User login
1.04 Common Clinical Diagnoses and Conditions: Altered Mental Status
Introduction
Altered mental status (AMS) is a descriptive term that encompasses a wide spectrum of signs and symptoms, ranging from vague complaints of atypical behavior and irritability, to more specific concerns related to both hyperactive states (such as agitation) and hypoactive states (such as lethargy, depressed levels of responsiveness, and loss of consciousness). AMS may be particularly difficult to recognize in very young children and children with medical complexity. Pediatric hospitalists frequently encounter children with AMS, either as a primary cause for admission or a secondary finding during hospitalization, and therefore they must be knowledgeable about the differential diagnosis and various organ system manifestations that may be involved. Pediatric hospitalists must be able to accurately recognize early signs of AMS, triage acuity, and provide prompt stabilization, which is critical to effective management of patients with this condition.
Knowledge
Pediatric Hospitalists should be able to:
- Compare and contrast the different presentations of AMS, and describe the differential diagnosis associated with each for varying chronological or developmental ages.
- Identify the elements of the Glasgow Coma Scale and discuss the implications of the score or a change in score on management of a child with AMS.
- Discuss the features of the medical history and physical examination that prompt specific diagnostic evaluation, including signs and symptoms that warrant urgent management.
- Compare and contrast different features of toxidromes that may present with AMS.
- Discuss approaches to stabilization of a child with AMS, including evaluation of airway, breathing, circulation, disability, exposure, and intracranial perfusion.
- Define the indications to activate a rapid response, code blue, or other local emergency system for children with AMS.
- Explain indications for hospitalization of children with AMS.
- Summarize the initial approach to management of common conditions presenting with AMS, including but not limited to: seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Discuss specific considerations for children with medical complexity presenting with AMS, including those with intellectual disability, impaired communication, epilepsy, dystonia, ventricular shunts, ventilator dependence, enteral feeding tubes, and multiple medications.
- Discuss the mechanisms of action of common medications used for delirium or agitation.
- Discuss the mechanisms of action of medications used for increased intracranial pressure (such as mannitol, 3% hypertonic saline, and others).
- List medications commonly used in the inpatient setting that may cause AMS as a side effect of use or withdrawal of use, such as seizure medications, opioids, benzodiazepines, anti-cholinergic medications, barbiturates, cannabinoids, and others.
- Explain the indications for chemical versus physical restraints, one-to-one supervision, and involvement of hospital security to ensure safety of the patient, family, and staff.
- Describe indications for urgent subspecialist consultation for children with AMS (such as toxicology, rheumatology, neurology, neurosurgery, and others).
- Discuss reasons for transfer to higher level of care, within the institution or elsewhere if pediatric-specific or psychiatric services are not available at the local facility.
- Describe the reasons for ancillary service involvement (such as physical, occupational, speech, feeding, behavioral therapies, and others) and durable medical equipment procurement for children with AMS.
- List criteria for inpatient rehabilitation.
- Discuss indications for involvement of social work, child protective services, or law enforcement for children with AMS.
Skills
Pediatric Hospitalists should be able to:
- Elicit a thorough medical history, attending to a detailed care provider history, past medical history, exposures, medications, and medications in the home.
- Perform a physical exam to elicit signs of AMS, including evaluation of airway, breathing, circulation, psychiatric status, and the central and autonomic nervous system.
- Assign an accurate Glasgow Coma Scale score.
- Identify children with potentially reversible, life-threatening conditions, and promptly provide stabilizing measures, activating code or rapid response teams as indicated.
- Review medication list and note any potentially relevant interactions or adverse effects.
- Direct an appropriate, cost-effective evaluation to identify the cause of AMS and correctly interpret results, including performance of a lumbar puncture as indicated.
- Perform careful reassessments (such as serial neurological exams, Glasgow Coma Scale scoring, and others), identifying indications for adjustment to the plan of care, frequency of monitoring, and type of monitoring indicated.
- Identify and manage children who present with altered mental status secondary to common conditions, such as seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Engage consultants, including neurologists, neurosurgeons, neuroradiologists, toxicologists, psychiatrists, and psychologists efficiently and appropriately.
- Coordinate care and communicate effectively with caregivers, primary care providers, and consultants about the mental status at the time of discharge and the transition plan, referring to ancillary or rehabilitation services as appropriate.
Attitudes
Pediatric Hospitalists should be able to:
- Realize responsibility for reporting of iatrogenic etiologies as appropriate.
- Acknowledge the need for effective communication with subspecialty providers, primary care providers, and the patients and the family/caregivers to ensure ongoing support and coordinated care.
- Realize responsibility for effective and compassionate communication with patients/caregivers regarding findings, prognosis, and treatments, accounting for the stresses of hospitalization.
- Collaborate with social work, child protective services, and law enforcement when indicated.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Work with hospital administration and staff to develop, implement, and assess outcomes of intervention strategies for hospitalized patients with deterioration of mental status to prevent adverse outcomes (such as rapid response, code blue, stroke teams, and others).
- Coordinate educational programs for front-line providers to promote early recognition of AMS.
- Lead, coordinate, or participate in institutional efforts to report and reduce cases of AMS due to iatrogenic causes or adverse effects of medications.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
Introduction
Altered mental status (AMS) is a descriptive term that encompasses a wide spectrum of signs and symptoms, ranging from vague complaints of atypical behavior and irritability, to more specific concerns related to both hyperactive states (such as agitation) and hypoactive states (such as lethargy, depressed levels of responsiveness, and loss of consciousness). AMS may be particularly difficult to recognize in very young children and children with medical complexity. Pediatric hospitalists frequently encounter children with AMS, either as a primary cause for admission or a secondary finding during hospitalization, and therefore they must be knowledgeable about the differential diagnosis and various organ system manifestations that may be involved. Pediatric hospitalists must be able to accurately recognize early signs of AMS, triage acuity, and provide prompt stabilization, which is critical to effective management of patients with this condition.
Knowledge
Pediatric Hospitalists should be able to:
- Compare and contrast the different presentations of AMS, and describe the differential diagnosis associated with each for varying chronological or developmental ages.
- Identify the elements of the Glasgow Coma Scale and discuss the implications of the score or a change in score on management of a child with AMS.
- Discuss the features of the medical history and physical examination that prompt specific diagnostic evaluation, including signs and symptoms that warrant urgent management.
- Compare and contrast different features of toxidromes that may present with AMS.
- Discuss approaches to stabilization of a child with AMS, including evaluation of airway, breathing, circulation, disability, exposure, and intracranial perfusion.
- Define the indications to activate a rapid response, code blue, or other local emergency system for children with AMS.
- Explain indications for hospitalization of children with AMS.
- Summarize the initial approach to management of common conditions presenting with AMS, including but not limited to: seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Discuss specific considerations for children with medical complexity presenting with AMS, including those with intellectual disability, impaired communication, epilepsy, dystonia, ventricular shunts, ventilator dependence, enteral feeding tubes, and multiple medications.
- Discuss the mechanisms of action of common medications used for delirium or agitation.
- Discuss the mechanisms of action of medications used for increased intracranial pressure (such as mannitol, 3% hypertonic saline, and others).
- List medications commonly used in the inpatient setting that may cause AMS as a side effect of use or withdrawal of use, such as seizure medications, opioids, benzodiazepines, anti-cholinergic medications, barbiturates, cannabinoids, and others.
- Explain the indications for chemical versus physical restraints, one-to-one supervision, and involvement of hospital security to ensure safety of the patient, family, and staff.
- Describe indications for urgent subspecialist consultation for children with AMS (such as toxicology, rheumatology, neurology, neurosurgery, and others).
- Discuss reasons for transfer to higher level of care, within the institution or elsewhere if pediatric-specific or psychiatric services are not available at the local facility.
- Describe the reasons for ancillary service involvement (such as physical, occupational, speech, feeding, behavioral therapies, and others) and durable medical equipment procurement for children with AMS.
- List criteria for inpatient rehabilitation.
- Discuss indications for involvement of social work, child protective services, or law enforcement for children with AMS.
Skills
Pediatric Hospitalists should be able to:
- Elicit a thorough medical history, attending to a detailed care provider history, past medical history, exposures, medications, and medications in the home.
- Perform a physical exam to elicit signs of AMS, including evaluation of airway, breathing, circulation, psychiatric status, and the central and autonomic nervous system.
- Assign an accurate Glasgow Coma Scale score.
- Identify children with potentially reversible, life-threatening conditions, and promptly provide stabilizing measures, activating code or rapid response teams as indicated.
- Review medication list and note any potentially relevant interactions or adverse effects.
- Direct an appropriate, cost-effective evaluation to identify the cause of AMS and correctly interpret results, including performance of a lumbar puncture as indicated.
- Perform careful reassessments (such as serial neurological exams, Glasgow Coma Scale scoring, and others), identifying indications for adjustment to the plan of care, frequency of monitoring, and type of monitoring indicated.
- Identify and manage children who present with altered mental status secondary to common conditions, such as seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Engage consultants, including neurologists, neurosurgeons, neuroradiologists, toxicologists, psychiatrists, and psychologists efficiently and appropriately.
- Coordinate care and communicate effectively with caregivers, primary care providers, and consultants about the mental status at the time of discharge and the transition plan, referring to ancillary or rehabilitation services as appropriate.
Attitudes
Pediatric Hospitalists should be able to:
- Realize responsibility for reporting of iatrogenic etiologies as appropriate.
- Acknowledge the need for effective communication with subspecialty providers, primary care providers, and the patients and the family/caregivers to ensure ongoing support and coordinated care.
- Realize responsibility for effective and compassionate communication with patients/caregivers regarding findings, prognosis, and treatments, accounting for the stresses of hospitalization.
- Collaborate with social work, child protective services, and law enforcement when indicated.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Work with hospital administration and staff to develop, implement, and assess outcomes of intervention strategies for hospitalized patients with deterioration of mental status to prevent adverse outcomes (such as rapid response, code blue, stroke teams, and others).
- Coordinate educational programs for front-line providers to promote early recognition of AMS.
- Lead, coordinate, or participate in institutional efforts to report and reduce cases of AMS due to iatrogenic causes or adverse effects of medications.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
Introduction
Altered mental status (AMS) is a descriptive term that encompasses a wide spectrum of signs and symptoms, ranging from vague complaints of atypical behavior and irritability, to more specific concerns related to both hyperactive states (such as agitation) and hypoactive states (such as lethargy, depressed levels of responsiveness, and loss of consciousness). AMS may be particularly difficult to recognize in very young children and children with medical complexity. Pediatric hospitalists frequently encounter children with AMS, either as a primary cause for admission or a secondary finding during hospitalization, and therefore they must be knowledgeable about the differential diagnosis and various organ system manifestations that may be involved. Pediatric hospitalists must be able to accurately recognize early signs of AMS, triage acuity, and provide prompt stabilization, which is critical to effective management of patients with this condition.
Knowledge
Pediatric Hospitalists should be able to:
- Compare and contrast the different presentations of AMS, and describe the differential diagnosis associated with each for varying chronological or developmental ages.
- Identify the elements of the Glasgow Coma Scale and discuss the implications of the score or a change in score on management of a child with AMS.
- Discuss the features of the medical history and physical examination that prompt specific diagnostic evaluation, including signs and symptoms that warrant urgent management.
- Compare and contrast different features of toxidromes that may present with AMS.
- Discuss approaches to stabilization of a child with AMS, including evaluation of airway, breathing, circulation, disability, exposure, and intracranial perfusion.
- Define the indications to activate a rapid response, code blue, or other local emergency system for children with AMS.
- Explain indications for hospitalization of children with AMS.
- Summarize the initial approach to management of common conditions presenting with AMS, including but not limited to: seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Discuss specific considerations for children with medical complexity presenting with AMS, including those with intellectual disability, impaired communication, epilepsy, dystonia, ventricular shunts, ventilator dependence, enteral feeding tubes, and multiple medications.
- Discuss the mechanisms of action of common medications used for delirium or agitation.
- Discuss the mechanisms of action of medications used for increased intracranial pressure (such as mannitol, 3% hypertonic saline, and others).
- List medications commonly used in the inpatient setting that may cause AMS as a side effect of use or withdrawal of use, such as seizure medications, opioids, benzodiazepines, anti-cholinergic medications, barbiturates, cannabinoids, and others.
- Explain the indications for chemical versus physical restraints, one-to-one supervision, and involvement of hospital security to ensure safety of the patient, family, and staff.
- Describe indications for urgent subspecialist consultation for children with AMS (such as toxicology, rheumatology, neurology, neurosurgery, and others).
- Discuss reasons for transfer to higher level of care, within the institution or elsewhere if pediatric-specific or psychiatric services are not available at the local facility.
- Describe the reasons for ancillary service involvement (such as physical, occupational, speech, feeding, behavioral therapies, and others) and durable medical equipment procurement for children with AMS.
- List criteria for inpatient rehabilitation.
- Discuss indications for involvement of social work, child protective services, or law enforcement for children with AMS.
Skills
Pediatric Hospitalists should be able to:
- Elicit a thorough medical history, attending to a detailed care provider history, past medical history, exposures, medications, and medications in the home.
- Perform a physical exam to elicit signs of AMS, including evaluation of airway, breathing, circulation, psychiatric status, and the central and autonomic nervous system.
- Assign an accurate Glasgow Coma Scale score.
- Identify children with potentially reversible, life-threatening conditions, and promptly provide stabilizing measures, activating code or rapid response teams as indicated.
- Review medication list and note any potentially relevant interactions or adverse effects.
- Direct an appropriate, cost-effective evaluation to identify the cause of AMS and correctly interpret results, including performance of a lumbar puncture as indicated.
- Perform careful reassessments (such as serial neurological exams, Glasgow Coma Scale scoring, and others), identifying indications for adjustment to the plan of care, frequency of monitoring, and type of monitoring indicated.
- Identify and manage children who present with altered mental status secondary to common conditions, such as seizures, increased intracranial pressure, intracranial hemorrhage, infectious or inflammatory encephalitis, sepsis, shock, hypoglycemia, diabetic ketoacidosis, renal or liver failure, neoplastic syndromes, suspected toxic ingestion, medication overdose, and adverse drug reaction.
- Engage consultants, including neurologists, neurosurgeons, neuroradiologists, toxicologists, psychiatrists, and psychologists efficiently and appropriately.
- Coordinate care and communicate effectively with caregivers, primary care providers, and consultants about the mental status at the time of discharge and the transition plan, referring to ancillary or rehabilitation services as appropriate.
Attitudes
Pediatric Hospitalists should be able to:
- Realize responsibility for reporting of iatrogenic etiologies as appropriate.
- Acknowledge the need for effective communication with subspecialty providers, primary care providers, and the patients and the family/caregivers to ensure ongoing support and coordinated care.
- Realize responsibility for effective and compassionate communication with patients/caregivers regarding findings, prognosis, and treatments, accounting for the stresses of hospitalization.
- Collaborate with social work, child protective services, and law enforcement when indicated.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Work with hospital administration and staff to develop, implement, and assess outcomes of intervention strategies for hospitalized patients with deterioration of mental status to prevent adverse outcomes (such as rapid response, code blue, stroke teams, and others).
- Coordinate educational programs for front-line providers to promote early recognition of AMS.
- Lead, coordinate, or participate in institutional efforts to report and reduce cases of AMS due to iatrogenic causes or adverse effects of medications.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
1. Lehman RK, Mink J. Altered mental status. Clin Pediatr Emerg Med. 2008; 9:68-75.
2. Avner JR. Altered states of consciousness. Pediatr Rev. 2006; 27:331-338. https://doi.org/10.1542/pir.27-9-331.
3. Malas N, Brahmbhatt K, McDermott C, Smith A. Ortiz-Aguayo R, Turkel S. Pediatric delirium: Evaluation, management, and special considerations. Curr Psychiatry Rep. 2017;19(9):65. https://doi.org/10.1007/s11920-017-0817-3.
1.03 Common Clinical Diagnoses and Conditions: Acute Respiratory Failure
Introduction
Respiratory failure is defined by inadequate gas exchange by the respiratory system that results in ineffective alveolar ventilation and/or oxygenation. Acute respiratory failure is more common in children than adults and is the primary cause of cardiopulmonary arrest in children. The differential diagnosis for acute respiratory failure in children is extensive, as failure may stem from any portion of the respiratory system or be a consequence of systemic disease. Pediatric hospitalists frequently encounter children with conditions affecting the respiratory system and should be able to anticipate, identify, and treat acute respiratory distress and acute respiratory failure in children, including those with chronic respiratory conditions and other comorbidities.
Knowledge
Pediatric hospitalists should be able to:
- Describe the structure and function respiratory system components, including upper and lower airways, muscles of respiration, and central and peripheral regulation systems.
- Explain developmental differences that contribute to acute respiratory failure in infants and young children, including upper airway size, lower airway growth and development, diaphragmatic muscle reserve, chest wall compliance, and respiratory regulatory center maturity.
- Discuss the basic principles of respiratory physiology, including the alveolar gas equation, minute ventilation, and alveolar-arterial gradient.
- Summarize the five causes of hypoxemia: ventilation-perfusion mismatch, hypoventilation, right to left shunt, diffusion impairment, and low inspired oxygen.
- Construct an age-based differential diagnosis for acute respiratory distress in children.
- List causes of poor respiratory muscle function, attending to age, neuromuscular disorders, central nervous system dysfunction, nerve injury, and others.
- Discuss comorbidities that place children at higher risk for acute respiratory failure.
- Summarize evaluation, monitoring, and treatment options for patients with worsening respiratory status, including mental status assessment, blood gas analysis, medications, and respiratory support.
- Describe the signs and symptoms of impending acute respiratory failure, including criteria for transfer to a higher level of care.
- Discuss the advantages and disadvantages of different supplemental oxygen delivery devices for children with and without medical complexity, such as low flow and heated high-flow nasal cannula, simple mask, partial rebreather or non-rebreather, and tracheostomy collar or mask.
- Summarize the modalities commonly available to support the airway and adequate gas exchange in children with worsening respiratory distress, including nasopharyngeal or oropharyngeal airways, bag-valve-mask ventilation, bi-level positive airway pressure, continuous positive airway pressure, endotracheal tube, and laryngeal-mask-airway intubation.
- Describe criteria for, risks of, and complications due to endotracheal or laryngeal-mask-airway intubation, including strategies to reduce these risks.
- Compare and contrast optimal treatment strategies for acute respiratory failure in children with common acute respiratory conditions, including asthma, bronchiolitis, croup, and pneumonia.
Skills
Pediatric hospitalists should be able to:
- Perform and teach other health care providers to perform a thorough respiratory assessment of a child with acute respiratory distress.
- Identify early warning signs of acute respiratory distress and institute corrective actions and therapies to avert further deterioration.
- Identify patients with comorbidities and other risk factors for progression to acute respiratory failure.
- Order appropriate monitoring and relevant testing (such as radiographs and blood gases) and correctly interpret their results.
- Diagnose and initiate medical management for systemic causes of acute respiratory failure.
- Identify signs and symptoms of impending acute respiratory failure and activate local emergency response teams and/or transfer patients to an appropriate site with critical care services in a safe and efficient manner.
- Initiate oxygen supplementation via oxygen delivery devices and escalate as required to manage hypoxia and/or acute respiratory distress.
- Stabilize the airway, using non-invasive airway management techniques independently and invasive airway management in collaboration with other services.
- Demonstrate proficiency in basic management of patients with chronic respiratory support needs.
- Identify patients requiring subspecialty care and obtain timely consults.
Attitudes
Pediatric hospitalists should be able to:
- Acknowledge the importance of collaboration with patients, the family/caregivers, hospital staff, and subspecialists to ensure family-centered, coordinated hospital care for children with conditions at risk for acute respiratory failure.
- Realize the value of providing consultation for healthcare providers in community settings to ensure transport of patients to higher acuity settings as needed.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in educational programs for the family/caregivers, hospital staff, and other healthcare providers regarding recognition of signs and symptoms of acute respiratory distress in children, particularly those at higher risk for acute respiratory failure.
- Work with hospital administration, hospital staff, subspecialists, and others to develop, implement, and assess outcomes of intervention strategies such as rapid response teams and early warning scores for hospitalized patients with deterioration in respiratory status in order to prevent adverse outcomes.
- Work with hospital administration, hospital staff, pharmacy, and others to ensure availability of medications and appropriately sized equipment for use in the management of acute respiratory failure in children.
1. Samson RA, Schexnayder SM, Hazinski MF, et al. Part 3 Systematic approach to the seriously ill or injured child, Part 6 Recognition of Respiratory Distress and Failure, and Part 7 Management of Respiratory Distress and Failure. In: Pediatric Advanced Life Support: Provider Manual. Dallas, TX: American Heart Association; 2016;29-68; 113-170.
2. Hammer J. Acute respiratory failure in children. Paediatr Respir Rev. 2013; 14:64-69. https://doi.org/10.1016/j.prrv.2013.02.001.
Introduction
Respiratory failure is defined by inadequate gas exchange by the respiratory system that results in ineffective alveolar ventilation and/or oxygenation. Acute respiratory failure is more common in children than adults and is the primary cause of cardiopulmonary arrest in children. The differential diagnosis for acute respiratory failure in children is extensive, as failure may stem from any portion of the respiratory system or be a consequence of systemic disease. Pediatric hospitalists frequently encounter children with conditions affecting the respiratory system and should be able to anticipate, identify, and treat acute respiratory distress and acute respiratory failure in children, including those with chronic respiratory conditions and other comorbidities.
Knowledge
Pediatric hospitalists should be able to:
- Describe the structure and function respiratory system components, including upper and lower airways, muscles of respiration, and central and peripheral regulation systems.
- Explain developmental differences that contribute to acute respiratory failure in infants and young children, including upper airway size, lower airway growth and development, diaphragmatic muscle reserve, chest wall compliance, and respiratory regulatory center maturity.
- Discuss the basic principles of respiratory physiology, including the alveolar gas equation, minute ventilation, and alveolar-arterial gradient.
- Summarize the five causes of hypoxemia: ventilation-perfusion mismatch, hypoventilation, right to left shunt, diffusion impairment, and low inspired oxygen.
- Construct an age-based differential diagnosis for acute respiratory distress in children.
- List causes of poor respiratory muscle function, attending to age, neuromuscular disorders, central nervous system dysfunction, nerve injury, and others.
- Discuss comorbidities that place children at higher risk for acute respiratory failure.
- Summarize evaluation, monitoring, and treatment options for patients with worsening respiratory status, including mental status assessment, blood gas analysis, medications, and respiratory support.
- Describe the signs and symptoms of impending acute respiratory failure, including criteria for transfer to a higher level of care.
- Discuss the advantages and disadvantages of different supplemental oxygen delivery devices for children with and without medical complexity, such as low flow and heated high-flow nasal cannula, simple mask, partial rebreather or non-rebreather, and tracheostomy collar or mask.
- Summarize the modalities commonly available to support the airway and adequate gas exchange in children with worsening respiratory distress, including nasopharyngeal or oropharyngeal airways, bag-valve-mask ventilation, bi-level positive airway pressure, continuous positive airway pressure, endotracheal tube, and laryngeal-mask-airway intubation.
- Describe criteria for, risks of, and complications due to endotracheal or laryngeal-mask-airway intubation, including strategies to reduce these risks.
- Compare and contrast optimal treatment strategies for acute respiratory failure in children with common acute respiratory conditions, including asthma, bronchiolitis, croup, and pneumonia.
Skills
Pediatric hospitalists should be able to:
- Perform and teach other health care providers to perform a thorough respiratory assessment of a child with acute respiratory distress.
- Identify early warning signs of acute respiratory distress and institute corrective actions and therapies to avert further deterioration.
- Identify patients with comorbidities and other risk factors for progression to acute respiratory failure.
- Order appropriate monitoring and relevant testing (such as radiographs and blood gases) and correctly interpret their results.
- Diagnose and initiate medical management for systemic causes of acute respiratory failure.
- Identify signs and symptoms of impending acute respiratory failure and activate local emergency response teams and/or transfer patients to an appropriate site with critical care services in a safe and efficient manner.
- Initiate oxygen supplementation via oxygen delivery devices and escalate as required to manage hypoxia and/or acute respiratory distress.
- Stabilize the airway, using non-invasive airway management techniques independently and invasive airway management in collaboration with other services.
- Demonstrate proficiency in basic management of patients with chronic respiratory support needs.
- Identify patients requiring subspecialty care and obtain timely consults.
Attitudes
Pediatric hospitalists should be able to:
- Acknowledge the importance of collaboration with patients, the family/caregivers, hospital staff, and subspecialists to ensure family-centered, coordinated hospital care for children with conditions at risk for acute respiratory failure.
- Realize the value of providing consultation for healthcare providers in community settings to ensure transport of patients to higher acuity settings as needed.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in educational programs for the family/caregivers, hospital staff, and other healthcare providers regarding recognition of signs and symptoms of acute respiratory distress in children, particularly those at higher risk for acute respiratory failure.
- Work with hospital administration, hospital staff, subspecialists, and others to develop, implement, and assess outcomes of intervention strategies such as rapid response teams and early warning scores for hospitalized patients with deterioration in respiratory status in order to prevent adverse outcomes.
- Work with hospital administration, hospital staff, pharmacy, and others to ensure availability of medications and appropriately sized equipment for use in the management of acute respiratory failure in children.
Introduction
Respiratory failure is defined by inadequate gas exchange by the respiratory system that results in ineffective alveolar ventilation and/or oxygenation. Acute respiratory failure is more common in children than adults and is the primary cause of cardiopulmonary arrest in children. The differential diagnosis for acute respiratory failure in children is extensive, as failure may stem from any portion of the respiratory system or be a consequence of systemic disease. Pediatric hospitalists frequently encounter children with conditions affecting the respiratory system and should be able to anticipate, identify, and treat acute respiratory distress and acute respiratory failure in children, including those with chronic respiratory conditions and other comorbidities.
Knowledge
Pediatric hospitalists should be able to:
- Describe the structure and function respiratory system components, including upper and lower airways, muscles of respiration, and central and peripheral regulation systems.
- Explain developmental differences that contribute to acute respiratory failure in infants and young children, including upper airway size, lower airway growth and development, diaphragmatic muscle reserve, chest wall compliance, and respiratory regulatory center maturity.
- Discuss the basic principles of respiratory physiology, including the alveolar gas equation, minute ventilation, and alveolar-arterial gradient.
- Summarize the five causes of hypoxemia: ventilation-perfusion mismatch, hypoventilation, right to left shunt, diffusion impairment, and low inspired oxygen.
- Construct an age-based differential diagnosis for acute respiratory distress in children.
- List causes of poor respiratory muscle function, attending to age, neuromuscular disorders, central nervous system dysfunction, nerve injury, and others.
- Discuss comorbidities that place children at higher risk for acute respiratory failure.
- Summarize evaluation, monitoring, and treatment options for patients with worsening respiratory status, including mental status assessment, blood gas analysis, medications, and respiratory support.
- Describe the signs and symptoms of impending acute respiratory failure, including criteria for transfer to a higher level of care.
- Discuss the advantages and disadvantages of different supplemental oxygen delivery devices for children with and without medical complexity, such as low flow and heated high-flow nasal cannula, simple mask, partial rebreather or non-rebreather, and tracheostomy collar or mask.
- Summarize the modalities commonly available to support the airway and adequate gas exchange in children with worsening respiratory distress, including nasopharyngeal or oropharyngeal airways, bag-valve-mask ventilation, bi-level positive airway pressure, continuous positive airway pressure, endotracheal tube, and laryngeal-mask-airway intubation.
- Describe criteria for, risks of, and complications due to endotracheal or laryngeal-mask-airway intubation, including strategies to reduce these risks.
- Compare and contrast optimal treatment strategies for acute respiratory failure in children with common acute respiratory conditions, including asthma, bronchiolitis, croup, and pneumonia.
Skills
Pediatric hospitalists should be able to:
- Perform and teach other health care providers to perform a thorough respiratory assessment of a child with acute respiratory distress.
- Identify early warning signs of acute respiratory distress and institute corrective actions and therapies to avert further deterioration.
- Identify patients with comorbidities and other risk factors for progression to acute respiratory failure.
- Order appropriate monitoring and relevant testing (such as radiographs and blood gases) and correctly interpret their results.
- Diagnose and initiate medical management for systemic causes of acute respiratory failure.
- Identify signs and symptoms of impending acute respiratory failure and activate local emergency response teams and/or transfer patients to an appropriate site with critical care services in a safe and efficient manner.
- Initiate oxygen supplementation via oxygen delivery devices and escalate as required to manage hypoxia and/or acute respiratory distress.
- Stabilize the airway, using non-invasive airway management techniques independently and invasive airway management in collaboration with other services.
- Demonstrate proficiency in basic management of patients with chronic respiratory support needs.
- Identify patients requiring subspecialty care and obtain timely consults.
Attitudes
Pediatric hospitalists should be able to:
- Acknowledge the importance of collaboration with patients, the family/caregivers, hospital staff, and subspecialists to ensure family-centered, coordinated hospital care for children with conditions at risk for acute respiratory failure.
- Realize the value of providing consultation for healthcare providers in community settings to ensure transport of patients to higher acuity settings as needed.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in educational programs for the family/caregivers, hospital staff, and other healthcare providers regarding recognition of signs and symptoms of acute respiratory distress in children, particularly those at higher risk for acute respiratory failure.
- Work with hospital administration, hospital staff, subspecialists, and others to develop, implement, and assess outcomes of intervention strategies such as rapid response teams and early warning scores for hospitalized patients with deterioration in respiratory status in order to prevent adverse outcomes.
- Work with hospital administration, hospital staff, pharmacy, and others to ensure availability of medications and appropriately sized equipment for use in the management of acute respiratory failure in children.
1. Samson RA, Schexnayder SM, Hazinski MF, et al. Part 3 Systematic approach to the seriously ill or injured child, Part 6 Recognition of Respiratory Distress and Failure, and Part 7 Management of Respiratory Distress and Failure. In: Pediatric Advanced Life Support: Provider Manual. Dallas, TX: American Heart Association; 2016;29-68; 113-170.
2. Hammer J. Acute respiratory failure in children. Paediatr Respir Rev. 2013; 14:64-69. https://doi.org/10.1016/j.prrv.2013.02.001.
1. Samson RA, Schexnayder SM, Hazinski MF, et al. Part 3 Systematic approach to the seriously ill or injured child, Part 6 Recognition of Respiratory Distress and Failure, and Part 7 Management of Respiratory Distress and Failure. In: Pediatric Advanced Life Support: Provider Manual. Dallas, TX: American Heart Association; 2016;29-68; 113-170.
2. Hammer J. Acute respiratory failure in children. Paediatr Respir Rev. 2013; 14:64-69. https://doi.org/10.1016/j.prrv.2013.02.001.
1.02 Common Clinical Diagnoses and Conditions: Acute Gastroenteritis
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1.01 Common Clinical Diagnoses and Conditions: Acute Abdominal Pain and Acute Abdomen
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Pediatric Hospital Medicine Core Competencies: 2020 Revision. Table of Contents
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
The Pediatric Hospital Medicine Core Competencies: 2020 Revision Dedication

Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
APPENDIX
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Research News: Neurologic Disorders (FULL)
Modest Evidence for Benefit in Studies of Cannabis in MS
While several dozen studies have been conducted into cannabis-based treatments for symptoms of multiple sclerosis (MS), a new systematic review deems most to be of fair to poor quality. Reviewers found modest evidence of benefit and plenty of room for more research.
“Cannabis-based medicine may be useful for refractory MS symptoms, especially spasticity and pain, and side effects are usually well tolerated,” study lead author Natasha Breward, a graduate student at the College of Pharmacy and Nutrition, University of Saskatchewan, Saskatoon, said in an interview. Breward spoke prior to the presentation of the study findings at the 2019 meeting of the Consortium of Multiple Sclerosis Centers.
For the review, Breward and colleagues focused on 60 studies—26 randomized controlled trials and 34 trials with other designs. Forty of the studies used nabiximols, an oromucosal spray that is derived from the cannabis sativa plant and approved for use in multiple countries but not yet in the US.
According to Breward, some of the other treatments included dried cannabis that is smoked or eaten and cannabidiol that’s typically delivered with tetrahydrocannabinol (THC) either oromucosally or as an oral capsule.
MS symptoms treated in the studies included spasticity (n = 29), pain (n = 8), and cognition (n = 6). The researchers considered 22 studies to be poor quality, 14 to be fair quality, and 24 to be good/excellent quality.
The researchers found that the cannabis-based medicine “significantly reduced spasticity and pain in several individual good-quality studies,” Breward said. The drugs seem to work by inhibiting neurotransmitter release via cannabinoids. “However, the variability in study quality—and in the products and regimens studied—make it hard to draw any conclusions about specific products and doses that may have the most potential benefit,” she added.
“Further research should focus on the use of different products and formulations of cannabis-based medicine such as cannabis oil and cannabidiol-prominent products, as no studies have focused on this area,” she said. “Research should also look at the potential of cannabis-based medicine for the treatment of disease progression, as cannabinoids are anti-inflammatory and immunomodulatory. Finally, more research regarding the potentially synergistic effects of cannabis-based medicine administered with current MS medications would also be useful.”
Randy Dotinga, MDedge.com/neurology
Brain Volumes After TBI Correlate With Clinical Features
Brain volumes of specific regions of interest can be used to classify traumatic brain injury subjects that fall into predetermined symptom categories, according to a study presented at the annual meeting of the American Academy of Neurology.
Traumatic brain injury (TBI) damages brain tissue and causes subsequent volume loss, which may result in clinical symptoms. It is a prevalent worldwide health problem caused by a mechanical insult to the head, resulting in transient or permanent alteration to brain tissue and/or function. Standard neuroimaging with computed cranial tomography (CT) and structural magnetic resonance imaging (MRI) is often unrevealing during the evaluation of patients with TBI, particularly those classified as mild TBI.
In this study, James Rock, MD, of Penn Presbyterian Medical Center and the University of Pennsylvania, and colleagues sought to examine the value of quantitative analysis of regional brain volumes in the evaluation of TBI. The investigators reviewed the medical records and MRI imaging from 44 patients with TBI evaluated at a Level I trauma center. They also read clinical notes to assess reported symptoms and physical findings.
Regional volumes from TBI subjects were derived using the software package Freesurfer image analysis suite (surfer.nmr.mgh.harvard.edu), which utilizes a T1-weighted structural scan to calculate volumetric information. A machine learning algorithm, random forests, was employed across volume measurements from 25 regions of interest to determine the most important regions for classifying subjects based on clinical outcome and symptomology.
Basal ganglia volume showed the highest variable importance with regards to classifying subjects who exhibited symptoms of cognitive dysfunction in quantitative analysis. Left lateral ventricle volume was important in classifying subjects with motor and vestibular alterations. Left choroid plexus volume was the most important region for classifying subjects with sensation and somatic dysfunction.
In an abstract, the researchers noted that their study is ongoing. “It will be extended to a larger cohort to determine whether volume changes in specific [regions of interest] can act as useful clinical biomarkers for chronic symptoms,” they said.
Dr. Diaz-Arrastia received personal compensation from Neural Analytics, Inc; BrainBox Solutions, Inc; and Bioscience Pharma Partners. Dr. Diaz-Arrastia holds stock and/or stock options in Neural Analytics, Inc and has received research support from BrainBox Solutions. The other authors reported no other disclosures.
Glenn S. Williams, MDedge.com/neurology
What Other Drugs Do Patients Take When They Start MS Therapy?
Concomitant medication use is common when patients with multiple sclerosis (MS) start disease-modifying drugs (DMDs), according to research presented at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. The likelihood of particular comorbidities and concomitant medications varies by age and sex, researchers reported.
“This may have implications for MS treatment,” said study author Jacqueline Nicholas, MD, MPH, of Ohio Multiple Sclerosis Center in Columbus and colleagues. “A better understanding of the effects of comorbidities and concomitant medications on the effectiveness and safety of DMDs is needed to support clinical decision making.”
Researchers have examined comorbidities in patients with MS, but concomitant medication use among patients starting DMDs is poorly understood, the authors said.
To study this question, Dr. Nicholas and colleagues analyzed retrospective administrative claims data from IQVIA Real-World Data Adjudicated Claims–US database from Jan. 1, 2010, to June 30, 2017. Their analysis included patients with ≥ 2 MS diagnosis claims and at least 1 DMD claim between Jan. 1, 2011, and June 30, 2015. Eligible patients were aged 18 to 63 years and had continuous eligibility with commercial insurance 1 year before and 2 years after DMD initiation. In addition, patients had no evidence of DMD use during the 1-year baseline period.
The investigators used International Classification of Diseases, 9th and 10th revisions, Clinical Modification codes and claims to evaluate patients’ comorbidities and concomitant medications during the study period.
The researchers identified 8,251 eligible patients. Patients had a mean age of 43.2 years, and 75.5% were female. Average baseline Charlson Comorbidity Index was 0.41. In the 2 years after DMD initiation, common comorbid diagnoses were hyperlipidemia (30.0%), hypertension (28.2%), gastrointestinal disorders (26.2%), depression (25.5%), and anxiety (20.1%).
Common concomitant medications included antibiotics (70.6%); analgesics (57.0%); corticosteroids (52.0%); antidepressants (47.7%); anticonvulsants (46.7%); anxiolytics, sedatives, or hypnotics (43.2%); spasticity medications (36.2%); and muscle relaxants (35.4%).
Most comorbidities and many medications, including bladder and antifatigue medications, were more common among patients aged ≥ 55 years. Hyperlipidemia, hypertension, and diabetes mellitus were more likely in males than in females. Females were more likely to have gastrointestinal disease, depression, thyroid disease, anxiety, lung disease, and arthritis. In addition, females were more likely than males to use many of the concomitant medications.
Dr. Nicholas disclosed grant support from EMD Serono. A coauthor is an employee of Health Services Consulting Corporation and received funding from EMD Serono to conduct the study. Other coauthors are employees of EMD Serono.
Jake Rem
Depression, Fatigue, Pain, and Anxiety Are Common in the Year After MS Diagnosis
In the 12 months after diagnosis, pain, fatigue, depression, and anxiety are common among patients with multiple sclerosis (MS), researchers reported at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. In a novel study, about half of patients with MS reported clinically significant symptoms of depression or pain, and about 60% reported fatigue during that time.
Pain, fatigue, depression, and anxiety are common in MS, but their prevalence in the first year after diagnosis is not well understood. To examine the rates of these conditions and how often they co-occur during that period, Anna L. Kratz, PhD, associate professor of physical medicine and rehabilitation at the University of Michigan in Ann Arbor, and her research colleagues had 231 adults with MS complete validated surveys at 1, 2, 3, 6, 9, and 12 months after diagnosis to assess symptoms of these conditions.
Overall, 47.2% of patients reported clinically significant levels of depression, 38.5% reported clinically significant levels of anxiety, 50.4% reported clinically significant pain, and 62.2% reported clinically significant fatigue at any point during the year after diagnosis. “Of those who did not have clinically significant symptoms at time of diagnosis, 21.3% went on to develop clinically significant depression, 17.0% anxiety, 30.9% pain, and 34.1% fatigue,” the authors reported.
About 23% of patients did not have clinically significant symptoms for any condition, while 20% had clinically significant symptoms for 1 condition, 21% for 2, 19% for 3, and 17% for all 4. Depression and fatigue had the highest rate of comorbidity, whereas pain and anxiety had the lowest rate of comorbidity.
“Important clinical symptoms associated with MS are present at high levels in the first year post diagnosis,” Dr. Kratz and colleagues concluded. “While the rates and severity are marginally lower than have been identified in studies of individuals farther into the MS disease course, this study is a reminder that early MS intervention should incorporate interventions for these symptoms that are known to have strong associations with quality of life.”
The researchers had no disclosures.
Jake Remaly, MDedge.com/neurology
Experts Propose New Definition and Recommendations for Alzheimer-like Disorder
An international group of experts has proposed a new name, staging criteria, and recommendations for a recently recognized brain disorder that mimics Alzheimer disease and is marked by a proteinopathy caused by malformed transactive response DNA-binding protein of 43 kDa (TDP-43).
The term limbic-predominant age-related TDP-43 encephalopathy (LATE) was coined in an effort to raise awareness and kick-start research into this “pathway to dementia,” the experts wrote in a report appearing in Brain. “As there is currently no universally agreed-upon terminology or staging system for common age-related TDP-43 proteinopathy, this condition is understudied and not well recognized, even among investigators in the field of dementia research,” wrote the authors of the report, led by Peter T. Nelson, MD, PhD, of the University of Kentucky, Lexington.
LATE neuropathologic changes, associated with a progressive amnesia syndrome that mimics Alzheimer, are seen in > 20% of individuals aged > 80 years, according to large, community-based autopsy series. It coexists with Alzheimer disease in many patients, lowering the threshold for developing dementia, authors said.
The term LATE is designed to encompass several other terms related to TDP-43 pathology, including hippocampal sclerosis and cerebral age-related TDP-43 with sclerosis, Dr. Nelson and colleagues noted.
The TDP-43 protein is encoded by the TARDBP gene and provides several functions related to the regulation of gene expression, the authors wrote.
Misfolded TDP-43 was known to play a causative role in amyotrophic lateral sclerosis and frontotemporal lobar degeneration, the authors noted, and then was also identified in the brains of older individuals with hippocampal sclerosis or Alzheimer disease neuropathologic changes.
The authors proposed a 3-stage classification system for LATE neuropathologic change based on TDP-43 immunohistochemistry performed during routine autopsy evaluation of the amygdala, hippocampus, and middle frontal gyrus. The amygdala is an area affected early in the course of the disease (Stage 1), whereas involvement of the hippocampus represents a more intermediate stage (Stage 2), and the middle frontal gyrus is more affected in advanced stages of the disease (Stage 3), according to the schema.
Five genes have been identified with risk alleles for LATE neuropathologic changes, authors said. Of note, several groups have found that the apolipoprotein E ∑ 4 allele, known to be a risk factor for Alzheimer disease neuropathologic changes and Lewy body disease, is also linked to increased risk of TDP-43 proteinopathy.
There are no established biomarkers specific to TDP-43 proteinopathy yet, which hampers development of clinical trials designed to test interventions to treat or prevent LATE, Dr. Nelson and colleagues said in their report. LATE also could obscure the effects of potentially disease-modifying agents being tested in Alzheimer disease clinical trials, which can complicate the interpretation of study results, they added.
“Until there are biomarkers for LATE, clinical trials should be powered to account for TDP-43 proteinopathy,” they wrote. Dr. Nelson and coauthors reported no author disclosures.
Source: Nelson PT, Dickson DW, Trojanowski JQ, et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): consensus working group report. Brain. 2019;142(6):1503-1527.
Andrew D. Bowser, MDedge.com/neurology
Modest Evidence for Benefit in Studies of Cannabis in MS
While several dozen studies have been conducted into cannabis-based treatments for symptoms of multiple sclerosis (MS), a new systematic review deems most to be of fair to poor quality. Reviewers found modest evidence of benefit and plenty of room for more research.
“Cannabis-based medicine may be useful for refractory MS symptoms, especially spasticity and pain, and side effects are usually well tolerated,” study lead author Natasha Breward, a graduate student at the College of Pharmacy and Nutrition, University of Saskatchewan, Saskatoon, said in an interview. Breward spoke prior to the presentation of the study findings at the 2019 meeting of the Consortium of Multiple Sclerosis Centers.
For the review, Breward and colleagues focused on 60 studies—26 randomized controlled trials and 34 trials with other designs. Forty of the studies used nabiximols, an oromucosal spray that is derived from the cannabis sativa plant and approved for use in multiple countries but not yet in the US.
According to Breward, some of the other treatments included dried cannabis that is smoked or eaten and cannabidiol that’s typically delivered with tetrahydrocannabinol (THC) either oromucosally or as an oral capsule.
MS symptoms treated in the studies included spasticity (n = 29), pain (n = 8), and cognition (n = 6). The researchers considered 22 studies to be poor quality, 14 to be fair quality, and 24 to be good/excellent quality.
The researchers found that the cannabis-based medicine “significantly reduced spasticity and pain in several individual good-quality studies,” Breward said. The drugs seem to work by inhibiting neurotransmitter release via cannabinoids. “However, the variability in study quality—and in the products and regimens studied—make it hard to draw any conclusions about specific products and doses that may have the most potential benefit,” she added.
“Further research should focus on the use of different products and formulations of cannabis-based medicine such as cannabis oil and cannabidiol-prominent products, as no studies have focused on this area,” she said. “Research should also look at the potential of cannabis-based medicine for the treatment of disease progression, as cannabinoids are anti-inflammatory and immunomodulatory. Finally, more research regarding the potentially synergistic effects of cannabis-based medicine administered with current MS medications would also be useful.”
Randy Dotinga, MDedge.com/neurology
Brain Volumes After TBI Correlate With Clinical Features
Brain volumes of specific regions of interest can be used to classify traumatic brain injury subjects that fall into predetermined symptom categories, according to a study presented at the annual meeting of the American Academy of Neurology.
Traumatic brain injury (TBI) damages brain tissue and causes subsequent volume loss, which may result in clinical symptoms. It is a prevalent worldwide health problem caused by a mechanical insult to the head, resulting in transient or permanent alteration to brain tissue and/or function. Standard neuroimaging with computed cranial tomography (CT) and structural magnetic resonance imaging (MRI) is often unrevealing during the evaluation of patients with TBI, particularly those classified as mild TBI.
In this study, James Rock, MD, of Penn Presbyterian Medical Center and the University of Pennsylvania, and colleagues sought to examine the value of quantitative analysis of regional brain volumes in the evaluation of TBI. The investigators reviewed the medical records and MRI imaging from 44 patients with TBI evaluated at a Level I trauma center. They also read clinical notes to assess reported symptoms and physical findings.
Regional volumes from TBI subjects were derived using the software package Freesurfer image analysis suite (surfer.nmr.mgh.harvard.edu), which utilizes a T1-weighted structural scan to calculate volumetric information. A machine learning algorithm, random forests, was employed across volume measurements from 25 regions of interest to determine the most important regions for classifying subjects based on clinical outcome and symptomology.
Basal ganglia volume showed the highest variable importance with regards to classifying subjects who exhibited symptoms of cognitive dysfunction in quantitative analysis. Left lateral ventricle volume was important in classifying subjects with motor and vestibular alterations. Left choroid plexus volume was the most important region for classifying subjects with sensation and somatic dysfunction.
In an abstract, the researchers noted that their study is ongoing. “It will be extended to a larger cohort to determine whether volume changes in specific [regions of interest] can act as useful clinical biomarkers for chronic symptoms,” they said.
Dr. Diaz-Arrastia received personal compensation from Neural Analytics, Inc; BrainBox Solutions, Inc; and Bioscience Pharma Partners. Dr. Diaz-Arrastia holds stock and/or stock options in Neural Analytics, Inc and has received research support from BrainBox Solutions. The other authors reported no other disclosures.
Glenn S. Williams, MDedge.com/neurology
What Other Drugs Do Patients Take When They Start MS Therapy?
Concomitant medication use is common when patients with multiple sclerosis (MS) start disease-modifying drugs (DMDs), according to research presented at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. The likelihood of particular comorbidities and concomitant medications varies by age and sex, researchers reported.
“This may have implications for MS treatment,” said study author Jacqueline Nicholas, MD, MPH, of Ohio Multiple Sclerosis Center in Columbus and colleagues. “A better understanding of the effects of comorbidities and concomitant medications on the effectiveness and safety of DMDs is needed to support clinical decision making.”
Researchers have examined comorbidities in patients with MS, but concomitant medication use among patients starting DMDs is poorly understood, the authors said.
To study this question, Dr. Nicholas and colleagues analyzed retrospective administrative claims data from IQVIA Real-World Data Adjudicated Claims–US database from Jan. 1, 2010, to June 30, 2017. Their analysis included patients with ≥ 2 MS diagnosis claims and at least 1 DMD claim between Jan. 1, 2011, and June 30, 2015. Eligible patients were aged 18 to 63 years and had continuous eligibility with commercial insurance 1 year before and 2 years after DMD initiation. In addition, patients had no evidence of DMD use during the 1-year baseline period.
The investigators used International Classification of Diseases, 9th and 10th revisions, Clinical Modification codes and claims to evaluate patients’ comorbidities and concomitant medications during the study period.
The researchers identified 8,251 eligible patients. Patients had a mean age of 43.2 years, and 75.5% were female. Average baseline Charlson Comorbidity Index was 0.41. In the 2 years after DMD initiation, common comorbid diagnoses were hyperlipidemia (30.0%), hypertension (28.2%), gastrointestinal disorders (26.2%), depression (25.5%), and anxiety (20.1%).
Common concomitant medications included antibiotics (70.6%); analgesics (57.0%); corticosteroids (52.0%); antidepressants (47.7%); anticonvulsants (46.7%); anxiolytics, sedatives, or hypnotics (43.2%); spasticity medications (36.2%); and muscle relaxants (35.4%).
Most comorbidities and many medications, including bladder and antifatigue medications, were more common among patients aged ≥ 55 years. Hyperlipidemia, hypertension, and diabetes mellitus were more likely in males than in females. Females were more likely to have gastrointestinal disease, depression, thyroid disease, anxiety, lung disease, and arthritis. In addition, females were more likely than males to use many of the concomitant medications.
Dr. Nicholas disclosed grant support from EMD Serono. A coauthor is an employee of Health Services Consulting Corporation and received funding from EMD Serono to conduct the study. Other coauthors are employees of EMD Serono.
Jake Rem
Depression, Fatigue, Pain, and Anxiety Are Common in the Year After MS Diagnosis
In the 12 months after diagnosis, pain, fatigue, depression, and anxiety are common among patients with multiple sclerosis (MS), researchers reported at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. In a novel study, about half of patients with MS reported clinically significant symptoms of depression or pain, and about 60% reported fatigue during that time.
Pain, fatigue, depression, and anxiety are common in MS, but their prevalence in the first year after diagnosis is not well understood. To examine the rates of these conditions and how often they co-occur during that period, Anna L. Kratz, PhD, associate professor of physical medicine and rehabilitation at the University of Michigan in Ann Arbor, and her research colleagues had 231 adults with MS complete validated surveys at 1, 2, 3, 6, 9, and 12 months after diagnosis to assess symptoms of these conditions.
Overall, 47.2% of patients reported clinically significant levels of depression, 38.5% reported clinically significant levels of anxiety, 50.4% reported clinically significant pain, and 62.2% reported clinically significant fatigue at any point during the year after diagnosis. “Of those who did not have clinically significant symptoms at time of diagnosis, 21.3% went on to develop clinically significant depression, 17.0% anxiety, 30.9% pain, and 34.1% fatigue,” the authors reported.
About 23% of patients did not have clinically significant symptoms for any condition, while 20% had clinically significant symptoms for 1 condition, 21% for 2, 19% for 3, and 17% for all 4. Depression and fatigue had the highest rate of comorbidity, whereas pain and anxiety had the lowest rate of comorbidity.
“Important clinical symptoms associated with MS are present at high levels in the first year post diagnosis,” Dr. Kratz and colleagues concluded. “While the rates and severity are marginally lower than have been identified in studies of individuals farther into the MS disease course, this study is a reminder that early MS intervention should incorporate interventions for these symptoms that are known to have strong associations with quality of life.”
The researchers had no disclosures.
Jake Remaly, MDedge.com/neurology
Experts Propose New Definition and Recommendations for Alzheimer-like Disorder
An international group of experts has proposed a new name, staging criteria, and recommendations for a recently recognized brain disorder that mimics Alzheimer disease and is marked by a proteinopathy caused by malformed transactive response DNA-binding protein of 43 kDa (TDP-43).
The term limbic-predominant age-related TDP-43 encephalopathy (LATE) was coined in an effort to raise awareness and kick-start research into this “pathway to dementia,” the experts wrote in a report appearing in Brain. “As there is currently no universally agreed-upon terminology or staging system for common age-related TDP-43 proteinopathy, this condition is understudied and not well recognized, even among investigators in the field of dementia research,” wrote the authors of the report, led by Peter T. Nelson, MD, PhD, of the University of Kentucky, Lexington.
LATE neuropathologic changes, associated with a progressive amnesia syndrome that mimics Alzheimer, are seen in > 20% of individuals aged > 80 years, according to large, community-based autopsy series. It coexists with Alzheimer disease in many patients, lowering the threshold for developing dementia, authors said.
The term LATE is designed to encompass several other terms related to TDP-43 pathology, including hippocampal sclerosis and cerebral age-related TDP-43 with sclerosis, Dr. Nelson and colleagues noted.
The TDP-43 protein is encoded by the TARDBP gene and provides several functions related to the regulation of gene expression, the authors wrote.
Misfolded TDP-43 was known to play a causative role in amyotrophic lateral sclerosis and frontotemporal lobar degeneration, the authors noted, and then was also identified in the brains of older individuals with hippocampal sclerosis or Alzheimer disease neuropathologic changes.
The authors proposed a 3-stage classification system for LATE neuropathologic change based on TDP-43 immunohistochemistry performed during routine autopsy evaluation of the amygdala, hippocampus, and middle frontal gyrus. The amygdala is an area affected early in the course of the disease (Stage 1), whereas involvement of the hippocampus represents a more intermediate stage (Stage 2), and the middle frontal gyrus is more affected in advanced stages of the disease (Stage 3), according to the schema.
Five genes have been identified with risk alleles for LATE neuropathologic changes, authors said. Of note, several groups have found that the apolipoprotein E ∑ 4 allele, known to be a risk factor for Alzheimer disease neuropathologic changes and Lewy body disease, is also linked to increased risk of TDP-43 proteinopathy.
There are no established biomarkers specific to TDP-43 proteinopathy yet, which hampers development of clinical trials designed to test interventions to treat or prevent LATE, Dr. Nelson and colleagues said in their report. LATE also could obscure the effects of potentially disease-modifying agents being tested in Alzheimer disease clinical trials, which can complicate the interpretation of study results, they added.
“Until there are biomarkers for LATE, clinical trials should be powered to account for TDP-43 proteinopathy,” they wrote. Dr. Nelson and coauthors reported no author disclosures.
Source: Nelson PT, Dickson DW, Trojanowski JQ, et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): consensus working group report. Brain. 2019;142(6):1503-1527.
Andrew D. Bowser, MDedge.com/neurology
Modest Evidence for Benefit in Studies of Cannabis in MS
While several dozen studies have been conducted into cannabis-based treatments for symptoms of multiple sclerosis (MS), a new systematic review deems most to be of fair to poor quality. Reviewers found modest evidence of benefit and plenty of room for more research.
“Cannabis-based medicine may be useful for refractory MS symptoms, especially spasticity and pain, and side effects are usually well tolerated,” study lead author Natasha Breward, a graduate student at the College of Pharmacy and Nutrition, University of Saskatchewan, Saskatoon, said in an interview. Breward spoke prior to the presentation of the study findings at the 2019 meeting of the Consortium of Multiple Sclerosis Centers.
For the review, Breward and colleagues focused on 60 studies—26 randomized controlled trials and 34 trials with other designs. Forty of the studies used nabiximols, an oromucosal spray that is derived from the cannabis sativa plant and approved for use in multiple countries but not yet in the US.
According to Breward, some of the other treatments included dried cannabis that is smoked or eaten and cannabidiol that’s typically delivered with tetrahydrocannabinol (THC) either oromucosally or as an oral capsule.
MS symptoms treated in the studies included spasticity (n = 29), pain (n = 8), and cognition (n = 6). The researchers considered 22 studies to be poor quality, 14 to be fair quality, and 24 to be good/excellent quality.
The researchers found that the cannabis-based medicine “significantly reduced spasticity and pain in several individual good-quality studies,” Breward said. The drugs seem to work by inhibiting neurotransmitter release via cannabinoids. “However, the variability in study quality—and in the products and regimens studied—make it hard to draw any conclusions about specific products and doses that may have the most potential benefit,” she added.
“Further research should focus on the use of different products and formulations of cannabis-based medicine such as cannabis oil and cannabidiol-prominent products, as no studies have focused on this area,” she said. “Research should also look at the potential of cannabis-based medicine for the treatment of disease progression, as cannabinoids are anti-inflammatory and immunomodulatory. Finally, more research regarding the potentially synergistic effects of cannabis-based medicine administered with current MS medications would also be useful.”
Randy Dotinga, MDedge.com/neurology
Brain Volumes After TBI Correlate With Clinical Features
Brain volumes of specific regions of interest can be used to classify traumatic brain injury subjects that fall into predetermined symptom categories, according to a study presented at the annual meeting of the American Academy of Neurology.
Traumatic brain injury (TBI) damages brain tissue and causes subsequent volume loss, which may result in clinical symptoms. It is a prevalent worldwide health problem caused by a mechanical insult to the head, resulting in transient or permanent alteration to brain tissue and/or function. Standard neuroimaging with computed cranial tomography (CT) and structural magnetic resonance imaging (MRI) is often unrevealing during the evaluation of patients with TBI, particularly those classified as mild TBI.
In this study, James Rock, MD, of Penn Presbyterian Medical Center and the University of Pennsylvania, and colleagues sought to examine the value of quantitative analysis of regional brain volumes in the evaluation of TBI. The investigators reviewed the medical records and MRI imaging from 44 patients with TBI evaluated at a Level I trauma center. They also read clinical notes to assess reported symptoms and physical findings.
Regional volumes from TBI subjects were derived using the software package Freesurfer image analysis suite (surfer.nmr.mgh.harvard.edu), which utilizes a T1-weighted structural scan to calculate volumetric information. A machine learning algorithm, random forests, was employed across volume measurements from 25 regions of interest to determine the most important regions for classifying subjects based on clinical outcome and symptomology.
Basal ganglia volume showed the highest variable importance with regards to classifying subjects who exhibited symptoms of cognitive dysfunction in quantitative analysis. Left lateral ventricle volume was important in classifying subjects with motor and vestibular alterations. Left choroid plexus volume was the most important region for classifying subjects with sensation and somatic dysfunction.
In an abstract, the researchers noted that their study is ongoing. “It will be extended to a larger cohort to determine whether volume changes in specific [regions of interest] can act as useful clinical biomarkers for chronic symptoms,” they said.
Dr. Diaz-Arrastia received personal compensation from Neural Analytics, Inc; BrainBox Solutions, Inc; and Bioscience Pharma Partners. Dr. Diaz-Arrastia holds stock and/or stock options in Neural Analytics, Inc and has received research support from BrainBox Solutions. The other authors reported no other disclosures.
Glenn S. Williams, MDedge.com/neurology
What Other Drugs Do Patients Take When They Start MS Therapy?
Concomitant medication use is common when patients with multiple sclerosis (MS) start disease-modifying drugs (DMDs), according to research presented at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. The likelihood of particular comorbidities and concomitant medications varies by age and sex, researchers reported.
“This may have implications for MS treatment,” said study author Jacqueline Nicholas, MD, MPH, of Ohio Multiple Sclerosis Center in Columbus and colleagues. “A better understanding of the effects of comorbidities and concomitant medications on the effectiveness and safety of DMDs is needed to support clinical decision making.”
Researchers have examined comorbidities in patients with MS, but concomitant medication use among patients starting DMDs is poorly understood, the authors said.
To study this question, Dr. Nicholas and colleagues analyzed retrospective administrative claims data from IQVIA Real-World Data Adjudicated Claims–US database from Jan. 1, 2010, to June 30, 2017. Their analysis included patients with ≥ 2 MS diagnosis claims and at least 1 DMD claim between Jan. 1, 2011, and June 30, 2015. Eligible patients were aged 18 to 63 years and had continuous eligibility with commercial insurance 1 year before and 2 years after DMD initiation. In addition, patients had no evidence of DMD use during the 1-year baseline period.
The investigators used International Classification of Diseases, 9th and 10th revisions, Clinical Modification codes and claims to evaluate patients’ comorbidities and concomitant medications during the study period.
The researchers identified 8,251 eligible patients. Patients had a mean age of 43.2 years, and 75.5% were female. Average baseline Charlson Comorbidity Index was 0.41. In the 2 years after DMD initiation, common comorbid diagnoses were hyperlipidemia (30.0%), hypertension (28.2%), gastrointestinal disorders (26.2%), depression (25.5%), and anxiety (20.1%).
Common concomitant medications included antibiotics (70.6%); analgesics (57.0%); corticosteroids (52.0%); antidepressants (47.7%); anticonvulsants (46.7%); anxiolytics, sedatives, or hypnotics (43.2%); spasticity medications (36.2%); and muscle relaxants (35.4%).
Most comorbidities and many medications, including bladder and antifatigue medications, were more common among patients aged ≥ 55 years. Hyperlipidemia, hypertension, and diabetes mellitus were more likely in males than in females. Females were more likely to have gastrointestinal disease, depression, thyroid disease, anxiety, lung disease, and arthritis. In addition, females were more likely than males to use many of the concomitant medications.
Dr. Nicholas disclosed grant support from EMD Serono. A coauthor is an employee of Health Services Consulting Corporation and received funding from EMD Serono to conduct the study. Other coauthors are employees of EMD Serono.
Jake Rem
Depression, Fatigue, Pain, and Anxiety Are Common in the Year After MS Diagnosis
In the 12 months after diagnosis, pain, fatigue, depression, and anxiety are common among patients with multiple sclerosis (MS), researchers reported at the 2019 meeting of the Consortium of Multiple Sclerosis Centers. In a novel study, about half of patients with MS reported clinically significant symptoms of depression or pain, and about 60% reported fatigue during that time.
Pain, fatigue, depression, and anxiety are common in MS, but their prevalence in the first year after diagnosis is not well understood. To examine the rates of these conditions and how often they co-occur during that period, Anna L. Kratz, PhD, associate professor of physical medicine and rehabilitation at the University of Michigan in Ann Arbor, and her research colleagues had 231 adults with MS complete validated surveys at 1, 2, 3, 6, 9, and 12 months after diagnosis to assess symptoms of these conditions.
Overall, 47.2% of patients reported clinically significant levels of depression, 38.5% reported clinically significant levels of anxiety, 50.4% reported clinically significant pain, and 62.2% reported clinically significant fatigue at any point during the year after diagnosis. “Of those who did not have clinically significant symptoms at time of diagnosis, 21.3% went on to develop clinically significant depression, 17.0% anxiety, 30.9% pain, and 34.1% fatigue,” the authors reported.
About 23% of patients did not have clinically significant symptoms for any condition, while 20% had clinically significant symptoms for 1 condition, 21% for 2, 19% for 3, and 17% for all 4. Depression and fatigue had the highest rate of comorbidity, whereas pain and anxiety had the lowest rate of comorbidity.
“Important clinical symptoms associated with MS are present at high levels in the first year post diagnosis,” Dr. Kratz and colleagues concluded. “While the rates and severity are marginally lower than have been identified in studies of individuals farther into the MS disease course, this study is a reminder that early MS intervention should incorporate interventions for these symptoms that are known to have strong associations with quality of life.”
The researchers had no disclosures.
Jake Remaly, MDedge.com/neurology
Experts Propose New Definition and Recommendations for Alzheimer-like Disorder
An international group of experts has proposed a new name, staging criteria, and recommendations for a recently recognized brain disorder that mimics Alzheimer disease and is marked by a proteinopathy caused by malformed transactive response DNA-binding protein of 43 kDa (TDP-43).
The term limbic-predominant age-related TDP-43 encephalopathy (LATE) was coined in an effort to raise awareness and kick-start research into this “pathway to dementia,” the experts wrote in a report appearing in Brain. “As there is currently no universally agreed-upon terminology or staging system for common age-related TDP-43 proteinopathy, this condition is understudied and not well recognized, even among investigators in the field of dementia research,” wrote the authors of the report, led by Peter T. Nelson, MD, PhD, of the University of Kentucky, Lexington.
LATE neuropathologic changes, associated with a progressive amnesia syndrome that mimics Alzheimer, are seen in > 20% of individuals aged > 80 years, according to large, community-based autopsy series. It coexists with Alzheimer disease in many patients, lowering the threshold for developing dementia, authors said.
The term LATE is designed to encompass several other terms related to TDP-43 pathology, including hippocampal sclerosis and cerebral age-related TDP-43 with sclerosis, Dr. Nelson and colleagues noted.
The TDP-43 protein is encoded by the TARDBP gene and provides several functions related to the regulation of gene expression, the authors wrote.
Misfolded TDP-43 was known to play a causative role in amyotrophic lateral sclerosis and frontotemporal lobar degeneration, the authors noted, and then was also identified in the brains of older individuals with hippocampal sclerosis or Alzheimer disease neuropathologic changes.
The authors proposed a 3-stage classification system for LATE neuropathologic change based on TDP-43 immunohistochemistry performed during routine autopsy evaluation of the amygdala, hippocampus, and middle frontal gyrus. The amygdala is an area affected early in the course of the disease (Stage 1), whereas involvement of the hippocampus represents a more intermediate stage (Stage 2), and the middle frontal gyrus is more affected in advanced stages of the disease (Stage 3), according to the schema.
Five genes have been identified with risk alleles for LATE neuropathologic changes, authors said. Of note, several groups have found that the apolipoprotein E ∑ 4 allele, known to be a risk factor for Alzheimer disease neuropathologic changes and Lewy body disease, is also linked to increased risk of TDP-43 proteinopathy.
There are no established biomarkers specific to TDP-43 proteinopathy yet, which hampers development of clinical trials designed to test interventions to treat or prevent LATE, Dr. Nelson and colleagues said in their report. LATE also could obscure the effects of potentially disease-modifying agents being tested in Alzheimer disease clinical trials, which can complicate the interpretation of study results, they added.
“Until there are biomarkers for LATE, clinical trials should be powered to account for TDP-43 proteinopathy,” they wrote. Dr. Nelson and coauthors reported no author disclosures.
Source: Nelson PT, Dickson DW, Trojanowski JQ, et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): consensus working group report. Brain. 2019;142(6):1503-1527.
Andrew D. Bowser, MDedge.com/neurology
Proton Pump Inhibitor Use and Risk of Dementia in the Veteran Population (FULL)
Proton pump inhibitors (PPIs) have become the mainstay of therapy in the treatment of acid-related disorders since their introduction in 1989. Due to their high potency, excellent tolerability, and generic availability, PPIs have largely replaced histamine-2 receptor antagonists for gastric problems. Since they were first released on the market, the use of PPIs has continued to rise in both the hospital and primary care settings.1 However, this rapid growth has led to the concern of overutilization. A study conducted at the Department of Veterans Affairs (VA) Ann Arbor Health Care System found that out of 946 patients in the ambulatory care setting taking PPIs, only 35% were appropriately prescribed PPIs.2
Although the short-term adverse effects of PPI use seem minimal, chronic PPI use consequences are a growing concern. Chronic PPI use is associated with increased risks of osteoporosis, pneumonia, and Clostridium difficile infections.3 Another long-term risk that has been associated with chronic PPI use is dementia. Dementia is a cognitive syndrome that is characterized by a progressive decline beyond what is expected in normal aging in 1 or more of the cognitive domains of memory, language, orientation, learning capacity, executive function, or social cognition.4 Because it interferes with activities of daily living, dementia is a major cause of disability in the elderly and is an immense burden for caregivers. Currently, about 47 million people globally live with dementia.5 This number is projected to nearly triple by 2050 to 132 million.5 With no cure, identification of risk factors and creation of protective measures are critical in decreasing the prevalence of dementia.
Although the exact pathophysiology behind the link between PPIs and dementia is unknown, several theories exist. One such theory is that PPI-induced vitamin B12 deficiency leads to cognitive decline.6,7 Another theory suggests that PPIs can directly cause dementia by inhibiting enzymes that normally degrade β amyloid.8 This leads to increased levels of β-amyloid plaques, which is a known characteristic of dementia patients. This theory is derived from animal studies that have shown increased amyloid levels in the brains of mice given PPIs.8
Current studies are conflicting regarding the association between PPIs and dementia. Two German prospective, cohort studies found statistically significant increased risks of dementia in patients taking PPIs with hazard ratios (HR) of 1.38 (95% CI, 1.04-1.83) and 1.44 (95% CI, 1.36-1.52), respectively.9,10 A study conducted in Taiwan also found an increased risk of dementia among PPI users with a HR of 1.22 (95% CI, 1.05-1.42).11 On the contrary, other studies have failed to show an increased risk of dementia with PPI use. In fact, Goldstein and colleagues found a decreased risk of dementia in PPI users with a HR of 0.78 (95% CI, 0.76-0.93).12 This study was an observational study conducted in the US using data from the National Alzheimer’s Coordinating Center database.12 Another recent retrospective study conducted in Finland showed that PPI use was not associated with a significantly increased risk of Alzheimer disease.13
Much is unknown about the cause of dementia, and no curative treatment exists. Investigation into potential risk factors for dementia can lead to the development of preventative measures, which can lead to significant improvement in quality of life for both patients and caregivers. Current studies regarding the association between PPIs and dementia are conflicting, and to our knowledge, no study analyzing the effects of PPIs and dementia has been conducted within the veteran population specifically. The objective of the current study is to investigate the association between PPI use and dementia in the veteran population.
Methods
This study is a retrospective, cohort, single-center, chart review study conducted at the Sioux Falls Veteran Affairs Health Care System (SFVAHCS). Data were extracted from the VA electronic health record (EHR) from January 1, 2005 through December 31, 2015. The study included both currently living and deceased veterans who received ≥ 2 documented outpatient visits at the SFVAHCS during the study time frame. Patients also had to be aged ≥ 60 years at the start of the study period. Patients were excluded if they received only a ≤ 30-day PPI prescription. Patients with dementia related to head trauma, acute intoxication, or other known diseases were excluded.
To analyze the primary endpoint of association between PPI use and dementia, the study compared the rate of dementia in a cohort of veterans who had received an outpatient prescription for a PPI within the study time frame vs the rate of dementia in a random, equal number of veterans who had never been prescribed PPIs within the study time frame. In this study, veterans were classified as having dementia if they had a diagnosis of dementia based on ICD-9 or ICD-10 codes (Table 1), or if they had been prescribed medications used to treat dementia (donepezil, ergoloid mesylates, galantamine, memantine, and rivastigmine).
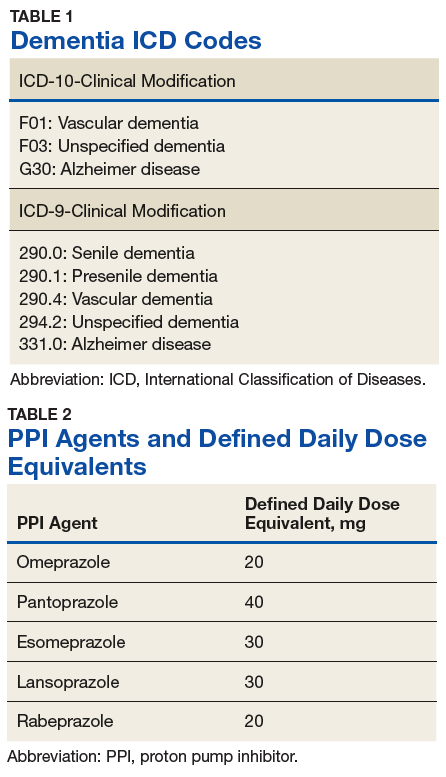
Secondary endpoints included analysis of the effects of PPI agent, PPI dose, and PPI duration on the risk of dementia. For the PPI dose analysis, cumulative doses were converted into defined daily doses (DDDs) using the World Health Organization calculation to equalize the different potencies of PPI agents (Table 2).14 In addition, the effect of PPI use on vitamin B12 levels was analyzed as an exploratory endpoint to investigate the hypothesis that PPI may be associated with vitamin B12 deficiency, which in turn may be associated with dementia.6,7
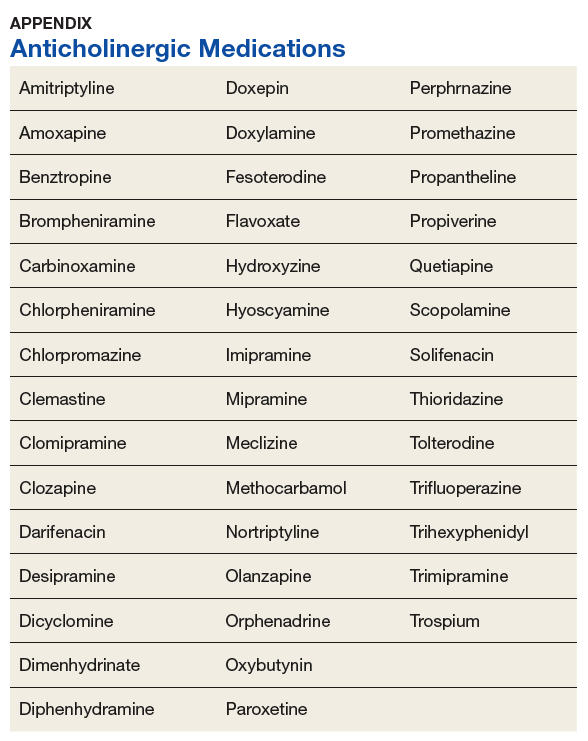
Baseline characteristics were collected to determine the variability between the treatment and control group. Data collected included age, gender, past medical history of diseases that may increase risk of dementia, and anticholinergic drug use. Anticholinergic drugs were included if they were classified as having “definite anticholinergic effects” based on the Aging Brain Care Anticholinergic Burden Scale (Appendix).15
Statistical Analysis
The primary endpoint was analyzed using a χ2 for association test. For the secondary endpoints, a χ2 for association test was used for endpoints with nominal data, and the Mood median test was used for endpoints with continuous data. The exploratory endpoint analyzing vitamin B12 levels was analyzed with the Mood median test. A P value of < .05 was defined as being statistically significant. Power analysis was not performed since all veterans who met the criteria were included in the study.
Results
Records of 23,656 veterans were included in the study with 11,828 veterans in both the PPI cohort and the non-PPI cohort (Table 3).
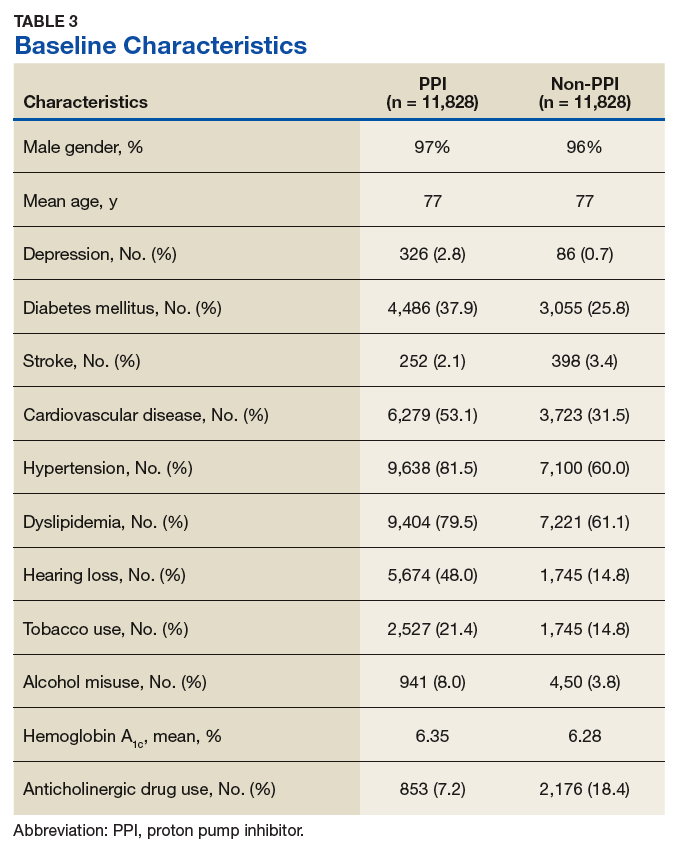
Primary Endpoint
Within the PPI group, 1,119 (9.5%) veterans had dementia compared with only 740 (6.3%) veterans in the non-PPI group. There was a statistically significant association between PPI use and dementia (P < .001). These results yielded an odds ratio of 1.55 for dementia risk in PPI users vs nonusers and a relative risk increase of 51.4% for dementia risk with PPI use compared with no PPI use.
Secondary Endpoints
Users of rabeprazole had the highest rate of dementia (12.8%), followed by lansoprazole (10.9%), omeprazole (9.7%), esomeprazole (7.7%), and pantoprazole (7.0%). The rate of dementia for non-PPI users was 6.3% (P < .001). The median cumulative doses of PPIs were not significant: 597 DDDs (95% CI, 540-630) in the dementia group vs 570 DDDs (95% CI, 540-624) in the nondementia group (P = .79). The median cumulative duration of PPI use in the dementia group was 4.6 years (95% CI, 4.25-4.92) vs 5.3 years (95% CI, 5.08-5.42) in the nondementia group (P < .001).
Exploratory Endpoint
The median B12 level in the PPI group was 521 pg/mL (95% CI, 509-533) compared with 480 pg/mL (95% CI, 465-496) in the non-PPI group (P < .001). However, both groups fell within the normal range for vitamin B12 (200-900 pg/mL).16
Discussion
The aim of this study was to determine whether an association existed between PPI use and dementia. This study showed a statistically significant association between PPI use and dementia within the veteran population. This study also showed a significant association between specific PPI agents and dementia. When analyzing the individual PPI agents, the rabeprazole group yielded the strongest relationship. However, this study was not powered to evaluate and compare risks of dementia between individual PPI agents. More data are needed to determine statistical and clinical significance of associations between individual PPI agents and risk of dementia.
The veterans with dementia had a higher median cumulative PPI dose than did the veterans without dementia; however, the results were not statistically significant. Therefore, the data cannot correlate higher doses of PPI use to increased risk of dementia.
The cumulative duration of PPI use was statistically significant but opposite of the expected outcome. The dementia group had a lower median lifetime duration of PPI use compared with that of the nondementia group. It is difficult to determine the reason for this outcome, but it seems that for this study population, a longer duration of PPI use was not associated with an increased risk of dementia.
Finally, the exploratory endpoint analyzed vitamin B12 levels, since it has been shown that PPI use can lead to vitamin B12 deficiency and that B12 deficiency can lead to dementia.6-8 This study found that the dementia group had significantly higher vitamin B12 levels than the nondementia group. These data suggest that PPI use may not be associated with vitamin B12 deficiency. However, it is important to note that this study was unable to collect data on the use of vitamin B12 supplementation due to the unreliability of over-the-counter (OTC) and non-VA medication use records. Therefore, it is possible that the PPI group had higher rates of B12 deficiency but were effectively treated with B12 supplementation. More research is needed to determine the exact relationship between PPI use, vitamin B12 deficiency, and dementia risk.
Strengths/Limitations
Strengths of this study that support its findings include the large population size. Additionally, the use of the VA EHR allowed for a complete drug dispensing history to be collected, which improves reliability of the data.
This study also had some limitations. First, the causal relationship of PPI use and dementia cannot be proven using a retrospective cohort design. This study’s design can show association, but it cannot prove causation. Also, due to the retrospective design, exposure to PPI use could not be randomized; thus, correlation between PPI use and dementia may be explained by confounding variables that are not captured within this study. This is especially true since the baseline characteristics were not equally distributed between the 2 groups. In fact, the PPI group had higher rates of many clinical comorbidities. This imbalance may have skewed the results of the primary endpoint. Lastly, OTC PPI use and non-VA PPI prescriptions were not available. Therefore, some of the patients included in the non-PPI group may have been PPI users if they received PPIs from OTC or non-VA sources, which could skew the results.
Conclusion
This study showed a significant association between PPI use and dementia within the veteran study population. The study also showed a significant association between PPI use and dementia within the secondary endpoint of individual PPI agent. Higher cumulative dose and duration of PPI use did not seem to increase risk of dementia. Finally, PPI use was not associated with significantly low vitamin B12 levels. More studies are needed to determine causation of dementia and its risk factors.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Sioux Falls VA Health Care System.
1. Savarino V, Dulbecco P, de Bortoli N, Ottonello A, Savarino E. The appropriate use of proton pump inhibitors (PPIs): need for a reappraisal. Eur J Intern Med. 2017;37:19-24.
2. Heidelbaugh J, Goldberg K, Inadomi J. Magnitude and economic effect of overuse of antisecretory therapy in the ambulatory care setting. Am J Manag Care. 2010;16(9):e228-e234.
3. Heidelbaugh JJ, Kim AH, Chang R. Walker PC. Overutilization of proton-pump inhibitors: what the clinician needs to know. Therap Adv Gastroenterol. 2012;5(4):219-232.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, (DSM-5). American Psychiatric Association: Washington, DC; 2013.
5. World Health Organization. Dementia. http://www.who.int/mediacentre/factsheets/fs362/en/. Published December 12, 2017. Accessed March 10, 2019.
6. Vogiatzoglou A, Smith AD, Nurk E, et al. Cognitive function in an elderly population: interaction between vitamin B12 status, depression, and apolipoprotein E ε4: the Hordaland Homocysteine Study. Psychosom Med. 2013;75(1):20-29.
7. Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 2013;310(22):2435-2442.
8. Badiola N, Alcalde V, Pujol A, et al. The proton-pump inhibitor lansoprazole enhances amyloid beta production. PLoS One. 2013;8(3):e58837.
9. Haenisch B, von Holt K, Wiese B, et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur Arch Psychiatry Clin Neurosci. 2015;265(5):419-428.
10. Gomm W, von Holt K, Thomé F, et al. Association between proton pump inhibitors with risk of dementia. A pharmacoepidemiological claims data analysis. JAMA Neurol. 2016;73(4):410-416.
11. Tai SY, Chien CY, Wu DC, et al. Risk of dementia from proton pump inhibitor use in Asian population: a nationwide cohort study in Taiwan. PLoS One. 2017;12(2):e0171006.
12. Goldstein FC, Steenland K, Zhao L, Wharton W, Levey AI, Hajjar I. Proton pump inhibitors and risk of mild cognitive impairment and dementia. J Am Geriatr Soc. 2017;65(9):1969-1674.
13. Taipale H, Tolppanen AM, Tiihonen M. Tanskanen A, Tiihonen J, Hartikainen S. No association between proton pump inhibitor use and risk of Alzheimer’s disease. Am J Gastroenterol. 2017;112(12):1801-1808.
14. World Health Organization Collaborating Centre for Drug Statistics Methodology. Definition and general considerations. https://www.whocc.no/ddd/definition_and_general_considera/. Updated February 7, 2018. Accessed March 13, 2019.
15. Indiana University Center for Aging Research, Aging Brain Program. Anticholinergic cognitive burden scale. http://www.idhca.org/wp-content/uploads/2018/02/DESAI_ACB_scale_-_Legal_size_paper.pdf. Updated 2012. Accessed March 10, 2019.
16. US National Library of Medicine, MedlinePlus. Vitamin B12 level. https://medlineplus.gov/ency/article/003705.htm. Updated March 7, 2019. Accessed March 13, 2019.
Proton pump inhibitors (PPIs) have become the mainstay of therapy in the treatment of acid-related disorders since their introduction in 1989. Due to their high potency, excellent tolerability, and generic availability, PPIs have largely replaced histamine-2 receptor antagonists for gastric problems. Since they were first released on the market, the use of PPIs has continued to rise in both the hospital and primary care settings.1 However, this rapid growth has led to the concern of overutilization. A study conducted at the Department of Veterans Affairs (VA) Ann Arbor Health Care System found that out of 946 patients in the ambulatory care setting taking PPIs, only 35% were appropriately prescribed PPIs.2
Although the short-term adverse effects of PPI use seem minimal, chronic PPI use consequences are a growing concern. Chronic PPI use is associated with increased risks of osteoporosis, pneumonia, and Clostridium difficile infections.3 Another long-term risk that has been associated with chronic PPI use is dementia. Dementia is a cognitive syndrome that is characterized by a progressive decline beyond what is expected in normal aging in 1 or more of the cognitive domains of memory, language, orientation, learning capacity, executive function, or social cognition.4 Because it interferes with activities of daily living, dementia is a major cause of disability in the elderly and is an immense burden for caregivers. Currently, about 47 million people globally live with dementia.5 This number is projected to nearly triple by 2050 to 132 million.5 With no cure, identification of risk factors and creation of protective measures are critical in decreasing the prevalence of dementia.
Although the exact pathophysiology behind the link between PPIs and dementia is unknown, several theories exist. One such theory is that PPI-induced vitamin B12 deficiency leads to cognitive decline.6,7 Another theory suggests that PPIs can directly cause dementia by inhibiting enzymes that normally degrade β amyloid.8 This leads to increased levels of β-amyloid plaques, which is a known characteristic of dementia patients. This theory is derived from animal studies that have shown increased amyloid levels in the brains of mice given PPIs.8
Current studies are conflicting regarding the association between PPIs and dementia. Two German prospective, cohort studies found statistically significant increased risks of dementia in patients taking PPIs with hazard ratios (HR) of 1.38 (95% CI, 1.04-1.83) and 1.44 (95% CI, 1.36-1.52), respectively.9,10 A study conducted in Taiwan also found an increased risk of dementia among PPI users with a HR of 1.22 (95% CI, 1.05-1.42).11 On the contrary, other studies have failed to show an increased risk of dementia with PPI use. In fact, Goldstein and colleagues found a decreased risk of dementia in PPI users with a HR of 0.78 (95% CI, 0.76-0.93).12 This study was an observational study conducted in the US using data from the National Alzheimer’s Coordinating Center database.12 Another recent retrospective study conducted in Finland showed that PPI use was not associated with a significantly increased risk of Alzheimer disease.13
Much is unknown about the cause of dementia, and no curative treatment exists. Investigation into potential risk factors for dementia can lead to the development of preventative measures, which can lead to significant improvement in quality of life for both patients and caregivers. Current studies regarding the association between PPIs and dementia are conflicting, and to our knowledge, no study analyzing the effects of PPIs and dementia has been conducted within the veteran population specifically. The objective of the current study is to investigate the association between PPI use and dementia in the veteran population.
Methods
This study is a retrospective, cohort, single-center, chart review study conducted at the Sioux Falls Veteran Affairs Health Care System (SFVAHCS). Data were extracted from the VA electronic health record (EHR) from January 1, 2005 through December 31, 2015. The study included both currently living and deceased veterans who received ≥ 2 documented outpatient visits at the SFVAHCS during the study time frame. Patients also had to be aged ≥ 60 years at the start of the study period. Patients were excluded if they received only a ≤ 30-day PPI prescription. Patients with dementia related to head trauma, acute intoxication, or other known diseases were excluded.
To analyze the primary endpoint of association between PPI use and dementia, the study compared the rate of dementia in a cohort of veterans who had received an outpatient prescription for a PPI within the study time frame vs the rate of dementia in a random, equal number of veterans who had never been prescribed PPIs within the study time frame. In this study, veterans were classified as having dementia if they had a diagnosis of dementia based on ICD-9 or ICD-10 codes (Table 1), or if they had been prescribed medications used to treat dementia (donepezil, ergoloid mesylates, galantamine, memantine, and rivastigmine).
Secondary endpoints included analysis of the effects of PPI agent, PPI dose, and PPI duration on the risk of dementia. For the PPI dose analysis, cumulative doses were converted into defined daily doses (DDDs) using the World Health Organization calculation to equalize the different potencies of PPI agents (Table 2).14 In addition, the effect of PPI use on vitamin B12 levels was analyzed as an exploratory endpoint to investigate the hypothesis that PPI may be associated with vitamin B12 deficiency, which in turn may be associated with dementia.6,7
Baseline characteristics were collected to determine the variability between the treatment and control group. Data collected included age, gender, past medical history of diseases that may increase risk of dementia, and anticholinergic drug use. Anticholinergic drugs were included if they were classified as having “definite anticholinergic effects” based on the Aging Brain Care Anticholinergic Burden Scale (Appendix).15
Statistical Analysis
The primary endpoint was analyzed using a χ2 for association test. For the secondary endpoints, a χ2 for association test was used for endpoints with nominal data, and the Mood median test was used for endpoints with continuous data. The exploratory endpoint analyzing vitamin B12 levels was analyzed with the Mood median test. A P value of < .05 was defined as being statistically significant. Power analysis was not performed since all veterans who met the criteria were included in the study.
Results
Records of 23,656 veterans were included in the study with 11,828 veterans in both the PPI cohort and the non-PPI cohort (Table 3).
Primary Endpoint
Within the PPI group, 1,119 (9.5%) veterans had dementia compared with only 740 (6.3%) veterans in the non-PPI group. There was a statistically significant association between PPI use and dementia (P < .001). These results yielded an odds ratio of 1.55 for dementia risk in PPI users vs nonusers and a relative risk increase of 51.4% for dementia risk with PPI use compared with no PPI use.
Secondary Endpoints
Users of rabeprazole had the highest rate of dementia (12.8%), followed by lansoprazole (10.9%), omeprazole (9.7%), esomeprazole (7.7%), and pantoprazole (7.0%). The rate of dementia for non-PPI users was 6.3% (P < .001). The median cumulative doses of PPIs were not significant: 597 DDDs (95% CI, 540-630) in the dementia group vs 570 DDDs (95% CI, 540-624) in the nondementia group (P = .79). The median cumulative duration of PPI use in the dementia group was 4.6 years (95% CI, 4.25-4.92) vs 5.3 years (95% CI, 5.08-5.42) in the nondementia group (P < .001).
Exploratory Endpoint
The median B12 level in the PPI group was 521 pg/mL (95% CI, 509-533) compared with 480 pg/mL (95% CI, 465-496) in the non-PPI group (P < .001). However, both groups fell within the normal range for vitamin B12 (200-900 pg/mL).16
Discussion
The aim of this study was to determine whether an association existed between PPI use and dementia. This study showed a statistically significant association between PPI use and dementia within the veteran population. This study also showed a significant association between specific PPI agents and dementia. When analyzing the individual PPI agents, the rabeprazole group yielded the strongest relationship. However, this study was not powered to evaluate and compare risks of dementia between individual PPI agents. More data are needed to determine statistical and clinical significance of associations between individual PPI agents and risk of dementia.
The veterans with dementia had a higher median cumulative PPI dose than did the veterans without dementia; however, the results were not statistically significant. Therefore, the data cannot correlate higher doses of PPI use to increased risk of dementia.
The cumulative duration of PPI use was statistically significant but opposite of the expected outcome. The dementia group had a lower median lifetime duration of PPI use compared with that of the nondementia group. It is difficult to determine the reason for this outcome, but it seems that for this study population, a longer duration of PPI use was not associated with an increased risk of dementia.
Finally, the exploratory endpoint analyzed vitamin B12 levels, since it has been shown that PPI use can lead to vitamin B12 deficiency and that B12 deficiency can lead to dementia.6-8 This study found that the dementia group had significantly higher vitamin B12 levels than the nondementia group. These data suggest that PPI use may not be associated with vitamin B12 deficiency. However, it is important to note that this study was unable to collect data on the use of vitamin B12 supplementation due to the unreliability of over-the-counter (OTC) and non-VA medication use records. Therefore, it is possible that the PPI group had higher rates of B12 deficiency but were effectively treated with B12 supplementation. More research is needed to determine the exact relationship between PPI use, vitamin B12 deficiency, and dementia risk.
Strengths/Limitations
Strengths of this study that support its findings include the large population size. Additionally, the use of the VA EHR allowed for a complete drug dispensing history to be collected, which improves reliability of the data.
This study also had some limitations. First, the causal relationship of PPI use and dementia cannot be proven using a retrospective cohort design. This study’s design can show association, but it cannot prove causation. Also, due to the retrospective design, exposure to PPI use could not be randomized; thus, correlation between PPI use and dementia may be explained by confounding variables that are not captured within this study. This is especially true since the baseline characteristics were not equally distributed between the 2 groups. In fact, the PPI group had higher rates of many clinical comorbidities. This imbalance may have skewed the results of the primary endpoint. Lastly, OTC PPI use and non-VA PPI prescriptions were not available. Therefore, some of the patients included in the non-PPI group may have been PPI users if they received PPIs from OTC or non-VA sources, which could skew the results.
Conclusion
This study showed a significant association between PPI use and dementia within the veteran study population. The study also showed a significant association between PPI use and dementia within the secondary endpoint of individual PPI agent. Higher cumulative dose and duration of PPI use did not seem to increase risk of dementia. Finally, PPI use was not associated with significantly low vitamin B12 levels. More studies are needed to determine causation of dementia and its risk factors.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Sioux Falls VA Health Care System.
Proton pump inhibitors (PPIs) have become the mainstay of therapy in the treatment of acid-related disorders since their introduction in 1989. Due to their high potency, excellent tolerability, and generic availability, PPIs have largely replaced histamine-2 receptor antagonists for gastric problems. Since they were first released on the market, the use of PPIs has continued to rise in both the hospital and primary care settings.1 However, this rapid growth has led to the concern of overutilization. A study conducted at the Department of Veterans Affairs (VA) Ann Arbor Health Care System found that out of 946 patients in the ambulatory care setting taking PPIs, only 35% were appropriately prescribed PPIs.2
Although the short-term adverse effects of PPI use seem minimal, chronic PPI use consequences are a growing concern. Chronic PPI use is associated with increased risks of osteoporosis, pneumonia, and Clostridium difficile infections.3 Another long-term risk that has been associated with chronic PPI use is dementia. Dementia is a cognitive syndrome that is characterized by a progressive decline beyond what is expected in normal aging in 1 or more of the cognitive domains of memory, language, orientation, learning capacity, executive function, or social cognition.4 Because it interferes with activities of daily living, dementia is a major cause of disability in the elderly and is an immense burden for caregivers. Currently, about 47 million people globally live with dementia.5 This number is projected to nearly triple by 2050 to 132 million.5 With no cure, identification of risk factors and creation of protective measures are critical in decreasing the prevalence of dementia.
Although the exact pathophysiology behind the link between PPIs and dementia is unknown, several theories exist. One such theory is that PPI-induced vitamin B12 deficiency leads to cognitive decline.6,7 Another theory suggests that PPIs can directly cause dementia by inhibiting enzymes that normally degrade β amyloid.8 This leads to increased levels of β-amyloid plaques, which is a known characteristic of dementia patients. This theory is derived from animal studies that have shown increased amyloid levels in the brains of mice given PPIs.8
Current studies are conflicting regarding the association between PPIs and dementia. Two German prospective, cohort studies found statistically significant increased risks of dementia in patients taking PPIs with hazard ratios (HR) of 1.38 (95% CI, 1.04-1.83) and 1.44 (95% CI, 1.36-1.52), respectively.9,10 A study conducted in Taiwan also found an increased risk of dementia among PPI users with a HR of 1.22 (95% CI, 1.05-1.42).11 On the contrary, other studies have failed to show an increased risk of dementia with PPI use. In fact, Goldstein and colleagues found a decreased risk of dementia in PPI users with a HR of 0.78 (95% CI, 0.76-0.93).12 This study was an observational study conducted in the US using data from the National Alzheimer’s Coordinating Center database.12 Another recent retrospective study conducted in Finland showed that PPI use was not associated with a significantly increased risk of Alzheimer disease.13
Much is unknown about the cause of dementia, and no curative treatment exists. Investigation into potential risk factors for dementia can lead to the development of preventative measures, which can lead to significant improvement in quality of life for both patients and caregivers. Current studies regarding the association between PPIs and dementia are conflicting, and to our knowledge, no study analyzing the effects of PPIs and dementia has been conducted within the veteran population specifically. The objective of the current study is to investigate the association between PPI use and dementia in the veteran population.
Methods
This study is a retrospective, cohort, single-center, chart review study conducted at the Sioux Falls Veteran Affairs Health Care System (SFVAHCS). Data were extracted from the VA electronic health record (EHR) from January 1, 2005 through December 31, 2015. The study included both currently living and deceased veterans who received ≥ 2 documented outpatient visits at the SFVAHCS during the study time frame. Patients also had to be aged ≥ 60 years at the start of the study period. Patients were excluded if they received only a ≤ 30-day PPI prescription. Patients with dementia related to head trauma, acute intoxication, or other known diseases were excluded.
To analyze the primary endpoint of association between PPI use and dementia, the study compared the rate of dementia in a cohort of veterans who had received an outpatient prescription for a PPI within the study time frame vs the rate of dementia in a random, equal number of veterans who had never been prescribed PPIs within the study time frame. In this study, veterans were classified as having dementia if they had a diagnosis of dementia based on ICD-9 or ICD-10 codes (Table 1), or if they had been prescribed medications used to treat dementia (donepezil, ergoloid mesylates, galantamine, memantine, and rivastigmine).
Secondary endpoints included analysis of the effects of PPI agent, PPI dose, and PPI duration on the risk of dementia. For the PPI dose analysis, cumulative doses were converted into defined daily doses (DDDs) using the World Health Organization calculation to equalize the different potencies of PPI agents (Table 2).14 In addition, the effect of PPI use on vitamin B12 levels was analyzed as an exploratory endpoint to investigate the hypothesis that PPI may be associated with vitamin B12 deficiency, which in turn may be associated with dementia.6,7
Baseline characteristics were collected to determine the variability between the treatment and control group. Data collected included age, gender, past medical history of diseases that may increase risk of dementia, and anticholinergic drug use. Anticholinergic drugs were included if they were classified as having “definite anticholinergic effects” based on the Aging Brain Care Anticholinergic Burden Scale (Appendix).15
Statistical Analysis
The primary endpoint was analyzed using a χ2 for association test. For the secondary endpoints, a χ2 for association test was used for endpoints with nominal data, and the Mood median test was used for endpoints with continuous data. The exploratory endpoint analyzing vitamin B12 levels was analyzed with the Mood median test. A P value of < .05 was defined as being statistically significant. Power analysis was not performed since all veterans who met the criteria were included in the study.
Results
Records of 23,656 veterans were included in the study with 11,828 veterans in both the PPI cohort and the non-PPI cohort (Table 3).
Primary Endpoint
Within the PPI group, 1,119 (9.5%) veterans had dementia compared with only 740 (6.3%) veterans in the non-PPI group. There was a statistically significant association between PPI use and dementia (P < .001). These results yielded an odds ratio of 1.55 for dementia risk in PPI users vs nonusers and a relative risk increase of 51.4% for dementia risk with PPI use compared with no PPI use.
Secondary Endpoints
Users of rabeprazole had the highest rate of dementia (12.8%), followed by lansoprazole (10.9%), omeprazole (9.7%), esomeprazole (7.7%), and pantoprazole (7.0%). The rate of dementia for non-PPI users was 6.3% (P < .001). The median cumulative doses of PPIs were not significant: 597 DDDs (95% CI, 540-630) in the dementia group vs 570 DDDs (95% CI, 540-624) in the nondementia group (P = .79). The median cumulative duration of PPI use in the dementia group was 4.6 years (95% CI, 4.25-4.92) vs 5.3 years (95% CI, 5.08-5.42) in the nondementia group (P < .001).
Exploratory Endpoint
The median B12 level in the PPI group was 521 pg/mL (95% CI, 509-533) compared with 480 pg/mL (95% CI, 465-496) in the non-PPI group (P < .001). However, both groups fell within the normal range for vitamin B12 (200-900 pg/mL).16
Discussion
The aim of this study was to determine whether an association existed between PPI use and dementia. This study showed a statistically significant association between PPI use and dementia within the veteran population. This study also showed a significant association between specific PPI agents and dementia. When analyzing the individual PPI agents, the rabeprazole group yielded the strongest relationship. However, this study was not powered to evaluate and compare risks of dementia between individual PPI agents. More data are needed to determine statistical and clinical significance of associations between individual PPI agents and risk of dementia.
The veterans with dementia had a higher median cumulative PPI dose than did the veterans without dementia; however, the results were not statistically significant. Therefore, the data cannot correlate higher doses of PPI use to increased risk of dementia.
The cumulative duration of PPI use was statistically significant but opposite of the expected outcome. The dementia group had a lower median lifetime duration of PPI use compared with that of the nondementia group. It is difficult to determine the reason for this outcome, but it seems that for this study population, a longer duration of PPI use was not associated with an increased risk of dementia.
Finally, the exploratory endpoint analyzed vitamin B12 levels, since it has been shown that PPI use can lead to vitamin B12 deficiency and that B12 deficiency can lead to dementia.6-8 This study found that the dementia group had significantly higher vitamin B12 levels than the nondementia group. These data suggest that PPI use may not be associated with vitamin B12 deficiency. However, it is important to note that this study was unable to collect data on the use of vitamin B12 supplementation due to the unreliability of over-the-counter (OTC) and non-VA medication use records. Therefore, it is possible that the PPI group had higher rates of B12 deficiency but were effectively treated with B12 supplementation. More research is needed to determine the exact relationship between PPI use, vitamin B12 deficiency, and dementia risk.
Strengths/Limitations
Strengths of this study that support its findings include the large population size. Additionally, the use of the VA EHR allowed for a complete drug dispensing history to be collected, which improves reliability of the data.
This study also had some limitations. First, the causal relationship of PPI use and dementia cannot be proven using a retrospective cohort design. This study’s design can show association, but it cannot prove causation. Also, due to the retrospective design, exposure to PPI use could not be randomized; thus, correlation between PPI use and dementia may be explained by confounding variables that are not captured within this study. This is especially true since the baseline characteristics were not equally distributed between the 2 groups. In fact, the PPI group had higher rates of many clinical comorbidities. This imbalance may have skewed the results of the primary endpoint. Lastly, OTC PPI use and non-VA PPI prescriptions were not available. Therefore, some of the patients included in the non-PPI group may have been PPI users if they received PPIs from OTC or non-VA sources, which could skew the results.
Conclusion
This study showed a significant association between PPI use and dementia within the veteran study population. The study also showed a significant association between PPI use and dementia within the secondary endpoint of individual PPI agent. Higher cumulative dose and duration of PPI use did not seem to increase risk of dementia. Finally, PPI use was not associated with significantly low vitamin B12 levels. More studies are needed to determine causation of dementia and its risk factors.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Sioux Falls VA Health Care System.
1. Savarino V, Dulbecco P, de Bortoli N, Ottonello A, Savarino E. The appropriate use of proton pump inhibitors (PPIs): need for a reappraisal. Eur J Intern Med. 2017;37:19-24.
2. Heidelbaugh J, Goldberg K, Inadomi J. Magnitude and economic effect of overuse of antisecretory therapy in the ambulatory care setting. Am J Manag Care. 2010;16(9):e228-e234.
3. Heidelbaugh JJ, Kim AH, Chang R. Walker PC. Overutilization of proton-pump inhibitors: what the clinician needs to know. Therap Adv Gastroenterol. 2012;5(4):219-232.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, (DSM-5). American Psychiatric Association: Washington, DC; 2013.
5. World Health Organization. Dementia. http://www.who.int/mediacentre/factsheets/fs362/en/. Published December 12, 2017. Accessed March 10, 2019.
6. Vogiatzoglou A, Smith AD, Nurk E, et al. Cognitive function in an elderly population: interaction between vitamin B12 status, depression, and apolipoprotein E ε4: the Hordaland Homocysteine Study. Psychosom Med. 2013;75(1):20-29.
7. Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 2013;310(22):2435-2442.
8. Badiola N, Alcalde V, Pujol A, et al. The proton-pump inhibitor lansoprazole enhances amyloid beta production. PLoS One. 2013;8(3):e58837.
9. Haenisch B, von Holt K, Wiese B, et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur Arch Psychiatry Clin Neurosci. 2015;265(5):419-428.
10. Gomm W, von Holt K, Thomé F, et al. Association between proton pump inhibitors with risk of dementia. A pharmacoepidemiological claims data analysis. JAMA Neurol. 2016;73(4):410-416.
11. Tai SY, Chien CY, Wu DC, et al. Risk of dementia from proton pump inhibitor use in Asian population: a nationwide cohort study in Taiwan. PLoS One. 2017;12(2):e0171006.
12. Goldstein FC, Steenland K, Zhao L, Wharton W, Levey AI, Hajjar I. Proton pump inhibitors and risk of mild cognitive impairment and dementia. J Am Geriatr Soc. 2017;65(9):1969-1674.
13. Taipale H, Tolppanen AM, Tiihonen M. Tanskanen A, Tiihonen J, Hartikainen S. No association between proton pump inhibitor use and risk of Alzheimer’s disease. Am J Gastroenterol. 2017;112(12):1801-1808.
14. World Health Organization Collaborating Centre for Drug Statistics Methodology. Definition and general considerations. https://www.whocc.no/ddd/definition_and_general_considera/. Updated February 7, 2018. Accessed March 13, 2019.
15. Indiana University Center for Aging Research, Aging Brain Program. Anticholinergic cognitive burden scale. http://www.idhca.org/wp-content/uploads/2018/02/DESAI_ACB_scale_-_Legal_size_paper.pdf. Updated 2012. Accessed March 10, 2019.
16. US National Library of Medicine, MedlinePlus. Vitamin B12 level. https://medlineplus.gov/ency/article/003705.htm. Updated March 7, 2019. Accessed March 13, 2019.
1. Savarino V, Dulbecco P, de Bortoli N, Ottonello A, Savarino E. The appropriate use of proton pump inhibitors (PPIs): need for a reappraisal. Eur J Intern Med. 2017;37:19-24.
2. Heidelbaugh J, Goldberg K, Inadomi J. Magnitude and economic effect of overuse of antisecretory therapy in the ambulatory care setting. Am J Manag Care. 2010;16(9):e228-e234.
3. Heidelbaugh JJ, Kim AH, Chang R. Walker PC. Overutilization of proton-pump inhibitors: what the clinician needs to know. Therap Adv Gastroenterol. 2012;5(4):219-232.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, (DSM-5). American Psychiatric Association: Washington, DC; 2013.
5. World Health Organization. Dementia. http://www.who.int/mediacentre/factsheets/fs362/en/. Published December 12, 2017. Accessed March 10, 2019.
6. Vogiatzoglou A, Smith AD, Nurk E, et al. Cognitive function in an elderly population: interaction between vitamin B12 status, depression, and apolipoprotein E ε4: the Hordaland Homocysteine Study. Psychosom Med. 2013;75(1):20-29.
7. Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 2013;310(22):2435-2442.
8. Badiola N, Alcalde V, Pujol A, et al. The proton-pump inhibitor lansoprazole enhances amyloid beta production. PLoS One. 2013;8(3):e58837.
9. Haenisch B, von Holt K, Wiese B, et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur Arch Psychiatry Clin Neurosci. 2015;265(5):419-428.
10. Gomm W, von Holt K, Thomé F, et al. Association between proton pump inhibitors with risk of dementia. A pharmacoepidemiological claims data analysis. JAMA Neurol. 2016;73(4):410-416.
11. Tai SY, Chien CY, Wu DC, et al. Risk of dementia from proton pump inhibitor use in Asian population: a nationwide cohort study in Taiwan. PLoS One. 2017;12(2):e0171006.
12. Goldstein FC, Steenland K, Zhao L, Wharton W, Levey AI, Hajjar I. Proton pump inhibitors and risk of mild cognitive impairment and dementia. J Am Geriatr Soc. 2017;65(9):1969-1674.
13. Taipale H, Tolppanen AM, Tiihonen M. Tanskanen A, Tiihonen J, Hartikainen S. No association between proton pump inhibitor use and risk of Alzheimer’s disease. Am J Gastroenterol. 2017;112(12):1801-1808.
14. World Health Organization Collaborating Centre for Drug Statistics Methodology. Definition and general considerations. https://www.whocc.no/ddd/definition_and_general_considera/. Updated February 7, 2018. Accessed March 13, 2019.
15. Indiana University Center for Aging Research, Aging Brain Program. Anticholinergic cognitive burden scale. http://www.idhca.org/wp-content/uploads/2018/02/DESAI_ACB_scale_-_Legal_size_paper.pdf. Updated 2012. Accessed March 10, 2019.
16. US National Library of Medicine, MedlinePlus. Vitamin B12 level. https://medlineplus.gov/ency/article/003705.htm. Updated March 7, 2019. Accessed March 13, 2019.
Understanding Psychosis in a Veteran With a History of Combat and Multiple Sclerosis (FULL)
A patient with significant combat history and previous diagnoses of multiple sclerosis and unspecified schizophrenia spectrum and other psychotic disorder was admitted with acute psychosis inconsistent with expected clinical presentations.
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease that affects > 700,000 people in the US.1 The hallmarks of MS pathology are axonal or neuronal loss, demyelination, and astrocytic gliosis. Of these, axonal or neuronal loss is the main underlying mechanism of permanent clinical disability.
MS also has been associated with an increased prevalence of psychiatric illnesses, with mood disorders affecting up to 40% to 60% of the population, and psychosis being reported in 2% to 4% of patients.2 The link between MS and mood disorders, including bipolar disorder and depression, was documented as early as 1926,with mood disorders hypothesized to be manifestations of central nervous system (CNS) inflammation.3 More recently, inflammation-driven microglia have been hypothesized to impair hippocampal connectivity and activate glucocorticoid-insensitive inflammatory cells that then overstimulate the hypothalamic-pituitary-adrenal axis.4,5
Although the prevalence of psychosis in patients with MS is significantly rarer, averaging between 2% and 4%.6 A Canadian study by Patten and colleagues reviewed data from 2.45 million residents of Alberta and found that those who identified as having MS had a 2% to 3% prevalence of psychosis compared with 0.5% to 1% in the general population.7 The connection between psychosis and MS, similar to that between mood disorders and MS, has been described as a common regional demyelination process. Supporting this, MS manifesting as psychosis has been found to present with distinct magnetic resonance imaging (MRI) findings, such as diffuse periventricular lesions.8 Still, no conclusive criteria have been developed to distinguish MS presenting as psychosis from a primary psychiatric illness, such as schizophrenia.
In patients with combat history, it is possible that both neurodegenerative and psychotic symptoms can be explained by autoantibody formation in response to toxin exposure. When soldiers were deployed to Iraq and Afghanistan, they may have been exposed to multiple toxicities, including depleted uranium, dust and fumes, and numerous infectious diseases.9 Gulf War illness (GWI) or chronic multisymptom illness (CMI) encompass a cluster of symptoms, such as chronic pain, chronic fatigue, irritable bowel syndrome, dermatitis, and seizures, as well as mental health issues such as depression and anxiety experienced following exposure to these combat environments.10,11
In light of this diagnostic uncertainty, the authors detail a case of a patient with significant combat history previously diagnosed with MS and unspecified schizophrenia spectrum and other psychotic disorder (USS & OPD) presenting with acute psychosis.
Case Presentation
A 35-year-old male veteran, with a history of MS, USS & OPD, posttraumatic stress disorder, and traumatic brain injuries (TBIs) was admitted to the psychiatric unit after being found by the police lying in the middle of a busy intersection, internally preoccupied. On admission, he reported a week of auditory hallucinations from birds with whom he had been communicating telepathically, and a recurrent visual hallucination of a tall man in white and purple robes. He had discontinued his antipsychotic medication, aripiprazole 10 mg, a few weeks prior for unknown reasons. He was brought to the hospital by ambulance, where he presented with disorganized thinking, tangential thought process, and active auditory and visual hallucinations. The differential diagnoses included USS & OPD, schizophrenia, schizoaffective disorder and ruled out substance-induced psychotic disorder, and psychosis as a manifestation of MS.
The patient had 2 psychotic episodes prior to this presentation. He was hospitalized for his first psychotic break in 2015 at age 32, when he had tailed another car “to come back to reality” and ended up in a motor vehicle accident. During that admission, he reported weeks of thought broadcasting, conspiratorial delusions, and racing thoughts. Two years later, he was admitted to a psychiatric intensive care unit for his second episode of severe psychosis. After several trials of different antipsychotic medications, his most recent pharmacologic regimen was aripiprazole 10 mg once daily.
His medical history was complicated by 2 TBIs, in November 2014 and January 2015, with normal computed tomography (CT) scans. He was diagnosed with MS in December 2017, when he presented with intractable emesis, left facial numbness, right upper extremity ataxia, nystagmus, and imbalance. An MRI scan revealed multifocal bilateral hypodensities in his periventricular, subcortical, and brain stem white matter. Multiple areas of hyperintensity were visualized, including in the right periatrial region and left brachium pontis. More than 5 oligoclonal bands on lumbar puncture confirmed the diagnosis.
He was treated with IV methylprednisolone followed by a 2-week prednisone taper. Within 1 week, he returned to the psychiatric unit with worsening symptoms and received a second dose of IV steroids and plasma exchange treatment. In the following months, he completed a course of rituximab infusions and physical therapy for his dysarthria, gait abnormality, and vision impairment.
His social history was notable for multiple first-degree relatives with schizophrenia. He reported a history of sexual and verbal abuse and attempted suicide once at age 13 years by hanging himself with a bathrobe. He left home at age 18 years to serve in the Marine Corps (2001-2006). His service included deployment to Afghanistan, where he received a purple heart. Upon his return, he received BA and MS degrees. He married and had 2 daughters but became estranged from his wife. By his most recent admission, he was unemployed and living with his half-sister.
On the first day of this most recent psychiatric hospitalization, he was restarted on aripiprazole 10 mg daily, and a medicine consult was sought to evaluate the progression of his MS. No new onset neurologic symptoms were noted, but he had possible residual lower extremity hyperreflexia and tandem gait incoordination. The episodes of psychotic and neurologic symptoms appeared independent, given that his psychiatric history preceded the onset of his MS.
The patient reported no visual hallucinations starting day 2, and he no longer endorsed auditory hallucinations by day 3. However, he continued to appear internally preoccupied and was noticed to be pacing around the unit. On day 4 he presented with newly pressured speech and flights of ideas, while his affect remained euthymic and his sleep stayed consistent. In combination with his ongoing pacing, his newfound symptoms were hypothesized to be possibly akathisia, an adverse effect (AE) of aripiprazole. As such, on day 5 his dose was lowered to 5 mg daily. He continued to report no hallucinations and demonstrated progressively increased emotional range. A MRI scan was done on day 6 in case a new lesion could be identified, suggesting a primary MS flare-up; however, the scan identified no enhancing lesions, indicating no ongoing demyelination. After a neurology consult corroborated this conclusion, he was discharged in stable condition on day 7.
As is the case with the majority of patients with MS-induced psychosis, he continued to have relapsing psychiatric disease even after MS treatment had been started. Unfortunately, because this patient had stopped taking his atypical antipsychotic medication several weeks prior to his hospitalization, we cannot clarify whether his psychosis stems from a primary psychiatric vs MS process.
Discussion
Presently, treatment preferences for MS-related psychosis are divided between atypical antipsychotics and glucocorticoids. Some suggest that the treatment remains similar between MS-related psychosis and primary psychotic disorders in that atypical antipsychotics are the standard of care.12 A variety of atypical antipsychotics have been used successfully in case reports, including zipradisone, risperidone, olanzapine, quetiapine, and aripiprazole.13,14 First-generation antipsychotics and other psychotropic drugs that can precipitate extra-pyramidal AEs are not recommended given their potential additive effect to motor deficits associated with MS.12 Alternatively, several case reports have found that MS-related psychotic symptoms respond to glucocorticoids more effectively, while cautioning that glucocorticoids can precipitate psychosis and depression.15,16 One review article found that 90% of patients who received corticosteroids saw an improvement in their psychotic symptoms.2
Finally, it is possible that our patient’s neuropsychiatric symptoms can be explained by autoantibody formation in response to toxin exposure during his time in Afghanistan. In a pilot study of veterans with GWI, Abou-Donia and colleagues found 2-to-9 fold increase in autoantibody reactivity levels of the following neuronal and glial-specific proteins relative to healthy controls: neurofilament triplet proteins, tubulin, microtubule-associated tau proteins, microtubule-associated protein-2, myelin basic protein, myelin-associated glycoprotein, glial fibrillary acidic protein, and calcium-calmodulin kinase II.17,18 Many of these autoantibodies are longstanding explicit markers for neurodegenerative disorders, given that they target proteins and antigens that support axonal transport and myelination. Still Gulf War veteran status has yet to be explicitly linked to an increased risk of MS,19 making this hypothesis less likely for our patient. Future research should address the clinical and therapeutic implications of different autoantibody levels in combat veterans with psychosis.
Conclusion
For patients with MS, mood disorder and psychotic symptoms should warrant a MRI given the possibility of a psychiatric manifestation of MS relapse. Ultimately, our patient’s presentation was inconsistent with the expected clinical presentations of both a primary psychotic disorder and psychosis as a manifestation of MS. His late age at his first psychotic break is atypical for primary psychotic disease, and the lack of MRI imaging done at his initial psychotic episodes cannot exclude a primary MS diagnosis. Still, his lack of MRI findings at his most recent hospitalization, negative symptomatology, and strong history of schizophrenia make a primary psychotic disorder likely.
Following his future clinical course will be necessary to determine the etiology of his psychotic episodes. Future episodes of psychosis with neurologic symptoms would suggest a primary MS diagnosis and potential benefit of immunosuppressant treatment, whereas repeated psychotic breaks with minimal temporal lobe involvement or demyelination as seen on MRI would be suspicious for separate MS and psychotic disease processes. Further research on treatment regimens for patients experiencing psychosis as a manifestation of MS is still necessary.
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040.
2. Camara-Lemarroy CR, Ibarra-Yruegas BE, Rodriguez-Gutierrez R, Berrios-Morales I, Ionete C, Riskind P. The varieties of psychosis in multiple sclerosis: a systematic review of cases. Mult Scler Relat Disord. 2017;12:9-14.
3. Cottrel SS, Wilson SA. The affective symptomatology of disseminated sclerosis: a study of 100 cases. J Neurol Psychopathology. 1926;7(25):1-30.
4. Johansson V, Lundholm C, Hillert J, et al. Multiple sclerosis and psychiatric disorders: comorbidity and sibling risk in a nationwide Swedish cohort. Mult Scler. 2014;20(14):1881-1891.
5. Rossi S, Studer V, Motta C, et al. Neuroinflammation drives anxiety and depression in relapsing-remitting multiple sclerosis. Neurology. 2017;89(13):1338-1347.
6. Gilberthorpe TG, O’Connell KE, Carolan A, et al. The spectrum of psychosis in multiple sclerosis: a clinical case series. Neuropsychiatric disease and treatment. 2017;13:303.
7. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;65(7):1123-1125.
8. Kosmidis MH, Giannakou M, Messinis L, Papathanasopoulos P. Psychotic features associated with multiple sclerosis. Int Rev Psychiatry. 2010; 22(1):55-66.
9. US Department of Veterans Affairs. Public health: military exposures. https://www.publichealth.va.gov/exposures/. Updated April 16, 2019. Accessed May 13, 2019.
10. DeBeer BB, Davidson D, Meyer EC, Kimbrel NA, Gulliver SB, Morissette SB. The association between toxic exposures and chronic multisymptom illness in veterans of the wars of Iraq and Afghanistan. J Occup Environ Med. 2017;59(1):54-60.
11. Kang HK, Li B, Mahan CM, Eisen SA, Engel CC. Health of US veterans of 1991 Gulf War: a follow-up survey in 10 years. J Occup Environ Med. 2009;51(4):401-410.
12. Murphy R, O’Donoghue S, Counihan T, et al. Neuropsychiatric syndromes of multiple sclerosis. J Neurol Neurosurg Psychiatry. 2017;88(8):697-708.
13. Davids E, Hartwig U, Gastpar, M. Antipsychotic treatment of psychosis associated with multiple sclerosis. Prog Neuro Psychopharmacol Biol Psychiatry. 2004;28(4):743-744.
14. Lo Fermo S, Barone R, Patti F, et al. Outcome of psychiatric symptoms presenting at onset of multiple sclerosis: a retrospective study. Mult Scler. 2010;16(6):742-748.
15. Enderami A, Fouladi R, Hosseini HS. First-episode psychosis as the initial presentation of multiple sclerosis: a case report. Int Medical Case Rep J. 2018;11:73-76.
16. Fragoso YD, Frota ER, Lopes JS, et al. Severe depression, suicide attempts, and ideation during the use of interferon beta by patients with multiple sclerosis. Clin Neuropharmacol. 2010;33(6):312-316.
17. Abou-Donia MB, Conboy LA, Kokkotou E, et al. Screening for novel central nervous system biomarkers in veterans with Gulf War Illness. Neurotoxicol Teratol. 2017;61:36-46.
18. Abou-Donia MB, Lieberman A, Curtis L. Neural autoantibodies in patients with neurological symptoms and histories of chemical/mold exposures. Toxicol Ind Health. 2018;34(1):44-53.
19. Wallin MT, Kurtzke JF, Culpepper WJ, et al. Multiple sclerosis in Gulf War era veterans. 2. Military deployment and risk of multiple sclerosis in the first Gulf War. Neuroepidemiology. 2014;42(4):226-234.
A patient with significant combat history and previous diagnoses of multiple sclerosis and unspecified schizophrenia spectrum and other psychotic disorder was admitted with acute psychosis inconsistent with expected clinical presentations.
A patient with significant combat history and previous diagnoses of multiple sclerosis and unspecified schizophrenia spectrum and other psychotic disorder was admitted with acute psychosis inconsistent with expected clinical presentations.
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease that affects > 700,000 people in the US.1 The hallmarks of MS pathology are axonal or neuronal loss, demyelination, and astrocytic gliosis. Of these, axonal or neuronal loss is the main underlying mechanism of permanent clinical disability.
MS also has been associated with an increased prevalence of psychiatric illnesses, with mood disorders affecting up to 40% to 60% of the population, and psychosis being reported in 2% to 4% of patients.2 The link between MS and mood disorders, including bipolar disorder and depression, was documented as early as 1926,with mood disorders hypothesized to be manifestations of central nervous system (CNS) inflammation.3 More recently, inflammation-driven microglia have been hypothesized to impair hippocampal connectivity and activate glucocorticoid-insensitive inflammatory cells that then overstimulate the hypothalamic-pituitary-adrenal axis.4,5
Although the prevalence of psychosis in patients with MS is significantly rarer, averaging between 2% and 4%.6 A Canadian study by Patten and colleagues reviewed data from 2.45 million residents of Alberta and found that those who identified as having MS had a 2% to 3% prevalence of psychosis compared with 0.5% to 1% in the general population.7 The connection between psychosis and MS, similar to that between mood disorders and MS, has been described as a common regional demyelination process. Supporting this, MS manifesting as psychosis has been found to present with distinct magnetic resonance imaging (MRI) findings, such as diffuse periventricular lesions.8 Still, no conclusive criteria have been developed to distinguish MS presenting as psychosis from a primary psychiatric illness, such as schizophrenia.
In patients with combat history, it is possible that both neurodegenerative and psychotic symptoms can be explained by autoantibody formation in response to toxin exposure. When soldiers were deployed to Iraq and Afghanistan, they may have been exposed to multiple toxicities, including depleted uranium, dust and fumes, and numerous infectious diseases.9 Gulf War illness (GWI) or chronic multisymptom illness (CMI) encompass a cluster of symptoms, such as chronic pain, chronic fatigue, irritable bowel syndrome, dermatitis, and seizures, as well as mental health issues such as depression and anxiety experienced following exposure to these combat environments.10,11
In light of this diagnostic uncertainty, the authors detail a case of a patient with significant combat history previously diagnosed with MS and unspecified schizophrenia spectrum and other psychotic disorder (USS & OPD) presenting with acute psychosis.
Case Presentation
A 35-year-old male veteran, with a history of MS, USS & OPD, posttraumatic stress disorder, and traumatic brain injuries (TBIs) was admitted to the psychiatric unit after being found by the police lying in the middle of a busy intersection, internally preoccupied. On admission, he reported a week of auditory hallucinations from birds with whom he had been communicating telepathically, and a recurrent visual hallucination of a tall man in white and purple robes. He had discontinued his antipsychotic medication, aripiprazole 10 mg, a few weeks prior for unknown reasons. He was brought to the hospital by ambulance, where he presented with disorganized thinking, tangential thought process, and active auditory and visual hallucinations. The differential diagnoses included USS & OPD, schizophrenia, schizoaffective disorder and ruled out substance-induced psychotic disorder, and psychosis as a manifestation of MS.
The patient had 2 psychotic episodes prior to this presentation. He was hospitalized for his first psychotic break in 2015 at age 32, when he had tailed another car “to come back to reality” and ended up in a motor vehicle accident. During that admission, he reported weeks of thought broadcasting, conspiratorial delusions, and racing thoughts. Two years later, he was admitted to a psychiatric intensive care unit for his second episode of severe psychosis. After several trials of different antipsychotic medications, his most recent pharmacologic regimen was aripiprazole 10 mg once daily.
His medical history was complicated by 2 TBIs, in November 2014 and January 2015, with normal computed tomography (CT) scans. He was diagnosed with MS in December 2017, when he presented with intractable emesis, left facial numbness, right upper extremity ataxia, nystagmus, and imbalance. An MRI scan revealed multifocal bilateral hypodensities in his periventricular, subcortical, and brain stem white matter. Multiple areas of hyperintensity were visualized, including in the right periatrial region and left brachium pontis. More than 5 oligoclonal bands on lumbar puncture confirmed the diagnosis.
He was treated with IV methylprednisolone followed by a 2-week prednisone taper. Within 1 week, he returned to the psychiatric unit with worsening symptoms and received a second dose of IV steroids and plasma exchange treatment. In the following months, he completed a course of rituximab infusions and physical therapy for his dysarthria, gait abnormality, and vision impairment.
His social history was notable for multiple first-degree relatives with schizophrenia. He reported a history of sexual and verbal abuse and attempted suicide once at age 13 years by hanging himself with a bathrobe. He left home at age 18 years to serve in the Marine Corps (2001-2006). His service included deployment to Afghanistan, where he received a purple heart. Upon his return, he received BA and MS degrees. He married and had 2 daughters but became estranged from his wife. By his most recent admission, he was unemployed and living with his half-sister.
On the first day of this most recent psychiatric hospitalization, he was restarted on aripiprazole 10 mg daily, and a medicine consult was sought to evaluate the progression of his MS. No new onset neurologic symptoms were noted, but he had possible residual lower extremity hyperreflexia and tandem gait incoordination. The episodes of psychotic and neurologic symptoms appeared independent, given that his psychiatric history preceded the onset of his MS.
The patient reported no visual hallucinations starting day 2, and he no longer endorsed auditory hallucinations by day 3. However, he continued to appear internally preoccupied and was noticed to be pacing around the unit. On day 4 he presented with newly pressured speech and flights of ideas, while his affect remained euthymic and his sleep stayed consistent. In combination with his ongoing pacing, his newfound symptoms were hypothesized to be possibly akathisia, an adverse effect (AE) of aripiprazole. As such, on day 5 his dose was lowered to 5 mg daily. He continued to report no hallucinations and demonstrated progressively increased emotional range. A MRI scan was done on day 6 in case a new lesion could be identified, suggesting a primary MS flare-up; however, the scan identified no enhancing lesions, indicating no ongoing demyelination. After a neurology consult corroborated this conclusion, he was discharged in stable condition on day 7.
As is the case with the majority of patients with MS-induced psychosis, he continued to have relapsing psychiatric disease even after MS treatment had been started. Unfortunately, because this patient had stopped taking his atypical antipsychotic medication several weeks prior to his hospitalization, we cannot clarify whether his psychosis stems from a primary psychiatric vs MS process.
Discussion
Presently, treatment preferences for MS-related psychosis are divided between atypical antipsychotics and glucocorticoids. Some suggest that the treatment remains similar between MS-related psychosis and primary psychotic disorders in that atypical antipsychotics are the standard of care.12 A variety of atypical antipsychotics have been used successfully in case reports, including zipradisone, risperidone, olanzapine, quetiapine, and aripiprazole.13,14 First-generation antipsychotics and other psychotropic drugs that can precipitate extra-pyramidal AEs are not recommended given their potential additive effect to motor deficits associated with MS.12 Alternatively, several case reports have found that MS-related psychotic symptoms respond to glucocorticoids more effectively, while cautioning that glucocorticoids can precipitate psychosis and depression.15,16 One review article found that 90% of patients who received corticosteroids saw an improvement in their psychotic symptoms.2
Finally, it is possible that our patient’s neuropsychiatric symptoms can be explained by autoantibody formation in response to toxin exposure during his time in Afghanistan. In a pilot study of veterans with GWI, Abou-Donia and colleagues found 2-to-9 fold increase in autoantibody reactivity levels of the following neuronal and glial-specific proteins relative to healthy controls: neurofilament triplet proteins, tubulin, microtubule-associated tau proteins, microtubule-associated protein-2, myelin basic protein, myelin-associated glycoprotein, glial fibrillary acidic protein, and calcium-calmodulin kinase II.17,18 Many of these autoantibodies are longstanding explicit markers for neurodegenerative disorders, given that they target proteins and antigens that support axonal transport and myelination. Still Gulf War veteran status has yet to be explicitly linked to an increased risk of MS,19 making this hypothesis less likely for our patient. Future research should address the clinical and therapeutic implications of different autoantibody levels in combat veterans with psychosis.
Conclusion
For patients with MS, mood disorder and psychotic symptoms should warrant a MRI given the possibility of a psychiatric manifestation of MS relapse. Ultimately, our patient’s presentation was inconsistent with the expected clinical presentations of both a primary psychotic disorder and psychosis as a manifestation of MS. His late age at his first psychotic break is atypical for primary psychotic disease, and the lack of MRI imaging done at his initial psychotic episodes cannot exclude a primary MS diagnosis. Still, his lack of MRI findings at his most recent hospitalization, negative symptomatology, and strong history of schizophrenia make a primary psychotic disorder likely.
Following his future clinical course will be necessary to determine the etiology of his psychotic episodes. Future episodes of psychosis with neurologic symptoms would suggest a primary MS diagnosis and potential benefit of immunosuppressant treatment, whereas repeated psychotic breaks with minimal temporal lobe involvement or demyelination as seen on MRI would be suspicious for separate MS and psychotic disease processes. Further research on treatment regimens for patients experiencing psychosis as a manifestation of MS is still necessary.
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease that affects > 700,000 people in the US.1 The hallmarks of MS pathology are axonal or neuronal loss, demyelination, and astrocytic gliosis. Of these, axonal or neuronal loss is the main underlying mechanism of permanent clinical disability.
MS also has been associated with an increased prevalence of psychiatric illnesses, with mood disorders affecting up to 40% to 60% of the population, and psychosis being reported in 2% to 4% of patients.2 The link between MS and mood disorders, including bipolar disorder and depression, was documented as early as 1926,with mood disorders hypothesized to be manifestations of central nervous system (CNS) inflammation.3 More recently, inflammation-driven microglia have been hypothesized to impair hippocampal connectivity and activate glucocorticoid-insensitive inflammatory cells that then overstimulate the hypothalamic-pituitary-adrenal axis.4,5
Although the prevalence of psychosis in patients with MS is significantly rarer, averaging between 2% and 4%.6 A Canadian study by Patten and colleagues reviewed data from 2.45 million residents of Alberta and found that those who identified as having MS had a 2% to 3% prevalence of psychosis compared with 0.5% to 1% in the general population.7 The connection between psychosis and MS, similar to that between mood disorders and MS, has been described as a common regional demyelination process. Supporting this, MS manifesting as psychosis has been found to present with distinct magnetic resonance imaging (MRI) findings, such as diffuse periventricular lesions.8 Still, no conclusive criteria have been developed to distinguish MS presenting as psychosis from a primary psychiatric illness, such as schizophrenia.
In patients with combat history, it is possible that both neurodegenerative and psychotic symptoms can be explained by autoantibody formation in response to toxin exposure. When soldiers were deployed to Iraq and Afghanistan, they may have been exposed to multiple toxicities, including depleted uranium, dust and fumes, and numerous infectious diseases.9 Gulf War illness (GWI) or chronic multisymptom illness (CMI) encompass a cluster of symptoms, such as chronic pain, chronic fatigue, irritable bowel syndrome, dermatitis, and seizures, as well as mental health issues such as depression and anxiety experienced following exposure to these combat environments.10,11
In light of this diagnostic uncertainty, the authors detail a case of a patient with significant combat history previously diagnosed with MS and unspecified schizophrenia spectrum and other psychotic disorder (USS & OPD) presenting with acute psychosis.
Case Presentation
A 35-year-old male veteran, with a history of MS, USS & OPD, posttraumatic stress disorder, and traumatic brain injuries (TBIs) was admitted to the psychiatric unit after being found by the police lying in the middle of a busy intersection, internally preoccupied. On admission, he reported a week of auditory hallucinations from birds with whom he had been communicating telepathically, and a recurrent visual hallucination of a tall man in white and purple robes. He had discontinued his antipsychotic medication, aripiprazole 10 mg, a few weeks prior for unknown reasons. He was brought to the hospital by ambulance, where he presented with disorganized thinking, tangential thought process, and active auditory and visual hallucinations. The differential diagnoses included USS & OPD, schizophrenia, schizoaffective disorder and ruled out substance-induced psychotic disorder, and psychosis as a manifestation of MS.
The patient had 2 psychotic episodes prior to this presentation. He was hospitalized for his first psychotic break in 2015 at age 32, when he had tailed another car “to come back to reality” and ended up in a motor vehicle accident. During that admission, he reported weeks of thought broadcasting, conspiratorial delusions, and racing thoughts. Two years later, he was admitted to a psychiatric intensive care unit for his second episode of severe psychosis. After several trials of different antipsychotic medications, his most recent pharmacologic regimen was aripiprazole 10 mg once daily.
His medical history was complicated by 2 TBIs, in November 2014 and January 2015, with normal computed tomography (CT) scans. He was diagnosed with MS in December 2017, when he presented with intractable emesis, left facial numbness, right upper extremity ataxia, nystagmus, and imbalance. An MRI scan revealed multifocal bilateral hypodensities in his periventricular, subcortical, and brain stem white matter. Multiple areas of hyperintensity were visualized, including in the right periatrial region and left brachium pontis. More than 5 oligoclonal bands on lumbar puncture confirmed the diagnosis.
He was treated with IV methylprednisolone followed by a 2-week prednisone taper. Within 1 week, he returned to the psychiatric unit with worsening symptoms and received a second dose of IV steroids and plasma exchange treatment. In the following months, he completed a course of rituximab infusions and physical therapy for his dysarthria, gait abnormality, and vision impairment.
His social history was notable for multiple first-degree relatives with schizophrenia. He reported a history of sexual and verbal abuse and attempted suicide once at age 13 years by hanging himself with a bathrobe. He left home at age 18 years to serve in the Marine Corps (2001-2006). His service included deployment to Afghanistan, where he received a purple heart. Upon his return, he received BA and MS degrees. He married and had 2 daughters but became estranged from his wife. By his most recent admission, he was unemployed and living with his half-sister.
On the first day of this most recent psychiatric hospitalization, he was restarted on aripiprazole 10 mg daily, and a medicine consult was sought to evaluate the progression of his MS. No new onset neurologic symptoms were noted, but he had possible residual lower extremity hyperreflexia and tandem gait incoordination. The episodes of psychotic and neurologic symptoms appeared independent, given that his psychiatric history preceded the onset of his MS.
The patient reported no visual hallucinations starting day 2, and he no longer endorsed auditory hallucinations by day 3. However, he continued to appear internally preoccupied and was noticed to be pacing around the unit. On day 4 he presented with newly pressured speech and flights of ideas, while his affect remained euthymic and his sleep stayed consistent. In combination with his ongoing pacing, his newfound symptoms were hypothesized to be possibly akathisia, an adverse effect (AE) of aripiprazole. As such, on day 5 his dose was lowered to 5 mg daily. He continued to report no hallucinations and demonstrated progressively increased emotional range. A MRI scan was done on day 6 in case a new lesion could be identified, suggesting a primary MS flare-up; however, the scan identified no enhancing lesions, indicating no ongoing demyelination. After a neurology consult corroborated this conclusion, he was discharged in stable condition on day 7.
As is the case with the majority of patients with MS-induced psychosis, he continued to have relapsing psychiatric disease even after MS treatment had been started. Unfortunately, because this patient had stopped taking his atypical antipsychotic medication several weeks prior to his hospitalization, we cannot clarify whether his psychosis stems from a primary psychiatric vs MS process.
Discussion
Presently, treatment preferences for MS-related psychosis are divided between atypical antipsychotics and glucocorticoids. Some suggest that the treatment remains similar between MS-related psychosis and primary psychotic disorders in that atypical antipsychotics are the standard of care.12 A variety of atypical antipsychotics have been used successfully in case reports, including zipradisone, risperidone, olanzapine, quetiapine, and aripiprazole.13,14 First-generation antipsychotics and other psychotropic drugs that can precipitate extra-pyramidal AEs are not recommended given their potential additive effect to motor deficits associated with MS.12 Alternatively, several case reports have found that MS-related psychotic symptoms respond to glucocorticoids more effectively, while cautioning that glucocorticoids can precipitate psychosis and depression.15,16 One review article found that 90% of patients who received corticosteroids saw an improvement in their psychotic symptoms.2
Finally, it is possible that our patient’s neuropsychiatric symptoms can be explained by autoantibody formation in response to toxin exposure during his time in Afghanistan. In a pilot study of veterans with GWI, Abou-Donia and colleagues found 2-to-9 fold increase in autoantibody reactivity levels of the following neuronal and glial-specific proteins relative to healthy controls: neurofilament triplet proteins, tubulin, microtubule-associated tau proteins, microtubule-associated protein-2, myelin basic protein, myelin-associated glycoprotein, glial fibrillary acidic protein, and calcium-calmodulin kinase II.17,18 Many of these autoantibodies are longstanding explicit markers for neurodegenerative disorders, given that they target proteins and antigens that support axonal transport and myelination. Still Gulf War veteran status has yet to be explicitly linked to an increased risk of MS,19 making this hypothesis less likely for our patient. Future research should address the clinical and therapeutic implications of different autoantibody levels in combat veterans with psychosis.
Conclusion
For patients with MS, mood disorder and psychotic symptoms should warrant a MRI given the possibility of a psychiatric manifestation of MS relapse. Ultimately, our patient’s presentation was inconsistent with the expected clinical presentations of both a primary psychotic disorder and psychosis as a manifestation of MS. His late age at his first psychotic break is atypical for primary psychotic disease, and the lack of MRI imaging done at his initial psychotic episodes cannot exclude a primary MS diagnosis. Still, his lack of MRI findings at his most recent hospitalization, negative symptomatology, and strong history of schizophrenia make a primary psychotic disorder likely.
Following his future clinical course will be necessary to determine the etiology of his psychotic episodes. Future episodes of psychosis with neurologic symptoms would suggest a primary MS diagnosis and potential benefit of immunosuppressant treatment, whereas repeated psychotic breaks with minimal temporal lobe involvement or demyelination as seen on MRI would be suspicious for separate MS and psychotic disease processes. Further research on treatment regimens for patients experiencing psychosis as a manifestation of MS is still necessary.
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040.
2. Camara-Lemarroy CR, Ibarra-Yruegas BE, Rodriguez-Gutierrez R, Berrios-Morales I, Ionete C, Riskind P. The varieties of psychosis in multiple sclerosis: a systematic review of cases. Mult Scler Relat Disord. 2017;12:9-14.
3. Cottrel SS, Wilson SA. The affective symptomatology of disseminated sclerosis: a study of 100 cases. J Neurol Psychopathology. 1926;7(25):1-30.
4. Johansson V, Lundholm C, Hillert J, et al. Multiple sclerosis and psychiatric disorders: comorbidity and sibling risk in a nationwide Swedish cohort. Mult Scler. 2014;20(14):1881-1891.
5. Rossi S, Studer V, Motta C, et al. Neuroinflammation drives anxiety and depression in relapsing-remitting multiple sclerosis. Neurology. 2017;89(13):1338-1347.
6. Gilberthorpe TG, O’Connell KE, Carolan A, et al. The spectrum of psychosis in multiple sclerosis: a clinical case series. Neuropsychiatric disease and treatment. 2017;13:303.
7. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;65(7):1123-1125.
8. Kosmidis MH, Giannakou M, Messinis L, Papathanasopoulos P. Psychotic features associated with multiple sclerosis. Int Rev Psychiatry. 2010; 22(1):55-66.
9. US Department of Veterans Affairs. Public health: military exposures. https://www.publichealth.va.gov/exposures/. Updated April 16, 2019. Accessed May 13, 2019.
10. DeBeer BB, Davidson D, Meyer EC, Kimbrel NA, Gulliver SB, Morissette SB. The association between toxic exposures and chronic multisymptom illness in veterans of the wars of Iraq and Afghanistan. J Occup Environ Med. 2017;59(1):54-60.
11. Kang HK, Li B, Mahan CM, Eisen SA, Engel CC. Health of US veterans of 1991 Gulf War: a follow-up survey in 10 years. J Occup Environ Med. 2009;51(4):401-410.
12. Murphy R, O’Donoghue S, Counihan T, et al. Neuropsychiatric syndromes of multiple sclerosis. J Neurol Neurosurg Psychiatry. 2017;88(8):697-708.
13. Davids E, Hartwig U, Gastpar, M. Antipsychotic treatment of psychosis associated with multiple sclerosis. Prog Neuro Psychopharmacol Biol Psychiatry. 2004;28(4):743-744.
14. Lo Fermo S, Barone R, Patti F, et al. Outcome of psychiatric symptoms presenting at onset of multiple sclerosis: a retrospective study. Mult Scler. 2010;16(6):742-748.
15. Enderami A, Fouladi R, Hosseini HS. First-episode psychosis as the initial presentation of multiple sclerosis: a case report. Int Medical Case Rep J. 2018;11:73-76.
16. Fragoso YD, Frota ER, Lopes JS, et al. Severe depression, suicide attempts, and ideation during the use of interferon beta by patients with multiple sclerosis. Clin Neuropharmacol. 2010;33(6):312-316.
17. Abou-Donia MB, Conboy LA, Kokkotou E, et al. Screening for novel central nervous system biomarkers in veterans with Gulf War Illness. Neurotoxicol Teratol. 2017;61:36-46.
18. Abou-Donia MB, Lieberman A, Curtis L. Neural autoantibodies in patients with neurological symptoms and histories of chemical/mold exposures. Toxicol Ind Health. 2018;34(1):44-53.
19. Wallin MT, Kurtzke JF, Culpepper WJ, et al. Multiple sclerosis in Gulf War era veterans. 2. Military deployment and risk of multiple sclerosis in the first Gulf War. Neuroepidemiology. 2014;42(4):226-234.
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040.
2. Camara-Lemarroy CR, Ibarra-Yruegas BE, Rodriguez-Gutierrez R, Berrios-Morales I, Ionete C, Riskind P. The varieties of psychosis in multiple sclerosis: a systematic review of cases. Mult Scler Relat Disord. 2017;12:9-14.
3. Cottrel SS, Wilson SA. The affective symptomatology of disseminated sclerosis: a study of 100 cases. J Neurol Psychopathology. 1926;7(25):1-30.
4. Johansson V, Lundholm C, Hillert J, et al. Multiple sclerosis and psychiatric disorders: comorbidity and sibling risk in a nationwide Swedish cohort. Mult Scler. 2014;20(14):1881-1891.
5. Rossi S, Studer V, Motta C, et al. Neuroinflammation drives anxiety and depression in relapsing-remitting multiple sclerosis. Neurology. 2017;89(13):1338-1347.
6. Gilberthorpe TG, O’Connell KE, Carolan A, et al. The spectrum of psychosis in multiple sclerosis: a clinical case series. Neuropsychiatric disease and treatment. 2017;13:303.
7. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;65(7):1123-1125.
8. Kosmidis MH, Giannakou M, Messinis L, Papathanasopoulos P. Psychotic features associated with multiple sclerosis. Int Rev Psychiatry. 2010; 22(1):55-66.
9. US Department of Veterans Affairs. Public health: military exposures. https://www.publichealth.va.gov/exposures/. Updated April 16, 2019. Accessed May 13, 2019.
10. DeBeer BB, Davidson D, Meyer EC, Kimbrel NA, Gulliver SB, Morissette SB. The association between toxic exposures and chronic multisymptom illness in veterans of the wars of Iraq and Afghanistan. J Occup Environ Med. 2017;59(1):54-60.
11. Kang HK, Li B, Mahan CM, Eisen SA, Engel CC. Health of US veterans of 1991 Gulf War: a follow-up survey in 10 years. J Occup Environ Med. 2009;51(4):401-410.
12. Murphy R, O’Donoghue S, Counihan T, et al. Neuropsychiatric syndromes of multiple sclerosis. J Neurol Neurosurg Psychiatry. 2017;88(8):697-708.
13. Davids E, Hartwig U, Gastpar, M. Antipsychotic treatment of psychosis associated with multiple sclerosis. Prog Neuro Psychopharmacol Biol Psychiatry. 2004;28(4):743-744.
14. Lo Fermo S, Barone R, Patti F, et al. Outcome of psychiatric symptoms presenting at onset of multiple sclerosis: a retrospective study. Mult Scler. 2010;16(6):742-748.
15. Enderami A, Fouladi R, Hosseini HS. First-episode psychosis as the initial presentation of multiple sclerosis: a case report. Int Medical Case Rep J. 2018;11:73-76.
16. Fragoso YD, Frota ER, Lopes JS, et al. Severe depression, suicide attempts, and ideation during the use of interferon beta by patients with multiple sclerosis. Clin Neuropharmacol. 2010;33(6):312-316.
17. Abou-Donia MB, Conboy LA, Kokkotou E, et al. Screening for novel central nervous system biomarkers in veterans with Gulf War Illness. Neurotoxicol Teratol. 2017;61:36-46.
18. Abou-Donia MB, Lieberman A, Curtis L. Neural autoantibodies in patients with neurological symptoms and histories of chemical/mold exposures. Toxicol Ind Health. 2018;34(1):44-53.
19. Wallin MT, Kurtzke JF, Culpepper WJ, et al. Multiple sclerosis in Gulf War era veterans. 2. Military deployment and risk of multiple sclerosis in the first Gulf War. Neuroepidemiology. 2014;42(4):226-234.