User login
ASH guidelines for venous thromboembolism: What family physicians need to know
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .

These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .
These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .
These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Tackling screen time from birth
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?

Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.

Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.
A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?
Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.
Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.
A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?
Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.
Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.
A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
On being an elite
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.

Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.
Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.
Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
COVID-19 vaccines and cancer patients: 4 things to know
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Flattening the hierarchy
What fellows can learn about leadership from aircraft crews
Fellowship is a time of great growth for pediatric hospital medicine fellows as clinicians, educators, scholars, and as leaders. Leadership is a crucial skill for hospitalists that is cultivated throughout fellowship. As fellows, we step into the role of clinical team leader for the first time and it is our responsibility to create a clinical and educational environment that is safe, inviting and engaging.

For possibly the first time in our careers, pediatric hospital medicine fellows are expected to make final decisions, big and small. We are faced with high-pressure situations almost daily, whether it is a rapid response on a patient, tough diagnostic and therapeutic decisions, difficult conversations with families, or dealing with challenging team members.
Soon after starting fellowship I was faced with a such a situation. The patient was a 6-month-old infant with trisomy 21 who was admitted because of feeding difficulties. They were working on oral feeds but required nasogastric (NG) feeds to meet caloric needs. On my first day on service, the residents indicated that the medical team desired the patient to have a gastrostomy tube (G-tube) placed. I was hoping to send the patient home for a few weeks with the NG tube to see if they were making progress on their oral feeds before deciding on the need for a G-tube. However, the patient’s parents pulled me aside in the hallway and said they were considering a third possibility.
The parents felt strongly about a trial period of a few weeks without the NG tube to see if the patient was able to maintain adequate weight gain with just oral feeds. The bedside nurse reiterated that the family felt their concerns had not been considered up until this point. As the fellow and team leader, it was my job to navigate between my resident team, myself, and the family in order to make a final decision. Through a bedside meeting and shared decision making, we were able to compromise and negotiate a decision, allowing the patient to go home on just oral feeds with close follow-up with their pediatrician. Afterwards, I found myself searching for strategies to be a better leader in these situations.
I found a potential answer in a recent article from the Harvard Business Review titled “What Aircraft Crews Know About Managing High-Pressure Situations.”1 The article discusses crew resource management (CRM), which was developed in the 1980s and is used in civil and military aviation worldwide. CRM is based on two principles to improve crisis management: The hierarchy on the flight deck must be flattened, and crew members must be actively integrated into the flight’s work flows and decision-making processes.
The authors of the article conducted two different studies to further understand CRM and its effects. The first study included observing 11 flight crews in emergency simulations. In the study, the flight crew had to react to an emergency, and then conduct a landing of the aircraft. What the authors found was that the captain’s style of communication had a major impact on crew performance in two major ways: Crews performed consistently better under times of pressure when the copilot was included in the decision-making process, and captains who asked open-ended questions (“How do you assess the situation”) came up with better solutions than captains who asked “yes or no” questions.
The authors conclude that “involving colleagues as equal decision partners by asking them questions…aids constructive, factual information exchange.” The second study consisted of conducting 61 interviews with flight crew members to better understand crisis management. In the interviews, the same theme occurred, that open-ended questions are vital in all decision-making processes and may be preventative against dangerous or imperfect outcomes. As fellows and team leaders we can learn from CRM and these studies. We need to flatten the hierarchy and ask open-ended questions.
To flatten the hierarchy, we should value the thoughts and opinions of all our team members. Now more than ever in this current COVID-19 pandemic with many hospitals instituting telehealth/telerounding for some or all team members, it is essential to utilize our entire “flight crew” (physicians, nurses, therapists, subspecialists, social worker, case managers, etc.) during routine decisions and high-stake decisions. We should make sure our flight crew, especially the bedside nurse is part of the decision-making process.2 This means we need to ensure they are present and given a voice on clinical rounds. To flatten the hierarchy, we must take pride in eliciting other team member’s opinions. We must realize that we alone do not have all the answers, and other team members may have different frameworks in which they process a decision.
Finally, in medicine, our patients and families are included in our flight crew. They too must have a voice in the decision-making process. Previous studies have shown that patients and families desire to be included in the decision-making process, and opportunities exist to improve shared decision-making in pediatrics.3-5 Lastly, we should commit to asking open-ended questions from our team and our patients. We should value their input and use their answers and frameworks to make the best decision for our patients.
I wasn’t aware at the time, but I was using some of the principles of CRM while navigating my high-pressure situation. A bedside meeting with all team members and the patient’s family helped to flatten the hierarchy by understanding and valuing each team member’s input. Asking open-ended questions of the different team members led to a more inviting and engaging clinical and learning environment. These strategies helped to lead our team into a clinical decision that wasn’t entirely clear at first but ended up being the best decision for the patient, as they are now thriving without ever requiring supplemental nutrition after discharge.
As physicians, we have learned a lot from the airline industry about wellness and the effect of fatigue on performance. It is clear now that we can also learn from them about clinical decision-making and leadership strategies. When adopted for health care, CRM principles have been shown to result in a culture of safety and long-term behavioral change.6,7 If we can model ourselves after the airline industry by following the principles of CRM, then we will be better clinicians, educators, and leaders.
Dr. Palmer is a second-year pediatric hospital medicine fellow at Children’s Hospital Los Angeles and is working toward a masters in academic medicine at the University of Southern California, Los Angeles, with a focus on curriculum development and educational scholarship production.
References
1. Hagan J et al. What Aircraft Crews Know About Managing High-Pressure Situations. Harvard Business Review. 2019 Dec. https://hbr.org/2019/12/what-aircraft-crews-know-about-managing-high-pressure-situations
2. Erickson J. Bedside nurse involvement in end-of-life decision-making: A brief review of the literature. Dimens Crit Care Nurs. 2013;32(2):65-8.
3. Richards CA et al. Physicians perceptions of shared decision-making in neonatal and pediatric critical care. Am J Hosp Palliat Care. 2018;35(4):669-76.
4. Boland L et al. Barriers and facilitators of pediatric shared decision-making: A systematic review. Implement Sci. 2019 Jan 18. doi: 10.1186/s13012-018-0851-5.
5. Blankenburg R et al. Shared decision-making during inpatient rounds: Opportunities for improvement in patient engagement and communication. J Hosp Med. 2018;13(7):453-61.
6. Kemper PF et al. Crew resource management training in the intensive care unit. A multisite controlled before-after study. BMJ Qual Saf. 2016;25(8):577-87.
7. Sax HC et al. Can aviation-based team training elicit sustainable behavioral change? Arch Surg. 2009;144(12):1133-7.
What fellows can learn about leadership from aircraft crews
What fellows can learn about leadership from aircraft crews
Fellowship is a time of great growth for pediatric hospital medicine fellows as clinicians, educators, scholars, and as leaders. Leadership is a crucial skill for hospitalists that is cultivated throughout fellowship. As fellows, we step into the role of clinical team leader for the first time and it is our responsibility to create a clinical and educational environment that is safe, inviting and engaging.
For possibly the first time in our careers, pediatric hospital medicine fellows are expected to make final decisions, big and small. We are faced with high-pressure situations almost daily, whether it is a rapid response on a patient, tough diagnostic and therapeutic decisions, difficult conversations with families, or dealing with challenging team members.
Soon after starting fellowship I was faced with a such a situation. The patient was a 6-month-old infant with trisomy 21 who was admitted because of feeding difficulties. They were working on oral feeds but required nasogastric (NG) feeds to meet caloric needs. On my first day on service, the residents indicated that the medical team desired the patient to have a gastrostomy tube (G-tube) placed. I was hoping to send the patient home for a few weeks with the NG tube to see if they were making progress on their oral feeds before deciding on the need for a G-tube. However, the patient’s parents pulled me aside in the hallway and said they were considering a third possibility.
The parents felt strongly about a trial period of a few weeks without the NG tube to see if the patient was able to maintain adequate weight gain with just oral feeds. The bedside nurse reiterated that the family felt their concerns had not been considered up until this point. As the fellow and team leader, it was my job to navigate between my resident team, myself, and the family in order to make a final decision. Through a bedside meeting and shared decision making, we were able to compromise and negotiate a decision, allowing the patient to go home on just oral feeds with close follow-up with their pediatrician. Afterwards, I found myself searching for strategies to be a better leader in these situations.
I found a potential answer in a recent article from the Harvard Business Review titled “What Aircraft Crews Know About Managing High-Pressure Situations.”1 The article discusses crew resource management (CRM), which was developed in the 1980s and is used in civil and military aviation worldwide. CRM is based on two principles to improve crisis management: The hierarchy on the flight deck must be flattened, and crew members must be actively integrated into the flight’s work flows and decision-making processes.
The authors of the article conducted two different studies to further understand CRM and its effects. The first study included observing 11 flight crews in emergency simulations. In the study, the flight crew had to react to an emergency, and then conduct a landing of the aircraft. What the authors found was that the captain’s style of communication had a major impact on crew performance in two major ways: Crews performed consistently better under times of pressure when the copilot was included in the decision-making process, and captains who asked open-ended questions (“How do you assess the situation”) came up with better solutions than captains who asked “yes or no” questions.
The authors conclude that “involving colleagues as equal decision partners by asking them questions…aids constructive, factual information exchange.” The second study consisted of conducting 61 interviews with flight crew members to better understand crisis management. In the interviews, the same theme occurred, that open-ended questions are vital in all decision-making processes and may be preventative against dangerous or imperfect outcomes. As fellows and team leaders we can learn from CRM and these studies. We need to flatten the hierarchy and ask open-ended questions.
To flatten the hierarchy, we should value the thoughts and opinions of all our team members. Now more than ever in this current COVID-19 pandemic with many hospitals instituting telehealth/telerounding for some or all team members, it is essential to utilize our entire “flight crew” (physicians, nurses, therapists, subspecialists, social worker, case managers, etc.) during routine decisions and high-stake decisions. We should make sure our flight crew, especially the bedside nurse is part of the decision-making process.2 This means we need to ensure they are present and given a voice on clinical rounds. To flatten the hierarchy, we must take pride in eliciting other team member’s opinions. We must realize that we alone do not have all the answers, and other team members may have different frameworks in which they process a decision.
Finally, in medicine, our patients and families are included in our flight crew. They too must have a voice in the decision-making process. Previous studies have shown that patients and families desire to be included in the decision-making process, and opportunities exist to improve shared decision-making in pediatrics.3-5 Lastly, we should commit to asking open-ended questions from our team and our patients. We should value their input and use their answers and frameworks to make the best decision for our patients.
I wasn’t aware at the time, but I was using some of the principles of CRM while navigating my high-pressure situation. A bedside meeting with all team members and the patient’s family helped to flatten the hierarchy by understanding and valuing each team member’s input. Asking open-ended questions of the different team members led to a more inviting and engaging clinical and learning environment. These strategies helped to lead our team into a clinical decision that wasn’t entirely clear at first but ended up being the best decision for the patient, as they are now thriving without ever requiring supplemental nutrition after discharge.
As physicians, we have learned a lot from the airline industry about wellness and the effect of fatigue on performance. It is clear now that we can also learn from them about clinical decision-making and leadership strategies. When adopted for health care, CRM principles have been shown to result in a culture of safety and long-term behavioral change.6,7 If we can model ourselves after the airline industry by following the principles of CRM, then we will be better clinicians, educators, and leaders.
Dr. Palmer is a second-year pediatric hospital medicine fellow at Children’s Hospital Los Angeles and is working toward a masters in academic medicine at the University of Southern California, Los Angeles, with a focus on curriculum development and educational scholarship production.
References
1. Hagan J et al. What Aircraft Crews Know About Managing High-Pressure Situations. Harvard Business Review. 2019 Dec. https://hbr.org/2019/12/what-aircraft-crews-know-about-managing-high-pressure-situations
2. Erickson J. Bedside nurse involvement in end-of-life decision-making: A brief review of the literature. Dimens Crit Care Nurs. 2013;32(2):65-8.
3. Richards CA et al. Physicians perceptions of shared decision-making in neonatal and pediatric critical care. Am J Hosp Palliat Care. 2018;35(4):669-76.
4. Boland L et al. Barriers and facilitators of pediatric shared decision-making: A systematic review. Implement Sci. 2019 Jan 18. doi: 10.1186/s13012-018-0851-5.
5. Blankenburg R et al. Shared decision-making during inpatient rounds: Opportunities for improvement in patient engagement and communication. J Hosp Med. 2018;13(7):453-61.
6. Kemper PF et al. Crew resource management training in the intensive care unit. A multisite controlled before-after study. BMJ Qual Saf. 2016;25(8):577-87.
7. Sax HC et al. Can aviation-based team training elicit sustainable behavioral change? Arch Surg. 2009;144(12):1133-7.
Fellowship is a time of great growth for pediatric hospital medicine fellows as clinicians, educators, scholars, and as leaders. Leadership is a crucial skill for hospitalists that is cultivated throughout fellowship. As fellows, we step into the role of clinical team leader for the first time and it is our responsibility to create a clinical and educational environment that is safe, inviting and engaging.
For possibly the first time in our careers, pediatric hospital medicine fellows are expected to make final decisions, big and small. We are faced with high-pressure situations almost daily, whether it is a rapid response on a patient, tough diagnostic and therapeutic decisions, difficult conversations with families, or dealing with challenging team members.
Soon after starting fellowship I was faced with a such a situation. The patient was a 6-month-old infant with trisomy 21 who was admitted because of feeding difficulties. They were working on oral feeds but required nasogastric (NG) feeds to meet caloric needs. On my first day on service, the residents indicated that the medical team desired the patient to have a gastrostomy tube (G-tube) placed. I was hoping to send the patient home for a few weeks with the NG tube to see if they were making progress on their oral feeds before deciding on the need for a G-tube. However, the patient’s parents pulled me aside in the hallway and said they were considering a third possibility.
The parents felt strongly about a trial period of a few weeks without the NG tube to see if the patient was able to maintain adequate weight gain with just oral feeds. The bedside nurse reiterated that the family felt their concerns had not been considered up until this point. As the fellow and team leader, it was my job to navigate between my resident team, myself, and the family in order to make a final decision. Through a bedside meeting and shared decision making, we were able to compromise and negotiate a decision, allowing the patient to go home on just oral feeds with close follow-up with their pediatrician. Afterwards, I found myself searching for strategies to be a better leader in these situations.
I found a potential answer in a recent article from the Harvard Business Review titled “What Aircraft Crews Know About Managing High-Pressure Situations.”1 The article discusses crew resource management (CRM), which was developed in the 1980s and is used in civil and military aviation worldwide. CRM is based on two principles to improve crisis management: The hierarchy on the flight deck must be flattened, and crew members must be actively integrated into the flight’s work flows and decision-making processes.
The authors of the article conducted two different studies to further understand CRM and its effects. The first study included observing 11 flight crews in emergency simulations. In the study, the flight crew had to react to an emergency, and then conduct a landing of the aircraft. What the authors found was that the captain’s style of communication had a major impact on crew performance in two major ways: Crews performed consistently better under times of pressure when the copilot was included in the decision-making process, and captains who asked open-ended questions (“How do you assess the situation”) came up with better solutions than captains who asked “yes or no” questions.
The authors conclude that “involving colleagues as equal decision partners by asking them questions…aids constructive, factual information exchange.” The second study consisted of conducting 61 interviews with flight crew members to better understand crisis management. In the interviews, the same theme occurred, that open-ended questions are vital in all decision-making processes and may be preventative against dangerous or imperfect outcomes. As fellows and team leaders we can learn from CRM and these studies. We need to flatten the hierarchy and ask open-ended questions.
To flatten the hierarchy, we should value the thoughts and opinions of all our team members. Now more than ever in this current COVID-19 pandemic with many hospitals instituting telehealth/telerounding for some or all team members, it is essential to utilize our entire “flight crew” (physicians, nurses, therapists, subspecialists, social worker, case managers, etc.) during routine decisions and high-stake decisions. We should make sure our flight crew, especially the bedside nurse is part of the decision-making process.2 This means we need to ensure they are present and given a voice on clinical rounds. To flatten the hierarchy, we must take pride in eliciting other team member’s opinions. We must realize that we alone do not have all the answers, and other team members may have different frameworks in which they process a decision.
Finally, in medicine, our patients and families are included in our flight crew. They too must have a voice in the decision-making process. Previous studies have shown that patients and families desire to be included in the decision-making process, and opportunities exist to improve shared decision-making in pediatrics.3-5 Lastly, we should commit to asking open-ended questions from our team and our patients. We should value their input and use their answers and frameworks to make the best decision for our patients.
I wasn’t aware at the time, but I was using some of the principles of CRM while navigating my high-pressure situation. A bedside meeting with all team members and the patient’s family helped to flatten the hierarchy by understanding and valuing each team member’s input. Asking open-ended questions of the different team members led to a more inviting and engaging clinical and learning environment. These strategies helped to lead our team into a clinical decision that wasn’t entirely clear at first but ended up being the best decision for the patient, as they are now thriving without ever requiring supplemental nutrition after discharge.
As physicians, we have learned a lot from the airline industry about wellness and the effect of fatigue on performance. It is clear now that we can also learn from them about clinical decision-making and leadership strategies. When adopted for health care, CRM principles have been shown to result in a culture of safety and long-term behavioral change.6,7 If we can model ourselves after the airline industry by following the principles of CRM, then we will be better clinicians, educators, and leaders.
Dr. Palmer is a second-year pediatric hospital medicine fellow at Children’s Hospital Los Angeles and is working toward a masters in academic medicine at the University of Southern California, Los Angeles, with a focus on curriculum development and educational scholarship production.
References
1. Hagan J et al. What Aircraft Crews Know About Managing High-Pressure Situations. Harvard Business Review. 2019 Dec. https://hbr.org/2019/12/what-aircraft-crews-know-about-managing-high-pressure-situations
2. Erickson J. Bedside nurse involvement in end-of-life decision-making: A brief review of the literature. Dimens Crit Care Nurs. 2013;32(2):65-8.
3. Richards CA et al. Physicians perceptions of shared decision-making in neonatal and pediatric critical care. Am J Hosp Palliat Care. 2018;35(4):669-76.
4. Boland L et al. Barriers and facilitators of pediatric shared decision-making: A systematic review. Implement Sci. 2019 Jan 18. doi: 10.1186/s13012-018-0851-5.
5. Blankenburg R et al. Shared decision-making during inpatient rounds: Opportunities for improvement in patient engagement and communication. J Hosp Med. 2018;13(7):453-61.
6. Kemper PF et al. Crew resource management training in the intensive care unit. A multisite controlled before-after study. BMJ Qual Saf. 2016;25(8):577-87.
7. Sax HC et al. Can aviation-based team training elicit sustainable behavioral change? Arch Surg. 2009;144(12):1133-7.
Should I be afraid of getting COVID again?
Is it over or do I have to brace myself for the possibility of a reinfection? Moreover, could the second time potentially be worse than the first?
I was diagnosed with COVID in March of this year. After spending 10 days in the hospital, and one night in the ICU, it took another 2 months for the air-hunger, headaches, and fatigue to completely resolve. Compared with many other unfortunate victims, I did all right – and I am very grateful for the care I received.
Now, as the surge in cases takes new life, I will be on the front lines taking care of patients. Having had an eventful personal encounter with the virus, I now have a unique vantage point and remain fully committed to paying my fortunate circumstances forward. Although I can’t help but have the same question faced by millions of others: Am I safe now?
It is no surprise that studies have shown health care workers comprising 6% of COVID hospital admissions, with one-third of these admissions being nurses. Recently, we heard that over 900 health care workers at Mayo Clinic had acquired the infection in the first 2 weeks of the ongoing second COVID surge. Are these frontline workers protected? Can they return to work with no fear of a rerun? Or, for that matter, anyone who has been afflicted by COVID – are they now forever immune?
There are no clear answers here. But to understand this a little, let’s quickly revisit some basic principles of immunity.
Innate and adaptive immunity
Simply put, there are two forms of immunity: innate and adaptive. Innate immunity encompasses our body’s natural protective mechanisms that come into play almost immediately. This enables recognition of the virus and activates an immediate antiviral defense and attempt at removal of the infective agent. This, however, does not always do the job. Accordingly, a couple weeks after the initial exposure to the pathogen, adaptive immunity is invoked. Circulating white blood cells within our body recognize the virus and set off an immune response, involving the activation of T and B cells that actively attack the infective agent. It is this T- and B-cell–mediated immunity that should protect one against a second infection with the same agent.
What about herd immunity?
Herd immunity is defined as essentially yielding to the virus and letting it spread naturally in order to develop community-wide immunity. By consequence of a large proportion of the population becoming immune after exposure to the disease, person-to-person spread can potentially be mitigated. This does not confer immunity to the virus at the individual level; rather, it reduces the risk of vulnerable people coming in contact with the pathogen.
Unfortunately, depending on herd immunity as a way to deal with COVID-19 has not worked well, even in well-contained countries like Sweden, where a disproportionate number of their most vulnerable populations have died. It is self-evident that containment strategies with vaccination may be our best way forward to achieve herd immunity. Not surrendering to the virus.
Am I safe from reinfection?
In all honesty, we’re not entirely sure. But it is important to recognize a few points when considering your relative safety.
- The immune system is far from perfect. Not everyone has a robust immune response. And in those who do, the immune response can wane over time, potentially allowing for reinfection. While rare, there have already been some clearly documented reinfections, four that have been confirmed and published; two patients (in Nevada and Ecuador) actually fared worse the second time around.
- The virus can mutate and escape detection by the immune system. One could still be susceptible to reinfection from a different strain. (At least, this remains the case with the influenza virus.) There is some evidence that SARS-CoV-2 does not mutate rapidly, and hence this may not be a problem. But we don’t know for certain, at least as of yet.
- Even a vigorous immune response can be overwhelmed by the virus. It is unclear whether the relative length of time and the amount of virus exposure could undermine a previously primed immune system.
A prior infection and a consequent healthy immunity may help you combat a reinfection but it does not prevent you from harboring or carrying the virus. You may be asymptomatic, but you can still be a carrier and spread the infection. I am a strong advocate for limiting your exposure to others no matter your previous exposure status, in order to limit the spread of the virus.
So, what should I do?
I guess the answer is that you can’t be too careful. Not everyone has had their antibody levels tested, and even if positive, it is unclear how well that affords protection. It is best to presume that you are vulnerable for a reinfection and that you can still carry and spread the virus. This may be the safest approach until we actually achieve herd immunity through vaccination.
Even then, for a period of time, there will remain a sense of uncertainty. So, containment strategies inclusive of distancing and masking will and should remain a way of life at least until mid-2021, when we will be in a better position to reassess the landscape.
The surge is back. As I repay my debt and get back to the front line, I will continue to mask up and practice distancing. I am taking no chances of getting reinfected or being an asymptomatic carrier.
I had COVID, I also have antibodies, and I will be taking the vaccine. I implore you all to do the same.
Jag Singh is a physician, scientist, and professor at Harvard. He is passionate about social issues, leadership, digital health, and medical innovations. You can follow him on Twitter @JagSinghMD.
A version of this article first appeared on Medscape.com.
Is it over or do I have to brace myself for the possibility of a reinfection? Moreover, could the second time potentially be worse than the first?
I was diagnosed with COVID in March of this year. After spending 10 days in the hospital, and one night in the ICU, it took another 2 months for the air-hunger, headaches, and fatigue to completely resolve. Compared with many other unfortunate victims, I did all right – and I am very grateful for the care I received.
Now, as the surge in cases takes new life, I will be on the front lines taking care of patients. Having had an eventful personal encounter with the virus, I now have a unique vantage point and remain fully committed to paying my fortunate circumstances forward. Although I can’t help but have the same question faced by millions of others: Am I safe now?
It is no surprise that studies have shown health care workers comprising 6% of COVID hospital admissions, with one-third of these admissions being nurses. Recently, we heard that over 900 health care workers at Mayo Clinic had acquired the infection in the first 2 weeks of the ongoing second COVID surge. Are these frontline workers protected? Can they return to work with no fear of a rerun? Or, for that matter, anyone who has been afflicted by COVID – are they now forever immune?
There are no clear answers here. But to understand this a little, let’s quickly revisit some basic principles of immunity.
Innate and adaptive immunity
Simply put, there are two forms of immunity: innate and adaptive. Innate immunity encompasses our body’s natural protective mechanisms that come into play almost immediately. This enables recognition of the virus and activates an immediate antiviral defense and attempt at removal of the infective agent. This, however, does not always do the job. Accordingly, a couple weeks after the initial exposure to the pathogen, adaptive immunity is invoked. Circulating white blood cells within our body recognize the virus and set off an immune response, involving the activation of T and B cells that actively attack the infective agent. It is this T- and B-cell–mediated immunity that should protect one against a second infection with the same agent.
What about herd immunity?
Herd immunity is defined as essentially yielding to the virus and letting it spread naturally in order to develop community-wide immunity. By consequence of a large proportion of the population becoming immune after exposure to the disease, person-to-person spread can potentially be mitigated. This does not confer immunity to the virus at the individual level; rather, it reduces the risk of vulnerable people coming in contact with the pathogen.
Unfortunately, depending on herd immunity as a way to deal with COVID-19 has not worked well, even in well-contained countries like Sweden, where a disproportionate number of their most vulnerable populations have died. It is self-evident that containment strategies with vaccination may be our best way forward to achieve herd immunity. Not surrendering to the virus.
Am I safe from reinfection?
In all honesty, we’re not entirely sure. But it is important to recognize a few points when considering your relative safety.
- The immune system is far from perfect. Not everyone has a robust immune response. And in those who do, the immune response can wane over time, potentially allowing for reinfection. While rare, there have already been some clearly documented reinfections, four that have been confirmed and published; two patients (in Nevada and Ecuador) actually fared worse the second time around.
- The virus can mutate and escape detection by the immune system. One could still be susceptible to reinfection from a different strain. (At least, this remains the case with the influenza virus.) There is some evidence that SARS-CoV-2 does not mutate rapidly, and hence this may not be a problem. But we don’t know for certain, at least as of yet.
- Even a vigorous immune response can be overwhelmed by the virus. It is unclear whether the relative length of time and the amount of virus exposure could undermine a previously primed immune system.
A prior infection and a consequent healthy immunity may help you combat a reinfection but it does not prevent you from harboring or carrying the virus. You may be asymptomatic, but you can still be a carrier and spread the infection. I am a strong advocate for limiting your exposure to others no matter your previous exposure status, in order to limit the spread of the virus.
So, what should I do?
I guess the answer is that you can’t be too careful. Not everyone has had their antibody levels tested, and even if positive, it is unclear how well that affords protection. It is best to presume that you are vulnerable for a reinfection and that you can still carry and spread the virus. This may be the safest approach until we actually achieve herd immunity through vaccination.
Even then, for a period of time, there will remain a sense of uncertainty. So, containment strategies inclusive of distancing and masking will and should remain a way of life at least until mid-2021, when we will be in a better position to reassess the landscape.
The surge is back. As I repay my debt and get back to the front line, I will continue to mask up and practice distancing. I am taking no chances of getting reinfected or being an asymptomatic carrier.
I had COVID, I also have antibodies, and I will be taking the vaccine. I implore you all to do the same.
Jag Singh is a physician, scientist, and professor at Harvard. He is passionate about social issues, leadership, digital health, and medical innovations. You can follow him on Twitter @JagSinghMD.
A version of this article first appeared on Medscape.com.
Is it over or do I have to brace myself for the possibility of a reinfection? Moreover, could the second time potentially be worse than the first?
I was diagnosed with COVID in March of this year. After spending 10 days in the hospital, and one night in the ICU, it took another 2 months for the air-hunger, headaches, and fatigue to completely resolve. Compared with many other unfortunate victims, I did all right – and I am very grateful for the care I received.
Now, as the surge in cases takes new life, I will be on the front lines taking care of patients. Having had an eventful personal encounter with the virus, I now have a unique vantage point and remain fully committed to paying my fortunate circumstances forward. Although I can’t help but have the same question faced by millions of others: Am I safe now?
It is no surprise that studies have shown health care workers comprising 6% of COVID hospital admissions, with one-third of these admissions being nurses. Recently, we heard that over 900 health care workers at Mayo Clinic had acquired the infection in the first 2 weeks of the ongoing second COVID surge. Are these frontline workers protected? Can they return to work with no fear of a rerun? Or, for that matter, anyone who has been afflicted by COVID – are they now forever immune?
There are no clear answers here. But to understand this a little, let’s quickly revisit some basic principles of immunity.
Innate and adaptive immunity
Simply put, there are two forms of immunity: innate and adaptive. Innate immunity encompasses our body’s natural protective mechanisms that come into play almost immediately. This enables recognition of the virus and activates an immediate antiviral defense and attempt at removal of the infective agent. This, however, does not always do the job. Accordingly, a couple weeks after the initial exposure to the pathogen, adaptive immunity is invoked. Circulating white blood cells within our body recognize the virus and set off an immune response, involving the activation of T and B cells that actively attack the infective agent. It is this T- and B-cell–mediated immunity that should protect one against a second infection with the same agent.
What about herd immunity?
Herd immunity is defined as essentially yielding to the virus and letting it spread naturally in order to develop community-wide immunity. By consequence of a large proportion of the population becoming immune after exposure to the disease, person-to-person spread can potentially be mitigated. This does not confer immunity to the virus at the individual level; rather, it reduces the risk of vulnerable people coming in contact with the pathogen.
Unfortunately, depending on herd immunity as a way to deal with COVID-19 has not worked well, even in well-contained countries like Sweden, where a disproportionate number of their most vulnerable populations have died. It is self-evident that containment strategies with vaccination may be our best way forward to achieve herd immunity. Not surrendering to the virus.
Am I safe from reinfection?
In all honesty, we’re not entirely sure. But it is important to recognize a few points when considering your relative safety.
- The immune system is far from perfect. Not everyone has a robust immune response. And in those who do, the immune response can wane over time, potentially allowing for reinfection. While rare, there have already been some clearly documented reinfections, four that have been confirmed and published; two patients (in Nevada and Ecuador) actually fared worse the second time around.
- The virus can mutate and escape detection by the immune system. One could still be susceptible to reinfection from a different strain. (At least, this remains the case with the influenza virus.) There is some evidence that SARS-CoV-2 does not mutate rapidly, and hence this may not be a problem. But we don’t know for certain, at least as of yet.
- Even a vigorous immune response can be overwhelmed by the virus. It is unclear whether the relative length of time and the amount of virus exposure could undermine a previously primed immune system.
A prior infection and a consequent healthy immunity may help you combat a reinfection but it does not prevent you from harboring or carrying the virus. You may be asymptomatic, but you can still be a carrier and spread the infection. I am a strong advocate for limiting your exposure to others no matter your previous exposure status, in order to limit the spread of the virus.
So, what should I do?
I guess the answer is that you can’t be too careful. Not everyone has had their antibody levels tested, and even if positive, it is unclear how well that affords protection. It is best to presume that you are vulnerable for a reinfection and that you can still carry and spread the virus. This may be the safest approach until we actually achieve herd immunity through vaccination.
Even then, for a period of time, there will remain a sense of uncertainty. So, containment strategies inclusive of distancing and masking will and should remain a way of life at least until mid-2021, when we will be in a better position to reassess the landscape.
The surge is back. As I repay my debt and get back to the front line, I will continue to mask up and practice distancing. I am taking no chances of getting reinfected or being an asymptomatic carrier.
I had COVID, I also have antibodies, and I will be taking the vaccine. I implore you all to do the same.
Jag Singh is a physician, scientist, and professor at Harvard. He is passionate about social issues, leadership, digital health, and medical innovations. You can follow him on Twitter @JagSinghMD.
A version of this article first appeared on Medscape.com.
13 best practices to increase hospitalist billing efficiency
As an aspiring physician, I like learning about how things work. Since medical students learn very little about the “business” of medicine in school, this led me to pioneer a project on missed billing by hospitalists at a medium-sized hospital in the northeastern US. Although hospitalists do a tremendous amount of work, they do not always bill for what they are doing. The question became: Why are hospitalists missing charges and what can we do to stop it?

Shortly into my study, I recognized there was little daily communication between the administrators and the hospitalists; neither the hospitalists nor administrators understood the different dynamics that the others faced in their own workplace. It became apparent that administrators needed to learn what was important to hospitalists and to address them at their level in order to bring about change.
Some trending themes emerged as I started shadowing the hospitalists. Many of them asked how this project would benefit them. They argued that administrative needs should be dealt with at the administrative level. A major point was made that current incentives, such as the bonuses given for exceeding a certain number of RVUs, were not the motivating force behind their work ethics. From my observations, the motivating factors were the quality of their patient care, the needs of their patients, and teaching. The hospitalists also were eager to teach and continually instructed me on clinical skills and how to be a better medical student.
Bonuses or notoriety didn’t seem to be the main incentives for them. However, efficiency – especially in rounding – was important, and that became the focal point of the project. I found several studies that showed that improvements in aspects of rounding led to increased quality of patient care, decreased burnout, increased patient satisfaction, and decreased workload and discussed some of those findings with the hospitalists.1-10 When the hospitalists felt that their concerns were being heard, they became even more involved in the project, and the administrators and hospitalists started working together as a team.
One hospitalist spent two hours helping me design the platform that would be used for hospitalists to report barriers in their rounding process that may cause them to miss a charge. Once we identified those barriers, we discussed the possibility of standardizing their workflow based off these data. Many hospitalists argued that each physician has unique skills and practices that make them successful; therefore, the disruption of an already established workflow may cause a decrease in efficiency.
The hospitalists and I talked a lot about the importance of them rounding more efficiently and how that could positively affect the time that they have with their patients and themselves. We discussed that due to the additional work missed billing causes, minimizing this burden can possibly help decrease burnout. As a result, seven hospitalists, the administrative staff, and I met and created thirteen best practices, six of which they were able to get approved to use immediately. To note, hospitalists bill differently; some use a software company, fill out paper forms still or have integration within their EMR. Although these solutions were made for a program which has the ability to bill within the EMR, many of the principles will apply to your program too.

The 13 best practices that the seven hospitalists agreed upon are the following:
When a doctor signs a note, it opens a charge option or there is a hard stop.
Charge delinquencies are sent via email to the hospitalist.
Standardize that hospitalists charge directly after writing a note consistently as part of their workflow.*
Prioritize discharges before rounding.*
Standardize the use of the “my prof charges” column, a feature of this hospital’s EMR system that tells them if they had made a charge to a patient or not, in order to remind them to/confirm billing a patient.*
Create reports by the EMR system to provide charge data for individual providers.
Create a report for bill vs note to help providers self-audit. At this hospital, this feature was offered to the administrators as a way to audit their providers and doctors.
Ensure that when a patient is seen by a physician hospitalist as well as an NP/PA hospitalist, the appropriate charge for the physician is entered.
Notifications get sent to the physician hospitalist if a charge gets deleted by another person (e.g., NP/PA hospitalist).
Handoff of daily rounding sheets, or a paper copy of the patients assigned to a hospitalist for his/her shift, at the end of the shift to the project specialist.*
To keep the rounding sheets a complete and accurate account of the patients seen by the hospitalist.*
Hospitalists are to complete and check all billing at the end of their shift at the latest.*
Hospitalists are to participate on Provider Efficiency Training to optimize workflow, by creating more efficient note-writing behavior using Dragon.
*Indicates the practices the hospitalists were able to implement immediately. Practices 1, 2, 6, 7, and 9 request EMR changes. Practice 8 was already an established practice the hospitalists wished to continue. Practice 13 was suggested by the Lean Director for the continuation of a previous project.
Six of the best practices were easier to implement right away because they were at the discretion of the hospitalists. We found that the hospitalists who had the highest billing performances were more likely to start writing notes and charge earlier while rounding. Those who had poorer billing performances were more likely to leave all note writing and billing towards the end of their shift. The few exceptions (hospitalists who left all note writing and charging to the end of their shift yet had high billing performances) were found to have a consistent and standardized workflow. This was unlike the hospitalists who had the lowest billing performances. Having practices that help remind hospitalists to bill will surely help prevent missed billing, but because of the findings from this project, it was important to have consistent and standardized practices to additionally improve missed billing.

When we followed up with the hospitalist division two months later, we learned they were making great progress. Not only were hospitalists using their best practices, but in working with the administrators, they were designing sessions to further educate fellow hospitalists to prevent further missed billing. These sessions outlined shortcuts, resources and ways hospitalists may modify their personal EMR accounts to prevent missed billing. None of the progress could have been made without first understanding and addressing what is truly important to the hospitalists.
In summary, we noted these general observations in this project:
- Hospitalists favor solutions that benefit them or their patients.
- Hospitalists want to be part of the solution process.
- Hospitalists were more likely to accept ideas to improve their rounding if it meant they could keep their routine.
Obstacles exist in our health care system that prevent administrators and hospitalists from working together as a team. The more we are able to communicate and collaborate to fix problems in the health system, the more we can use the system to our mutual advantage. With the ongoing changes in medicine, especially during uncertain times, better communication needs be a major priority to affect positive change.
Ms. Mirabella attends the Frank H. Netter MD School of Medicine at Quinnipiac University, Hamden, Conn., in the class of 2022. She has interests in internal/hospital medicine, primary care, and health management and leadership. Dr. Rosenberg is associate professor at the Frank H. Netter MD School of Medicine at Quinnipiac University where she is director of clinical skills coaching. Dr. Kiassat is associate dean of the School of Engineering and associate clinical professor at Frank H. Netter MD School of Medicine, at Quinnipiac University. His research interests are in process improvement in health care, using Lean Six Sigma.
References
1. Burdick K, et al. Bedside interprofessional rounding. J Patient Exp. 2017;4(1):22-27. doi: 10.1177/2374373517692910.
2. Patel CR. Improving communication between hospitalists and consultants. The Hospital Leader. 2018. https://thehospitalleader.org/improving-communication-between-hospitalists-and-consultants/.
3. Adams TN, et al. Hospitalist perspective of interactions with medicine subspecialty consult services. J Hosp Med. 2018;13(5):318-323. doi: 10.12788/jhm.2882.
4. Michtalik HJ, et al. Impact of attending physician workload on patient care: A survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377. doi: 10.1001/jamainternmed.2013.1864.
5. Chandra R, et al. How hospitalists can improve efficiency on inpatient wards. The Hospitalist. 2014. https://www.the-hospitalist.org/hospitalist/article/126231/how-hospitalists-can-improve-efficiency-inpatient-wards.
6. Chand DV. Observational study using the tools of lean six sigma to improve the efficiency of the resident rounding process. J Grad Med Educ. 2011;3(2):144-150. doi: 10.4300/JGME-D-10-00116.1.
7. O’Leary KJ, et al. How hospitalists spend their time: Insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93. doi: 10.1002/jhm.88.
8. Wachter RM. Hospitalist workload: The search for the magic number. JAMA Intern Med. 2014;174(5):794-795. doi: 10.1001/jamainternmed.2014.18.
9. Bryson C, et al. Geographical assignment of hospitalists in an urban teaching hospital: Feasibility and impact on efficiency and provider satisfaction. Hospital Practice. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884.
10. Calderon AS, et al. Transforming ward rounds through rounding-in-flow. J Grad Med Educ. 2014 Dec;6(4):750-5. doi: 10.4300/JGME-D-13-00324.1.
As an aspiring physician, I like learning about how things work. Since medical students learn very little about the “business” of medicine in school, this led me to pioneer a project on missed billing by hospitalists at a medium-sized hospital in the northeastern US. Although hospitalists do a tremendous amount of work, they do not always bill for what they are doing. The question became: Why are hospitalists missing charges and what can we do to stop it?
Shortly into my study, I recognized there was little daily communication between the administrators and the hospitalists; neither the hospitalists nor administrators understood the different dynamics that the others faced in their own workplace. It became apparent that administrators needed to learn what was important to hospitalists and to address them at their level in order to bring about change.
Some trending themes emerged as I started shadowing the hospitalists. Many of them asked how this project would benefit them. They argued that administrative needs should be dealt with at the administrative level. A major point was made that current incentives, such as the bonuses given for exceeding a certain number of RVUs, were not the motivating force behind their work ethics. From my observations, the motivating factors were the quality of their patient care, the needs of their patients, and teaching. The hospitalists also were eager to teach and continually instructed me on clinical skills and how to be a better medical student.
Bonuses or notoriety didn’t seem to be the main incentives for them. However, efficiency – especially in rounding – was important, and that became the focal point of the project. I found several studies that showed that improvements in aspects of rounding led to increased quality of patient care, decreased burnout, increased patient satisfaction, and decreased workload and discussed some of those findings with the hospitalists.1-10 When the hospitalists felt that their concerns were being heard, they became even more involved in the project, and the administrators and hospitalists started working together as a team.
One hospitalist spent two hours helping me design the platform that would be used for hospitalists to report barriers in their rounding process that may cause them to miss a charge. Once we identified those barriers, we discussed the possibility of standardizing their workflow based off these data. Many hospitalists argued that each physician has unique skills and practices that make them successful; therefore, the disruption of an already established workflow may cause a decrease in efficiency.
The hospitalists and I talked a lot about the importance of them rounding more efficiently and how that could positively affect the time that they have with their patients and themselves. We discussed that due to the additional work missed billing causes, minimizing this burden can possibly help decrease burnout. As a result, seven hospitalists, the administrative staff, and I met and created thirteen best practices, six of which they were able to get approved to use immediately. To note, hospitalists bill differently; some use a software company, fill out paper forms still or have integration within their EMR. Although these solutions were made for a program which has the ability to bill within the EMR, many of the principles will apply to your program too.
The 13 best practices that the seven hospitalists agreed upon are the following:
When a doctor signs a note, it opens a charge option or there is a hard stop.
Charge delinquencies are sent via email to the hospitalist.
Standardize that hospitalists charge directly after writing a note consistently as part of their workflow.*
Prioritize discharges before rounding.*
Standardize the use of the “my prof charges” column, a feature of this hospital’s EMR system that tells them if they had made a charge to a patient or not, in order to remind them to/confirm billing a patient.*
Create reports by the EMR system to provide charge data for individual providers.
Create a report for bill vs note to help providers self-audit. At this hospital, this feature was offered to the administrators as a way to audit their providers and doctors.
Ensure that when a patient is seen by a physician hospitalist as well as an NP/PA hospitalist, the appropriate charge for the physician is entered.
Notifications get sent to the physician hospitalist if a charge gets deleted by another person (e.g., NP/PA hospitalist).
Handoff of daily rounding sheets, or a paper copy of the patients assigned to a hospitalist for his/her shift, at the end of the shift to the project specialist.*
To keep the rounding sheets a complete and accurate account of the patients seen by the hospitalist.*
Hospitalists are to complete and check all billing at the end of their shift at the latest.*
Hospitalists are to participate on Provider Efficiency Training to optimize workflow, by creating more efficient note-writing behavior using Dragon.
*Indicates the practices the hospitalists were able to implement immediately. Practices 1, 2, 6, 7, and 9 request EMR changes. Practice 8 was already an established practice the hospitalists wished to continue. Practice 13 was suggested by the Lean Director for the continuation of a previous project.
Six of the best practices were easier to implement right away because they were at the discretion of the hospitalists. We found that the hospitalists who had the highest billing performances were more likely to start writing notes and charge earlier while rounding. Those who had poorer billing performances were more likely to leave all note writing and billing towards the end of their shift. The few exceptions (hospitalists who left all note writing and charging to the end of their shift yet had high billing performances) were found to have a consistent and standardized workflow. This was unlike the hospitalists who had the lowest billing performances. Having practices that help remind hospitalists to bill will surely help prevent missed billing, but because of the findings from this project, it was important to have consistent and standardized practices to additionally improve missed billing.
When we followed up with the hospitalist division two months later, we learned they were making great progress. Not only were hospitalists using their best practices, but in working with the administrators, they were designing sessions to further educate fellow hospitalists to prevent further missed billing. These sessions outlined shortcuts, resources and ways hospitalists may modify their personal EMR accounts to prevent missed billing. None of the progress could have been made without first understanding and addressing what is truly important to the hospitalists.
In summary, we noted these general observations in this project:
- Hospitalists favor solutions that benefit them or their patients.
- Hospitalists want to be part of the solution process.
- Hospitalists were more likely to accept ideas to improve their rounding if it meant they could keep their routine.
Obstacles exist in our health care system that prevent administrators and hospitalists from working together as a team. The more we are able to communicate and collaborate to fix problems in the health system, the more we can use the system to our mutual advantage. With the ongoing changes in medicine, especially during uncertain times, better communication needs be a major priority to affect positive change.
Ms. Mirabella attends the Frank H. Netter MD School of Medicine at Quinnipiac University, Hamden, Conn., in the class of 2022. She has interests in internal/hospital medicine, primary care, and health management and leadership. Dr. Rosenberg is associate professor at the Frank H. Netter MD School of Medicine at Quinnipiac University where she is director of clinical skills coaching. Dr. Kiassat is associate dean of the School of Engineering and associate clinical professor at Frank H. Netter MD School of Medicine, at Quinnipiac University. His research interests are in process improvement in health care, using Lean Six Sigma.
References
1. Burdick K, et al. Bedside interprofessional rounding. J Patient Exp. 2017;4(1):22-27. doi: 10.1177/2374373517692910.
2. Patel CR. Improving communication between hospitalists and consultants. The Hospital Leader. 2018. https://thehospitalleader.org/improving-communication-between-hospitalists-and-consultants/.
3. Adams TN, et al. Hospitalist perspective of interactions with medicine subspecialty consult services. J Hosp Med. 2018;13(5):318-323. doi: 10.12788/jhm.2882.
4. Michtalik HJ, et al. Impact of attending physician workload on patient care: A survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377. doi: 10.1001/jamainternmed.2013.1864.
5. Chandra R, et al. How hospitalists can improve efficiency on inpatient wards. The Hospitalist. 2014. https://www.the-hospitalist.org/hospitalist/article/126231/how-hospitalists-can-improve-efficiency-inpatient-wards.
6. Chand DV. Observational study using the tools of lean six sigma to improve the efficiency of the resident rounding process. J Grad Med Educ. 2011;3(2):144-150. doi: 10.4300/JGME-D-10-00116.1.
7. O’Leary KJ, et al. How hospitalists spend their time: Insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93. doi: 10.1002/jhm.88.
8. Wachter RM. Hospitalist workload: The search for the magic number. JAMA Intern Med. 2014;174(5):794-795. doi: 10.1001/jamainternmed.2014.18.
9. Bryson C, et al. Geographical assignment of hospitalists in an urban teaching hospital: Feasibility and impact on efficiency and provider satisfaction. Hospital Practice. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884.
10. Calderon AS, et al. Transforming ward rounds through rounding-in-flow. J Grad Med Educ. 2014 Dec;6(4):750-5. doi: 10.4300/JGME-D-13-00324.1.
As an aspiring physician, I like learning about how things work. Since medical students learn very little about the “business” of medicine in school, this led me to pioneer a project on missed billing by hospitalists at a medium-sized hospital in the northeastern US. Although hospitalists do a tremendous amount of work, they do not always bill for what they are doing. The question became: Why are hospitalists missing charges and what can we do to stop it?
Shortly into my study, I recognized there was little daily communication between the administrators and the hospitalists; neither the hospitalists nor administrators understood the different dynamics that the others faced in their own workplace. It became apparent that administrators needed to learn what was important to hospitalists and to address them at their level in order to bring about change.
Some trending themes emerged as I started shadowing the hospitalists. Many of them asked how this project would benefit them. They argued that administrative needs should be dealt with at the administrative level. A major point was made that current incentives, such as the bonuses given for exceeding a certain number of RVUs, were not the motivating force behind their work ethics. From my observations, the motivating factors were the quality of their patient care, the needs of their patients, and teaching. The hospitalists also were eager to teach and continually instructed me on clinical skills and how to be a better medical student.
Bonuses or notoriety didn’t seem to be the main incentives for them. However, efficiency – especially in rounding – was important, and that became the focal point of the project. I found several studies that showed that improvements in aspects of rounding led to increased quality of patient care, decreased burnout, increased patient satisfaction, and decreased workload and discussed some of those findings with the hospitalists.1-10 When the hospitalists felt that their concerns were being heard, they became even more involved in the project, and the administrators and hospitalists started working together as a team.
One hospitalist spent two hours helping me design the platform that would be used for hospitalists to report barriers in their rounding process that may cause them to miss a charge. Once we identified those barriers, we discussed the possibility of standardizing their workflow based off these data. Many hospitalists argued that each physician has unique skills and practices that make them successful; therefore, the disruption of an already established workflow may cause a decrease in efficiency.
The hospitalists and I talked a lot about the importance of them rounding more efficiently and how that could positively affect the time that they have with their patients and themselves. We discussed that due to the additional work missed billing causes, minimizing this burden can possibly help decrease burnout. As a result, seven hospitalists, the administrative staff, and I met and created thirteen best practices, six of which they were able to get approved to use immediately. To note, hospitalists bill differently; some use a software company, fill out paper forms still or have integration within their EMR. Although these solutions were made for a program which has the ability to bill within the EMR, many of the principles will apply to your program too.
The 13 best practices that the seven hospitalists agreed upon are the following:
When a doctor signs a note, it opens a charge option or there is a hard stop.
Charge delinquencies are sent via email to the hospitalist.
Standardize that hospitalists charge directly after writing a note consistently as part of their workflow.*
Prioritize discharges before rounding.*
Standardize the use of the “my prof charges” column, a feature of this hospital’s EMR system that tells them if they had made a charge to a patient or not, in order to remind them to/confirm billing a patient.*
Create reports by the EMR system to provide charge data for individual providers.
Create a report for bill vs note to help providers self-audit. At this hospital, this feature was offered to the administrators as a way to audit their providers and doctors.
Ensure that when a patient is seen by a physician hospitalist as well as an NP/PA hospitalist, the appropriate charge for the physician is entered.
Notifications get sent to the physician hospitalist if a charge gets deleted by another person (e.g., NP/PA hospitalist).
Handoff of daily rounding sheets, or a paper copy of the patients assigned to a hospitalist for his/her shift, at the end of the shift to the project specialist.*
To keep the rounding sheets a complete and accurate account of the patients seen by the hospitalist.*
Hospitalists are to complete and check all billing at the end of their shift at the latest.*
Hospitalists are to participate on Provider Efficiency Training to optimize workflow, by creating more efficient note-writing behavior using Dragon.
*Indicates the practices the hospitalists were able to implement immediately. Practices 1, 2, 6, 7, and 9 request EMR changes. Practice 8 was already an established practice the hospitalists wished to continue. Practice 13 was suggested by the Lean Director for the continuation of a previous project.
Six of the best practices were easier to implement right away because they were at the discretion of the hospitalists. We found that the hospitalists who had the highest billing performances were more likely to start writing notes and charge earlier while rounding. Those who had poorer billing performances were more likely to leave all note writing and billing towards the end of their shift. The few exceptions (hospitalists who left all note writing and charging to the end of their shift yet had high billing performances) were found to have a consistent and standardized workflow. This was unlike the hospitalists who had the lowest billing performances. Having practices that help remind hospitalists to bill will surely help prevent missed billing, but because of the findings from this project, it was important to have consistent and standardized practices to additionally improve missed billing.
When we followed up with the hospitalist division two months later, we learned they were making great progress. Not only were hospitalists using their best practices, but in working with the administrators, they were designing sessions to further educate fellow hospitalists to prevent further missed billing. These sessions outlined shortcuts, resources and ways hospitalists may modify their personal EMR accounts to prevent missed billing. None of the progress could have been made without first understanding and addressing what is truly important to the hospitalists.
In summary, we noted these general observations in this project:
- Hospitalists favor solutions that benefit them or their patients.
- Hospitalists want to be part of the solution process.
- Hospitalists were more likely to accept ideas to improve their rounding if it meant they could keep their routine.
Obstacles exist in our health care system that prevent administrators and hospitalists from working together as a team. The more we are able to communicate and collaborate to fix problems in the health system, the more we can use the system to our mutual advantage. With the ongoing changes in medicine, especially during uncertain times, better communication needs be a major priority to affect positive change.
Ms. Mirabella attends the Frank H. Netter MD School of Medicine at Quinnipiac University, Hamden, Conn., in the class of 2022. She has interests in internal/hospital medicine, primary care, and health management and leadership. Dr. Rosenberg is associate professor at the Frank H. Netter MD School of Medicine at Quinnipiac University where she is director of clinical skills coaching. Dr. Kiassat is associate dean of the School of Engineering and associate clinical professor at Frank H. Netter MD School of Medicine, at Quinnipiac University. His research interests are in process improvement in health care, using Lean Six Sigma.
References
1. Burdick K, et al. Bedside interprofessional rounding. J Patient Exp. 2017;4(1):22-27. doi: 10.1177/2374373517692910.
2. Patel CR. Improving communication between hospitalists and consultants. The Hospital Leader. 2018. https://thehospitalleader.org/improving-communication-between-hospitalists-and-consultants/.
3. Adams TN, et al. Hospitalist perspective of interactions with medicine subspecialty consult services. J Hosp Med. 2018;13(5):318-323. doi: 10.12788/jhm.2882.
4. Michtalik HJ, et al. Impact of attending physician workload on patient care: A survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377. doi: 10.1001/jamainternmed.2013.1864.
5. Chandra R, et al. How hospitalists can improve efficiency on inpatient wards. The Hospitalist. 2014. https://www.the-hospitalist.org/hospitalist/article/126231/how-hospitalists-can-improve-efficiency-inpatient-wards.
6. Chand DV. Observational study using the tools of lean six sigma to improve the efficiency of the resident rounding process. J Grad Med Educ. 2011;3(2):144-150. doi: 10.4300/JGME-D-10-00116.1.
7. O’Leary KJ, et al. How hospitalists spend their time: Insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93. doi: 10.1002/jhm.88.
8. Wachter RM. Hospitalist workload: The search for the magic number. JAMA Intern Med. 2014;174(5):794-795. doi: 10.1001/jamainternmed.2014.18.
9. Bryson C, et al. Geographical assignment of hospitalists in an urban teaching hospital: Feasibility and impact on efficiency and provider satisfaction. Hospital Practice. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884.
10. Calderon AS, et al. Transforming ward rounds through rounding-in-flow. J Grad Med Educ. 2014 Dec;6(4):750-5. doi: 10.4300/JGME-D-13-00324.1.
Six big changes coming for office-visit coding
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
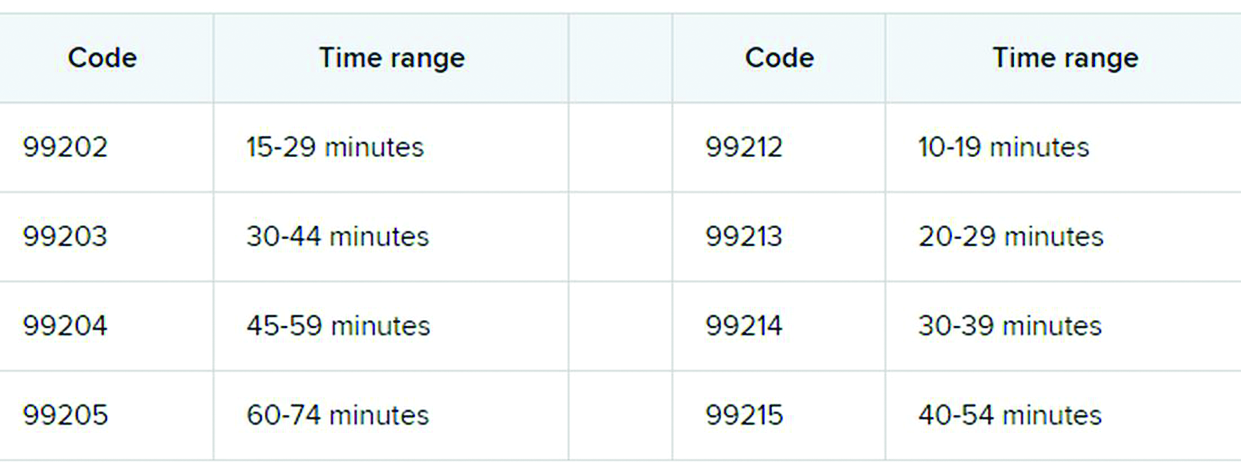
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
COVID-19 and patient safety in the medical office
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
As the pandemic hits its third nationwide surge, families are gathering for the holidays, and medical practices are preparing for a potential increase in cases. Medical offices in states that were not strongly affected by the first and second waves of the virus may now be facing an influx of COVID-19 patients. Therefore, medical offices must remain very attentive to the widespread outbreak of COVID-19, continuing to proactively take steps to safely manage patients while protecting clinical staff.
Here are tips and resources for this season of the pandemic:
- Documentation: Maintain administrative records of how you have adapted to the evolving crisis, including the challenges you faced. For details, see Keep a COVID-19 Diary: Document Now in Case of Future Lawsuits.
- Legislation and Guidance: Reference the CDC; your state medical board; professional societies; and federal, state, and local authorities daily for public health guidance and new legislation, as this continues to be a fluid situation.
- Screening Criteria: Follow the CDC’s patient assessment protocol for early disease detection for patients presenting to your practice. Patients should be screened using these guidelines: Overview of Testing for SARS-CoV-2 (COVID-19). Essential visitors to your facility should also be assessed for symptoms of coronavirus and contact exposure and redirected to remain outside if suspect.
- Accepting Patients: Do not turn patients away simply because a patient calls with acute respiratory symptoms. Refusing assessment/care may lead to concerns of patient abandonment.
- Designated Triage Location: Check with your local public health authorities for locations designated to triage suspected patients, so exposure is limited in general medical offices.
- Telehealth Triage: Licensed staff should be trained in triage protocol to determine which patients can be managed safely at home. See Healthcare Facilities: Managing Operations During the COVID-19 Pandemic. The Doctors Company offers resources on telemedicine in our COVID-19 Telehealth Resource Center.
- Patient Testing: When there is a reasonable presumption that a patient may have been exposed to COVID-19, contact the local or state health department to coordinate testing using available community resources. See the CDC’s Testing for COVID-19 , the COVID-19 Testing Overview, and the Clinician Call Center.
- Elective Services: Check with regional governmental and health authorities on the provision of nonessential and elective health care visits and group-related activities. Many states continue or have reinstated restrictions on the provision of nonurgent, elective surgeries and procedures.
- Patient Precautions: Educational resources, including posters for use in the medical office, are available from the WHO and for health care workers from the CDC (Contact Precautions, Droplet Precautions, and Airborne Precautions). Reference the CDC’s and Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19) for patient management guidance.
- Provider/Staff Precautions: Follow Standard Precautions and Transmission-Based Precautions, including gloves, gowns, protective eyewear, and NIOSH-certified N95 respirators that have been properly fit-tested. If there is a shortage of N95 respirators in your facility, access current CDC respirator recommendations and review Optimizing Personal Protective Equipment (PPE) Supplies.
- Limit Exposure: Limit staff exposure to suspected patients, with the exam room door kept closed. Ideally, the designated exam room should be at the back of the office, far away from other staff and patients.
- Surface Disinfection: Once the patient exits the room, conduct surface disinfection while staff continues to wear PPE.
- Patient Education: Provide up-to-date, factual information on the virus to suspected COVID-19–positive patients and their close contacts.
- Provider/Staff Exposure: Screen health care personnel daily for symptoms/contacts relevant to COVID-19. Any unprotected occupational exposure by staff members should be assessed and monitored. See Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19. Should providers and/or staff test positive within your facility, conduct and document a risk assessment identifying contacts, type of interaction, and PPE in use, then contact local health authorities for additional instruction. The CDC provides guidance here under the section “Infection Control.” The health department may assist with patient notification if determined to be necessary. For return-to-work guidance, review the Criteria for Return to Work for Healthcare Personnel with SARS-CoV-2 Infection (Interim Guidance).
- Staff Training: Provide and document additional staff training as protocols change. Maintain training records in administrative files.
Ms. Hill is senior patient safety risk manager at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
As the pandemic hits its third nationwide surge, families are gathering for the holidays, and medical practices are preparing for a potential increase in cases. Medical offices in states that were not strongly affected by the first and second waves of the virus may now be facing an influx of COVID-19 patients. Therefore, medical offices must remain very attentive to the widespread outbreak of COVID-19, continuing to proactively take steps to safely manage patients while protecting clinical staff.
Here are tips and resources for this season of the pandemic:
- Documentation: Maintain administrative records of how you have adapted to the evolving crisis, including the challenges you faced. For details, see Keep a COVID-19 Diary: Document Now in Case of Future Lawsuits.
- Legislation and Guidance: Reference the CDC; your state medical board; professional societies; and federal, state, and local authorities daily for public health guidance and new legislation, as this continues to be a fluid situation.
- Screening Criteria: Follow the CDC’s patient assessment protocol for early disease detection for patients presenting to your practice. Patients should be screened using these guidelines: Overview of Testing for SARS-CoV-2 (COVID-19). Essential visitors to your facility should also be assessed for symptoms of coronavirus and contact exposure and redirected to remain outside if suspect.
- Accepting Patients: Do not turn patients away simply because a patient calls with acute respiratory symptoms. Refusing assessment/care may lead to concerns of patient abandonment.
- Designated Triage Location: Check with your local public health authorities for locations designated to triage suspected patients, so exposure is limited in general medical offices.
- Telehealth Triage: Licensed staff should be trained in triage protocol to determine which patients can be managed safely at home. See Healthcare Facilities: Managing Operations During the COVID-19 Pandemic. The Doctors Company offers resources on telemedicine in our COVID-19 Telehealth Resource Center.
- Patient Testing: When there is a reasonable presumption that a patient may have been exposed to COVID-19, contact the local or state health department to coordinate testing using available community resources. See the CDC’s Testing for COVID-19 , the COVID-19 Testing Overview, and the Clinician Call Center.
- Elective Services: Check with regional governmental and health authorities on the provision of nonessential and elective health care visits and group-related activities. Many states continue or have reinstated restrictions on the provision of nonurgent, elective surgeries and procedures.
- Patient Precautions: Educational resources, including posters for use in the medical office, are available from the WHO and for health care workers from the CDC (Contact Precautions, Droplet Precautions, and Airborne Precautions). Reference the CDC’s and Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19) for patient management guidance.
- Provider/Staff Precautions: Follow Standard Precautions and Transmission-Based Precautions, including gloves, gowns, protective eyewear, and NIOSH-certified N95 respirators that have been properly fit-tested. If there is a shortage of N95 respirators in your facility, access current CDC respirator recommendations and review Optimizing Personal Protective Equipment (PPE) Supplies.
- Limit Exposure: Limit staff exposure to suspected patients, with the exam room door kept closed. Ideally, the designated exam room should be at the back of the office, far away from other staff and patients.
- Surface Disinfection: Once the patient exits the room, conduct surface disinfection while staff continues to wear PPE.
- Patient Education: Provide up-to-date, factual information on the virus to suspected COVID-19–positive patients and their close contacts.
- Provider/Staff Exposure: Screen health care personnel daily for symptoms/contacts relevant to COVID-19. Any unprotected occupational exposure by staff members should be assessed and monitored. See Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19. Should providers and/or staff test positive within your facility, conduct and document a risk assessment identifying contacts, type of interaction, and PPE in use, then contact local health authorities for additional instruction. The CDC provides guidance here under the section “Infection Control.” The health department may assist with patient notification if determined to be necessary. For return-to-work guidance, review the Criteria for Return to Work for Healthcare Personnel with SARS-CoV-2 Infection (Interim Guidance).
- Staff Training: Provide and document additional staff training as protocols change. Maintain training records in administrative files.
Ms. Hill is senior patient safety risk manager at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
As the pandemic hits its third nationwide surge, families are gathering for the holidays, and medical practices are preparing for a potential increase in cases. Medical offices in states that were not strongly affected by the first and second waves of the virus may now be facing an influx of COVID-19 patients. Therefore, medical offices must remain very attentive to the widespread outbreak of COVID-19, continuing to proactively take steps to safely manage patients while protecting clinical staff.
Here are tips and resources for this season of the pandemic:
- Documentation: Maintain administrative records of how you have adapted to the evolving crisis, including the challenges you faced. For details, see Keep a COVID-19 Diary: Document Now in Case of Future Lawsuits.
- Legislation and Guidance: Reference the CDC; your state medical board; professional societies; and federal, state, and local authorities daily for public health guidance and new legislation, as this continues to be a fluid situation.
- Screening Criteria: Follow the CDC’s patient assessment protocol for early disease detection for patients presenting to your practice. Patients should be screened using these guidelines: Overview of Testing for SARS-CoV-2 (COVID-19). Essential visitors to your facility should also be assessed for symptoms of coronavirus and contact exposure and redirected to remain outside if suspect.
- Accepting Patients: Do not turn patients away simply because a patient calls with acute respiratory symptoms. Refusing assessment/care may lead to concerns of patient abandonment.
- Designated Triage Location: Check with your local public health authorities for locations designated to triage suspected patients, so exposure is limited in general medical offices.
- Telehealth Triage: Licensed staff should be trained in triage protocol to determine which patients can be managed safely at home. See Healthcare Facilities: Managing Operations During the COVID-19 Pandemic. The Doctors Company offers resources on telemedicine in our COVID-19 Telehealth Resource Center.
- Patient Testing: When there is a reasonable presumption that a patient may have been exposed to COVID-19, contact the local or state health department to coordinate testing using available community resources. See the CDC’s Testing for COVID-19 , the COVID-19 Testing Overview, and the Clinician Call Center.
- Elective Services: Check with regional governmental and health authorities on the provision of nonessential and elective health care visits and group-related activities. Many states continue or have reinstated restrictions on the provision of nonurgent, elective surgeries and procedures.
- Patient Precautions: Educational resources, including posters for use in the medical office, are available from the WHO and for health care workers from the CDC (Contact Precautions, Droplet Precautions, and Airborne Precautions). Reference the CDC’s and Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19) for patient management guidance.
- Provider/Staff Precautions: Follow Standard Precautions and Transmission-Based Precautions, including gloves, gowns, protective eyewear, and NIOSH-certified N95 respirators that have been properly fit-tested. If there is a shortage of N95 respirators in your facility, access current CDC respirator recommendations and review Optimizing Personal Protective Equipment (PPE) Supplies.
- Limit Exposure: Limit staff exposure to suspected patients, with the exam room door kept closed. Ideally, the designated exam room should be at the back of the office, far away from other staff and patients.
- Surface Disinfection: Once the patient exits the room, conduct surface disinfection while staff continues to wear PPE.
- Patient Education: Provide up-to-date, factual information on the virus to suspected COVID-19–positive patients and their close contacts.
- Provider/Staff Exposure: Screen health care personnel daily for symptoms/contacts relevant to COVID-19. Any unprotected occupational exposure by staff members should be assessed and monitored. See Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19. Should providers and/or staff test positive within your facility, conduct and document a risk assessment identifying contacts, type of interaction, and PPE in use, then contact local health authorities for additional instruction. The CDC provides guidance here under the section “Infection Control.” The health department may assist with patient notification if determined to be necessary. For return-to-work guidance, review the Criteria for Return to Work for Healthcare Personnel with SARS-CoV-2 Infection (Interim Guidance).
- Staff Training: Provide and document additional staff training as protocols change. Maintain training records in administrative files.
Ms. Hill is senior patient safety risk manager at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Etonogestrel implants may be bent, fractured by trauma or during sports
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.