the COVID pandemic but finally decided to put you professional players in a ‘bubble.’ What did you have to go through to get there? You, your teammates, coaches, trainers, etc. And what’s the ongoing plan to be sure you continue to be safe?
Plumlee: Back to when the season shut down in March, the NBA shut down the practice facilities at the same time. Most people went home. I went back to Indiana. And then, as the idea of this bubble came up and the NBA formalized a plan to start the season again, players started to go back to market. I went back to Denver and was working out there.
About two weeks before we were scheduled to arrive in Orlando, they started testing us every other day. They used the deep nasal swab as well as the throat swab. But they were also taking two to three blood tests in that time period. You needed a certain number of consecutive negative tests before they would allow you to fly on the team plane down to Orlando. So there was an incredible amount of testing in the market. Once you got to Orlando, you went into a 48-hour quarantine. You had to have two negative tests with 48 hours between them before you could leave your hotel room.
Since then, it’s been quite strict down here. And although it’s annoying in a lot of ways, I think it’s one of the reasons our league has been able to pull this off. We’ve had no positive tests within the bubble and we are tested every day. A company called BioReference Laboratories has a setup in one of the meeting rooms here, and it’s like clockwork—we go in, we get our tests. One of my teammates missed a test and they made him stay in his room until he could get another test and get the results, so he missed a game because of that.
Henry: During this bubble time, no one has tested positive—players, coaches, staff?
Plumlee: Correct.
Henry: That’s incredible, and it’s allowed those of us who want to watch the NBA and those of you who are in it professionally to continue the sport. It must be a real nuisance for you and your family and friends, because no one can visit you, right?
Plumlee: Right. There’s no visitation. We had one false positive. It was our media relations person and the actions they took when that positive test came in -- they quarantined him in his room and interviewed everybody he had talked to; they tested anyone who had any interaction with him and those people had to go into quarantine. They’re on top of things down here. In addition to the testing, we each have a pulse oximeter and a thermometer, and we use these to check in everyday on an app. So, they’re getting all the insight they need. After the first round of the playoffs, they’re going to open the bubble to friends and family, but those friends and family will be subject to all the same protocols that we were coming in and once they’re here as well.
Henry: I’m sure you’ve heard about the Broadway star [Nick Cordero] who was healthy and suddenly got sick, lost a leg, and then lost his life. There have been some heart attacks that surprised us. Have your colleagues—players, coaches, etc.—been worried? Or are they thinking, what’s the big deal? Has the sense of how serious this is permeated through this sport?
Plumlee: The NBA is one of the groups that has heightened the understanding and awareness of this by shutting down. I think a lot of people were moving forward as is, and then, when the NBA decided to cancel the season, it let the world know, look, this is to be taken seriously.
Henry: A couple of players did test positive early on.
Plumlee: Exactly. A couple of people tested positive. I think at the outset, the unknown is always scarier. As we’ve learned more about the virus, the guys have become more comfortable. You know, I tested positive back in March. At the time, a loss of taste and smell was not a reported symptom.
Henry: And you had that?
Plumlee: I did have that, but I didn’t know what to think. More research has come out and we have a better understanding of that. I think most of the players are comfortable with the virus. We’re at a time in our lives where we’re healthy, we’re active, and we should be able to fight it off. We know the numbers for our age group. Even still, I think nobody wants to get it. Nobody wants to have to go through it. So why chance it?
Henry: Hats off to you and your sport. Other sports such as Major League Baseball haven’t been quite so successful. Of course, they’re wrestling with the players testing positive, and this has stopped games this season.
I was looking over your background prior to the interview and learned that your mother and father have been involved in the medical arena. Can you tell us about that and how it’s rubbed off on you?
Plumlee: Definitely. My mom is a pharmacist, so I spent a lot of time as a kid going to see her at work. And my dad is general counsel for an orthopedic company. My hometown is Warsaw, Ind. Some people refer to it as the “Orthopedic Capital of the World.” Zimmer Biomet is headquartered there. DePuy Synthes is there. Medtronic has offices there, as well as a lot of cottage businesses that support the orthopedic industry. In my hometown, the rock star was Dane Miller, who founded Biomet. I have no formal education in medicine or health care, but I’ve seen the impact of it. From my parents and some cousins, uncles who are doctors and surgeons, it’s been interesting to see their work and learn about what’s the latest and greatest in health care.
Henry: What’s so nice about you in particular is, with that background of interests from your family and your celebrity and accomplishments in professional basketball, you have used that to explore and promote ways to make progress in health care and help others who are less fortunate. For example, you’re involved in a telehealth platform for all-in-one practice management; affordable telehealth for pediatrics; health benefits for small businesses; prior authorization—if you can help with prior authorization, we will be in the stands for you at every game because it’s the bane of our existence; radiotherapy; and probably from mom’s background, pharmacy benefit management. Pick any of those you’d like to talk about, and tell us about your involvement and how it’s going.
Plumlee: My ticket into the arena is investment. Nobody’s calling me, asking for my expertise. But a lot of these visionary founders need financial support, and that’s where I get involved. Then also, with the celebrity angle from being an athlete, sometimes you can open doors for a start-up founder that they may not be able to open themselves.
I’m happy to speak about any of those companies. I am excited about the relaxed regulation that’s come from the pandemic; not that it’s like the Wild West out here, but I think it has allowed companies to implement solutions or think about problems in a way that they couldn’t before the pandemic. Take the prior authorization play, for example, and a company called Banjo Health, with one of my favorite founders, a guy named Saar Mahna. Medicare mandates that you turn around prior authorizations within three days. This company has an artificial intelligence and machine-learning play on prior authorizations that can deliver on that.
So efficiencies, things that increase access or affordability, better outcomes, those are the things that attract me. I lean on other people for the due diligence. The pediatric play that you referenced is a company called Blueberry Pediatrics. You have a monthly subscription for $15 that can be reimbursed by Medicaid. They send two devices to your home—an otoscope and an oximeter. The company is live in Florida right now, and it’s diverting a ton of emergency room (ER) visits. From home, for $15 a month, a mom has an otoscope and an oximeter, and she can chat or video conference with a pediatrician. There’s no additional fee. So that’s saving everyone time and saving the system money. Those are the kinds of things I’m attracted to.
Henry: You’ve touched on a couple of hot button issues for us. In oncology, unfortunately, most of our patients have pain. I am mystified every time I try to get a narcotic or a strong painkiller for a patient on a Friday night and I’m told it requires prior authorization and they’ll open up again on Monday. Well, that’s insane. These patients need something right away. So if you have a special interest in helping all of us with prior authorization, the artificial intelligence is a no brainer. If this kind of computer algorithm could happen overnight, that would be wonderful.
You mentioned the ER. Many people go to the ER as a default. They don’t know what else to do. In the COVID era, we’re trying to dial that down because we want to be able to see the sickest and have the non-sick get care elsewhere. If this particular person or people don’t know what to do, they go to the ER, it costs money, takes a lot of time, and others who may be sick are diverted from care. Families worry terribly about their children, so a device for mom and access to a pediatrician for $15 a month is another wonderful idea. These are both very interesting. Another company is in the pharmacy benefit management (PBM) space. Anything you could say about how that works?
Plumlee: I can give an overview of how I look at this as an investor in the PBM space. Three companies control about 75% of a multibillion dollar market. Several initiatives have been pursued politically to provide transparent pricing between these PBMs and pharmaceutical companies, and a lot of people are pointing fingers, but ultimately, drug prices just keep going up. Everybody knows it.
A couple of start-up founders are really set on bringing a competitive marketplace back to the pharmacy benefit manager. As an investor, when you see three people controlling a market, and you have small or medium PBMs that depend on aggregators to get competitive pricing with those big three, you get interested. It’s an interesting industry. My feeling is that somebody is going to disrupt it and bring competition back to that space. Ultimately, drug prices will come down because it’s not sustainable. The insurance companies just accommodate whatever the drug pricing is. If the drug prices go up, your premiums go up. I think these new companies will be level-setting.
Henry: In my world of oncology, we’re just a little more than halfway through 2020 and we’ve had five, six, seven new drugs approved. They all will be very expensive. One of the nicer things that’s happening and may help to tamp this down involves biosimilars. When you go to CVS or Rite Aid, you go down the aspirin aisle and see the generics, and they’re identical to the brand name aspirin. Well, these very complex molecules we used to treat cancer are antibodies or proteins, and they’re made in nature’s factories called cells. They’re not identical to the brand name drugs, but they’re called biosimilars. They work exactly the same as the branded drugs with exactly the same safety–our U.S. FDA has done a nice job of vetting that, to be sure. X, Y, Z Company has copied the brand drug after the patent expires. They were hoping for about a 30% discount in price but we’re seeing more like 15%. Nothing’s ever easy. So you make a very good point. This is not sustainable and the competition will be wonderful to tamp down these prices.
Plumlee: My hope is that those biosimilars and generics get placement in these formularies because the formularies are what’s valuable to the drug manufacturers. But they have to accommodate what the Big Three want in the PBM space. To me, making things affordable and accessible is what a lot of these startups are trying to do. And hopefully they will win.
Henry: What have you been going through, in terms of COVID? Have you recovered fully? Have your taste and smell returned, and you’re back to normal?
Plumlee: I’m all good. It caught me off guard but the symptoms weren’t too intense. For me, it was less than a flu, but more than a cold. And I’m all good today.
Henry: We’re so glad and wish you the best of luck.
Dr. Henry is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia and the host of the Blood & Cancer podcast. He has no relevant financial conflicts.
Mr. Plumlee is a board advisor to both Formsense and the Prysm Institute and a board observer with Voiceitt.
Age, smoking among leading cancer risk factors for SLE patients
A new study has quantified cancer risk factors in patients with systemic lupus erythematosus, including smoking and the use of certain medications.
“As expected, older age was associated with cancer overall, as well as with the most common cancer subtypes,” wrote Sasha Bernatsky, MD, PhD, of McGill University, Montreal, and coauthors. The study was published in Arthritis Care & Research.
To determine the risk of cancer in people with clinically confirmed incident systemic lupus erythematosus (SLE), the researchers analyzed data from 1,668 newly diagnosed lupus patients with at least one follow-up visit. All patients were enrolled in the Systemic Lupus International Collaborating Clinics inception cohort from across 33 different centers in North America, Europe, and Asia. A total of 89% (n = 1,480) were women, and 49% (n = 824) were white. The average follow-up period was 9 years.
Of the 1,668 SLE patients, 65 developed some type of cancer. The cancers included 15 breast;, 10 nonmelanoma skin; 7 lung; 6 hematologic, 6 prostate; 5 melanoma; 3 cervical; 3 renal; 2 gastric; 2 head and neck; 2 thyroid; and 1 rectal, sarcoma, thymoma, or uterine. No patient had more than one type, and the mean age of the cancer patients at time of SLE diagnosis was 45.6 (standard deviation, 14.5).
Almost half of the 65 cancers occurred in past or current smokers, including all of the lung cancers, while only 33% of patients without cancers smoked prior to baseline. After univariate analysis, characteristics associated with a higher risk of all cancers included older age at SLE diagnosis (adjusted hazard ratio, 1.05; 95% confidence interval, 1.03-1.06), White race/ethnicity (aHR 1.34; 95% CI, 0.76-2.37), and smoking (aHR 1.21; 95% CI, 0.73-2.01).
After multivariate analysis, the two characteristics most associated with increased cancer risk were older age at SLE diagnosis and being male. The analyses also confirmed that older age was a risk factor for breast cancer (aHR 1.06; 95% CI, 1.02-1.10) and nonmelanoma skin cancer (aHR, 1.06; 95% CI, 1.02-1.11), while use of antimalarial drugs was associated with a lower risk of both breast (aHR, 0.28; 95% CI, 0.09-0.90) and nonmelanoma skin (aHR, 0.23; 95% CI, 0.05-0.95) cancers. For lung cancer, the highest risk factor was smoking 15 or more cigarettes a day (aHR, 6.64; 95% CI, 1.43-30.9); for hematologic cancers, it was being in the top quartile of SLE disease activity (aHR, 7.14; 95% CI, 1.13-45.3).
The authors acknowledged their study’s limitations, including the small number of cancers overall and purposefully not comparing cancer risk in SLE patients with risk in the general population. Although their methods – “physicians recording events at annual visits, confirmed by review of charts” – were recognized as very suitable for the current analysis, they noted that a broader comparison would “potentially be problematic due to differential misclassification error” in cancer registry data.
Two of the study’s authors reported potential conflicts of interest, including receiving grants and consulting and personal fees from various pharmaceutical companies. No other potential conflicts were reported.
SOURCE: Bernatsky S et al. Arthritis Care Res. 2020 Aug 19. doi: 10.1002/acr.24425.
A new study has quantified cancer risk factors in patients with systemic lupus erythematosus, including smoking and the use of certain medications.
“As expected, older age was associated with cancer overall, as well as with the most common cancer subtypes,” wrote Sasha Bernatsky, MD, PhD, of McGill University, Montreal, and coauthors. The study was published in Arthritis Care & Research.
To determine the risk of cancer in people with clinically confirmed incident systemic lupus erythematosus (SLE), the researchers analyzed data from 1,668 newly diagnosed lupus patients with at least one follow-up visit. All patients were enrolled in the Systemic Lupus International Collaborating Clinics inception cohort from across 33 different centers in North America, Europe, and Asia. A total of 89% (n = 1,480) were women, and 49% (n = 824) were white. The average follow-up period was 9 years.
Of the 1,668 SLE patients, 65 developed some type of cancer. The cancers included 15 breast;, 10 nonmelanoma skin; 7 lung; 6 hematologic, 6 prostate; 5 melanoma; 3 cervical; 3 renal; 2 gastric; 2 head and neck; 2 thyroid; and 1 rectal, sarcoma, thymoma, or uterine. No patient had more than one type, and the mean age of the cancer patients at time of SLE diagnosis was 45.6 (standard deviation, 14.5).
Almost half of the 65 cancers occurred in past or current smokers, including all of the lung cancers, while only 33% of patients without cancers smoked prior to baseline. After univariate analysis, characteristics associated with a higher risk of all cancers included older age at SLE diagnosis (adjusted hazard ratio, 1.05; 95% confidence interval, 1.03-1.06), White race/ethnicity (aHR 1.34; 95% CI, 0.76-2.37), and smoking (aHR 1.21; 95% CI, 0.73-2.01).
After multivariate analysis, the two characteristics most associated with increased cancer risk were older age at SLE diagnosis and being male. The analyses also confirmed that older age was a risk factor for breast cancer (aHR 1.06; 95% CI, 1.02-1.10) and nonmelanoma skin cancer (aHR, 1.06; 95% CI, 1.02-1.11), while use of antimalarial drugs was associated with a lower risk of both breast (aHR, 0.28; 95% CI, 0.09-0.90) and nonmelanoma skin (aHR, 0.23; 95% CI, 0.05-0.95) cancers. For lung cancer, the highest risk factor was smoking 15 or more cigarettes a day (aHR, 6.64; 95% CI, 1.43-30.9); for hematologic cancers, it was being in the top quartile of SLE disease activity (aHR, 7.14; 95% CI, 1.13-45.3).
The authors acknowledged their study’s limitations, including the small number of cancers overall and purposefully not comparing cancer risk in SLE patients with risk in the general population. Although their methods – “physicians recording events at annual visits, confirmed by review of charts” – were recognized as very suitable for the current analysis, they noted that a broader comparison would “potentially be problematic due to differential misclassification error” in cancer registry data.
Two of the study’s authors reported potential conflicts of interest, including receiving grants and consulting and personal fees from various pharmaceutical companies. No other potential conflicts were reported.
SOURCE: Bernatsky S et al. Arthritis Care Res. 2020 Aug 19. doi: 10.1002/acr.24425.
A new study has quantified cancer risk factors in patients with systemic lupus erythematosus, including smoking and the use of certain medications.
“As expected, older age was associated with cancer overall, as well as with the most common cancer subtypes,” wrote Sasha Bernatsky, MD, PhD, of McGill University, Montreal, and coauthors. The study was published in Arthritis Care & Research.
To determine the risk of cancer in people with clinically confirmed incident systemic lupus erythematosus (SLE), the researchers analyzed data from 1,668 newly diagnosed lupus patients with at least one follow-up visit. All patients were enrolled in the Systemic Lupus International Collaborating Clinics inception cohort from across 33 different centers in North America, Europe, and Asia. A total of 89% (n = 1,480) were women, and 49% (n = 824) were white. The average follow-up period was 9 years.
Of the 1,668 SLE patients, 65 developed some type of cancer. The cancers included 15 breast;, 10 nonmelanoma skin; 7 lung; 6 hematologic, 6 prostate; 5 melanoma; 3 cervical; 3 renal; 2 gastric; 2 head and neck; 2 thyroid; and 1 rectal, sarcoma, thymoma, or uterine. No patient had more than one type, and the mean age of the cancer patients at time of SLE diagnosis was 45.6 (standard deviation, 14.5).
Almost half of the 65 cancers occurred in past or current smokers, including all of the lung cancers, while only 33% of patients without cancers smoked prior to baseline. After univariate analysis, characteristics associated with a higher risk of all cancers included older age at SLE diagnosis (adjusted hazard ratio, 1.05; 95% confidence interval, 1.03-1.06), White race/ethnicity (aHR 1.34; 95% CI, 0.76-2.37), and smoking (aHR 1.21; 95% CI, 0.73-2.01).
After multivariate analysis, the two characteristics most associated with increased cancer risk were older age at SLE diagnosis and being male. The analyses also confirmed that older age was a risk factor for breast cancer (aHR 1.06; 95% CI, 1.02-1.10) and nonmelanoma skin cancer (aHR, 1.06; 95% CI, 1.02-1.11), while use of antimalarial drugs was associated with a lower risk of both breast (aHR, 0.28; 95% CI, 0.09-0.90) and nonmelanoma skin (aHR, 0.23; 95% CI, 0.05-0.95) cancers. For lung cancer, the highest risk factor was smoking 15 or more cigarettes a day (aHR, 6.64; 95% CI, 1.43-30.9); for hematologic cancers, it was being in the top quartile of SLE disease activity (aHR, 7.14; 95% CI, 1.13-45.3).
The authors acknowledged their study’s limitations, including the small number of cancers overall and purposefully not comparing cancer risk in SLE patients with risk in the general population. Although their methods – “physicians recording events at annual visits, confirmed by review of charts” – were recognized as very suitable for the current analysis, they noted that a broader comparison would “potentially be problematic due to differential misclassification error” in cancer registry data.
Two of the study’s authors reported potential conflicts of interest, including receiving grants and consulting and personal fees from various pharmaceutical companies. No other potential conflicts were reported.
SOURCE: Bernatsky S et al. Arthritis Care Res. 2020 Aug 19. doi: 10.1002/acr.24425.
FROM ARTHRITIS CARE & RESEARCH
Subgroups predict adjuvant chemoradiotherapy benefits in low-grade glioma
Adjuvant chemoradiotherapy beat radiotherapy alone for treatment of certain patients with World Health Organization (WHO)–defined low-grade glioma (LGG), according to researchers.
Prior results from this trial, NRG Oncology/RTOG 9802 (NCT00003375), demonstrated an increase in progression-free survival (PFS) and overall survival (OS) when procarbazine, lomustine, and vincristine (PCV) chemotherapy was added to radiation in patients with high-risk LGG.
The current results, published in the Journal of Clinical Oncology, displayed highly variable survival outcomes depending on molecular subgroup.
The initial report included only IDH1 R132H immunohistochemistry data because of limited tissue availability. However, retrospective retrieval of additional tissues subsequently enabled rigorous examination of the prognostic and predictive significance of these genetic biomarkers.
Prognostic and predictive
The trial included 251 patients with LGG (grade 2). Among the 106 eligible patients with WHO-defined molecular groups successfully profiled, 26 (24%) were IDH wild-type, 43 (41%) were IDH-mutant/non-codeleted, and 37 (35%) were IDH-mutant/codeleted.
After adjustment for clinical variables and treatment, multivariate analysis confirmed WHO-defined subgroup was a significant predictor of survival. All predictive analyses, however, were considered exploratory because of small sample sizes for patients with specific biomarker features in most cases.
In prognostic multivariable analyses, significantly favorable molecular subgroup associations were observed for OS in the IDH-mutant subgroups versus that in the wild type group (IDH-mutant/codeleted group HR, 0.18; P < .0001; IDH mutant/non-codeleleted group HR, 0.56; P = .048). Individually, the statistical significance was maintained for favorable OS for IDH1/2 mutations and 1p/19q codeletions.
In the predictive analyses, OS was longer for patients harboring IDH mutant/codeleted tumors receiving radiotherapy plus PCV than for those receiving radiotherapy alone (HR, 0.21; P = .029). The median OS was 13.9 years for radiotherapy and was not reached for PCV and radiotherapy.
PFS in the IDH-mutant/codeleted subgroup also was longer for patients receiving PCV (HR, 0.13; P < .001). The median PFS was 5.8 years for radiotherapy alone and was not reached for added PCV.
In the IDH-mutant/non-codeleted subgroup, OS was longer with PCV (HR, 0.38; P = .013). The median OS was 4.3 years for radiotherapy alone and 11.4 years when PCV was added.
PFS was also longer in the IDH-mutant/non-codeleted subgroup (HR, 0.32; P = .003). The median PFS was 3.3 years for radiotherapy and 10.4 years with PCV added.
IDH–wild type patients displayed no significant clinical benefit from the addition of PCV.
“Historically, many have thought that primarily patients with codeletions received benefit from PCV,” study author Erica H. Bell, PhD, of The Ohio State University in Columbus, said in an interview. “But we showed here that there is benefit in both IDH-mutant groups.”
Primary predictor
“Our evidence suggests that IDH mutation status could serve as the primary predictor of response to PCV in addition to radiotherapy in high-risk, low-grade gliomas and is a more accurate predictor of response than historical histopathological classifications,” Dr. Bell and colleagues wrote. “Consideration should be given for adjuvant PCV in the setting of high-risk, low-grade glioma patients harboring IDH mutations.”
High-risk was defined as being 40 years or older or having a subtotal resection biopsy.
“While both IDH mutant subgroups received benefit from the addition of PCV for both overall survival and PFS, the patients in the wild-type subgroup did not do well," Dr. Bell said. "We need to treat them more aggressively. We need to determine exactly what therapy modality they should receive. This is an active question in our field.”
“Another conclusion from the study,” she added, “is that upfront tissue collection and molecular subtyping are absolutely necessary for moving our field forward.”
Finding novel biomarkers and novel therapeutic targets remain as a further goal.
Dr. Bell commented that results of the CODEL trial of temozolomide in newly diagnosed 1p/19q-codeleted anaplastic glioma are widely anticipated.
“PCV is a very toxic treatment," she said. "If another agent that is less toxic, but just as efficacious, becomes available, we would rather use that. At this point, though, there are no head-to-head trials comparing temozolomide with PCV in codeleted populations.”
The current study was sponsored by the National Cancer Institute and The Ohio State University. The authors disclosed patents, royalties, and other intellectual property.
SOURCE: Bell EH et al. J Clin Oncol. 2020. doi: 10.1200/JCO.19.02983.
Adjuvant chemoradiotherapy beat radiotherapy alone for treatment of certain patients with World Health Organization (WHO)–defined low-grade glioma (LGG), according to researchers.
Prior results from this trial, NRG Oncology/RTOG 9802 (NCT00003375), demonstrated an increase in progression-free survival (PFS) and overall survival (OS) when procarbazine, lomustine, and vincristine (PCV) chemotherapy was added to radiation in patients with high-risk LGG.
The current results, published in the Journal of Clinical Oncology, displayed highly variable survival outcomes depending on molecular subgroup.
The initial report included only IDH1 R132H immunohistochemistry data because of limited tissue availability. However, retrospective retrieval of additional tissues subsequently enabled rigorous examination of the prognostic and predictive significance of these genetic biomarkers.
Prognostic and predictive
The trial included 251 patients with LGG (grade 2). Among the 106 eligible patients with WHO-defined molecular groups successfully profiled, 26 (24%) were IDH wild-type, 43 (41%) were IDH-mutant/non-codeleted, and 37 (35%) were IDH-mutant/codeleted.
After adjustment for clinical variables and treatment, multivariate analysis confirmed WHO-defined subgroup was a significant predictor of survival. All predictive analyses, however, were considered exploratory because of small sample sizes for patients with specific biomarker features in most cases.
In prognostic multivariable analyses, significantly favorable molecular subgroup associations were observed for OS in the IDH-mutant subgroups versus that in the wild type group (IDH-mutant/codeleted group HR, 0.18; P < .0001; IDH mutant/non-codeleleted group HR, 0.56; P = .048). Individually, the statistical significance was maintained for favorable OS for IDH1/2 mutations and 1p/19q codeletions.
In the predictive analyses, OS was longer for patients harboring IDH mutant/codeleted tumors receiving radiotherapy plus PCV than for those receiving radiotherapy alone (HR, 0.21; P = .029). The median OS was 13.9 years for radiotherapy and was not reached for PCV and radiotherapy.
PFS in the IDH-mutant/codeleted subgroup also was longer for patients receiving PCV (HR, 0.13; P < .001). The median PFS was 5.8 years for radiotherapy alone and was not reached for added PCV.
In the IDH-mutant/non-codeleted subgroup, OS was longer with PCV (HR, 0.38; P = .013). The median OS was 4.3 years for radiotherapy alone and 11.4 years when PCV was added.
PFS was also longer in the IDH-mutant/non-codeleted subgroup (HR, 0.32; P = .003). The median PFS was 3.3 years for radiotherapy and 10.4 years with PCV added.
IDH–wild type patients displayed no significant clinical benefit from the addition of PCV.
“Historically, many have thought that primarily patients with codeletions received benefit from PCV,” study author Erica H. Bell, PhD, of The Ohio State University in Columbus, said in an interview. “But we showed here that there is benefit in both IDH-mutant groups.”
Primary predictor
“Our evidence suggests that IDH mutation status could serve as the primary predictor of response to PCV in addition to radiotherapy in high-risk, low-grade gliomas and is a more accurate predictor of response than historical histopathological classifications,” Dr. Bell and colleagues wrote. “Consideration should be given for adjuvant PCV in the setting of high-risk, low-grade glioma patients harboring IDH mutations.”
High-risk was defined as being 40 years or older or having a subtotal resection biopsy.
“While both IDH mutant subgroups received benefit from the addition of PCV for both overall survival and PFS, the patients in the wild-type subgroup did not do well," Dr. Bell said. "We need to treat them more aggressively. We need to determine exactly what therapy modality they should receive. This is an active question in our field.”
“Another conclusion from the study,” she added, “is that upfront tissue collection and molecular subtyping are absolutely necessary for moving our field forward.”
Finding novel biomarkers and novel therapeutic targets remain as a further goal.
Dr. Bell commented that results of the CODEL trial of temozolomide in newly diagnosed 1p/19q-codeleted anaplastic glioma are widely anticipated.
“PCV is a very toxic treatment," she said. "If another agent that is less toxic, but just as efficacious, becomes available, we would rather use that. At this point, though, there are no head-to-head trials comparing temozolomide with PCV in codeleted populations.”
The current study was sponsored by the National Cancer Institute and The Ohio State University. The authors disclosed patents, royalties, and other intellectual property.
SOURCE: Bell EH et al. J Clin Oncol. 2020. doi: 10.1200/JCO.19.02983.
Adjuvant chemoradiotherapy beat radiotherapy alone for treatment of certain patients with World Health Organization (WHO)–defined low-grade glioma (LGG), according to researchers.
Prior results from this trial, NRG Oncology/RTOG 9802 (NCT00003375), demonstrated an increase in progression-free survival (PFS) and overall survival (OS) when procarbazine, lomustine, and vincristine (PCV) chemotherapy was added to radiation in patients with high-risk LGG.
The current results, published in the Journal of Clinical Oncology, displayed highly variable survival outcomes depending on molecular subgroup.
The initial report included only IDH1 R132H immunohistochemistry data because of limited tissue availability. However, retrospective retrieval of additional tissues subsequently enabled rigorous examination of the prognostic and predictive significance of these genetic biomarkers.
Prognostic and predictive
The trial included 251 patients with LGG (grade 2). Among the 106 eligible patients with WHO-defined molecular groups successfully profiled, 26 (24%) were IDH wild-type, 43 (41%) were IDH-mutant/non-codeleted, and 37 (35%) were IDH-mutant/codeleted.
After adjustment for clinical variables and treatment, multivariate analysis confirmed WHO-defined subgroup was a significant predictor of survival. All predictive analyses, however, were considered exploratory because of small sample sizes for patients with specific biomarker features in most cases.
In prognostic multivariable analyses, significantly favorable molecular subgroup associations were observed for OS in the IDH-mutant subgroups versus that in the wild type group (IDH-mutant/codeleted group HR, 0.18; P < .0001; IDH mutant/non-codeleleted group HR, 0.56; P = .048). Individually, the statistical significance was maintained for favorable OS for IDH1/2 mutations and 1p/19q codeletions.
In the predictive analyses, OS was longer for patients harboring IDH mutant/codeleted tumors receiving radiotherapy plus PCV than for those receiving radiotherapy alone (HR, 0.21; P = .029). The median OS was 13.9 years for radiotherapy and was not reached for PCV and radiotherapy.
PFS in the IDH-mutant/codeleted subgroup also was longer for patients receiving PCV (HR, 0.13; P < .001). The median PFS was 5.8 years for radiotherapy alone and was not reached for added PCV.
In the IDH-mutant/non-codeleted subgroup, OS was longer with PCV (HR, 0.38; P = .013). The median OS was 4.3 years for radiotherapy alone and 11.4 years when PCV was added.
PFS was also longer in the IDH-mutant/non-codeleted subgroup (HR, 0.32; P = .003). The median PFS was 3.3 years for radiotherapy and 10.4 years with PCV added.
IDH–wild type patients displayed no significant clinical benefit from the addition of PCV.
“Historically, many have thought that primarily patients with codeletions received benefit from PCV,” study author Erica H. Bell, PhD, of The Ohio State University in Columbus, said in an interview. “But we showed here that there is benefit in both IDH-mutant groups.”
Primary predictor
“Our evidence suggests that IDH mutation status could serve as the primary predictor of response to PCV in addition to radiotherapy in high-risk, low-grade gliomas and is a more accurate predictor of response than historical histopathological classifications,” Dr. Bell and colleagues wrote. “Consideration should be given for adjuvant PCV in the setting of high-risk, low-grade glioma patients harboring IDH mutations.”
High-risk was defined as being 40 years or older or having a subtotal resection biopsy.
“While both IDH mutant subgroups received benefit from the addition of PCV for both overall survival and PFS, the patients in the wild-type subgroup did not do well," Dr. Bell said. "We need to treat them more aggressively. We need to determine exactly what therapy modality they should receive. This is an active question in our field.”
“Another conclusion from the study,” she added, “is that upfront tissue collection and molecular subtyping are absolutely necessary for moving our field forward.”
Finding novel biomarkers and novel therapeutic targets remain as a further goal.
Dr. Bell commented that results of the CODEL trial of temozolomide in newly diagnosed 1p/19q-codeleted anaplastic glioma are widely anticipated.
“PCV is a very toxic treatment," she said. "If another agent that is less toxic, but just as efficacious, becomes available, we would rather use that. At this point, though, there are no head-to-head trials comparing temozolomide with PCV in codeleted populations.”
The current study was sponsored by the National Cancer Institute and The Ohio State University. The authors disclosed patents, royalties, and other intellectual property.
SOURCE: Bell EH et al. J Clin Oncol. 2020. doi: 10.1200/JCO.19.02983.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Diabetes plus weight loss equals increased risk of pancreatic cancer
A new study has linked recent-onset diabetes and subsequent weight loss to an increased risk of pancreatic cancer, indicating a distinct group of individuals to screen early for this deadly disease.
“The likelihood of a pancreatic cancer diagnosis was even further elevated among individuals with older age, healthy weight before weight loss, and unintentional weight loss,” wrote Chen Yuan, ScD, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston. The study was published in JAMA Oncology.
To determine whether an association exists between diabetes plus weight change and pancreatic cancer, the researchers analyzed decades of medical history data from the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS). The study population from the NHS included 112,818 women with a mean age of 59 years; the population from the HPFS included 46,207 men with a mean age of 65 years. Since enrollment – the baseline was 1978 for the NHS and 1988 for the HPFS – participants have provided follow-up information via biennial questionnaires.
Recent diabetes onset, weight loss boost cancer risk
From those combined groups, 1,116 incident cases of pancreatic cancer (0.7%) were identified. Compared with patients with no diabetes, patients with recent-onset diabetes had triple the risk of pancreatic cancer (age-adjusted hazard ratio, 2.97; 95% confidence interval, 2.31-3.82) and patients with longstanding diabetes had more than double the risk (HR, 2.16; 95% CI, 1.78-2.60). Patients with longer disease duration also had more than twice the risk of pancreatic cancer, with HRs of 2.25 for those with diabetes for 4-10 years (95% CI, 1.74-2.92) and 2.07 for more than 10 years (95% CI, 1.61-2.66).
Compared with patients who hadn’t lost any weight, patients who reported a 1- to 4-pound weight loss (HR, 1.25; 95% CI, 1.03-1.52), a 5- to 8-pound weight loss (HR, 1.33; 95% CI, 1.06-1.66), and a more than 8-pound weight loss (HR, 1.92; 95% CI, 1.58-2.32) had higher risks of pancreatic cancer. Patients with recent-onset diabetes and a 1- to 8-pound weight loss (91 incident cases per 100,000 person-years; 95% CI, 55-151) or a weight loss of more than 8 pounds (164 incident cases per 100,000 person years; 95% CI, 114-238) had a much higher incidence of pancreatic cancer, compared with patients with neither (16 incident cases per 100,000 person-years; 95% CI, 14-17).
After stratified analyses of patients with both recent-onset diabetes and weight loss, rates of pancreatic cancer were also notably high in those 70 years or older (234 cases per 100,000 person years), those with a body mass index of less than 25 kg/m2 before weight loss (400 cases per 100,000 person years), and those with a low likelihood of intentional weight loss (334 cases per 100,000 person years).

“I like the study because it reminds us of the importance of not thinking everyone that presents with type 2 diabetes necessarily has garden-variety diabetes,” Paul Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “I have always been concerned when a new-onset diabetic individual presents with no family history of diabetes or prediabetes, especially if they’re neither overweight nor obese. I have sometimes screened those individuals for pancreatic abnormalities.”
A call for screening
“This study highlights the consideration for further screening to those with weight loss at the time of diabetes diagnosis, which is very sensible given how unusual weight loss is as a presenting symptom at the time of diagnosis of typical type 2 diabetes,” Dr. Jellinger added. “The combination of weight loss and no family history of diabetes at the time of diagnosis should be an even stronger signal for pancreatic cancer screening and potential detection at a much earlier stage.”
The authors acknowledged their study’s limitations, including some patients with pancreatic cancer not returning their questionnaires and the timing of the questionnaires meaning that patients could’ve developed diabetes after returning it. In addition, they recognized that the participants were “predominantly White health professionals” and recommended a study of “additional patient populations” in the future.
The authors noted numerous potential conflicts of interest, including receiving grants and personal fees from various initiatives, organizations, and pharmaceutical companies.
Review the “AGA Clinical Practice Update on Pancreas Cancer Screening in High-Risk Individuals: Expert Review” for best practice advice for clinicians screening and diagnosing pancreatic cancer in high-risk individuals. Learn more at http://ow.ly/vwTR30r4Zwu.
SOURCE: Yuan C et al. JAMA Oncol. 2020 Aug 13. doi: 10.1001/jamaoncol.2020.2948.
A new study has linked recent-onset diabetes and subsequent weight loss to an increased risk of pancreatic cancer, indicating a distinct group of individuals to screen early for this deadly disease.
“The likelihood of a pancreatic cancer diagnosis was even further elevated among individuals with older age, healthy weight before weight loss, and unintentional weight loss,” wrote Chen Yuan, ScD, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston. The study was published in JAMA Oncology.
To determine whether an association exists between diabetes plus weight change and pancreatic cancer, the researchers analyzed decades of medical history data from the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS). The study population from the NHS included 112,818 women with a mean age of 59 years; the population from the HPFS included 46,207 men with a mean age of 65 years. Since enrollment – the baseline was 1978 for the NHS and 1988 for the HPFS – participants have provided follow-up information via biennial questionnaires.
Recent diabetes onset, weight loss boost cancer risk
From those combined groups, 1,116 incident cases of pancreatic cancer (0.7%) were identified. Compared with patients with no diabetes, patients with recent-onset diabetes had triple the risk of pancreatic cancer (age-adjusted hazard ratio, 2.97; 95% confidence interval, 2.31-3.82) and patients with longstanding diabetes had more than double the risk (HR, 2.16; 95% CI, 1.78-2.60). Patients with longer disease duration also had more than twice the risk of pancreatic cancer, with HRs of 2.25 for those with diabetes for 4-10 years (95% CI, 1.74-2.92) and 2.07 for more than 10 years (95% CI, 1.61-2.66).
Compared with patients who hadn’t lost any weight, patients who reported a 1- to 4-pound weight loss (HR, 1.25; 95% CI, 1.03-1.52), a 5- to 8-pound weight loss (HR, 1.33; 95% CI, 1.06-1.66), and a more than 8-pound weight loss (HR, 1.92; 95% CI, 1.58-2.32) had higher risks of pancreatic cancer. Patients with recent-onset diabetes and a 1- to 8-pound weight loss (91 incident cases per 100,000 person-years; 95% CI, 55-151) or a weight loss of more than 8 pounds (164 incident cases per 100,000 person years; 95% CI, 114-238) had a much higher incidence of pancreatic cancer, compared with patients with neither (16 incident cases per 100,000 person-years; 95% CI, 14-17).
After stratified analyses of patients with both recent-onset diabetes and weight loss, rates of pancreatic cancer were also notably high in those 70 years or older (234 cases per 100,000 person years), those with a body mass index of less than 25 kg/m2 before weight loss (400 cases per 100,000 person years), and those with a low likelihood of intentional weight loss (334 cases per 100,000 person years).
“I like the study because it reminds us of the importance of not thinking everyone that presents with type 2 diabetes necessarily has garden-variety diabetes,” Paul Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “I have always been concerned when a new-onset diabetic individual presents with no family history of diabetes or prediabetes, especially if they’re neither overweight nor obese. I have sometimes screened those individuals for pancreatic abnormalities.”
A call for screening
“This study highlights the consideration for further screening to those with weight loss at the time of diabetes diagnosis, which is very sensible given how unusual weight loss is as a presenting symptom at the time of diagnosis of typical type 2 diabetes,” Dr. Jellinger added. “The combination of weight loss and no family history of diabetes at the time of diagnosis should be an even stronger signal for pancreatic cancer screening and potential detection at a much earlier stage.”
The authors acknowledged their study’s limitations, including some patients with pancreatic cancer not returning their questionnaires and the timing of the questionnaires meaning that patients could’ve developed diabetes after returning it. In addition, they recognized that the participants were “predominantly White health professionals” and recommended a study of “additional patient populations” in the future.
The authors noted numerous potential conflicts of interest, including receiving grants and personal fees from various initiatives, organizations, and pharmaceutical companies.
Review the “AGA Clinical Practice Update on Pancreas Cancer Screening in High-Risk Individuals: Expert Review” for best practice advice for clinicians screening and diagnosing pancreatic cancer in high-risk individuals. Learn more at http://ow.ly/vwTR30r4Zwu.
SOURCE: Yuan C et al. JAMA Oncol. 2020 Aug 13. doi: 10.1001/jamaoncol.2020.2948.
A new study has linked recent-onset diabetes and subsequent weight loss to an increased risk of pancreatic cancer, indicating a distinct group of individuals to screen early for this deadly disease.
“The likelihood of a pancreatic cancer diagnosis was even further elevated among individuals with older age, healthy weight before weight loss, and unintentional weight loss,” wrote Chen Yuan, ScD, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston. The study was published in JAMA Oncology.
To determine whether an association exists between diabetes plus weight change and pancreatic cancer, the researchers analyzed decades of medical history data from the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS). The study population from the NHS included 112,818 women with a mean age of 59 years; the population from the HPFS included 46,207 men with a mean age of 65 years. Since enrollment – the baseline was 1978 for the NHS and 1988 for the HPFS – participants have provided follow-up information via biennial questionnaires.
Recent diabetes onset, weight loss boost cancer risk
From those combined groups, 1,116 incident cases of pancreatic cancer (0.7%) were identified. Compared with patients with no diabetes, patients with recent-onset diabetes had triple the risk of pancreatic cancer (age-adjusted hazard ratio, 2.97; 95% confidence interval, 2.31-3.82) and patients with longstanding diabetes had more than double the risk (HR, 2.16; 95% CI, 1.78-2.60). Patients with longer disease duration also had more than twice the risk of pancreatic cancer, with HRs of 2.25 for those with diabetes for 4-10 years (95% CI, 1.74-2.92) and 2.07 for more than 10 years (95% CI, 1.61-2.66).
Compared with patients who hadn’t lost any weight, patients who reported a 1- to 4-pound weight loss (HR, 1.25; 95% CI, 1.03-1.52), a 5- to 8-pound weight loss (HR, 1.33; 95% CI, 1.06-1.66), and a more than 8-pound weight loss (HR, 1.92; 95% CI, 1.58-2.32) had higher risks of pancreatic cancer. Patients with recent-onset diabetes and a 1- to 8-pound weight loss (91 incident cases per 100,000 person-years; 95% CI, 55-151) or a weight loss of more than 8 pounds (164 incident cases per 100,000 person years; 95% CI, 114-238) had a much higher incidence of pancreatic cancer, compared with patients with neither (16 incident cases per 100,000 person-years; 95% CI, 14-17).
After stratified analyses of patients with both recent-onset diabetes and weight loss, rates of pancreatic cancer were also notably high in those 70 years or older (234 cases per 100,000 person years), those with a body mass index of less than 25 kg/m2 before weight loss (400 cases per 100,000 person years), and those with a low likelihood of intentional weight loss (334 cases per 100,000 person years).
“I like the study because it reminds us of the importance of not thinking everyone that presents with type 2 diabetes necessarily has garden-variety diabetes,” Paul Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “I have always been concerned when a new-onset diabetic individual presents with no family history of diabetes or prediabetes, especially if they’re neither overweight nor obese. I have sometimes screened those individuals for pancreatic abnormalities.”
A call for screening
“This study highlights the consideration for further screening to those with weight loss at the time of diabetes diagnosis, which is very sensible given how unusual weight loss is as a presenting symptom at the time of diagnosis of typical type 2 diabetes,” Dr. Jellinger added. “The combination of weight loss and no family history of diabetes at the time of diagnosis should be an even stronger signal for pancreatic cancer screening and potential detection at a much earlier stage.”
The authors acknowledged their study’s limitations, including some patients with pancreatic cancer not returning their questionnaires and the timing of the questionnaires meaning that patients could’ve developed diabetes after returning it. In addition, they recognized that the participants were “predominantly White health professionals” and recommended a study of “additional patient populations” in the future.
The authors noted numerous potential conflicts of interest, including receiving grants and personal fees from various initiatives, organizations, and pharmaceutical companies.
Review the “AGA Clinical Practice Update on Pancreas Cancer Screening in High-Risk Individuals: Expert Review” for best practice advice for clinicians screening and diagnosing pancreatic cancer in high-risk individuals. Learn more at http://ow.ly/vwTR30r4Zwu.
SOURCE: Yuan C et al. JAMA Oncol. 2020 Aug 13. doi: 10.1001/jamaoncol.2020.2948.
FROM JAMA ONCOLOGY