User login
FDA approves new Merkel cell carcinoma treatment
the agency announced.
This marks the first regulatory approval for the PD-1 inhibitor. The FDA granted accelerated approval for the drug on the basis of tumor response rate and duration of response from the POD1UM-201 trial. Drugmaker Incyte said that “continued approval of Zynyz for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.”
MCC is a rare and aggressive skin cancer with a high rate of metastatic disease and an estimated 5-year overall survival of just 14% among those who present with metastatic disease. Incidence is rapidly increasing in the United States, particularly among adults older than 65 years, Incyte noted.
“More than a third of patients with MCC present with regional or distant metastases, which are associated with high rates of mortality,” principal author Shailender Bhatia, MD, of the University of Washington and Fred Hutchinson Cancer Center, both in Seattle, said in a news release. “The approval of Zynyz offers health care providers another first-line treatment option against MCC that can result in durable responses in patients with metastatic disease.”
POD1UM-201 was an open-label, single-arm, phase 2 study that evaluated the agent in 65 systemic treatment–naive adults with metastatic or recurrent locally advanced MCC.
Overall, 52% of patients had an objective response rate. A complete response was observed in 12 patients (18%), and a partial response was observed in 22 patients (34%).
Duration of response ranged from 1.1 to 24.9 months; 76% of responders experienced responses of 6 months or longer, and 62% experienced responses of 12 months or longer.
Study participants received a 500-mg dose of retifanlimab every 4 weeks for up to 24 weeks or until disease progression or unacceptable toxicity. Serious adverse events occurred in 22% of patients and most often included fatigue, arrhythmia, and pneumonitis; 11% of patients discontinued treatment because of serious adverse events.
Retifanlimab may cause a severe or life-threatening immune response during treatment or after discontinuation. Patients should be advised to immediately report any new or worsening signs or symptoms to their health care provider. Side effects can also be reported to the FDA.
A version of this article first appeared on Medscape.com.
the agency announced.
This marks the first regulatory approval for the PD-1 inhibitor. The FDA granted accelerated approval for the drug on the basis of tumor response rate and duration of response from the POD1UM-201 trial. Drugmaker Incyte said that “continued approval of Zynyz for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.”
MCC is a rare and aggressive skin cancer with a high rate of metastatic disease and an estimated 5-year overall survival of just 14% among those who present with metastatic disease. Incidence is rapidly increasing in the United States, particularly among adults older than 65 years, Incyte noted.
“More than a third of patients with MCC present with regional or distant metastases, which are associated with high rates of mortality,” principal author Shailender Bhatia, MD, of the University of Washington and Fred Hutchinson Cancer Center, both in Seattle, said in a news release. “The approval of Zynyz offers health care providers another first-line treatment option against MCC that can result in durable responses in patients with metastatic disease.”
POD1UM-201 was an open-label, single-arm, phase 2 study that evaluated the agent in 65 systemic treatment–naive adults with metastatic or recurrent locally advanced MCC.
Overall, 52% of patients had an objective response rate. A complete response was observed in 12 patients (18%), and a partial response was observed in 22 patients (34%).
Duration of response ranged from 1.1 to 24.9 months; 76% of responders experienced responses of 6 months or longer, and 62% experienced responses of 12 months or longer.
Study participants received a 500-mg dose of retifanlimab every 4 weeks for up to 24 weeks or until disease progression or unacceptable toxicity. Serious adverse events occurred in 22% of patients and most often included fatigue, arrhythmia, and pneumonitis; 11% of patients discontinued treatment because of serious adverse events.
Retifanlimab may cause a severe or life-threatening immune response during treatment or after discontinuation. Patients should be advised to immediately report any new or worsening signs or symptoms to their health care provider. Side effects can also be reported to the FDA.
A version of this article first appeared on Medscape.com.
the agency announced.
This marks the first regulatory approval for the PD-1 inhibitor. The FDA granted accelerated approval for the drug on the basis of tumor response rate and duration of response from the POD1UM-201 trial. Drugmaker Incyte said that “continued approval of Zynyz for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.”
MCC is a rare and aggressive skin cancer with a high rate of metastatic disease and an estimated 5-year overall survival of just 14% among those who present with metastatic disease. Incidence is rapidly increasing in the United States, particularly among adults older than 65 years, Incyte noted.
“More than a third of patients with MCC present with regional or distant metastases, which are associated with high rates of mortality,” principal author Shailender Bhatia, MD, of the University of Washington and Fred Hutchinson Cancer Center, both in Seattle, said in a news release. “The approval of Zynyz offers health care providers another first-line treatment option against MCC that can result in durable responses in patients with metastatic disease.”
POD1UM-201 was an open-label, single-arm, phase 2 study that evaluated the agent in 65 systemic treatment–naive adults with metastatic or recurrent locally advanced MCC.
Overall, 52% of patients had an objective response rate. A complete response was observed in 12 patients (18%), and a partial response was observed in 22 patients (34%).
Duration of response ranged from 1.1 to 24.9 months; 76% of responders experienced responses of 6 months or longer, and 62% experienced responses of 12 months or longer.
Study participants received a 500-mg dose of retifanlimab every 4 weeks for up to 24 weeks or until disease progression or unacceptable toxicity. Serious adverse events occurred in 22% of patients and most often included fatigue, arrhythmia, and pneumonitis; 11% of patients discontinued treatment because of serious adverse events.
Retifanlimab may cause a severe or life-threatening immune response during treatment or after discontinuation. Patients should be advised to immediately report any new or worsening signs or symptoms to their health care provider. Side effects can also be reported to the FDA.
A version of this article first appeared on Medscape.com.
Celebrity death finally solved – with locks of hair
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.

We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
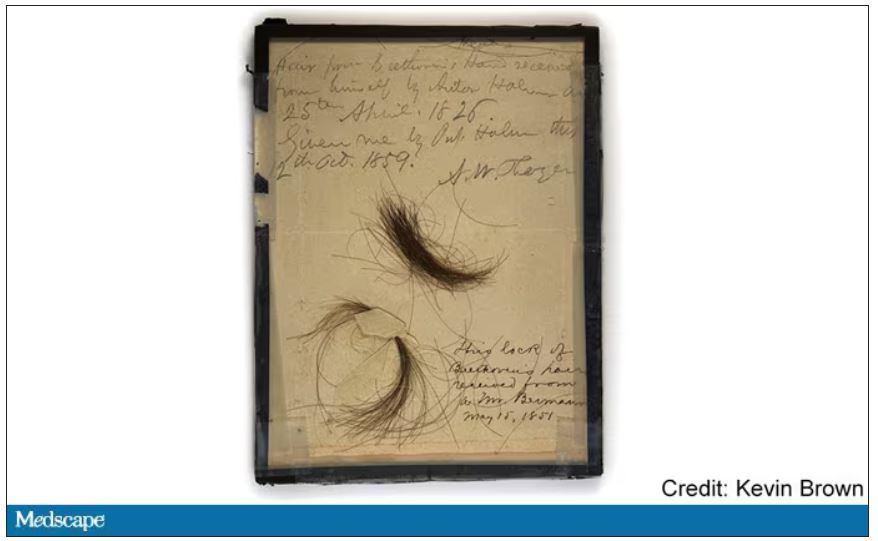
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
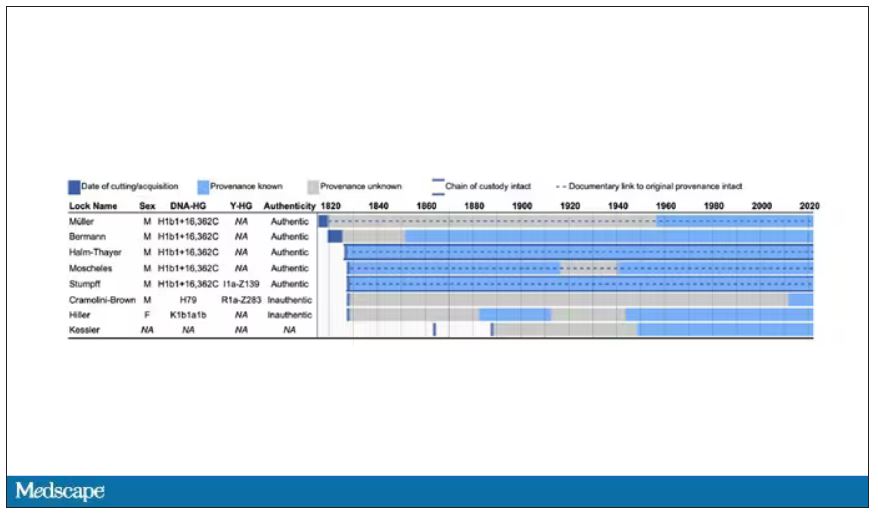
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
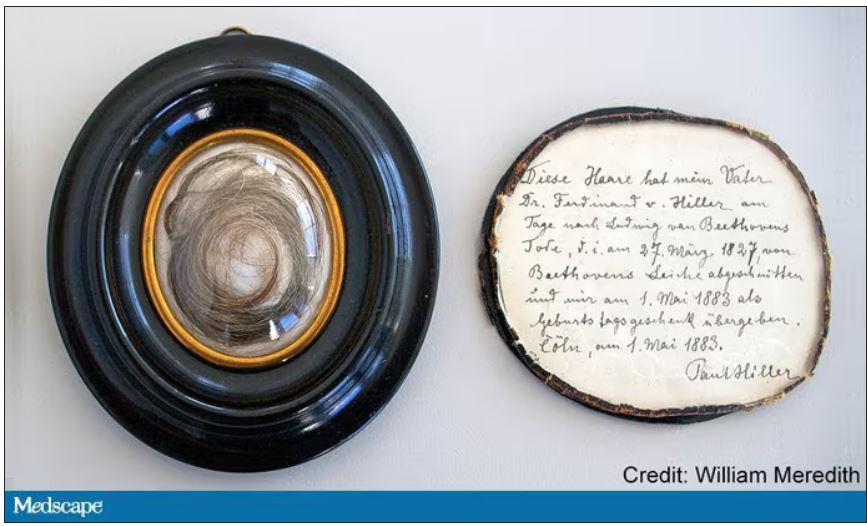
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
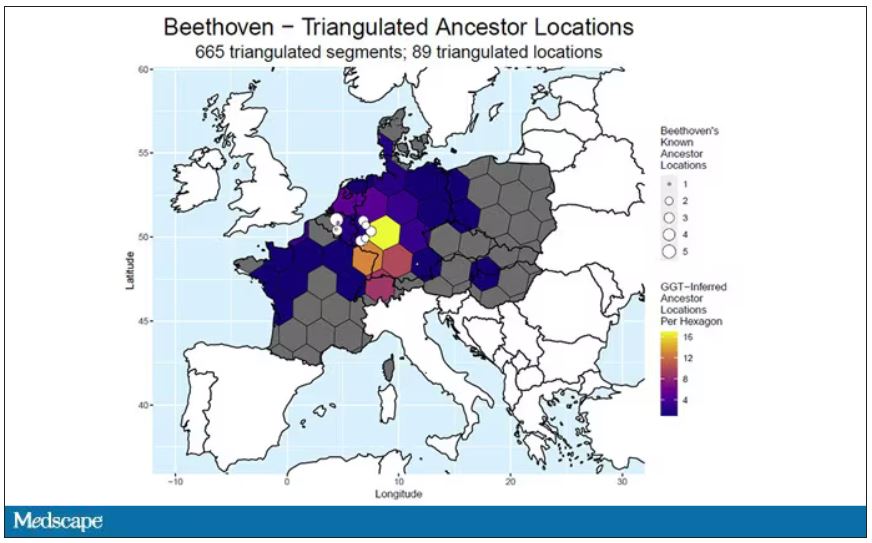
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Tyrosine kinase inhibitors – a new weapon against respiratory viruses?
Five different nonreceptor tyrosine kinase inhibitors were effective against viral replication of pandemic viruses and seasonal influenza viruses in an ex vivo lung model.
Influenza viruses remain a high cause of morbidity and mortality worldwide as viral mutations outwit vaccine efficacy, Robert Meineke, PhD, of the University of Veterinary Medicine in Hannover, Germany, and colleagues wrote.
“As with previous influenza pandemics and the current SARS-CoV-2 pandemic, effective vaccines are not readily available at early stages of a pandemic,” they noted. To help manage the limitations of timing and effectiveness of current vaccines, the researchers proposed repurposing nonreceptor tyrosine kinase inhibitors (NRTKIs) to block seasonal flu and COVID-19 viral replication.
In a study published in iScience, the researchers identified six NRTKIs currently approved by the U.S. Food and Drug Administration that showed in vitro inhibition of both pandemic viruses (H1N1) and seasonal influenza viruses (H3N2). These included defactinib, acalabrutinib, saracatinib, and bosutinib, all of which reduced hPCLS infectivity by approximately 50%. In addition, ibrutinib and bosutinib had the largest impact on viral titers. The antiviral effects of NRTKIs appeared to be independent of multiplicity of infection.
The researchers then tested the NRIKIs on an ex vivo model of human precision-cut lung slices to validate the effects of NRTKIs as antivirals against influenza A viruses (IAVs).
In this model, the highest peak titers were achieved at 48 hpi following infection with virus strains NL09 and NL11. The hPCLS models also showed consistent tolerability to 1x concentrations. “Our cytotoxicity cut-off was 20% of the positive control treatment; none of the NRTKIs surpassed this cutoff at [1x] max,” the researchers wrote.
Five of the six identified NRTKIs were validated in the ex vivo setting. All five reduced viral titers by at least 10-fold to more than 1,000-fold. Of these, ibrutinib, bosutinib, and bosutinib showed a significant effect at all concentrations, while treatments with acalabrutinib and defactinib were significant at 24 hpi and 48 hpi. The NRTKs also showed a high genetic barrier against emerging resistant virus mutations.
The study demonstrates the ability of NRTKIs to target kinases required for replication of IAV, the researchers wrote, and that NRTKIs “represent promising drugs for the development of the next generation of antivirals.”
More research is needed to determine the therapeutic window given that NRTKIs are targeting host factors versus virus-targeted antivirals, but the advantages of NRTKIs include localized delivery that can limit possible cytotoxic effects, and their safety and bioavailability are well established, they said.
The findings were limited by several factors including the use of lung tissue mainly from older donors with lung cancer, the researchers noted. However, this population could be considered at increased risk for IAVs and therefore the data are more clinically applicable.
In addition, “because many viruses utilize the same (or related) host kinases to facilitate replication and transmission, our studies have broader implications for the potential use of these SMKIs to treat infections by other viruses,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Five different nonreceptor tyrosine kinase inhibitors were effective against viral replication of pandemic viruses and seasonal influenza viruses in an ex vivo lung model.
Influenza viruses remain a high cause of morbidity and mortality worldwide as viral mutations outwit vaccine efficacy, Robert Meineke, PhD, of the University of Veterinary Medicine in Hannover, Germany, and colleagues wrote.
“As with previous influenza pandemics and the current SARS-CoV-2 pandemic, effective vaccines are not readily available at early stages of a pandemic,” they noted. To help manage the limitations of timing and effectiveness of current vaccines, the researchers proposed repurposing nonreceptor tyrosine kinase inhibitors (NRTKIs) to block seasonal flu and COVID-19 viral replication.
In a study published in iScience, the researchers identified six NRTKIs currently approved by the U.S. Food and Drug Administration that showed in vitro inhibition of both pandemic viruses (H1N1) and seasonal influenza viruses (H3N2). These included defactinib, acalabrutinib, saracatinib, and bosutinib, all of which reduced hPCLS infectivity by approximately 50%. In addition, ibrutinib and bosutinib had the largest impact on viral titers. The antiviral effects of NRTKIs appeared to be independent of multiplicity of infection.
The researchers then tested the NRIKIs on an ex vivo model of human precision-cut lung slices to validate the effects of NRTKIs as antivirals against influenza A viruses (IAVs).
In this model, the highest peak titers were achieved at 48 hpi following infection with virus strains NL09 and NL11. The hPCLS models also showed consistent tolerability to 1x concentrations. “Our cytotoxicity cut-off was 20% of the positive control treatment; none of the NRTKIs surpassed this cutoff at [1x] max,” the researchers wrote.
Five of the six identified NRTKIs were validated in the ex vivo setting. All five reduced viral titers by at least 10-fold to more than 1,000-fold. Of these, ibrutinib, bosutinib, and bosutinib showed a significant effect at all concentrations, while treatments with acalabrutinib and defactinib were significant at 24 hpi and 48 hpi. The NRTKs also showed a high genetic barrier against emerging resistant virus mutations.
The study demonstrates the ability of NRTKIs to target kinases required for replication of IAV, the researchers wrote, and that NRTKIs “represent promising drugs for the development of the next generation of antivirals.”
More research is needed to determine the therapeutic window given that NRTKIs are targeting host factors versus virus-targeted antivirals, but the advantages of NRTKIs include localized delivery that can limit possible cytotoxic effects, and their safety and bioavailability are well established, they said.
The findings were limited by several factors including the use of lung tissue mainly from older donors with lung cancer, the researchers noted. However, this population could be considered at increased risk for IAVs and therefore the data are more clinically applicable.
In addition, “because many viruses utilize the same (or related) host kinases to facilitate replication and transmission, our studies have broader implications for the potential use of these SMKIs to treat infections by other viruses,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Five different nonreceptor tyrosine kinase inhibitors were effective against viral replication of pandemic viruses and seasonal influenza viruses in an ex vivo lung model.
Influenza viruses remain a high cause of morbidity and mortality worldwide as viral mutations outwit vaccine efficacy, Robert Meineke, PhD, of the University of Veterinary Medicine in Hannover, Germany, and colleagues wrote.
“As with previous influenza pandemics and the current SARS-CoV-2 pandemic, effective vaccines are not readily available at early stages of a pandemic,” they noted. To help manage the limitations of timing and effectiveness of current vaccines, the researchers proposed repurposing nonreceptor tyrosine kinase inhibitors (NRTKIs) to block seasonal flu and COVID-19 viral replication.
In a study published in iScience, the researchers identified six NRTKIs currently approved by the U.S. Food and Drug Administration that showed in vitro inhibition of both pandemic viruses (H1N1) and seasonal influenza viruses (H3N2). These included defactinib, acalabrutinib, saracatinib, and bosutinib, all of which reduced hPCLS infectivity by approximately 50%. In addition, ibrutinib and bosutinib had the largest impact on viral titers. The antiviral effects of NRTKIs appeared to be independent of multiplicity of infection.
The researchers then tested the NRIKIs on an ex vivo model of human precision-cut lung slices to validate the effects of NRTKIs as antivirals against influenza A viruses (IAVs).
In this model, the highest peak titers were achieved at 48 hpi following infection with virus strains NL09 and NL11. The hPCLS models also showed consistent tolerability to 1x concentrations. “Our cytotoxicity cut-off was 20% of the positive control treatment; none of the NRTKIs surpassed this cutoff at [1x] max,” the researchers wrote.
Five of the six identified NRTKIs were validated in the ex vivo setting. All five reduced viral titers by at least 10-fold to more than 1,000-fold. Of these, ibrutinib, bosutinib, and bosutinib showed a significant effect at all concentrations, while treatments with acalabrutinib and defactinib were significant at 24 hpi and 48 hpi. The NRTKs also showed a high genetic barrier against emerging resistant virus mutations.
The study demonstrates the ability of NRTKIs to target kinases required for replication of IAV, the researchers wrote, and that NRTKIs “represent promising drugs for the development of the next generation of antivirals.”
More research is needed to determine the therapeutic window given that NRTKIs are targeting host factors versus virus-targeted antivirals, but the advantages of NRTKIs include localized delivery that can limit possible cytotoxic effects, and their safety and bioavailability are well established, they said.
The findings were limited by several factors including the use of lung tissue mainly from older donors with lung cancer, the researchers noted. However, this population could be considered at increased risk for IAVs and therefore the data are more clinically applicable.
In addition, “because many viruses utilize the same (or related) host kinases to facilitate replication and transmission, our studies have broader implications for the potential use of these SMKIs to treat infections by other viruses,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM ISCIENCE
Nurse makes millions selling her licensing exam study sheets
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Disease burden is higher in women vs men with psoriatic arthritis
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3
Apremilast safe and effective in biologic-naive patients with early PsA
Key clinical point: Early initiation of apremilast led to rapid and sustained improvements in psoriatic arthritis (PsA) manifestations with a consistent safety profile in a real-world cohort of biologic-naive patients who were intolerant of conventional synthetic disease-modifying antirheumatic drugs (csDMARD).
Major finding: Among patients with baseline swollen joint count (SJC) and tender joint count (TJC) of >0, significant median decreases in SJC (50% and 90%, respectively) and TJC (50% and 80%, respectively) were observed at 16 and 52 weeks (all P < .001), with 55.2% of evaluable patients achieving minimal disease activity at 52 weeks. Overall, 13.8% of patients experienced ≥1 adverse event, with all except one being non-serious.
Study details: This prospective study included 167 biologic-naive patients with early peripheral PsA and intolerance or inadequate response to csDMARD who initiated apremilast.
Disclosures: This study was funded by Genesis Pharma and Celgene. Some authors reported ties with various sources, including Genesis Pharma. A Kekki and N Antonakopoulos reported being employees of Genesis Pharma.
Source: Sfikakis PP et al. Apremilast for biologic-naïve, peripheral psoriatic arthritis, including patients with early disease: Results from the APROACH observational prospective study. Rheumatol Int. 2023 (Mar 1). Doi: 10.1007/s00296-022-05269-z
Key clinical point: Early initiation of apremilast led to rapid and sustained improvements in psoriatic arthritis (PsA) manifestations with a consistent safety profile in a real-world cohort of biologic-naive patients who were intolerant of conventional synthetic disease-modifying antirheumatic drugs (csDMARD).
Major finding: Among patients with baseline swollen joint count (SJC) and tender joint count (TJC) of >0, significant median decreases in SJC (50% and 90%, respectively) and TJC (50% and 80%, respectively) were observed at 16 and 52 weeks (all P < .001), with 55.2% of evaluable patients achieving minimal disease activity at 52 weeks. Overall, 13.8% of patients experienced ≥1 adverse event, with all except one being non-serious.
Study details: This prospective study included 167 biologic-naive patients with early peripheral PsA and intolerance or inadequate response to csDMARD who initiated apremilast.
Disclosures: This study was funded by Genesis Pharma and Celgene. Some authors reported ties with various sources, including Genesis Pharma. A Kekki and N Antonakopoulos reported being employees of Genesis Pharma.
Source: Sfikakis PP et al. Apremilast for biologic-naïve, peripheral psoriatic arthritis, including patients with early disease: Results from the APROACH observational prospective study. Rheumatol Int. 2023 (Mar 1). Doi: 10.1007/s00296-022-05269-z
Key clinical point: Early initiation of apremilast led to rapid and sustained improvements in psoriatic arthritis (PsA) manifestations with a consistent safety profile in a real-world cohort of biologic-naive patients who were intolerant of conventional synthetic disease-modifying antirheumatic drugs (csDMARD).
Major finding: Among patients with baseline swollen joint count (SJC) and tender joint count (TJC) of >0, significant median decreases in SJC (50% and 90%, respectively) and TJC (50% and 80%, respectively) were observed at 16 and 52 weeks (all P < .001), with 55.2% of evaluable patients achieving minimal disease activity at 52 weeks. Overall, 13.8% of patients experienced ≥1 adverse event, with all except one being non-serious.
Study details: This prospective study included 167 biologic-naive patients with early peripheral PsA and intolerance or inadequate response to csDMARD who initiated apremilast.
Disclosures: This study was funded by Genesis Pharma and Celgene. Some authors reported ties with various sources, including Genesis Pharma. A Kekki and N Antonakopoulos reported being employees of Genesis Pharma.
Source: Sfikakis PP et al. Apremilast for biologic-naïve, peripheral psoriatic arthritis, including patients with early disease: Results from the APROACH observational prospective study. Rheumatol Int. 2023 (Mar 1). Doi: 10.1007/s00296-022-05269-z
Concurrent onset of skin and joint symptoms tied to high disease activity in PsA
Key clinical point: Concurrent onset of skin lesions and joint symptoms increased the likelihood of moderate or high disease activity in patients with psoriatic arthritis (PsA), highlighting the importance of sequence in which skin and joint symptoms appear in disease management.
Major finding: Patients with concurrent onset of skin and joint symptoms (adjusted odds ratio 4.65; P = .007) were more likely to have a moderate or high disease activity (Psoriatic Arthritis Disease Activity Score >3.2).
Study details: Findings are from a retrospective cross-sectional study including 286 patients with PsA.
Disclosures: This study was funded by the National Natural Science Foundation of China. No conflicts of interest were declared.
Source: Tan M et al. Concurrent onset of skin and joint symptoms correlates with higher psoriatic arthritis disease activity: A single-center retrospective study. J Am Acad Dermatol. 2023 (Mar 6). Doi: 10.1016/j.jaad.2023.02.045
Key clinical point: Concurrent onset of skin lesions and joint symptoms increased the likelihood of moderate or high disease activity in patients with psoriatic arthritis (PsA), highlighting the importance of sequence in which skin and joint symptoms appear in disease management.
Major finding: Patients with concurrent onset of skin and joint symptoms (adjusted odds ratio 4.65; P = .007) were more likely to have a moderate or high disease activity (Psoriatic Arthritis Disease Activity Score >3.2).
Study details: Findings are from a retrospective cross-sectional study including 286 patients with PsA.
Disclosures: This study was funded by the National Natural Science Foundation of China. No conflicts of interest were declared.
Source: Tan M et al. Concurrent onset of skin and joint symptoms correlates with higher psoriatic arthritis disease activity: A single-center retrospective study. J Am Acad Dermatol. 2023 (Mar 6). Doi: 10.1016/j.jaad.2023.02.045
Key clinical point: Concurrent onset of skin lesions and joint symptoms increased the likelihood of moderate or high disease activity in patients with psoriatic arthritis (PsA), highlighting the importance of sequence in which skin and joint symptoms appear in disease management.
Major finding: Patients with concurrent onset of skin and joint symptoms (adjusted odds ratio 4.65; P = .007) were more likely to have a moderate or high disease activity (Psoriatic Arthritis Disease Activity Score >3.2).
Study details: Findings are from a retrospective cross-sectional study including 286 patients with PsA.
Disclosures: This study was funded by the National Natural Science Foundation of China. No conflicts of interest were declared.
Source: Tan M et al. Concurrent onset of skin and joint symptoms correlates with higher psoriatic arthritis disease activity: A single-center retrospective study. J Am Acad Dermatol. 2023 (Mar 6). Doi: 10.1016/j.jaad.2023.02.045
Ultrasound helps screen patients with moderate-to-severe psoriasis progressing to subclinical PsA
Key clinical point: In patients with moderate-to-severe psoriasis, the presence of synovio-enthesitis on ultrasound, particularly in lower limbs, indicated progression to subclinical psoriatic arthritis (PsA). Therefore, routine ultrasound screening should be performed irrespective of arthritis symptoms.
Major finding: Only synovio-enthesitis diagnosis differed significantly among patients with silent psoriasis vs control individuals (16.1% vs 1.3%; P < .001), with 12.7% of patients diagnosed with synovio-enthesitis progressing to subclinical PsA and the top four sites with synovio-enthesitis involvement being in lower limbs. Body surface area and Psoriasis Area and Severity Index scores were not different in psoriasis, subclinical PsA, and prodromal/active PsA phases.
Study details: This cross-sectional study included 490 patients with moderate-to-severe psoriasis, of which 384 and 106 patients without and with arthritis symptoms formed the silent psoriasis and clinical PsA groups, respectively, and 80 age- and sex-matched control individuals without psoriasis.
Disclosures: This study was supported by the National Natural Science Foundation of China and other sources. The authors declared no conflicts of interest.
Source: Chen ZT et al. The role of ultrasound in screening subclinical psoriatic arthritis in patients with moderate to severe psoriasis. Eur Radiol. 2023 (Feb 28). Doi: 10.1007/s00330-023-09493-4
Key clinical point: In patients with moderate-to-severe psoriasis, the presence of synovio-enthesitis on ultrasound, particularly in lower limbs, indicated progression to subclinical psoriatic arthritis (PsA). Therefore, routine ultrasound screening should be performed irrespective of arthritis symptoms.
Major finding: Only synovio-enthesitis diagnosis differed significantly among patients with silent psoriasis vs control individuals (16.1% vs 1.3%; P < .001), with 12.7% of patients diagnosed with synovio-enthesitis progressing to subclinical PsA and the top four sites with synovio-enthesitis involvement being in lower limbs. Body surface area and Psoriasis Area and Severity Index scores were not different in psoriasis, subclinical PsA, and prodromal/active PsA phases.
Study details: This cross-sectional study included 490 patients with moderate-to-severe psoriasis, of which 384 and 106 patients without and with arthritis symptoms formed the silent psoriasis and clinical PsA groups, respectively, and 80 age- and sex-matched control individuals without psoriasis.
Disclosures: This study was supported by the National Natural Science Foundation of China and other sources. The authors declared no conflicts of interest.
Source: Chen ZT et al. The role of ultrasound in screening subclinical psoriatic arthritis in patients with moderate to severe psoriasis. Eur Radiol. 2023 (Feb 28). Doi: 10.1007/s00330-023-09493-4
Key clinical point: In patients with moderate-to-severe psoriasis, the presence of synovio-enthesitis on ultrasound, particularly in lower limbs, indicated progression to subclinical psoriatic arthritis (PsA). Therefore, routine ultrasound screening should be performed irrespective of arthritis symptoms.
Major finding: Only synovio-enthesitis diagnosis differed significantly among patients with silent psoriasis vs control individuals (16.1% vs 1.3%; P < .001), with 12.7% of patients diagnosed with synovio-enthesitis progressing to subclinical PsA and the top four sites with synovio-enthesitis involvement being in lower limbs. Body surface area and Psoriasis Area and Severity Index scores were not different in psoriasis, subclinical PsA, and prodromal/active PsA phases.
Study details: This cross-sectional study included 490 patients with moderate-to-severe psoriasis, of which 384 and 106 patients without and with arthritis symptoms formed the silent psoriasis and clinical PsA groups, respectively, and 80 age- and sex-matched control individuals without psoriasis.
Disclosures: This study was supported by the National Natural Science Foundation of China and other sources. The authors declared no conflicts of interest.
Source: Chen ZT et al. The role of ultrasound in screening subclinical psoriatic arthritis in patients with moderate to severe psoriasis. Eur Radiol. 2023 (Feb 28). Doi: 10.1007/s00330-023-09493-4
Real world study finds no evidence of increased cancer risk with JAKi vs TNFi in PsA
Key clinical point: The short-term risk for cancer other than non-melanoma skin cancer (NMSC) or NMSC was not significantly higher among patients with psoriatic arthritis (PsA) who initiated Janus kinase inhibitors (JAKi) than those who initiated tumor necrosis factor inhibitors (TNFi).
Major finding: JAKi vs TNFi was not significantly associated with a higher risk for cancer other than NMSC (adjusted hazard ratio [aHR] 1.88; 95% CI 0.68-5.16) or NMSC (aHR 2.05; 95% CI 0.79-5.31) in patients with PsA.
Study details: The data come from an observational cohort study that evaluated prospectively collected data of 4443 patients with PsA and 10,447 patients with RA, all without previous cancer, who received JAKi, TNFi, or other non-TNFi biologic disease-modifying antirheumatic drugs.
Disclosures: This study was funded by the Karolinska Institute Region Stockholm funds (ALF), Swedish Research Council, and others. T Frisell and H Bower declared being partly employed by the ARTIS project. J Askling reported research agreements with various sources.
Source: Huss V et al on behalf of the ARTIS group. Cancer risks with JAKi and biological disease-modifying antirheumatic drugs in patients with rheumatoid arthritis or psoriatic arthritis: A national real-world cohort study. Ann Rheum Dis. 2023 (Mar 3). Doi: 10.1136/ard-2022-223636
Key clinical point: The short-term risk for cancer other than non-melanoma skin cancer (NMSC) or NMSC was not significantly higher among patients with psoriatic arthritis (PsA) who initiated Janus kinase inhibitors (JAKi) than those who initiated tumor necrosis factor inhibitors (TNFi).
Major finding: JAKi vs TNFi was not significantly associated with a higher risk for cancer other than NMSC (adjusted hazard ratio [aHR] 1.88; 95% CI 0.68-5.16) or NMSC (aHR 2.05; 95% CI 0.79-5.31) in patients with PsA.
Study details: The data come from an observational cohort study that evaluated prospectively collected data of 4443 patients with PsA and 10,447 patients with RA, all without previous cancer, who received JAKi, TNFi, or other non-TNFi biologic disease-modifying antirheumatic drugs.
Disclosures: This study was funded by the Karolinska Institute Region Stockholm funds (ALF), Swedish Research Council, and others. T Frisell and H Bower declared being partly employed by the ARTIS project. J Askling reported research agreements with various sources.
Source: Huss V et al on behalf of the ARTIS group. Cancer risks with JAKi and biological disease-modifying antirheumatic drugs in patients with rheumatoid arthritis or psoriatic arthritis: A national real-world cohort study. Ann Rheum Dis. 2023 (Mar 3). Doi: 10.1136/ard-2022-223636
Key clinical point: The short-term risk for cancer other than non-melanoma skin cancer (NMSC) or NMSC was not significantly higher among patients with psoriatic arthritis (PsA) who initiated Janus kinase inhibitors (JAKi) than those who initiated tumor necrosis factor inhibitors (TNFi).
Major finding: JAKi vs TNFi was not significantly associated with a higher risk for cancer other than NMSC (adjusted hazard ratio [aHR] 1.88; 95% CI 0.68-5.16) or NMSC (aHR 2.05; 95% CI 0.79-5.31) in patients with PsA.
Study details: The data come from an observational cohort study that evaluated prospectively collected data of 4443 patients with PsA and 10,447 patients with RA, all without previous cancer, who received JAKi, TNFi, or other non-TNFi biologic disease-modifying antirheumatic drugs.
Disclosures: This study was funded by the Karolinska Institute Region Stockholm funds (ALF), Swedish Research Council, and others. T Frisell and H Bower declared being partly employed by the ARTIS project. J Askling reported research agreements with various sources.
Source: Huss V et al on behalf of the ARTIS group. Cancer risks with JAKi and biological disease-modifying antirheumatic drugs in patients with rheumatoid arthritis or psoriatic arthritis: A national real-world cohort study. Ann Rheum Dis. 2023 (Mar 3). Doi: 10.1136/ard-2022-223636
JAKi effective for PsA but higher doses may have increased toxicity
Key clinical point: All Janus kinase inhibitors (JAKi) were more effective than placebo in patients with psoriatic arthritis (PsA), but led to a higher overall incidence of adverse events, particularly at higher doses.
Major finding: JAKi vs placebo were associated with a significantly higher American College of Rheumatology 20 response rate (relative risk [RR] 2.09; P < .00001), with the response being the highest for filgotinib (RR 2.40; P < .00001), followed by upadacitinib, tofacitinib, and deucravacitinib. However, the overall incidence of adverse events was higher with JAKi vs placebo (RR 1.17; P < .00001) and significantly higher with 10 mg vs 5 mg tofacitinib (P = .03).
Study details: The data come from a systematic review and meta-analysis of 17 phase 2/3 randomized controlled trials including 6802 patients with PsA or moderate-to-severe plaque psoriasis who received ≥1 JAKi.
Disclosures: This study was supported by the National Basic Research Program of China. The authors declared no conflicts of interest.
Source: Yang F et al. Efficacy and safety of Janus kinase inhibitors in patients with psoriasis and psoriatic arthritis: A systematic review and meta‑analysis. Clin Rheumatol. 2023 (Feb 10). Doi: 10.1007/s10067-023-06529-4
Key clinical point: All Janus kinase inhibitors (JAKi) were more effective than placebo in patients with psoriatic arthritis (PsA), but led to a higher overall incidence of adverse events, particularly at higher doses.
Major finding: JAKi vs placebo were associated with a significantly higher American College of Rheumatology 20 response rate (relative risk [RR] 2.09; P < .00001), with the response being the highest for filgotinib (RR 2.40; P < .00001), followed by upadacitinib, tofacitinib, and deucravacitinib. However, the overall incidence of adverse events was higher with JAKi vs placebo (RR 1.17; P < .00001) and significantly higher with 10 mg vs 5 mg tofacitinib (P = .03).
Study details: The data come from a systematic review and meta-analysis of 17 phase 2/3 randomized controlled trials including 6802 patients with PsA or moderate-to-severe plaque psoriasis who received ≥1 JAKi.
Disclosures: This study was supported by the National Basic Research Program of China. The authors declared no conflicts of interest.
Source: Yang F et al. Efficacy and safety of Janus kinase inhibitors in patients with psoriasis and psoriatic arthritis: A systematic review and meta‑analysis. Clin Rheumatol. 2023 (Feb 10). Doi: 10.1007/s10067-023-06529-4
Key clinical point: All Janus kinase inhibitors (JAKi) were more effective than placebo in patients with psoriatic arthritis (PsA), but led to a higher overall incidence of adverse events, particularly at higher doses.
Major finding: JAKi vs placebo were associated with a significantly higher American College of Rheumatology 20 response rate (relative risk [RR] 2.09; P < .00001), with the response being the highest for filgotinib (RR 2.40; P < .00001), followed by upadacitinib, tofacitinib, and deucravacitinib. However, the overall incidence of adverse events was higher with JAKi vs placebo (RR 1.17; P < .00001) and significantly higher with 10 mg vs 5 mg tofacitinib (P = .03).
Study details: The data come from a systematic review and meta-analysis of 17 phase 2/3 randomized controlled trials including 6802 patients with PsA or moderate-to-severe plaque psoriasis who received ≥1 JAKi.
Disclosures: This study was supported by the National Basic Research Program of China. The authors declared no conflicts of interest.
Source: Yang F et al. Efficacy and safety of Janus kinase inhibitors in patients with psoriasis and psoriatic arthritis: A systematic review and meta‑analysis. Clin Rheumatol. 2023 (Feb 10). Doi: 10.1007/s10067-023-06529-4