User login
Bezlotoxumab may lower risk of C. difficile readmissions
Clostridium difficile infection (CDI) patients treated with bezlotoxumab were less likely to be readmitted for recurring symptoms within 30 days of discharge, according to a phase 3 trial funded by Merck.
Recurrent CDI is a burden on both patients and providers, increasing health risks with each recurrence and eating through hospital resources, according to Vimalanand S. Prabhu, PhD, associate principal scientist for Merck.
In a randomized, double-blind, placebo-controlled, study of 1,050 CDI patients, a total of 27 (5%) of 530 of those given bezlotoxumab were re-hospitalized 30 days after discharge, compared with 58 (11%) of 520 patients in the placebo group (Clin Infect Dis. 2017 Aug 11. doi. 10.1093/cid/cix523).
Patients were gathered from 322 sites across 30 countries between November 2011 and May 2015.
When measuring CDI-related readmissions, the investigators found use of bezlotoxumab reduced rCDI hospitalizations by 6%, and by approximately 8% in high-risk patients, such as those over 65 years old or with severe CDI.
Bezlotoxumab works by binding to CDI toxin B, a primary cause of CDI symptoms, according to Dr. Prabhu and fellow investigators. The researchers suggested that bezlotoxumab could be a prevailing factor in fighting the rate of CDI infections, which accounted for 29,000 deaths in 2011 (N Engl J Med. 2015 Jun 11;372[24]:2368-9).
Investigators acknowledged that patients admitted for the study may be healthier than the real-world CDI population.
All investigators reported some financial involvement, whether being a full-time employee or acting as a consultant, for Merck, which funded the study. Individually, investigators reported financial ties to similar medical companies, such as Pfizer and AstraZeneca.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Clostridium difficile infection (CDI) patients treated with bezlotoxumab were less likely to be readmitted for recurring symptoms within 30 days of discharge, according to a phase 3 trial funded by Merck.
Recurrent CDI is a burden on both patients and providers, increasing health risks with each recurrence and eating through hospital resources, according to Vimalanand S. Prabhu, PhD, associate principal scientist for Merck.
In a randomized, double-blind, placebo-controlled, study of 1,050 CDI patients, a total of 27 (5%) of 530 of those given bezlotoxumab were re-hospitalized 30 days after discharge, compared with 58 (11%) of 520 patients in the placebo group (Clin Infect Dis. 2017 Aug 11. doi. 10.1093/cid/cix523).
Patients were gathered from 322 sites across 30 countries between November 2011 and May 2015.
When measuring CDI-related readmissions, the investigators found use of bezlotoxumab reduced rCDI hospitalizations by 6%, and by approximately 8% in high-risk patients, such as those over 65 years old or with severe CDI.
Bezlotoxumab works by binding to CDI toxin B, a primary cause of CDI symptoms, according to Dr. Prabhu and fellow investigators. The researchers suggested that bezlotoxumab could be a prevailing factor in fighting the rate of CDI infections, which accounted for 29,000 deaths in 2011 (N Engl J Med. 2015 Jun 11;372[24]:2368-9).
Investigators acknowledged that patients admitted for the study may be healthier than the real-world CDI population.
All investigators reported some financial involvement, whether being a full-time employee or acting as a consultant, for Merck, which funded the study. Individually, investigators reported financial ties to similar medical companies, such as Pfizer and AstraZeneca.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Clostridium difficile infection (CDI) patients treated with bezlotoxumab were less likely to be readmitted for recurring symptoms within 30 days of discharge, according to a phase 3 trial funded by Merck.
Recurrent CDI is a burden on both patients and providers, increasing health risks with each recurrence and eating through hospital resources, according to Vimalanand S. Prabhu, PhD, associate principal scientist for Merck.
In a randomized, double-blind, placebo-controlled, study of 1,050 CDI patients, a total of 27 (5%) of 530 of those given bezlotoxumab were re-hospitalized 30 days after discharge, compared with 58 (11%) of 520 patients in the placebo group (Clin Infect Dis. 2017 Aug 11. doi. 10.1093/cid/cix523).
Patients were gathered from 322 sites across 30 countries between November 2011 and May 2015.
When measuring CDI-related readmissions, the investigators found use of bezlotoxumab reduced rCDI hospitalizations by 6%, and by approximately 8% in high-risk patients, such as those over 65 years old or with severe CDI.
Bezlotoxumab works by binding to CDI toxin B, a primary cause of CDI symptoms, according to Dr. Prabhu and fellow investigators. The researchers suggested that bezlotoxumab could be a prevailing factor in fighting the rate of CDI infections, which accounted for 29,000 deaths in 2011 (N Engl J Med. 2015 Jun 11;372[24]:2368-9).
Investigators acknowledged that patients admitted for the study may be healthier than the real-world CDI population.
All investigators reported some financial involvement, whether being a full-time employee or acting as a consultant, for Merck, which funded the study. Individually, investigators reported financial ties to similar medical companies, such as Pfizer and AstraZeneca.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM CLINICAL INFECTIOUS DISEASES
Key clinical point:
Major finding: A total of 27 of 530 (5%) bezlotoxumab patients were readmitted within 30 days of discharge compared with 58 of 520 (11%) placebo patients.
Data source: Randomized, double-blind, placebo-controlled, multicenter, global phase 3 trials conducted from November 2011-May 2015 at 322 sites in 30 countries.
Disclosures: All investigators report employment or financial support with Merck and have individually reported financial ties to similar companies like Astellas, AstraZeneca, Pfizer, and others.
Bar soaps may be better than body washes for contact dermatitis patients
SAN FRANCISCO – Chronic contact dermatitis often is tied to hidden allergens found in shampoos, soaps, and body washes, according to Cory Dunnick, MD.“A lot of patients who get referred to my patch test clinic will have chronic dermatitis that isn’t responding to treatment or is worsening despite treatment, or they present with a pattern that is suggestive of contact dermatitis,” she said in an interview.
There is also a common perception that liquid body washes are better than bar soaps because they may be more moisturizing, but the results of a recently published study suggest otherwise, Dr. Dunnick of the department of dermatology at the University of Colorado at Denver, Aurora, said at the annual meeting of the Pacific Dermatologic Association.
Dr. Dunnick was one of the investigators in a study that compared ingredients in the top-selling 50 bar soaps and 50 body washes on Amazon.com to determine if there was a difference with respect to allergen content. They obtained the ingredients list for all the products and compared them with the American Contact Dermatitis Society Core Allergen Series. Counter to the common belief, results of the study indicated that liquid soaps were likely the worse choice for sensitive patients: They contained far more preservative and surfactant allergens than bar soaps, and there was no difference in fragrance content between the two classes (Dermatitis. 2017 May 23. doi: 10.1097/DER.0000000000000289).
Of the 50 liquid soaps, 44 had one or more preservative allergens, compared with none of the bar soaps (P less than .001), and 34 had at least one surfactant allergen, compared with seven of the bar soaps (P less than .001). Forty-eight body washes had fragrance, as did 47 of the bar soaps.
The most common allergens in body washes were methylisothiazolinone (19 of 50), quaternium-15 (16), sodium benzoate (15), methylchloroisothiazolinone/methylisothiazolinone (12), DMDM hydantoin (10), and phenoxyethanol (9). None of these allergens appeared in any of the bar soaps.
“If you have a patient who you suspect has a contact allergy to a preservative or surfactant ingredient, then you can recommend perhaps switching to a bar soap, maybe one that is fragrance free,” advised Dr. Dunnick.
The most common allergen they found in body washes, methylisothiazolinone (MI), is becoming an increasing concern, she said. It has been around for many years but became more prevalent when the Food and Drug Administration decided in 2005 to allow higher concentrations of MI to be used in skin care products. “It’s a pretty strong sensitizer. As a result, we’re seeing a lot more allergy,” she noted.
This soap/body-wash allergen study sends a clear message to dermatologists to individualize recommendations, she said. “A lot of dermatologists recommend what they think are mild soaps, but they don’t necessarily think about what contact allergens might be in those soaps, so maybe they need to make more specific recommendations. They might recommend Dove soap,” but there are different Dove soaps, she pointed out.
A bigger challenge is finding a shampoo for sensitive patients. Almost all contain fragrances, and MI is an ingredient in many shampoos as well. Dr. Dunnick has found the DHS brand, which is fragrance free, to be helpful in some cases, and the Nonscents brand, also fragrance free, is sometimes recommended as safe.
But, in the end, recommendations must be individualized for the patient’s specific allergies, and that requires a thorough work-up. “You don’t know what they are unless you do the patch test,” she said.
Dr. Dunnick reported having no relevant financial disclosures.
SAN FRANCISCO – Chronic contact dermatitis often is tied to hidden allergens found in shampoos, soaps, and body washes, according to Cory Dunnick, MD.“A lot of patients who get referred to my patch test clinic will have chronic dermatitis that isn’t responding to treatment or is worsening despite treatment, or they present with a pattern that is suggestive of contact dermatitis,” she said in an interview.
There is also a common perception that liquid body washes are better than bar soaps because they may be more moisturizing, but the results of a recently published study suggest otherwise, Dr. Dunnick of the department of dermatology at the University of Colorado at Denver, Aurora, said at the annual meeting of the Pacific Dermatologic Association.
Dr. Dunnick was one of the investigators in a study that compared ingredients in the top-selling 50 bar soaps and 50 body washes on Amazon.com to determine if there was a difference with respect to allergen content. They obtained the ingredients list for all the products and compared them with the American Contact Dermatitis Society Core Allergen Series. Counter to the common belief, results of the study indicated that liquid soaps were likely the worse choice for sensitive patients: They contained far more preservative and surfactant allergens than bar soaps, and there was no difference in fragrance content between the two classes (Dermatitis. 2017 May 23. doi: 10.1097/DER.0000000000000289).
Of the 50 liquid soaps, 44 had one or more preservative allergens, compared with none of the bar soaps (P less than .001), and 34 had at least one surfactant allergen, compared with seven of the bar soaps (P less than .001). Forty-eight body washes had fragrance, as did 47 of the bar soaps.
The most common allergens in body washes were methylisothiazolinone (19 of 50), quaternium-15 (16), sodium benzoate (15), methylchloroisothiazolinone/methylisothiazolinone (12), DMDM hydantoin (10), and phenoxyethanol (9). None of these allergens appeared in any of the bar soaps.
“If you have a patient who you suspect has a contact allergy to a preservative or surfactant ingredient, then you can recommend perhaps switching to a bar soap, maybe one that is fragrance free,” advised Dr. Dunnick.
The most common allergen they found in body washes, methylisothiazolinone (MI), is becoming an increasing concern, she said. It has been around for many years but became more prevalent when the Food and Drug Administration decided in 2005 to allow higher concentrations of MI to be used in skin care products. “It’s a pretty strong sensitizer. As a result, we’re seeing a lot more allergy,” she noted.
This soap/body-wash allergen study sends a clear message to dermatologists to individualize recommendations, she said. “A lot of dermatologists recommend what they think are mild soaps, but they don’t necessarily think about what contact allergens might be in those soaps, so maybe they need to make more specific recommendations. They might recommend Dove soap,” but there are different Dove soaps, she pointed out.
A bigger challenge is finding a shampoo for sensitive patients. Almost all contain fragrances, and MI is an ingredient in many shampoos as well. Dr. Dunnick has found the DHS brand, which is fragrance free, to be helpful in some cases, and the Nonscents brand, also fragrance free, is sometimes recommended as safe.
But, in the end, recommendations must be individualized for the patient’s specific allergies, and that requires a thorough work-up. “You don’t know what they are unless you do the patch test,” she said.
Dr. Dunnick reported having no relevant financial disclosures.
SAN FRANCISCO – Chronic contact dermatitis often is tied to hidden allergens found in shampoos, soaps, and body washes, according to Cory Dunnick, MD.“A lot of patients who get referred to my patch test clinic will have chronic dermatitis that isn’t responding to treatment or is worsening despite treatment, or they present with a pattern that is suggestive of contact dermatitis,” she said in an interview.
There is also a common perception that liquid body washes are better than bar soaps because they may be more moisturizing, but the results of a recently published study suggest otherwise, Dr. Dunnick of the department of dermatology at the University of Colorado at Denver, Aurora, said at the annual meeting of the Pacific Dermatologic Association.
Dr. Dunnick was one of the investigators in a study that compared ingredients in the top-selling 50 bar soaps and 50 body washes on Amazon.com to determine if there was a difference with respect to allergen content. They obtained the ingredients list for all the products and compared them with the American Contact Dermatitis Society Core Allergen Series. Counter to the common belief, results of the study indicated that liquid soaps were likely the worse choice for sensitive patients: They contained far more preservative and surfactant allergens than bar soaps, and there was no difference in fragrance content between the two classes (Dermatitis. 2017 May 23. doi: 10.1097/DER.0000000000000289).
Of the 50 liquid soaps, 44 had one or more preservative allergens, compared with none of the bar soaps (P less than .001), and 34 had at least one surfactant allergen, compared with seven of the bar soaps (P less than .001). Forty-eight body washes had fragrance, as did 47 of the bar soaps.
The most common allergens in body washes were methylisothiazolinone (19 of 50), quaternium-15 (16), sodium benzoate (15), methylchloroisothiazolinone/methylisothiazolinone (12), DMDM hydantoin (10), and phenoxyethanol (9). None of these allergens appeared in any of the bar soaps.
“If you have a patient who you suspect has a contact allergy to a preservative or surfactant ingredient, then you can recommend perhaps switching to a bar soap, maybe one that is fragrance free,” advised Dr. Dunnick.
The most common allergen they found in body washes, methylisothiazolinone (MI), is becoming an increasing concern, she said. It has been around for many years but became more prevalent when the Food and Drug Administration decided in 2005 to allow higher concentrations of MI to be used in skin care products. “It’s a pretty strong sensitizer. As a result, we’re seeing a lot more allergy,” she noted.
This soap/body-wash allergen study sends a clear message to dermatologists to individualize recommendations, she said. “A lot of dermatologists recommend what they think are mild soaps, but they don’t necessarily think about what contact allergens might be in those soaps, so maybe they need to make more specific recommendations. They might recommend Dove soap,” but there are different Dove soaps, she pointed out.
A bigger challenge is finding a shampoo for sensitive patients. Almost all contain fragrances, and MI is an ingredient in many shampoos as well. Dr. Dunnick has found the DHS brand, which is fragrance free, to be helpful in some cases, and the Nonscents brand, also fragrance free, is sometimes recommended as safe.
But, in the end, recommendations must be individualized for the patient’s specific allergies, and that requires a thorough work-up. “You don’t know what they are unless you do the patch test,” she said.
Dr. Dunnick reported having no relevant financial disclosures.
AT PDA 2017
Metabolically healthy obese still at elevated cardiovascular risk
Obese individuals with no metabolic abnormalities, such as dyslipidemia, high blood pressure, or high blood sugar levels, still have a higher risk of cardiovascular disease than do metabolically healthy people of normal weight, new data suggests.
“Our study robustly challenges the assertion that MHO [metabolically healthy obese] is a benign condition and adds to the evidence base that MHO is a high-risk state for future CVD events,” wrote Rishi Caleyachetty, MD, of the University of Birmingham, England, and his coauthors online (J Am Coll Cardiol. 2017, Sep 11. doi. 10.1016/j.jacc.2017.07.763).
Dr. Caleyachetty and his associates reported findings from a population-based study using the electronic health records of nearly 3.5 million individuals aged 18 years or older who were free of cardiovascular disease at baseline.
Overall, 15% of the population were classified as being metabolically healthy obese, meaning that they had a body mass index (BMI) of at least 30 kg/m2 with no sign of diabetes, hypertension, or hyperlipidemia, and 26% were overweight with no metabolic abnormalities. Despite their lack of metabolic disease, these obese individuals still had a significant 49% higher risk of coronary heart disease, 7% higher risk of cerebrovascular disease, and 96% higher risk of heart failure, compared with normal-weight individuals with no metabolic disease, after researchers adjusted for age, sex, smoking status, and social deprivation.
Individuals who were overweight but metabolically healthy had a 30% increased risk of ischemic heart disease, 11% increased risk of heart failure, and the same risk of cerebrovascular disease as normal-weight, healthy individuals.
They also saw an increasing risk of ischemic heart disease, cerebrovascular disease, heart failure, and peripheral vascular disease with each additional metabolic abnormality, even among underweight and normal-weight individuals, and suggested that a focus on screening overweight and obese individuals only could miss metabolic abnormalities in many patients.
Overweight and obese individuals without metabolic disease had a significantly lower risk of peripheral vascular disease, compared with healthy normal-weight individuals. The authors said this was a surprising finding but suggested cigarette smoking could be a confounding factor, as this is associated with both peripheral vascular disease and lower BMI.
“In sensitivity analyses restricted to individuals who were obese with no metabolic abnormalities and reported never smoking cigarettes, risk for PVD [peripheral vascular disease] was increased, compared [with] normal-weight individuals with no metabolic abnormalities,” Dr. Caleyachetty and his coinvestigators wrote.
Over the mean follow-up of 5.4 years, 5.6% of initially metabolically healthy obese individuals developed diabetes, 11.5% developed hyperlipidemia and 10.5% developed hypertension. In contrast, among the metabolically healthy overweight individuals at baseline, 1.9% developed diabetes, 9.4% developed hyperlipidemia, and 7.2% developed hypertension.
While the analysis adjusted for sex, the authors did note that women who were overweight or obese but metabolically healthy had stronger positive associations than did males with cerebrovascular disease and heart failure.
“Clinicians need to be aware that individuals who would otherwise be considered nonobese, based on a normal BMI, can have metabolic abnormalities, and therefore also be at high risk for CVD events,” the investigators concluded.
No conflicts of interest were declared.
Recently, studies have consistently placed metabolically healthy obese individuals between metabolically healthy lean and metabolically unhealthy obese individuals in terms of cardiovascular disease risk, occult cardiac dysfunction, and type 2 diabetes. Thus, either metabolic dysfunction or elevated body mass index appears to increases CVD risk factors.
Often, one or two metabolic risk factors in normal weight individuals are dismissed as unimportant because they are of healthy weight; however, these data suggest that the normal-weight group is at similar risk, compared with overweight, and at times, obese individuals, when metabolic abnormalities are present. The study not only definitively counters the concept of metabolically benign obesity but also demonstrates great risk to normal weight individuals if metabolic dysfunction is present. Thus, we would suggest an increased need for screening in the normal-weight population.
Jennifer W. Bea, PhD, is from the Collaboratory for Metabolic Disease Prevention and Treatment in Tucson, Ariz., and Nancy K. Sweitzer, MD, is chief of the division of cardiology at the Sarver Heart Center. These comments are taken from an accompanying editorial (J Am Coll Cardiol. 2017 Sep 19;70:1438-40. doi. org/10.1016/j.jacc.2017.07.742). No conflicts of interest were declared.
Recently, studies have consistently placed metabolically healthy obese individuals between metabolically healthy lean and metabolically unhealthy obese individuals in terms of cardiovascular disease risk, occult cardiac dysfunction, and type 2 diabetes. Thus, either metabolic dysfunction or elevated body mass index appears to increases CVD risk factors.
Often, one or two metabolic risk factors in normal weight individuals are dismissed as unimportant because they are of healthy weight; however, these data suggest that the normal-weight group is at similar risk, compared with overweight, and at times, obese individuals, when metabolic abnormalities are present. The study not only definitively counters the concept of metabolically benign obesity but also demonstrates great risk to normal weight individuals if metabolic dysfunction is present. Thus, we would suggest an increased need for screening in the normal-weight population.
Jennifer W. Bea, PhD, is from the Collaboratory for Metabolic Disease Prevention and Treatment in Tucson, Ariz., and Nancy K. Sweitzer, MD, is chief of the division of cardiology at the Sarver Heart Center. These comments are taken from an accompanying editorial (J Am Coll Cardiol. 2017 Sep 19;70:1438-40. doi. org/10.1016/j.jacc.2017.07.742). No conflicts of interest were declared.
Recently, studies have consistently placed metabolically healthy obese individuals between metabolically healthy lean and metabolically unhealthy obese individuals in terms of cardiovascular disease risk, occult cardiac dysfunction, and type 2 diabetes. Thus, either metabolic dysfunction or elevated body mass index appears to increases CVD risk factors.
Often, one or two metabolic risk factors in normal weight individuals are dismissed as unimportant because they are of healthy weight; however, these data suggest that the normal-weight group is at similar risk, compared with overweight, and at times, obese individuals, when metabolic abnormalities are present. The study not only definitively counters the concept of metabolically benign obesity but also demonstrates great risk to normal weight individuals if metabolic dysfunction is present. Thus, we would suggest an increased need for screening in the normal-weight population.
Jennifer W. Bea, PhD, is from the Collaboratory for Metabolic Disease Prevention and Treatment in Tucson, Ariz., and Nancy K. Sweitzer, MD, is chief of the division of cardiology at the Sarver Heart Center. These comments are taken from an accompanying editorial (J Am Coll Cardiol. 2017 Sep 19;70:1438-40. doi. org/10.1016/j.jacc.2017.07.742). No conflicts of interest were declared.
Obese individuals with no metabolic abnormalities, such as dyslipidemia, high blood pressure, or high blood sugar levels, still have a higher risk of cardiovascular disease than do metabolically healthy people of normal weight, new data suggests.
“Our study robustly challenges the assertion that MHO [metabolically healthy obese] is a benign condition and adds to the evidence base that MHO is a high-risk state for future CVD events,” wrote Rishi Caleyachetty, MD, of the University of Birmingham, England, and his coauthors online (J Am Coll Cardiol. 2017, Sep 11. doi. 10.1016/j.jacc.2017.07.763).
Dr. Caleyachetty and his associates reported findings from a population-based study using the electronic health records of nearly 3.5 million individuals aged 18 years or older who were free of cardiovascular disease at baseline.
Overall, 15% of the population were classified as being metabolically healthy obese, meaning that they had a body mass index (BMI) of at least 30 kg/m2 with no sign of diabetes, hypertension, or hyperlipidemia, and 26% were overweight with no metabolic abnormalities. Despite their lack of metabolic disease, these obese individuals still had a significant 49% higher risk of coronary heart disease, 7% higher risk of cerebrovascular disease, and 96% higher risk of heart failure, compared with normal-weight individuals with no metabolic disease, after researchers adjusted for age, sex, smoking status, and social deprivation.
Individuals who were overweight but metabolically healthy had a 30% increased risk of ischemic heart disease, 11% increased risk of heart failure, and the same risk of cerebrovascular disease as normal-weight, healthy individuals.
They also saw an increasing risk of ischemic heart disease, cerebrovascular disease, heart failure, and peripheral vascular disease with each additional metabolic abnormality, even among underweight and normal-weight individuals, and suggested that a focus on screening overweight and obese individuals only could miss metabolic abnormalities in many patients.
Overweight and obese individuals without metabolic disease had a significantly lower risk of peripheral vascular disease, compared with healthy normal-weight individuals. The authors said this was a surprising finding but suggested cigarette smoking could be a confounding factor, as this is associated with both peripheral vascular disease and lower BMI.
“In sensitivity analyses restricted to individuals who were obese with no metabolic abnormalities and reported never smoking cigarettes, risk for PVD [peripheral vascular disease] was increased, compared [with] normal-weight individuals with no metabolic abnormalities,” Dr. Caleyachetty and his coinvestigators wrote.
Over the mean follow-up of 5.4 years, 5.6% of initially metabolically healthy obese individuals developed diabetes, 11.5% developed hyperlipidemia and 10.5% developed hypertension. In contrast, among the metabolically healthy overweight individuals at baseline, 1.9% developed diabetes, 9.4% developed hyperlipidemia, and 7.2% developed hypertension.
While the analysis adjusted for sex, the authors did note that women who were overweight or obese but metabolically healthy had stronger positive associations than did males with cerebrovascular disease and heart failure.
“Clinicians need to be aware that individuals who would otherwise be considered nonobese, based on a normal BMI, can have metabolic abnormalities, and therefore also be at high risk for CVD events,” the investigators concluded.
No conflicts of interest were declared.
Obese individuals with no metabolic abnormalities, such as dyslipidemia, high blood pressure, or high blood sugar levels, still have a higher risk of cardiovascular disease than do metabolically healthy people of normal weight, new data suggests.
“Our study robustly challenges the assertion that MHO [metabolically healthy obese] is a benign condition and adds to the evidence base that MHO is a high-risk state for future CVD events,” wrote Rishi Caleyachetty, MD, of the University of Birmingham, England, and his coauthors online (J Am Coll Cardiol. 2017, Sep 11. doi. 10.1016/j.jacc.2017.07.763).
Dr. Caleyachetty and his associates reported findings from a population-based study using the electronic health records of nearly 3.5 million individuals aged 18 years or older who were free of cardiovascular disease at baseline.
Overall, 15% of the population were classified as being metabolically healthy obese, meaning that they had a body mass index (BMI) of at least 30 kg/m2 with no sign of diabetes, hypertension, or hyperlipidemia, and 26% were overweight with no metabolic abnormalities. Despite their lack of metabolic disease, these obese individuals still had a significant 49% higher risk of coronary heart disease, 7% higher risk of cerebrovascular disease, and 96% higher risk of heart failure, compared with normal-weight individuals with no metabolic disease, after researchers adjusted for age, sex, smoking status, and social deprivation.
Individuals who were overweight but metabolically healthy had a 30% increased risk of ischemic heart disease, 11% increased risk of heart failure, and the same risk of cerebrovascular disease as normal-weight, healthy individuals.
They also saw an increasing risk of ischemic heart disease, cerebrovascular disease, heart failure, and peripheral vascular disease with each additional metabolic abnormality, even among underweight and normal-weight individuals, and suggested that a focus on screening overweight and obese individuals only could miss metabolic abnormalities in many patients.
Overweight and obese individuals without metabolic disease had a significantly lower risk of peripheral vascular disease, compared with healthy normal-weight individuals. The authors said this was a surprising finding but suggested cigarette smoking could be a confounding factor, as this is associated with both peripheral vascular disease and lower BMI.
“In sensitivity analyses restricted to individuals who were obese with no metabolic abnormalities and reported never smoking cigarettes, risk for PVD [peripheral vascular disease] was increased, compared [with] normal-weight individuals with no metabolic abnormalities,” Dr. Caleyachetty and his coinvestigators wrote.
Over the mean follow-up of 5.4 years, 5.6% of initially metabolically healthy obese individuals developed diabetes, 11.5% developed hyperlipidemia and 10.5% developed hypertension. In contrast, among the metabolically healthy overweight individuals at baseline, 1.9% developed diabetes, 9.4% developed hyperlipidemia, and 7.2% developed hypertension.
While the analysis adjusted for sex, the authors did note that women who were overweight or obese but metabolically healthy had stronger positive associations than did males with cerebrovascular disease and heart failure.
“Clinicians need to be aware that individuals who would otherwise be considered nonobese, based on a normal BMI, can have metabolic abnormalities, and therefore also be at high risk for CVD events,” the investigators concluded.
No conflicts of interest were declared.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Obese individuals without any sign of metabolic disease, such as hypertension or dyslipidemia, still have a greater risk of cardiovascular disease than do normal weight individuals.
Major finding: Metabolically healthy obese individuals have a 49% higher risk of coronary heart disease and 96% higher risk of heart failure than metabolically healthy normal weight individuals.
Data source: Population-based electronic health record study of 3.5 million people.
Disclosures: No conflicts of interest were declared.
ASCO issues guideline on communication with patients
Recommendations for improved communication between oncologists and their patients are the focus of a new guideline issued by a panel convened by the American Society of Clinical Oncology (ASCO).
The guideline recommends that oncologists establish care goals with each patient, address the costs of care, and initiate discussion of end-of-life preferences early in the course of incurable disease.
Patients also should be made aware of all treatment options, which may include clinical trials and, for certain patients, palliative care alone, the panel recommended.
The ASCO Expert Panel included medical oncologists, psychiatrists, nurses, and experts in hospice and palliative medicine, communication skills, health disparities, and advocacy. Their consensus-based, patient-clinician communication guideline drew on the panel’s systematic evaluation of guidelines, reviews and meta-analyses, and randomized, controlled trials published from 2006 through Oct. 1, 2016.
More specifics on the guideline are available here and feedback can be provided at asco.org/guidelineswiki.
Dr. Gilligan of the Taussig Cancer Institute and the Center for Excellence in Healthcare Communication, Cleveland Clinic, disclosed support from WellPoint; other panel members disclosed various consultancy roles or funding from pharmaceutical companies and CVS Health.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Recommendations for improved communication between oncologists and their patients are the focus of a new guideline issued by a panel convened by the American Society of Clinical Oncology (ASCO).
The guideline recommends that oncologists establish care goals with each patient, address the costs of care, and initiate discussion of end-of-life preferences early in the course of incurable disease.
Patients also should be made aware of all treatment options, which may include clinical trials and, for certain patients, palliative care alone, the panel recommended.
The ASCO Expert Panel included medical oncologists, psychiatrists, nurses, and experts in hospice and palliative medicine, communication skills, health disparities, and advocacy. Their consensus-based, patient-clinician communication guideline drew on the panel’s systematic evaluation of guidelines, reviews and meta-analyses, and randomized, controlled trials published from 2006 through Oct. 1, 2016.
More specifics on the guideline are available here and feedback can be provided at asco.org/guidelineswiki.
Dr. Gilligan of the Taussig Cancer Institute and the Center for Excellence in Healthcare Communication, Cleveland Clinic, disclosed support from WellPoint; other panel members disclosed various consultancy roles or funding from pharmaceutical companies and CVS Health.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Recommendations for improved communication between oncologists and their patients are the focus of a new guideline issued by a panel convened by the American Society of Clinical Oncology (ASCO).
The guideline recommends that oncologists establish care goals with each patient, address the costs of care, and initiate discussion of end-of-life preferences early in the course of incurable disease.
Patients also should be made aware of all treatment options, which may include clinical trials and, for certain patients, palliative care alone, the panel recommended.
The ASCO Expert Panel included medical oncologists, psychiatrists, nurses, and experts in hospice and palliative medicine, communication skills, health disparities, and advocacy. Their consensus-based, patient-clinician communication guideline drew on the panel’s systematic evaluation of guidelines, reviews and meta-analyses, and randomized, controlled trials published from 2006 through Oct. 1, 2016.
More specifics on the guideline are available here and feedback can be provided at asco.org/guidelineswiki.
Dr. Gilligan of the Taussig Cancer Institute and the Center for Excellence in Healthcare Communication, Cleveland Clinic, disclosed support from WellPoint; other panel members disclosed various consultancy roles or funding from pharmaceutical companies and CVS Health.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Learn how to manage your patients’ behavior problems
One of the presentations you’ll definitely want to attend is Dr. Barbara J. Howard’s “As Easy as A-B-C-G: Office Management of Behavior Problems in Children.”
She’ll teach you the A, B, C, and G of managing behavior problems:
- A = Antecedents/meaning
- B = Behavior
- C = Consequences
- G = Gap in skills
Dr. Howard, an assistant professor of pediatrics at the Johns Hopkins University, Baltimore, will use case presentations to show you how this model works in detail. She’ll describe how best to organize a session with a patient, how to engage the family, and how to approach the objectives of family interviewing.
Dr. Howard goes into much more detail, giving examples in each case, explaining how to assist the parent-child relationship, providing parents with bypass strategies for various issues, and teaching behavior modification for dysfunctional patterns.
That is just one case presentation. Others detail how to handle a toddler who refuses to go to bed, an aggressive 5-year-old, a clingy 9-year-old suffering from anxiety, and a 12-year-old who has recently begun wetting the bed and stealing from her mother.
At the American Academy of Pediatrics’ annual meeting in Chicago, Dr. Howard will be presenting Sunday, Sept. 17, from 4 p.m. to 5:30 p.m., and Monday, Sept. 18, from 8:30 a.m. to 10 a.m. You don’t want to miss it!
One of the presentations you’ll definitely want to attend is Dr. Barbara J. Howard’s “As Easy as A-B-C-G: Office Management of Behavior Problems in Children.”
She’ll teach you the A, B, C, and G of managing behavior problems:
- A = Antecedents/meaning
- B = Behavior
- C = Consequences
- G = Gap in skills
Dr. Howard, an assistant professor of pediatrics at the Johns Hopkins University, Baltimore, will use case presentations to show you how this model works in detail. She’ll describe how best to organize a session with a patient, how to engage the family, and how to approach the objectives of family interviewing.
Dr. Howard goes into much more detail, giving examples in each case, explaining how to assist the parent-child relationship, providing parents with bypass strategies for various issues, and teaching behavior modification for dysfunctional patterns.
That is just one case presentation. Others detail how to handle a toddler who refuses to go to bed, an aggressive 5-year-old, a clingy 9-year-old suffering from anxiety, and a 12-year-old who has recently begun wetting the bed and stealing from her mother.
At the American Academy of Pediatrics’ annual meeting in Chicago, Dr. Howard will be presenting Sunday, Sept. 17, from 4 p.m. to 5:30 p.m., and Monday, Sept. 18, from 8:30 a.m. to 10 a.m. You don’t want to miss it!
One of the presentations you’ll definitely want to attend is Dr. Barbara J. Howard’s “As Easy as A-B-C-G: Office Management of Behavior Problems in Children.”
She’ll teach you the A, B, C, and G of managing behavior problems:
- A = Antecedents/meaning
- B = Behavior
- C = Consequences
- G = Gap in skills
Dr. Howard, an assistant professor of pediatrics at the Johns Hopkins University, Baltimore, will use case presentations to show you how this model works in detail. She’ll describe how best to organize a session with a patient, how to engage the family, and how to approach the objectives of family interviewing.
Dr. Howard goes into much more detail, giving examples in each case, explaining how to assist the parent-child relationship, providing parents with bypass strategies for various issues, and teaching behavior modification for dysfunctional patterns.
That is just one case presentation. Others detail how to handle a toddler who refuses to go to bed, an aggressive 5-year-old, a clingy 9-year-old suffering from anxiety, and a 12-year-old who has recently begun wetting the bed and stealing from her mother.
At the American Academy of Pediatrics’ annual meeting in Chicago, Dr. Howard will be presenting Sunday, Sept. 17, from 4 p.m. to 5:30 p.m., and Monday, Sept. 18, from 8:30 a.m. to 10 a.m. You don’t want to miss it!
Ethics in compulsory treatment of patients with severe mental illness
“Ethics is knowing the difference between what you have a right to do and what is right to do.”
– Potter Stewart, U.S. Supreme Court Justice
An understanding of the difference between what is allowed or even recommended and what is ethical often is contemplated in the treatment of mental illness. Mental illnesses can impair judgment in patients confronted with complex decisions about their treatment. A provider, therefore, has to make a decision between respecting autonomy and/or engaging in what may be considered beneficent. While the line separating beneficent care and the respect for the autonomy of a patient may not be present, the question often arises – especially in inpatient care of patients with severe mental illness.

In the inpatient units, I was taught to justify and be mindful of any removal of someone’s right. I learned the responsibility of stripping someone’s freedom. Not only would I find myself preventing someone from going where they wanted or from talking to whomever they wanted, but frequently, we involuntary injected patients with neuroactive chemicals. Those measures are used only in extreme circumstances: In most states, one has to be unable to provide themselves with food, clothing, or shelter secondary to mental illness to be subjected to such aggressive treatment.
Currently, the United States is seeing an increase in the focus on providing more treatment: an emphasis on beneficence over autonomy. This change can be witnessed in the passage of compulsory outpatient treatment laws. Those rulings, such as Laura’s Law in California and Kendra’s Law in New York, have been promoted in response to an increased concern over the consequences of untreated mental illness in crime. In this commentary, I present a case where I felt that despite being given the right and expectation to involuntary treat someone, I did not feel that it was ethical to involuntarily medicate him. (I have made appropriate changes to the patient’s case to maintain confidentiality.)
Our facility
The Psychiatric Stabilization Unit (PSU) of the San Diego Jails is a 30-bed acute psychiatric unit. We serve the 4,500 male inmates and one of the largest mental health systems in the county. The vast majority (from 70% to 90% at any one time) of patients suffer from a psychotic illness, and more than 50% have a comorbid substance use disorder. Contrary to most inpatient units, we do not have pressure from insurance or utilization review to regularly change dosages or medications, and we do not have significant pressure to discharge patients within a certain time frame. The unit serves very disenfranchised patients with most being homeless prior to their arrest and many having no emergency contact or social support of any sort. The unit is staffed by one attending psychiatrist and two therapists. We are subjected to the same involuntary commitment and involuntary medication laws as are community psychiatric hospitals, but we get a significant number of patients under court orders.
The patient presented in this case came under such court order for restoration of his competency to stand trial. In the United States, one cannot stand trial unless competent. Competency is defined as one’s ability to take a meaningful or active part in a trial, the capacity to understand laws, the capacity to understand personal responsibility, the ability to express a plea, and the capability to instruct legal counsel. When patients are found incompetent, they commonly get court ordered to an unit like the PSU with a court order that they cannot understand the risk, benefits, and alternatives of psychotropic treatment and thus can be involuntarily medicated. Often, including in this case, the court order will mention that the patient will not become competent without treatment, including involuntary antipsychotics.
Overview of the case
George is a 50-year-old white male without psychiatric history. He had never been hospitalized psychiatrically voluntarily or involuntarily. He has never engaged in outpatient psychiatric care, has never taken psychotropic medication, and has never been diagnosed with mental illness. He mentions no prior episode of self-harm, suicidality, or suicide attempt. He occasionally drinks alcohol and has smoked marijuana on a few occasions. He despises other drugs, saying that they are “dangerous.” He mentions that his parents had “difficult personalities” but denies any knowledge of them having formal mental illness.
He was born in rural Louisiana to a British mother and an American father. His parents divorced while he was in preschool. His mother remarried, to a salesman, which required them to move frequently to different states for his work. He mentions having performed moderately in school, but poor grades were secondary to his “boredom.” He graduated high school and went to vocational school in technological manufacturing but was unable to graduate. He has since held a series of low-level jobs in retail and janitorial services. He mentions having been in romantic relationships, but when asked to elaborate, he is unable to name any past girlfriends or describe any past relationships. Nonetheless, he describes a wide array of social supports with many friends, though it must be noted that all of his friends have some form of mental illness or intellectual disability.
At this time, he lives with his friend Harry. Harry has a moderate form of autism. George helps him with everything from grocery shopping to financial matters to assistance in personal hygiene. In exchange, Harry provides him with housing that he inherited and financial assistance from his disability benefits. They have lived in the same home for 2 years, since Harry asked George to move in because of concern that he would lose his home over the unsanitary conditions that were present at that time.
George had never been arrested prior to this incarceration. The circumstances of his arrest are unusual. After a neighbor had made complaints that Harry and George were illegally lodging in Harry’s home, the city investigated the matter. George’s report was that Harry was unable to fill out the forms appropriately and was asked to present himself in court. George came along for moral support but became extremely upset when lawyers and judges asked his friend to answer questions he did not have the cognitive ability to answer. Without second thought, George voiced his anger but was asked to remain quiet while not on the stand. He was asked to remain seated and was demanded to follow orders. A few moments later, George was arrested for contempt of court and obstruction to an officer.
Once incarcerated, he declined having any mental illness or needing any treatment during the customary triage visit. He had no problem as an inmate and was never referred to psychiatric services. However, when meeting with his public defender, George derailed into delusions. He talked about how the cops had been conspiring against him all of his life, with his current incarceration as a culmination. He mentioned how the judge was purposely trying to get them evicted so that he could own the house himself. He asked his lawyer to countersue the judge for a violation of his rights. The public defender filed for a competency evaluation of his client.
The forensic psychiatrist evaluated the patient and had a similar interpretation. This was a patient who had delusions and was perseverating on them to the point of being unable to engage in meaningful work with his attorney. The psychiatrist recommended involuntary treatment with an antipsychotic after diagnosing the patient with a psychotic illness.
My interactions with George
George is a loud and bucolic man with an usual mix of Southern idioms, a slightly British accent, and East Coast humor. He insisted on telling me why he wanted the staff to refer to him by his Native American nickname prior to the start our interview. He then asked me to listen to his life story to understand why Harry meant so much to him. Despite recounting their truly meaningful relationship, his affect was odd with poor reactivity; he had an incongruent and somewhat ungenuine joyfulness.
Once I heard his account of their friendship, I asked him about his charges and the incident in the courtroom. His answer was a long diatribe about the wrongs that had been done to him, but most of his speech was a series of illogical delusions. I informed him of my thoughts about his fixed and false beliefs, but he was not able to understand my comments. Nonetheless, I felt that he related to me well and that we had established good rapport.
As I was informing him about the antipsychotic I had chosen for his involuntary treatment, he asked me to hold off. He asked me to consider working with him for some time without medications. After all, he did not believe that he had a mental illness and wanted to attempt to engage in the competency training with our therapist without being medicated.
My conceptualization of him
George is a peculiar case. Practically all patients who are committed to my unit for competency restoration are psychotic, and their psychosis prevents their engagement with their attorneys. They have poor insight into their illness, which leads to their commitment. On admission, I confirm the assessment of the forensic psychiatrist and start the ordered involuntary treatment on patients. Many of them are gravely disabled – making the ethical dilemma easier to navigate. For other patients, the idea that they will be kept incarcerated until found competent also makes the forced treatment a simpler decision.
George was different – his impeccable grooming, his dislike of jail food, and his request for appropriately fitting jail clothes were far from disorganized. More importantly, however, he had adequate shelter outside of jail, income for assisting Harry, and a rich network of friends. Despite being riddled with delusions, his thought process was linear, and he was redirectable – even when discussing his delusions. I conceptualized the ethical conflict as such: Not treating him might lead to a longer period of incompetence and a longer incarceration; treating him would go against his desire to remain untreated.
After contacting Harry, I was fairly certain that George had suffered from his delusions for at least a significant part of his adult life, if not in its entirety. However, Harry was infinitely thankful for George’s assistance and felt that George had a good life. This added another fundamental question: Would forcing George to engage in formal mental health treatment lead him to have a better life? He was happy, had meaningful relationships, and contributed to his life as well as his friends’ lives in a deep way.
I diagnosed him as having an unspecified psychotic disorder, likely schizophrenia; he had delusions and negative symptoms, like his impaired affect. Despite this diagnosis, I decided to hold off from using involuntary treatment. I met with him daily for more than 2 weeks, and we discussed his story, his feelings, and his beliefs. On occasion, it was hard to separate the delusions from justifiable anger at the system. He had felt that he and Harry had been wronged, when society should have protected their vulnerability. He learned to trust me, and his therapist taught him competency training. Despite a possible 1-year commitment, we declared him competent to stand trial in 2 weeks. He had learned and excelled in all facets of the training.
George still had delusions, but he understood his charges, that he had acted inappropriately in the courtroom, and how to discuss his case with his legal counsel. Harry found George to be at his baseline during visits. George acted appropriately; he followed the complex rules set on inmates and engaged in all groups that are held on the unit.
Discussion
I certainly do not question the value of involuntary psychiatric treatment for many patients with grave disabilities, violent tendencies, or incompetence. However, George’s case makes me wonder if many people living with schizophrenia can have rich and meaningful lives without ever being in contact with a mental health provider. I wonder if our almost-obsessive attention to antipsychotics makes us lose sight. Our biological reductionism may lead us to see patients such as George as someone with overactive dopaminergic pathways in need of antidopaminergic antipsychotic. Unfortunately for many, biological reductionism often is based on unsubstantiated evidence.
George reminds me that life, including schizophrenia, is more interesting and complicated than a set of genes, pathways, neurons, or neurotransmitters. Our patients’ lives may be convoluted with delusions, often stemming from truth or impaired affects, which are nonetheless genuine. I don’t know what will happen to George, but his past 50 years suggest that he will continue to have friends, and he will continue to live without being impaired by his delusions. Strangely, I worry less about him than many of my other patients.
Many mental health providers have advocated for a wider and easier access to involuntarily medicate our patients. I think that there is a misguided belief that involuntary antipsychotic treatment will lead to a rise in their use. However, if Carl Rogers, PhD, and others were right in stating that our relationship with our patients was the ultimate factor in their recovery, at what cost are we willing to jeopardize this? My fear is that this cost will be the loss of trust, which is so necessary in treatment. I hope that my short relationship with George did not scare him from ever seeing a psychiatrist again. In some ways, I suspect that by simply listening to George and withholding forced treatment, he will be more inclined to seek treatment in the future.
Take-home points
- Certain patients with psychosis have fairly high functioning.
- Milieu therapy is, in certain cases, able to assuage some symptoms of psychosis.
- Compulsory antipsychotic administration may not be ethical in certain cases of acute psychosis.
- Biological reductionism may undermine a complete ethical understanding of psychosis.
- Psychiatric disorders are etiologically complex and multifactorial.
- Involuntary treatment may provide short-term gains, but prevent long-term trust between patient and provider.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre also mentors several residents on projects, including reduction in the use of solitary confinement of patients with mental illness, reduction in the use of involuntary treatment of the mentally ill, and examination of the mentally ill offender.
“Ethics is knowing the difference between what you have a right to do and what is right to do.”
– Potter Stewart, U.S. Supreme Court Justice
An understanding of the difference between what is allowed or even recommended and what is ethical often is contemplated in the treatment of mental illness. Mental illnesses can impair judgment in patients confronted with complex decisions about their treatment. A provider, therefore, has to make a decision between respecting autonomy and/or engaging in what may be considered beneficent. While the line separating beneficent care and the respect for the autonomy of a patient may not be present, the question often arises – especially in inpatient care of patients with severe mental illness.
In the inpatient units, I was taught to justify and be mindful of any removal of someone’s right. I learned the responsibility of stripping someone’s freedom. Not only would I find myself preventing someone from going where they wanted or from talking to whomever they wanted, but frequently, we involuntary injected patients with neuroactive chemicals. Those measures are used only in extreme circumstances: In most states, one has to be unable to provide themselves with food, clothing, or shelter secondary to mental illness to be subjected to such aggressive treatment.
Currently, the United States is seeing an increase in the focus on providing more treatment: an emphasis on beneficence over autonomy. This change can be witnessed in the passage of compulsory outpatient treatment laws. Those rulings, such as Laura’s Law in California and Kendra’s Law in New York, have been promoted in response to an increased concern over the consequences of untreated mental illness in crime. In this commentary, I present a case where I felt that despite being given the right and expectation to involuntary treat someone, I did not feel that it was ethical to involuntarily medicate him. (I have made appropriate changes to the patient’s case to maintain confidentiality.)
Our facility
The Psychiatric Stabilization Unit (PSU) of the San Diego Jails is a 30-bed acute psychiatric unit. We serve the 4,500 male inmates and one of the largest mental health systems in the county. The vast majority (from 70% to 90% at any one time) of patients suffer from a psychotic illness, and more than 50% have a comorbid substance use disorder. Contrary to most inpatient units, we do not have pressure from insurance or utilization review to regularly change dosages or medications, and we do not have significant pressure to discharge patients within a certain time frame. The unit serves very disenfranchised patients with most being homeless prior to their arrest and many having no emergency contact or social support of any sort. The unit is staffed by one attending psychiatrist and two therapists. We are subjected to the same involuntary commitment and involuntary medication laws as are community psychiatric hospitals, but we get a significant number of patients under court orders.
The patient presented in this case came under such court order for restoration of his competency to stand trial. In the United States, one cannot stand trial unless competent. Competency is defined as one’s ability to take a meaningful or active part in a trial, the capacity to understand laws, the capacity to understand personal responsibility, the ability to express a plea, and the capability to instruct legal counsel. When patients are found incompetent, they commonly get court ordered to an unit like the PSU with a court order that they cannot understand the risk, benefits, and alternatives of psychotropic treatment and thus can be involuntarily medicated. Often, including in this case, the court order will mention that the patient will not become competent without treatment, including involuntary antipsychotics.
Overview of the case
George is a 50-year-old white male without psychiatric history. He had never been hospitalized psychiatrically voluntarily or involuntarily. He has never engaged in outpatient psychiatric care, has never taken psychotropic medication, and has never been diagnosed with mental illness. He mentions no prior episode of self-harm, suicidality, or suicide attempt. He occasionally drinks alcohol and has smoked marijuana on a few occasions. He despises other drugs, saying that they are “dangerous.” He mentions that his parents had “difficult personalities” but denies any knowledge of them having formal mental illness.
He was born in rural Louisiana to a British mother and an American father. His parents divorced while he was in preschool. His mother remarried, to a salesman, which required them to move frequently to different states for his work. He mentions having performed moderately in school, but poor grades were secondary to his “boredom.” He graduated high school and went to vocational school in technological manufacturing but was unable to graduate. He has since held a series of low-level jobs in retail and janitorial services. He mentions having been in romantic relationships, but when asked to elaborate, he is unable to name any past girlfriends or describe any past relationships. Nonetheless, he describes a wide array of social supports with many friends, though it must be noted that all of his friends have some form of mental illness or intellectual disability.
At this time, he lives with his friend Harry. Harry has a moderate form of autism. George helps him with everything from grocery shopping to financial matters to assistance in personal hygiene. In exchange, Harry provides him with housing that he inherited and financial assistance from his disability benefits. They have lived in the same home for 2 years, since Harry asked George to move in because of concern that he would lose his home over the unsanitary conditions that were present at that time.
George had never been arrested prior to this incarceration. The circumstances of his arrest are unusual. After a neighbor had made complaints that Harry and George were illegally lodging in Harry’s home, the city investigated the matter. George’s report was that Harry was unable to fill out the forms appropriately and was asked to present himself in court. George came along for moral support but became extremely upset when lawyers and judges asked his friend to answer questions he did not have the cognitive ability to answer. Without second thought, George voiced his anger but was asked to remain quiet while not on the stand. He was asked to remain seated and was demanded to follow orders. A few moments later, George was arrested for contempt of court and obstruction to an officer.
Once incarcerated, he declined having any mental illness or needing any treatment during the customary triage visit. He had no problem as an inmate and was never referred to psychiatric services. However, when meeting with his public defender, George derailed into delusions. He talked about how the cops had been conspiring against him all of his life, with his current incarceration as a culmination. He mentioned how the judge was purposely trying to get them evicted so that he could own the house himself. He asked his lawyer to countersue the judge for a violation of his rights. The public defender filed for a competency evaluation of his client.
The forensic psychiatrist evaluated the patient and had a similar interpretation. This was a patient who had delusions and was perseverating on them to the point of being unable to engage in meaningful work with his attorney. The psychiatrist recommended involuntary treatment with an antipsychotic after diagnosing the patient with a psychotic illness.
My interactions with George
George is a loud and bucolic man with an usual mix of Southern idioms, a slightly British accent, and East Coast humor. He insisted on telling me why he wanted the staff to refer to him by his Native American nickname prior to the start our interview. He then asked me to listen to his life story to understand why Harry meant so much to him. Despite recounting their truly meaningful relationship, his affect was odd with poor reactivity; he had an incongruent and somewhat ungenuine joyfulness.
Once I heard his account of their friendship, I asked him about his charges and the incident in the courtroom. His answer was a long diatribe about the wrongs that had been done to him, but most of his speech was a series of illogical delusions. I informed him of my thoughts about his fixed and false beliefs, but he was not able to understand my comments. Nonetheless, I felt that he related to me well and that we had established good rapport.
As I was informing him about the antipsychotic I had chosen for his involuntary treatment, he asked me to hold off. He asked me to consider working with him for some time without medications. After all, he did not believe that he had a mental illness and wanted to attempt to engage in the competency training with our therapist without being medicated.
My conceptualization of him
George is a peculiar case. Practically all patients who are committed to my unit for competency restoration are psychotic, and their psychosis prevents their engagement with their attorneys. They have poor insight into their illness, which leads to their commitment. On admission, I confirm the assessment of the forensic psychiatrist and start the ordered involuntary treatment on patients. Many of them are gravely disabled – making the ethical dilemma easier to navigate. For other patients, the idea that they will be kept incarcerated until found competent also makes the forced treatment a simpler decision.
George was different – his impeccable grooming, his dislike of jail food, and his request for appropriately fitting jail clothes were far from disorganized. More importantly, however, he had adequate shelter outside of jail, income for assisting Harry, and a rich network of friends. Despite being riddled with delusions, his thought process was linear, and he was redirectable – even when discussing his delusions. I conceptualized the ethical conflict as such: Not treating him might lead to a longer period of incompetence and a longer incarceration; treating him would go against his desire to remain untreated.
After contacting Harry, I was fairly certain that George had suffered from his delusions for at least a significant part of his adult life, if not in its entirety. However, Harry was infinitely thankful for George’s assistance and felt that George had a good life. This added another fundamental question: Would forcing George to engage in formal mental health treatment lead him to have a better life? He was happy, had meaningful relationships, and contributed to his life as well as his friends’ lives in a deep way.
I diagnosed him as having an unspecified psychotic disorder, likely schizophrenia; he had delusions and negative symptoms, like his impaired affect. Despite this diagnosis, I decided to hold off from using involuntary treatment. I met with him daily for more than 2 weeks, and we discussed his story, his feelings, and his beliefs. On occasion, it was hard to separate the delusions from justifiable anger at the system. He had felt that he and Harry had been wronged, when society should have protected their vulnerability. He learned to trust me, and his therapist taught him competency training. Despite a possible 1-year commitment, we declared him competent to stand trial in 2 weeks. He had learned and excelled in all facets of the training.
George still had delusions, but he understood his charges, that he had acted inappropriately in the courtroom, and how to discuss his case with his legal counsel. Harry found George to be at his baseline during visits. George acted appropriately; he followed the complex rules set on inmates and engaged in all groups that are held on the unit.
Discussion
I certainly do not question the value of involuntary psychiatric treatment for many patients with grave disabilities, violent tendencies, or incompetence. However, George’s case makes me wonder if many people living with schizophrenia can have rich and meaningful lives without ever being in contact with a mental health provider. I wonder if our almost-obsessive attention to antipsychotics makes us lose sight. Our biological reductionism may lead us to see patients such as George as someone with overactive dopaminergic pathways in need of antidopaminergic antipsychotic. Unfortunately for many, biological reductionism often is based on unsubstantiated evidence.
George reminds me that life, including schizophrenia, is more interesting and complicated than a set of genes, pathways, neurons, or neurotransmitters. Our patients’ lives may be convoluted with delusions, often stemming from truth or impaired affects, which are nonetheless genuine. I don’t know what will happen to George, but his past 50 years suggest that he will continue to have friends, and he will continue to live without being impaired by his delusions. Strangely, I worry less about him than many of my other patients.
Many mental health providers have advocated for a wider and easier access to involuntarily medicate our patients. I think that there is a misguided belief that involuntary antipsychotic treatment will lead to a rise in their use. However, if Carl Rogers, PhD, and others were right in stating that our relationship with our patients was the ultimate factor in their recovery, at what cost are we willing to jeopardize this? My fear is that this cost will be the loss of trust, which is so necessary in treatment. I hope that my short relationship with George did not scare him from ever seeing a psychiatrist again. In some ways, I suspect that by simply listening to George and withholding forced treatment, he will be more inclined to seek treatment in the future.
Take-home points
- Certain patients with psychosis have fairly high functioning.
- Milieu therapy is, in certain cases, able to assuage some symptoms of psychosis.
- Compulsory antipsychotic administration may not be ethical in certain cases of acute psychosis.
- Biological reductionism may undermine a complete ethical understanding of psychosis.
- Psychiatric disorders are etiologically complex and multifactorial.
- Involuntary treatment may provide short-term gains, but prevent long-term trust between patient and provider.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre also mentors several residents on projects, including reduction in the use of solitary confinement of patients with mental illness, reduction in the use of involuntary treatment of the mentally ill, and examination of the mentally ill offender.
“Ethics is knowing the difference between what you have a right to do and what is right to do.”
– Potter Stewart, U.S. Supreme Court Justice
An understanding of the difference between what is allowed or even recommended and what is ethical often is contemplated in the treatment of mental illness. Mental illnesses can impair judgment in patients confronted with complex decisions about their treatment. A provider, therefore, has to make a decision between respecting autonomy and/or engaging in what may be considered beneficent. While the line separating beneficent care and the respect for the autonomy of a patient may not be present, the question often arises – especially in inpatient care of patients with severe mental illness.
In the inpatient units, I was taught to justify and be mindful of any removal of someone’s right. I learned the responsibility of stripping someone’s freedom. Not only would I find myself preventing someone from going where they wanted or from talking to whomever they wanted, but frequently, we involuntary injected patients with neuroactive chemicals. Those measures are used only in extreme circumstances: In most states, one has to be unable to provide themselves with food, clothing, or shelter secondary to mental illness to be subjected to such aggressive treatment.
Currently, the United States is seeing an increase in the focus on providing more treatment: an emphasis on beneficence over autonomy. This change can be witnessed in the passage of compulsory outpatient treatment laws. Those rulings, such as Laura’s Law in California and Kendra’s Law in New York, have been promoted in response to an increased concern over the consequences of untreated mental illness in crime. In this commentary, I present a case where I felt that despite being given the right and expectation to involuntary treat someone, I did not feel that it was ethical to involuntarily medicate him. (I have made appropriate changes to the patient’s case to maintain confidentiality.)
Our facility
The Psychiatric Stabilization Unit (PSU) of the San Diego Jails is a 30-bed acute psychiatric unit. We serve the 4,500 male inmates and one of the largest mental health systems in the county. The vast majority (from 70% to 90% at any one time) of patients suffer from a psychotic illness, and more than 50% have a comorbid substance use disorder. Contrary to most inpatient units, we do not have pressure from insurance or utilization review to regularly change dosages or medications, and we do not have significant pressure to discharge patients within a certain time frame. The unit serves very disenfranchised patients with most being homeless prior to their arrest and many having no emergency contact or social support of any sort. The unit is staffed by one attending psychiatrist and two therapists. We are subjected to the same involuntary commitment and involuntary medication laws as are community psychiatric hospitals, but we get a significant number of patients under court orders.
The patient presented in this case came under such court order for restoration of his competency to stand trial. In the United States, one cannot stand trial unless competent. Competency is defined as one’s ability to take a meaningful or active part in a trial, the capacity to understand laws, the capacity to understand personal responsibility, the ability to express a plea, and the capability to instruct legal counsel. When patients are found incompetent, they commonly get court ordered to an unit like the PSU with a court order that they cannot understand the risk, benefits, and alternatives of psychotropic treatment and thus can be involuntarily medicated. Often, including in this case, the court order will mention that the patient will not become competent without treatment, including involuntary antipsychotics.
Overview of the case
George is a 50-year-old white male without psychiatric history. He had never been hospitalized psychiatrically voluntarily or involuntarily. He has never engaged in outpatient psychiatric care, has never taken psychotropic medication, and has never been diagnosed with mental illness. He mentions no prior episode of self-harm, suicidality, or suicide attempt. He occasionally drinks alcohol and has smoked marijuana on a few occasions. He despises other drugs, saying that they are “dangerous.” He mentions that his parents had “difficult personalities” but denies any knowledge of them having formal mental illness.
He was born in rural Louisiana to a British mother and an American father. His parents divorced while he was in preschool. His mother remarried, to a salesman, which required them to move frequently to different states for his work. He mentions having performed moderately in school, but poor grades were secondary to his “boredom.” He graduated high school and went to vocational school in technological manufacturing but was unable to graduate. He has since held a series of low-level jobs in retail and janitorial services. He mentions having been in romantic relationships, but when asked to elaborate, he is unable to name any past girlfriends or describe any past relationships. Nonetheless, he describes a wide array of social supports with many friends, though it must be noted that all of his friends have some form of mental illness or intellectual disability.
At this time, he lives with his friend Harry. Harry has a moderate form of autism. George helps him with everything from grocery shopping to financial matters to assistance in personal hygiene. In exchange, Harry provides him with housing that he inherited and financial assistance from his disability benefits. They have lived in the same home for 2 years, since Harry asked George to move in because of concern that he would lose his home over the unsanitary conditions that were present at that time.
George had never been arrested prior to this incarceration. The circumstances of his arrest are unusual. After a neighbor had made complaints that Harry and George were illegally lodging in Harry’s home, the city investigated the matter. George’s report was that Harry was unable to fill out the forms appropriately and was asked to present himself in court. George came along for moral support but became extremely upset when lawyers and judges asked his friend to answer questions he did not have the cognitive ability to answer. Without second thought, George voiced his anger but was asked to remain quiet while not on the stand. He was asked to remain seated and was demanded to follow orders. A few moments later, George was arrested for contempt of court and obstruction to an officer.
Once incarcerated, he declined having any mental illness or needing any treatment during the customary triage visit. He had no problem as an inmate and was never referred to psychiatric services. However, when meeting with his public defender, George derailed into delusions. He talked about how the cops had been conspiring against him all of his life, with his current incarceration as a culmination. He mentioned how the judge was purposely trying to get them evicted so that he could own the house himself. He asked his lawyer to countersue the judge for a violation of his rights. The public defender filed for a competency evaluation of his client.
The forensic psychiatrist evaluated the patient and had a similar interpretation. This was a patient who had delusions and was perseverating on them to the point of being unable to engage in meaningful work with his attorney. The psychiatrist recommended involuntary treatment with an antipsychotic after diagnosing the patient with a psychotic illness.
My interactions with George
George is a loud and bucolic man with an usual mix of Southern idioms, a slightly British accent, and East Coast humor. He insisted on telling me why he wanted the staff to refer to him by his Native American nickname prior to the start our interview. He then asked me to listen to his life story to understand why Harry meant so much to him. Despite recounting their truly meaningful relationship, his affect was odd with poor reactivity; he had an incongruent and somewhat ungenuine joyfulness.
Once I heard his account of their friendship, I asked him about his charges and the incident in the courtroom. His answer was a long diatribe about the wrongs that had been done to him, but most of his speech was a series of illogical delusions. I informed him of my thoughts about his fixed and false beliefs, but he was not able to understand my comments. Nonetheless, I felt that he related to me well and that we had established good rapport.
As I was informing him about the antipsychotic I had chosen for his involuntary treatment, he asked me to hold off. He asked me to consider working with him for some time without medications. After all, he did not believe that he had a mental illness and wanted to attempt to engage in the competency training with our therapist without being medicated.
My conceptualization of him
George is a peculiar case. Practically all patients who are committed to my unit for competency restoration are psychotic, and their psychosis prevents their engagement with their attorneys. They have poor insight into their illness, which leads to their commitment. On admission, I confirm the assessment of the forensic psychiatrist and start the ordered involuntary treatment on patients. Many of them are gravely disabled – making the ethical dilemma easier to navigate. For other patients, the idea that they will be kept incarcerated until found competent also makes the forced treatment a simpler decision.
George was different – his impeccable grooming, his dislike of jail food, and his request for appropriately fitting jail clothes were far from disorganized. More importantly, however, he had adequate shelter outside of jail, income for assisting Harry, and a rich network of friends. Despite being riddled with delusions, his thought process was linear, and he was redirectable – even when discussing his delusions. I conceptualized the ethical conflict as such: Not treating him might lead to a longer period of incompetence and a longer incarceration; treating him would go against his desire to remain untreated.
After contacting Harry, I was fairly certain that George had suffered from his delusions for at least a significant part of his adult life, if not in its entirety. However, Harry was infinitely thankful for George’s assistance and felt that George had a good life. This added another fundamental question: Would forcing George to engage in formal mental health treatment lead him to have a better life? He was happy, had meaningful relationships, and contributed to his life as well as his friends’ lives in a deep way.
I diagnosed him as having an unspecified psychotic disorder, likely schizophrenia; he had delusions and negative symptoms, like his impaired affect. Despite this diagnosis, I decided to hold off from using involuntary treatment. I met with him daily for more than 2 weeks, and we discussed his story, his feelings, and his beliefs. On occasion, it was hard to separate the delusions from justifiable anger at the system. He had felt that he and Harry had been wronged, when society should have protected their vulnerability. He learned to trust me, and his therapist taught him competency training. Despite a possible 1-year commitment, we declared him competent to stand trial in 2 weeks. He had learned and excelled in all facets of the training.
George still had delusions, but he understood his charges, that he had acted inappropriately in the courtroom, and how to discuss his case with his legal counsel. Harry found George to be at his baseline during visits. George acted appropriately; he followed the complex rules set on inmates and engaged in all groups that are held on the unit.
Discussion
I certainly do not question the value of involuntary psychiatric treatment for many patients with grave disabilities, violent tendencies, or incompetence. However, George’s case makes me wonder if many people living with schizophrenia can have rich and meaningful lives without ever being in contact with a mental health provider. I wonder if our almost-obsessive attention to antipsychotics makes us lose sight. Our biological reductionism may lead us to see patients such as George as someone with overactive dopaminergic pathways in need of antidopaminergic antipsychotic. Unfortunately for many, biological reductionism often is based on unsubstantiated evidence.
George reminds me that life, including schizophrenia, is more interesting and complicated than a set of genes, pathways, neurons, or neurotransmitters. Our patients’ lives may be convoluted with delusions, often stemming from truth or impaired affects, which are nonetheless genuine. I don’t know what will happen to George, but his past 50 years suggest that he will continue to have friends, and he will continue to live without being impaired by his delusions. Strangely, I worry less about him than many of my other patients.
Many mental health providers have advocated for a wider and easier access to involuntarily medicate our patients. I think that there is a misguided belief that involuntary antipsychotic treatment will lead to a rise in their use. However, if Carl Rogers, PhD, and others were right in stating that our relationship with our patients was the ultimate factor in their recovery, at what cost are we willing to jeopardize this? My fear is that this cost will be the loss of trust, which is so necessary in treatment. I hope that my short relationship with George did not scare him from ever seeing a psychiatrist again. In some ways, I suspect that by simply listening to George and withholding forced treatment, he will be more inclined to seek treatment in the future.
Take-home points
- Certain patients with psychosis have fairly high functioning.
- Milieu therapy is, in certain cases, able to assuage some symptoms of psychosis.
- Compulsory antipsychotic administration may not be ethical in certain cases of acute psychosis.
- Biological reductionism may undermine a complete ethical understanding of psychosis.
- Psychiatric disorders are etiologically complex and multifactorial.
- Involuntary treatment may provide short-term gains, but prevent long-term trust between patient and provider.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre also mentors several residents on projects, including reduction in the use of solitary confinement of patients with mental illness, reduction in the use of involuntary treatment of the mentally ill, and examination of the mentally ill offender.
CREST syndrome and PBC are often associated
Primary biliary cholangitis can be associated with limited cutaneous systemic sclerosis (CREST syndrome), according to a clinical communication to the editor from Amirali Kiyani, MD, and Shannon Ursu, MD.
In their case study, a 56-year-old woman presented to the emergency department with a syncopal episode. The patient’s medical history included primary biliary cholangitis (PBC), breast cancer status post lumpectomy and chemoradiation, gastroesophageal reflux disease, Raynaud’s phenomenon, and multiple episodes of gastrointestinal bleeding. Vital signs were normal at the time of admission.
After examination and testing, the patient was found to have low serum complement levels and elevated C-reactive protein. Anti-Scl 70 antibody, SSA, and SSB antibody were negative, and thyroid-stimulating hormone and antitransglutaminase antibodies were normal. No evidence of heart failure or pulmonary hypertension was seen in a transthoracic echocardiogram, and the patient was diagnosed with limited cutaneous systemic sclerosis.
Sjögren’s syndrome and autoimmune thyroiditis are the most common extrahepatic autoimmune disorders associated with PBC, but PBC is associated with CREST syndrome in 1%-6% of cases, according to the literature the investigators reviewed, they said.
“Primary biliary cholangitis is commonly associated with extrahepatic autoimmune disorders such as limited cutaneous systemic sclerosis. … Screening for these autoimmune disorders can prevent further morbidity and keep patients viable candidates for liver transplant,” they concluded.
Find the full clinical communication in the American Journal of Medicine (doi: 10.1016/j.amjmed.2017.05.019).
This story was updated on 9/13/2017.
Primary biliary cholangitis can be associated with limited cutaneous systemic sclerosis (CREST syndrome), according to a clinical communication to the editor from Amirali Kiyani, MD, and Shannon Ursu, MD.
In their case study, a 56-year-old woman presented to the emergency department with a syncopal episode. The patient’s medical history included primary biliary cholangitis (PBC), breast cancer status post lumpectomy and chemoradiation, gastroesophageal reflux disease, Raynaud’s phenomenon, and multiple episodes of gastrointestinal bleeding. Vital signs were normal at the time of admission.
After examination and testing, the patient was found to have low serum complement levels and elevated C-reactive protein. Anti-Scl 70 antibody, SSA, and SSB antibody were negative, and thyroid-stimulating hormone and antitransglutaminase antibodies were normal. No evidence of heart failure or pulmonary hypertension was seen in a transthoracic echocardiogram, and the patient was diagnosed with limited cutaneous systemic sclerosis.
Sjögren’s syndrome and autoimmune thyroiditis are the most common extrahepatic autoimmune disorders associated with PBC, but PBC is associated with CREST syndrome in 1%-6% of cases, according to the literature the investigators reviewed, they said.
“Primary biliary cholangitis is commonly associated with extrahepatic autoimmune disorders such as limited cutaneous systemic sclerosis. … Screening for these autoimmune disorders can prevent further morbidity and keep patients viable candidates for liver transplant,” they concluded.
Find the full clinical communication in the American Journal of Medicine (doi: 10.1016/j.amjmed.2017.05.019).
This story was updated on 9/13/2017.
Primary biliary cholangitis can be associated with limited cutaneous systemic sclerosis (CREST syndrome), according to a clinical communication to the editor from Amirali Kiyani, MD, and Shannon Ursu, MD.
In their case study, a 56-year-old woman presented to the emergency department with a syncopal episode. The patient’s medical history included primary biliary cholangitis (PBC), breast cancer status post lumpectomy and chemoradiation, gastroesophageal reflux disease, Raynaud’s phenomenon, and multiple episodes of gastrointestinal bleeding. Vital signs were normal at the time of admission.
After examination and testing, the patient was found to have low serum complement levels and elevated C-reactive protein. Anti-Scl 70 antibody, SSA, and SSB antibody were negative, and thyroid-stimulating hormone and antitransglutaminase antibodies were normal. No evidence of heart failure or pulmonary hypertension was seen in a transthoracic echocardiogram, and the patient was diagnosed with limited cutaneous systemic sclerosis.
Sjögren’s syndrome and autoimmune thyroiditis are the most common extrahepatic autoimmune disorders associated with PBC, but PBC is associated with CREST syndrome in 1%-6% of cases, according to the literature the investigators reviewed, they said.
“Primary biliary cholangitis is commonly associated with extrahepatic autoimmune disorders such as limited cutaneous systemic sclerosis. … Screening for these autoimmune disorders can prevent further morbidity and keep patients viable candidates for liver transplant,” they concluded.
Find the full clinical communication in the American Journal of Medicine (doi: 10.1016/j.amjmed.2017.05.019).
This story was updated on 9/13/2017.
FROM THE AMERICAN JOURNAL OF MEDICINE
Domperidone appears safe galactagogue for mothers and infants
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
EXPERT ANALYSIS FROM TERATOLOGY SOCIETY 2017
Key clinical point:
Major finding: The use of the domperidone reduced the proportion of women using infant formula by an absolute 22%.
Data source: A retrospective study of 985 women who were prescribed domperidone as a galactagogue at the International Breastfeeding Centre in Toronto.
Disclosures: Dr. Madjunkov reported having no financial conflicts of interest related to the study.
Development and Implementation of a Homeless Mobile Medical/Mental Veteran Intervention
Research has consistently identified remarkably high rates of addiction, mental illness, and health problems in the homeless population.1-9 Yet in spite of extensive service needs for these problems, abundant evidence exists of consistent underuse of health care services by homeless populations.10-12 Most of the homeless population reside in emergency shelters or in transitional or supportive housing, but many remain in places not meant for human habitation.
Homelessness is significantly overrepresented among military veterans.13 The January 2016 national point-in-time count identified 39,471 veterans experiencing homelessness.13 Iraq and Afghanistan veterans seem to have an especially high risk for homelessness.13-15 Disheartening statistics such as these prompted former VA Secretary Eric Shinseki to pledge to end veteran homelessness by December 2015.16 He argued in support of this mission that 85% of veteran homeless resources go to health care—implying that homelessness among veterans is primarily a health care issue, which is heavily burdened by substance abuse and other psychiatric and medical illnesses.17
Health care service use has been associated with improved health, mental health, and outcomes among homeless populations.12,18 Unfortunately, access to these services is limited by barriers associated with homelessness, such as transportation or lack of proper identification.19,20 Veterans experiencing homelessness also face these common barriers to health care, and unsheltered veterans especially underutilize VA health care services.21
Housing First—a successful model that places individuals into housing without prerequisites for sobriety, active participation in treatment, or other behavioral accomplishments, such as gainful employment—has not managed yet to place all the disengaged homeless veteran population into stable housing.22 However, the Housing First model, which is based on the individual’s priorities, is consistent with the approach of a new program at the VA North Texas Health Care System (VANTHCS).
The VHA, similar to other health care systems, is engaged in a cultural transformation to convert its health care approach from a traditional medical model to patient-centered care (PCC).23 In this priority area, a strategic objective is for the VHA to partner with each veteran to create a personalized, proactive strategy to optimize health and well-being and when needed provide state-of-the-art disease management. Patient-centered care is designed to address veterans’ specific needs in spiritual, environmental, physical, mental, and social domains and empower veterans to become active participants in their care. Patient-centered care differs from the traditional medical model in that patients are active participants in their treatment, partnering and collaborating with their providers on care that is quality-of-life centered instead of disease centered.23 This model is based on both respect for patients as unique individuals and on the obligation to care for them on their own terms, focused on their self-identified goals and aspirations.24
At VANTHCS, the Homeless Mobile Medical/Mental Veteran (HMMM-V) pilot program was designed to deliver effective health care services to a homeless subpopulation of veterans who historically have been the most difficult to serve—those living in unsheltered environments, such as under bridges and in encampments. The purpose of the HMMM-V program was to contact and serve veterans not currently being reached by the VA system of care, using a PCC model.
This pilot program was initially funded in January 2013 by a 2-year grant from the Office of Patient Centered Care and Cultural Transformation to apply the PCC approach to engage veteran participation. For this project, the VA Personal Health Inventory tool—originally designed for use with the general veteran population—was adapted for use with the homeless veteran population. The grant funding period covered the design, development, and implementation of the HMMM-V program; thereafter, VANTHCS provided resources through its Comprehensive Homeless Center Programs to assure its sustainability and continued use of the clinical assessment tool created for this project. 
This article describes the development and implementation of this novel program with sufficient detail to inform the development of similar programs in other sites. Descriptions of the program and staffing, creation of community partnerships, and modification of an assessment instrument are provided. It also illustrates the original implementation period of the HMMM-V program through presentation of self-reported data on the first homeless veterans it served.
Equipment and Staffing
A custom 28-foot mobile outreach vehicle was assembled according to specifications identified by the HMMM-V team as necessary to conduct the program’s interventions. The van became fully operational on April 8, 2015, after it underwent all the required reviews and inspections (eg, safety, infection control, etc) and was accredited in 2015 by the Commission on Accreditation of Rehabilitation Facilities.
The HMMM-V van has a driver compartment that is separate from its services rooms, which include a patient registration area, a fully equipped examination room, a laboratory area, and a bathroom. The vehicle is equipped with a wheelchair lift and an awning to shade outdoor areas where tables and chairs are set up for patient/staff waiting and rest areas. The vehicle is stocked with essential equipment and supplies needed to conduct work in off-street locations, vacant lots, under bridges, fields, unpaved paths, etc. It also is equipped with telemedicine capabilities to provide clinical supervision and access to attending physicians and specialists at VANTHCS. Personnel carry cell phones and laptop computers with secure Internet connections using a commercially available mobile wireless Wi-Fi hotspot to facilitate documentation of medical records and communication from the field.
This reliable type of equipment is routine for use in VA field operations; the only hurdle using these technologies for the program was acquiring funding and purchasing the equipment. The vehicle is further equipped with a refrigerator solely for secure storage of pharmaceutical supplies, a second refrigerator for specimens, and wall-mounted blood pressure and otoscope/ophthalmoscope units. The vehicle is supplied with thermometers, scales, phlebotomy supplies, and first-aid kits and is stocked with vaccines and medications, including antibiotic, hypertensive, diabetic, allergy, and over-the-counter pain medications. A more comprehensive list of supplies for the vehicle is available from the authors on request.
Medication provisions supplied to the HMMM-V mobile clinic conform to the Texas State Board of Pharmacy compliance regulations. Because the vehicle is designated as federal property and has U.S. government license plates, it is considered an extension of VANTHCS Pharmacy Service and falls under its pharmacy license. A medication formulary was created with input from HMMM-V prescribers and Dallas VAMC Pharmacy Service pharmacists. To safeguard the integrity of these pharmaceutical agents, the HMMM-V physician assistant picks up the medications before field deployment and returns the unused medications to the Dallas VAMC at the end of the day. The medications are transported in locked containers and placed either in a locked medication refrigerator or cabinet on the mobile unit.
For medication prescriptions that need laboratory testing before prescribing them, HMMM-V prescribers can check the VA electronic medical record from the field to determine whether these tests have been completed recently. If not, then HMMM-V team has an agreement with Dallas VA Pathology and Laboratory Medicine Service for testing samples obtained in the field.
The program was designed for staffing of the vehicle by 2 professional teams, each includes medical (physician’s assistant or registered nurse), mental health (psychiatrist, residents), and social work providers (licensed social workers, clinical social workers); trainees of these disciplines; a peer support specialist; and an administrative clerk. The staffing varies daily, depending on available personnel. When personnel deploy to the field, they go in pairs or groups to address potential safety issues. Cell phones are available to summon police or ambulance services in an emergency. Systematic safety training was conducted with all field personnel before their first deployment to guard against vulnerability to danger in these settings.
Once in the field, personnel engage unsheltered homeless individuals to assess eligibility for VA services. Veterans found ineligible are assisted with application for military discharge upgrade, service-connected compensation, or appeal for health care coverage. Veterans eligible for VA care receive physical examinations, vital and glucose checks, influenza and pneumonia vaccinations, first-aid skin and wound care, medication management with limited medications provided at point of care, blood and urine testing, peer support services, suicide assessments, clinical mental health evaluations, and social work services through the HMMM-V program.
Social work assistance provided includes psychosocial assessment and care coordination for psychosocial needs such as mental health, substance abuse, vision, dental, housing, employment, legal aid, transportation, food, income, hygiene, and weather-appropriate provision needs.
Community Partnerships
The HMMM-V program benefitted from a number of partnerships with community agencies. During development of the program, HMMM-V personnel accompanied the Dallas Police Department’s Crisis Intervention Unit on typical homeless crisis services deployments into the field to learn about the locations and nature of encampments and homeless peregrination patterns in the Dallas area.
To aid in the design and selection of features for the mobile outreach vehicle, team members toured Homeless Outreach Medical Service mobile clinics from 2 local county hospitals, Parkland Hospital and John Peter Smith Hospital. The staff for these mobile clinics were interviewed about their experience with various components of their programs and their recommendations for optimal design of the mobile medical clinic for service delivery.
Numerous agencies in the Dallas area that serve the homeless population assisted with locating and connecting homeless veterans to HMMM-V programs. These partnering agencies also serve homeless individuals who do not qualify for the HMMM-V program, such as veterans with other-than-honorable military discharges.
The HMMM-V mobile outreach vehicle travels to partnering agencies and provides services on a recurring basis. These agencies are the Dallas International Street Church, a church and faith-based agency aiding the recovery of people with “broken lives”; Cornerstone Ministries, a church-based ministry serving people with adverse circumstances; and City Square’s Opportunity Center, human services and community development programs for low-income city residents. The mobile clinic also travels regularly to other areas to serve homeless veterans residing in unsheltered locations, such as homeless encampments and under bridges.
Clinical Assessment
The project used a modification of the VA Personalized Health Inventory (PHI) for general veteran populations, which assesses 8 areas of self-identified needs to address the specific concerns of homeless veterans served by a mobile clinic.25 Version 19 of the PHI (revised September 18, 2012), the version of the instrument available to the team at the inception of the project, was deployed with the HMMM-V personnel into the field. It imposed a heavy interview time burden (several hours), and its content areas did not seem appropriate to address the immediate concerns of homeless populations (eg, sections pertaining to personal development through hobbies, recreation, or volunteering; healthy living spaces with plenty of lighting and color; “eating healthy, balanced meals with plenty of fruits and vegetables each day”).25
Based on HMMM-V personnel feedback, the team modified this tool and developed a patient-centered health inventory (P-CHI) for homeless veterans that was acceptable in length and applicable to the situational characteristics of homeless existence. The tool’s 10 “current and desired states” were revised to remove domains of exercise and flexibility, sleep and relaxation, and mind-body techniques. The intervention and prevention domains were combined. A material needs (clothing, furniture, transportation, financial benefits) domain was added, and a new domain on reducing alcohol/drug use was created by moving this material from the food and drink domain. 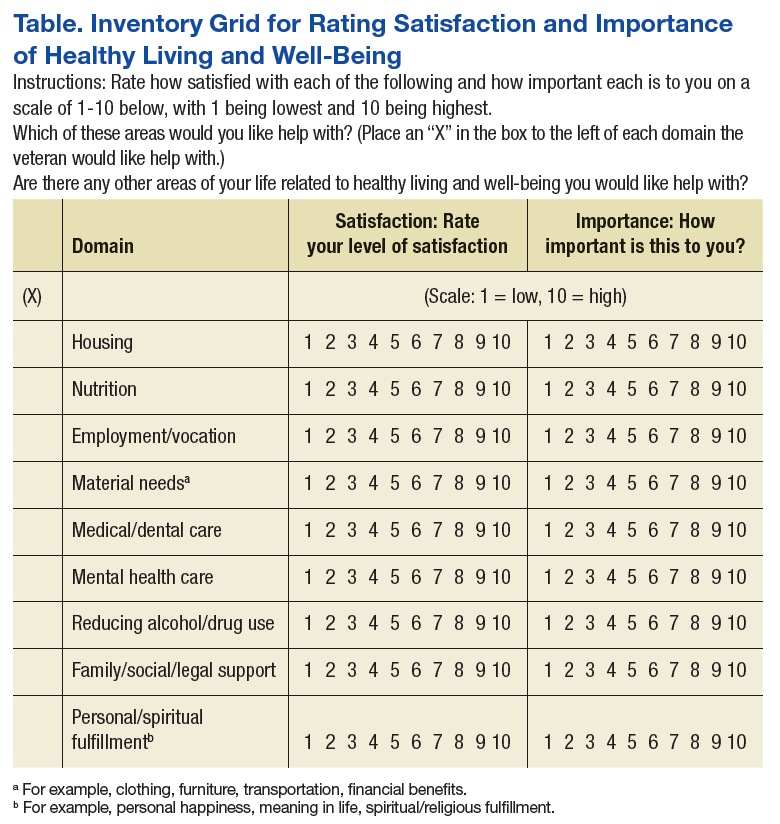
The remaining domains were modified to fit the homeless living situation (Food and Drink = Nutrition; Personal Development = Employment/Vocation; Family, Friends, and Co-Workers = Family/Social/Legal Support; Spirit and Soul = Personal/Spiritual Fulfillment; Surroundings = Housing). Current state ratings were revised to reflect level of satisfaction, and ratings of Desired State were replaced with level of importance.
The modifications resulted in 9 domains, which were assembled into a grid for efficient rating of both satisfaction and importance for each domain (rated 1 to 10, lowest to highest, respectively), followed by an instruction to mark an X in a designated space in all the domains with which the individual would like help (Table). The intent was to reduce the burden of the instrument by having the participant complete sections providing detailed information about only the domains selected by the participant.
The details of each domain in the original VA PHI tool were captured through open-ended questions in text responses provided by the veteran. Because open-ended text responses are not conducive for summarizing characteristics of the population served or for evaluating program activities, the detailed sections covering the domains were revised completely to capture data within categoric and numeric variables. Items from the validated Homeless Supplement Interview were added to collect information not provided in the Homeless Operations Management and Evaluation System interview that is routinely administered to all veterans accessing homeless VA services.26-28
The information collected in these domains cover duration of current homeless episode, lifetime number of homeless episodes, current living arrangements and dissatisfactions with these arrangements, frequency and source of meals, employment history and current work status, sources of income, special material needs, medical and dental problems and sources of care, current medications, mental health problems and sources of care, urgent mental health concerns, current amount and frequency of alcohol and drug use, substance abuse treatment history, relationships with family and intimate partners, legal assistance needs, and self-identified needs for spiritual and personal fulfillment. This instrument is available on request to the authors.
Veterans Served
The project began with 1 team of professionals deploying with the HMMM-V vehicle while a second team was being assembled. Currently, the 2 HMMM-V teams deploy the mobile clinic 4 days per week. The mobile clinic visits agencies that serve the homeless, including emergency shelters and food ministries, as well as homeless encampments. To date, 195 homeless veterans have been served by the mobile clinic, 111 were currently enrolled with the VA, 8 were not enrolled but eligible for services, and 77 were not eligible for VA services. Of the unenrolled veterans, those eligible for services were offered VA enrollment assistance; those ineligible for VA services were offered a community referral.
For the veterans encountered in the field, the following interventions were provided: 49 housing placement referrals, 4 rental assistance referrals, 4 legal referrals, 27 medical care interventions, 13 dental referrals, 11 vision/hearing referrals, 12 mental health interventions, 9 substance abuse treatment referrals, 14 employment assistance referrals, 13 disability benefit applications, 18 transportation assists, 23 goods delivered, and 159 information assists. The HMMM-V mobile clinic also is deployed to participate in various educational and outreach events. At the time this article was written, the mobile clinic has reached nearly 2,000 veterans and community partners in at least 25 such events.
Of the veterans served to date, 73 completed the P-CHI. These veterans were predominantly male (77%), and the majority (60%) were black. The median age of the sample was 58 years, and typically they had a high school level of education (12.7; SD, 2.1 mean years of education). About half (49%) the sample were separated or divorced, and only a minority were currently married (8%). Half (50%) the sample served in the U.S. Army, with the post-Vietnam era being the era of service most represented (19%). Few (21%) veterans reported exposure to hostile or friendly fire during their service. More than three-fourths (80%) of the sample had experienced a homeless episode prior to their current one. On average, members of the sample had experienced a median of 3 lifetime homeless episodes. They had a mean 4.1 (SD, 5.8) lifetime number of years of homelessness, and 3.0 (SD, 5.2) years in their current homeless episode. Nearly one-third (31%) reported that they were currently staying in a homeless shelter, and nearly one-sixth (16%) were currently unsheltered in street settings, such as under bridges or in outdoor encampments at the time of the initial visit.
The mean number of minutes spent completing the P-CHI was 18.5 (SD, 9.4). The veterans indicated that they would like assistance with a mean 3.2 (SD, 2.2) number of domains. The domains with the highest average importance ratings were housing (mean, 9.4; SD, 1.7) and medical/dental care (mean, 8.9; SD, 2.2); the domains with the lowest average importance rating were reducing alcohol/drug use (mean, 6.4; SD, 4.1) and employment/vocation (mean, 6.3; SD, 4.2). The domains with the highest average satisfaction ratings were personal/spiritual fulfillment (mean, 7.3; SD, 2.9) and reducing substance use (mean, 5.9; SD, 4.0), and the domains with the lowest average satisfaction ratings were housing (mean, 2.9; SD, 2.9), material needs (mean, 4.2; SD, 3.3), and employment/vocation (mean, 4.2; SD, 3.2). The domain with the greatest indication of desire for help was housing, endorsed by more than four-fifths (84%) of the sample. This highly endorsed housing domain also was one of the lowest in satisfaction. The domains with the least expressed interest in obtaining help were reducing substance use (18%) and personal/spiritual fulfillment (15%).Reducing substance abuse also was one of the lowest domains of importance and the least for dissatisfaction.
Challenges and Barriers
As anticipated from its inception, this project encountered many challenges and barriers. The first was with the design, construction, and delivery of the mobile clinic unit. The vehicle took more than 2 years to be delivered. There were delays in progress necessitated by required selection of an approved vendor to build the vehicle, extensive specification of details and features, and stocking it with equipment and supplies. The weight of the unit had to be < 26,000 pounds to avoid the requirement of a commercial driver’s license, which limited the size of the vehicle to 28 feet. Stocking the unit with equipment and supplies required attention to a myriad of specifications and decisions. For example, separate refrigerators were needed for specimens, medications, and food; pharmaceutical regulations governing medications in mobile clinics required strict adherence; and difficulties were encountered in attempting to establish adequate and secure connectivity for communications devices in the field. 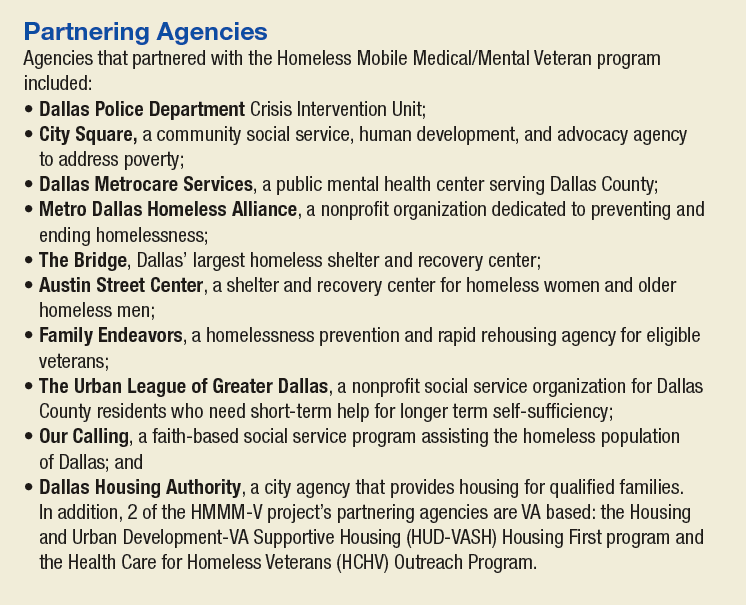
Once the mobile unit was delivered and prepared for deployment, the next set of challenges pertained to learning all of the instructions required to operate and drive the vehicle and learning how to maneuver the vehicle in the field. Specific challenges for driving the vehicle encountered included unexpectedly low overpasses that prohibited passage, narrow spaces for passage, rough and uneven terrain in off-road settings, and lateral and vertical tilt of roads creating potential for sideswipes and undercarriage scrapes. Maintenance schedules needed to be developed and implemented for cleaning the unit, inspection compliance, repairs, refueling, and emptying waste materials.
Staffing the vehicle required the development of unique job specifications addressing special expertise in accessing VA databases for veteran verification and registration and for driving the mobile clinic vehicle. Schedules and deployment plans for 2 teams that shared the same vehicle had to be established and followed. Locating veterans in unsheltered settings, such as under bridges and in encampments, required community intelligence facilitated through partnerships with knowledgeable members of the Dallas police crisis unit and by gaining field experience to locate where the usual homeless gathering places are, especially those inhabited by veterans. Safety of team members and equipment/supplies in the field was paramount from the start, and additional steps beyond safety training required extra measures, such as special care in navigating known dangerous areas. Provision of services necessitated completion of everything needed in a single visit due to the likelihood of loss to follow-up and acceptance of the limited types of service that could be provided in a mobile clinic. Special procedures were needed to provide referrals to sources of available care for non-VA-qualifying veterans.
Discussion
The HMMM-V program for delivery of PCC to homeless veterans is an innovative pilot program designed to connect with difficult-to-reach homeless veterans and engage them in care. The deliverables provided by this project are (1) A mobile outreach vehicle to deliver care to homeless veterans and outreach to other veterans and community agencies in North Texas; (2) The P-CHI assessment tool for homeless veterans modified and adapted for use with this special population; and (3) pilot data on its first cohort of homeless veterans served, describing their baseline characteristics and their stated satisfaction and preferences about their goals and aspirations for their physical, emotional, and mental health and well-being.
The HMMM-V program successfully identified homeless veterans in need of services, and more than one-third of these veterans were not previously engaged in VA services. Compared with the “typical” veterans served at VANTHCS homeless programs, veterans served by the HMMM-V comprised a greater proportion of minorities and a higher proportion who had been exposed to combat.29 Age and gender characteristics were similar.29 When compared with veterans who access care at VANTHCS and have not experienced homelessness, those served by the HMMM-V were younger and more likely to belong to a minority group; however, they were similar in combat exposure and gender.1 The veterans served by the HMMM-V program also were considerably older and had more homeless chronicity than did nonveteran homeless populations, consistent with other research.4,29,30
The veterans served by the HMMM-V program not surprisingly made housing their top priority in need of help, consistent with the Housing First model.22,31 They also indicated that employment/vocation and reducing substance use were of lower importance. Need for assistance with reducing substance use and social support were the domains least often identified as areas where help was needed, which seems inconsistent with the higher established rates of substance abuse problems among homeless veterans.1
With additional fieldwork, the HMMM-V program is expected to allow refinement of procedures for identifying and serving veterans from a patient-centered care perspective. The P-CHI will be further tested and developed, and the next step will be to create and pilot intervention templates for a Patient-Centered Health Improvement Plan, based on the P-CHI results. This process parallels the original development treatment plans for the VA’s Personalized Health Plan based on the PHI.25 Once the HMMM-V program is fully established in Dallas, the plans are for an expansion that will cover a broader geographic area in North Texas that includes rural areas.
The HMMM-V program was designed to address the barriers to health care that are encountered by homeless veterans. It is unique in homeless veteran care due to its patient-centered approach that partners with homeless veterans to prioritize their needs as determined by them rather than based solely on policies or provider conceptualizations of their needs. Access to services, engagement in care, and successful utilization of needed services may lead to measurable improvements in health care outcomes among homeless populations of veterans. Desired goals include remission of illness through appropriate medical intervention, preventing morbidity, achieving healthy lifestyles, recovery from addiction, stabilization of psychiatric illness, and attainment of stable housing.
The first hurdle for implementing this type of program in other settings is the identification of resources needed for these efforts. Need of additional staffing resources, however, may be circumvented by allowing employees working in other areas to rotate in community outreach shifts in the mobile unit. Another hurdle encountered in implementation of the HMMM-V initiative was the initial difficulty finding homeless veterans in community settings, especially those in unsheltered locations. The HMMM-V program addressed this issue by partnering with other agencies serving the homeless in the community. Therefore, a general recommendation for other entities seeking to implement this type of program is to reach out to these community partners from the outset.
Conclusion
The HMMM-V has the potential to engage the most difficult-to-reach homeless veterans in need of health services by delivering care and providing resources in challenging environments. Further work is needed to validate the P-CHI for use with this program and to conduct well-designed and implemented research to demonstrate effectiveness of this intervention on veteran outcomes, especially quality of life. Once this additional work is accomplished, this innovative program can potentially be implemented by VAMCs across the nation, and potentially in more general community care settings, to more effectively reach out and deliver services to homeless members of the community.
Acknowledgments
Grant support was received from the Department of Veterans Affairs, Office of Patient Centered Care. The authors would like to acknowledge all the clinicians, trainees, and support staff who have contributed to the success of the HMMM-V program: Tara Ayala, Jose Cabrera, Tony Castillo, Rachael Lynn David, Teresa DeShazo, Sylvia Figueroa, Steven Fisher, Eric Gary, Evelyn Gibbs, Kevin Hosey, JoAnn Joseph, Taly Drimer Kagan, Miranda Kelly, Michelle King-Thompson, Sharon Marcus, Shiji Mathew, Moneeza Matin, John Moreno, Joseph Neifert, Joel Price, Tiffany Price, Natalie Qualls, Reginald Robertson, Kristine Rodrigues, Jon Saffelder, Jill Stokes, Scott Stone, and John Smith.
1. LePage JP, Bradshaw LD, Cipher DJ, Crawford AM, Hooshyar D. The effects of homelessness on veterans’ health care service use: an evaluation of independence from comorbidities. Public Health. 2014;128(11):985-992.
2. Fischer PJ, Breakey WR. The epidemiology of alcohol, drug, and mental disorders among homeless persons. Am Psychol. 1991;46(11):1115-1128.
3. Robertson MJ, Zlotnick C, Westerfelt A. Drug use disorders and treatment contact among homeless adults in Alameda County, California. Am J Public Health. 1997;87(2):221-228.
4. North CS, Eyrich KM, Pollio DE, Spitznagel EL. Are rates of psychiatric disorders in the homeless population changing? Am J Public Health. 2004;94(1):103-108.
5. Fazel S, Khosla V, Doll H, Geddes J. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. PLoS Med. 2008;5(12):e225.
6. Harpaz-Rotem I, Rosenheck RA, Desai R. The mental health of children exposed to maternal mental illness and homelessness. Community Ment Health J. 2006;42(5):437-448.
7. Pollio DE, Eyrich-Garg KM, North CS. The homeless. In: Johnson BA, ed. Addiction Medicine: Science and Practice. New York, NY: Springer; 2011:1487-1504.
8. Padgett D, Struening EL, Andrews H. Factors affecting the use of medical, mental health, alcohol, and drug treatment services by homeless adults. Med Care. 1990;28(9):805-821.
9. Baggett TP, Singer DE, Rao SR, O’Connell JJ, Bharel M, Rigotti NA. Food insufficiency and health services utilization in a national sample of homeless adults. J Gen Intern Med. 2011;26(6):627-634.
10. Folsom DP, Hawthorne W, Lindamer L, et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry. 2005;162(2):370-376.
11. Fuehrlein BS, Cowell AJ, Pollio D, Cupps L, Balfour ME, North CS. A prospective study of the associations among housing status and costs of services in a homeless population. Psychiatr Serv. 2015;66(1):27-32.
12. Pollio DE, North CS, Eyrich KM, Foster DA, Spitznagel E. Modeling service access in a homeless population. J Psychoactive Drugs. 2003;35(4):487-495.
13. U.S. Department of Housing and Urban Development Office of Community Planning and Development. The 2016 Annual Homeless Assessment Report (AHAR) to Congress. Part 1: point-in-time estimates of homelessness. https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Published 2016. Accessed August 7, 2017.
14. Tsai J, Rosenheck RA. Risk factors for homelessness among U.S. veterans. Epidemiol Rev. 2015;37:177-195.
15. Williamson V, Mulhall E. Coming home: the housing crisis and homelessness threaten new veterans. Iraq and Afghanistan Veterans of America, January, 2009. http://media.iava.org/IAVA_coming_home_2009%20The%20Housing%20Crisis%20and%20Homelessness%20Threaten%20New%20Veterans.pdf. Accessed August 10, 2017
16. Shinseki EK. Remarks by Secretary Eric K. Shinseki. National Summit on Homeless Veterans; November 3, 2009; Washington, DC. https://www.va.gov/opa/speeches/2009/09_1103.asp. Updated August 8, 2016. Accessed August 7, 2017.
17. Shinseki EK. Remarks by Secretary Eric K. Shinseki. 2014 National Coalition for Homeless Veterans Annual Meeting; May 30, 2014; Arlington, VA. https://www.va.gov/opa/speeches/2014/05_30_2014.asp. Updated April 21, 2015. Accessed August 7, 2017.
18. Pollio DE, Spitznagel EL, North CS, Thompson S, Foster DA. Service use over time and achievement of stable housing in a mentally ill homeless population. Psychiatr Serv. 2000;51(12):1536-1543.
19. Page J. Barriers to transferring care of homeless people with serious mental illnesses to community mental health organizations: perspectives of street-based programs. Best Practices in Mental Health: An International Journal. 2007;3(1):26.
20. Young AS, Chinman MJ, Cradock-O’Leary JA, et al. Characteristics of individuals with severe mental illness who use emergency services. Community Ment Health J. 2005;41(2):159-168.
21. Gabrielian S, Yuan AH, Andersen RM, Rubenstein LV, Gelberg L. VA health service utilization for homeless and low-income veterans: a spotlight on the VA Supportive Housing (VASH) program in greater Los Angeles. Med Care. 2014;52(5):454-461.
22. Tsemberis S, Gulcur L, Nakae M. Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. Am J Public Health. 2004;94(4):651-656.
23. U.S. Department of Veterans Affairs, Veterans Health Administration. VA Patient Centered Care. http://www.va.gov/patientcenteredcare. Updated July 24,2017. Accessed August 7, 2017.
24. Epstein RM, Street RL Jr. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100-103.
25. U.S. Department of Veterans Affairs, Office of Patient Centered Care and Cultural Transformation. My story: personal health inventory. https://www.va.gov/PATIENTCENTEREDCARE/docs/VA-OPCC-Personal-Health-Inventory-final-508.pdf. Published October 7, 2013. Accessed August 7, 2017
26. North CS, Smith EM, Pollio DE. The Homeless Supplement to the Diagnostic Interview Schedule (DIS/HS). St. Louis: Washington University, 2004.
27. North CS, Eyrich KM, Pollio DE, Foster DA, Cottler LB, Spitznagel EL. The homeless supplement to the diagnostic interview schedule: test-retest analyses. Int J Methods Psychiatr Res. 2004;13(3):184-191.
28. LaSalle JL. Homeless Operations Management and Evaluation System (HOMES) user manual-phase 1. http://www.vfwsc.org/homes.pdf. Published April 19, 2011. Accessed August 7, 2017.
29. Petrovich JC, Pollio DE, North CS. Characteristics and service use of homeless veterans and nonveterans residing in a low-demand emergency shelter. Psychiatr Serv. 2014;65(6):751-757.
30. North CS, Smith EM. A comparison of homeless men and women: different populations, different needs. Community Ment Health J. 1993;29(5):423-431.
31. Kertesz SG, Austin EL, Holmes SK, et al. Making housing first happen: organizational leadership in VA’s expansion of permanent supportive housing. J Gen Intern Med. 2014;29(suppl 4):835-844.
Research has consistently identified remarkably high rates of addiction, mental illness, and health problems in the homeless population.1-9 Yet in spite of extensive service needs for these problems, abundant evidence exists of consistent underuse of health care services by homeless populations.10-12 Most of the homeless population reside in emergency shelters or in transitional or supportive housing, but many remain in places not meant for human habitation.
Homelessness is significantly overrepresented among military veterans.13 The January 2016 national point-in-time count identified 39,471 veterans experiencing homelessness.13 Iraq and Afghanistan veterans seem to have an especially high risk for homelessness.13-15 Disheartening statistics such as these prompted former VA Secretary Eric Shinseki to pledge to end veteran homelessness by December 2015.16 He argued in support of this mission that 85% of veteran homeless resources go to health care—implying that homelessness among veterans is primarily a health care issue, which is heavily burdened by substance abuse and other psychiatric and medical illnesses.17
Health care service use has been associated with improved health, mental health, and outcomes among homeless populations.12,18 Unfortunately, access to these services is limited by barriers associated with homelessness, such as transportation or lack of proper identification.19,20 Veterans experiencing homelessness also face these common barriers to health care, and unsheltered veterans especially underutilize VA health care services.21
Housing First—a successful model that places individuals into housing without prerequisites for sobriety, active participation in treatment, or other behavioral accomplishments, such as gainful employment—has not managed yet to place all the disengaged homeless veteran population into stable housing.22 However, the Housing First model, which is based on the individual’s priorities, is consistent with the approach of a new program at the VA North Texas Health Care System (VANTHCS).
The VHA, similar to other health care systems, is engaged in a cultural transformation to convert its health care approach from a traditional medical model to patient-centered care (PCC).23 In this priority area, a strategic objective is for the VHA to partner with each veteran to create a personalized, proactive strategy to optimize health and well-being and when needed provide state-of-the-art disease management. Patient-centered care is designed to address veterans’ specific needs in spiritual, environmental, physical, mental, and social domains and empower veterans to become active participants in their care. Patient-centered care differs from the traditional medical model in that patients are active participants in their treatment, partnering and collaborating with their providers on care that is quality-of-life centered instead of disease centered.23 This model is based on both respect for patients as unique individuals and on the obligation to care for them on their own terms, focused on their self-identified goals and aspirations.24
At VANTHCS, the Homeless Mobile Medical/Mental Veteran (HMMM-V) pilot program was designed to deliver effective health care services to a homeless subpopulation of veterans who historically have been the most difficult to serve—those living in unsheltered environments, such as under bridges and in encampments. The purpose of the HMMM-V program was to contact and serve veterans not currently being reached by the VA system of care, using a PCC model.
This pilot program was initially funded in January 2013 by a 2-year grant from the Office of Patient Centered Care and Cultural Transformation to apply the PCC approach to engage veteran participation. For this project, the VA Personal Health Inventory tool—originally designed for use with the general veteran population—was adapted for use with the homeless veteran population. The grant funding period covered the design, development, and implementation of the HMMM-V program; thereafter, VANTHCS provided resources through its Comprehensive Homeless Center Programs to assure its sustainability and continued use of the clinical assessment tool created for this project.
This article describes the development and implementation of this novel program with sufficient detail to inform the development of similar programs in other sites. Descriptions of the program and staffing, creation of community partnerships, and modification of an assessment instrument are provided. It also illustrates the original implementation period of the HMMM-V program through presentation of self-reported data on the first homeless veterans it served.
Equipment and Staffing
A custom 28-foot mobile outreach vehicle was assembled according to specifications identified by the HMMM-V team as necessary to conduct the program’s interventions. The van became fully operational on April 8, 2015, after it underwent all the required reviews and inspections (eg, safety, infection control, etc) and was accredited in 2015 by the Commission on Accreditation of Rehabilitation Facilities.
The HMMM-V van has a driver compartment that is separate from its services rooms, which include a patient registration area, a fully equipped examination room, a laboratory area, and a bathroom. The vehicle is equipped with a wheelchair lift and an awning to shade outdoor areas where tables and chairs are set up for patient/staff waiting and rest areas. The vehicle is stocked with essential equipment and supplies needed to conduct work in off-street locations, vacant lots, under bridges, fields, unpaved paths, etc. It also is equipped with telemedicine capabilities to provide clinical supervision and access to attending physicians and specialists at VANTHCS. Personnel carry cell phones and laptop computers with secure Internet connections using a commercially available mobile wireless Wi-Fi hotspot to facilitate documentation of medical records and communication from the field.
This reliable type of equipment is routine for use in VA field operations; the only hurdle using these technologies for the program was acquiring funding and purchasing the equipment. The vehicle is further equipped with a refrigerator solely for secure storage of pharmaceutical supplies, a second refrigerator for specimens, and wall-mounted blood pressure and otoscope/ophthalmoscope units. The vehicle is supplied with thermometers, scales, phlebotomy supplies, and first-aid kits and is stocked with vaccines and medications, including antibiotic, hypertensive, diabetic, allergy, and over-the-counter pain medications. A more comprehensive list of supplies for the vehicle is available from the authors on request.
Medication provisions supplied to the HMMM-V mobile clinic conform to the Texas State Board of Pharmacy compliance regulations. Because the vehicle is designated as federal property and has U.S. government license plates, it is considered an extension of VANTHCS Pharmacy Service and falls under its pharmacy license. A medication formulary was created with input from HMMM-V prescribers and Dallas VAMC Pharmacy Service pharmacists. To safeguard the integrity of these pharmaceutical agents, the HMMM-V physician assistant picks up the medications before field deployment and returns the unused medications to the Dallas VAMC at the end of the day. The medications are transported in locked containers and placed either in a locked medication refrigerator or cabinet on the mobile unit.
For medication prescriptions that need laboratory testing before prescribing them, HMMM-V prescribers can check the VA electronic medical record from the field to determine whether these tests have been completed recently. If not, then HMMM-V team has an agreement with Dallas VA Pathology and Laboratory Medicine Service for testing samples obtained in the field.
The program was designed for staffing of the vehicle by 2 professional teams, each includes medical (physician’s assistant or registered nurse), mental health (psychiatrist, residents), and social work providers (licensed social workers, clinical social workers); trainees of these disciplines; a peer support specialist; and an administrative clerk. The staffing varies daily, depending on available personnel. When personnel deploy to the field, they go in pairs or groups to address potential safety issues. Cell phones are available to summon police or ambulance services in an emergency. Systematic safety training was conducted with all field personnel before their first deployment to guard against vulnerability to danger in these settings.
Once in the field, personnel engage unsheltered homeless individuals to assess eligibility for VA services. Veterans found ineligible are assisted with application for military discharge upgrade, service-connected compensation, or appeal for health care coverage. Veterans eligible for VA care receive physical examinations, vital and glucose checks, influenza and pneumonia vaccinations, first-aid skin and wound care, medication management with limited medications provided at point of care, blood and urine testing, peer support services, suicide assessments, clinical mental health evaluations, and social work services through the HMMM-V program.
Social work assistance provided includes psychosocial assessment and care coordination for psychosocial needs such as mental health, substance abuse, vision, dental, housing, employment, legal aid, transportation, food, income, hygiene, and weather-appropriate provision needs.
Community Partnerships
The HMMM-V program benefitted from a number of partnerships with community agencies. During development of the program, HMMM-V personnel accompanied the Dallas Police Department’s Crisis Intervention Unit on typical homeless crisis services deployments into the field to learn about the locations and nature of encampments and homeless peregrination patterns in the Dallas area.
To aid in the design and selection of features for the mobile outreach vehicle, team members toured Homeless Outreach Medical Service mobile clinics from 2 local county hospitals, Parkland Hospital and John Peter Smith Hospital. The staff for these mobile clinics were interviewed about their experience with various components of their programs and their recommendations for optimal design of the mobile medical clinic for service delivery.
Numerous agencies in the Dallas area that serve the homeless population assisted with locating and connecting homeless veterans to HMMM-V programs. These partnering agencies also serve homeless individuals who do not qualify for the HMMM-V program, such as veterans with other-than-honorable military discharges.
The HMMM-V mobile outreach vehicle travels to partnering agencies and provides services on a recurring basis. These agencies are the Dallas International Street Church, a church and faith-based agency aiding the recovery of people with “broken lives”; Cornerstone Ministries, a church-based ministry serving people with adverse circumstances; and City Square’s Opportunity Center, human services and community development programs for low-income city residents. The mobile clinic also travels regularly to other areas to serve homeless veterans residing in unsheltered locations, such as homeless encampments and under bridges.
Clinical Assessment
The project used a modification of the VA Personalized Health Inventory (PHI) for general veteran populations, which assesses 8 areas of self-identified needs to address the specific concerns of homeless veterans served by a mobile clinic.25 Version 19 of the PHI (revised September 18, 2012), the version of the instrument available to the team at the inception of the project, was deployed with the HMMM-V personnel into the field. It imposed a heavy interview time burden (several hours), and its content areas did not seem appropriate to address the immediate concerns of homeless populations (eg, sections pertaining to personal development through hobbies, recreation, or volunteering; healthy living spaces with plenty of lighting and color; “eating healthy, balanced meals with plenty of fruits and vegetables each day”).25
Based on HMMM-V personnel feedback, the team modified this tool and developed a patient-centered health inventory (P-CHI) for homeless veterans that was acceptable in length and applicable to the situational characteristics of homeless existence. The tool’s 10 “current and desired states” were revised to remove domains of exercise and flexibility, sleep and relaxation, and mind-body techniques. The intervention and prevention domains were combined. A material needs (clothing, furniture, transportation, financial benefits) domain was added, and a new domain on reducing alcohol/drug use was created by moving this material from the food and drink domain.
The remaining domains were modified to fit the homeless living situation (Food and Drink = Nutrition; Personal Development = Employment/Vocation; Family, Friends, and Co-Workers = Family/Social/Legal Support; Spirit and Soul = Personal/Spiritual Fulfillment; Surroundings = Housing). Current state ratings were revised to reflect level of satisfaction, and ratings of Desired State were replaced with level of importance.
The modifications resulted in 9 domains, which were assembled into a grid for efficient rating of both satisfaction and importance for each domain (rated 1 to 10, lowest to highest, respectively), followed by an instruction to mark an X in a designated space in all the domains with which the individual would like help (Table). The intent was to reduce the burden of the instrument by having the participant complete sections providing detailed information about only the domains selected by the participant.
The details of each domain in the original VA PHI tool were captured through open-ended questions in text responses provided by the veteran. Because open-ended text responses are not conducive for summarizing characteristics of the population served or for evaluating program activities, the detailed sections covering the domains were revised completely to capture data within categoric and numeric variables. Items from the validated Homeless Supplement Interview were added to collect information not provided in the Homeless Operations Management and Evaluation System interview that is routinely administered to all veterans accessing homeless VA services.26-28
The information collected in these domains cover duration of current homeless episode, lifetime number of homeless episodes, current living arrangements and dissatisfactions with these arrangements, frequency and source of meals, employment history and current work status, sources of income, special material needs, medical and dental problems and sources of care, current medications, mental health problems and sources of care, urgent mental health concerns, current amount and frequency of alcohol and drug use, substance abuse treatment history, relationships with family and intimate partners, legal assistance needs, and self-identified needs for spiritual and personal fulfillment. This instrument is available on request to the authors.
Veterans Served
The project began with 1 team of professionals deploying with the HMMM-V vehicle while a second team was being assembled. Currently, the 2 HMMM-V teams deploy the mobile clinic 4 days per week. The mobile clinic visits agencies that serve the homeless, including emergency shelters and food ministries, as well as homeless encampments. To date, 195 homeless veterans have been served by the mobile clinic, 111 were currently enrolled with the VA, 8 were not enrolled but eligible for services, and 77 were not eligible for VA services. Of the unenrolled veterans, those eligible for services were offered VA enrollment assistance; those ineligible for VA services were offered a community referral.
For the veterans encountered in the field, the following interventions were provided: 49 housing placement referrals, 4 rental assistance referrals, 4 legal referrals, 27 medical care interventions, 13 dental referrals, 11 vision/hearing referrals, 12 mental health interventions, 9 substance abuse treatment referrals, 14 employment assistance referrals, 13 disability benefit applications, 18 transportation assists, 23 goods delivered, and 159 information assists. The HMMM-V mobile clinic also is deployed to participate in various educational and outreach events. At the time this article was written, the mobile clinic has reached nearly 2,000 veterans and community partners in at least 25 such events.
Of the veterans served to date, 73 completed the P-CHI. These veterans were predominantly male (77%), and the majority (60%) were black. The median age of the sample was 58 years, and typically they had a high school level of education (12.7; SD, 2.1 mean years of education). About half (49%) the sample were separated or divorced, and only a minority were currently married (8%). Half (50%) the sample served in the U.S. Army, with the post-Vietnam era being the era of service most represented (19%). Few (21%) veterans reported exposure to hostile or friendly fire during their service. More than three-fourths (80%) of the sample had experienced a homeless episode prior to their current one. On average, members of the sample had experienced a median of 3 lifetime homeless episodes. They had a mean 4.1 (SD, 5.8) lifetime number of years of homelessness, and 3.0 (SD, 5.2) years in their current homeless episode. Nearly one-third (31%) reported that they were currently staying in a homeless shelter, and nearly one-sixth (16%) were currently unsheltered in street settings, such as under bridges or in outdoor encampments at the time of the initial visit.
The mean number of minutes spent completing the P-CHI was 18.5 (SD, 9.4). The veterans indicated that they would like assistance with a mean 3.2 (SD, 2.2) number of domains. The domains with the highest average importance ratings were housing (mean, 9.4; SD, 1.7) and medical/dental care (mean, 8.9; SD, 2.2); the domains with the lowest average importance rating were reducing alcohol/drug use (mean, 6.4; SD, 4.1) and employment/vocation (mean, 6.3; SD, 4.2). The domains with the highest average satisfaction ratings were personal/spiritual fulfillment (mean, 7.3; SD, 2.9) and reducing substance use (mean, 5.9; SD, 4.0), and the domains with the lowest average satisfaction ratings were housing (mean, 2.9; SD, 2.9), material needs (mean, 4.2; SD, 3.3), and employment/vocation (mean, 4.2; SD, 3.2). The domain with the greatest indication of desire for help was housing, endorsed by more than four-fifths (84%) of the sample. This highly endorsed housing domain also was one of the lowest in satisfaction. The domains with the least expressed interest in obtaining help were reducing substance use (18%) and personal/spiritual fulfillment (15%).Reducing substance abuse also was one of the lowest domains of importance and the least for dissatisfaction.
Challenges and Barriers
As anticipated from its inception, this project encountered many challenges and barriers. The first was with the design, construction, and delivery of the mobile clinic unit. The vehicle took more than 2 years to be delivered. There were delays in progress necessitated by required selection of an approved vendor to build the vehicle, extensive specification of details and features, and stocking it with equipment and supplies. The weight of the unit had to be < 26,000 pounds to avoid the requirement of a commercial driver’s license, which limited the size of the vehicle to 28 feet. Stocking the unit with equipment and supplies required attention to a myriad of specifications and decisions. For example, separate refrigerators were needed for specimens, medications, and food; pharmaceutical regulations governing medications in mobile clinics required strict adherence; and difficulties were encountered in attempting to establish adequate and secure connectivity for communications devices in the field.
Once the mobile unit was delivered and prepared for deployment, the next set of challenges pertained to learning all of the instructions required to operate and drive the vehicle and learning how to maneuver the vehicle in the field. Specific challenges for driving the vehicle encountered included unexpectedly low overpasses that prohibited passage, narrow spaces for passage, rough and uneven terrain in off-road settings, and lateral and vertical tilt of roads creating potential for sideswipes and undercarriage scrapes. Maintenance schedules needed to be developed and implemented for cleaning the unit, inspection compliance, repairs, refueling, and emptying waste materials.
Staffing the vehicle required the development of unique job specifications addressing special expertise in accessing VA databases for veteran verification and registration and for driving the mobile clinic vehicle. Schedules and deployment plans for 2 teams that shared the same vehicle had to be established and followed. Locating veterans in unsheltered settings, such as under bridges and in encampments, required community intelligence facilitated through partnerships with knowledgeable members of the Dallas police crisis unit and by gaining field experience to locate where the usual homeless gathering places are, especially those inhabited by veterans. Safety of team members and equipment/supplies in the field was paramount from the start, and additional steps beyond safety training required extra measures, such as special care in navigating known dangerous areas. Provision of services necessitated completion of everything needed in a single visit due to the likelihood of loss to follow-up and acceptance of the limited types of service that could be provided in a mobile clinic. Special procedures were needed to provide referrals to sources of available care for non-VA-qualifying veterans.
Discussion
The HMMM-V program for delivery of PCC to homeless veterans is an innovative pilot program designed to connect with difficult-to-reach homeless veterans and engage them in care. The deliverables provided by this project are (1) A mobile outreach vehicle to deliver care to homeless veterans and outreach to other veterans and community agencies in North Texas; (2) The P-CHI assessment tool for homeless veterans modified and adapted for use with this special population; and (3) pilot data on its first cohort of homeless veterans served, describing their baseline characteristics and their stated satisfaction and preferences about their goals and aspirations for their physical, emotional, and mental health and well-being.
The HMMM-V program successfully identified homeless veterans in need of services, and more than one-third of these veterans were not previously engaged in VA services. Compared with the “typical” veterans served at VANTHCS homeless programs, veterans served by the HMMM-V comprised a greater proportion of minorities and a higher proportion who had been exposed to combat.29 Age and gender characteristics were similar.29 When compared with veterans who access care at VANTHCS and have not experienced homelessness, those served by the HMMM-V were younger and more likely to belong to a minority group; however, they were similar in combat exposure and gender.1 The veterans served by the HMMM-V program also were considerably older and had more homeless chronicity than did nonveteran homeless populations, consistent with other research.4,29,30
The veterans served by the HMMM-V program not surprisingly made housing their top priority in need of help, consistent with the Housing First model.22,31 They also indicated that employment/vocation and reducing substance use were of lower importance. Need for assistance with reducing substance use and social support were the domains least often identified as areas where help was needed, which seems inconsistent with the higher established rates of substance abuse problems among homeless veterans.1
With additional fieldwork, the HMMM-V program is expected to allow refinement of procedures for identifying and serving veterans from a patient-centered care perspective. The P-CHI will be further tested and developed, and the next step will be to create and pilot intervention templates for a Patient-Centered Health Improvement Plan, based on the P-CHI results. This process parallels the original development treatment plans for the VA’s Personalized Health Plan based on the PHI.25 Once the HMMM-V program is fully established in Dallas, the plans are for an expansion that will cover a broader geographic area in North Texas that includes rural areas.
The HMMM-V program was designed to address the barriers to health care that are encountered by homeless veterans. It is unique in homeless veteran care due to its patient-centered approach that partners with homeless veterans to prioritize their needs as determined by them rather than based solely on policies or provider conceptualizations of their needs. Access to services, engagement in care, and successful utilization of needed services may lead to measurable improvements in health care outcomes among homeless populations of veterans. Desired goals include remission of illness through appropriate medical intervention, preventing morbidity, achieving healthy lifestyles, recovery from addiction, stabilization of psychiatric illness, and attainment of stable housing.
The first hurdle for implementing this type of program in other settings is the identification of resources needed for these efforts. Need of additional staffing resources, however, may be circumvented by allowing employees working in other areas to rotate in community outreach shifts in the mobile unit. Another hurdle encountered in implementation of the HMMM-V initiative was the initial difficulty finding homeless veterans in community settings, especially those in unsheltered locations. The HMMM-V program addressed this issue by partnering with other agencies serving the homeless in the community. Therefore, a general recommendation for other entities seeking to implement this type of program is to reach out to these community partners from the outset.
Conclusion
The HMMM-V has the potential to engage the most difficult-to-reach homeless veterans in need of health services by delivering care and providing resources in challenging environments. Further work is needed to validate the P-CHI for use with this program and to conduct well-designed and implemented research to demonstrate effectiveness of this intervention on veteran outcomes, especially quality of life. Once this additional work is accomplished, this innovative program can potentially be implemented by VAMCs across the nation, and potentially in more general community care settings, to more effectively reach out and deliver services to homeless members of the community.
Acknowledgments
Grant support was received from the Department of Veterans Affairs, Office of Patient Centered Care. The authors would like to acknowledge all the clinicians, trainees, and support staff who have contributed to the success of the HMMM-V program: Tara Ayala, Jose Cabrera, Tony Castillo, Rachael Lynn David, Teresa DeShazo, Sylvia Figueroa, Steven Fisher, Eric Gary, Evelyn Gibbs, Kevin Hosey, JoAnn Joseph, Taly Drimer Kagan, Miranda Kelly, Michelle King-Thompson, Sharon Marcus, Shiji Mathew, Moneeza Matin, John Moreno, Joseph Neifert, Joel Price, Tiffany Price, Natalie Qualls, Reginald Robertson, Kristine Rodrigues, Jon Saffelder, Jill Stokes, Scott Stone, and John Smith.
Research has consistently identified remarkably high rates of addiction, mental illness, and health problems in the homeless population.1-9 Yet in spite of extensive service needs for these problems, abundant evidence exists of consistent underuse of health care services by homeless populations.10-12 Most of the homeless population reside in emergency shelters or in transitional or supportive housing, but many remain in places not meant for human habitation.
Homelessness is significantly overrepresented among military veterans.13 The January 2016 national point-in-time count identified 39,471 veterans experiencing homelessness.13 Iraq and Afghanistan veterans seem to have an especially high risk for homelessness.13-15 Disheartening statistics such as these prompted former VA Secretary Eric Shinseki to pledge to end veteran homelessness by December 2015.16 He argued in support of this mission that 85% of veteran homeless resources go to health care—implying that homelessness among veterans is primarily a health care issue, which is heavily burdened by substance abuse and other psychiatric and medical illnesses.17
Health care service use has been associated with improved health, mental health, and outcomes among homeless populations.12,18 Unfortunately, access to these services is limited by barriers associated with homelessness, such as transportation or lack of proper identification.19,20 Veterans experiencing homelessness also face these common barriers to health care, and unsheltered veterans especially underutilize VA health care services.21
Housing First—a successful model that places individuals into housing without prerequisites for sobriety, active participation in treatment, or other behavioral accomplishments, such as gainful employment—has not managed yet to place all the disengaged homeless veteran population into stable housing.22 However, the Housing First model, which is based on the individual’s priorities, is consistent with the approach of a new program at the VA North Texas Health Care System (VANTHCS).
The VHA, similar to other health care systems, is engaged in a cultural transformation to convert its health care approach from a traditional medical model to patient-centered care (PCC).23 In this priority area, a strategic objective is for the VHA to partner with each veteran to create a personalized, proactive strategy to optimize health and well-being and when needed provide state-of-the-art disease management. Patient-centered care is designed to address veterans’ specific needs in spiritual, environmental, physical, mental, and social domains and empower veterans to become active participants in their care. Patient-centered care differs from the traditional medical model in that patients are active participants in their treatment, partnering and collaborating with their providers on care that is quality-of-life centered instead of disease centered.23 This model is based on both respect for patients as unique individuals and on the obligation to care for them on their own terms, focused on their self-identified goals and aspirations.24
At VANTHCS, the Homeless Mobile Medical/Mental Veteran (HMMM-V) pilot program was designed to deliver effective health care services to a homeless subpopulation of veterans who historically have been the most difficult to serve—those living in unsheltered environments, such as under bridges and in encampments. The purpose of the HMMM-V program was to contact and serve veterans not currently being reached by the VA system of care, using a PCC model.
This pilot program was initially funded in January 2013 by a 2-year grant from the Office of Patient Centered Care and Cultural Transformation to apply the PCC approach to engage veteran participation. For this project, the VA Personal Health Inventory tool—originally designed for use with the general veteran population—was adapted for use with the homeless veteran population. The grant funding period covered the design, development, and implementation of the HMMM-V program; thereafter, VANTHCS provided resources through its Comprehensive Homeless Center Programs to assure its sustainability and continued use of the clinical assessment tool created for this project.
This article describes the development and implementation of this novel program with sufficient detail to inform the development of similar programs in other sites. Descriptions of the program and staffing, creation of community partnerships, and modification of an assessment instrument are provided. It also illustrates the original implementation period of the HMMM-V program through presentation of self-reported data on the first homeless veterans it served.
Equipment and Staffing
A custom 28-foot mobile outreach vehicle was assembled according to specifications identified by the HMMM-V team as necessary to conduct the program’s interventions. The van became fully operational on April 8, 2015, after it underwent all the required reviews and inspections (eg, safety, infection control, etc) and was accredited in 2015 by the Commission on Accreditation of Rehabilitation Facilities.
The HMMM-V van has a driver compartment that is separate from its services rooms, which include a patient registration area, a fully equipped examination room, a laboratory area, and a bathroom. The vehicle is equipped with a wheelchair lift and an awning to shade outdoor areas where tables and chairs are set up for patient/staff waiting and rest areas. The vehicle is stocked with essential equipment and supplies needed to conduct work in off-street locations, vacant lots, under bridges, fields, unpaved paths, etc. It also is equipped with telemedicine capabilities to provide clinical supervision and access to attending physicians and specialists at VANTHCS. Personnel carry cell phones and laptop computers with secure Internet connections using a commercially available mobile wireless Wi-Fi hotspot to facilitate documentation of medical records and communication from the field.
This reliable type of equipment is routine for use in VA field operations; the only hurdle using these technologies for the program was acquiring funding and purchasing the equipment. The vehicle is further equipped with a refrigerator solely for secure storage of pharmaceutical supplies, a second refrigerator for specimens, and wall-mounted blood pressure and otoscope/ophthalmoscope units. The vehicle is supplied with thermometers, scales, phlebotomy supplies, and first-aid kits and is stocked with vaccines and medications, including antibiotic, hypertensive, diabetic, allergy, and over-the-counter pain medications. A more comprehensive list of supplies for the vehicle is available from the authors on request.
Medication provisions supplied to the HMMM-V mobile clinic conform to the Texas State Board of Pharmacy compliance regulations. Because the vehicle is designated as federal property and has U.S. government license plates, it is considered an extension of VANTHCS Pharmacy Service and falls under its pharmacy license. A medication formulary was created with input from HMMM-V prescribers and Dallas VAMC Pharmacy Service pharmacists. To safeguard the integrity of these pharmaceutical agents, the HMMM-V physician assistant picks up the medications before field deployment and returns the unused medications to the Dallas VAMC at the end of the day. The medications are transported in locked containers and placed either in a locked medication refrigerator or cabinet on the mobile unit.
For medication prescriptions that need laboratory testing before prescribing them, HMMM-V prescribers can check the VA electronic medical record from the field to determine whether these tests have been completed recently. If not, then HMMM-V team has an agreement with Dallas VA Pathology and Laboratory Medicine Service for testing samples obtained in the field.
The program was designed for staffing of the vehicle by 2 professional teams, each includes medical (physician’s assistant or registered nurse), mental health (psychiatrist, residents), and social work providers (licensed social workers, clinical social workers); trainees of these disciplines; a peer support specialist; and an administrative clerk. The staffing varies daily, depending on available personnel. When personnel deploy to the field, they go in pairs or groups to address potential safety issues. Cell phones are available to summon police or ambulance services in an emergency. Systematic safety training was conducted with all field personnel before their first deployment to guard against vulnerability to danger in these settings.
Once in the field, personnel engage unsheltered homeless individuals to assess eligibility for VA services. Veterans found ineligible are assisted with application for military discharge upgrade, service-connected compensation, or appeal for health care coverage. Veterans eligible for VA care receive physical examinations, vital and glucose checks, influenza and pneumonia vaccinations, first-aid skin and wound care, medication management with limited medications provided at point of care, blood and urine testing, peer support services, suicide assessments, clinical mental health evaluations, and social work services through the HMMM-V program.
Social work assistance provided includes psychosocial assessment and care coordination for psychosocial needs such as mental health, substance abuse, vision, dental, housing, employment, legal aid, transportation, food, income, hygiene, and weather-appropriate provision needs.
Community Partnerships
The HMMM-V program benefitted from a number of partnerships with community agencies. During development of the program, HMMM-V personnel accompanied the Dallas Police Department’s Crisis Intervention Unit on typical homeless crisis services deployments into the field to learn about the locations and nature of encampments and homeless peregrination patterns in the Dallas area.
To aid in the design and selection of features for the mobile outreach vehicle, team members toured Homeless Outreach Medical Service mobile clinics from 2 local county hospitals, Parkland Hospital and John Peter Smith Hospital. The staff for these mobile clinics were interviewed about their experience with various components of their programs and their recommendations for optimal design of the mobile medical clinic for service delivery.
Numerous agencies in the Dallas area that serve the homeless population assisted with locating and connecting homeless veterans to HMMM-V programs. These partnering agencies also serve homeless individuals who do not qualify for the HMMM-V program, such as veterans with other-than-honorable military discharges.
The HMMM-V mobile outreach vehicle travels to partnering agencies and provides services on a recurring basis. These agencies are the Dallas International Street Church, a church and faith-based agency aiding the recovery of people with “broken lives”; Cornerstone Ministries, a church-based ministry serving people with adverse circumstances; and City Square’s Opportunity Center, human services and community development programs for low-income city residents. The mobile clinic also travels regularly to other areas to serve homeless veterans residing in unsheltered locations, such as homeless encampments and under bridges.
Clinical Assessment
The project used a modification of the VA Personalized Health Inventory (PHI) for general veteran populations, which assesses 8 areas of self-identified needs to address the specific concerns of homeless veterans served by a mobile clinic.25 Version 19 of the PHI (revised September 18, 2012), the version of the instrument available to the team at the inception of the project, was deployed with the HMMM-V personnel into the field. It imposed a heavy interview time burden (several hours), and its content areas did not seem appropriate to address the immediate concerns of homeless populations (eg, sections pertaining to personal development through hobbies, recreation, or volunteering; healthy living spaces with plenty of lighting and color; “eating healthy, balanced meals with plenty of fruits and vegetables each day”).25
Based on HMMM-V personnel feedback, the team modified this tool and developed a patient-centered health inventory (P-CHI) for homeless veterans that was acceptable in length and applicable to the situational characteristics of homeless existence. The tool’s 10 “current and desired states” were revised to remove domains of exercise and flexibility, sleep and relaxation, and mind-body techniques. The intervention and prevention domains were combined. A material needs (clothing, furniture, transportation, financial benefits) domain was added, and a new domain on reducing alcohol/drug use was created by moving this material from the food and drink domain.
The remaining domains were modified to fit the homeless living situation (Food and Drink = Nutrition; Personal Development = Employment/Vocation; Family, Friends, and Co-Workers = Family/Social/Legal Support; Spirit and Soul = Personal/Spiritual Fulfillment; Surroundings = Housing). Current state ratings were revised to reflect level of satisfaction, and ratings of Desired State were replaced with level of importance.
The modifications resulted in 9 domains, which were assembled into a grid for efficient rating of both satisfaction and importance for each domain (rated 1 to 10, lowest to highest, respectively), followed by an instruction to mark an X in a designated space in all the domains with which the individual would like help (Table). The intent was to reduce the burden of the instrument by having the participant complete sections providing detailed information about only the domains selected by the participant.
The details of each domain in the original VA PHI tool were captured through open-ended questions in text responses provided by the veteran. Because open-ended text responses are not conducive for summarizing characteristics of the population served or for evaluating program activities, the detailed sections covering the domains were revised completely to capture data within categoric and numeric variables. Items from the validated Homeless Supplement Interview were added to collect information not provided in the Homeless Operations Management and Evaluation System interview that is routinely administered to all veterans accessing homeless VA services.26-28
The information collected in these domains cover duration of current homeless episode, lifetime number of homeless episodes, current living arrangements and dissatisfactions with these arrangements, frequency and source of meals, employment history and current work status, sources of income, special material needs, medical and dental problems and sources of care, current medications, mental health problems and sources of care, urgent mental health concerns, current amount and frequency of alcohol and drug use, substance abuse treatment history, relationships with family and intimate partners, legal assistance needs, and self-identified needs for spiritual and personal fulfillment. This instrument is available on request to the authors.
Veterans Served
The project began with 1 team of professionals deploying with the HMMM-V vehicle while a second team was being assembled. Currently, the 2 HMMM-V teams deploy the mobile clinic 4 days per week. The mobile clinic visits agencies that serve the homeless, including emergency shelters and food ministries, as well as homeless encampments. To date, 195 homeless veterans have been served by the mobile clinic, 111 were currently enrolled with the VA, 8 were not enrolled but eligible for services, and 77 were not eligible for VA services. Of the unenrolled veterans, those eligible for services were offered VA enrollment assistance; those ineligible for VA services were offered a community referral.
For the veterans encountered in the field, the following interventions were provided: 49 housing placement referrals, 4 rental assistance referrals, 4 legal referrals, 27 medical care interventions, 13 dental referrals, 11 vision/hearing referrals, 12 mental health interventions, 9 substance abuse treatment referrals, 14 employment assistance referrals, 13 disability benefit applications, 18 transportation assists, 23 goods delivered, and 159 information assists. The HMMM-V mobile clinic also is deployed to participate in various educational and outreach events. At the time this article was written, the mobile clinic has reached nearly 2,000 veterans and community partners in at least 25 such events.
Of the veterans served to date, 73 completed the P-CHI. These veterans were predominantly male (77%), and the majority (60%) were black. The median age of the sample was 58 years, and typically they had a high school level of education (12.7; SD, 2.1 mean years of education). About half (49%) the sample were separated or divorced, and only a minority were currently married (8%). Half (50%) the sample served in the U.S. Army, with the post-Vietnam era being the era of service most represented (19%). Few (21%) veterans reported exposure to hostile or friendly fire during their service. More than three-fourths (80%) of the sample had experienced a homeless episode prior to their current one. On average, members of the sample had experienced a median of 3 lifetime homeless episodes. They had a mean 4.1 (SD, 5.8) lifetime number of years of homelessness, and 3.0 (SD, 5.2) years in their current homeless episode. Nearly one-third (31%) reported that they were currently staying in a homeless shelter, and nearly one-sixth (16%) were currently unsheltered in street settings, such as under bridges or in outdoor encampments at the time of the initial visit.
The mean number of minutes spent completing the P-CHI was 18.5 (SD, 9.4). The veterans indicated that they would like assistance with a mean 3.2 (SD, 2.2) number of domains. The domains with the highest average importance ratings were housing (mean, 9.4; SD, 1.7) and medical/dental care (mean, 8.9; SD, 2.2); the domains with the lowest average importance rating were reducing alcohol/drug use (mean, 6.4; SD, 4.1) and employment/vocation (mean, 6.3; SD, 4.2). The domains with the highest average satisfaction ratings were personal/spiritual fulfillment (mean, 7.3; SD, 2.9) and reducing substance use (mean, 5.9; SD, 4.0), and the domains with the lowest average satisfaction ratings were housing (mean, 2.9; SD, 2.9), material needs (mean, 4.2; SD, 3.3), and employment/vocation (mean, 4.2; SD, 3.2). The domain with the greatest indication of desire for help was housing, endorsed by more than four-fifths (84%) of the sample. This highly endorsed housing domain also was one of the lowest in satisfaction. The domains with the least expressed interest in obtaining help were reducing substance use (18%) and personal/spiritual fulfillment (15%).Reducing substance abuse also was one of the lowest domains of importance and the least for dissatisfaction.
Challenges and Barriers
As anticipated from its inception, this project encountered many challenges and barriers. The first was with the design, construction, and delivery of the mobile clinic unit. The vehicle took more than 2 years to be delivered. There were delays in progress necessitated by required selection of an approved vendor to build the vehicle, extensive specification of details and features, and stocking it with equipment and supplies. The weight of the unit had to be < 26,000 pounds to avoid the requirement of a commercial driver’s license, which limited the size of the vehicle to 28 feet. Stocking the unit with equipment and supplies required attention to a myriad of specifications and decisions. For example, separate refrigerators were needed for specimens, medications, and food; pharmaceutical regulations governing medications in mobile clinics required strict adherence; and difficulties were encountered in attempting to establish adequate and secure connectivity for communications devices in the field.
Once the mobile unit was delivered and prepared for deployment, the next set of challenges pertained to learning all of the instructions required to operate and drive the vehicle and learning how to maneuver the vehicle in the field. Specific challenges for driving the vehicle encountered included unexpectedly low overpasses that prohibited passage, narrow spaces for passage, rough and uneven terrain in off-road settings, and lateral and vertical tilt of roads creating potential for sideswipes and undercarriage scrapes. Maintenance schedules needed to be developed and implemented for cleaning the unit, inspection compliance, repairs, refueling, and emptying waste materials.
Staffing the vehicle required the development of unique job specifications addressing special expertise in accessing VA databases for veteran verification and registration and for driving the mobile clinic vehicle. Schedules and deployment plans for 2 teams that shared the same vehicle had to be established and followed. Locating veterans in unsheltered settings, such as under bridges and in encampments, required community intelligence facilitated through partnerships with knowledgeable members of the Dallas police crisis unit and by gaining field experience to locate where the usual homeless gathering places are, especially those inhabited by veterans. Safety of team members and equipment/supplies in the field was paramount from the start, and additional steps beyond safety training required extra measures, such as special care in navigating known dangerous areas. Provision of services necessitated completion of everything needed in a single visit due to the likelihood of loss to follow-up and acceptance of the limited types of service that could be provided in a mobile clinic. Special procedures were needed to provide referrals to sources of available care for non-VA-qualifying veterans.
Discussion
The HMMM-V program for delivery of PCC to homeless veterans is an innovative pilot program designed to connect with difficult-to-reach homeless veterans and engage them in care. The deliverables provided by this project are (1) A mobile outreach vehicle to deliver care to homeless veterans and outreach to other veterans and community agencies in North Texas; (2) The P-CHI assessment tool for homeless veterans modified and adapted for use with this special population; and (3) pilot data on its first cohort of homeless veterans served, describing their baseline characteristics and their stated satisfaction and preferences about their goals and aspirations for their physical, emotional, and mental health and well-being.
The HMMM-V program successfully identified homeless veterans in need of services, and more than one-third of these veterans were not previously engaged in VA services. Compared with the “typical” veterans served at VANTHCS homeless programs, veterans served by the HMMM-V comprised a greater proportion of minorities and a higher proportion who had been exposed to combat.29 Age and gender characteristics were similar.29 When compared with veterans who access care at VANTHCS and have not experienced homelessness, those served by the HMMM-V were younger and more likely to belong to a minority group; however, they were similar in combat exposure and gender.1 The veterans served by the HMMM-V program also were considerably older and had more homeless chronicity than did nonveteran homeless populations, consistent with other research.4,29,30
The veterans served by the HMMM-V program not surprisingly made housing their top priority in need of help, consistent with the Housing First model.22,31 They also indicated that employment/vocation and reducing substance use were of lower importance. Need for assistance with reducing substance use and social support were the domains least often identified as areas where help was needed, which seems inconsistent with the higher established rates of substance abuse problems among homeless veterans.1
With additional fieldwork, the HMMM-V program is expected to allow refinement of procedures for identifying and serving veterans from a patient-centered care perspective. The P-CHI will be further tested and developed, and the next step will be to create and pilot intervention templates for a Patient-Centered Health Improvement Plan, based on the P-CHI results. This process parallels the original development treatment plans for the VA’s Personalized Health Plan based on the PHI.25 Once the HMMM-V program is fully established in Dallas, the plans are for an expansion that will cover a broader geographic area in North Texas that includes rural areas.
The HMMM-V program was designed to address the barriers to health care that are encountered by homeless veterans. It is unique in homeless veteran care due to its patient-centered approach that partners with homeless veterans to prioritize their needs as determined by them rather than based solely on policies or provider conceptualizations of their needs. Access to services, engagement in care, and successful utilization of needed services may lead to measurable improvements in health care outcomes among homeless populations of veterans. Desired goals include remission of illness through appropriate medical intervention, preventing morbidity, achieving healthy lifestyles, recovery from addiction, stabilization of psychiatric illness, and attainment of stable housing.
The first hurdle for implementing this type of program in other settings is the identification of resources needed for these efforts. Need of additional staffing resources, however, may be circumvented by allowing employees working in other areas to rotate in community outreach shifts in the mobile unit. Another hurdle encountered in implementation of the HMMM-V initiative was the initial difficulty finding homeless veterans in community settings, especially those in unsheltered locations. The HMMM-V program addressed this issue by partnering with other agencies serving the homeless in the community. Therefore, a general recommendation for other entities seeking to implement this type of program is to reach out to these community partners from the outset.
Conclusion
The HMMM-V has the potential to engage the most difficult-to-reach homeless veterans in need of health services by delivering care and providing resources in challenging environments. Further work is needed to validate the P-CHI for use with this program and to conduct well-designed and implemented research to demonstrate effectiveness of this intervention on veteran outcomes, especially quality of life. Once this additional work is accomplished, this innovative program can potentially be implemented by VAMCs across the nation, and potentially in more general community care settings, to more effectively reach out and deliver services to homeless members of the community.
Acknowledgments
Grant support was received from the Department of Veterans Affairs, Office of Patient Centered Care. The authors would like to acknowledge all the clinicians, trainees, and support staff who have contributed to the success of the HMMM-V program: Tara Ayala, Jose Cabrera, Tony Castillo, Rachael Lynn David, Teresa DeShazo, Sylvia Figueroa, Steven Fisher, Eric Gary, Evelyn Gibbs, Kevin Hosey, JoAnn Joseph, Taly Drimer Kagan, Miranda Kelly, Michelle King-Thompson, Sharon Marcus, Shiji Mathew, Moneeza Matin, John Moreno, Joseph Neifert, Joel Price, Tiffany Price, Natalie Qualls, Reginald Robertson, Kristine Rodrigues, Jon Saffelder, Jill Stokes, Scott Stone, and John Smith.
1. LePage JP, Bradshaw LD, Cipher DJ, Crawford AM, Hooshyar D. The effects of homelessness on veterans’ health care service use: an evaluation of independence from comorbidities. Public Health. 2014;128(11):985-992.
2. Fischer PJ, Breakey WR. The epidemiology of alcohol, drug, and mental disorders among homeless persons. Am Psychol. 1991;46(11):1115-1128.
3. Robertson MJ, Zlotnick C, Westerfelt A. Drug use disorders and treatment contact among homeless adults in Alameda County, California. Am J Public Health. 1997;87(2):221-228.
4. North CS, Eyrich KM, Pollio DE, Spitznagel EL. Are rates of psychiatric disorders in the homeless population changing? Am J Public Health. 2004;94(1):103-108.
5. Fazel S, Khosla V, Doll H, Geddes J. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. PLoS Med. 2008;5(12):e225.
6. Harpaz-Rotem I, Rosenheck RA, Desai R. The mental health of children exposed to maternal mental illness and homelessness. Community Ment Health J. 2006;42(5):437-448.
7. Pollio DE, Eyrich-Garg KM, North CS. The homeless. In: Johnson BA, ed. Addiction Medicine: Science and Practice. New York, NY: Springer; 2011:1487-1504.
8. Padgett D, Struening EL, Andrews H. Factors affecting the use of medical, mental health, alcohol, and drug treatment services by homeless adults. Med Care. 1990;28(9):805-821.
9. Baggett TP, Singer DE, Rao SR, O’Connell JJ, Bharel M, Rigotti NA. Food insufficiency and health services utilization in a national sample of homeless adults. J Gen Intern Med. 2011;26(6):627-634.
10. Folsom DP, Hawthorne W, Lindamer L, et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry. 2005;162(2):370-376.
11. Fuehrlein BS, Cowell AJ, Pollio D, Cupps L, Balfour ME, North CS. A prospective study of the associations among housing status and costs of services in a homeless population. Psychiatr Serv. 2015;66(1):27-32.
12. Pollio DE, North CS, Eyrich KM, Foster DA, Spitznagel E. Modeling service access in a homeless population. J Psychoactive Drugs. 2003;35(4):487-495.
13. U.S. Department of Housing and Urban Development Office of Community Planning and Development. The 2016 Annual Homeless Assessment Report (AHAR) to Congress. Part 1: point-in-time estimates of homelessness. https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Published 2016. Accessed August 7, 2017.
14. Tsai J, Rosenheck RA. Risk factors for homelessness among U.S. veterans. Epidemiol Rev. 2015;37:177-195.
15. Williamson V, Mulhall E. Coming home: the housing crisis and homelessness threaten new veterans. Iraq and Afghanistan Veterans of America, January, 2009. http://media.iava.org/IAVA_coming_home_2009%20The%20Housing%20Crisis%20and%20Homelessness%20Threaten%20New%20Veterans.pdf. Accessed August 10, 2017
16. Shinseki EK. Remarks by Secretary Eric K. Shinseki. National Summit on Homeless Veterans; November 3, 2009; Washington, DC. https://www.va.gov/opa/speeches/2009/09_1103.asp. Updated August 8, 2016. Accessed August 7, 2017.
17. Shinseki EK. Remarks by Secretary Eric K. Shinseki. 2014 National Coalition for Homeless Veterans Annual Meeting; May 30, 2014; Arlington, VA. https://www.va.gov/opa/speeches/2014/05_30_2014.asp. Updated April 21, 2015. Accessed August 7, 2017.
18. Pollio DE, Spitznagel EL, North CS, Thompson S, Foster DA. Service use over time and achievement of stable housing in a mentally ill homeless population. Psychiatr Serv. 2000;51(12):1536-1543.
19. Page J. Barriers to transferring care of homeless people with serious mental illnesses to community mental health organizations: perspectives of street-based programs. Best Practices in Mental Health: An International Journal. 2007;3(1):26.
20. Young AS, Chinman MJ, Cradock-O’Leary JA, et al. Characteristics of individuals with severe mental illness who use emergency services. Community Ment Health J. 2005;41(2):159-168.
21. Gabrielian S, Yuan AH, Andersen RM, Rubenstein LV, Gelberg L. VA health service utilization for homeless and low-income veterans: a spotlight on the VA Supportive Housing (VASH) program in greater Los Angeles. Med Care. 2014;52(5):454-461.
22. Tsemberis S, Gulcur L, Nakae M. Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. Am J Public Health. 2004;94(4):651-656.
23. U.S. Department of Veterans Affairs, Veterans Health Administration. VA Patient Centered Care. http://www.va.gov/patientcenteredcare. Updated July 24,2017. Accessed August 7, 2017.
24. Epstein RM, Street RL Jr. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100-103.
25. U.S. Department of Veterans Affairs, Office of Patient Centered Care and Cultural Transformation. My story: personal health inventory. https://www.va.gov/PATIENTCENTEREDCARE/docs/VA-OPCC-Personal-Health-Inventory-final-508.pdf. Published October 7, 2013. Accessed August 7, 2017
26. North CS, Smith EM, Pollio DE. The Homeless Supplement to the Diagnostic Interview Schedule (DIS/HS). St. Louis: Washington University, 2004.
27. North CS, Eyrich KM, Pollio DE, Foster DA, Cottler LB, Spitznagel EL. The homeless supplement to the diagnostic interview schedule: test-retest analyses. Int J Methods Psychiatr Res. 2004;13(3):184-191.
28. LaSalle JL. Homeless Operations Management and Evaluation System (HOMES) user manual-phase 1. http://www.vfwsc.org/homes.pdf. Published April 19, 2011. Accessed August 7, 2017.
29. Petrovich JC, Pollio DE, North CS. Characteristics and service use of homeless veterans and nonveterans residing in a low-demand emergency shelter. Psychiatr Serv. 2014;65(6):751-757.
30. North CS, Smith EM. A comparison of homeless men and women: different populations, different needs. Community Ment Health J. 1993;29(5):423-431.
31. Kertesz SG, Austin EL, Holmes SK, et al. Making housing first happen: organizational leadership in VA’s expansion of permanent supportive housing. J Gen Intern Med. 2014;29(suppl 4):835-844.
1. LePage JP, Bradshaw LD, Cipher DJ, Crawford AM, Hooshyar D. The effects of homelessness on veterans’ health care service use: an evaluation of independence from comorbidities. Public Health. 2014;128(11):985-992.
2. Fischer PJ, Breakey WR. The epidemiology of alcohol, drug, and mental disorders among homeless persons. Am Psychol. 1991;46(11):1115-1128.
3. Robertson MJ, Zlotnick C, Westerfelt A. Drug use disorders and treatment contact among homeless adults in Alameda County, California. Am J Public Health. 1997;87(2):221-228.
4. North CS, Eyrich KM, Pollio DE, Spitznagel EL. Are rates of psychiatric disorders in the homeless population changing? Am J Public Health. 2004;94(1):103-108.
5. Fazel S, Khosla V, Doll H, Geddes J. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. PLoS Med. 2008;5(12):e225.
6. Harpaz-Rotem I, Rosenheck RA, Desai R. The mental health of children exposed to maternal mental illness and homelessness. Community Ment Health J. 2006;42(5):437-448.
7. Pollio DE, Eyrich-Garg KM, North CS. The homeless. In: Johnson BA, ed. Addiction Medicine: Science and Practice. New York, NY: Springer; 2011:1487-1504.
8. Padgett D, Struening EL, Andrews H. Factors affecting the use of medical, mental health, alcohol, and drug treatment services by homeless adults. Med Care. 1990;28(9):805-821.
9. Baggett TP, Singer DE, Rao SR, O’Connell JJ, Bharel M, Rigotti NA. Food insufficiency and health services utilization in a national sample of homeless adults. J Gen Intern Med. 2011;26(6):627-634.
10. Folsom DP, Hawthorne W, Lindamer L, et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry. 2005;162(2):370-376.
11. Fuehrlein BS, Cowell AJ, Pollio D, Cupps L, Balfour ME, North CS. A prospective study of the associations among housing status and costs of services in a homeless population. Psychiatr Serv. 2015;66(1):27-32.
12. Pollio DE, North CS, Eyrich KM, Foster DA, Spitznagel E. Modeling service access in a homeless population. J Psychoactive Drugs. 2003;35(4):487-495.
13. U.S. Department of Housing and Urban Development Office of Community Planning and Development. The 2016 Annual Homeless Assessment Report (AHAR) to Congress. Part 1: point-in-time estimates of homelessness. https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Published 2016. Accessed August 7, 2017.
14. Tsai J, Rosenheck RA. Risk factors for homelessness among U.S. veterans. Epidemiol Rev. 2015;37:177-195.
15. Williamson V, Mulhall E. Coming home: the housing crisis and homelessness threaten new veterans. Iraq and Afghanistan Veterans of America, January, 2009. http://media.iava.org/IAVA_coming_home_2009%20The%20Housing%20Crisis%20and%20Homelessness%20Threaten%20New%20Veterans.pdf. Accessed August 10, 2017
16. Shinseki EK. Remarks by Secretary Eric K. Shinseki. National Summit on Homeless Veterans; November 3, 2009; Washington, DC. https://www.va.gov/opa/speeches/2009/09_1103.asp. Updated August 8, 2016. Accessed August 7, 2017.
17. Shinseki EK. Remarks by Secretary Eric K. Shinseki. 2014 National Coalition for Homeless Veterans Annual Meeting; May 30, 2014; Arlington, VA. https://www.va.gov/opa/speeches/2014/05_30_2014.asp. Updated April 21, 2015. Accessed August 7, 2017.
18. Pollio DE, Spitznagel EL, North CS, Thompson S, Foster DA. Service use over time and achievement of stable housing in a mentally ill homeless population. Psychiatr Serv. 2000;51(12):1536-1543.
19. Page J. Barriers to transferring care of homeless people with serious mental illnesses to community mental health organizations: perspectives of street-based programs. Best Practices in Mental Health: An International Journal. 2007;3(1):26.
20. Young AS, Chinman MJ, Cradock-O’Leary JA, et al. Characteristics of individuals with severe mental illness who use emergency services. Community Ment Health J. 2005;41(2):159-168.
21. Gabrielian S, Yuan AH, Andersen RM, Rubenstein LV, Gelberg L. VA health service utilization for homeless and low-income veterans: a spotlight on the VA Supportive Housing (VASH) program in greater Los Angeles. Med Care. 2014;52(5):454-461.
22. Tsemberis S, Gulcur L, Nakae M. Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. Am J Public Health. 2004;94(4):651-656.
23. U.S. Department of Veterans Affairs, Veterans Health Administration. VA Patient Centered Care. http://www.va.gov/patientcenteredcare. Updated July 24,2017. Accessed August 7, 2017.
24. Epstein RM, Street RL Jr. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100-103.
25. U.S. Department of Veterans Affairs, Office of Patient Centered Care and Cultural Transformation. My story: personal health inventory. https://www.va.gov/PATIENTCENTEREDCARE/docs/VA-OPCC-Personal-Health-Inventory-final-508.pdf. Published October 7, 2013. Accessed August 7, 2017
26. North CS, Smith EM, Pollio DE. The Homeless Supplement to the Diagnostic Interview Schedule (DIS/HS). St. Louis: Washington University, 2004.
27. North CS, Eyrich KM, Pollio DE, Foster DA, Cottler LB, Spitznagel EL. The homeless supplement to the diagnostic interview schedule: test-retest analyses. Int J Methods Psychiatr Res. 2004;13(3):184-191.
28. LaSalle JL. Homeless Operations Management and Evaluation System (HOMES) user manual-phase 1. http://www.vfwsc.org/homes.pdf. Published April 19, 2011. Accessed August 7, 2017.
29. Petrovich JC, Pollio DE, North CS. Characteristics and service use of homeless veterans and nonveterans residing in a low-demand emergency shelter. Psychiatr Serv. 2014;65(6):751-757.
30. North CS, Smith EM. A comparison of homeless men and women: different populations, different needs. Community Ment Health J. 1993;29(5):423-431.
31. Kertesz SG, Austin EL, Holmes SK, et al. Making housing first happen: organizational leadership in VA’s expansion of permanent supportive housing. J Gen Intern Med. 2014;29(suppl 4):835-844.
Checkmate 238: Nivolumab bests ipilimumab for resectable stage III or IV melanoma
MADRID – For patients with resectable stage III melanoma, adjuvant therapy with the programmed death 1 (PD-1) immune checkpoint inhibitor nivolumab (Opdivo) was associated with significantly longer relapse-free survival compared with the cytotoxic T-lymphocyte antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy), results of a randomized phase 3 trial show.
Among 906 patients who underwent complete resection of stage IIIB, IIIC, or stage IV melanoma in the Checkmate 238 trial, the rates of relapse-free survival (RFS), the primary endpoint, were 71% at 12 months for patients assigned to adjuvant nivolumab, compared with 61% for adjuvant ipilimumab. At 18 months, the respective RFS rates were 66% and 53%, reported Jeffrey Weber, MD, PhD, of NYU Langone Health’s Perlmutter Cancer Center in New York City.
However, longer follow-up will be needed to see whether the RFS advantage of nivolumab translates into an overall survival advantage, he acknowledged.
In the trial, patients with high-risk, completely resected stage IIIB, IIIC, or IV melanoma were stratified by disease stage and PD-L1 status at baseline and randomly assigned in cohorts of 453 patients each to receive either nivolumab 3 mg/kg intravenously every 2 weeks and ipilimumab placebo every 3 weeks for four doses, or to ipilimumab 10 mg/kg IV every 3 weeks for four doses, then every 12 weeks from week 24, and nivolumab placebo IV every 2 weeks.
The maximum duration of therapy was 1 year.
For the primary RFS endpoint, the hazard ratio (HR) favoring nivolumab was 0.65 (P less than .0001).
The benefit for nivolumab was observed across the majority of prespecified subgroups tested, including PD-L1 and BRAF mutational status, Dr. Weber said.
Nivolumab also had a better safety profile, with a 14.4% incidence of grade 3 or 4 treatment-related adverse events, compared with 45.9% for ipilimumab. Grade 3 or 4 treatment-related adverse events leading to discontinuation of therapy occurred in 4.6% of patients on nivolumab, compared with 30.9% of those on ipilimumab.
Two patients in the ipilimumab arm died from toxicities related to therapy, one from marrow aplasia, and one from colitis. Both of these deaths occurred more than 100 days after the patients received their last dose of ipilimumab. There were no treatment-related deaths in the nivolumab arm.
Commenting on both the Checkmate 238 trial and a second trial reported at ESMO (COMBI-AD) looking at a combination of dabrafenib and trametinib for patients with stage III melanoma with a BRAF V600 mutation, Olivier Michielin, MD, PhD, said that “we now have, with the data, two fantastic new options. We couldn’t dream those studies to be so positive. This is really something that will open new futures for our patients.”
Dr. Michielin and Dr. Dummer were invited commentators at the briefing. Dr. Michielin was not involved in either trial. Dr. Dummer was a coinvestigator for the COMBI-AD trial.
The study was published simultaneously online by the New England Journal of Medicine.
Checkmate 238 was funded by Bristol-Myers Squibb and Ono Pharmaceutical. Dr. Weber disclosed honoraria, consulting fees, and travel accommodations/expenses from BMS and multiple other companies. Dr. Michielin disclosed consulting and/or honoraria from Amgen, BMS, Roche, MSD, Novartis, and GSK. Dr. Dummer reported advising/consulting roles with BMS and others.
MADRID – For patients with resectable stage III melanoma, adjuvant therapy with the programmed death 1 (PD-1) immune checkpoint inhibitor nivolumab (Opdivo) was associated with significantly longer relapse-free survival compared with the cytotoxic T-lymphocyte antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy), results of a randomized phase 3 trial show.
Among 906 patients who underwent complete resection of stage IIIB, IIIC, or stage IV melanoma in the Checkmate 238 trial, the rates of relapse-free survival (RFS), the primary endpoint, were 71% at 12 months for patients assigned to adjuvant nivolumab, compared with 61% for adjuvant ipilimumab. At 18 months, the respective RFS rates were 66% and 53%, reported Jeffrey Weber, MD, PhD, of NYU Langone Health’s Perlmutter Cancer Center in New York City.
However, longer follow-up will be needed to see whether the RFS advantage of nivolumab translates into an overall survival advantage, he acknowledged.
In the trial, patients with high-risk, completely resected stage IIIB, IIIC, or IV melanoma were stratified by disease stage and PD-L1 status at baseline and randomly assigned in cohorts of 453 patients each to receive either nivolumab 3 mg/kg intravenously every 2 weeks and ipilimumab placebo every 3 weeks for four doses, or to ipilimumab 10 mg/kg IV every 3 weeks for four doses, then every 12 weeks from week 24, and nivolumab placebo IV every 2 weeks.
The maximum duration of therapy was 1 year.
For the primary RFS endpoint, the hazard ratio (HR) favoring nivolumab was 0.65 (P less than .0001).
The benefit for nivolumab was observed across the majority of prespecified subgroups tested, including PD-L1 and BRAF mutational status, Dr. Weber said.
Nivolumab also had a better safety profile, with a 14.4% incidence of grade 3 or 4 treatment-related adverse events, compared with 45.9% for ipilimumab. Grade 3 or 4 treatment-related adverse events leading to discontinuation of therapy occurred in 4.6% of patients on nivolumab, compared with 30.9% of those on ipilimumab.
Two patients in the ipilimumab arm died from toxicities related to therapy, one from marrow aplasia, and one from colitis. Both of these deaths occurred more than 100 days after the patients received their last dose of ipilimumab. There were no treatment-related deaths in the nivolumab arm.
Commenting on both the Checkmate 238 trial and a second trial reported at ESMO (COMBI-AD) looking at a combination of dabrafenib and trametinib for patients with stage III melanoma with a BRAF V600 mutation, Olivier Michielin, MD, PhD, said that “we now have, with the data, two fantastic new options. We couldn’t dream those studies to be so positive. This is really something that will open new futures for our patients.”
Dr. Michielin and Dr. Dummer were invited commentators at the briefing. Dr. Michielin was not involved in either trial. Dr. Dummer was a coinvestigator for the COMBI-AD trial.
The study was published simultaneously online by the New England Journal of Medicine.
Checkmate 238 was funded by Bristol-Myers Squibb and Ono Pharmaceutical. Dr. Weber disclosed honoraria, consulting fees, and travel accommodations/expenses from BMS and multiple other companies. Dr. Michielin disclosed consulting and/or honoraria from Amgen, BMS, Roche, MSD, Novartis, and GSK. Dr. Dummer reported advising/consulting roles with BMS and others.
MADRID – For patients with resectable stage III melanoma, adjuvant therapy with the programmed death 1 (PD-1) immune checkpoint inhibitor nivolumab (Opdivo) was associated with significantly longer relapse-free survival compared with the cytotoxic T-lymphocyte antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy), results of a randomized phase 3 trial show.
Among 906 patients who underwent complete resection of stage IIIB, IIIC, or stage IV melanoma in the Checkmate 238 trial, the rates of relapse-free survival (RFS), the primary endpoint, were 71% at 12 months for patients assigned to adjuvant nivolumab, compared with 61% for adjuvant ipilimumab. At 18 months, the respective RFS rates were 66% and 53%, reported Jeffrey Weber, MD, PhD, of NYU Langone Health’s Perlmutter Cancer Center in New York City.
However, longer follow-up will be needed to see whether the RFS advantage of nivolumab translates into an overall survival advantage, he acknowledged.
In the trial, patients with high-risk, completely resected stage IIIB, IIIC, or IV melanoma were stratified by disease stage and PD-L1 status at baseline and randomly assigned in cohorts of 453 patients each to receive either nivolumab 3 mg/kg intravenously every 2 weeks and ipilimumab placebo every 3 weeks for four doses, or to ipilimumab 10 mg/kg IV every 3 weeks for four doses, then every 12 weeks from week 24, and nivolumab placebo IV every 2 weeks.
The maximum duration of therapy was 1 year.
For the primary RFS endpoint, the hazard ratio (HR) favoring nivolumab was 0.65 (P less than .0001).
The benefit for nivolumab was observed across the majority of prespecified subgroups tested, including PD-L1 and BRAF mutational status, Dr. Weber said.
Nivolumab also had a better safety profile, with a 14.4% incidence of grade 3 or 4 treatment-related adverse events, compared with 45.9% for ipilimumab. Grade 3 or 4 treatment-related adverse events leading to discontinuation of therapy occurred in 4.6% of patients on nivolumab, compared with 30.9% of those on ipilimumab.
Two patients in the ipilimumab arm died from toxicities related to therapy, one from marrow aplasia, and one from colitis. Both of these deaths occurred more than 100 days after the patients received their last dose of ipilimumab. There were no treatment-related deaths in the nivolumab arm.
Commenting on both the Checkmate 238 trial and a second trial reported at ESMO (COMBI-AD) looking at a combination of dabrafenib and trametinib for patients with stage III melanoma with a BRAF V600 mutation, Olivier Michielin, MD, PhD, said that “we now have, with the data, two fantastic new options. We couldn’t dream those studies to be so positive. This is really something that will open new futures for our patients.”
Dr. Michielin and Dr. Dummer were invited commentators at the briefing. Dr. Michielin was not involved in either trial. Dr. Dummer was a coinvestigator for the COMBI-AD trial.
The study was published simultaneously online by the New England Journal of Medicine.
Checkmate 238 was funded by Bristol-Myers Squibb and Ono Pharmaceutical. Dr. Weber disclosed honoraria, consulting fees, and travel accommodations/expenses from BMS and multiple other companies. Dr. Michielin disclosed consulting and/or honoraria from Amgen, BMS, Roche, MSD, Novartis, and GSK. Dr. Dummer reported advising/consulting roles with BMS and others.
AT ESMO 2017
Key clinical point: Nivolumab improved relapse-free survival over ipilimumab in patients with stage III or IV resectable melanoma.
Major finding: The rates of relapse-free survival were 71% at 12 months for patients assigned to adjuvant nivolumab, compared with 61% for adjuvant ipilimumab.
Data source: Randomized clinical trial in 906 patients with completely resectable stage III melanoma.
Disclosures: Checkmate 238 was funded by Bristol-Myers Squibb and Ono Pharmaceutical. Dr. Weber disclosed honoraria, consulting fees, and travel accommodations/expenses from BMS and other companies. Dr. Michielin disclosed consulting and/or honoraria from Amgen, BMS, Roche, MSD, Novartis, and GSK.. Dr. Dummer reported advising/consulting roles with BMS and others.