User login
For preterm birth, we must avoid being too quick to prescribe therapeutic measures
As ob.gyns., our decisions not only deeply affect the health and well-being of our patients, but can also dramatically impact their children and families. Perhaps nowhere else is the gravity of our medical choices more felt than in the management of premature labor. Premature birth is one of the major drivers of infant mortality, which remains a significant public health problem in the United States where the rate of infant mortality is nearly 6 of every 1,000 live births.

Therefore, when the two seminal studies were published that showed using injectable or vaginal progesterone successfully delayed labor with fewer neonatal complications, the findings were quickly embraced and applied clinically. However, subsequent studies indicated that progesterone is only beneficial to a certain subset of patients – those with singleton pregnancies and a short cervix. The variance in the results of this research highlights an important point: We must treat each patient as an individual, based on her unique medical history, circumstances, and, yes, symptoms. One size does not fit all.
Equally important is a greater need across our practice to avoid being too quick to prescribe therapeutic measures that do not treat the root of the problem. We must instead provide guidance based on rigorously conducted research and analysis. However, even very promising results should not necessarily be used to guide all of clinical practice, and certainly not without scrutiny and considerable analysis.
To dissect the available data and present the most current findings regarding progesterone use to prevent preterm labor, we have invited Steve Caritis, MD, professor of obstetrics, gynecology, and reproductive sciences at Magee-Womens Hospital, University of Pittsburgh, to be the guest author for this month’s Master Class.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
As ob.gyns., our decisions not only deeply affect the health and well-being of our patients, but can also dramatically impact their children and families. Perhaps nowhere else is the gravity of our medical choices more felt than in the management of premature labor. Premature birth is one of the major drivers of infant mortality, which remains a significant public health problem in the United States where the rate of infant mortality is nearly 6 of every 1,000 live births.
Therefore, when the two seminal studies were published that showed using injectable or vaginal progesterone successfully delayed labor with fewer neonatal complications, the findings were quickly embraced and applied clinically. However, subsequent studies indicated that progesterone is only beneficial to a certain subset of patients – those with singleton pregnancies and a short cervix. The variance in the results of this research highlights an important point: We must treat each patient as an individual, based on her unique medical history, circumstances, and, yes, symptoms. One size does not fit all.
Equally important is a greater need across our practice to avoid being too quick to prescribe therapeutic measures that do not treat the root of the problem. We must instead provide guidance based on rigorously conducted research and analysis. However, even very promising results should not necessarily be used to guide all of clinical practice, and certainly not without scrutiny and considerable analysis.
To dissect the available data and present the most current findings regarding progesterone use to prevent preterm labor, we have invited Steve Caritis, MD, professor of obstetrics, gynecology, and reproductive sciences at Magee-Womens Hospital, University of Pittsburgh, to be the guest author for this month’s Master Class.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
As ob.gyns., our decisions not only deeply affect the health and well-being of our patients, but can also dramatically impact their children and families. Perhaps nowhere else is the gravity of our medical choices more felt than in the management of premature labor. Premature birth is one of the major drivers of infant mortality, which remains a significant public health problem in the United States where the rate of infant mortality is nearly 6 of every 1,000 live births.
Therefore, when the two seminal studies were published that showed using injectable or vaginal progesterone successfully delayed labor with fewer neonatal complications, the findings were quickly embraced and applied clinically. However, subsequent studies indicated that progesterone is only beneficial to a certain subset of patients – those with singleton pregnancies and a short cervix. The variance in the results of this research highlights an important point: We must treat each patient as an individual, based on her unique medical history, circumstances, and, yes, symptoms. One size does not fit all.
Equally important is a greater need across our practice to avoid being too quick to prescribe therapeutic measures that do not treat the root of the problem. We must instead provide guidance based on rigorously conducted research and analysis. However, even very promising results should not necessarily be used to guide all of clinical practice, and certainly not without scrutiny and considerable analysis.
To dissect the available data and present the most current findings regarding progesterone use to prevent preterm labor, we have invited Steve Caritis, MD, professor of obstetrics, gynecology, and reproductive sciences at Magee-Womens Hospital, University of Pittsburgh, to be the guest author for this month’s Master Class.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Objective response rate correlates poorly with overall survival in checkpoint-inhibitor trials
Objective response rate (ORR) correlated poorly with overall survival (OS), but 6-month progression-free survival was a better predictor of 12-month OS, according to a systematic review and meta-analysis of phase 2 and phase 3 trials of checkpoint inhibitors in advanced solid cancers.
Six-month progression-free survival is recommended in place of objective response rate as an endpoint in future phase 2 checkpoint-inhibitor trials, investigators wrote. The report was published in JAMA Oncology.
Appropriate selection of a primary endpoint in phase 2 checkpoint-inhibitor trials is critical to proceed to phase 3 testing. In checkpoint inhibitor trials, the validity of ORR, as determined by RECIST, and PFS as surrogates for OS remains unclear.
The investigators conducted a systematic search of electronic databases for trial results from January 2000 to January 2017, identified through PREMEDLINE, MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials. In addition, abstracts and conference presentations on the European Society for Medical Oncology and American Society of Clinical Oncology websites were hand-searched, wrote Georgia Ritchie, MBBS, of the Cancer Care Centre, St. George Hospital, Sydney, and associates.
Inclusion criteria comprised trials that used checkpoint inhibitors in advanced solid cancers in single-arm or randomized controlled trials of phase 2 and phase 3 designs.
Within the checkpoint inhibitor arms of the trials, r correlation coefficients between ORR with 6-month PFS, ORR with 12-month OS, and 6-month PFS with 12-month OS were 0.37 (95% confidence interval, −0.06 to 0.95), 0.08 (95% confidence interval, −0.17 to 0.70), and 0.74 (95% confidence interval, 0.57-0.92), respectively, Dr. Ritchie and associates reported. To validate an OS prediction model, the investigators found a good calibration between 6-month PFS and actual and predicted 12-month OS. However, when ORR was used to predict 6-month PFS and 12-month OS rates, the actual vs. predicted rates calibrated poorly, they said.
A strength of the study is its generalizability, because of a heterogeneous population of patients with advanced cancer. “Future phase 2 trials might require a larger sample size, and more resources to report on this result than RECIST ORR,” reported the authors. Further research is required to assess the validity of milestone analysis with 6-month PFS as a potential surrogate for OS in treatment comparisons between checkpoint inhibitors and standard of care therapy, they added.
The authors reported no conflicts of interest.
SOURCE: Ritchie G et al., JAMA Oncol. 2018 Feb 22 doi: 10.1001/jamaoncol.2017.5236.
Objective response rate (ORR) correlated poorly with overall survival (OS), but 6-month progression-free survival was a better predictor of 12-month OS, according to a systematic review and meta-analysis of phase 2 and phase 3 trials of checkpoint inhibitors in advanced solid cancers.
Six-month progression-free survival is recommended in place of objective response rate as an endpoint in future phase 2 checkpoint-inhibitor trials, investigators wrote. The report was published in JAMA Oncology.
Appropriate selection of a primary endpoint in phase 2 checkpoint-inhibitor trials is critical to proceed to phase 3 testing. In checkpoint inhibitor trials, the validity of ORR, as determined by RECIST, and PFS as surrogates for OS remains unclear.
The investigators conducted a systematic search of electronic databases for trial results from January 2000 to January 2017, identified through PREMEDLINE, MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials. In addition, abstracts and conference presentations on the European Society for Medical Oncology and American Society of Clinical Oncology websites were hand-searched, wrote Georgia Ritchie, MBBS, of the Cancer Care Centre, St. George Hospital, Sydney, and associates.
Inclusion criteria comprised trials that used checkpoint inhibitors in advanced solid cancers in single-arm or randomized controlled trials of phase 2 and phase 3 designs.
Within the checkpoint inhibitor arms of the trials, r correlation coefficients between ORR with 6-month PFS, ORR with 12-month OS, and 6-month PFS with 12-month OS were 0.37 (95% confidence interval, −0.06 to 0.95), 0.08 (95% confidence interval, −0.17 to 0.70), and 0.74 (95% confidence interval, 0.57-0.92), respectively, Dr. Ritchie and associates reported. To validate an OS prediction model, the investigators found a good calibration between 6-month PFS and actual and predicted 12-month OS. However, when ORR was used to predict 6-month PFS and 12-month OS rates, the actual vs. predicted rates calibrated poorly, they said.
A strength of the study is its generalizability, because of a heterogeneous population of patients with advanced cancer. “Future phase 2 trials might require a larger sample size, and more resources to report on this result than RECIST ORR,” reported the authors. Further research is required to assess the validity of milestone analysis with 6-month PFS as a potential surrogate for OS in treatment comparisons between checkpoint inhibitors and standard of care therapy, they added.
The authors reported no conflicts of interest.
SOURCE: Ritchie G et al., JAMA Oncol. 2018 Feb 22 doi: 10.1001/jamaoncol.2017.5236.
Objective response rate (ORR) correlated poorly with overall survival (OS), but 6-month progression-free survival was a better predictor of 12-month OS, according to a systematic review and meta-analysis of phase 2 and phase 3 trials of checkpoint inhibitors in advanced solid cancers.
Six-month progression-free survival is recommended in place of objective response rate as an endpoint in future phase 2 checkpoint-inhibitor trials, investigators wrote. The report was published in JAMA Oncology.
Appropriate selection of a primary endpoint in phase 2 checkpoint-inhibitor trials is critical to proceed to phase 3 testing. In checkpoint inhibitor trials, the validity of ORR, as determined by RECIST, and PFS as surrogates for OS remains unclear.
The investigators conducted a systematic search of electronic databases for trial results from January 2000 to January 2017, identified through PREMEDLINE, MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials. In addition, abstracts and conference presentations on the European Society for Medical Oncology and American Society of Clinical Oncology websites were hand-searched, wrote Georgia Ritchie, MBBS, of the Cancer Care Centre, St. George Hospital, Sydney, and associates.
Inclusion criteria comprised trials that used checkpoint inhibitors in advanced solid cancers in single-arm or randomized controlled trials of phase 2 and phase 3 designs.
Within the checkpoint inhibitor arms of the trials, r correlation coefficients between ORR with 6-month PFS, ORR with 12-month OS, and 6-month PFS with 12-month OS were 0.37 (95% confidence interval, −0.06 to 0.95), 0.08 (95% confidence interval, −0.17 to 0.70), and 0.74 (95% confidence interval, 0.57-0.92), respectively, Dr. Ritchie and associates reported. To validate an OS prediction model, the investigators found a good calibration between 6-month PFS and actual and predicted 12-month OS. However, when ORR was used to predict 6-month PFS and 12-month OS rates, the actual vs. predicted rates calibrated poorly, they said.
A strength of the study is its generalizability, because of a heterogeneous population of patients with advanced cancer. “Future phase 2 trials might require a larger sample size, and more resources to report on this result than RECIST ORR,” reported the authors. Further research is required to assess the validity of milestone analysis with 6-month PFS as a potential surrogate for OS in treatment comparisons between checkpoint inhibitors and standard of care therapy, they added.
The authors reported no conflicts of interest.
SOURCE: Ritchie G et al., JAMA Oncol. 2018 Feb 22 doi: 10.1001/jamaoncol.2017.5236.
FROM JAMA ONCOLOGY
Key clinical point: Immune checkpoint inhibitors activate anti-tumor T-cells to detect and destroy tumor cells and have become the standard of care for many patients with advanced solid cancers. The most appropriate primary endpoint in phase 2 trials of checkpoint inhibitors remains uncertain.
Major finding: In this systematic review and meta-analysis of phase 2 and phase 3 trials of checkpoint inhibitors in advanced solid cancers, objective response rate correlated poorly with overall survival, but 6-month progression-free survival was a better predictor of 12-month overall survival.
Study details: Trials listed in electronic databases from 2000 to 2017 (PREMEDLINE, MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials).
Disclosures: None reported.
Source: Ritchie G et al. JAMA Oncol. 2018 Feb 22. doi: 10.1001/jamaoncol.2017.5236.
Hospital chemo carries higher price tag than the office
Commercial insurers are spending nearly twice as much on chemotherapy administered in hospital outpatient departments as they are for therapy administered in a physician’s office, according to an analysis of a decade of claims data.
Commercial insurance data from 283,502 patients who initiated treatment with infused chemotherapy and remained enrolled continuously for 6 months, without receiving infused chemotherapy in the preceding 6 months, revealed that spending at the drug level was “significantly lower in offices vs. in HOPDs [hospital outpatient departments],” Aaron Winn, PhD, of the Medical College of Wisconsin, Milwaukee, and his colleagues wrote in a research letter published Feb. 22 in JAMA Oncology.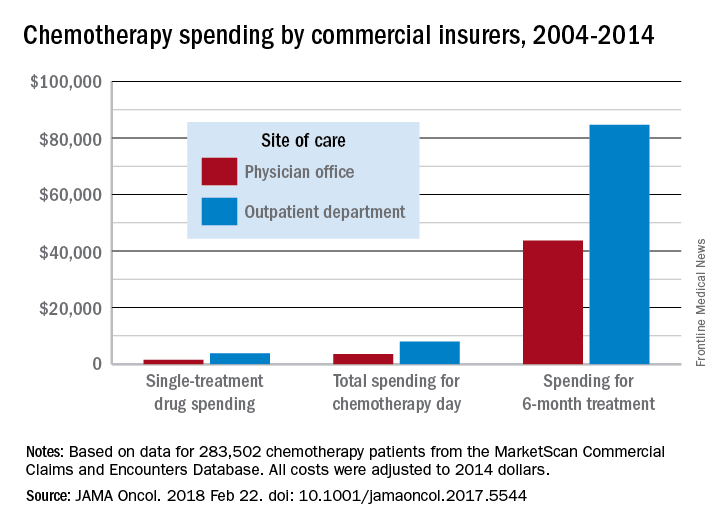
During the review period from Jan. 1, 2004 through Dec. 31, 2014, the rate of commercially-insured patients receiving chemotherapy in HOPDs grew from 6% in 2004 to 43% in 2014. The spending data was adjusted for various factors, including, sex, comorbidity, year of diagnosis, drug administered, and location.
“Shifting the provision of infused chemotherapy from physician offices to HOPDs is increasing and is associated with increased spending for chemotherapy services,” the researchers wrote. “Potential targets for reduction of excess spending can come from private insurers following Medicaid’s lead, which has started to equalize payments across sites of care.”
“I was a little surprised that the site location was converging on 50-50 across the country,” Dr. Carole Miller, director of the Cancer Institute at St. Agnes Hospital, Baltimore, said in an interview, adding that the spending figures were not a surprise.
Dr. Miller noted that another thing the claims data does not capture are the kinds of additional services that patients are receiving in their respective sites of care, which could also account for the difference in total reimbursement. For example, hospital-based cancer centers may offer more social support service given that the patients tend to be older and may have more social service needs as well as more uncompensated care.
David Henry, MD, an oncologist who practices in a community setting that is part of the University of Pennsylvania hospital system, said the data fits with his experience. “Is the care better? I don’t think so. Is the overhead bigger? Sure.”
Part of what makes the care better in the community setting is the patient experience, said Dr. Henry, who serves as editor-in-chief of the Journal of Community and Supportive Oncology, which is published by this news organization.
The office setting can often boast a streamlined experience, he added. In the hospital, the administrative elements and travel across the hospital campus can make an infusion a day-long task, versus going to a community office setting where the total infusion process, including the administrative aspects, can be handled in a few hours.
Dr. Henry acknowledged that the hospital setting does have an advantage in terms of depth of services, including specialists to deal with a variety of tumors.
Dr. Henry noted that the current analysis does not address the shift to paying for value and the move away from fee-for-service payment. Speaking about whether Medicare’s Quality Payment Program can level the playing field in some ways between the two settings of care, he said “the idea has potential” but the success will be determined by how it is implemented.
This article was updated on 2/22/18.
gtwachtman@frontlinemedcom.com
SOURCE: Winn A et al., JAMA Oncol. 2018 Feb 22. doi: 10.1001/jamaoncol.2017.5544.
Commercial insurers are spending nearly twice as much on chemotherapy administered in hospital outpatient departments as they are for therapy administered in a physician’s office, according to an analysis of a decade of claims data.
Commercial insurance data from 283,502 patients who initiated treatment with infused chemotherapy and remained enrolled continuously for 6 months, without receiving infused chemotherapy in the preceding 6 months, revealed that spending at the drug level was “significantly lower in offices vs. in HOPDs [hospital outpatient departments],” Aaron Winn, PhD, of the Medical College of Wisconsin, Milwaukee, and his colleagues wrote in a research letter published Feb. 22 in JAMA Oncology.
During the review period from Jan. 1, 2004 through Dec. 31, 2014, the rate of commercially-insured patients receiving chemotherapy in HOPDs grew from 6% in 2004 to 43% in 2014. The spending data was adjusted for various factors, including, sex, comorbidity, year of diagnosis, drug administered, and location.
“Shifting the provision of infused chemotherapy from physician offices to HOPDs is increasing and is associated with increased spending for chemotherapy services,” the researchers wrote. “Potential targets for reduction of excess spending can come from private insurers following Medicaid’s lead, which has started to equalize payments across sites of care.”
“I was a little surprised that the site location was converging on 50-50 across the country,” Dr. Carole Miller, director of the Cancer Institute at St. Agnes Hospital, Baltimore, said in an interview, adding that the spending figures were not a surprise.
Dr. Miller noted that another thing the claims data does not capture are the kinds of additional services that patients are receiving in their respective sites of care, which could also account for the difference in total reimbursement. For example, hospital-based cancer centers may offer more social support service given that the patients tend to be older and may have more social service needs as well as more uncompensated care.
David Henry, MD, an oncologist who practices in a community setting that is part of the University of Pennsylvania hospital system, said the data fits with his experience. “Is the care better? I don’t think so. Is the overhead bigger? Sure.”
Part of what makes the care better in the community setting is the patient experience, said Dr. Henry, who serves as editor-in-chief of the Journal of Community and Supportive Oncology, which is published by this news organization.
The office setting can often boast a streamlined experience, he added. In the hospital, the administrative elements and travel across the hospital campus can make an infusion a day-long task, versus going to a community office setting where the total infusion process, including the administrative aspects, can be handled in a few hours.
Dr. Henry acknowledged that the hospital setting does have an advantage in terms of depth of services, including specialists to deal with a variety of tumors.
Dr. Henry noted that the current analysis does not address the shift to paying for value and the move away from fee-for-service payment. Speaking about whether Medicare’s Quality Payment Program can level the playing field in some ways between the two settings of care, he said “the idea has potential” but the success will be determined by how it is implemented.
This article was updated on 2/22/18.
gtwachtman@frontlinemedcom.com
SOURCE: Winn A et al., JAMA Oncol. 2018 Feb 22. doi: 10.1001/jamaoncol.2017.5544.
Commercial insurers are spending nearly twice as much on chemotherapy administered in hospital outpatient departments as they are for therapy administered in a physician’s office, according to an analysis of a decade of claims data.
Commercial insurance data from 283,502 patients who initiated treatment with infused chemotherapy and remained enrolled continuously for 6 months, without receiving infused chemotherapy in the preceding 6 months, revealed that spending at the drug level was “significantly lower in offices vs. in HOPDs [hospital outpatient departments],” Aaron Winn, PhD, of the Medical College of Wisconsin, Milwaukee, and his colleagues wrote in a research letter published Feb. 22 in JAMA Oncology.
During the review period from Jan. 1, 2004 through Dec. 31, 2014, the rate of commercially-insured patients receiving chemotherapy in HOPDs grew from 6% in 2004 to 43% in 2014. The spending data was adjusted for various factors, including, sex, comorbidity, year of diagnosis, drug administered, and location.
“Shifting the provision of infused chemotherapy from physician offices to HOPDs is increasing and is associated with increased spending for chemotherapy services,” the researchers wrote. “Potential targets for reduction of excess spending can come from private insurers following Medicaid’s lead, which has started to equalize payments across sites of care.”
“I was a little surprised that the site location was converging on 50-50 across the country,” Dr. Carole Miller, director of the Cancer Institute at St. Agnes Hospital, Baltimore, said in an interview, adding that the spending figures were not a surprise.
Dr. Miller noted that another thing the claims data does not capture are the kinds of additional services that patients are receiving in their respective sites of care, which could also account for the difference in total reimbursement. For example, hospital-based cancer centers may offer more social support service given that the patients tend to be older and may have more social service needs as well as more uncompensated care.
David Henry, MD, an oncologist who practices in a community setting that is part of the University of Pennsylvania hospital system, said the data fits with his experience. “Is the care better? I don’t think so. Is the overhead bigger? Sure.”
Part of what makes the care better in the community setting is the patient experience, said Dr. Henry, who serves as editor-in-chief of the Journal of Community and Supportive Oncology, which is published by this news organization.
The office setting can often boast a streamlined experience, he added. In the hospital, the administrative elements and travel across the hospital campus can make an infusion a day-long task, versus going to a community office setting where the total infusion process, including the administrative aspects, can be handled in a few hours.
Dr. Henry acknowledged that the hospital setting does have an advantage in terms of depth of services, including specialists to deal with a variety of tumors.
Dr. Henry noted that the current analysis does not address the shift to paying for value and the move away from fee-for-service payment. Speaking about whether Medicare’s Quality Payment Program can level the playing field in some ways between the two settings of care, he said “the idea has potential” but the success will be determined by how it is implemented.
This article was updated on 2/22/18.
gtwachtman@frontlinemedcom.com
SOURCE: Winn A et al., JAMA Oncol. 2018 Feb 22. doi: 10.1001/jamaoncol.2017.5544.
FROM JAMA ONCOLOGY
Key clinical point:
Major finding: Total reimbursement during the 6-month treatment episode was lower in offices ($43,700) than in hospital outpatient departments ($84,660).
Study details: An examination of claims data from 283,502 patients who initiated treatment with infused chemotherapy and remained enrolled continuously for 6 months between Jan. 1, 2004, and Dec. 31, 2014.
Disclosures: The researchers reported having no financial conflicts of interest.
Source: Winn A et al., JAMA Oncol. 2018 Feb 22. doi: 10.1001/jamaoncol.2017.5544.
Cyberliability insurance: Should you purchase a policy?
As hackers become more sophisticated, these .
In 2017, there were at least 477 publicly reported health data breaches in the United States, affecting some 5.6 million patients, up from 450 health care breaches in 2016, according to Protenus, a health care cybersecurity vendor that tracks data breaches reported to the U.S. Department of Health & Human Services.
“A breach is very expensive,” said Mr. Cohen, chair for the New York City Bar Association Committee on Medical Malpractice. “You have the fine to the Office for Civil Rights, which can be in the millions of dollars, and you’re going to have to ameliorate the breach, which can be hundreds of dollars per person, let alone deal with lawsuits from the patients.”
Cyberliability: What’s the risk?
Cyberliability refers to legal dangers arising from data breaches, privacy law violations, and ransomware/cyberextortion threats, as well as data loss and business interruption from computer system failures.
Of the 477 breaches in 2017 analyzed by Protenus, 37% were from hacking, 37% resulted from insider incidents, and 16% stemmed from data loss or theft. About 10% of cases resulted from unknown reasons, according to the report.
Data breaches caused by hackers and malware attacks are rising in the health care sector, said Katherine Keefe, global head of breach response services for Beazley, a national cyberliability insurer and risk management company. Beazley handled 2,615 data breaches in 2017, more than half of which were health care–related, Ms. Keefe said in an interview. The top three causes of health care breaches reported to Beazley in 2017 were accidental disclosure, hack or malware, and insider incidents, according to a recent report from that company
“We see an awful lot of that,” Ms. Keefe said. “There’s been a real surge in successful phishing emails and social engineering that enables criminals to identify medical practice leaders. It’s not hard to dress up an email to look like it’s coming from a specific individual. There are all kinds of increasingly sophisticated tactics to trick people into letting criminals into their systems or tricking people into forwarding money or valuable information.”
Hackers frequently use phishing emails to get employees to download a payload, the portion of malware that performs malicious actions, Mr. Cohen added. Once downloaded, payloads can do significant damage to a medical practice.
“Once you get hit with these payloads, not only can they start pulling information out of the computer system, they can also start doing things, such as turning on laptop cameras, reading emails, listening in on computer microphones,” he said. “All they need is one employee to click.”
Considering cybercoverage
To protect themselves from potential breach expenses, more medical practices are purchasing cyberliability insurance policies. A 2017 survey of 270 insurance brokers and 125 underwriters found that health care has more first-time buyers of stand-alone cyberliability insurance than does any other industry.
However, Mr. Cohen advises that practices should do their research before buying and be aware of the different types of policies, coverage limits, and insurance options.
“Be careful about what it covers,” he said. “Are they going to pay for all the amelioration for all the patients affected? Some policies will cover ‘repairing and disinfecting the system,’ but they will not likely cover all the [Office for Civil Rights] fines.”
The Doctors Company, a national medical liability insurer, provides $50,000 in cybersecurity coverage to all its insured physician members and the option to increase coverage by $1 million in additional protection, according to Crystal Brown, senior vice president of underwriting for the Doctors Company. The coverage protects against regulatory and liability claims arising from theft, loss, or accidental transmission of patient or financial information as well as the cost of data recovery. Another policy offered protects against claims arising from administrative actions pertaining to utilization, licensing, credentialing, and misconduct.
Meanwhile, national medical liability insurer ProAssurance offers health providers a basic cyberliability coverage endorsement in most states on its medical professional liability policy. The insurer also has a branded cyberprogram that allows clients to buy additional and broader coverage at a discounted premium.
“In today’s electronic environment, we are hearing about breaches occurring at both small and large health care practices,” said Melanie Tullos, vice president for ProAssurance. “Small physician practices are just as vulnerable, if not more so, to a cyberbreach and should take the necessary steps to protect patient data against an attack at all measures, including, but not limited to, purchasing cyberliability coverage.
The price of cyberliability insurance varies by risk and other factors, Ms. Tullos said. Generally, the cost of a $1 million cyberliability policy for a single physician practice is less than $1,000, whereas a group of 10 physicians can pay up to $8,000-$9,000, she said in an interview.
Beazley offers policies that cover the expenses and services associated with investigating whether a data breach has occurred, responding to breaches, and liability that may arise from the breach, said Ms. Keefe, of Beazley, which works with companies such as the Doctors Company to provide coverage and also works with state-run malpractice programs to offer a cyberliability component for a small, additional premium, she said.
Ms. Keefe stressed that cyberliability coverage can ensure that physician practices don’t run up a hefty bill in the event of a data breach by paying for separate specialists and damage control.
“One of the reasons doctors should have cyberliability coverage are the costs associated with figuring out what to do if patient records are lost or stolen,” she said. “The cost of hiring a lawyer, hiring a forensics investigator to assess the situation, the cost of notifying the patients, and taking all the steps required by HIPAA can really add up. Most practices don’t have those costs built into their annual budgets. A cyberpolicy acts as a buffer against those expenses.”
Manage risk before a breach
Of course, there is plenty that practices can do to prevent – and protect themselves from – a health data breach before it happens. Providing employee awareness training is an important step, said Craig Musgrave, chief information officer of the Doctors Company. Institute a training program for staff at all levels and go over the basics, such as refraining from opening emails from senders they don’t know, Mr. Musgrave wrote in a recent column. Updating all software regularly and backing up data is also essential. And Mr. Musgrave emphasizes the importance of “whitelisting.”
“Health care systems are fragmented in their management of systems and data,” Mr. Musgrave wrote in his column. “Their ability to patch legacy systems and employ cybersecurity staff varies enormously. Therefore, application whitelisting is essential. Rather than blacklisting known malicious software, an application whitelist prevents the launching of any executable program (known or unknown) that does not have explicit authorization. This, in combination with strong firewalls and network segmentation tools like micro-segmentation, provides stronger security.”
In addition, consider implementing data security policies and incident response protocols as well as employee training on securing patient data, ProAssurance’s Ms. Tullos said.
“A breach can also occur within a third-party vendors system and infiltrate the physician’s records, so it is important to discuss cybersecurity with those vendors and all parties should purchase cyberliability insurance,” she said.

Michael E. Nelson, MD, FCCP, comments: Being old enough to remember a paper chart and scheduling book, I can't help but marvel at the how the electronic health record (EHR) has fallen short of its expectations and added to the cost of medical care. Well, let's add cybersecurity insurance to the cost of doing business. While I love the ability to look at a chest x-ray or CT without a viewbox, I can't think of many other things that the EHR has done to make me a more efficient physician. It has, however, spawned many cottage industries that provide "must have" services with their attendant fees. The ever-increasing regulatory and administrative burdens and costs placed on physicians' practices is making it impossible for smaller practices to remain financially viable, leaving smaller communities without medical services. I don't think this was the intent when we decided to "modernize" medicine. It makes me want to go back to those Halcyon days of the paper chart - try phishing one of those, you hackers.
Michael E. Nelson, MD, FCCP, comments: Being old enough to remember a paper chart and scheduling book, I can't help but marvel at the how the electronic health record (EHR) has fallen short of its expectations and added to the cost of medical care. Well, let's add cybersecurity insurance to the cost of doing business. While I love the ability to look at a chest x-ray or CT without a viewbox, I can't think of many other things that the EHR has done to make me a more efficient physician. It has, however, spawned many cottage industries that provide "must have" services with their attendant fees. The ever-increasing regulatory and administrative burdens and costs placed on physicians' practices is making it impossible for smaller practices to remain financially viable, leaving smaller communities without medical services. I don't think this was the intent when we decided to "modernize" medicine. It makes me want to go back to those Halcyon days of the paper chart - try phishing one of those, you hackers.
Michael E. Nelson, MD, FCCP, comments: Being old enough to remember a paper chart and scheduling book, I can't help but marvel at the how the electronic health record (EHR) has fallen short of its expectations and added to the cost of medical care. Well, let's add cybersecurity insurance to the cost of doing business. While I love the ability to look at a chest x-ray or CT without a viewbox, I can't think of many other things that the EHR has done to make me a more efficient physician. It has, however, spawned many cottage industries that provide "must have" services with their attendant fees. The ever-increasing regulatory and administrative burdens and costs placed on physicians' practices is making it impossible for smaller practices to remain financially viable, leaving smaller communities without medical services. I don't think this was the intent when we decided to "modernize" medicine. It makes me want to go back to those Halcyon days of the paper chart - try phishing one of those, you hackers.
As hackers become more sophisticated, these .
In 2017, there were at least 477 publicly reported health data breaches in the United States, affecting some 5.6 million patients, up from 450 health care breaches in 2016, according to Protenus, a health care cybersecurity vendor that tracks data breaches reported to the U.S. Department of Health & Human Services.
“A breach is very expensive,” said Mr. Cohen, chair for the New York City Bar Association Committee on Medical Malpractice. “You have the fine to the Office for Civil Rights, which can be in the millions of dollars, and you’re going to have to ameliorate the breach, which can be hundreds of dollars per person, let alone deal with lawsuits from the patients.”
Cyberliability: What’s the risk?
Cyberliability refers to legal dangers arising from data breaches, privacy law violations, and ransomware/cyberextortion threats, as well as data loss and business interruption from computer system failures.
Of the 477 breaches in 2017 analyzed by Protenus, 37% were from hacking, 37% resulted from insider incidents, and 16% stemmed from data loss or theft. About 10% of cases resulted from unknown reasons, according to the report.
Data breaches caused by hackers and malware attacks are rising in the health care sector, said Katherine Keefe, global head of breach response services for Beazley, a national cyberliability insurer and risk management company. Beazley handled 2,615 data breaches in 2017, more than half of which were health care–related, Ms. Keefe said in an interview. The top three causes of health care breaches reported to Beazley in 2017 were accidental disclosure, hack or malware, and insider incidents, according to a recent report from that company
“We see an awful lot of that,” Ms. Keefe said. “There’s been a real surge in successful phishing emails and social engineering that enables criminals to identify medical practice leaders. It’s not hard to dress up an email to look like it’s coming from a specific individual. There are all kinds of increasingly sophisticated tactics to trick people into letting criminals into their systems or tricking people into forwarding money or valuable information.”
Hackers frequently use phishing emails to get employees to download a payload, the portion of malware that performs malicious actions, Mr. Cohen added. Once downloaded, payloads can do significant damage to a medical practice.
“Once you get hit with these payloads, not only can they start pulling information out of the computer system, they can also start doing things, such as turning on laptop cameras, reading emails, listening in on computer microphones,” he said. “All they need is one employee to click.”
Considering cybercoverage
To protect themselves from potential breach expenses, more medical practices are purchasing cyberliability insurance policies. A 2017 survey of 270 insurance brokers and 125 underwriters found that health care has more first-time buyers of stand-alone cyberliability insurance than does any other industry.
However, Mr. Cohen advises that practices should do their research before buying and be aware of the different types of policies, coverage limits, and insurance options.
“Be careful about what it covers,” he said. “Are they going to pay for all the amelioration for all the patients affected? Some policies will cover ‘repairing and disinfecting the system,’ but they will not likely cover all the [Office for Civil Rights] fines.”
The Doctors Company, a national medical liability insurer, provides $50,000 in cybersecurity coverage to all its insured physician members and the option to increase coverage by $1 million in additional protection, according to Crystal Brown, senior vice president of underwriting for the Doctors Company. The coverage protects against regulatory and liability claims arising from theft, loss, or accidental transmission of patient or financial information as well as the cost of data recovery. Another policy offered protects against claims arising from administrative actions pertaining to utilization, licensing, credentialing, and misconduct.
Meanwhile, national medical liability insurer ProAssurance offers health providers a basic cyberliability coverage endorsement in most states on its medical professional liability policy. The insurer also has a branded cyberprogram that allows clients to buy additional and broader coverage at a discounted premium.
“In today’s electronic environment, we are hearing about breaches occurring at both small and large health care practices,” said Melanie Tullos, vice president for ProAssurance. “Small physician practices are just as vulnerable, if not more so, to a cyberbreach and should take the necessary steps to protect patient data against an attack at all measures, including, but not limited to, purchasing cyberliability coverage.
The price of cyberliability insurance varies by risk and other factors, Ms. Tullos said. Generally, the cost of a $1 million cyberliability policy for a single physician practice is less than $1,000, whereas a group of 10 physicians can pay up to $8,000-$9,000, she said in an interview.
Beazley offers policies that cover the expenses and services associated with investigating whether a data breach has occurred, responding to breaches, and liability that may arise from the breach, said Ms. Keefe, of Beazley, which works with companies such as the Doctors Company to provide coverage and also works with state-run malpractice programs to offer a cyberliability component for a small, additional premium, she said.
Ms. Keefe stressed that cyberliability coverage can ensure that physician practices don’t run up a hefty bill in the event of a data breach by paying for separate specialists and damage control.
“One of the reasons doctors should have cyberliability coverage are the costs associated with figuring out what to do if patient records are lost or stolen,” she said. “The cost of hiring a lawyer, hiring a forensics investigator to assess the situation, the cost of notifying the patients, and taking all the steps required by HIPAA can really add up. Most practices don’t have those costs built into their annual budgets. A cyberpolicy acts as a buffer against those expenses.”
Manage risk before a breach
Of course, there is plenty that practices can do to prevent – and protect themselves from – a health data breach before it happens. Providing employee awareness training is an important step, said Craig Musgrave, chief information officer of the Doctors Company. Institute a training program for staff at all levels and go over the basics, such as refraining from opening emails from senders they don’t know, Mr. Musgrave wrote in a recent column. Updating all software regularly and backing up data is also essential. And Mr. Musgrave emphasizes the importance of “whitelisting.”
“Health care systems are fragmented in their management of systems and data,” Mr. Musgrave wrote in his column. “Their ability to patch legacy systems and employ cybersecurity staff varies enormously. Therefore, application whitelisting is essential. Rather than blacklisting known malicious software, an application whitelist prevents the launching of any executable program (known or unknown) that does not have explicit authorization. This, in combination with strong firewalls and network segmentation tools like micro-segmentation, provides stronger security.”
In addition, consider implementing data security policies and incident response protocols as well as employee training on securing patient data, ProAssurance’s Ms. Tullos said.
“A breach can also occur within a third-party vendors system and infiltrate the physician’s records, so it is important to discuss cybersecurity with those vendors and all parties should purchase cyberliability insurance,” she said.
As hackers become more sophisticated, these .
In 2017, there were at least 477 publicly reported health data breaches in the United States, affecting some 5.6 million patients, up from 450 health care breaches in 2016, according to Protenus, a health care cybersecurity vendor that tracks data breaches reported to the U.S. Department of Health & Human Services.
“A breach is very expensive,” said Mr. Cohen, chair for the New York City Bar Association Committee on Medical Malpractice. “You have the fine to the Office for Civil Rights, which can be in the millions of dollars, and you’re going to have to ameliorate the breach, which can be hundreds of dollars per person, let alone deal with lawsuits from the patients.”
Cyberliability: What’s the risk?
Cyberliability refers to legal dangers arising from data breaches, privacy law violations, and ransomware/cyberextortion threats, as well as data loss and business interruption from computer system failures.
Of the 477 breaches in 2017 analyzed by Protenus, 37% were from hacking, 37% resulted from insider incidents, and 16% stemmed from data loss or theft. About 10% of cases resulted from unknown reasons, according to the report.
Data breaches caused by hackers and malware attacks are rising in the health care sector, said Katherine Keefe, global head of breach response services for Beazley, a national cyberliability insurer and risk management company. Beazley handled 2,615 data breaches in 2017, more than half of which were health care–related, Ms. Keefe said in an interview. The top three causes of health care breaches reported to Beazley in 2017 were accidental disclosure, hack or malware, and insider incidents, according to a recent report from that company
“We see an awful lot of that,” Ms. Keefe said. “There’s been a real surge in successful phishing emails and social engineering that enables criminals to identify medical practice leaders. It’s not hard to dress up an email to look like it’s coming from a specific individual. There are all kinds of increasingly sophisticated tactics to trick people into letting criminals into their systems or tricking people into forwarding money or valuable information.”
Hackers frequently use phishing emails to get employees to download a payload, the portion of malware that performs malicious actions, Mr. Cohen added. Once downloaded, payloads can do significant damage to a medical practice.
“Once you get hit with these payloads, not only can they start pulling information out of the computer system, they can also start doing things, such as turning on laptop cameras, reading emails, listening in on computer microphones,” he said. “All they need is one employee to click.”
Considering cybercoverage
To protect themselves from potential breach expenses, more medical practices are purchasing cyberliability insurance policies. A 2017 survey of 270 insurance brokers and 125 underwriters found that health care has more first-time buyers of stand-alone cyberliability insurance than does any other industry.
However, Mr. Cohen advises that practices should do their research before buying and be aware of the different types of policies, coverage limits, and insurance options.
“Be careful about what it covers,” he said. “Are they going to pay for all the amelioration for all the patients affected? Some policies will cover ‘repairing and disinfecting the system,’ but they will not likely cover all the [Office for Civil Rights] fines.”
The Doctors Company, a national medical liability insurer, provides $50,000 in cybersecurity coverage to all its insured physician members and the option to increase coverage by $1 million in additional protection, according to Crystal Brown, senior vice president of underwriting for the Doctors Company. The coverage protects against regulatory and liability claims arising from theft, loss, or accidental transmission of patient or financial information as well as the cost of data recovery. Another policy offered protects against claims arising from administrative actions pertaining to utilization, licensing, credentialing, and misconduct.
Meanwhile, national medical liability insurer ProAssurance offers health providers a basic cyberliability coverage endorsement in most states on its medical professional liability policy. The insurer also has a branded cyberprogram that allows clients to buy additional and broader coverage at a discounted premium.
“In today’s electronic environment, we are hearing about breaches occurring at both small and large health care practices,” said Melanie Tullos, vice president for ProAssurance. “Small physician practices are just as vulnerable, if not more so, to a cyberbreach and should take the necessary steps to protect patient data against an attack at all measures, including, but not limited to, purchasing cyberliability coverage.
The price of cyberliability insurance varies by risk and other factors, Ms. Tullos said. Generally, the cost of a $1 million cyberliability policy for a single physician practice is less than $1,000, whereas a group of 10 physicians can pay up to $8,000-$9,000, she said in an interview.
Beazley offers policies that cover the expenses and services associated with investigating whether a data breach has occurred, responding to breaches, and liability that may arise from the breach, said Ms. Keefe, of Beazley, which works with companies such as the Doctors Company to provide coverage and also works with state-run malpractice programs to offer a cyberliability component for a small, additional premium, she said.
Ms. Keefe stressed that cyberliability coverage can ensure that physician practices don’t run up a hefty bill in the event of a data breach by paying for separate specialists and damage control.
“One of the reasons doctors should have cyberliability coverage are the costs associated with figuring out what to do if patient records are lost or stolen,” she said. “The cost of hiring a lawyer, hiring a forensics investigator to assess the situation, the cost of notifying the patients, and taking all the steps required by HIPAA can really add up. Most practices don’t have those costs built into their annual budgets. A cyberpolicy acts as a buffer against those expenses.”
Manage risk before a breach
Of course, there is plenty that practices can do to prevent – and protect themselves from – a health data breach before it happens. Providing employee awareness training is an important step, said Craig Musgrave, chief information officer of the Doctors Company. Institute a training program for staff at all levels and go over the basics, such as refraining from opening emails from senders they don’t know, Mr. Musgrave wrote in a recent column. Updating all software regularly and backing up data is also essential. And Mr. Musgrave emphasizes the importance of “whitelisting.”
“Health care systems are fragmented in their management of systems and data,” Mr. Musgrave wrote in his column. “Their ability to patch legacy systems and employ cybersecurity staff varies enormously. Therefore, application whitelisting is essential. Rather than blacklisting known malicious software, an application whitelist prevents the launching of any executable program (known or unknown) that does not have explicit authorization. This, in combination with strong firewalls and network segmentation tools like micro-segmentation, provides stronger security.”
In addition, consider implementing data security policies and incident response protocols as well as employee training on securing patient data, ProAssurance’s Ms. Tullos said.
“A breach can also occur within a third-party vendors system and infiltrate the physician’s records, so it is important to discuss cybersecurity with those vendors and all parties should purchase cyberliability insurance,” she said.
Treatment of Melasma Using Tranexamic Acid: What’s Known and What’s Next
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Resident Pearl
- Oral tranexamic acid is an antifibrinolytic agent that can be used off-label for the treatment of melasma.

ACIP unanimously recommends HEPLISAV-B
At a meeting of the Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices, members unanimously voted to include HEPLISAV-B on the ACIP list of recommended products to vaccinate adults against hepatitis B.
“I think this is a huge advance, and a step forward “ said David S. Stephens, MD, of Emory University, Atlanta, who is a voting member of ACIP.![]()
According to Sarah Schillie, MD, of ACIP’s Hepatitis Work Group, the reduction from three doses to two also will improve vaccine series completion rates, providing more effective protection. This could be very important for health care professionals, with only about 60% of treated individuals fulfilling the three doses necessary for complete HBV protection.
Although fewer doses are needed with HEPLISAV-B, it displays similar immunogenicity to similar vaccines (90.0%-100% vs. 70.5%-90.2%). It is also more effective, compared with similar vaccines in those with type II diabetes (90.0% vs. 65.1%) and chronic kidney disease (89.9% vs. 81.1%).
HEPLISAV-B uses an adjuvant, but it appears to be safe and well tolerated. The rate of mild (45.6% vs. 45.7%) and serious (5.4% vs. 6.3%) reactions were similar among HEPLISAV-B and comparable vaccines, although cardiovascular events were more common with this vaccine than with others (0.27% vs. 0.14%).
Dr. Stephens, who supported the recommendation of HEPLISAV-B, voiced reservations about these findings. “I am concerned about the myocardial infarction signal and the use of this new adjuvant and certainly urge us to look at the postmarketing data carefully.”
While the reported incidence rate of acute HBV cases consistently fell during 2000-2015, it began to rise again at the end of 2015. This is linked with concomitant rise in injection drug use, which also is a risk factor in transmitting HBV. Over the same period, the incidence of HBV was highest in people aged 30-49 years. With these factors to consider, the vote by ACIP for HEPLISAV-B as a recommended vaccine is timely and may help reduce HBV infections in adults.
At a meeting of the Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices, members unanimously voted to include HEPLISAV-B on the ACIP list of recommended products to vaccinate adults against hepatitis B.
“I think this is a huge advance, and a step forward “ said David S. Stephens, MD, of Emory University, Atlanta, who is a voting member of ACIP.![]()
According to Sarah Schillie, MD, of ACIP’s Hepatitis Work Group, the reduction from three doses to two also will improve vaccine series completion rates, providing more effective protection. This could be very important for health care professionals, with only about 60% of treated individuals fulfilling the three doses necessary for complete HBV protection.
Although fewer doses are needed with HEPLISAV-B, it displays similar immunogenicity to similar vaccines (90.0%-100% vs. 70.5%-90.2%). It is also more effective, compared with similar vaccines in those with type II diabetes (90.0% vs. 65.1%) and chronic kidney disease (89.9% vs. 81.1%).
HEPLISAV-B uses an adjuvant, but it appears to be safe and well tolerated. The rate of mild (45.6% vs. 45.7%) and serious (5.4% vs. 6.3%) reactions were similar among HEPLISAV-B and comparable vaccines, although cardiovascular events were more common with this vaccine than with others (0.27% vs. 0.14%).
Dr. Stephens, who supported the recommendation of HEPLISAV-B, voiced reservations about these findings. “I am concerned about the myocardial infarction signal and the use of this new adjuvant and certainly urge us to look at the postmarketing data carefully.”
While the reported incidence rate of acute HBV cases consistently fell during 2000-2015, it began to rise again at the end of 2015. This is linked with concomitant rise in injection drug use, which also is a risk factor in transmitting HBV. Over the same period, the incidence of HBV was highest in people aged 30-49 years. With these factors to consider, the vote by ACIP for HEPLISAV-B as a recommended vaccine is timely and may help reduce HBV infections in adults.
At a meeting of the Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices, members unanimously voted to include HEPLISAV-B on the ACIP list of recommended products to vaccinate adults against hepatitis B.
“I think this is a huge advance, and a step forward “ said David S. Stephens, MD, of Emory University, Atlanta, who is a voting member of ACIP.![]()
According to Sarah Schillie, MD, of ACIP’s Hepatitis Work Group, the reduction from three doses to two also will improve vaccine series completion rates, providing more effective protection. This could be very important for health care professionals, with only about 60% of treated individuals fulfilling the three doses necessary for complete HBV protection.
Although fewer doses are needed with HEPLISAV-B, it displays similar immunogenicity to similar vaccines (90.0%-100% vs. 70.5%-90.2%). It is also more effective, compared with similar vaccines in those with type II diabetes (90.0% vs. 65.1%) and chronic kidney disease (89.9% vs. 81.1%).
HEPLISAV-B uses an adjuvant, but it appears to be safe and well tolerated. The rate of mild (45.6% vs. 45.7%) and serious (5.4% vs. 6.3%) reactions were similar among HEPLISAV-B and comparable vaccines, although cardiovascular events were more common with this vaccine than with others (0.27% vs. 0.14%).
Dr. Stephens, who supported the recommendation of HEPLISAV-B, voiced reservations about these findings. “I am concerned about the myocardial infarction signal and the use of this new adjuvant and certainly urge us to look at the postmarketing data carefully.”
While the reported incidence rate of acute HBV cases consistently fell during 2000-2015, it began to rise again at the end of 2015. This is linked with concomitant rise in injection drug use, which also is a risk factor in transmitting HBV. Over the same period, the incidence of HBV was highest in people aged 30-49 years. With these factors to consider, the vote by ACIP for HEPLISAV-B as a recommended vaccine is timely and may help reduce HBV infections in adults.
REPORTING FROM AN ACIP MEETING
MDedge Daily News: The human cost of depression’s wonder drug
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Does depression’s wonder drug have a long-term cost? CPAP compliance may prevent return trips to the hospital, stem cells deliver durable results in stroke, and short-term health plans may be poised for a comeback.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Does depression’s wonder drug have a long-term cost? CPAP compliance may prevent return trips to the hospital, stem cells deliver durable results in stroke, and short-term health plans may be poised for a comeback.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Does depression’s wonder drug have a long-term cost? CPAP compliance may prevent return trips to the hospital, stem cells deliver durable results in stroke, and short-term health plans may be poised for a comeback.
Listen to the MDedge Daily News podcast for all the details on today’s top news.

‘Antagonistic’ Markers for Cancer Prognosis
ATP-dependent chromatin remodeling is fundamental to DNA metabolism, and SMARCA4 (or BRG1) is the most frequently mutated chromatin remodeling ATPase in cancer.
SMARCA4 is often mutated or silenced in tumors, suggesting a role as tumor suppressor, say researchers from Universidad de Sevilla-Universidad Pablo de Olavide in Spain. However, they note, recent reports show SMARCA4 also is required for tumor cell growth. So they performed a meta-analysis using gene expression, prognosis, and clinicopathologic data to clarify the role of SMARCA4 in cancer.
The researchers concluded that expression of SMARCA4 and another ATPase, SMARCA2, have a “high prognostic value.” Although the SMARCA4 gene is mostly overexpressed in tumors, the researchers say, SMARCA2 is almost invariably downregulated.
The data demonstrate that levels of SMARCA4 and SMARCA2 expression correlate with opposite prognosis in several types of tumors. The SMARCA4 upregulation is associated with a poor prognosis for breast and ovarian cancer, lung adenocarcinoma, liposarcoma, and uveal melanoma, for instance. High expression of SMARCA4 can be used as a prognosis marker for those types of tumors, the researchers say. Exactly how the outcomes are linked to SMARCA4 is not yet clear, but the researchers point to research that found SMARCA4 promotes breast cancer by reprogramming lipid synthesis and is required for maintaining repopulation of hematopoietic stem cells in leukemia. (SMARCA4 is highly expressed in stem cells.)
By contrast, high levels of SMARCA2 expression were associated with a good prognosis in breast and ovarian cancer, lung adenocarcinoma, and liposarcoma.
The researchers say that SMARCA4 expression is mostly associated to cell types that constantly undergo proliferation or self-renewal and SMARCA2 is absent from stem cells and inversely correlated with proliferation in several types of cells, suggesting the “attractive possibility” that they contribute to a type of equilibrium in proliferating-undifferentiated vs quiescent-differentiated conditions. That “antagonistic” behavior, the researchers suggest, should be taken into account when designing specific drugs that target one but not the other ATPase.
Source:
Guerrero-Martínez JA, Reyes JC. Scientific Reports. 2018;8:2043.
doi: 10.1038/s41598-018-20217-3.
ATP-dependent chromatin remodeling is fundamental to DNA metabolism, and SMARCA4 (or BRG1) is the most frequently mutated chromatin remodeling ATPase in cancer.
SMARCA4 is often mutated or silenced in tumors, suggesting a role as tumor suppressor, say researchers from Universidad de Sevilla-Universidad Pablo de Olavide in Spain. However, they note, recent reports show SMARCA4 also is required for tumor cell growth. So they performed a meta-analysis using gene expression, prognosis, and clinicopathologic data to clarify the role of SMARCA4 in cancer.
The researchers concluded that expression of SMARCA4 and another ATPase, SMARCA2, have a “high prognostic value.” Although the SMARCA4 gene is mostly overexpressed in tumors, the researchers say, SMARCA2 is almost invariably downregulated.
The data demonstrate that levels of SMARCA4 and SMARCA2 expression correlate with opposite prognosis in several types of tumors. The SMARCA4 upregulation is associated with a poor prognosis for breast and ovarian cancer, lung adenocarcinoma, liposarcoma, and uveal melanoma, for instance. High expression of SMARCA4 can be used as a prognosis marker for those types of tumors, the researchers say. Exactly how the outcomes are linked to SMARCA4 is not yet clear, but the researchers point to research that found SMARCA4 promotes breast cancer by reprogramming lipid synthesis and is required for maintaining repopulation of hematopoietic stem cells in leukemia. (SMARCA4 is highly expressed in stem cells.)
By contrast, high levels of SMARCA2 expression were associated with a good prognosis in breast and ovarian cancer, lung adenocarcinoma, and liposarcoma.
The researchers say that SMARCA4 expression is mostly associated to cell types that constantly undergo proliferation or self-renewal and SMARCA2 is absent from stem cells and inversely correlated with proliferation in several types of cells, suggesting the “attractive possibility” that they contribute to a type of equilibrium in proliferating-undifferentiated vs quiescent-differentiated conditions. That “antagonistic” behavior, the researchers suggest, should be taken into account when designing specific drugs that target one but not the other ATPase.
Source:
Guerrero-Martínez JA, Reyes JC. Scientific Reports. 2018;8:2043.
doi: 10.1038/s41598-018-20217-3.
ATP-dependent chromatin remodeling is fundamental to DNA metabolism, and SMARCA4 (or BRG1) is the most frequently mutated chromatin remodeling ATPase in cancer.
SMARCA4 is often mutated or silenced in tumors, suggesting a role as tumor suppressor, say researchers from Universidad de Sevilla-Universidad Pablo de Olavide in Spain. However, they note, recent reports show SMARCA4 also is required for tumor cell growth. So they performed a meta-analysis using gene expression, prognosis, and clinicopathologic data to clarify the role of SMARCA4 in cancer.
The researchers concluded that expression of SMARCA4 and another ATPase, SMARCA2, have a “high prognostic value.” Although the SMARCA4 gene is mostly overexpressed in tumors, the researchers say, SMARCA2 is almost invariably downregulated.
The data demonstrate that levels of SMARCA4 and SMARCA2 expression correlate with opposite prognosis in several types of tumors. The SMARCA4 upregulation is associated with a poor prognosis for breast and ovarian cancer, lung adenocarcinoma, liposarcoma, and uveal melanoma, for instance. High expression of SMARCA4 can be used as a prognosis marker for those types of tumors, the researchers say. Exactly how the outcomes are linked to SMARCA4 is not yet clear, but the researchers point to research that found SMARCA4 promotes breast cancer by reprogramming lipid synthesis and is required for maintaining repopulation of hematopoietic stem cells in leukemia. (SMARCA4 is highly expressed in stem cells.)
By contrast, high levels of SMARCA2 expression were associated with a good prognosis in breast and ovarian cancer, lung adenocarcinoma, and liposarcoma.
The researchers say that SMARCA4 expression is mostly associated to cell types that constantly undergo proliferation or self-renewal and SMARCA2 is absent from stem cells and inversely correlated with proliferation in several types of cells, suggesting the “attractive possibility” that they contribute to a type of equilibrium in proliferating-undifferentiated vs quiescent-differentiated conditions. That “antagonistic” behavior, the researchers suggest, should be taken into account when designing specific drugs that target one but not the other ATPase.
Source:
Guerrero-Martínez JA, Reyes JC. Scientific Reports. 2018;8:2043.
doi: 10.1038/s41598-018-20217-3.
Shock Treatment When It’s Needed Most
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
Exercise doesn’t offset VTE risk from TV viewing

Getting the recommended amount of physical activity does not eliminate the increased risk of venous thromboembolism (VTE) associated with frequent TV viewing, according to research published in the Journal of Thrombosis and Thrombolysis.
In a study of more than 15,000 Americans, people who reported watching TV “very often” had nearly twice the risk of VTE as people who said they “never or seldom” watched TV.
People who watched TV very often had an increased VTE risk even when researchers adjusted for physical activity levels, smoking status, body mass index, and other factors.
“These results suggest that even individuals who regularly engage in physical activity should not ignore the potential harms of prolonged sedentary behaviors such as TV viewing,” said study author Yasuhiko Kubota, of the University of Minnesota in Minneapolis.
“Avoiding frequent TV viewing, increasing physical activity, and controlling body weight might be beneficial to prevent VTE.”
Kubota and his colleagues came to these conclusions after analyzing data from the Atherosclerosis Risk in Communities (ARIC) Study, an ongoing, population-based, prospective study conducted in the US.
The researchers evaluated 15,158 Americans who were 45 to 64 years of age when ARIC started in 1987.
Study subjects were initially asked about their health status, whether they exercised or smoked, and whether they were overweight or not. Over the years, ARIC team members have been in regular contact with subjects to ask about any hospital treatment they might have received.
When subjects were asked about their TV viewing habits, most said they watched TV “sometimes” (n=7094). Fewer subjects said they watched TV “often” (n=4023), “never or seldom” (n=2815), and “very often” (n=1226).
Results
Via hospital records and imaging tests, Kubota and his colleagues identified 691 cases of VTE in the study cohort.
In assessing the risk of VTE, the researchers compared the “never or seldom” TV viewing group to the other viewing groups.
In a model adjusted for age, sex, and race, “sometimes” viewers had a hazard ratio (HR) of VTE of 1.17, the “often” group had an HR of 1.31, and the “very often” group had an HR of 1.88.
In a second model, the researchers adjusted for the aforementioned factors as well as smoking status, leisure-time physical activity, eGFR, and prevalent cardiovascular disease.
In this model, “sometimes” viewers had an HR of VTE of 1.16, the “often” group had an HR of 1.26, and the “very often” group had an HR of 1.71.
In a third model, Kubota and his colleagues adjusted for all of the aforementioned factors as well as body mass index.
In this model, “sometimes” viewers had an HR of VTE of 1.13, the “often” group had an HR of 1.20, and the “very often” group had an HR of 1.53.
The researchers noted that subjects who met the American Heart Association’s recommended level of physical activity but watched TV “very often” had an HR of VTE of 1.80. Subjects with a poor physical activity level who watched TV “very often” had an HR of 2.07.
Kubota and his colleagues also found that obese subjects had an increased risk of VTE, and TV viewing appeared to add to that risk.
Obese subjects who watched TV “very often” had an HR of VTE of 3.70. For obese subjects who “never or seldom” watched TV, the HR was 1.90.
Getting the recommended amount of physical activity does not eliminate the increased risk of venous thromboembolism (VTE) associated with frequent TV viewing, according to research published in the Journal of Thrombosis and Thrombolysis.
In a study of more than 15,000 Americans, people who reported watching TV “very often” had nearly twice the risk of VTE as people who said they “never or seldom” watched TV.
People who watched TV very often had an increased VTE risk even when researchers adjusted for physical activity levels, smoking status, body mass index, and other factors.
“These results suggest that even individuals who regularly engage in physical activity should not ignore the potential harms of prolonged sedentary behaviors such as TV viewing,” said study author Yasuhiko Kubota, of the University of Minnesota in Minneapolis.
“Avoiding frequent TV viewing, increasing physical activity, and controlling body weight might be beneficial to prevent VTE.”
Kubota and his colleagues came to these conclusions after analyzing data from the Atherosclerosis Risk in Communities (ARIC) Study, an ongoing, population-based, prospective study conducted in the US.
The researchers evaluated 15,158 Americans who were 45 to 64 years of age when ARIC started in 1987.
Study subjects were initially asked about their health status, whether they exercised or smoked, and whether they were overweight or not. Over the years, ARIC team members have been in regular contact with subjects to ask about any hospital treatment they might have received.
When subjects were asked about their TV viewing habits, most said they watched TV “sometimes” (n=7094). Fewer subjects said they watched TV “often” (n=4023), “never or seldom” (n=2815), and “very often” (n=1226).
Results
Via hospital records and imaging tests, Kubota and his colleagues identified 691 cases of VTE in the study cohort.
In assessing the risk of VTE, the researchers compared the “never or seldom” TV viewing group to the other viewing groups.
In a model adjusted for age, sex, and race, “sometimes” viewers had a hazard ratio (HR) of VTE of 1.17, the “often” group had an HR of 1.31, and the “very often” group had an HR of 1.88.
In a second model, the researchers adjusted for the aforementioned factors as well as smoking status, leisure-time physical activity, eGFR, and prevalent cardiovascular disease.
In this model, “sometimes” viewers had an HR of VTE of 1.16, the “often” group had an HR of 1.26, and the “very often” group had an HR of 1.71.
In a third model, Kubota and his colleagues adjusted for all of the aforementioned factors as well as body mass index.
In this model, “sometimes” viewers had an HR of VTE of 1.13, the “often” group had an HR of 1.20, and the “very often” group had an HR of 1.53.
The researchers noted that subjects who met the American Heart Association’s recommended level of physical activity but watched TV “very often” had an HR of VTE of 1.80. Subjects with a poor physical activity level who watched TV “very often” had an HR of 2.07.
Kubota and his colleagues also found that obese subjects had an increased risk of VTE, and TV viewing appeared to add to that risk.
Obese subjects who watched TV “very often” had an HR of VTE of 3.70. For obese subjects who “never or seldom” watched TV, the HR was 1.90.
Getting the recommended amount of physical activity does not eliminate the increased risk of venous thromboembolism (VTE) associated with frequent TV viewing, according to research published in the Journal of Thrombosis and Thrombolysis.
In a study of more than 15,000 Americans, people who reported watching TV “very often” had nearly twice the risk of VTE as people who said they “never or seldom” watched TV.
People who watched TV very often had an increased VTE risk even when researchers adjusted for physical activity levels, smoking status, body mass index, and other factors.
“These results suggest that even individuals who regularly engage in physical activity should not ignore the potential harms of prolonged sedentary behaviors such as TV viewing,” said study author Yasuhiko Kubota, of the University of Minnesota in Minneapolis.
“Avoiding frequent TV viewing, increasing physical activity, and controlling body weight might be beneficial to prevent VTE.”
Kubota and his colleagues came to these conclusions after analyzing data from the Atherosclerosis Risk in Communities (ARIC) Study, an ongoing, population-based, prospective study conducted in the US.
The researchers evaluated 15,158 Americans who were 45 to 64 years of age when ARIC started in 1987.
Study subjects were initially asked about their health status, whether they exercised or smoked, and whether they were overweight or not. Over the years, ARIC team members have been in regular contact with subjects to ask about any hospital treatment they might have received.
When subjects were asked about their TV viewing habits, most said they watched TV “sometimes” (n=7094). Fewer subjects said they watched TV “often” (n=4023), “never or seldom” (n=2815), and “very often” (n=1226).
Results
Via hospital records and imaging tests, Kubota and his colleagues identified 691 cases of VTE in the study cohort.
In assessing the risk of VTE, the researchers compared the “never or seldom” TV viewing group to the other viewing groups.
In a model adjusted for age, sex, and race, “sometimes” viewers had a hazard ratio (HR) of VTE of 1.17, the “often” group had an HR of 1.31, and the “very often” group had an HR of 1.88.
In a second model, the researchers adjusted for the aforementioned factors as well as smoking status, leisure-time physical activity, eGFR, and prevalent cardiovascular disease.
In this model, “sometimes” viewers had an HR of VTE of 1.16, the “often” group had an HR of 1.26, and the “very often” group had an HR of 1.71.
In a third model, Kubota and his colleagues adjusted for all of the aforementioned factors as well as body mass index.
In this model, “sometimes” viewers had an HR of VTE of 1.13, the “often” group had an HR of 1.20, and the “very often” group had an HR of 1.53.
The researchers noted that subjects who met the American Heart Association’s recommended level of physical activity but watched TV “very often” had an HR of VTE of 1.80. Subjects with a poor physical activity level who watched TV “very often” had an HR of 2.07.
Kubota and his colleagues also found that obese subjects had an increased risk of VTE, and TV viewing appeared to add to that risk.
Obese subjects who watched TV “very often” had an HR of VTE of 3.70. For obese subjects who “never or seldom” watched TV, the HR was 1.90.