User login
FDA approves continuous glucose monitor with AI assistant
between the ages of 14 and 75 years old.
The first CGM to use artificial intelligence for this purpose, the Guardian Connect system is intended to help people with diabetes who use multiple daily injections of insulin to manage their diabetes by helping them prevent hyperglycemia and hypoglycemia, according to a statement from Medtronic.
Guardian Connect utilizes a predictive algorithm that alerts patients of significant swings in blood glucose levels up to 60 minutes prior to the event. When combined with the Guardian Sensor 3, which is placed on the abdomen to monitor blood glucose levels, the Guardian Connect system was accurate and was able to alert patients about 98.5% of hypoglycemic events, according to the results of a clinical trial. This information can also be shared and monitored with care takers and family member in real time or via text message.
Perhaps the most intriguing aspect of using the Guardian Connect system is exclusive access to the Sugar.IQ smart diabetes assistant. Utilizing artificial intelligence technology from IBM Watson Health, the Sugar.IQ assistant continually analyzes how patient’s blood glucose levels respond to factors like food intake, insulin dosages, and daily routines. The combination of continuous monitoring and real-time analysis may be able to identify patterns and lead to personalized insights that will help patients with diabetes keep their blood glucose levels under control.
“Despite proven benefits and advances in technology, only a minority of insulin-using people with diabetes currently use continuous glucose monitors,” Timothy Bailey, MD, the director of the AMCR Institute and a clinical associate professor at University of California, San Diego, said in a statement. “Newer sensors paired with intelligent algorithms that help to both predict and understand glucose excursions, particularly hypoglycemia, will make diabetes safer and more comprehensible for people who inject insulin. Greater utilization of smarter CGM systems promises to allow our patients to achieve more glycemic time-in-range and to further reduce the risk of hypoglycemia,” he said.
Similar products have been approved in the last 6 months, but they have not utilized artificial intelligence and continuous analysis.
No serious adverse events were reported in the clinical trial of Guardian Connect, but less serious adverse events were observed, including gastroenteritis, upper respiratory infection, worsening of benign prostatic hyperplasia, rash, and blisters.
Guardian Connect should be available commercially sometime this summer.
between the ages of 14 and 75 years old.
The first CGM to use artificial intelligence for this purpose, the Guardian Connect system is intended to help people with diabetes who use multiple daily injections of insulin to manage their diabetes by helping them prevent hyperglycemia and hypoglycemia, according to a statement from Medtronic.
Guardian Connect utilizes a predictive algorithm that alerts patients of significant swings in blood glucose levels up to 60 minutes prior to the event. When combined with the Guardian Sensor 3, which is placed on the abdomen to monitor blood glucose levels, the Guardian Connect system was accurate and was able to alert patients about 98.5% of hypoglycemic events, according to the results of a clinical trial. This information can also be shared and monitored with care takers and family member in real time or via text message.
Perhaps the most intriguing aspect of using the Guardian Connect system is exclusive access to the Sugar.IQ smart diabetes assistant. Utilizing artificial intelligence technology from IBM Watson Health, the Sugar.IQ assistant continually analyzes how patient’s blood glucose levels respond to factors like food intake, insulin dosages, and daily routines. The combination of continuous monitoring and real-time analysis may be able to identify patterns and lead to personalized insights that will help patients with diabetes keep their blood glucose levels under control.
“Despite proven benefits and advances in technology, only a minority of insulin-using people with diabetes currently use continuous glucose monitors,” Timothy Bailey, MD, the director of the AMCR Institute and a clinical associate professor at University of California, San Diego, said in a statement. “Newer sensors paired with intelligent algorithms that help to both predict and understand glucose excursions, particularly hypoglycemia, will make diabetes safer and more comprehensible for people who inject insulin. Greater utilization of smarter CGM systems promises to allow our patients to achieve more glycemic time-in-range and to further reduce the risk of hypoglycemia,” he said.
Similar products have been approved in the last 6 months, but they have not utilized artificial intelligence and continuous analysis.
No serious adverse events were reported in the clinical trial of Guardian Connect, but less serious adverse events were observed, including gastroenteritis, upper respiratory infection, worsening of benign prostatic hyperplasia, rash, and blisters.
Guardian Connect should be available commercially sometime this summer.
between the ages of 14 and 75 years old.
The first CGM to use artificial intelligence for this purpose, the Guardian Connect system is intended to help people with diabetes who use multiple daily injections of insulin to manage their diabetes by helping them prevent hyperglycemia and hypoglycemia, according to a statement from Medtronic.
Guardian Connect utilizes a predictive algorithm that alerts patients of significant swings in blood glucose levels up to 60 minutes prior to the event. When combined with the Guardian Sensor 3, which is placed on the abdomen to monitor blood glucose levels, the Guardian Connect system was accurate and was able to alert patients about 98.5% of hypoglycemic events, according to the results of a clinical trial. This information can also be shared and monitored with care takers and family member in real time or via text message.
Perhaps the most intriguing aspect of using the Guardian Connect system is exclusive access to the Sugar.IQ smart diabetes assistant. Utilizing artificial intelligence technology from IBM Watson Health, the Sugar.IQ assistant continually analyzes how patient’s blood glucose levels respond to factors like food intake, insulin dosages, and daily routines. The combination of continuous monitoring and real-time analysis may be able to identify patterns and lead to personalized insights that will help patients with diabetes keep their blood glucose levels under control.
“Despite proven benefits and advances in technology, only a minority of insulin-using people with diabetes currently use continuous glucose monitors,” Timothy Bailey, MD, the director of the AMCR Institute and a clinical associate professor at University of California, San Diego, said in a statement. “Newer sensors paired with intelligent algorithms that help to both predict and understand glucose excursions, particularly hypoglycemia, will make diabetes safer and more comprehensible for people who inject insulin. Greater utilization of smarter CGM systems promises to allow our patients to achieve more glycemic time-in-range and to further reduce the risk of hypoglycemia,” he said.
Similar products have been approved in the last 6 months, but they have not utilized artificial intelligence and continuous analysis.
No serious adverse events were reported in the clinical trial of Guardian Connect, but less serious adverse events were observed, including gastroenteritis, upper respiratory infection, worsening of benign prostatic hyperplasia, rash, and blisters.
Guardian Connect should be available commercially sometime this summer.
CAR T before transplant yields durable remission in B-cell malignancies
SALT LAKE CITY – Chimeric antigen receptor (CAR) T-cell therapy may be an effective bridge to hematopoietic cell transplant (HCT) for high-risk B-cell malignancies, according to a systematic analysis of patient data from the National Cancer Institute.
Additionally, patients who have received CAR T-cell therapy are likely to enter HCT with a minimal residual disease (MRD)–negative complete response, which raises the possibility of a significantly less intense conditioning regimen that could omit total body irradiation (TBI), Haneen Shalabi, DO, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“Patients who underwent HCT post–CAR T therapy did not have increased transplant-related morbidity or mortality,” said Dr. Shalabi, a pediatric oncologist in the hematologic diseases division of the National Cancer Institute’s pediatric oncology branch.
The combined approach also overcomes the frequent relapses seen after CAR T-cell therapy in this population. Of the 45 patients who received CAR T-cell therapy and achieved MRD-negative complete response as measured by flow cytometry, 20 did not go on to receive HCT. Of the 20 who didn’t receive HCT, 16 (80%) relapsed; 19 of the 20 (95%) had received prior HCT, said Dr. Shalabi.
However, of the 25 patients who proceeded on to receive HCT, 15 (60%) were in ongoing remission, with a median duration of 35 months (range, 11-55 months). Six patients (24%) experienced transplant-related mortality; four of these patients had no prior HCT. Ten patients (40%) experienced acute graft-versus-host disease (GVHD); two of these patients experienced grade 4 GVHD, and one experienced grade 3 GVHD.
Of the 25 patients who went on to HCT, 19 were receiving their first transplant, with a median time to transplant after CAR T-cell therapy of 57 days. Five patients (20%) had primary refractory disease. Most patients (n = 18; 72%) had TBI-based conditioning prior to their post–CAR T-cell therapy HCT. The median patient age was 15 (range, 5-30) years.
The systematic review included patients from two phase 1 studies; one was of CD19-28z CAR T-cell therapy for children and young adults with B-cell leukemia or lymphoma, and the other was of CD22-41BB CAR T-cell therapy for children and young adults with recurrent or refractory B-cell malignancies expressing CD22.
To weigh the benefit of the combined CAR T-cell therapy/HCT approach, Dr. Shalabi and her colleagues used a competing risk analysis to determine the risk of relapse post-HCT versus the risk of transplant-related mortality. Among patients undergoing their first HCT, the researchers found a 12-month cumulative incidence of relapse of 5.3% with the combined CAR T-cell therapy/HCT approach (95% confidence interval, 0.3%-22.1%). The 24-month cumulative incidence of relapse was 11.3% (95% CI, 1.7%-31.1%).
The analysis also showed the value of next-generation sequencing (NGS). “As we think about utilizing CAR T therapy as a bridge to transplant, we wanted to study the depth of CAR T–induced remission by next-gen sequencing,” Dr. Shalabi said.
Eight patients on the CD22 CAR trial had MRD analyses based on both flow cytometry and NGS. According to flow cytometry, all eight were MRD negative by 1 month; however, according to NGS, two did have detectable disease, which decreased with time. “Next-gen sequencing can identify earlier time points for relapse or ongoing remission” than flow cytometry can, she said.
An additional finding was that two-thirds of the patients who received the CD19/CD28z CAR T cells had no detectable CAR T cells when the pre-HCT conditioning regimen was initiated, said Dr. Shalabi. “CAR persistence – or lack thereof – didn’t impact post-HCT outcomes,” she said, adding that shorter-acting CAR T cells may actually be preferable when HCT is readily available as an option.
“The impact of CAR persistence peritransplant requires further analysis,” Dr. Shalabi said. It’s possible, though, that “consolidative HCT following CAR may synergistically improve event-free and overall survival for this high-risk population.”
Looking forward, Dr. Shalabi and her team are asking bigger questions: “For future directions – and this is a very big question that those in the room would probably like to know – by inducing NGS-negativity, can CAR T therapy allow for HCT conditioning deintensification, potentially reducing the risk of TRM [transplant-related mortality] and long term comorbidities?”
A future trial will explore outcomes for a conditioning regimen that omits TBI for patients who are MRD-negative by NGS, said Dr. Shalabi.
Another direction for her team’s research is to see whether introducing CAR T-cell therapy earlier in a very-high-risk population may improve outcomes; the current study population was heavily pretreated, Dr. Shalabi said.
Dr. Shalabi is employed by the National Cancer Institute. She reported no conflicts of interest.
SOURCE: Shalabi H et al. 2018 BMT Tandem Meetings, Abstract 6.
SALT LAKE CITY – Chimeric antigen receptor (CAR) T-cell therapy may be an effective bridge to hematopoietic cell transplant (HCT) for high-risk B-cell malignancies, according to a systematic analysis of patient data from the National Cancer Institute.
Additionally, patients who have received CAR T-cell therapy are likely to enter HCT with a minimal residual disease (MRD)–negative complete response, which raises the possibility of a significantly less intense conditioning regimen that could omit total body irradiation (TBI), Haneen Shalabi, DO, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“Patients who underwent HCT post–CAR T therapy did not have increased transplant-related morbidity or mortality,” said Dr. Shalabi, a pediatric oncologist in the hematologic diseases division of the National Cancer Institute’s pediatric oncology branch.
The combined approach also overcomes the frequent relapses seen after CAR T-cell therapy in this population. Of the 45 patients who received CAR T-cell therapy and achieved MRD-negative complete response as measured by flow cytometry, 20 did not go on to receive HCT. Of the 20 who didn’t receive HCT, 16 (80%) relapsed; 19 of the 20 (95%) had received prior HCT, said Dr. Shalabi.
However, of the 25 patients who proceeded on to receive HCT, 15 (60%) were in ongoing remission, with a median duration of 35 months (range, 11-55 months). Six patients (24%) experienced transplant-related mortality; four of these patients had no prior HCT. Ten patients (40%) experienced acute graft-versus-host disease (GVHD); two of these patients experienced grade 4 GVHD, and one experienced grade 3 GVHD.
Of the 25 patients who went on to HCT, 19 were receiving their first transplant, with a median time to transplant after CAR T-cell therapy of 57 days. Five patients (20%) had primary refractory disease. Most patients (n = 18; 72%) had TBI-based conditioning prior to their post–CAR T-cell therapy HCT. The median patient age was 15 (range, 5-30) years.
The systematic review included patients from two phase 1 studies; one was of CD19-28z CAR T-cell therapy for children and young adults with B-cell leukemia or lymphoma, and the other was of CD22-41BB CAR T-cell therapy for children and young adults with recurrent or refractory B-cell malignancies expressing CD22.
To weigh the benefit of the combined CAR T-cell therapy/HCT approach, Dr. Shalabi and her colleagues used a competing risk analysis to determine the risk of relapse post-HCT versus the risk of transplant-related mortality. Among patients undergoing their first HCT, the researchers found a 12-month cumulative incidence of relapse of 5.3% with the combined CAR T-cell therapy/HCT approach (95% confidence interval, 0.3%-22.1%). The 24-month cumulative incidence of relapse was 11.3% (95% CI, 1.7%-31.1%).
The analysis also showed the value of next-generation sequencing (NGS). “As we think about utilizing CAR T therapy as a bridge to transplant, we wanted to study the depth of CAR T–induced remission by next-gen sequencing,” Dr. Shalabi said.
Eight patients on the CD22 CAR trial had MRD analyses based on both flow cytometry and NGS. According to flow cytometry, all eight were MRD negative by 1 month; however, according to NGS, two did have detectable disease, which decreased with time. “Next-gen sequencing can identify earlier time points for relapse or ongoing remission” than flow cytometry can, she said.
An additional finding was that two-thirds of the patients who received the CD19/CD28z CAR T cells had no detectable CAR T cells when the pre-HCT conditioning regimen was initiated, said Dr. Shalabi. “CAR persistence – or lack thereof – didn’t impact post-HCT outcomes,” she said, adding that shorter-acting CAR T cells may actually be preferable when HCT is readily available as an option.
“The impact of CAR persistence peritransplant requires further analysis,” Dr. Shalabi said. It’s possible, though, that “consolidative HCT following CAR may synergistically improve event-free and overall survival for this high-risk population.”
Looking forward, Dr. Shalabi and her team are asking bigger questions: “For future directions – and this is a very big question that those in the room would probably like to know – by inducing NGS-negativity, can CAR T therapy allow for HCT conditioning deintensification, potentially reducing the risk of TRM [transplant-related mortality] and long term comorbidities?”
A future trial will explore outcomes for a conditioning regimen that omits TBI for patients who are MRD-negative by NGS, said Dr. Shalabi.
Another direction for her team’s research is to see whether introducing CAR T-cell therapy earlier in a very-high-risk population may improve outcomes; the current study population was heavily pretreated, Dr. Shalabi said.
Dr. Shalabi is employed by the National Cancer Institute. She reported no conflicts of interest.
SOURCE: Shalabi H et al. 2018 BMT Tandem Meetings, Abstract 6.
SALT LAKE CITY – Chimeric antigen receptor (CAR) T-cell therapy may be an effective bridge to hematopoietic cell transplant (HCT) for high-risk B-cell malignancies, according to a systematic analysis of patient data from the National Cancer Institute.
Additionally, patients who have received CAR T-cell therapy are likely to enter HCT with a minimal residual disease (MRD)–negative complete response, which raises the possibility of a significantly less intense conditioning regimen that could omit total body irradiation (TBI), Haneen Shalabi, DO, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“Patients who underwent HCT post–CAR T therapy did not have increased transplant-related morbidity or mortality,” said Dr. Shalabi, a pediatric oncologist in the hematologic diseases division of the National Cancer Institute’s pediatric oncology branch.
The combined approach also overcomes the frequent relapses seen after CAR T-cell therapy in this population. Of the 45 patients who received CAR T-cell therapy and achieved MRD-negative complete response as measured by flow cytometry, 20 did not go on to receive HCT. Of the 20 who didn’t receive HCT, 16 (80%) relapsed; 19 of the 20 (95%) had received prior HCT, said Dr. Shalabi.
However, of the 25 patients who proceeded on to receive HCT, 15 (60%) were in ongoing remission, with a median duration of 35 months (range, 11-55 months). Six patients (24%) experienced transplant-related mortality; four of these patients had no prior HCT. Ten patients (40%) experienced acute graft-versus-host disease (GVHD); two of these patients experienced grade 4 GVHD, and one experienced grade 3 GVHD.
Of the 25 patients who went on to HCT, 19 were receiving their first transplant, with a median time to transplant after CAR T-cell therapy of 57 days. Five patients (20%) had primary refractory disease. Most patients (n = 18; 72%) had TBI-based conditioning prior to their post–CAR T-cell therapy HCT. The median patient age was 15 (range, 5-30) years.
The systematic review included patients from two phase 1 studies; one was of CD19-28z CAR T-cell therapy for children and young adults with B-cell leukemia or lymphoma, and the other was of CD22-41BB CAR T-cell therapy for children and young adults with recurrent or refractory B-cell malignancies expressing CD22.
To weigh the benefit of the combined CAR T-cell therapy/HCT approach, Dr. Shalabi and her colleagues used a competing risk analysis to determine the risk of relapse post-HCT versus the risk of transplant-related mortality. Among patients undergoing their first HCT, the researchers found a 12-month cumulative incidence of relapse of 5.3% with the combined CAR T-cell therapy/HCT approach (95% confidence interval, 0.3%-22.1%). The 24-month cumulative incidence of relapse was 11.3% (95% CI, 1.7%-31.1%).
The analysis also showed the value of next-generation sequencing (NGS). “As we think about utilizing CAR T therapy as a bridge to transplant, we wanted to study the depth of CAR T–induced remission by next-gen sequencing,” Dr. Shalabi said.
Eight patients on the CD22 CAR trial had MRD analyses based on both flow cytometry and NGS. According to flow cytometry, all eight were MRD negative by 1 month; however, according to NGS, two did have detectable disease, which decreased with time. “Next-gen sequencing can identify earlier time points for relapse or ongoing remission” than flow cytometry can, she said.
An additional finding was that two-thirds of the patients who received the CD19/CD28z CAR T cells had no detectable CAR T cells when the pre-HCT conditioning regimen was initiated, said Dr. Shalabi. “CAR persistence – or lack thereof – didn’t impact post-HCT outcomes,” she said, adding that shorter-acting CAR T cells may actually be preferable when HCT is readily available as an option.
“The impact of CAR persistence peritransplant requires further analysis,” Dr. Shalabi said. It’s possible, though, that “consolidative HCT following CAR may synergistically improve event-free and overall survival for this high-risk population.”
Looking forward, Dr. Shalabi and her team are asking bigger questions: “For future directions – and this is a very big question that those in the room would probably like to know – by inducing NGS-negativity, can CAR T therapy allow for HCT conditioning deintensification, potentially reducing the risk of TRM [transplant-related mortality] and long term comorbidities?”
A future trial will explore outcomes for a conditioning regimen that omits TBI for patients who are MRD-negative by NGS, said Dr. Shalabi.
Another direction for her team’s research is to see whether introducing CAR T-cell therapy earlier in a very-high-risk population may improve outcomes; the current study population was heavily pretreated, Dr. Shalabi said.
Dr. Shalabi is employed by the National Cancer Institute. She reported no conflicts of interest.
SOURCE: Shalabi H et al. 2018 BMT Tandem Meetings, Abstract 6.
REPORTING FROM THE 2018 BMT TANDEM MEETINGS
Key clinical point:
Major finding: Of 20 patients receiving CAR T before HCT, 15 (60%) were in ongoing remission of a median 35 months.
Study details: Systematic analysis of 42 patients with B-cell malignancies receiving CAR T-cell therapy at the National Cancer Institute.
Disclosures: The study was conducted at the National Cancer Institute, where Dr. Shalabi is employed.
Source: Shalabi H et al. 2018 BMT Tandem Meetings, Abstract 6.
Emerging data help inform immunotherapy for urothelial cancer
SAN FRANCISCO – Emerging data from phase 3 clinical trials are better clarifying the efficacy and safety of immunotherapy in advanced urothelial cancer and helping identify patients most likely to benefit.
An updated analysis of the KEYNOTE-045 trial showed that, compared with chemotherapy, pembrolizumab (Keytruda), an antibody to programmed death-1 (PD-1), almost doubled the 2-year survival rate in patients with recurrent or advanced urothelial cancer. No cumulative toxicity was seen.
Biomarker analyses from the IMvigor 211 trial showed that, compared with chemotherapy, atezolizumab (Tecentriq), an antibody to programmed cell death ligand 1 (PD-L1), prolonged survival by more than 7 months in patients with platinum-treated locally advanced or metastatic disease whose tumors were positive for this ligand and had a high mutational burden. The difference translated to a halving of the risk of death.
Results of both trials were reported at the 2018 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
“It is clear that PD-1 and PD-L1 targeted immunotherapy now has a role in most patients with advanced urothelial cancer,” Robert J. Jones, MBChB, PhD, professor of clinical cancer research, University of Glasgow, Beatson West of Scotland Cancer Centre, commented in an invited discussion. “It is also true that cytotoxic chemotherapy maintains a role for many, and that both modalities are often ineffective and may be toxic.”
KEYNOTE-045 trial update
Initial results of KEYNOTE-045, at a median follow-up of 14.1 months, provided level I evidence for the safety and efficacy of pembrolizumab over chemotherapy as second-line therapy for recurrent, advanced urothelial cancer (N Engl J Med. 2017;376:1015-26), leading to approval for that indication. (Pembrolizumab is also approved as first-line therapy for cisplatin-ineligible patients).
Lead investigator Joaquim Bellmunt, MD, PhD, an associate professor of medicine at Harvard Medical School and director of the Bladder Cancer Center, Dana-Farber Cancer Institute, both in Boston, reported a trial update, now at a median follow-up of 27.7 months.
Results among 542 patients showed that the initial overall survival benefit of pembrolizumab over chemotherapy (vinflunine, paclitaxel, or docetaxel) (hazard ratio, 0.73; P = .0022) was sustained and in fact now somewhat greater with longer follow-up (HR, 0.70; P = .00017).
Median overall survival was 10.3 months and 7.3 months, respectively. Corresponding 1-year survival rates were 44.4% and 29.8%, and corresponding 2-year survival rates, 27.0% and 14.3%.
At 24 months, 60.6% of patients in the chemotherapy arm had received an immunotherapy agent, including some who had received pembrolizumab as part of crossover, Dr. Bellmunt noted.
Overall survival benefit was generally similar across subgroups, including patients with PD-L1–positive tumors (defined as a combined positive score of 10% or higher) (HR, 0.56; P = .00153) and patients with PD-L1–negative tumors (HR, 0.75; P = .00859).
The lack of a progression-free survival benefit of pembrolizumab over chemotherapy in the initial analysis (HR, 0.98; P = .420) persisted in the updated analysis (HR, 0.96; P = .317).
The overall response rate now was 21.1% with pembrolizumab and 11.0% with chemotherapy. In the former group, the rate of complete response had increased from 7.0% to 9.3% with the longer follow-up. Median time to response was identical, at 2.1 months, but duration of response was longer with pembrolizumab (not reached vs. 4.4 months).
“We haven’t seen any signals of cumulative toxicity with subsequent follow-up,” Dr. Bellmunt reported. Similar to findings of the initial analysis, the most common grade 3-5 treatment-related adverse events were pruritus, fatigue, and diarrhea with pembrolizumab, and neutropenia, anemia, and fatigue with chemotherapy. As expected, the pembrolizumab group had higher rates of hypothyroidism, pneumonitis, hyperthyroidism, and colitis.
“The overall survival benefit and superior safety of pembrolizumab versus chemotherapy in this second-line patient population is maintained after 2 years of follow-up. At 24 months, 27% of patients are alive, and this is similar to what we are seeing with other immune-sensitive diseases like melanoma,” he concluded. “Results in patients with PD-L1–positive or –negative tumors were consistent with the intent-to-treat population. We have seen some hints with this biomarker, but they are not very striking.”
IMvigor 211 trial biomarker analyses
The IMvigor 211 trial enrolled 931 patients with locally advanced or metastatic urothelial carcinoma who had experienced progression during or after platinum-based chemotherapy and had received at most two prior lines of therapy.
At a median follow-up of 17.3 months, the trial did not meet its primary endpoint of significantly better overall survival with atezolizumab versus chemotherapy (vinflunine, docetaxel, or paclitaxel) in patients having PD-L1–positive tumors, defined as immunohistochemical staining of 2 or 3 (HR, 0.87; 95% confidence interval, 0.63-1.21; P = .41) (Lancet. 2018;391:748-57).
Findings were similar in the entire intention-to-treat population (HR, 0.85; 95% CI, 0.73-0.99) and in the subset with tumors having PD-L1–negative tumors, defined as immunohistochemical staining of 0 or 1 (HR, 0.84; 0.71-1.00). In an unexpected finding, PD-L1 positivity was associated with better outcome in both treatment arms.
“So PD-L1 is a classic prognostic, not predictive, biomarker,” commented lead investigator Thomas Powles, MBBS, MRCP, MD, a clinical professor of genitourinary oncology with Barts Health NHS Trust, St. Bartholomew’s Hospital, London. The investigators therefore conducted a series of analyses in the intent-to-treat population to identify predictive biomarkers.
Results were essentially the same with the tumor gene expression 3 (tGE3) signature, an RNA signature that captures expression of the genes encoding interferon gamma, a chemokine ligand, and PD-L1, and that is a marker for preexisting T-cell immunity. And they were also similar with the DNA damage response (DDR) biomarker.
However, a different pattern was seen with tumor mutational burden (TMB), a FoundationOne panel. Patients with TMB-high tumors had a substantial gain in overall survival from atezolizumab versus chemotherapy (HR, 0.68; 95% CI, 0.51-0.90), whereas those with TMB-low tumors did not (HR, 1.00; 95% CI, 0.75-1.32).
“TMB appears to be a predictive but not a prognostic biomarker,” Dr. Powles said. “It’s not perfect. Complete and partial responses and long overall survival were seen in both arms. Nevertheless, it seems like a step in the right direction.”
Finally, with insight on the nature and relationships of the various biomarkers, the investigators assessed the combination of TMB with PD-L1, finding that atezolizumab had a marked overall survival benefit in patients with TMB-high and PD-L1–positive tumors (17.8 vs. 10.6 months; HR, 0.50; 95% CI, 0.29-0.86).
“I think by using combinations of biomarkers, first-generation and second-generation, we may actually be able to better select patients for treatment in the future,” Dr. Powles concluded.
New data, new insights
“We already know the KEYNOTE-045 trial is positive,” commented the invited discussant, Dr. Jones. “This longer follow-up data is important because we need to better describe the magnitude of benefit.”
The updated survival findings are exciting because they resemble those seen with ipilimumab in melanoma, with about a fifth of patients still alive several years out, he said. Longer follow-up is needed, but “the data we see today are in keeping with the possibility that we might be seeing a similar long-term tail – the so-called immuno-oncology tail – of survival for patients with urothelial cancer as well.”
Although not statistically significant, the difference in progression-free survival is clinically important, according to Dr. Jones. This benefit is driven by both higher response rate and longer duration of response with pembrolizumab.
Long-term toxicity, especially immune-related toxicity, is also a consideration. “There is a small increment in the number of some of these toxicities, but essentially it hasn’t changed. So it would appear that there is certainly not an unexpected peak of latent immunotoxicity with this treatment,” he noted.
“Our confidence in the data for second-line pembrolizumab, if it needed to be further increased, is increased. This does help our patients make an informed decision about whether or not to accept this treatment,” he summarized.
Turning to the IMvigor 211 biomarker study, Dr. Jones said, “I would argue that the choice of second-line therapy in advanced urothelial cancer is not a clinically important decision. The reason for saying that is the case for second-line chemotherapy is poor. We’ve all used it, but we’ve never had high level evidence of benefit. … But it’s important because when we consider moving into the first-line setting, where there are active alternatives, or maybe even more into the perioperative setting, it actually could be vitally important.”
Studies of immunotherapies and targeted therapies in other cancers suggest that a clinically useful predictive biomarker will identify patients who will derive at least a doubling of favorable outcome or a halving of unfavorable outcome when given the drug as compared with a control. “So it appears that the bar has been set quite high,” Dr. Jones said.
“These IMvigor 211 data are exploratory, and they would need further independent validation, in my view,” he said. Nevertheless, “this may provide us the opportunity to use combinations of biomarkers where now we are seeing a hazard ratio of 0.50 [for risk of death] combining PD-L1 with high tumor mutational burden (TMB). That hazard ratio is bringing it into the area where it may be of a magnitude big enough to use in clinical practice, if this could be validated.”
“I would say that none of these data support a role for second-line cytotoxics after failure of platinum, at least not in preference to a checkpoint inhibitor,” Dr. Jones concluded. “There is still no biomarker to inform a choice in second-line treatment. However, TMB, either alone or in combination with other markers, shows promise, which we need to validate in future randomized trials.”
SOURCE: Bellmunt J et al. GUC 2018 Abstract 410; Powles T et al. GUC 2018, Abstract 409.
SAN FRANCISCO – Emerging data from phase 3 clinical trials are better clarifying the efficacy and safety of immunotherapy in advanced urothelial cancer and helping identify patients most likely to benefit.
An updated analysis of the KEYNOTE-045 trial showed that, compared with chemotherapy, pembrolizumab (Keytruda), an antibody to programmed death-1 (PD-1), almost doubled the 2-year survival rate in patients with recurrent or advanced urothelial cancer. No cumulative toxicity was seen.
Biomarker analyses from the IMvigor 211 trial showed that, compared with chemotherapy, atezolizumab (Tecentriq), an antibody to programmed cell death ligand 1 (PD-L1), prolonged survival by more than 7 months in patients with platinum-treated locally advanced or metastatic disease whose tumors were positive for this ligand and had a high mutational burden. The difference translated to a halving of the risk of death.
Results of both trials were reported at the 2018 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
“It is clear that PD-1 and PD-L1 targeted immunotherapy now has a role in most patients with advanced urothelial cancer,” Robert J. Jones, MBChB, PhD, professor of clinical cancer research, University of Glasgow, Beatson West of Scotland Cancer Centre, commented in an invited discussion. “It is also true that cytotoxic chemotherapy maintains a role for many, and that both modalities are often ineffective and may be toxic.”
KEYNOTE-045 trial update
Initial results of KEYNOTE-045, at a median follow-up of 14.1 months, provided level I evidence for the safety and efficacy of pembrolizumab over chemotherapy as second-line therapy for recurrent, advanced urothelial cancer (N Engl J Med. 2017;376:1015-26), leading to approval for that indication. (Pembrolizumab is also approved as first-line therapy for cisplatin-ineligible patients).
Lead investigator Joaquim Bellmunt, MD, PhD, an associate professor of medicine at Harvard Medical School and director of the Bladder Cancer Center, Dana-Farber Cancer Institute, both in Boston, reported a trial update, now at a median follow-up of 27.7 months.
Results among 542 patients showed that the initial overall survival benefit of pembrolizumab over chemotherapy (vinflunine, paclitaxel, or docetaxel) (hazard ratio, 0.73; P = .0022) was sustained and in fact now somewhat greater with longer follow-up (HR, 0.70; P = .00017).
Median overall survival was 10.3 months and 7.3 months, respectively. Corresponding 1-year survival rates were 44.4% and 29.8%, and corresponding 2-year survival rates, 27.0% and 14.3%.
At 24 months, 60.6% of patients in the chemotherapy arm had received an immunotherapy agent, including some who had received pembrolizumab as part of crossover, Dr. Bellmunt noted.
Overall survival benefit was generally similar across subgroups, including patients with PD-L1–positive tumors (defined as a combined positive score of 10% or higher) (HR, 0.56; P = .00153) and patients with PD-L1–negative tumors (HR, 0.75; P = .00859).
The lack of a progression-free survival benefit of pembrolizumab over chemotherapy in the initial analysis (HR, 0.98; P = .420) persisted in the updated analysis (HR, 0.96; P = .317).
The overall response rate now was 21.1% with pembrolizumab and 11.0% with chemotherapy. In the former group, the rate of complete response had increased from 7.0% to 9.3% with the longer follow-up. Median time to response was identical, at 2.1 months, but duration of response was longer with pembrolizumab (not reached vs. 4.4 months).
“We haven’t seen any signals of cumulative toxicity with subsequent follow-up,” Dr. Bellmunt reported. Similar to findings of the initial analysis, the most common grade 3-5 treatment-related adverse events were pruritus, fatigue, and diarrhea with pembrolizumab, and neutropenia, anemia, and fatigue with chemotherapy. As expected, the pembrolizumab group had higher rates of hypothyroidism, pneumonitis, hyperthyroidism, and colitis.
“The overall survival benefit and superior safety of pembrolizumab versus chemotherapy in this second-line patient population is maintained after 2 years of follow-up. At 24 months, 27% of patients are alive, and this is similar to what we are seeing with other immune-sensitive diseases like melanoma,” he concluded. “Results in patients with PD-L1–positive or –negative tumors were consistent with the intent-to-treat population. We have seen some hints with this biomarker, but they are not very striking.”
IMvigor 211 trial biomarker analyses
The IMvigor 211 trial enrolled 931 patients with locally advanced or metastatic urothelial carcinoma who had experienced progression during or after platinum-based chemotherapy and had received at most two prior lines of therapy.
At a median follow-up of 17.3 months, the trial did not meet its primary endpoint of significantly better overall survival with atezolizumab versus chemotherapy (vinflunine, docetaxel, or paclitaxel) in patients having PD-L1–positive tumors, defined as immunohistochemical staining of 2 or 3 (HR, 0.87; 95% confidence interval, 0.63-1.21; P = .41) (Lancet. 2018;391:748-57).
Findings were similar in the entire intention-to-treat population (HR, 0.85; 95% CI, 0.73-0.99) and in the subset with tumors having PD-L1–negative tumors, defined as immunohistochemical staining of 0 or 1 (HR, 0.84; 0.71-1.00). In an unexpected finding, PD-L1 positivity was associated with better outcome in both treatment arms.
“So PD-L1 is a classic prognostic, not predictive, biomarker,” commented lead investigator Thomas Powles, MBBS, MRCP, MD, a clinical professor of genitourinary oncology with Barts Health NHS Trust, St. Bartholomew’s Hospital, London. The investigators therefore conducted a series of analyses in the intent-to-treat population to identify predictive biomarkers.
Results were essentially the same with the tumor gene expression 3 (tGE3) signature, an RNA signature that captures expression of the genes encoding interferon gamma, a chemokine ligand, and PD-L1, and that is a marker for preexisting T-cell immunity. And they were also similar with the DNA damage response (DDR) biomarker.
However, a different pattern was seen with tumor mutational burden (TMB), a FoundationOne panel. Patients with TMB-high tumors had a substantial gain in overall survival from atezolizumab versus chemotherapy (HR, 0.68; 95% CI, 0.51-0.90), whereas those with TMB-low tumors did not (HR, 1.00; 95% CI, 0.75-1.32).
“TMB appears to be a predictive but not a prognostic biomarker,” Dr. Powles said. “It’s not perfect. Complete and partial responses and long overall survival were seen in both arms. Nevertheless, it seems like a step in the right direction.”
Finally, with insight on the nature and relationships of the various biomarkers, the investigators assessed the combination of TMB with PD-L1, finding that atezolizumab had a marked overall survival benefit in patients with TMB-high and PD-L1–positive tumors (17.8 vs. 10.6 months; HR, 0.50; 95% CI, 0.29-0.86).
“I think by using combinations of biomarkers, first-generation and second-generation, we may actually be able to better select patients for treatment in the future,” Dr. Powles concluded.
New data, new insights
“We already know the KEYNOTE-045 trial is positive,” commented the invited discussant, Dr. Jones. “This longer follow-up data is important because we need to better describe the magnitude of benefit.”
The updated survival findings are exciting because they resemble those seen with ipilimumab in melanoma, with about a fifth of patients still alive several years out, he said. Longer follow-up is needed, but “the data we see today are in keeping with the possibility that we might be seeing a similar long-term tail – the so-called immuno-oncology tail – of survival for patients with urothelial cancer as well.”
Although not statistically significant, the difference in progression-free survival is clinically important, according to Dr. Jones. This benefit is driven by both higher response rate and longer duration of response with pembrolizumab.
Long-term toxicity, especially immune-related toxicity, is also a consideration. “There is a small increment in the number of some of these toxicities, but essentially it hasn’t changed. So it would appear that there is certainly not an unexpected peak of latent immunotoxicity with this treatment,” he noted.
“Our confidence in the data for second-line pembrolizumab, if it needed to be further increased, is increased. This does help our patients make an informed decision about whether or not to accept this treatment,” he summarized.
Turning to the IMvigor 211 biomarker study, Dr. Jones said, “I would argue that the choice of second-line therapy in advanced urothelial cancer is not a clinically important decision. The reason for saying that is the case for second-line chemotherapy is poor. We’ve all used it, but we’ve never had high level evidence of benefit. … But it’s important because when we consider moving into the first-line setting, where there are active alternatives, or maybe even more into the perioperative setting, it actually could be vitally important.”
Studies of immunotherapies and targeted therapies in other cancers suggest that a clinically useful predictive biomarker will identify patients who will derive at least a doubling of favorable outcome or a halving of unfavorable outcome when given the drug as compared with a control. “So it appears that the bar has been set quite high,” Dr. Jones said.
“These IMvigor 211 data are exploratory, and they would need further independent validation, in my view,” he said. Nevertheless, “this may provide us the opportunity to use combinations of biomarkers where now we are seeing a hazard ratio of 0.50 [for risk of death] combining PD-L1 with high tumor mutational burden (TMB). That hazard ratio is bringing it into the area where it may be of a magnitude big enough to use in clinical practice, if this could be validated.”
“I would say that none of these data support a role for second-line cytotoxics after failure of platinum, at least not in preference to a checkpoint inhibitor,” Dr. Jones concluded. “There is still no biomarker to inform a choice in second-line treatment. However, TMB, either alone or in combination with other markers, shows promise, which we need to validate in future randomized trials.”
SOURCE: Bellmunt J et al. GUC 2018 Abstract 410; Powles T et al. GUC 2018, Abstract 409.
SAN FRANCISCO – Emerging data from phase 3 clinical trials are better clarifying the efficacy and safety of immunotherapy in advanced urothelial cancer and helping identify patients most likely to benefit.
An updated analysis of the KEYNOTE-045 trial showed that, compared with chemotherapy, pembrolizumab (Keytruda), an antibody to programmed death-1 (PD-1), almost doubled the 2-year survival rate in patients with recurrent or advanced urothelial cancer. No cumulative toxicity was seen.
Biomarker analyses from the IMvigor 211 trial showed that, compared with chemotherapy, atezolizumab (Tecentriq), an antibody to programmed cell death ligand 1 (PD-L1), prolonged survival by more than 7 months in patients with platinum-treated locally advanced or metastatic disease whose tumors were positive for this ligand and had a high mutational burden. The difference translated to a halving of the risk of death.
Results of both trials were reported at the 2018 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
“It is clear that PD-1 and PD-L1 targeted immunotherapy now has a role in most patients with advanced urothelial cancer,” Robert J. Jones, MBChB, PhD, professor of clinical cancer research, University of Glasgow, Beatson West of Scotland Cancer Centre, commented in an invited discussion. “It is also true that cytotoxic chemotherapy maintains a role for many, and that both modalities are often ineffective and may be toxic.”
KEYNOTE-045 trial update
Initial results of KEYNOTE-045, at a median follow-up of 14.1 months, provided level I evidence for the safety and efficacy of pembrolizumab over chemotherapy as second-line therapy for recurrent, advanced urothelial cancer (N Engl J Med. 2017;376:1015-26), leading to approval for that indication. (Pembrolizumab is also approved as first-line therapy for cisplatin-ineligible patients).
Lead investigator Joaquim Bellmunt, MD, PhD, an associate professor of medicine at Harvard Medical School and director of the Bladder Cancer Center, Dana-Farber Cancer Institute, both in Boston, reported a trial update, now at a median follow-up of 27.7 months.
Results among 542 patients showed that the initial overall survival benefit of pembrolizumab over chemotherapy (vinflunine, paclitaxel, or docetaxel) (hazard ratio, 0.73; P = .0022) was sustained and in fact now somewhat greater with longer follow-up (HR, 0.70; P = .00017).
Median overall survival was 10.3 months and 7.3 months, respectively. Corresponding 1-year survival rates were 44.4% and 29.8%, and corresponding 2-year survival rates, 27.0% and 14.3%.
At 24 months, 60.6% of patients in the chemotherapy arm had received an immunotherapy agent, including some who had received pembrolizumab as part of crossover, Dr. Bellmunt noted.
Overall survival benefit was generally similar across subgroups, including patients with PD-L1–positive tumors (defined as a combined positive score of 10% or higher) (HR, 0.56; P = .00153) and patients with PD-L1–negative tumors (HR, 0.75; P = .00859).
The lack of a progression-free survival benefit of pembrolizumab over chemotherapy in the initial analysis (HR, 0.98; P = .420) persisted in the updated analysis (HR, 0.96; P = .317).
The overall response rate now was 21.1% with pembrolizumab and 11.0% with chemotherapy. In the former group, the rate of complete response had increased from 7.0% to 9.3% with the longer follow-up. Median time to response was identical, at 2.1 months, but duration of response was longer with pembrolizumab (not reached vs. 4.4 months).
“We haven’t seen any signals of cumulative toxicity with subsequent follow-up,” Dr. Bellmunt reported. Similar to findings of the initial analysis, the most common grade 3-5 treatment-related adverse events were pruritus, fatigue, and diarrhea with pembrolizumab, and neutropenia, anemia, and fatigue with chemotherapy. As expected, the pembrolizumab group had higher rates of hypothyroidism, pneumonitis, hyperthyroidism, and colitis.
“The overall survival benefit and superior safety of pembrolizumab versus chemotherapy in this second-line patient population is maintained after 2 years of follow-up. At 24 months, 27% of patients are alive, and this is similar to what we are seeing with other immune-sensitive diseases like melanoma,” he concluded. “Results in patients with PD-L1–positive or –negative tumors were consistent with the intent-to-treat population. We have seen some hints with this biomarker, but they are not very striking.”
IMvigor 211 trial biomarker analyses
The IMvigor 211 trial enrolled 931 patients with locally advanced or metastatic urothelial carcinoma who had experienced progression during or after platinum-based chemotherapy and had received at most two prior lines of therapy.
At a median follow-up of 17.3 months, the trial did not meet its primary endpoint of significantly better overall survival with atezolizumab versus chemotherapy (vinflunine, docetaxel, or paclitaxel) in patients having PD-L1–positive tumors, defined as immunohistochemical staining of 2 or 3 (HR, 0.87; 95% confidence interval, 0.63-1.21; P = .41) (Lancet. 2018;391:748-57).
Findings were similar in the entire intention-to-treat population (HR, 0.85; 95% CI, 0.73-0.99) and in the subset with tumors having PD-L1–negative tumors, defined as immunohistochemical staining of 0 or 1 (HR, 0.84; 0.71-1.00). In an unexpected finding, PD-L1 positivity was associated with better outcome in both treatment arms.
“So PD-L1 is a classic prognostic, not predictive, biomarker,” commented lead investigator Thomas Powles, MBBS, MRCP, MD, a clinical professor of genitourinary oncology with Barts Health NHS Trust, St. Bartholomew’s Hospital, London. The investigators therefore conducted a series of analyses in the intent-to-treat population to identify predictive biomarkers.
Results were essentially the same with the tumor gene expression 3 (tGE3) signature, an RNA signature that captures expression of the genes encoding interferon gamma, a chemokine ligand, and PD-L1, and that is a marker for preexisting T-cell immunity. And they were also similar with the DNA damage response (DDR) biomarker.
However, a different pattern was seen with tumor mutational burden (TMB), a FoundationOne panel. Patients with TMB-high tumors had a substantial gain in overall survival from atezolizumab versus chemotherapy (HR, 0.68; 95% CI, 0.51-0.90), whereas those with TMB-low tumors did not (HR, 1.00; 95% CI, 0.75-1.32).
“TMB appears to be a predictive but not a prognostic biomarker,” Dr. Powles said. “It’s not perfect. Complete and partial responses and long overall survival were seen in both arms. Nevertheless, it seems like a step in the right direction.”
Finally, with insight on the nature and relationships of the various biomarkers, the investigators assessed the combination of TMB with PD-L1, finding that atezolizumab had a marked overall survival benefit in patients with TMB-high and PD-L1–positive tumors (17.8 vs. 10.6 months; HR, 0.50; 95% CI, 0.29-0.86).
“I think by using combinations of biomarkers, first-generation and second-generation, we may actually be able to better select patients for treatment in the future,” Dr. Powles concluded.
New data, new insights
“We already know the KEYNOTE-045 trial is positive,” commented the invited discussant, Dr. Jones. “This longer follow-up data is important because we need to better describe the magnitude of benefit.”
The updated survival findings are exciting because they resemble those seen with ipilimumab in melanoma, with about a fifth of patients still alive several years out, he said. Longer follow-up is needed, but “the data we see today are in keeping with the possibility that we might be seeing a similar long-term tail – the so-called immuno-oncology tail – of survival for patients with urothelial cancer as well.”
Although not statistically significant, the difference in progression-free survival is clinically important, according to Dr. Jones. This benefit is driven by both higher response rate and longer duration of response with pembrolizumab.
Long-term toxicity, especially immune-related toxicity, is also a consideration. “There is a small increment in the number of some of these toxicities, but essentially it hasn’t changed. So it would appear that there is certainly not an unexpected peak of latent immunotoxicity with this treatment,” he noted.
“Our confidence in the data for second-line pembrolizumab, if it needed to be further increased, is increased. This does help our patients make an informed decision about whether or not to accept this treatment,” he summarized.
Turning to the IMvigor 211 biomarker study, Dr. Jones said, “I would argue that the choice of second-line therapy in advanced urothelial cancer is not a clinically important decision. The reason for saying that is the case for second-line chemotherapy is poor. We’ve all used it, but we’ve never had high level evidence of benefit. … But it’s important because when we consider moving into the first-line setting, where there are active alternatives, or maybe even more into the perioperative setting, it actually could be vitally important.”
Studies of immunotherapies and targeted therapies in other cancers suggest that a clinically useful predictive biomarker will identify patients who will derive at least a doubling of favorable outcome or a halving of unfavorable outcome when given the drug as compared with a control. “So it appears that the bar has been set quite high,” Dr. Jones said.
“These IMvigor 211 data are exploratory, and they would need further independent validation, in my view,” he said. Nevertheless, “this may provide us the opportunity to use combinations of biomarkers where now we are seeing a hazard ratio of 0.50 [for risk of death] combining PD-L1 with high tumor mutational burden (TMB). That hazard ratio is bringing it into the area where it may be of a magnitude big enough to use in clinical practice, if this could be validated.”
“I would say that none of these data support a role for second-line cytotoxics after failure of platinum, at least not in preference to a checkpoint inhibitor,” Dr. Jones concluded. “There is still no biomarker to inform a choice in second-line treatment. However, TMB, either alone or in combination with other markers, shows promise, which we need to validate in future randomized trials.”
SOURCE: Bellmunt J et al. GUC 2018 Abstract 410; Powles T et al. GUC 2018, Abstract 409.
REPORTING FROM GUCS 2018
Key clinical point:
Major finding: Pembrolizumab yielded a higher 2-year rate of survival vs. chemotherapy (27.0% vs. 14.3%). Atezolizumab had a marked survival benefit vs. chemotherapy in patients with TMB-high, PD-L1–positive tumors (17.8 vs. 10.6 months; HR, 0.50).
Data source: Two-year follow-up of a phase 3 randomized trial among 542 patients with recurrent, advanced urothelial cancer (KEYNOTE-045 trial). Biomarker analyses of a phase 3 randomized trial among 931 patients with platinum-treated locally advanced or metastatic urothelial cancer (IMvigor 211 trial).
Disclosures: Dr. Bellmunt disclosed that he has a consulting or advisory role with Astellas Pharma, AstraZeneca/MedImmune, Bristol-Myers Squibb, Genentech, Merck, Novartis, Pfizer, and Pierre Fabre; that his institution receives research funding from Millennium and Sanofi; and that he receives travel, accommodations, and/or expenses from MSD Oncology and Pfizer. KEYNOTE-045 was funded by Merck & Co. Dr. Powles disclosed that he receives honoraria from Bristol-Myers Squibb, Merck, and Roche/Genentech; has a consulting or advisory role with AstraZeneca; Bristol-Myers Squibb, Roche/Genentech, Merck, and Novartis; receives research funding from AstraZeneca/MedImmune and Roche/Genentech; and has another relationship with Bristol-Myers Squibb and Ipsen. IMvigor 211 was sponsored by Hoffmann-La Roche.
Sources: Bellmunt J et al. GUC 2018 Abstract 410; Powles T et al. GUC 2018, Abstract 409.
Easing into laparoscopic colectomy
LAS VEGAS – , including reduced hospital length of stay, less pain, faster return to work, and reduced incidence of adhesive small bowel obstructions. But the methods are underutilized, in part because they can be challenging to learn.
There are some tools and methods that can help surgeons perform surgeries laparoscopically, including hand-assisted laparoscopy and the use of single-incision laparoscopic colectomy (SILC). These methods were the subject of a talk at the Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Between 2009 and 2012, a little over 30% of colon cancer cases in the United States and about half of diverticulitis cases were performed laparoscopically. The percentage of laparoscopic procedures ticked up slightly from 2009 to 2012, but only by a few percentage points. “The fact is, we’re just not doing [minimally invasive procedures],” Ian M. Paquette, MD, FACS, associate professor of surgery at the University of Cincinnati, said during his talk.
When a laparoscopic procedure proves challenging, one option is the hand-assist technique. The literature hasn’t been very supportive of the method, with one study of data from the American College of Surgeons National Surgical Quality Improvement Program showing that it offers no improvement in operation time, compared with standard laparoscopy, and that it has slightly higher complication rates (J Gastrointest Surg. 2016 Nov;20[11]:1854-60). “They say you should do everything laparoscopically,” said Dr. Paquette.
One high-volume surgeon showed what happened over time when his practice employed hand-assisted laparoscopy for diverticulitis cases (Dis Colon Rectum. 2014;57[9]1090-7). Initially, most cases were done with the hand-assist technique. Over time, that percentage dropped precipitously and the number that were performed laparoscopically rose sharply. Throughout the study period, the percentage of open procedures remained very low, dropping to almost zero near the conclusion. “They were able to keep their experience of open surgery quite low by using hand-assisted techniques to help with the tough cases of diverticular disease and get over that learning curve,” said Dr. Paquette.
In colon cancer, the study found that laparoscopic procedures hovered around 50%, while open and hand-assisted techniques tended to be around 20%. The higher incidence of open procedures was probably due to the desire of surgeons to be certain that the entire tumor has been excised. “If you’re in doubt, you don’t compromise on oncology. You do an open procedure if you need to,” said Dr. Paquette.
Another tool available to surgeons is single-incision laparoscopic colectomy, as opposed to conventional multiport laparoscopic colectomy. The method results in a very small incision, but can be challenging because the instruments are closer together and it is tricky when the surgeon has to cross the instrument, he said.
Dr. Paquette’s own group also looked at extraction in hand-assisted sigmoid colectomy, in which the surgeon went in laparoscopically, mobilized the colon laterally as would be done in an open procedure, and then performed the colectomy through a small extraction incision. The length of stay was about 15% shorter, there was a lower readmission rate, and gastrointestinal function returned more quickly (Surg Endosc. 2016 Aug;30[8]:3567-72).
Can patients who previously underwent a midline laparotomy be treated laparoscopically? “The answer is possibly yes,” said Dr. Paquette. He noted one study that showed higher rates of minor morbidity, ileotomy, and longer length of stay with laparoscopic treatment (Surg Endosc. 2015;29[3]537-42). “It’s a worth a try if you carefully plan where you’re going to go in through your ports, get in off the midline somewhere if you have to, and just take a look. If you have some adhesions of the omentum to the abdominal wall, it’s really no problem and you can proceed. If you have a frozen abdomen, just do the right thing and open the patient,” said Dr. Paquette.
When it comes to extraction options, Pfannenstiel incisions have the lowest rates of incisional hernias, at 1.9%, according to a survey of 2,148 cases at the Cleveland Clinic. The periumbilical midline incision had the highest frequency at 16.2% (Dis Colon Rectum. 2016 Aug;59[8]:743-50).
“If I’m doing a laparoscopic sigmoid or a laparoscopic low anterior, I do prefer to do a Pfannenstiel incision if I can. If you think that you may need to convert that patient for some reason, don’t do the Pfannenstiel first – nobody wants that big T-shaped incision,” said Dr. Paquette.
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Paquette has consulted for Ethicon.
LAS VEGAS – , including reduced hospital length of stay, less pain, faster return to work, and reduced incidence of adhesive small bowel obstructions. But the methods are underutilized, in part because they can be challenging to learn.
There are some tools and methods that can help surgeons perform surgeries laparoscopically, including hand-assisted laparoscopy and the use of single-incision laparoscopic colectomy (SILC). These methods were the subject of a talk at the Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Between 2009 and 2012, a little over 30% of colon cancer cases in the United States and about half of diverticulitis cases were performed laparoscopically. The percentage of laparoscopic procedures ticked up slightly from 2009 to 2012, but only by a few percentage points. “The fact is, we’re just not doing [minimally invasive procedures],” Ian M. Paquette, MD, FACS, associate professor of surgery at the University of Cincinnati, said during his talk.
When a laparoscopic procedure proves challenging, one option is the hand-assist technique. The literature hasn’t been very supportive of the method, with one study of data from the American College of Surgeons National Surgical Quality Improvement Program showing that it offers no improvement in operation time, compared with standard laparoscopy, and that it has slightly higher complication rates (J Gastrointest Surg. 2016 Nov;20[11]:1854-60). “They say you should do everything laparoscopically,” said Dr. Paquette.
One high-volume surgeon showed what happened over time when his practice employed hand-assisted laparoscopy for diverticulitis cases (Dis Colon Rectum. 2014;57[9]1090-7). Initially, most cases were done with the hand-assist technique. Over time, that percentage dropped precipitously and the number that were performed laparoscopically rose sharply. Throughout the study period, the percentage of open procedures remained very low, dropping to almost zero near the conclusion. “They were able to keep their experience of open surgery quite low by using hand-assisted techniques to help with the tough cases of diverticular disease and get over that learning curve,” said Dr. Paquette.
In colon cancer, the study found that laparoscopic procedures hovered around 50%, while open and hand-assisted techniques tended to be around 20%. The higher incidence of open procedures was probably due to the desire of surgeons to be certain that the entire tumor has been excised. “If you’re in doubt, you don’t compromise on oncology. You do an open procedure if you need to,” said Dr. Paquette.
Another tool available to surgeons is single-incision laparoscopic colectomy, as opposed to conventional multiport laparoscopic colectomy. The method results in a very small incision, but can be challenging because the instruments are closer together and it is tricky when the surgeon has to cross the instrument, he said.
Dr. Paquette’s own group also looked at extraction in hand-assisted sigmoid colectomy, in which the surgeon went in laparoscopically, mobilized the colon laterally as would be done in an open procedure, and then performed the colectomy through a small extraction incision. The length of stay was about 15% shorter, there was a lower readmission rate, and gastrointestinal function returned more quickly (Surg Endosc. 2016 Aug;30[8]:3567-72).
Can patients who previously underwent a midline laparotomy be treated laparoscopically? “The answer is possibly yes,” said Dr. Paquette. He noted one study that showed higher rates of minor morbidity, ileotomy, and longer length of stay with laparoscopic treatment (Surg Endosc. 2015;29[3]537-42). “It’s a worth a try if you carefully plan where you’re going to go in through your ports, get in off the midline somewhere if you have to, and just take a look. If you have some adhesions of the omentum to the abdominal wall, it’s really no problem and you can proceed. If you have a frozen abdomen, just do the right thing and open the patient,” said Dr. Paquette.
When it comes to extraction options, Pfannenstiel incisions have the lowest rates of incisional hernias, at 1.9%, according to a survey of 2,148 cases at the Cleveland Clinic. The periumbilical midline incision had the highest frequency at 16.2% (Dis Colon Rectum. 2016 Aug;59[8]:743-50).
“If I’m doing a laparoscopic sigmoid or a laparoscopic low anterior, I do prefer to do a Pfannenstiel incision if I can. If you think that you may need to convert that patient for some reason, don’t do the Pfannenstiel first – nobody wants that big T-shaped incision,” said Dr. Paquette.
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Paquette has consulted for Ethicon.
LAS VEGAS – , including reduced hospital length of stay, less pain, faster return to work, and reduced incidence of adhesive small bowel obstructions. But the methods are underutilized, in part because they can be challenging to learn.
There are some tools and methods that can help surgeons perform surgeries laparoscopically, including hand-assisted laparoscopy and the use of single-incision laparoscopic colectomy (SILC). These methods were the subject of a talk at the Annual Minimally Invasive Surgery Symposium by Global Academy for Medical Education.
Between 2009 and 2012, a little over 30% of colon cancer cases in the United States and about half of diverticulitis cases were performed laparoscopically. The percentage of laparoscopic procedures ticked up slightly from 2009 to 2012, but only by a few percentage points. “The fact is, we’re just not doing [minimally invasive procedures],” Ian M. Paquette, MD, FACS, associate professor of surgery at the University of Cincinnati, said during his talk.
When a laparoscopic procedure proves challenging, one option is the hand-assist technique. The literature hasn’t been very supportive of the method, with one study of data from the American College of Surgeons National Surgical Quality Improvement Program showing that it offers no improvement in operation time, compared with standard laparoscopy, and that it has slightly higher complication rates (J Gastrointest Surg. 2016 Nov;20[11]:1854-60). “They say you should do everything laparoscopically,” said Dr. Paquette.
One high-volume surgeon showed what happened over time when his practice employed hand-assisted laparoscopy for diverticulitis cases (Dis Colon Rectum. 2014;57[9]1090-7). Initially, most cases were done with the hand-assist technique. Over time, that percentage dropped precipitously and the number that were performed laparoscopically rose sharply. Throughout the study period, the percentage of open procedures remained very low, dropping to almost zero near the conclusion. “They were able to keep their experience of open surgery quite low by using hand-assisted techniques to help with the tough cases of diverticular disease and get over that learning curve,” said Dr. Paquette.
In colon cancer, the study found that laparoscopic procedures hovered around 50%, while open and hand-assisted techniques tended to be around 20%. The higher incidence of open procedures was probably due to the desire of surgeons to be certain that the entire tumor has been excised. “If you’re in doubt, you don’t compromise on oncology. You do an open procedure if you need to,” said Dr. Paquette.
Another tool available to surgeons is single-incision laparoscopic colectomy, as opposed to conventional multiport laparoscopic colectomy. The method results in a very small incision, but can be challenging because the instruments are closer together and it is tricky when the surgeon has to cross the instrument, he said.
Dr. Paquette’s own group also looked at extraction in hand-assisted sigmoid colectomy, in which the surgeon went in laparoscopically, mobilized the colon laterally as would be done in an open procedure, and then performed the colectomy through a small extraction incision. The length of stay was about 15% shorter, there was a lower readmission rate, and gastrointestinal function returned more quickly (Surg Endosc. 2016 Aug;30[8]:3567-72).
Can patients who previously underwent a midline laparotomy be treated laparoscopically? “The answer is possibly yes,” said Dr. Paquette. He noted one study that showed higher rates of minor morbidity, ileotomy, and longer length of stay with laparoscopic treatment (Surg Endosc. 2015;29[3]537-42). “It’s a worth a try if you carefully plan where you’re going to go in through your ports, get in off the midline somewhere if you have to, and just take a look. If you have some adhesions of the omentum to the abdominal wall, it’s really no problem and you can proceed. If you have a frozen abdomen, just do the right thing and open the patient,” said Dr. Paquette.
When it comes to extraction options, Pfannenstiel incisions have the lowest rates of incisional hernias, at 1.9%, according to a survey of 2,148 cases at the Cleveland Clinic. The periumbilical midline incision had the highest frequency at 16.2% (Dis Colon Rectum. 2016 Aug;59[8]:743-50).
“If I’m doing a laparoscopic sigmoid or a laparoscopic low anterior, I do prefer to do a Pfannenstiel incision if I can. If you think that you may need to convert that patient for some reason, don’t do the Pfannenstiel first – nobody wants that big T-shaped incision,” said Dr. Paquette.
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Paquette has consulted for Ethicon.
REPORTING FROM MISS

Olopatadine/mometasone combo is safe and effective
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point: Twice-daily combination therapy improved reflective total nasal symptom scores better than either component alone.
Major finding: Combination therapy significantly improved total nasal symptom scores (P less than .001).
Study details: Phase 3, double-blind, randomized, parallel-group study of 1,180 patients aged 12 years and older with seasonal allergic rhinitis.
Disclosures: Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies.
Source: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
Tofacitinib: FDA panel recommends ulcerative colitis indication
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study; two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2); a 53-week, phase 3 maintenance trial (OCTAVE Sustain); and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.
Patients who did not achieve remission but showed some clinical response (decrease in Mayo score of at least 3 points) were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5-mg and 10-mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior tumor necrosis factor–blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks, as part of an open-label extension study. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated patients, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection, “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair Jean-Pierre Raufman, MD, and vice chair Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
Visit www.gastro.org/IBD for patient education guides that you can share with your ulcerative colitis patients.
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study; two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2); a 53-week, phase 3 maintenance trial (OCTAVE Sustain); and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.
Patients who did not achieve remission but showed some clinical response (decrease in Mayo score of at least 3 points) were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5-mg and 10-mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior tumor necrosis factor–blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks, as part of an open-label extension study. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated patients, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection, “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair Jean-Pierre Raufman, MD, and vice chair Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
Visit www.gastro.org/IBD for patient education guides that you can share with your ulcerative colitis patients.
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study; two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2); a 53-week, phase 3 maintenance trial (OCTAVE Sustain); and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.
Patients who did not achieve remission but showed some clinical response (decrease in Mayo score of at least 3 points) were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5-mg and 10-mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior tumor necrosis factor–blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks, as part of an open-label extension study. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated patients, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection, “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair Jean-Pierre Raufman, MD, and vice chair Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
Visit www.gastro.org/IBD for patient education guides that you can share with your ulcerative colitis patients.
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING
Beware the con
As I stepped from an exam room one recent busy morning, my office manager pulled me aside. “Someone from the county courthouse is on the phone and needs to talk to you,” she whispered.
“You know better than that,” I said. “While I’m seeing patients, I don’t take calls from anyone except colleagues and immediate family.”
I took the call.
“You failed to appear for jury duty,” the official-sounding voice said. “That’s a violation of state law, as you were warned when you received your summons. You’ll have to come down here and surrender yourself immediately, or else we’ll have to send deputies to your office. I don’t think you’ll want to be led through your waiting room in handcuffs.”
“Wait a minute,” I replied nervously. “I haven’t received a jury summons for 2 years, at least. There must be some mistake.”
“Perhaps we’ve confused you with a citizen with the same or a similar name,” he said. “Let me have your Social Security number and birth date.”
Alarm bells! “You should have that information already,” I replied. “Why don’t you read me what you have?”
A short silence, and then … click.
I immediately called the courthouse. “Citizens who fail to appear receive a warning letter and a new questionnaire, not a phone call,” said the jury manager. “And we use driver license numbers to keep track of jurors.”
The phone company traced the call, which dead-ended at a VoIP circuit, to no one’s surprise. The downside of VoIP (Voice over Internet Protocol) and similar technologies is that unscrupulous individuals can use them to appear to be calling you from a legitimate business when they are not.
Those of us of a certain age remember phony office calls offering great deals on supplies or waiting room magazine subscriptions. Those capers eventually disappeared; but scam artists are endlessly creative. This is especially true since the Internet took over, well, everything. There’s a real dark side to the information age.
The jury duty scheme, I learned, is an increasingly popular one. Others involve calls or e-mails from the “fraud department” of your bank, claiming to be investigating a breach of your account, or one of your credit or debit cards. Another purports to be a “Customs official” informing you that you owe a big duty payment on an overseas shipment. Victims of power outages due to natural disasters are hearing from crooks claiming to be from the local power company; the power won’t be restored, they say, without an advance payment.
In most cases, the common denominator – and the biggest red flag – is a request for a social security number, a birth date, a credit card number, or other private information that could be used to steal your identity or empty your accounts.

Here’s a summary of what my recent experience taught (or reminded) me:
- Never give out a bank account, social security, or credit card number online or over the telephone if you didn’t initiate the contact, no matter how legitimate the caller sounds. This is true of anyone claiming to be from a bank, a service company, or a government office, as well as anyone trying to sell you anything.
- No federal or state court will call to say you’ve missed jury duty – or that they are assembling jury pools and need to “prescreen” those who might be selected to serve on them. The jury manager I spoke with said she knew of no reason why anyone in my state would ever be called about jury service before mailing back a completed questionnaire, and even then, such a call would be extraordinary.
- Never send anyone a “commission” or “finder’s fee” as a condition of receiving funds. In legitimate transactions, such fees are merely deducted from the money being paid out.
- Examine your credit card and bank account statements each month. Immediately challenge any charges you don’t recognize.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
As I stepped from an exam room one recent busy morning, my office manager pulled me aside. “Someone from the county courthouse is on the phone and needs to talk to you,” she whispered.
“You know better than that,” I said. “While I’m seeing patients, I don’t take calls from anyone except colleagues and immediate family.”
I took the call.
“You failed to appear for jury duty,” the official-sounding voice said. “That’s a violation of state law, as you were warned when you received your summons. You’ll have to come down here and surrender yourself immediately, or else we’ll have to send deputies to your office. I don’t think you’ll want to be led through your waiting room in handcuffs.”
“Wait a minute,” I replied nervously. “I haven’t received a jury summons for 2 years, at least. There must be some mistake.”
“Perhaps we’ve confused you with a citizen with the same or a similar name,” he said. “Let me have your Social Security number and birth date.”
Alarm bells! “You should have that information already,” I replied. “Why don’t you read me what you have?”
A short silence, and then … click.
I immediately called the courthouse. “Citizens who fail to appear receive a warning letter and a new questionnaire, not a phone call,” said the jury manager. “And we use driver license numbers to keep track of jurors.”
The phone company traced the call, which dead-ended at a VoIP circuit, to no one’s surprise. The downside of VoIP (Voice over Internet Protocol) and similar technologies is that unscrupulous individuals can use them to appear to be calling you from a legitimate business when they are not.
Those of us of a certain age remember phony office calls offering great deals on supplies or waiting room magazine subscriptions. Those capers eventually disappeared; but scam artists are endlessly creative. This is especially true since the Internet took over, well, everything. There’s a real dark side to the information age.
The jury duty scheme, I learned, is an increasingly popular one. Others involve calls or e-mails from the “fraud department” of your bank, claiming to be investigating a breach of your account, or one of your credit or debit cards. Another purports to be a “Customs official” informing you that you owe a big duty payment on an overseas shipment. Victims of power outages due to natural disasters are hearing from crooks claiming to be from the local power company; the power won’t be restored, they say, without an advance payment.
In most cases, the common denominator – and the biggest red flag – is a request for a social security number, a birth date, a credit card number, or other private information that could be used to steal your identity or empty your accounts.
Here’s a summary of what my recent experience taught (or reminded) me:
- Never give out a bank account, social security, or credit card number online or over the telephone if you didn’t initiate the contact, no matter how legitimate the caller sounds. This is true of anyone claiming to be from a bank, a service company, or a government office, as well as anyone trying to sell you anything.
- No federal or state court will call to say you’ve missed jury duty – or that they are assembling jury pools and need to “prescreen” those who might be selected to serve on them. The jury manager I spoke with said she knew of no reason why anyone in my state would ever be called about jury service before mailing back a completed questionnaire, and even then, such a call would be extraordinary.
- Never send anyone a “commission” or “finder’s fee” as a condition of receiving funds. In legitimate transactions, such fees are merely deducted from the money being paid out.
- Examine your credit card and bank account statements each month. Immediately challenge any charges you don’t recognize.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
As I stepped from an exam room one recent busy morning, my office manager pulled me aside. “Someone from the county courthouse is on the phone and needs to talk to you,” she whispered.
“You know better than that,” I said. “While I’m seeing patients, I don’t take calls from anyone except colleagues and immediate family.”
I took the call.
“You failed to appear for jury duty,” the official-sounding voice said. “That’s a violation of state law, as you were warned when you received your summons. You’ll have to come down here and surrender yourself immediately, or else we’ll have to send deputies to your office. I don’t think you’ll want to be led through your waiting room in handcuffs.”
“Wait a minute,” I replied nervously. “I haven’t received a jury summons for 2 years, at least. There must be some mistake.”
“Perhaps we’ve confused you with a citizen with the same or a similar name,” he said. “Let me have your Social Security number and birth date.”
Alarm bells! “You should have that information already,” I replied. “Why don’t you read me what you have?”
A short silence, and then … click.
I immediately called the courthouse. “Citizens who fail to appear receive a warning letter and a new questionnaire, not a phone call,” said the jury manager. “And we use driver license numbers to keep track of jurors.”
The phone company traced the call, which dead-ended at a VoIP circuit, to no one’s surprise. The downside of VoIP (Voice over Internet Protocol) and similar technologies is that unscrupulous individuals can use them to appear to be calling you from a legitimate business when they are not.
Those of us of a certain age remember phony office calls offering great deals on supplies or waiting room magazine subscriptions. Those capers eventually disappeared; but scam artists are endlessly creative. This is especially true since the Internet took over, well, everything. There’s a real dark side to the information age.
The jury duty scheme, I learned, is an increasingly popular one. Others involve calls or e-mails from the “fraud department” of your bank, claiming to be investigating a breach of your account, or one of your credit or debit cards. Another purports to be a “Customs official” informing you that you owe a big duty payment on an overseas shipment. Victims of power outages due to natural disasters are hearing from crooks claiming to be from the local power company; the power won’t be restored, they say, without an advance payment.
In most cases, the common denominator – and the biggest red flag – is a request for a social security number, a birth date, a credit card number, or other private information that could be used to steal your identity or empty your accounts.
Here’s a summary of what my recent experience taught (or reminded) me:
- Never give out a bank account, social security, or credit card number online or over the telephone if you didn’t initiate the contact, no matter how legitimate the caller sounds. This is true of anyone claiming to be from a bank, a service company, or a government office, as well as anyone trying to sell you anything.
- No federal or state court will call to say you’ve missed jury duty – or that they are assembling jury pools and need to “prescreen” those who might be selected to serve on them. The jury manager I spoke with said she knew of no reason why anyone in my state would ever be called about jury service before mailing back a completed questionnaire, and even then, such a call would be extraordinary.
- Never send anyone a “commission” or “finder’s fee” as a condition of receiving funds. In legitimate transactions, such fees are merely deducted from the money being paid out.
- Examine your credit card and bank account statements each month. Immediately challenge any charges you don’t recognize.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
Jump-starting the day
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”

The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”
The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”
The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
MDedge Daily News: Why the barber’s chair can help hypertension
Why the barber’s chair can help hypertension, how family history affects colorectal cancer risk, a steroid shot could ease hip osteoarthritis pain, and why excessive daytime sleepiness could lead to dementia.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
Why the barber’s chair can help hypertension, how family history affects colorectal cancer risk, a steroid shot could ease hip osteoarthritis pain, and why excessive daytime sleepiness could lead to dementia.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
Why the barber’s chair can help hypertension, how family history affects colorectal cancer risk, a steroid shot could ease hip osteoarthritis pain, and why excessive daytime sleepiness could lead to dementia.
Listen to the MDedge Daily News podcast for all the details on today’s top news.

Incidence and Management of Asymptomatic Hypertensive Urgency at a VA Emergency Department
Hypertension affects more than 65 million individuals in the U.S., accounting for nearly 30% of the adult population.1 Less than 50% of those with hypertension are taking appropriate pharmacotherapy.2 Hypertension contributes to cardiovascular events, including cerebrovascular accident, transient ischemic attack, hypertensive retinopathy, renal failure, myocardial infarction, and heart failure.1 Chronic hypertension mainly is an asymptomatic condition, earning the nickname “the silent killer.”2 An acute, symptomatic elevation in blood pressure (BP) often is referred to as hypertensive emergency. Symptoms of end-organ damage can include headache, blurry vision, chest pain, shortness of breath, altered mental status, epistaxis, and oliguria.2 Although rare, hypertensive emergencies should be treated immediately. The Seventh Report of the Joint National Committee (JNC 7), and the more recent JNC 8, have published guidelines on managing chronic hypertension.3,4 However, neither report provides guidance on hypertensive emergency or the appropriate actions in cases of extremely elevated BP in an asymptomatic patient.3,4
Acute hypertensive episodes—often referred to as hypertensive crises—are responsible for nearly 8 million hospitalizations each year and 20 million visits to the emergency department (ED).5,6 Most of these visits are same-day “treat-and-release” events.5 There is no universally accepted BP value associated with a hypertensive crisis, but most resources state that a BP ≥ 180/110 mm Hg requires attention.2,7 Without other symptoms, elevated BP is not an emergency, yet ED referral for acute management is common.7
Three terms fall under the umbrella of hypertensive crises: hypertensive emergency, hypertensive urgency, and asymptomatic hypertension (AH).2 In a 2007 article, the American College of Chest Physicians defined hypertensive emergency as BP ≥ 180/110 mm Hg with evidence of end-organ damage.2 Symptoms are almost always present in true hypertensive emergencies, and immediate medical intervention is required to halt further organ damage. In the same article, hypertensive urgency is defined as BP ≥ 180/110 mm Hg without end-organ damage.2 The definition of hypertensive urgency could be further refined to include the presence of cardiovascular and renal risk factors, although this additional point is not consistent across the literature. Asymptomatic hypertension is similar to hypertensive urgency; however, there is an absence of signs or symptoms of end-organ damage.2 There is ambiguity in the literature concerning managing hypertensive urgency and AH, but both share a basic tenet: Immediate BP reduction is not essential. Gradual dosage adjustment(s) of oral medications, preferably by a primary care provider (PCP), and follow-up within 7 days are recommended.7
Limited evidence exists to guide ED providers in managing AH. Long-term outcomes and guidelines intended for the primary care setting should not be extrapolated to acute management in the ED. With limited treatment guidelines, providers might be more likely to refer patients with AH to the ED for evaluation. In 2013, the American College of Emergency Physicians (ACEP) created a clinical policy concerning AH in the ED. The ACEP concluded that screening for target organ injury and medical intervention in the ED does not reduce rates of adverse events (AEs) and could lead to overtreatment and acute hypoperfusion.7 More recently, Patel and colleagues published findings on hypertensive urgency in the ambulatory care setting, which similarly found that referral to the ED was associated with increased use of health care resources and no change in short-term major AEs.8 The ACEP recommends that patients presenting with AH be referred to primary care clinics where long-term monitoring and medication adjustments can be achieved more cost-effectively.7
The objective of this retrospective evaluation was to assess the incidence and management of AH within a VA ED. The authors aimed to provide insight into how these patients are managed and discuss alternatives to ED use.
Methods
This retrospective observational study was conducted within the North Florida/South Georgia Veterans Health System (NFSGVHS), which provides patient care at 2 medical centers in Gainesville and Lake City, Florida, as well as 11 outpatient clinics located throughout North Florida and South Georgia. The NFSGVHS serves rural and urban veteran populations. Study approval was granted by the NFSGVHS Institutional Review Board and Research and Development Committee.
Inclusion/Exclusion Criteria
Adult patients who were ordered at least 1 antihypertensive medication in the ED from July 1, 2011 to July 1, 2014, in addition to being asymptomatic with BP ≥ 180/110 mm Hg at ED triage were included. Based on clinical experience, the authors estimated that 3 years would provide a sample size of more than 100 patients. Patients were excluded if they presented with any acute symptoms or were hospitalized for further management.
Data Collection
Baseline demographics were collected for all participants. During the ED encounter, pre- and postintervention vital signs were recorded and prespecified laboratory data obtained. Interrater reliability was accounted for by performing random reviews of previously collected data to ensure consistency during the chart review process. Renal end-organ damage was defined using Acute Kidney Injury Network criteria, a serum creatinine 50% above baseline, or an absolute increase in baseline serum creatinine by 0.3 mg/dL.9 Additional laboratory markers of organ damage included cardiac troponin levels. Urinalysis results also were assessed to determine the presence of hematuria or proteinuria. Patient-reported nonadherence with medications was determined by reviewing ED provider and/or nurse documentation notes for the index ED encounter.
Investigators documented the route (IV or oral) and antihypertensive(s) medication selected for each patient. Adverse effects and any changes to patients’ outpatient medication regimens were noted. Investigators also assessed days to next medical contact after ED discharge to determine whether follow-up occurred according to the recommended standard of 7 days.9 Days to next medical contact was defined as any contact—in person or by telephone—that was documented in the electronic health record after the index ED visit.
Statistical Analysis
Descriptive statistics, including mean, median, and standard deviation, were used to analyze data.
Results
A total of 1,052 patients presented with BP ≥ 180/110 mm Hg and for whom antihypertensive medication was ordered but not necessarily given in the ED. Of the total, 724 patients were excluded because of hospital admission for other primary diagnoses; however, 6 of these patients were admitted for hypertensive urgency. The final analysis included 132 patients who presented with the primary condition of elevated BP without any accompanying symptoms. Among these patients, 2 had repeat ED visits for AH during the specified time frame. 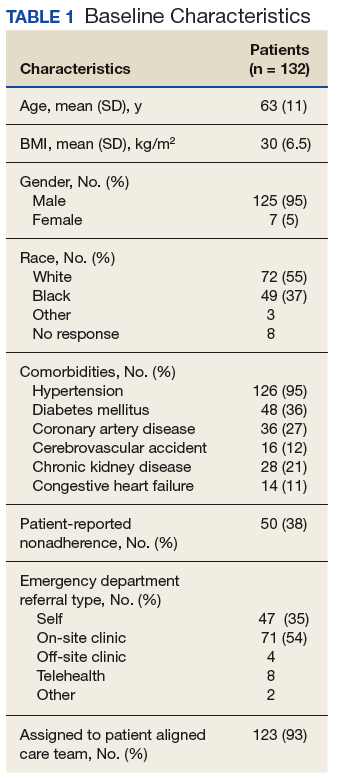
Most patients were male with an average age of 63 years and documented history of hypertension. Nearly all patients had established primary care within the NFSGVHS. The most common comorbidity was diabetes mellitus (36%), followed by coronary artery disease (27%) and chronic kidney disease (CKD) (21%) (Table 1). About one-third of patients presented to the ED on their own volition, and slightly more than half were referred to the ED by primary care or specialty clinics. 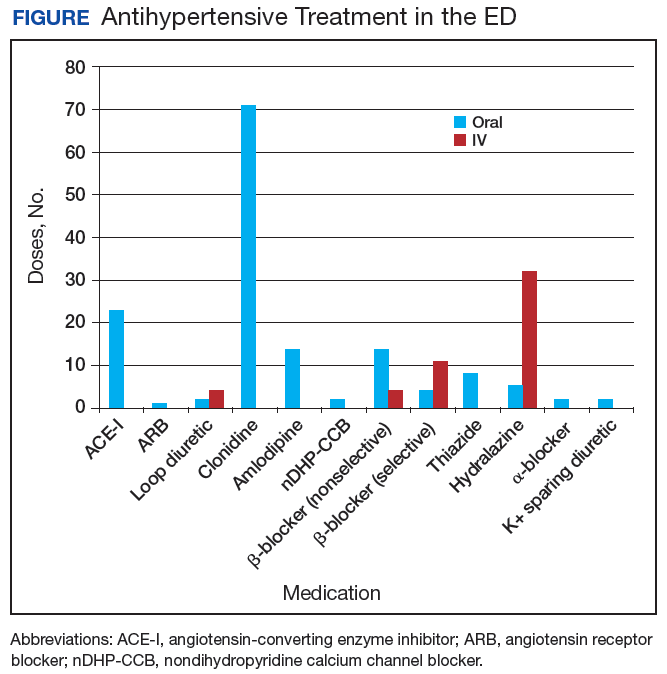
In the ED, 130 patients received BP treatment (Table 2). Medication was ordered for 2 patients who did not receive treatment. In total, 12 different medication classes were used for treating patients with AH in the ED (Figure). 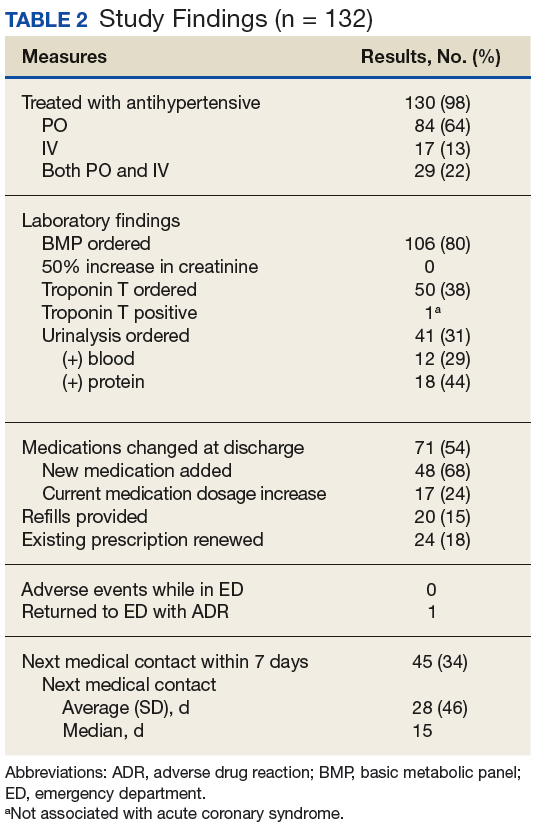
Treatment in the ED resulted in an average BP and heart rate reduction of 27/20 mm Hg and 5 beats per minute, respectively. About 80% of patients had a basic metabolic panel drawn, and there were no instances of acute kidney injury. Of the patients in the study 38% had cardiac enzymes collected, and only 1 patient had a positive result, which was determined to be unrelated to acute coronary syndrome. Forty-one (31%) of patients had a urinalysis; 12 has positive results for hematuria, and 18 revealed proteinuria. Of note, the 6 patients who were hospitalized for hypertensive urgency had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. The reason these patients were admitted is unclear.
At discharge, ED providers made changes to 54% of patients’ outpatient antihypertensive regimens. These changes included adding a new medication (68%), increasing the dosage of an existing medication (24%), or multiple changes (8%). Refills were provided for 18% of prescriptions. Follow-up within 7 days from ED discharge was recorded for 34% of patients. One patient received follow-up outside the NFSGVHS and was not included in this analysis.
Discussion
The aim of this retrospective study was to determine the incidence of AH in a VA ED and describe how these patients were managed. Overall, the rate of patients presenting to the ED with AH during the study period was about 1 patient every 8 days or 45 patients per year. By comparison, more than 30,000 patients are seen at the NFSGVHS ED annually. Although AH seems to be an uncommon occurrence, study findings raise questions about the value of managing the condition in the ED.
This study found several management strategies as well as noteworthy trends. For example, laboratory tests were not ordered routinely for all patients, suggesting that some ED providers question their use for AH. There were no patients with acute elevations in serum creatinine that indicated acute kidney injury, and although hematuria and proteinuria were common findings, neither were specific for acute injury. However, there were findings typical of chronic hypertension, and urinalysis may provide little benefit when testing for acute kidney injury. Only 1 patient showed elevated cardiac enzymes, which was determined to be a result of CKD.
Although not included in the final analysis, the 6 patients who were hospitalized for hypertensive urgency were similar in that they had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. Collectively, these findings support existing literature that questions the utility of laboratory testing of patients with AH in the ED.10
Patients also were treated with a variety of antihypertensive agents in the ED. One explanation might be outpatient nonadherence with medications. In patients with AH, it is common to provide doses of chronic medications that the patient might have missed and should be taking on a regular basis. Therefore, assessing adherence with current medications before modifying chronic therapy is an important initial step when managing AH.
Although oral agents primarily were used, IV antihypertensives were administered to about one-third of patients. Preference for IV administration in the ED might be related to its ability to lower BP quickly. The practice of obtaining IV access for medication in a patient with AH is costly, unnecessary, and potentially harmful.7 The authors theorize that this practice is performed, in many cases, as an attempt to expedite ED discharge after an acceptable BP reading is documented.
Rapid reductions in BP can precipitate hypoperfusion inadvertently and are more likely to occur with IV agents than with oral ones. Therefore, the safety, convenience, and cost savings associated with oral administration make it the preferred route for managing AH. 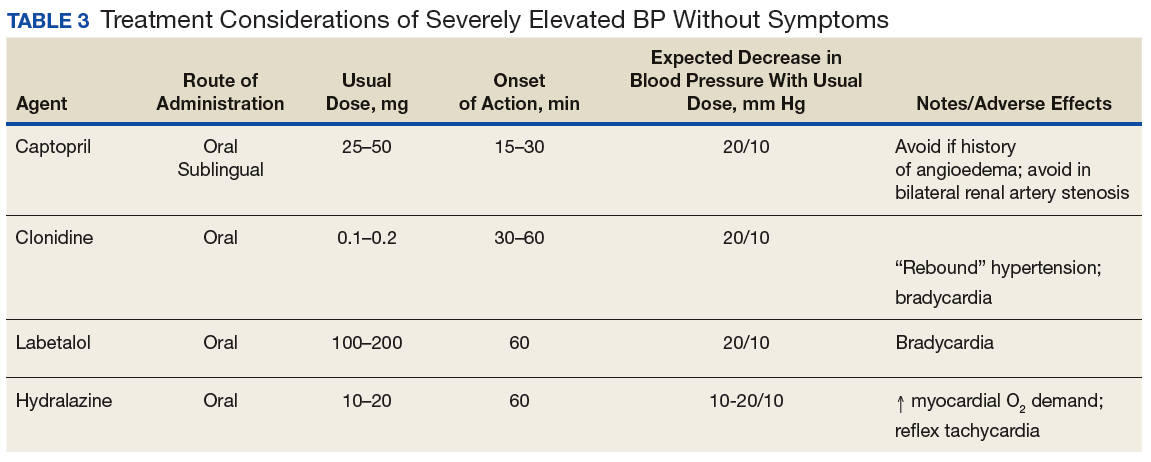
Best Practices
Primary care clinics are best suited to manage AH because medication adjustments and long-term monitoring are easier to perform and at substantially lower costs when compared with that of the ED. Rather than immediately referring a patient to the ED, clinicians should consider factors that could elevate BP, such as medication nonadherence, anxiety, acute pain, recent tobacco or caffeine use, or white coat syndrome. Staff should be well educated on proper BP measurement and instructed to repeat the reading for confirmation. Before measuring BP, allow the patient to sit quietly for 5 minutes with the feet flat on the floor and arm supported.3 Ideally, the measurement used should be the average of 3 BP readings on an automated device.11 If BP readings are high, staff should ask the patient about medication adherence and missed medication(s) should be administered.
It also is reasonable to have the patient rest quietly for up to 30 minutes because rest has been shown to reduce BP in some patients.12 The drawback to the prolonged rest strategy is the potential to cause delays in care for other patients. However, it is important to remember that wait times in the ED often are measured in hours, which causes frustration for patients referred to the ED for AH management. Before completing the office visit, the provider should recheck BP using proper technique and confirm that the patient has antihypertensive medication(s) in his/her possession; a follow-up appointment should be scheduled for no later than 1 week.
Primary care providers might be concerned about taking on additional liability and could favor ED referral, but legislation makes it difficult for EDs to defer nonemergent issues to primary care clinics. The Emergency Medical Treatment and Labor Act states that hospitals are prohibited from denying a patient care during an emergency.13 Despite evidence that AH is not an emergency, many patients continue to be referred to the ED. One-third of patients presented to the ED on their own volition and more than one-half were referred by health care personnel. This strongly suggests that both patients and health care personnel consider AH an emergency medical condition requiring immediate attention. However, patients with AH rarely are found to have any acute end-organ damage; therefore, acute treatment and extensive laboratory or diagnostic testing in the ED provides little, if any, benefit.10 The authors believe the ACEP clinical policy should be adopted into mainstream practice to help reduce health care costs and preserve ED resources for patients with true emergencies.
Another pervasive issue that could contribute to inappropriate AH referrals to the ED is the shortage of PCPs and limited same-day appointments for nonemergent conditions. In a 2017 survey, the average wait time for a PCP appointment ranged between 12 and 109 days, depending on the metropolitan area. The national average wait time conducted by this survey was 29.3 days.14 When primary care appointments are unavailable, triage staff could recommend that patients seek care in the ED. Additionally, patients might choose to seek ED care rather than wait for the next available PCP appointment. Clinic proximity to an ED could influence referral rates. In other words, medical centers or health systems with primary care clinics and ED services under one roof could experience more frequent ED referrals.
A promising strategy to help overcome the challenges of addressing AH and avoiding ED referrals is increasing patient access to and use of qualified, nonphysician providers, such as clinical pharmacists and nurse practitioners. Large health systems such as the VA and Kaiser Permanente have employed clinical pharmacist providers to reduce follow-up times for patients in primary care settings.15 Furthermore, there is substantial evidence that supports the cost-effectiveness and clinical success of pharmacist-driven hypertension clinics.16-18 Nurse-driven efforts to improve hypertension control have been successfully implemented in health systems.19 Both clinical pharmacist and nurse-managed hypertension clinics are effective solutions to manage patients with AH who might otherwise use costly ED services.For example, the average cost of a single ED visit is $740 to $3,437.20 In comparison, a 2010 report from the Agency for Healthcare Research and Quality showed the average annual cost of managing hypertension in ambulatory care clinics was $442 per adult, a cost considerably lower than that of the ED.21
Limitations
The retrospective and observational design of this study are inherent limitations. This study was not designed to evaluate cardiovascular outcomes after ED encounters. The sample size could have been larger if patients with BP < 180/110 mm Hg at ED triage were included; however, the 180/110 mm Hg threshold was chosen because it was the most widely agreed on BP value in the literature. This study did not capture patients who presented with AH and did not receive any acute treatment in the ED.Prescribing patterns based on provider training (eg, emergency medicine, family medicine, or internal medicine) were not tracked and might have accounted for differences in selection of diagnostic tests, laboratory ordering, and route of drug administration preference.
A small subset of patients reported positive pain scores at triage but did not describe acute pain. Pain scores are highly subjective, and few primary literature sources link chronic pain with increased BP.22,23 Nevertheless, patients who reported acute pain and elevated BP were excluded in order to identify truly asymptomatic patients. VA hospitals are unique health systems and data obtained from this study might not be applicable to other public or private facilities. Last, the study did not take into account patients’ psychosocial circumstances that might have fostered a disproportionate reliance on the ED for health care.
Conclusion
Asymptomatic patients with elevated BP are treated in the ED despite no evidence supporting improved outcomes after acute BP lowering in this population. Follow-up after ED encounters for AH did not occur consistently within guideline-recommended 7 days, a trend that also occurs in non-VA systems.8 Clinics and health care systems could establish policies to prevent or minimize management of AH in the ED. Ideally, AH should be managed in a clinic setting by a PCP, but growing clinician workload might lead to increasing wait times and difficultly obtaining same-day appointments. Nurse-led clinics and clinical pharmacists operating under a scope of practice and working closely with a PCP are a cost-effective solution to ensure timely treatment and appropriate follow-up of patients with uncontrolled hypertension.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the North Florida South Georgia Veterans Health System in Gainesville, Florida.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):
1-8.
2. Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
3. Chobanian AV, Bakris GL, Black HR, et al; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206-1252.
4. James, PA, Oparil, S, Carter, BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. American Heart Association. High blood pressure ER visits jumped 25 percent in 2006-11. http://newsroom.heart.org/news/high-blood-pressure-er-visits-jumped-25-percent-in-2006-11. Published September 9, 2014. Accessed January 19, 2018.
6. Owens P, Mutter R. Statistical brief #100: emergency department visits for adults in community hospitals. Agency for Healthcare Research and Quality. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb100.pdf. Published November 2010. Accessed January 19, 2018.
7. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
8. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988.
9. Acute Kidney Injury Network. AKIN studies. http://www.akinet.org/akinstudies.php. Updated 2017. Accessed January 19, 2018.
10. Karras DJ, Kruus LK, Cienki JJ, et al. Utility of routine testing for patients with asymptomatic severe blood pressure elevation in the emergency department. Ann Emerg Med. 2008;51(3):231-239.
11. The SPRINT Research Group. A Randomized trial of Intensive versus standard blood pressure control. N Engl J Med. 2015;373:2103-2116.
12. Grassi D, O’Flaherty M, Pellizzari M, et al; Group of Investigators of the REHASE Program. Hypertensive urgencies in the emergency department: evaluating blood pressure response to rest and to antihypertensive drugs with different profiles. J Clin Hypertens (Greenwich). 2008;10(9):662-667.
13. Canters for Medicare & Medicaid Services. Emergency medical treatment & labor act (EMTALA). https://www.cms.gov/Regulations-and-Guidance/Legislation/EMTALA/index.html. Updated March 26, 2012. Accessed January 19, 2018.
14. Merritt Hawkins. 2017 Survey of physician appointment wait times and Medicare and Medicaid acceptance rates. https://www.merritthawkins.com/uploadedFiles/Merritt-Hawkins/Pdf/mha2017waittimesurveyPDF.pdf. Published 2017. Accessed January 19, 2018.
15. Galewitz P. VA treats patients’ impatience with clinical pharmacists. USA Today. http://www.usatoday.com/story/news/2016/10/24/kaiser-va-treats-patients-impatience-clinical-pharmacists/92479132/. Published October 24, 2016. Accessed January 19, 2018.
16. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169(21):1996-2002.
17. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized comparative trial. Pharmacotherapy. 2003;23(2):209-216.
18. Okamoto MP, Nakahiro RK. Pharmacoeconomic evaluation of a pharmacist-managed hypertension clinic. Pharmacotherapy. 2001;21(11):1337-1344.
19. Brown VM. Managing patients with hypertension in nurse-led clinics. Nursing. 2017;47(4):16-19.
20. Caldwell N, Srebotnjak T, Wang T, Hsia R. “How Much Will I Get Charged for This?” Patient charges for top ten diagnoses in the emergency department. PLoS ONE. 2013;8(2): e55491.
21. Davis KE. Expenditures for hypertension among adults age 18 and older, 2010: estimates for the U.S. civilian noninstitutionalized population. Agency for Healthcare Research and Quality. https://meps.ahrq.gov/data_files/publications/st404/stat404.shtml. Published April 2013. Accessed January 19, 2018.
22. Marco CA, Plewa MC, Buderer N, et al. Self-reported pain scores in the emergency department: lack of association with vital signs. Acad Emerg Med. 2006;13(9):974-979.
23. Wood D, Goodnight S, Haig AJ, Nasari T. Body mass index, but not blood pressure is related to the level of pain in persons with chronic pain. J Back Musculoskelet Rehabil. 2011;24(2):
111-115.
Hypertension affects more than 65 million individuals in the U.S., accounting for nearly 30% of the adult population.1 Less than 50% of those with hypertension are taking appropriate pharmacotherapy.2 Hypertension contributes to cardiovascular events, including cerebrovascular accident, transient ischemic attack, hypertensive retinopathy, renal failure, myocardial infarction, and heart failure.1 Chronic hypertension mainly is an asymptomatic condition, earning the nickname “the silent killer.”2 An acute, symptomatic elevation in blood pressure (BP) often is referred to as hypertensive emergency. Symptoms of end-organ damage can include headache, blurry vision, chest pain, shortness of breath, altered mental status, epistaxis, and oliguria.2 Although rare, hypertensive emergencies should be treated immediately. The Seventh Report of the Joint National Committee (JNC 7), and the more recent JNC 8, have published guidelines on managing chronic hypertension.3,4 However, neither report provides guidance on hypertensive emergency or the appropriate actions in cases of extremely elevated BP in an asymptomatic patient.3,4
Acute hypertensive episodes—often referred to as hypertensive crises—are responsible for nearly 8 million hospitalizations each year and 20 million visits to the emergency department (ED).5,6 Most of these visits are same-day “treat-and-release” events.5 There is no universally accepted BP value associated with a hypertensive crisis, but most resources state that a BP ≥ 180/110 mm Hg requires attention.2,7 Without other symptoms, elevated BP is not an emergency, yet ED referral for acute management is common.7
Three terms fall under the umbrella of hypertensive crises: hypertensive emergency, hypertensive urgency, and asymptomatic hypertension (AH).2 In a 2007 article, the American College of Chest Physicians defined hypertensive emergency as BP ≥ 180/110 mm Hg with evidence of end-organ damage.2 Symptoms are almost always present in true hypertensive emergencies, and immediate medical intervention is required to halt further organ damage. In the same article, hypertensive urgency is defined as BP ≥ 180/110 mm Hg without end-organ damage.2 The definition of hypertensive urgency could be further refined to include the presence of cardiovascular and renal risk factors, although this additional point is not consistent across the literature. Asymptomatic hypertension is similar to hypertensive urgency; however, there is an absence of signs or symptoms of end-organ damage.2 There is ambiguity in the literature concerning managing hypertensive urgency and AH, but both share a basic tenet: Immediate BP reduction is not essential. Gradual dosage adjustment(s) of oral medications, preferably by a primary care provider (PCP), and follow-up within 7 days are recommended.7
Limited evidence exists to guide ED providers in managing AH. Long-term outcomes and guidelines intended for the primary care setting should not be extrapolated to acute management in the ED. With limited treatment guidelines, providers might be more likely to refer patients with AH to the ED for evaluation. In 2013, the American College of Emergency Physicians (ACEP) created a clinical policy concerning AH in the ED. The ACEP concluded that screening for target organ injury and medical intervention in the ED does not reduce rates of adverse events (AEs) and could lead to overtreatment and acute hypoperfusion.7 More recently, Patel and colleagues published findings on hypertensive urgency in the ambulatory care setting, which similarly found that referral to the ED was associated with increased use of health care resources and no change in short-term major AEs.8 The ACEP recommends that patients presenting with AH be referred to primary care clinics where long-term monitoring and medication adjustments can be achieved more cost-effectively.7
The objective of this retrospective evaluation was to assess the incidence and management of AH within a VA ED. The authors aimed to provide insight into how these patients are managed and discuss alternatives to ED use.
Methods
This retrospective observational study was conducted within the North Florida/South Georgia Veterans Health System (NFSGVHS), which provides patient care at 2 medical centers in Gainesville and Lake City, Florida, as well as 11 outpatient clinics located throughout North Florida and South Georgia. The NFSGVHS serves rural and urban veteran populations. Study approval was granted by the NFSGVHS Institutional Review Board and Research and Development Committee.
Inclusion/Exclusion Criteria
Adult patients who were ordered at least 1 antihypertensive medication in the ED from July 1, 2011 to July 1, 2014, in addition to being asymptomatic with BP ≥ 180/110 mm Hg at ED triage were included. Based on clinical experience, the authors estimated that 3 years would provide a sample size of more than 100 patients. Patients were excluded if they presented with any acute symptoms or were hospitalized for further management.
Data Collection
Baseline demographics were collected for all participants. During the ED encounter, pre- and postintervention vital signs were recorded and prespecified laboratory data obtained. Interrater reliability was accounted for by performing random reviews of previously collected data to ensure consistency during the chart review process. Renal end-organ damage was defined using Acute Kidney Injury Network criteria, a serum creatinine 50% above baseline, or an absolute increase in baseline serum creatinine by 0.3 mg/dL.9 Additional laboratory markers of organ damage included cardiac troponin levels. Urinalysis results also were assessed to determine the presence of hematuria or proteinuria. Patient-reported nonadherence with medications was determined by reviewing ED provider and/or nurse documentation notes for the index ED encounter.
Investigators documented the route (IV or oral) and antihypertensive(s) medication selected for each patient. Adverse effects and any changes to patients’ outpatient medication regimens were noted. Investigators also assessed days to next medical contact after ED discharge to determine whether follow-up occurred according to the recommended standard of 7 days.9 Days to next medical contact was defined as any contact—in person or by telephone—that was documented in the electronic health record after the index ED visit.
Statistical Analysis
Descriptive statistics, including mean, median, and standard deviation, were used to analyze data.
Results
A total of 1,052 patients presented with BP ≥ 180/110 mm Hg and for whom antihypertensive medication was ordered but not necessarily given in the ED. Of the total, 724 patients were excluded because of hospital admission for other primary diagnoses; however, 6 of these patients were admitted for hypertensive urgency. The final analysis included 132 patients who presented with the primary condition of elevated BP without any accompanying symptoms. Among these patients, 2 had repeat ED visits for AH during the specified time frame.
Most patients were male with an average age of 63 years and documented history of hypertension. Nearly all patients had established primary care within the NFSGVHS. The most common comorbidity was diabetes mellitus (36%), followed by coronary artery disease (27%) and chronic kidney disease (CKD) (21%) (Table 1). About one-third of patients presented to the ED on their own volition, and slightly more than half were referred to the ED by primary care or specialty clinics.
In the ED, 130 patients received BP treatment (Table 2). Medication was ordered for 2 patients who did not receive treatment. In total, 12 different medication classes were used for treating patients with AH in the ED (Figure).
Treatment in the ED resulted in an average BP and heart rate reduction of 27/20 mm Hg and 5 beats per minute, respectively. About 80% of patients had a basic metabolic panel drawn, and there were no instances of acute kidney injury. Of the patients in the study 38% had cardiac enzymes collected, and only 1 patient had a positive result, which was determined to be unrelated to acute coronary syndrome. Forty-one (31%) of patients had a urinalysis; 12 has positive results for hematuria, and 18 revealed proteinuria. Of note, the 6 patients who were hospitalized for hypertensive urgency had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. The reason these patients were admitted is unclear.
At discharge, ED providers made changes to 54% of patients’ outpatient antihypertensive regimens. These changes included adding a new medication (68%), increasing the dosage of an existing medication (24%), or multiple changes (8%). Refills were provided for 18% of prescriptions. Follow-up within 7 days from ED discharge was recorded for 34% of patients. One patient received follow-up outside the NFSGVHS and was not included in this analysis.
Discussion
The aim of this retrospective study was to determine the incidence of AH in a VA ED and describe how these patients were managed. Overall, the rate of patients presenting to the ED with AH during the study period was about 1 patient every 8 days or 45 patients per year. By comparison, more than 30,000 patients are seen at the NFSGVHS ED annually. Although AH seems to be an uncommon occurrence, study findings raise questions about the value of managing the condition in the ED.
This study found several management strategies as well as noteworthy trends. For example, laboratory tests were not ordered routinely for all patients, suggesting that some ED providers question their use for AH. There were no patients with acute elevations in serum creatinine that indicated acute kidney injury, and although hematuria and proteinuria were common findings, neither were specific for acute injury. However, there were findings typical of chronic hypertension, and urinalysis may provide little benefit when testing for acute kidney injury. Only 1 patient showed elevated cardiac enzymes, which was determined to be a result of CKD.
Although not included in the final analysis, the 6 patients who were hospitalized for hypertensive urgency were similar in that they had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. Collectively, these findings support existing literature that questions the utility of laboratory testing of patients with AH in the ED.10
Patients also were treated with a variety of antihypertensive agents in the ED. One explanation might be outpatient nonadherence with medications. In patients with AH, it is common to provide doses of chronic medications that the patient might have missed and should be taking on a regular basis. Therefore, assessing adherence with current medications before modifying chronic therapy is an important initial step when managing AH.
Although oral agents primarily were used, IV antihypertensives were administered to about one-third of patients. Preference for IV administration in the ED might be related to its ability to lower BP quickly. The practice of obtaining IV access for medication in a patient with AH is costly, unnecessary, and potentially harmful.7 The authors theorize that this practice is performed, in many cases, as an attempt to expedite ED discharge after an acceptable BP reading is documented.
Rapid reductions in BP can precipitate hypoperfusion inadvertently and are more likely to occur with IV agents than with oral ones. Therefore, the safety, convenience, and cost savings associated with oral administration make it the preferred route for managing AH.
Best Practices
Primary care clinics are best suited to manage AH because medication adjustments and long-term monitoring are easier to perform and at substantially lower costs when compared with that of the ED. Rather than immediately referring a patient to the ED, clinicians should consider factors that could elevate BP, such as medication nonadherence, anxiety, acute pain, recent tobacco or caffeine use, or white coat syndrome. Staff should be well educated on proper BP measurement and instructed to repeat the reading for confirmation. Before measuring BP, allow the patient to sit quietly for 5 minutes with the feet flat on the floor and arm supported.3 Ideally, the measurement used should be the average of 3 BP readings on an automated device.11 If BP readings are high, staff should ask the patient about medication adherence and missed medication(s) should be administered.
It also is reasonable to have the patient rest quietly for up to 30 minutes because rest has been shown to reduce BP in some patients.12 The drawback to the prolonged rest strategy is the potential to cause delays in care for other patients. However, it is important to remember that wait times in the ED often are measured in hours, which causes frustration for patients referred to the ED for AH management. Before completing the office visit, the provider should recheck BP using proper technique and confirm that the patient has antihypertensive medication(s) in his/her possession; a follow-up appointment should be scheduled for no later than 1 week.
Primary care providers might be concerned about taking on additional liability and could favor ED referral, but legislation makes it difficult for EDs to defer nonemergent issues to primary care clinics. The Emergency Medical Treatment and Labor Act states that hospitals are prohibited from denying a patient care during an emergency.13 Despite evidence that AH is not an emergency, many patients continue to be referred to the ED. One-third of patients presented to the ED on their own volition and more than one-half were referred by health care personnel. This strongly suggests that both patients and health care personnel consider AH an emergency medical condition requiring immediate attention. However, patients with AH rarely are found to have any acute end-organ damage; therefore, acute treatment and extensive laboratory or diagnostic testing in the ED provides little, if any, benefit.10 The authors believe the ACEP clinical policy should be adopted into mainstream practice to help reduce health care costs and preserve ED resources for patients with true emergencies.
Another pervasive issue that could contribute to inappropriate AH referrals to the ED is the shortage of PCPs and limited same-day appointments for nonemergent conditions. In a 2017 survey, the average wait time for a PCP appointment ranged between 12 and 109 days, depending on the metropolitan area. The national average wait time conducted by this survey was 29.3 days.14 When primary care appointments are unavailable, triage staff could recommend that patients seek care in the ED. Additionally, patients might choose to seek ED care rather than wait for the next available PCP appointment. Clinic proximity to an ED could influence referral rates. In other words, medical centers or health systems with primary care clinics and ED services under one roof could experience more frequent ED referrals.
A promising strategy to help overcome the challenges of addressing AH and avoiding ED referrals is increasing patient access to and use of qualified, nonphysician providers, such as clinical pharmacists and nurse practitioners. Large health systems such as the VA and Kaiser Permanente have employed clinical pharmacist providers to reduce follow-up times for patients in primary care settings.15 Furthermore, there is substantial evidence that supports the cost-effectiveness and clinical success of pharmacist-driven hypertension clinics.16-18 Nurse-driven efforts to improve hypertension control have been successfully implemented in health systems.19 Both clinical pharmacist and nurse-managed hypertension clinics are effective solutions to manage patients with AH who might otherwise use costly ED services.For example, the average cost of a single ED visit is $740 to $3,437.20 In comparison, a 2010 report from the Agency for Healthcare Research and Quality showed the average annual cost of managing hypertension in ambulatory care clinics was $442 per adult, a cost considerably lower than that of the ED.21
Limitations
The retrospective and observational design of this study are inherent limitations. This study was not designed to evaluate cardiovascular outcomes after ED encounters. The sample size could have been larger if patients with BP < 180/110 mm Hg at ED triage were included; however, the 180/110 mm Hg threshold was chosen because it was the most widely agreed on BP value in the literature. This study did not capture patients who presented with AH and did not receive any acute treatment in the ED.Prescribing patterns based on provider training (eg, emergency medicine, family medicine, or internal medicine) were not tracked and might have accounted for differences in selection of diagnostic tests, laboratory ordering, and route of drug administration preference.
A small subset of patients reported positive pain scores at triage but did not describe acute pain. Pain scores are highly subjective, and few primary literature sources link chronic pain with increased BP.22,23 Nevertheless, patients who reported acute pain and elevated BP were excluded in order to identify truly asymptomatic patients. VA hospitals are unique health systems and data obtained from this study might not be applicable to other public or private facilities. Last, the study did not take into account patients’ psychosocial circumstances that might have fostered a disproportionate reliance on the ED for health care.
Conclusion
Asymptomatic patients with elevated BP are treated in the ED despite no evidence supporting improved outcomes after acute BP lowering in this population. Follow-up after ED encounters for AH did not occur consistently within guideline-recommended 7 days, a trend that also occurs in non-VA systems.8 Clinics and health care systems could establish policies to prevent or minimize management of AH in the ED. Ideally, AH should be managed in a clinic setting by a PCP, but growing clinician workload might lead to increasing wait times and difficultly obtaining same-day appointments. Nurse-led clinics and clinical pharmacists operating under a scope of practice and working closely with a PCP are a cost-effective solution to ensure timely treatment and appropriate follow-up of patients with uncontrolled hypertension.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the North Florida South Georgia Veterans Health System in Gainesville, Florida.
Hypertension affects more than 65 million individuals in the U.S., accounting for nearly 30% of the adult population.1 Less than 50% of those with hypertension are taking appropriate pharmacotherapy.2 Hypertension contributes to cardiovascular events, including cerebrovascular accident, transient ischemic attack, hypertensive retinopathy, renal failure, myocardial infarction, and heart failure.1 Chronic hypertension mainly is an asymptomatic condition, earning the nickname “the silent killer.”2 An acute, symptomatic elevation in blood pressure (BP) often is referred to as hypertensive emergency. Symptoms of end-organ damage can include headache, blurry vision, chest pain, shortness of breath, altered mental status, epistaxis, and oliguria.2 Although rare, hypertensive emergencies should be treated immediately. The Seventh Report of the Joint National Committee (JNC 7), and the more recent JNC 8, have published guidelines on managing chronic hypertension.3,4 However, neither report provides guidance on hypertensive emergency or the appropriate actions in cases of extremely elevated BP in an asymptomatic patient.3,4
Acute hypertensive episodes—often referred to as hypertensive crises—are responsible for nearly 8 million hospitalizations each year and 20 million visits to the emergency department (ED).5,6 Most of these visits are same-day “treat-and-release” events.5 There is no universally accepted BP value associated with a hypertensive crisis, but most resources state that a BP ≥ 180/110 mm Hg requires attention.2,7 Without other symptoms, elevated BP is not an emergency, yet ED referral for acute management is common.7
Three terms fall under the umbrella of hypertensive crises: hypertensive emergency, hypertensive urgency, and asymptomatic hypertension (AH).2 In a 2007 article, the American College of Chest Physicians defined hypertensive emergency as BP ≥ 180/110 mm Hg with evidence of end-organ damage.2 Symptoms are almost always present in true hypertensive emergencies, and immediate medical intervention is required to halt further organ damage. In the same article, hypertensive urgency is defined as BP ≥ 180/110 mm Hg without end-organ damage.2 The definition of hypertensive urgency could be further refined to include the presence of cardiovascular and renal risk factors, although this additional point is not consistent across the literature. Asymptomatic hypertension is similar to hypertensive urgency; however, there is an absence of signs or symptoms of end-organ damage.2 There is ambiguity in the literature concerning managing hypertensive urgency and AH, but both share a basic tenet: Immediate BP reduction is not essential. Gradual dosage adjustment(s) of oral medications, preferably by a primary care provider (PCP), and follow-up within 7 days are recommended.7
Limited evidence exists to guide ED providers in managing AH. Long-term outcomes and guidelines intended for the primary care setting should not be extrapolated to acute management in the ED. With limited treatment guidelines, providers might be more likely to refer patients with AH to the ED for evaluation. In 2013, the American College of Emergency Physicians (ACEP) created a clinical policy concerning AH in the ED. The ACEP concluded that screening for target organ injury and medical intervention in the ED does not reduce rates of adverse events (AEs) and could lead to overtreatment and acute hypoperfusion.7 More recently, Patel and colleagues published findings on hypertensive urgency in the ambulatory care setting, which similarly found that referral to the ED was associated with increased use of health care resources and no change in short-term major AEs.8 The ACEP recommends that patients presenting with AH be referred to primary care clinics where long-term monitoring and medication adjustments can be achieved more cost-effectively.7
The objective of this retrospective evaluation was to assess the incidence and management of AH within a VA ED. The authors aimed to provide insight into how these patients are managed and discuss alternatives to ED use.
Methods
This retrospective observational study was conducted within the North Florida/South Georgia Veterans Health System (NFSGVHS), which provides patient care at 2 medical centers in Gainesville and Lake City, Florida, as well as 11 outpatient clinics located throughout North Florida and South Georgia. The NFSGVHS serves rural and urban veteran populations. Study approval was granted by the NFSGVHS Institutional Review Board and Research and Development Committee.
Inclusion/Exclusion Criteria
Adult patients who were ordered at least 1 antihypertensive medication in the ED from July 1, 2011 to July 1, 2014, in addition to being asymptomatic with BP ≥ 180/110 mm Hg at ED triage were included. Based on clinical experience, the authors estimated that 3 years would provide a sample size of more than 100 patients. Patients were excluded if they presented with any acute symptoms or were hospitalized for further management.
Data Collection
Baseline demographics were collected for all participants. During the ED encounter, pre- and postintervention vital signs were recorded and prespecified laboratory data obtained. Interrater reliability was accounted for by performing random reviews of previously collected data to ensure consistency during the chart review process. Renal end-organ damage was defined using Acute Kidney Injury Network criteria, a serum creatinine 50% above baseline, or an absolute increase in baseline serum creatinine by 0.3 mg/dL.9 Additional laboratory markers of organ damage included cardiac troponin levels. Urinalysis results also were assessed to determine the presence of hematuria or proteinuria. Patient-reported nonadherence with medications was determined by reviewing ED provider and/or nurse documentation notes for the index ED encounter.
Investigators documented the route (IV or oral) and antihypertensive(s) medication selected for each patient. Adverse effects and any changes to patients’ outpatient medication regimens were noted. Investigators also assessed days to next medical contact after ED discharge to determine whether follow-up occurred according to the recommended standard of 7 days.9 Days to next medical contact was defined as any contact—in person or by telephone—that was documented in the electronic health record after the index ED visit.
Statistical Analysis
Descriptive statistics, including mean, median, and standard deviation, were used to analyze data.
Results
A total of 1,052 patients presented with BP ≥ 180/110 mm Hg and for whom antihypertensive medication was ordered but not necessarily given in the ED. Of the total, 724 patients were excluded because of hospital admission for other primary diagnoses; however, 6 of these patients were admitted for hypertensive urgency. The final analysis included 132 patients who presented with the primary condition of elevated BP without any accompanying symptoms. Among these patients, 2 had repeat ED visits for AH during the specified time frame.
Most patients were male with an average age of 63 years and documented history of hypertension. Nearly all patients had established primary care within the NFSGVHS. The most common comorbidity was diabetes mellitus (36%), followed by coronary artery disease (27%) and chronic kidney disease (CKD) (21%) (Table 1). About one-third of patients presented to the ED on their own volition, and slightly more than half were referred to the ED by primary care or specialty clinics.
In the ED, 130 patients received BP treatment (Table 2). Medication was ordered for 2 patients who did not receive treatment. In total, 12 different medication classes were used for treating patients with AH in the ED (Figure).
Treatment in the ED resulted in an average BP and heart rate reduction of 27/20 mm Hg and 5 beats per minute, respectively. About 80% of patients had a basic metabolic panel drawn, and there were no instances of acute kidney injury. Of the patients in the study 38% had cardiac enzymes collected, and only 1 patient had a positive result, which was determined to be unrelated to acute coronary syndrome. Forty-one (31%) of patients had a urinalysis; 12 has positive results for hematuria, and 18 revealed proteinuria. Of note, the 6 patients who were hospitalized for hypertensive urgency had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. The reason these patients were admitted is unclear.
At discharge, ED providers made changes to 54% of patients’ outpatient antihypertensive regimens. These changes included adding a new medication (68%), increasing the dosage of an existing medication (24%), or multiple changes (8%). Refills were provided for 18% of prescriptions. Follow-up within 7 days from ED discharge was recorded for 34% of patients. One patient received follow-up outside the NFSGVHS and was not included in this analysis.
Discussion
The aim of this retrospective study was to determine the incidence of AH in a VA ED and describe how these patients were managed. Overall, the rate of patients presenting to the ED with AH during the study period was about 1 patient every 8 days or 45 patients per year. By comparison, more than 30,000 patients are seen at the NFSGVHS ED annually. Although AH seems to be an uncommon occurrence, study findings raise questions about the value of managing the condition in the ED.
This study found several management strategies as well as noteworthy trends. For example, laboratory tests were not ordered routinely for all patients, suggesting that some ED providers question their use for AH. There were no patients with acute elevations in serum creatinine that indicated acute kidney injury, and although hematuria and proteinuria were common findings, neither were specific for acute injury. However, there were findings typical of chronic hypertension, and urinalysis may provide little benefit when testing for acute kidney injury. Only 1 patient showed elevated cardiac enzymes, which was determined to be a result of CKD.
Although not included in the final analysis, the 6 patients who were hospitalized for hypertensive urgency were similar in that they had neither symptoms at presentation to the ED nor laboratory findings indicating end-organ damage. Collectively, these findings support existing literature that questions the utility of laboratory testing of patients with AH in the ED.10
Patients also were treated with a variety of antihypertensive agents in the ED. One explanation might be outpatient nonadherence with medications. In patients with AH, it is common to provide doses of chronic medications that the patient might have missed and should be taking on a regular basis. Therefore, assessing adherence with current medications before modifying chronic therapy is an important initial step when managing AH.
Although oral agents primarily were used, IV antihypertensives were administered to about one-third of patients. Preference for IV administration in the ED might be related to its ability to lower BP quickly. The practice of obtaining IV access for medication in a patient with AH is costly, unnecessary, and potentially harmful.7 The authors theorize that this practice is performed, in many cases, as an attempt to expedite ED discharge after an acceptable BP reading is documented.
Rapid reductions in BP can precipitate hypoperfusion inadvertently and are more likely to occur with IV agents than with oral ones. Therefore, the safety, convenience, and cost savings associated with oral administration make it the preferred route for managing AH.
Best Practices
Primary care clinics are best suited to manage AH because medication adjustments and long-term monitoring are easier to perform and at substantially lower costs when compared with that of the ED. Rather than immediately referring a patient to the ED, clinicians should consider factors that could elevate BP, such as medication nonadherence, anxiety, acute pain, recent tobacco or caffeine use, or white coat syndrome. Staff should be well educated on proper BP measurement and instructed to repeat the reading for confirmation. Before measuring BP, allow the patient to sit quietly for 5 minutes with the feet flat on the floor and arm supported.3 Ideally, the measurement used should be the average of 3 BP readings on an automated device.11 If BP readings are high, staff should ask the patient about medication adherence and missed medication(s) should be administered.
It also is reasonable to have the patient rest quietly for up to 30 minutes because rest has been shown to reduce BP in some patients.12 The drawback to the prolonged rest strategy is the potential to cause delays in care for other patients. However, it is important to remember that wait times in the ED often are measured in hours, which causes frustration for patients referred to the ED for AH management. Before completing the office visit, the provider should recheck BP using proper technique and confirm that the patient has antihypertensive medication(s) in his/her possession; a follow-up appointment should be scheduled for no later than 1 week.
Primary care providers might be concerned about taking on additional liability and could favor ED referral, but legislation makes it difficult for EDs to defer nonemergent issues to primary care clinics. The Emergency Medical Treatment and Labor Act states that hospitals are prohibited from denying a patient care during an emergency.13 Despite evidence that AH is not an emergency, many patients continue to be referred to the ED. One-third of patients presented to the ED on their own volition and more than one-half were referred by health care personnel. This strongly suggests that both patients and health care personnel consider AH an emergency medical condition requiring immediate attention. However, patients with AH rarely are found to have any acute end-organ damage; therefore, acute treatment and extensive laboratory or diagnostic testing in the ED provides little, if any, benefit.10 The authors believe the ACEP clinical policy should be adopted into mainstream practice to help reduce health care costs and preserve ED resources for patients with true emergencies.
Another pervasive issue that could contribute to inappropriate AH referrals to the ED is the shortage of PCPs and limited same-day appointments for nonemergent conditions. In a 2017 survey, the average wait time for a PCP appointment ranged between 12 and 109 days, depending on the metropolitan area. The national average wait time conducted by this survey was 29.3 days.14 When primary care appointments are unavailable, triage staff could recommend that patients seek care in the ED. Additionally, patients might choose to seek ED care rather than wait for the next available PCP appointment. Clinic proximity to an ED could influence referral rates. In other words, medical centers or health systems with primary care clinics and ED services under one roof could experience more frequent ED referrals.
A promising strategy to help overcome the challenges of addressing AH and avoiding ED referrals is increasing patient access to and use of qualified, nonphysician providers, such as clinical pharmacists and nurse practitioners. Large health systems such as the VA and Kaiser Permanente have employed clinical pharmacist providers to reduce follow-up times for patients in primary care settings.15 Furthermore, there is substantial evidence that supports the cost-effectiveness and clinical success of pharmacist-driven hypertension clinics.16-18 Nurse-driven efforts to improve hypertension control have been successfully implemented in health systems.19 Both clinical pharmacist and nurse-managed hypertension clinics are effective solutions to manage patients with AH who might otherwise use costly ED services.For example, the average cost of a single ED visit is $740 to $3,437.20 In comparison, a 2010 report from the Agency for Healthcare Research and Quality showed the average annual cost of managing hypertension in ambulatory care clinics was $442 per adult, a cost considerably lower than that of the ED.21
Limitations
The retrospective and observational design of this study are inherent limitations. This study was not designed to evaluate cardiovascular outcomes after ED encounters. The sample size could have been larger if patients with BP < 180/110 mm Hg at ED triage were included; however, the 180/110 mm Hg threshold was chosen because it was the most widely agreed on BP value in the literature. This study did not capture patients who presented with AH and did not receive any acute treatment in the ED.Prescribing patterns based on provider training (eg, emergency medicine, family medicine, or internal medicine) were not tracked and might have accounted for differences in selection of diagnostic tests, laboratory ordering, and route of drug administration preference.
A small subset of patients reported positive pain scores at triage but did not describe acute pain. Pain scores are highly subjective, and few primary literature sources link chronic pain with increased BP.22,23 Nevertheless, patients who reported acute pain and elevated BP were excluded in order to identify truly asymptomatic patients. VA hospitals are unique health systems and data obtained from this study might not be applicable to other public or private facilities. Last, the study did not take into account patients’ psychosocial circumstances that might have fostered a disproportionate reliance on the ED for health care.
Conclusion
Asymptomatic patients with elevated BP are treated in the ED despite no evidence supporting improved outcomes after acute BP lowering in this population. Follow-up after ED encounters for AH did not occur consistently within guideline-recommended 7 days, a trend that also occurs in non-VA systems.8 Clinics and health care systems could establish policies to prevent or minimize management of AH in the ED. Ideally, AH should be managed in a clinic setting by a PCP, but growing clinician workload might lead to increasing wait times and difficultly obtaining same-day appointments. Nurse-led clinics and clinical pharmacists operating under a scope of practice and working closely with a PCP are a cost-effective solution to ensure timely treatment and appropriate follow-up of patients with uncontrolled hypertension.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the North Florida South Georgia Veterans Health System in Gainesville, Florida.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):
1-8.
2. Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
3. Chobanian AV, Bakris GL, Black HR, et al; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206-1252.
4. James, PA, Oparil, S, Carter, BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. American Heart Association. High blood pressure ER visits jumped 25 percent in 2006-11. http://newsroom.heart.org/news/high-blood-pressure-er-visits-jumped-25-percent-in-2006-11. Published September 9, 2014. Accessed January 19, 2018.
6. Owens P, Mutter R. Statistical brief #100: emergency department visits for adults in community hospitals. Agency for Healthcare Research and Quality. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb100.pdf. Published November 2010. Accessed January 19, 2018.
7. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
8. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988.
9. Acute Kidney Injury Network. AKIN studies. http://www.akinet.org/akinstudies.php. Updated 2017. Accessed January 19, 2018.
10. Karras DJ, Kruus LK, Cienki JJ, et al. Utility of routine testing for patients with asymptomatic severe blood pressure elevation in the emergency department. Ann Emerg Med. 2008;51(3):231-239.
11. The SPRINT Research Group. A Randomized trial of Intensive versus standard blood pressure control. N Engl J Med. 2015;373:2103-2116.
12. Grassi D, O’Flaherty M, Pellizzari M, et al; Group of Investigators of the REHASE Program. Hypertensive urgencies in the emergency department: evaluating blood pressure response to rest and to antihypertensive drugs with different profiles. J Clin Hypertens (Greenwich). 2008;10(9):662-667.
13. Canters for Medicare & Medicaid Services. Emergency medical treatment & labor act (EMTALA). https://www.cms.gov/Regulations-and-Guidance/Legislation/EMTALA/index.html. Updated March 26, 2012. Accessed January 19, 2018.
14. Merritt Hawkins. 2017 Survey of physician appointment wait times and Medicare and Medicaid acceptance rates. https://www.merritthawkins.com/uploadedFiles/Merritt-Hawkins/Pdf/mha2017waittimesurveyPDF.pdf. Published 2017. Accessed January 19, 2018.
15. Galewitz P. VA treats patients’ impatience with clinical pharmacists. USA Today. http://www.usatoday.com/story/news/2016/10/24/kaiser-va-treats-patients-impatience-clinical-pharmacists/92479132/. Published October 24, 2016. Accessed January 19, 2018.
16. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169(21):1996-2002.
17. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized comparative trial. Pharmacotherapy. 2003;23(2):209-216.
18. Okamoto MP, Nakahiro RK. Pharmacoeconomic evaluation of a pharmacist-managed hypertension clinic. Pharmacotherapy. 2001;21(11):1337-1344.
19. Brown VM. Managing patients with hypertension in nurse-led clinics. Nursing. 2017;47(4):16-19.
20. Caldwell N, Srebotnjak T, Wang T, Hsia R. “How Much Will I Get Charged for This?” Patient charges for top ten diagnoses in the emergency department. PLoS ONE. 2013;8(2): e55491.
21. Davis KE. Expenditures for hypertension among adults age 18 and older, 2010: estimates for the U.S. civilian noninstitutionalized population. Agency for Healthcare Research and Quality. https://meps.ahrq.gov/data_files/publications/st404/stat404.shtml. Published April 2013. Accessed January 19, 2018.
22. Marco CA, Plewa MC, Buderer N, et al. Self-reported pain scores in the emergency department: lack of association with vital signs. Acad Emerg Med. 2006;13(9):974-979.
23. Wood D, Goodnight S, Haig AJ, Nasari T. Body mass index, but not blood pressure is related to the level of pain in persons with chronic pain. J Back Musculoskelet Rehabil. 2011;24(2):
111-115.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):
1-8.
2. Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
3. Chobanian AV, Bakris GL, Black HR, et al; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206-1252.
4. James, PA, Oparil, S, Carter, BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. American Heart Association. High blood pressure ER visits jumped 25 percent in 2006-11. http://newsroom.heart.org/news/high-blood-pressure-er-visits-jumped-25-percent-in-2006-11. Published September 9, 2014. Accessed January 19, 2018.
6. Owens P, Mutter R. Statistical brief #100: emergency department visits for adults in community hospitals. Agency for Healthcare Research and Quality. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb100.pdf. Published November 2010. Accessed January 19, 2018.
7. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
8. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988.
9. Acute Kidney Injury Network. AKIN studies. http://www.akinet.org/akinstudies.php. Updated 2017. Accessed January 19, 2018.
10. Karras DJ, Kruus LK, Cienki JJ, et al. Utility of routine testing for patients with asymptomatic severe blood pressure elevation in the emergency department. Ann Emerg Med. 2008;51(3):231-239.
11. The SPRINT Research Group. A Randomized trial of Intensive versus standard blood pressure control. N Engl J Med. 2015;373:2103-2116.
12. Grassi D, O’Flaherty M, Pellizzari M, et al; Group of Investigators of the REHASE Program. Hypertensive urgencies in the emergency department: evaluating blood pressure response to rest and to antihypertensive drugs with different profiles. J Clin Hypertens (Greenwich). 2008;10(9):662-667.
13. Canters for Medicare & Medicaid Services. Emergency medical treatment & labor act (EMTALA). https://www.cms.gov/Regulations-and-Guidance/Legislation/EMTALA/index.html. Updated March 26, 2012. Accessed January 19, 2018.
14. Merritt Hawkins. 2017 Survey of physician appointment wait times and Medicare and Medicaid acceptance rates. https://www.merritthawkins.com/uploadedFiles/Merritt-Hawkins/Pdf/mha2017waittimesurveyPDF.pdf. Published 2017. Accessed January 19, 2018.
15. Galewitz P. VA treats patients’ impatience with clinical pharmacists. USA Today. http://www.usatoday.com/story/news/2016/10/24/kaiser-va-treats-patients-impatience-clinical-pharmacists/92479132/. Published October 24, 2016. Accessed January 19, 2018.
16. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169(21):1996-2002.
17. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized comparative trial. Pharmacotherapy. 2003;23(2):209-216.
18. Okamoto MP, Nakahiro RK. Pharmacoeconomic evaluation of a pharmacist-managed hypertension clinic. Pharmacotherapy. 2001;21(11):1337-1344.
19. Brown VM. Managing patients with hypertension in nurse-led clinics. Nursing. 2017;47(4):16-19.
20. Caldwell N, Srebotnjak T, Wang T, Hsia R. “How Much Will I Get Charged for This?” Patient charges for top ten diagnoses in the emergency department. PLoS ONE. 2013;8(2): e55491.
21. Davis KE. Expenditures for hypertension among adults age 18 and older, 2010: estimates for the U.S. civilian noninstitutionalized population. Agency for Healthcare Research and Quality. https://meps.ahrq.gov/data_files/publications/st404/stat404.shtml. Published April 2013. Accessed January 19, 2018.
22. Marco CA, Plewa MC, Buderer N, et al. Self-reported pain scores in the emergency department: lack of association with vital signs. Acad Emerg Med. 2006;13(9):974-979.
23. Wood D, Goodnight S, Haig AJ, Nasari T. Body mass index, but not blood pressure is related to the level of pain in persons with chronic pain. J Back Musculoskelet Rehabil. 2011;24(2):
111-115.